
Submitted:
19 September 2024
Posted:
20 September 2024
You are already at the latest version
Abstract
Background/Objectives: Women's reproductive and overall well-being are intricately associated to vitamin D levels. In Morocco, vitamin D deficiency is a major issue for premenopausal women, yet little data exists on their dietary intake of this nutrient. This study explores vitamin D dietary intake, socio-demographic determinants, and its correlation with serum 25-hydroxyvitamin D [25(OH)D3] in premenopausal Moroccan women. Methods: A cross-sectional study was conducted with 355 women aged 18-49 in Meknes, Morocco, using validated questionnaires to assess dietary intake and sun exposure. Potential covariates such as physical activity and BMI were also assessed . Serum 25(OH)D was measured via chemiluminescence immunoassay. Chi-square tests and Spearman correlation were used to identify socio-demographic factors influencing vitamin D intake. Linear and multivariate regression analysis determined the main predictors of serum 25(OH)D levels. Results :The median (interquartile range) vitamin D dietary intake was 2.8 (2.7) µg/day , with less than 20% of women meeting the recommended 5 µg/day. Major dietary sources were fish (48%), dairy (24.3%), and meat (9.4%), with fortified foods contributing only for 7%. Lower intake was linked to younger age (p=0.004) and rural living (p=0.024). While no significant association was found between dietary intake and serum 25(OH)D ((β(SE): 0.155(0.094), p=0.340 ) , sun exposure positively predicted serum levels(β(SE): 0.343 (0.128), p=0.008) , and BMI negatively affected them (β(SE): -1.128 (0.337), p=0.001). Conclusions: Our findings highlight insufficient vitamin D intake among premenopausal Moroccan women, especially younger and rural women. Nutritional interventions are needed to address this deficiency, promoting better dietary habits, sun exposure, and healthy weight.
Keywords:
dietary intake
; food sources
; food fortification
; sociodemographic
; serum 25-hydroxyvitamin D
; sun exposure
; BMI
; premenopausal women
1. Introduction
Vitamin D is a group of fat-soluble steroid compounds of different origins, with similar chemical structures and the same biological effects [1]. Often referred to as pro-hormone with complex endocrine regulation [2], it plays a major role in controlling calcium and phosphate homeostasis, normal bone growth and mineralization [3,4]. It is also crucial in the immune response, promoting an anti-inflammatory state and maintaining the balance between pro- and anti-inflammatory activities [5]. Inadequate vitamin D status is associated with a wide range of health implications across different age groups. In children, it can lead to growth retardation and rickets [4,6], while in adults, it is linked to osteoporosis [4], and chronic conditions such as diabetes [7], autoimmune diseases [8], psychiatric disorders [9], cardiovascular diseases [10] and cancers [11]. Additionally, adverse pregnancy outcomes and complications in reproductive age are also connected to vitamin D deficiency [12]. These health issues significantly impact quality of life, increase mortality rates, and raise healthcare costs [13,14].
Uniquely, vitamin D can be synthesized endogenously by the human body [15] In response to ultraviolet rays, at wavelengths between 290 and 315 nm, 7-dehydrocholesterol in the skin converts to vitamin D3 [15]. A 20-minute whole-body exposure to summer sun can produce up to 250 µg of vitamin D3, achieving the recommended serum level (≥30 ng/ml) of its metabolite, 25-hydroxyvitamin D [25(OH)D]. However, skin photosynthesis of vitamin D is not always reliable due to factors like seasonal variations, high latitude, atmospheric pollution and pigmented skin [16]. Additionally, sun exposure has become less viable due to the intentional avoidance of direct sunlight, use of sunscreen, sedentary indoor lifestyles, and covering dress due to cultural or religious practices [15,17,18].
As a result, vitamin D deficiency (VDD), has become a global pandemic [19,20,21], even in sunny countries [4,22]. Over a third (34.22%) of Africans are vitamin D deficient, with a high prevalence of severe deficiency (25(OH)D3 < 12 ng/ml) and worsening status in northern African countries [21]. A recent meta-analysis estimated that hypovitaminosis D (25(OH)D3 < 30 ng/ml) affects up to 96% of children, teenagers, and adult women in the Mediterranean, Middle East, and North Africa (MENA) region. In this area, female sex is a significant risk factor for hypovitaminosis D [17]. Women are disproportionately vulnerable to VDD not only due of physiological factors such as pregnancy, lactation, and menopause [23] or unfavorable sun exposure behaviors [14] but also as result unhealthy dietary pattern and evidently inadequate vitamin D intake [24,25].
Vitamin D3 (cholecalciferol) and vitamin D2 (ergocalciferol) are the predominant forms of vitamin D in foods and are effective in maintaining vitamin D status [26,27]. Vitamin D2 is synthesized by fungi, while vitamin D3 is found in animal sources, such as fatty fish and fish oil, egg yolks, and red meat [28]. Despite this, achieving optimal plasma vitamin D levels through diet alone is challenging. Food fortification is recognized as a viable approach to increase dietary vitamin D intake and improve 25(OH)D levels in populations [29]. Fortification strategies vary by country, with commonly fortified products including milk, yogurt, juices, and breakfast cereals [29]. surveys in the US [30], Canada [31], and Europe [29,32] report high prevalence of inadequate vitamin D intake, with exceptions in Scandinavian countries where fish consumption is high, and fortification policies are in place [29,33,34]. Likewise, a previous, global review indicated that dietary supplement use may contribute 6–47% of the average vitamin D intake in some of these countries [35].
In Morocco, 78.8% of women of reproductive age (WRA) are vitamin D deficient (25(OH)D < 20 ng/ml), with over one-third (31.3%) severely deficient (25(OH)D < 10 ng/ml) according to the latest national nutritional survey [36]. Despite the implementation of food fortification strategies 24 years ago, vitamin D dietary intake and sources among the general population remain largely unexplored. Previous research on vitamin D status in Moroccan women has largely concentrated on the influence of sun exposure and lifestyle behaviors as primary determinants [37,38,39]. However, a single crosse sectional study by Benhammou et al (2016), indicated that average vitamin D intake among 101 Moroccan women accounted for a mere 12.36% of the recommended daily allowance, reflecting the potential adverse influence of Westernized dietary patterns on nutrient intake [40].
Therefore, our study aimed to address this gap by comprehensively exploring the components of dietary vitamin D intake among Moroccan women of reproductive age investigating its potential determinants and examining its association with vitamin D status. Addressing dietary habits could offer a modifiable target for improving overall vitamin D status in this population.
2. Materials and Methods
2.1. Study Population
We conducted a cross-sectional study involving women of reproductive age living in the prefecture of Meknes, located in north-central Morocco between February and December 2022. Participants were recruited from among apparently healthy women visiting private medical clinics and laboratories collaborating in the study project.
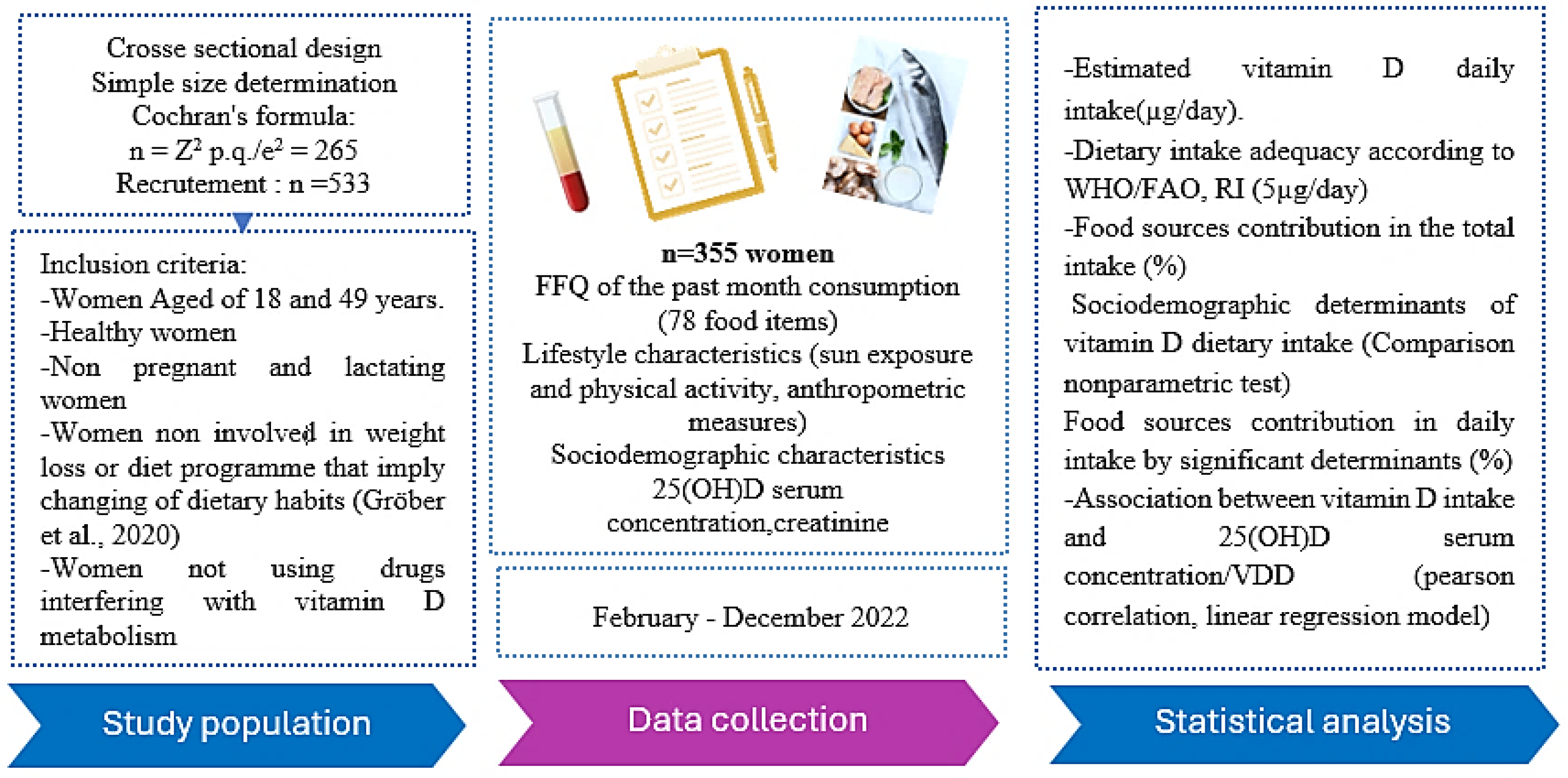
The sample size was determined using Cochran’s formula [41] for an estimate of VDD prevalence (25(OH)D3 < 20 ng/ml) at 78.8% among WRA at the national level. A minimum sample size of 256 women was targeted. To increase the statistical power, 533 female participants were recruited, of which 355 women met the inclusion criteria, completed the study questionnaires, and provided written consent (see flow chart below)
Figure 1.
