
Submitted:
17 September 2024
Posted:
18 September 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Cycle threshold (Ct) values of SARS-CoV-2 real-time reverse transcriptase-polymerase chain reaction (RT-PCR) tests are associated with infectivity and viral load, and they could be an aid to forecast the evolution of SARS-CoV-2 outbreaks. The objective was to know the Ct values related to the incidence and reinfection of SARS-CoV-2 in successive outbreaks, which took place in nursing homes in Castellon (Spain) during 2020-2022, and to test its usefulness as an instrument of epidemic surveillance in nursing homes. Poisson regression and multinomial logistic regression were used in the analysis. We studied four nursing home SARS-CoV-2 outbreaks, and the average infection rate, reinfection rate, and case fatality were 72.7%, 19.9%, and 5.5%, respectively; 98.9% of residents were vaccinated with three doses of a mRNA SARS-CoV-2 vaccine. Ct values for first infections and reinfections were 27.1±6.6 and 31.9±5.4 (p = 0.000). Considering Ct values ≥30 versus
Keywords:
SARS-CoV-2
; PCR
; cycle threshold
; infections
; nursing homes
; outbreaks
; retrospective cohort
1. Introduction
Cycle threshold (Ct) values of the real-time reverse transcriptase-polymerase chain reaction (RT-PCR) have been considered in the diagnosis, follow-up, and infectivity of SARS-CoV-2 in many studies [1,2,3,4]. However, the intrinsic values of Ct in SARS-CoV-2 outbreaks in nursing homes have been less studied [5,6,7], and its utility as a tool for forecasting epidemics and new variants has been only described in the general population [8,9,10]. Nursing homes were crucial points of the SARS-CoV-2 pandemic, considering the devastating impact on the elderly population residents, who had a high risk of infection, and many of this population presented immune deficiencies that increased the persistence and viral SARS-CoV-2 load [11,12].
Preventive and control measures to stop the transmission of the virus can be made considering Ct values, which are correlated with duration, infectivity, and viral load of infected patients [13,14]. In addition, SARS-CoV-2 vaccines can increase Ct after one or two doses, producing a lower viral load and decreasing virus transmission [15,16].
However, the use of Ct values in clinical and epidemiological contexts has controversy; Ct values are not standardized, and its limits have been the subject of some discussion, but more than 34 cycles are considered negative [17,18,19]. On the other hand, considering Ct values higher than 35 as negative to transmit the virus would be a limitation, given that it has been estimated that around 4.7 and 8.3% of patients with Ct values higher than 35 are infectious [13,20]. In addition, some research has indicated that Ct values are not associated with the clinical history of the disease and are only weakly associated with symptomatology at the time of test [21]. Routine reporting of Ct values is not recommended after considering several critical points, including collected samples, transport, analytic methods, and international standardization [22,23]. However, at a population level, Ct values could be used to know the evolution of the epidemic with a standardized assay [10].
The objective of this study was to estimate the Ct values related to the incidence and reinfection of SARS-CoV-2 in four outbreaks that took place in nursing homes in Castellon (Spain) and to test Ct values as an instrument of epidemic surveillance in these facilities.
2. Materials and Methods
2.1. Retrospective Cohortstudy
The study population corresponds to residents in four nursing homes in the Health Department of Castellon, Valencia Community (Spain), during the period 2020-2022, where COVID-19 outbreaks took place. The Epidemiology Division of the Public Health Center of Castelló de la Plana implemented the actions to control these outbreaks in order to break SARS-CoV-2 transmissions and prevent new cases. From the information collected, a retrospective cohort design was used to address the objective of the study. In total, four outbreaks occurred in the four studied nursing homes from February 2021 to April 2022.
All SARS-CoV-2 cases had a laboratory confirmation test by a positive RT-PCR carried out by the Microbiology`s Services of the University General Hospital in Castellon and the University Hospital of La Plana in Vila-real. For the RT-PCR we were using Roche Lightmix Modular SARS-CoV-2 (Roche-TIB MOLBIOL D-12103) [24] the VIASURE SARS-CoV-2 Real Time PCR Detection Kit (CerTest Biotec S.L), Abbott Real-Time SARS-CoV-2 (Abbott Laboratory), and Argene SARS-CoV-2 R-Gene (Biomérieux SA). Less than 30 Ct values were considered positive following the official protocol of health authorities [25].
We defined reinfection as a new SARS-CoV-2 infection more than 60 days after the previous SARS-CoV-2 infection and confirmed by PCR test or a rapid antigen test (RAT) [26]. The first infection must have been confirmed by PCR, RAT, or positive anti-Nucleocapsid IgG antibodies.
2.2. Statistical Analysis
Comparisons of qualitative and quantitative variables were made with Chi2, Fisher’s test, and Kruskall-Wallis, respectively. First, we used Ct values as a quantitative dependent variable and SARS-CoV-2 reinfection as an explicative variable. One-way analysis of variance (ANOVA) and robust bivariate and multivariable linear regressions were employed in the analysis. Second, we used Ct value as a dependent variable, considering Ct value ≥ 30.0 as value 1 and Ct value <30 as value 0. SARS-CoV-2 reinfection was considered a predictor variable, and covariate variables were age, sex, time elapsed from SARS-CoV-2 outbreak, and nursing home center. Poisson regression was employed to calculate the crude relative risk (cRR) and adjusted relative risk (aRR) with a 95% confidence interval (CI). Age, sex, nursing home and elapsed time from the first SARS-CoV-2 outbreak were included in the multivariable models as confounding factors following the Directed Acyclic Graphics (DAGs) method in order to measure the relationship between reinfection and Ct values [27]. Stata® program 14 version 2 was used for the statistical analysis.
Following a suggestion of the American Association for Clinical Chemistry [28], and to confirm the results of the first analysis, we performed a sensitivity analysis considering semi-quantitative Ct values. The levels of Ct can be separated into three groups, according to Quiroz-Ruiz and co-authors [29].These authors proposed considering the clinical severity and the Ct value: minor (Ct < 18.83), medium (Ct ≥ 18.83-30.10), and high (Ct > 30.10). Multinomial logistic regression analysis was performed considering crude and adjusted odds ratios (OR) with potential confounding factors as indicated before.
