
Submitted:
16 September 2024
Posted:
18 September 2024
You are already at the latest version
Abstract
Peri-implant infective diseases seem to be the most common cause for the late dental implant failure. Therefore, peri-implant microbiota has been intensively studied in modern implantology. Many studies showed a presence of extremely varied microflora in cases of peri-implant infective diseases. The main scope of this observational single-blind study was to analyze the presence of some microbial species in a group of patients with clinical signs of peri-implant mucositis compared to two other groups (patients treated with dental implants but without any clinical signs of peri-implant inflammation and patients treated with no dental implants). The identification of microorganisms was followed by an antibiogram in order to find their sensitivity to various antibiotics. The results showed a microbiota not necessarily specific for each situation (peri-implant infective diseases, healthy tissues around dental implants and healthy natural teeth and gums) with species like Candida albicans, Neisseria mucosa, Prevotella, Staphylococcus aureus, Streptococcus and others. Peri-implant infective diseases presented more bacterial species than other conditions.
Keywords:
peri-implant infective diseases
; microbiota
; antibiogram
1. Introduction
The dental implant treatment currently has a high rate of success, but sometimes it fails. Lack of primary stability, infection or surgical trauma appear to be the most common causes of early implant failure [1]. The position of implants and smoking history are also part of it [2]. Peri-implantitis seems to be the most frequent factor involved in the late failure [1], while common risk factors are rather the patient history, posterior implant location and decisions made by the clinician [3]. The 10-years survival rate of dental implants varies between 95.2% and 97.5% [4] with a mean value of 95.5% [5], while the 2 to 9 years survival rate is reported as 97,4% [6]. However, the factors associated with late implant failure are known but not fully understood and they are generally considered to be related to peri-implant microbial environment, host tissues features and many others [7,8,9]. For a high rate of success in these cases, a more accurate knowledge about dental implant treatment failures is needed [10]. Many studies showed that peri-implant infective diseases (PIIDs) are very similar to gingivitis or periodontitis (e.g. Fusobacterium and Prevotella [11], or Porphiromonas gingivalis, Treponema denticola and Tannerella forsythia [12]) having common risk factors [13], but also having significant differences compared to periodontal diseases [14]. Some authors found an imbalance between oral microflora dysbiosis and deregulation of the immune system in cases of peri-implantitis [15].
The aim of our study is to analyze the presence of certain bacterial species in a group of patients with clinical signs of peri-implant mucositis (PIM) compared to two other groups, one with patients treated with dental implants but who did not present any clinical signs of peri-implant inflammation and one consisting of patients with no dental implant treatment. The identification of microorganisms was followed by the antibiogram in order to observe their sensitivity to various antibiotics.
The present study leads to the idea that peri-implant microbiota is very complex in case of PIM, but also around the implants without any clinical signs of peri-implant inflammation. It is recommended for dentists to deal with cases of PIIDs by requesting a laboratory bacterial identification followed by an antibiogram in order to offer the most effective treatment, individualized and more focused on each patient.
2. Materials and Methods
This study is analytical and observational.
2.1. Selection of Patients and Creating the Study Groups:
The study was conducted on a group of 15 patients from 2 cities in Romania: Bucharest and Râmnicu Vâlcea. After they signed the informed consent form and learned about the procedures to be followed, the patients were divided into 3 groups, 5 each. The first 10 patients (from group 1 and 2) were selected from a larger base group who had been enrolled in a previous study, consisting of 62 patients with dental implants. All these 62 patients were clinically checked-up for peri-implant mucositis (PIM) or periimplantitis clinical signs.
All the patients were asked about the pain and bleeding in the area of implants.
One examiner was trained and calibrated (k = 0.81) before the study in order to perform the clinical check-ups of all 62 patients and avoid any clinical record bias. The clinical check-up recorded the following data: gingival or peri-implant mucosa color modifications, gingival or mucosa swelling, bleeding on probing, depth of probing.
The probing was performed with a CP 15 periodontal probe, after careful air dry of the mucosal / gingival margin. The probing was also performed in 6 points for each tooth or implant as it follows: central buccal, central oral, mesial-buccal, distal-buccal, mesial-oral and distal-oral, the last four points of probing being directed towards the papilla. Bleeding or no bleeding was recorded for each of the 6 probing points.
We assigned score values to assess the peri-implant mucosal or dental gingival health status as it follows (according to the Silness-Loe gingival index (GI) [16]:
- 0.
- - healthy peri-implant mucosa / dental gingiva. No color modification, no swelling, no bleeding on probing;
- 1.