Flow chart of the study design.
2.3. Questionnaires
Dietary intake was assessed using our previously developed and validated vitamin D food frequency questionnaire (VitD-FFQ) with 78items food list [42]. Food sources containing high levels of vitamin D are included in the list, along with fortified foods available at the local market. Four to five quantities of consumption for each food item (expressed in g, ml, and domestic measures; slice, tablespoon, or cap) and six frequencies of intake (monthly, weekly, and daily) have been inserted into the FFQ to estimate the daily intake of vitamin D during the last month [42].
Total daily intake of vitamin D in µg/day was calculated by multiplying the amount reported in the questionnaire by the corresponding value in the French/USDA composition tables as described previously. For fortified foods, nutrient content information from the packages was employed. The WHO/FAO vitamin D required intake of 5 µg/day for adult women was used to examine the adequacy of our participants’ intake [43].
Sun exposure behaviors were measured via our sun exposure questionnaire previously validated with Moroccan women of childbearing age [44]. The scores assessed reflected the determinants of the amount of vitamin D that can be produced under the skin after sun exposure, namely frequency, duration, time slot and parts of the body routinely exposed to the sun, as well as sun protection practices such as the use of sunscreens and the type of clothing worn. The classification of was used to determine the skin phototype of the participants (type V & VI, type III & IV, type II, type I) and thus adjust according to the estimated exposure score on a scale of 0.25 to 1. Participants were subsequently classified according to their estimated scores as low (SES < 7.5 points), moderate (SES = 7.5 to 15), adequate (SES = 15 to 30), and high (SES > 30) [42,44]
To assess physical activity levels (PAQ), the short-form version of the International Physical Activity Questionnaire (IPAQ-SF) was used, consisting of seven closed-ended questions, in relation to activities done in the previous week [45],The participants’ scores were classified into three NAPs; low intensity (< 600 MET min/week), moderate intensity (at least 600 MET-min/week) and strenuous/vigorous (at least 3000 MET-min/week) [46].
The data collection process for each participant was conducted through a one-on-one interview with a dietitian and nurses who also collected information on socio-demographic characteristics (age, marital status, occupation, geographic location and education level).
2.3. Measures
Participants’ weights and heights were performed with standard procedures, while participants were scantily clad and without shoes. Anthropometric status was classified according to the WHO BMI classification as follows: Underweight: BMI<18.5 kg/m², Normal: BMI: 18.5-24.9 kg/m², Overweight: BMI 25-29.9 kg/m², and Obese 30 kg/m² [46]
10 mL fasting venous blood was collected from each participant by a nurse and analysed on the same day. Serum 25(OH)D was performed with a one-step electrochemiluminescence immunochemical assay according to the manufacturer’s instructions. Creatinine was performed using an Abbott Architect ci4100 COBAS E411 Chemistry Analyzer.
VDD was defined as serum levels of 25(OH)D3 <20 ng/ml [47,48,49] while vitamin D insufficiency was defined as levels between 20 and 30 ng/ml [47,49] Women with serum concentrations of 25(OH)D3 >30 ng/mL were considered to have adequate levels [47,49].
In addition, since serum levels of 25-hydroxyvitamin D may be affected by kidney function [50], the Dietary Modification in Kidney Disease (MDRD) formula was used to assess participants’ kidney function [51] Only women with glomerular filtration rates greater than 60 ml/min/1.73 m2 were included in the final analysis (Levey, 1999).
2.3. Ethics
All women participants give signed informed consent, and all surveys procedures were conducted in accordance with the principles of the Declaration of Helsinki. The Biomedical Research Ethics Committee of Moulay Ismail University (reference; No. 1/CERB-UMI/19) approved the study protocol.
2.4. Statistical Analysis
The normality of the continuous data was assessed using the Kolmogorov-Smirnov and Shapiro wilk tests (n>50) respectively. Not all variables were normally distributed, therefore only non-parametric tests were applied. Descriptive analysis was performed, and data were presented in mean and standard deviation in addition to median with interquartile rang for continuous variables and in frequencies and percentages for categorical variables.
Participants were classified into subgroups based on their vitamin D intake adequacy. Kruskal-Wallis and Bonferroni tests were used to compare estimated daily intake of vitamin D across sociodemographic status subgroups, while the e-chi-square test/fisher exact test was used to measure the difference in frequency for categorical variables.
The relationship of serum 25(OH)D3 with dietary vitamin D intake and sun exposure score was depicted in scatter plots after log-transforming the variables to meet normality. Finally, we examined the relationship by linear regression analysis. In the models, serum 25(OH)D3 was a dependent variable, with dietary vitamin D intake and UV exposure simultaneously included as independent variables. Other covariates were selected from factors possibly related to serum vitamin D concentration by stepwise selection.
Data were analyzed using R package, statistical tests were two-sided, and p values of <0.05 were considered statistically significant.
3. Results
The demographic characteristics of the study participants (n=355) are summarized in the Table 1. The median age of the participants was 29.0 years, with an interquartile range of 11.0 years. The age distribution’s indicating a predominance of young to middle-aged women 25.4% and 55.5% respectively.
In terms of education, a minor proportion of 18.0% were Illiterate. A more than a half of our women participants were married (63.9%), unemployed (55.8), residing urban areas (67.3%) and exhibiting overweight/obesity (57.8%).
The mean estimated vitamin D intake from food was 3.63 µg/day (±2.73) and the median intake, was 2.87 µg/day (IQR: 2.76) which is lower than the required vitamin D intake established by the joint WHO/FAO expert of 5µg/day(200IU/day). Only 19.72% of the participants meet the WHO/FAO recommended intake for vitamin D (≥5 µg/day), while the vast majority (80.28%) have intakes below this threshold (88.28%). Only eight women were taken medical vitamin D supplementation and were excluded from dietary analysis.
A The median level of 25(OH)D3 was 15.7 ng/ml with an interquartile range (IQR) of 12.4 ng/ml, indicating a significant proportion (65.1%) of the participants that are vitamin D deficient (25(OH)D3<20 ng/ml). The median physical activity level was 1778.2 MET-minutes/week, with a broad IQR of 1765.0. The vast majority (93.2%) of our participants had moderate to low physical activity levels, with only 6.8% that were engaged in high levels of physical activity. Lastly, the seasonal distribution of participants showed a relatively highest representation of participants recruited during the summer season (40.9%), followed by autumn (24.2%), spring (18.6%) and then wintereven (16.9%).
The Figure 2 presents vitamin D intake food sources among the study participants. The primary food source of the total intake was fish and sea products, contributing to 48%, followed by Milk, diary products and beverages (24.39%). To a lesser extent, Meat, poultry and related products provide 9.40% while fortified oils and margarines and eggs consumption accounting for 6.27% and 6.23% respectively of the total intake. Bakery and Moroccan sweet mostly prepared with eggs and fortified oils account for 3.49% while other commercial fortified foods such as breakfast cereal and cacao provide less than 2% of the intake.
The Table 2 illustrates the frequency of consumption for various food items categorized by their respective food sources. Notable variations in consumption frequencies are observed across different types of fish. Fatty fish, such as Sardin (either fresh/frozen or canned in tomato sauce), are predominantly consumed by over half of the participants (54.2% and 50.98%, respectively) 1-3 times per month, with a lesser proportion consuming them up to once a week (27.04% and 6.19%, respectively). Conversely, other types of fish, such as Mackerel, white fish, canned Tuna/Mackerel, or Shellfish, are rarely consumed, with most women participants abstaining or consuming them less than once per month (rangingfrom 85.35% for white fish to 91.54% for Shellfish).
Rich vitamin D meat products, such as liver, are also rarely consumed by the majority (81.14%) of participants. Poultry, particularly chicken and turkey, are more frequently consumed, with approximately half of the participants consuming them once a week (45.53%). However, a similar proportion (43.66%) either never or rarely consume red meat compared to 14.36% who consume it once a week.
Egg consumption frequencies are diverse regardless of the preparation method. More than a third of participants consume eggs less frequently or never (38.6%), nearly a third consume eggs once a week (28.56%), while 10.42% consume them more frequently, maximum, 5-6 times a week.
Cow milk, including vitamin D fortified, is consumed every day by a substantial proportion of participants (40%). Melted cheese in portions is predominantly consumed 5 to 6 times a week and every day by 29.28% and 18.62% of participants, respectively. Flavored or fruit yogurt is also consumed, albeit less frequently, mostly once a week by 27.04% of participants.
Bakery products are predominantly consumed once a week by 41.7% of participants. A significant proportion of participants (77.18%) consume fortified oil almost daily, while 22.82% do not consume it. Specifically, near a half of participants (45.63%) do not consume fortified margarine, while 21.15% consume it every day. Other vitamin D fortified and riche food sources such as breakfast cereals, chocolate, and cacao are consumed less frequently or never by most of our women participants.
Table 3 presents the correlation between dietary vitamin D intake and studies demographic factors. A statistically significant relationship was found between vitamin D consumption and age (p = 0.002). Notably, young women (less than 36 years) were found to have lowest vitamin D intake than the older one (p < 0.027).
Regarding education level, vitamin D intake exhibited slight variations, although these differences did not reach statistical significance (p = 0.351). Similar observations were made regarding the association between vitamin D intake and marital status and employment.
Furthermore, urban women demonstrated significantly higher vitamin D intake compared to their rural counterparts, with median intakes of 3.18 µg/day and 2.73 µg/day, respectively (p=0.014).
There was no difference in the distribution of vitamin D intake categories across participant demographic determinants.
Figure 3.
Food source of vitamin D by associated participants characteristics: Age (chart A), and localization (chart B).
Figure 3.
Food source of vitamin D by associated participants characteristics: Age (chart A), and localization (chart B).
