
Submitted:
13 September 2024
Posted:
17 September 2024
You are already at the latest version
Abstract
Maximal athletic performance can be limited by various factors, including restricted respiratory function. These limitations can be mitigated through targeted respiratory muscle training, as supported by numerous studies. However, the full potential of respiratory training in competitive finswimming has not been fully investigated. This case study aims to evaluate performance variability during underwater phases in an elite Bi-Fins swimmer (current world record holder and multiple world championship medallist) over a 200m race simulation after an eight-week respiratory training using Airofit PRO™. Performance variability was assessed based on pre-test, inter-test, and post-test data. Each measurement included pulmonary function, body composition, and swim performance evaluations. The swimmer followed a 28-day training program with the AiroFit PRO™ respiratory trainer between tests. Significant improvements were observed in Wilcoxon paired-sample test between the pre-test and post-test in underwater distance (p=0.012; d=1.26), underwater time (p=0.012; d=1.26), and number of underwater kicks (p=0.043; d=1.01), resulting in a 14.23% longer underwater distance, 14.08% longer underwater time, and 14.94% increase in underwater kicks. Despite increased distance and time, underwater velocity remained stable, indicating improved underwater performance efficiency. The results suggest that the AiroFit PRO™ respiratory trainer has practical applications in finswimming training programs.
Keywords:
Swim training
; Video-analysis
; Finswimming performance
; Respiratory muscle training
; Underwater phases
1. Introduction
The aim of sports training is to prepare athletes to achieve their maximum performance and surpass their competitors. Athletic performance can be significantly affected by respiratory system limitations [1]. Fatigue in respiratory muscles limit ventilation, increase perceived exertion, disrupt the coordination between breathing and movement, eventually decreasing performance [2,3,4,5]. Respiratory muscle training (RMT) is widely used in physiotherapy and pulmonary rehabilitation to improve respiratory function and strength [6,7,8,9,10]. However, it is also considered a modern training method that can be applied in sports practice to enhance athletic performance [11,12]. While the benefits of RMT are well-documented in dry-land endurance sports [13,14,15,16], its application in water sports is less clear [17]. However, several studies suggest that integrating RMT into training programs can improve respiratory parameters and swim performance [18,19,20,21].
Recent studies [22,23] emphasize the potential for performance enhancement in swimming, especially in acyclic phases (start and turns), where swimmers are allowed to swim underwater for up to 15 meters. These sections of the race allow higher velocities due to reduced wave drag [24] as well as higher initial velocities attained after the dive [25,26] or wall push-offs [27]. Changes in performance are primarily observed during underwater phases, often exhibited as shortened underwater distance, fewer kicks, or reduced velocity [22,23]. Underwater distances vary from 5 to 14 meters, depending on the discipline [28,29,30], and swimmers typically utilize a sinusoidal motion consisting of up-kicks and down-kicks [31]. The importance of the underwater phase has recently been confirmed also in finswimming in the Bi-fins category [32]. However, it is important to consider the role of breath holding and the associated discomfort due to the lack of oxygen, which may limit the benefits of a long underwater phase. Despite this, no studies have yet examined changes in race parameters during simulated or real race conditions following supplementary RMT application. This gap presents an opportunity to explore modern training technologies applicable in both pulmonary rehabilitation and sports training [33]. Hence, this case study aims to evaluate changes in underwater phase performance during a 200m Bi-Fins race simulation after an eight-week program using tele-rehabilitation device Airofit PRO for RMT in a case study with the current World record holder and multiple World championship medalist.
2. Materials and Methods
2.1. Participant
Elite female fin-swimmer (age 24 years; height 186 cm; body mass 89.8 kg) who is a current world record holder (400 m Bi-Fins) and a medalist in world championships 2022 (100, 200 m Bi-Fins) participated in this case study. Seasonal training program consists of swim sessions (7 ± 1.5 hours per week) and dry-land sessions (2 ± 1.5 hours per week) within the framework of traditional linear periodization. The volume of swimming training during the selected period ranged from 16.8 ± 3.4 km per week. Throughout the chosen training mesocycles, no long-lasting specific training blocks with focus on the development of hypoxia was implemented in the swimmer’s preparation. The participant agreed with all testing procedures and provided informed consent in compliance with ethical committee and procedures of Palacký University Olomouc (under reference number 57/2022). This study was in line with the Code of Ethics of the World Medical Association (Declaration of Helsinki).
2.2. Procedure
Pre-, inter- and post-test were used to evaluate results in this study. Testing process consisted of three major parts (pulmonary function tests, body composition measurements, and a swim test). The swim test (200 m Bi-Fins race simulation) was performed in a 25m pool (27.3 ± 0.3 °C). The test was preceded by a standard warm-up divided into a general part (without fins) and a specific part (with fins). The race simulation was conducted 30-minutes after the warm-up and according to international CMAS rules [34]. Swim test was assessed using a standardized video-analysis methodological procedure [35]. Immediately after each race simulation, the swimmer’s perceived level of breathlessness was subjectively assessed on a modified Borg Dyspnea 0-10 Scale [36]. The intervention in the swimmer’s training process was implemented by integrating supplementary RMT using the Airofit PRO™ respiratory trainer. This device is a small, portable, lightweight, and non-invasive pressure meter with a rubber flange mouthpiece designed for respiratory muscle training. The Airofit PRO™ E-unit contains pressure sensors and a Bluetooth transmitter, allowing the measurement of breathing patterns and their visualization on a mobile device through the Airofit PRO™ Sport smart application. Additionally, the Airofit PRO™ respiratory trainer provides adjustable airflow resistance. The level of resistance is set based on the initial measurement, the selected type of training program, the duration of the training unit, and its intensity. For purposes of this study, a 28-day training program for competitive swimming was chosen, which included daily diagnostics and training of inspiratory (2-3 min) and expiratory (4-5 min) muscles for 6-10 minutes per day. The lung test records her accessible vital lung capacity (5.00±1.13 l), Maximal Inspiratory Pressure (105±7.01 cmH2O) and Maximal Expiratory Pressure (91±12.578 cmH2O). Following this, the swimmer received a visualization in the app with instructions for setting resistance to airflow during respiration. Inhalation air resistance (grade A-F) ranged from 20-140 cmH2O / (l/s) and exhalation air resistance (grade 1-6) ranged from 30-200 cmH2O / (l/s). Throughout the 28-day periodization protocol, progressive overload in the form of increasing resistance to airflow during respiration was monitored and adjusted based on the swimmer’s current condition. However, the results of studies observed in competitive swimmers after 6-8 weeks [19,37]. Therefore, the 28-day training program was repeated after the intermediate test. The validity of the Airofit PRO™ respiratory trainer was confirmed by the study [33]. The Airofit PRO™ training system is designed in accordance with the Medical Device Directive - MDD 2007/47/EC.
