Submitted:
13 September 2024
Posted:
16 September 2024
You are already at the latest version
Abstract
This literature review focusses on diagnostics of Equine Asthma (EA), possible influencing factors on diagnostic techniques and latest developments in diagnosing horses during EA remission or in case of subclinical disease. Routine EA diagnostics include clinical examination of the respiratory system including percussion and auscultation, clinical pathology including white blood cells and arterial blood gas analysis, bronchoscopy to evaluate the amount and viscosity of respiratory secretion, bronchoalveolar lavage and cytology of tracheal aspirates (TA) and bronchoalveolar lavage fluid (BALF). Grading of EA severity and inflammatory subtype is based on BALF cy-tology, while TA cytology helps to rule out previous bacterial infections. Different factors have an impact on the airways regarding structure of the epithelium, cytology and inflammatory markers possibly influencing the diagnosis of EA. Short-term exercise increases the total cell count and inflammatory mediators in BALF of men, asymptomatic horses and other species. Further factors involve cold or chlorinated air, long-term training effects and the co-incidence of further respir-atory disease, in particular exercise-induced pulmonary hemorrhage. As BALF cytology may be unremarkable during EA remission and low-grade disease, exercise and other factors stressing the bronchial epithelium may help to diagnose these patients.
Keywords:
horse
; chronic respiratory disease
; inflammatory airway disease
1. Introduction
Equine asthma is a chronic disease of the lower airways in horses. It is characterized by mass hypertrophy of the smooth bronchial musculature and resulting obstruction, as well as hyperplasia of the goblet cells and dyscrinia. Until today, the role and type of hypersensitivity reaction to environmental antigens remains a topic of debate in the scientific community [1,2,3].
While over 200 endotypes are known in human asthma [4] only two phenotypes have been defined in horses: a mild-to-moderate (MEA) and a severe form (SEA). MEA, formerly known as inflammatory airway disease (IAD), is more frequently diagnosed in horses under the age of seven, while SEA, formerly known as recurrent airway obstruction (RAO) or heaves is more prevalent in older horses. Coughing and a slight decline in performance may be the only clinical signs in MEA. EA is a chronic disease, so owners report of recurrent clinical signs or lasting minimum of four weeks. A high disease prevalence of up to 70% was found in various studies for MEA [5,6,7]. A prevalence of up to 14% is documented globally for SEA [8]. Disease exacerbation is characterized by an elevated respiratory rate, dyspnea at rest, and abdominal breathing resulting from bronchospasm of the bronchial muscles. Furthermore, there is evidence suggesting that the severe form can evolve from the mild-to-moderate form [1,9].
It is recommended that an early diagnosis be sought, as the remodeling of the bronchial smooth muscle, the extracellular matrix of the lamina propria, and the pulmonary arteries progresses during the course of the disease. In particular, the remodeling of the bronchial smooth muscle is not fully reversible. Even in remission, equine asthmatics still exhibit 50% more airway smooth muscle (ASM) mass than healthy horses [10]. The remodeling of the extracellular matrix and pulmonary arteries appears to be largely reversible after postural optimization and inhalation therapy [11,12]. The earlier EA is diagnosed, the less irreversible remodeling of the ASM has taken place, which significantly increases the chance of recovery. EA with irreversible remodeling is not curable and can therefore only be managed effectively through good management.
2. Diagnostics of EA
Clinical Examination and Blood Work
Although multiple techniques, laboratory tests and biomarkers have been evaluated regarding their efficacy in diagnosing equine asthma, history of recurrent expiratory dyspnoea and a detailed clinical examination of the respiratory system during exacerbation remains the basis of diagnosing equine asthma. In addition, a venous blood test for leukocytes helps to rule out respiratory infection and an arterial blood gas analysis (PaO2, PaCO2, AaDO2) to grade the severity of gas exchange impairment. Unfortunately, these basic diagnostics are often unremarkable during SEA remission or in MEA. Additionally, musculoskeletal disorders and upper airway disease may manifest as poor performance [2].
Bronchoscopy
Endoscopy of the upper airways is a valuable tool for the diagnosis of upper respiratory tract diseases affecting the larynx, pharynx and guttural pouches. These conditions have the potential to cause obstruction, irregular breathing sounds, and impaired performance [1].
Bronchoscopy is employed for the assessment of the quantity and viscosity of tracheal and bronchial secretions [13]. The quantity of mucus is significantly correlated with the neutrophil count in tracheal aspirates (TA) and bronchoalveolar lavage fluid (BALF) cytology, exhibiting a substantial degree of interobserver agreement. While there is considerable interobserver variance in grading mucus viscosity, color, and location, mucus volume within the trachea has a high interobserver agreement [13].
Mucus accumulation is not an unambiguous indicator of EA, but a common finding in respiratory disease. Furthermore, some healthy horses also display a minimal amount of mucus (120ml/day) within the trachea [7,13]. As the mucus containing cells from the lungs is transported along the trachea, a sample from the trachea contains older cells and not all the cells, which could be found in the lungs [13]. It is not possible to differentiate between bacterial infections and equine asthma macroscopically. Therefore, tracheal aspirates should be taken through the endoscopic working channel or as a transcutaneous tracheal aspirate. Although the later are not commonly taken anymore, transcutaneous tracheal aspiration or wash technique offers the advantage of reduced pharyngeal contamination and easier mucus aspiration with high viscosity due to dilution [14].
The cytology of the tracheal aspirate is evaluated through microscopic examination following Diff-Quick staining [15]. Furthermore, the sample is cultured for aerobic and anaerobic bacteria.
A diagnosis of airway inflammation may be made if TA cytology reveals a neutrophil count of greater than 20%. The presence of intracellular bacteria, phagocytosed by macrophages, indicates an infectious disease. Additionally, the sample may be contaminated with bacteria from the oropharynx, which appear extracellular in cytology, or fungal hyphae and pollen [14]. For this reason, BAL cytology is a more sensitive method for diagnosing EA, especially MEA [16,17,18].
Bronchoalveolar lavage fluid (BALF) cytology is a more sensitive method for the diagnosis and grading of EA, as BALF is less contaminated with environmental particles than tracheobronchial secretions. This is due to the fact that the probe is not taken from the trachea but from the small airways, a more peripheral lung area [18] yielding fresher cells. Several studies found no correlation between cytology results comparing TA and BALF in horses with chronic lung disease [19,20]. One study found a correlation of neutrophil percantages in TA and BALF cytology [16]. Nevertheless, TA is an ineffective method for diagnosing mild-to-moderate equine asthma, mainly because of the different subtypes and mild courses [18,20].
Bronchoalveolar lavage (BAL) can be performed under endoscopic control or blindly with a BAL catheter [14]. Both methods are commonly used as described elsewhere [16,19]. A volume of 250 – 500ml of saline is recommended for this purpose [2]. It would be advisable to standardize the volume more, as the amount of neutrophils is higher when a smaller volume of saline is used [21]. The volume used for BAL do not exhibit a notable influence on total cell count (TCC) and percentages of other cell types than neutrophils in BALF. The total cell count can be determined by either a hemocytometer or an automated hematology analyzer, provided that the sample is free from visible mucus [14]. Nevertheless, the implementation of a standardized BALF volume would enhance the comparability of the results. In addition, the utilization of “total cell count in epithelial lining fluid” (ELF) would serve as a superior parameter for ensuring comparability. The total cell count in ELF can be calculated by measuring urea in blood plasma and BALF. Urea diffuses through numerous body compartments, including the lungs. This assumption reduces the effect of dilution. The calculation is as follows: ELF (ml) = [total amount of urea in BALF recovered (mg)] / [concentration of urea in plasma (mg/ml)] [22]. With the recovered volume of BALF, total cell count in BALF (haemocytometer) and urea in blood plasma and BALF, it is possible to calculate the absolute cell count in ELF and thereby the total cell count in ELF in cells/μL. The physiological cell count in ELF is estimated to be below 15,500 to 21,700 cells per microliter [23]. At the moment it is uncommon to specify the total cell count in ELF, but it is more comparable than TCC in BALF.
The BALF cytology in MEA is characterized by an increase in neutrophil granulocytes to a minimum of 10% and/or eosinophil granulocytes and/or mast cells to a minimum of 5% [2].
In exacerbation of SEA, an increase in neutrophil granulocytes to 25% is observed in the cytology of BALF [2]. Up to date, it is not possible to differentiate between MEA and SEA in remission.
Use of Biomarkers
Multiple biomarkers have been studied regarding their efficacy in supporting a diagnosis of EA (Table 1). While they are widely used in research to study the pathogenesis of EA, they are not commonly used during clinical routine. Unfortunately, most work better using BALF than peripheral blood. The advantage of blood biomarkers would be the easy execution in the field, where BALF is rarely taken routinely. Lung-specific biomarkers and non-specific inflammation markers (e.g. acute phase proteins) have been described, commonly based on ELISA techniques [24]. Unfortunately, blood biomarkers often have a low sensitivity and/or specificity [25]. In general, a considerable number of biomarkers are only applicable to SEA diagnostics and frequently unable to be utilized for more specific MEA diagnostics or during SEA remission [26].
