
Submitted:
13 September 2024
Posted:
13 September 2024
You are already at the latest version
Abstract
Background: Mitral regurgitation (MR) is a common valvular disorder linked to high morbidity and mortality. For patients unsuitable for surgery, transcatheter mitral edge-to-edge repair (TEER) with the MitraClip® G4 system offers an alternative. This study aims to evaluate procedural, echocardiographic, functional, and quality of life (QoL) outcomes in patients who underwent TEER with the MitraClip® G4 system, along with possible predictors of New York Heart Associa-tion (NYHA) class I at 30 days and 1 year. Methods: Patients with moderate-to-severe (3+) or se-vere (4+) degenerative MR (DMR) or functional MR (FMR), classified as NYHA class III or IV, who underwent TEER with the MitraClip® G4 system at our center between January 2021 and De-cember 2023 were included. Results: A total of 83 patients [71% FMR, 66% male, median (IQR) age 70 (11) years] underwent TEER, with 100% procedural success. MR ≤2+ was achieved in 100% and 98% of patients at 30 days and 1 year, respectively. NYHA class I or II was achieved in 100% and 96.8% of patients at 30 days and 1 year, respectively. The Kansas City Cardiomyopathy Ques-tionnaire (KCCQ) score improved from 51±20 at baseline to 69±15 at 30 days (p< 0.001) and 70.5±15 at 1 year (p< 0.001). Lower baseline N-terminal pro-brain natriuretic peptide (NT-proBNP) pre-dicted achieving NYHA class I at 30 days (HR: 0.63, 95% CI: 0.41–0.95, p = 0.030), while lower Eu-ropean System for Cardiac Operative Risk Evaluation II (EuroSCORE II) and NT-proBNP pre-dicted it at 1 year [(HR: 0.50, 95% CI: 0.28–0.89, p = 0.019), (HR: 0.67, 95% CI: 0.44–0.99, p = 0.049), respectively]. Conclusions: The MitraClip® G4 system provides significant improvements in MR severity, functional class, and QoL. Lower NT-proBNP and EuroSCORE II were strong predictors of achieving optimal functional status (NYHA class I).
Keywords:
mitral regurgitation
; transcatheter edge-to-edge repair
; MitraClip
; MR severity
; QoL
; NYHA class
1. Introduction
Mitral Regurgitation (MR) stands as the second most common valvular disorder, prevalent in approximately 10% of individuals aged 75 years and above, imposing significant morbidity and mortality burdens [1,2,3,4]. The landscape of MR management has witnessed a paradigm shift with the introduction of transcatheter edge-to-edge repair (TEER) utilizing the MitraClip® system (Abbott Vascular, Santa Clara, CA, USA). While surgical mitral valve repair has historically been the cornerstone for degenerative MR (DMR), TEER has emerged as a promising alternative, particularly for patients previously ineligible for surgical intervention [5].
EVEREST II trial demonstrated promising outcomes in low-risk DMR patients [6], yet with a higher recurrence rate after 4-year results [7]. TEER induction in treating severe functional or secondary mitral regurgitation (FMR) was assessed by the discordant results of the MITRA-FR [8] and COAPT trials [9]. While MITRA-FR failed to demonstrate a significant impact on mortality or heart failure hospitalizations at one year, the COAPT trial illuminated a survival advantage associated with TEER, stimulating ongoing discourse and inquiry into the optimal role of TEER in MR management. Furthermore, EXPAND G4 study [10] evaluated the one-year outcomes of patients treated with the fourth generation MitraClip ® device, concluding to its safety and efficacy over a one-year period, with a significant reduction in the MR severity to ≤1+ in over 90% of the patients. The most recent randomized controlled trial, RESHAPE-HF2, demonstrated that the addition of transcatheter mitral valve repair significantly improved outcomes in patients with moderate-to-severe MR, including reduction in heart failure-related hospitalizations and improvement in quality of life (QoL), compared to medical therapy alone [11].
This dynamic landscape underscores the need for continued research and collaborative efforts to refine patient selection, optimize outcomes, and elucidate the true potential of TEER in addressing the complexities of MR and its sequelae. This study aims to assess the 1-year outcomes in subjects who underwent treatment with the Mitraclip ® G4 system, particularly focusing on its safety and performance in a real-world context.
2. Materials and Methods
This retrospective observational cohort study encompasses data extracted from the medical records of all patients who underwent TEER at our structural heart disease expert center from January 2021 to December 2023. The study received approval from the Institutional Review Board of our center, adhering to the principles outlined in the Declaration of Helsinki.
2.1. Inclusion Criteria
All patients diagnosed with moderate-to-severe (3+) or severe (4+) degenerative MR (DMR) or functional MR (FMR), classified as New York Heart Association (NYHA) class III or IV, and who underwent TEER using the MitraClip® G4 system in the Hybrid Operating Room at Interbalkan Medical Center were included. DMR was defined as MR resulting from a compromised mitral valve, while FMR was characterized as MR stemming from compromised left ventricle or atria while the valve remained anatomically intact. The decision to perform the transcatheter procedure was made by the local Heart Team, guided by the 2021 European Society of Cardiology (ESC) / European Association for Cardio-Thoracic Surgery (EACTS) guidelines [12].
2.2. TEER Procedure
The transcatheter edge-to-edge repair (TEER) procedure was performed under general anesthesia in the Hybrid Operating Room at the Interbalkan Medical Center, utilizing the MitraClip® G4 system (Abbott Vascular, Santa Clara, CA, USA).
Venous access was established via the right femoral vein using a large-bore sheath. A transseptal puncture was performed using a specialized needle to gain access to the left atrium, ensuring an optimal puncture site to facilitate subsequent navigation towards the mitral valve. A steerable guide catheter (SGC) was then advanced into the left atrium under real-time fluoroscopic and transesophageal echocardiographic guidance
Once the left atrium was accessed, the MitraClip Delivery System (CDS) was carefully maneuvered towards the mitral valve through the SGC. Continuous TEE monitoring was employed to assess the orientation and position of the catheter relative to the mitral leaflets. Precise manipulation of the clip delivery system was necessary to align the MitraClip with the target mitral leaflets. The device was positioned at the site of regurgitation, typically at the A2-P2 scallop, which is the most common location for mitral valve prolapse or flail.
After ensuring optimal positioning and alignment, the clip was opened and advanced to grasp both the anterior and posterior mitral leaflets. The clip arms were closed to approximate the leaflets, creating a double orifice and reducing the regurgitant flow. TEE was used extensively throughout this phase to confirm adequate leaflet capture, ensure proper coaptation, and evaluate the immediate reduction in MR. If the reduction in MR was deemed insufficient or if clip positioning was suboptimal, the clip could be repositioned, or additional clips could be deployed as needed.
