Submitted:
13 September 2024
Posted:
15 September 2024
You are already at the latest version
Abstract
The global landscape of health and disease has undergone significant transformations over the past several decades. While infectious diseases once dominated the morbidity and mortality statistics, non-communicable diseases (NCDs) have emerged as the leading cause of death and disability worldwide. This shift has profound implications for public health systems, healthcare delivery, and global health policies. This introduction aims to explore the main tendencies of disease burden, morbidity, and mortality in the world, with a special emphasis on NCDs and the Implications of Emerging AI Technologies. By examining the current trends and underlying factors, we can better understand the challenges and opportunities for improving global health outcomes.
Keywords:
Disease Burden
; NCD
; Emerging AI
1. Introduction
- The Global Burden of Disease
The Global Burden of Disease (GBD) study provides a comprehensive assessment of health loss across diseases, injuries, and risk factors. The GBD study quantifies disability-adjusted life years (DALYs), a measure that combines the burden of premature mortality and disability, allowing for a more holistic understanding of health impacts.
According to the latest GBD study, NCDs are responsible for over 70% of all deaths globally, with cardiovascular diseases, cancers, chronic respiratory diseases, and diabetes being the leading contributors (Murray et al., 2020). This represents a significant shift from previous decades when infectious diseases such as lower respiratory infections, HIV/AIDS, and diarrheal diseases were the primary causes of death.
- The Rise of Non-Communicable Diseases
Cardiovascular diseases (CVDs), including heart attacks and strokes, are the leading cause of death globally. The World Health Organization (WHO) estimates that CVDs claim approximately 17.9 million lives each year, accounting for 31% of all global deaths (WHO, 2021). The increase in CVDs is attributed to a combination of factors, including an aging population, increased prevalence of risk factors such as hypertension, diabetes, obesity, and unhealthy lifestyle choices such as poor diet, physical inactivity, and tobacco use (Benjamin et al., 2019).
Cancer is the second leading cause of death worldwide, responsible for nearly 10 million deaths annually. The most common types of cancer globally include lung, breast, colorectal, prostate, and stomach cancers. The rise in cancer incidence is linked to aging populations, lifestyle factors such as smoking, alcohol consumption, and poor diet, as well as environmental and occupational exposures to carcinogens (Bray et al., 2018).
Chronic respiratory diseases, such as chronic obstructive pulmonary disease (COPD) and asthma, are among the top causes of death and disability. COPD alone is responsible for approximately 3.23 million deaths annually. The primary risk factors for chronic respiratory diseases include smoking, air pollution, and occupational exposures (Vos et al., 2020).
Diabetes is a growing public health concern, with the number of people living with diabetes reaching 463 million in 2019. Diabetes is a significant risk factor for cardiovascular disease, kidney failure, and blindness. The global increase in diabetes prevalence is driven by rising rates of obesity and sedentary lifestyles (Cho et al., 2018).
1.2. The Double Burden of Disease
Many low- and middle-income countries (LMICs) face a double burden of disease, where the health systems must contend with both infectious diseases and the rising tide of NCDs. This dual challenge strains healthcare systems that are often already under-resourced and ill-equipped to manage chronic conditions. The coexistence of infectious diseases and NCDs can exacerbate health outcomes, as individuals with NCDs are more susceptible to infections and their complications.
Key behavioral risk factors contributing to the NCD burden include tobacco use, physical inactivity, unhealthy diet, and harmful use of alcohol. These risk factors are modifiable and addressing them is critical to reducing the burden of NCDs. For instance, tobacco use is responsible for over 8 million deaths annually, with most of these deaths occurring in LMICs (WHO, 2020). Similarly, unhealthy diets and lack of physical activity are major contributors to obesity and related NCDs.
Metabolic risk factors such as hypertension, hyperglycemia, hyperlipidemia, and obesity are significant contributors to the NCD burden. Hypertension, for example, affects approximately 1.13 billion people worldwide and is a major risk factor for cardiovascular diseases, stroke, and kidney disease (Forouzanfar et al., 2017).
Socioeconomic determinants such as income, education, and occupation play a crucial role in health outcomes. Individuals from lower socioeconomic backgrounds often have limited access to healthcare services, nutritious food, and opportunities for physical activity. This socioeconomic gradient in health is evident across both high-income and LMICs, highlighting the importance of addressing social determinants of health to reduce health inequities (Marmot et al., 2008).
1.3. The Impact of Urbanization and Aging
Rapid urbanization, particularly in LMICs, has significant implications for health. Urban environments often promote sedentary lifestyles, poor dietary habits, and increased exposure to air pollution. These factors contribute to the rise of NCDs in urban populations. However, urbanization also presents opportunities for health promotion through better infrastructure, healthcare access, and health education (Ezzati et al., 2005).
- Aging Population
The global population is aging, with the number of people aged 60 years and older expected to double by 2050 (please see images 1 and 2). Aging is a significant risk factor for NCDs, as the prevalence of chronic conditions increases with age. This demographic shift necessitates a reorientation of health systems to focus on chronic disease management, long-term care, and palliative care (Kowal et al., 2016). Also, Frailty Syndrome rises as a major influential factor in morbidity and mortality (Montgomery R. M., Aprahamian, I. 2018).
