
Submitted:
19 September 2024
Posted:
20 September 2024
You are already at the latest version
Abstract
Objectives: This study examined the effects of kinesio tape (KT) on the rectus femoris muscle under pre- and post-fatigue conditions, with trained and novice participants. Methods: Nineteen male volunteers took part, and fatigue was assessed using the Borg CR10 Scale. Kinematic and kinetic data were collected using Vicon MX13+ infrared cameras (250 Hz) and Kistler force platforms (1500 Hz), respectively. Visual 3D software analyzed the data, focusing on parameters like angular displacement, ground reaction forces (GRF), impulse, and joint moments during a stop-jump task. A two-way mixed-design ANOVA was used to assess group, fatigue, and KT effects. Results: The results showed significant differences in knee flexion range of motion (ROM), hip flexion moment, vertical impulse, and peak vertical GRF between pre- and post-fatigue conditions (all p < 0.05). The trained group exhibited less knee valgus ROM, higher hip flexion velocity at initial contact, and prolonged time to peak proximal tibia anterior shear force. Conclusions: KT application was found to reduce lower limb loading, improve force acceptance and joint stability, and alleviate fatigue-induced disparities. These findings highlight the potential of KT in enhancing lower limb strength and performance, particularly under fatigue.
Keywords:
quadriceps
; lower limb
; performance enhancement
; athletic training
; exercise physiology
1. Introduction
The rupture of the Anterior Cruciate Ligament (ACL) is a serious injury commonly seen in sports involving landing or jumping [1,2]. Notably prevalent in disciplines volleyball, basketball, and handball [3,4], ACL injuries are documented to arise predominantly from non-contact maneuvers, constituting over 70% of reported cases [5]. These incidents frequently occur during landing sequences characterized by rapid deceleration or abrupt changes in direction [3,5]. Recent research highlights the role of neuromuscular fatigue in worsening ACL injury susceptibility [6,7]. Supporters of the "fatigue theory" [6,8,9] suggest that fatigue reduces muscle strength, alters lower limb muscle activation patterns, and disrupts hip and knee kinematics. This cascade of effects can increase ground reaction forces during landing or cutting maneuvers, correlating with a higher frequency of non-contact ACL injuries, particularly in later athletic stages [10].
In sports with jumping, the landing phase of the stop jump task poses a significant risk to lower limb injuries, especially the anterior cruciate ligament (ACL) [11]. This vulnerability arises from the unique mechanics of rapid deceleration followed by a jump, increasing anterior tibial shear force [12] and potentially exceeding the ACL's load-bearing capacity [6], thereby raising the risk of ACL injury. Some literature suggests that greater muscle strength and knee joint mobility contribute to reducing ground reaction forces (GRF) on the ACL during the stop jump task [13,14]. Fatigue-induced muscle weakness can disrupt lower limb joint mechanics, increasing ACL injury risk during the stop jump [8,9,15]. xcessive dynamic knee valgus [16], poor trunk control [16,17], excessive knee flexion [17], and high ground reaction forces (6) also heighten ACL injury susceptibility. Therefore, strategies to prevent fatigue or improve joint stability during the stop jump task are crucial for reducing sports-related injuries.
Amidst similar physical exertion levels, ACL injury susceptibility rises with prolonged exercise. Athletes often use Kinesio-taping (KT) to reduce joint loading or delay fatigue onset. KT is widely used in sports medicine and rehabilitation to treat musculoskeletal issues [18], It helps by expanding range of motion, reducing pain, and supporting joint and muscle function [19]. Numerous studies suggest that KT can bolster muscle activation in healthy athletes, augment muscle reaction speed, and refine proprioception [20,21]. Nonetheless, the efficacy of KT in terms of enhancing muscle strength and joint mobility remains contentious [22,23,24]. Furthermore, its effectiveness may be influenced by intangible placebo effects [25] and other factors such as experiment design, KT application techniques, or participant population demographics [26].
Previous research has primarily focused on immediate impacts of KT, leaving gaps in understanding its sustained efficacy after fatigue. Definitive evidence on its effects across diverse demographic groups is lacking [27]. While KT shows promise in postoperative scenarios, its impact on lower limb muscle function in healthy individuals is unclear [24,26]. This study aims to compare KT effects on athletes and novice students under fatigue. We hypothesize that KT will mitigate biomechanical disruptions in lower limb kinetics and kinematics during the stop-jump task post-fatigue.
2. Materials and Methods
Nine Division II-level basketball players (age: 21.7 ± 1.55; height: 176.95 ± 5.07; weight: 69.55 ± 5.85) who underwent regular training sessions of approximately 3 hours per day for 5 days a week, and ten healthy students (age: 20.1 ± 0.83; height: 176.78 ± 3.58; weight: 72.33 ± 5.52) who engaged in regular exercise for approximately 1.5 hours a day for 3 days a week were recruited and assigned to the trained and novice groups, respectively. The number of participants for each group was determined based on pilot data using G*Power software version 3.1.9.7 (ES=0.61, α = 0.05, and β = 0.2)[28]. All participants had no history of orthopedic or neurological issues or lower limb injuries. Additionally, they reported no discomfort during the testing procedures. Written consent was obtained from each participant, and the study was conducted in accordance with the guidelines approved by the Human Ethics Committee of Taiwan Normal University.
Two conditions were examined: one involving the application of KT on the rectus femoris muscle and the other without KT application in each fatiguing scenario. The independent variables included the fatiguing condition (pre- and post-fatigue) and the presence of KT application (with- and without-KT) in the two groups. To evaluate the effects of the KT intervention, the experiment was carried out on two separate days. Prior to task performance and data collection, participants underwent warm-up exercises, consisting of a 5-minute treadmill run at 6 km/hour followed by a 5-minute dynamic stretching protocol for the major muscle groups of the lower extremities. Participants were given time to familiarize themselves with the stop-jump task before formal testing commenced. The fatiguing protocol involved consecutive vertical jumps performed for 90 seconds (1 jump per second) until the participants reached a state of volitional exhaustion, following the method described by Bosco, et al. [29]. A set was terminated if a subject failed to maintain the metronome pace for five consecutive beeps or was unable to continue with the task. Verbal encouragement was consistently provided during the protocol to encourage maximal effort. Upon completion of the fatigue protocol, subjects' perceived exertion levels were assessed using the Borg CR10 Scale [30]. Eeach subject was required to rate their perceived exertion at least at level 7 on the Borg Scale to be considered fatigued. Certified athletic trainers applied Kinesio tape to each subject, extending from the anterior inferior iliac spine to the tibial tuberosity, using a total tape length at 120% tension, with two I-shaped stickers covering the rectus femoris (see Figure 1) on both legs. Jump trials were repeated five times for each condition, with a 1-minute rest period between trials.