After successful deployment of the MitraClip, a comprehensive echocardiographic assessment was performed to evaluate the final result. This included checking for residual MR, assessing leaflet mobility, adequate leaflet grasping and confirming that no significant mitral stenosis had been induced. Hemodynamic measurements were repeated to assess the improvement in cardiac function post-procedure.
Following the procedure, patients were transferred to the intensive care unit for close monitoring. Post-procedural TEE was typically performed within 24 hours to confirm the stability of the MitraClip and to reassess MR severity.
2.3. Definition of the Variables
Baseline characteristics including age, sex, estimated glomerular filtration rate (eGFR), European System for Cardiac Operative Risk Evaluation II (EuroSCORE II), cardiopulmonary comorbidities (e.g., prior heart failure hospitalization, atrial fibrillation [AF], prior myocardial infarction [MI], diabetes, chronic obstructive pulmonary disease [COPD]), presence of permanent pacemaker (PPM) or implantable cardioverter defibrillator (ICD), cardiac resynchronization therapy (CRT), N-terminal pro-brain natriuretic peptide (NT-proBNP), and NYHA class were recorded. Transthoracic echocardiography (TTE) was conducted to assess left ventricular ejection fraction (LVEF), left ventricular end-diastolic diameter (LVDD), effective regurgitant orifice (ERO), and MR severity. MR severity classification comprises of trivial (0+), mild (1+), moderate (2+), moderate-to-severe (3+), and severe (4+). All TTEs were conducted by the same examiner. Right heart catheterization was performed before each procedure to measure mean right atrial pressure (mRAP), pulmonary capillary wedge pressure (PCWP), systolic pulmonary artery pressure (PASP), mean pulmonary artery pressure (mPAP), and cardiac index (CI). MR etiology was classified as DMR or FMR by the Heart Team.
2.4. Study Objectives
A TTE was performed at baseline, at 30-day, and 1-year follow-up to assess MR severity. NYHA class and Kansas City Cardiomyopathy Questionnaire (KCCQ) score were, also, recorded at baseline, 30-day and 1-year follow-up. Survival and hospitalization data were obtained either through telephone contact or via the national electronic health record, when available. The main objectives of the study were to report 1-year mortality and hospitalization rate, to analyze the change in MR severity, NYHA class and QoL throughout follow-up visits and identify plausible baseline prognostic factors for NYHA class I classification at 30-days and 1-year.
2.5. Statistical Analysis
Continuous variables following normal distribution were presented as mean and standard deviation (SD), while variables that were not distributed normally were presented as median and interquartile range (IQR). Normality of distribution was assessed by comparing mean and median values, graphical representation of the distribution of the variables and by using the Kolmogorov–Smirnov test. Qualitative variables were summarized using absolute and relative frequencies [n/N (%)]. Statistical comparisons of continuous variables that exhibited normal distribution were performed using the student t-test, while the Wilcoxon rank-sum test was employed for variables that did not follow a normal distribution. Categorical variables were compared with the χ2 test or the Fisher exact test if cell counts were small (≤5). The Kruskal-Wallis test was used for comparison of continuous variables between more than two independent samples. A multivariate Cox proportional hazards model was fitted to identify independent predictors of NYHA class I in 30-day or 1-year follow-up. The purposeful selection process was used to identify candidate variables for our model. Variables with a p-value <0.2 in the univariate analysis were included in our model. The ratio of events to explanatory variables was 10, to avoid over-fitting of the model. The application of a Cox proportional hazards model yielded hazard ratios and 95% confidence intervals. The Akaike Information Criterion (AIC) was used to select the model with the better fit. All statistical analyses were performed on RStudio version 2023.03.0+386.
3. Results
3.1. Baseline Characteristics and Procedural Results
A total of 83 patients (71% FMR, 66% male) underwent TEER, with a median age of 70 years (IQR: 11) years at baseline. A comprehensive overview of the baseline characteristics of the patients according to the MR etiology is presented in Table 1. Patients with FMR exhibited a higher prevalence of prior myocardial infarction (MI) and presence of permanent pacemaker (PPM), implantable cardioverter-defibrillator (ICD), or cardiac resynchronization therapy (CRT). Additionally, the FMR group had lower left ventricular ejection fraction (LVEF), lower cardiac index (CI), and larger left ventricular end-diastolic diameter (LVDD). In contrast, patients with degenerative mitral regurgitation (DMR) had larger effective regurgitant orifice (ERO). There was no statistically significant difference in the incidence of severe MR between the two groups.
Overall, median post-TEER transmitral gradient was 3.53 (IQR: 1.2), showing no significant mitral stenosis and similar results between FMR and DMR group. Implantation and procedural time were lower in DMR group, with no significant difference reported in number of clips implanted, MR severity at discharge or hospitalization days.
3.2. One-Year Outcomes
After 1 year of follow-up, 10 patients (12%) were hospitalized due to heart failure, of whom 8 subsequently died, resulting in a 1-year mortality rate of 9.6%.
Figure 1 illustrates the longitudinal distribution of NYHA class among patients. Overall, 31 patients (37%) were asymptomatic (NYHA class I) at 30 days, increasing to 37 patients (44.4%) at 1 year. At the 30-day mark, all patients achieved NYHA class I or II, with 96.8% remaining in this status at 1 year. There was a statistically significant improvement in NYHA class from baseline to both the 30-day and 1-year follow-up visits (p < 0.001, p < 0.001, respectively).
Figure 2 illustrates the distribution of MR severity over time. At 30-day follow-up, no severe MR was reported and MR ≤2+ was achieved in 81 (98%) patients. At 1-year follow-up, MR ≤2+ was achieved in 80 (96%) patients. Notably, 19 (23%) patients that were classified in 4+ MR severity at baseline, after 1 year they had only mild MR. Substantial improvement in MR severity is reported from baseline to 30-day and 1 year follow-up (p < 0.001, p < 0.001, respectively).
Figure 3 illustrates the distribution of KCQQ score over time. At the 30-day and 1-year follow-up, there was a statistically significant increase in KCCQ scores compared to baseline values [median (IQR): 69 (53) versus 51 (38); p = 0.031 and median (IQR): 70.5 (55) versus 51 (38); p = 0.02, respectively].
3.3. NYHA Class I Prognostic Factors
Thirty-one (37%) and 37 (44.4%) patients were classified as NYHA class I at 30 days and 1 year after TEER, respectively. Table 2 presents the cox regression analysis of potential prognostic factors for achieving NYHA class I at 30 days post-TEER. For every unit decrease in the natural logarithm of NT-proBNP values, the likelihood of a patient being classified as NYHA class I at 30 days post-TEER increased by 1.59 times (hazard ratio [HR]: 0.63, 95% confidence interval [CI]: 0.41–0.95, p = 0.030).