2.3. Data Collection and Analysis
2.3.1. Body Composition
The body composition of the participant was measured using the multifrequency BIA (Bioelectrical Impedance Analysis) method with the InBody 720 device from Biospace Co., Seoul, Korea. The following body composition parameters were utilized and described: body weight (Weight) [kg], skeletal muscle mass (SMM) [kg], percentage of body fat (Fat) [%] and ratio of the total amount of extracellular fluid and blood in the body (ECW) [%]. Body composition measurements were conducted in laboratory conditions according to established standards outlined in the device’s manual. This method is non-invasive and has a high degree of validity and reliability [38]. The device was calibrated before each measurement session.
2.3.2. Pulmonary Function Test
The Geratherm Respiratory DIFFUSTIK device (Geratherm Respiratory GmbH, Bad Kissingen, Germany) with diagnostic software BLUE CHERRY® (V 1.3.0.1) was used to measure, evaluate, and display the results of each individual tests. Following selected respiratory parameters were assessed: Vital Capacity (VC), Expiratory Reserve Volume (ERV), Inspiratory Capacity (IC), Forced Expiratory Vital Capacity (FVCex), Forced Expiratory Volume in one second (FEV1), Peak Expiratory Flow (PEF), Maximal Inspiratory Pressure (PImax), Maximal Expiratory Pressure (PEmax), The Index of Respiratory Work, used for assessing muscle fatigue (TTmus).
2.3.2. Perceive Exertion Evaluation
As additional evaluation (after the swim test only) of perceived breathlessness, the Modified Borg Dyspnea Scale (MBS) was used, which represents a modified Borg scale for subjective evaluation of the degree of perceived breathlessness, chest pain, and lower limb discomfort [39]. It is a categorical scale with a numerical rating ranging from 0 to 10, where 0 (as a breathlessness rating) corresponds to the sensation of normal breathing (absence of breathlessness), and 10 corresponds to the subject’s maximum possible sensation of breathlessness. Since the perception of exercise-induced breathlessness depends on the stimulus to which the athlete was exposed, the assessment using the Borg scale should ideally be performed at the same workload [40].
2.3.3. Swim Test
A camera (Sony FDR-AX700, Tokyo, Japan) was positioned 12 m above the water level and its optical axis was perpendicular to the direction of swimming, in the middle of the pool. Video footage was recorded in mp4 format (Full HD, 1920x1080, 50fps) and subsequently analysed using the Dartfish software (Live S, Fribourg, Switzerland). Selected phases of the simulated race (individual distances travelled under and above water) were assessed when the swimmer’s head passed marks visible on the lane ropes. Before each race simulation, the accuracy of all markers was re-measured and controlled using a measuring tape. The light flash signal indicated the start of the race simulation and was synchronized with the camera. First wall contact of the fin or the hand determined the 25m split times during each lap of the test [22,23]. Simultaneously the split times as well as final time was controlled by 3 other persons using hand stopwatches (Casio, HS-80TW-1EF, Tokio, Japan), which were only used to double-check the data of the video analysis but were not used for the statistical analysis. During each underwater phase, the following parameters were assessed: underwater distance [m], underwater time [s], underwater velocity [m.s-1], number of underwater kicks. As an additional control parameter, individual surface velocity [m.s-1] was assessed to determine whether the expected changes in underwater phase negatively or positively also affected the above water phase.
2.3.4. Statistical Analysis
The data were processed using STATISTICA software version 31.4.0.14 (Stat-Soft Inc., Tulsa, USA). To verify the accuracy between repeated measurements, two other analysts simultaneously assessed this dataset. The intraclass correlation coefficient (ICC) was used, with an average value ranging from 0.988 to 0.989. The normal distribution of the data was verified by Shapiro-Wilk test. To evaluate the variability in performance during the underwater phases a non-parametric Wilcoxon paired-sample test for two dependent samples was used. The level of statistical significance was set at α=0.05. To determine, whether the intervention had a real practical effect, Cohen’s d was used with corresponding range scale as follows: d ≥ 0.80 = large effect; d (0.50–0.80) = medium effect; d (0.20–0.50) = small effect [40].
3. Results
3.1. Body Composition
Table 1 reflects the variability of selected body composition parameters of the swimmer between pre-, inter- and post-test. A gradual decrease from pre- through inter- to post- test was observed by Weight (4.56%; 0.35%; 4.90%) and Fat (9.23%; 2.97%; 11.92%). ECW decreased from pre- to inter-test (0.79%) and remained consistent up post-test by SMM most pronounced decrease was found between pre-test and inter-test (1.07%), followed by increase between inter- and post-test (0.54%), thus resulted in slightly reduced decrease between pre-test and post-test (0.53%).
