
Submitted:
19 September 2024
Posted:
22 September 2024
You are already at the latest version
Abstract
This study presents a systematic review to evaluate the effectiveness of virtual patients in enhancing clinical reasoning skills in medical education, utilizing a hybrid methodology that combines human reviewers and ChatGPT. By analyzing various studies involving conversational virtual patients, the review examines the impact of these digital tools on student learning outcomes and satisfaction. Consistent with previous systematic reviews, our findings suggest that conversational virtual patients can improve clinical competencies, particularly in history-taking and clinical reasoning. Regarding student feedback, satisfaction tends to be higher when virtual patients’ interactions are more realistic, often due to the use of artificial intelligence (AI) and natural language processing (NLP) in the simulators. Furthermore, the study compares the accuracy of AI-driven reviews with human assessments, revealing comparable results. This research highlights AI’s potential to complement human expertise in academic evaluations, contributing to more efficient and consistent systematic reviews in rapidly evolving educational fields.
Keywords:
virtual patients
; medical education
; clinical reasoning
; ChatGPT
1. Introduction
1.1. Objective and Scope of This Article
The primary objective of this article is to conduct a systematic review of the literature on the use of virtual patients in medical education. Virtual patients, which are computer-based programs simulating real-life clinical scenarios, represent a significant advancement in digital education aimed at enhancing clinical reasoning skills among medical students. This review aims to evaluate the effectiveness of these tools in improving diagnostic accuracy and clinical reasoning, as well as to provide a comprehensive analysis of the latest trends and developments in the use of virtual patients in medical education.
In addition to assessing the current state of research on virtual patients, this review seeks to validate the performance of ChatGPT-4 as a reviewer in comparison to human experts. The use of ChatGPT-4 in the review process offers an innovative approach to handling large volumes of academic literature, providing consistent and objective evaluations, and potentially accelerating the review process [1,2].
By combining human expertise with the analytical capabilities of ChatGPT-4, we aim to determine whether AI can match or even enhance the quality of systematic reviews traditionally conducted by human reviewers.
Ultimately, this article contributes to the growing body of knowledge on digital education tools in healthcare, while exploring the potential of AI to support and enhance academic research processes. This dual focus on educational innovation and methodological advancement underscores the significance of integrating AI into systematic reviews to keep pace with rapid technological advancements in medical training.
1.2. Importance and Challenges of Teaching Clinical Reasoning in Medical Education
Clinical reasoning, encompassing the cognitive processes underlying medical decision-making, is a fundamental competency in clinical practice, serving as the bedrock for diagnostic and therapeutic actions [3]. Hence, it is imperative to train medical students not only in technical knowledge but also in clinical reasoning and critical reflection skills to adeptly navigate the complexity and ambiguity inherent in clinical practice [4].
Despite its significance, clinical reasoning is often explicitly taught to a limited extent within medical curricula [5]. This shortfall persists even though experts advocate for its integration at all stages of medical education, citing barriers such as curriculum time constraints and insufficient faculty expertise [6]. As a result, newly trained physicians frequently report feeling inadequately prepared for clinical reasoning and diagnosis [7].
Digital education offers a potential solution to these challenges, utilizing various tools designed to enhance learning and clinical reasoning skills. A focal point of our research is the employment of virtual patients. Virtual patients are computer-based programs that simulate real-life clinical scenarios, enabling students to practice decision-making in a controlled, interactive environment [8]. These simulations can incorporate complex case data, provide immediate feedback, and present diverse clinical contexts, thereby serving as a powerful educational resource to improve diagnostic accuracy and clinical reasoning skills [9,10].
Since the early 2000s, virtual patients have been employed in medical education to address escalating training expectations amid dwindling training resources [10]. The interactivity of virtual patients ranges from basic textual simulations to intricate environments featuring multimedia elements such as images and sounds [11]. More recently, the advent of AI has facilitated conversational simulations, allowing students to interact with patients in real-time [12,13]. These tools not only enhance students’ clinical skills but also offer a safe space to make mistakes and learn from them without endangering actual patients [12].
Although there are several reviews on this topic [14], many focus on communication skills and do not adequately address the effectiveness of virtual patients in improving clinical reasoning skills. Additionally, rapid technological advancements necessitate the inclusion of recent studies in these reviews. For instance, recent reviews [15] explore AI and machine learning-based systems, which were not considered in earlier reviews.
1.3. Use of ChatGPT or Other LLMs as Article Reviewers
In recent years, artificial intelligence (AI) has emerged as a valuable tool in various fields of academic and medical research. Large language models (LLMs), such as ChatGPT developed by OpenAI, exemplify how AI can contribute to the systematic review process of scientific articles. These models, particularly those based on the GPT-4 architecture, possess the capability to analyze large volumes of text, identify patterns, and provide detailed feedback in significantly less time than human reviewers. For instance, in [16], the remarkable advancement of language models, particularly GPT-4, is highlighted. This research evaluates GPT-4’s performance on the Bar Exam, including the multiple-choice, essay, and practical tests. GPT-4 significantly outperformed its predecessors and even achieved higher scores than the average human examinee in several areas.
The use of LLMs like ChatGPT as article reviewers offers several advantages. First, AI can efficiently handle repetitive tasks and data analysis, allowing human reviewers to focus on more complex and critical aspects of the review process. Second, ChatGPT can assist in identifying grammatical errors, coherence issues, and other technical aspects of the manuscript, thereby enhancing the overall quality of the text prior to final human review
Moreover, integrating ChatGPT into the review process ensures greater consistency and objectivity in manuscript evaluation. AI can apply the same evaluation criteria uniformly, reducing potential bias that may arise from the differing perceptions and experiences of human reviewers. This not only improves the quality of the review but also expedites the process, which is particularly valuable in rapidly evolving fields such as medical education and health technologies [17].
It is crucial to acknowledge, however, that the role of ChatGPT should be complementary to that of human reviewers. While AI can provide valuable preliminary analysis, the expertise and clinical judgment of human experts remain irreplaceable for assessing scientific relevance, innovation, and clinical applicability of articles. Therefore, a collaborative approach that combines the strengths of AI and human review can yield the best results in the evaluation of scientific literature [18].