Table 3 presents the cox regression analysis of potential prognostic factors for achieving NYHA class I at 1 year post-TEER. For every unit decrease in the natural logarithm of EuroSCORE II and NT-proBNP values, the likelihood of a patient being classified as NYHA class I at 1 year post-TEER increased by 2 times (HR: 0.50, 95% CI: 0.28–0.89, p = 0.019) and 1.49 times (HR: 0.67, 95% CI: 0.44–0.99, p = 0.049), respectively.
4. Discussion
This single center study summarizes the 1-year outcomes of patients underwent TEER for either DMR or FMR and demonstrates a substantial improvement in both quality of life and functional and echocardiographic status, with favorable survival outcomes. Additionally, the study identifies NT-proBNP and EuroSCORE II as potential prognostic indicators for achieving NYHA class I within 30 days or 1 year post-TEER.
In detail, the 1-year mortality rate was 9.6% which is comparable to those reported from Japan (14.9%) [13], COAPT trial device group (18.8%) [9], EXPAND study (14.9%) [14], and OCEAN-mitral registry (12.3%) [15]. However, higher 1-year mortality rates were observed in the TRAMI (20.2%) [16] (20.2%) and TVT (25.8%) [17] registries, which included larger patient populations. In our study, one-third of the patients were already asymptomatic (NYHA class I) within 30 days after TEER and NYHA class I/II was achieved by the total cohort. At 1 year, 96.8% achieved NYHA class I/II, which is comparable to OCEAN-mitral registry (94.1%) [15] and results from Japan (93%) [13], thus higher than EXPAND study (80.3%) [10]. Similar were the results for the residual MR severity at 1-year, with our study reporting 96% of patients with MR ≤2+, which is higher than the 88.1% reported in the Japanese study [13] and comparable to the 94.1% and 97.5% reported in the OCEAN-mitral registry [15] and the EXPAND study [10], respectively.
This improvement could be predicted by baseline Euroscore II and NT-proBNP values, which were strongly associated with achieving NYHA class I status in 30 days and 1 year. These associations were consistent regardless of MR etiology and residual severity, contrasting with previously established knowledge.
Our study’s primary limitations include a relatively small sample size and a single-center design, potentially restricting the generalizability of our findings. However, it’s noteworthy that our center acts as a referral hub for structural heart disease patients across a broader region in northern Greece, mitigating potential selection biases. Moreover, the retrospective nature of our study may introduce biases related to data collection and patient selection.
5. Conclusions
In conclusion, the MitraClip® G4 system proved to be a safe and effective option for treating MR, significantly reducing MR severity and improving both functional status and quality of life, with key baseline markers such as NT-proBNP and EuroSCORE II predicting better clinical outcomes. As the field of transcatheter mitral valve repair continues to evolve, future research should focus on optimizing patient selection and exploring long-term outcomes across broader populations to further enhance the therapeutic potential of this intervention.
Author Contributions
Conceptualization, G.P. and V.N.; methodology, G.P. and V.N.; software, G.P. and V.N.; validation, G.P. and V.N.; formal analysis, G.P. and V.N.; investigation, I.N., S.E., A.I. and V.N.; resources, G.P. and V.N.; data curation, G.P. and V.N.; writing—original draft preparation, G.P.; writing—review and editing, V.N.; visualization, G.P. and V.N.; supervision, V.N.; project administration, V.N. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of Interbalkan Medical Center (protocol code 2335/9.9.2024)
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to ethical restrictions.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Agricola, E.; Ielasi, A.; Oppizzi, M.; Faggiano, P.; Ferri, L.; Calabrese, A.; Vizzardi, E.; Alfieri, O.; Margonato, A. Long-term prognosis of medically treated patients with functional mitral regurgitation and left ventricular dysfunction. European Journal of Heart Failure 2009, 11, 581–587. [Google Scholar] [CrossRef] [PubMed]
- Enriquez-Sarano, M.; Akins, C.W.; Vahanian, A. Mitral regurgitation. The Lancet 2009, 373, 1382–1394. [Google Scholar] [CrossRef]
- Nkomo, V.T.; Gardin, J.M.; Skelton, T.N.; Gottdiener, J.S.; Scott, C.G.; Enriquez-Sarano, M. Burden of valvular heart diseases: a population-based study. The Lancet 2006, 368, 1005–1011. [Google Scholar] [CrossRef] [PubMed]
- Rossi, A.; Dini, F.L.; Faggiano, P.; Agricola, E.; Cicoira, M.; Frattini, S.; Simioniuc, A.; Gullace, M.; Ghio, S.; Enriquez-Sarano, M.; Temporelli, P.L. Independent prognostic value of functional mitral regurgitation in patients with heart failure. A quantitative analysis of 1256 patients with ischaemic and non-ischaemic dilated cardiomyopathy. Heart 2011, 97, 1675–1680. [Google Scholar] [CrossRef] [PubMed]
- Taramasso, M.; Buzzatti, N.; La Canna, G.; Colombo, A.; Alfieri, O.; Maisano, F. Interventional vs. surgical mitral valve therapy. Which technique for which patient? Herz 2013, 38, 460–6. [Google Scholar] [CrossRef] [PubMed]
- Feldman, T.; Foster, E.; Glower, D.D.; Kar, S.; Rinaldi, M.J.; Fail, P.S.; Smalling, R.W.; Siegel, R.; Rose, G.A.; Engeron, E.; Loghin, C.; Trento, A.; Skipper, E.R.; Fudge, T.; Letsou, G.V.; Massaro, J.M.; Mauri, L. Percutaneous Repair or Surgery for Mitral Regurgitation. New England Journal of Medicine 2011, 364, 1395–1406. [Google Scholar] [CrossRef] [PubMed]