- - reduced peri-implant mucosal / dental gingival inflammation. Reduced color modification and/or swelling, no bleeding on probing;
- 2.
- - mild peri-implant mucosal / dental gingival inflammation. Obvious color modification and/or swelling, bleeding on probing;
- 3.
- - severe peri-implant mucosal / dental gingival inflammation. Obvious color modification and/or swelling, spontaneous bleeding or bleeding on air dry.
We excluded from the present study the patients with the score value of 3 because of the uncertainty of diagnosis between peri-implant mucositis vs. periimplantitis.
The depth of probing for each probing point was compared with the bone level for each implant or tooth as it could be measured on the X-ray. Patients with an implant probing depth going deeper than the measured bone level were considered to suffer from peri-implantitis and were excluded from the present study.
In the first group were included patients with implant-supported prosthesis with clinical signs of PIM which persisted after efficient oral hygiene procedures were performed in the previous study. These hygiene procedures included professional oral hygiene with scaling and Perio-flow and the following instructions for patients: rigorous brushing at the inflammation site with soft brushes, interdental cleaning 2 times per day with dental floss, super floss or interdental brushes, use of anti-microbial mouth wash with or without an oral irrigator and local application of chlorhexidine gel.
The second group had patients with implant-supported prosthesis (such as individual crowns, bridges or overdentures) but with no clinical signs of PIM.
In the third group were included patients with individual dental crowns, without any dental implant treatment.
One selection criterion for all the patients involved in the study was for them to have natural teeth (without any prosthesis) as well.
2.2. Selection of Peri-Implant/Periodontal Sites
2 sites for each patient were chosen to collect dental plaque or peri-implant sulcus/gingival crevicular fluid.
The first samples in the first two groups were collected from the peri-implant sulcus while in the third group was taken from the gingival sulcus of teeth with dental crowns.
The second sample was collected from gingival sulcus of natural teeth without any crown from all 15 patients included in the study. The second harvesting site for each patient was located at distance from the first harvesting site – on the opposite side of the same arch or on the opposite arch. When it was possible we tried to use for the second sample the same tooth from the same arch, but in the other side (e.g. first harvesting site 25, and second harvesting site 15).
2.3. Workflow procedure:
First, we informed the patients about the sample collecting and processing procedures and asked them to sign the informed consent form. The patients were requested to avoid any oral hygiene procedures (including toothbrushing, interdental cleaning, using mouth wash, oral irrigators or chewing gum) or taking any antibiotics for 24 hours before the collection procedure. The sample collecting procedure was performed by one examiner, using sterile paper cones inserted into the peri-implant or gingival sulcus (Figure 1 and Figure 2). We did not use any antimicrobial substances before samples collection. After the collection procedure, the paper cones were placed into sterile containers (Figure 3) and send to the laboratory for the microbiological culture procedures. The sample collecting and processing procedures followed the next guidelines:
- - in cases of PIM, we collected from sites that were most likely to be the starting point of peri-implant infection, where the scores for assessing the peri-implant mucosal or dental gingival health were higher;
- - the paper cones were inserted into the gingival / mucosal sulcus as deep as possible, without generating pain or discomfort for the patient and removed after approximatively 5 second in order to have enough time to collect bacteria and crevicular fluid;
- - we always tried to collect a sufficient amount of fluid; the paper cones had to be obviously wet on the whole depth of insertion before removing and being further processed;
- - every container received a label with the patient and site numbers (e.g. “patient no. 3, site no. 1”); the study was simple-blind – so, the laboratory technician did not receive any information about the patient or about the origin of the sample (implants, dental crowns or natural teeth);
- - the external surface of the containers was disinfected after they have been used and introduced in single use plastic bags; then, they were stored in safe, clean place until were picked up for sending to the laboratory;
- - the transport took place in the same day of collecting;
- - we used specific procedures for the transport of microbiological samples; also, the transports were processed as fast as possible in order to prevent the samples degradation;
- - each sample received a unique serial number;
- - the laboratory staff established the correct procedure for sowing, cultivating and analyzing the samples;
- - an antibiogram was performed for each of the 30 bacterial cultures.
2.4. Statistical Analysis
The data were entered into a computer using a SPSS processor (v. 24 – IBM, USA). First, we used chi-square tests for categorical values but because of low number of cases the tests were invalid (more than 20% cells were expected count less than 5). After, we used the Fisher’s Exact Test for testing the differences between groups.
The scheme of entire protocol is shown in Figure 4.
3. Results
9 women and 6 men, aged between 22 and 63 years were involved in this study. Patients from groups 1 and 2 had between 1 and 6 dental implants. One patient had a removable dental prosthesis, the rest of 9 having dental crowns or bridges.