For this study, the approval of an Ethics Committee was not needed considering the epidemic situation of the COVID-19 pandemic in accordance with Spanish legislation.
3. Results
Nursing home characteristics, SARS-CoV-2 infections, and reinfections are shown in Table 1. The SARS-CoV-2 variants of the four outbreaks were Delta B.1.617.2, one outbreak in April 2021, and Omicron, three from January to March 2022. The four nursing homes had a total of 472 residents; the mean age was 83.1±9.8 years with 318 females (67.4%), and 467 were vaccinated with two doses of the SARS-CoV-2 vaccine (98.9%). The median of the elapsed time from the former SARS-CoV-2 outbreak was 391.8 days, with a range of 339.9 and 634.9 days. In the four nursing homes, the means attack rates of infections and reinfections were 72.7% (range 45.6%-96.2%) and 19.9% (range 0.9%-47.7%), respectively, and the means mortality and case fatality rate were 4.0% and 5.5%.
Considering the 472 residents, a total of 343 residents suffered SARS-CoV-2 new infections (Figure 1). From them, 249 first infections and 94 reinfections were reported. Ct values determinations were made for 252 residents, 185 with new infections and 67 with reinfections that supposed a participation rate of 73.5%.
The characteristics of participants and Ct values of SARS-CoV-2 infections and reinfections are shown in Table 2. The mean of reinfections was 26.6% (range 1.1%-53.3%). When comparing Ct at each nursing home, the mean Ct values were 28.4±6.7 (range 25.2±6.2-30.9±7.0). The Ct mean in reinfection of residents was 31.9±5.4 versus 27.1±6.6 in residents with the first infections (p = 0.000). Respect to quantitative Ct values, in a crude analysis of robust bivariate linear regression, the regression coefficient was 4.75 (95% CI 2.97-6.52, p = 0.000) and in a robust multivariable linear regression, it was 4.78 (95% CI 2.80-6.76, p = 0.000).
A comparison of Ct values ≥30 versus <30 by Poisson regression is presented in Table 3. In the adjusted analysis, the elapse time from the former SARS-CoV-2 outbreak was significantly less in the group with Ct values <30. In three nursing homes, patients with SRAR-CoV-2 reinfections had a higher Ct than patients with the first infection, but only in a center with a significant difference. In the four nursing homes, patients with reinfections had higher Ct values than patients with the first infection, adjusted relative risk 1.66 (96% CI 1.10-2.51, p = 0.015).
Results of sensitivity analysis are shown in Table 4. Patients with SARS-CoV-2 reinfections had significantly more elevated Ct values than patients with new SARS-CoV-2 infection, adjusted odds ratio 17.63 (95% CI 2.22-139.86, p = 0.007) for Ct values >30.1 with respect to Ct values <18.83.
4. Discussion
Our results suggest the usefulness of Ct values in SARS-CoV-2 outbreaks in nursing homes for knowing the epidemic´s evolution and being an appropriate surveillance tool in outbreaks. The Ct values have increased in SARS-CoV-2 reinfections, and the epidemic situation has decreased with less transmission and severity, following the paradigm of hybrid immunity [30,31]. The mortality and case fatality were considerably reduced in the four nursing homes compared with the first COVID-19 epidemic from March 2020 to January 2021 in the nursing homes in the Castellón Health Department, when mortality and case fatality means were 8.7% and 22.7%, respectively [12]. Although there were elevated proportions of SARS-CoV-2 vaccinated residents, the incidence of SARS-CoV-2 infections was high, suggesting that vaccination has a limited efficacy against viral transmission, and non-pharmacological measures in these nursing homes need to be improved to reduce transmission of SARS-CoV-2 infections [32,33].
In three nursing homes Ct values were associated with SARS-CoV-2 reinfection, except in a center, where elapsed time from the former SARS-CoV-2 outbreak was longer than one year and a half. Anti-SARS-CoV-2 antibodies decline over time after infection or vaccination [34], and the study of cellular immunity in nursing home residents could be useful [35].
In a SARS-CoV-2 outbreak, a serial of Ct values can provide information on the clinical and epidemiological situation of residents and staff and take adequate measures of control and prevention, such as non-pharmaceutical interventions to prevent transmission [36]. In Massachusetts, Ct values for staff and residents of nursing homes had no differences between symptomatic and asymptomatic patients at the time of sampling, with mean Ct values of 25.7 and 26.4, respectively [37]. During a SARS-CoV-2 outbreak in a nursing home in Holland, Paad and co-authors [38] reported similar findings in residents. However, Wilson and co-authors [39] found that residents and healthcare personnel in nursing homes with specimen Ct<30 were more likely to have symptoms, and only 17% of positive SARS-CoV-2 individuals after more than 90 days of the first infection had Ct values less than 30. Testing for infectivity should be performed without considering symptoms of infection. In addition, SARS-CoV-2 vaccines (ChAdOx1 nCoV-19 and BNT162b2) one or two doses can increase the Ct values of vaccinated residents in nursing homes compared with no vaccinated residents and suggest that vaccine may protect against virus transmission [16]. Shrotri and co-authors found [40] that the mean of Ct values was higher for infection after vaccination than infection before vaccination (31.3% versus 26.6%, p<0·0001).
At a population level, routine screening of Ct values can be useful for monitoring the SARS-CoV-2 epidemic [41]. In the general population of Pakistan, Shoaib and co-authors [42] found an increase in Ct values in asymptomatic cases of SARS-CoV-2 to decrease epidemic possibility. In Iran, Dehesh and co-authors [43] found that the average daily Ct value can predict increases in the number of positive confirmed COVID-19 cases. In England during the period 2020-2022, Harrison and co-authors [10] found that mean Ct values decreased 6-29 days before the number of positive tests increased, and Ct values provided indication of new variants. In Delta variant outbreaks, Ct values were a predictor for hospitalization in Belgium [44]. Measures of Ct values for future SARS-CoV-2 epidemics have been highlighted using the third generation of RT-PCR [45]. In addition, a method of standardization of Ct values in function of the clinical sample has been proposed [46,47].