In this context, our article employs a combination of human reviewers and ChatGPT, specifically GPT-4 (released on March 14th, 2023) and GPT-4o (released on May 13th, 2024), to conduct a systematic review and technological trend analysis on the use of virtual patients in medical education. This hybrid methodology aims to leverage the strengths of both approaches, ensuring a thorough and rigorous review of the available literature.
2. Materials and Methods
This review strictly follows the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines [19]. Additionally, it has been registered in the PROSPERO International Prospective Register of Systematic Reviews under registration number CRD42024574334, ensuring transparency and adherence to established protocols for systematic reviews.
2.1. Eligibility Criteria
We excluded review articles and all trials related to fields other than medicine or nursing. Participants in the included studies were required to be enrolled in a health education or training program. This included students from disciplines such as medicine, dentistry, nursing and midwifery, medical diagnostic and treatment technology, physiotherapy and rehabilitation, or pharmacy.
This review focused on studies where the virtual patient was conversational, either by voice or by keyboard, using natural language in all cases, and where virtual patient-based training was compared to a control group or an alternative method.
Articles were not considered eligible if the goal of the training was not to diagnose correctly or to determine the correct treatment for a patient. Additionally, duplicate entries, papers not fulfilling the inclusion criteria according to the title and abstract, and papers not fulfilling the inclusion criteria according to their full texts were also excluded.
The primary eligible outcomes were learning impact, represented as clinical competencies measured post-intervention with validated or non-validated instruments, and student satisfaction, measured with satisfaction surveys. However, studies that do not directly measure learning impact but include a conversational model related to education were also considered.
2.2. Search Strategy
Concerning the systematic review, four databases were used for the search: PubMed, EMBASE, Scopus and ProQuest. Database searches were performed on April 2024 with the following key search query: (“virtual patient” OR “virtual standardized patient”) AND (“diagnose” OR “clinical reasoning”) in title, abstract and keywords. The search was limited to studies published from year 1998 (according to our searches, this is the first appearance of the term “virtual patient”), in any language. The reference lists of other systematic reviews previously identified as relevant to the study topic were also examined. This approach allowed the identification of additional studies that might not have been retrieved in the initial search due to potential limitations of the databases or the search terms used.
2.3. Data Collection and Analysis
The search results were consolidated into a single Microsoft Excel document. Two independent human reviewers assessed the titles and abstracts to identify potentially eligible studies, which then progressed to a second filtering phase. Full-text articles were retrieved and evaluated based on predefined eligibility criteria. Any discrepancies were resolved through discussion.
The PRISMA flow diagram presented in Figure 1 outlines the process. A total of 486 records were identified: 192 from Scopus, 137 from EMBASE, 90 from PUBMED, and 67 from PROQUEST. After removing 242 duplicate records, 246 records remained for screening. Of these, 174 records were excluded after abstract screening as they did not meet the inclusion criteria. The remaining 72 records were assessed for eligibility, and 62 reports were excluded due to being non-conversational VPs. Ultimately, 10 studies were included in the systematic review.
2.4. Comparison between Human Reviewers and GPTs
Once the articles were selected for review, we engaged two human reviewers (HR1 and HR2) and two versions of the artificial intelligence ChatGPT (GPT-4 and GPT-4o) configured for review tasks. Information extraction using AI was carried out by a third reviewer who did not influence the two manual reviews conducted by humans.
This reviewer uploaded the PDF versions of the scientific articles to ChatGPT. Each article was processed in three separate conversations with the initial prompt for information extraction (Supplementary file 1). Subsequently, we consolidated the three resulting tables (Supplementary file 2) to create a single results table per article. Our method ensured that no information was omitted from the search and no false information was generated or included in the articles. We extracted relevant information independently for each included study, covering: the software/AI used for creating the virtual patient, the number of participants and their division into control and other groups, the specialty or hospital area to which the students belonged, the impact on student learning, and student satisfaction. All relevant data were extracted using a structured form in Microsoft Excel.
The third human reviewer compared the answers of all other reviewers (human and AIs) and, in case of discrepancies, took the decision on which was the correct answer. Once all the correct answers were determined, it was possible to rate the reviewers, verifying whether each reviewer correctly identified each of the following categories in every article: Software/AI used, Software description, Participants, Control and other groups, Hospital Area, Learning Impact, and Student Satisfaction.
Frequency tables will be used for counts. The accuracy in each category will be compared using the chi-square test for each pair of reviewers.
3. Results
This section presents the detailed results of the literature review on the use of virtual patients in medical education, focusing primarily on the aspects of “Software/AI Used”, “Learning Impact”, and “Student Satisfaction”. Finally, the comparison between human reviewers and GPTs will be discussed.
Table 1 below summarizes the main results obtained from the literature review. This table provides an overview of the analyzed studies, highlighting the software used, the number of participants, the impact on learning, and student satisfaction.
3.1. Software Used
Among the reviewed studies, we found a wide variety of software utilized. For instance, Kleinheksel et al. [20], Isaza-Restrepo et al. [26], and Kamath et al. [29] used web-based platforms that create interactive clinical scenarios and simulate patient interactions through chat interfaces and virtual tools. In contrast, Graham et al. [21] utilized the Virtual Human Toolkit, which features videos of patient interactions for students to observe and learn from.
More advanced technologies were also used. Lin et al. [22] incorporated NERVE (Neurological Examination Rehearsal Virtual Environment), which leverages voice recognition and virtual controllers. Maicher et al. [23] employed ChatScript and Unity 3D to manage conversations between students and virtual patients through natural language processing (NLP) in 3D environments. The Julia chatbot developed by Suarez et al. [24] employed Dialogflow for AI-powered conversational flows, while Wang et al. [25] also utilized AI and NLP to simulate real-time clinical encounters. Finally, Yadav et al. [28] integrated virtual reality via Oculus Quest, combining modeling, animation, and patient interaction.
3.2. Learning Impact
The reviewed studies indicate that the use of virtual simulations has had a notable impact on various clinical competencies of the students. In general, these tools have improved clinical history-taking skills and diagnostic reasoning. For example, in studies like those by Lin et al. [22] and Maicher et al. [23], it was observed that students were able to practice these skills in a safe and standardized environment, resulting in greater diagnostic accuracy and stronger clinical skills.