After the laboratory processing, we received the analysis reports. The microbiological data are shown in Table 1.
Candida albicans (p = 0.05) and group C streptococcus (p = 0.06) were found more often in groups with no inflammation (2 and 3). Also, we discovered group C streptococcus more frequent in women in second samples collected from healthy gingiva of all groups (p = 0.14).
The antibiogram for Neisseria, Staphylococci and Streptococci was performed with the following antibiotics: oxacillin, vancomycin, penicillin, cefixime, amikacin, trimethoprim/sulfamethoxazole, amoxicillin/clavulanic acid, moxifloxacin, azithromycin, ofloxacin, gentamicin, ampicillin, ampicillin/sulbactam, clarithromycin, erythromycin, cefadroxil, fosfomycin following common protocols [17,18,19].
The results for antibiogram were as it follows: Staphylococci generally showed resistance to oxacillin, penicillin and ampicillin and in particular to moxifloxacin (one case) and intermediate resistance to clarithromycin and gentamicin (one case). Streptococci have been shown to be sensitive to all antibiotics. Neisseria showed resistance to penicillin, ampicillin and ofloxacin and to moxifloxacin (one case).
The antibiogram for Prevotella and Veillonella was performed with penicillin, ampicillin and erythromycin and also with chloramphenicol, clindamycin, cefoxitin and metronidazole [21]. The isolated species showed resistance to penicillin, ampicillin and erythromycin, except for one case for erythromycin.
The fungigram for Candida was performed with miconazole, amphotericin B, ketoconazole, itraconazole, voriconazole, fluconazole and econazole [22]. With two exceptions, the isolated species showed resistance to amphotericin B and sensitivity to the rest.
All patients who presented peri-implant mucositis (PIM) or periodontal diseases reported no pain or discomfort in the affected areas. Also, none of the patients who presented these conditions was concerned about the presence of occasional gingival / mucosal bleeding, when it appeared, and did not feel the need to present to a dental office for professional care.
4. Discussion
The use of dental implants to replace missing teeth has become a first-choice-norm in oral rehabilitation these days. Although implants have shown predictable and effective results, the increased usage of implants in dental treatments is also related with an increasing number of implant failures, the most common cause being peri-implantitis. Peri-implantitis is a chronic progressive destructive disease which has bacterial or mechanical origin and affects the soft and hard tissues surrounding dental implant and usually begins with an infection and inflammation of the peri-implant mucosa, namely PIM [23].
The results presented above report the presence of certain bacterial species in the peri-implant microbiota present in dental implants with and without PIM and in natural teeth treated with dental crowns, compared to the microbiota present in natural teeth in the same group of patients.
The prevalence of PIIDs, at the implant level varies between 6.5%-47%. The prevalence of PIIDs at the patient level varies between 18.8%-47%. These two statistical values are different in most studies because one patient with PIID may be treated with only one dental implant while another patient with PIID may be treated with two or more dental implants and does not necessarily present PIID to all the implants [23].
Dental plaque and some bacteria in particular have been largely identified as the primary etiological factors. There are also a series of risk factors which have been related to peri-implant diseases such as trauma, local factors (e.g. local anatomical factors, parafunctions), general factors (e.g. age, genetics, medical conditions, etc.), behavioral factors (e.g. maintaining oral hygiene, patient follow-up [23].
When analyzing the effects of systemic diseases on peri-implant tissues, diabetes was the most frequently associated risk factor. Patients with uncontrolled diabetes have been shown to be at higher risk of peri-implant infections compared with controlled diabetes and healthy patients [23].
Analyzing the evidence on the microbiological component of peri-implant infections, various and conflicting results are reported. So, some microorganisms are more prevalent: Porphyromonas gingivalis (PG), Prevotella intermedia, Treponema denticola (TD), Tannerella forsythia and Staphylococcus [23].
In the case of PIIDs, most studies indicate a non-specific flora, gram-negative and anaerobic species being most usually found [23]. Therefore, it was difficult for us to choose a reasonable number of microbial species and check their presence in every site. After we studied and identified a large group of microorganisms with peri-implant pathogenic potential, we chose to look for a number of 9 bacteria species, namely Staphylococcus, Streptococcus, Candida, Neisseria, Bacteroides, Porphyromonas, Prevotella, Veillonella and Fusobacterium, the last six being gram-negative and anaerobic.
The composition of the submucosal microbiota associated with peri-implant infective diseases (PIIDs) and periodontitis appear to be similar, such as Prevotella nigrescens, Fusobacterium, Campylobacter rectus and Aggregatibacter actinomycetemcomitans, as well as Staphylococcus aureus, Enteric bacilli, and Candida albicans [11,24,25].