The strengths of this study include: first, a cohort design that reduces bias in selection and information. Second, the participation rate was elevated. Third, confirmatory tests were completed for all the residents. Fourth, only 2 laboratories with the same RT-PCR technique carried out all the samples. Fifth, multivariable models were used for the control confounding factors. Sixth, the sensitivity analysis confirms the results.
The RT-PCR is a qualitative test, and its use as a quantitative test or semi-quantitative test is the more important limitation of our study [22,28,48,49,50]. More limitations include: First, the Ct groups used in our study are based on clinical severity [51]. Second, Ct values present changes associated with the duration of the illness, increasing with the elapsed time from the onset of the illness [13,52]. Third, during an outbreak, the timing of sampling could present a mix of different durations of the disease. Fourth, in the comparisons of Ct values among laboratories, differences could occur considering the specific work of each laboratory, such as expertise and protocols used [13,23,53].
5. Conclusions
In our cohort study with a high proportion of SARS-CoV-2 vaccinated residents, reinfections were associated with high Ct values that correspond with hybrid immunity, suggesting a decrease in transmission and severity, and can be a tool of epidemiological surveillance of SARS-CoV-2 epidemics in nursing homes.
Author Contributions
Conceptualization, J.C.G.-L., M.G-F., M.D.T.-B., O.P.-O. and J.B.B.-B; methodology, J.C.G.-L., M.G.-F., M.D.T.-B., A.A.-P. and J.B.B.-B .; software, N.M.-F.,LL.LL.-B.,A.A.-P., and J.B.B.-B.; validation, O.S.-B., O.P.-O., N.H.-P., M.G.-F., M.D.T.-B., and I.G.-A.; formal analysis, A.A.-P. and J.B.B.-B.; investigation, J.C.G-L., N.M.-F.,O.S.-B., O.P.-O., I.G.-A., S.P.-G., N.H.-P., and V.R.; resources, M.G.-F., and M.D.T.-B.; data curation, O.S.-B., I.G.-A.,S.P.-G., and N.H.-P ; writing—original draft preparation, J.C.G.-L, A.A.-P., and J.B.B.-B.; writing—review and editing, A,A.-P and J.B.B-B.; visualization, I.G.-A., and S.P.-G.; supervision, M.G.-F., and M.D.T.-B.; project administration, J.B.B.-B; funding acquisition, M.G.-F., and M.D.T.-B All authors have read and agreed to the published version of the manuscript
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical review and approval were waived for this study due to the epidemiologic surveillance of the NHs motivated by the COVID-19 pandemic according to Spanish laws and regulations
Informed Consent Statement
Patient consent was waived due to surveillance epidemiological of NHs motivated by the COVID-19 pandemic, and we used aggregated data of each NS.
Data Availability Statement
Authorization of the Public Health Center’s direction will be required to consult the data set of this study.
Acknowledgments
The authors thank the residents and the staff of the 5 nursing homes for the help to perform this study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Rao, S.N.; Manissero, D.; Steele, V.R.; Pareja, J. A systematic review of the clinical utility of cycle threshold values in the context of COVID-19. Infect Dis Ther 2020, 9, 573–586. [Google Scholar] [CrossRef]
- Aranha, C.; Patel, V.; Bhor, V.; Gogoi, D. Cycle threshold values in RT-PCR to determine dynamics of SARS-CoV-2 viral load: An approach to reduce the isolation period for COVID-19 patients. J Med Virol 2021, 93, 6794–6797. [Google Scholar] [CrossRef] [PubMed]
- Hwang, J.; Yuen, A.; Rhoades, J.; Barnes, D.; Zakowski, P.; Megna, D.J.; Catarino, P.; Zaffiri, L.; Rampolla, R. Real-time transcription polymerase chain reaction cycle threshold values as criteria for utilization of incidental COVID-19 positive lung donors. J Heart Lung Transplant 2022, 28, S1053–2498. [Google Scholar] [CrossRef] [PubMed]
- Yang, D.; Hansel, D.E.; Curlin, M.E.; Townes, J.M.; Messer, W.B.; Fan, G.; Qin, X. Bimodal distribution pattern associated with the PCR cycle threshold (Ct) and implications in COVID-19 infections. Sci Rep 2022, 12, 14544. [Google Scholar] [CrossRef]
- Kimball, A.; Hatfield, K.M.; Arons, M.; James, A.; Taylor, J.; Spicer, K.; Bardossy, A.C.; Oakley, L.P.; Tanwar, S.; Chisty, Z.; et al. Asymptomatic and presymptomatic SARS-CoV-2 infections in residents of a long-term care skilled nursing facility - King County, Washington, March 2020. MMWR Morb Mortal Wkly Rep 2020, 69, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Arons, M.M.; Hatfield, K.M.; Reddy, S.C.; Kimball, A.; James, A.; Jacobs, J.R.; Taylor, J.; Spicer, K.; Bardossy, A.C.; Oakley, L.P.; et al. Presymptomatic SARS-CoV-2 infections and transmission in a skilled nursing facility. N Engl J Med 2020, 382, 2081–2090. [Google Scholar] [CrossRef] [PubMed]
- Paap, K.C.; van Loon, A.M.; Koene, F.M.; van Buul, L.W.; Jurriaans, S.; Smalbrugge, M.; de Jong, M.D.; Hertogh, C.M.P.M. Clinical evaluation of single-swab sampling for rapid COVID-19 detection in outbreak settings in Dutch nursing homes. Eur Geriatr Med. 2022, 13, 711–718. [Google Scholar] [CrossRef]