Moreover, the use of AI and NLP, as seen in the systems developed by Suárez et al. [24] and Wang et al. [25], increased student confidence and competence. These technologies facilitated self-directed learning and early exposure to clinical scenarios, allowing students to practice communication and clinical decision-making in complex situations.
Similarly, in studies like those by Courteille et al. [27] and Yadav et al. [28], the use of high-fidelity interactive simulations and virtual reality significantly improved students’ clinical reasoning and decision-making skills. These simulations provided a more immersive and realistic learning experience, facilitating not only the practice of technical skills but also the development of more structured and logical clinical thinking.
3.3. Student Satisfaction
Overall, students reported high levels of satisfaction with simulators that utilized advanced technologies such as AI and NLP. In studies like those by Suárez et al. [42] and Wang et al. [25], students appreciated interacting with chatbots and virtual patients that provided real-time feedback, which increased their confidence and clinical competence.
Virtual reality also received positive evaluations. In the study by Yadav et al. [8], students found that the Oculus Quest platform improved their understanding of clinical concepts and was easy to use once they became familiar with the system. The immersive experience provided by virtual reality was particularly well received, enhancing both clinical reasoning and decision-making skills. Similarly, interactive software like that shown by Lin et al. [22] reported improvements in students’ examination and clinical history-taking skills. These simulators allowed for repetitive practice in a standardized environment, which was seen as beneficial for their training. This sense of security was also reported in studies by Isaza-Restrepo et al. [26] and Kamath et al. [29].
However, not all experiences were uniformly positive. For example, in the study by Courteille et al. [27], while most students found the virtual patient case realistic and engaging, some reported frustration with the system’s limitations, particularly in the interactive dialogue with the patient.
3.4. Comparison between Human Reviewers and GPTs
The results of the comparison between human reviewers (HR1 and HR2) and the artificial intelligence models (GPT-4 and GPT-4o) demonstrate that both AI systems achieved a high level of accuracy in identifying key categories within the scientific articles.
The results indicate that GPT-4 achieved 91.4% correct responses with an error rate of 8.6%. GPT-4o demonstrated higher accuracy, with 97.1% correct responses and a 2.9% error rate. Human reviewers HR1 and HR2 achieved 95.7% and 97.1% correct responses, with error rates of 4.3% and 2.9%, respectively, as shown in Figure 2. Although GPT-4 displayed a higher error rate across different categories, the statistical tests presented in Table 2 indicated no significant differences between the human reviewers and the AI models.
GPT-4o, in particular, exhibited performance comparable to or surpassing that of the human reviewers across several categories. The results for each category are presented in Figure 3.
GPT-4.0 demonstrates superior performance in certain categories compared to human reviewers, particularly in the ‘Software description’ category, where it outperforms both human reviewers. However, Chat GPT-4 falls slightly behind, being the only evaluator to make at least two errors within the same category. Specifically, it shows lower accuracy in ‘Software description’ and in identifying ‘Control and other groups’.
4. Discussion
The total number of studies selected for review (10 studies) is lower than expected, despite the potential interest in conversational virtual patients for medical and health education. The most likely cause is the novelty of the technologies enabling the creation of these virtual patients. An increase in studies on this topic is expected in the coming years, thanks to advances in AI and the relative ease with which a conversational virtual patient can currently be created. It would be beneficial to conduct a new search in approximately one year to confirm the predicted trend.
Besides, conversational VPs are, nowadays, even more useful for training medicine students, due to the increase in the use of teleconsultations. A teleconsultation is almost perfectly simulated with a conversational VP, since the interaction is in both cases through a computer screen. The use of teleconsultation has increased significantly since the pandemic. According to the report presented in a recent analysis [30], teleconsultation usage in 2023 has been 5 times that of 2019 and it is expected to keep increasing in the following years. In this sense, conversational VPs should be considered a highly valuable tool for both current and future medical practice.
Concerning comparisons with other reviews, there are not many previous reviews related to conversational virtual patients, making it difficult to draw direct comparisons with the results of our study. We can only mention two: first, the one presented in Milne-Ives et al. [12], which is specific to training of communication and counselling skills for pharmacy students and pharmacists. Such study identifies four aspects in which VPs provide improvements: knowledge and skills, confidence, engagement with learning, and satisfaction; two of which are precisely the outcomes sought in our research (knowledge/skills and satisfaction). Although the studies analyzed in [12] show improvements in the four previous aspects, the authors note that many studies were small scale without robust findings and, consequently, further quality research was required. The second previous review, presented in Richardson et al. [14], analyzes a total of 12 studies, but only six are related to conversational virtual patients; since the rest analyze other uses of AI and Machine Learning. Among the six studies related to our work, the role of linguistic authenticity in the context of communication skills is emphasized. This result aligns with our selection of studies, in which we exclusively considered conversational virtual patients using natural language communication and excluded semi-conversational environments (typically involving option selection from lists rather than using natural language), as they offer less authenticity.
Regarding the review process itself, AI has demonstrated accuracy comparable to that of human reviewers in extracting information from articles (Table 2), with GPT-4o achieving a success rate equal to or greater than human reviewers. It is reasonable to assume that in the near future, AI will be capable of conducting systematic reviews more reliably than humans; the question is how close that future is. Given the pace at which AI is improving in various tasks, this timeframe is likely measured in months rather than years. The progress is so rapid that benchmarks or comparative tests of AI capabilities against human abilities quickly become outdated. This phenomenon is illustrated in the study presented in Kiela et al. [31], which shows the necessity of proposing increasingly complex tests, and in all cases, AIs rapidly achieve human-level performance on these new tests.
This improvement speed is also evident in Katz et al. [16], where it is shown that in 2023 (with OpenAI’s GPT-4), AIs had already surpassed the average human performance in law exams. This is a remarkable improvement, considering that just one year earlier, in 2022, their results were generally worse than random guessing.
The speed in the improvement of AI capabilities is also patent on our hybrid review results, which demonstrate that GPT-4.o clearly outperforms GPT-4. The differences between GPT-4 and GPT-4.o are due to their respective stages in the evolution of large language models (LLMs). While GPT-4 is known for generating coherent and contextually accurate text across various topics, GPT-4.o introduces several improvements, including enhanced accuracy, faster processing speeds, and a greater ability to handle complex language. Additionally, GPT-4.o benefits from more extensive training data and refined algorithms, making it a superior tool for specialized tasks such as medical education and systematic reviews.