The variations of the soft and hard tissues (clinically defined as an increase in pocket depth and bone loss) seem to be related to important changes in the composition of the subgingival / submucosal microbiota, [26]: a greater total bacterial load leads to an increased number of species such as Aggregatibacter actinomycetemcomitans, Fusobacterium, Prevotella intermedia and Porphyromonas gingivalis, a decrease in the percentage of all cocci, and an important proportion of motile organisms and spirochetes [25]. Staphylococcus aureus seems to play an important role in the development of a PIIDs [27]. This bacteria shows a high affinity to titanium and has a high negative (90%) predictive value, according to the results of Salvi et al. [28].
The bacterial species of sub-mucosal plaque seems to be different in case of PIIDs lesions in patients with natural teeth compared to fully edentulous patients. Plaque samples of partially edentulous patients presented a greater number of gram-negative anaerobic bacterial species when compared to the plaque collected from fully edentulous patients [29]. Results from the various studies have revealed that pathogenic microorganisms such as Aggregatibacter actinomycetemcomitans, Porphyromonas gingivalis, Tannerella forsythia, and Treponema denticola are often present in the peri-implant sulcus of partially edentulous patients, but these microorganisms were not usually detected in edentulous patients [30].
The microbiological analysis identified 11 species of microorganisms (see Table 1). The microbiological analysis did not identify Bacteroides, Porphyromonas and Fusobacterium species in any samples.
In this study we identified a number of microbial species from the gingival sulcus of a number of patients treated with or without dental implants, with or without crowns, affected or not by periodontitis. We also identified more microorganisms in the peri-implant sites and around teeth affected by periodontitis than in healthy sites, but there was no microbial specificity related to any type of pathology. These findings are similar to other studies. Charalampakis et al., for example concluded that microbiological data do not always correspond to the severity of the PIIDs, but they can show that peri-implantitis is nothing but a multi-microbial condition with an increased number of aerobic gram-negative bacilli in about 18,6% of cases. The microbiological testing in the case of PIIDs must be improved in order to find out what the microbiological profile actually is [31].
On the other hand, Pye et al. concluded that the main microorganisms involved in the etiology and progression of PIIDs are cocci and gram-negative anaerobic bacilli such as Porphyromonas gingivalis, Prevotella intermedia, Veillonella, spirochetes, including also Treponema denticola. The authors also believe that the involvement of Staphylococcus aureus, Candida and coliform bacteria in this pathology is questionable and it should be taken seriously [32]. Other authors detected in cases of PIIDs a microbiota very similar to that involved in periodontitis [13].
Kumar et al. associated less PIIDs to Prevotella and Leptotrichia and more with species like Actinomyces, Peptococcus, Campylobacter, Streptococci non-mutans and Butyrivibrio. They also found lower levels of species in peri-implantitis compared to periodontitis, such as Prevotella, non-mutans Streptococci, Lactobacilli, Selenomonas, Leptotrichia and Actinomyces and higher levels of Peptococci, Mycoplasma, Eubacterium, Campylobacter, Butyrivibrio, S. mutans and Treponema. PIIDs microbiota is less complex than one from periodontitis [33].
There is no consensus in the scientific community about microbiota associated with PIIDs. However, it seems that the type of surface of dental implants does not change the microbiota in the PIIDs [34,35].
A clear correlation between the highly pathogenic microbiota, bleeding score and peri-implant pockets depth must be made. This leads to the need of more studies development focused on biofilm control [36].
Our study showed that the microorganisms detected in the sampling sites have sensitivity to different antibiotics. However, considering the variety of species we found, the local application of just a single antibiotic cannot be efficient. For this reason, there are still no standards accepted for antibiotics protocols in case of peri-implantitis [32,37].
Anaerobic microorganisms usually showed an increased resistance to antibiotics over time [38]. A specific study which included more than 70 patients with PIIDs found that microorganisms are resistant to one or more antibiotics [39]. Minocycline and doxycycline seem to be efficient in local applications in the case of moderate peri-implantitis. At this moment there are no arguments for systemic administration of antibiotics in PIIDs [40].
Therefore, scientifically based clinical studies including local usage of antibiotics in case of PIIDs treatment are needed in the future.
