Submitted:
20 September 2024
Posted:
23 September 2024
You are already at the latest version
Abstract
Background/Objectives: Catastrophization and other comorbid psychological factors that increase awareness of pain are known to hinder chronic pain recovery. Five pilot studies, reported here, indicate that increased pain awareness from frequent pain assessment may impede chronic pain recovery through similar mechanisms. Methods: All study participants were asked to use a biofeedback device at least twice daily. Studies 1 and 2 required pain assessment before and after each biofeedback session, while Studies 3-5 did not. Pain levels were measured by the McGill Pain Inventory (McGill PI) at the start and end of each study. Results: Studies 3-5 replicated our prior work, demonstrating changes in pain, anxiety, and satisfaction and recovery following a home-use biofeedback program. Participants in the studies without frequent pain assessment experienced greater overall reductions in pain compared to participants in studies that did not require pain assessment. The results are, however, statistically inconclusive due to high variability, so further research is necessary. Conclusion: The results of our study suggest that frequent pain assessment may hinder pain reduction, likely by facilitating negative thought patterns and neural circuits involved in chronic pain. These findings can be applied to developing better research designs and more effective chronic pain recovery programs.
Keywords:
chronic pain
; neuroplastic pain
; sensitization
; catastrophization
; repetitive negative thinking
; pain assessment
; pain recovery
; thermal IR biofeedback
; home-use biofeedback
; calming sessions
1. Introduction
Chronic pain affects a significant proportion of the population worldwide and remains a leading issue in public health today. Typically defined as pain persisting for at least 3 months, chronic pain affects about 20.8% of adults in the U.S. and 35% to 51.3% of adults in the UK [1,2,3,4]. Along with musculoskeletal pain, common chronic pain conditions include fibromyalgia, rheumatoid arthritis, frequent headaches or migraines, and more [5]. The recovery process is often complicated by various comorbid psychological factors and disorders such as anxiety and catastrophization [6,7,8,9].
Chronic pain-related neuroplasticity is caused by central nervous system sensitization [10,11,12,13], driven by repetitive negative thought patterns and hypervigilance to pain [14,15]. Chronic pain researchers report compelling evidence of repetitive negative thinking (RNT) exacerbating pain intensity through increased catastrophization [16,17,18]. Given the evidence linking RNT to chronic pain [16,17,18], this study aims to investigate a potentially similar impact caused by frequent pain assessment. Such assessments may have an effect comparable to catastrophization by amplifying negative cognitive patterns that exacerbate pain. Along with increased pain intensity, catastrophization also diminishes the quality of life for chronic pain patients [17]. Understanding the effect of frequent pain self-assessment on negative thought patterns could allow for the development of more effective chronic pain recovery programs and improved research methodology.
In this report, we compare the results of five pilot studies involving participants with chronic pain who used a biofeedback device for recovery. Two studies include pain assessment four times daily [19], while the other three do not. We hypothesize that participants who do not frequently assess their pain will experience greater pain reduction than those who do.
2. Materials and Methods
Study 1
A group of six participants with lower back pain, pelvic pain, or fibromyalgia were recruited through referrals, posters, and emails. Inclusion criteria included a minimum age of eighteen, internet and app store access, and pain persisting for at least six months. Participants utilized a hand-held biofeedback device for ten minutes at least twice daily and reported their anxiety and pain levels in a mobile app before and after each use over the course of four weeks. Hand temperature data was also recorded. Along with the biofeedback device, participants attended a weekly educational Zoom meeting and were provided with the book “The Way Out” by Alan Gordon. Pain, anxiety, and satisfaction and recovery changes were measured at the end of the four weeks [19].
Study 2
A group of nine participants with chronic pain were recruited through referrals, posters, and emails. This study followed a similar protocol to Study 1, however, the inclusion criteria expanded to include all types of chronic pain.
An in-depth description of materials and methods for Studies 1 and 2 has been previously published [19].
Study 3
A group of six participants with chronic musculoskeletal pain lasting longer than 6 months was recruited through clinician referrals, email lists, and posters. Inclusion criteria included a minimum age of eighteen, musculoskeletal pain or fibromyalgia persisting longer than 6 months, and a minimum average pain level of 4 measured by the Visual Analogue Scale [20,21]. Participant demographics including age, sex, race, and pain history were collected (Table 1). Once participants consented to the study, they were assigned a weekly group meeting time.
The study lasted 5 weeks, beginning with an initial in-person interview followed by Zoom meetings once a week for the entire study duration. Each Zoom meeting consisted of educational PowerPoint presentations followed by group discussions on the presented content. Participants were also assigned educational videos and worksheets to complete before each weekly Zoom meeting to reinforce their understanding of the material. Participants were provided with a hand-temperature biofeedback device for use at least twice daily. The biofeedback device was used with the book “The Way Out” by Alan Gordon to learn concepts important to chronic pain recovery. Measurements of pain, anxiety, and satisfaction and recovery were reported in the initial applicant survey, at the start and end of the trial, and a 6-month follow-up. Pain levels were measured using the Short-Form McGill Pain Questionnaire (SF-MPQ) [22,23,24]. Anxiety was measured on the Short-Form State-Trait Anxiety Inventory (STAI) [25,26] and health-related satisfaction and recovery was evaluated on the Satisfaction and Recovery Index (SRI) [27,28,29].
The thermal biofeedback device used in this study monitored changes in hand temperature. The device was designed for portability and was small enough to fit in the user’s palm for use in any setting. Its display comprised six lights which collectively represented a range of temperatures. The lights changed color one by one in a clockwise direction as hand temperature increased, indicating greater blood flow as a result of vasodilation that occurs during relaxation. Participants used the device for at least two ten-minute sessions per day for 5 weeks.
Study 4
A group of four participants with chronic pain and headaches persisting longer than 6 months were recruited through clinician referrals, emails, and posters. Participants were included if they met the inclusion criteria for having pain lasting longer than 6 months, a minimum age of 18, and a minimum average pain of 4 measured on the VAS. Participant demographics including age, sex, race, and pain history were collected.
This 5-week-long study followed the same protocol as Study 3 and utilized the same biofeedback device. Pain, anxiety, and satisfaction and recovery measurements were collected before and after the trial, and 6 months later.
Figure 1.
Flow diagram of participant selection and study timeline for Studies 3-5 from initial screening to 6-month follow-up.
Figure 1.
Flow diagram of participant selection and study timeline for Studies 3-5 from initial screening to 6-month follow-up.