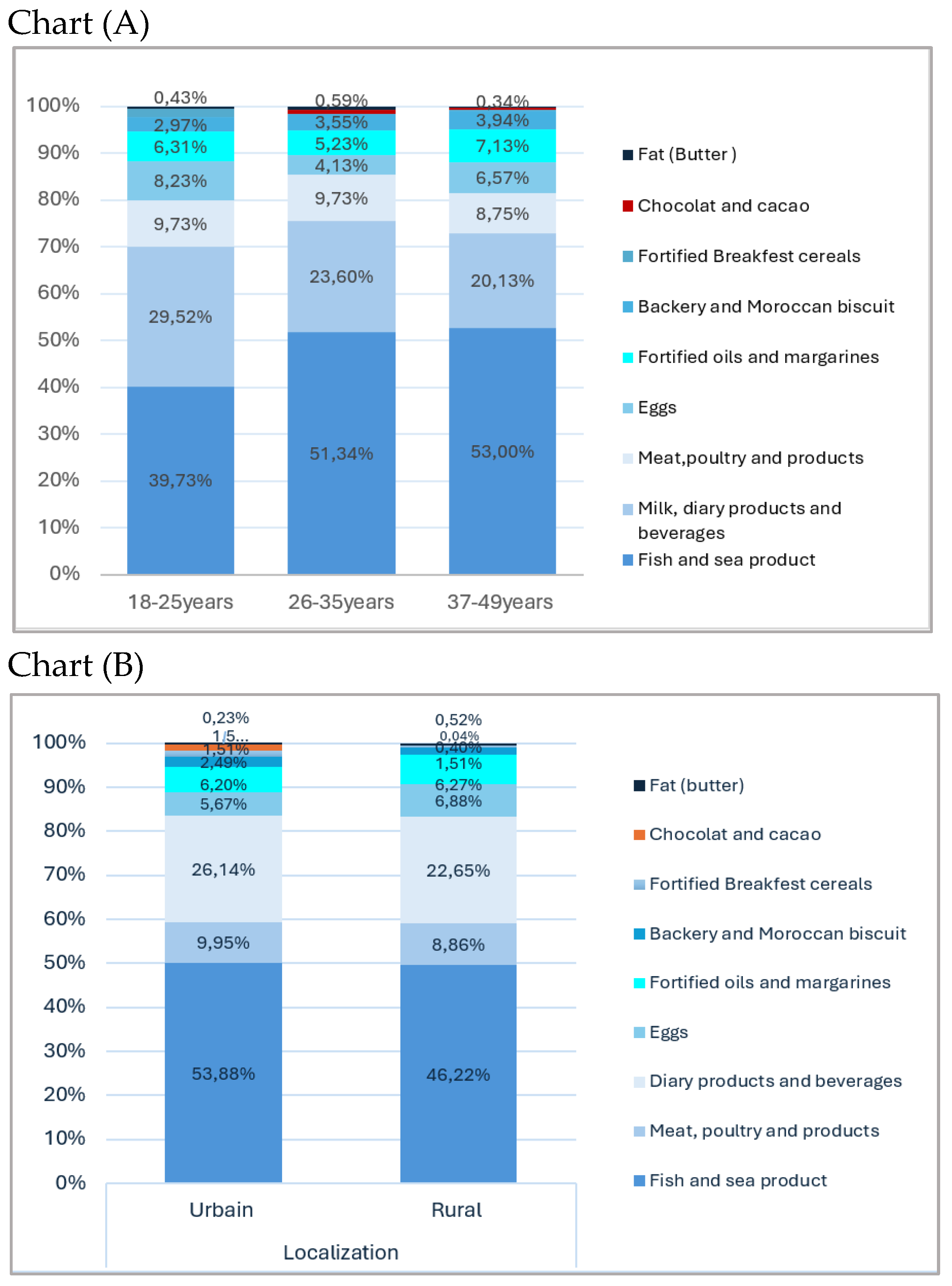
The consumption of vitamin D from dairy products, including fortified milk, progressively decreases with age, thru breakfast cereals becoming non-consumed after the age of 35 years. Conversely, there is a slight increase in the consumption of meat products and eggs among older women. Additionally, fish and seafood products are more commonly consumed by women in the middle age classed (65%).
Fish consumption is more common in rural areas compared to urban one (64% vs. 56%), while meat products and fortified products such as dairy, cereal breakfast items, cacao, and chocolate are more frequently consumed by urban women. Vitamin D intake from eggs, bakery products, and Moroccan biscuits remains similar across both urban and rural areas. Dairy products, eggs, and fortified oils and margarines are more commonly consumed in autumn and summer, while fish consumption is lowest in autumn, highest in summer, and similar in both spring and winter. Meat products, fortified oils and margarine, breakfast cereals, and bakery items are more frequently consumed in spring and winter.
Figure 4 presents the correlation between dietary intake and sun exposure with serum 25(OH)D3 levels. Both, dietary vitamin D intake and the sun exposure score showed a weak linear correlation to participant vitamin D levels with R²=0.010, p=0.031 and R²=0.010, p=0.031 respectively.

Table 4.
Predictors of 25(OH)D3 levels in the study participants (n=355).
| Predicators | Unstandardized Coefficients | 95.0% Confidence Interval for β | t | P value | ||
|---|---|---|---|---|---|---|
| β | Std. Error | Lower Bound | Upper Bound | |||
| Dietary vitamin D intake (µg/day) | 0.155 | 0.094 | 1.108 | 1.204 | 0.030 | 0.340 |
| Sun exposure score | 0.343 | 0.128 | 0.092 | 0.595 | 2.683 | 0.008 |
| IMC (kg/m2) | −1.128 | 0.337 | −1.790 | −0.466 | −3.350 | 0.001 |
In the adjusted stepwise linear regression model with 25(OH)D as the dependent variable and selecting significant covariates, vitamin D dietary intake had no significant effect on circulating 25(OH)D (β(SE): 0.155 (0.094), p=0.340). In contrast, the sun exposure score remained statistically significant, with a positive effect (β(SE): 0.343 (0.128), p=0.008), indicating a moderate increase in serum concentration per one-unit change in the estimated score. Furthermore, BMI was a strong predictor of vitamin D levels (p=0.001) showing an inverse relationship with a potential reduction of β(SE): -1.128 (0.337) in 25(OH)D levels for each one-unit increase in BMI.
4. Discussion
In this study, we reported important information regarding the current dietary intake and food sources of vitamin D among Moroccan premenopausal women. The results showed that the estimated vitamin D dietary intake is inadequate compared to nutritional requirements. The richest sources of vitamin D, including fortified foods, are insufficiently consumed, particularly by young women and those living in rural areas, who exhibited significantly lower intakes in our sample. Consequently, the prevalence of vitamin D insufficiency/deficiency was high, suggesting that lifestyle factors, including sun exposure and BMI, have a greater influence on vitamin D concentrations in our participants than dietary vitamin D intake.
Average intake
The average vitamin D intake from food was 3.63 (2.73) µg/day, which is in line to the mean intake reported in women from countries with comparable dietary patterns and cultural practices, such as Saudi Arabia (3.52 µg/day), Libya (3.9 µg/day), and Egypt (3.27 ± 3.53 µg/day). A national nutritional survey in Canada among the same age group showed a similar intake of 3.70 µg/day. The European Prospective Investigation into Cancer and Nutrition (EPIC) study observed a slightly lower intake of 3.3 µg/day among women in ten European countries (excluding supplements), with higher estimates in northern regions like Norway, Sweden, and Denmark.
Nationally, Benhamou et al. reported a much lower vitamin D intake of 1.85 µg/day in 101 Moroccan women compared to our participants. Accurate comparison of vitamin D intake between studies is challenging due to variations in dietary assessment methodologies [24,52]. We used a vitamin D-specific item and a validated FFQ for Moroccan WRA whereas the cited study employed an adapted FFQ focusing on adherence to the Mediterranean diet in populations from Palestine, Spain, and Morocco, rather than on precise nutrient intake. Additionally, the two FFQs had different time frames; one month for our assessment versus twelve months for the previous study potentially leading to underestimation of daily vitamin D intake due to recall bias. Differences in age classification and food composition tables also need to be considered.
Adequacy of intake and food sources:
International nutritional guidelines for evaluating vitamin D dietary intake adequacy have sparked significant controversy. The Institute of Medicine, the European Food Safety Authority, and the Endocrine Society state that a target vitamin D status corresponding to a blood level of 20 ng/mL in adults of both sexes can be achieved with dietary vitamin D intakes of 15 μg/day (600 IU), assuming minimal sun exposure. In contrast, Nordic countries, France, and the United Kingdom recommend 10 μg/day, while DACH countries recommend up to 20 μg/day [53]. Conversely, the WHO/FAO assumes that dietary vitamin D requirements can be lower, even set to zero with regular UVB sunlight exposure and adequate skin synthesis. They recommend an intake of 5 μg/day for the general population aged 0 to 50 years, including pregnant and lactating women [43]. Moroccan national recommendations, applied within the context of the food fortification policy, use the same reference value of 5 μg/day [54]. Additionally, the Ministry of Health and Social Protection has implemented oral supplementation of vitamin D2 for children, pregnant, and lactating women in primary healthcare settings.
Despite these guidelines, our results indicate that the majority (88.28%) of the women in our study did not meet the adequate level of 5 μg/day. The estimated intake would be considerably lower if we refer to the Institute of Medicine’s recommendation of 15 μg/day, representing only 19.33% of the participants’ vitamin D requirements. This finding reflects a common issue observed worldwide among women, regardless of variations in nutrient requirements, seen in the Middle East [55,56], North Africa [57,58], US [59], Canada [31], UK (Public health England and food standard agency, 2020). In the EPIC study, the average vitamin D intake below current recommendations for a significant proportion of the European female population (up to 98%) except in Nordic countries (Freisling, 2010). For instance, Finland’s 2012 FINDIET national survey showed an average intake of 8.6 μg/day among women, covering over 86% of their 10 μg vitamin D requirement, primarily due to systematic fortification of dairy products, margarine, and fat spreads since 2010 [34].
In Morocco, few staple foods are vitamin D fortified on a voluntary basis. Ninety percent of edible oils available in markets are fortified with vitamin D3 at a level of 7.5 μg/100g, intended to supply 30% of daily vitamin D requirements [54,61]. Most commercial margarines contain the same amount. Pasteurized cow milk used to be fortified with 0.85 μg/100 ml of vitamin D3, aiming to meet 17% of daily requirements, but most commercial milk now is half-skimmed and lack explicit fortification labels except for few brands of ultra-high-temperature and lactose-reduced milk. Some other brands of plant-based milk, beverages, yogurts, and breakfast cereals label vitamin D content exceeding 0.95 μg/100 ml. However, it is likely challenging for most individuals to achieve sufficient vitamin D intake through current fortification practices alone. For example, to reach an intake of 5 μg/day, one would need to consume the equivalent of 4-5 tablespoons of margarine, 6 tablespoons of edible oil, or 600 ml of fortified milk daily. Despite combined consumption, achieving the necessary frequency and quantity is challenging and unlikely to benefit the general population.
Our analysis of vitamin D food sources confirmed that fortified items are not part of the participants’ daily consumption patterns. While 77.18% of participants consumed edible oil daily, over 46% and 88% did not consume margarine or breakfast cereals, respectively. Consequently, these foods contributed only 6.19% to the participants’ total vitamin D intake. Dairy products, including fortified milk, were consumed daily by 58.6% of women and accounted for 24.5% of total intake. The high consumption of tea among Moroccan women (97.29%) has reduced the daily consumption frequency of dairy beverages [36], limiting the benefit of bioavailable added vitamin D in these products for improving 25(OH) D status.
The major food sources of vitamin D vary according to fortification practices. In countries with mandatory fortification policies like the US, milk is a significant contributor to vitamin D intake among women (39%). In Canada, fortified milk, soy beverages, and powdered milk contribute 27.1% of intake, while margarine contributes 17.3%, and meat and alternatives contribute 17.8% [31]. In the FINDIET study, fortified products contributed 38% of total vitamin D intake among young women, primarily through dairy products and fat spreads, with fish contributing 18% [34]. The national individual food consumption (INCA 3) study in France showed that vitamin D intake mainly comes from meat, fish, eggs, and derived products (39%), with 25% from dairy [62]. The latest National Diet and Nutrition Survey (SACN) in the UK indicates a higher percentage of contribution from meat and meat products (25%), eggs and egg products (22%), and fish (17%), with notable contributions from fortified cereals (16%) and lesser from dairy products (8%) [60].