The lack of pain and discomfort at the level of peri-implant mucous membranes affected by infection and inflammation is a factor with an unfavorable prognosis, as the absence of disturbing symptomatology leads patients suffering from this condition to consider that the peri-implant health status is good and the early stages of PIIDs can go unnoticed if they neglect the mandatory treatment follow-up. Therefore, when the patient is undergoing a treatment with dental implants, it seems mandatory that the professionals performing these treatments insist, repeatedly, at each appointment, on the need for a rigorous control of the oral biofilm and regular follow-up controls, regardless of the presence or absence of any type of symptomatology at the level of dental implants
The major limit of our study was that we had a low number of cases. However, the complexity and the costs related to this research were high and made us to proceed in this way.
5. Conclusions
The present research showed that peri-implant microbiota is complex in the first stage of PIIDs, but also around implants without any clinical sign of peri-implant inflammation.
Most studies did find gram-negative anaerobic microorganisms in PIIDs, but also there are others that did not. Also, many authors reported different results about the similarity between the microbiota in periodontitis and PIIDs. Consequently, there is no consensus about a single pattern of microbiota in case of PIIDs. Moreover, there is no standard protocol for topical usage of antibiotics in PIIDs and also more research is needed. There are also no arguments for the oral administration of antibiotics for PIIDs. Therefore, it can be recommended for the dentist to request a microbiological laboratory exam followed by an antibiogram prior to clinical treatment for a better personalized approach in case of PIIDs. Some correlations between highly pathogenic microorganisms and the clinical signs of PIIDs were made, which leads to the need for more studies focused on peri-implant biofilm control.
Author Contributions
A.T.Ț. was the primary investigator; he took part at the conceptualization, methodology and validation procedures and on writing—original draft preparation; C.F. – supervision and writing—review and editing; O.S. – visualization; C.T.P. – supervision.
Funding
Publication of this paper was supported by the University of Medicine and Pharmacy Carol Davila through the institutional program “Publish not Perish”.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee for the approval of clinical studies within the CMI (Individual Medical Office) DR. ȚANDĂRĂ CORINA MIHAELA by decision no. 01 / 8.02.2024.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
The authors want to give special thanks to all of the administrative and technical stuff involved in this study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Sakka S, Baroudi K, Nassani MZ. Factors associated with early and late failure of dental implants. J Investig Clin Dent. 2012 Nov;3(4):258-61. [CrossRef]
- Basson AA, Mann J, Findler M, Chodick G. Correlates of Early Dental Implant Failure: A Retrospective Study. Int J Oral Maxillofac Implants 2023 Oct 17;38(5):897-906. [CrossRef]
- Do TA, Le HS, Shen YW, Huang HL, Fuh LJ. Risk Factors related to Late Failure of Dental Implant-A Systematic Review of Recent Studies. Int J Environ Res Public Health. 2020 Jun 2;17(11):3931. [CrossRef] [PubMed] [PubMed Central]
- Howe MS, Keys W, Richards D. Long-term (10-year) dental implant survival: A systematic review and sensitivity meta-analysis. J Dent. 2019 May:84:9-21. [CrossRef]
- Wittneben JG, Buser D, Salvi GE, Bürgin W, Hicklin S, Brägger U. Complication and failure rates with implant-supported fixed dental prostheses and single crowns: a 10-year retrospective study. Clin Implant Dent Relat Res. 2014 Jun;16(3):356-64. [CrossRef]