3.2. Respiratory Parameters
The results of the Pulmonary Function Test are demonstrated in Table 2. VC showed a gradual increase from pre- through inter- to post-test (0.78%; 2.12%; 2.91%) respectively. ERW considerably decreased from pre- to inter-test (11.60%), then showed a substantial increase between inter- and post-test (19.38%), resulting in a total increase between pre- and post-test of (5.52%). IC increased from pre- to inter-test (5.07%), then decreased from inter- to post-test (3.41%) resulting in a total increase between pre- and post-test (1.49%). FVCex showed decrease from pre- to inter-test (0.78%) followed by increase from inter- to post-test (3.71%) with total increase from pre- to post-test (2.91%). FEV1 increased from pre- to inter-test (5.34%), decreased between inter- and post-test (1.32%) and showed total increase from pre- to post-test (3.94%). By PEF a gradual increase from pre- through inter- to post-test was observed (4.60%; 6.07%; 10.95%). For PImax and PEmax, a similar pattern with increase from pre- to inter-test (40.22%; 14.17%), followed by decrease between inter- to post-test (4.65%; 2.07%) resulting in total increase between pre- and post-test (33.70%; 11.81%) occurred. TTmus showed a gradual decrease from pre- through inter- to post-test (36.36%; 14.29%; 45.45%). RPE of dyspnea showed a decrease between pre-test (9) and inter-test (8). The ratio of values between inter-test (8) and post-test (8) remained unchanged.
3.3. Swim Test
Table 3 shows the changes in total swim time as well as in the underwater performance parameters during the swim test. The total swim time increased from pre- to inter-test (0.86%) and then decreased from inter- to post-test (-3.10%), resulting in overall time reduction from pre- to post-test (-2.27%). A gradual increase from pre- through inter- to post-test was observed in Underwater distance (10.67%; 3.21%; 14.23%) as well as in Underwater time (13.15%; 0.83%; 14.08%) respectively. Underwater velocity decreased from pre- to inter-test (-1.79%), increased from inter- to post-test (1.83%) and remain stable between pre- and post-test. Number of underwater kicks increased from pre- through inter- to post-test (10.15%; 4.35%; 14.94%). Surface water velocity decreased from pre- to inter-test (-1.78%), then increased from inter- to post-test (3.61%), with overall increase from pre- to post-test (1.78%).
Except of the underwater velocity, a significant difference (p<0.001) and large effect (d ≥ 0.80) was found in all tested kinematical parameters (Table 4). Underwater distance was significantly extended (p=0.012) between pre-test (9.56 ± 2.22) and post-test (10.92 ± 2.14). Underwater time became significantly longer (p=0.049; p=0.012) between pre-test (4.26 ± 0.76) and inter-test (4.82 ± 0.40), as well as between pre-test (4.26 ± 0.76) and post-test (4.86 ± 0.71). Number of underwater kicks significantly (p=0.043) increased from pre-test (5.25 ± 1.48) to post-test (6.00 ± 1.5).
Comparing the underwater and surface velocity, a significant difference (p=0.012) and large effect (d=1.26) was found from pre- through inter- to post-test (Figure 1).
4. Discussion
The purpose of the present study was to evaluate the variability of simulated swimming performance in the underwater phases in an elite finswimmer, who is the current World record holder and multiple World championship medalist, after applying an eight-week respiratory training program with Airofit PRO™, which allows comprehensive training of the respiratory muscles.
4.1. Body Composition
The results show a decreasing trend in body weight, with a decline of 4.56% between the pre-test and inter-test, and 4.90% between the pre-test and post-test. This trend supports the study by [41], which found that changes in swimmers’ performance are often associated with changes in body weight and muscle mass, highlighting the need for regular monitoring of body composition. Compared to the general population, competitive female swimmers possess a lower percentage of body fat due to highly intensive training programs. The average body fat percentage, expressed as a proportion of total body weight, was found around 16% for young swimmers [42], while for adult college swimmers between 14% to 28% depending on age [43,44]. This range fully corresponds to the results presented in this study, where body fat was reduced from 26% to 22.9%. According to [45], no relationship between body density, fat mass or percentage of fat, and young female swimmers’ performance was found. Instead, swim performance is related more to SMM, which can reflect increased muscle hypertrophy [46,47]. This trend is not evident in the presented study, as there was a reduction in skeletal muscle mass from 37.4 kg to 37.2 kg between the initial and final measurements, representing a decrease of 0.53%.
4.2. Respiratory Parameters
The eight-week specific training program with Airofit PRO™ led to improving selected respiratory parameters. This chosen duration of the intervention appears to be sufficient and supports the findings of [19] and [48]. The most noticeable effect was the percentage improvement in PImax, demonstrating a 40.22% increase in inspiratory muscle strength between the pre- and inter-tests. This increase was followed by a slight decrease of 4.65% between the inter- and post-tests, resulting in an overall improvement of 33.70%. Overall, these results fall within the 19-45% range previously confirmed in rowers [13,16], cyclists [15], football players [49], and young competitive finswimmers [50]. However, none of these studies included an intervention programme with a tele-rehabilitation device such as the Airofit PRO™. A similar trend was also observed in PEmax, which increased by 14.17% and subsequently decreased by 2.07%. The overall improvement thus represented 11.81%, which is percentage-wise lower compared to [19]. This may be due to a different intervention program focused exclusively on improving respiratory muscle endurance. It is also worth noting that percentage differences between inspiratory and expiratory muscle strength are common in studies, particularly in clinical diagnostics [51]. Nevertheless, it can be said that improvements in PImax and PEmax can lead to better control of breathing rhythm and reduced respiratory muscle fatigue during high-intensity exertion [4].The results further demonstrate an improvement in VC and FVCex, both by 2.91%. This correspond with the findings of [48], who reported a 7% increase in FVCex in their study on football players following RMT. The percentage difference in the results of both studies may be attributed to the earlier adaptation of swimmers to the specific aquatic environment, which in itself provides a significant conditioning stimulus to the respiratory system. This increase reflects the potential for increased diaphragm thickness and improved functional capacity during exercise in healthy subjects [52,53]. This is directly related to the improvement in ERW (5.52%), which may reflect adaptive changes in respiratory management following the application of RMT. These changes can help optimize the expiratory phase of breathing, thereby enhancing breathing efficiency under increased physical load. This is crucial for proper swimming technique and minimizing fatigue [54]. Additionally, there was a decrease in TTmus by 45.45%, indicating increased efficiency of the respiratory muscles as a result of the training. Even though the muscles are stronger, they can work more efficiently and with less energy expenditure, potentially leading to a lower sense of fatigue during long race segments. However, this phenomenon requires further research to understand the long-term effects of RMT on muscle fatigue and performance. The study also assessed the level of subjectively perceived dyspnea immediately after completing the race simulation, which showed a declining trend, similar to the findings of [18].