In our study, fish consumption was the primary dietary source of vitamin D (48%), followed by meat, poultry, and related products (9.4%) and eggs (6.27%). This reflects a Mediterranean diet pattern characterized by plant-based foods, moderate fish and seafood consumption, and limited meat intake. Our findings align with studies in northern Mediterranean areas like Libya [57], Egypt [63], and Spain [64], where fish significantly contributes to women’s vitamin D intake (63%, 56.26%, and 30.4%, respectively). Among fish, sardines, both fresh and canned, were the most frequently consumed, followed by mackerel. Morocco, as the world’s largest producer and exporter of sardines [65], provides affordable and accessible sources rich in vitamin D3 (14 µg/100 g fresh, 12.5 µg/100 g grilled). Promoting fish consumption, particularly sardines, at an adequate frequency (one-two servings per week) and with appropriate culinary techniques could significantly improve vitamin D intake and 25(OH)D status in premenopausal [66] Moroccan women, potentially benefiting bone mass and density [67] and health issues like breast cancer [68] and metabolic syndrome [69] among many others.
Vitamin D dietary intake determinants
Related to determinants of vitamin D intake, special attention should be given to young and rural women. Our analysis indicates that younger women (18-25 years) exhibit concerningly lower intake and lower achievement rates of the recommended intake (RI). Their dietary patterns are more inclined towards a Western diet, with a 14% reduction in fish consumption (36.73%) and higher intake of dairy products and red meats or poultry (29%), contrasting with older women’s dietary habits. Accumulating evidence shows that the richest sources of vitamin D are frequently not included in sufficient amounts in young women’s diets. In a study of 1,032 young Polish women aged 19-30 years, 95% had insufficient vitamin D intake, despite the strong association between consumption of fatty fish (sardines, salmon, and tuna) and vitamin D intake (0.53, p<0.0001) [70]. Similarly, the 2003-2006 National Health and Nutrition Examination Survey (NHANES) reported the lowest vitamin D intake in young female age groups (19-30 years). Brouzes et al. (2020) found similar results in 130 Egyptian urban women aged 19-30, where intake was high in energy and sodium but showed a high prevalence of inadequate vitamin D intake (82%), along with other essential micronutrients like iron and folate [63].
In another study, Zareif et al. (2018) showed that increased age was an independent determinant of sufficient vitamin D intake in 257 premenopausal women in Jeddah, Saudi Arabia (p<0.001). Middle-aged women (31-50 years) had higher intake of vitamin D-rich foods and supplements (44%) compared to younger women (20-30 years, 25%), who were at greater risk of deficiency [56]. However, systematic supplementation of vitamin D is not a common practice in Morocco, apart from medical prescriptions [71]. In our analysis, we could not conclude the impact of supplement use on total intake due to limited information on the types of supplements consumed and the low number of supplement users, who were excluded.
Regarding the influence of other sociodemographic factors on habitual vitamin D intake, previous research suggests that higher education levels are positively associated with healthier diets, better adherence to vitamin D dietary recommendations, and increased vitamin D intake [72,73,74,75,76]. In contrast, we did not observe such an association in our sample. Although, illiterate women exhibited slightly lower vitamin D intake compared to higher education level groups, this difference did not reach statistical significance. One possible reason is the relatively small proportion of illiterate participants in our study, accounting for only 18% of the sample.
Urban residency significantly contributes to higher vitamin D intake, with urban women more inclined to consume animal-rich sources, including fish, meat-poultry, and dairy, compared to rural women (54% vs. 46%, respectively). Similarly, a study in Lebanon found that rural residence negatively impacted vitamin D intake, reflecting higher consumption of fortified milk, meats, poultry, and sweets among urban dwellers. This finding is moroeovre in concert with local research, reporting geographic disparities in food consumption and dietary habit [75,77], In rural Moroccan populations, including WRA, access to fresh produce and nutrient-dense foods is limited due to geographical distance from markets and the reduced availability of food variety [36,75]. Additionally, the COVID-19 crisis has enlarged poverty and unemployment in rural household, leading to a significant reduction in food consumption, specifically animal derived sources of vitamin D [78]
Predictors of serum 25(OH)D
Lastly, we investigated the association between estimated vitamin D dietary intake and circulating 25(OH)D concentration. The average serum 25(OH)D concentration was 15.7 ng/mL (±12.4), with only 11.8% of women having optimal levels, while the majority had either vitamin D deficiency (65.1%) or insufficiency (23.1%). This highlights that vitamin D inadequacy is a significant concern among Moroccan premenopausal women [36,79]. Despite this, dietary vitamin D intake in our participants showed no significant effect on serum 25(OH)D levels, although a weak linear correlation was noted in the initial analysis. Similarly, an observational study conducted in Spain demonstrated that when dietary intake is inadequate, it does not exhibit a meaningful correlation with serum 25(OH)D levels. Other reports have hypothesized that the relationship between vitamin D intake and its biomarkers may not follow a simple linear pattern due to interindividual variations in response [80]. It has been estimated that the response of serum 25(OH)D to 1 μg of vitamin D3 intake is inversely dependent on the basal 25(OH)D concentration [81]. Thus, we assume that even with adequate dietary intake, the potential correlation in our sample may not have been observed, particularly given the low baseline 25(OH)D levels in our sample. Vitamin D supplementation is likely necessary, especially for women with low baseline 25(OH)D levels, to achieve and maintain optimal vitamin D status.
Additionally, the sun exposure score was a positive predictor of participants’ serum 25(OH)D3 levels, independent of other sociodemographic and lifestyle factors (p = 0.008). Each one-point increase in the sun exposure score corresponded to a 0.343 ng/mL rise in 25(OH)D3 levels. Although the observed effect was moderate, it aligns with findings from other studies that used a similar scoring system to assess sun exposure behavior in women [82]. In contrast, studies using direct measures of UV exposure with dosimeters reported that a 10-minute increase in UV exposure time, particularly in the summer, was sufficient to increase participants’ 25(OH)D by 0.47 ng/mL [83]. Thus, promoting UV light exposure as a crucial source of dermal vitamin D synthesis [15], would contribute to improved 25(OH)D levels in our women participants.
Additionally, considering individual characteristics and lifestyle factors is important in interpreting 25(OH)D concentrations. Increasing age was positively associated with higher 25(OH)D levels, likely due to greater vitamin D intake and fish consumption. However, higher BMI was a strong negative determinant of 25(OH)D levels (β(SE): −1.128 (0.337)). This observation supports the hypothesis that High content of body fat acts as a reservoir for lipid soluble vitamin D and increases its sequestration, thus lead to low bioavailability [84] and inadequate vitamin D status at individual level [85]. The high prevalence of overweight and obesity (57.8%) observed in our analysis further justifies the need for future research to explore the role of diet, sun exposure, and other factors in characterizing vitamin D status among obese Moroccan women, particularly in the context of the double burden of malnutrition in our country.
Limits and strengths
There are some strengths and limitations in the presents study we need to address. We used validated questionnaires, specifically designed to assess the main variables under study (food-frequency questionnaire for vitamin D intake and sun exposure score questionnaire for sun exposure behavior estimates), which adds accuracy to our analysis. This is the first initiative to simultaneously evaluate the contributions of both endogenous (UV exposure) and exogenous (vitamin D intake) sources to serum vitamin D concentration in the Moroccan context. In addition, we collected detailed covariate data, allowing for adjustments for relevant confounding variables, which enhances the reliability of our findings.
However, the sample size was based on a power calculation using vitamin D deficiency as the primary endpoint in women living in the city of Meknes. Therefore, our results may not be representative of all premenopausal women in Morocco. Furthermore, we did not apply the energy adjusted intake in the analysis, as the used VitD-FFQ was not designed for energy assessment. Thus, we focused on both continuous and categories comparison of the absolute vitamin D intake with respect to socio-demographic characteristics.
5. Conclusions
In conclusion, the dietary intake of vitamin D among premenopausal Moroccan women is insufficient to meet their requirements, with young women and rural dwellers being particularly at risk. Current levels of vitamin D food fortification are inadequate to achieve the required intake or to prevent widespread VDD among these women. To effectively address this issue, it is crucial to identify suitable food vehicles, preferably staple foods, that can significantly enhance the vitamin D intake of the target group. Fortifying wheat flour, a staple in Morocco, may be a cost-effective strategy to reduce vitamin D deficiency [86]. A recent study have moreover, demonstrated the effectiveness of milk fortification in improving vitamin D levels among children form rural region in Morocco [87]. Expanding mandatory milk fortification could similarly benefit young women and other vulnerable populations. Furthermore, balancing the environmental advantage of sunlight viability alongside increased dietary intake and addressing obesity could further enhance serum vitamin D levels in premenopausal women in Morocco.
Author Contributions
Conceptualization, N.Z, Y.F.Z, and S.E.J; methodology N.Z; software, N.Z, Y.F.Z.; validation, NZ, YFZ; formal analysis, N.Z, Y.F.Z; investigation, N.Z; IL; resources, NZ; IL; data curation, N.Z, Y.F.Z; writing—original draft preparation, N.Z.; writing—review and editing, NZ, A.E.M, Y.F.Z and LG; visualization, N.Z.; supervision, N.Z; Y.F.Z; S.E.J and L.G; project administration, Y.F.Z; S.E.J; funding acquisition, Y.F.Z and LG. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the Institutional University Cooperation program with Moulay Ismail University, which is funded by the VLIR-UOS (Phase I: 2017-2021; Contract no MA2017IUC038A104) and by the Research and Development Project “SEBIO” (Morocco, 2017–2021), funded by the ARES-CCD of the Belgian Cooperation for Development. The supporting source had no such involvement or restrictions regarding publication.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the ethics committee of biomedical research at Moulay Ismail University (reference; N°1/CERB-UMI/19).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The datasets generated and analyzed for the current study are available from the corresponding author, upon reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Janoušek, J.; Pilařová, V.; Macáková, K.; Nomura, A.; Veiga-Matos, J.; Silva, D.D.D.; Remião, F.; Saso, L.; Malá-Ládová, K.; Malý, J.; et al. Vitamin D: Sources, Physiological Role, Biokinetics, Deficiency, Therapeutic Use, Toxicity, and Overview of Analytical Methods for Detection of Vitamin D and Its Metabolites. Crit. Rev. Clin. Lab. Sci. 2022, 59, 517–554. [Google Scholar] [CrossRef] [PubMed]
- DeLuca, H.F. Vitamin D. In Vitamins & Hormones; Elsevier, 2016; Vol. 100, pp. 1–20 ISBN 978-0-12-804824-5.
