
Submitted:
16 September 2024
Posted:
17 September 2024
You are already at the latest version
Abstract
This analysis investigates health outcomes by cause and income group across European and African countries, highlighting significant disparities tied to economic status. Low and lower-middle-income countries in Africa face a greater burden of disease, particularly in acute lower respiratory infections, diarrheal diseases, bacterial infections, HIV/AIDS, and maternal conditions. This is primarily due to limited access to clean water, sanitation, and healthcare services. In contrast, high-income African countries exhibit better health outcomes. European countries show variations: lower-middle-income nations suffer more fro4m acute respiratory infections and HIV/AIDS, while high-income countries report higher incidences of cancer and bacterial infections. These differences reflect disparities in healthcare quality and social determinants. The study emphasizes the need for targeted policy initiatives to address these disparities by focusing on socioeconomic factors and improving healthcare access and quality across all income groups.
Keywords:
Health disparities
; Socioeconomic status
; Disease burden
; Healthcare access
; European and African countries
; Public Health Policy
1. Introduction
Health disparities between continents, particularly between European and African countries, are closely linked to socioeconomic factors. Low- and lower-middle-income countries in Africa bear a higher disease burden, including acute lower respiratory infections, diarrheal diseases, bacterial infections, HIV/AIDS, and maternal conditions. This elevated burden is primarily due to limited access to clean water, sanitation, and healthcare services (Braveman & Gottlieb, 2014). In contrast, high-income African countries tend to exhibit better health outcomes. Disparities also exist within European countries; lower-middle-income nations experience higher rates of acute respiratory infections and HIV/AIDS, whereas high-income countries report greater incidences of cancer and bacterial infections. These variations reflect differences in healthcare quality and social determinants (Braveman & Gottlieb, 2014).
Social determinants of health are crucial in shaping health outcomes and contributing to disparities observed across different populations (Abbott & Williams, 2015). Socioeconomic status (SES) is a significant factor in health research, influencing findings and implications for practice and policy (Braveman et al., 2005). It is well established that SES affects dietary habits and health-related outcomes (Vlismas et al., 2009). Additionally, disparities in health outcomes are associated with ethnic background, economic conditions, and social class (Lauritano et al., 2021).
Research has demonstrated that socioeconomic factors play a pivotal role in determining health outcomes. For instance, disparities in survival rates for retinoblastoma have been observed between higher-income and lower-income countries (Canturk et al., 2010; Wong et al., 2022). Furthermore, socioeconomic factors are linked to mortality rates among European cystic fibrosis patients, underscoring the impact of SES on health (McKone et al., 2021).
Addressing health disparities necessitates targeted policy initiatives that focus on socioeconomic factors and aim to improve healthcare access and quality across all income groups (Braveman & Gottlieb, 2014). By understanding and addressing the social determinants of health, policymakers can work toward reducing disparities and enhancing overall health outcomes globally.
2. Data and Methods
2.1. Data Source
The data on neonatal deaths by cause across all WHO regions (Africa, the Americas, Eastern Mediterranean, Europe, South-East Asia, and Western Pacific), spanning 30 years, have been meticulously collected from the World Health Organization's Maternal, Newborn, Child, and Adolescent Health and Ageing Database since 1990. This database includes high-quality, verified data reported by health ministries or national agencies of member states, ensuring its reliability for routine monitoring.
The indicator "Number of neonatal deaths by cause" aims to capture deaths occurring within the first 28 days of life, categorized by specific causes as defined by ICD-10 codes. The primary data sources are civil registration systems with comprehensive coverage (at least 80%) and medical certification of cause of death. In regions where civil registration data are unavailable, nationally representative epidemiological studies are employed, including specialized studies based on verbal autopsies or other methodologies.
Estimates of neonatal causes of death are carefully prepared by the WHO's Child and Adolescent Cause of Death group (CA CODE). Methodologies for these estimations are detailed in publications such as Perin et al.'s systematic analysis of global causes of under-5 mortality and subsequent updates. These estimates provide insights into global and regional aggregates, adjusted for data availability and reliability among UN Member States.
In addition to civil registration, alternative data sources include population-based surveys, census data, and specialized studies focusing on child mortality causes. However, civil registration remains the preferred source due to its superior reliability and completeness.
Data collection occurs biennially to ensure timely updates and dissemination, thereby supporting informed policy-making and program development aimed at reducing neonatal mortality globally. While these estimates are invaluable for tracking trends and making broad regional comparisons, they may present limitations in granularity for sub-national analysis or program-specific monitoring.
The WHO database on neonatal deaths by cause serves as a crucial resource for understanding and addressing global child health challenges. It highlights the importance of robust data collection methodologies and international collaboration in improving neonatal survival and informing health interventions across diverse regions.
2.2. Methodology
In researching the relationship between health outcomes and income groups, a crucial methodological approach involves data aggregation. This process entails constructing a pivot table to consolidate data points for each income group and cause. The aggregated value for a specific income group and cause is derived by summing the "Value Numeric" for that group and cause, while taking into account the number of data points available for that particular income group and cause.
Research has demonstrated a robust correlation between health and income, both within and across countries. However, the causal relationship between income improvements and health outcomes remains a topic of ongoing debate. Methodological choices in data aggregation, particularly in models related to infectious diseases influenced by human mobility, significantly affect the reliability of these models.
Studies have explored the effects of income inequality on health outcomes, revealing that the level of spatial aggregation can influence the association between income inequality and morbidity, especially among older populations. Additionally, the relationship between income and health is bidirectional: low income levels can lead to adverse health outcomes, while chronic childhood illnesses can negatively impact family income.
It is essential to consider income shocks and their implications for health, highlighting the need to understand the dynamic relationship between health outcomes and income across diverse countries. Furthermore, individual-level factors such as income and education are identified as critical predictors of health outcomes, underscoring the importance of socioeconomic status in health disparities.
Employing rigorous data aggregation techniques and addressing the multifaceted relationship between income and health outcomes are vital for advancing our understanding of health inequalities and the impact of income disparities on health metrics.
3. Results and Discussion
3.1. Health Outcomes by Cause and Income Group in European and African Countries
The analysis of health outcomes by cause and income group (Figure 1) in European and African countries reveals significant disparities closely associated with economic status. Low- and lower-middle-income countries in Africa experience a pronounced disease burden compared to their higher-income counterparts across various health issues. These disparities often reflect challenges such as limited access to clean water, sanitation, and healthcare services, which are more prevalent in economically disadvantaged regions.
Health outcomes vary substantially across income groups in both European and African countries, highlighting disparities in disease burden and healthcare access. In African nations, low-income countries face higher rates of acute lower respiratory infections (ALRI), diarrheal diseases (DD), bacterial and other blood infections (BABT), cancer (CA), HIV/AIDS, injuries, maternal and endocrine conditions (M/E), serious infections in children (SICN), and premature deaths (Prem) (Adler & Newman, 2002). These disparities suggest challenges in healthcare access and preventive programs, likely due to insufficient healthcare services for mothers and children. Conversely, high-income countries in Africa exhibit lower burdens for most health outcomes studied, indicating the effectiveness of their healthcare systems and broader social determinants of health (Adler & Newman, 2002).
In European countries, disparities in health outcomes across income groups are also evident. Upper-middle-income countries show higher rates of ALRI, while high-income countries report increased burdens of BABT, CA, and negligible cases of DD, reflecting better diagnostic facilities and reporting systems (Adler & Newman, 2002). The prevalence of HIV/AIDS is notably higher in lower-middle-income countries in Europe, suggesting potential gaps in preventive measures and treatment access. Injuries are more prevalent in upper-middle-income countries, possibly due to socio-environmental factors such as occupational hazards and traffic accidents (Adler & Newman, 2002). Maternal and endocrine conditions are most common in upper-middle-income countries in Europe, highlighting variations in healthcare access within the region (Adler & Newman, 2002).
These discrepancies underscore the necessity of policy initiatives targeting socioeconomic factors (income, education, and occupation) and the pathways through which these determinants influence health (Adler & Newman, 2002). A comprehensive strategy that addresses both social determinants of health and healthcare access is essential for mitigating these disparities. Global disparities in cancer outcomes, for instance, reflect differing national investments in cancer control, emphasizing the importance of equitable access to high-quality medical treatment (Souza et al., 2016). Persistent health gaps related to cardiovascular outcomes by income level highlight the significance of addressing socioeconomic variables in healthcare delivery (Beckman et al., 2017).
Disparities in health outcomes are not only observed between high-, middle-, and low-income countries but also within countries, underscoring the need to address structural disparities in healthcare access that perpetuate inequalities (Guo et al., 2022). Challenges in diagnosing and treating cancer in low- and middle-income countries compared to high-income countries highlight the need for improved healthcare infrastructure and access to medical resources (K., 2023). Additionally, the disproportionate health disparities faced by Indigenous populations due to historical injustices and inadequate support systems emphasize the broader social determinants of health contributing to inequities in healthcare outcomes (Lopez-Carmen, 2022).