Kinematic data were captured using 10 infrared cameras operating at a frequency of 250 Hz (Vicon MX13+; Oxford Metrics Ltd., Oxford, UK), while kinetic data were gathered using two force platforms operating at a frequency of 1500 Hz (Kistler 9260AA6; Instruments, Inc., Winterthur, Switzerland). Fifty-three reflective markers were strategically positioned to track eight rigid segments representing the kinematics of the lower extremities. These markers were placed on specific anatomical landmarks, including left and right skull temples, left and right acromioclavicular joint, medial and lateral condyles of the elbow, centers of the upper arm and forearm, inside and outside of the wrist joint, second palm of the hand, seventh section of the spine, thoracic seventh section, clavicle, xiphoid and right back, anterior iliac spine and posterior superior iliac spine, greater trochanter, lateral thigh and lateral calf, medial and lateral condyles of the knee joint, medial and lateral condyles of the ankle, medial metatarsal head, proximal second metatarsal head, lateral metatarsal head, and heel. Subsequently, kinematic and kinetic data were processed using Visual 3D software (C-motion, Rockville, MD, USA). The 3D trajectories of the markers and ground reaction force (GRF) data were filtered using a fourth-order zero-lag Butterworth digital filter with cut-off frequencies set at 10 Hz for marker trajectories [31] and 50 Hz for GRF data.
Anatomical reference frames for the body segments were established with clarity: the positive x-axis (medial/lateral) directed towards the right, the positive y-axis (anterior/posterior) oriented forwards, and the positive z-axis (superior/inferior) directed upwards. The landing phase was defined as the period from the initial ground contact (IC) to the attainment of maximum knee flexion angle was reached, while the take-off phase was spanned from the maximum knee flexion angle to the moment of take-off. Variables were analyzed for the leg that made initial ground contact (the first touchdown leg). Dempster's normative anthropometric data were utilized to determine limb segment masses and moments of inertia [32]. Angular displacement, GRF, impulse, and joint moments were calculated to quantify biomechanical parameters indicative of ACL loading during the stop-jump task. Kinetic data were normalized to the participant’s body weight.
This study provided the participants' demographics and various parameters using descriptive statistics (mean ± standard deviation). Statistical analysis was conducted using SPSS 18.0 software (SPSS, Inc., Chicago, IL). A two-way mixed-design analysis of variance (ANOVA) was utilized, incorporating four within-subject factors: pre-fatigue, post-fatigue, and KT application on both pre and post-fatigue conditions, alongside one between-subjects factor, group (comprising trained and novice subjects). This analysis aimed to assess the effects of KT, fatigue, group, and their interactions on all jump parameters. Bonferroni post hoc analysis was utilized to compare means differences among conditions. Shapiro-Wilk test was utilized to assess the normality of data distribution. Statistical significance was considered for p-values less than 0.05. Effect sizes were determined using partial eta-squared (η²), with values of η²= 0.01 indicating a small effect, η²= 0.06 denoting a moderate effect, and η² = 0.14 signifying a large effect [33].
3. Results
Table 1 presents the outcomes of interactions and group differences for key biomechanical variables. No significant interaction was detected between groups and intervention. However, significant main effects between interventions were observed for knee flexion range of motion (ROM), peak hip flexion moment, horizontal impulse in the first 50 ms after IC, vertical impulse in breaking phase, peak vertical GRF, breaking time, push off time, total time, and jump height (all p < 0.05).
Bonferroni post hoc analysis was employed to further examine biomechanical variables related to kinematics (Figure 2), kinetics (Figure 3), and ground contact time (Figure 4). It revealed that knee flexion ROM, hip peak flexion moment, vertical impulse during the breaking phase, and peak vertical GRF were significantly greater in post-fatigue compared to pre-fatigue conditions (all p < 0.05).
Table 2 presents the evaluations of pre-to-post changes with the application of KT intervention concerning major biomechanical variables in both trained and novice individuals (refer to Figure 5 and Figure 6). A statistically significant decrease in knee valgus ROM was observed within the trained group (p = 0.027, η2 = 0.257, power = 0.629). Additionally, compared to the novice group, the trained cohort demonstrated a significantly higher hip flexion velocity at IC (p = 0.050, η2 = 0.208, power = 0.513) and a prolonged time to reach peak proximal tibia anterior shear force (p = 0.010, η2 = 0.328, power = 0.774).
4. Discussion
The present study aimed to scrutinize the impact of KT on the stop-jump task subsequent to a fatigue-inducing intervention, comparing outcomes between professional athletes and typical college students. Findings unveiled that post-fatigue, the 'stop-jump task' prompted escalated lower limb loading and expanded joint range of motion, coupled with prolonged push-off duration. Nonetheless, application of kinesiology tape demonstrated a mitigated loading response, prolonged force absorption during ground contact, and augmented joint stability. While Csapo and Alegre [26] have underscored KT's limited capacity to bolster muscle strength in healthy cohorts, our study illuminates its potential efficacy within the realm of human physical activity, particularly when fatigue serves as an intervention.
In the examination of kinematic variables, an increase in knee flexion range of motion was evident under the post-fatigue condition, aligning with prior research indicating fatigue-induced increases in knee joint range of motion [17,34], thereby elevating injury risk. Notably, when assessing KT application, no significant disparities emerged between pre- and post-fatigue conditions. This suggests that KT application of indeed contributes to maintaining superior knee joint flexion performance, potentially reducing injury occurrence [23]. Furthermore, in the inter-group comparison during the stop-jump process, the training group displayed a smaller knee valgus range and a faster initial hip flexion velocity, indicative of enhanced knee joint stability. However, in the post-test following fatigue and KT intervention, no statistical differences were noted in knee and hip joint kinematic parameters. This implies that the use of KT may assist in mitigating the discrepancies in knee valgus angles due to varying skill levels or fatigue effects [35], thereby reinforcing KT's stabilizing effect on knee joint dynamics among novice individuals and under fatigue conditions.
Following fatigue induction, elevated stress loading was evident, encompassing parameters such as peak hip flexion moment, horizontal impulse in the initial 50 ms post-initial contact, vertical impulse in the breaking phase, and peak vertical ground reaction force. Subsequent to KT intervention, a discernible reduction in lower limb stress was noted. These findings collectively underscore that integrating KT during the post-fatigue stop-jump task effectively mitigates lower limb loading, thereby diminishing the susceptibility to ACL injuries. While prior research has indicated the ineffectiveness of KT in enhancing muscle strength in healthy individuals or young athletes [22,26], and some argue that the tactile input from KT may affect central nervous system excitability [36]. Its purported limited impact on optimizing movement control contrasts with the current findings. In this study, KT application demonstrated significant benefits in lower limb muscle strength and performance post-fatigue, resulting in a substantial reduction in loading across multiple aspects of lower limb stress. This observation diverges from previous findings [22], suggesting that, in the context of fatigue, KT may indeed play a significant role in influencing lower limb biomechanics and performance. Such effects could be crucial in mitigating the impact of fatigue on the lower limbs and reducing the likelihood of injuries, particularly concerning ACL injuries.