- Bergwitz, C.; Jüppner, H. Regulation of Phosphate Homeostasis by PTH, Vitamin D, and FGF23. Annu. Rev. Med. 2010, 61, 91–104. [Google Scholar] [CrossRef] [PubMed]
- Bouillon, R.; Marcocci, C.; Carmeliet, G.; Bikle, D.; White, J.H.; Dawson-Hughes, B.; Lips, P.; Munns, C.F.; Lazaretti-Castro, M.; Giustina, A.; et al. Skeletal and Extraskeletal Actions of Vitamin D: Current Evidence and Outstanding Questions. Endocr. Rev. 2019, 40, 1109–1151. [Google Scholar] [CrossRef] [PubMed]
- Hanel, A.; Carlberg, C. Time-Resolved Gene Expression Analysis Monitors the Regulation of Inflammatory Mediators and Attenuation of Adaptive Immune Response by Vitamin D. Int. J. Mol. Sci. 2022, 23, 911. [Google Scholar] [CrossRef]
- Creo, A.L.; Thacher, T.D.; Pettifor, J.M.; Strand, M.A.; Fischer, P.R. Nutritional Rickets around the World: An Update. Paediatr. Int. Child Health 2017, 37, 84–98. [Google Scholar] [CrossRef]
- Berridge, M.J. Vitamin D Deficiency and Diabetes. Biochem. J. 2017, 474, 1321–1332. [Google Scholar] [CrossRef]
- Ghaseminejad-Raeini, A.; Ghaderi, A.; Sharafi, A.; Nematollahi-Sani, B.; Moossavi, M.; Derakhshani, A.; Sarab, G.A. Immunomodulatory Actions of Vitamin D in Various Immune-Related Disorders: A Comprehensive Review. Front. Immunol. 2023, 14, 950465. [Google Scholar] [CrossRef]
- Cuomo, A.; Maina, G.; Bolognesi, S.; Rosso, G.; Beccarini Crescenzi, B.; Zanobini, F.; Goracci, A.; Facchi, E.; Favaretto, E.; Baldini, I.; et al. Prevalence and Correlates of Vitamin D Deficiency in a Sample of 290 Inpatients With Mental Illness. Front. Psychiatry 2019, 10, 167. [Google Scholar] [CrossRef]
- Jorge, A.J.L.; Cordeiro, J.R.; Rosa, M.L.G.; Bianchi, D.B.C. Vitamin D Deficiency and Cardiovascular Diseases. Int. J. Cardiovasc. Sci. 2018. [Google Scholar] [CrossRef]
- McCullough, M.L.; Zoltick, E.S.; Weinstein, S.J.; Fedirko, V.; Wang, M.; Cook, N.R.; Eliassen, A.H.; Zeleniuch-Jacquotte, A.; Agnoli, C.; Albanes, D.; et al. Circulating Vitamin D and Colorectal Cancer Risk: An International Pooling Project of 17 Cohorts. JNCI J. Natl. Cancer Inst. 2019, 111, 158–169. [Google Scholar] [CrossRef]
- Fernando, M.; Ellery, S.J.; Marquina, C.; Lim, S.; Naderpoor, N.; Mousa, A. Vitamin D-Binding Protein in Pregnancy and Reproductive Health. Nutrients 2020, 12, 1489. [Google Scholar] [CrossRef] [PubMed]
- Binkley, N.; Bikle, D.D.; Dawson-Hughes, B.; Plum, L.; Sempos, C.; DeLuca, H.F. Nonskeletal Effects of Vitamin D. In Principles of Bone Biology; Elsevier, 2020; pp. 757–774 ISBN 978-0-12-814841-9.
- Grant, W.B.; Cross, H.S.; Garland, C.F.; Gorham, E.D.; Moan, J.; Peterlik, M.; Porojnicu, A.C.; Reichrath, J.; Zittermann, A. Estimated Benefit of Increased Vitamin D Status in Reducing the Economic Burden of Disease in Western Europe. Prog. Biophys. Mol. Biol. 2009, 99, 104–113. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. Ultraviolet B Radiation: The Vitamin D Connection. Adv. Exp. Med. Biol. 2017, 996, 137–154. [Google Scholar] [CrossRef] [PubMed]
- Clemens, T.L.; Henderson, S.L.; Adams, J.S.; Holick, M.F. INCREASED SKIN PIGMENT REDUCES THE CAPACITY OF SKIN TO SYNTHESISE VITAMIN D3. The Lancet 1982, 319, 74–76. [Google Scholar] [CrossRef] [PubMed]
- Chakhtoura, M.; Rahme, M.; Chamoun, N.; El-Hajj Fuleihan, G. Vitamin D in the Middle East and North Africa. Bone Rep. 2018, 8, 135–146. [Google Scholar] [CrossRef]
- McCarty, C.A. Sunlight Exposure Assessment: Can We Accurately Assess Vitamin D Exposure from Sunlight Questionnaires? Am. J. Clin. Nutr. 2008, 87, 1097S–1101S. [Google Scholar] [CrossRef]
- Cashman, K.D.; Dowling, K.G.; Škrabáková, Z.; Gonzalez-Gross, M.; Valtueña, J.; De Henauw, S.; Moreno, L.; Damsgaard, C.T.; Michaelsen, K.F.; Mølgaard, C.; et al. Vitamin D Deficiency in Europe: Pandemic? Am. J. Clin. Nutr. 2016, 103, 1033–1044. [Google Scholar] [CrossRef]
- Holick, M.F. The Vitamin D Deficiency Pandemic: Approaches for Diagnosis, Treatment and Prevention. Rev. Endocr. Metab. Disord. 2017, 18, 153–165. [Google Scholar] [CrossRef]
- Mogire, R.M.; Mutua, A.; Kimita, W.; Kamau, A.; Bejon, P.; Pettifor, J.M.; Adeyemo, A.; Williams, T.N.; Atkinson, S.H. Prevalence of Vitamin D Deficiency in Africa: A Systematic Review and Meta-Analysis. Lancet Glob. Health 2020, 8, e134–e142. [Google Scholar] [CrossRef]
- Lips, P.; Cashman, K.D.; Lamberg-Allardt, C.; Bischoff-Ferrari, H.A.; Obermayer-Pietsch, B.; Bianchi, M.L.; Stepan, J.; El-Hajj Fuleihan, G.; Bouillon, R. Current Vitamin D Status in European and Middle East Countries and Strategies to Prevent Vitamin D Deficiency: A Position Statement of the European Calcified Tissue Society. Eur. J. Endocrinol. 2019, 180, P23–P54. [Google Scholar] [CrossRef]
- Brannon, P.M.; Picciano, M.F. Vitamin D in Pregnancy and Lactation in Humans. Annu. Rev. Nutr. 2011, 31, 89–115. [Google Scholar] [CrossRef] [PubMed]
- Cashman, K.D. Global Differences in Vitamin D Status and Dietary Intake: A Review of the Data. Endocr. Connect. 2022, 11, e210282. [Google Scholar] [CrossRef] [PubMed]
- Ganji, V.; Shi, Z.; Al-Abdi, T.; Al Hejap, D.; Attia, Y.; Koukach, D.; Elkassas, H. Association between Food Intake Patterns and Serum Vitamin D Concentrations in US Adults. Br. J. Nutr. 2023, 129, 864–874. [Google Scholar] [CrossRef] [PubMed]
- Armas, L.A.G.; Hollis, B.W.; Heaney, R.P. Vitamin D 2 Is Much Less Effective than Vitamin D 3 in Humans. J. Clin. Endocrinol. Metab. 2004, 89, 5387–5391. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F.; Biancuzzo, R.M.; Chen, T.C.; Klein, E.K.; Young, A.; Bibuld, D.; Reitz, R.; Salameh, W.; Ameri, A.; Tannenbaum, A.D. Vitamin D2 Is as Effective as Vitamin D3 in Maintaining Circulating Concentrations of 25-Hydroxyvitamin D. J. Clin. Endocrinol. Metab. 2008, 93, 677–681. [Google Scholar] [CrossRef]
- Roseland, J.M.; Phillips, K.M.; Patterson, K.Y.; Pehrsson, P.R.; Taylor, C.L. Vitamin D in Foods. In Vitamin D; Elsevier, 2018; pp. 41–77 ISBN 978-0-12-809963-6.
- Niedermaier, T.; Gredner, T.; Kuznia, S.; Schöttker, B.; Mons, U.; Lakerveld, J.; Ahrens, W.; Brenner, H. On behalf of the PEN-Consortium Vitamin D Food Fortification in European Countries: The Underused Potential to Prevent Cancer Deaths. Eur. J. Epidemiol. 2022, 37, 309–320. [Google Scholar] [CrossRef]
- Usual Nutrient Intake from Food and Beverages, by Gender and Age, What We Eat in America, NHANES 2013-2016. 2019. Available online: http://Www.Ars.Usda.Gov/Nea/Bhnrc/Fsrg.
- Vatanparast, H.; Patil, R.P.; Islam, N.; Shafiee, M.; Whiting, S.J. Vitamin D Intake from Supplemental Sources but Not from Food Sources Has Increased in the Canadian Population Over Time. J. Nutr. 2020, 150, 526–535. [Google Scholar] [CrossRef]
- Spiro, A.; Buttriss, J.L. Vitamin D: An Overview of Vitamin D Status and Intake in E Urope. Nutr. Bull. 2014, 39, 322–350. [Google Scholar] [CrossRef]
- Petrenya, N.; Lamberg-Allardt, C.; Melhus, M.; Broderstad, A.R.; Brustad, M. Vitamin D Status in a Multi-Ethnic Population of Northern Norway: The SAMINOR 2 Clinical Survey. Public Health Nutr. 2020, 23, 1186–1200. [Google Scholar] [CrossRef]
- Raulio, S.; Erlund, I.; Männistö, S.; Sarlio-Lähteenkorva, S.; Sundvall, J.; Tapanainen, H.; Vartiainen, E.; Virtanen, S.M. Successful Nutrition Policy: Improvement of Vitamin D Intake and Status in Finnish Adults over the Last Decade. Eur. J. Public Health 2016, ckw154. [Google Scholar] [CrossRef]
- Calvo, M.S.; Whiting, S.J.; Barton, C.N. Vitamin D Intake: A Global Perspective of Current Status. J. Nutr. 2005, 135, 310–316. [Google Scholar] [CrossRef] [PubMed]
- PNN, Enquête Nationale sur la Nutrition, Diversité alimentaire, Carence en Fer, Carence en Vitamine A, Carence en Iode, 2019. Available online: https://www.sante.gov.ma/Documents/2022/07/rapport%20ENN%202019-2020%20ajout%20preface%20(1).pdf.