- Mauri, L.; Foster, E.; Glower, D.D.; Apruzzese, P.; Massaro, J.M.; Herrmann, H.C.; Hermiller, J.; Gray, W.; Wang, A.; Pedersen, W.R.; Bajwa, T.; Lasala, J.; Low, R.; Grayburn, P.; Feldman, T. 4-Year Results of a Randomized Controlled Trial of Percutaneous Repair Versus Surgery for Mitral Regurgitation. Journal of the American College of Cardiology 2013, 62, 317–328. [Google Scholar] [CrossRef] [PubMed]
- Obadia, J.-F.; Messika-Zeitoun, D.; Leurent, G.; Iung, B.; Bonnet, G.; Piriou, N.; Lefèvre, T.; Piot, C.; Rouleau, F.; Carrié, D.; Nejjari, M.; Ohlmann, P.; Leclercq, F.; Etienne, C.S.; Teiger, E.; Leroux, L.; Karam, N.; Michel, N.; Gilard, M.; Donal, E.; Trochu, J.-N.; Cormier, B.; Armoiry, X.; Boutitie, F.; Maucort-Boulch, D.; Barnel, C.; Samson, G.; Guerin, P.; Vahanian, A.; Mewton, N. Percutaneous Repair or Medical Treatment for Secondary Mitral Regurgitation. New England Journal of Medicine 2018, 379, 2297–2306. [Google Scholar] [CrossRef] [PubMed]
- Stone, G.W.; Lindenfeld, J.; Abraham, W.T.; Kar, S.; Lim, D.S.; Mishell, J.M.; Whisenant, B.; Grayburn, P.A.; Rinaldi, M.; Kapadia, S.R.; Rajagopal, V.; Sarembock, I.J.; Brieke, A.; Marx, S.O.; Cohen, D.J.; Weissman, N.J.; Mack, M.J. Transcatheter Mitral-Valve Repair in Patients with Heart Failure. New England Journal of Medicine 2018, 379, 2307–2318. [Google Scholar] [CrossRef] [PubMed]
- Bardeleben, R.S. v.; Mahoney, P.; Morse, M.A.; Price, M.J.; Denti, P.; Maisano, F.; Rogers, J.H.; Rinaldi, M.; Marco, F.D.; Rollefson, W.; Chehab, B.; Williams, M.; Leurent, G.; Asch, F.M.; Rodriguez, E. 1-Year Outcomes With Fourth-Generation Mitral Valve Transcatheter Edge-to-Edge Repair From the EXPAND G4 Study. JACC: Cardiovascular Interventions 2023, 16, 2600–2610. [Google Scholar] [CrossRef] [PubMed]
- Anker, S.D.; Friede, T.; Bardeleben, R.-S. v.; Butler, J.; Khan, M.-S.; Diek, M.; Heinrich, J.; Geyer, M.; Placzek, M.; Ferrari, R.; Abraham, W.T.; Alfieri, O.; Auricchio, A.; Bayes-Genis, A.; Cleland, J.G.F.; Filippatos, G.; Gustafsson, F.; Haverkamp, W.; Kelm, M.; Kuck, K.-H.; Landmesser, U.; Maggioni, A.P.; Metra, M.; Ninios, V.; Petrie, M.C.; Rassaf, T.; Ruschitzka, F.; Schäfer, U.; Schulze, P.C.; Spargias, K.; Vahanian, A.; Zamorano, J.L.; Zeiher, A.; Karakas, M.; Koehler, F.; Lainscak, M.; Öner, A.; Mezilis, N.; Theofilogiannakos, E.K.; Ninios, I.; Chrissoheris, M.; Kourkoveli, P.; Papadopoulos, K.; Smolka, G.; Wojakowski, W.; Reczuch, K.; Pinto, F.J.; Wiewiórka, Ł.; Kalarus, Z.; Adamo, M.; Santiago-Vacas, E.; Ruf, T.F.; Gross, M.; Tongers, J.; Hasenfuss, G.; Schillinger, W.; Ponikowski, P. Transcatheter Valve Repair in Heart Failure with Moderate to Severe Mitral Regurgitation. New England Journal of Medicine, ahead of print. 2024. [Google Scholar]
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; Delgado, V.; Freemantle, N.; Gilard, M.; Haugaa, K.H.; Jeppsson, A.; Jüni, P.; Pierard, L.; Prendergast, B.D.; Sádaba, J.R.; Tribouilloy, C.; Wojakowski, W.; Group, E.E.S.D.; Societies, E.N.C. 2021 ESC/EACTS Guidelines for the management of valvular heart disease: Developed by the Task Force for the management of valvular heart disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). European Heart Journal 2021, 43, 561–632. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, T.; Kubo, S.; Izumo, M.; Mizuno, S.; Shirai, S. MitraClip Treatment of Moderate-to-Severe and Severe Mitral Regurgitation in High Surgical Risk Patients—Real-World 1-Year Outcomes From Japan. Circ J 2022, 86, 402–411. [Google Scholar] [CrossRef] [PubMed]
- Kar, S.; von Bardeleben, R.S.; Rottbauer, W.; Mahoney, P.; Price, M.J.; Grasso, C.; Williams, M.; Lurz, P.; Ahmed, M.; Hausleiter, J.; Chehab, B.; Zamorano, J.L.; Asch, F.M.; Maisano, F. Contemporary Outcomes Following Transcatheter Edge-to-Edge Repair: 1-Year Results From the EXPAND Study. JACC Cardiovasc Interv 2023, 16, 589–602. [Google Scholar] [CrossRef] [PubMed]
- Kubo, S.; Yamamoto, M.; Saji, M.; Asami, M.; Enta, Y.; Nakashima, M.; Shirai, S.; Izumo, M.; Mizuno, S.; Watanabe, Y.; Amaki, M.; Kodama, K.; Yamaguchi, J.; Nakajima, Y.; Naganuma, T.; Bota, H.; Ohno, Y.; Yamawaki, M.; Ueno, H.; Mizutani, K.; Adachi, Y.; Otsuka, T.; Hayashida, K.; Hayashida, K.; Adachi, Y.; Yamamoto, M.; Yamamoto, M.; Shirai, S.; Watanabe, Y.; Naganuma, T.; Yamawaki, M.; Enta, Y.; Nakashima, M.; Mizuno, S.; Ueno, H.; Ohno, Y.; Nakajima, Y.; Izumo, M.; Bota, H.; Kodama, K.; Yamaguchi, J.; Kubo, S.; Amaki, M.; Asami, M.; Saji, M.; Mizutani, K. One-year outcomes and their relationship to residual mitral regurgitation after transcatheter edge-to-edge repair with MitraClip device: Insights from the OCEAN-Mitral registry. Journal of the American Heart Association 2023, 12, e030747. [Google Scholar] [CrossRef] [PubMed]
- Puls, M.; Lubos, E.; Boekstegers, P.; von Bardeleben, R.S.; Ouarrak, T.; Butter, C.; Zuern, C.S.; Bekeredjian, R.; Sievert, H.; Nickenig, G.; Eggebrecht, H.; Senges, J.; Schillinger, W. One-year outcomes and predictors of mortality after MitraClip therapy in contemporary clinical practice: results from the German transcatheter mitral valve interventions registry. Eur Heart J 2016, 37, 703–12. [Google Scholar] [CrossRef] [PubMed]
- Sorajja, P.; Vemulapalli, S.; Feldman, T.; Mack, M.; Holmes, D.R., Jr.; Stebbins, A.; Kar, S.; Thourani, V.; Ailawadi, G. Outcomes With Transcatheter Mitral Valve Repair in the United States: An STS/ACC TVT Registry Report. J Am Coll Cardiol 2017, 70, 2315–2327. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
New York Heart Association (NYHA) distribution over time. Abbreviations: NYHA: New York Heart Association.
Figure 1.