Surfactant protein-D is a protective protein in pulmonary inflammation, which increases in serum, particularly in the context of mild and severe neutrophilic asthma. Haptoglobin is an acute-phase protein that is elevated in serum even in horses suffering from MEA [24]. The combination of the measurement of both biomarkers demonstrates a sensitivity and specificity of 100% [25]. Secretoglobin is secreted by club cells and is an anti-inflammatory protein that is reduced in the BALF of asthmatic horses [24,27]. No significant decline can be detected in the blood. However, in combination with a HOARSI score [28] greater than 2, it is a viable blood biomarker [24]. The acute phase protein Serumamyloid A (SAA) is elevated in blood in acute inflammatory phases of EA in exacerbation as a marker of systemic inflammation [26].
Neutrophil gelatinase-associated lipocalin (NGAL) is a biomarker for kidney disease that has been identified in human medicine. It is produced by neutrophil granulocytes and epithelial cells of various organs, including the kidneys, intestines, liver, and lungs. The concentration of NGAL in BALF has been observed to increase in correlation with the severity of the disease, although no significant difference has been noted between the various MEA subtypes. Consequently, the diagnostic value in MEA is limited [29].
Matrix metalloproteinases (MMPs) and their tissue inhibitors (TIMPs) have been demonstrated to be useful in the diagnosis of various lung diseases, given that they are no longer in equilibrium during lung remodeling processes. The ratio of MMP-8 and TIMP-1 in BALF has been shown to be effective in differentiating between MEA and SEA, with the ratio increasing in SEA and decreasing in MEA and SEA in remission [30].
Procalcitonin as a precursor protein of calcitonin has the potential to serve as a promising blood biomarker as it is elevated in the blood serum of horses with chronic pneumopathies. The possibility of differentiating the various respiratory diseases with the aid of procalcitonin still requires further research [31].
In addition, numerous biomarkers are suitable for diagnostics of severe equine asthma (Table 1). In this review, the authors concentrate on diagnostics of mild-moderate equine asthma.

Table 1.
List of various biomarkers detectable either in bloodserum, BALF, exhaled breath condensate or surfactant. Some biomarkers are verifiable only in SEA, some in MEA as well.
Table 1.
List of various biomarkers detectable either in bloodserum, BALF, exhaled breath condensate or surfactant. Some biomarkers are verifiable only in SEA, some in MEA as well.
| Biomarker | Suitable for MEA/SEA | BALF/bloodserum | Increase or decrease | Literature |
| Surfactantprotein-D | MEA + SEA | bloodserum | increase | [24,25] |
| Haptoglobin | MEA + SEA | bloodserum | increase | [24,25,26] |
| Secretoglobin | MEA + SEA | BALF, (bloodserum) | decrease | [24,27] |
| SAA | SEA | bloodserum | increase | [26] |
| Neutrophil gelatinase-associated Lipocalin | (MEA +) SEA | BALF | increase | [29] |
| MMPs + TIMPs | MEA + SEA | BALF | disturbed balance | [30] |
| Procalcitonin | (MEA +) SEA | bloodserum | increase | [31] |
| NETs | SEA | BALF | increase | [32] |
| Myeloperoxidase | SEA, even in remission | BALF | increase | [33] |
| Myo-Isonitol | SEA | BALF | decrease | [34] |
| Formate | SEA | BALF | increase | [34] |
| Isopropanol | SEA | BALF | increase | [34] |
| Ethanol | SEA | Exhaled breath condensate | increase | [34] |
| Interleukin-1beta | SEA | BALF | increase | [35] |
| Tumor Necrosis Factor-alpha | SEA | BALF | increase | [35,36] |
| Interleukin-8 | SEA | BALF | increase | [35,36] |
| Interleukin-4 | SEA | BALF | increase | [35] |
| Interferon-gamma | SEA | BALF | increase | [35,36] |
| Thromboxane B2 | SEA | bloodserum | increase | [37] |
| Prostaglandin E2 | SEA | BALF | increase | [38] |
| Prostaglandin F | SEA | BALF | increase | [38] |
| Histamin | SEA, even in remission | BALF | increase | [39] |
| Cyclic phosphatidic acid | SEA | Surfactant | increase | [40] |
| Diacylglycerol | SEA | Surfactant | increase | [40] |
| 8-hydroxy-2-deoxyguanosine | SEA | bloodserum | increase | [41] |
| Transferrin | SEA | BALF | decrease | [27] |
| IgE + IgG antibodies specific for Aspergillus fumigatus | SEA | BALF | increase | [42] |
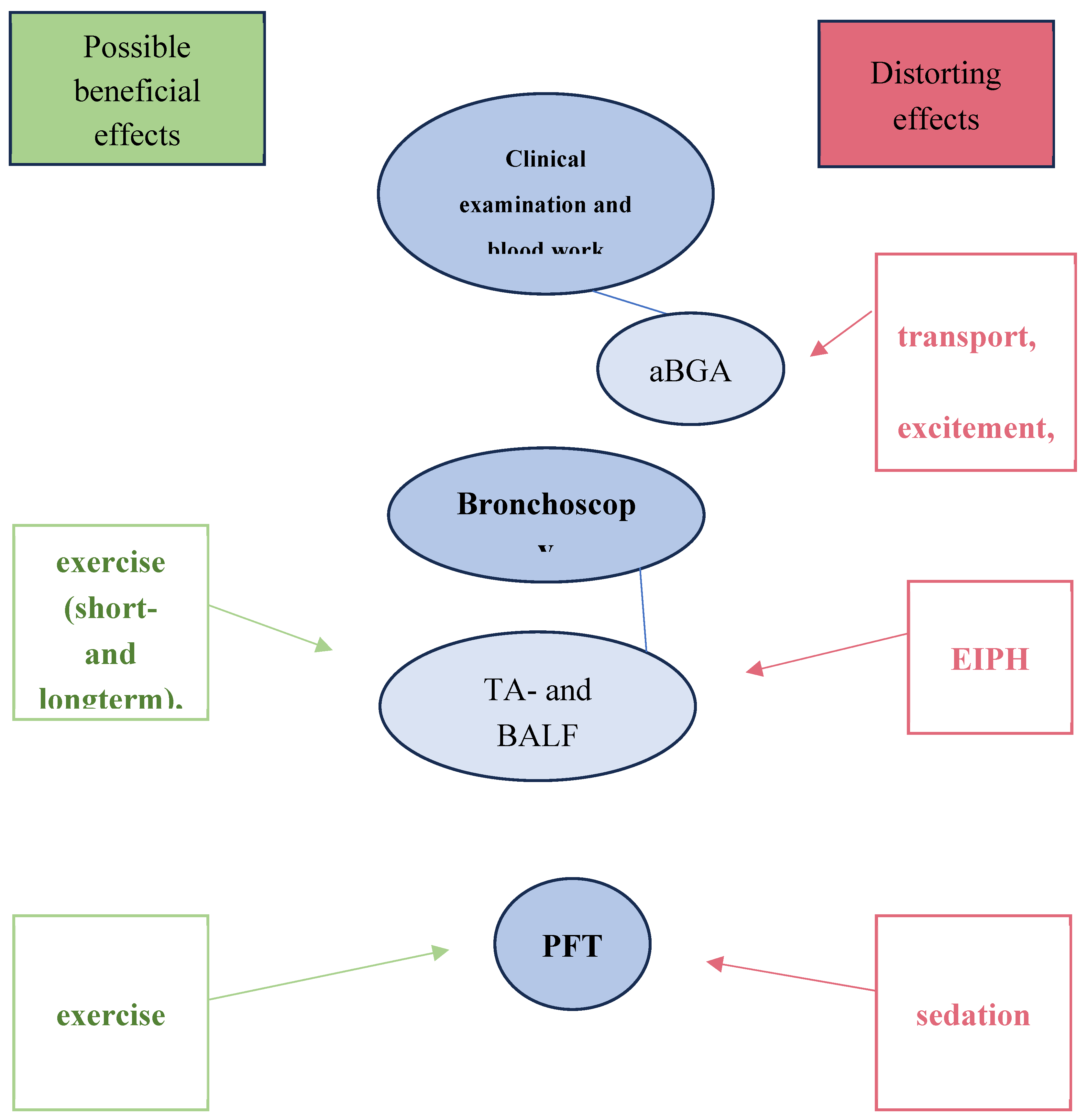
At the most recent Havemeyer workshop (2019), it was emphasized that further research is required to improve the diagnosis of mild-to-moderate EA cases. The objective should be to diagnose EA at an earlier stage, allowing for a differentiation between mild and moderate cases. It is conceivable that horses with performance insufficiency, but without any clinical signs could be phenotypically assigned to the mild form, while horses with respiratory symptoms could be assigned to the moderate form. The manner in which this classification would manifest cytologically is yet to be determined. There are several scoring systems for EA [43,44], but it is quite difficult to distinguish mildly affected horses from healthy subjects or those suffering from SEA in remission. Therefore, research concerning possibilities of differentiation of healthy or mild asthmatics is needed [1]. For this reason, it might be beneficial to have a look on stress factors influencing diagnostics, which help to identify horses affected by subclinical disease. It is important to note that certain diagnostic parameters are susceptible to stress-related distortions in results, such as those observed in arterial blood gas analysis (aBGA). Conversely, other parameters may offer greater sensitivity for diagnostic purposes concerning the classification of EA (Figure 1).