- Allali, F.; El Aichaoui, S.; Khazani, H.; Benyahia, B.; Saoud, B.; El Kabbaj, S.; Bahiri, R.; Abouqal, R.; Hajjaj-Hassouni, N. High Prevalence of Hypovitaminosis D in Morocco: Relationship to Lifestyle, Physical Performance, Bone Markers, and Bone Mineral Density. Semin. Arthritis Rheum. 2009, 38, 444–451. [Google Scholar] [CrossRef]
- Baki, S.; El Mghari, G.; El Ansari, N.; Harkati, I.; Tali, A.; Chabaa, L. Statut de la vitamine de la vitamine D chez les femmes marocaines vivant a Marrakech. Ann. Endocrinol. 2015, 76, 490. [Google Scholar] [CrossRef]
- Dadda, S.; Azekour, K.; Sebbari, F.; El Houate, B.; El Bouhali, B. Sun Exposure, Dressing Habits, and Vitamin D Status in Morocco. E3S Web Conf. 2021, 319, 01097. [Google Scholar] [CrossRef]
- Benhammou, S.; Heras-González, L.; Ibáñez-Peinado, D.; Barceló, C.; Hamdan, M.; Rivas, A.; Mariscal-Arcas, M.; Olea-Serrano, F.; Monteagudo, C. Comparison of Mediterranean Diet Compliance between European and Non-European Populations in the Mediterranean Basin. Appetite 2016, 107, 521–526. [Google Scholar] [CrossRef] [PubMed]
- Glenn, D.I.; Glenn, D.; Israel. Determining Sample Size 1. University of Florida IFAS Extension. pp. 1–5. Available online: Http://Edis.Ifas.Ufl.Edu (accessed on 10 February 2019).
- Zouine, N.; Lhilali, I.; Menouni, A.; Godderis, L.; El Midaoui, A.; El Jaafari, S.; Zegzouti Filali, Y. Development and Validation of Vitamin D- Food Frequency Questionnaire for Moroccan Women of Reproductive Age: Use of the Sun Exposure Score and the Method of Triad’s Model. Nutrients 2023, 15, 796. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO)and Food and Agriculture Organization (FAO). Vitamin and Mineral Requirments in Human Nutrition.Second Edition [Cited 2023 Oct 15]; Available from: Https://Iris.Who.Int/Bitstream/Handle/10665/42716/9241546123.PDF Sequence=1; WHO and FAO, Ed.; 2. ed.; Geneva, 2004; ISBN 978-92-4-154612-6.
- Lhilali, I.; Zouine, N.; Menouni, A.; Godderis, L.; Kestemont, M.-P.; El Midaoui, A.; El Jaafari, S.; Filali-Zegzouti, Y. Sun Exposure Score and Vitamin D Levels in Moroccan Women of Childbearing Age. Nutrients 2023, 15, 688. [Google Scholar] [CrossRef]
- Graig et al Craig, C., Marshall, A., Sjostrom, M.; et al. International Physical Activity Questionnaire-Short Form. J Am Coll Health, 2017, Vol. 65, No 7, p. 492-501.; 2017.
- Forde Forde, C. Scoring the International Physical Activity Questionnaire (IPAQ); University of Dublin: Dublin, Ireland, 2018; p. 3I. [Google Scholar]
- Holick, M.F. The Vitamin D Deficiency Pandemic: Approaches for Diagnosis, Treatment and Prevention. Rev. Endocr. Metab. Disord. 2017, 18, 153–165. [Google Scholar] [CrossRef]
- Bouillon, R.; Van Schoor, N.M.; Gielen, E.; Boonen, S.; Mathieu, C.; Vanderschueren, D.; Lips, P. Optimal Vitamin D Status: A Critical Analysis on the Basis of Evidence-Based Medicine. J. Clin. Endocrinol. Metab. 2013, 98, E1283–E1304. [Google Scholar] [CrossRef]
- Holick, M.F. Vitamin D Status: Measurement, Interpretation, and Clinical Application. Ann. Epidemiol. 2009, 19, 73–78. [Google Scholar] [CrossRef]
- Geng, J.; Qiu, Y.; Li, Y.; Li, J.; Liao, R.; Du, H.; Jiang, L.; Wang, L.; Qin, Z.; Yang, Q.; et al. Associations Between 25-Hydroxyvitamin D, Kidney Function, and Insulin Resistance Among Adults in the United States of America. Front. Nutr. 2022, 8, 716878. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S. A More Accurate Method To Estimate Glomerular Filtration Rate from Serum Creatinine: A New Prediction Equation. Ann. Intern. Med. 1999, 130, 461. [Google Scholar] [CrossRef]
- Spiro, A.; Buttriss, J.L. Vitamin D: An Overview of Vitamin D Status and Intake in E Urope. Nutr. Bull. 2014, 39, 322–350. [Google Scholar] [CrossRef]
- Bouillon, R. Comparative Analysis of Nutritional Guidelines for Vitamin D. Nat. Rev. Endocrinol. 2017, 13, 466–479. [Google Scholar] [CrossRef] [PubMed]
- Benazouz, E.M.; Majdi, M.; Aguenaou, H.; Benazouz, E.M.; Majdi, M.; Aguenaou, H. Référentiel Législatif et Réglementaire Relatif à La Fortification Des Denrées Alimentaires Par l’adjonction de Vitamines et de Minéraux, ONSSA/MS/GAIN/UNICEF: Maroc, 2006; 2006.
- Gannagé-Yared; Chemali; Sfeir; Maalouf; Halaby Dietary Calcium and Vitamin D Intake in an Adult Middle Eastern Population: Food Sources and Relation to Lifestyle and PTH. Int. J. Vitam. Nutr. Res. 2005, 75, 281–289. [CrossRef]
- Zareef, T.A.; Jackson, R.T.; Alkahtani, A.A. Vitamin D Intake among Premenopausal Women Living in Jeddah: Food Sources and Relationship to Demographic Factors and Bone Health. J. Nutr. Metab. 2018, 2018, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Faid, F.; Nikolic, M.; Milesevic, J.; Zekovic, M.; Kadvan, A.; Gurinovic, M.; Glibetic, M. Assessment of Vitamin D Intake among Libyan Women—Adaptation and Validation of Specific Food Frequency Questionnaire. Libyan J. Med. 2018, 13, 1502028. [Google Scholar] [CrossRef] [PubMed]
- Naifar, M.; Jerbi, A.; Turki, M.; Fourati, S.; Sawsan, F.; Bel Hsan, K.; Elleuch, A.; Chaabouni, K.; Ayedi, F. Valeurs de référence de la vitamine D chez la Femme du Sud Tunisien. Nutr. Clin. Métabolisme 2020, 34, 169–176. [Google Scholar] [CrossRef]
- Andrade, J.M.; Grandoff, P.G.; Schneider, S.T. Vitamin D Intake and Factors Associated With Self-Reported Vitamin D Deficiency Among US Adults: A 2021 Cross-Sectional Study. Front. Nutr. 2022, 9, 899300. [Google Scholar] [CrossRef]
- Public health Englend and food standard agency. National nutrition and diet survey (NNDS): Yeras 9 to 11 of the rolling programme (2016-2017) to (2018-2019). Available online: https://www.gov.uk/government/statistics/ndns-results-from-years-9-to-11-2016-to-2017-and-2018-to-2019.
- Aguenaou, H.; Rahmani, M. Dossier Technique de la Fortification du Lait. 2007.
- Anses Anses et Rapport d’expertise Collective Saisine 2014-SA-0234 « Etude INCA3 » Étude Individuelle Nationale Des Consommations Alimentaires 3 (INCA 3); 2014.
- Brouzes, C.M.; Darcel, N.; Tomé, D.; Dao, M.C.; Bourdet-Sicard, R.; Holmes, B.A.; Lluch, A. Urban Egyptian Women Aged 19–30 Years Display Nutrition Transition-Like Dietary Patterns, with High Energy and Sodium Intakes, and Insufficient Iron, Vitamin D, and Folate Intakes. Curr. Dev. Nutr. 2020, 4, nzz143. [Google Scholar] [CrossRef]
- González-Rodríguez, L.G.; Estaire, P.; Peñas-Ruiz, C.; Ortega, R.M. UCM Research Group VALORNUT (920030) Vitamin D Intake and Dietary Sources in a Representative Sample of Spanish Adults. J. Hum. Nutr. Diet. Off. J. Br. Diet. Assoc. 2013, 26 Suppl 1, 64–72. [Google Scholar] [CrossRef]
- Naji, M.; Fatih, M.; Ebndaoud, G. Moroccan Canned Sardines Value Chain: Governance and Value Added Distribution. Int. J. Dev. Econ. Sustain. 2015, 3(2), 11–24. [Google Scholar]
- Lehmann, U.; Gjessing, H.R.; Hirche, F.; Mueller-Belecke, A.; Gudbrandsen, O.A.; Ueland, P.M.; Mellgren, G.; Lauritzen, L.; Lindqvist, H.; Hansen, A.L.; et al. Efficacy of Fish Intake on Vitamin D Status: A Meta-Analysis of Randomized Controlled Trials. Am. J. Clin. Nutr. 2015, 102, 837–847. [Google Scholar] [CrossRef] [PubMed]
- Del Brutto, O.H.; Mera, R.M.; Rumbea, D.A.; Arias, E.E.; Guzmán, E.J.; Sedler, M.J. On the Association between Dietary Oily Fish Intake and Bone Mineral Density in Frequent Fish Consumers of Amerindian Ancestry. The Three Villages Study. Arch. Osteoporos. 2024, 19, 31. [Google Scholar] [CrossRef] [PubMed]
- Nindrea, R.D.; Aryandono, T.; Lazuardi, L.; Dwiprahasto, I. Protective Effect of Omega-3 Fatty Acids in Fish Consumption Against Breast Cancer in Asian Patients: A Meta-Analysis. Asian Pac. J. Cancer Prev. 2019, 20, 327–332. [Google Scholar] [CrossRef]
- Mendivil, C.O. Fish Consumption: A Review of Its Effects on Metabolic and Hormonal Health. Nutr. Metab. Insights 2021, 14, 117863882110223. [Google Scholar] [CrossRef]
- Utri, Z.; Głąbska, D. Vitamin D Intake in a Population-Based Sample of Young Polish Women, Its Major Sources and the Possibility of Meeting the Recommendations. Foods 2020, 9, 1482. [Google Scholar] [CrossRef]
- Abourazzak, F.E.; Khazzani, H.; Mansouri, S.; Ali, S.; Alla, O.; Allali, F.; Maghraoui, A.E.; Larhrissi, S.; Rachidi, W.; Ichchou, L. Recommandations de la Société Marocaine de Rhumatologie sur la vitamine D chez l’Adulte. 2016.