4.3. Swim Test
Recent studies [22,23,28] focusing on detailed analysis of swimming performances highlighted the potential for improvement, particularly in race sections involving starts or turns. According to [32], the underwater phases after each turn in competitive finswimming can be considered decisive part of the race that significantly change overall race performance. Previous studies have found that RMT leads to an extension of dynamic apnea in finswimmers [21,50]. However, extending the underwater phase carries the risk of increased physiological fatigue in swimmers due to excessively high hypoxic stimulation [27,55]. Therefore, the distance travelled underwater should be evaluated together with the underwater velocity, which is considered a more relevant parameter for underwater phase assessment [32,56]. Optimal underwater strategy is also related to exact number of underwater kicks, whose technical execution directly affect acceleration between 5-10 m out of the wall after each turn and varies depending on the race distance [57,58]. Lengthening the underwater phase, the higher number of underwater kicks would lead to more physiological fatigue and in turn would decrease efficiency in the locomotion pattern [59]. Based on the larger fatigue resistance after the respiratory training, the results of this study show a progressive trend of increasing underwater distance (14.23%) with more underwater kicks (14.94%), while at the same time maintaining the same underwater velocity in the pre- and post-test (2.23±0.15 m.s-1). Since, no evident negative impact on the clean swim speed, these results suggest increased efficiency of the underwater phase. Together with higher clean swim speed, both contribute to overall enhancing of swim performance by 2.27%.
4.4. Limitation
The study was conducted with the current World record holder and multiple World championship medallist. While this limits the number of participants and generalization of the results, it provides insights into the highest athletic performance level possible. Using swimmers of lower performance level, future research in this area should focus on a larger sample in comparison to a control group. Additionaly, underwater velocity may be also affected by the push-off force after the start and after each turn [22,26]. Although force assessment was not included in the present study, we recommend to monitor this parameter in future research to provide a more comprehensive understanding. The single-case nature and observed decreases in body weight and muscle mass limit the study’s generalizability, emphasizing the need for research with larger sample sizes and control groups.
5. Conclusions
After an 8-week RMT application, a progressive increase in underwater distance and kicks was observed, while maintaining consistent underwater velocity. There was no negative impact on clean swim speed, indicating improved efficiency during the underwater phase. This improvement, coupled with a higher clean swim speed, leads to an overall enhancement in swimming performance. Based on these results, Airofit PRO™ can be recommended for use in finswimmer´s training, however further research is necessary to fully understand its impact and optimize its use.
Author Contributions
Conceptualization, T.M.; methodology, M.P.; software, J.B.; validation, M.P., D-P.B. and T.M.; formal analysis, J.B.; investigation, E.K.; resources, T.M.; data curation, J.B.; writing—original draft preparation, T.M. and M.P.; writing—review and editing, T.M., E.K. and D-P.B.; visualization, J.B.; supervision, Z.S. and E.K.; project administration, T.M. and J.M.; funding acquisition, T.M. All authors have read and agreed to the published version of the manuscript.” All authors have read and agreed to the published version of the manuscript.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This study was supported by Palacký University Olomouc under Grant IGA_FTK_2024_014 and by the research project of the science and technology park BALUO Application Centre of Faculty of Physical Culture, Palacký University Olomouc, entitled “Assessment of the effectiveness of healthy and active lifestyle of adult individuals on selected health indicators with the subjects of research conducted by BALUO Application Centre of Faculty of Physical Culture, Palacký University Olomouc–retrospective study”.
Institutional Review Board Statement
The participant agreed with all testing procedures and provided informed consent in compliance with ethical committee and procedures of Palacký University Olomouc (under reference number 57/2022). This study was in line with the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data from this study are available from the corresponding author upon reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Boutellier, U.; Piwko, P. The Respiratory System as an Exercise Limiting Factor in Normal Sedentary Subjects. Eur. J. Appl. Physiol. 1992, 64, 145–152. [Google Scholar] [CrossRef] [PubMed]
- Dempsey, J.A. Respiratory Determinants of Exercise Limitation. Clin. Chest Med. 2019, 40, 331–342. [Google Scholar] [CrossRef] [PubMed]
- Complete Guide to Respiratory Care in Athletes; Dickinson, J., Hull, J., Eds.; Routledge: Abingdon, Oxon, 2020. [Google Scholar]
- Lomax, M.; McConnell, A. Inspiratory Muscle Fatigue in Swimmers after a Single 200 m Swim. J. Sports Sci. 2003, 21, 659–664. [Google Scholar] [CrossRef]
- McConnell, A. Respiratory Muscle Training: Theory and Practice; Churchill Livingstone/Elsevier: Edinburgh ; New York, 2013. [Google Scholar]
- Aslan, G.K.; Huseyinsinoglu, B.E.; Oflazer, P.; Gurses, N.; Kiyan, E. Inspiratory Muscle Training in Late-Onset Pompe Disease: The Effects on Pulmonary Function Tests, Quality of Life, and Sleep Quality. Lung 2016, 194, 555–561. [Google Scholar] [CrossRef] [PubMed]