3. Effects of Sedation and Exercise on aBGA
Arterial blood gas analysis (aBGA) is an effective method for assessing alveolar ventilation and thus gas exchange. However, it is not a reliable diagnostic tool for horses with MEA or EA in remission, as it does not always demonstrate pathological changes in these cases [45]. In horses with SEA, the most significant value is the decreased PaO2. Some horses also exhibit increased PaCO2 and low pH values. [46].
The impact of sedation on the aBGA should not be neglected [47]. The potential for negative effects should be considered, and therefore arterial blood sampling with aBGA should be conducted prior to sedation for bronchoscopy. Sedation with detomidine and butorphanol results in a decrease in PaO2 and PvO2 and an increase in PaCO2 and P(A-a)O2 because of hypoventilation and therefore imbalance of ventilation and perfusion [48]. Furthermore, a decrease in heart rate is observed. While the respiratory rate remains largely unaltered following sedation with detomidine, the addition of butorphanol results in a notable decline. The interplay between pulmonary and cardiovascular effects ultimately leads to impaired gas exchange. Among sedation regimens involving romifidine and butorphanol, the combination of these agents demonstrates more pronounced negative effects on oxygen saturation than the combination of romifidine, butorphanol, and acepromacin [49].
In addition, exercise has a negative impact on aBGA especially the PaO2 due to alveolar hypoventilation resulting from augmented pulmonary resistance and increased work of breathing during exercise. The range of alteration concerning pO2, pCO2, and pO2(A-a) after exercise is highly variable, depending on the training status and condition of the horse [50,51]. For this reason, the effect is not suitable for more sensitive diagnostics, as even healthy horses exhibit exercise-induced hypoxemia [52]. Furthermore, no correlation was identified between the aBGA results of MEA-affected horses after exercise and the cytological MEA subtypes [53]. Consequently, the blood sample for aBGA should not only be obtained prior to sedation, but also prior to the exercise test. Additionally, the strain caused by transportation to the clinic, for instance, must be taken into account. It is recommended that the horses be kept in a stable for a few minutes/hours after arrival to allow for a period of calm before examine the arterial blood gases [54,55].
4. Effect of Exercise and Sedation on Pulmonary Function Tests
Pulmonary function testing (PFT) is a valuable method for determining the extent of lung function limitation [56]. As it is only offered by a few equine clinics due to its challenging and expensive implementation, its relevance is currently limited.
The gold standard in horses for measuring airflow and pleural pressure is esophageal balloon pneumotachography. This method is invasive, as it requires the insertion of a balloon catheter into the esophagus, which is then connected to a pressure transducer. The method is employed to ascertain pulmonary resistance, elastance, pleural pressure, and compliance [57].
In human medicine, the gold standard is spirometry [58]. This enables the formulation of statements pertaining to respiratory rate, peak inspiratory and expiratory flows, tidal volume, time to peak flow, and forced vital capacity. However, the implementation of these tests in horses is considerably more complex than in humans. The masks must be available in a range of sizes to accommodate the varying dimensions of the horses, and the horses themselves must be cooperative concerning the procedure. In the future, test protocols will have to be developed for the equine species. It is important to note that it is challenging to achieve a timed, forced, and complete inspiration and expiration in horses [56]. The results of the spirometry tests conducted with spontaneous breathing at rest indicate that there are no significant differences between the healthy and MEA affected horses [17]. In contrast, deviations from physiological values become more obvious during an exercise test. During such a test, horses suffering from bronchitis have a decreased ratio of time for expiration to time for inspiration in comparison to healthy ones. In addition, according to the exercise test, there is a significant correlation between the spirometry measurement results and the percentage of neutrophils in the TA [59]. This indicates that spirometry after exercise provides valuable information about the limitation of lung function due to EA. Apart from this, it is feasible to perform a single forced exhalation in sedated horses [17]. However, this is challenging to execute in a practical setting.
In flowmetric plethysmography with histamine bronchoprovocation at rest, both circumferential changes in the body are measured using sensors and the airflow from the nostrils using a face mask (pneumotachograph) [60]. The discrepancy between the airflow at the nose and the airflow at the chest represents the respiratory resistance [57]. This method is straightforward to perform, but it lacks the sensitivity required to detect minor limitations in lung function [61], among other things for the reason of dependence on environmental factors [62].
Another method for determining respiratory resistance is impulse oscillometry [63]. In forced oscillatory mechanics, pulses are sent into the lungs and the return path is measured using sensors. In the presence of bronchoconstriction or a large accumulation of mucus due to EA, the return impulse is smaller, allowing for the assessment of respiratory resistance [57].
In comparison to the diagnosis of SEA, these methods, particularly esophageal balloon pneumotachography, demonstrate reduced sensitivity in the diagnosis of MEA [64]. In horses with mild symptoms, the aforementioned methods can be combined with histamine bronchoprovocation or bronchodilation with albuterol. Horses with MEA demonstrate bronchoconstriction at lower histamine doses than healthy horses. In horses with increased pulmonary resistance, the bronchodilator challenge presents an opportunity to measure the capacity of the airways to bronchodilate [1,57].
Electrical impedance tomography (EIT) has been demonstrated to be an effective method for visualizing lung ventilation and perfusion without sedation or anesthesia [65,66]. Electrodes are placed around the equine thorax, which then generate a cross-sectional image of impedance changes based on changing ratios of air, fluid, fat, and ion concentration [67]. This allows for the detection of pathological changes such as pulmonary fibrosis and fluid accumulation [65]. While implementation for equine medicine are still under development, approaches are already available [56]. EIT enables the precise determination of peak inspiratory and expiratory flow, which enables the measurement of bronchoconstriction induced by exercise. This is observed to be enhanced in horses with severe equine asthma following an exercise test, in comparison to healthy horses. Conversely, no significant correlation is evident in horses with mild asthma, which renders this method unsuitable for the early diagnosis of mild asthma [68].
Apart from exercise prior to pulmonary function testing, sedation with alpha 2 - agonists also affects the outcomes of pulmonary function tests. Sedation with detomidine and butorphanol results in hypoventilation of the lungs in consequence of reduced respiratory rate [47] and bronchoconstriction due to parasympathetic stimulation [66,69]. Furthermore, obstruction of the upper airways by nasal mucous membrane swelling is caused by the lowering of the head during sedation [70]. Additionally, the reverse bronchodilator effects of xylazine, detomidine, and acepromazine following initiated bronchoconstriction may lead to the falsification of the PFT - outcomes [66,69].
In contrast to arterial blood gas analysis, in which both factors, exercise and sedation, have a negative influence on the results, the PFT - results are falsified by sedation, whereas exercise leads to more sensitive PFT - diagnostics.
In general, diagnostics using PFT should always be combined with further diagnostics such as the BALF cytology examination [59]. The reason for this is that PFT alone is not sufficiently informative. The correlation between PFT and BAL cytology is described in disparate ways in the literature. Some studies find a significant correlation [17,61,71], while others do not [72,73].
5. Effects of Short-Term Exercise on Lower Airways
It may also be beneficial to consider the potential benefits of short-term exercise prior to EA diagnostics, particularly in the context of more comprehensive diagnostic procedures. An exercise test can diagnose subclinical, asymptomatic racehorses as equine asthmatics based on the total cell count in BALF exceeding 530 cells/microlitre [74]. Following a standardized exercise test, the cytology of BALF can indicate equine asthma in approximately 50% of asymptomatic racehorses. In particular, the total cell count appears to be a factor that increases after exercise [74]. The number of neutrophil and eosinophil granulocytes does not increase in all horses exhibiting an elevated total cell count in BALF. The heart rate, respiratory rate and rectal temperature of horses diagnosed with EA-positive cytology and classified as healthy did not exhibit significant differences following exercise. It remains unclear whether the exercise-induced alterations in BALF cytology are exclusive to EA-positive horses or extend to healthy individuals as well. It is unresolved whether an increased total cell count in BALF after exercise is sufficient for diagnosing EA. In particular, it may be more reliable to utilize the total cell count in ELF, as previously described by the authors.
