
Submitted:
18 September 2024
Posted:
18 September 2024
You are already at the latest version
Abstract
Background:The association between ABO and Rh blood groups and diseases is an intriguing topic that continues to be studied. However, how mandibular symmetry may vary by blood group has not been investigated. This study explored the relationship between these blood groups and mandibular condyle and ramal asymmetries in the Turkish adult population.
Methods:The study included 149 adult patients (67 males and 82 females) without systemic diseases or temporomandibular disorder complaints. Asymmetry was assessed in panoramic radiographic images using a formula developed in a previous study. The chi-square and Kruskal-Wallis tests were used to analyze differences among ABO groups while the Mann-Whitney U test was used for Rh groups.
Results:There were no statistically significant differences among the ABO blood groups, nor the Rh groups, in terms of sex, Rh factor, and age distribution. However, a comparison of the ABO and Rh blood groups revealed that condylar asymmetries were significantly more common in the AB group.
Conclusions:These results suggest that mandibular asymmetry may be associated with the ABO blood group. These findings may guide future research to gain a deeper understanding of the relationship between mandibular asymmetry and blood groups.
Keywords:
Blood groups
; Condylar Asymmetry
; Ramal Asymmetry
1. Introduction
The etiology of temporomandibular disorders (TMDs) has been extensively investigated, revealing that factors, such as trauma, stress, arthritic changes resulting from systemic conditions, and parafunctional habits, can contribute to TMD symptoms. While craniofacial morphology plays a role in TMD, mandibular and facial asymmetries have also been observed in individuals without TMD symptoms. Emotional and psychological aspects may also influence the occurrence of TMD. In addition, the craniofacial morphology plays a role.[1]
Bilateral symmetry is defined as the equal distribution of parts on two sides of the body. Facial symmetry, encompassing various components, is defined as the overall harmony among these components. Conversely, asymmetry refers to the lack of this harmony. [2] Aesthetic changes in the face can significantly impact quality of life, being particularly important for young individuals, in whom appearance may directly influence social relationships. [3] Mandibular asymmetry directly influences facial appearance and can cause functional problems due to the mandible’s role in the stomatognathic system. Because condylar asymmetry is a primary cause of mandibular asymmetry, it holds great importance in terms of its impact on TMDs and facial asymmetry. Therefore, radiological evaluation of condylar asymmetry is an essential component of assessing TMD patients. [4] A method of quantifying vertical asymmetry during mandibular condylar and ramal assessment has been widely adopted by researchers. [5]
Infection or failure of condylar cartilage has been reported to cause asymmetry, with endochondral ossification and bone attachment likely to be the primary growth factors. In addition, muscle activity also has an effect on facial asymmetry, given the differences in cases of unilateral crossbite. [6]. Although studies have shown that ethnicity and gender differences have no effect on asymmetry perception, the relationship between ethnicity and gender variables and asymmetry has not been well investigated. Although racial differences have been found in dental anatomy and cranial morphology, the role of race in the pathogenesis of mandibular asymmetry has not been addressed[6].
The ABO blood grouping system categorizes blood into four groups: O, A, B, and AB. Group O produces antibodies against A and B antigens, while groups A and B have erythrocytes with A and B antigens, respectively, and produce antibodies against the opposite antigen. Group AB carries both A and B antigens, and does not form antibodies against either antigen. [7]
Blood type, a hereditary factor, is associated with various diseases.[8] The Rhesus (Rh) blood grouping system classifies blood as Rh negative or positive based on the presence of the D antigen in red blood cells (RBCs). Both the ABO and Rh blood groups have been linked to diseases, including diabetes mellitus, cardiovascular disorders, periodontal disease, infections, and cancer. RBCs play a crucial role in the inborn immune response, contributing to the emergence and maintenance of immunity. [9,10]
Several studies have investigated the relationship between ABO blood groups and various systemic diseases. Significant differences between ABO groups have been observed in studies on oral cancers, salivary gland tumors, pancreatic tumors, colitis, diabetes, and ischemic heart diseases. [11] Maxillofacial deformities can be acquired or inherited. It is clear that genetics plays an important role in inherited maxillofacial deformities. Facial development is multifactorial and this multifactoriality can make it difficult to determine the genetic pattern of deformities. Nevertheless, epidemiologic evaluations may find associations between certain deformities and certain genetic traits and contribute to the literature in terms of diagnosis and treatment. One of the most important human genetic traits is the ABO and Rh blood group systems. [12]
Panoramic radiographs The method applied by Habets et al. [5] provides an index of the height difference between the right and left condyle. The vertical component of the structures visible on these radiographs is less subject to distortion in the posterior regions than in the anterior regions, making this method sufficiently accurate. The fact that panoramic radiographs do not require high radiation doses and complex equipment, as well as their widespread use in dental practice, make them suitable for routine evaluation in the clinical setting. [13]
To our knowledge, the literature has not previously specifically examined the potential impact of various blood groups, particularly ABO and Rh blood groups, on the TMJ and surrounding anatomical structures. While the relationship between systemic diseases and blood groups has been extensively studied, including conditions affecting other parts of the body, there is a significant gap in the literature regarding the role that these genetic factors may play in maxillofacial anatomy, particularly in relation to TMJ function and structural asymmetry. Given the complex and multifactorial nature of TMJ-related disorders, it is possible that blood groups contribute to subtle anatomical variations that affect joint symmetry and consequently have an indirect effect on facial appearance and function. Our study was planned as a pilot study to fill this gap in the literature by aiming to examine the relationship between ABO and Rh blood groups and condylar and ramal asymmetry indices. In this study, we aim to conduct a detailed analysis in an adult Turkish population, focusing on individuals without TMJ disorders or facial asymmetry symptoms, and to establish a clear basis for understanding these relationships in a healthy cohort. Widely recognized and validated in the literature for the assessment of vertical asymmetry in mandibular condylar and ramal height, Habets et al. [5], this research will generate data that can serve as a basis for future studies in this area.