- Wang Y, Fan Y, Lin Z, Song Z, Shu R, Xie Y. Survival rate and potential risk indicators of implant loss in non-smokers and systemically healthy periodontitis patients: An up to 9-year retrospective study. J Periodontal Res. 2021 Jun;56(3):547-557. [CrossRef] [PubMed]
- Jemt, T. Jemt T. A retro-prospective effectiveness study on 3448 implant operations at one referral clinic: A multifactorial analysis. Part II: Clinical factors associated to peri-implantitis surgery and late implant failures. Clin Implant Dent Relat Res. 2017 Dec;19(6):972-979. [CrossRef] [PubMed]
- Staedt H, Rossa M, Lehmann KM, Al-Nawas B, Kämmerer PW, Heimes D. Potential risk factors for early and late dental implant failure: a retrospective clinical study on 9080 implants. Int J Implant Dent. 2020 Nov 30;6(1):81. [CrossRef] [PubMed] [PubMed Central]
- Takamoli J, Pascual A, Martinez-Amargant J, Garcia-Mur B, Nart J, Valles C. Implant failure and associated risk indicators: A retrospective study. Clin Oral Implants Res. 2021 May;32(5):619-628. [CrossRef] [PubMed]
- Marcantonio C, Nicoli LG, Marcantonio Junior E, Zandim-Barcelos DL. Prevalence and Possible Risk Factors of Peri-implantitis: A Concept Review. J Contemp Dent Pract. 2015 Sep 1;16(9):750-7. [CrossRef] [PubMed]
- Zhou N, Huang H, Liu H, Li Q, Yang G, Zhang Y, Ding M, Dong H, Mou Y. Microbiota analysis of peri-implant mucositis in patients with periodontitis history. Clin Oral Investig. 2022 Oct;26(10):6223-6233. [CrossRef] [PubMed] [PubMed Central]
- Alves CH, Russi KL, Rocha NC, Bastos F, Darrieux M, Parisotto TM, Girardello R. Host-microbiome interactions regarding peri-implantitis and dental implant loss. J Transl Med. 2022 Sep 23;20(1):425. [CrossRef] [PubMed] [PubMed Central]
- Sato J, Gomi K, Makino T, Kawasaki F, Yashima A, Ozawa T, Maeda N, Arai T. The evaluation of bacterial flora in progress of peri-implant disease. Aust Dent J. 2011 Jun;56(2):201-6. [CrossRef]
- Pokrowiecki R, Mielczarek A, Zaręba T, Tyski S. Oral microbiome and peri-implant diseases: where are we now? Ther Clin Risk Manag. 2017 Nov 29:13:1529-1542. eCollection 2017. [CrossRef]
- Rahnama-Hezavah M, Mertowska P, Mertowski S, Skiba J, Krawiec K, Łobacz M, Grywalska E. How Can Imbalance in Oral Microbiota and Immune Response Lead to Dental Implant Problems? Int J Mol Sci. 2023 Dec 18;24(24):17620. [CrossRef] [PubMed] [PubMed Central]
- Cuculescu, M. Indici utilizați în medicina dentară. In Prevenție primară în carie și parodontopatii. Publisher: Editura didactică și pedagogică R.A. Bucharest, Romania, 2010, pp. 96-97.
- Rostamian M, Chegene Lorestani R, Jafari S, Mansouri R, Rezaeian S, Ghadiri K, Akya A. A systematic review and meta-analysis on the antibiotic resistance of Neisseria meningitidis in the last 20 years in the world. Indian J Med Microbiol. 2022 Jul-Sep;40(3):323-329. [CrossRef] [PubMed]
- Lee Y, Kim CK, Kim M, Yong D, Lee K, Chong Y. Detection of mecA in strains with oxacillin and cefoxitin disk tests for detection of methicillin-resistant Staphylococcus. Korean J Lab Med. 2007 Aug;27(4):276-80. Korean. [CrossRef] [PubMed]
- Keleş E, Aral M, Alpay HC. Antibiotic sensitivities of Streptococcus pneumoniae, viridans streptococci, and group A hemolytic streptococci isolated from the maxillary and ethmoid sinuses. Kulak Burun Bogaz Ihtis Derg. 2006;16(1):18-24. [PubMed]
- Lakhssassi N, Elhajoui N, Lodter JP, Pineill JL, Sixou M. Antimicrobial susceptibility variation of 50 anaerobic periopathogens in aggressive periodontitis: an interindividual variability study. Oral Microbiol Immunol. 2005 Aug;20(4):244-52. [CrossRef] [PubMed]
- Li J, Wang H, Li N, Zhang Y, Lü X, Liu B. Antibiotic susceptibility and biofilm-forming ability of Veillonella strains. Anaerobe. 2022 Dec;78:102667. [CrossRef] [PubMed]
- Mareş M, Mareş M, Rusu M. Antifungal susceptibility of 95 yeast strains isolated from oral mycoses in HIV-negative and HIV-positive patients. Bacteriol Virusol Parazitol Epidemiol. 2008 Jan-Mar;53(1):41-2. [PubMed]
- Umar M, Jananni M, Saravana Kumar R, Pratebha B, Peri implantitis - A narrative review. IP Int J Periodontol Implantol 2021;6(4):204-211.