TA cytology is also affected by exercise with the percentage of neutrophils rising in the TA by 24–87% compared to the pre-exercise state. This is presumably due to an increase in lung movement, expiratory flow, and mucociliary transport, which brings the cytology closer to the true cytologic composition in the lungs [75,76]. The prior exercise can be used to advantage in the diagnosis of subclinical cases, although BALF cytology is still preferable to TA cytology as it is clearly more representative [19].
In addition to its impact on cytology, exercise stress on the airways alters the composition of inflammatory mediators. In horses with EA in exacerbation, the concentration of endothelin, a bronchoconstrictive and vasoactive peptide, is significantly higher in BALF and blood samples compared to healthy horses. Furthermore, the concentration of endothelin in BALF of asthmatic horses increases following exercise, whereas healthy horses do not demonstrate a comparable increase. The precise relationship between this increase and the impairment of lung function and the cytology of BALF remains unclear. An increase in neutrophils in the BALF of healthy horses has been demonstrated after exercise, whereas no significant effect has been recognized in asthmatic horses [77]. A comparison of the overall cytology of BALF, rather than merely the neutrophils has not been published to our knowledge.
Looking at other species, several other factors may be relevant for the horse: In men, asthmatics with exercise-induced bronchoconstriction (EIB) demonstrate an elevation in histamine and interleukin-8 (neutrophil chemotactic factor) in the blood following an exercise test on a treadmill [78]. Additionally, the concentration of high-sensitivity C-reactive protein (hs-CRP) in the blood serum is elevated following acute exercise in asthmatics with exercise-induced bronchoconstriction (EIB) [79]. Moreover, this physical exertion affects the airway epithelium, leading to an overexpression of cysteinyl leukotrienes [80], a relative underproduction of prostaglandin E2, and an increase in eosinophilia within the airways [81,82]. The cytology of induced sputum from individuals who develop exercise-induced bronchoconstriction demonstrates a higher concentration of epithelial cells [82].
Similar outcomes have been observed in healthy human subjects. An increase in the total cell count, leukocyte count, and epithelial cell count in the nasal lavage fluid was found after 180 minutes of exercise [83]. In response to physical stress, catecholamine and cortisol levels rise, which results in an increase in inflammatory mediators, including cytokines, leukotrienes, and prostaglandins from the lower airways [84]. The exercise-induced damage to the airway epithelium is attributed to osmotic changes and inadequate conditioning of the air. An increase in bronchial epithelial cells in the sputum following a half marathon serves as evidence of damage to the airway epithelium. Additionally, an increase in interleukin-8 has been observed in induced sputum [85]. In horses, interleukin-8 increase after exercise is known in bloodserum [86].These findings collectively indicate the presence of an inflammatory response, characterised by increased epithelial permeability, resulting from epithelial injury. This, in turn, leads to a heightened release of inflammatory mediators, a larger volume of sputum, and an increased presence of granulocytes within the airways.
Further research is required to elucidate the effect of exercise stress on asthma diagnostics in mild cases, particularly in horses.
6. Effects of Long-Term Exercise on Lower Airways
In addition to short-term exercise just before the diagnostic examination, routine training has been demonstrated to impact the cytology of the BALF, particularly in racehorses. This does not affect the percentages of neutrophils, eosinophils and mast cells, but rather the total cell count, erythrocytes and hemosiderophages. This is an indicator of non-specific pneumonia of unknown origin and additionally indicates a correlation between the intensity and duration of exercise and the occurrence of exercise-induced pulmonary hemorrhage (EIPH) [87]. A greater proportion of erythrocytes and also neutrophil granulocytes can be observed in racehorses subjected to a high exercise load in comparison to those under a lower exercise load [88].
Conversely, other findings are inconsistent, indicating reduced total cell counts and neutrophil levels in horses examined over a 10-week training period [89]. It seems plausible that the lower airways adapt to prior-examination training. The authors also postulate that different BAL volumes and environmental conditions may be contributing factors. The proportion of neutrophils in the cytology of the BALF is significantly higher with a smaller BAL volume (250 ml) than with a larger volume (500 ml). The total cell count yielded no statistically significant results with regard to different BAL volumes [21]. In other studies, a lower proportion of mast cells, a higher total cell count, and a higher number of macrophages and lymphocytes were observed in small volumes [90].
In humans, research on the incidence of exercise-induced asthma indicates that competitive swimmers have a higher risk of developing asthma due to chlorine exposure than tennis players. Inflammation of the airways with granulocytes, macrophages, and lymphocytes, as well as airway remodeling, have been demonstrated [84,91,92]. Regular running also increases the number of polymorphonuclear leukocytes (PMNs) in sputum, but there is no evidence of activation of these cells [93].
In mice, the bronchial epithelium shows a loss of ciliated cells after regular exercise, a slight increase in thickness, an unchanged presence of club cells (secretory active), increased apoptosis and proliferation. The number of leukocytes in the wall and lumen of bronchioles is higher in exercised than in unexercised mice. However, these inflammatory cells do not appear to be activated [94].
Obviously, the results regarding the effects of long-term exercise on the airways are not really consistent. It is difficult to compare the literature, which consists of different training constructs and study designs. The aspect of influencing the airways is understandable, but regarding the goal of early diagnosis of mild EA, short-term exercise seems to be more appropriate.
7. Influence of Inhaling Cold Air on the Airways
In addition to short- and long-term exercise (training), respiratory stress due to environmental factors such as cold or chlorinated air has an impact on cytology. These factors trigger an inflammatory response in the lungs because the cold and dry air is not sufficiently warmed by the time it reaches the lungs [84]. In humans, this is known as “ski asthma” [95]. The resulting epithelial damage leads to the release of inflammatory mediators and neutrophilia in the airways, lung tissue remodeling, and bronchial hyperreactivity [96]. The damage is caused by inhalation of cold air or, in swimmers, by inhalation of chlorinated air [93,97].
In healthy horses, inhalation of cold air during exercise results in an increase in bronchial epithelial cells and cytokines characteristic of the Th2 phenotype in BALF. Upregulated cytokines after cold air inhalation (-5 degrees) are IL-4, IL-5 and IL-10 to a large extent and IL-2 and IL-6 to a lesser extent. Activated mast cells are known to be involved in Th2 cytokine production, although other sources may be involved as BALF contains very low levels of mast cells after cold air exercise. It is suggested that lower respiratory tract lymphocytes amplify the cytokine response, while their production is preceded by other cells such as mast cells. A cellular inflammatory response cannot be detected in BALF five hours after exercise, which may be due to the timing of BAL. This means that inhalation of cold air promotes inflammatory processes in the lungs that appear to be similar to asthma [98]. Further research on horses suffering from EA and the influence of exercise under cold air conditions just prior to BAL may provide another way to stress the airways for a more significant cellular representation of EA. Of course, compared to a standardized exercise test under natural environmental conditions, a cold air exercise test requires a much more elaborate implementation. It would be beneficial for future research to explore if this complexity provides an added value in terms of more sensitive EA diagnosis.
8. Co-Incidence of Pulmonary Hemosiderosis and Other Respiratory Diseases
In addition to the aforementioned diagnostic influences, other diseases may precipitate the occurrence of EA or vice versa.
Hemosiderophages can be detected in the BALF of asthmatic horses. The more severe the equine asthma, the more hemosiderophages are found in the BALF [99].
Notably and contrary to the authors’ expectations, MEA horses have a higher incidence of BALF hemosiderophages than horses with SEA [100]. It should be noted that highly stressed horses, such as racehorses, were not excluded from this study, which may have biased the results. Horses with EIPH are often racehorses, which are usually young. If these horses also suffer from equine asthma, it is usually the mild to moderate form, which is often diagnosed in horses under 7 years of age.
BALF cytology in EA, EIPH or combined disease shows no significant difference in leucocytes. Therefore, the inflammatory response appears to be similar with one disease possibly causing the other. In EIPH, the bleeding in the lungs causes an inflammatory response that is able to induce equine asthma. The resulting bronchoconstriction leads to increased intrapleural pressure, which in turn increases the risk of EIPH [101].
Experimentally induced pneumonia also increases the risk of EIPH [102]. This is due to the altered vascular permeability caused by the inflammation. In the case of severe exercise, the increase in blood pressure is an important cause of EIPH. Angiogenesis and fibrosis induced by inflammation exacerbate the situation [103].
A correlation between respiratory disease and the occurrence of pulmonary hemosiderosis is also common in dogs and cats [104]. Hemosiderophages can be detected in 75% of tracheal lavage samples from cats suffering from feline asthma. Increased erythrocyte diapedesis is the result of increased pulmonary vascular congestion due to cytokine release and vasodilation. In addition, microtrauma of the pulmonary vessels due to coughing may contribute [105].
In humans, idiopathic pulmonary hemosiderosis is known to induce asthma-like episodes of bronchiolitis [106].
With regard to the diagnosis of EA, this aspect means that a coexistence of EA and EIPH is plausible and that one condition may cause the other. Consequently, the etiology of EA may differ from the conventionally accepted cause. This is of paramount importance for the management and treatment of the disease.