Regarding stop-jump motion technique analysis, noteworthy distinctions emerged in breaking time, push-off time, total time, and jump height between fatigue conditions in the present study. Upon closer examination, it became apparent that the primary discernible distinctions originated from the fatigue intervention. Interestingly, the application of KT resulted in a reduction in breaking time and an increase in push-off time, potentially enhancing jump performance. However, these effects did not manifest within the scope of the current study. In the overall execution of the stop-jump motion, both total time and jump height were significantly influenced by the fatigue intervention, while the utilization of KT failed to yield notable differences. This concurs with consistent findings from previous research, suggesting that the effects of KT on athletic performance may fall short of anticipated expectations [23,24,25]. Even if there are discernible influences, they may not exert a substantial impact on performance behaviors.
There are limitations that necessitate careful consideration in the present study. Firstly, it is pivotal to acknowledge that KT application was confined solely to the rectus femoris muscle, prompting concerns regarding the extrapolation of observed effects to other muscle groups. Second, the absence of specific performance tests for participant stratification into trained and novice groups introduces a level of variability that necessitates caution in drawing definitive conclusions. Third, the study primarily focuses on acute effects, offering immediate insights into KT application and fatigue. Nevertheless, the sustainability of these effects over an extended period remains uncertain, emphasizing the need for longitudinal investigations. Fourth, while the incorporation of consecutive vertical jumps in the fatiguing protocol is relevant, it may not wholly replicate typical athletic scenarios, potentially compromising the ecological validity of the study.
5. Conclusions
This study explored the influence of KT on the stop-jump task following fatigue in trained and novice college students. At post-fatigue, the stop-jump task induced heightened lower limb loading and joint range of motion. The application of KT yielded a significant reduction in loading, prolonged force absorption during ground contact, and enhanced joint stability, particularly in maintaining superior knee joint flexion performance. Notably, the trained group exhibited enhanced knee joint stability with a smaller knee valgus range and faster hip flexion velocity during the stop-jump. Nonetheless, post-fatigue and KT intervention failed to reveal significant differences in knee and hip joint kinematics, suggesting KT's potential in mitigating skill-level or fatigue-induced disparities. Moreover, KT intervention led to a notable decrease in lower limb stress, including peak hip flexion moment and ground reaction forces, underscoring its effectiveness in alleviating lower limb loading and reducing the risk of ACL injuries. This study unveiled substantial benefits of KT in enhancing lower limb muscle strength and performance post-fatigue. Despite limitations such as exclusive KT application to the rectus femoris muscle and potential participant grouping variability, these findings offer insights into the advantageous role of KT in human physical activity, particularly under conditions of fatigue.
Author Contributions
Conceptualization, C.-Y.T. and C.-Y.T.; methodology, C.-F.H.; investigation, C.-Y.T.; data curation, C.-Y.T. and C.-Y.T.; writing—original draft preparation, C.-Y.T. and C.-Y.T.; writing—review and editing, W.-H.T. and H.-T.P.; project administration, C.-F.H. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of National Taiwan Normal University, for studies involving humans.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
All data generated or analysed during this study are included in this published article.
Acknowledgments
This project was supported by the Educational Science Research Project of Fujian Province (No. JAT220269); and the Social Science Foundation of Fujian Province (No. FJ2023T011).
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Fortington, L.V.; Donaldson, A.; Finch, C.F. Self-reported worst injuries in women's Australian football identify lower limb injuries as a prevention priority. BMJ Open Sport—Exercise Medicine 2016, 2. [Google Scholar] [CrossRef] [PubMed]
- Ardern, C.L.; Webster, K.E.; Taylor, N.F.; Feller, J.A. Return to sport following anterior cruciate ligament reconstruction surgery: a systematic review and meta-analysis of the state of play. British journal of sports medicine 2011. [Google Scholar] [CrossRef] [PubMed]
- Griffin, L.Y.; Agel, J.; Albohm, M.J.; Arendt, E.A.; Dick, R.W.; Garrett, W.E.; Garrick, J.G.; Hewett, T.E.; Huston, L.; Ireland, M.L. Noncontact anterior cruciate ligament injuries: risk factors and prevention strategies. JAAOS-Journal of the American Academy of Orthopaedic Surgeons 2000, 8, 141–150. [Google Scholar] [CrossRef]
- Renstrom, P.; Ljungqvist, A.; Arendt, E.; Beynnon, B.; Fukubayashi, T.; Garrett, W.; Georgoulis, T.; Hewett, T.E.; Johnson, R.; Krosshaug, T. Non-contact ACL injuries in female athletes: an International Olympic Committee current concepts statement. British journal of sports medicine 2008, 42, 394. [Google Scholar] [CrossRef]
- Boden, B.P.; Sheehan, F.T. Mechanism of non-contact ACL injury: OREF Clinical Research Award 2021. Journal of Orthopaedic Research® 2022, 40, 531–540. [Google Scholar] [CrossRef] [PubMed]
- Benjaminse, A.; Webster, K.E.; Kimp, A.; Meijer, M.; Gokeler, A. Revised approach to the role of fatigue in anterior cruciate ligament injury prevention: a systematic review with meta-analyses. Sports medicine 2019, 49, 565–586. [Google Scholar] [CrossRef]
- Smeets, A.; Vanrenterghem, J.; Staes, F.; Vandenneucker, H.; Claes, S.; Verschueren, S. Are ACL reconstructed athletes more vulnerable to fatigue than uninjured athletes? Medicine and Science in Sports and Exercise 2020, 52, 345–353. [Google Scholar] [CrossRef]
- Kernozek, T.W.; Torry, M.R.; Iwasaki, M. Gender differences in lower extremity landing mechanics caused by neuromuscular fatigue. The American journal of sports medicine 2008, 36, 554–565. [Google Scholar] [CrossRef]
- Benjaminse, A.; Habu, A.; Sell, T.C.; Abt, J.P.; Fu, F.H.; Myers, J.B.; Lephart, S.M. Fatigue alters lower extremity kinematics during a single-leg stop-jump task. Knee Surgery, Sports Traumatology, Arthroscopy 2008, 16, 400–407. [Google Scholar] [CrossRef]