New York Heart Association (NYHA) distribution over time. Abbreviations: NYHA: New York Heart Association.
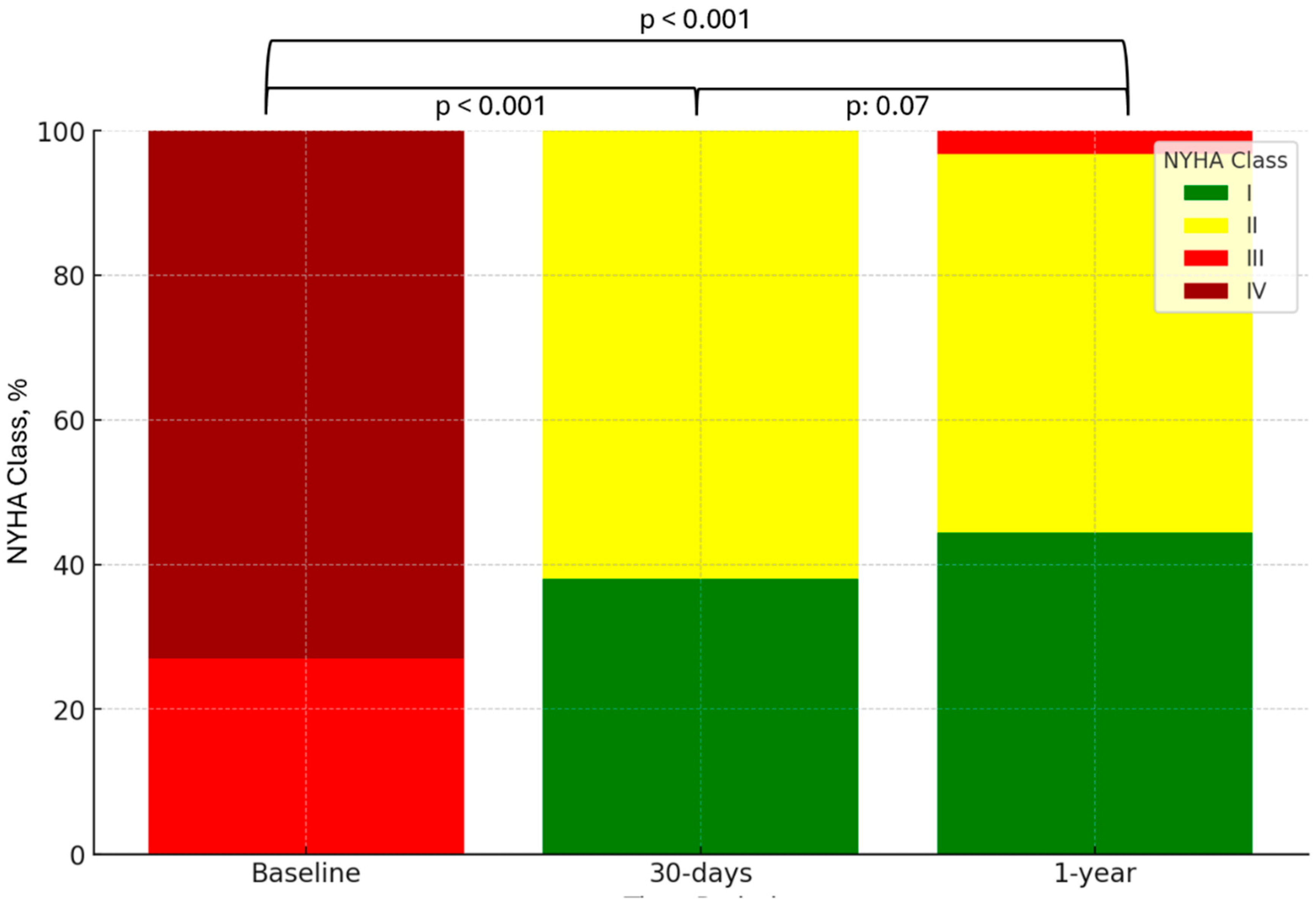
Figure 2.
Mitral regurgitation (MR) severity distribution over time. Abbreviations: MR: Mitral Regurgitation.
Figure 2.
Mitral regurgitation (MR) severity distribution over time. Abbreviations: MR: Mitral Regurgitation.
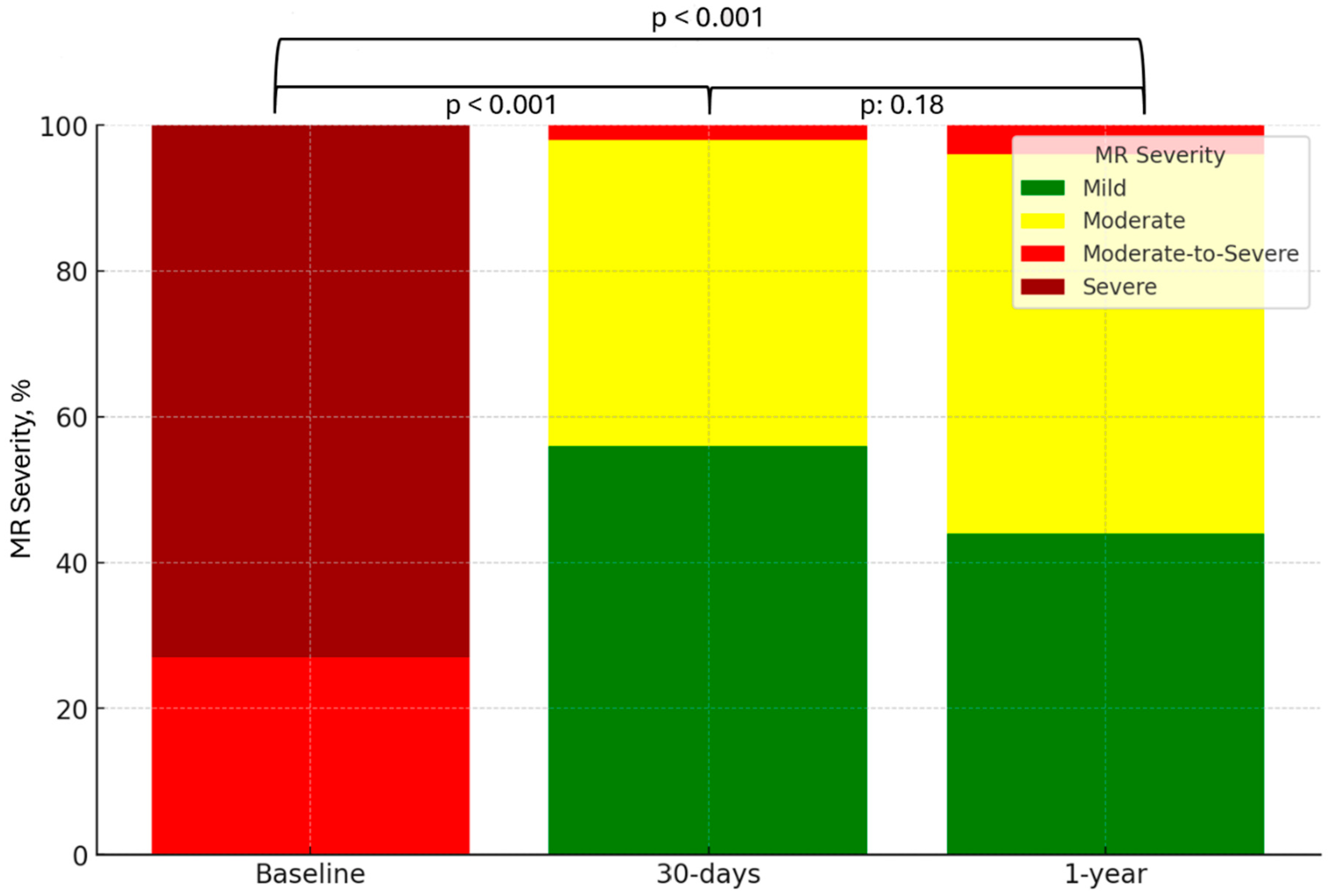
Figure 3.