2. Materials and Methods
This crosectional pilot study was implemented to evaluate the demographic and radiographic data of patients referred to the Department of Oral and Maxillofacial Surgery at Harran University Faculty of Dentistry. The specific focus of this study was asymmetry index measurements on panoramic radiographs. Panoramic radiographs of 149 patients without systemic diseases, craniofacial deformity, orthodontic treatment history and also who had no TMJ-related complaints, were included. . The inclusion and exclusion criteria for the study are presented in detail in Table 1. The total study cohort included 67 male and 82 female patients as seen in Table 2 and Table 3. In order to conduct an accurate and reliable study, only patients who had panoramic film records with radiograph quality that could be used for asymmetry index calculation and whose age, gender and blood group information were recorded in the patient files were included in the final analysis. Subjects with insufficient demographic information or unsuitable panoramic images for asymmetry index measurement were excluded from the studyThe study was conducted in accordance with Harran University Clinical Research Ethics Committee (approval number: HRU/24.02.69). Thus, compliance with ethical norms was ensured.
Panoramic images were acquired using a PaX-I machine (Vatech Panoramic imaging machine, South Korea), with standardized settings of mA = 8, kVp = 60, and an exposure time of 10 seconds for consistent image quality. The images were evaluated using EasyDent software (version 4.1.5.9), is a software that contains the parameters used in the calculation of asymmetry, such as calibration, measurement and angulation.
To evaluate the anatomical structures needed for mandibular asymmetry measurements the most distal points of the mandibular condylar process and mandibular ramus were identified and marked as points A and B, respectively, and after this a straight reference line (X) was drawn between these points. In order to analyze the condylar height correctly a perpendicular line (Y) was drawn from the uppermost point of the condyle on either side, intersecting the X line at point C as illustrated in Figure 1. Condyle height (CH) was measured as the distance between points C and A, and ramal height (RH) as the distance between points A and B. These measurements were consistently performed by the same investigator to avoid measurement variability. the measurements were also performed in a blinded manner, ensuring that the investigator was unaware of patient details to minimize potential bias. The calibration tool provided by EasyDent software was used to improve accuracy throughout the measurement process. To calculate mandibular condylar and ramal asymmetries, we used the Habets formula, which is based on radiographic data, widely used and accepted in the literature.[5] A detailed illustration of the measurement method is presented in Figure 1 and Figure 2.
Statistical analysis was performed using SPSS Statistics version 20.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics were calculated, and the significance level was set at p < 0.05 for all tests. The normality of the condylar asymmetry index (CAI) and ramal asymmetry index (RAI) variables was tested using the Kolmogorov-Smirnov test. Chi-square tests were used to analyze the sex and Rh factor prevalence in ABO blood groups. The Kruskal-Wallis test was used to assess differences among ABO blood groups, while the Mann-Whitney U test was used for Rh groups.
3. Results
The Ethics Committee of Harran University reviewed and granted approved the study protocol and procedures with confirming adherence to the required ethical standards (approval number: HRU/24.02.69). The study sample consisted of 149 panoramic radiographs carefully selected from a total of 67 male and 82 female patients. These patients were not related to symmetry or temporomandibular joint (TMJ). The patient selection criteria aimed to minimize factors that might influence patients' index to asymmetry.
CAI, RAI, and age variables were were statistically analyzed to assess their distribution patterns by using the Kolmogorov-Smirnov test, which indicated that they did not follow a normal distribution and also the need for nonparametric statistical analyses to ensure the robustness and accuracy of the results.
Table 2 and 3 provides a detailed breakdown of the descriptive statistics and the results of the statistical analyses for the patients in each group. Sex distribution, Rh distribution, and patient ages across the ABO groups were analyzed using chi-square and nonparametric tests, revealing no statistically significant differences among the groups. These tables (tables 2 and 3) not only summarize key demographic variables, but also highlight specific findings regarding asymmetry indices between different blood groups and indicate which statistical tests were used.