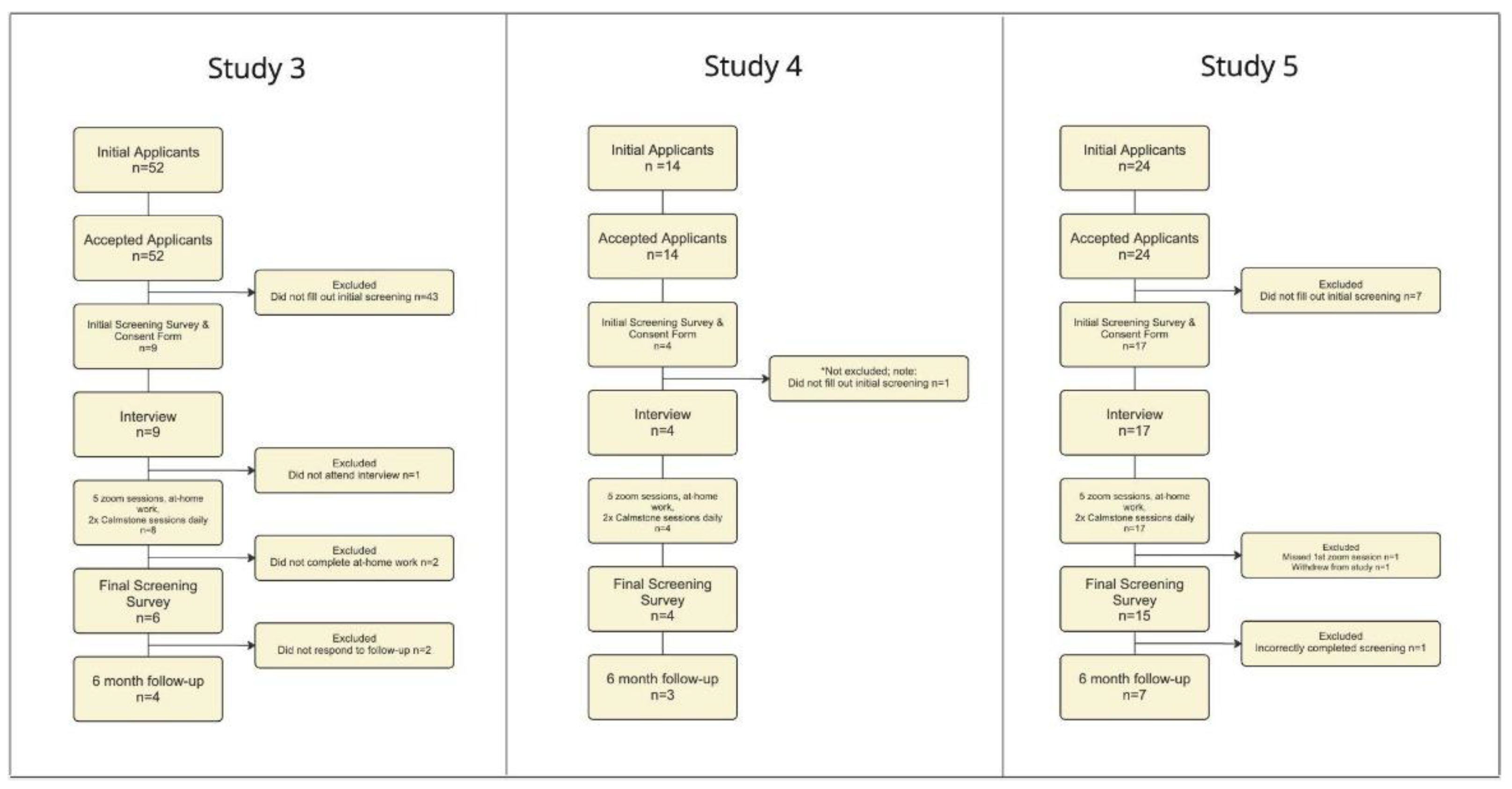

Table 1.
Demographics and pain history for participants across all five studies. The studies listed as “Study 1 and Study 2” in this paper were previously listed as “Study 2 and Study 3,” respectively, in the previously published paper. We have renumbered the studies because data from Study 1 was excluded from the research we have done in this paper.
Table 1.
Demographics and pain history for participants across all five studies. The studies listed as “Study 1 and Study 2” in this paper were previously listed as “Study 2 and Study 3,” respectively, in the previously published paper. We have renumbered the studies because data from Study 1 was excluded from the research we have done in this paper.
| Characteristic | Total (n=39) |
Study 1 (n-6) |
Study 2 (n=9) |
Study 3 (n=6) |
Study 4 (n=4) |
Study 5 (n=14) |
|---|---|---|---|---|---|---|
| Age, mean (SD) | 53.22 (16) | 38.7 (16.4) | 45.9 (13.2) | 63.3 (13.6) | 50.5 (4.8) | 49.9 (18.8) |
| Sex | ||||||
| Male | 13 | 4 | 1 | 2 | 1 | 5 |
| Female | 26 | 2 | 8 | 4 | 3 | 9 |
| Race | ||||||
| Caucasian | 33 | 5 | 7 | 6 | 4 | 11 |
| Asian/Pacific Islander | 3 | 1 | 1 | 0 | 0 | 1 |
| African American | 2 | 0 | 1 | 0 | 0 | 1 |
| American Indian/Alaska Native | 0 | 0 | 0 | 0 | 0 | 0 |
| Other | 1 | 0 | 0 | 0 | 0 | 1 |
| Number of Pain Conditions | ||||||
| 1 | 14 | 2 | 3 | 1 | 3 | 5 |
| 2 | 9 | 2 | 3 | 1 | 0 | 3 |
| 3+ | 16 | 2 | 3 | 4 | 1 | 6 |
| Duration of Pain | ||||||
| 6-12 months | 3 | 1 | 1 | 0 | 0 | 1 |
| 1-5 years | 15 | 2 | 4 | 1 | 2 | 6 |
| >5 years | 21 | 3 | 4 | 5 | 2 | 7 |
| Medications taken | ||||||
| Opioids | 3 | 0 | 0 | 2 | 0 | 1 |
| NSAID/Acetaminophen | 9 | 2 | 3 | 3 | 0 | 1 |
| Adjunctive Pain Medication | 3 | 1 | 0 | 0 | 0 | 2 |
| None/Did not specify | 24 | 1 | 5 | 0 | 2 | 6 |
Study 5
A group of 14 participants with chronic pain and headaches were recruited through clinician referrals, emails, and posters. Inclusion criteria included pain lasting longer than 6 months, a minimum age of eighteen, and a minimum average pain of 4 measured on the VAS. Participant demographics including age, sex, race, and pain history were collected.
This study followed the same protocol as the previous two studies but used the book “The Explain Pain Handbook: Protectometer” by Lorimer Mosely rather than “The Way Out” by Allen Gordon. Pain, anxiety, and satisfaction and recovery measurements were collected before and after the trial, and 6 months later.