- Chung, H.Y.; Jian, M.J.; Chang, C.K.; Lin, J.C.; Yeh, K.M.; Chen, C.W.; Hsieh, S.S.; Hung, K.S.; Tang, S.H.; Perng, C.L; et al. Emergency SARS-CoV-2 variants of concern: Novel multiplex real-time RT-PCR assay for rapid detection and surveillance. Microbiol Spectr 2022, 10, e0251321. [Google Scholar] [CrossRef] [PubMed]
- Tso, C.F.; Garikipati, A.; Green-Saxena, A.; Mao, Q.; Das, R. Correlation of population SARS-CoV-2 cycle threshold values to local disease dynamics: Exploratory observational study. JMIR Public Health Surveill 2021, 7, e28265. [Google Scholar] [CrossRef]
- Harrison, R.E.; Hamada, A.; Haswell, N.; Groves, A.; Vihta, K.D.; Cella, K.; Garner, S.; Walker, A.S.; Seale, A.C. Cycle threshold values as indication of increasing SARS-CoV-2 new variants, England, 2020-2022. Emerg Infect Dis. 2023, 29, 2024–2031. [Google Scholar] [CrossRef] [PubMed]
- Konetzka, R.T.; White, E.M.; Pralea, A.; Grabowski, D.C.; Mor, V. A systematic review of long-term care facility characteristics associated with COVID-19 outcomes. J Am Geriatr Soc 2021, 69, 2766–2777. [Google Scholar] [CrossRef] [PubMed]
- Arnedo-Pena, A.; Romeu-Garcia, M.A.; Gascó-Laborda, J.C.; Meseguer-Ferrer, N.; Safont-Adsuara, L.; Prades-Vila, L.; Flores-Medina, M.; Rusen, V.; Tirado-Balaguer, M.D.; Sabater-Vidal, S.; et al. Incidence, mortality, and risk factors of COVID-19 in nursing homes. Epidemiologia (Basel) 2022, 3, 179–190. [Google Scholar] [CrossRef] [PubMed]
- Singanayagam, A.; Patel, M.; Charlett, A.; Lopez Bernal, J.; Saliba, V.; Ellis, J.; Ladhani, S.; Zambon, M.; Gopal, R. ; Duration of infectiousness and correlation with RT-PCR cycle threshold values in cases of COVID-19, England, January to May 2020. Euro Surveill 2020, 25, 2001483. [Google Scholar] [CrossRef]
- Girón Pérez, D.A.; Fonseca-Agüero, A.; Toledo-Ibarra, G.A.; Gomez-Valdivia, J.J.; Díaz-Resendiz, K.J.G.; Benitez-Trinidad, A.B.; Razura-Carmona, F.F.; Navidad-Murrieta, M.S.; Covantes-Rosales, C.E.; Giron-Pérez, M.I. Post-COVID-19 syndrome in outpatients and its association with viral load. Int J Environ Res Public Health 2022, 19, 15145. [Google Scholar] [CrossRef] [PubMed]
- Eyre, D.W.; Taylor, D.; Purver, M.; Chapman, D.; Fowler, T.; Pouwels, K.B.; Walker, A.S.; Peto, T.E.A. Effect of Covid-19 vaccination on transmission of Alpha and Delta variants. N Engl J Med 2022, 386, 744–756. [Google Scholar] [CrossRef] [PubMed]
- McEllistrem, M.C.; Clancy, C.J.; Buehrle, D.J.; Lucas, A.; Decker, B.K. Single dose of an mRNA Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-Cov-2) vaccine is associated With lower nasopharyngeal viral load among nursing home residents with asymptomatic coronavirus disease 2019 (COVID-19). Clin Infect Dis 2021, 73, e1365–e1367. [Google Scholar] [CrossRef]
- Kapoor, M.; Kalita, D.; Panda, P.K. Cycle threshold values versus reverse transcription-polymerase chain reaction positivity in COVID-19 de-isolation. Indian J Med Microbiol 2021, 39, 133–135. [Google Scholar] [CrossRef] [PubMed]
- Wünsch, K.; Anastasiou, O.E.; Alt, M.; Brochhagen, L.; Cherneha, M.; Thümmler, L.; van Baal, L.; Madel, R.J.; Lindemann, M.; Taube, C.; et al. COVID-19 in elderly, immunocompromised or diabetic patients-From immune monitoring to clinical management in the hospital. Viruses 2022, 14, 746. [Google Scholar] [CrossRef]
- McKay, S.L.; Tobolowsky, F.A.; Moritz, E.D.; Hatfield, K.M.; Bhatnagar, A.; LaVoie, S.P.; Jackson, D.A.; Lecy, K.D.; Bryant-Genevier, J.; Campbell, D.; et al. Performance evaluation of serial SARS-CoV-2 rapid antigen testing during a nursing home outbreak. Ann Intern Med 2021, 174, 945–951. [Google Scholar] [CrossRef] [PubMed]
- Leitão, I.C.; Calil, P.T.; Galliez, R.M.; Moreira, F.R.R.; Mariani, D.; Castiñeiras, A.C.P.; da Silva, G.P.D.; Maia, R.A.; Corrêa, I.A.; Monteiro, F.L.L.; et al. Prolonged SARS-CoV-2 positivity in immunocompetent patients: virus isolation, genomic integrity, and transmission risk. Microbiol Spectr 2021, 9, e0085521. [Google Scholar] [CrossRef]
- Shoaib, N.; Noureen, N.; Faisal, A.; Zaheer, M.; Imran, M.; Ahsan, A.; Munir, R.; Zaidi, N. Factors associated with cycle threshold values (Ct-values) of SARS-CoV2-rRT-PCR. Mol Biol Rep 2022, 49, 4101–4106. [Google Scholar] [CrossRef]
- Rhoads, D.D.; Pinsky, B.A. The truth about SARS-CoV-2 cycle threshold values is rarely pure and never simple. Clin Chem 2021, 68, 16–18. [Google Scholar] [CrossRef]
- Fan, G.; Jin, Y.; Wang, Q.; Yue, Y. Assessing the comparability of cycle threshold values derived from five external quality assessment rounds for Omicron nucleic acid testing. Virol J 2023, 20, 119. [Google Scholar] [CrossRef] [PubMed]
- Yip, C.C.; Sridhar, S.; Cheng, A.K.; Leung, K.H.; Choi, G.K.; Chen, J.H.; Poon, R.W.; Chan, K.H.; Wu, A.K.; Chan, H.S.; et al. Evaluation of the commercially available LightMix® Modular E-gene kit using clinical and proficiency testing specimens for SARS-CoV-2 detection. J Clin Virol 2020, 129, 104476. [Google Scholar] [CrossRef] [PubMed]
- Ministerio de Sanidad. Estrategia de detección precoz, vigilancia y control de COVID-19. Centro de Coordinación de Alertas y Emergencias Sanitarias. Actualizado 22 de diciembre de 2021. Available online: https://www.mscbs.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov/documentos/COVID19_Estrategia_vigilancia_y_control_e_indicadores.pdf (accessed on 28 June 2022).