In Africa, the prevalence of childhood stunting in low- and lower-middle-income countries highlights the need to address socioeconomic factors and improve nutrition and healthcare access to combat this public health issue (Tamir, 2024). The impact of health expenditure on maternal and child mortality in African countries underscores the critical role of government spending in enhancing health outcomes and reducing mortality rates among vulnerable populations (Bayero et al., 2022). Moreover, the global shortage of health workers poses a threat to achieving equity and universal health coverage, necessitating strategic workforce planning and investments in healthcare personnel (Boniol et al., 2022).
Addressing the complex interplay of social, economic, and healthcare factors in low- and middle-income countries in Africa is essential for improving health outcomes, reducing disparities, and advancing towards sustainable and equitable healthcare systems. By prioritizing mental health support, strengthening health systems, enhancing research collaborations, and investing in healthcare infrastructure and workforce, African nations can work towards achieving better health outcomes and promoting overall well-being for their populations.
3.2. Age-Specific Health Conditions in European and African Countries
The comparative analysis of age-specific health conditions (Figure 2) between African and European countries for the 0-28-year-old age group underscores significant disparities in health outcomes, shaped by geographic, economic, and infrastructural differences.
The disparities in the prevalence of various health conditions between African and European countries highlight differences in public health infrastructure and healthcare access. African nations exhibit higher rates of acute lower respiratory infections (ALRI), bacterial and other blood infections (BABT), diarrheal diseases (DD), HIV/AIDS, injury-related health outcomes (Inj), maternal and endocrine conditions (M/E), premature deaths (Prem), serious infections in children (SICN), and tetanus (Tet) compared to Europe. Conversely, cancer occurrences in young populations are more prevalent in Europe, possibly due to better diagnostic facilities or different lifestyle and genetic factors. The burden of infectious diseases in Africa, particularly in BABT, is attributed to challenges in disease control stemming from inadequate sanitary conditions and healthcare systems (He, 2023; Heaney et al., 2019).
Diarrheal diseases in Africa pose a significant public health concern, with studies emphasizing the impact of diarrheal pathogens on children under five (Page et al., 2011; Tareke et al., 2022). Factors such as poor water quality, sanitation, and hygiene practices contribute to the high burden of diarrheal diseases in African countries (Yaya et al., 2018). Additionally, harmful practices in managing childhood diarrhea worsen the situation (Carter et al., 2015). The lack of infrastructure for diagnosis in sub-Saharan Africa hampers the identification of the causes of diarrhea, making it challenging to implement effective interventions (Page et al., 2011).
The burden of diarrheal diseases in Africa is closely linked to poverty, with under-five children being particularly vulnerable (He, 2023). The prevalence of diarrheal diseases in Africa is associated with various modifiable and non-modifiable risk factors, highlighting the necessity for targeted interventions to address this public health issue (He, 2023). Continuous efforts to reduce the burden of diarrheal diseases in low-income communities are essential for improving health outcomes (Vasco et al., 2014).
The prevalence of diarrhea in young children from low-income countries, particularly in Africa, has been associated with significant alterations in intestinal microbiota composition (Pop et al., 2014). Studies have shown that diarrheal diseases, including those caused by pathogens like rotavirus, are major contributors to severe diarrheal illnesses in African children (Mwenda et al., 2010). The presence of diarrheagenic Escherichia coli in sub-Saharan Africa further emphasizes the need to broaden pathogen surveillance and enhance detection capabilities in local laboratories to address diarrheal diseases effectively (Okeke, 2009).
Healthcare-seeking behavior for diarrhea in children under five in rural areas has been found to vary by context, highlighting the importance of developing appropriate care strategies and estimating disease burden (Page et al., 2011). Improving water, sanitation, and hygiene practices has been identified as crucial in preventing diarrhea among under-five children in Africa, emphasizing the significance of environmental factors in disease prevention (Yaya et al., 2018). Additionally, harmful practices in the management of childhood diarrhea in low- and middle-income countries underscore the need for improved healthcare practices and interventions (Carter et al., 2015).
The burden of acute lower respiratory infections among children under five in Africa has been associated with various social, economic, and environmental risk factors, emphasizing the impact of seasonal variations on disease prevalence (Harerimana et al., 2016). The prevalence of respiratory syncytial virus in pediatric populations with acute respiratory tract illnesses in Africa highlights the importance of prevention and control strategies for respiratory infections in children (Tafa et al., 2023). Furthermore, the impact of climate change on children's health in South Africa underscores the need to address diseases like diarrhea and respiratory infections in the context of changing environmental conditions (Adeboyejo et al., 2012).
Addressing the burden of diarrheal diseases and respiratory infections in African children requires a multifaceted approach that considers factors such as microbiota composition, pathogen surveillance, healthcare-seeking behavior, water and sanitation practices, and environmental influences. Targeted interventions focusing on improving healthcare practices, enhancing surveillance capabilities, and implementing preventive measures are essential to reduce the prevalence of these diseases and improve health outcomes among vulnerable populations in Africa.