In this context, there are already studies proposing the use of AI to enhance systematic review processes, such as the one presented in Fabiano et al. [32]. Additionally, several tools are being introduced that enable semi-automated reviews, such as LASERAI [33].
Regarding future prospects, it becomes clear that advancements in various technologies are making virtual patients increasingly realistic. It is worth considering which technologies have contributed to this process and which are most relevant today. To graphically illustrate this evolution, we conducted an additional experiment using the ProQuest database (as this tool allows for the automated extraction of full texts from all retrieved articles). First, we relaxed the search criteria to increase the number of relevant works, retaining only “virtual patient” OR “virtual standardized patient” as the search terms, without mentioning “diagnose” OR “clinical reasoning.” With this broader search, ProQuest returned 557 articles related to virtual patients. Second, we extracted the full texts of these articles and measured the frequency of several terms representative of the most influential technologies in virtual patient creation. Specifically: “head-mounted display” (or its abbreviation “HMD”); “3D”; “virtual reality” (or its abbreviation “VR”); “avatar”; “natural language processing” (or its abbreviation “NLP”); and “artificial intelligence” (or its abbreviation “AI”).
The results obtained are displayed in Figure 4. Such results show some interesting facts. First, as expected, the term VR is present from the first studies and its appearance frequency has kept increasing. Other interesting evolution is that of the term “avatar”, that first appeared in 2009 and is progressively gaining incidence. On the other hand, terms like HMD or NLP should not be considered relevant trends. Finally, we can see that the initial studies on the use of virtual patients were rarely associated with AI techniques. However, from 2010 on, the term appears with increasing frequency. Due to the recent advances in AI (particularly, in conversational chatbots like Open AI’s ChatGPT [CITAR]), an even higher increase in the relevance of this term is expected for the following months and years. Globally, according to the dot clouds, the combination of AI, 3D and avatars seems to reflect the current priorities for virtual patient development.
5. Conclusions
This study demonstrates the significant potential of virtual patients, particularly those enhanced by AI, in improving clinical reasoning skills within medical education. The findings highlight the growing importance of integrating advanced digital tools into educational practices to enhance learning outcomes. By comparing human and AI-driven reviews, we found that AI tools like GPT-4 and GPT-4.o can effectively complement human expertise, offering consistent and accurate evaluations. Future research should continue exploring AI’s role in refining and optimizing systematic reviews and educational assessments.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization, M.A.V.R. and C.F.P.; methodology, D.G.T., M.A.V.R. and C.F.P.; software, D.G.T. and M.A.V.R.; validation, D.G.T., M.A.V.R., C.F.P. and J.J.M.S.; formal analysis, D.G.T..; investigation, D.G.T.; resources, D.G.T., C.F.P. and M.A.V.R.; data curation, D.G.T; writing—original draft preparation, D.G.T., C.F.P. and M.A.V.R.; writing—review and editing, D.G.T. and M.A.V.R.; visualization, C.F.P. and J.J.M.S.;.; supervision, J.J.M.S.; funding acquisition, M.A.V.R., C.F.P. and J.J.M.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by MCIN (Ministry of Science and Innovation)/AEI (State Re-search Agency)/DOI 10.13039/501100011033 (Digital Object Identifier) (TED 2021-130383B-I00), and by the European Union “NextGenerationEU”/PRTR (Recovery, Transformation and Resilience Plan). Additional funding was provided by the Ministry of Equality (MI) through the LOVELACE project (Ref: 30-2-ID23).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Research Ethics Committee of the Miguel Hernández University in Elche (reference 240425092013, April 2024).
Informed Consent Statement
Not applicable.
Data Availability Statement
The data extracted automatically by the AI tools used in this study are available as Supplementary files #1 and #2 at https://lcsi.umh.es/hybrid-review. Where appropriate, additional data or information will be shared upon receiving a reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Syriani, E. , David, I., & Kumar, G. Assessing the ability of ChatGPT to screen articles for systematic reviews. arXiv 2023, arXiv:2307.06464. 2023. [Google Scholar]
- Qureshi, R. , Shaughnessy, D., Gill, K. A., Robinson, K. A., Li, T., & Agai, E. Are ChatGPT and large language models “the answer” to bringing us closer to systematic review automation? Systematic Reviews 2023, 12, 72. [Google Scholar] [CrossRef]
- Epstein, R.M.; Hundert, E.M. Defining and Assessing Professional Competence. JAMA 2002, 287, 226. [Google Scholar] [CrossRef]
- Mamede, S.; Schmidt, H.G. The structure of reflective practice in medicine. Medical Education 2004, 38, 1302–1308. [Google Scholar] [CrossRef]
- Harendza, S.; Krenz, I.; Klinge, A.; Wendt, U.; Janneck, M. Implementation of a Clinical Reasoning Course in the Internal Medicine trimester of the final year of undergraduate medical training and its effect on students’ case presentation and differential diagnostic skills. DOAJ 2017, 34, Doc66. [Google Scholar] [CrossRef]
- Rencic, J.; Trowbridge, R.L.; Fagan, M.; Szauter, K.; Durning, S. Clinical Reasoning Education at US Medical Schools: Results from a National Survey of Internal Medicine Clerkship Directors. Journal of General Internal Medicine 2017, 32, 1242–1246. [Google Scholar] [CrossRef]
- Monrouxe, L.V.; Grundy, L.; Mann, M.; John, Z.; Panagoulas, E.; Bullock, A.; Mattick, K. How prepared are UK medical graduates for practice? A rapid review of the literature 2009–2014. BMJ Open 2017, 7, e013656. [Google Scholar] [CrossRef]
