
Submitted:
19 September 2024
Posted:
23 September 2024
You are already at the latest version
Abstract
The increasing diffusion of antimicrobial resistance represents one of the major public health problems worldwide. In the last years, novel antimicrobial molecules have been developed to contrast the emergence of antimicrobial resistance and to provide a valuable therapeutic options against multi drug-resistant (MDR) GNB microorganisms. A new siderophore cephalosporin, Cefiderocol, represents a novel valuable antimicrobial drug for the treatment of infections caused by MDR-GNB. The mechanism of cefiderocol to penetrate trough the outer membrane of bacterial cell with a particular mechanism defined at “Trojan horse” render this molecule unique and immune against the different strategies adopted by GNB to counteract the activity of antimicrobial molecules. The broad spectrum of activity against different GNB species, the potent antibacterial activity, the pharmacokinetics properties, safety, and tolerability render cefiderocol a fundamental drug for the treatment of infections due MDR strains. Although this novel antimicrobial molecule has revolutionized the therapeutic antimicrobial armamentarium against MDR-GNB, the recent emergence of cefiderocol resistant strains have redefined its role in clinical practice and requested novel strategies to preserve its antibacterial activity. In this review, we discuss the mechanism of action of Cefiderocol, emerging resistance mechanisms, pharmacokinetic/pharmacodynamic (PK/PD) properties, efficacy data against the main Gram-negative bacteria, and future prospectives.
Keywords:
Antimicrobials
; MultiDrug Resistance
; Cephalosporins
; PK/PD
; Emerging Resistance
1. Introduction
Multi-drug resistant Gram-negative bacterial infections are among the most significant threats to human health, especially for critically ill and hospitalized patients [1]. In recent years, several therapeutic agents have been developed to enhance the anti-infective arsenal against difficult-to-treat Gram-negative bacteria [2,3]. However, effective therapies for metallo-β-lactamase (MBL)-producing Enterobacterales and glucose-nonfermenting Gram-negative organisms, such as Pseudomonas aeruginosa, Acinetobacter baumannii complex, and Stenotrophomonas maltophilia, remain scarce [4,5].
Cefiderocol was approved in the USA in 2019 and in Europe in 2020 for the treatment of infections caused by Gram-negative microorganisms in adult patients. The indication for cefiderocol is specifically limited to patients who have limited or no alternative treatment options, such as those with infections caused by carbapenem-resistant Enterobacterales, P. aeruginosa, A. baumannii, and other difficult-to-treat pathogens. As a result, cefiderocol has become a key agent in the armamentarium against carbapenem-resistant Gram-negative infections [6]. Cefiderocol is a novel siderophore cephalosporin that employs a 'Trojan horse' strategy to enter the bacterial cell; it binds to extracellular free iron and utilizes bacterial active iron transport channels to hijack the cell and penetrate the outer cell membrane [7]. Cefiderocol primarily targets penicillin-binding protein 3 (PBP3), disrupting cell wall synthesis [8], however, modifications to PBP3 may confer resistance to cefiderocol [9].
Cefiderocol circumvents resistance mechanisms related to porin channel mutations and upregulated efflux pumps; it also possesses intrinsic stability against hydrolysis by carbapenemases [7]. In particular, its side-chain properties confer high stability against hydrolysis by a range of β-lactamases, including serine β-lactamases, such as ESBLs, and metallo-β-lactamases. This makes cefiderocol one of the few effective options against difficult-to-treat Gram-negative bacteria that produce metallo-β-lactamases, making it particularly useful in treating infections caused by pathogens resistant to almost all other β-lactams [10].
According to large cohort studies [11,12,13], cefiderocol demonstrates effectiveness against most strains of Enterobacterales, P. aeruginosa, S. maltophilia and A. baumannii, including those resistant to carbapenems, β-lactam/β-lactamase inhibitor combinations and polymyxins. However, resistance to cefiderocol has been reported in certain cohorts [14,15,16], and increasing evidence highlights the emergence of resistance during treatment [9,17,18,19,20].
2. Cefiderocol: Mechanism of Action and In Vitro Activity
Cefiderocol (formerly S-649266, GSK2696266) is a new catechol-conjugated cephalosporin developed and marketed by Shionogi & Co., Ltd. as promising drug for treatment of multidrug resistant Gram-negative bacilli infections [21]. Its structure, which has similar features to those of cefepime and ceftazidime, is characterized by several constituent groups that are the basis of its multiple mechanisms of action (refer to Figure 1) [22].
On the C-7 side chain, aminothiazole, oxime and dimethyl groups, and carboxylic acid provide antibacterial activity, stability to β-lactamases hydrolysis, and permeability to outer membrane, respectively [22]. On the C-3 side chain, essential carboxylic acid, pyrrolidinium group, and chlorocathecol improve penicillin-binding proteins affinity, antibacterial activity and stability to β-lactamases hydrolysis, and confers the ability to bind free ferric ions, respectively [22]. It is precisely this latter siderophore activity in the extracellular environment that represents the unique and distinctive mechanism of action of cefiderocol. In fact, this property, which has been renamed the Trojan horse strategy, allows cefiderocol to enter the bacterial cell via the iron transport system, overcoming resistance mechanisms responsible for outer membrane impermeability (i.e. regulation efflux pump, loss of the porin channel) (refer to Figure 2).