3.3. Trend of Diseases Over Time in European Countries
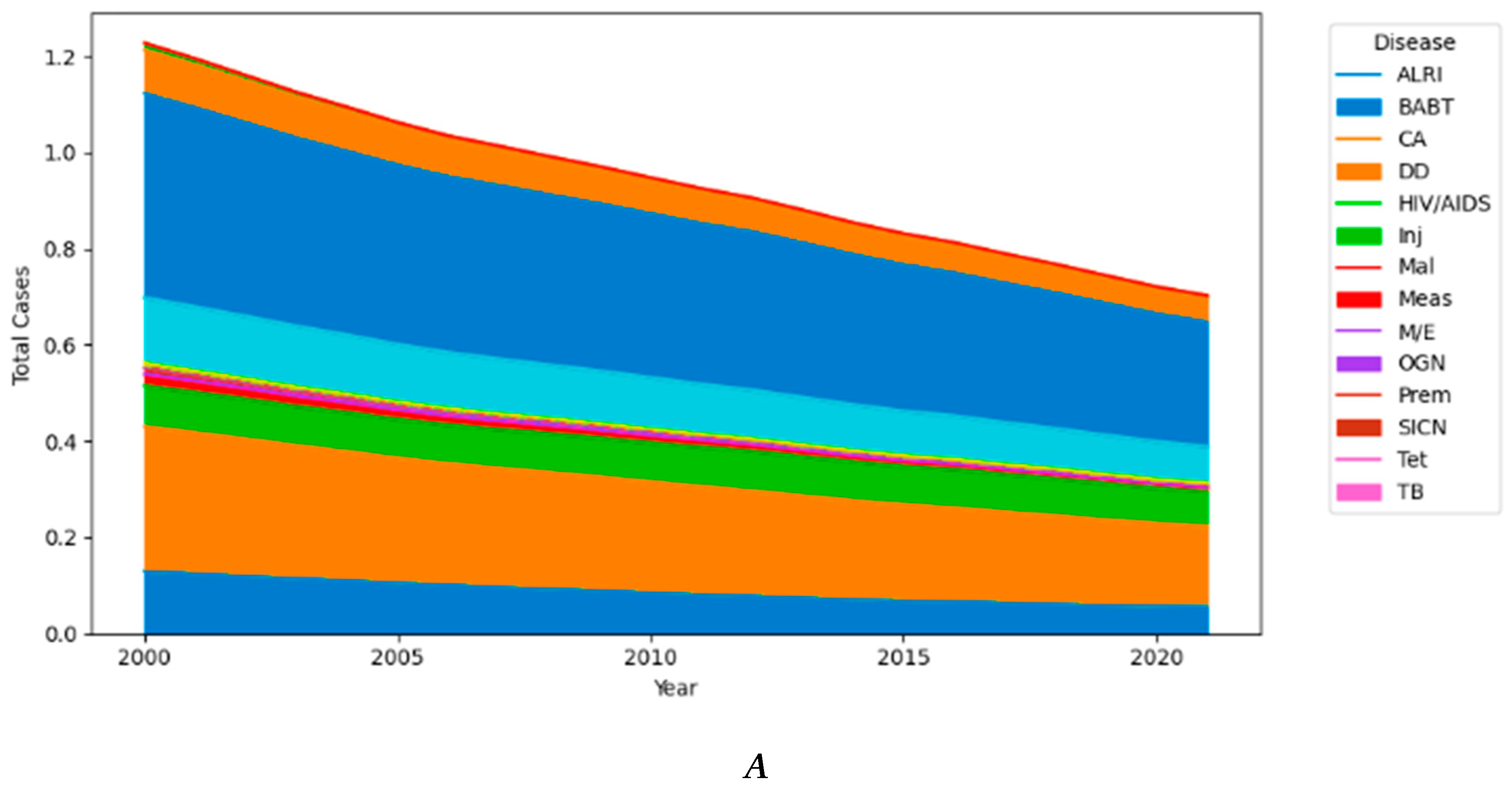
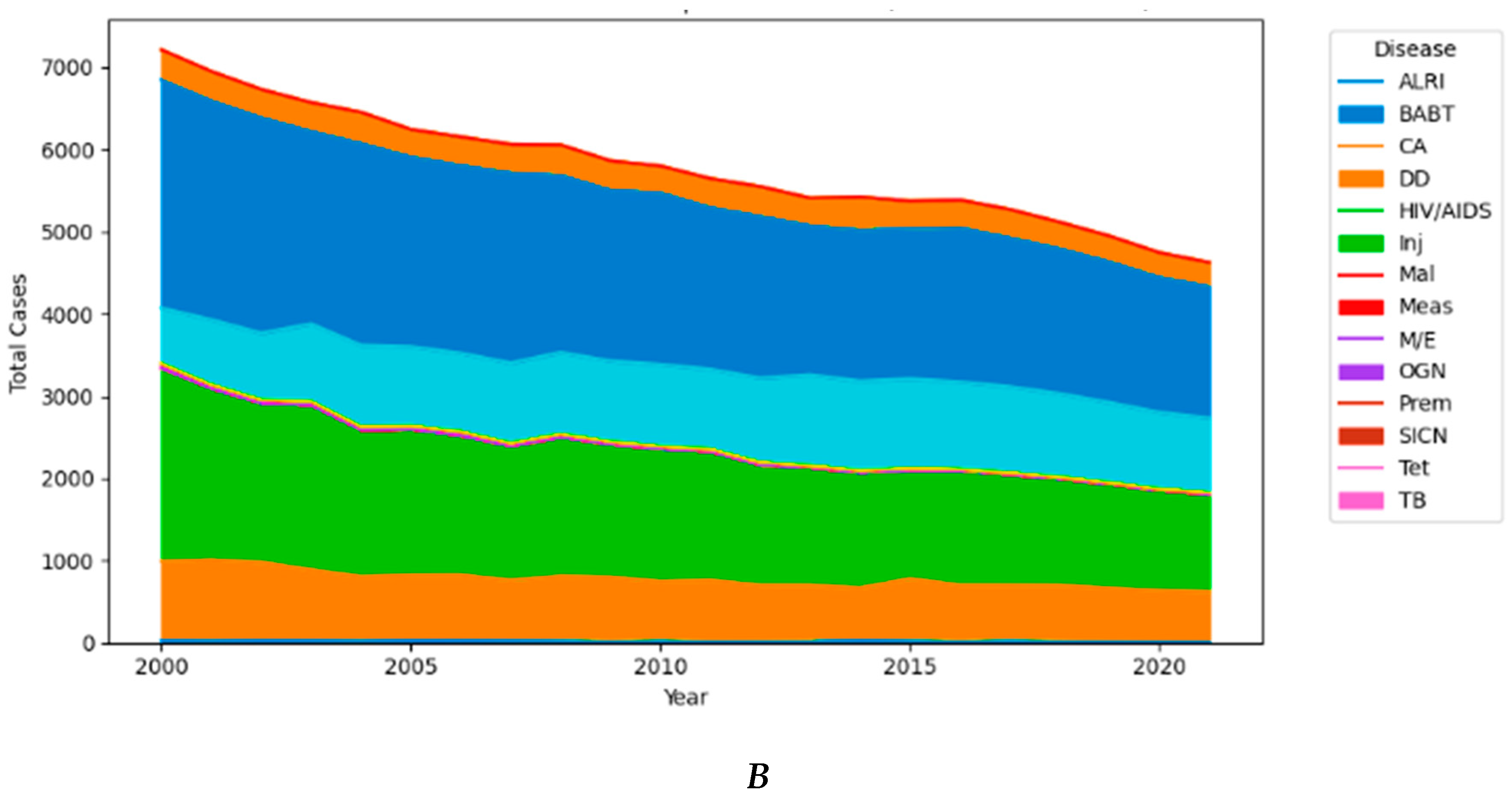
The trends in disease prevalence over time (Figure 3) across African and European countries reveal significant health challenges, with a focus on premature deaths, infectious diseases, and organ-specific conditions. Premature deaths stand out as a dominant issue, constituting approximately 35.84% of total cases in both regions. This high percentage underscores urgent health concerns leading to early mortality, likely influenced by factors such as infectious diseases, inadequate healthcare infrastructure, and limited access to medical services.
Infections, particularly bacterial and blood-related ones, are significant contributors to morbidity and mortality in both African and European countries. The prevalence of these infections is influenced by factors such as poor sanitation and limited access to clean water, which are more pronounced in regions with inadequate public health measures (He et al., 2020). Organ-specific conditions affecting the liver, heart, or lungs, as well as acute lower respiratory infections, underscore the critical role of air quality and respiratory pathogens as major public health concerns (Dockery, 2009). The rising prevalence of cancer cases in both regions may be attributed to lifestyle changes, environmental factors, and improved diagnostic capabilities, although challenges in cancer diagnosis and treatment availability persist (Deguen & Zmirou-Navier, 2010).
The impact of infectious diseases on public health is substantial, with conditions such as typhoid intestinal perforation and HIV-associated cryptococcal meningitis posing significant health risks, particularly in sub-Saharan Africa. The burden of these diseases underscores the importance of strengthening healthcare systems, enhancing surveillance capabilities, and implementing preventive measures to mitigate the spread of infectious pathogens and reduce associated morbidity and mortality (Ha et al., 2022; Giovanni, 2022; Gelband et al., 2020; Denkyira et al., 2022; Oduoye, 2024). Furthermore, the prevalence of infectious diseases highlights the critical need for pharmacovigilance systems in resource-limited settings to monitor adverse drug reactions, enhance drug safety, and improve public health outcomes. Strengthening national pharmacovigilance centers in Africa is essential to address challenges related to medication safety and ensure the effective management of infectious diseases and other health conditions (Boschi-Pinto et al., 2008; Pillay, 2023).
The impact of organ-specific conditions affecting the liver, heart, or lungs underscores the critical role of air quality and respiratory pathogens in public health. Acute lower respiratory infections, in particular, emerge as a major concern, emphasizing the necessity for improved air quality and more effective management of respiratory diseases. The prevalence of these conditions is influenced by environmental factors, including air pollution and exposure to respiratory pathogens, which can significantly impact respiratory health outcomes in both African and European countries (Ferkol & Schraufnagel, 2014; Ren et al., 2009). Respiratory infections caused by common viruses such as influenza, parainfluenza, and respiratory syncytial virus pose a significant health risk, particularly in vulnerable populations. Understanding the prevalence and impact of these respiratory pathogens is crucial for developing effective prevention and treatment strategies to mitigate the burden of respiratory diseases. The ongoing COVID-19 pandemic has further highlighted the importance of respiratory health and the need for robust public health measures to address infectious diseases (Groves et al., 2021; Dhefer, 2021; Lukšić et al., 2013). The detection and surveillance of respiratory viruses play a vital role in public health preparedness and response. High-throughput sequencing and metagenomic approaches have revolutionized the identification of viral pathogens, enabling rapid and accurate diagnosis of respiratory infections. These advancements in diagnostic technologies are essential for informing public health interventions and optimizing resource allocation to combat respiratory diseases effectively (Gussow et al., 2020). Furthermore, the impact of air pollution on respiratory health is well-documented, with studies highlighting the association between poor air quality and respiratory diseases. Monitoring air quality and implementing measures to reduce pollution levels are critical for protecting respiratory health and preventing respiratory infections. Public health initiatives aimed at raising awareness of air quality issues and promoting respiratory health can contribute to reducing the burden of respiratory diseases in communities (Verhein et al., 2018; Lekana-Douki et al., 2018; Pennington et al., 2019).
The burden of cancer in Africa is substantial, with breast, bladder, liver, prostate, lung, colorectal, esophageal, and cervical cancers being prevalent in various regions. Late diagnosis and advanced disease presentation are common challenges in African countries, leading to poorer cancer outcomes. The lack of specialized health personnel, including oncologists and pathologists, limited health system infrastructure, and financial constraints among patients contribute to the difficulties in delivering optimal cancer care in Africa (Lukamba et al., 2018; Vanderpuye et al., 2019; Jaddaoui et al., 2020; Hamdi et al., 2021; Canga et al., 2022).
Children are particularly vulnerable to serious infections, often exacerbated by malnutrition and insufficient pediatric healthcare services (Berry et al., 2017). Diarrheal diseases remain a significant public health issue, primarily driven by poor sanitation and hygiene practices (Moshammer & Wallner, 2011). Diseases like injuries, tetanus, and HIV/AIDS show lower percentages, indicating effective control measures or potential underreporting due to other prevailing health crises (Baryarama et al., 2006). The absence or minimal cases of diseases like malaria, measles, and tuberculosis may suggest successful eradication efforts or underreporting due to diagnostic and reporting limitations (Pacheco et al., 2011).