9. Conclusions
The respiratory tract reacts differently to various stresses. Apart from short- and long-term exercise like physical training, cold and chlorinated air as well as sedation has an effect on the airways. These stress factors influence various parameters in EA diagnostics including aBGA, PFT, scoring of respiratory secretion and TA or BALF cytology. Transport, excitement and sedation affect aBGA. In contrast, the impact of exercise and cold air stress on cytology might be useful to amplify the diagnostic findings for an early diagnosis during a low stage of disease. EA-diagnostics may be improved by a standardized exercise-test before performing the bronchoalveolar lavage to differentiate between mild and moderate disease. Further research will help to classify low-grade disease in equine asthma and possibly to identify more endotypes as known in human medicine.
Author Contributions
Conceptualization, A.B.; writing—original draft preparation, L.L.; writing—review and editing, A.B.; visualization, L.L.; supervision, A.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Couetil, L.; Cardwell, J.M.; Leguillette, R.; Mazan, M.; Richard, E.; Bienzle, D.; Bullone, M.; Gerber, V.; Ivester, K.; Lavoie, J.-P.; et al. Equine Asthma: Current Understanding and Future Directions. Front. Vet. Sci. 2020, 7, 450. [Google Scholar] [CrossRef]
- Couëtil, L.L.; Cardwell, J.M.; Gerber, V.; Lavoie, J. -P.; Léguillette, R.; Richard, E.A. Inflammatory Airway Disease of Horses—Revised Consensus Statement. J. Vet. Intern. Med. 2016, 30, 503–515. [Google Scholar] [CrossRef] [PubMed]
- Couëtil, L. What Do We Know About the Pathophysiology of Equine Asthma? AAEP Proceedings 2021, 67, 460–464. [Google Scholar]
- Martin, JG. Classification of Asthma. Proceedings of the 2nd Havemeyer Workshop on IAD 2014, Cabourg, Frankreich: 11-13.
- Allen, K.J.; Tremaine, W.H. Prevalence of Inflammatory Airway Disease in National Hunt Horses Referred for Investigation of Poor Athletic Performance. Equine Vet. J. 2006, 36, 529–534. [Google Scholar] [CrossRef] [PubMed]
- Robinson, N.E.; Karmaus, W.; Holcombe, S.J.; Carr, E.A.; Derksen, F.J. Airway Inflammation in Michigan Pleasure Horses: Prevalence and Risk Factors. Equine Vet. J. 2006, 38, 293–299. [Google Scholar] [CrossRef]
- Gerber, V.; Robinson, N.E.; Luethi, S.; Marti, E.; Wampfler, B.; Straub, R. Airway Inflammation and Mucus in Two Age Groups of Asymptomatic Well-Performing Sport Horses. Equine Vet. J. 2003, 35, 491–495. [Google Scholar] [CrossRef]
- Pirie, R.S. Recurrent Airway Obstruction: A Review. Equine Vet. J. 2014, 46, 276–288. [Google Scholar] [CrossRef]
- Bosshard, S.; Gerber, V. Evaluation of Coughing and Nasal Discharge as Early Indicators for An Increased Risk to Develop Equine Recurrent Airway Obstruction (RAO). J. Vet. Intern. Med. 2014, 28, 618–623. [Google Scholar] [CrossRef]
- Leclere, M.; Lavoie-Lamoureux, A.; Gélinas-Lymburner, É.; David, F.; Martin, J.G.; Lavoie, J.-P. Effect of Antigenic Exposure on Airway Smooth Muscle Remodeling in an Equine Model of Chronic Asthma. Am. J. Respir. Cell Mol. Biol. 2011, 45, 181–187. [Google Scholar] [CrossRef]
- Leclere, M.; Lavoie-Lamoureux, A.; Joubert, P.; Relave, F.; Setlakwe, E.L.; Beauchamp, G.; Couture, C.; Martin, J.G.; Lavoie, J.-P. Corticosteroids and Antigen Avoidance Decrease Airway Smooth Muscle Mass in an Equine Asthma Model. Am. J. Respir. Cell Mol. Biol. 2012, 47, 589–596. [Google Scholar] [CrossRef]
- Ceriotti, S.; Bullone, M.; Leclere, M.; Ferrucci, F.; Lavoie, J.-P. Severe Asthma Is Associated with a Remodeling of the Pulmonary Arteries in Horses. PLOS ONE 2020, 15, e0239561. [Google Scholar] [CrossRef] [PubMed]
- Gerber, V.; Straub, R.; Marti, E.; Hauptman, J.; Herholz, C.; King, M.; Imhof, A.; Tahon, L.; Robinson, N.E. Endoscopic Scoring of Mucus Quantity and Quality: Observer and Horse Variance and Relationship to Inflammation, Mucus Viscoelasticity and Volume. Equine Vet. J. 2004, 36, 576–582. [Google Scholar] [CrossRef] [PubMed]
- Couetil, L.L.; Thompson, C.A. Airway Diagnostics. Vet. Clin. North Am. Equine Pract. 2020, 36, 87–103. [Google Scholar] [CrossRef] [PubMed]
- Cian, F.; Monti, P.; Durham, A. Cytology of the Lower Respiratory Tract in Horses: An Updated Review. Equine Vet. Educ. 2015, 27, 544–553. [Google Scholar] [CrossRef]
- Rossi, H.; Virtala, A.-M.; Raekallio, M.; Rahkonen, E.; Rajamäki, M.M.; Mykkänen, A. Comparison of Tracheal Wash and Bronchoalveolar Lavage Cytology in 154 Horses With and Without Respiratory Signs in a Referral Hospital Over 2009−2015. Front. Vet. Sci. 2018, 5, 61. [Google Scholar] [CrossRef] [PubMed]
- Couëtil, L.L.; Rosenthal, F.S.; DeNicola, D.B.; Chilcoat, C.D. Clinical Signs, Evaluation of Bronchoalveolar Lavage Fluid, and Assessment of Pulmonary Function in Horses with Inflammatory Respiratory Disease. Am. J. Vet. Res. 2001, 62, 538–546. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, A.M. Bronchoalveolar Lavage: Sampling Technique and Guidelines for Cytologic Preparation and Interpretation. Vet. Clin. North Am. Equine Pract. 2008, 24, 423–435. [Google Scholar] [CrossRef]
- Derksen, F.J.; Brown, C.M.; Sonea, I.; Darien, B.J.; Robinson, N.E. Comparison of Transtracheal Aspirate and Bronchoalveolar Lavage Cytology in 50 Horses with Chronic Lung Disease. Equine Vet. J. 1989, 21, 23–26. [Google Scholar] [CrossRef]
- Malikides, N.; Hughes, K.; Hodgson, D.; Hodgson, J. Comparison of Tracheal Aspirates and Bronchoalveolar Lavage in Racehorses 2. Evaluation of the Diagnostic Significance of Neutrophil Percentage. Aust. Vet. J. 2003, 81, 685–687. [Google Scholar] [CrossRef]
- Orard, M.; Depecker, M.; Hue, E.; Pitel, P.-H.; Couroucé-Malblanc, A.; Richard, E.A. Influence of Bronchoalveolar Lavage Volume on Cytological Profiles and Subsequent Diagnosis of Inflammatory Airway Disease in Horses. Vet. J. 2016, 207, 193–195. [Google Scholar] [CrossRef]
- Rennard, S.I.; Basset, G.; Lecossier, D.; O’Donnell, K.M.; Pinkston, P.; Martin, P.G.; Crystal, R.G. Estimation of Volume of Epithelial Lining Fluid Recovered by Lavage Using Urea as Marker of Dilution. J. Appl. Physiol. 1986, 60, 532–538. [Google Scholar] [CrossRef] [PubMed]
- McGorum, B.C.; Dixon, P.M.; Halliwell, R.E.W.; Irving, P. Evaluation of Urea and Albumen as Endogenous Markers of Dilution of Equine Bronchoalveolar Lavage Fluid. Res. Vet. Sci. 1993, 55, 52–56. [Google Scholar] [CrossRef] [PubMed]
- Gy, C.; Leclere, M.; Vargas, A.; Grimes, C.; Lavoie, J. Investigation of Blood Biomarkers for the Diagnosis of Mild to Moderate Asthma in Horses. J. Vet. Intern. Med. 2019, 33, 1789–1795. [Google Scholar] [CrossRef] [PubMed]
- Bullone, M.; De Lagarde, M.; Vargas, A.; Lavoie, J. -P. Serum Surfactant Protein D and Haptoglobin as Potential Biomarkers for Inflammatory Airway Disease in Horses. J. Vet. Intern. Med. 2015, 29, 1707–1711. [Google Scholar] [CrossRef]