The distribution of gender, Rh factor and patient age among the various ABO blood groups was analyzed using the chi-square test for categorical variables and the nonparametric Kruskal wallis tests for numerical variables. The analyses showed that there were no statistically significant differences in these demographic variables between ABO blood groups, indicating a balanced distribution of these variables. However, comparisons of asymmetry indices between different ABO blood groups revealed significant differences in relation to CAI that reached statistical significance, suggesting that blood group may be an important factor in condylar asymmetry (p < 0.05). In particular, pairwise comparisons revealed that patients of blood group AB exhibited significantly higher CAI values compared to those of blood group B. In contrast to the results for ABO blood groups, analyses within Rh groups did not reveal a statistically significant difference in CAI or RAI.
4. Discussion
Although several studies have evaluated the relationship between condylar asymmetry and occlusal asymmetry, TMJ diseases, and crossbite, the relationship between condylar asymmetry and the ABO and Rh blood groups has not previously been investigated.[14] Asymmetrical use can lead to asymmetrical mandibular development. In addition, asymmetries between the sides of the mandible may result from an adaptive response, leading to condylar remodeling.[15]
The incidence of TMD is higher in individuals with asymmetries, indicating that asymmetry may be a significant factor in TMD development.[16] Mandibular asymmetry can be assessed using several different methods, including panoramic radiographic evaluation, which has frequently been used in previous studies. [17] Panoramic radiographs offer advantages, such as low cost and low radiation exposure, but they also have limitations due to magnification risks, distortion, and superimposition of anatomical structures. [17,18]
Cone-beam computed tomography is considered the gold standard for assessing mandibular asymmetries.[16] However, its disadvantages include limited use in routine dental imaging, high radiation dose, and high cost. Therefore, we utilized panoramic radiographs. This was the first study to investigate the relationship between the ABO and Rh blood groups and vertical condylar and ramal asymmetry using the method of Habets et al.[5]
Lundstrom [20] classified the possible causes of facial and dental arch asymmetries as genetic, environmental, or a combination of these factors. Autoimmune diseases and inflammatory conditions have also been associated with TMDs.[21] The ABO system is the most widely used blood grouping system. Other important blood grouping systems include the Rh and MN systems. The clinically significant and widely used ABO and Rh systems are determined based on the nature of different proteins found at the surfaces of RBCs. [11]
The genes encoding ABO and Rh blood group antigens are located on chromosomes 9q34.2 and 1p36.11, respectively. Several studies have demonstrated a relationship between certain rheumatic and autoimmune diseases and blood groups. Two studies that evaluated pemphigus vulgaris, an autoimmune condition, found no significant relationship with ABO blood groups.[22] Glycoconjugate structures on RBCs have various functions, including roles as receptors, transporters, channels, structural proteins, adhesion molecules, and enzymes. Although the exact mechanisms explaining the relationships between blood group antigens and adhesion molecules are not fully understood, these may play a role in disease processes. [23]
Such structures also play active roles in cell physiology and pathology. Despite the significant association between ABO blood groups and various diseases, there are controversies regarding resistance to certain diseases due to the absence of antigens in some groups. The presence or absence of these antigens is associated with health and disease. Such antigens are not only found in RBCs but also in leukocytes, platelets, plasma proteins, and enzymes. They can also be present in soluble form in body fluids such as sweat, saliva, amniotic fluid, and urine. [24,25,26,27]
The presence or absence of A/B antigens affects host defense against infection. Although many studies have demonstrated a relationship between ABO blood groups and diseases, some researchers have published contradictory findings. Non-O blood groups are generally more susceptible to diseases compared to O blood groups.[23]
The relationship between ABO blood groups and a variety of diseases warrants further investigation. A meta-analysis of 17 relevant studies reported a statistically significant difference between the AB group and other blood groups in terms of periodontitis.[28] However, there were no differences for gingivitis, and inconsistencies were noted among the studies. The authors emphasized the need for further studies with larger samples.
In Kundu et al.,[26] the incidence of aggressive periodontitis was higher in individuals with the AB blood group. We similarly found a higher rate of condylar asymmetry in such patients. We believe that the presence of both A and B antigens in the AB group may explain this outcome.
There may be a relationship between blood groups and periodontal and dental diseases. Individuals with AB type blood are less resistant to childhood caries.[30,31] This finding corresponds with the higher rates of condylar asymmetry in the AB group observed in our study. However, further research using comprehensive and homogeneous study groups is needed to investigate the association between blood group types and diseases.
In our study, homogeneity was ensured by the balanced distribution of sexes and ages across the groups, which did not result in significant differences. We believe that our findings regarding the relationship between blood groups and condylar asymmetry address an unexplored area in the literature, potentially providing a foundation for future studies.
The inconsistencies among studies may be due to varying methodologies as well as to geographical and genetic influences of blood groups in different populations.[32]
In a study of oropharyngeal and oral cancer cases, a positive correlation was noted between blood groups A and AB and cancer incidence. [33] The authors attributed this to the immunological properties of cancer cell antigens, which resemble those of blood group A. In individuals with blood group O, these antigens may inhibit tumor growth, offering a protective mechanism. Individuals with blood types A and AB, who lack A antibodies, may be at greater risk for carcinomas.