The vulnerability of children to severe infections, exacerbated by factors like malnutrition and inadequate pediatric healthcare services, highlights the critical issue of diarrheal diseases as a major public health concern. Poor sanitation and hygiene practices, coupled with inadequate waste management and clean water supply, contribute to frequent outbreaks and high mortality rates among children (Bekele et al., 2023; Alexander et al., 2013; Asefa et al., 2020; Degefa et al., 2018).
Interestingly, lower percentages of diseases such as injuries, tetanus, and HIV/AIDS in the data may suggest effective control measures like widespread vaccination and improved public health initiatives. However, it could also indicate potential underreporting due to the overshadowing presence of other health crises (Bekele et al., 2023; Alexander et al., 2013; Asefa et al., 2020; Degefa et al., 2018).
The near absence or minimal reporting of diseases like malaria, measles, and tuberculosis may imply successful eradication efforts in some regions or, conversely, underreporting due to diagnostic limitations and reporting challenges. Despite significant reduction efforts for malaria globally, concerns about underreporting persist, especially in rural and underserved areas (Bekele et al., 2023; Alexander et al., 2013; Asefa et al., 2020; Degefa et al., 2018).
Efforts to address childhood diarrheal diseases require a multifaceted approach, including improving sanitation, promoting hygiene practices, enhancing healthcare-seeking behavior, and addressing factors contributing to delays in seeking treatment (Adam et al., 2018; Getachew et al., 2018; Tafere et al., 2020; Abuzerr et al., 2019). Additionally, studies on community readiness and the impact of interventions on reducing childhood diarrheal diseases underscore the importance of collaborative strategies to prevent and treat such illnesses (Anderson et al., 2020).
The similarity in disease percentages across regions raises questions about data representation and underlying factors influencing these patterns. It implies a combination of universal health challenges and unique regional issues that shape disease prevalence and management strategies (Haverkos et al., 2003). Tailored healthcare policies and interventions are crucial to address both global health challenges and region-specific health issues, aiming to enhance health outcomes across diverse populations.
3.4. Contrasting Health Profiles between Africa vs. Europe
The descriptive statistics for health causes in Africa and Europe present a stark contrast in terms of both mean values and variability. In Africa, several health causes exhibit significantly higher mean values compared to Europe. For instance, the mean value for ALRI (Acute Lower Respiratory Infections) in Africa is 2361.1, with a standard deviation of 6894.4, highlighting the wide variability and higher burden of this health issue. In contrast, Europe has a much lower mean value for ALRI at 10.8 and a standard deviation of 30.8, indicating a more consistent and significantly lesser impact.
In Africa, health issues such as Acute Lower Respiratory Infections (ALRI) exhibit significantly higher mean values compared to Europe, indicating a greater burden of disease in Africa. The mean value for ALRI in Africa is 2361.1 with a standard deviation of 6894.4, while in Europe, the mean value is much lower at 10.8 with a standard deviation of 30.8 (Yuyun et al., 2020). This disparity in health outcomes between Africa and Europe is further highlighted by the mortality-incidence ratio, which is substantially higher in Africa compared to high-income countries (Vanderpuye et al., 2019).
To address the health disparities in Africa, various studies emphasize the need for improved healthcare infrastructure and resources. For instance, there is a call for action to modernize diagnostic medicine across Africa to provide essential care to patients (Nelson et al., 2016). Additionally, efforts to enhance healthcare delivery are crucial, especially in regions like South Africa where disparities in health spending, staffing levels, and accessibility persist between public and private sectors (Ogunbodede et al., 2015).
Moreover, the impact of environmental factors on health outcomes in Africa cannot be overlooked. Air pollution has been identified as a significant health hazard in Africa, responsible for a considerable number of deaths annually. Household air pollution, driven by solid biofuel use, and outdoor air pollution contribute significantly to the health burden in the region (Isaxon et al., 2022).
Similarly, causes like BABT (Bacterial, Viral, and Parasitic Diseases) and Premature Births (Prem) in Africa show mean values of 5035.7 and 6578.4, respectively, with high standard deviations, reflecting the substantial impact and variability across the continent. These figures dwarf the European statistics for the same causes, where the mean values for BABT and Prem are 56.7 and 175.7, respectively. This significant discrepancy underscores the greater health challenges faced by African countries.
The burden of disease in sub-Saharan Africa is primarily dominated by infectious diseases, but there is an ongoing demographic transition leading to an increasing prevalence of noncommunicable diseases (NCDs) in the region (Maphumulo & Bhengu, 2019). High blood pressure, or hypertension, is identified as the most common underlying risk factor for cardiovascular disease in sub-Saharan Africa (Cappuccio & Miller, 2016). The epidemiology of cardiovascular diseases in sub-Saharan Africa, including mortality rates and disease burden, has been studied extensively, highlighting the significant impact of these conditions on the region (Moran et al., 2013).
African countries experience more than 100 disease outbreaks and health emergencies annually, emphasizing the critical need for robust public health emergency response systems in the region (Masiira et al., 2020). Additionally, the rise in non-communicable diseases is adding further complexity to the burden faced by African health systems (Karamagi et al., 2022). Strengthening research capacity in Africa is crucial for understanding the social determinants of health and developing interventions to improve health outcomes and health systems in the region (Ezeh et al., 2010).
Certain health causes like HIV/AIDS, Injuries (Inj), and Malnutrition/Electrolyte Imbalance (M/E) also display considerable differences. In Africa, the mean for HIV/AIDS is 29.3, and for Injuries, is 80.6, both with substantial standard deviations, indicating notable prevalence and variation. Europe, however, has almost negligible mean values for these causes, pointing to better health infrastructure and preventive measures.
Interestingly, some causes like Malaria (Mal) and Measles (Meas) show negligible or zero mean values in both continents, reflecting effective eradication or control measures in place. However, Africa still shows a slightly higher burden for Malaria, though the mean value is close to zero, indicating isolated cases.
In Africa, health causes like HIV/AIDS and Injuries exhibit significantly higher mean values compared to Europe, indicating a higher prevalence and variation in these conditions (Nkumama et al., 2017). The mean values for HIV/AIDS and Injuries in Africa are 29.3 and 80.6, respectively, with substantial standard deviations, highlighting the notable burden of these health issues (Nkumama et al., 2017). Conversely, Europe shows almost negligible mean values for these causes, suggesting better health infrastructure and preventive measures in place (Nkumama et al., 2017).
Regarding Malnutrition/Electrolyte Imbalance (M/E), Africa faces challenges with a slightly higher burden for Malaria compared to Europe, although both continents show negligible or zero mean values for Malaria and Measles, reflecting effective control measures (Nkumama et al., 2017). Studies indicate that the burden of malaria in Africa is decreasing, supported by large-scale modeling techniques and the Global Burden of Disease 2017 study (Nkumama et al., 2017; Battle et al., 2019). Additionally, research emphasizes the importance of tracking trends in malaria risk in Africa systematically to understand the evolving landscape of transmission (Gething et al., 2014).
Furthermore, the impact of the COVID-19 pandemic on malaria control in Africa has been a concern, with disruptions to effective malaria case management potentially affecting the malaria burden in sub-Saharan Africa (Dzianach et al., 2023). Studies have shown that interruptions in treatment and prevention services could lead to a doubling of the death toll from malaria (Aborode et al., 2021).
The statistics comparing the prevalence of Diarrheal Diseases (DD), Cancer (CA), and Neonatal Causes (SICN) between Africa and Europe indicate significant differences, with Africa showing a higher mean value for Cancer at 1135.1 compared to 119.9 in Europe (Alexander et al., 2013). This disparity in disease burden can be attributed to various factors. Studies have shown that climate change can exacerbate the public health threat of diarrheal diseases in regions like Botswana (Okeke, 2009). Additionally, research emphasizes the importance of broadening the scope of pathogens studied in epidemiological surveys to include diarrheagenic Escherichia coli, especially in sub-Saharan Africa (Rojas-López et al., 2018). The Global Enteric Multicenter Study (GEMS) is a significant ongoing effort in Africa and Asia aimed at identifying the etiology and burden of pediatric diarrheal diseases (Levine et al., 2012). Furthermore, open defecation prevalence in sub-Saharan Africa has been linked to diarrheal disease outbreaks, highlighting the importance of sanitation in disease prevention (Galan et al., 2013).
In terms of cancer, the risk of cervical cancer in women living with HIV across continents, including Europe and South Africa, has been studied extensively (Rohner et al., 2019). Moreover, the emergence of colorectal cancer in West Africa over the past few decades underscores the changing landscape of cancer incidence in the region (Irabor, 2017). The impact of rotavirus vaccines in reducing severe rotavirus diarrhea in countries like Ghana has been significant, demonstrating the effectiveness of vaccination programs in combating diarrheal diseases (Armah et al., 2016). However, challenges remain in fully realizing the potential benefits of rotavirus vaccines in Africa (Steele et al., 2023).
Overall, these statistics highlight the significant disparities in health burdens between Africa and Europe. Africa shows higher mean values and variability for most health causes, suggesting a greater prevalence and impact of these health issues. This disparity emphasizes the need for enhanced healthcare infrastructure, preventive measures, and targeted interventions in African countries to address these pressing health challenges. In contrast, Europe’s relatively lower mean values for these health causes reflect better healthcare systems, preventive strategies, and overall public health management.