- Xu, D.; Zhou, H.; Quan, W.; Gusztav, F.; Wang, M.; Baker, J.S.; Gu, Y. Accurately and effectively predict the ACL force: Utilizing biomechanical landing pattern before and after-fatigue. Computer Methods and Programs in Biomedicine 2023, 241, 107761. [Google Scholar] [CrossRef]
- Yu, B.; Lin, C.-F.; Garrett, W.E. Lower extremity biomechanics during the landing of a stop-jump task. Clinical biomechanics 2006, 21, 297–305. [Google Scholar] [CrossRef] [PubMed]
- DeMorat, G.; Weinhold, P.; Blackburn, T.; Chudik, S.; Garrett, W. Aggressive quadriceps loading can induce noncontact anterior cruciate ligament injury. The American journal of sports medicine 2004, 32, 477–483. [Google Scholar] [CrossRef] [PubMed]
- Nagai, T.; Sell, T.C.; House, A.J.; Abt, J.P.; Lephart, S.M. Knee proprioception and strength and landing kinematics during a single-leg stop-jump task. Journal of athletic training 2013, 48, 31–38. [Google Scholar] [CrossRef]
- Schmitz, R.J.; Kulas, A.S.; Perrin, D.H.; Riemann, B.L.; Shultz, S.J. Sex differences in lower extremity biomechanics during single leg landings. Clinical biomechanics 2007, 22, 681–688. [Google Scholar] [CrossRef]
- Wojtys, E.M.; Beaulieu, M.L.; Ashton-Miller, J.A. New perspectives on ACL injury: on the role of repetitive sub-maximal knee loading in causing ACL fatigue failure. Journal of Orthopaedic Research® 2016, 34, 2059–2068. [Google Scholar] [CrossRef]
- Kristianslund, E.; Faul, O.; Bahr, R.; Myklebust, G.; Krosshaug, T. Sidestep cutting technique and knee abduction loading: implications for ACL prevention exercises. British journal of sports medicine 2013. [Google Scholar] [CrossRef]
- Donnelly, C.; Elliott, B.C.; Ackland, T.R.; Doyle, T.L.; Beiser, T.F.; Finch, C.F.; Cochrane, J.; Dempsey, A.R.; Lloyd, D. An anterior cruciate ligament injury prevention framework: incorporating the recent evidence. Research in sports medicine 2012, 20, 239–262. [Google Scholar] [CrossRef] [PubMed]
- Griebert, M.C.; Needle, A.R.; McConnell, J.; Kaminski, T.W. Lower-leg Kinesio tape reduces rate of loading in participants with medial tibial stress syndrome. Physical therapy in sport 2016, 18, 62–67. [Google Scholar] [CrossRef]
- Williams, S.; Whatman, C.; Hume, P.A.; Sheerin, K. Kinesio taping in treatment and prevention of sports injuries: a meta-analysis of the evidence for its effectiveness. Sports medicine 2012, 42, 153–164. [Google Scholar] [CrossRef]
- Wu, C.-K.; Lin, Y.-C.; Lai, C.-P.; Wang, H.-P.; Hsieh, T.-H. Dynamic taping improves landing biomechanics in young volleyball athletes. International Journal of Environmental Research and Public Health 2022, 19, 13716. [Google Scholar] [CrossRef]
- Mao, H.-Y.; Hu, M.-T.; Yen, Y.-Y.; Lan, S.-J.; Lee, S.-D. Kinesio Taping Relieves Pain and Improves Isokinetic Not Isometric Muscle Strength in Patients with Knee Osteoarthritis—A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health 2021, 18, 10440. [Google Scholar] [CrossRef]
- Collins, K.S.; Smedley, K.; Riegel, H.; Christensen, B.; Lyman, K. EFFECT OF TWO KINESIO TAPE TECHNIQUES ON KNEE KINEMATICS DURING A DROP JUMP TEST. ISBS Proceedings Archive 2022, 40, 126. [Google Scholar]
- Yam, M.L.; Yang, Z.; Zee, B.C.-Y.; Chong, K.C. Effects of Kinesio tape on lower limb muscle strength, hop test, and vertical jump performances: a meta-analysis. BMC Musculoskeletal Disorders 2019, 20, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Lu, Z.; Li, X.; Chen, R.; Guo, C. Kinesio taping improves pain and function in patients with knee osteoarthritis: A meta-analysis of randomized controlled trials. International Journal of Surgery 2018, 59, 27–35. [Google Scholar] [CrossRef]
- Poon, K.Y.; Li, S.M.; Roper, M.; Wong, M.; Wong, O.; Cheung, R. Kinesiology tape does not facilitate muscle performance: A deceptive controlled trial. Manual therapy 2015, 20, 130–133. [Google Scholar] [CrossRef] [PubMed]
- Csapo, R.; Alegre, L.M. Effects of Kinesio® taping on skeletal muscle strength—A meta-analysis of current evidence. Journal of Science and Medicine in Sport 2015, 18, 450–456. [Google Scholar] [CrossRef]
- Boobphachart, D.; Manimmanakorn, N.; Manimmanakorn, A.; Thuwakum, W.; Hamlin, M.J. Effects of elastic taping, non-elastic taping and static stretching on recovery after intensive eccentric exercise. Research in Sports Medicine 2017, 25, 181–190. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G* Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behavior research methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Bosco, C.; Komi, P.; Tihanyi, J.; Fekete, G.; Apor, P. Mechanical power test and fiber composition of human leg extensor muscles. European journal of applied physiology and occupational physiology 1983, 51, 129–135. [Google Scholar] [CrossRef]
- Borg, G. Psychophysical scaling with applications in physical work and the perception of exertion. Scandinavian journal of work, environment & health 1990, 55-58.
- Yu, B.; Gabriel, D.; Noble, L.; An, K.-N. Estimate of the optimum cutoff frequency for the Butterworth low-pass digital filter. Journal of Applied Biomechanics 1999, 15, 318–329. [Google Scholar] [CrossRef]
- Dempster, W.T. Space requirements of the seated operator: geometrical, kinematic, and mechanical aspects of the body with special reference to the limbs; Wright Air Development Center Wright-Patterson Air Force Base, Ohio: 1955; Volume 159.
- Cohen, J. Statistical power analysis for the behavioral sciences; Academic press: 2013.
- Yu, P.; Gong, Z.; Meng, Y.; Baker, J.S.; István, B.; Gu, Y. The acute influence of running-induced fatigue on the performance and biomechanics of a countermovement jump. Applied Sciences 2020, 10, 4319. [Google Scholar] [CrossRef]
- Sheikhi, B.; Letafatkar, A.; Hogg, J.; Naseri-Mobaraki, E. The influence of kinesio taping on trunk and lower extremity motions during different landing tasks: implications for anterior cruciate ligament injury. Journal of Experimental Orthopaedics 2021, 8, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Raza, A.; Zaki, S.; Alam, M.F.; Sharma, S.; Aysha, T.; Khiyami, A.T.; Althobaiti, A.J.; Alnefaie, H.A.; Nuhmani, S. Effects of facilitatory and inhibitory Kinesio taping on lateral gastrocnemius muscle activity, motor neuron excitability, and countermovement jump height in university athletes from multiple sports: A randomized controlled trial. Heliyon 2023, 9. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Application Protocol of Kinesio Tape on the rectus femoris.

Figure 2.
