
Submitted:
13 September 2024
Posted:
14 September 2024
You are already at the latest version
Abstract
Understanding the interplay between infections and severe acute malnutrition is critical in attaining good clinical outcomes in managing malnourished children. However, review studies describing the profile of the associated pathogens in the malnourished African pediatric population are sparse in the literature. We aimed to identify the spectrum of pathogens from studies reporting infections in malnourished African children, as well as the antibiotic resistance pattern and clinical outcomes. A systematic literature of the PubMed database was conducted following PRISMA guidelines from January 2001 to June 2024. The search algorithm was ((marasmus) OR (kwashiorkor) OR (severe acute malnutrition) OR (protein energy malnutrition)) AND (Africa). For a more comprehensive retrieval, an additional search algorithm was deployed: (HIV OR tuberculosis) AND (severe acute malnutrition). We included 67 studies conducted between 2001 and 2024. Most of the studies were from East Africa (n=53, 79.1%) and Southern Africa (n=5, 7.4%). A total of 7,056 pathogens were identified comprising 3,030 Viruses, 2,381 bacteria, 1,452 parasites and 193 fungal pathogens. The predominant pathogens were HIV, Mycobacterium tuberculosis, and malaria parasites accounting for 42.5%, 25.2%, and 17.1% respectively. Antibiotic susceptibility testing was documented in only three studies. Fatality rates were reported in 49 studies and ranged from 2% to 56% regardless of the category of pathogen. This review affirms the deleterious effect of infections in malnourished patients and suggests a gross underdiagnosis as studies were found from only 17 (31.5%) African countries. Moreover, data on fungal infections in malnourished African children was nearly absent despite being at risk. There is also a need to prioritize research investigating African children with severe acute malnutrition for fungal infections besides other opportunistic pathogens and improve the availability of diagnostic tools and the optimized usage of antibiotics through the implementation of antimicrobial stewardship programmes.
Keywords:
Severe acute malnutrition
; tuberculosis
; HIV/AIDS
; immunocompromised
; Africa
1. Introduction
Severe acute malnutrition (SAM) is a significant global health issue, defined by the World Health Organization (WHO) and United Nations International Children’s Emergency Fund (UNICEF) based on specific criteria: a weight-for-height z-score (WHZ) below -3, a mid-upper arm circumference (MUAC) under 115 mm, or the presence of nutritional edema [1]. According to UNICEF (2022), 45 million children under five were impacted by wasting, with 13.7 million categorized as severely wasted [2]. The burden of SAM is predominantly concentrated in South Asia and sub-Saharan Africa, where factors such as drought, armed conflict, poverty, food insecurity, inadequate healthcare infrastructure, and socioeconomic instability exacerbate the prevalence of malnutrition [3]. Despite global efforts, the continent continues to struggle with high rates of undernutrition, micronutrient deficiencies, obesity, and non-communicable diseases. According to a recent report by United Nations agencies, nearly 282 million people in Africa, or about 20% of the population, were undernourished in 2022 [4]. Malnutrition rates vary significantly across African regions, with sub-Saharan Africa bearing the heaviest burden. In Eastern Africa, countries such as Ethiopia, South Sudan, and Somalia have some of the highest stunting rates, often exceeding 30% [5].
The role of climate change in exacerbating SAM is particularly concerning. The Intergovernmental Panel on Climate Change (IPCC) reports that global warming is intensifying food insecurity, especially in tropical regions where 95% of malnourished individuals reside [6]. Rising temperatures and more frequent extreme weather events, such as droughts, lead to reduced agricultural productivity, directly contributing to increased rates of malnutrition. The interconnectedness of climate change and food security highlights the need for comprehensive approaches that address environmental factors in the fight against malnutrition.
SAM leads to physical wasting and severely compromises the immune system, increasing susceptibility to infections. These infections—whether bacterial, viral, parasitic, or fungal—tend to be more frequent and severe in SAM patients, further elevating metabolic demands and depleting already scarce nutrient reserves. This creates a vicious cycle where malnutrition and infection exacerbate each other, complicating recovery and worsening health outcomes [7]. Infectious diseases pose significant health risks, particularly in regions afflicted by high rates of malnutrition, such as sub-Saharan Africa. The widespread prevalence of malnutrition and opportunistic infections in sub-Saharan Africa underscores the formidable health challenges facing the region. The immune dysfunction associated with SAM can lead to a higher risk of morbidity and mortality from common childhood illnesses such as diarrhea and pneumonia [7]. It is a major public health issue in Africa, affecting millions of people, particularly children under five [8]. However, large-scale reviews describing the spectrum of pathogens in children with SAM are lacking in the literature, particularly for the African setting. In addition, data on the susceptibility profile of these pathogens are fragmented in the literature. Previous reviews focused on undernutrition and associated factors among HIV-infected children in sub-Saharan Africa [9], while reviews summarizing data on pathogens in African children with SAM have largely been focused on HIV [10,11]. Studies on other groups of pathogens in this at-risk group and their antimicrobial-resistance pattern are lacking. Thus, the overarching aim of this review was to highlight the burden of pathogens reported in African children with SAM, and the need to drive antimicrobial stewardship practices in this setting and invariably improve clinical outcomes.
2. Materials and Methods
2.1. Study Design
We conducted a scoping review of literature adhering to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) guidelines [12].
2.2. Search Strategy
We conducted a systematic literature search of the PubMed database between January 2001 to June 2024 (BEE). The search algorithm was ((marasmus) OR (kwashiorkor) OR (severe acute malnutrition) OR (protein energy malnutrition)) AND (Africa). An additional search algorithm was deployed for a more comprehensive retrieval: (HIV OR tuberculosis) AND (severe acute malnutrition). No language restrictions were applied.
2.3. Inclusion and Exclusion Criteria
All articles with primary data on pathogens in malnourished African children were eligible for inclusion. Studies reporting infections in malnourished children outside Africa or in children who were not classified as ‘malnourished’ were excluded. Review articles were also excluded.
2.4. Selection Process
Two authors (BEE and OFA) conducted the initial screening of titles and abstracts, focusing on studies reporting pathogens in malnourished African children. Selected studies were further screened, and duplicates were removed as more than one search algorithm was deployed. Full-text assessment was thereafter performed and followed by data extraction. Discrepancies in inclusion/exclusion decisions were resolved through a discussion.
2.5. Data Extraction
Data on study authors, study location, (country and region in Africa), study period, study design, age range, pathogens, clinical presentation, investigation/diagnostic measures, and treatment outcomes (fatality/mortality rates) were extracted. Four authors (BEE, OFA, UIE, and AGO) performed data extraction, and any indifferences revolved by a consensus. Descriptive statistics was used to summarize the findings.
3. Results
3.1. Search Results
Our initial search yielded 1,023 articles and 311 articles following an additional search, amounting to a total of 1,334. After the selection process, 91 articles were identified as having met the inclusion criteria. Others were excluded for several reasons including lack of information regarding this review, clinical trial studies, reviews, guidelines, studies reporting infections in the non-African paediatric population, studies reporting infection in adults, amongst others. Of the 91, 31 duplicates were removed, remaining 60 articles. Seven articles were added from other sources, thus a total of 67 articles were included in this review, Figure 1.
3.2. Demographics
We included 67 studies conducted between 2001 and 2024. Data was found from only 17 (31.5%) of the 54 African countries including Ethiopia (n=25), Uganda (n=10), South Africa (n=5), Zambia (n=5), Malawi (n=3), Mozambique (n=3), Kenya (n=2), Sudan (n=2), Nigeria (n=2), Niger (n=2) and Cameroon, Senegal, Zimbabwe, Sierra Leone, Democratic Republic of Congo and Ghana (one study each). Two studies were conducted in centres located in two different countries: Kenya/Tanzania and Zambia/Zimbabwe. When stratified by regions, most of the studies were from East Africa (n=53, 79.1%) and Southern Africa (n=5, 7.4%).
3.3. Study Designs
Of the sixty-seven, the study designs were retrospective (47.8%, n=32), prospective (28.4%, n=19), cross-sectional (n=20.9%, n=14), and case-control (3%, n=2). 95.5% (n=64) were hospital-based studies, 3% (n=2) were community-based studies and 1.5% (n=1), an outpatient therapeutic programme. The study population was children with SAM in fifty-seven studies, complicated SAM in seven, a combination of SAM and moderate acute malnutrition (MAM) in two studies, and undernourished children in one study.
3.4. Pathogens
A total of 7,056 pathogens were identified. Viruses comprised 42.9% (n=3,030) and predominantly HIV (99.1%, n=3,002), bacteria, 33.7% (n=2,381), majorly Mycobacterium tuberculosis (74.7%, n=1,779), parasites, 20.6% (n=1,452), commonest amongst which was malaria parasite (83.4%, n=1,207) and fungal pathogens (2.7%, n=193). HIV infection, TB, and malaria accounted for 42.5%, 25.2%, and 17.1%. Figure 2 shows a snapshot of the number of all pathogens identified in their respective categories. Cases of infections without a mention of associated pathogens were excluded from the analysis of pathogens identified in this review. Overall, Viruses were majorly implicated followed by bacteria and parasites. Fatality rates were reported in 49 studies and ranged from 2% to 56% regardless of the category of pathogen, Table 1.