KCCQ score distribution over time. Abbreviations: KCCQ: Kansas City Cardiomyopathy Questionnaire.
Figure 3.
KCCQ score distribution over time. Abbreviations: KCCQ: Kansas City Cardiomyopathy Questionnaire.
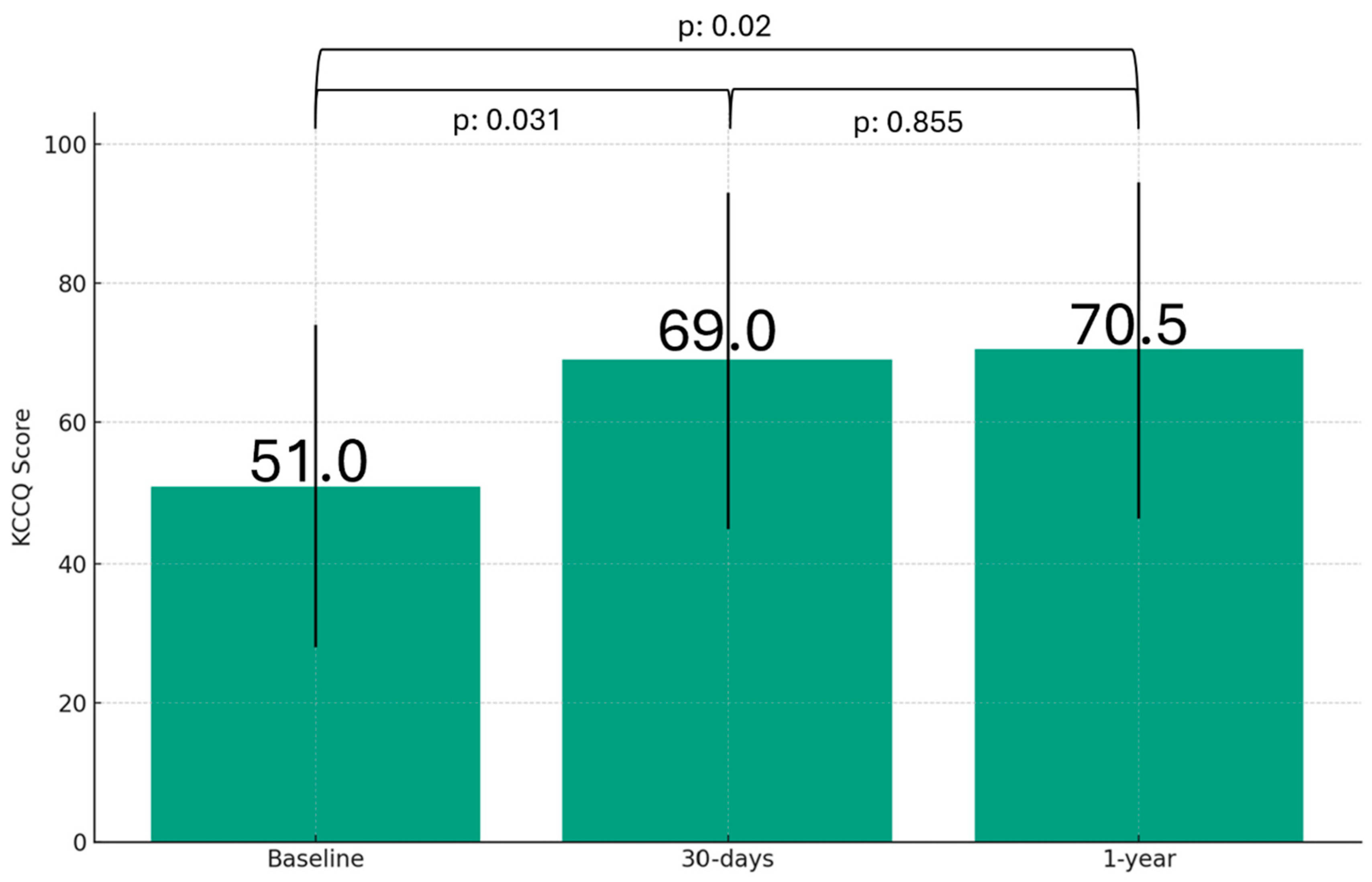

Table 1.
Patients’ baseline characteristics.