- Enright, S.J.; Unnithan, V.B. Effect of Inspiratory Muscle Training Intensities on Pulmonary Function and Work Capacity in People Who Are Healthy: A Randomized Controlled Trial. Phys. Ther. 2011, 91, 894–905. [Google Scholar] [CrossRef] [PubMed]
- Jones, H.N.; Crisp, K.D.; Robey, R.R.; Case, L.E.; Kravitz, R.M.; Kishnani, P.S. Respiratory Muscle Training (RMT) in Late-Onset Pompe Disease (LOPD): Effects of Training and Detraining. Mol. Genet. Metab. 2016, 117, 120–128. [Google Scholar] [CrossRef]
- Lotters, F.; van Tol, B.; Kwakkel, G.; Gosselink, R. Effects of Controlled Inspiratory Muscle Training in Patients with COPD: A Meta-Analysis. Eur. Respir. J. 2002, 20, 570–577. [Google Scholar] [CrossRef]
- Witt, J.D.; Guenette, J.A.; Rupert, J.L.; McKenzie, D.C.; Sheel, A.W. Inspiratory Muscle Training Attenuates the Human Respiratory Muscle Metaboreflex: Cardiovascular Effects of Training Respiratory Muscle. J. Physiol. 2007, 584, 1019–1028. [Google Scholar] [CrossRef]
- HajGhanbari, B.; Yamabayashi, C.; Buna, T.R.; Coelho, J.D.; Freedman, K.D.; Morton, T.A.; Palmer, S.A.; Toy, M.A.; Walsh, C.; Sheel, A.W.; et al. Effects of Respiratory Muscle Training on Performance in Athletes: A Systematic Review With Meta-Analyses. J. Strength Cond. Res. 2013, 27, 1643–1663. [Google Scholar] [CrossRef]
- McConnell, A. Breathe Strong, Perform Better; Human Kinetics: Champaign, IL, 2011. [Google Scholar]
- Griffiths, L.A.; McConnell, A.K. The Influence of Inspiratory and Expiratory Muscle Training upon Rowing Performance. Eur. J. Appl. Physiol. 2007, 99, 457–466. [Google Scholar] [CrossRef]
- Johnson, M.A.; Sharpe, G.R.; Brown, P.I. Inspiratory Muscle Training Improves Cycling Time-Trial Performance and Anaerobic Work Capacity but Not Critical Power. Eur. J. Appl. Physiol. 2007, 101, 761–770. [Google Scholar] [CrossRef] [PubMed]
- Romer, L.M.; Mcconnell, A.K.; Jones, D.A. Inspiratory Muscle Fatigue in Trained Cyclists: Effects of Inspiratory Muscle Training: Med. Sci. Sports Exerc. 2002, 34, 785–792. [Google Scholar] [CrossRef] [PubMed]
- Volianitis, S.; Mcconnell, A.K.; Koutedakis, Y.; Mcnaughton, L.; Backx, K.; Jones, D.A. Inspiratory Muscle Training Improves Rowing Performance: Med. Sci. Sports Exerc. 2001, 803–809. [Google Scholar] [CrossRef] [PubMed]
- Aspenes, S.T.; Karlsen, T. Exercise-Training Intervention Studies in Competitive Swimming. Sports Med. 2012, 42, 527–543. [Google Scholar] [CrossRef] [PubMed]
- Kilding, A.E.; Brown, S.; McConnell, A.K. Inspiratory Muscle Training Improves 100 and 200 m Swimming Performance. Eur. J. Appl. Physiol. 2010, 108, 505–511. [Google Scholar] [CrossRef]
- Lemaitre, F.; Coquart, J.B.; Chavallard, F.; Castres, I.; Mucci, P.; Costalat, G.; Chollet, D. Effect of Additional Respiratory Muscle Endurance Training in Young Well-Trained Swimmers. J. Sports Sci. Med. 2013, 12, 630–638. [Google Scholar]
- Wilson, E.E.; McKeever, T.M.; Lobb, C.; Sherriff, T.; Gupta, L.; Hearson, G.; Martin, N.; Lindley, M.R.; Shaw, D.E. Respiratory Muscle Specific Warm-up and Elite Swimming Performance. Br. J. Sports Med. 2014, 48, 789–791. [Google Scholar] [CrossRef]
- Wylegala, J.A.; Pendergast, D.R.; Gosselin, L.E.; Warkander, D.E.; Lundgren, C.E.G. Respiratory Muscle Training Improves Swimming Endurance in Divers. Eur. J. Appl. Physiol. 2007, 99, 393–404. [Google Scholar] [CrossRef]
- Born, D.-P.; Kuger, J.; Polach, M.; Romann, M. Start and Turn Performances of Elite Male Swimmers: Benchmarks and Underlying Mechanisms. Sports Biomech. 2021, 1–19. [Google Scholar] [CrossRef]
- Born, D.-P.; Kuger, J.; Polach, M.; Romann, M. Turn Fast and Win: The Importance of Acyclic Phases in Top-Elite Female Swimmers. Sports 2021, 9, 122. [Google Scholar] [CrossRef]
- Vennell, R.; Pease, D.; Wilson, B. Wave Drag on Human Swimmers. J. Biomech. 2006, 39, 664–671. [Google Scholar] [CrossRef] [PubMed]
- Born, D.-P.; Stöggl, T.; Petrov, A.; Burkhardt, D.; Lüthy, F.; Romann, M. Analysis of Freestyle Swimming Sprint Start Performance After Maximal Strength or Vertical Jump Training in Competitive Female and Male Junior Swimmers. J. Strength Cond. Res. 2020, 34, 323–331. [Google Scholar] [CrossRef] [PubMed]
- Březina, J.; Polach, M.; Michalica, T.; Svozil, Z. Effect of Pull-out Technique on Acyclic Phases in Elite Male 50 m Breaststroke Swimmers. Tělesná Kult. 2022, 45. [Google Scholar] [CrossRef]
- Veiga, S.; Lorenzo, J.; Trinidad, A.; Pla, R.; Fallas-Campos, A.; de la Rubia, A. Kinematic Analysis of the Underwater Undulatory Swimming Cycle: A Systematic and Synthetic Review. Int. J. Environ. Res. Public. Health 2022, 19, 12196. [Google Scholar] [CrossRef] [PubMed]
- Marinho, D.A.; Barbosa, T.M.; Neiva, H.P.; Silva, A.J.; Morais, J.E. Comparison of the Start, Turn and Finish Performance of Elite Swimmers in 100 m and 200 m Races. J. Sports Sci. Med. 2020, 19, 397–407. [Google Scholar] [PubMed]
- Morais, J.E.; Marinho, D.A.; Arellano, R.; Barbosa, T.M. Start and Turn Performances of Elite Sprinters at the 2016 European Championships in Swimming. Sports Biomech. 2019, 18, 100–114. [Google Scholar] [CrossRef] [PubMed]
- Polach, M.; Thiel, D.; Kreník, J.; Born, D.-P. Swimming Turn Performance: The Distinguishing Factor in 1500 m World Championship Freestyle Races? BMC Res. Notes 2021, 14, 248. [Google Scholar] [CrossRef]
- Taormina, S.; Gaines, R. Swim Speed Strokes for Swimmers and Triathletes: Master Butterfly, Backstroke, Breaststroke, and Freestyle for Your Fastest Swimming; VeloPress: Boulder, Colorado, 2014. [Google Scholar]
- Michalica, T.; Polach, M.; Březina, J.; Agalliu, E. Porovnání Výkonů v Obrátkových Úsecích u Elitních Českých a Světových Plavkyň s Ploutvemi v Disciplínách 100 a 200 Metrů Bi-Fins; Fakulta tělesné kultury: Olomouc, 2023. [Google Scholar]
- Stavrou, V.T.; Tourlakopoulos, K.N.; Daniil, Z.; Gourgoulianis, K.I. Respiratory Muscle Strength: New Technology for Easy Assessment. Cureus 2021. [Google Scholar] [CrossRef]
- Finswimming CMAS Rules, 2023. https://www.cmas.org/document?sessionId=&fileId=5763&language=1.