- Posel, N.; Mcgee, J.B.; Fleiszer, D.M. Twelve tips to support the development of clinical reasoning skills using virtual patient cases. Medical Teacher 2014, 37, 813–818. [Google Scholar] [CrossRef]
- Manesh, R.; Dhaliwal, G. Digital Tools to Enhance Clinical Reasoning. Medical Clinics of North America 2018, 102, 559–565. [Google Scholar] [CrossRef]
- Kononowicz, A.A.; Woodham, L.A.; Edelbring, S.; Stathakarou, N.; Davies, D.; Saxena, N.; Car, L.T.; Carlstedt-Duke, J.; Car, J.; Zary, N. Virtual Patient Simulations in Health Professions Education: Systematic Review and Meta-Analysis by the Digital Health Education Collaboration. JMIR 2019, 21, e14676. [Google Scholar] [CrossRef]
- Cook, D.A.; Triola, M.M. Virtual patients: a critical literature review and proposed next steps. Medical Education 2009, 43, 303–311. [Google Scholar] [CrossRef] [PubMed]
- Milne-Ives, M.; De Cock, C.; Lim, E.; Shehadeh, M.H.; De Pennington, N.; Mole, G.; Normando, E.; Meinert, E. The Effectiveness of Artificial Intelligence Conversational Agents in Health Care: Systematic Review. JMIR 2020, 22, e20346. [Google Scholar] [CrossRef] [PubMed]
- Dolianiti, F.; Tsoupouroglou, I.; Antoniou, P.; Konstantinidis, S.; Anastasiades, S.; Bamidis, P. Chatbots in Healthcare Curricula: The Case of a Conversational Virtual Patient. Lecture Notes in Computer Science 2020, 137–147. [Google Scholar]
- Richardson, C.L.; White, S.; Chapman, S. Virtual patient technology to educate pharmacists and pharmacy students on patient communication: a systematic review. BMJ Simulation & Technology Enhanced Learning 2019, 6, 332–338. [Google Scholar] [CrossRef]
- Stamer, T.; Steinhäuser, J.; Flägel, K. Artificial Intelligence Supporting the Training of Communication Skills in the Education of Health Care Professions: Scoping Review. JMIR 2023, 25, e43311. [Google Scholar] [CrossRef] [PubMed]
- Katz, Daniel & Bommarito, Michael & Gao, Shang & Arredondo, Pablo. GPT-4 passes the bar exam. Phil. Trans. R. Soc. A. 2024, 382. [CrossRef]
- Smith, L. & Kosslyn, S. M. Cognitive benefits of artificial intelligence (AI) in education and training. International Journal of Educational Technology in Higher Education 2020, 17, 1–15. [Google Scholar] [CrossRef]
- Esteva, A. , Robicquet, A., Ramsundar, B., Kuleshov, V., DePristo, M., Chou, K.,... & Dean, J. A guide to deep learning in healthcare. Nature Medicine 2021, 25, 24–29. [Google Scholar] [CrossRef]
- Moher, D. , Shamseer, L., Clarke, M., Ghersi, D., Liberati, A., Petticrew, M.,... & Prisma-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Systematic reviews 2015, 4, 1–9. [Google Scholar] [CrossRef]
- Kleinheksel, A. J. Transformative Learning through Virtual Patient Simulations: Predicting Critical Student Reflections. Clinical Simulation in Nursing 2014, 10, e301–e308. [Google Scholar] [CrossRef]
- Graham, F. , Beattie, E., & Fielding, E. (2022). Hospital nurses’ management of agitation in older cognitively impaired patients: Do they recognise pain-related agitation? Age and Ageing 2022, 51, afac140. [Google Scholar] [CrossRef]
- Lin, C. , Laserna, C., Lind, D. S., Kalaria, C., Aryal, T., Lok, B., Johnsen, K., Kotranza, A., Cendan, J., & Pruitt, J. N. User Response to the Simulation of a Virtual Patient with Cranial Nerve Injury. Bio-Algorithms and Med-Systems 2012, 8, 1. [Google Scholar] [CrossRef]
- Maicher, K. , Danforth, D., Price, A., Zimmerman, L., Wilcox, B., Liston, B., Cronau, H., Belknap, L., Ledford, C., Way, D., Post, D., Macerollo, A., & Rizer, M. Developing a Conversational Virtual Standardized Patient to Enable Students to Practice History-Taking Skills. Simulation in Healthcare: The Journal of the Society for Simulation in Healthcare 2017, 12, 124–131. [Google Scholar] [CrossRef]
- Suárez, A. , Adanero, A., Díaz-Flores García, V., Freire, Y., & Algar, J. Using a Virtual Patient via an Artificial Intelligence Chatbot to Develop Dental Students’ Diagnostic Skills. International Journal of Environmental Research and Public Health 2022, 19, 8735. [Google Scholar] [CrossRef]
- Wang, S. , Chen, C., & Tsai, T. Learning clinical reasoning with virtual patients. Medical Education 2020, 54, 481–481. [Google Scholar] [CrossRef] [PubMed]
- Isaza-Restrepo, A. , Gómez, M. T., Cifuentes, G., & Argüello, A. The virtual patient as a learning tool: A mixed quantitative qualitative study. BMC Medical Education 2018, 18, 297. [Google Scholar] [CrossRef]
- Courteille, O. , Bergin, R., Courteille, O., Bergin, R., Stockeld, D., Ponzer, S., & Fors, U. The use of a virtual patient case in an OSCE-based exam – A pilot study. Medical Teacher 2008, 30, e66–e76. [Google Scholar] [CrossRef]
- Yadav, V. , Shrivastava, T., Naqvi, W. M., & Bhurane, A. A Study to Design a Learning Tool “Virtual Patient” for Functional Diagnosis and Clinical Reasoning of Respiratory Dysfunction in the Undergraduate Physiotherapy Curriculum. Cureus 2023. [Google Scholar] [CrossRef]
- Kamath, A. , & Ullal, S. D. Learning and clinical reasoning experience of second-year medical pharmacology students and teachers with virtual patients developed using OpenLabyrinth. Electronic Journal of General Medicine 2023, 20, 20–em509. [Google Scholar] [CrossRef]
- Statista: Online Doctor Consultations - Worldwide. Available online: https://www.statista.com/outlook/hmo/digital-health/online-doctor-consultations/worldwide#revenue (accessed on on September 9, 2024).
- Kiela, D., Thrush, T., Ethayarajh, K., & Singh, A. Plotting progress in AI. Contextual AI Blog 2023. Available online: https://contextual.ai/blog/plotting-progress (accessed on 9 September 2024).
- Fabiano, N. , Gupta, A., Bhambra, N., Luu, B., Wong, S., Maaz, M.,... & Solmi, M. How to optimize the systematic review process using AI tools. JCPP advances 2024, 4, e12234. [Google Scholar] [CrossRef]
- LASERAI. Available online: https://www.laser.ai/ (accessed on 9 September 2024).