The high activity of cefiderocol has been reported in several in vitro studies (refer to Table 1) [23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49], the most robust reported in a recent systematic review and meta-analysis [23].
Karakonstantis et al analysed 78 studies reporting more than 82000 worldwide clinical isolates. Prevalence of cefiderocol non-susceptibility was low overall but varied according to 1) species (Enterobacterales 3.0%, P. aeruginosa 1.4%, A. baumannii 8.8%, and S. maltophilia 0.4%), 2) phenotype (carbapenem-resistant Enterobacterales 12.4% and carbapenem-resistant A. baumannii 13.2%), and 3) genotype (New Delhi metallo-β-lactamase-producing Enterobacterales 38.8%, New Delhi metallo-β-lactamase-producing P. aeruginosa 22.9%, New Delhi metallo-β-lactamase-producing A. baumannii 44.7%, and ceftazidime/avibactam-resistant Enterobacterales 36.6%) [23]. Further evidence has been added to these data over the past year. Data from the main published series show that cefiderocol retains potent activity (>90%) against the main Gram-negative bacteria, with the exception of Klebsiella pneumoniae strains reported in an Indian study [24] and P. aeruginosa [33], S. maltophilia, Achromobacter and Burkholderia species isolates [39] detected from patients with cystic fibrosis. The data on susceptibility to cefiderocol tended to be reduced in sub-analyses that only considered collections of carbapenem non-susceptible strains, mainly involving K. pneumoniae (80.6%) [24], P. aeruginosa (60.3% and 70.6%) [33,36], A. baumannii (85%) [35], and Achromobacter species (88.5%) [42]. Suboptimal activity of cefiderocol has been also reported in recent Czech [28] and Turkish [46] studies on carbapenem-non-susceptible Enterobacterales (82%), P. aeruginosa (84%), and A. baumannii (59.6%) isolates, respectively. Among studies characterising carbapenemase-producing strains, cefiderocol showed <90% activity against Enterobacterales (86-90%; 83.4-87.5%; 83.3%) [27,40,48] and P. aeruginosa (69%, 79.5%) strains collections [34,44]. In all cases, the most common concerned mechanism of resistance is metallo-β-lactamase production, especially New Delhi metallo-β-lactamase-type. On contrast, over 90% activity of cefiderocol against carbapenemase-producing A. baumannii (91.2% and 97.9%) has been shown in two reports of Japanese and American bacterial surveillance programmes [47,48].
3. Mechanisms of Cefiderocol Resistance
The key characteristics of cefiderocol are its active uptake mechanisms by Gram-negative bacteria under iron-depleted conditions and its improved stability to the hydrolytic activity of various types of β-lactamases. However, a variety of mechanisms may be involved in the acquisition of cefiderocol resistance, and they can be summarized into four groups: mutations in genes related to iron transfer systems, expression of β-lactamases, mutations in penicillin binding proteins, porin loss or efflux pump overexpression. Each of these mechanisms alone is generally not sufficient to increase cefiderocol MICs above PK/PD breakpoints. Therefore, resistance to cefiderocol is typically acquired as a consequence of various combinations of the above resistance mechanisms.
3.1. Mutations in Genes Related to Iron Transfer Systems
The role of siderophore receptor mutations in cefiderocol resistance has been shown by studies both on isogenic mutants and clinical isolates. Among the receptors recognized for cefiderocol uptake in P. aeruginosa and A. baumannii are two TonB-dependent receptors (TBDRs), PiuA and PirA [50]. Inactivation of piuA has been associated with a 16 to 32-fold increase of cefiderocol MIC in P. aeruginosa mutants [50,51]. Similarly, the deletion of piuD (an ortholog of piuA) increased cefiderocol MICs 32-fold in P. aeruginosa [51]. Moreover, deletion of pirA in P. aeruginosa was associated with low (two-fold increase) or no impact on cefiderocol MIC [50,51], but combining deletion of piuA or piuD with deletion of pirA the increase was of 32-fold and 64-fold, respectively [50,51]. In vivo emergence of cefiderocol resistance involving iron transport receptors has been reported in patients treated with ceftazidime/avibactam or ceftolozane/tazobactam [52,53]. Gomis-Font et al. reported the emergence of in vivo cefiderocol resistance development in P. aeruginosa caused by a large genomic deletion, including the piuDC region and the ampC regulator AmpD, in the absence of cefiderocol treatment. This deletion led to co-resistance to cefiderocol and ceftazidime/avibactam as result of AmpC overespression and PiuDC loss [52]. Streling et al. reported a P. aeruginosa isolate that acquired resistance to cefiderocol after ceftolozane/tazobactam treatment and exhibited the substitution L147F in AmpC gene together with mutations in piuA and pirR genes compared to the ancestor isolate [53]. The relevant role of PiuA in cefiderocol resistance has also been demonstrated in A. baumannii. Genomic analysis of cefiderocol-resistant A. baumannii clinical isolates revealed deficiency of piuA alone or associated with reduced expression of pirA [54,55]. Recently, Findlay et al. reported the in vivo emergence of cefiderocol resistance following 10 days of cefiderocol treatment in a burn ICU patient with A. baumannii bloodstream infection. WGS analysis of cefiderocol-resistant and the ancestor cefiderocol-susceptible isolate revealed a three nucleotides deletion upstream of piuA causing the down expression of the gene [56]. Huang et al. identified pirA inactivation of by insertion of an ISAba36 element as key resistance mechanism following cefiderocol treatment in a patient with OXA-72-producing A. baumannii infection. [57].