- European Centre for Disease Prevention and Control Reinfection with SARS-CoV-2: Implementation of a Surveillance Case Definition within the EU/EEA. 2021. Available online: https://www.ecdc.europa.eu/en/publications-data/reinfection-sars-cov-2-implementation-surveillance-case-definition-within-eueea (accessed on 20 June 2022).
- Textor, J.; van der Zander, B.; Gilthorpe, M.S.; Liskiewicz, M.; Ellison, G.T. Robust causal inference using directed acyclic graphs: the R package 'dagitty'. Int J Epidemiol 2016, 45, 1887–1894. [Google Scholar] [CrossRef]
- American Association for Clinical Chemistry.Recommendation for reporting SARS-CoV-2 cycle threshold (CT) values. Available online: https://www.aacc.org/-/media/Files/Science-and-Practice/Statements/Recommendationsreporting-SARSCoV2-CT-values.pdf?la=en&hash=0E62FEDEA43FED8AF44404A9B2177756DDC84394 (accessed on 1 March 2023).
- Quiroz-Ruiz, H.R.; Chimoy-Effio, P.J.; Vértiz-Osores, J.J.; Bazán-Mayra, J.E. Correlación entre el umbral de ciclo de la RPC en tiempo real y la clasificación clínica de la COVID-19. Rev Chilena Infectol 2022, 39, 35–44. [Google Scholar] [CrossRef] [PubMed]
- Bobrovitz, N.; Ware, H.; Ma, X.; Li, Z.; Hosseini, R.; Cao, C.; Selemon, A.; Whelan, M.; Premji, Z.; Issa, H.; et al. Protective effectiveness of previous SARS-CoV-2 infection and hybrid immunity against the omicron variant and severe disease: a systematic review and meta-regression. Lancet Infect Dis 2023, 23, 556–567. [Google Scholar] [CrossRef] [PubMed]
- Gascó-Laborda, J.C.; Gil-Fortuño, M.; Ortiz-Rambla, J.; Meseguer-Ferrer, N.; Pérez-Olaso, Ó.; Lluch-Bacas, L.; Moya-Malo, R.; Moliner-Urdiales, D.; Bellido-Blasco, J.B. COVID-19 outbreak in a properly vaccinated nursing home. Influence of hybrid immunity on viral load, risk of infection and risk of disease progression. Rev Esp Salud Publica 2024, 98, e202405036. [Google Scholar]
- Mauriz, E.; Fernández-Vázquez, J.P.; Díez-Flecha, C.; Reguero-Celada, S.; Fernández-Villa, T.; Fernández-Somoano, A.; Caylà, J.A.; Lozano-García, J.A.; Vázquez-Casares, A.M.; Martín-Sánchez, V. Impact of a COVID-19 outbreak in an elderly care home after primary vaccination. Vaccines (Basel) 2023, 11, 1382. [Google Scholar] [CrossRef] [PubMed]
- Henriques, H.R.; Sousa, D.; Faria, J.; Pinto, J.; Costa, A.; Henriques, M.A.; Durão, M.C. Learning from the covid-19 outbreaks in long-term care facilities: a systematic review. BMC Geriatr 2023, 23, 618. [Google Scholar] [CrossRef] [PubMed]
- Meyers, E.; Deschepper, E.; Duysburgh, E.; De Rop, L.; De Burghgraeve, T.; Van Ngoc, P.; Digregorio, M.; Delogne, S.; Coen, A.; De Clercq, N.; et al. Declining prevalence of SARS-CoV-2 antibodies among vaccinated nursing home residents and staff six months after the primary BNT162b2 vaccination campaign in Belgium: A prospective cohort study. Viruses. 2022, 14, 2361. [Google Scholar] [CrossRef] [PubMed]
- Moyet, J.; Helle, F.; Bourdenet, G.; Joseph, C.; Gubler, B.; Deschasse, G.; Defouilloy, I.; Slovenski, T.; François, C.; Liabeuf, S.; et al. Kinetics of SARS-CoV-2-neutralising antibodies of residents of long-term care facilities. J Nutr Health Aging 2022, 26, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Petersen, J.; Jhala, D. COVID-19 cycle threshold/cycle number testing at a community living center. Fed Pract 2022, 39, 254–260. [Google Scholar] [CrossRef] [PubMed]
- Lennon, N.J.; Bhattacharyya, R.P.; Mina, M.J.; Rehm, H.L.; Hung, D.T.; Smole, S.; Woolley, A.; Lander, E.S.; Gabriel, S.B. Cross-Sectional assessment of SARS-CoV-2 viral load by symptom status in Massachusetts congregate living facilities. J Infect Dis 2021, 224, 1658–1663. [Google Scholar] [CrossRef]
- Paap, K.C.; van Loon, A.M.; van Rijs, S.M.; Helmich, E.; Buurman, B.M.; Smalbrugge, M.; Hertogh, C.M.P.M. Symptom- and prevention-based testing of COVID-19 in nursing home residents: A retrospective cohort study. Gerontol Geriatr Med 2021, 7, 23337214211055338. [Google Scholar] [CrossRef] [PubMed]
- Wilson, W.W.; Hatfield, K.M.; Tressler, S.; Bicking Kinsey, C.; Parra, G.; Zell, R.; Denson, A.; Williams, C.; Spicer, K.B.; et al. Characteristics of nursing home residents and healthcare personnel with repeated severe acute respiratory coronavirus virus 2 (SARS-CoV-2) tests positive ≥90 days after initial infection: Four US jurisdictions, July 2020-March 2021. Infect Control Hosp Epidemiol 2023, 44, 809–812. [Google Scholar] [CrossRef] [PubMed]