4. Conclusion
The comparative analysis of health outcomes by cause and income group in African and European countries reveals disparities closely linked to economic status and healthcare infrastructure. In African nations, particularly low and lower-middle-income countries, conditions like acute lower respiratory infections (ALRI), diarrheal diseases (DD), and bacterial and other blood infections (BABT) pose significant burdens. Moreover, chronic diseases like cancer (CA) are increasingly prevalent in these countries, indicating a shift in disease patterns amidst improving diagnostic capabilities.
Conversely, high-income European countries exhibit minimal burdens for most health outcomes, showcasing the effectiveness of their healthcare systems and broader social determinants of health. While upper-middle-income European countries have higher ALRI rates, high-income countries face substantial burdens of bacterial infections and cancer, likely due to advanced diagnostic facilities and robust reporting systems.
The analysis underscores the critical public health challenges in low-income African countries, with high rates of HIV/AIDS, maternal and endocrine conditions, and serious infections in children, leading to alarming premature deaths (Bayero et al., 2022). In contrast, European countries experience similar disease distributions but within the context of superior healthcare systems. Premature deaths and bacterial infections are notable concerns, reflecting issues like aging populations, chronic diseases, and healthcare-associated infections.
The disparities highlighted call for targeted health policies and interventions in African countries to address infectious and non-communicable diseases by enhancing healthcare infrastructure, improving sanitation, strengthening disease surveillance, and boosting health education. Simultaneously, European countries must focus on maintaining infection control measures and advancing antibiotic stewardship programs to tackle their unique health challenges.
The findings emphasize the urgent need for international cooperation and focused efforts to improve health outcomes and bridge the health gap between Africa and Europe, underscoring the importance of tailored strategies to address the specific health challenges faced by each region.
Author Contributions
Ahmed Ould Boudia: was responsible for the conceptualization and design of the study, data collection, and analysis, and played a leading role in drafting the manuscript. Contributed to the data analysis and interpretation. Frank Adusei-Mensah: was involved in critically revising the manuscript for important intellectual content. Bismark Sarfo: provided expertise in specific technical and methodological aspect, significantly contributing to the methodology section and data interpretation, and assisted in manuscript revision.
Funding
No founding.
Data Availability
Not applicable.
Ethics Approval
Not applicable.
Consent to Participate
All authors agreed to contribute to this study.
Consent for Publication
Not applicable.
Competing Interests
The authors declare no competing interests.
References
- Abbott, L. and Williams, C. (2015). Influences of social determinants of health on african americans living with hiv in the rural southeast: a qualitative meta-synthesis. Journal of the Association of Nurses in Aids Care, 26(4), 340-356. [CrossRef]
- Aborode, A., David, K., Uwishema, O., Nathaniel, A., Imisioluwa, J., Onigbinde, S., … & Farooq, F. (2021). Fighting covid-19 at the expense of malaria in africa: the consequences and policy options. American Journal of Tropical Medicine and Hygiene, 104(1), 26-29. [CrossRef]
- Abuzerr, S., Nasseri, S., Yunesian, M., Mirfazaelian, H., Mahvi, A., Nabizadeh, R., … & Mustafa, A. (2019). Prevalence of diarrheal illness and healthcare-seeking behavior by age-group and sex among the population of gaza strip: a community-based cross-sectional study. BMC Public Health, 19(1). [CrossRef]
- Adam, M., Wang, J., Enan, K., Shen, H., Wang, H., Hussein, A., … & Ma, X. (2018). Molecular survey of viral and bacterial causes of childhood diarrhea in khartoum state, sudan. Frontiers in Microbiology, 9. [CrossRef]
- Adeboyejo, T., Matamale, L., & Kharidza, S. (2012). Impact of climate change on children’s health in limpopo province, south africa. International Journal of Environmental Research and Public Health, 9(3), 831-854. [CrossRef]
- Adler, N. and Newman, K. (2002). Socioeconomic disparities in health: pathways and policies. Health Affairs, 21(2), 60-76. [CrossRef]
- Alexander, K., Carzolio, M., Goodin, D., & Vance, E. (2013). Climate change is likely to worsen the public health threat of diarrheal disease in botswana. International Journal of Environmental Research and Public Health, 10(4), 1202-1230. [CrossRef]
- Anderson, D., Rees, D., & Wang, T. (2020). The phenomenon of summer diarrhea and its waning, 1910-1930. Explorations in Economic History, 78, 101341. [CrossRef]
- Armah, G., Pringle, K., Enweronu-Laryea, C., Ansong, D., Mwenda, J., Diamenu, S., … & Lopman, B. (2016). Impact and effectiveness of monovalent rotavirus vaccine against severe rotavirus diarrhea in ghana. Clinical Infectious Diseases, 62(suppl 2), S200-S207. [CrossRef]
- Asefa, A., Qanche, Q., Asaye, Z., & Abebe, L. (2020). <p>determinants of delayed treatment-seeking for childhood diarrheal diseases in southwest ethiopia: a case–control study</p>. Pediatric Health Medicine and Therapeutics, Volume 11, 171-178. [CrossRef]
- Baryarama, F., Mugisha, J., & Luboobi, L. (2006). Mathematical model for hiv/aids with complacency in a population with declining prevalence. Computational and Mathematical Methods in Medicine, 7(1), 27-35. [CrossRef]
- Battle, K. E., Lucas, T. C. D., Nguyen, M., Howes, R. E., Nandi, A. K., Twohig, K. A., Pfeffer, D. A., Cameron, E., Rao, P. C., Casey, D., Gibson, H. S., Rozier, J. A., Dalrymple, U., Keddie, S. H., Collins, E. L., Harris, J. R., Guerra, C. A., Thorn, M. P., Bisanzio, D.,... Gething, P. W. (2019). Mapping the global endemicity and clinical burden of Plasmodium vivax, 2000–17: a spatial and temporal modelling study. Lancet, 394(10195), 332–343. [CrossRef]
- Bayero, S., Safiyanu, B., & Gurin, I. (2022). The impact of health expenditure on maternal and child mortality in african countries. International Review of Social Sciences Research, 2(3), 20-36. [CrossRef]
- Beckman, A., Herrin, J., Nasir, K., Desai, N., & Spatz, E. (2017). Trends in cardiovascular health of us adults by income, 2005-2014. Jama Cardiology, 2(7), 814. [CrossRef]
- Bekele, M., Urgessa, M., Kumsa, K., & Sinba, E. (2023). Contributing factors of delay in seeking treatment for childhood diarrheal diseases in berbere woreda, ethiopia: an unmatched case–control study. Journal of Health Population and Nutrition, 42(1). [CrossRef]
- Berry, M., Nickerson, N., & Odum, A. (2017). Delay discounting as an index of sustainable behavior: devaluation of future air quality and implications for public health. International Journal of Environmental Research and Public Health, 14(9), 997. [CrossRef]
- Boniol, M., Kunjumen, T., Nair, T., Siyam, A., Campbell, J., & Diallo, K. (2022). The global health workforce stock and distribution in 2020 and 2030: a threat to equity and ‘universal’ health coverage?. BMJ Global Health, 7(6), e009316. [CrossRef]
- Braveman, P. and Gottlieb, L. (2014). The social determinants of health: it's time to consider the causes of the causes. Public Health Reports, 129(1_suppl2), 19-31. [CrossRef]
- Braveman, P., Cubbin, C., Egerter, S., Chideya, S., Marchi, K., Metzler, M., … & Posner, S. (2005). Socioeconomic status in health research. Jama, 294(22), 2879. [CrossRef]
- Canturk, S., Qaddoumi, I., Khetan, V., Ma, Z., Furmanchuk, A., Antoneli, C., … & Chantada, G. (2010). Survival of retinoblastoma in less-developed countries impact of socioeconomic and health-related indicators. British Journal of Ophthalmology, 94(11), 1432-1436. [CrossRef]
- Cappuccio, F. and Miller, M. (2016). Cardiovascular disease and hypertension in sub-saharan africa: burden, risk and interventions. Internal and Emergency Medicine, 11(3), 299-305. [CrossRef]
- Carter, E., Bryce, J., Perin, J., & Newby, H. (2015). Harmful practices in the management of childhood diarrhea in low- and middle-income countries: a systematic review. BMC Public Health, 15(1). [CrossRef]