- Ata-Ali J, Candel-Marti ME, Flichy-Fernández AJ, Peñarrocha-Oltra D, Balaguer-Martinez JF, Peñarrocha Diago M. Peri-implantitis: associated microbiota and treatment. Med Oral Patol Oral Cir Bucal. 2011 Nov 1;16(7):e937-43. [CrossRef]
- Berglundh T, Zitzmann NU, Donati M. Are peri-implantitis lesions different from periodontitis lesions? J Clin Periodontol 2011; 38(Suppl. 11): 188-202. [CrossRef]
- Quirynen M, De Soete M, van Steenberghe D. Infectious risks for oral implants: A review of the literature. Clin Oral Implants Res 2002; 13(1): 1-19. [CrossRef]
- Cai Z, Li Y, Wang Y, Chen S, Jiang S, Ge H, Lei L, Huang X. Antimicrobial effects of photodynamic therapy with antiseptics on Staphylococcus aureus biofilm on titanium surface. Photodiagnosis Photodyn Ther. 2019 Mar;25:382-388. [CrossRef] [PubMed]
- Salvi GE, Fürst MM, Lang NP, Persson GR. One-year bacterial colonization patterns of Staphylococcus aureus and other bacteria at implants and adjacent teeth. Clin Oral Implants Res 2008; 19(3): 242-8. [CrossRef]
- Apse P, Ellen RP, Overall CM, Zarb GA. Microbiota and crevicular fluid collagenase activity in the osseointegrated dental implant sulcus: A comparison of sites in edentulous and partially edentulous patients. J Periodontal Res 1989; 24(2): 96-105. [CrossRef]
- Kocar M, Seme K, Hren NI. Characterization of the normal bacterial flora in peri-implant sulci of partially and completely edentulous patients. Int J Oral Maxillofac Implants 2010; 25(4): 690-8.
- Charalampakis G, Leonhardt Å, Rabe P, Dahlén G. Clinical and microbiological characteristics of peri-implantitis cases: a retrospective multicentre study. Clin Oral Implants Res. 2012 Sep;23(9):1045-54. [CrossRef]
- Tambone E, Marchetti A, Ceresa C, Piccoli F, Anesi A, Nollo G, Caola I, Bosetti M, Fracchia L, Ghensi P, Tessarolo F. Counter-Acting Candida albicans-Staphylococcus aureus Mixed Biofilm on Titanium Implants Using Microbial Biosurfactants. Polymers (Basel). 2021 Jul 23;13(15):2420. [CrossRef] [PubMed] [PubMed Central]
- Kumar PS, Mason MR, Brooker MR, O’Brien K. Pyrosequencing reveals unique microbial signatures associated with healthy and failing dental implants. J Clin Periodontol. 2012 May;39(5):425-33. [CrossRef]
- De Bruyn H, Christiaens V, Doornewaard R, Jacobsson M, Cosyn J, Jacquet W, Vervaeke S. Implant surface roughness and patient factors on long-term peri-implant bone loss. Periodontol 2000. 2017 Feb;73(1):218-227. [CrossRef] [PubMed]
- de Freitas MM, da Silva CH, Groisman M, Vidigal GM Jr. Comparative analysis of microorganism species succession on three implant surfaces with different roughness: an in vivo study. Implant Dent. 2011 Apr;20(2):e14-23. [CrossRef]
- Al-Radha AS, Pal A, Pettemerides AP, Jenkinson HF. Molecular analysis of microbiota associated with peri-implant diseases. J Dent. 2012 Nov;40(11):989-98. [CrossRef]
- Ramanauskaite A, Schwarz F. Current concepts for the treatment of peri-implant disease. Int J Prosthodont. 2023 Nov 21;0(0):1-32. [CrossRef] [PubMed]
- Gomes BP, Jacinto RC, Montagner F, Sousa EL, Ferraz CC. Analysis of the antimicrobial susceptibility of anaerobic bacteria isolated from endodontic infections in Brazil during a period of nine years. J Endod. 2011 Aug;37(8):1058-62. [CrossRef]
- Thomas E Rams, John E Degener, Arie J van Winkelhoff. Antibiotic resistance in human peri-implantitis microbiota. Clin Oral Implants Res. 2014 Jan;25(1):82-90. [CrossRef]
- van Winkelhoff AJ. Antibiotics in the treatment of peri-implantitis. Eur J Oral Implantol. 2012;5 Suppl:S43-50.
Figure 1.
Gingival fluid sample collection using sterile paper cones from a dental crown level.

Figure 2.
Gingival fluid sample collection using sterile paper cones from a dental implant crown level.
Figure 2.
Gingival fluid sample collection using sterile paper cones from a dental implant crown level.

Figure 3.
Sterile containers and paper cones.

Figure 4.
Protocol scheme.