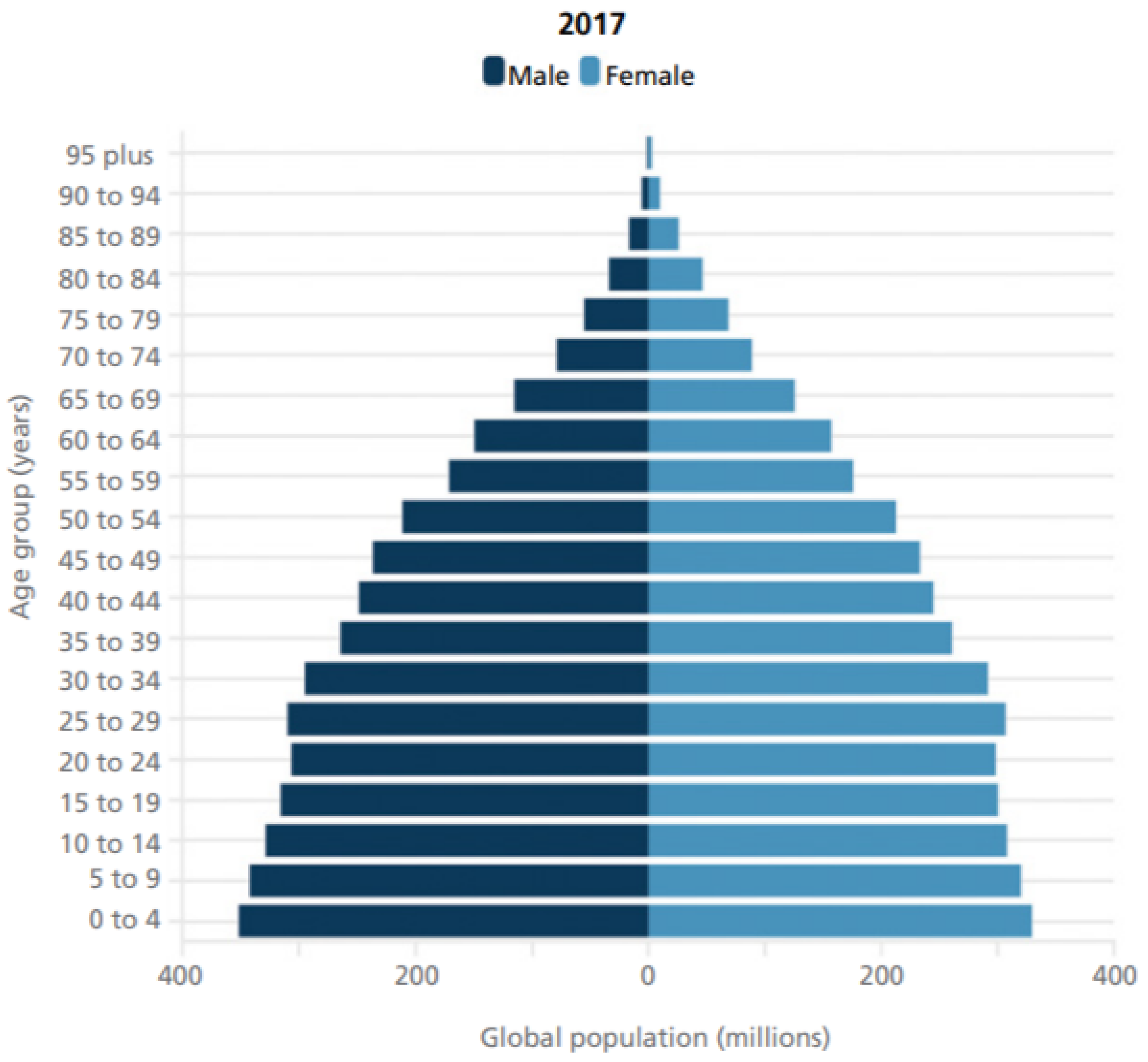
Image 1. Population Pyramid estimated in 2017, already showing aging tendencies noted by the subtle “engorgement” of the middle age horizontal bars. This pyramid is probably largely outdated by the pandemics (2020-2022). We still wait for further conclusions. (Source: Worldometer 2023).
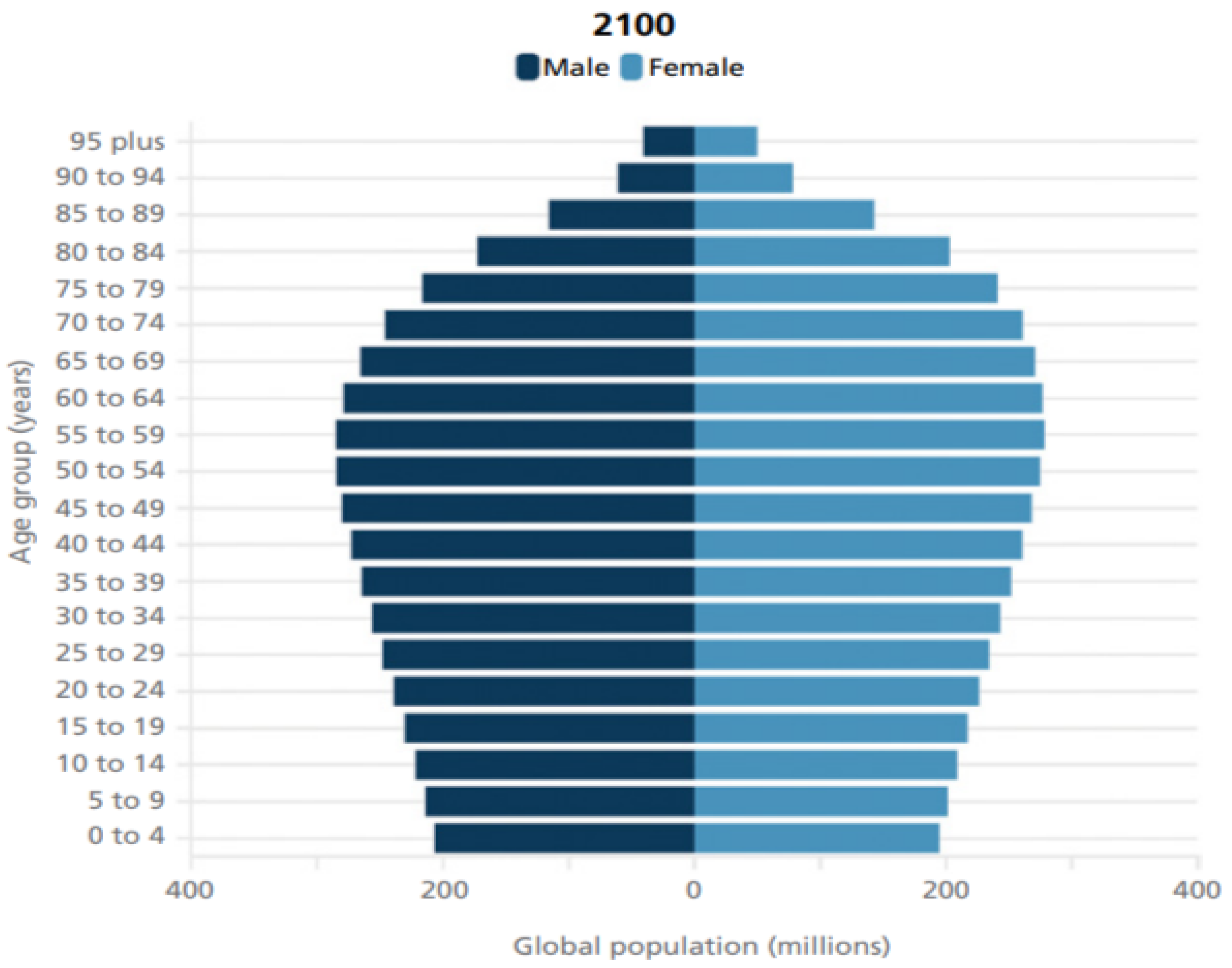
Image 2. Highlight of the 2100 projected age “pyramid” population. This projection is also likely outdated by pandemics