Statistical Analysis
To assess differences in pain outcomes between studies which frequently assessed pain levels vs. those that did not, we fit hierarchical Bayesian models, allowing us to pool data across studies while accounting for intra-/inter-study variability in outcomes (cf. meta-analytic or meta-regressive modeling approaches). Models were specified and estimated using Stan (https://mc-stan.org/) and brms [30] in R. Each model followed the same generalized linear form, where differences in pain outcomes (Final - Baseline) were regressed against a categorical predictor indicating whether pain levels were frequently vs. infrequently assessed during the course of the biofeedback program (formally, coded using a sum-to-zero deviation contrast, capturing the mean difference in outcomes between study types). Baseline scores were also included as a covariate to control for the fact that the magnitude of the Final - Baseline difference is likely correlated with initial pain levels. Finally, we further included a random intercept term conditioned on study ID (broadly accounting for inter-study variability in outcomes).
We specified a series of weakly-informative priors over each parameter, robustly-defined in part by the median absolute deviation (MAD) of each outcome measure. For example, the prior densities over the slope parameters were defined by a normal (Gaussian) distribution with mean = 0 and standard deviation = 2.5 x MAD(dy), where dy gives the vector of Final - Baseline difference scores. The model intercept was defined using a Student t-distribution with 3 degrees of freedom and location/scale parameters given by median(dy) and MAD(dy), respectively. Residual variances and random effects variances were similarly defined using a half-Student t-distribution, with 3 degrees of freedom and location/scale parameters given by 0 and MAD(dy), respectively (i.e., constraining the variances to be positive).
Robust exploration of the posterior parameter space for all models was achieved using Hamiltonian Monte Carlo (HMC), with four independent chains comprised of 15000 sampling iterations each (5000 of which were used as warm-up samples). We ensured that all chains properly converged to equilibrium for all parameters using classical benchmarks, including: the effective sample size (considering the autocorrelation between successive HMC transitions); the Monte Carlo standard error (relative to the posterior SD); R-hat (the variance ratio between each chain relative to all chains); and no divergent HMC transitions after warm-up.
For statistical inference, we consider 95% credibility intervals around the posterior mean parameter estimates (using the highest posterior density interval, HDI) along with the ‘probability of direction’ (pd), capturing the proportion of the posterior density above or below zero. Here, pd can range from 0.50 (indicating that the posterior density is perfectly-centered at zero) to 1 (in the most extreme case, that no proportion of the posterior density intersects zero)—thus, pd values closer to 1 indicate more posterior evidence for the presence of a nonzero effect. We also provide a fully-probabilistic Bayesian analogue of Cohen’s d to further quantify standardized mean differences (i.e., effect sizes): following conventions for hierarchical linear models [31], here we took the posterior draws corresponding to the mean difference between study types, or measurement occasions, and divided them by the square root of the summed residual variances and random effects variances.
3. Results
Biofeedback-related changes in self-reported pain have previously been detailed for Studies 1 and 2 [19]. In brief, we found that hand temperature biofeedback programs were associated with reduced pain and anxiety on average (comparing reported pain and anxiety levels before and after each biofeedback session)—and in some individuals, the magnitude of the change in anxiety predicted the magnitude of the change in pain, such that greater reductions in anxiety after each session were associated with greater reductions in pain. We also showed modest, overall reductions in pain and anxiety metrics when comparing ratings given at baseline (prior to beginning the biofeedback program) to those provided after finishing the program.
Our first goal was, therefore, to determine whether we could replicate our prior results [19] now in Studies 3-5, comparing Final vs. Baseline scores on a number of self-assessed metrics, including: average, minimum, and maximum pain levels (rated on a 0-10 VAS); the McGill Pain Inventory; the Satisfaction and Recovery Index; and the State-Trait Anxiety Inventory. A full set of descriptive statistics for each of these scales is shown in Table 2. With respect to VAS ratings (Figure 2A), we observed the largest reductions in self-assessed average pain levels (d = -0.92, 95CI = [-1.47, -0.34]; b = -1.77, SD = 0.48, 95CI = [-2.72, -0.85], pd = 1), followed by maximum pain (d = -0.70, 95CI = [-1.18, -0.22]; b = -1.73, SD = 0.52, 95CI = [-2.77, -0.69], pd = 0.999) and minimum pain levels (d = -0.65, 95CI = [-1.05, -0.22]; b = -1.65, SD = 0.44, 95CI = [-2.52, -0.78], pd = 1). These findings align with our prior work showing consistent reductions in self-assessed pain at multiple levels.
With respect to our additional survey measures (Figure 2B), we both replicated and exceeded the effects previously reported in Studies 1-2. Where we initially observed a small-to-moderate reduction in anxiety (d = -0.39), we now see evidence for a much larger effect (d = -1.00, 95CI = [-1.50, -0.51]; b = -6.46, SD = 1.23, 95CI = [-8.90, -4.02], pd = 1). Using the Satisfaction and Recovery Index, our last pair of studies failed to identify any evidence for a positive effect (d = 0.04); however, in the current group of studies, we observed moderate increases in participants’ health-related satisfaction (d = -0.46, 95CI = [0.02, 0.93]; b = 9.27, SD = 4.23, 95CI = [0.90, 17.64], pd = 0.984)—although we note the posterior variance is quite large here, indicating greater uncertainty. Finally, the reduction in pain assessed by the McGill Pain Inventory exceeded Studies 1-2 (d = 0.30) nearly fourfold (d = -1.15, 95CI = [-1.78, -0.55]; b = -8.74, SD = 1.70, 95CI = [-12.14, -5.35], pd = 1).
Taken together, these results anecdotally suggest that frequent pain assessments (i.e., before and after each biofeedback session, as in Studies 1-2) may partially hinder recovery, producing weaker effects than those observed when participants are not regularly asked to assess their pain (as in Studies 3-5). We therefore sought to explicitly test this hypothesis by contrasting average reductions in pain between studies using different types of experimental designs. Here we focus primarily on pain assessments derived via the McGill Pain Inventory, which showed the largest effect in Studies 3-5 and appeared to drastically outperform what we previously observed in Studies 1-2 [19].
When considering the variability both within and between study groups, we were unable to identify a reliable difference between these two design approaches. While biofeedback studies that eschewed frequent pain assessment generally showed stronger reductions in pain, there was nevertheless considerable overlap with studies that did frequently assess pain (Figure 3A). Consistent with this, under the model, we observed a moderately large difference between studies, such that infrequent pain assessment was associated with greater changes from Baseline to Final ratings (d = 0.71, 95CI = [-0.27, 1.74]; b = 4.73, SD = 3.64, 95CI = [-2.73, 11.97], pd = 0.921)—while this trend is indeed in the direction we anticipated, the 95% credibility interval around the effect intersects zero, so we cannot conclude that the difference in pain reduction between studies is statistically meaningful (Figure 3B).
Notably, the trend described above was specific to pain-related outcomes. When assessing changes in trait anxiety levels before and after the biofeedback program (Figure 4A), we saw no difference between study types—both groups demonstrated similar degrees of anxiety reduction, despite the fact that Studies 1-2 also asked participants to assess their anxiety levels before and after each biofeedback session (d = 0.04, 95CI = [-1.05, 1.07]; b = 0.16, SD = 3.38, 95CI = [-7.11, 6,70], pd = 0.543; Figure 4B).