In Enterobacterales, alterations in siderophore receptors CirA and/or Fiu have been associated with reduced susceptibility or resistance to cefiderocol. Various mutations in cirA resulted in increased cefiderocol MIC values in K. pneumoniae and Enterobacter cloacae complex strains, both on isogenic mutants and in vitro induced resistant strains [58,59]. Most of the cefiderocol-resistant K. pneumoniae or Escherichia coli clinical isolates presenting mutations in cirA were also producers of NDM metallo-β-lactamases, highlighting the role of certain β-lactamases in contributing to resistance [60,61,62,63,64]. Experiments on isogenic mutants of E. coli showed that loss of Fiu resulted to two-fold increase of cefiderocol MIC, increasing up to 16-fold when combined with deletion of cirA [50]. Mutations in other iron uptake and transport related genes (e.g., fhuA, fepA, iutA, cirA, sitC, apbC, fepG, fepC, fetB, yicI, yicJ, and yicL) were identified in cefiderocol-resistant K. pneumoniae isolates [65]. Alterations in genes encoding three inner membrane proteins which transfer energy to the outer membrane for iron transport (TonB–ExbB–ExbD), other tonB-dependent receptors (fecA), ferric iron ABC transporter (fbpA), iron uptake system component (efeo) were also identified in in vitro derived cefiderocol-resistant K. pneumoniae mutants [66,67,68]. Moreover, mutations in fhuA (ferrichrome iron receptor) or fepA (ferric enterobactin receptor) were identified in two K. pneumoniae clinical isolates with cefiderocol MIC of 2 mg/L [69].
With regard to acquired resistance to cefiderocol in S. maltophilia, the data available in the literature are currently very limited. However, mutations affecting iron transport (tonB, exbD, smlat1148, cirA) were reported in in vitro derived cefiderocol-resistant S. maltophilia isolates [70,71].
Overall, given the multitude and diversity of genes involved in iron transfer systems suggest that further studies are needed to fully understand all possible pathways leading to cefiderocol resistance and their role in combinations including other types of resistance mechanisms.
3.2. Expression of β-Lactamases
Overall, although cefiderocol maintains relatively good activity against most carbapenem-resistant strains, its stability is incomplete especially against phenotypes including NDM-producing Enterobacterales and A. baumannii and ceftazidime/avibactam-resistant KPC-producing Enterobacterales [23]. In addition, this finding is further supported by the enhanced activity of cefiderocol when combined with clinically available β-lactamases inhibitors and dipicolinic acid in serine-β-lactamases- and metallo-β-lactamase-producing Gram-negative bacteria, respectively [72,73]. The contribution of the various types of β-lactamases is different as suggested by both cloning and mutagenesis experiments, and investigations on clinical isolates [9].
3.2.1. Metallo β-Lactamases
Contribution of NDM-type metallo-β-lactamase to cefiderocol hydrolysis was shown by cloning experiments in E. coli, P. aeruginosa and A. baumannii [75–78]. Four- to 64-fold increases in MIC values were observed, without significant difference among the different NDM variants (e.g. NDM-1, NDM-5, NDM-7, NDM-9) [73,74,75,76]. The combined effect of NDM expression and cirA deficiency in K. pneumoniae and E. coli was observed in several clinical isolates [60,61,62,63,64]. Moreover, increased copy number of blaNDM-5 together with increased expression of NDM-5 was associated with reduced susceptibility to cefiderocol in E. coli isolates [77,78]. In addition to the NDM type, other MBLs may be implicated although currently available evidence is limited. In vitro studies showed that introduction of SPM-1 gene caused significant decrease in cefiderocol activity in E. coli and P. aeruginosa, whereas VIM-2, AIM-1, and GIM-1 expression had low or no impact [75].
3.2.2. KPC Variants
One of the first pieces of evidence in favour of cross-resistance between ceftazidime/avibactam and cefiderocol in KPC-producing K. pneumoniae emerged by observing a significantly higher rate of cefiderocol resistance among ceftazidime/avibactam-resistant isolates than among susceptible ones (82.5% vs. 6.7%) [79]. To date, more than 200 variants of KPC have been reported worldwide and most of them were discovered in the last five years, following the introduction of ceftazidime/avibactam into clinical practice. Sequencing of blaKPC in clinical isolates with reduced susceptibility to cefiderocol and cloning experiments in isogenic strains confirmed that cross-resistance is due to expression of specific KPC variants, mostly with mutations in Ω loop of KPC (e.g. KPC-31, KPC-33, KPC-41, KPC-50, KPC-25, KPC-29, KPC-44, KPC-121, KPC-203, KPC-109, KPC-216) [80,81,82,83,84,85]. Given the structural similarity between ceftazidime and cefiderocol, mutations that increase the hydrolytic activity of the β-lactamase towards ceftazidime lead to co-resistance or reduced susceptibility to cefiderocol. Indeed, in this regard, combination of cefiderocol with new β-lactamase inhibitors such as avibactam, vaborbactam or relebactam seems promising to enhance its activity [72].