Bonferroni post hoc analysis of kinematics; KT, kinesio-taping; preF, per-fatigue; postF, post-fatigue; p < 0.05.
Figure 2.
Bonferroni post hoc analysis of kinematics; KT, kinesio-taping; preF, per-fatigue; postF, post-fatigue; p < 0.05.
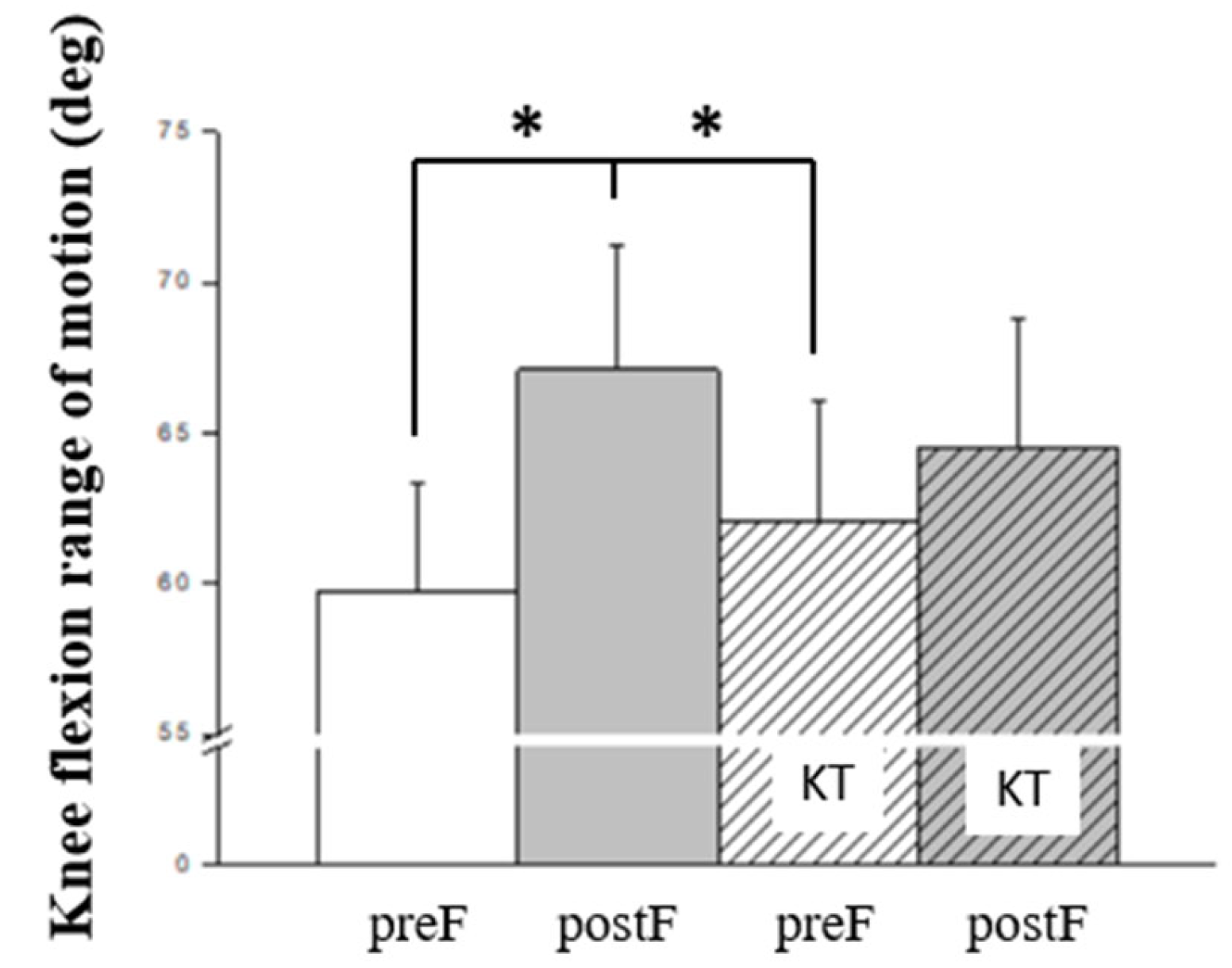
Figure 3.
Bonferroni post hoc analysis of kinetics; (A) Peak vertical GRF; (B) Vertical impulse in breaking phase; (C) Horizontal impulse before 50ms; (D) Hip-peak flexion moment. GRF, ground reaction force; KT, kinesio-taping; preF, per-fatigue; postF, post-fatigue; p < 0.05.
Figure 3.
Bonferroni post hoc analysis of kinetics; (A) Peak vertical GRF; (B) Vertical impulse in breaking phase; (C) Horizontal impulse before 50ms; (D) Hip-peak flexion moment. GRF, ground reaction force; KT, kinesio-taping; preF, per-fatigue; postF, post-fatigue; p < 0.05.
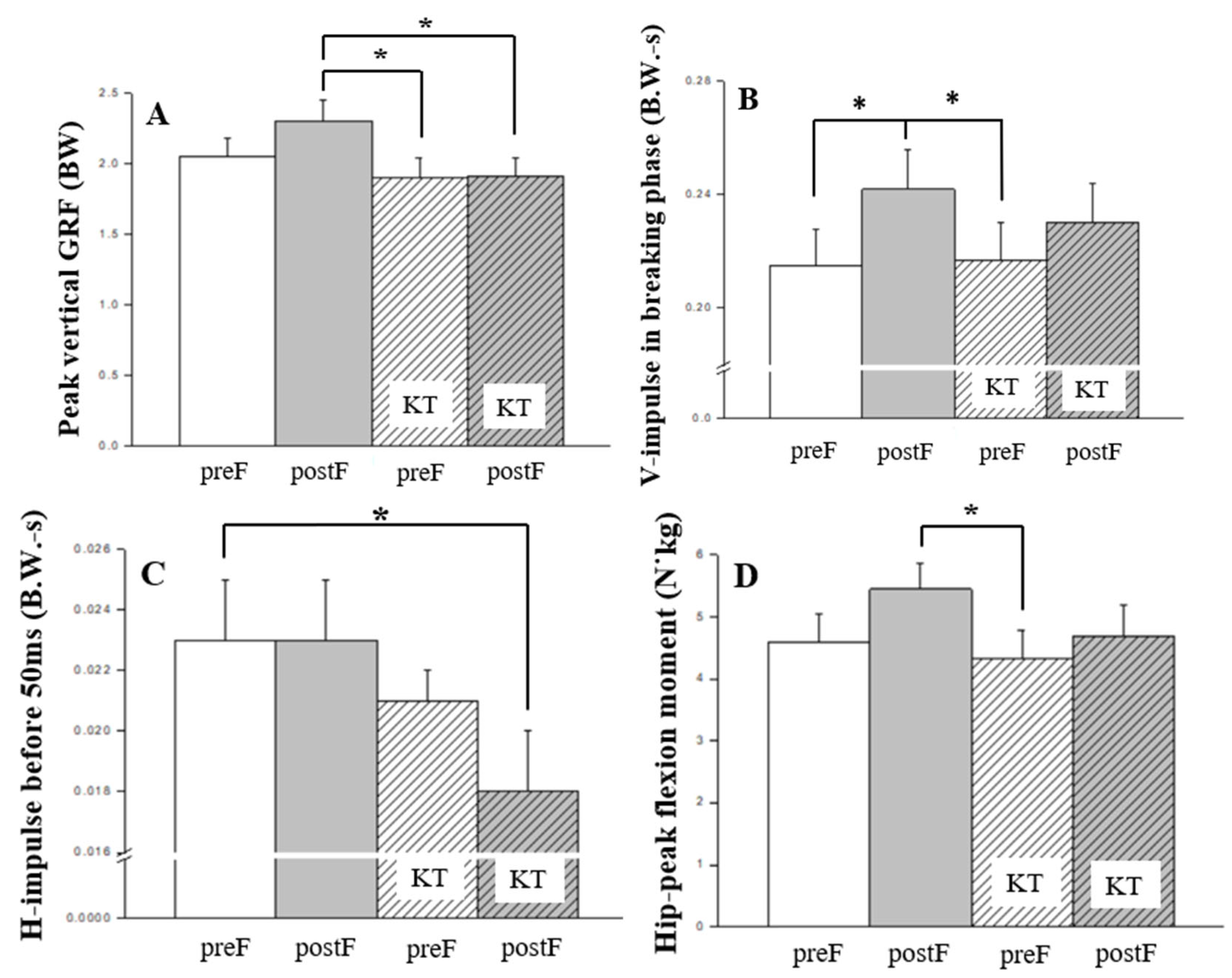
Figure 4.