When comparing the right- and left-sided CH and RH values across ABO and Rh blood groups, no differences were observed between the Rh groups. However, a statistically significant difference was found among the ABO groups, with significantly higher asymmetry scores in the AB group. The absence of differences between Rh groups and the similarity in sex, age, and Rh group distributions among the ABO groups indicate the homogeneity of our study population, enhancing the reliability of our comparisons.
ABO antigens are thought to be evolutionarily useful for conferring resistance to pathogens. [34] A and B antigens are mostly secreted by cells and are present in the human bloodstream. Groups that do not secrete antigens are considered at greater risk for various infections. [35] In our study, the higher asymmetry index in AB group patients may be attributable to the synthesis of both antigen groups in these patients. However, the effects of these antigens on condylar resorption need to be supported by cellular studies. The lack of a significant difference in ramal asymmetry values may be explained by the absence of ramal resorption.
TMDs have a multifactorial etiology, including psychological components. Psychological studies have shown that TMD patients exhibit psychological dysfunctions similar to those seen in other chronic musculoskeletal pain disorders. [36] A study on psychiatric patients found that the frequency of psychiatric disorders in individuals with the AB blood group was almost three times higher than in other blood groups. Nitric oxide excretion is faster in individuals with the B and AB blood types, and neurotransmitters may be responsible for depression and other psychiatric disorders due to their critical functions. [37] The high rates of condylar asymmetry in AB group individuals found in our study may be related to the psychological profiles of these patients, suggesting the need for further studies to evaluate the psychological status of individuals with different ABO blood groups.
A clinical cross-sectional study reported higher preoperative anxiety levels in individuals with the AB blood group compared to other blood groups. [38] The authors attributed the results to the role of glycosyltransferases, which catalyze ABO blood group antigens. Different glycosyltransferase activities are observed in different blood groups, and these enzymes play a role in the neuroinflammatory response. They are also reported to be important in nerve injury repair and regeneration through the glycosylation of glycoproteins in Schwann cells.
The strengths of our study include the similarity of gender and age distributions of patient blood groups, the fact that our study is a subject that has never been addressed in the literature before, the measurement of condylar and ramal asymmetries by software and calibration, and the selection of patients free of factors that may affect mandibular asymmetry. However, our study was conducted on panoramic images and with a relatively limited sample size. Similar detailed studies on the subject are needed in more crowded populations.
5. Conclusions
Due to the lack of previous studies investigating condylar and ramal asymmetries across different blood groups, comparisons of our results were not possible. Overall, these results provide important insights into the relationship between blood groups and asymmetry indices in a population without TMJ complaints, history of systemic disease and orthodontic treatment. The statistically significant differences observed between AB and B blood groups in relation to condylar asymmetry suggest that blood type may be a factor influencing anatomical variations in the mandible. The study findings also highlight the complexity of maxillofacial asymmetry, which may be influenced by a combination of genetic and environmental factors. Further studies are needed to confirm these findings and determine the mechanism underlying the association between blood group and mandibular asymmetry.
Author Contributions
Author Contributions:“Conceptualiza tion, M.E.P. and H.I.D.; methodology, M.E.P; software, M.G.; validation, M.E.P., H.I.D. and M.G.; formal analysis, M.E.P.; investigation, M.E.P; resources, M.E.P., H.I.D. and M.G.; data curation, M.G.; writing—original draft preparation, M.G.; writing—review and editing, M.E.P., H.I.D. and M.G.; visualization, M.E.P., H.I.D. and M.G.; supervision, H.I.D.;All authors have read and agreed to the published version of the manuscript.”, please turn to the CRediT taxonomy for the term explanation. Authorship must belimited to those who have contributed substantially to the work reported.
Funding
There is no funding.
Institutional Review Board Statement
Ethics committee approval was obtained from the Harran University Clinical Research Ethics Committee (approval number: HRU/24.02.69).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
We encourage all authors of articles published in MDPI journals to share their research data. In this section, please provide details regarding where data supporting reported results can be found, including links to publicly archived datasets analyzed or generated during the study. Where no new data were created, or where data is unavailable due to privacy or ethical restrictions, a statement is still required. Suggested Data Availability Statements are available in section “MDPI Research Data Policies” at https://www.mdpi.com/ethics. Acknowledgments: In this section you can acknowledge any support given which is not covered by the author contribution or funding sections. This may include administrative and technical support, or donations in kind (e.g., materials used for experiments).
Conflicts of Interest
None declared.