3.2.3. OXA-Type β-Lactamases
The effect of OXA-type β-lactamases expression on cefiderocol resistance is limited. Cloning experiments showed that both narrow-spectrum (OXA-1) and most of carbapenem-hydrolyzing (OXA-23, OXA-48, OXA-58) class D β-lactamases do not affect cefiderocol susceptibility [73,74,75,76]. In contrast, the recently identified carbapenemase OXA-427 showed significant hydrolytic activity against cefiderocol [74,75,76], although a low effect on cefiderocol MIC (two-fold increase) was demonstrated in E. coli isogenic mutants [75]. In addition, resistance to cefiderocol was reported in a collection of OXA-427-producing Enterobacterales in Belgium [86].
3.2.4. AmpC β-Lactamases
The involvement of AmpC variants in cefiderocol resistance is demonstrated by clinical reports and cloning experiments. The A292_L293del AmpC variant was associated with cross-resistance to cefepime, ceftazidime/avibactam and cefiderocol in E. cloacae complex. Cloning of the encoding-gene into E. coli TOP10 led to resistance to cefepime and ceftazidime/avibactam, and > 32-fold increase in the MIC of cefiderocol [87]. The role of four amino acid substitutions (A114E, Q120K, V211S, and N346Y) in CMY-2 AmpC (CMY-185) in development of cross resistance to ceftazidime/avibactam and cefiderocol was also shown in a E. coli clinical isolate [88]. Similarly, a new variant of CMY β-lactamase (CMY-186) characterized by a V159G amino acid substitution in the YXN loop of the enzyme was observed in a clinical isolate of K. pneumoniae [89].
3.2.5. Other β-Lactamases
Several in vitro studies have demonstrated high rates of cefiderocol resistance in A. baumannii and P. aeruginosa isolates expressing PER-type β-lactamases [15,73,91]. Cloning experiments of the various blaPER-like genes into E. coli, P. aeruginosa A. baumannii isogenic mutants showed a two- to 64-fold increase in the MIC of cefiderocol [73,74,75]. SHV-type EBSLs and BEL-type β-lactamases have been associated with increased cefiderocol MICs of cefiderocol following their introduction into isogenic mutants [73,74,75]. Amplification of blaSHV-12 has been associated with cefiderocol resistance in two hypervirulent K. pneumoniae clinical isolates in China [92]. In addition, the cephalosporinase PDC-30 was detected in two cases of in vivo cefiderocol-resistant P. aeruginosa, as the introduction of the respective gene in E. coli caused an eight-fold increase in the MIC of cefiderocol [17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93].
3.3. Mutations in Penicillin Binding Proteins
Since PBP-3 is the primary target of cefiderocol to exert its antibacterial effect, the presence of PBP-3 mutants represents the main mechanisms of resistance to cefiderocol at this level, although often in combination with other resistance markers (expression of β-lactamases and/or mutations in the in genes related to iron transfer systems). In detail, YRIN insertion in PBP-3 was observed in E. coli isolates with increased cefiderocol MIC values [60,68]. Barker et al. showed that PBP-3 mutant (insYRIN) alone was not sufficient to cause cefiderocol resistance, but its combination with NDM expression and/or cirA deletion was required [63]. This evidence is supported by cloning experiments of the gene encoding the mutated PBP-3 in E. coli, which showed only a two-fold increase in the MIC of cefiderocol [68]. Various mutations in PBP-3 among cefiderocol-resistant A. baumannii clinical isolates has been identified as potential resistance mechanisms to cefiderocol [54,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93]. However, their effective contribution to cefiderocol resistance needs further investigations.
3.4. Porin Loss or Efflux Pump Overexpression
The mechanism of porin loss has been associated to cefiderocol resistance in K. pneumoniae (ompK35, ompK36, ompK37) [94,95], E. cloacae (ompC and ompF) [94], and P. aeruginosa clinical isolates (Opr-D) [17]. Furthermore, deletion of ompK35/ompK36 and oprD in E. coli and P. aeruginosa isogenic mutants showed a two-to four-fold increase of the MIC values of cefiderocol, respectively [50,96]. The role of efflux transport proteins overexpression in cefiderocol resistance emerged in carbapenem-resistant K. pneumoniae [95], P. aeruginosa (MexAB–OprM) [96], S. maltophilia (SmeDEF) [73], and Achromobacter xylosoxidans (AxyABM) isolates [97].