4. Discussion
SAM poses a significant public health concern, particularly affecting children under the age of five. It is characterized by extreme thinness and severe deficiencies in essential nutrients. The World Health Organization (WHO) reports that almost 16 million children globally are impacted by SAM, with a higher prevalence in sub-Saharan Africa [80]. The clinical indicators of SAM encompass substantial weight loss, low weight-for-height, and frequently, edema. The criteria for identification include mid-upper arm circumference (MUAC) and weight-for-height Z-score evaluations [1]. Children afflicted by SAM face a significantly heightened risk of mortality due to compromised immune function stemming from malnutrition [16]. Malnutrition undermines the body's defence against infections by compromising physical barriers such as the skin and mucous membranes, facilitating pathogen entry, and increasing infection risk. It also disrupts immune cell production and function, resulting in reduced T cell and B cell counts and activity, which are pivotal for an effective immune response [80]. In addition, SAM can incite an imbalance in cytokine production, thus increasing vulnerability to various diseases including pneumonia, diarrhea, tuberculosis, and opportunistic infections [81]. Also, SAM may yield long-term developmental issues, affecting physical growth and cognitive development [82]. In contrast, infections can also predispose to malnutrition in children with diarrheal disease following gastrointestinal infection. Cachexia and anaemia can also result from infections like HIV/AIDS and TB, and nutrient deprivation resulting from parasitic infections [81]. Our review highlights over five thousand cases of opportunistic infections in malnourished children living in Africa over the past two decades with HIV, Mycobacterium tuberculosis and malaria parasite being the predominant associated pathogens. A significant proportion of these data was obtained from studies conducted in East African countries and Southern Africa with few cases from West and North Africa which suggests an underestimation of the burden of infectious diseases in this at-risk group.
4.1. Viral Infection
The predominance of HIV amongst pathogens reported in malnourished African children may be associated with the high burden of HIV in Africa. As of 2022, about 25.6 million people were living with HIV in Africa accounting for more than two-thirds of the people living with HIV worldwide (WHO). Malnutrition exerts a deleterious effect on the production and functionality of immune cells, thereby diminishing the body's capacity to combat infections such as HIV. Concomitantly, economic challenges impede access to nourishing sustenance and healthcare, exacerbating malnutrition and elevating the susceptibility to HIV infection, creating a cycle that further weakens the immune system [3].
The high prevalence of HIV among SAM children may also be linked with vertical transmission [83]. Malnourished pregnant women with HIV are more likely to have higher viral loads, increasing the risk of passing the virus to their children during pregnancy, childbirth, or breastfeeding [84]. Furthermore, in regions affected by severe poverty and malnutrition, individuals may engage in high-risk behaviours such as transactional sex to obtain food or income, increasing the risk of HIV transmission [85]. HIV worsens malnutrition by causing loss of appetite, poor absorption of nutrients, and increasing metabolic demands. This sets in motion a challenging cycle where malnutrition worsens HIV outcomes, and HIV further deteriorates nutritional status, leading to rapid health decline [86]. This scenario is buttressed in a study to ascertain 52-week mortality in children discharged from hospitals for management of complicated SAM, conducted in three hospitals in Zambia and Zimbabwe. Children with underlying HIV infection were observed to have an almost 4-fold higher mortality compared with children without underlying HIV infection [20]. In Nigeria, HIV was shown to drive undernutrition as the prevalence of stunting, underweight, and wasting among the HIV-infected subjects was significantly higher compared with the controls [39]. Similarly, a Mozambican study evaluating the adherence of malnourished children to nutritional rehabilitation programs reported a higher prevalence of SAM amongst participants with underlying HIV infection [23]. Thus, besides predisposing to malnutrition, HIV infection in malnourished children is associated with fatal clinical outcomes.
4.2. Bacterial Infection
Next to HIV are bacterial infections presenting as TB, pneumonia, diarrheal disease, and urinary tract infections. The commonest among these clinical conditions was TB. TB and SAM are a major cause of mortality especially in resource-limited settings for children under the age of five years. The coexistence of both further worsened morbidities and clinical outcomes with fatality rates reaching up to 56% [16]. Moreover, children under five years have the highest risk of progressing from Mycobacterium tuberculosis infection to disease, and to disseminated forms of TB [87]. The relationship between TB and malnutrition exists in a bidirectional manner. Malnutrition heightens susceptibility to active TB by undermining cell-mediated immunity, pivotal for controlling Mycobacterium tuberculosis, or by inciting the reactivation of latent TB infections [88]. On the other hand, TB worsens malnutrition as it causes increased metabolic demands, nutrient malabsorption, and chronic inflammation. Thus, the risk of TB disease increases with undernutrition and TB can cause or worsen undernutrition [81]. One study estimated that 26% of overall TB cases in 22 high-burden countries are attributable to undernutrition [89]. Similarly, a recent review of 51 cohort studies with over 27 million participants from the six WHO regions reported undernutrition probably increases the risk of TB two-fold in the short term (< 10 years) and may also increase the risk in the long term (> 10 years) [90]. In contrast, studies included in this review revealed delayed recovery from SAM and high fatality rates in malnourished children with coexisting TB disease compared with cohorts without TB disease [16,30,31].
The high prevalence of TB in malnourished African children can be linked to several socioeconomic factors. Low socioeconomic status, overcrowded living conditions, and food insecurity are common in regions with high rates of SAM and thus contribute to the spread of TB. Additionally, natural or man-made disasters, such as conflicts and displacement, exacerbate food insecurity and poor living conditions, further increasing the risk of TB and other infectious diseases. These factors create an environment where communicable diseases can thrive, especially among individuals with compromised immune systems.
Children afflicted by both TB and SAM frequently present with chronic cough, weight loss, and fever—symptoms that conflate with those of severe malnutrition—thereby rendering diagnosis challenging [87,88]. Besides this is the difficulty in making a confirmatory diagnosis using Gene Xpert or cultures as most studies have shown these methods to be unreliable. The diagnosis of TB in the African paediatric population hinges on the ability of the attending physician to make a clinical diagnosis based on presenting symptoms and radiological presentations of the index patient with or without a confirmatory result from the laboratory. Authors opined guidelines should be designed for the diagnosis of TB in malnourished children especially in a resource-limited setting where proven diagnostic tools are often limited [15,34].
Besides Mycobacterium tuberculosis, other respiratory pathogens such as Streptococcus pneumoniae and Haemophilus influenzae also contributed to morbidities [37,62], frequently precipitating pneumonia in malnourished children. Consequently, malnourished children often experience protracted illness owing to compromised infection clearance, due to weakened respiratory muscles and diminished secretion of protective lung fluids. Furthermore, the weakened immune system in children with SAM amplifies their susceptibility and the gravity of pneumonia. In one study, lower respiratory tract infections were the most common complications second to diarrheal disease with a frequency of 42.4% (405/ 956) and associated with 1.6 times higher odds of dying compared to those who did not have lower respiratory tract infections [18]. Thus, malnutrition induces deficiencies in essential nutrients crucial for a robust immune response, further impeding the body's ability to combat respiratory infections.
4.3. Parasitic Infection
Parasitic infections were also associated with morbidities in malnourished children with malaria parasites accounting for over 80% of the cases. Besides malaria parasites, other parasites were also documented including Ascaris lumbricoides, Cryptosporidium species, Trichuris trichiura, Trichomonas intestinalis, Entamoeba histolytica, Entamoeba dispar/histolytica, Giardia intestinalis, Strongyloides stercoralis, Schistosoma haematobium, Schistosoma mansoni, and Endolimax nana [22,26,31,72]. Overall, only one study reported a significant correlation between parasite infection with clinical outcomes; a study from Ethiopia aimed at assessing the time to recovery from SAM and its predictors reported a high chance of recovery for children who had no anaemia, TB, or malaria infection at admission compared with their counterparts [30].
4.4. Fungal Infection
Data on fungal infections in children with SAM was found in only two studies further affirming the gross neglect of fungal diseases, especially in the paediatric population including Africa. As previously narrated, malnutrition not only results in nutritional deficiencies but also compromises immune function, disrupts the gut microbiota, and alters host defense mechanisms [81]. Consequently, it creates an environment conducive to fungal colonization and infection, heightening the risk for vulnerable populations. Several factors contribute to malnourished children's increased susceptibility to fungal infections; poor hygiene standards, congested living situations, limited access to clean water and sanitation facilities, and malnutrition-related immunological dysfunction, all contribute to fungal colonization and infection in children. In addition, comorbid illnesses like HIV infection raise the risk of fungal infections in malnourished children, emphasizing the importance of integrated healthcare methods that address the complex determinants of health. Despite these myriad factors, the cognizance for fungal infections is yet low compared with bacterial and viral infections as seen in this review. Contrastingly, recent estimates showed invasive fungal infections have an annual incidence of 6·5 million and account for about 3·8 million deaths globally [91]. This seeming neglect may be accounted for by the sparse data on fungal infections in malnourished children particularly in the African setting. We recommend prioritizing research investigating malnourished children for invasive mycoses to ascertain the burden of IFIs in this at-risk population, drive awareness of fungal diseases, and decrease morbidity.