- Degefa, G., Gebreslassie, M., Meles, K. G., & Jackson, R. (2018). Determinants of delay in timely treatment seeking for diarrheal diseases among mothers with under-five children in central Ethiopia: A case control study. PloS One, 13(3), e0193035. [CrossRef]
- Deguen, S. and Zmirou-Navier, D. (2010). Social inequalities resulting from health risks related to ambient air quality--a european review. European Journal of Public Health, 20(1), 27-35. [CrossRef]
- Dockery, D. (2009). Health effects of particulate air pollution. Annals of Epidemiology, 19(4), 257-263. [CrossRef]
- Dzianach, P., Rumisha, S., Lubinda, J., Saddler, A., Berg, M., Gelaw, Y., … & Weiss, D. (2023). Evaluating covid-19-related disruptions to effective malaria case management in 2020–2021 and its potential effects on malaria burden in sub-saharan africa. Tropical Medicine and Infectious Disease, 8(4), 216. [CrossRef]
- Ezeh, A., Izugbara, C., Kabiru, C., Fonn, S., Kahn, K., Manderson, L., … & Thorogood, M. (2010). Building capacity for public and population health research in africa: the consortium for advanced research training in africa (carta) model. Global Health Action, 3(1), 5693. [CrossRef]
- Fisher, J., Mello, M., Patel, V., Rahman, A., Tran, T., Holton, S., … & Holmes, W. (2011). Prevalence and determinants of common perinatal mental disorders in women in low- and lower-middle-income countries: a systematic review. Bulletin of the World Health Organization, 90(2), 139-149H. [CrossRef]
- Galan, D., Kim, S., & Graham, J. (2013). Exploring changes in open defecation prevalence in sub-saharan africa based on national level indices. BMC Public Health, 13(1). [CrossRef]
- Getachew, A., Guadu, T., Tadie, A., Gizaw, Z., Gebrehiwot, M., Cherkos, D., … & Gebrecherkos, T. (2018). Diarrhea prevalence and sociodemographic factors among under-five children in rural areas of north gondar zone, northwest ethiopia. International Journal of Pediatrics, 2018, 1-8. [CrossRef]
- Gething, P., Battle, K., Bhatt, S., Smith, D., Eisele, T., Cibulskis, R., … & Hay, S. (2014). Declining malaria in africa: improving the measurement of progress. Malaria Journal, 13(1). [CrossRef]
- Gouda, H., Charlson, F., Sorsdahl, K., Ahmadzada, S., Ferrari, A., Erskine, H., … & Whiteford, H. (2019). Burden of non-communicable diseases in sub-saharan africa, 1990–2017: results from the global burden of disease study 2017. The Lancet Global Health, 7(10), e1375-e1387. [CrossRef]
- Guo, J., Hernandez, I., Dickson, S., Tang, S., Essien, U., Mair, C., … & Berenbrok, L. (2022). Income disparities in driving distance to health care infrastructure in the united states: a geographic information systems analysis. BMC Research Notes, 15(1). [CrossRef]
- Harerimana, J., Nyirazinyoye, L., Thomson, D., & Ntaganira, J. (2016). Social, economic and environmental risk factors for acute lower respiratory infections among children under five years of age in rwanda. Archives of Public Health, 74(1). [CrossRef]
- Haverkos, H., Chung, R., & Perez, L. (2003). Is there an epidemic of hiv/aids among heterosexuals in the usa?. Postgraduate Medical Journal, 79(934), 444-448. [CrossRef]
- He, G., Pan, Y., & Tanaka, T. (2020). The short-term impacts of covid-19 lockdown on urban air pollution in china. Nature Sustainability, 3(12), 1005-1011. [CrossRef]
- He, Z. (2023). Diarrhea as a disease of poverty among under-five children in sub-saharan africa: a cross-sectional study. Inquiry the Journal of Health Care Organization Provision and Financing, 60. [CrossRef]
- Heaney, A., Shaman, J., & Alexander, K. (2019). El niño-southern oscillation and under-5 diarrhea in botswana. Nature Communications, 10(1). [CrossRef]
- Hedt-Gauthier, B., Jeufack, H., Neufeld, N., Alem, A., Sauer, S., Odhiambo, J., … & Volmink, J. (2019). Stuck in the middle: a systematic review of authorship in collaborative health research in africa, 2014–2016. BMJ Global Health, 4(5), e001853. [CrossRef]
- Irabor, D. (2017). Emergence of colorectal cancer in west africa: accepting the inevitable. Nigerian Medical Journal, 58(3), 87. [CrossRef]
- Isaxon, C., Abera, A., Asfaw, A., Bililign, S., Eriksson, A., Malmqvist, E., … & Roba, K. (2022). A call for action: air pollution, a serious health and economic hazard suffocating africa. Clean Air Journal, 32(2). [CrossRef]
- K., V. (2023). Enhancing logistic support during chemotherapy to nonlocal children with cancer and their families through home away from home program. Indian Journal of Medical and Paediatric Oncology, 45(02), 173-175. [CrossRef]
- Karamagi, H., Charif, A., Kidane, S., Yohanes, T., Kariuki, D., Titus, M., … & Droti, B. (2022). Investments for effective functionality of health systems towards universal health coverage in africa: a scoping review. Plos Global Public Health, 2(9), e0001076. [CrossRef]
- Lal, A., Erondu, N., Heymann, D., Gitahi, G., & Yates, R. (2021). Fragmented health systems in covid-19: rectifying the misalignment between global health security and universal health coverage. The Lancet, 397(10268), 61-67. [CrossRef]
- Lauritano, D., Moreo, G., Campanella, V., Vella, F., & Petruzzi, M. (2021). Oral health status among migrants from middle- and low-income countries to europe: a systematic review. International Journal of Environmental Research and Public Health, 18(22), 12203. [CrossRef]
- Lekana-Douki, S. E., Behillil, S., Enouf, V., Leroy, E. M., & Berthet, N. (2018). Detection of human bocavirus-1 in both nasal and stool specimens from children under 5 years old with influenza-like illnesses or diarrhea in Gabon. BMC Research Notes, 11(1). [CrossRef]
- Levine, M., Kotloff, K., Nataro, J., & Muhsen, K. (2012). The global enteric multicenter study (gems): impetus, rationale, and genesis. Clinical Infectious Diseases, 55(suppl 4), S215-S224. [CrossRef]
- Lopez-Carmen, V. (2022). The “elephants in the room” in u.s. global health: indigenous nations and white settler colonialism. Plos Global Public Health, 2(7), e0000719. [CrossRef]
- Maphumulo, W. and Bhengu, B. (2019). Challenges of quality improvement in the healthcare of south africa post-apartheid: a critical review. Curationis, 42(1). [CrossRef]
- Masiira, B., Antara, S., Kazoora, H., Namusisi, O., Gombe, N., Magazani, A., … & Tshimanga, M. (2020). Building a new platform to support public health emergency response in africa: the afenet corps of disease detectives, 2018–2019. BMJ Global Health, 5(10), e002874. [CrossRef]
- McKone, E., Ariti, C., Jackson, A., Zolin, A., Carr, S., Orenti, A., … & Naehrlich, L. (2021). Survival estimates in european cystic fibrosis patients and the impact of socioeconomic factors: a retrospective registry cohort study. European Respiratory Journal, 58(3), 2002288. [CrossRef]
- Moran, A., Forouzanfar, M., Sampson, U., Chugh, S., Feigin, V., & Mensah, G. (2013). The epidemiology of cardiovascular diseases in sub-saharan africa: the global burden of diseases, injuries and risk factors 2010 study. Progress in Cardiovascular Diseases, 56(3), 234-239. [CrossRef]
- Moshammer, H. and Wallner, P. (2011). Air quality as respiratory health indicator — a critical review. International Journal of Occupational Medicine and Environmental Health, 24(3). [CrossRef]
- Mwenda, J., Ntoto, K., Abebe, A., Enweronu-Laryea, C., Ismail, A., Mchomvu, J., … & Steele, A. (2010). Burden and epidemiology of rotavirus diarrhea in selected african countries: preliminary results from the african rotavirus surveillance network. The Journal of Infectious Diseases, 202(S1), S5-S11. [CrossRef]
- Nkumama, I., O’Meara, W., & Osier, F. (2017). Changes in malaria epidemiology in africa and new challenges for elimination. Trends in Parasitology, 33(2), 128-140. [CrossRef]
- Novignon, J., Olakojo, S., & Nonvignon, J. (2012). The effects of public and private health care expenditure on health status in sub-saharan africa: new evidence from panel data analysis. Health Economics Review, 2(1). [CrossRef]
- Ogunbodede, E., Kida, I., Madjapa, H., Amedari, M., Ehizele, A., Mutave, R., … & Okoye, L. (2015). Oral health inequalities between rural and urban populations of the african and middle east region. Advances in Dental Research, 27(1), 18-25. [CrossRef]