4. Pharmacokinetic/Pharmacodynamic Features
Similar to other beta-lactams, cefiderocol is a time-dependent cephalosporin characterized by linear pharmacokinetics, limited volume of distribution (approximatively 15 L), short half-life (2-3 hours), moderate protein binding (equal to 58%), and predominant renal clearance [98]. The fraction of dosing interval during which the free drug concentrations exceeds the minimum inhibitory concentration (%fT>MIC) represents the best pharmacokinetic/pharmacodynamic (PK/PD) predictor of cefiderocol efficacy in infections caused by Enterobacterales, P. aeruginosa, A. baumannii, and S. maltophilia strains [99]. Notably, several preclinical models [100,101,102,103] reported that a bacteriostatic effect was observed with the attainment of a cefiderocol PK/PD target equal to 40-70%fT>MIC, whereas a bactericidal effect corresponding to ≥1-log kill reduction was reported with cefiderocol PK/PD target of 55-88%fT>MIC. Specifically, a P. aeruginosa neutropenic murine thigh model found that a fT>MIC of 76.3%, 81.9%, and 88.2% was required for stasis, 1-log kill, and 2-log kill reduction in bacterial burden, respectively [102]. Similarly, in murine thigh and lung infection models, the mean cefiderocol %fT>MIC needed for a 1-log kill reduction against 10 strains of Enterobacteriaceae and 3 strains of P. aeruginosa in the thigh infection models were 73.3% and 77.2%, respectively, whereas the mean %fT>MIC against Enterobacteriaceae, P. aeruginosa, A. baumannii, and S. maltophilia in the lung infection model were 64.4%, 70.3%, 88.1%, and 53.9%, respectively [104]. Overall, these preclinical data support the adoption of 2g every 8h administered over 3-h infusion for attaining the PK/PD target of 75%fT>MIC against Gram-negative pathogens showing MIC values of ≤4 mg/L [99].
However, recent preclinical and clinical studies suggested that the attainment of beta-lactam aggressive PK/PD targets (i.e., at least 100% fT>4 x MIC) may be recommended for maximizing not only clinical efficacy, but also for minimizing microbiological failure and suppressing resistance development [105; 106]. Notably, a recent meta-analysis including 21 observational studies with a total of 4,833 critically ill patients found that attaining aggressive PK/PD targets was significantly associated with higher clinical cure rate (OR=1.69; 95%CI 1.15–2.49) and lower risk of beta-lactam resistance development (OR=0.06; 95%CI 0.01–0.29). Conversely, failure in attaining aggressive PK/PD targets was significantly associated with higher risk of microbiological failure (OR=26.08; 95%CI 8.72–77.95) [106]. Although evidence concerning the adoption of aggressive PK/PD targets with novel beta-lactams are currently limited, this strategy should be pursued also in this setting, including patients receiving cefiderocol.
In this regard, although evidence investigating the relationship between cefiderocol PK/PD target attainment and clinical/microbiological outcome are limited, some interesting clues have been raised. Interestingly, a recent case series of 13 critically ill patients affected by severe COVID-19 pneumonia developing carbapenem-resistant A. baumannii bloodstream infections (BSIs) and/or ventilator-associated pneumonia treated with cefiderocol administered by extended infusion (EI) over 3-hours showed that only 38% attained aggressive PK/PD target (defined as a free trough concentration [fCmin]/MIC ratio > 4). Notably, patients attaining suboptimal PK/PD target attainment (i.e., a fCmin/MIC ratio < 1) had higher microbiological failure rate (80%) compared with those having quasi-optimal (i.e., a fCmin/MIC ratio 1–4) or optimal PK/PD targets (29%) [107]. Similarly, other two case series including respectively three patients affected by carbapenem-resistant A. baumannii infections and receiving cefiderocol administered by 3-hour EI during renal replacement therapy [108] and four cases of difficult-to-treat resistant (DTR) P. aeruginosa BSIs and/or nosocomial pneumonia treated with 3-hour EI cefiderocol [109] reported the attainment of optimal PK/PD targets in 67% and 75% of cases, respectively.
These findings could support the rationale for implementing cefiderocol altered dosing strategies by continuous infusion (CI) (i.e. 2 g every 8 hours over 8 h infusion according to aqueous stability restriction) after proper loading (2 g over 2-3 h) for maximizing the attainment of aggressive PK/PD targets. Indeed, in a recent case series of five critically ill patients affected by severe carbapenem-resistant A. baumannii infections and receiving CI cefiderocol (i.e., 2 g q8h over 8-h infusion) during continuous veno-venous hemodiafiltration aggressive PK/PD targets were attained in all included patients, ensuring optimal coverage for MIC up to 4 mg/L included [110].
It is noteworthy that optimal penetration and consequent attainment of aggressive PK/PD targets in infection sites represent a mandatory goal in the treatment of deep-seated infections, as suggested by the “antimicrobial puzzle” concepts [111]. In this scenario, evidence concerning cefiderocol penetration and absolute tissue concentrations are available for lung, central nervous system (CNS), and abdominal fluid.
Specifically, a prospective observational study investigating epithelial lining fluid (ELF) penetration of cefiderocol administered at a dosage of 2 g every 8 hours by EI over in 7 critically ill patients affected by ventilator-associated pneumonia reported a mean ELF-to-plasma ratio of 0.34, being the attainment of aggressive PK/PD targets ensured only for MIC up to 0.5 mg/L included [ 112; 113].