Abbreviations:
The following abbreviations are used in this manuscript:
| TMDs: | temporomandibular disorders |
| RH: | The Rhesus |
| RBCS: | Red Blood Cells |
| TMJ: | Temporomandibular Joint |
| CH: | Condyle Height |
| RH: | Ramal Height |
| CAI: | Condylar Asymmetry Index |
| RAI: | Ramal Asymmetry Index |
References
- Sfondrini, M.F.; Bolognesi, L.; Bosco, M.; Gandini, P.; Scribante, A. Skeletal divergence and condylar asymmetry in patients with temporomandibular disorders (TMD): A retrospective study. BioMed Res. Int. 2021, 1, 8042910. [Google Scholar] [CrossRef]
- Halicioglu, K.; Celikoglu, M.; Buyuk, S.K.; Sekerci, A.E.; Candirli, C. Effects of early unilateral mandibular first molar extraction on condylar and ramal vertical asymmetry. Eur. J. Dent. 2014, 8, 178–183. [Google Scholar] [CrossRef] [PubMed]
- Dikson, C.; Traebert, J. Malocclusion, dental aesthetic self-perception and quality of life in a 18 to 21 year-old population: A cross section study. BMC Oral. Health 2013, 13, 1–6. [Google Scholar]
- Sezgin, O.S.; Celenk, P.; Arici, S. Mandibular asymmetry in different occlusion patterns. Angle Orthod. 2007, 77, 803–807. [Google Scholar] [CrossRef] [PubMed]
- Habets, L.L.; Bezuur, J.N.; Naeiji, M.; Hansson, T.L. The orthopantomogram, an aid in diagnosis of temporomandibular joint problems. II. The vertical symmetry. J. Oral. Rehabil. 1988, 15, 465–471. [Google Scholar] [CrossRef] [PubMed]
- Hikosaka, Y.; Koizumi, S.; Kim, Y.I.; Adel, M.; Nadim, M.; Hikita, Y.; Yamaguchi, T. Comparison of Mandibular Volume and Linear Measurements in Patients with Mandibular Asymmetry. Diagnostics 2023, 13, 1331. [Google Scholar] [CrossRef]
- Mostafa, D.; Elkhatat, E.I.; Koppolu, P.; Mahgoub, M.; Dhaifullah, E.; Hassan, A.H. Correlation of ABO Blood Groups and Rh Factor with The Severity of Generalized Chronic Periodontitis: Across Sectional Study in Riyadh, Saudi Arabia. Open Access Maced. J. Med. Sci. 2019, 7, 617–622. [Google Scholar] [CrossRef]
- Watins, W.M. ABO blood group system: Historical background. Transfus. Med. 2001, 11, 243–265. [Google Scholar] [CrossRef] [PubMed]
- Salem, G.I.; Gamal, N.M.; Talaat, E.A.; El-Hammady, D.H.; Hammam, N.; Gheita, T.A. Clinical Impact of the ABO Blood Type in Patients with Rheumatic Diseases: Is there a Link to the ABO and Rhesus? Mediterr J Rheumatol 2021, 32, 237–242. [Google Scholar] [CrossRef] [PubMed]
- Anderson, H.L.; Brodsky, I.E.; Mangalmurti, N.S. The Evolving Erythrocyte: Red Blood Cells as Modulators of Innate Immunity. J. Immunol. Baltim. Md. 1950 2018, 201, 1343–1351. [Google Scholar] [CrossRef] [PubMed]
- Gautam, A.; Mittal, N.; Singh, T.B.; Srivastava, R.; Verma, P.K. Correlation of ABO blood group phenotype and rhesus factor with periodontal disease: An observational study. Contemp. Clin. Dent. 2017, 8, 253. [Google Scholar] [CrossRef] [PubMed]
- Gheisari, R.; Ghoreishian, M.; Movahedian, B.; Roozbehi, A. The association between blood groups and maxillofacial deformities. Indian. J. Plast. Surg. 2008, 41, 138–140. [Google Scholar] [CrossRef] [PubMed]
- Tortarolo, A.; Rotolo, R.; Nucci, L.; Tepedino, M.; Crincoli, V.; Piancino, M.G. Condylar asymmetry in children with unilateral posterior crossbite malocclusion: A comparative cross-sectional study. Children 2022, 9, 1772. [Google Scholar] [CrossRef] [PubMed]
- Polat, M.; Odabası, O. Can cystic lesions of the jaws be considered as the cause of mandibular asymmetry? Med. Oral. Patol. Oral. Cir. Bucal. 2022, 27, e159–e163. [Google Scholar] [CrossRef] [PubMed]
- Pirttiniemi, P.; Kantomaa, T. Relation of glenoid fossa morphology to mandibulofacial asymmetry, studied in dry human Lapp skulls. Acta Odontol. Scand. 1992, 50, 235–243. [Google Scholar] [CrossRef] [PubMed]
- Almășan, O.; Leucuța, D.C.; Buduru, S. Disc Displacement of the Temporomandibular Joint and Facial Asymmetry in Children and Adolescents: A Systematic Review and Meta-Analysis. Child. (Basel) 2022, 9, 1297. [Google Scholar] [CrossRef]
- Yanez-Vico, R.M.; Iglesias-Linares, A.; Torres-Lagares, D.; Gu tierrez-Perez, J.L.; Solano-Reina, E. Three-dimensional evaluation of craniofacial asymmetry: An analysis using computed tomography. Clin. Oral. Investig. 2011, 15, 729–736. [Google Scholar] [CrossRef] [PubMed]
- Celik, S.; Celikoglu, M.; Buyuk, S.K.; Sekerci, A.E. Mandibular vertical asymmetry in adult orthodontic patients with different vertical growth patterns: A cone beam computed tomography study. Angle Orthod. 2016, 271–277. [Google Scholar] [CrossRef]
- Sanders, D.A.; Rigali, P.H.; Neace, W.P.; Uribe, F.; Nanda, R. Skeletal and dental asymmetries in Class II subdivision malocclusions using cone-beam computed tomography. Am. J. Orthod. Dentofac. Orthop. 2010, 138, e1–e20. [Google Scholar] [CrossRef]
- Lundstrom, A. Some asymmetries of the dental arches, jaws, and skull, and their etiological signifi cance. Am. J. Orthod. Dentofac. Orthop. 1961, 47, 81–106. [Google Scholar] [CrossRef]
- Staniszewski, K.; Lygre, H.; Berge, T.; Rosén, A. Serum Analysis in Patients with Temporomandibular Disorders: A Controlled Cross-Sectional Study in Norway. Pain. Res. Manag. 2019, 1360725. [Google Scholar] [CrossRef]
- Islamoğlu, Z.G.K.; Unal, M. Is there an association of ABO blood groups and Rhesus factor with alopecia areata? J. Cosmet. Dermatol. 2018, 17, 1271–1274. [Google Scholar] [CrossRef]
- Abegaz, S.B. Human ABO Blood Groups and Their Associations with Different Diseases. Biomed. Res. Int. 2021, 6629060. [Google Scholar] [CrossRef]
- Abdulganiyu. Distribution of ABO and Rh (D) blood groups and associated traits: A study of the College of Nursing and Midwifery. Msc Thesis, Dissertation, Kogi State, Obangede, 2016.