- Lavoie-Lamoureux, A.; Leclere, M.; Lemos, K.; Wagner, B.; Lavoie, J.-P. Markers of Systemic Inflammation in Horses with Heaves. J. Vet. Intern. Med. 2012, 26, 1419–1426. [Google Scholar] [CrossRef]
- Miskovic Feutz, M.; Couetil, L.L.; Riley, C.P.; Zhang, X.; Adamec, J.; Raskin, R.E. Secretoglobin and Transferrin Expression in Bronchoalveolar Lavage Fluid of Horses with Chronic Respiratory Disease. J. Vet. Intern. Med. 2015, 29, 1692–1699. [Google Scholar] [CrossRef]
- Ramseyer, A.; Gaillard, C.; Burger, D.; Straub, R.; Jost, U.; Boog, C.; Marti, E.; Gerber, V. Effects of Genetic and Environmental Factors on Chronic Lower Airway Disease in Horses. J. Vet. Intern. Med. 2007, 21, 149–156. [Google Scholar] [CrossRef]
- Hansen, S.; Otten, N.D.; Spang-Hanssen, L.; Bendorff, C.; Jacobsen, S. Neutrophil Gelatinase-associated Lipocalin as a Potential Biomarker for Equine Asthma. Equine Vet. J. 2024, 56, 44–50. [Google Scholar] [CrossRef]
- Barton, A.K.; Shety, T.; Bondzio, A.; Einspanier, R.; Gehlen, H. Metalloproteinases and Their Tissue Inhibitors in Comparison between Different Chronic Pneumopathies in the Horse. Mediators Inflamm. 2015, 2015, 1–9. [Google Scholar] [CrossRef]
- Barton, A.K.; Pelli, A.; Rieger, M.; Gehlen, H. Procalcitonin as a Biomarker in Equine Chronic Pneumopathies. BMC Vet. Res. 2016, 12, 281. [Google Scholar] [CrossRef]
- Janssen, P.; Tosi, I.; Hego, A.; Maréchal, P.; Marichal, T.; Radermecker, C. Neutrophil Extracellular Traps Are Found in Bronchoalveolar Lavage Fluids of Horses With Severe Asthma and Correlate With Asthma Severity. Front. Immunol. 2022, 13, 921077. [Google Scholar] [CrossRef]
- Art, T.; Franck, T.; Lekeux, P.; de Moffarts, B.; Couëtil, L.; Becker, M.; Kohnen, S.; Deby-Dupont, G.; Serteyn, D. Myeloperoxidase Concentration in Bronchoalveolar Lavage Fluid from Healthy Horses and Those with Recurrent Airway Obstruction. The Canadian Journal of Veterinary Research 2006, 70, 291–296. [Google Scholar] [PubMed]
- Bazzano, M.; Laghi, L.; Zhu, C.; Magi, G.E.; Tesei, B.; Laus, F. Respiratory Metabolites in Bronchoalveolar Lavage Fluid (BALF) and Exhaled Breath Condensate (EBC) Can Differentiate Horses Affected by Severe Equine Asthma from Healthy Horses. BMC Vet. Res. 2020, 16, 233. [Google Scholar] [CrossRef] [PubMed]
- GigueÁre, S.; Viel, L.; Lee, E.; MacKay, R.J.; Hernandez, J.; Franchini, M. Cytokine Induction in Pulmonary Airways of Horses with Heaves and Effect of Therapy with Inhaled ¯uticasone Propionate. Vet. Immunol. Immunopathol. 2002, 85, 147–158. [Google Scholar] [CrossRef] [PubMed]
- Woodrow, J.S.; Hines, M.; Sommardahl, C.; Flatland, B.; Lo, Y.; Wang, Z.; Sheats, M.K.; Lennon, E.M. Initial Investigation of Molecular Phenotypes of Airway Mast Cells and Cytokine Profiles in Equine Asthma. Front. Vet. Sci. 2023, 9, 997139. [Google Scholar] [CrossRef]
- Gray, P.R.; Derksen, F.J.; Robinson, N.E.; Carpenter-Deyo, L.J.; Johnson, H.G.; Roth, R.A. The Role of Cyclooxygenase Products in the Acute Airway Obstruction and Airway Hyperreactivity of Ponies with Heaves. Am. Rev. Respir. Dis. 1989, 140, 154–160. [Google Scholar] [CrossRef]
- Watson, E.D.; Sweeney, C.R.; Steensma, K.A. Arachidonate Metabolites in Bronchoalveolar Lavage Fluid from Horses with and without COPD. Equine Vet. J. 1992, 24, 379–381. [Google Scholar] [CrossRef]
- Hare, J.E.; Viel, L.; Conlon, P.D.; Marshall, J.S. In vitro allergen-induced degranulation of pulmonary mast cells from horses with recurrent airway obsruction (heaves). Am. J. Vet. Res. 1999, 60, 841–847. [Google Scholar] [CrossRef]
- Christmann, U.; Hite, R.D.; Witonsky, S.G.; Buechner-Maxwell, V.A.; Wood, P.L. Evaluation of Lipid Markers in Surfactant Obtained from Asthmatic Horses Exposed to Hay. Am. J. Vet. Res. 2019, 80, 300–305. [Google Scholar] [CrossRef]
- Niedzwiedz, A.; Borowicz, H.; Januszewska, L.; Markiewicz-Gorka, I.; Jaworski, Z. Serum 8-Hydroxy-2-Deoxyguanosine as a Marker of DNA Oxidative Damage in Horses with Recurrent Airway Obstruction. Acta Vet. Scand. 2015, 58, 38. [Google Scholar] [CrossRef]
- Schmallenbach, K.H.; Rahman, I.; Sasse, H.H.L.; Dixon, P.M.; Halliwell, R.E.W.; McGorum, B.C.; Crameri, R.; Miller, H.R.P. Studies on Pulmonary and Systemic Aspergillus Fumigatus-Specific IgE and IgG Antibodies in Horses Affected with Chronic Obstructive Pulmonary Disease (COPD). Vet. Immunol. Immunopathol. 1998, 66, 245–256. [Google Scholar] [CrossRef]
- Calzetta, L.; Rogliani, P.; Page, C.; Roncada, P.; Pistocchini, E.; Soggiu, A.; Piras, C.; Urbani, A.; Matera, M.G. Clinical Effect of Corticosteroids in Asthma-affected Horses: A Quantitative Synthesis. Equine Vet. J. 2018, 50, 594–601. [Google Scholar] [CrossRef]
- Gehlen, H.; Oey, L.; Rohn, K.; Bilzer, T.; Stadler, P. Pulmonary Dysfunction and Skeletal Muscle Changes in Horses with RAO. J. Vet. Intern. Med. 2008, 22, 1014–1021. [Google Scholar] [CrossRef]
- Ferro, E.; Ferrucci, F.; Zucca, E.; Di Fabio, V.; Castoldi, S. Arterial Blood Gas Analysis in 53 Racehorses with a Diagnosis of Small Airway Inflammatory Disease (SAID). J. Equine Vet. Sci. 2002, 22, 165–168. [Google Scholar] [CrossRef]
- Simões, J.; Batista, M.; Tilley, P. The Immune Mechanisms of Severe Equine Asthma—Current Understanding and What Is Missing. Animals 2022, 12, 744. [Google Scholar] [CrossRef]
- Lavoie, J.P.; Phan, S.T.; Blais, D. Effects of a combination of detomidine and butorphanol on respiratory function in horses with or without chronic obstructive pulmonary disease. Am. J. Vet. Res. 1996, 57, 705–709. [Google Scholar] [CrossRef]
- Nyman, G.; Marntell, S.; Edner, A.; Funkquist, P.; Morgan, K.; Hedenstierna, G. Effect of Sedation with Detomidine and Butorphanol on Pulmonary Gas Exchange in the Horse. Acta Vet. Scand. 2009, 51, 22. [Google Scholar] [CrossRef]
- Marntell, S.; Nyman, G.; Funkquist, P.; Hedenstierna, G. Effects of Acepromazine on Pulmonary Gas Exchange and Circulation during Sedation and Dissociative Anaesthesia in Horses. Vet. Anaesth. Analg. 2005, 32, 83–93. [Google Scholar] [CrossRef]
- Klein, H.-J.; Deegen, E. Beurteilung von Blutgasparametern des arteriellen Blutes von Pferden unter besonderer Berücksichtigung der alveoloarteriellen Sauerstoffdifferenz. Pferdeheilkunde 2 1986, 6, 331–336. [Google Scholar] [CrossRef]
- Durando, M.M.; Martin, B.B.; Davidson, E.J.; Birks, E.K. Correlations between Exercising Arterial Blood Gas Values, Tracheal Wash Findings and Upper Respiratory Tract Abnormalities in Horses Presented for Poor Performance. Equine Vet. J. 2006, 38, 523–528. [Google Scholar] [CrossRef] [PubMed]
- Wagner, P.D.; Gillespie, J.R.; Landgren, G.L.; Fedde, M.R.; Jones, B.W.; DeBowes, R.M.; Pieschl, R.L.; Erickson, H.H. Mechanism of Exercise-Induced Hypoxemia in Horses. J. Appl. Physiol. 1989, 66, 1227–1233. [Google Scholar] [CrossRef] [PubMed]