Bonferroni post hoc analysis of ground contact time; (A) Breaking time; (B) Push off time; (C) Total time. KT, kinesio-taping; preF, per-fatigue; postF, post-fatigue; p < 0.05.
Figure 4.
Bonferroni post hoc analysis of ground contact time; (A) Breaking time; (B) Push off time; (C) Total time. KT, kinesio-taping; preF, per-fatigue; postF, post-fatigue; p < 0.05.
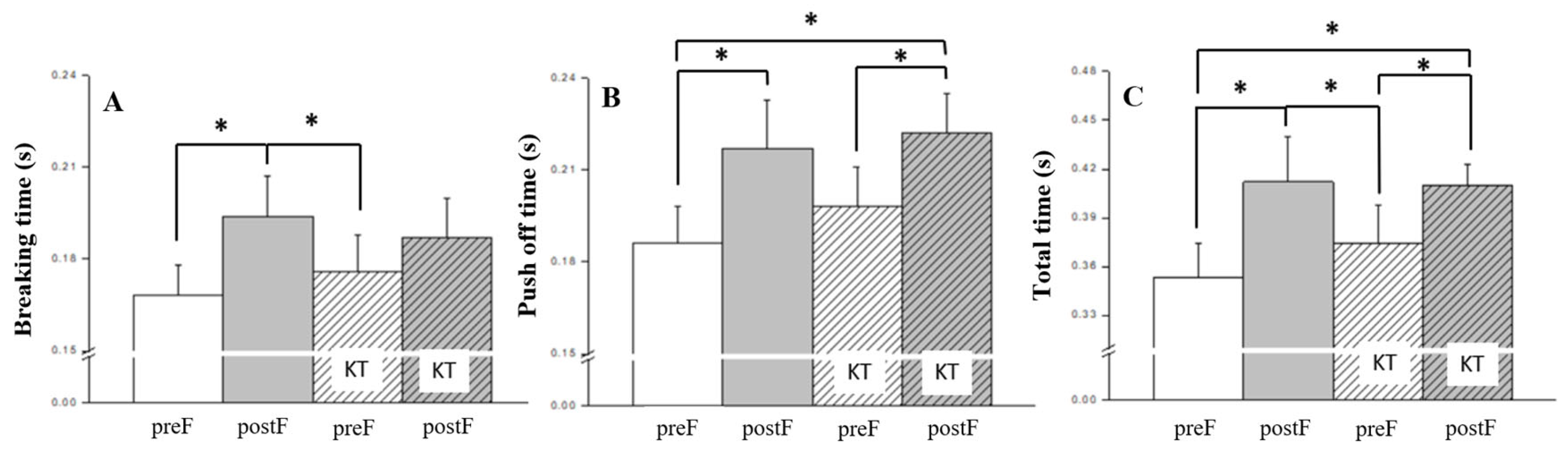
Figure 5.
The kinematics variables that significant differences between novices and trained; (A) Knee valgus range of motion; (B) Hip flexion velocity at IC. IC, initial ground contact; p < 0.05.
Figure 5.
The kinematics variables that significant differences between novices and trained; (A) Knee valgus range of motion; (B) Hip flexion velocity at IC. IC, initial ground contact; p < 0.05.
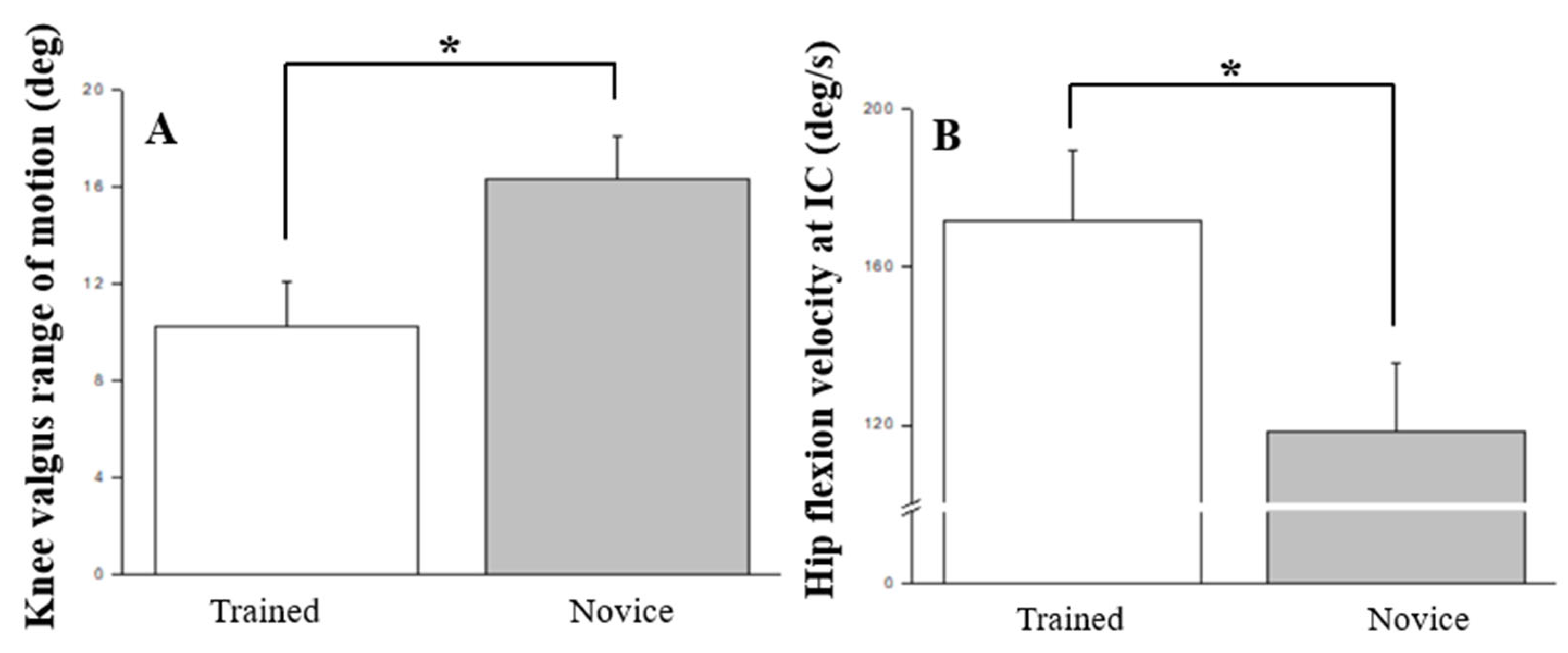
Figure 6.