with expected exacerbating tendencies. and the rapid and still unknown changes that Artificial Intelligence will provoke. (Source: Worldometer 2023).
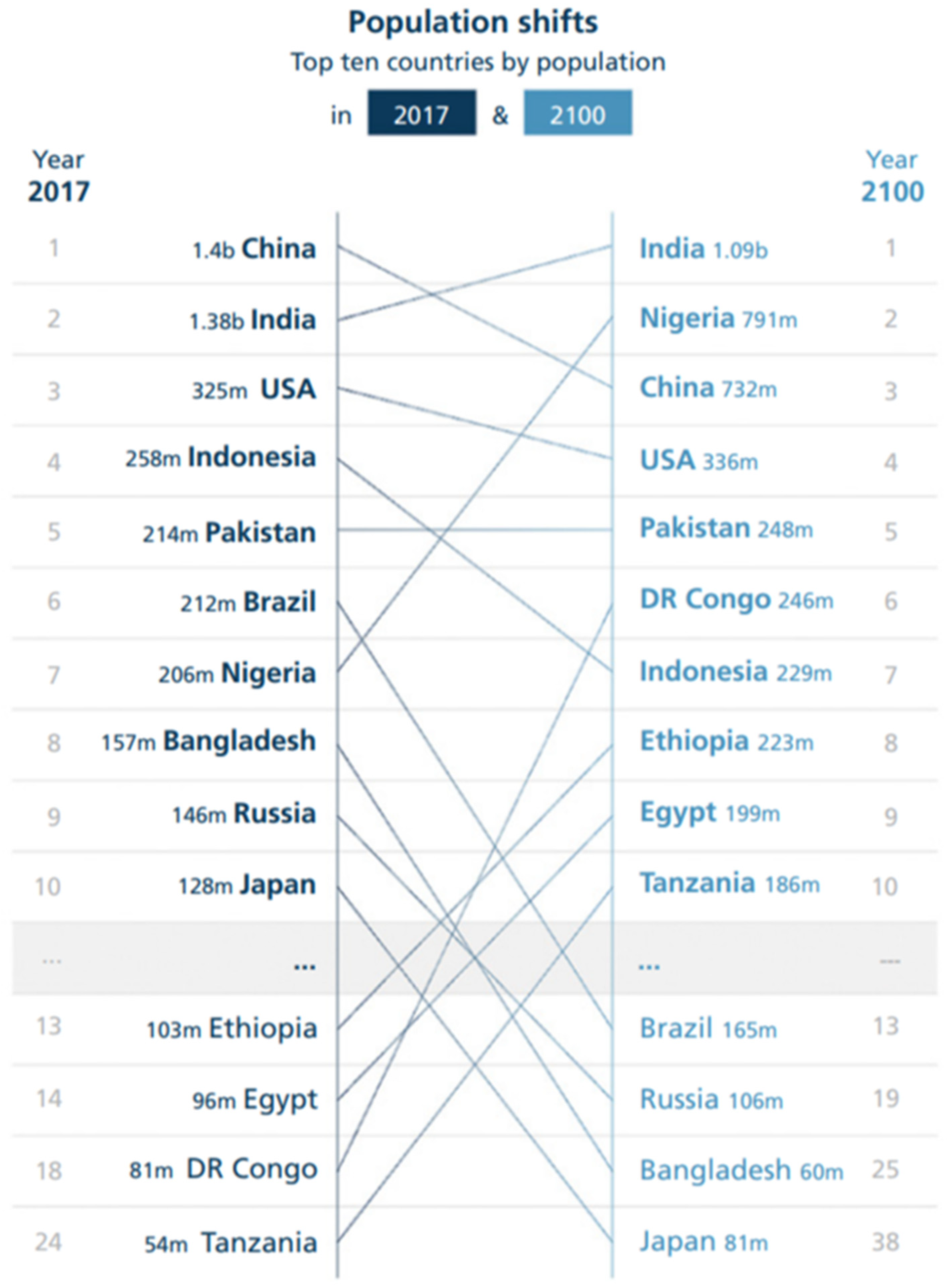
Image 3. Changing populations from 2017 to 2100. India and China stay where they are now, with a drastic reduction in its populations. Nigeria more than triples its population and, surprisingly, Brazil, a middle-income country, has almost the same descent curve as Japan. Source (Vollset et all. (2020).