- Nolen-Walston, R.D.; Harris, M.; Agnew, M.E.; Martin, B.B.; Reef, V.B.; Boston, R.C.; Davidson, E.J. Clinical and Diagnostic Features of Inflammatory Airway Disease Subtypes in Horses Examined Because of Poor Performance: 98 Cases (2004–2010). J. Am. Vet. Med. Assoc. 2013, 242, 1138–1145. [Google Scholar] [CrossRef] [PubMed]
- Art, T.; Lekeux, P. Ventilatory and Arterial Blood Gas Tension Adjustments to Strenuous Exercise in Standardbreds. Am. J. Vet. Res. 1995, 56, 1332–1337. [Google Scholar] [CrossRef]
- Padilla, D.J.; McDonough, P.; Kindig, C.A.; Erickson, H.H.; Poole, D.C. Ventilatory Dynamics and Control of Blood Gases after Maximal Exercise in the Thoroughbred Horse. J. Appl. Physiol. 2004, 96, 2187–2193. [Google Scholar] [CrossRef]
- Kozłowska, N.; Wierzbicka, M.; Jasiński, T.; Domino, M. Advances in the Diagnosis of Equine Respiratory Diseases: A Review of Novel Imaging and Functional Techniques. Animals 2022, 12, 381. [Google Scholar] [CrossRef]
- Robins, T.-J.; Bedenice, D.; Mazan, M. A Longitudinal Analysis of Equine Asthma Presentation and Response to Treatment Using Lung Function Testing and BAL Cytology Analysis in Combination with Owner Perception. Animals 2023, 13, 3387. [Google Scholar] [CrossRef] [PubMed]
- Agustí, A.; Celli, B.R.; Criner, G.J.; Halpin, D.; Anzueto, A.; Barnes, P.; Bourbeau, J.; Han, M.K.; Martinez, F.J.; Montes De Oca, M.; et al. Global Initiative for Chronic Obstructive Lung Disease 2023 Report: GOLD Executive Summary. Eur. Respir. J. 2023, 61, 2300239. [Google Scholar] [CrossRef]
- Evans, D.L.; Kiddell, L.; Smith, C.L. Pulmonary Function Measurements Immediately after Exercise Are Correlated with Neutrophil Percentage in Tracheal Aspirates in Horses with Poor Racing Performance. Res. Vet. Sci. 2011, 90, 510–515. [Google Scholar] [CrossRef]
- Hoffman, A.M.; Mazan, M.R. How to Test for Airway Hyper-Reactivity: Toward a Better Diagnosis of Inflammatory Airway Disease. AAEP Proceedings 2005, 51, 265–269. [Google Scholar]
- Bedenice, D.; Mazan, M.R.; Hoffman, A.M. Association between Cough and Cytology of Bronchoalveolar Lavage Fluid and Pulmonary Function in Horses Diagnosed with Inflammatory Airway Disease. J. Vet. Intern. Med. 2008, 22, 1022–1028. [Google Scholar] [CrossRef]
- Nolen-Walston, R.D.; Kuehn, H.; Boston, R.C.; Mazan, M.R.; Wilkins, P.A.; Bruns, S.; Hoffman, A.M. Reproducibility of Airway Responsiveness in Horses Using Flowmetric Plethysmography and Histamine Bronchoprovocation. J. Vet. Intern. Med. 2009, 23, 631–635. [Google Scholar] [CrossRef]
- Van Erck, E.; Votion, D.; Art, T.; Lekeux, P. Measurement of Respiratory Function by Impulse Oscillometry in Horses. Equine Vet. J. 2004, 36, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Simões, J.; Tilley, P. Decision Making in Severe Equine Asthma—Diagnosis and Monitoring. Animals 2023, 13, 3872. [Google Scholar] [CrossRef]
- Frerichs, I.; Amato, M.B.P.; Van Kaam, A.H.; Tingay, D.G.; Zhao, Z.; Grychtol, B.; Bodenstein, M.; Gagnon, H.; Böhm, S.H.; Teschner, E.; et al. Chest Electrical Impedance Tomography Examination, Data Analysis, Terminology, Clinical Use and Recommendations: Consensus Statement of the TRanslational EIT developmeNt stuDy Group. Thorax 2017, 72, 83–93. [Google Scholar] [CrossRef]
- Secombe, C.; Adler, A.; Hosgood, G.; Raisis, A.; Mosing, M. Can Bronchoconstriction and Bronchodilatation in Horses Be Detected Using Electrical Impedance Tomography? J. Vet. Intern. Med. 2021, 35, 2035–2044. [Google Scholar] [CrossRef]
- Wang, Y.-M.; Sun, X.-M.; Zhou, Y.-M.; Chen, J.-R.; Cheng, K.-M.; Li, H.-L.; Yang, Y.-L.; Zhang, L.; Zhou, J.-X. Use of Electrical Impedance Tomography (EIT) to Estimate Global and Regional Lung Recruitment Volume (VREC) Induced by Positive End-Expiratory Pressure (PEEP): An Experiment in Pigs with Lung Injury. Med. Sci. Monit. 2020, 26. [Google Scholar] [CrossRef]
- Herteman, N.; Mosing, M.; Waldmann, A.D.; Gerber, V.; Schoster, A. Exercise-induced Airflow Changes in Horses with Asthma Measured by Electrical Impedance Tomography. J. Vet. Intern. Med. 2021, 35, 2500–2510. [Google Scholar] [CrossRef]
- Hoffman, A.M. Clinical Application of Pulmonary Function Testing in Horses. International Veterinary Information Service 2002. [Google Scholar]
- Lavoie, J.P.; Pascoe, J.R.; Kurpershoek, J.C. Effect of head and neck position on respiratory mechanics in horses sedated with xylazine. Am. J. Vet. Res. 1992, 53, 1652–1657. [Google Scholar] [CrossRef]
- Richard, E.A.; Fortier, G.D.; Denoix, J. -M.; Art, T.; Lekeux, P.M.; Erck, E.V. Influence of Subclinical Inflammatory Airway Disease on Equine Respiratory Function Evaluated by Impulse Oscillometry. Equine Vet. J. 2009, 41, 384–389. [Google Scholar] [CrossRef] [PubMed]
- Wichtel, M.; Gomez, D.; Burton, S.; Wichtel, J.; Hoffman, A. Relationships between Equine Airway Reactivity Measured by Flowmetric Plethysmography and Specific Indicators of Airway Inflammation in Horses with Suspected Inflammatory Airway Disease. Equine Vet. J. 2016, 48, 466–471. [Google Scholar] [CrossRef]
- Cullimore, A.; Secombe, C.; Lester, G.; Robertson, I. Bronchoalveolar Lavage Fluid Cytology and Airway Hyper-reactivity in Clinically Normal Horses. Aust. Vet. J. 2018, 96, 291–296. [Google Scholar] [CrossRef] [PubMed]
- Beling, J.C.F.; Santos, D.M.S.A.; Ferreira, M.P.; Silva, P.C.A.R.; Costa, M.F.M.; Lessa, D.A.B. Post-exercise Endoscopic and Cytologic Diagnosis of Equine Asthma Syndrome in Asymptomatic Brazilian Pacers. Equine Vet. Educ. 2022, 34, 355–361. [Google Scholar] [CrossRef]
- Malikides, N.; Hughes, K.; Hodgson, J. Comparison of Tracheal Aspirates before and after High-speed Treadmill Exercise in Racehorses. Aust. Vet. J. 2007, 85, 414–419. [Google Scholar] [CrossRef] [PubMed]
- Martin, B.B.; Beech, J.; Parente, E.J. Cytologic Examination of Specimens Obtained by Means of Tracheal Washes Performed before and after High-Speed Treadmill Exercise in Horses with a History of Poor Performance. J. Am. Vet. Med. Assoc. 1999, 214, 673–677. [Google Scholar] [CrossRef]
- Benamou, A.E.; Art, T.; Marlin, D.J.; Roberts, C.A.; Lekeux, P. Effect of exercise on concentrations of immunoreactive endothelin in bronchoalveolar lavage fluid of normal horses and horses with chronic obstructive pulmonary disease. Equine Vet. J. 1999, 31, 92–95. [Google Scholar] [CrossRef] [PubMed]
- Lee, T.H.; Walport, M.J. Exercise-Induced Release of Hisbmine and Neutrophil Chemotactic Factor in Atopic Asthmatics. J ALLERGY CLIN IMMUNOL 1982, 70. [Google Scholar] [CrossRef] [PubMed]
- Zietkowski, Z.; Skiepko, R.; Tomasiak-Lozowska, M.M.; Mroczko, B.; Szmitkowski, M.; Bodzenta-Lukaszyk, A. Changes in High-Sensitivity C-Reactive Protein in Serum and Exhaled Breath Condensate after Intensive Exercise in Patients with Allergic Asthma. Int. Arch. Allergy Immunol. 2010, 153, 75–85. [Google Scholar] [CrossRef]