Four case report assessed penetration rate and absolute concentrations of cefiderocol in cerebrospinal fluid (CSF) [114]. Specifically, cefiderocol CSF-to-plasma ratio ranged from 0.04 to 0.50, whereas absolute fCmin ranged from 0.65 mg/L to 10.46 mg/L with administration of 2g every 6-8 hours over 3 hours EI. Although retrieved concentrations allowed to attain optimal cefiderocol PK/PD target in three out of 4 cases according to the MIC values of isolated pathogens, only in one case observed concentrations ensured the attainment of optimal PK/PD target for MIC up to the clinical breakpoint of 2 mg/L [114].
In regard to abdominal fluid penetration, a case report of a critically ill patient affected by DTR P. aeruginosa infection and treated with CI cefiderocol during continuous venovenous hemofiltration reported absolute concentrations in abdominal drain fluid equal to 15.3 mg/L, ensuring the attainment of optimal PK/PD target for MIC values up to the clinical breakpoint of 2 mg/L [115].
Overall, these findings may strongly support the adoption of cefiderocol altered dosing strategies consisting in high dosage coupled with CI administration for maximizing the attainment of optimal PK/PD targets in case of deep-seated infections [116].
5. Clinical Usage
Multi-drug resistant (MDR) and extensively drug resistant (XDR) gram-negative bacteria (GNB) are an alarming clinical challenge, burdened by a mortality rate of 30-50%, and scarce therapeutic options. In this context, the advent of cefiderocol represented a crucial innovation for clinicians who are called to face this issue.
Between 2019 and 2020, commercialization of cefiderocol was approved by Food and Drug Administration (FDA) for treatment of complicated urinary tract infections (cUTIs) [117] and for hospital acquired pneumonia (HAP) and ventilator acquired pneumonia (VAP), based on the results of CREDIBLE-CR, APEKS cUTI and APEKS NP phase III clinical trials [18,118,119]. Subsequently, in 2020, European Medicines Agency (EMA) approved cefiderocol for treatment of infections caused by GNB with limited therapeutic options, including carbapenem resistant P. aeruginosa (CRPa), S. maltophilia, carbapenem resistant Enterobacterales, carbapenem resistant A. baumanni (CRAb) [120].
Despite the approval was limited to certain clinical syndromes, cefiderocol has immediately gained its place in therapy for the treatment of serious CR-GNB infections as salvage therapy, whereas treatment options are tight.
5.1. Carbapenem Resistant Pseudomonas aeruginosa
The introduction of cefiderocol between the therapeutic opportunities was a game changer for treatment of P. aeruginosa infection. Indeed, P.aeruginosa is provided with different mechanism of antibiotic resistance, and the prevalence of carbapenem resistant strains is between 10 and 25% in most European countries, and reaches 50% in Eastern regions [121]. Moreover, resistance to newer betalactams/beta lactamase inhibitors (BL/BLI) in CRPa is spreading; however, cefidercol seems to retain sensitivity against these strains [122]. By exploring real-world studies, de La Fuente et al. reported in a cohort of 13 patients mainly affected by CRPa pneumonia a 28-day crude mortality of 23%, with achievement of clinical and microbiological cure of 84.6% (assessed 7 days after the end of treatment) [123]. A larger real-world case series published by Gavaghan et al. including 24 subjects with CR-GNB infections (mainly CRAb-14,5% and CRPa-10,4%) treated with cefiderocol reported a clinical success of 46% and a 30-day mortality of 42% [124].
A paper including 27 ICU patients affected by difficult to treat non-fermenting gram-negative bacteria infection (P.aeruginosa in 81,5% of cases) treated with cefiderocol compared with 54 patients who received the best available therapy (BAT) showed a higher relapse rate in cefiderocol with a comparable result in clinical cure or mortality rates compared to BAT [125].
A recent retrospective, multicenter, observational chart review study named PERSEUS, found an overall clinical success rate, defined as the composite outcome of clinical cure and/or survival at day 28 of 84.3% and a 28-day all-cause mortality of 21.5% in patients treated with cefiderocol for GNB infection, mainly P.aeruginosa (66,7%) [133.]
5.2. Stenotrophomonas maltophilia
Despite their poor frequency, treatment of infections caused by other fermenting gram negative bacteria, including S.maltophilia, result challenging due to the inherent antibiotic resistance of these pathogens. Mortality rates in S.maltophilia infection ranges to 21 and 69% [127]. Even in this scenario, cefiderocol seems to play a crucial role, as showed in a case series including 19 patients diagnosed with S.maltophilia infection treated with cefiderocol an in-hospital all-cause mortality at 14-day and 28-day of 36,8% and 21% respectively [128].