| Characteristic | Overall, N = 831 | DMR, N = 24 | FMR, N = 59 | p-value2 |
| Age, years | 76 (11) | 79 (9) | 75 (11) | 0.2 |
| Male sex | 55 / 83 (66) | 16 / 24 (67) | 39 / 59 (66) | >0.9 |
| NYHA class | >0.9 | |||
| III | 22 / 83 (27) | 6 / 24 (25) | 16 / 59 (27) | |
| IV | 61 / 83 (73) | 18 / 24 (75) | 41 / 59 (73) | |
| Euroscore II, % | 0.07 (0.06) | 0.06 (0.03) | 0.08 (0.07) | 0.074 |
| eGFR, mL/min/1.73 m² | 48 (30) | 59 (25) | 45 (30) | 0.12 |
| NT-proBNP, pg/mL | 2,755 (3,351) | 1,788 (3,786) | 2,876 (3,375) | 0.072 |
| HF hospitalization | 57 / 83 (69) | 17 / 24 (71) | 40 / 59 (68) | 0.8 |
| MI | 23 / 83 (28) | 1 / 24 (4.2) | 22 / 59 (37) | 0.002 |
| AF | 54 / 83 (65) | 13 / 24 (54) | 41 / 59 (69) | 0.2 |
| PPM | 12 / 83 (14) | 0 / 24 (0) | 12 / 59 (20) | 0.015 |
| COPD | 31 / 83 (37) | 10 / 24 (42) | 21 / 59 (36) | 0.6 |
| Diabetes | 15 / 83 (18) | 5 / 24 (21) | 10 / 59 (17) | 0.8 |
| ICD / CRT | 0.023 | |||
| None | 61 / 83 (73) | 22 / 24 (92) | 39 / 59 (66) | |
| ICD | 11 / 83 (13) | 2 / 24 (8.3) | 9 / 59 (15) | |
| CRT | 11 / 83 (13) | 0 / 24 (0) | 11 / 59 (19) | |
| Echocardiography | ||||
| Severe (4+) MR | 73 / 83 (88) | 21 / 24 (88) | 52 / 59 (88) | >0.9 |
| ERO, mm | 42 (11) | 52 (17) | 41 (9) | <0.001 |
| LVEF, % | <0.001 | |||
| < 40 | 36 / 83 (43) | 3 / 24 (13) | 33 / 59 (56) | |
| 41-49 | 30 / 83 (36) | 8 / 24 (33) | 22 / 59 (37) | |
| ≥ 50 | 17 / 83 (20) | 13 / 24 (54) | 4 / 59 (6.8) | |
| LVDD, cm | 6.10 (1.20) | 5.30 (0.75) | 6.20 (0.85) | <0.001 |
| Hemodynamics | ||||
| CI, mL/min/m2 | 1.90 (0.60) | 2.05 (0.53) | 1.80 (0.60) | 0.027 |
| PASP, mmHg | 55 (15) | 53 (20) | 55 (15) | 0.6 |
| mPAP, mmHg | 33 (11) | 33 (11) | 33 (14) | 0.4 |
| PCWP, mmHg | 24 (11) | 24 (11) | 24 (10) | 0.4 |
| mRAP, mmHg | 10.0 (5.0) | 9.5 (6.3) | 10.0 (6.8) | 0.4 |
| Procedural results | ||||
| Procedural success | 83 / 83 (100) | 24 / 24 (100) | 59 / 59 (100) | >0.9 |
| Implantation time, mins | 26 (8) | 30 (10) | 25 (5) | <0.001 |
| Procedural time, mins | 55 (11) | 63 (10) | 52 (7) | <0.001 |
| Number of clips implanted | 0.060 | |||
| 1 | 57 / 83 (69) | 15 / 24 (63) | 42 / 59 (71) | |
| 2 | 23 / 83 (28) | 6 / 24 (25) | 17 / 59 (29) | |
| 3 | 2 / 83 (2.4) | 2 / 24 (8.3) | 0 / 59 (0) | |
| 4 | 1 / 83 (1.2) | 1 / 24 (4.2) | 0 / 59 (0) | |
| MR severity at discharge | >0.9 | |||
| 1+ (mild) | 6 / 83 (7.2) | 1 / 24 (4.2) | 5 / 59 (8.5) | |
| 2+ (moderate) | 46 / 83 (55) | 13 / 24 (54) | 33 / 59 (56) | |
| 3+ (moderate-to-severe) | 28 / 83 (34) | 9 / 24 (38) | 19 / 59 (32) | |
| 4+ (severe) | 3 / 83 (3.6) | 1 / 24 (4.2) | 2 / 59 (3.4) | |
| Transmitral gradient, mmHg | 3.53 (1.2) | 3.82 (1.3) | 3.47 (1.2) | 0.3 |
| Hospital length of stay, days | 3 (1) | 3 (1) | 3 (1) | >0.9 |
1 Median (IQR); n / N (%); 2 Kruskal-Wallis rank sum test; Pearson’s Chi-squared test; Fisher’s exact test; Note: Continuous variables are presented as median value with interquartile range (IQR). Categorical variables are presented as n / N (%). Abbreviations: DMR: Degenerative Mitral Regurgitation, FMR: Functional Mitral Regurgitation, NYHA: New York Heart Association, eGFR: estimated Glomerular Filtration Rate, NT-proBNP: N terminal-pro brain natriuretic peptide, HF: Heart Failure, MI: Myocardial Infarction, AF: Atrial Fibrillation, PPM: Permanent Pacemaker, COPD: Chronic Obstructive Pulmonary Disease, ICD: Implantable Cardioverter Defibrillator, CRT: Cardiac Resynchronization Therapy, MR: Mitral Regurgitation, ERO: Effective Regurgitant Orifice, LVEF: Left Ventricular Ejection Fraction, LVDD: Left Ventricular End-Diastolic Diameter, CI: Cardiac Index, PASP: Pulmonary Artery Systolic Pressure, mPAP: mean Pulmonary Artery Pressure, PCWP: Pulmonary Capillary Wedge Pressure, mRAP: mean Right Atrial Pressure.
Table 2.
Adjusted and Unadjusted Hazard Ratios of NYHA class I in 30 days.