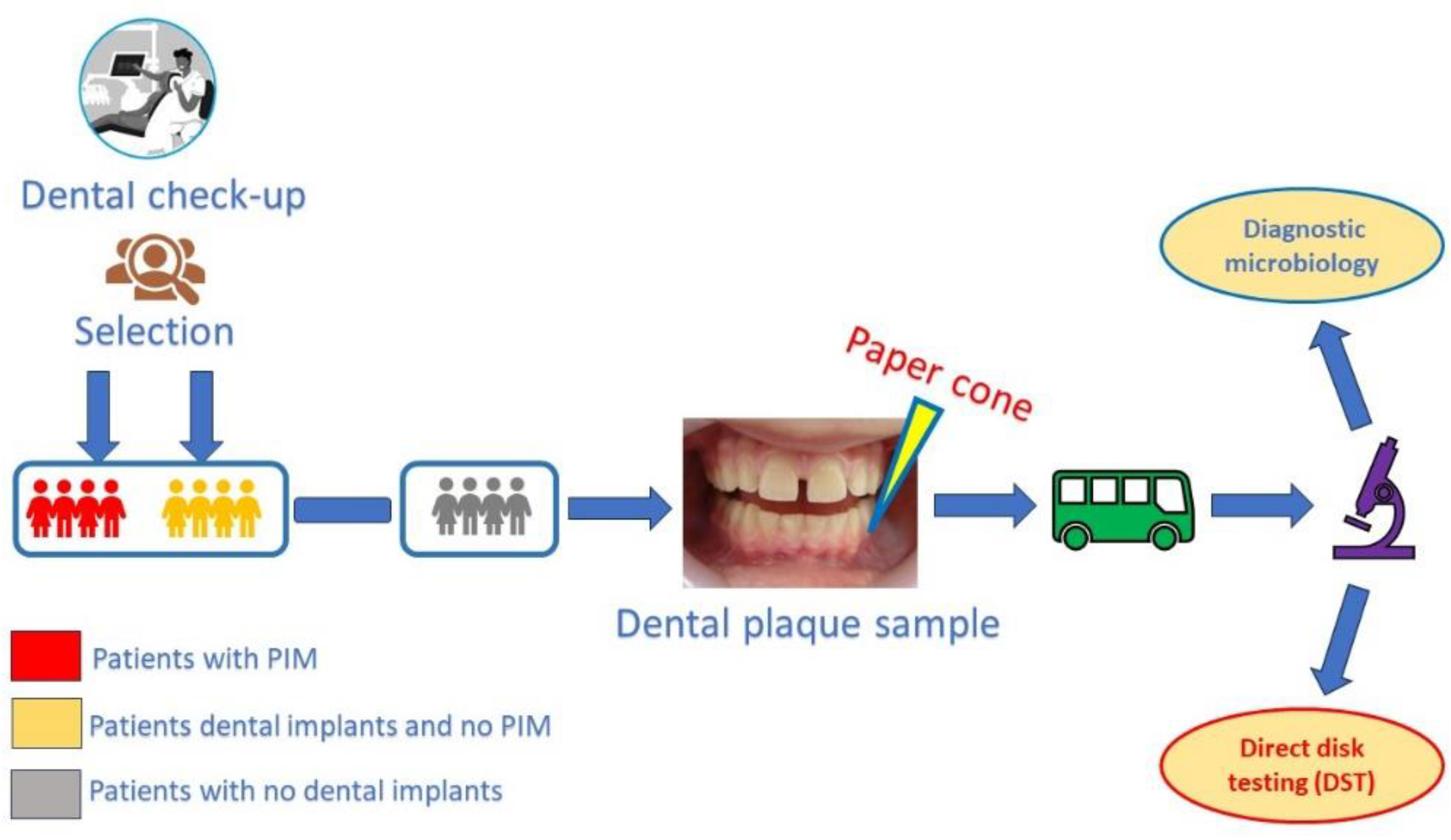

Table 1.
Microbiological data from our sample.
| Microorganism | Number of sites | PIMa | MPATb | PATc | HSd |
|---|---|---|---|---|---|
| Candida albicans (Cand. a.) | 7 | 3 | 1 | 2 | 1 |
| Candida krusei (Cand. k.) | 3 | 0 | 0 | 1 | 2 |
| Candida parapsilosis (Cand. p.) | 2 | 1 | 0 | 1 | 0 |
| Neisseria mucosa (Neis. m.) | 2 | 2 | 0 | 0 | 0 |
| Prevotella (Prev.) | 7 | 3 | 1 | 3 | 0 |
| Staphylococcus aureus (Staph. a.) | 3 | 1 | 2 | 0 | 0 |
| Group A beta hemolytic streptococcus (Strept. A.) |
5 | 1 | 0 | 1 | 3 |
| Group C streptococcus (Strept. C.) | 3 | 2 | 0 | 0 | 1 |
| Group G streptococcus (Strept. G.) | 3 | 0 | 1 | 2 | 0 |
| Pyogenic streptococcus (Strept. Pyo.) | 2 | 0 | 0 | 1 | 1 |
| Veillonella (Veil.) | 3 | 1 | 2 | 0 | 0 |
aPeri-implant mucositis. bPeriodontally affected tooth with crown. cPeriodontally affected tooth. dHealthy site.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