The kinetic variables that significant differences between novices and trained; ASF, anterior shear force; p < 0.05.
Figure 6.
The kinetic variables that significant differences between novices and trained; ASF, anterior shear force; p < 0.05.
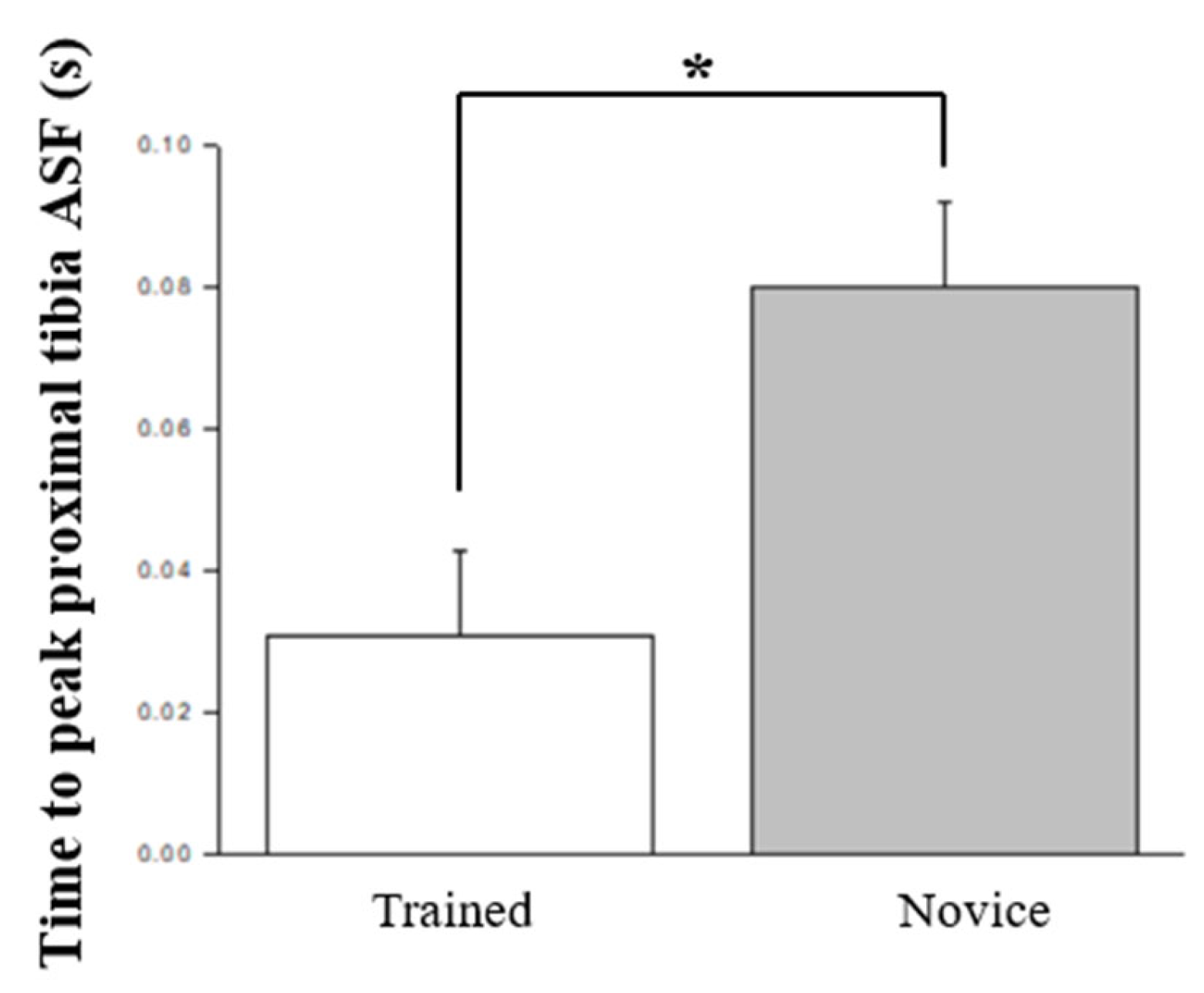

Table 1.
Two-way mixed-design ANOVA analysis for key biomechanical variables in the stop jump task.