4.5. Susceptibility Testing of Pathogens
The hallmark of antimicrobial stewardship (AMS) is to ensure the optimized usage of antibiotics and invariably improve clinical outcomes. Its role in preserving and protecting the currently available antibiotics and tackling antimicrobial resistance cannot be over-emphasized. Adherence to AMS strategies implies the indication for antimicrobial therapy is stated and the antibiotic sensitivity pattern of the associated pathogen is provided and deployed to manage an index case. However, in this review, we identified only three studies reporting the antibiotic susceptibility profile of the associated pathogens (bacteria). This is yet indicative of the existing gaps regarding antimicrobial usage in a resource-limited setting like Africa and the need to prioritize funding for innovative studies seeking to explore mechanisms or approaches to limit the exposure of malnourished patients to infectious diseases while setting up and ensuring adherence to AMS programs.
In one of the three, authors reported a high level of resistance to commonly used antibiotics and advocated for clinical trials to determine the most feasible combination of antibiotics for managing bacteraemia in severely malnourished children [37]. In another study, authors suggested an increased investment in antibiotic stewardship programmes, in the face of increasing rates of drug-resistant bacterial infections amongst HIV-infected children with SAM [62]. On the other, the authors emphasized the need to tackle the emergence of antibiotic-resistant bacteria by improving diagnostics, ensuring infection control practices, and reinforcing regional antimicrobial resistance surveillance [22].
4.6. Clinical Outcomes and Treatment Relapse
Regardless of the setting, whether studies were hospital or community-based, the treatment outcomes were largely influenced by comorbidities and predominantly of infectious origin [13,14,16,20,21,25,27,28,31,32,33,35,44,45,54]. Regarding treatment relapse, an Ethiopian study reported the odds of SAM relapse was significantly higher in children with mothers who had no exposure to education and promotion about infant and young child feeding practices, children who were not fully immunized for their age, and children with mid-upper arm circumference of < 12.5 cm at discharge than their counterparts [24]. Similarly, another study reported a lower chance of recovery among children who were not fully vaccinated [30]. Yet in another study, the time to recovery from SAM was delayed in children with comorbidities such as HIV, TB and pneumonia [42]. The authors recommend the provision of supplementary food for children with low MUAC at discharge, the promotion of nutrition education, and the improvement of child immunization services and coverage to help reduce SAM relapse [24]. In addition, Special emphasis should be given to prevent and treat comorbidities [42].
5. Limitations
Some studies reported comorbidities such as pneumonia, diarrhoea, anaemia, gastroenteritis, urinary tract infections, respiratory tract infections, dysentery, meningitis or sepsis without specifying the associated pathogen which may have undermined the burden of pathogens identified in this review. Also, the diagnosis of TB was presented in some studies as a clinical diagnosis. A confirmatory diagnosis like the Gene Xpert test or culture or lipoarabinomannan assay was lacking. However, having reviewed a significant number of cases from over 60 studies in Africa within the past two decades, we affirm that the findings from this index review can be applied to encourage research on pathogens in African children with SAM, strengthening antimicrobial stewardship programmes in this setting and invariably decrease morbidity and mortality.
6. Conclusion
Ensuring early and accurate diagnosis and treatment of infections in severely malnourished patients is critical to obtaining good clinical outcomes. Strengthening healthcare systems, particularly in resource-limited settings, is crucial to ensuring that SAM patients receive timely and effective treatment for infections. In addition, public health strategies that integrate nutrition and infection control, such as immunization programs and improved sanitation, are essential components in reducing the global burden of SAM.
Author Contributions
Bassey E. Ekeng: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing-original draft, Writing- review & editing. Olufunke F. Adedokun: Data curation, Formal analysis, Investigation, Methodology, Resources, Validation, Visualization, Writing- review & editing. Vivien M. Otu: Investigation, Methodology, Visualization, Resources, Writing- review & editing. Stella T. Chukwuma: Investigation, Formal analysis, Visualization, Resources, Writing- review & editing. Agatha G. Okah: Data curation, Investigation, Formal analysis, Validation, Visualization Rsesources, Writing- review & editing. Osamagbe A. Asemota: Methodology, Investigation, Visualization, Resources, Writing- review & editing Ubokobong I. Eshiet: Data curation, Methodology, Formal analysis, visualization, Resources, Writing- review & editing. Akpan U. Morgan: Methodology, Investigation, Visualization, Resources, Writing- review & editing. Rosa E. Nwagboso: Investigation, Formal analysis, Visualization, Resources, Writing- review & editing. Eti N. Ebiekpi: Methodology, Investigation, Visualization, Resources, Writing- review & editing. Emmanuella Umoren: Methodology, Investigation, Visualization, validation, Resources, Writing- review & editing. Edet O. Usun: Investigation, Formal analysis, Visualization, Resources, Writing- review & editing
Institutional Review Board Statement
Not applicable
Informed Consent Statement
Not applicable
Data Availability Statement
All underlying data have been included in the manuscript
Conflicts of Interest
The authors declare no conflicts of interest.
References
- André B, Measuring the Burden of Severe Acute Malnutrition: Current Challenges. Global Nutrition Report 2022. Available at https://globalnutritionreport.org/blog/measuring-burden-severe-acute-malnutrition-current-challenges/. Assessed :10th August 2024.
- United Nations Children’s Fund (UNICEF), Stunting has declined steadily since 2000 – but faster progress is needed to reach the 2030 target. Wasting persists at alarming rates and overweight will require a reversal in trajectory if the 2030 target is to be achieved. Unicef,2023. Available: https://data.unicef.org/topic/nutrition/malnutrition/. Accessed :10th August 2024.
- Black RE, Victora CG, Walker SP, Bhutta ZA, Christian P, de Onis M, et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. The Lancet. 2013; 382(9890): 427-451. [CrossRef]
- Madhumita Paul .Nearly 282 million people in Africa were undernourished in 2022: UN https://www.downtoearth.org.in/news/africa/nearly-282-million-people-in-africa-were-undernourished-in-2022-un-93345.Accessed 25/5/24.
- UNICEF, WHO & World Bank Group (2018) Levels and Trends in Child Malnutrition. Geneva: World Health Organization; available at https://www.who.int/nutgrowthdb/2018-jme-brochure.pdf (accessed May 2024).
- Moyer JD, Bohl DK, Petry C, Scott A, Solórzano JR, Kuhn R. The persistent global burden of severe acute malnutrition: Cross-country estimates, models and forecasts. Global Transitions. 2020;2:167-79. [CrossRef]
- Walson JL, Berkley JA. The impact of malnutrition on childhood infections. Curr Opin Infect Dis. 2018;31(3):231-236. [CrossRef]
- Otiti MI, Allen SJ. Severe acute malnutrition in low-and middle-income countries. Paediatrics and Child Health. 2021;31(8):301-7. [CrossRef]
- Nigussie J, Girma B, Molla A, Mareg M, Mihretu E. Under-nutrition and associated factors among children infected with human immunodeficiency virus in sub-Saharan Africa: a systematic review and meta-analysis. Arch Public Health. 2022;80(1):19. [CrossRef]
- Fergusson P, Tomkins A. HIV prevalence and mortality among children undergoing treatment for severe acute malnutrition in sub-Saharan Africa: a systematic review and meta-analysis. Trans R Soc Trop Med Hyg. 2009;103(6):541-8. [CrossRef]
- Desyibelew HD, Bayih MT, Baraki AG, Dadi AF. The recovery rate from severe acute malnutrition among under-five years of children remains low in sub-Saharan Africa. A systematic review and meta-analysis of observational studies. PLoS One. 2020;15(3):e0229698. [CrossRef]
- Tricco AC, Lillie E, Zarin W, O'Brien KK, Colquhoun H, Levac D, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018,169(7):467-473.