5.3. Carbapenem Resistant Enterobacterales
Cefiderocol, differently from the newer BL/BLI, retains efficacy against both serine- and metallo- beta lactamase. However, due to the lack of active drugs against metallo beta lactamase (MBL), cefiderocol could gain its place in therapy against Enterobacterales producing NDM, VIM, IMP. A subanalysis on results of CREDIBLE-CR and APEKS-NP trial including MBL infections (both Enterobacterales and on fermenting GNB) give us encouraging results, with higher rates of clinical cure, microbiological eradication and 28-day all-cause mortality, if compared to BAT or high dose meropenem respectively [129]. Nevertheless, some concerns should be investigated. In a real-world case series including 21 patients with infections caused by MBL-producing CR-Enterobacterales, the rate of cefiderocol resistance was 9,5% [130]. Indeed, according to microbiological data, cefiderocol resistance rates among NDM strains are of 81% and 12% using EUCAST and CLSI interpretive criteria, respectively [131].
According to these data, the empirical use of cefiderocol for treatment of MBL-Enterobacterales infections should be discouraged until result of microbiological susceptibility test.
5.4. Carbapenem Resistant Acinetobacter baumannii
Finally, during the last years, cefiderocol has been largely used for treatment of CRAb infections, primarily BSI and VAP, in context of intensive care units (ICU) wards.
Hence, several case series and comparative studies exploring the efficacy and safety of this new drug in “real-world” have been published. Bavaro et al. reported 13 cases of treated with cefiderocol-based combination therapy (10/13 CRAb), with a rate of microbiological eradication of 100% and a 30-day survival rate of 77% [132]. Similarly, another interesting case series including 10 critically ill patients with bloodstream infection (BSI) or VAP mainly caused by CRAb, stated a clinical success of 70%, while 30-day mortality was of 10% [133]. Another study including 118 patients with CRAb monomicrobial bacteremia showed a significantly lower 30-day mortality in patients treated with cefiderocol if compared to patients treated with colistin (40% vs 59%, p = 0.045), and cefiderocol based treatment resulted protective. [134].
Dalfino et al. explored the difference in terms of clinical failure between patients affected by CRAb VAP treated with cefiderocol-based regimens and colistin-based regimen: a higher Charlson comorbidity index independently predicted the occurrence of clinical failure, while timely targeted antibiotic treatment and cefiderocol-based first-line regimens reduced the risk of treatment failure [135]. Further studies highlighted how the use of cefiderocol for treatment of VAP caused by CRAb was associated with a benefit on 28-day [136] and 30-day mortality [137] An additional study including patients affected by CRAb BSI treated with cefiderocol or colistin showed a significantly higher clinical cure in cefiderocol group, lower rate of adverse events; particularly, in HAP/VAP group treatment with cefiderocol was associated with lower 30-day mortality and higher clinical cure [138]
An Italian multicentric retrospective study by Pascale et al, including 107 patients admitted in ICU for COVID19 who developed CRAb infection treated with cefiderocol as monotherapy in 45% of cases and colistin-based regimens in 55%, showed any difference in all-cause 28-day mortality rate between the two groups; however, in multivariable analysis, cefiderocol was associated with a non-significant lower mortality risk [139].
The ARES study, a multicentric retrospective cohort study including critically ill patients treated with cefiderocol for CRAb infection, resulted in a clinical success rate of 53 %, with better results in subjects who were not affected by septic shock and COVID19, and with a lower SOFA score [140].
Overall, the results of real-world studies are more encouraging if compared to CREDIBLE-CR, where cefiderocol was non-inferior if compared to best available therapy in terms of clinical and microbiological response but resulted in a higher mortality rate (49% vs 18%), with the majority of deaths in CRAb group. Notably, cefiderocol group included patients with higher SOFA and CCI score, who experienced previous failure to BAT.
On the basis of the current available data, the latest Infectious Diseases Society of America (IDSA) guidance for treatment of Antimicrobial Resistant Gram-Negative Infections recommends limiting the use of cefiderocol as salvage therapy for CRAb infections, only in case of resistance or intolerance to other regimens, as part of a combination therapy [141].
6. Prospectives and Open Questions
Accordingly, the above-mentioned document of guidance opens another important and still unresolved question: the use of the molecule as monotherapy or as part of combination regimens.
Regarding combination therapy, despite its usefulness in clinical trials is not demonstrated, this strategy could be successful in clinical practice for different reasons: i) the synergistic effect; ii) to avoid resistance development; iii) to extend spectrum of antimicrobial activity in the first phase of treatment, when the causative pathogen and its sensitivity profile are still unknown. In this sense, a good partner for cefiderocol could be intravenous fosfomycin, even for CRAb, which results intrinsically resistant to the epoxide molecule [142]: indeed, its mechanism of action lead to a stressful condition that make pathogens more sensitive to other antimicrobial agents and prevent the development of resistance [143].
Despite resistance to cefiderocol is not frequently detected, it should be taken into account, when susceptibility test is not available. Interestingly, multiple mechanisms contribute to this condition: increased expression of beta-lactamase (metallo beta lactamase), mutation of target protein or siderophore receptor and outer membrane porine, overexpression of efflux transport proteins [9,144].
Moreover, the rise of resistance in course of treatment has been described. In particular, among different reasons, the phenomenon of heteroresistance could be involved in this process: it occurs when a small proportion of bacteria develop resistance under antibiotic pressure; as a consequence, the unsusceptible population grows in course of prolonged antibiotic exposure [86,91,145–147]
Combination therapy could play a role in reducing this phenomenon, along with the optimization of pharmacokinetics/pharmacodynamics parameters of cefiderocol [148].