- Chandra, T.; Gupta, A. Association and distribution of hypertension, obesity and ABO blood groups in blood donors Iranian. J. Paediatr. Haematol. Oncol. 2012, 2, 140–145. [Google Scholar]
- Ewaldand, R.; Sumner, S. Blood type biochemistry and human disease,” Wiley Interdisciplinary Reviews. Syst. Biol. Med. 2016, 8, 571–35. [Google Scholar]
- Daniels, G. Human Blood Groups. In Blackwell Science, Oxford, 2nd edition, 2002.
- Al-Askar, M. Is there an association between periodontal diseases and ABO blood group? Systematic review and meta-analysis. Quintessence Int. 2022, 53, 404–412. [Google Scholar] [CrossRef]
- Kundu, D.; Bandyopadhyay, P.; Nair, V.; Chowdhury, M.; Mukherjee, S.; Nayek, M. Aggressive periodontitis: A clinico-hematological appraisal. J. Indian. Soc. Periodontol. 2014, 18, 166–171. [Google Scholar] [CrossRef]
- Solanki, J.; Dileep, C.L.; Adyanthaya, B.R.; Mishra, P.; Yadav, O. Association betweengn different blood groups, depression and oral health status of dental students. Clujul Med. 2018, 91, 317–321. [Google Scholar] [CrossRef]
- Alsadat-Hashemipour, M.; Tahmasbi-Arashlow, M.; Fahimi-Hanzaei, F. Incidence of impacted mandibular and maxillary third molars-a radiographic study in a Southeast Iran population. Medicina Oral, Patologia Oral y Cirurgia Bucal 2013, 18, e140–5. [Google Scholar] [CrossRef] [PubMed]
- Koregol, A.; Raghavendra, M.; Nainegali, S.; Kalburgi, N.; Varma, S. ABO blood groups and Rhesus factor: An exploring link to periodontal diseases. Indian J. Dent. Res. 2010, 21, 364. [Google Scholar] [CrossRef] [PubMed]
- Aditi, P. Assessment of Relationship of ABO-RH Blood Group in Oral Cancer Patients: A Prospective Cohort Study of Hospital Patients. Int. J of Life Sci., Biotechnology and Pharma Research 2023, 2, 1661–1671. [Google Scholar]
- Than, N.G.; Romero, R.; Meiri, H.; Erez, O.; Xu, Y.; Tarquini, F.; Barna, L.; Szilagyi, A.; Ackerman, R.; Sammar, M.; et al. PP13, Maternal ABO Blood Groups and the Risk Assessment of Pregnancy Compli cations. PLoS ONE 2011, 7, e21564. [Google Scholar]
- Naeini, A.E.; Rostami, M.; Naeini, S.E. Chronic viral hep atitis and their relation to ABO blood groups and rhesus (Rh) factor. Med. Case Stud. 2010, 1, 5–7. [Google Scholar]
- Anna, S.; Stelcer, B.; Roy, M. Is there a relationship between psychological factors and TMD? Brain Behav. 2019, 9, e01360. [Google Scholar]
- Pisk, S.V.; Vuk, T.; Ivezic, E.; Jukic, I.; Bingulac-Popovic, J.; Filipcic, I. ABO blood groups and psychiatric disorders: A Croatian study. Blood Transfus. 2019, 17, 66–71. [Google Scholar] [CrossRef]
- Xu, F.; Yin, J.W.; Xiong, E.F.; He, H.; Zhang, Q.T.; Fan, S.W.; Qin, X.L.; Wang, S. Correlation between Preoperative Anxiety and ABO Blood Types: Evidence from a Clinical Cross-Sectional Study. Disease Markers 2019, 1761693. [Google Scholar] [CrossRef]
Figure 1.
Habet’s Formula for Asymmetry.