- Agodi, A.; Maugeri, A.; Magnano San Lio, R.; Favara, G.; Vinciguerra, M.; Barchitta, M. How Does Education Affect Diet in Women? A Comparison between Central and Southern Europe Cohorts. Eur. J. Public Health 2019, 29, ckz185.386. [Google Scholar] [CrossRef]
- Alonso-Cabezas, M.; Pollán, M.; Alonso-Ledesma, I.; Fernández De Larrea-Baz, N.; Lucas, P.; Sierra, Á.; Castelló, A.; Pino, M.N.; Pérez-Gómez, B.; Martínez-Cortés, M.; et al. Sociodemographic and Lifestyle Determinants of Adherence to Current Dietary Recommendations and Diet Quality in Middle-Aged Spanish Premenopausal Women. Front. Nutr. 2022, 9, 904330. [Google Scholar] [CrossRef]
- Amaya-Montoya, M.; Duarte-Montero, D.; Nieves-Barreto, L.D.; Montaño-Rodríguez, A.; Betancourt-Villamizar, E.C.; Salazar-Ocampo, M.P.; Mendivil, C.O. 100 YEARS OF VITAMIN D: Dietary Intake and Main Food Sources of Vitamin D and Calcium in Colombian Urban Adults. Endocr. Connect. 2021, 10, 1584–1593. [Google Scholar] [CrossRef]
- El Rhazi, K.; Nejjari, C.; Romaguera, D.; Feart, C.; Obtel, M.; Zidouh, A.; Bekkali, R.; Gateau, P.B. Adherence to a Mediterranean Diet in Morocco and Its Correlates: Cross-Sectional Analysis of a Sample of the Adult Moroccan Population. BMC Public Health 2012, 12, 345. [Google Scholar] [CrossRef] [PubMed]
- Shahrokhabadi, M.; Abbasnezhad, A.; Kazemnejad, A.; Ghaheri, A.; Zayeri, F. Dietary Intake of Vitamin D Pattern and Its Sociodemographic Determinants in the Southwest of Iran, Khuzestan: An Application of Marginalised Two-Part Model. Adv. Hum. Biol. 2019, 9, 210. [Google Scholar] [CrossRef]
- Nabdi, S.; Boujraf, S.; Benzagmout, M. Evaluation of Rural-Urban Patterns in Dietary Intake: A Descriptive Analytical Study—Case Series. Ann. Med. Surg. 2022, 84. [Google Scholar] [CrossRef] [PubMed]
- Haut Commissariat au Plan du Maroc RépeRcussions de La Pandémie Covid-19 suR La Situation Économique Des Ménages.2ème panel sur l’impact du coronavirus sur la situation économique, sociale et psychologique des ménages; 2022.
- Lhilali, I.; Zouine, N.; Godderis, L.; El Midaoui, A.; El Jaafari, S.; Filali-Zegzouti, Y. Relationship between Vitamin D Insufficiency, Lipid Profile and Atherogenic Indices in Healthy Women Aged 18–50 Years. Eur. J. Investig. Health Psychol. Educ. 2024, 14, 2337–2357. [Google Scholar] [CrossRef]
- Institute of Medicine (US) Committee to Review Dietary Reference Intakes for Vitamin D and Calcium. Dietary Reference Intakes for Calcium and Vitamin D; Ross, A.C., Taylor, C.L., Yaktine, A.L., Del Valle, H.B., Eds.; The National Academies Collection: Reports funded by National Institutes of Health; National Academies Press (US): Washington, DC, USA, 2011. [Google Scholar]
- Aloia, J.F.; Patel, M.; DiMaano, R.; Li-Ng, M.; Talwar, S.A.; Mikhail, M.; Pollack, S.; Yeh, J.K. Vitamin D Intake to Attain a Desired Serum 25-Hydroxyvitamin D Concentration. Am. J. Clin. Nutr. 2008, 87, 1952–1958. [Google Scholar] [CrossRef]
- Mansibang, N.M.M.; Yu, M.G.Y.; Jimeno, C.A.; Lantion-Ang, F.L. Association of Sunlight Exposure with 25-Hydroxyvitamin D Levels among Working Urban Adult Filipinos. Osteoporos. Sarcopenia 2020, 6, 133–138. [Google Scholar] [CrossRef]
- Asakura, K.; Etoh, N.; Imamura, H.; Michikawa, T.; Nakamura, T.; Takeda, Y.; Mori, S.; Nishiwaki, Y. Vitamin D Status in Japanese Adults: Relationship of Serum 25-Hydroxyvitamin D with Simultaneously Measured Dietary Vitamin D Intake and Ultraviolet Ray Exposure. Nutrients 2020, 12, 743. [Google Scholar] [CrossRef]
- Wortsman, J.; Matsuoka, L.Y.; Chen, T.C.; Lu, Z.; Holick, M.F. Decreased Bioavailability of Vitamin D in Obesity. Am. J. Clin. Nutr. 2000, 72, 690–693. [Google Scholar] [CrossRef]
- Mehdad, S.; Belghiti, H.; Zahrou, F.E.; Guerinech, H.; Mouzouni, F.Z.; El Hajjab, A.; El Berri, H.; El Ammari, L.; Benaich, S.; Benkirane, H.; et al. Vitamin D Status and Its Relationship with Obesity Indicators in Moroccan Adult Women. Nutr. Health 2022, 2601060221094376. [Google Scholar] [CrossRef]
- Aguiar, M.; Andronis, L.; Pallan, M.; Högler, W.; Frew, E. The Economic Case for Prevention of Population Vitamin D Deficiency: A Modelling Study Using Data from England and Wales. Eur. J. Clin. Nutr. 2020, 74, 825–833. [Google Scholar] [CrossRef]
- Benjeddou, K.; Qandoussi, L.; Mekkaoui, B.; Rabi, B.; El Hamdouchi, A.; Raji, F.; Saeid, N.; Belghiti, H.; Elkari, K.; Aguenaou, H. Effect of Multiple Micronutrient Fortified Milk Consumption on Vitamin D Status among School-Aged Children in Rural Region of Morocco. Appl. Physiol. Nutr. Metab. 2019, 44, 461–467. [Google Scholar] [CrossRef] [PubMed]
Figure 2.
Food sources contribution in the total estimated vitamin D intake.
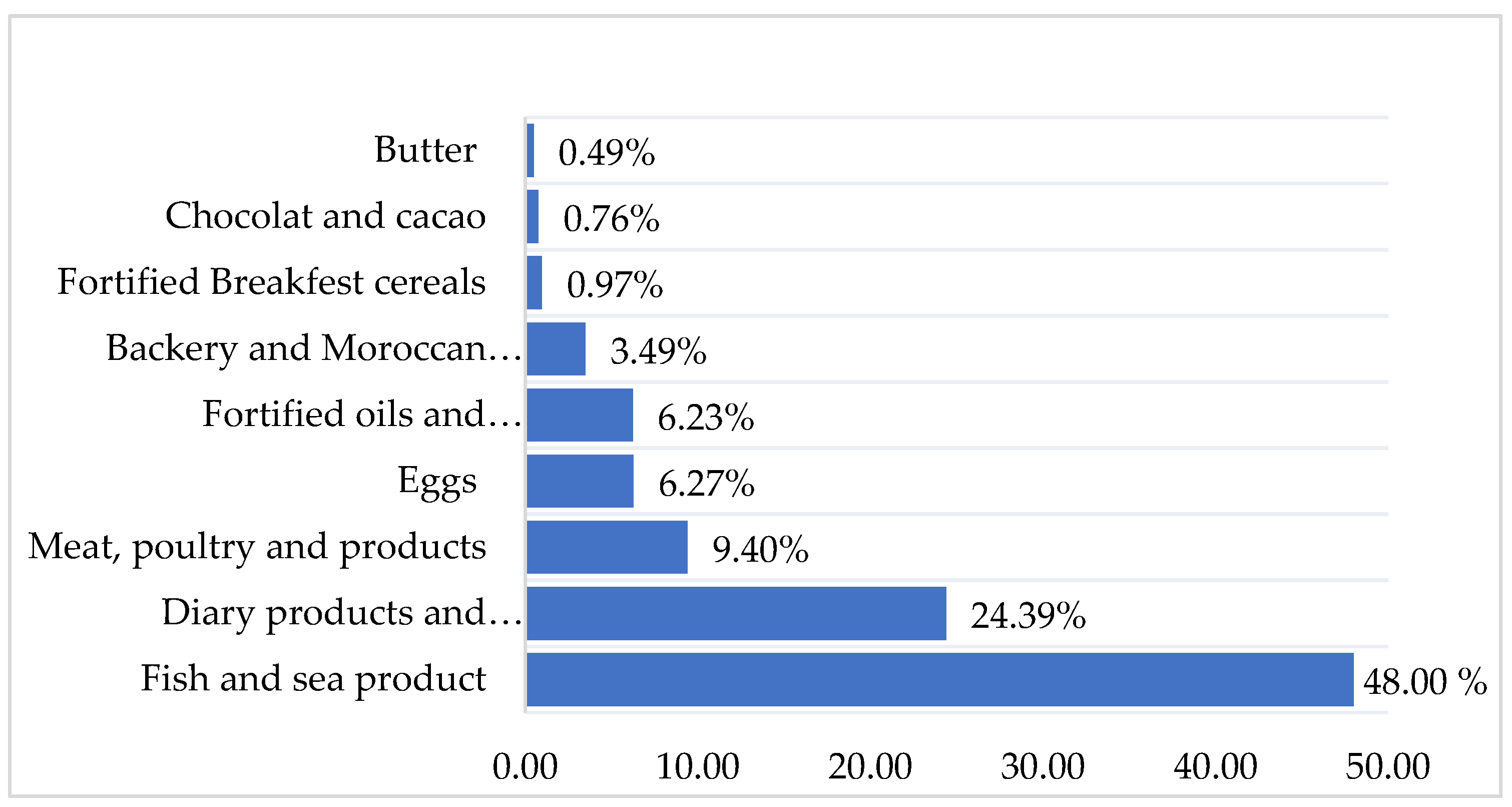
Figure 4.
Satter plot of vitamin D concentrations according to participants dietary intake (µg/day) and sun exposure score.
Figure 4.
Satter plot of vitamin D concentrations according to participants dietary intake (µg/day) and sun exposure score.