- Shrotri, M.; Krutikov, M.; Palmer, T.; Giddings, R.; Azmi, B.; Subbarao, S.; Fuller, C.; Irwin-Singer, A.; Davies, D.; Tut, G.; et al. Vaccine effectiveness of the first dose of ChAdOx1 nCoV-19 and BNT162b2 against SARS-CoV-2 infection in residents of long-term care facilities in England (VIVALDI): A prospective cohort study. Lancet Infect Dis 2021, 21, 1529–1538. [Google Scholar] [CrossRef] [PubMed]
- Johnson, B.N.; Cooper, L.; Beck, J.J.; Finnicum, C.T.; Davis, C.M.; Van Asselt, A.J.; Kallsen, N.; Silvernail, C.; Viet, S.; Long, K.; et al. More than results: the clinical and research relationship in the evolving detection and surveillance of SARS-CoV-2. S D Med 2023, 76, 248–256. [Google Scholar] [PubMed]
- Shoaib, N.; Iqbal, A.; Shah, F.A.; Zainab, W.; Qasim, M.; Zerqoon, N.; Naseem, M.O.; Munir, R.; Zaidi, N. Population-level median cycle threshold (Ct) values for asymptomatic COVID-19 cases can predict the trajectory of future cases. PLoS One 2023, 18, e0281899. [Google Scholar] [CrossRef] [PubMed]
- Dehesh, P.; Baradaran, H.R.; Eshrati, B.; Motevalian, S.A.; Salehi, M.; Donyavi, T. The relationship between population-level SARS-CoV-2 cycle threshold values and trend of COVID-19 infection: Longitudinal study. JMIR Public Health Surveill 2022, 8, e36424. [Google Scholar] [CrossRef]
- Boogaerts, H.L.F.; Smits, P.; Hans, G.; Bouly, L.; Coeck, E.; Vandamme, S.; Jansens, H.; Goossens, H.; Matheeussen, V. Laboratory analysis of two Delta SARS-CoV-2 variant outbreaks in the Port of Antwerp. Acta Clin Belg 2022, 77, 925–932. [Google Scholar] [CrossRef] [PubMed]
- Nyaruaba, R.; Mwaliko, C.; Dobnik, D.; Neužil, P.; Amoth, P.; Mwau, M.; Yu, J.; Yang, H.; Wei, H. Digital PCR Applications in the SARS-CoV-2/COVID-19 era: A roadmap for future outbreaks. Clin Microbiol Rev 2022, 35, e0016821. [Google Scholar] [CrossRef]
- Miranda, R.L.; Guterres, A.; de Azeredo Lima, C.H.; Filho, P.N.; Gadelha, M.R. Misinterpretation of viral load in COVID-19 clinical outcomes. Virus Res 2021, 296, 198340. [Google Scholar] [CrossRef]
- Han, M.S.; Byun, J.H.; Cho, Y.; Rim, J.H. RT-PCR for SARS-CoV-2: quantitative versus qualitative. Lancet Infect Dis 2021, 21, 165. [Google Scholar] [CrossRef] [PubMed]
- Infectious Disease Society of America and Association for Molecular Pathology joint statement on the use of SARS-CoV-2 PCR cycle threshold (Ct) values for clinical decision-making. Available online: https://www.idsociety.org/globalassets/idsa/public-health/covid-19/idsa-amp-statement.pdf (accessed on 1 March 2024).
- Michaelis, S.; Schneider, C.; Schnedl, W.J.; Baranyi, A.; Enko, D. Comparison of cycle-threshold-values between two commercial SARS-CoV-2 PCR assays. EXCLI J 2023, 22, 397–399. [Google Scholar] [PubMed]
- Dahdouh, E.; Lázaro-Perona, F.; Romero-Gómez, M.P.; Mingorance, J.; García-Rodriguez, J. Ct values from SARS-CoV-2 diagnostic PCR assays should not be used as direct estimates of viral load. J Infect 2021, 82, 414–451. [Google Scholar] [CrossRef] [PubMed]
- Ingberg, E.; Ahlstrand, E.; Cajander, P.; Löf, E.; Sundqvist, M.; Wegener, M.; Lidén, M.; Cajander, S. RT-PCR cycle threshold value in combination with visual scoring of chest computed tomography at hospital admission predicts outcome in COVID-19. Infect Dis (Lond) 2022, 54, 431–440. [Google Scholar] [CrossRef]
- Markewitz, R.; Dargvainiene, J.; Junker, R.; Wandinger, K.P. Cycle threshold of SARS-CoV-2 RT-PCR as a driver of retesting. Sci Rep 2024, 14, 2423. [Google Scholar] [CrossRef] [PubMed]
- Buchta, C.; Görzer, I.; Chiba, P.; Camp, J.V.; Holzmann, H.; Puchhammer-Stöckl, E.; Mayerhofer, M.; Müller, M.M.; Aberle, S.W. Variability of cycle threshold values in an external quality assessment scheme for detection of the SARS-CoV-2 virus genome by RT-PCR. Clin Chem Lab Med 2020, 59, 987–994. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Flow diagram showing the residents of nursing homes participants with cycle thresholds values (Ct) in the study.
Figure 1.
Flow diagram showing the residents of nursing homes participants with cycle thresholds values (Ct) in the study.