| Major biomechanical variables | main effects | interaction | |||
| p | η2 | p | η2 | ||
| kinematics | Hip- flexion angle at IC (deg) | 0.111 | 0.123 | 0.266 | 0.075 |
| Knee- flexion angle at IC (deg) | 0.223 | 0.084 | 0.352 | 0.060 | |
| Hip-peak flexion angle (deg) | 0.312 | 0.065 | 0.347 | 0.060 | |
| Knee-peak flexion angle (deg) | 0.085 | 0.121 | 0.287 | 0.071 | |
| Knee flexion range of motion (deg)* | 0.015 | 0.184 | 0.735 | 0.024 | |
| Knee Valgus range of motion (deg) | 0.395 | 0.056 | 0.959 | 0.006 | |
| Knee internal rotation range of motion (deg) | 0.419 | 0.049 | 0.438 | 0.047 | |
| Hip-flexion velocity at IC (deg/s) | 0.394 | 0.056 | 0.979 | 0.004 | |
| Knee-flexion velocity at IC (deg/s) | 0.649 | 0.031 | 0.696 | 0.028 | |
| Hip-peak flexion velocity (deg/s) | 0.422 | 0.053 | 0.379 | 0.058 | |
| Knee-peak flexion velocity (deg/s) | 0.921 | 0.009 | 0.744 | 0.042 | |
| kinetics | Hip-peak flexion moment (N/kg)* | 0.017 | 0.179 | 0.179 | 0.091 |
| Knee-peak flexion moment (N/kg) | 0.219 | 0.087 | 0.831 | 0.007 | |
| Peak knee anterior force (N/kg) | 0.067 | 0.161 | 0.667 | 0.019 | |
| Horizontal impulse in the first 50 ms after IC (BW/s)* | 0.046 | 0.162 | 0.803 | 0.014 | |
| Vertical impulse in the first 50 ms after IC (BW/s) | 0.060 | 0.134 | 0.699 | 0.027 | |
| Horizontal impulse in breaking phsae (BW/s) | 0.251 | 0.352 | 0.781 | 0.116 | |
| Vertical impulse in breaking phsae (BW/s)* | 0.002 | 0.246 | 0.990 | 0.002 | |
| Peak horizontal GRF (BW) | 0.106 | 0.128 | 0.863 | 0.007 | |
| Peak vertical GRF (BW)* | 0.000 | 0.352 | 0.862 | 0.094 | |
| performance | Time to peak proximal tibia anterior shear force (s) | 0.133 | 0.111 | 0.203 | 0.089 |
| Time to peak knee extension moment (s) | 0.838 | 0.415 | 0.399 | 0.049 | |
| Breaking time (s)* | 0.001 | 0.325 | 0.780 | 0.021 | |
| Push off time (s)* | 0.002 | 0.294 | 0.217 | 0.085 | |
| Total time (s)* | 0.001 | 0.354 | 0.392 | 0.054 | |
| Jump height (m)* | 0.000 | 0.618 | 0.908 | 0.004 | |
*p < 0.05. IC refers to initial ground contact, BW stands for body weight, and GRF represents ground reaction force.
Table 2.
Pre-to-post changes in key biomechanical variables with kinesio tape intervention for trained and novice Individuals.
Table 2.
Pre-to-post changes in key biomechanical variables with kinesio tape intervention for trained and novice Individuals.
| Major biomechanical variables | trained | novice | F | p | η2 | power | |
| Kinematics | Hip flexion angle at IC (deg) | 61.75 ± 4.25 | 49.65 ± 4.03 | 4.279 | 0.054 | 0.201 | 0.497 |
| Knee flexion angle at IC (deg) | 36.25 ± 3.16 | 30.69 ± 3.00 | 1.628 | 0.219 | 0.087 | 0.226 | |
| Hip peak flexion angle (deg) | 82.03 ± 5.81 | 69.90 ± 5.51 | 2.298 | 0.148 | 0.119 | 0.299 | |
| Knee peak flexion angle (deg) | 103.08 ± 7.72 | 93.10 ± 7.33 | 0.880 | 0.361 | 0.049 | 0.144 | |
| Knee flexion range of motion (deg) | 64.28 ± 5.42 | 62.44 ± 5.14 | 0.061 | 0.809 | 0.004 | 0.056 | |
| Knee valgus range of motion (deg) * | 10.24 ± 1.83 | 16.35 ± 1.73 | 5.888 | 0.027 | 0.257 | 0.629 | |
| Knee internal rotation range of motion (deg) | 19.06 ± 2.85 | 23.85 ± 2.71 | 1.488 | 0.239 | 0.080 | 0.210 | |
| Hip flexion velocity at IC (deg/s) * | 171.52 ± 18.23 | 118.47 ± 17.29 | 4.459 | 0.050 | 0.208 | 0.513 | |
| Knee flexion velocity at IC (deg/s) | 330.91 ± 34.98 | 273.23 ± 33.18 | 1.431 | 0.248 | 0.078 | 0.204 | |
| Hip peak flexion velocity (deg/s) | 330.29 ± 37.26 | 350.77 ± 35.35 | 0.159 | 0.695 | 0.009 | 0.066 | |
| Knee-peak flexion velocity (deg/s) | 800.68 ± 67.92 | 685.13 ± 64.43 | 1.524 | 0.233 | 0.082 | 0.214 | |
| Kinetics | Hip-peak flexion moment (N/kg) | 5.03 ± 0.58 | 4.50 ± 0.55 | 0.440 | 0.516 | 0.025 | 0.096 |
| Knee-peak flexion moment (N/kg) | 2.79 ± 0.34 | 3.24 ± 3.23 | 0.919 | 0.351 | 0.051 | 0.148 | |
| Peak knee anterior force (N/kg) | 12.40 ± 1.38 | 11.98 ± 1.31 | 0.050 | 0.826 | 0.003 | 0.055 | |
| Horizontal impulse before 50ms (BW/s) | 0.021 ± .002 | 0.021 ± .002 | 0.075 | 0.788 | 0.004 | 0.058 | |
| Vertical impulse before 50ms (BW/s) | 0.058 ± 0.01 | 0.055 ± 0.01 | 0.182 | 0.672 | 0.011 | 0.069 | |
| Horizontal impulse in breaking phsae (BW/s) | 0.09 ± 0.01 | 0.08 ± 0.01 | 0.159 | 0.695 | 0.009 | 0.066 | |
| Vertical impulse in breaking phsae (BW/s) | 0.23 ± 0.02 | 0.22 ± 0.02 | 0.416 | 0.527 | 0.024 | 0.094 | |
| Peak horizontal GRF (BW) | 0.877 ± 0.082 | 0.809 ± 0.878 | 0.364 | 0.554 | 0.021 | 0.088 | |
| Peak vertical GRF (BW) | 2.077 ± 0.189 | 2.004 ± 0.179 | 0.080 | 0.781 | 0.005 | 0.058 | |
| Performance | Time to peak proximal tibia anterior shear force (s) * | 0.031 ± 0.012 | 0.080 ± 0.012 | 8.286 | 0.010 | 0.328 | 0.774 |
| Time to peak knee extension moment (s) | 0.064 ± 0.009 | 0.075 ± 0.008 | 0.768 | 0.393 | 0.043 | 0.131 | |
| Breaking time (s) | 0.176 ± 0.016 | 0.187 ± 0.016 | 0.198 | 0.662 | 0.011 | 0.070 | |
| Push off time (s) | 0.203 ± 0.20 | 0.208 ± 0.19 | 0.030 | 0.865 | 0.002 | 0.053 | |
| Total time (s) | 0.379 ± 0.035 | 0.395 ± 0.034 | 0.106 | 0.749 | 0.006 | 0.061 | |
| Jump height (m) | 0.468 ± 0.038 | 0.395 ± 0.036 | 1.891 | 0.187 | 0.100 | 0.255 |
* p < 0.05. IC refers to initial ground contact, BW stands for body weight, and GRF represents ground reaction force.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