2. Discussion
2.1. Global Health Initiatives and Policies
The United Nations Sustainable Development Goals (SDGs) include a specific target to reduce premature mortality from NCDs by one-third by 2030 (United Nations, 2015). Achieving this target requires a multi-sectoral approach that addresses the social, economic, and environmental determinants of health.
The WHO has also developed a Global Action Plan for the Prevention and Control of NCDs, which outlines a set of cost-effective interventions known as "best buys." These interventions include measures to reduce tobacco and alcohol use, promote healthy diets, and improve physical activity levels. The action plan also emphasizes the need for robust health systems that can provide chronic care management and ensure access to essential medicines and technologies (WHO, 2013).
- National and Regional Efforts
Many countries have implemented national policies and programs to address NCDs. For example, tobacco control measures such as taxation, advertising bans, and smoke-free laws have been effective in reducing smoking rates. Similarly, initiatives to promote healthy diets and physical activity are being integrated into public health strategies worldwide (Montgomery, 2024a). Regional collaborations and partnerships are also critical in addressing NCDs, as they facilitate the sharing of best practices and resources (Nugent et al., 2018).
Strengthening health systems to address NCDs requires a focus on primary care, prevention, and integrated care models. Primary care providers are often the first point of contact for individuals with NCDs, and they play a crucial role in early detection, management, and referral. Integrated care models that combine prevention, treatment, and rehabilitation services can improve health outcomes and reduce healthcare costs (Beaglehole et al., 2011).
Health education and promotion are essential components of NCD prevention. Public health campaigns that raise awareness about the risks of NCDs and promote healthy lifestyles can empower individuals to make informed health choices. School-based programs, workplace wellness initiatives, and community health interventions can all contribute to reducing the burden of NCDs (Nutbeam, 2000).
- Research and Innovation
Continued research is needed to better understand the epidemiology of NCDs and develop effective interventions. Research priorities include identifying the genetic, environmental, and behavioral factors that contribute to NCDs, as well as evaluating the impact of policies and interventions. Innovation in medical technologies, treatments, and healthcare delivery models can also play a critical role in addressing the NCD burden (Lozano et al., 2013).
The global burden of disease has shifted dramatically, with NCDs now representing the leading cause of morbidity and mortality worldwide. This shift presents significant challenges for public health systems, particularly in LMICs. However, it also offers opportunities for innovation and collaboration in addressing the underlying risk factors and determinants of health. By focusing on prevention, early detection, and comprehensive care, the global community can make meaningful progress in reducing the burden of NCDs and improving health outcomes for all.
2.3. The Alarming Tendencies of Non-Communicable Diseases and the Role of Artificial Intelligence
Non-communicable diseases (NCDs) have become a significant global health challenge, causing a substantial burden on healthcare systems and economies. This discussion explores the regions most affected by these tendencies, potential solutions to mitigate their impact, and the pivotal role of emerging technologies, particularly artificial intelligence (AI), in addressing these issues. Special emphasis is placed on neurological diseases due to aging and the rise of obesity, as well as the potential for AI to revolutionize healthcare over the next five years.
- Regional Disparities in NCD Burden
- High-Income Countries
High-income countries, such as the United States, Canada, and many Western European nations, have some of the highest rates of NCDs. The prevalence of cardiovascular diseases, cancers, diabetes, and neurological disorders like Alzheimer's disease is particularly high. Factors contributing to this include aging populations, high levels of obesity, sedentary lifestyles, and unhealthy dietary habits.