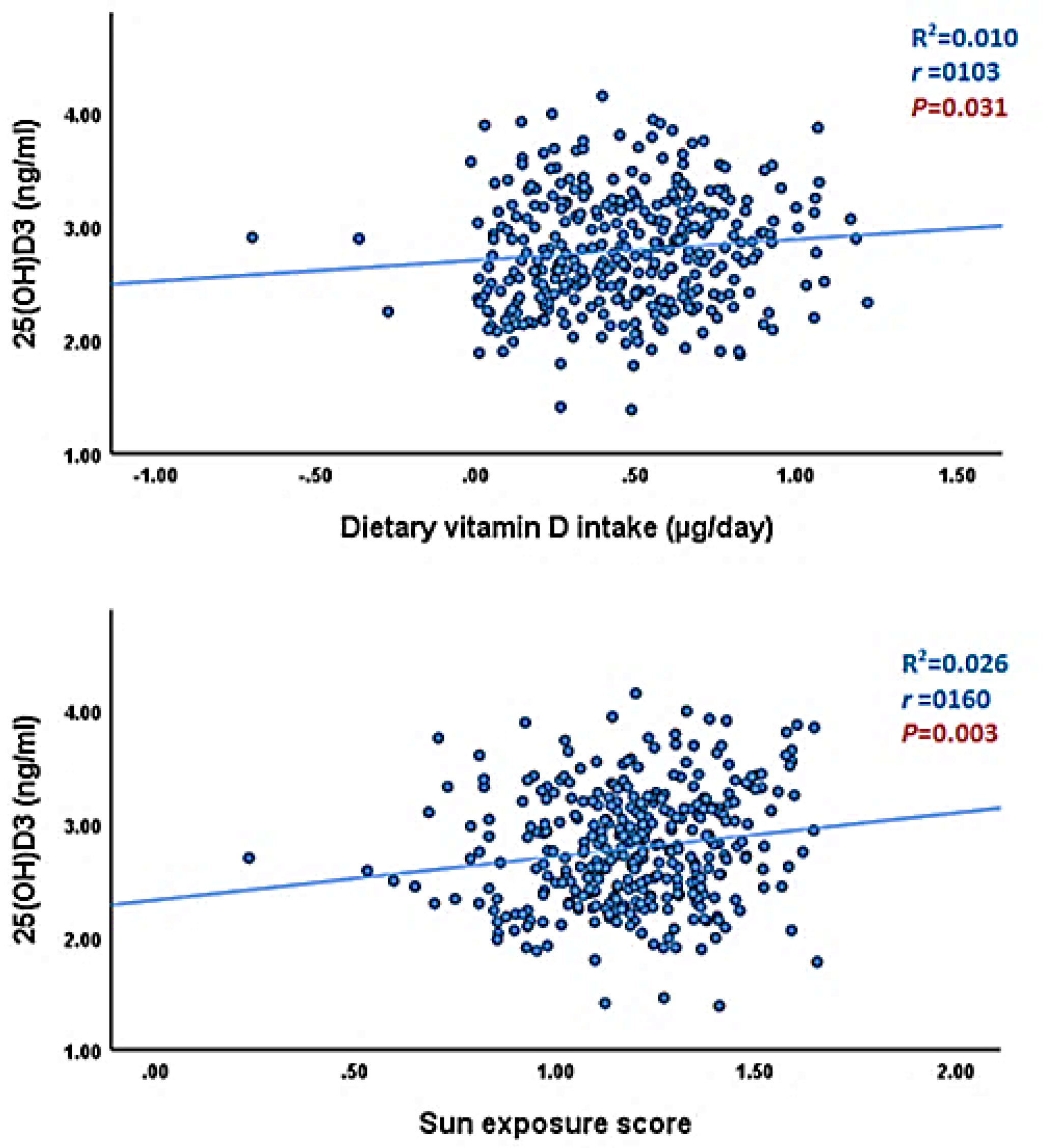
Table 1.
Participants’ general characteristics estimated dietary vitamin D intake (n = 355).
| Variables | All Participants (n = 355) |
|---|---|
| Age (year). median (IQR) | 29.0(11.0) |
| Age classe (n. %) 18-25 26-36 37-49 |
90(25.4) 197(55.5) 68(19.2) |
| Education (n. %) Illiterate ≤10 years (secondary college) ≥11years (university or higher) |
64(18.0) 166(46.8) 125(35.2) |
| Marital status (n. %) Married Unmarried |
227(63.9) 128(36.1) |
| Employment (n. %) Yes No |
157(44.2) 198(55.8) |
| Localization (n. %) Urban Rural |
239(67.3) 116(32.7) |
| Vitamin D intake (µg/day) Mean (SD) Median (IQR) |
3.63(2.73) 2.87(2.76) |
| Intake adequacy (WHO/FAO RI) (n.%) Adequate (≥5µg/day) Low (<5µg/day) |
70 (19.72) 285 (88.28) |
| BMI (Kg/m2) Normal weight Underweight Overweight Obese |
25.7(6.2) 145 (40.8) 5(1.4) 133(37.5) 72(20.3) |
| 25(OH)D (ng/ml) Mean (SD) Median (IQR) |
18.2(9.4) 15.7(12.4) |
| VD deficiency (25(OH)D<20ng.ml) VD Insufficiency (20≤25(OH)D<30ng/ml) VD Sufficiency (25(OH)D≥30ng/ml) |
231(65.1) 82(23.1) 42(11.8) |
| Sun exposure score Median (IQR) | 15.9(10.5) |
| Sun exposure categories (n.%) Insufficient-moderate Sufficient-high |
156 (43.9) 199(56.1) |
| Physical activity MET min/week, Median (IQR) Physical activity level categories (n.%) Moderate-low High |
1778.2(1765.0) 330(93.2) 24(6.8) |
| Season (n.%) Summer Autumn Winter Spring |
143(40.9) 86(24.2) 60(16.9) 66(18.6) |
Abbreviations; IQR: interquartile range, MET: Metabolic Equivalent of Task.
Table 2.
Percent frequency of consuming vitamin D in foods sources (n = 355).
| Food sources | Items | Never or less than once per month | 1-3 times per month | 1time per Week | 2-4 days per week | 5-6 days per week | Every day |
|---|---|---|---|---|---|---|---|
| Fish and sea products | Fatty fish fresh and frozen (Sardin) | 18.76 | 54.2 | 27.04 | 0 | 0 | 0 |
| Fatty fish fresh and frozen (Mackerel) | 87.32 | 8.16 | 4.52 | 0 | 0 | 0 | |
| White fish fresh and frozen (sole, whiting, sea bream…) | 85.35 | 0 | 12.39 | 2.26 | 0 | 0 | |
| Sardine, canned in tomato sauce | 42.83 | 50.98 | 6.19 | 0 | 0 | 0 | |
| Tuna and mackerel, canned in vegetable oil | 87.32 | 12.68 | 0 | 0 | 0 | 0 | |
| Shellfish (calmer, scampi. Shrimps, mussels) | 91.54 | 8.46 | 0 | 0 | 0 | 0 | |
| Meat products | Red meat (Beef, veal. sheep...,), eaten with or without fat | 43.66 | 20.56 | 14.36 | 16.61 | 4.81 | 0 |
| Organ meats (kidney) | 93.53 | 4.22 | 2.25 | 0 | 0 | 0 | |
| Organ meats (liver) | 81.14 | 16.61 | 2.25 | 0 | 0 | 0 | |
| Poultry (chicken and turkey) | 14.36 | 6.19 | 45.53 | 22.53 | 12.38 | 0 | |
| Smoked meats or charcuterie (chorizo, salami, Ham, casheer, mortadella. etc.) | 84.79 | 8.45 | 3.50 | 3.26 | 0 | 0 | |
| Entire eggs | Eggs (Pan-fried, crambled and boiled) | 38.6 | 18.6 | 28.16 | 4.22 | 10.42 | 0 |
| Dairy Products and beverages | Cow milk vitamin D fortified. farm-fresh cow’s milk | 12.4 | 0 | 2.25 | 24.5 | 20.85 | 40 |
| Milk drink. or drinking yogurt. flavored or with fruit. sweetened | 52.11 | 25.07 | 18.58 | 1.97 | 2.27 | 0 | |
| Yogurt flavored or with fruit. sweetened. non-reduced fat | 25.07 | 22.25 | 27.04 | 18.6 | 7.04 | 0 | |
| Semi-hard cheese (Gouda. Edam. Munster) | 81.12 | 8.16 | 8.16 | 2.56 | 0 | 0 | |
| Fresh cheese (ricotta. Mozarelle.) | 95.8 | 4.2 | 0 | 0 | 0 | 0 | |
| Soft cheese (Camembert. Brie) | 87.6 | 4.22 | 6.47 | 1.71 | 0 | 0 | |
| Melted cheese in portions or spreadable cubes | 0 | 22.81 | 25.07 | 4.22 | 29.28 | 18.62 | |
| Cottage cheese natural or aromatic | 93.8 | 2.25 | 2.25 | 0 | 1.7 | 0 | |
| Fat Products | Vegetable oil vitamin D fortified | 22.82 | 0 | 0 | 0 | 0 | 77.18 |
| Margarine vitamin D fortified | 45.63 | 0 | 4.22 | 24.78 | 4.22 | 21.15 | |
| Butter | 42.81 | 4.22 | 2.25 | 22.81 | 4.22 | 23. 66 | |
| Breakfast cereals | Cereal vitamin D fortified | 87.32 | 6.19 | 6.49 | 0 | 0 | 0 |
| Chocolate | chocolate bars (with milk or dark 70% cocoa minimum or with dried fruits) | 66.47 | 14.64 | 10.42 | 4.22 | 4.25 | 0 |
| Cacao | Sweet cocoa or chocolate powder for drinks, enriched with vitamins and minerals | 87.32 | 0 | 8.16 | 4.52 | 0 | 0 |
| Backery and Moroccan biscuit | Ordinary homemade cake or prepackaged Madeleine. Viennoiserie (krachel. chocolate bread, raisin bread, croissant. brioche) Moroccan biscuits (thee dry biscuit, Fekkas, date biscuit) |
18.87 |
10.42 |
41.7 |
6.47 |
22.54 |
0 |
Table 3.
Socio-demographic determinant of vitamin D dietary intake in study participants (n=355).
| Characteristics | Dietary intake (µg/d) | ||||
|---|---|---|---|---|---|
| Mean (SD) | Median(IQR) | P value | Below RI (n, %) |
P Value d | |
| Age (years) | 0.004a | ||||
| Age classes (n. %) 18-25 26-36 37-49 |
3. 32(2.58) 3.58(2.73) 4.16(2.84) |
2.62(2.30) 2.79(2.68) 3.67(3.25) |
0.029b 0.027C |
67(23.50) 160(56.10) 58(20.40) |
0.146 |
| Education (%) Illiterate ≤10 years (Secondary -college) ≥11years (University or higher) |
3.70(3.39) 3.86(2.84) 3.28(2.11) |
2.79(2.92) 2.93(2.11) 2.87(2.64) |
0.351 | 53(18.60) 125(43.90) 103(37.50) |
0.219 |
| Marital status Married Unmarried |
3.73(2.85) 3.44(2.48) |
2.93(2.84) 2.63(2.73) |
0.471 | 177(62.1) 108(37.9) |
0.219 |
| Employment (%) Yes No |
3.57(2.57) 3.67(2.84) |
2.82(2.83) 2.93(2.75) |
0.982 | 122(42.80) 163(57.20) |
0.278 |
| Localization Rural Urban |
3.27(2.33) 4.25(3.22) |
2.73(2.46) 3.18(3.93) |
0.014 b | 193(67.70) 92(32.30) |
0.204 |
Abbreviations; IQR: interquartile range, RI: recommanded intake. a: Spearman correlation, b kruskul Wallis test; c: pairwaiz comparaison, p adjusted for Bonferroni correction for multiple test; d: Chi-squar test. Significance level: p < 0.05.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