- Gonjo, T.; Olstad, B.H. Race Analysis in Competitive Swimming: A Narrative Review. Int. J. Environ. Res. Public. Health 2020, 18, 69. [Google Scholar] [CrossRef]
- Mador, M.J.; Rodis, A.; Magalang, U.J. Reproducibility of Borg Scale Measurements of Dyspnea During Exercise in Patients With COPD. Chest 1995, 107, 1590–1597. [Google Scholar] [CrossRef]
- Mackała, K.; Kurzaj, M.; Okrzymowska, P.; Stodółka, J.; Coh, M.; Rożek-Piechura, K. The Effect of Respiratory Muscle Training on the Pulmonary Function, Lung Ventilation, and Endurance Performance of Young Soccer Players. Int. J. Environ. Res. Public. Health 2019, 17, 234. [Google Scholar] [CrossRef] [PubMed]
- McLester, C.N.; Nickerson, B.S.; Kliszczewicz, B.M.; McLester, J.R. Reliability and Agreement of Various InBody Body Composition Analyzers as Compared to Dual-Energy X-Ray Absorptiometry in Healthy Men and Women. J. Clin. Densitom. 2020, 23, 443–450. [Google Scholar] [CrossRef] [PubMed]
- Borg, G. Psychophysical Scaling with Applications in Physical Work and the Perception of Exertion. Scand. J. Work. Environ. Health 1990, 16, 55–58. [Google Scholar] [CrossRef]
- Crisafulli, E.; Clini, E.M. Measures of Dyspnea in Pulmonary Rehabilitation. Multidiscip. Respir. Med. 2010, 5, 202. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 0 ed.; Routledge, 2013. [CrossRef]
- Dopsaj, M.; Zuoziene, I.J.; Milić, R.; Cherepov, E.; Erlikh, V.; Masiulis, N.; di Nino, A.; Vodičar, J. Body Composition in International Sprint Swimmers: Are There Any Relations with Performance? Int. J. Environ. Res. Public. Health 2020, 17, 9464. [Google Scholar] [CrossRef] [PubMed]
- Duché, P.; Falgairette, G.; Bedu, M.; Lac, G.; Robert, A.; Coudert, J. Analysis of Performance of Prepubertal Swimmers Assessed from Anthropometric and Bio-Energetic Characteristics. Eur. J. Appl. Physiol. 1993, 66, 467–471. [Google Scholar] [CrossRef]
- Siders, W.A.; Lukaski, H.C.; Bolonchuk, W.W. Relationships among Swimming Performance, Body Composition and Somatotype in Competitive Collegiate Swimmers. J. Sports Med. Phys. Fitness 1993, 33, 166–171. [Google Scholar]
- Vaccaro, P.; Ostrove, S.M.; VanderVelden, L.; Goldfarb, A.H.; Clarke, D.H.; Dummer, G.M. Body Composition and Physiological Responses of Masters Female Swimmers 20 to 70 Years of Age. Res. Q. Exerc. Sport 1984, 55, 278–284. [Google Scholar] [CrossRef]
- Stager, J.; Cordain, L.; Becker, T.J. Relationship of Body Composition to Swimming Performance in Female Swimmers. J. Swim. Res. 1984, 1, 21–26. [Google Scholar]
- Pyne, D.B.; Anderson, M.E.; Hopkins, W.G. Monitoring Changes in Lean Mass of Elite Male and Female Swimmers. Int. J. Sports Physiol. Perform. 2006, 1, 14–26. [Google Scholar] [CrossRef]
- World Book of Swimming: From Science to Performance; Seifert, L., Chollet, D., Eds.; Nova Science Publishers: New York, 2011. [Google Scholar]