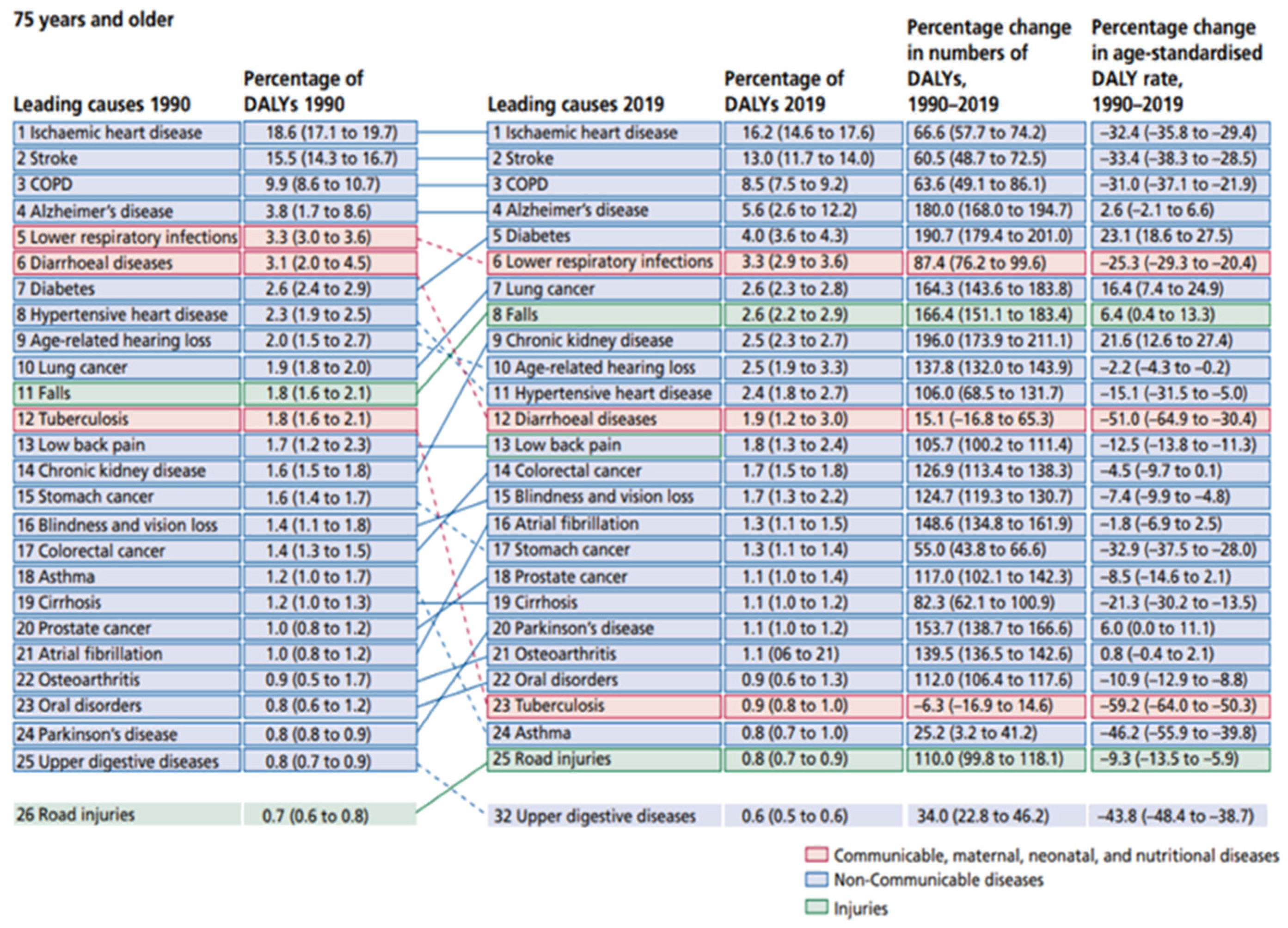
Image 3. Changes from 1990 and 2019 for individuals above 75 years old, just before the first case that initiated the global pandemics. We see a drastic change to NCD’s as cause of mortality. Source: reproduced from GBD 2019 Diseases and Injuries Collaborators (2020).
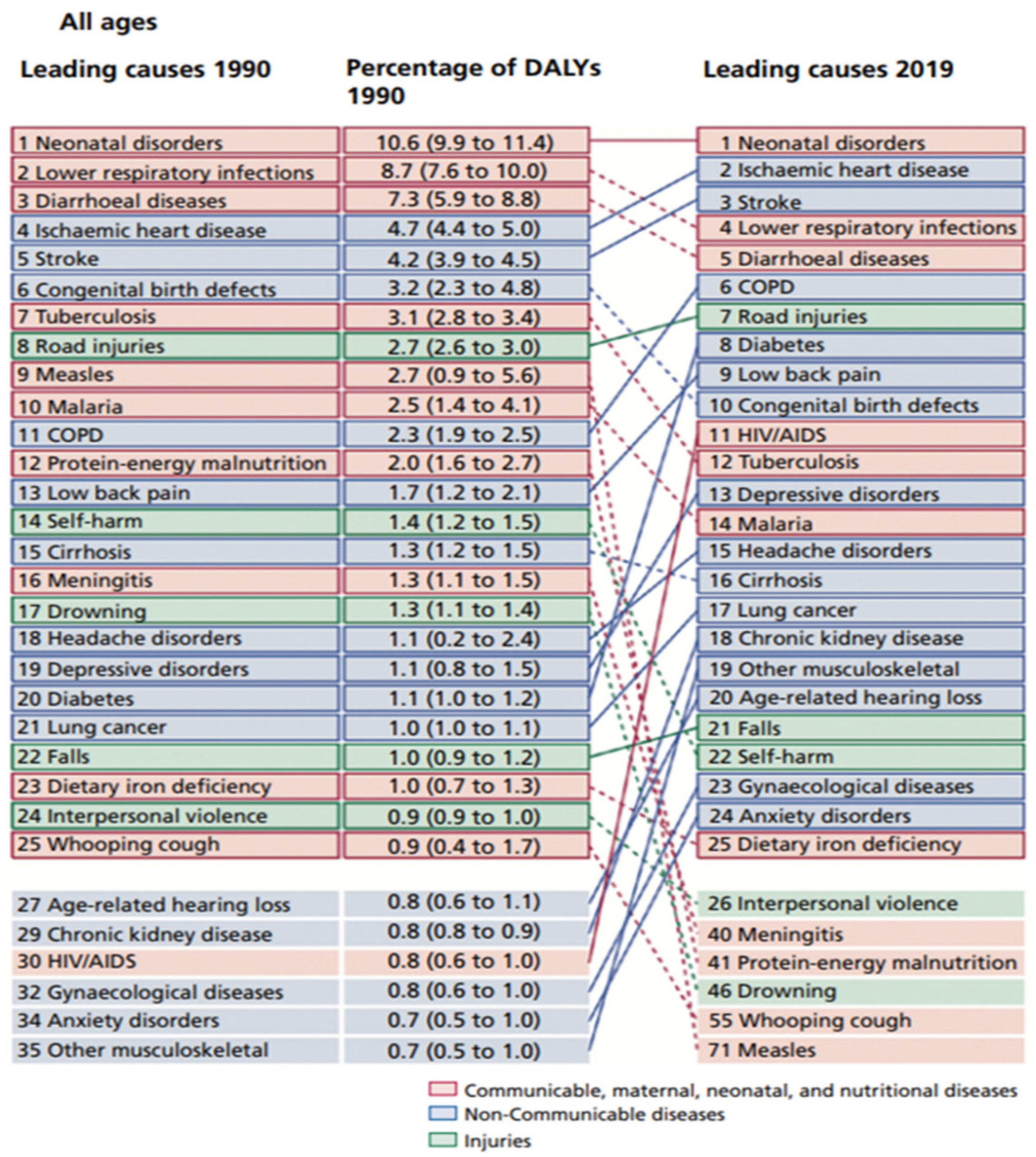
Image 4. Changes from 1990 and 2019 for all individuals, just before the first case that initiated the global pandemics. Though less drastic, we see a movement towards NCD’s. Source: reproduced with permission from GBD 2019 Diseases and Injuries Collaborators (2020).