While we are ultimately unable to precisely determine the extent to which frequent vs. infrequent pain assessments affect pain outcomes, it is worth noting that the magnitude of the difference is still quite large (Figure 5). These initial results appear promising despite being a purely retrospective analysis across a number of smaller pilot studies with varying degrees of heterogeneity. It will be essential for future studies to more systematically test these differences in a more controlled fashion.
4. Discussion
This study investigated the impact of frequent pain assessment on chronic pain recovery across five pilot studies. In the studies without frequent pain assessment, we found the reduction in pain measured on the SF-MPI to be almost twice as great compared to those with frequent pain assessment. While this trend was not statistically significant due to large error variance and small sample size, the substantial difference in pain decrease between the two groups strongly suggests that frequent pain assessment may hinder pain reduction.
In the studies without frequent pain assessment, participants were also instructed to avoid discussing their pain with others to further minimize pain attentiveness. We believe this allowed for more effective pain reduction by preventing additional reinforcement of negative thought patterns involved in chronic pain. Frequent pain assessment may catalyze RNT and thus catastrophization, which delays pain recovery by maintaining chronic pain-causing networks in the brain [32,33]. Our results are consistent with prior studies that have demonstrated the role of maladaptive thought patterns in the persistence and exacerbation of chronic pain [34,35,36]. Each time participants reassess their pain and are reminded of it, sensitization of neural patterns that create the experience of pain is reinforced [10,11,12,13].
Additionally, much research has demonstrated the role of operant conditioning in maintaining behaviors and neural patterns involved in chronic pain [37,38,39]. While further research is necessary to determine statistical significance, our results supplement the findings in these studies [37,38,39] as it’s likely that consistent pain assessment, four times daily, over multiple weeks can become a source of negative reinforcement.
There are several limitations to this study. The small sample size and the need for a control group across all five pilot studies limits the generalizability of our findings. These studies also do not address the implications of additional comorbidities that may affect chronic pain recovery. Furthermore, the inclusion criteria in Studies 3-5 was expanded to accept participants with additional types of chronic pain, whereas Studies 1 and 2 accepted exclusively musculoskeletal pain and fibromyalgia participants. The variance in pain inclusion criteria likely caused the high standard deviation in our data and decreased the effect size. While our findings suggest a considerably greater pain reduction in studies without frequent pain assessment, further research with a larger sample population and consistent inclusion criteria is required to establish statistical significance.
The trend we have observed in this research, though not statistically significant, suggests that eliminating frequent pain assessments will improve the efficacy of chronic pain recovery programs.
Author Contributions
Formal analysis, writing–original draft preparation, and visualization, K.H.; data curation and formal analysis, D.A.; investigation and project administration, J.R.; formal analysis, writing–review and editing, T.S.; software, Z.Z., S.S.; writing–review and editing, K.I.; methodology, project administration, and investigation, P.H.
Funding
This research was supported by grant W911NF-19-0026 from the US Army Research Office and Institute for Collaborative Biotechnologies (T.S.). John and Kathy Kirtley and Atiye Bayman provided additional private funding.
Institutional Review Board Statement
All studies were conducted in accordance with the UCSB Office of Research, and approved by the UCSB Human Subjects Committee: Study 3: Protocol No. 3-22-0768 (05/30/2023) Study 4: Protocol No. 3-22-0768 with Modification (05/30/2023) Study 5: Protocol No. 10-23-0730 (02/13/2024)
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors upon request.
Acknowledgements
We thank John and Kathy Kirtley, Atiye Bayman, Maury Hayashida for their helpful insights. We thank Dr. Michael Bordofsky and Dr. Ericka Dixon for referring participants and helpful insights.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Yong, R.J.; Mullins, P.M.; Bhattacharyya, N. Prevalence of chronic pain among adults in the United States. Pain 2022, 163, e328–e332. [Google Scholar] [CrossRef]
- Nahin, R.L.; Feinberg, T.; Kapos, F.P.; Terman, G.W. Estimated Rates of Incident and Persistent Chronic Pain Among US Adults, 2019-2020. JAMA Netw. Open 2023, 6, e2313563. [Google Scholar] [CrossRef]
- Treede, R.-D.; Rief, W.; Barke, A.; Aziz, Q.; Bennett, M.I.; Benoliel, R.; Cohen, M.; Evers, S.; Finnerup, N.B.; First, M.B.; et al. Chronic pain as a symptom or a disease: The IASP Classification of Chronic Pain for the International Classification of Diseases (ICD-11). Pain 2019, 160, 19–27. [Google Scholar] [CrossRef]
- Fayaz, A.; Croft, P.; Langford, R.M.; Donaldson, L.J.; Jones, G.T. Prevalence of chronic pain in the UK: a systematic review and meta-analysis of population studies. BMJ Open 2016, 6, e010364. [Google Scholar] [CrossRef]
- Crofford, L.J. Chronic Pain: Where the Body Meets the Brain. Trans. Am. Clin. Climatol. Assoc. 2015, 126, 167–183. [Google Scholar]
- Martinez-Calderon, J.; Jensen, M.P.; Morales-Asencio, J.M.; Luque-Suarez, A. Pain Catastrophizing and Function In Individuals With Chronic Musculoskeletal Pain. Clin. J. Pain 2019, 35, 279–293. [Google Scholar] [CrossRef]
- Wertli, M.M.; Eugster, R.; Held, U.; Steurer, J.; Kofmehl, R.; Weiser, S. Catastrophizing—a prognostic factor for outcome in patients with low back pain: a systematic review. Spine J. 2014, 14, 2639–2657. [Google Scholar] [CrossRef]
- Tegethoff, M.; Belardi, A.; Stalujanis, E.; Meinlschmidt, G. Comorbidity of Mental Disorders and Chronic Pain: Chronology of Onset in Adolescents of a National Representative Cohort. J. Pain 2015, 16, 1054–1064. [Google Scholar] [CrossRef]
- Kuch, K. Psychological Factors and the Development of Chronic Pain. Clin. J. Pain 2001, 17, S33–S38. [Google Scholar] [CrossRef]
- Sator-Katzenschlager, S. Pain and neuroplasticity. Rev. Medica Clin. Las Condes 2014, 25, 699–706. [Google Scholar] [CrossRef]