- Mackała, K.; Kurzaj, M.; Okrzymowska, P.; Stodółka, J.; Coh, M.; Rożek-Piechura, K. The Effect of Respiratory Muscle Training on the Pulmonary Function, Lung Ventilation, and Endurance Performance of Young Soccer Players. Int. J. Environ. Res. Public. Health 2019, 17, 234. [Google Scholar] [CrossRef] [PubMed]
- Cavalcante Silva, R.L.; Hall, E.; Maior, A.S. Inspiratory Muscle Training Improves Performance of a Repeated Sprints Ability Test in Professional Soccer Players. J. Bodyw. Mov. Ther. 2019, 23, 452–455. [Google Scholar] [CrossRef] [PubMed]
- Vašíčková, J.; Neumannová, K.; Svozil, Z. The Effect of Respiratory Muscle Training on Fin-Swimmers’ Performance. J. Sports Sci. Med. 2017, 16, 521–526. [Google Scholar] [PubMed]
- Aznar-Lain, S.; Webster, A.; Cañete, S.; San Juan, A.; López Mojares, L.; Pérez, M.; Lucia, A.; Chicharro, J. Effects of Inspiratory Muscle Training on Exercise Capacity and Spontaneous Physical Activity in Elderly Subjects: A Randomized Controlled Pilot Trial. Int. J. Sports Med. 2007, 28, 1025–1029. [Google Scholar] [CrossRef] [PubMed]
- Enright, S.J.; Unnithan, V.B.; Heward, C.; Withnall, L.; Davies, D.H. Effect of High-Intensity Inspiratory Muscle Training on Lung Volumes, Diaphragm Thickness, and Exercise Capacity in Subjects Who Are Healthy. Phys. Ther. 2006, 86, 345–354. [Google Scholar] [CrossRef]
- Sheel, A.W.; Derchak, P.A.; Pegelow, D.F.; Dempsey, J.A. Threshold Effects of Respiratory Muscle Work on Limb Vascular Resistance. Am. J. Physiol.-Heart Circ. Physiol. 2002, 282, H1732–H1738. [Google Scholar] [CrossRef]
- Lavin, K.M.; Guenette, J.A.; Smoliga, J.M.; Zavorsky, G.S. Controlled-frequency Breath Swimming Improves Swimming Performance and Running Economy. Scand. J. Med. Sci. Sports 2015, 25, 16–24. [Google Scholar] [CrossRef]
- Figueiredo, P.; Rouard, A.; Vilas-Boas, J.P.; Fernandes, R.J. Upper and Lower Limb Muscular Fatigue during the 200-m Front Crawl. Appl. Physiol. Nutr. Metab. 2013, 38, 716–724. [Google Scholar] [CrossRef]
- Veiga, S.; Cala, A.; Mallo, J.; Navarro, E. A New Procedure for Race Analysis in Swimming Based on Individual Distance Measurements. J. Sports Sci. 2013, 31, 159–165. [Google Scholar] [CrossRef]
- Takeda, T.; Sakai, S.; Takagi, H. Underwater Flutter Kicking Causes Deceleration in Start and Turn Segments of Front Crawl. Sports Biomech. 2022, 21, 1224–1233. [Google Scholar] [CrossRef]
- Zamparo, P.; Vicentini, M.; Scattolini, A.; Rigamonti, M.; Bonifazi, M. The Contribution of Underwater Kicking Efficiency in Determining “Turning Performance” in Front Crawl Swimming. J. Sports Med. Phys. Fitness 2012, 52, 457–464. [Google Scholar] [PubMed]
- Nicol, E.; Ball, K.; Tor, E. The Biomechanics of Freestyle and Butterfly Turn Technique in Elite Swimmers. Sports Biomech. 2021, 20, 444–457. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Underwater and surface velocity during pre-, inter- and post-test.
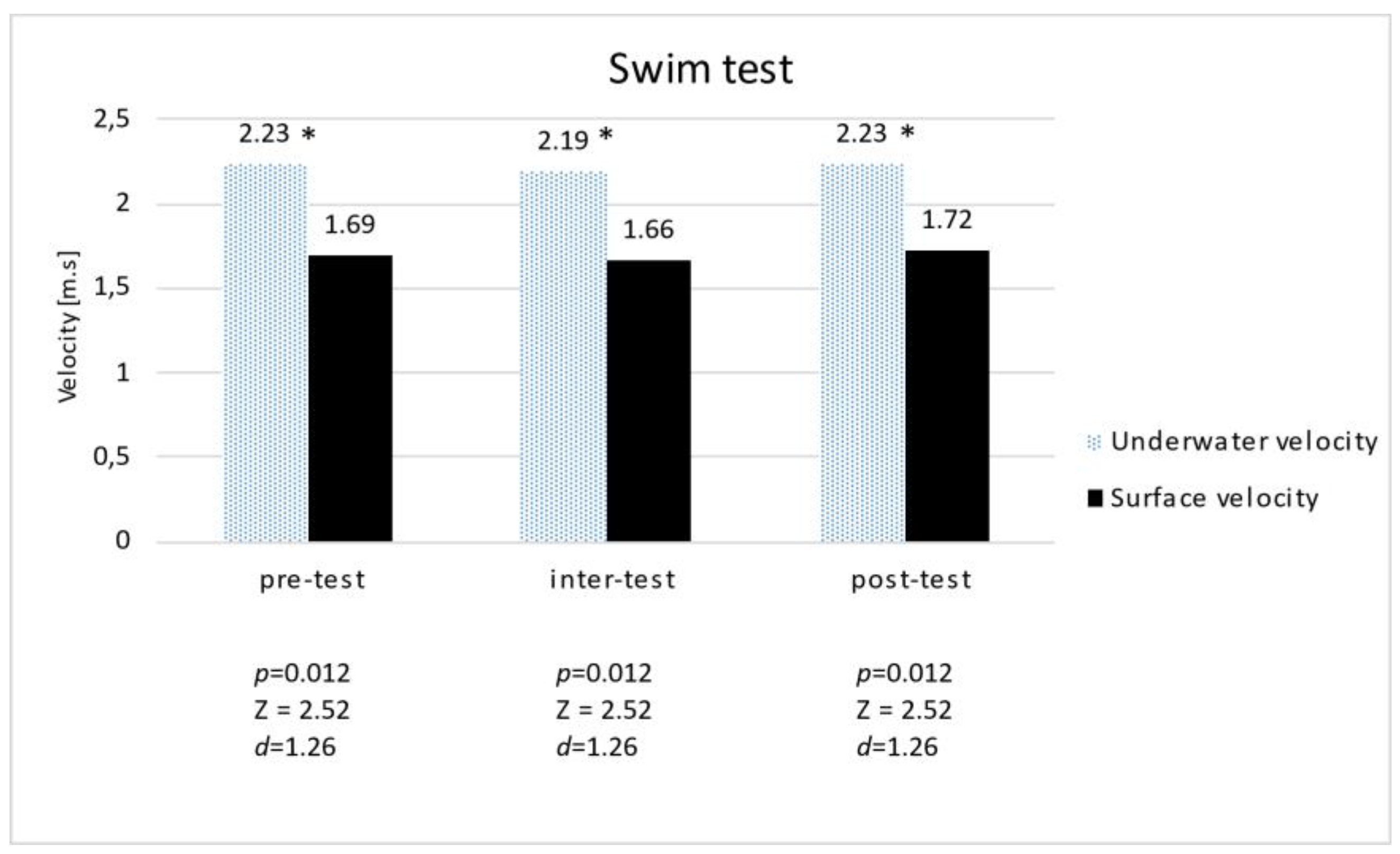

Table 1.