- Explanation:
- High Income Countries
In the United States, heart disease remains the leading cause of death, accounting for approximately 655,000 deaths each year (Benjamin et al., 2019). Europe has some of the highest cancer incidence rates, with over 3.9 million new cases and 1.9 million deaths annually (Ferlay et al., 2020).
The prevalence of diabetes in high-income countries is significant, with approximately 10% of the population affected in the United States (Centers for Disease Control and Prevention [CDC], 2020).
- Low- and Middle-Income Countries (LMICs)
LMICs are experiencing a rapid rise in NCDs, which is compounded by the continued burden of infectious diseases. Countries in Sub-Saharan Africa, South Asia, and parts of Latin America are particularly affected.
In India, cardiovascular diseases have become the leading cause of death, responsible for 28.1% of total deaths in 2016 (India State-Level Disease Burden Initiative CVD Collaborators, 2018). China has the highest number of adults with diabetes, with over 116 million cases in 2019 (International Diabetes Federation [IDF], 2019). Africa is witnessing a rise in cancer incidence, partly due to lifestyle changes and increased exposure to risk factors such as tobacco and alcohol (Bray et al., 2018).
2.4. The Growing Burden of Neurological Diseases
- Alzheimer's Disease and Other Dementias
Neurological diseases, particularly Alzheimer's disease and other dementias, are a growing concern due to aging populations. Alzheimer's disease affects approximately 50 million people worldwide, with nearly 10 million new cases each year (World Health Organization [WHO], 2020).
- High-Income Countries
In the United States, Alzheimer's disease is the sixth leading cause of death, with over 5 million Americans living with the disease (Alzheimer's Association, 2020).
- Low and Middle Income Countries
The burden of dementia is also rising in LMICs, where awareness and healthcare infrastructure are often lacking. By 2050, it is estimated that over 70% of people with dementia will live in LMICs (Prince et al., 2015).
- Parkinson's Disease
Parkinson's disease is another neurological disorder that is increasing with aging populations. It affects approximately 6.1 million people globally, and this number is expected to double by 2040 (Dorsey et al., 2018).
2.5. The Rise of Obesity
Obesity is a major risk factor for NCDs, including cardiovascular diseases, diabetes, and certain cancers. The global prevalence of obesity has nearly tripled since 1975, with over 650 million adults and 340 million children and adolescents classified as obese in 2016 (World Health Organization [WHO], 2021). The United States has one of the highest obesity rates, with over 40% of adults classified as obese (Hales et al., 2020).
Obesity is also rising in LMICs, driven by urbanization, changes in dietary patterns, and reduced physical activity. Countries like Mexico and South Africa are experiencing significant increases in obesity rates (Swinburn et al., 2019).
2.6. Potential Solutions to Mitigate NCD Burden
- Public Health Policies, Interventions and the Crucial Role of AI
Effective public health policies are crucial in addressing NCDs. These policies should focus on prevention, early detection, and management of chronic conditions.
- Implementing strict tobacco control measures, including taxation, advertising bans, and smoking cessation programs, can reduce smoking rates and associated NCDs (World Health Organization [WHO], 2020).
- Nutrition and Physical Activity: Promoting healthy diets and regular physical activity through public health campaigns, school programs, and community initiatives can help combat obesity and related diseases (World Health Organization [WHO], 2021).
- Healthcare Access: Ensuring access to healthcare services, particularly in LMICs, is essential for early detection and treatment of NCDs. This includes improving primary care services and ensuring the availability of essential medicines (World Health Organization [WHO], 2013).
- Technological innovations, particularly in the field of artificial intelligence (AI), hold great promise for addressing NCDs. AI will enhance early diagnosis, personalize treatment plans, and improve healthcare delivery.
- Early Diagnosis and Screening: AI-driven diagnostic tools can improve the early detection of NCDs, including neurological diseases and cancers. Machine learning algorithms are already been used to analyze medical images, genomic data, and patient records to identify patterns and predict disease risk.
- Cancer Screening: AI algorithms have demonstrated the ability to detect cancers, such as breast and lung cancer, at earlier stages through the analysis of imaging data (McKinney et al., 2020).
- Neurological Diseases: AI can assist in the early diagnosis of Alzheimer's disease by analyzing neuroimaging data and identifying subtle changes in the brain that indicate the onset of the disease (Ding et al., 2020).