- De Maayer T, Saloojee H. Clinical outcomes of severe malnutrition in a high tuberculosis and HIV setting. Arch Dis Child. 2011;96(6):560-4. [CrossRef]
- Girum T, Kote M, Tariku B, Bekele H. Survival status and predictors of mortality among severely acute malnourished children< 5 years of age admitted to stabilization centers in Gedeo Zone: a retrospective cohort study. Therapeutics and clinical risk management. 2017:101-10. [CrossRef]
- Ide LE. Prevalence of tuberculosis among children with severe acute malnutrition at Ola during Children’s Hospital in Freetown Sierra Leone. J Adv Med Med Res. 2019;30(3):1-7. [CrossRef]
- Kasonka L, Munthali G, Rehman AM, Chisenga M, Wells S, Wells JCK, et al. Anthropometry, body composition and chronic disease risk factors among Zambian school-aged children who experienced severe malnutrition in early childhood. Br J Nutr. 2022;128(3):453-460. [CrossRef]
- Osório DV, Munyangaju I, Muhiwa A, Nacarapa E, Nhangave AV, Ramos JM. Lipoarabinomannan Antigen Assay (TB-LAM) for Diagnosing Pulmonary Tuberculosis in Children with Severe Acute Malnutrition in Mozambique. J Trop Pediatr. 2021;67(3):fmaa072. [CrossRef]
- Gavhi F, Kuonza L, Musekiwa A, Motaze NV. Factors associated with mortality in children under five years old hospitalized for Severe Acute Malnutrition in Limpopo province, South Africa, 2014-2018: A cross-sectional analytic study. PLoS One. 2020;15(5):e0232838. [CrossRef]
- Musiime V, Rujumba J, Kakooza L, Namisanvu H, Atuhaire L, Naguti E, et al. HIV prevalence among children admitted with severe acute malnutrition and associated factors with mother-to-child HIV transmission at Mulago Hospital, Uganda: A mixed methods study. PLoS One. 2024;19(4):e0301887. [CrossRef]
- Bwakura-Dangarembizi M, Dumbura C, Amadi B, Ngosa D, Majo FD, Nathoo KJ, et al. Risk factors for postdischarge mortality following hospitalization for severe acute malnutrition in Zimbabwe and Zambia. Am J Clin Nutr. 2021;113(3):665-674. [CrossRef]
- Chinkhumba J, Tomkins A, Banda T, Mkangama C, Fergusson P. The impact of HIV on mortality during in-patient rehabilitation of severely malnourished children in Malawi. Trans R Soc Trop Med Hyg. 2008;102(7):639-44. [CrossRef]
- Page AL, de Rekeneire N, Sayadi S, Aberrane S, Janssens AC, Rieux C, et al. Infections in children admitted with complicated severe acute malnutrition in Niger. PLoS One. 2013;8(7):e68699. [CrossRef]
- Calgaro S, Isidoris V, Girotto C, Chhaganlal K, Moiane J, Putoto G, et al. Children's Nutritional Rehabilitation Program in Beira, Mozambique: A Retrospective Study. Am J Trop Med Hyg. 2021;105(6):1631-1637.
- Teshale EB, Nigatu YD, Delbiso TD. Relapse of severe acute malnutrition among children discharged from outpatient therapeutic program in western Ethiopia. BMC Pediatr. 2023;23(1):441. [CrossRef]
- Yohannes T, Laelago T, Ayele M, Tamrat T. Mortality and morbidity trends and predictors of mortality in under-five children with severe acute malnutrition in Hadiya zone, South Ethiopia: a four-year retrospective review of hospital-based records (2012-2015). BMC Nutr. 2017;3:18. [CrossRef]
- CossaMoiane I, Roucher C, Campos-Ponce M, Doak C, Bauhofer A, Chissaque A, et al. Profile of Children with Undernutrition Admitted in Two Secondary-Level Hospitals in Maputo City, Mozambique. Nutrients. 2024;16(7):1056. [CrossRef]
- Amadi B, Imikendu M, Sakala M, Banda R, Kelly P. Integration of HIV care into community management of acute childhood malnutrition permits good outcomes: retrospective analysis of three years of a programme in Lusaka. PLoS One. 2016;11(3):e0149218. [CrossRef]
- Heydenrych N, De Maayer T, Nel M, van den Berg L. A retrospective cohort analysis of factors associated with the development of refeeding syndrome in children 0-59 months diagnosed with severe acute malnutrition in a South African setting. Heliyon. 2024;10(9):e30091. [CrossRef]
- Asafo-Agyei SB, Antwi S, Nguah SB. HIV infection in severely malnourished children in Kumasi, Ghana: a cross-sectional prospective study. BMC Pediatr. 2013;13:181. [CrossRef]
- Wondim A, Tigabu B, Kelkay MM. Time to Recovery from Severe Acute Malnutrition and Its Predictors among Admitted Children Aged 6-59 Months at the Therapeutic Feeding Center of Pawi General Hospital, Northwest Ethiopia: A Retrospective Follow-Up Study. Int J Pediatr. 2020;2020:8406597. [CrossRef]
- Oumer A, Mesfin L, Tesfahun E, Ale A. Predictors of Death from Complicated Severe Acute Malnutrition in East Ethiopia: Survival Analysis. Int J Gen Med. 2021; 14:8763-8773. [CrossRef]
- Bilal JA, Eltahir HG, Al-Nafeesah A, Al-Wutayd O, Adam I. Acute severe malnutrition treatment outcomes in children ages 6–59 months admitted to Singa Hospital, Sudan. Trans R Soc Trop Med Hyg. 2020;114(8):612-7. [CrossRef]
- Talbert A, Thuo N, Karisa J, Chesaro C, Ohuma E, Ignas J, et al. Diarrhoea complicating severe acute malnutrition in Kenyan children: a prospective descriptive study of risk factors and outcome. PloS one. 2012;7(6):e38321. [CrossRef]
- LaCourse SM, Chester FM, Preidis G, McCrary LM, Arscott-Mills T, Maliwichi M, et al. Use of Xpert for the diagnosis of pulmonary tuberculosis in severely malnourished hospitalized Malawian children. Pediatr Infect Dis J. 2014;33(11):1200-2. [CrossRef]
- Sunguya B. Effects of infections on severely malnourished children in Kilifi-Mombasa and Dar es Salaam: a comparative study. Dar Es Salaam Medical Students' Journal. 2006;14(1):27-35. [CrossRef]
- Schramm B, Nganaboy RC, Uwiragiye P, Mukeba D, Abdoubara A, Abdou I, et al.. Potential value of urine lateral-flow lipoarabinomannan (LAM) test for diagnosing tuberculosis among severely acute malnourished children. PLoS One. 2021;16(5):e0250933. [CrossRef]
- Bachou H, Tylleskär T, Downing R, Tumwine JK. Severe malnutrition with and without HIV-1 infection in hospitalised children in Kampala, Uganda: differences in clinical features, haematological findings and CD4+ cell counts. Nutrition journal. 2006;5:1-7. [CrossRef]
- Moramarco S, Amerio G, Ciarlantini C, Chipoma JK, Simpungwe MK, Nielsen-Saines K, et al. Community-Based Management of Child Malnutrition in Zambia: HIV/AIDS Infection and Other Risk Factors on Child Survival. Int J Environ Res Public Health. 2016;13(7):666. [CrossRef]
- Sudawa A, Ahmad AA, Adeleke S, Umar L, Rogo LD. HIV Infection among Under-Five Malnourished Children in Kano State. World Journal of AIDS. 2013;3(04):350. [CrossRef]
- Atalell KA, Haile RN, Techane MA. Magnitude of tuberculosis and its associated factors among under-five children admitted with severe acute malnutrition to public hospitals in the city of Dire Dawa, Eastern Ethiopia, 2021: multi-center cross-sectional study. IJID regions. 2022;3:256-60. [CrossRef]
- Muzigaba M, Puoane T, Sartorius B, Sanders D. Independent and interactive effects of HIV infection, clinical stage and other comorbidities on survival of children treated for severe malnutrition in rural South Africa: A retrospective multicohort study. South African Journal of Child Health. 2017;11(1):46-53.
- Baraki AG, Akalu TY, Wolde HF, Takele WW, Mamo WN, Derseh B, et al. Time to recovery from severe acute malnutrition and its predictors: a multicentre retrospective follow-up study in Amhara region, north-west Ethiopia. BMJ Open. 2020;10(2):e034583. [CrossRef]
- Kambale RM, Ngaboyeka GA, Ntagazibwa JN, Bisimwa MI, Kasole LY, Habiyambere V, et al. Severe acute malnutrition in children admitted in an Intensive Therapeutic and Feeding Centre of South Kivu, Eastern Democratic Republic of Congo: Why do our patients die? PLoS One. 2020;15(7):e0236022. [CrossRef]
- Bitew ZW, Alebel A, Worku T, Alemu A. Recovery rate and its predictors among children with severe acute malnutrition in Addis Ababa, Ethiopia: A retrospective cohort study. PLoS One. 2020;15(7):e0235259. [CrossRef]
- Mena MB, Dedefo MG, Billoro BB. Treatment Outcome of Severe Acute Malnutrition and Its Determinants among Pediatric Patients in West Ethiopia. Int J Pediatr. 2018;2018:8686501. [CrossRef]
- Kabeta A, Bekele G. Factors associated with treatment outcomes of under-five children with severe acute malnutrition admitted to therapeutic feeding unit of Yirgalem hospital. Clinics Mother Child Health. 2017;14(261):2.
- Banga D, Baren M, Ssonko NV, Sikakulya FK, Tibamwenda Y, Banga C, et al. Comorbidities and Factors Associated with Mortality among Children under Five Years Admitted with Severe Acute Malnutrition in the Nutritional Unit of Jinja Regional Referral Hospital, Eastern Uganda. Int J Pediatr. 2020;2020:7809412. [CrossRef]
- Fikrie A, Alemayehu A, Gebremedhin S. Treatment outcomes and factors affecting time-to-recovery from severe acute malnutrition in 6-59 months old children admitted to a stabilization center in Southern Ethiopia: A retrospective cohort study. Ital J Pediatr. 2019;45(1):46. [CrossRef]
- Abeje AT, Gudayu TW, Malefia YD, Befftu BB. Analysis of hospital records on treatment outcome of severe acute malnutrition: the case of Gondar University Tertiary Hospital. Pediatrics & Therapeutics. 2016;6(2):2161-0665.