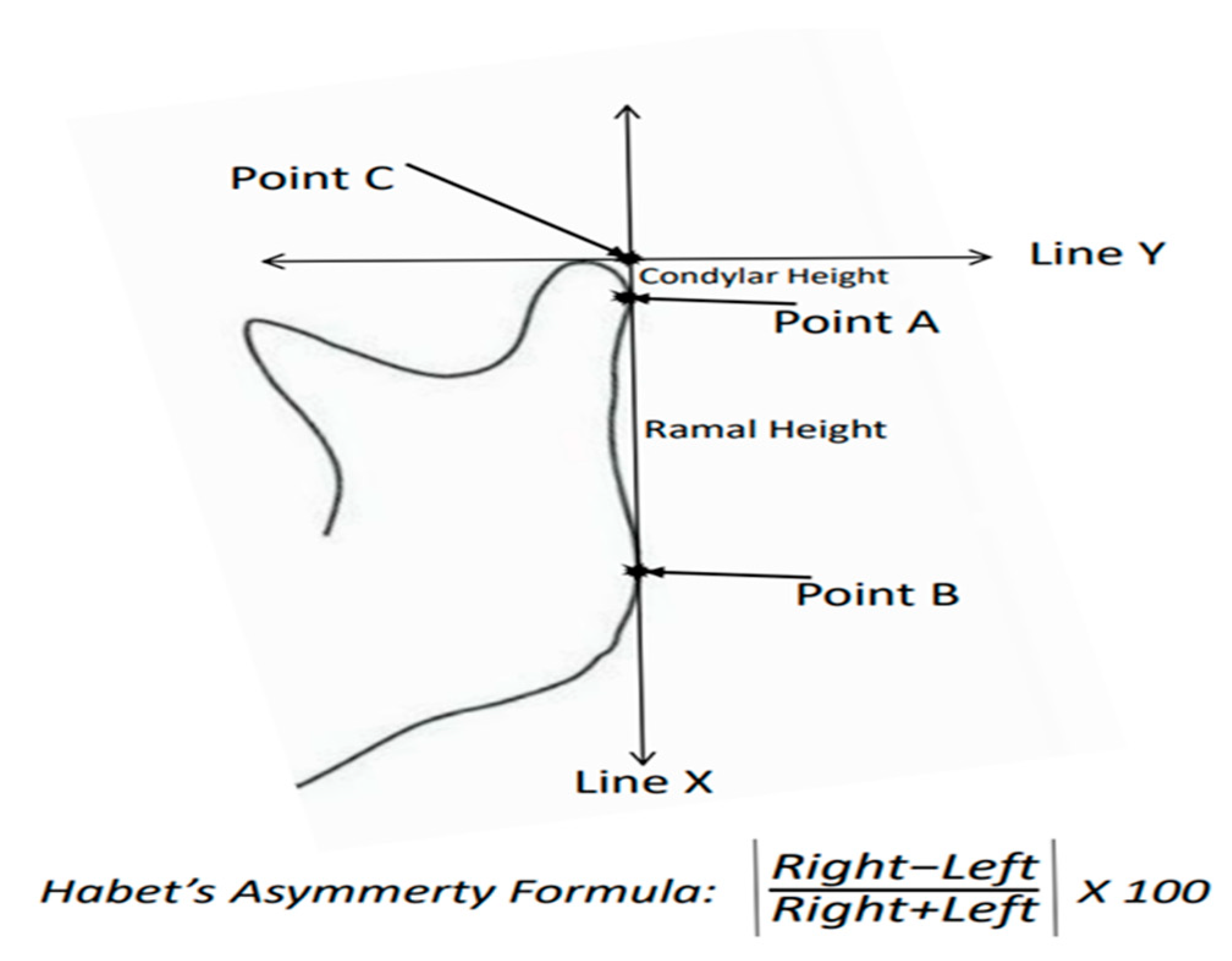
Figure 2.
A panoramic drawing for Habet’s formula calculation.