- Personalized Medicine: AI enables the development of personalized treatment plans based on individual patient data, including genetics, lifestyle, and environmental factors. This approach can improve treatment outcomes and reduce adverse effects.
- Precision Medicine: AI can identify the most effective treatments for individual patients, such as selecting the optimal chemotherapy regimen for cancer patients based on genetic profiles (Topol, 2019).
- Chronic Disease Management: AI-powered applications can help manage chronic conditions like diabetes by providing real-time monitoring, personalized recommendations, and alerts for healthcare providers (Krittanawong et al., 2017).
- Healthcare Delivery and Management: AI can streamline healthcare delivery and improve resource allocation, particularly in resource-constrained settings.
- Telemedicine: AI-powered telemedicine platforms can provide remote consultations, monitor patient health, and deliver care to underserved populations (Dorsey et al., 2020). It´s already a source of knowledge for large startct of the world population, a fact that may contribute to decrease medical-patient information bias (Montgomery, 2023).
- Resource Allocation: AI can optimize resource allocation in hospitals and healthcare systems by predicting patient admissions, managing bed capacity, and reducing wait times (Yoon et al., 2020). This optimization is already happening in several countries like Brazil and USA, with drastic cuts in costs and faster attending to urgent diseased patients.
2.7. Exponential Growth of Artificial Intelligence
- Current Capabilities and Limitations
AI technologies have made significant advancements in recent years, driven by improvements in machine learning, natural language processing, and data analytics. However, there are still limitations to be addressed.
- Data Quality and Availability
The effectiveness of AI algorithms depends on the quality and availability of data. In many healthcare settings, data is fragmented, incomplete, or inaccessible due to privacy concerns (Chen & Asch, 2017).
- Interpretability and Trust
AI models often function as "black boxes," making it difficult for healthcare providers to understand and trust their recommendations. Improving the interpretability of AI systems is crucial for their adoption in clinical practice (Liang & Zhang, 2020).
- Projected Developments in the Next Five Years
Despite that, and with reasonable certainty, the next five years are expected to see exponential growth in AI capabilities, driven by advancements in computing power, data availability, and algorithmic improvements. We are maybe approaching a new paradigm in civilization, with major and unpredictable shocks all over society tracts.
Enhanced Algorithms: Improved machine learning algorithms, including deep learning and reinforcement learning, will enable more accurate and efficient analysis of complex healthcare data (LeCun et al., 2015). AI will become more integrated into healthcare systems, with seamless interoperability between electronic health records (EHRs), diagnostic tools, and treatment platforms (Topol, 2019). If we analyze it rationally, many high and low complex healthcare activities are already replaceable with far better results by AI. As it is happening with autonomous cars, it only takes the time for society acceptance of this facts.
The development of robust regulatory and ethical frameworks will have to ensure the safe and equitable deployment of AI in healthcare, addressing concerns related to data privacy, bias, and accountability (Price & Cohen, 2019).
- Bias and Fairness
AI algorithms can perpetuate or exacerbate existing biases in healthcare, leading to inequitable outcomes. Ensuring that AI systems are fair and unbiased is critical for their ethical deployment. For example, training data from distance places and different populations (until now almost only white north Europeans) is an obvious example.
Regular auditing of AI algorithms for bias and fairness, as well as the development of diverse training datasets, can help mitigate these issues (Obermeyer et al., 2019).
Ensuring transparency in AI decision-making processes and establishing clear accountability mechanisms can enhance trust and acceptance of AI technologies in healthcare (Liang & Zhang, 2020).
3. Conclusion
The global burden of non-communicable diseases, particularly neurological diseases and obesity, presents significant challenges for healthcare systems worldwide. However, the integration of artificial intelligence into healthcare offers promising solutions to address these issues. AI can enhance early diagnosis, personalize treatment plans, and improve healthcare delivery, ultimately reducing the burden of NCDs. The exponential growth of AI technologies over the next five years holds great potential for transforming healthcare and improving patient outcomes. However, it is crucial to address ethical and regulatory considerations to ensure the responsible and equitable use of AI in healthcare. By leveraging the power of AI, the global community can make meaningful progress in combating NCDs and improving health outcomes for all.
Conflicts of Interest
The Author claims no conflicts of interest.
References
- Alzheimer's Association. (2020). 2020 Alzheimer's disease facts and figures. Alzheimer's & Dementia, 16(3), 391-460.
- Beaglehole, R., Bonita, R., Horton, R., Adams, C., Alleyne, G., Asaria, P.,... & Watt, J. (2011). Priority actions for the non-communicable disease crisis. The Lancet, 377(9775), 1438-1447.
- Benjamin, E. J., Muntner, P., Alonso, A., Bittencourt, M. S., Callaway, C. W., Carson, A. P.,... & Virani, S. S. (2019). Heart disease and stroke statistics—2019 update: a report from the American Heart Association. Circulation, 139(10), e56-e528.
- Benjamin, E. J., Muntner, P., Alonso, A., Bittencourt, M. S., Callaway, C. W., Carson, A. P.,... & Virani, S. S. (2019). Heart disease and stroke statistics—2019 update: a report from the American Heart Association. Circulation, 139(10), e56-e528.
- Bray, F., Ferlay, J., Soerjomataram, I., Siegel, R. L., Torre, L. A., & Jemal, A. (2018). Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: a cancer journal for clinicians, 68(6), 394-424.
- Bray, F., Ferlay, J., Soerjomataram, I., Siegel, R. L., Torre, L. A., & Jemal, A. (2018). Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: a cancer journal for clinicians, 68(6), 394-424.