- Desta K. Survival status and predictors of mortality among children aged 0–59 months with severe acute malnutrition admitted to stabilization center at Sekota Hospital Waghemra Zone. J Nutr Disord Ther. 2015;5(2):1-1.
- Negussie AS, Tadesse AW. Predictors of undesirable treatment outcomes of severe acute malnutrition among inpatient children in Addis Ababa, Ethiopia: a retrospective cohort study. BMC Public Health. 2020;20(1):1532. [CrossRef]
- Ikobah JM, Uhegbu K, Akpan F, Muoneke L, Ekanem E. Predictors of In-Patient Mortality of Severe Acute Malnutrition of Hospitalised Children in a Tertiary Facility in Southern Nigeria. Cureus. 2022;14(4):e24195. [CrossRef]
- Mekuria G, Derese T, Hailu G. Treatment outcome and associated factors of severe acute malnutrition among 6-59 months old children in Debre Markos and Finote Selam hospitals, Northwest Ethiopia: a retrospective cohort study. BMC Nutr. 2017;3:42.
- Nabukeera-Barungi N, Grenov B, Lanyero B, Namusoke H, Mupere E, Christensen VB, et al. Predictors of mortality among hospitalized children with severe acute malnutrition: a prospective study from Uganda. Pediatric research. 2018;84(1):92-8. [CrossRef]
- Desyibelew HD, Fekadu A, Woldie H. Recovery rate and associated factors of children age 6 to 59 months admitted with severe acute malnutrition at inpatient unit of Bahir Dar Felege Hiwot Referral hospital therapeutic feeding unite, northwest Ethiopia. PLoS One. 2017;12(2):e0171020. [CrossRef]
- Chiabi A, Malangue B, Nguefack S, Dongmo FN, Fru F, Takou V, et al. The clinical spectrum of severe acute malnutrition in children in Cameroon: a hospital-based study in Yaounde, Cameroon. Transl Pediatr. 2017;6(1):32-39. [CrossRef]
- Ba A, Thiongane A, Niang B, Keïta Y, Ly F, Ndongo AA, et al. Outcome after Discharge from Hospital of Children with Complicated Severe Acute Malnutrition and Predictors Factors of Non-Response during Outpatient Treatment, in Senegal. Open Journal of Pediatrics. 2023;13(4):473-83. [CrossRef]
- Asiimwe O, Ndezi G, Nduwimana M, Namukasa F, Mutisya CM, Abdirahman SH, et al. Prevalence, radio-clinical patterns and factors associated with pulmonary tuberculosis among children with severe acute malnutrition: A crossectional study in Uganda.
- Girma T, Kæstel P, Mølgaard C, Michaelsen KF, Hother AL, Friis H. Predictors of oedema among children hospitalized with severe acute malnutrition in Jimma University Hospital, Ethiopia: a cross-sectional study. BMC pediatrics. 2013;13:1-8. [CrossRef]
- Bizuneh FK, Tolossa T, Bekonjo NE, Wakuma B. Time to recovery from severe acute malnutrition and its predictors among children aged 6-59 months at Asosa general hospital, Northwest Ethiopia. A retrospective follow up study. PLoS One. 2022;17(8):e0272930.
- Abate BB, Tilahun BD, Kassie AM, Kassaw MW. Treatment outcome of Severe Acute Malnutrition and associated factors among under-five children in outpatient therapeutics unit in Gubalafto Wereda, North Wollo Zone, Ethiopia, 2019. PLoS One. 2020;15(9):e0238231. [CrossRef]
- Archary M, Adler H, La Russa P, Mahabeer P, Bobat RA. Bacterial infections in HIV-infected children admitted with severe acute malnutrition in Durban, South Africa. Paediatr Int Child Health. 2017;37(1):6-13. [CrossRef]
- Aye A, Amare F, Sosengo T. Treatment outcomes and associated factors among children with severe acute malnutrition at Hiwot Fana Specialized University Hospital, Harar, Eastern Ethiopia: a retrospective cohort study. Sudan J Paediatr. 2023;23(1):32-41. [CrossRef]
- Adem F, Edessa D, Bayissa B, Mohammed Hassen M, Mohammed MA. Treatment Outcomes and Associated Factors in Hospitalised Children with Severe Acute Malnutrition: A Prospective Cohort Study. Pediatric Health Med Ther. 2020;11:235-243. [CrossRef]
- Mody A, Bartz S, Hornik CP, Kiyimba T, Bain J, Muehlbauer M, et al. Effects of HIV infection on the metabolic and hormonal status of children with severe acute malnutrition. PLoS One. 2014;9(7):e102233. [CrossRef]
- Hussen Kabthymer R, Gizaw G, Belachew T. Time to Cure and Predictors of Recovery Among Children Aged 6-59 Months with Severe Acute Malnutrition Admitted in Jimma University Medical Center, Southwest Ethiopia: A Retrospective Cohort Study. Clin Epidemiol. 2020;12:1149-1159. [CrossRef]
- Vonasek BJ, Kumwenda T, Gumulira J, Nyirongo M, Heller T, Palmer M, et al. Point-of-Care Ultrasound for Tuberculosis in Young Children with Severe Acute Malnutrition. Pediatr Infect Dis J. 2024;43(2):e65-e67. [CrossRef]
- Wake AD. Survival Status and Predictors of Tuberculosis Development Among Under 5 Children Admitted With Severe Acute Malnutrition in Ethiopia: A Retrospective Cohort Study. Glob Pediatr Health. 2024;11:2333794X231226071. [CrossRef]
- Kassaw A, Amare D, Birhanu M, Tesfaw A, Zeleke S, Arage G, et al. Survival and predictors of mortality among severe acute malnourished under-five children admitted at Felege-Hiwot comprehensive specialized hospital, northwest, Ethiopia: a retrospective cohort study. BMC Pediatr. 2021;21(1):176. [CrossRef]
- Nduhukire T, Atwine D, Rachel L, Byonanebye JE. Predictors of in-hospital mortality among under-five children with severe acute malnutrition in South-Western Uganda. PLoS One. 2020;15(6):e0234343. [CrossRef]
- Ngari MM, Obiero C, Mwangome MK, Nyaguara A, Mturi N, Murunga S, et al. Mortality during and following hospital admission among school-aged children: a cohort study. Wellcome Open Res. 2021;5:234.
- Amadi B, Kelly P, Mwiya M, Mulwazi E, Sianongo S, Changwe F, et al. Intestinal and systemic infection, HIV, and mortality in Zambian children with persistent diarrhea and malnutrition. J Pediatr Gastroenterol Nutr. 2001;32(5):550-4.
- Nalwanga D, Musiime V, Kizito S, Kiggundu JB, Batte A, Musoke P, et al. Mortality among children under five years admitted for routine care of severe acute malnutrition: a prospective cohort study from Kampala, Uganda. BMC Pediatr. 2020;20(1):182. [CrossRef]
- Suliman OS, Salih MA, Karrar ZA, Mohammed AO, Helsing C. Infection and immunoglobulin levels in Sudanese children with severe protein-energy malnutrition. Sudan J Paediatr. 2011;11(2):32-42.
- Rytter MJ, Babirekere-Iriso E, Namusoke H, Christensen VB, Michaelsen KF, Ritz C, et al. Risk factors for death in children during inpatient treatment of severe acute malnutrition: a prospective cohort study. Am J Clin Nutr. 2017;105(2):494-502. [CrossRef]
- Ahmed JA, Yusuf N, Wilfong T, Tukeni KN, Berhanu H, Roba KT. Treatment outcomes among children admitted stabilization centers in Eastern Ethiopia: retrospective study. Front Public Health. 2023;11:1165858. [CrossRef]
- Asare H, Carboo J, Nel ED, Dolman RC, Conradie C, Lombard MJ, et al. Mortality in relation to profiles of clinical features in Ghanaian severely undernourished children aged 0-59 months: an observational study. Br J Nutr. 2021;125(10):1157-1165. [CrossRef]
- Irena AH, Mwambazi M, Mulenga V. Diarrhea is a major killer of children with severe acute malnutrition admitted to inpatient set-up in Lusaka, Zambia. Nutr J. 2011;10:110. [CrossRef]
- Muwanguzi E, Oboi JE, Nabbamba A, Wanyama R. Treatment outcome and associated factors for severely malnourished children (1-5 years) admitted to Lacor Hospital and Gulu Regional Referral Hospital in Uganda. J Nutr Sci. 2021;10:e33. [CrossRef]
- Bourke CD, Berkley JA, Prendergast AJ. Immune Dysfunction as a Cause and Consequence of Malnutrition. Trends Immunol. 2016;37(6):386-398. [CrossRef]
- Schaible UE, Kaufmann SH. Malnutrition and infection: complex mechanisms and global impacts. PLoS Med. 2007;4(5):e115.