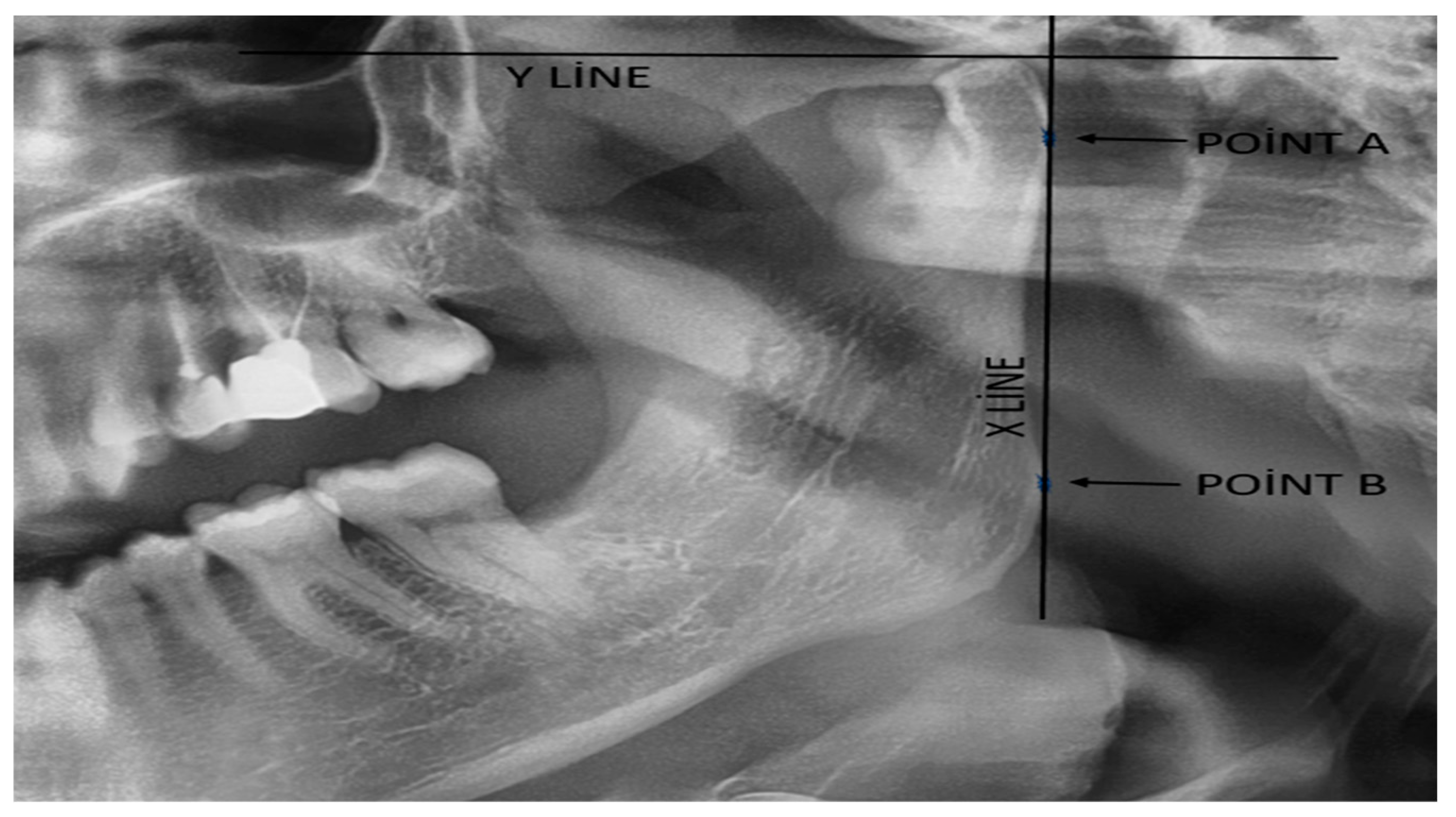

Table 1.
Intrusion and Exclusuion Criteria.
| Intrusion Criteria | Exclusuion Criteria |
|---|---|
| Age ≥ 18 years | Age < 18 years |
| Suitable panoramic film quality (for asymmetry index calculation) | Unsuitable panoramic film quality (for asymmetry index calculation) |
| Complete demographic information (age, gender, blood type) | Inomplete demographic information (age, gender, blood type) |
| systemic disease free | Presence of systemic diseases (e.g., diabetes, autoimmune diseases). |
| craniofacial deformity free | craniofacial deformity presence (congenital or acquired) |
| No orthodontic treatment history. | History of orthodontic treatment or current orthodontic appliances. |
| TMJ complaint free | TMJ-related complaint presence |
| Inconsistent or incomplete patient records. |
Table 2.
Statistical analyse for ABO Groups.
| ABO groups | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| A | B | AB | O | P value | |||||
| Sex distrubution | Male | Female | Male | Female | Male | Female | Male | Female | ,613 a |
| 26 | 28 | 12 | 11 | 6 | 12 | 23 | 31 | ||
| Age distrubution | 26,12±7.38 | 26,69±7,81 | 31,33±11,66 | 28,12±7,32 | ,148 b | ||||
| Condylar asymmetry score | 9,82±11,86 x y | 7,33±6,46 y | 13,60±9,79 x | 9,40±9,95 x y | ,044 c | ||||
| Ramal asymmetry score | 5,45±13,51 | 3,15±3,00 | 3,45±2,35 | 2,79±3,51 | ,344 b | ||||
| a Chi square test b Kruskal Wallis test c Kruskal Wallis test with pairwise comparison inculding Bonferroni correction | |||||||||
Table 3.
Statistical analyse for RH Groups.
| RH Groups | |||||
|---|---|---|---|---|---|
| Rh + | Rh - | P value | |||
| Sex distrubution | Male | Female | Male | Female | ,744 a |
| 43 | 76 | 4 | 6 | ||
| Age distrubution | 27,81±8,13 | 30,30±7,97 | ,109 b | ||
| Condylar asymmetry score | 9,99±10,56 | 6,18±3,78 | ,371 b | ||
| Ramal asymmetry score | 3,97±8,84 | 2,79±2,16 | ,952 b | ||
| a Chi square test b Mann Whitney U test | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