- Okeke, I. (2009). Diarrheagenic escherichia coli in sub-saharan africa: status, uncertainties and necessities. The Journal of Infection in Developing Countries, 3(11), 817-842. [CrossRef]
- Pacheco, A., Saraceni, V., Tuboi, S., Lauria, L., Moulton, L., Faulhaber, J., … & Schechter, M. (2011). Estimating the extent of underreporting of mortality among hiv-infected individuals in rio de janeiro, brazil. Aids Research and Human Retroviruses, 27(1), 25-28. [CrossRef]
- Page, A., Hustache, S., Luquero, F., Djibo, A., Manzo, M., & Grais, R. (2011). Health care seeking behavior for diarrhea in children under 5 in rural niger: results of a cross-sectional survey. BMC Public Health, 11(1). [CrossRef]
- Pop, M., Walker, A., Paulson, J., Lindsay, B., Antonio, M., Hossain, M., … & Stine, O. (2014). Diarrhea in young children from low-income countries leads to large-scale alterations in intestinal microbiota composition. Genome Biology, 15(6), R76. [CrossRef]
- Rohner, E., Bütikofer, L., Schmidlin, K., Sengayi, M., Maskew, M., Giddy, J., … & Bohlius, J. (2019). Cervical cancer risk in women living with hiv across four continents: a multicohort study. International Journal of Cancer, 146(3), 601-609. [CrossRef]
- Rojas-López, M., Monterio, R., Pizza, M., Desvaux, M., & Rosini, R. (2018). Intestinal pathogenic escherichia coli: insights for vaccine development. Frontiers in Microbiology, 9. [CrossRef]
- Simo, F., Bigna, J., Kenmoe, S., Ndangang, M., Temfack, E., Moundipa, P., … & Demanou, M. (2019). Dengue virus infection in people residing in africa: a systematic review and meta-analysis of prevalence studies. Scientific Reports, 9(1). [CrossRef]
- Souza, J., Hunt, B., Asirwa, F., Adebamowo, C., & Lopes, G. (2016). Global health equity: cancer care outcome disparities in high-, middle-, and low-income countries. Journal of Clinical Oncology, 34(1), 6-13. [CrossRef]
- Steele, A., Armah, G., Mwenda, J., & Kirkwood, C. (2023). The full impact of rotavirus vaccines in africa has yet to be realized. Clinical Infectious Diseases, 76(Supplement_1), S1-S4. [CrossRef]
- Tafa, B., Gebrewold, L., Mekuria, W., & Assefa, N. (2023). Molecular epidemiology of respiratory syncytial virus in children with acute respiratory illnesses in africa: a systematic review and meta-analysis. Journal of Global Health, 13. [CrossRef]
- Tafere, Y., Abate, B., Enyew, H., & Mekonnen, A. (2020). Diarrheal diseases in under-five children and associated factors among farta district rural community, amhara regional state, north central ethiopia: a comparative cross-sectional study. Journal of Environmental and Public Health, 2020, 1-7. [CrossRef]
- Tamir, T. (2024). Prevalence of childhood stunting and determinants in low and lower-middle income african countries: evidence from standard demographic and health survey. Plos One, 19(4), e0302212. [CrossRef]
- Tareke, A., Enyew, E., & Takele, B. (2022). Pooled prevalence and associated factors of diarrhea among under-five years children in east africa: a multilevel logistic regression analysis. Plos One, 17(4), e0264559. [CrossRef]
- Vanderpuye, V., Hammad, N., Martei, Y., Hopman, W., Fundytus, A., Sullivan, R., … & Booth, C. (2019). Cancer care workforce in africa: perspectives from a global survey. Infectious Agents and Cancer, 14(1). [CrossRef]
- Vasco, G., Trueba, G., Atherton, R., Calvopiña, M., Cevallos, W., Andrade, T., … & Eisenberg, J. (2014). Identifying etiological agents causing diarrhea in low income ecuadorian communities. American Journal of Tropical Medicine and Hygiene, 91(3), 563-569. [CrossRef]
- Vlismas, K., Stavrinos, V., & Panagiotakos, D. (2009). Socio-economic status, dietary habits and health-related outcomes in various parts of the world: a review. Central European Journal of Public Health, 17(2), 55-63. [CrossRef]
- Wong, E., Choy, R., Zhang, Y., Chu, W., Chen, L., Pang, C., … & Yam, J. (2022). Global retinoblastoma survival and globe preservation: a systematic review and meta-analysis of associations with socioeconomic and health-care factors. The Lancet Global Health, 10(3), e380-e389. [CrossRef]
- Yaya, S., Hudani, A., Udenigwe, O., Shah, V., Ekholuenetale, M., & Bishwajit, G. (2018). Improving water, sanitation and hygiene practices, and housing quality to prevent diarrhea among under-five children in nigeria. Tropical Medicine and Infectious Disease, 3(2), 41. [CrossRef]
- Yuyun, M., Sliwa, K., Kengne, A., Mocumbi, A., & Bukhman, G. (2020). Cardiovascular diseases in sub-saharan africa compared to high-income countries: an epidemiological perspective. Global Heart, 15(1), 15. [CrossRef]
- Boschi-Pinto, C. (2008). Estimating child mortality due to diarrhoea in developing countries. Bulletin of the World Health Organization, 86(9), 710–717. [CrossRef]
- Braveman, P., & Gottlieb, L. (2014). The social determinants of health: It’s time to consider the causes of the causes. Public Health Reports, 129(1_suppl2), 19–31. [CrossRef]
- Denkyira, S. A., Adesola, R. O., Idris, I., Yelarge, K., Asaaseasa, K. T., Danquah, C. A., & Opuni, E. (2022). Marburg virus in Ghana: A public health threat to Ghanaians and to Africans. Public Health Challenges, 1(4). [CrossRef]
- Dhefer, I. H. (2021). Liver damage during infections with coronavirus. Journal of Techniques, 3(2), 79–85. [CrossRef]
- Ferkol, T., & Schraufnagel, D. (2014). The global burden of respiratory disease. Annals of the American Thoracic Society, 11(3), 404–406. [CrossRef]
- Gelband, H., Bogoch, I. I., Rodriguez, P. S., Ngai, M., Peer, N., Watson, L. K., & Jha, P. (2020). Is Malaria an Important Cause of Death among Adults? ˜the œAmerican Journal of Tropical Medicine and Hygiene, 103(1), 41–47. [CrossRef]
- Groves, H. E., Piché-Renaud, P., Peci, A., Farrar, D. S., Buckrell, S., Bancej, C., Sevenhuysen, C., Campigotto, A., Gubbay, J. B., & Morris, S. K. (2021). The impact of the COVID-19 pandemic on influenza, respiratory syncytial virus, and other seasonal respiratory virus circulation in Canada: A population-based study. ˜the œLancet Regional Health. Americas, 1, 100015. [CrossRef]
- Gussow, A. B., Auslander, N., Faure, G., Wolf, Y. I., Zhang, F., & Koonin, E. V. (2020). Genomic determinants of pathogenicity in SARS-CoV-2 and other human coronaviruses. Proceedings of the National Academy of Sciences of the United States of America, 117(26), 15193–15199. [CrossRef]
- Ha, L. T. (2022). Effects of digitalization on financialization: Empirical evidence from European countries. Technology in Society, 68, 101851. [CrossRef]
- Hamdi, Y., Zass, L., Othman, H., Radouani, F., Allali, I., Hanachi, M., Okeke, C. J., Chaouch, M., Tendwa, M. B., Samtal, C., Sallam, R. M., Alsayed, N., Turkson, M., Ahmed, S., Benkahla, A., Romdhane, L., Souiai, O., Bishop, Ö. T., Ghedira, K.,... Kassim, S. K. (2021). Human OMICs and Computational Biology research in Africa: Current challenges and prospects. Omics, 25(4), 213–233. [CrossRef]
- Jaddaoui, I. E., Allali, I., Sehli, S., Ouldim, K., Hamdi, S., Idrissi, N. A., Nejjari, C., Amzazi, S., Bakri, Y., & Ghazal, H. (2020). Cancer omics in Africa: present and prospects. Frontiers in Oncology, 10. [CrossRef]
- Lukamba, R. M., Yao, J. A., Kabesha, T. A., Budiongo, A. N., Monga, B. B., Mwembo, A. T., Bey, P., Chenge, G. B., Desjardins, L., Luboya, O. N., Doz, F., & Stefan, C. D. (2018). Retinoblastoma in Sub-Saharan Africa: Case Studies of the Republic of Côte d’Ivoire and the Democratic Republic of the Congo. Journal of Global Oncology, 4, 1–8. [CrossRef]
- Lukšić, I., Mulić, R., Falconer, R., Orban, M., Sidhu, S., & Rudan, I. (2013). Estimating global and regional morbidity from acute bacterial meningitis in children: assessment of the evidence. Croatian Medical Journal, 54(6), 510–518. [CrossRef]
- Oduoye, M. O., Fatima, E., Muzammil, M. A., Dave, T., Irfan, H., Fariha, F. N. U., Marbell, A., Ubechu, S. C., Scott, G. Y., & Elebesunu, E. E. (2024). Impacts of the advancement in artificial intelligence on laboratory medicine in low- and middle-income countries: Challenges and recommendations—A literature review. Health Science Reports, 7(1). [CrossRef]
- Pennington, B. F., McGrath, L. M., & Peterson, R. L. (2020). Diagnosing Learning Disorders, third edition: From Science to Practice. Guilford Publications.