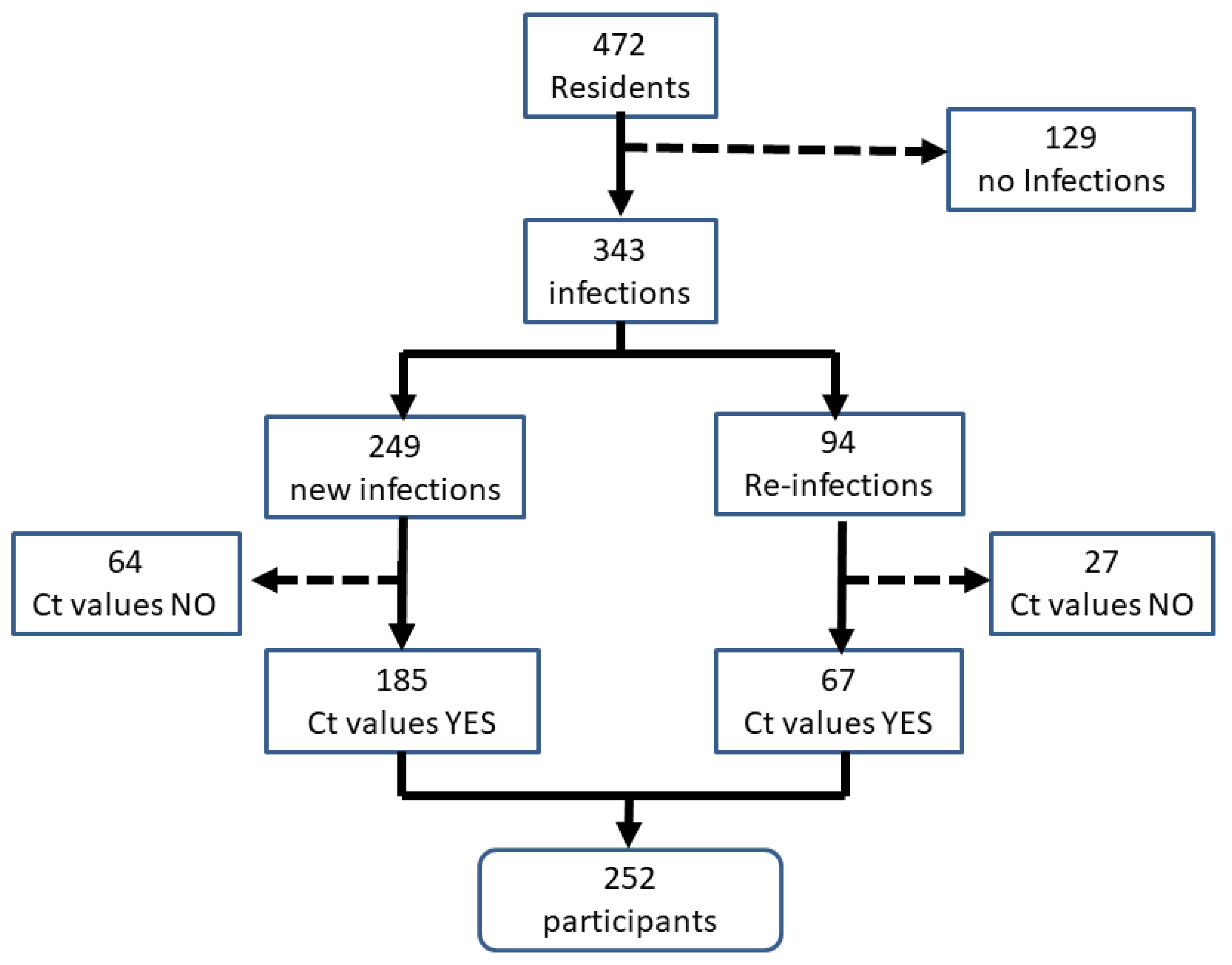

Table 1.
Description of nursing homes SARS-CoV-2 outbreaks, dates, SARS-CoV-2 variants, demographic characteristics, SARS-CoV-2 vaccination levels, and SARS-CoV-2 infections, reinfections, and case fatality rates.
Table 1.
Description of nursing homes SARS-CoV-2 outbreaks, dates, SARS-CoV-2 variants, demographic characteristics, SARS-CoV-2 vaccination levels, and SARS-CoV-2 infections, reinfections, and case fatality rates.
| Nursing homes | |||||
| Variables | Center 1 N (%) |
Center 2 N(%) |
Center 3 N(%) |
Center 4 N (%) |
Total N (%) |
| Date of reporting (months/year) | August 2021 | March 2022 | January 2022 | February 2022 | |
| COVID-19 Variant outbreak | Delta B.1.617.2 | Omicrom | Omicrom | Omicrom | |
| Total residents | 125 | 130 | 111 | 106 | 472 |
| Age (years) mean SD | 84.4±8.3 | 82.0±11.0 | 83.8±8.9 | 82.4±10.8 | 83.1±9.8 |
| Female | 90 (72) | 92(70.8) | 74(66.7) | 62 (58.5) | 318(67.4) |
| Male | 35 (28) | 38(29.2) | 37(33.3) | 44 (41.5) | 154(32.6) |
| Elapsed time from former SARS-COV-2 outbreak (days) | 339.9 | 433.1 | 350.5 | 634.9 | 391.81 |
| SARS-CoV-2 Vaccine | 122 (97.6) | 130 (100) | 111(100) | 104 (98.1) | 467(98.9) |
| Elapsed time from last vaccine doses mean SD (days) | 177±28.4 | 154 ±73.6 | 108±36.2 | 154±22.2 | 157±50.1 |
| Total SARS-CoV-2 infections | 57 (45.6) | 125 (96.2) | 94(84.7) | 67(63.2) | 343(72.7) |
| Incidence attack rate (%)2 | 45.6% | 96.2% | 84.7% | 63.2% | 72.7% |
| New SARS-CoV-2 infections | 50 (40) | 63 (48.5) | 93 (83.8) | 43(40.6) | 249(52.8) |
| SARS-CoV-2 reinfections | 7 (5.6) | 62 (47.7) | 1(0.90) | 24(22,6) | 94 (19.9) |
| Reinfections attack rate (%)2 | 5.6% | 47.7% | 0.90% | 22.6% | 19.9% |
| Mortality rate | 6 (4.8%) | 7 (5.4%) | 6(5.4%) | 0 | 19 (4.0%) |
| Fatality rate | 10.6% | 17.9% | 1.1% | 0 | 5.5% |
1 Median. 2 On the total of residents in each center.
Table 2.
Characteristics of residents with SARS-CoV-2 infections and reinfections and cycle threshold values (Ct) in nursing homes.
Table 2.