| Univariate | Multivariate | ||||||
| Characteristic | N | HR1 | 95% CI1 | p-value | HR1 | 95% CI1 | p-value |
| Age | 83 | 1.0 | 0.96, 1.03 | 0.7 | |||
| Male sex | 83 | 0.91 | 0.44, 1.90 | 0.8 | |||
| Euroscore II2 | 83 | 0.50 | 0.28, 0.88 | 0.017 | 0.64 | 0.35, 1.14 | 0.13 |
| eGFR | 83 | 1.01 | 0.99, 1.03 | 0.4 | |||
| NT-proBNP2 | 83 | 0.55 | 0.37, 0.82 | 0.003 | 0.63 | 0.41, 0.95 | 0.030 |
| HF Hospitalization | 83 | 0.56 | 0.27, 1.14 | 0.11 | |||
| MI | 83 | 0.57 | 0.23, 1.38 | 0.2 | |||
| AF | 83 | 0.82 | 0.40, 1.68 | 0.6 | |||
| PPM | 83 | 0.35 | 0.08, 1.47 | 0.2 | |||
| COPD | 83 | 1.77 | 0.87, 3.58 | 0.11 | |||
| Diabetes | 83 | 0.84 | 0.32, 2.20 | 0.7 | |||
| ICD / CRT | 83 | 0.90 | 0.54, 1.50 | 0.7 | |||
| MR etiology | 83 | ||||||
| DMR | — | — | — | — | |||
| FMR | 0.48 | 0.23, 0.98 | 0.044 | 0.66 | 0.31, 1.41 | 0.3 | |
| Number of clips implanted | 83 | ||||||
| 1 | — | — | |||||
| 2 | 1.34 | 0.63, 2.86 | 0.5 | ||||
| 3 | 5.02 | 0.67, 37.7 | 0.12 | ||||
| MR severity at 30 days | 83 | ||||||
| 1+ | — | — | |||||
| 2+ | 1.22 | 0.59, 2.51 | 0.6 | ||||
| 3+ | 1.60 | 0.21, 12.0 | 0.6 | ||||
| MR severity at 1 year | 83 | ||||||
| 1+ | — | — | |||||
| 2+ | 1.14 | 0.40, 3.29 | 0.8 | ||||
| 3+ | 0.00 | 0.00, Inf | >0.9 | ||||
| Hospital stay | 83 | 0.72 | 0.37, 1.40 | 0.3 | |||
| Echocardiography | |||||||
| LVEF | 83 | 5.37 | 0.16, 182 | 0.4 | |||
| LVDD | 83 | 0.72 | 0.42, 1.24 | 0.2 | |||
| ERO | 83 | 1.00 | 0.97, 1.03 | >0.9 | |||
| Hemodynamics | |||||||
| PASP | 83 | 0.99 | 0.96, 1.03 | 0.6 | |||
| PCWP | 83 | 0.98 | 0.93, 1.03 | 0.4 | |||
| mRAP | 83 | 0.98 | 0.91, 1.05 | 0.5 | |||
| mPAP | 83 | 0.97 | 0.93, 1.02 | 0.3 | |||
| CI | 83 | 2.21 | 1.07, 4.59 | 0.033 | |||
1 HR = Hazard Ratio, CI = Confidence Interval; 2 Presented as Natural Logarithm (ln); Abbreviations: DMR: Degenerative Mitral Regurgitation, FMR: Functional Mitral Regurgitation, eGFR: estimated Glomerular Filtration Rate, NTpro-BNP: N terminal-pro brain natriuretic peptide, HF: Heart Failure, MI: Myocardial Infarction, AF: Atrial Fibrillation, PPM: Permanent Pacemaker, COPD: Chronic Obstructive Pulmonary Disease, ICD: Implantable Cardioverter Defibrillator, CRT: Cardiac Resynchronization Therapy, MR: Mitral Regurgitation, ERO: Effective Regurgitant Orifice, LVEF: Left Ventricular Ejection Fraction, LVDD: Left Ventricular End-Diastolic Diameter, CI: Cardiac Index, PASP: Pulmonary Artery Systolic Pressure, mPAP: mean Pulmonary Artery Pressure, PCWP: Pulmonary Capillary Wedge Pressure, mRAP: mean Right Atrial Pressure.
Table 3.
Adjusted and Unadjusted Hazard Ratios of NYHA class I in 1 year.
| Univariate | Multivariate | ||||||
| Characteristic | N | HR1 | 95% CI1 | p-value | HR1 | 95% CI1 | p-value |
| Age | 83 | 0.98 | 0.95, 1.01 | 0.12 | |||
| Male sex | 83 | 0.92 | 0.45, 1.85 | 0.8 | |||
| Euroscore II2 | 83 | 0.40 | 0.23, 0.69 | 0.001 | 0.50 | 0.28, 0.89 | 0.019 |
| eGFR | 83 | 1.02 | 1.00, 1.04 | 0.025 | |||
| NT-proBNP2 | 83 | 0.58 | 0.40, 0.85 | 0.004 | 0.67 | 0.44, 0.99 | 0.049 |
| HF hospitalization | 83 | 0.49 | 0.25, 0.96 | 0.037 | 0.64 | 0.32, 1.26 | 0.2 |
| MI | 83 | 0.49 | 0.20, 1.18 | 0.11 | |||
| AF | 83 | 0.61 | 0.31, 1.19 | 0.15 | |||
| PPM | 83 | 0.51 | 0.16, 1.66 | 0.3 | |||
| COPD | 83 | 1.44 | 0.73, 2.83 | 0.3 | |||
| Diabetes | 83 | 0.96 | 0.40, 2.33 | >0.9 | |||
| ICD/CRT | 83 | 0.89 | 0.55, 1.46 | 0.6 | |||
| MR etiology | 83 | ||||||
| DMR | — | — | |||||
| FMR | 0.49 | 0.25, 0.97 | 0.040 | ||||
| Number of clips implanted | 83 | ||||||
| 1 | — | — | |||||
| 2 | 0.98 | 0.46, 2.13 | >0.9 | ||||
| 3 | 4.24 | 0.57, 31.6 | 0.2 | ||||
| MR severity at 30 days | 83 | ||||||
| 1+ | — | — | |||||
| 2+ | 1.47 | 0.73, 2.94 | 0.3 | ||||
| 3+ | 1.60 | 0.21, 12.0 | 0.6 | ||||
| MR severity at 1 year | 83 | ||||||
| 1+ | — | — | |||||
| 2+ | 0.93 | 0.36, 2.42 | 0.9 | ||||
| 3+ | 0.00 | 0.00, Inf | >0.9 | ||||
| Hospital stay | 83 | 0.77 | 0.40, 1.46 | 0.4 | |||
| Echocardiography | |||||||
| LVEF | 83 | 4.44 | 0.15, 131 | 0.4 | |||
| LVDD | 83 | 0.79 | 0.47, 1.32 | 0.4 | |||
| ERO | 83 | 1.00 | 0.97, 1.03 | 0.9 | |||
| Hemodynamics | |||||||
| PASP | 83 | 0.99 | 0.96, 1.02 | 0.5 | |||
| PCWP | 83 | 0.98 | 0.93, 1.02 | 0.3 | |||
| mRAP | 83 | 0.95 | 0.88, 1.02 | 0.14 | |||
| mPAP | 83 | 0.97 | 0.93, 1.02 | 0.2 | |||
| CI | 83 | 1.73 | 0.87, 3.45 | 0.12 | |||
1 HR = Hazard Ratio, CI = Confidence Interval; 2 Presented as Natural Logarithm (ln); Abbreviations: DMR: Degenerative Mitral Regurgitation, FMR: Functional Mitral Regurgitation, eGFR: estimated Glomerular Filtration Rate, NTpro-BNP: N terminal-pro brain natriuretic peptide, HF: Heart Failure, MI: Myocardial Infarction, AF: Atrial Fibrillation, PPM: Permanent Pacemaker, COPD: Chronic Obstructive Pulmonary Disease, ICD: Implantable Cardioverter Defibrillator, CRT: Cardiac Resynchronization Therapy, MR: Mitral Regurgitation, ERO: Effective Regurgitant Orifice, LVEF: Left Ventricular Ejection Fraction, LVDD: Left Ventricular End-Diastolic Diameter, CI: Cardiac Index, PASP: Pulmonary Artery Systolic Pressure, mPAP: mean Pulmonary Artery Pressure, PCWP: Pulmonary Capillary Wedge Pressure, mRAP: mean Right Atrial Pressure. .
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