- Melzack, R.; Coderre, T.J.; Katz, J.; Vaccarino, A.L. Central Neuroplasticity and Pathological Pain. Ann. New York Acad. Sci. 2001, 933, 157–174. [Google Scholar] [CrossRef] [PubMed]
- Deitos, A.M.; Dussán-Sarria, J.A.; de Souza, A.M.; Medeiros, L.M.; Tarragô, M.d.G.; Sehn, F.M.; Chassot, M.M.; Zanette, S.; Schwertner, A.; Fregni, F.; et al. Clinical Value of Serum Neuroplasticity Mediators in Identifying the Central Sensitivity Syndrome in Patients With Chronic Pain With and Without Structural Pathology. Clin. J. Pain 2015, 31, 959–967. [Google Scholar] [CrossRef]
- Hiraga, S.-I.; Itokazu, T.; Nishibe, M.; Yamashita, T. Neuroplasticity related to chronic pain and its modulation by microglia. Inflamm. Regen. 2022, 42, 15. [Google Scholar] [CrossRef] [PubMed]
- McCracken, L.M. “Attention” to pain in persons with chronic pain: A behavioral approach. Behav. Ther. 1997, 28, 271–284. [Google Scholar] [CrossRef]
- Garland, E.L.; Howard, M.O. Mindfulness-Oriented Recovery Enhancement Reduces Pain Attentional Bias in Chronic Pain Patients. Psychother. Psychosom. 2013, 82, 311–318. [Google Scholar] [CrossRef]
- Schütze, R.; Rees, C.; Smith, A.; Slater, H.; O’sullivan, P. Metacognition, perseverative thinking, and pain catastrophizing: A moderated-mediation analysis. Eur. J. Pain 2020, 24, 223–233. [Google Scholar] [CrossRef]
- Semeru, G.M.; Halim, M.S. Acceptance versus catastrophizing in predicting quality of life in patients with chronic low back pain. Korean J. Pain 2019, 32, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Darnall, B.; Sturgeon, J.; Kao, M.-C.; Hah, J.; Mackey, S. From Catastrophizing to Recovery: a pilot study of a single-session treatment for pain catastrophizing. J. Pain Res. 2014, 7, 219–226. [Google Scholar] [CrossRef]
- Ly, F.S.; Santander, T.; Pavlov, S.; Zhao, J.; Zhang, M.; Arroyo, D.; Sokolovskiy, S.; Iyer, A.; Yankauskas, Y.; Chen, J.; et al. Home-Use and Portable Biofeedback Lowers Anxiety and Pain in Chronic Pain Subjects. Am. J. Lifestyle Med. 2023, 15598276231221112. [Google Scholar] [CrossRef]
- Thong, I.S.K.; Jensen, M.P.; Miró, J.; Tan, G. The validity of pain intensity measures: what do the NRS, VAS, VRS, and FPS-R measure? Scand. J. Pain 2018, 18, 99–107. [Google Scholar] [CrossRef]
- Price, D.D.; McGrath, P.A.; Rafii, A.; Buckingham, B. The validation of visual analogue scales as ratio scale measures for chronic and experimental pain. Pain 1983, 17, 45–56. [Google Scholar] [CrossRef]
- Lovejoy, T.I.; Turk, D.C.; Morasco, B.J. Evaluation of the Psychometric Properties of the Revised Short-Form McGill Pain Questionnaire. J. Pain 2012, 13, 1250–1257. [Google Scholar] [CrossRef]
- Dworkin, R.H.; Turk, D.C.; Trudeau, J.J.; Benson, C.; Biondi, D.M.; Katz, N.P.; Kim, M. Validation of the Short-Form McGill Pain Questionnaire-2 (SF-MPQ-2) in Acute Low Back Pain. J. Pain 2015, 16, 357–366. [Google Scholar] [CrossRef]
- Jumbo, S.U.M.; MacDermid, J.C.; Kalu, M.E.M.; Packham, T.L.; Athwal, G.S.; Faber, K.J. Measurement Properties of the Brief Pain Inventory-Short Form (BPI-SF) and Revised Short McGill Pain Questionnaire Version-2 (SF-MPQ-2) in Pain-related Musculoskeletal Conditions: A Systematic Review. Clin. J. Pain 2021, 37, 454–474. [Google Scholar] [CrossRef]
- Marteau, T.M.; Bekker, H. The development of a six-item short-form of the state scale of the Spielberger State—Trait Anxiety Inventory (STAI). Br. J. Clin. Psychol. 1992, 31, 301–306. [Google Scholar] [CrossRef]
- Zsido, A.N.; Teleki, S.A.; Csokasi, K.; Rozsa, S.; Bandi, S.A. Development of the short version of the spielberger state—trait anxiety inventory. Psychiatry Res. 2020, 291, 113223. [Google Scholar] [CrossRef]
- Modarresi, S.; Walton, D.M. Reliability, discriminative accuracy, and an exploration of response shift as measured using the satisfaction and Recovery Index over 12 months from musculoskeletal trauma. Musculoskelet. Sci. Pr. 2020, 51, 102300. [Google Scholar] [CrossRef]
- Walton, D.M.; MacDermid, J.C.; Pulickal, M.; Rollack, A.; Veitch, J. Development and Initial Validation of the Satisfaction and Recovery Index (SRI) for Measurement of Recovery from Musculoskeletal Trauma. Open Orthop. J. 2014, 8, 316–325. [Google Scholar] [CrossRef]
- Modarresi, S.; Farzad, M.; Shafiee, E.; Modarresi, G.; Maleki, M.; Bakhshi, E.; Hosseini, S.A.; Walton, D.M. Cross-cultural Adaptation and Psychometric Evaluation of the Persian Version of the Satisfaction and Recovery Index (SRI): Structural Validity, Construct Validity, Internal Consistency, and Test-retest Reliability. Arch. Bone Jt. Surg. 2023, 11, 53–63. [Google Scholar] [CrossRef]
- Bürkner, P.-C. brms: An R Package for Bayesian Multilevel Models Using Stan. J. Stat. Softw. 2017, 80, 1–28. [Google Scholar] [CrossRef]
- Westfall, J.; Kenny, D.A.; Judd, C.M. Statistical power and optimal design in experiments in which samples of participants respond to samples of stimuli. J. Exp. Psychol. Gen. 2014, 143, 2020–2045. [Google Scholar] [CrossRef]
- Delgado-Gallén, S.; Soler, M.D.; Cabello-Toscano, M.; Abellaneda-Pérez, K.; Solana-Sánchez, J.; España-Irla, G.; Roca-Ventura, A.; Bartrés-Faz, D.; Tormos, J.M.; Pascual-Leone, A.; et al. Brain system segregation and pain catastrophizing in chronic pain progression. Front. Neurosci. 2023, 17, 1148176. [Google Scholar] [CrossRef] [PubMed]
- Gracely, R.H.; Geisser, M.E.; Giesecke, T.; Grant, M.A.B.; Petzke, F.; Williams, D.A.; Clauw, D.J. Pain catastrophizing and neural responses to pain among persons with fibromyalgia. Brain 2004, 127, 835–843. [Google Scholar] [CrossRef] [PubMed]
- Linton, S.J.; Flink, I.K.; Vlaeyen, J.W.S. Understanding the Etiology of Chronic Pain From a Psychological Perspective. Phys. Ther. 2018, 98, 315–324. [Google Scholar] [CrossRef]
- Linton, S.J.; Shaw, W.S. Impact of Psychological Factors in the Experience of Pain. Phys. Ther. 2011, 91, 700–711. [Google Scholar] [CrossRef]
- Edwards, R.R.; Dworkin, R.H.; Sullivan, M.D.; Turk, D.C.; Wasan, A.D. The Role of Psychosocial Processes in the Development and Maintenance of Chronic Pain. J. Pain 2016, 17, T70–T92. [Google Scholar] [CrossRef] [PubMed]
- Nees, F.; Becker, S. Psychological Processes in Chronic Pain: Influences of Reward and Fear Learning as Key Mechanisms - Behavioral Evidence, Neural Circuits, and Maladaptive Changes. Neuroscience 2018, 387, 72–84. [Google Scholar] [CrossRef]
- Hölzl, R.; Kleinböhl, D.; Huse, E. Implicit operant learning of pain sensitization. Pain 2005, 115, 12–20. [Google Scholar] [CrossRef]
- van Wilgen, C.P.; Keizer, D. The Sensitization Model to Explain How Chronic Pain Exists Without Tissue Damage. Pain Manag. Nurs. 2012, 13, 60–65. [Google Scholar] [CrossRef]
Figure 2.