Characteristics of residents with SARS-CoV-2 infections and reinfections and cycle threshold values (Ct) in nursing homes.
| Nursing homes | |||||
| Variables | Centre 1 N (%) |
Centre 2 N (%) |
Centre 3 N (%) |
Centre 4 N (%) |
Total N (%) |
| Residents with PCR-Ct | 38 | 90 | 92 | 32 | 252 |
| Age | 85.0±6.7 | 81.9±11.6 | 84.7±8.4 | 80.4±12.0 | 83.2±10.0 |
| Female | 32(84.2) | 66(73.3) | 66(71.7) | 20(62.5) | 184(73.0) |
| Male | 6 (15.8) | 24(26.7) | 26(28.3) | 12(37.5) | 68(27.0) |
| Fist infection with PCR-Ct | 33( 86.8) | 42(46.7) | 91(98.9) | 19(59.4) | 185(73.4) |
| Reinfections with PCR-Ct | 5 (13.2) | 48 (53.3) | 1(1.1) | 13(40.6) | 67(26.6) |
| Reinfections without PCR-Ct | 2 (5.3) | 14(15.6) | 0 | 11(34.4) | 27(10.7) |
| Cycle threshold (median-range) | 23.3(17-38) | 33.5(11-39) | 27 (17-38) | 29(15-37) | 29(11-39) |
| Cycle threshold mean ± SD | 25.2±6.2 | 30.9±7.0 | 27.2±5.7 | 28.4±6.6 | 28.4±6.7 |
| Ct SARS-CoV-2 reinfections | 36.4±3.0 | 32.5±4.9 | 26.0 | 28.1±5.7 | 31.9±5.4 |
| Ct first SARS-CoV-2 infections | 23.5±4.5 | 29.0±8.5 | 27.3±5.7 | 28.6±7.3 | 27.1±6.6 |
| p-values | 0.000 | 0.016 | 0.876 | 0.820 | 0.000 |
Table 3.
Comparison of cycle thresholds ≥30 versus <30 for demographic, elapsed time from the former SARS-CoV-2 outbreak, nursing homes, and first SARS-CoV-2 infections and reinfections by Poisson regression. Crude and adjusted relative risk (cRR) and (aRR) 95% Confidence Interval (CI).
Table 3.
Comparison of cycle thresholds ≥30 versus <30 for demographic, elapsed time from the former SARS-CoV-2 outbreak, nursing homes, and first SARS-CoV-2 infections and reinfections by Poisson regression. Crude and adjusted relative risk (cRR) and (aRR) 95% Confidence Interval (CI).
| Cycle thresholds | ||||||||
| Ct ≥30 n=123(%) |
Ct<30 n=129 (%) |
Total | cRR | 95% CI | aRR | 95% CI | p-value | |
| Age1 mean±SD | 82.9±10.1 | 83.5±10.0 | - | 1.00 | 0.98-1.01 | 0.991 | 0.98-1.01 | 0.675 |
| Male2 | 32(47.1) | 36(52.9) | 68 | 0.95 | 0.64-1.42 | 0.922 | 0.59-1.42 | 0.703 |
| Female | 91(49.5) | 93(50.5) | 184 | 1.00 | 1.00 | |||
| Elapse time from former SARS-CoV-2 outbreak 3 (days) mean±SD | 427.9±86.8 | 401.7±97.3 | - | 1.00 | 0.99-1.00 | 1.003 | 1.00-1.01 | 0.031 |
| Nursing homes4 | ||||||||
| Centre 1 | ||||||||
| SARS-CoV-2 Reinfections | 5(100) | 0(0) | 5 | 6.60 | 1.91-22.80 | 6.70 | 1.80-25.0 | 0.005 |
| First SARS-CoV-2 Infections | 5(15.2) | 28(84.8) | 33 | 1.00 | ||||
| Centre 2 | ||||||||
| SARS-CoV-2 Reinfections | 39(81.3) | 9(18.8) | 48 | 1.31 | 0.80-2.16 | 1.31 | 0.80-2.15 | 0.287 |
| First SARS-CoV-2 Infections | 26(61.9) | 16(38.1) | 42 | 1.00 | ||||
| Centre 3 | ||||||||
| SARS-CoV-2 Reinfections | 0 (0) | 1(100) | 1 | 1.935 | 0.0-10.76 | 2.186 | 0.0-14.25 | 1.000 |
| First SARS-CoV-2 Infections | 33(34.1) | 58(63.7) | 91 | 1.00 | ||||
| Centre 4 | ||||||||
| SARS-CoV-2 Reinfections | 5 (38.5) | 8(61.5) | 13 | 0.73 | 0.20-2.34 | 0.70 | 0.24-2.05 | 0.513 |
| First SARS-CoV-2 Infections | 10(52.6) | 9(47.4) | 19 | 1.00 | ||||
| Total nursing homes7 | ||||||||
| SARS-CoV-2 Reinfections | 49(73.1) | 18 (26.9) | 67 | 1.83 | 1.27-2.62 | 1.66 | 1.10-2.51 | 0.015 |
| First SARS-CoV-2 Infections | 74 (40.0) | 111 (60.0) | 185 | 1.00 | 1.00 | |||
1 Adjusted for sex.2 Adjusted for age.3 Adjusted for age sex and nursing homes.4 Adjusted for age sex. 5 Exact Poisson regression. 6 Exact Poisson regression. 7 Adjusted for age sex elapsed time from former SARS-CoV-2 outbreak and nursing homes.
Table 4.
Sensitivity analysis: multinomial logistic regression. Cycle threshold groups and reinfections. Crude and adjusted odds ratios (cOR) and (aOR) 95% confidence interval (CI).
Table 4.
Sensitivity analysis: multinomial logistic regression. Cycle threshold groups and reinfections. Crude and adjusted odds ratios (cOR) and (aOR) 95% confidence interval (CI).
| Reinfections | |||||||
| Yes n=67 | No n=185 | cOR | 95% CI | aOR | 95% | p-value | |
| Cycle threshold1 | N (%) | N (%) | |||||
| Minor (<18.83) | 1 (1.5) | 19 (10.3) | 1.00 | 1.00 | |||
| Medium (≥18.83-30.10) | 17 (25.4) | 99 (53.5) | 3.26 | 0.41-26.00 | 5.98 | 0.73-49.12 | 0.096 |
| High (>30.10) | 49 (73.1) | 67 (36.2) | 13.90 | 1.80-107.33 | 17.63 | 2.22-139.86 | 0.007 |
1 Adjusted age sex elapsed time from former SARS-CoV-2 outbreak nursing homes.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