- Mwene-Batu P, Bisimwa G, Baguma M, Chabwine J, Bapolisi A, Chimanuka C, et al. Long-term effects of severe acute malnutrition during childhood on adult cognitive, academic and behavioural development in African fragile countries: The Lwiro cohort study in Democratic Republic of the Congo. PLoS One. 2020;15(12):e0244486. [CrossRef]
- Toska E, Laurenzi CA, Roberts KJ, Cluver L, Sherr L. Adolescent mothers affected by HIV and their children: A scoping review of evidence and experiences from sub-Saharan Africa. Glob Public Health. 2020;15(11):1655-1673. [CrossRef]
- Chilaka VN, Konje JC. HIV in pregnancy - An update. Eur J Obstet Gynecol Reprod Biol. 2021;256:484-491.
- Transactional sex and HIV risk: from analysis to action. Geneva: Joint United Nations Programme on HIV/AIDS and STRIVE; 2018.
- Rezazadeh L, Ostadrahimi A, Tutunchi H, Naemi Kermanshahi M, Pourmoradian S. Nutrition interventions to address nutritional problems in HIV-positive patients: translating knowledge into practice. J Health Popul Nutr. 2023;42(1):94. [CrossRef]
- Vonasek BJ, Radtke KK, Vaz P, Buck WC, Chabala C, McCollum ED, et al. Tuberculosis in children with severe acute malnutrition. Expert Rev Respir Med. 2022;16(3):273-284. [CrossRef]
- Sinha P, Davis J, Saag L, Wanke C, Salgame P, Mesick J, et al. Undernutrition and Tuberculosis: Public Health Implications. J Infect Dis. 2019;219(9):1356-1363. [CrossRef]
- Lönnroth K, Castro KG, Chakaya JM, Chauhan LS, Floyd K, Glaziou P, et al. Tuberculosis control and elimination 2010-50: cure, care, and social development. Lancet. 2010;375(9728):1814-29.
- Franco JV, Bongaerts B, Metzendorf MI, Risso A, Guo Y, Peña Silva L, et al. Undernutrition as a risk factor for tuberculosis disease. Cochrane Database Syst Rev. 2024;6(6):CD015890.
- Denning DW. Global incidence and mortality of severe fungal disease. Lancet Infect Dis. 2024;24(7):e428-e438. [CrossRef]
Figure 1.
PRISMA flow diagram.
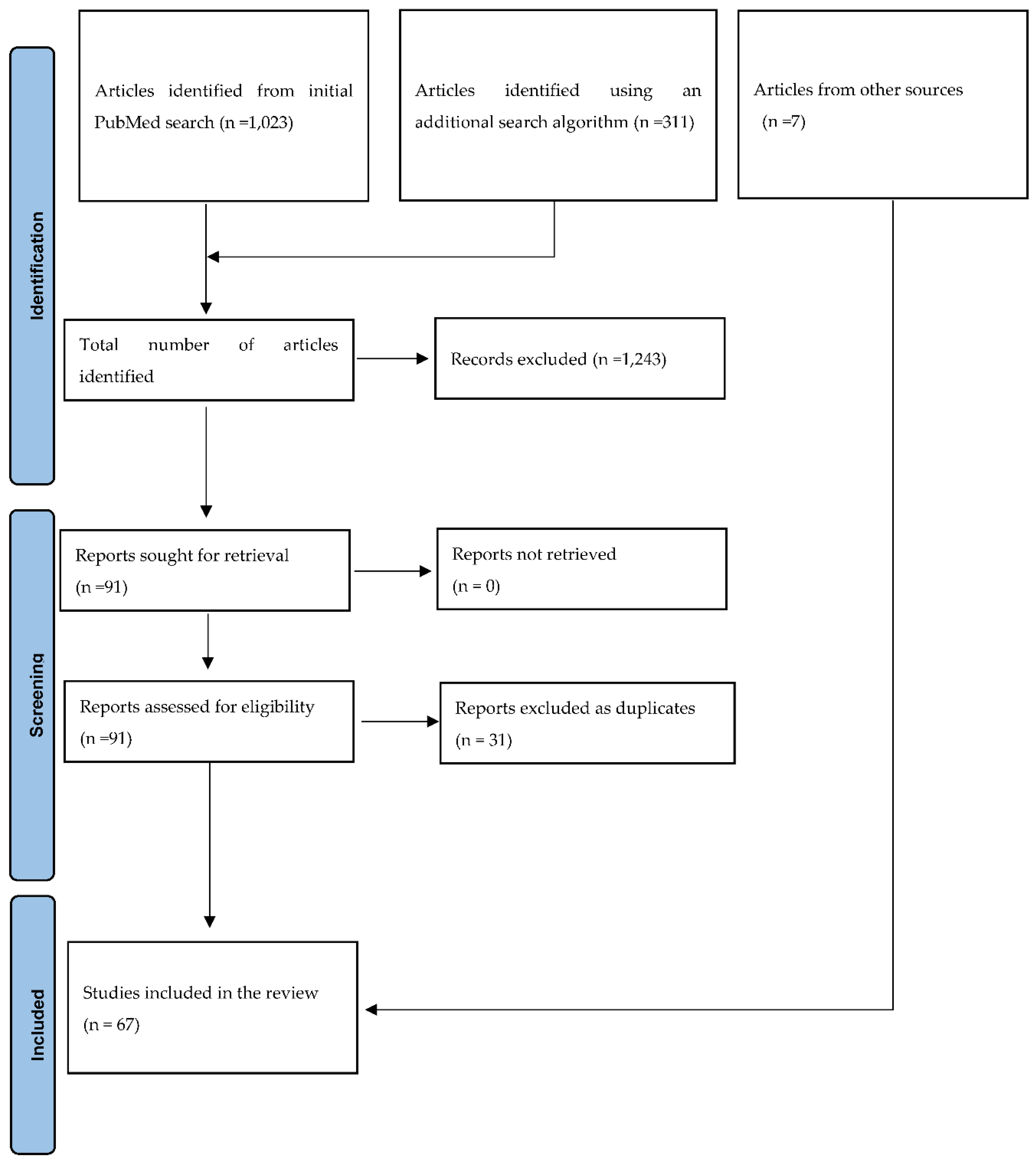
Figure 2.
A pictorial representation of pathogens in malnourished African children.
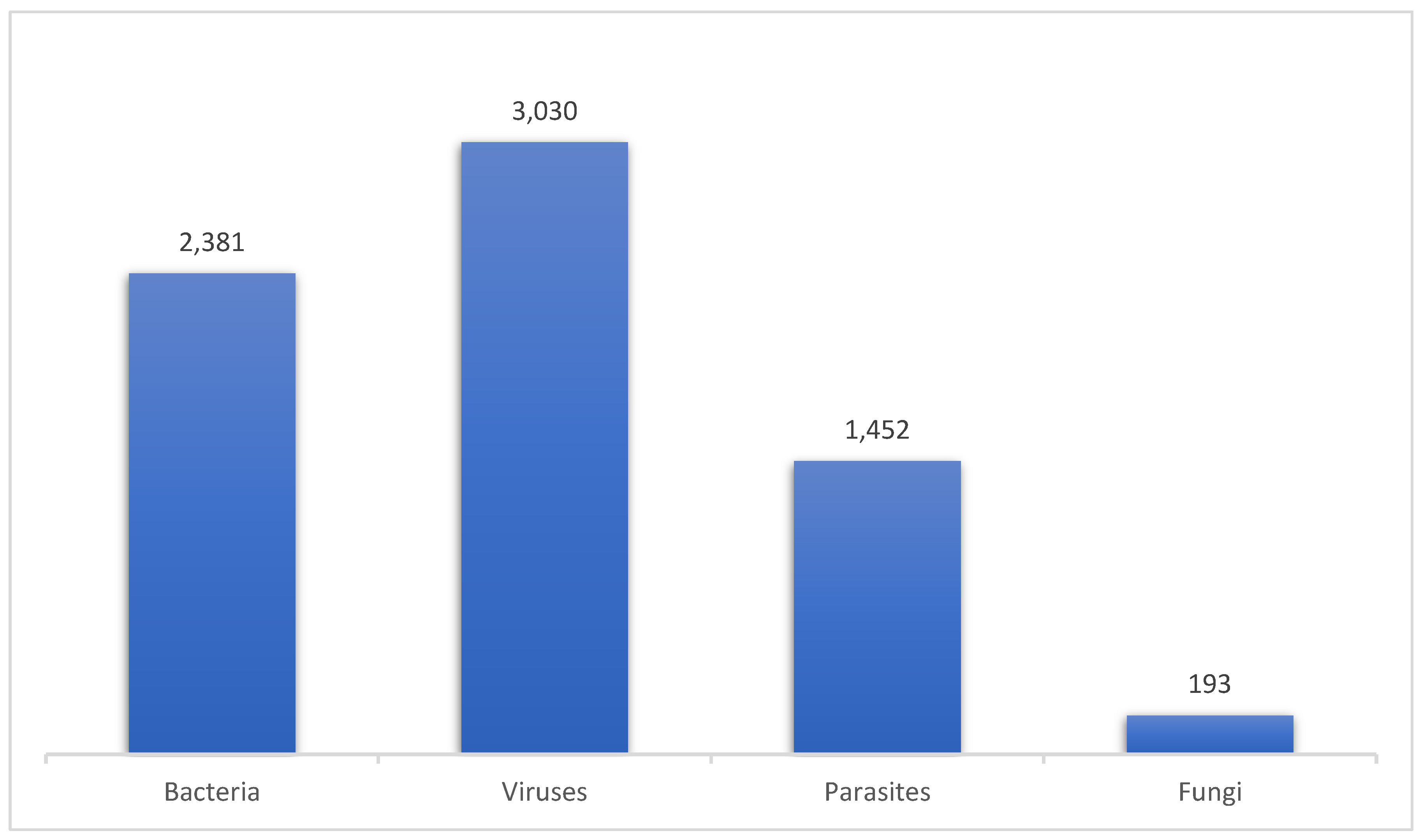

Table 1.