Changes in pain, anxiety, and health-related satisfaction in Studies 3-5. All differences were estimated as a contrast between Final - Baseline measurements. (A) Mean reductions in self-assessed pain (given with respect to minimum, average, and maximum pain levels on a 0-10 visual analogue scale). (B) Mean reductions in anxiety (assessed by the State-Trait Anxiety Inventory) and pain (assessed by the McGill Pain Inventory), along with a mean increase in health-related satisfaction. In both (A) and (B), we provide 90-95% highest-density intervals around the posterior mean differences, shown as point intervals. No effects intersect zero at these intervals, suggesting robust evidence for nonzero effects.
Figure 2.
Changes in pain, anxiety, and health-related satisfaction in Studies 3-5. All differences were estimated as a contrast between Final - Baseline measurements. (A) Mean reductions in self-assessed pain (given with respect to minimum, average, and maximum pain levels on a 0-10 visual analogue scale). (B) Mean reductions in anxiety (assessed by the State-Trait Anxiety Inventory) and pain (assessed by the McGill Pain Inventory), along with a mean increase in health-related satisfaction. In both (A) and (B), we provide 90-95% highest-density intervals around the posterior mean differences, shown as point intervals. No effects intersect zero at these intervals, suggesting robust evidence for nonzero effects.
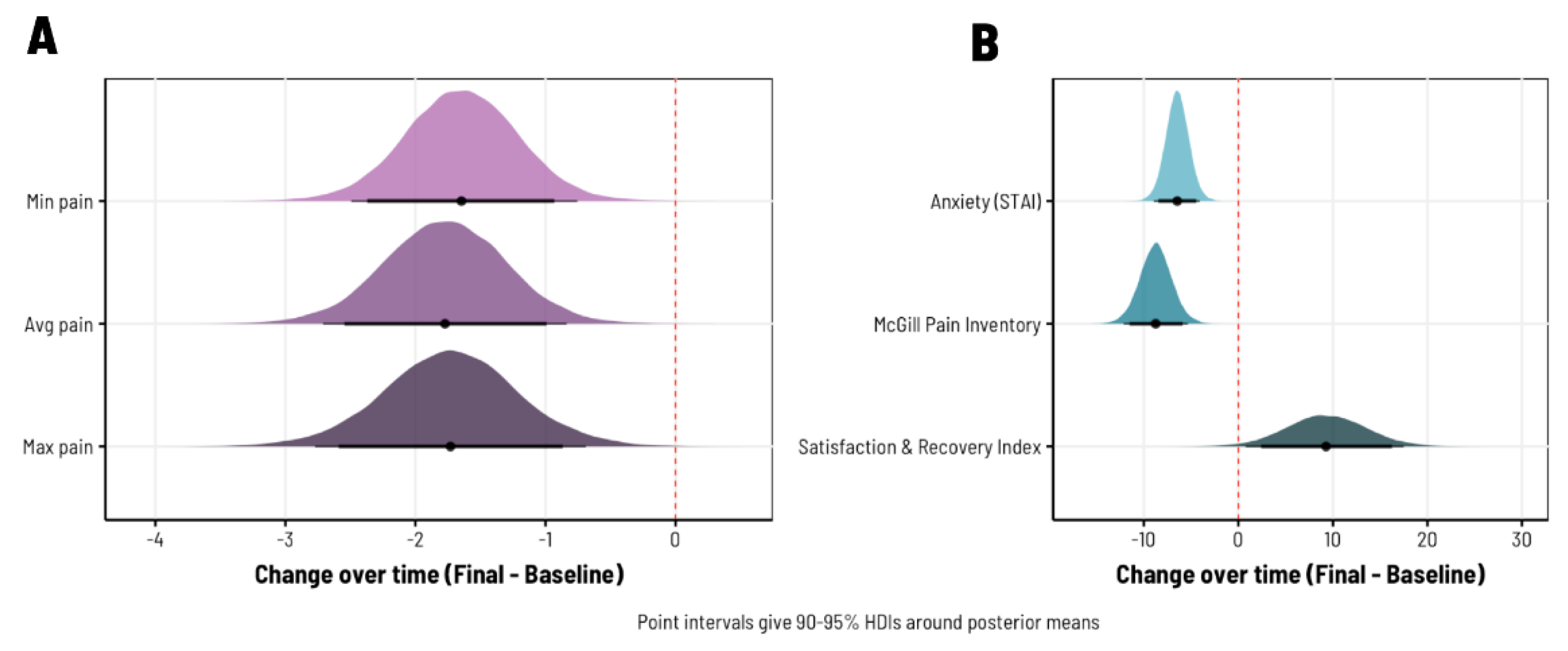
Figure 3.
Differences in pain-related outcomes between studies that infrequently vs. frequently ask participants to assess their pain. (A) Raw changes in pain self-assessed using the McGill Pain Inventory. Each point represents an individual participant under each group of studies; the ‘With frequent pain assessment’ group is comprised of Studies 1-2 [19], while ‘Without frequent pain assessment’ covers Studies 3-5. Boxplots are overlaid to further visualize the distribution of datapoints in each group. (B) The standardized mean difference in pain reduction between study types. As reflected in (A), studies without frequent pain assessment generally show a greater change from Baseline to Final measurement occasions; however, given the amount of overlapping variance, we lack sufficient posterior evidence for a nonzero effect (note that the 90-95% highest density interval around the standardized mean difference includes zero).
Figure 3.