- Bikov, A.; Gajdócsi, R.; Huszár, É.; Szili, B.; Lázár, Z.; Antus, B.; Losonczy, G.; Horvath, I. Exercise Increases Exhaled Breath Condensate Cysteinyl Leukotriene Concentration in Asthmatic Patients. J. Asthma 2010, 47, 1057–1062. [Google Scholar] [CrossRef]
- Kivity, S.; Argaman, A.; Onn, A.; Shwartz, Y.; Man, A.; Greif, J.; Fireman, E. Eosinophil Influx into the Airways in Patients with Exercise-Induced Asthma. Respir. Med. 2000, 94, 1200–1205. [Google Scholar] [CrossRef]
- Hallstrand, T.S.; Moody, M.W.; Aitken, M.L.; Henderson Jr., W. R. Airway Immunopathology of Asthma with Exercise-Induced Bronchoconstriction. J. Allergy Clin. Immunol. 2005, 116, 586–593. [Google Scholar] [CrossRef] [PubMed]
- Elkhatib, S.K.; Alley, J.; Jepsen, M.; Smeins, L.; Barnes, A.; Naik, S.; Ackermann, M.R.; Verhoeven, D.; Kohut, M.L. Exercise duration modulates upper and lower respiratory fluid cellularity, antiviral activity, and lung gene expression. Physiol. Rep. 2021, 9. [Google Scholar] [CrossRef]
- Araneda, O.F.; Carbonell, T.; Tuesta, M. Update on the Mechanisms of Pulmonary Inflammation and Oxidative Imbalance Induced by Exercise. Oxid. Med. Cell. Longev. 2016, 2016, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Chimenti, L.; Morici, G.; Paternò, A.; Santagata, R.; Bonanno, A.; Profita, M.; Riccobono, L.; Bellia, V.; Bonsignore, M.R. Bronchial epithelial damage after a half-marathon in nonasthmatic amateur runners. Am. J. Physiol.-Lung Cell. Mol. Physiol. 2010, 298, L857–L862. [Google Scholar] [CrossRef]
- Taylor, S.D.; Ivester, K.M.; Stewart, C.; Page, A.E.; Horohov, D.W.; Couetil, L.L. The Effect of Lower Airway Inflammation on Inflammatory Cytokine Gene Expression in Bronchoalveolar Lavage Fluid and Whole Blood in Racing Thoroughbreds. Vet. Immunol. Immunopathol. 2021, 237, 110266. [Google Scholar] [CrossRef]
- McKANE, S.A.; Rose, R.J. Effects of exercise intensity and training on bronchoalveolar lavage cytology. Equine Vet. J. 1995, 27, 58–62. [Google Scholar] [CrossRef]
- McKANE, S.; Canfield, P.; Rose, R. Equine Bronchoalveolar Lavage Cytology: Survey of Thoroughbred Racehorses in Training. Aust. Vet. J. 1993, 70, 401–404. [Google Scholar] [CrossRef]
- Clark, C.; Lester, G.; Vetro, T.; Rice, B. Bronchoalveolar Lavage in Horses: Effect of Exercise and Repeated Sampling on Cytology. Aust. Vet. J. 1995, 72, 249–252. [Google Scholar] [CrossRef]
- Sweeney, C.R.; Kassier, Y.; Ziemer, E.L.; Lindborg, S. Effects of Hing Site and Fluid Volume on Results of Bronchoalveolar Lavage Fluid Analysis in Horses. Am. J. Vet. Res. 1992, 53. [Google Scholar] [CrossRef]
- Romberg, K.; Tufvesson, E.; Bjermer, L. Asthma symptoms, mannitol reactivity and exercise-induced bronchoconstriction in adolescent swimmers versus tennis players. J. Asthma Allergy 2017, Volume10, 249–260. [Google Scholar] [CrossRef]
- Bonsignore, M.R.; Morici, G.; Vignola, A.M.; Riccobono, L.; Bonanno, A.; Profita, M.; Abate, P.; Scichilone, N.; Amato, G.; Bellia, V.; Bonsignore, G. Increased airway inflammatory cells in endurance athletes: what do they mean? Clin. Exp. Allergy 2003, 33, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Bonsignore, M.R.; Morici, G.; Riccobono, L.; Insalaco, G.; Bonanno, A.; Profita, M.; Paternò, A.; Vassalle, C.; Mirabella, A.; Vignola, A.M. Airway Inflammation in Nonasthmatic Amateur Runners. Am. J. Physiol.-Lung Cell. Mol. Physiol. 2001, 281, L668–L676. [Google Scholar] [CrossRef]
- Chimenti, L.; Morici, G.; Paternò, A.; Bonanno, A.; Siena, L.; Licciardi, A.; Veca, M.; Guccione, W.; Macaluso, F.; Bonsignore, G.; et al. Endurance Training Damages Small Airway Epithelium in Mice. Am. J. Respir. Crit. Care Med. 2007, 175, 442–449. [Google Scholar] [CrossRef] [PubMed]
- Davis, M.; McKenzie, E.; Royer, C.; Williamson, K.; Payton, M.; Nelson, S. Effect of training and recovery on airway inflammation in an animal model of ‘ski asthma. ’ Equine Comp. Exerc. Physiol. 2005, 2, 133–138. [Google Scholar] [CrossRef]
- Sue-Chu, M. Winter Sports Athletes: Long-Term Effects of Cold Air Exposure. Br. J. Sports Med. 2012, 46, 397–401. [Google Scholar] [CrossRef] [PubMed]
- Bougault, V.; Turmel, J.; St-Laurent, J.; Bertrand, M.; Boulet, L.-P. Asthma, Airway Inflammation and Epithelial Damage in Swimmers and Cold-Air Athletes. Eur. Respir. J. 2009, 33, 740–746. [Google Scholar] [CrossRef]
- Davis, M.S.; Malayer, J.R.; Vandeventer, L.; Royer, C.M.; McKenzie, E.C.; Williamson, K.K. Cold Weather Exercise and Airway Cytokine Expression. J Appl Physiol 2005, 98, 2132–2136. [Google Scholar] [CrossRef]
- Mahalingam-Dhingra, A.; Bedenice, D.; Mazan, M.R. Bronchoalveolar Lavage Hemosiderosis in Lightly Active or Sedentary Horses. J. Vet. Intern. Med. 2023, 37, 1243–1249. [Google Scholar] [CrossRef]
- Lo Feudo, C.; Stucchi, L.; Alberti, E.; Stancari, G.; Conturba, B.; Zucca, E.; Ferrucci, F. The Role of Thoracic Ultrasonography and Airway Endoscopy in the Diagnosis of Equine Asthma and Exercise-Induced Pulmonary Hemorrhage. Vet. Sci. 2021, 8, 276. [Google Scholar] [CrossRef]
- Sundman, E.A.; Chigerwe, M.; Hunyadi, L.M. A retrospective study of bronchoalveolar lavage fluid analysis in barrel racing horses with exercise-induced pulmonary hemorrhage and asthma in Texas from 2016 to 2018. Research in Veterinary Science 2020, 132, 338–341. [Google Scholar] [CrossRef]
- McKANE, S.A.; Slocombe, R.F. Experimental mild pulmonary inflammation promotes the development of exercise-induced pulmonary haemorrhage. Equine Vet. J. 2010, 42, 235–239. [Google Scholar] [CrossRef] [PubMed]
- Michelotto, P.V.; Muehlmann, L.A.; Zanatta, A.L.; Bieberbach, E.W.R.; Kryczyk, M.; Fernandes, L.C.; Nishiyama, A. Pulmonary inflammation due to exercise-induced pulmonary haemorrhage in Thoroughbred colts during race training. Vet. J. 2011, 190, e3–e6. [Google Scholar] [CrossRef] [PubMed]
- Hooi, K.S.; Defarges, A.M.; Jelovcic, S.V.; Bienzle, D. Bronchoalveolar lavage hemosiderosis in dogs and cats with respiratory disease. Vet. Clin. Pathol. 2019, 48, 42–49. [Google Scholar] [CrossRef] [PubMed]
- DeHeer, H.L.; McManus, P. Frequency and severity of tracheal wash hemosiderosis and association with underlying disease in 96 cats: 2002–2003. Vet. Clin. Pathol. 2005, 34, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Eldem, İ.; İleri, T.; İnce, E.; Asarcikli, F.; Pekpak, E.; Çakmakli, H.F.; Ceyhan, K.; Uysal, Z. Idiopathic Pulmonary Hemosiderosis With Allergic Asthma Diagnosis in a Pediatric Patient. J. Pediatr. Hematol. Oncol. 2015, 37, e435–e437. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Different factors influencing the techniques used for EA-diagnostics.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