Summary of original studies reporting pathogens in malnourished African children.
| Location/ Country |
Type of Study | HB/CB/ OTP |
Study period | Study population | Sample size (n) | Age range or Median age | Number of Pathogens/Infection cases (n) | Fatality rates | Authors/Year of publication | No. of reference | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| South Africa | Prospective, observational study | HB | NS | SAM | 113 | < 5 years | HIV (n=58), TB (n=27) | 11.5% (n=13) | De Maayer et al 2011 | [13] | |||||||
| aEthiopia | Retrospective cohort study | HB | 2013 to 2015 | SAM | 545 | < 5 years | Malaria (n=37), TB (n=41) |
9.3% (n=51) | Girum et al 2017 | [14] | |||||||
| Sierra Leone | Descriptive cross-sectional study | HB | Over 6 months in 2018 | SAM | 74 | Median age of 11 months | TB (n=20) | - | Ide et al, 2019 | [15] | |||||||
| Zambia | Retrospective study | HB | 2009 to 2013 | SAM | 9,450 | 0 to 59 months | TB (n=151) | 56% (n=84) | Munthali et al 2017 | [16] | |||||||
| Mozambique | Retrospective study | HB | February to August 2018 | SAM | 45 | 0 to 59 months | TB (n=17) | - | Osorio et al. 2020 | [17] | |||||||
| aSouth Africa | Cross-sectional study | HB | 2014 – 2018 | SAM | 956 | Children under 5 years | HIV (n=181) TB (n=127) Malaria (n=4) |
25.9% (n=248) | Gavhi et al.2019(2020) | [18] | |||||||
| Uganda | Cross-sectional study | HB | June 2021 to December 2022 | SAM | 797 | 1 month to 5 years | HIV (n=76) | - | Musiime et al. 2024 | [19] | |||||||
|
bZambia/ Zimbabwe |
Prospective cohort study | HB | July 2016 and March 2019 | SAM | 649 | 1 to 59 months | HIV (n=130) | 8.5% (n=55) | Bwakura-Dangarembizi et al, 2021 | [20] | |||||||
| Malawi | Prospective cohort study | HB | NS | SAM | 454 | 6 to 59 months | HIV (n=79) | 14.8% (n=67) | Chinkhumba et al, 2008 | [21] | |||||||
| aNiger | Prospective study | HB | November 2007 to July 2008 | Complicated SAM | 311 | 6 to 59 months | Bacteremia, n=79, malaria parasite, n=44, enteric pathogens isolated from stool (bacteria, n=36, viruses, n=23, intestinal parasites, n=6), TB (n=4), pathogens isolated from the urinary tract (bacteria, n=48), pathogens identified from nasal swabs (viruses, n=5) | 9% (n=29) | Page et al, 2013 | [22] | |||||||
| Mozambique | Retrospective observational study | HB | March 2016 to February 2017 | SAM | 1,231 | 0 to 5 years | HIV (n=157) | - | Calgaro et al, 2021 | [23] | |||||||
| Ethiopia | Cross-sectional study | HB | April – June 2020 | SAM | 208 | 6 to 59 | HIV (n=11) | - | Teshale et al, 2023 | [24] | |||||||
| aEthiopia | Retrospective cohort study | HB | January 2012 to December 2015 | SAM | 500 | Under 5 years | TB (n=15) | 7% (NS) | Yohannes et al, 2017 | [25] | |||||||
| aMozambique | Cross-sectional study | HB | January 2018 to March 2020 | Undernourished children | 449 | 1 to 14 years | HIV (n=120), malaria (n=12), intestinal parasitic infections (n=90) | - | Cossa-Moiane et al, 2024 | [26] | |||||||
| Zambia | Retrospective study | CB | October 2009 and September 2012 | SAM (n=1,195) MAM (n=664) | 1,859 | Median age of 16 months | HIV in children with SAM (n=134) HIV in children with MAM (n=51) |
2.9% (n=53) | Amadi et al, 2016 | [27] | |||||||
| aSouth Africa | Retrospective cohort study | HB | October 2014 to December 2018. | SAM | 126 | 0 to 59 months | HIV (n=23), TB (n=17) | 15.1 % (n=19) | Heydenrych et al, 2024 | [28] | |||||||
| aGhana | Cross-sectional prospective study | HB | February 2010 to October 2010 | SAM | 246 | 3 months to 13 years | HIV (n=67), TB (n=23), malaria (n=34), bacteremia (n=85) | 17.5% (n=43) | Asafo-Agyei et al 2013 | [29] | |||||||
| aEthiopia | Retrospective follow-up study | HB | March to April, 2018 | SAM | 398 | 6 to 59 months | HIV (n=1), malaria (n=76), TB (n=27) | - | Wondim et al, 2020 | [30] | |||||||
| aEthiopia | Retrospective cohort study | HB | September 2017 to March 2020. | Complicated SAM | 665 | 0 to 59 months | HIV (n=5), TB (n=23), malaria (n=2) | 9% (60) | Oumer et al, 2021 | [31] | |||||||
| Sudan | Prospective hospital-based study | HB | April to October 2018 | SAM | 376 | 6 to 59 months | Malaria (n=131), intestinal parasites (n=24) | 3.7% (n=14) | Bilal et al, 2020 | [32] | |||||||
| Kenya | Prospective descriptive study | HB | June 2005 to June 2009 | SAM | 1,206 | 6 to 12 years | HIV (n=229), malaria parasitemia (n=227), bacteremia (n=86) | 16% (194) | Talbert et al, 2012 | [33] | |||||||
| Malawi | Cross-sectional observational study | HB | February to May 2012 | SAM | 300 | 6 to 60 months | HIV (n=52), TB (n=2) | 9.7% (n=29) | LaCourse et al. 2014 | [34] | |||||||
| bKenya/Tanzania | A retrospective study | HB | 2004 to 2005 | SAM | 1121 | NS | Malaria (n=404), candidiasis (n=119), TB (n=293) | 19% (n=64) 28% (n=222) |
Sunguya et al, 2006 | [35] | |||||||
| Niger | Cross-sectional study | HB | 2016 to 2017 | SAM | 202 | < 5 years | TB (n=90) | 19.6% (n=20) | Schramm et al. 2021 | [36] | |||||||
| aUganda | Prospective study | HB | September-November 2003 and September-December 2004 | SAM | 450 | < 60 months | HIV (n=151), bacteremia (n=76) | 28.9% (n=22) | Bachou et al, 2006 | [37] | |||||||
| Zambia | Retrospective | CB | 2012 to 2014 | SAM | 858 | 6 to 59 months | HIV (n=63), malaria (n=7) | 5.6% (n=48) | Moramarco et al, 2016 | [38] | |||||||
| Nigeria | Cross-sectional study | HB | - | SAM | 400 | < 5 years | HIV (n=31) | - | Sudawa et al, 2013 | [39] | |||||||
| aEthiopia | Retrospective cross-sectional study | HB | 2018 – 2020 | SAM | 414 | < 5 years | Malaria (n=7), HIV (n=20), TB (n=43) | - | Atalell et al, 2021 | [40] | |||||||
| aSouth Africa | A retrospective multicohort study | HB | 2009 – 2013 | SAM | 454 | 6 to 60 months | HIV (n=196) | 24.4% (n=108) | Muzigaba et al, 2017 | [41] | |||||||
| aEthiopia | Retrospective | HB | 2012 - 2016 | SAM | 1690 | The majority of the participants were < 2 years | TB (n=107), HIV (n=54) | - | Baraki et al, 2020 | [42] | |||||||
| aDemocratic Republic of Congo | Retrospective | HB | 2017 - 2018 | SAM | 633 | 1 month to 18 years | HIV (n=14), malaria (n=33), bacteremia (n=38) | 9.2% (n=58) | Kambale et al, 2020 | [43] | |||||||
| aEthiopia | Retrospective cohort study | HB | 2012 – 2019, (may to June 2019) | SAM | 515 | Majority were < 24 months | TB (n=71) | 9% (n=46) | Bitew et al, 2020 | [44] | |||||||
| aEthiopia | Retrospective cross-sectional study | HB | 2015 - 2017 | SAM | 205 | 1 month – 14 years | HIV (n=21), TB (n=16), malaria (n=30) | 4.4% (n=9) | Mena et al, 2018 | [45] | |||||||