Differences in pain-related outcomes between studies that infrequently vs. frequently ask participants to assess their pain. (A) Raw changes in pain self-assessed using the McGill Pain Inventory. Each point represents an individual participant under each group of studies; the ‘With frequent pain assessment’ group is comprised of Studies 1-2 [19], while ‘Without frequent pain assessment’ covers Studies 3-5. Boxplots are overlaid to further visualize the distribution of datapoints in each group. (B) The standardized mean difference in pain reduction between study types. As reflected in (A), studies without frequent pain assessment generally show a greater change from Baseline to Final measurement occasions; however, given the amount of overlapping variance, we lack sufficient posterior evidence for a nonzero effect (note that the 90-95% highest density interval around the standardized mean difference includes zero).
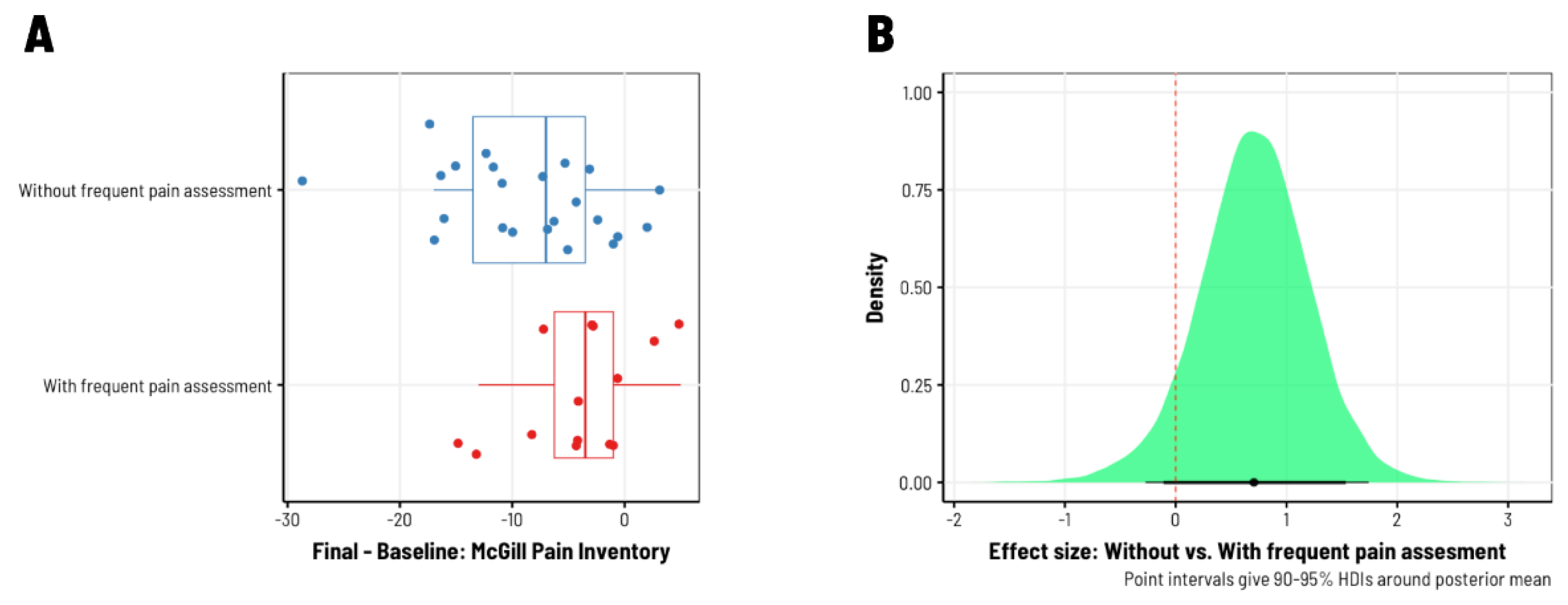
Figure 4.
Differences in anxiety reduction between studies that infrequently vs. frequently ask participants to assess their pain. (A) Raw changes in trait anxiety self-assessed using the State-Trait Anxiety Inventory (STAI). Each point represents an individual participant under each group of studies; the ‘With frequent pain assessment’ group is comprised of Studies 1-2 [19], while ‘Without frequent pain assessment’ covers Studies 3-5. Boxplots are overlaid to further visualize the distribution of datapoints in each group. (B) The standardized mean difference in anxiety reduction between study types. As reflected in (A), there were no differences in the extent to which anxiety was reduced from Baseline to Final measurement occasions (note that the 90-95% highest density interval around the standardized mean difference is nearly centered at zero).
Figure 4.
Differences in anxiety reduction between studies that infrequently vs. frequently ask participants to assess their pain. (A) Raw changes in trait anxiety self-assessed using the State-Trait Anxiety Inventory (STAI). Each point represents an individual participant under each group of studies; the ‘With frequent pain assessment’ group is comprised of Studies 1-2 [19], while ‘Without frequent pain assessment’ covers Studies 3-5. Boxplots are overlaid to further visualize the distribution of datapoints in each group. (B) The standardized mean difference in anxiety reduction between study types. As reflected in (A), there were no differences in the extent to which anxiety was reduced from Baseline to Final measurement occasions (note that the 90-95% highest density interval around the standardized mean difference is nearly centered at zero).
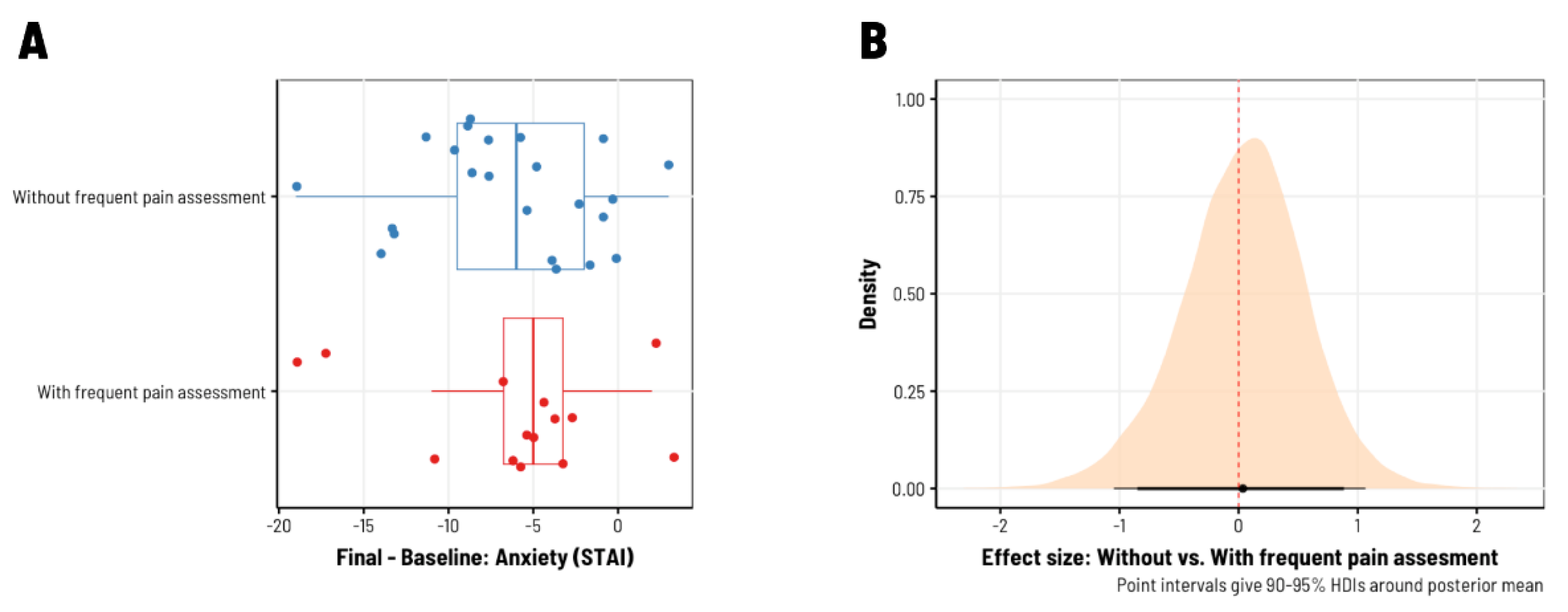
Figure 5.