Figure 1.
Flow diagram of the studies through the revision process.
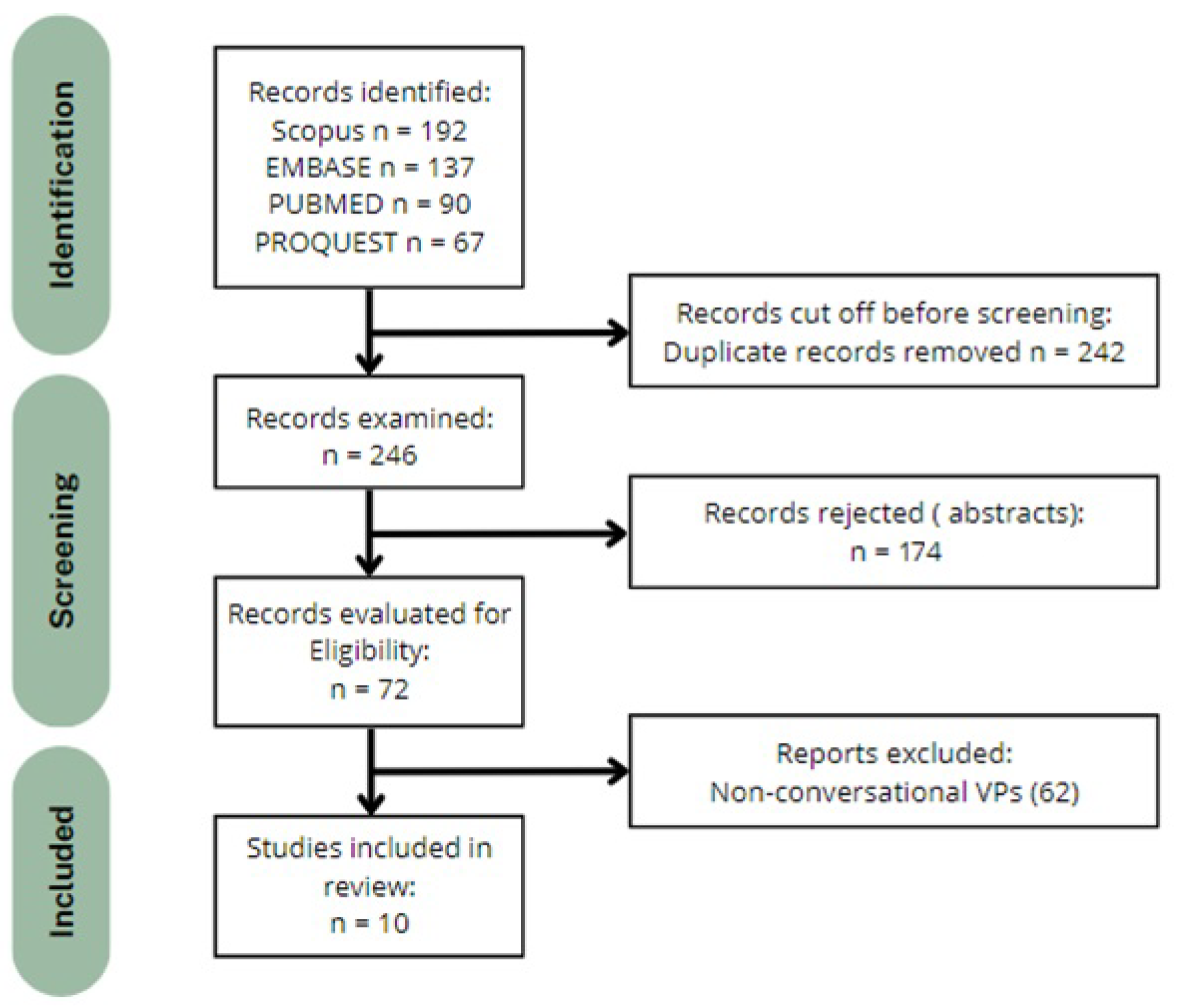
Figure 2.
Percentage of Correct Responses by Evaluator.
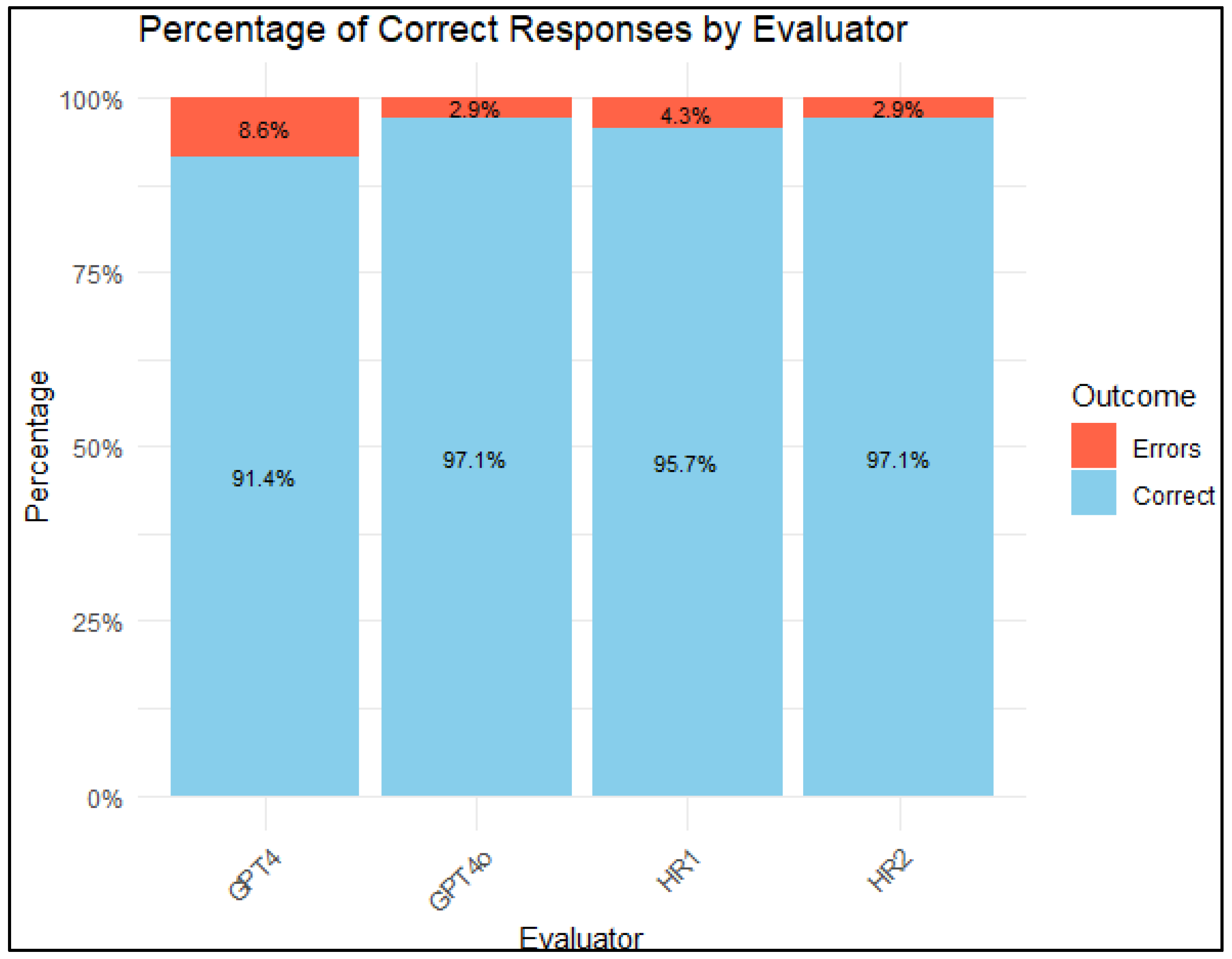
Figure 3.