- Pillay, J. (2022). Difficulties experienced by South African adolescents during COVID-19 lockdown: implications for early mental health interventions. South African Journal of Psychology, 53(2), 211–224. [CrossRef]
- Verhein, K. C., Vellers, H. L., & Kleeberger, S. R. (2018). Inter-individual variation in health and disease associated with pulmonary infectious agents. Mammalian Genome, 29(1–2), 38–47. [CrossRef]
- He, X., Lau, E. H. Y., Wu, P., Deng, X., Wang, J., Hao, X., Lau, Y. C., Wong, J. Y., Guan, Y., Tan, X., Mo, X., Chen, Y., Liao, B., Chen, W., Hu, F., Zhang, Q., Zhong, M., Wu, Y., Zhao, L.,... Leung, G. M. (2020). Temporal dynamics in viral shedding and transmissibility of COVID-19. Nature Medicine, 26(5), 672–675. [CrossRef]
Figure 1.
Disparities in Health Outcomes by Cause and Income Group: Insights from European (A) and African (B) Countries.
Figure 1.
Disparities in Health Outcomes by Cause and Income Group: Insights from European (A) and African (B) Countries.
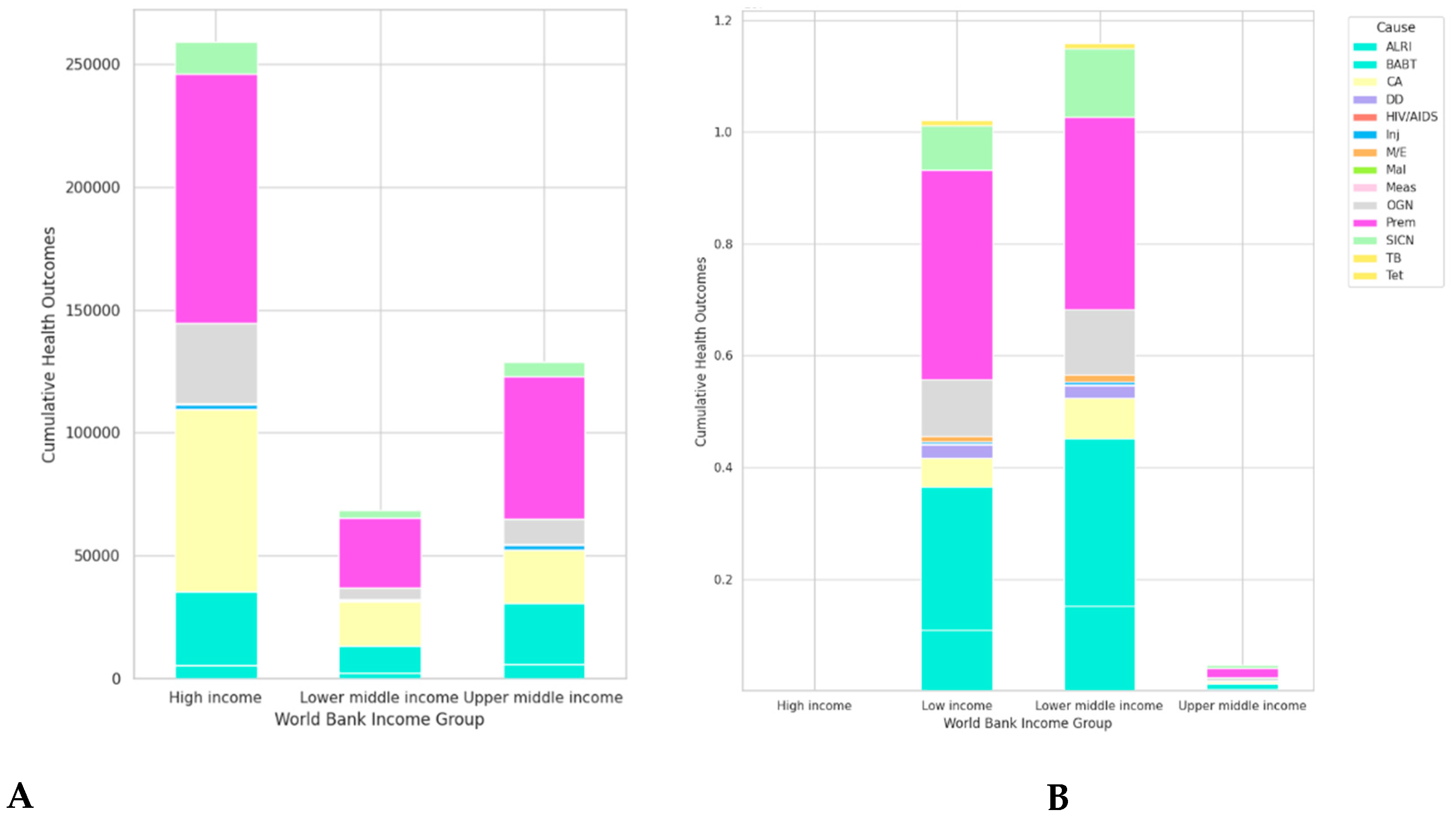
Figure 2.
Age-specific Health Conditions in African and European Countries.
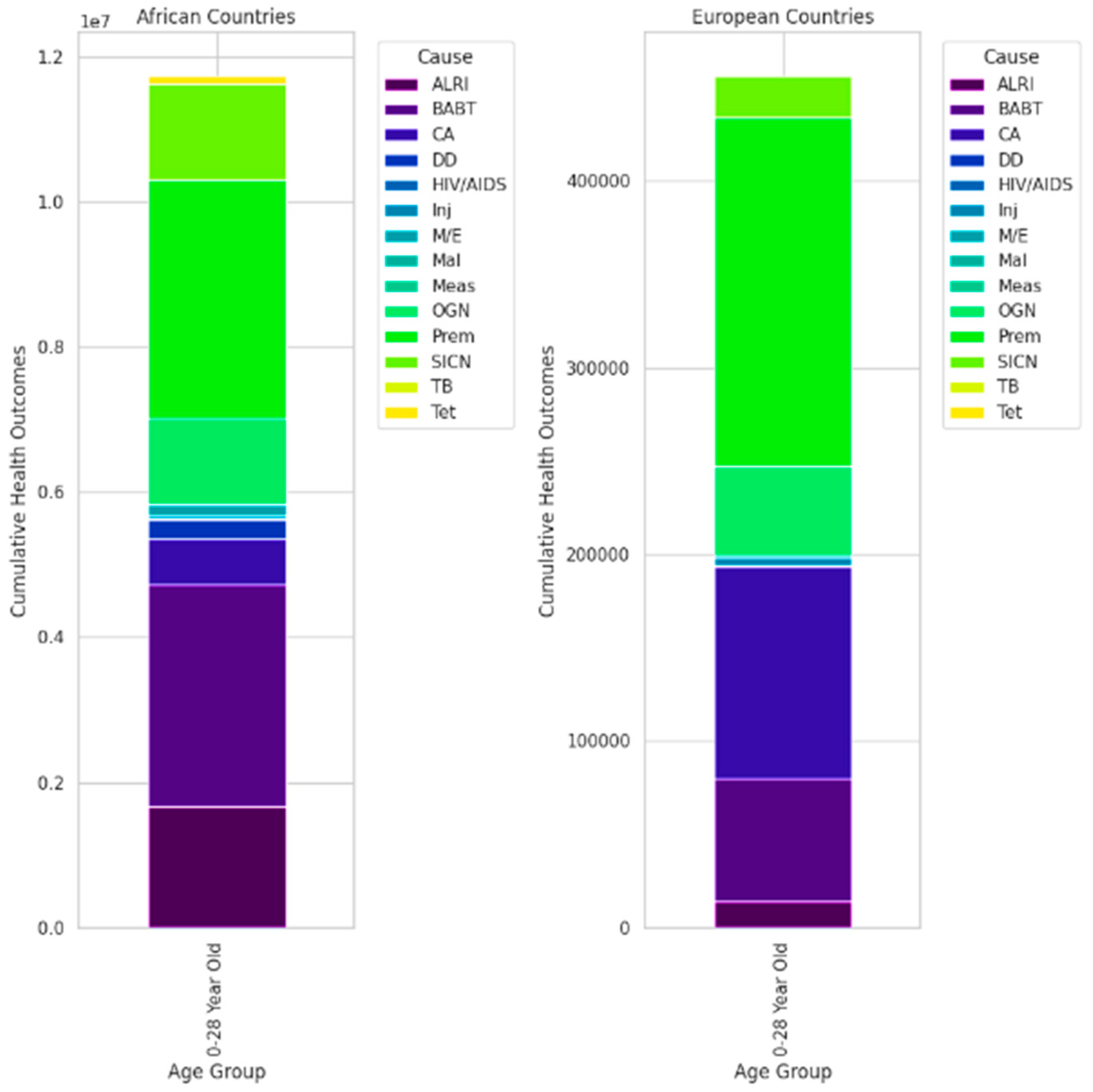
Figure 3.
Comparative Disease Trends between Europe (A) vs. Africa (B) countries.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