- Centers for Disease Control and Prevention (CDC). (2020). National Diabetes Statistics Report, 2020. Centers for Disease Control and Prevention.
- Chen, J. H., & Asch, S. M. (2017). Machine learning and prediction in medicine—precision medicine or blunt instruments? New England Journal of Medicine, 376(23), 2211-2213.
- Cho, N. H., Shaw, J. E., Karuranga, S., Huang, Y., da Rocha Fernandes, J. D., Ohlrogge, A. W., & Malanda, B. (2018). IDF Diabetes Atlas: Global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Research and Clinical Practice, 138, 271-281.
- Daneault, J. F., Gagnon, J. F., Duval, C., Desautels, A., Gosselin, N., Tampieri, D.,... & Montplaisir, J. (2019). Diagnostic accuracy of a deep learning model for the prediction of Parkinson's disease using clinical data. Movement Disorders, 34(8), 1149-1158.
- Demiris, G., Rantz, M., Aud, M., Marek, K. D., Tyrer, H. W., & Stahl, S. M. (2018). Older adults' attitudes towards smart home technologies: Implications for research and practice. Journal of Telemedicine and Telecare, 13(4), 232-234.
- Ding, Y., Zhou, X., He, Z., & Zeng, J. (2020). Deep learning for Alzheimer's disease: a systematic review. Frontiers in Neuroscience, 14, 887.
- Dorsey, E. R., Achey, M. A., Beck, C. A., Beran, D. B., Biglan, K. M., Boyd, C. M.,... & Sherer, T. (2018). National randomized controlled trial of virtual house calls for Parkinson disease. Neurology, 90(15), e1278-e1285.
- Dorsey, E. R., Glidden, A. M., Holloway, M. R., Birbeck, G. L., & Schwamm, L. H. (2020). Teleneurology and mobile technologies: access, equity, and cost. Annals of Neurology, 87(5), 655-665.
- Ezzati, M., Lopez, A. D., Rodgers, A., Hoorn, S. V., & Murray, C. J. (2005). Selected major risk factors and global and regional burden of disease. The Lancet, 360(9343), 1347-1360.
- Ferlay, J., Ervik, M., Lam, F., Colombet, M., Mery, L., Pincon, A.,... & Bray, F. (2020). Global Cancer Observatory: Cancer Today. International Agency for Research on Cancer.
- Forouzanfar, M. H., Liu, P., Roth, G. A., Ng, M., Biryukov, S., Marczak, L.,... & Murray, C. J. (2017). Global burden of hypertension and systolic blood pressure of at least 110 to 115 mm Hg, 1990-2015. JAMA, 317(2), 165-182.
- Hales, C. M., Carroll, M. D., Fryar, C. D., & Ogden, C. L. (2020). Prevalence of obesity and severe obesity among adults: United States, 2017–2018. NCHS Data Brief, 360, 1-8.
- Hssayeni, M. D., Jimenez, S., Shaikh, M. F., & Ghoraani, B. (2020). A deep learning approach for prediction of freezing of gait in Parkinson’s disease. IEEE Journal of Biomedical and Health Informatics, 24(5), 1470-1478.
- Kowal, P., Dowd, J. E., & Chatterji, S. (2016). Ageing and adult health status in eight lower-income countries: the INDEPTH WHO-SAGE collaboration. Global Health Action, 9(1), 29405.
- Lozano, R., Naghavi, M., Foreman, K., Lim, S., Shibuya, K., Aboyans, V.,... & AlMazroa, M. A. (2013). Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. The Lancet, 380(9859), 2095-2128.
- Marmot, M., Friel, S., Bell, R., Houweling, T. A., Taylor, S., & Commission on Social Determinants of Health. (2008). Closing the gap in a generation: health equity through action on the social determinants of health. The Lancet, 372(9650), 1661-1669.
- Montgomery, R. M.; Aprahamian, I. (2018). Thesis: Fragilidade e Doença de Parkinson. (2018). University of São Paulo. [CrossRef]
- (Montgomery, R. M. 2024). The Shift from Aerobic to Anaerobic Strength Training A Paradigm Change in Preventing Frailty, Morbidity, and Mortality in Older Adults. (2024). [CrossRef]
- (Montgomery, R. M. 2024). A Comparative Analysis of Mortality Rates in Public vs. Private Healthcare Systems Worldwide"(2024). [CrossRef]
- Murray, C. J., Aravkin, A. Y., Zheng, P., Abbafati, C., Abbas, K. M., Abbasi-Kangevari, M.,... & Vos, T. (2020). Global burden of 87 risk factors in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. The Lancet, 396(10258), 1223-1249.
- Nugent, R., Bertram, M. Y., Jan, S., Niessen, L. W., Sassi, F., Jamison, D. T.,... & Zheng, Y. (2018). Investing in non-communicable disease prevention and management to advance the Sustainable Development Goals. The Lancet, 392(10152), 1036-1038.
- Nutbeam, D. (2000). Health literacy as a public health goal: a challenge for contemporary health education and communication strategies into the 21st century. Health Promotion International, 15(3), 259-267.
- United Nations. (2015). Transforming our world: the 2030 Agenda for Sustainable Development. United Nations.
- Vos, T., Lim, S. S., Abbafati, C., Abbas, K. M., Abbasi, M., Abbasi-Kangevari, M.,... & Murray, C. J. (2020). Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. The Lancet, 396(10258), 1204-1222.
- World Health Organization. (2013). Global action plan for the prevention and control of noncommunicable diseases 2013-2020. World Health Organization.
- World Health Organization. (2020). Tobacco. World Health Organization.
- World Health Organization. (2021). Cardiovascular diseases (CVDs). World Health Organization.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