Accuracy of Human Reviewers and AI Models in Identifying Key Categories.
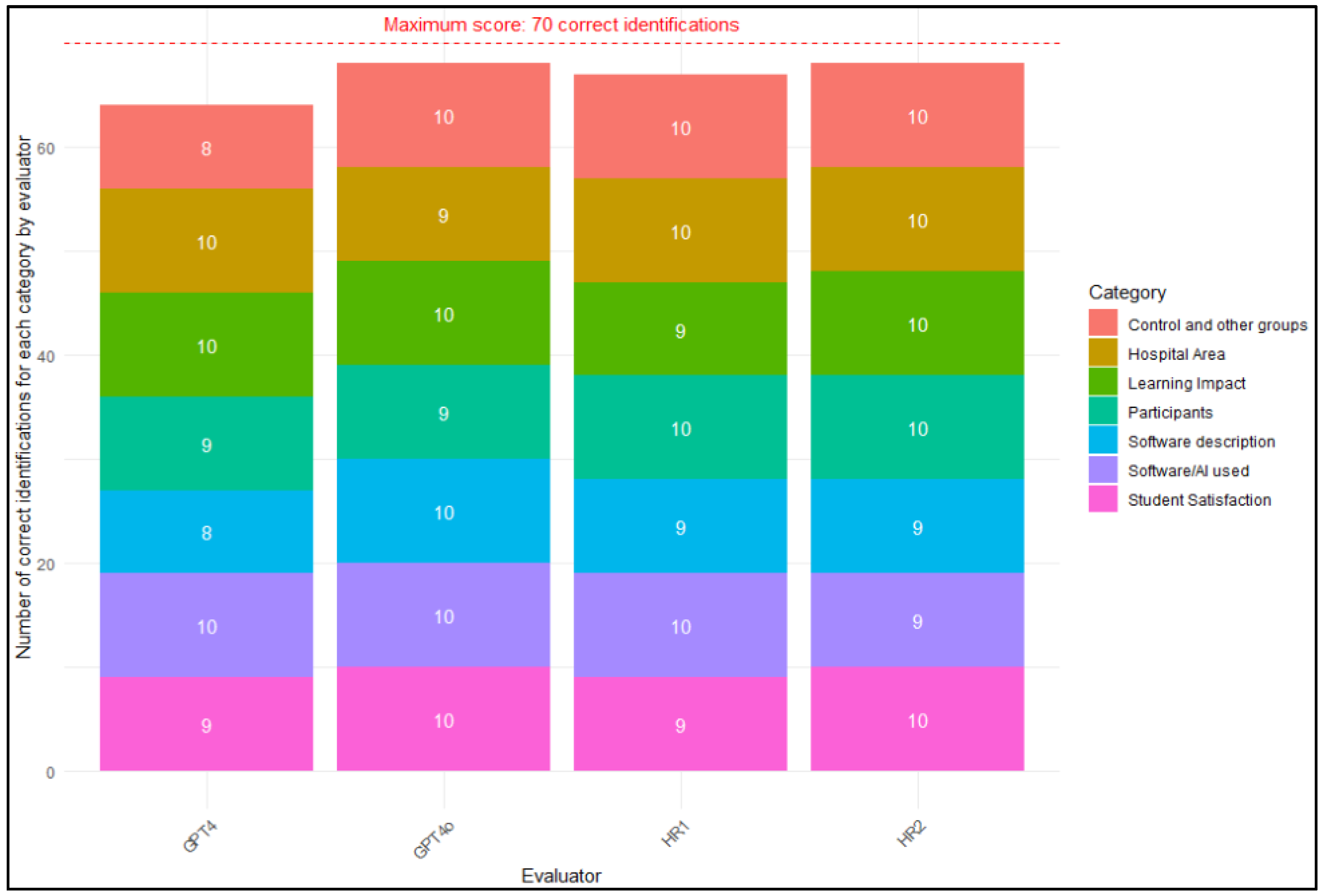
Figure 4.
Technological trend analysis in papers related to virtual patients or virtual standardized patients.
Figure 4.
Technological trend analysis in papers related to virtual patients or virtual standardized patients.