| aEthiopia | Retrospective study | HB | 2013 - 2015 | SAM | 196 | Median age: 12+8.5 months. | TB (n=27), malaria (n=2) | 16% (NS) | Kabeta et al, 2017 | [46] | |||||||
| aUganda | Analytical and Descriptive Prospective Cohort Study | HB | July to September 2019 | SAM | 338 | < 5 years | Malaria (n=72), bacteremia (n=23), HIV (n=20), TB (n=17) | 14.5% (49) | Banga et al, 2020 | [47] | |||||||
| aEthiopia | Retrospective cohort study | HB | 2015 to 2017 | SAM | 420 | 6 to 59 months | HIV (n=3), TB (n=87), malaria (n=10) | 10.8% (n=41) | Fikrie et al, 2019 | [48] | |||||||
| aEthiopia | Cross-sectional study | HB | 2010 to 2012 | SAM | 298 | 2 to 59 months | HIV (n=5) | 11.7% (n=35) | Abeje et al 2016 | [49] | |||||||
| aEthiopia | A Retrospective Cohort Study | HB | 2011 to 2013 | SAM | 415 | 0 to 59 months | TB (n=9), HIV (n=17), malaria (n=77) | 28.7% (n=119) | Desta et al, 2015 | [50] | |||||||
| aEthiopia | A Retrospective Cohort Study | HB | 2013 to 2016 | Complicated SAM | 259 | 6 to 59 months | TB (n=18), HIV (n=11) | 12.2% (n=37) | Negussie et al, 2020 | [51] | |||||||
| aNigeria | Prospective cohort study | HB | 2017 to 2019 | SAM | 100 | Mean age: 14.28 ± 14.04 months | HIV (n=81), TB (n=79) | 7.7% (NS) | Ikobah et al, 2022 | [52] | |||||||
| aEthiopia | Retrospective cohort study | HB | 2014 to 2016 | SAM | 253 | 6 to 59 months | TB (n=19) | 5.5% (n=14) | Mekuria et al, 2017 | [53] | |||||||
| aUganda | Prospective cohort study | HB | 2014 to 2015 | SAM | 400 | 6 to 59 months | HIV (n=43) | 9.8% (39) | Nabukeera-Barungi et al, 2017 | [54] | |||||||
| aEthiopia | Cross-sectional study | HB | 2012 to 2016 | SAM | 401 | 6 to 59 months | TB (n=37), HIV (n=26), malaria (n=13) | 8.5% (n=34) | Desyibelew et al 2017 | [55] | |||||||
| aCameroon | Retrospective study | HB | 2006 to 2015 | SAM | 179 | < 15 years | Malaria (n=27) | 15% (n=27) | Chiabi et al, 2016 | [56] | |||||||
| aSenegal | Descriptive and analytical cross-sectional study | HB | March to November, 2021 | Complicated SAM | 103 | 6 to 59 months | TB (n=2), HIV (n=6) | 2.9% (n=3) | Ba et al, 2023 | [57] | |||||||
| Uganda | Cross sectional study | HB | 2023 - 2024 | SAM | 137 | 6-59 months | TB (n=32) | - | Asiimwe et al, 2024 | [58] | |||||||
| aEthiopia | Cross sectional study | HB | Not stated | SAM | 351 | 0.5-14 years | HIV (n=9), TB (n=17), malaria (n=9) | - | Girma et al 2013 | [59] | |||||||
| aEthiopia | Retrospective study | HB | 2015 - 2019 | SAM | 454 | 6 – 59 months | HIV (n=15), TB (n=35) | - | Bizuneh et al 2022 | [60] | |||||||
| aEthiopia | Retrospective cohort study | OTP | 2016 - 2019 | SAM | 600 | Birth to 59 months | HIV (n=12), TB (n=12) | 2.0% (n=12) | Abate et al 2020 | [61] | |||||||
| South Africa | Prospective | HB | 2012 - 2015 | SAM | 82 | 1 month to 10.6 years | HIV (n=82), Bacteria (n=51) | - | Archary et al, 2016 | [62] | |||||||
| aEthiopia | A retrospective cohort study | HB | January to February, 2021 | SAM | 162 | 6 – 59 months | Malaria (n=9), HIV (n=12) | 6.8% (n=11) | Aye et al, 2023 | [63] | |||||||
| aEthiopia | A prospective cohort study | HB | March to July, 2018 | SAM | 133 | 6 – 59 months | TB (n=24), HIV (n=3), malaria (n=3) | 3.8% (NS) | Adem et al, 2020 | [64] | |||||||
| Uganda | A prospective cohort study | HB | 2010 - 2011 | SAM | 74 | 6 months – 5 years | HIV (n=18), malaria (n=7) | 12% (n=9) | Mody et all, 2014 | [65] | |||||||
| Ethiopia | A Retrospective Cohort Study | HB | 2015 – 2017 | SAM | 375 | 6 – 59 months | HIV (n=15), TB (n=54), malaria (n=21) | 12.3% (n=43) | Kabthymer et al, 2020 | [66] | |||||||
| Malawi | Prospective observational study | HB | 2021 - 2022 | Complicated SAM | 131 | 6 – 59 months | TB (n=4) | - | Vonasek et al, 2024 | [67] | |||||||
| Ethiopia | Retrospective cohort study | HB | 2018 - 2022 | SAM | 247 | < 5 years | TB (n=24) | - | Wake et al, 2024 | [68] | |||||||
| aEthiopia | Retrospective, Cohort study | HB | 2016 to 2019 | SAM | 476 | < 5 years | HIV (n=31) TB (n=61) |
11.3% (n=54) | Kassaw et al 2021 | [69] | |||||||
| Uganda | Prospective cohort study | HB | June to August 2015 | SAM | 122 | Children under 5 years | HIV (n=9) Malaria (n=25) |
- | Nduhukire et al.2020 | [70] | |||||||
| Kenya | Retrospective cohort study | HB | 2007-2016 | SAM | 3090 | 5-12yrs | HIV (n=197) | 3.4% (n=132) | Ngari et al, 2021 | [71] | |||||||
| Zambia | Cross-sectional study | HB | 19982000 | SAM | 200 | 6 to 24months | HIV (n=106), TB (n=27), bacteremia (n=26), Intesstinal infection [Cryptosporidium parvum (n=47), Isospora belli (n=4), Giardia intestinalis (n=11), Blastocystis hominis (n=4), Microsporidia (n=1), Salmonella spp. (n=35), Shigella spp.(n=4), Vibrio cholerae (n=6), Hookworm (n=3), Ascaris lumbricoides (n=10), Yeast cells (n=74) | 19.5% (39) | Amadi et al, 2001 | [72] | |||||||
| Uganda | Prospective cohort study | HB | November 2007 to July 2008 | SAM | 270 | <5yrs | HIV (n=33) | 25% (n=67) | Nwalanga et al 2020 | [73] | |||||||
| aSudan | Case control study | HB | 1992-1993 | SAM | 81 | 0 to 5 years | TB (n=8), intestinal parasitic infection (n=24), UTI [(E. coli, (n=6), Proteus species (n=2), Klebsiella species (n=2)] | - | Suliman et al, 2011 | [74] | |||||||
| aUganda | Prospective observational study | HB | 2012 - 2013 | SAM | 120 | 6 – 59 months | HIV (n=20) | 14% (n=17) | Rytter et al, 2017 | [75] | |||||||
| aEthiopia | Retrospective cohort study | HB | December 10-30, 2021 | SAM | 712 | 6 months to 59 months | TB (n=43), HIV (n=3) |
5.9% | Ahmed et al, 2023 | [76] | |||||||
| aGhana | Prospective observational study | HB | 2013 to 2018 | SAM | 601 | 0 to 59 months | HIV (54), TB (n=32), malaria(n=110) | 16.5% (n=99) | Asare et al, 2021 | [77] | |||||||
| Zambia | Cohort study | HB | August - December 2009 | Complicated SAM | 430 | 6 months to 59 months | HIV (n=161) TB (n=6) |
40.5% (n=174) | Irena et al 2013 | [78] | |||||||
| Uganda | Retrospective observational study | HB | January to December 2017 | Complicated SAM | 330 | 1-5yrs | HIV (n=86) | 22% (70) | Muwanguzi et al, 2021 | [79] | |||||||
SAM: Severe acute malnutrition, MAM: Moderate acute malnutrition, OTP: Outpatient Therapeutic Program, HB: Hospital base, CB: Community base, HIV: Human immunodeficiency virus, UTI: Urinary tract infection, TB: Tuberculosis, a: studies reporting other infections, but pathogen not identified, b: Multicenter study.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