Pain, as assessed by the Short-Form McGill Pain Inventory (SF-MPI), decreased more in studies that did not include pain assessment four times daily (i.e., before and after each biofeedback session, completed twice per day).
Figure 5.
Pain, as assessed by the Short-Form McGill Pain Inventory (SF-MPI), decreased more in studies that did not include pain assessment four times daily (i.e., before and after each biofeedback session, completed twice per day).
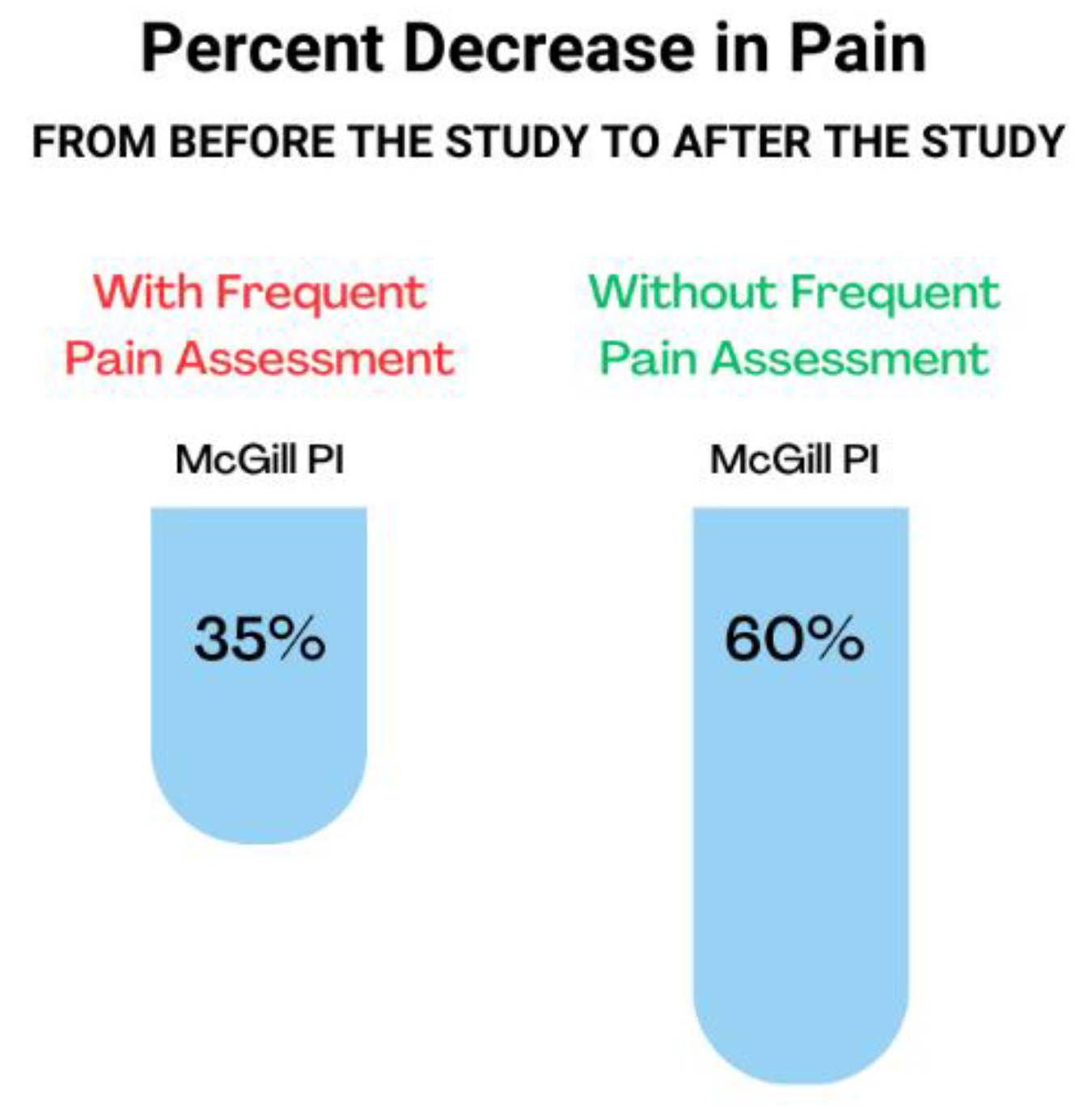
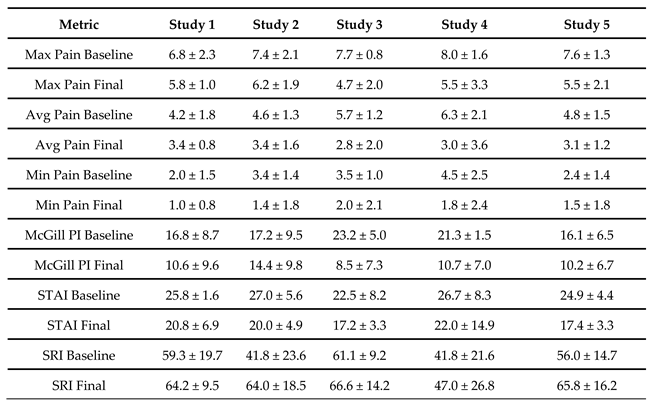
Table 2.
Results of baseline to final metrics for all studies. Metrics used include minimum, average, and maximum pain (VAS), quality and intensity of pain (SF-MPI), anxiety (SF-STAI), and health-related satisfaction and recovery (SRI).
Table 2.
Results of baseline to final metrics for all studies. Metrics used include minimum, average, and maximum pain (VAS), quality and intensity of pain (SF-MPI), anxiety (SF-STAI), and health-related satisfaction and recovery (SRI).
 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