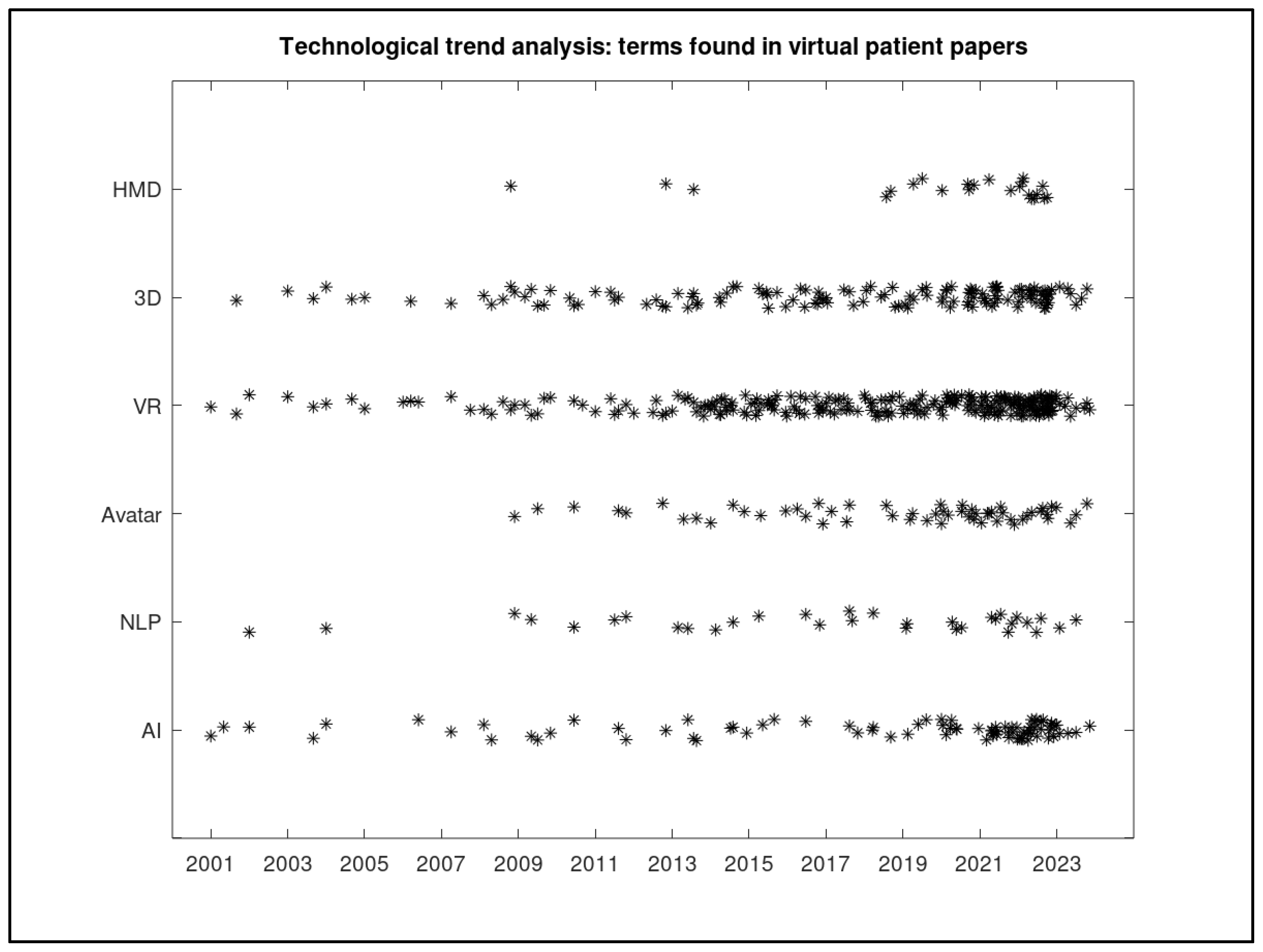

Table 1.
Results of the literature review.
| References | Software used | Number of Patients/ Groups / Hospital Area | Learning Impact | Student Satisfaction |
|---|---|---|---|---|
| Kleinheksel [20] | Shadow Health Digital Clinical Experience (DCE) | 130 students (Master of Science in nursing), Nursery | Deeper learning through exploration of clinical findings | Not measured |
| Graham et al. [21] | Virtual Human Toolkit (Institute of Creative Technologies, University of Southern California) | 274 medical and surgical nurses, Nursery | Identified gaps in pain recognition and treatment practices | Not measured |
| Lin et al. [22] | NERVE: Neurological Examination Rehearsal Virtual Environment | 69 (9 clinicians, 7 residents, 53 students), Neurology | Improved exam techniques and history-taking skills | General high ratings from surveys |
| Maicher et al. [23] | ChatScript for conversation; Unity for animation | 141 students. 12000 questions asked to the virtual patient, Medicine | Improved history-taking and diagnostic skills | Not measured |
| Suárez et al. [24] | Dialogflow application. | 193 students of 4th or 5th year of dentistry, Dentistry | Improved communication skills and confidence | Generally positive, especially interaction satisfaction |
| Wang et al. [25] | Not mentioned. | 112 medical students, Medicine | Increased confidence and proficiency | Increased confidence and proficiency |
| Isaza-Restrepo et al. [26] | Own software: “the virtual patient: simulation of clinical cases” | 20 medical students, Medicine | Significant improvement in history taking and clinical reasoning | Found it easy-to-use and motivating |
| Courteille et al. [27] | ISP (Interactive Simulation of Patients) | 110 medical students (4th year), Medicine | Differentiated student performances and enhanced clinical reasoning | Mixed reviews on usability and examination tool potential |
| Yadav et al. [28] | Unity and Oculus Quest. | 113 in total: 98 students and 15 faculty members. But 7 students did not fill the questionnaires (so real total 106), Physiotherapy | Enhanced clinical reasoning and decision-making skills | Generally positive, especially on concept understanding and ease of use |
| Kamath & Ullal [29] | OpenLabyrinth | 20 students and 12 teachers, but one student did not provide feedback, so total 31, pharmacology | Improved understanding of patient interaction, multiple viewpoints, and clinical reasoning | Positive feedback on real-life decision-making simulation |
Table 2.
Statistical Comparison of Accuracy Between Human Reviewers and AI Models.
| Comparison | Chi square | P-value |
|---|---|---|
| HR1 – HR2 | 0.15 | 1.00 |
| HR1 – GPT4 | 0.32 | 0.99 |
| HR1 – GPT4o | 0.26 | 1.00 |
| HR2 – GPT4 | 0.32 | 0.99 |
| HR2 – GPT4o | 0.21 | 1.00 |
| GPT4 – GPT4o | 0.43 | 0.99 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