Body composition.
| Weight [kg] | Fat [%] | SMM [kg] | ECW [%] | |
|---|---|---|---|---|
| M | M | M | M | |
| Pre-test | 89.80 | 26.00 | 37.40 | 0.378 |
| Inter-test | 85.70 | 23.60 | 37.00 | 0.375 |
| Post-test | 85.40 | 22.90 | 37.20 | 0.375 |
| % pre-test vs. inter-test | -4.56 | -9.23 | -1.07 | -0.79 |
| % inter-test vs. post-test | -0.35 | -2.97 | 0.54 | 0 |
| % pre-test vs. post-test | -4.90 | -11.92 | -0.53 | -0.79 |
* Legend: SSM = Skeletal muscle mass; ECW = Extracellular water; M = Median; % = Percentage difference.
Table 2.
Pulmonary function test.
| VC [l] |
ERV [l] |
IC [l] |
FVCex [l] | FEV1 [l] | PEF [l/s] | PImax [kPa] | PEmax [kPa] | TTmus | |
|---|---|---|---|---|---|---|---|---|---|
| M | M | M | M | M | M | M | M | M | |
| Pre-test | 5.16 | 1.81 | 3.35 | 5.16 | 4.31 | 9.13 | 9.20 | 12.70 | 0.11 |
| Inter-test | 5.20 | 1.60 | 3.52 | 5.12 | 4.54 | 9.55 | 12.90 | 14.50 | 0.07 |
| Post-test | 5.31 | 1.91 | 3.40 | 5.31 | 4.48 | 10.13 | 12.30 | 14.20 | 0.06 |
| % pre-test vs. inter-test | 0.78 | -11.60 | 5.07 | -0.78 | 5.34 | 4.60 | 40.22 | 14.17 | -36.36 |
| % inter-test vs. post-test | 2.12 | 19.38 | -3.41 | 3.71 | -1.32 | 6.07 | -4.65 | -2.07 | -14.29 |
| % pre-test vs. post-test | 2.91 | 5.52 | 1.49 | 2.91 | 3.94 | 10.95 | 33.70 | 11.81 | -45.45 |
* Legend: M = Median; VC = Vital Capacity; ERV = Expiratory Reserve Volume; IC =Inspiratory Capacity; FVCex = Forced Expiratory Vital Capacity; FEV1 = Forced Expiratory Volume; PEF = Peak Expiratory Flow; PImax = Maximal Inspiratory Pressure; PEmax = Maximal Expiratory Pressure; TTmus = The tension-time index of the inspiratory muscles; % = percentage difference.
Table 3.
Swim test – Performance parameters.
| Performance parameters | ||||||
|---|---|---|---|---|---|---|
| Total swim time [s] | Underwater distance [m] | Underwater time [s] |
Underwater velocity [m.s-1] |
Underwater kicks | Surface water velocity [m.s-1] | |
| M±SD | M±SD | M±SD | M±SD | M±SD | ||
| Pre-test | 106.72 | 9.56 ± 2.22 | 4.26 ± 0.76 | 2.23 ± 0.15 | 5.25 ± 1.48 | 1.69 ± 0.10 |
| Inter-test | 107.64 | 10.58 ± 1.35 | 4.82 ± 0.40 | 2.19 ± 0.17 | 5.75 ± 0.97 | 1.66 ± 0.09 |
| Post-test | 104.30 | 10.92 ± 2.14 | 4.86 ± 0.71 | 2.23 ± 0.15 | 6.00 ± 1.5 | 1.72 ± 0.13 |
| % pre-test vs. inter-test | 0.86 | 10.67 | 13.15 | -1.79 | 10.15 | -1.78 |
| % inter-test vs. post-test | -3.10 | 3.21 | 0.83 | 1.83 | 4.35 | 3.61 |
| % pre-test vs. post-test | -2.27 | 14.23 | 14.08 | 0 | 14.94 | 1.78 |
* Legend: M = Median; % = Percentage difference; SD = Standard deviation.
Table 4.
Swim test – Statistical analysis.
| Underwater distance [m] | |||
| p | Z | d | |
| Pre-test vs. inter-test | 0.068 | 1.82 | 0.91 |
| Inter-test vs. post-test | 0.401 | 0.84 | 0.42 |
| Pre-test vs. post-test | 0.012* | 2.52 | 1.26 |
| Underwater time [s] | |||
| p | Z | d | |
| Pre-test vs. inter-test | 0.049* | 1.96 | 0.98 |
| Inter-test vs. post-test | 0.889 | 0.14 | 0.07 |
| Pre-test vs. post-test | 0.012* | 2.52 | 1.26 |
| Underwater velocity [m.s-1] | |||
| p | Z | d | |
| Pre-test vs. inter-test | 0.262 | 1.12 | 0.56 |
| Inter-test vs. post-test | 0.123 | 1.54 | 0.77 |
| Pre-test vs. post-test | 1.000 | 0 | 0 |
| Underwater kicks | |||
| p | Z | d | |
| Pre-test vs. inter-test | 0.345 | 0.94 | 0.47 |
| Inter-test vs. post-test | 0.554 | 0.59 | 0.30 |
| Pre-test vs. post-test | 0.043* | 2.02 | 1.01 |
* Legend: p = statistically significant; * = Statistically significant difference at the p < 0.05 level; Z = nonparametric Wilcoxon test; d = Cohen’s d.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