Despite the innovativeness of this molecule, the encouraging results of real-world study in terms of safety and effectiveness, and the need of new antibiotic for treatment of XDR GNB, some open questions about its use in daily clinical practice remain. The prescription of cefiderocol in hospital settings where the rate of CR-GNB is high could be considered in case of severe infections and septic shock, in absence of other therapeutic chances, in order to provide promptly an effective therapy.Further clinical trial to optimize the use of cefiderocol are warranted.
7. Conclusions
The limited antimicrobial options for treatment of infections due to MDR microorganisms poses the urgent need of new antimicrobial drugs. To fight this plague and to contrast the increasing diffusion of the antimicrobial resistance in gram negative bacteria, in the last years, the development of novel antimicrobial molecules have been proposed. In this context, Cefiderocol, a new siderofore-conjugated cephalosporin, have revolutionated the therapeutic schemes of treatment for infections due to MDR pathogens. In contrast to other cephalosporin, cefiderocol is a siderophore compound with a the catechol residue acting as an iron chelator able to cross the outer membrane of Gram-negative bacteria through the siderophore iron uptake system. The unique mechanism of entry into the bacterial cells by taking advantage of the iron uptake system, have defined this strategy as a “Trojan horse”. This innovative strategy used by Cefiderocol render this molecules protect against the different bacteria mechanisms to counteract the bacteria cells import of different antimicrobial drugs such as mutations (i.e. efflux pumps’ overexpression and porins’ downregulation or truncation) by altering the outer membrane permeability.
The numerous advantages offered by cefiderocol including the high antibacterial activity, the excellent profile of safety and tolerability and the broad range of activity against various gram negative pathogens has earned the role of “promising antibiotic“ for treatment against MDR bacteria posed the basis for novel antimicrobial weapons by defining new paradigms of treatment for the and infections especially in critical ill patients.
Despite the initial promising in vitro and in vivo results, the emergence of resistant to cefiderocol have been observed worldwide with an increasing number of clinical reports. Therefore, the adaptability to the different antimicrobial molecules is a common strategy observed in the bacterial’s world. In this context, the development of different mechanisms to counteract to the activity of cefiderocol is not immune. However, the broad range of activity against different MDR pathogens, the high penetrability in several anatomical sites and the evidence of the efficacy and safety render this molecule a fundamental tool in the clinical real-life especially for the treatment of Difficult-to-treat (DTR) infections due to MDR pathogens.
Author Contributions
All authors write the original version of the manuscript and reviewed the final version.
Funding
This work was supported by FUR2024 from University o Verona to Paolo Gaibani.
Conflicts of Interest
All authors declare no conflict of interest.
References
- Bloom DE, Black S, Salisbury D, Rappuoli R. Antimicrobial resistance and the role of vaccines. Proc Natl Acad Sci U S A. 2018; 115(51):12868-12871. [CrossRef] [PubMed] [PubMed Central]
- Shi Z, Zhang J, Tian L, Xin L, Liang C, Ren X, Li M. A Comprehensive Overview of the Antibiotics Approved in the Last Two Decades: Retrospects and Prospects. Molecules. 2023; 28(4):1762. [CrossRef] [PubMed] [PubMed Central]
- Bassetti M, Kanj SS, Kiratisin P, Rodrigues C, Van Duin D, Villegas MV, Yu Y. Early appropriate diagnostics and treatment of MDR Gram-negative infections. JAC Antimicrob Resist. 2022; 4(5):dlac089. [CrossRef] [PubMed] [PubMed Central]
- Parmanik A, Das S, Kar B, Bose A, Dwivedi GR, Pandey MM. Current Treatment Strategies Against Multidrug-Resistant Bacteria: A Review. Curr Microbiol. 2022; 79(12):388. [CrossRef] [PubMed] [PubMed Central]
- Boyd SE, Livermore DM, Hooper DC, Hope WW. Metallo-β-Lactamases: Structure, Function, Epidemiology, Treatment Options, and the Development Pipeline. Antimicrob Agents Chemother. 2020; 64(10):e00397-20. [CrossRef] [PubMed] [PubMed Central]
- Echols R, Ariyasu M, Nagata TD. Pathogen-focused Clinical Development to Address Unmet Medical Need: Cefiderocol Targeting Carbapenem Resistance. Clin Infect Dis. 2019; 69(Suppl 7):S559-S564. [CrossRef] [PubMed] [PubMed Central]
- Heil EL, Tamma PD. Cefiderocol: the Trojan horse has arrived but will Troy fall? Lancet Infect Dis. 2021; 21(2):153-155. Reference for challenges with MBL-producing Enterobacterales. [CrossRef] [PubMed]
- Abdul-Mutakabbir JC, Alosaimy S, Morrisette T, Kebriaei R, Rybak MJ. Cefiderocol: A Novel Siderophore Cephalosporin against Multidrug-Resistant Gram-Negative Pathogens. Pharmacotherapy. 2020; 40(12):1228-1247. [CrossRef] [PubMed]
- Karakonstantis S, Rousaki M, Kritsotakis EI. Cefiderocol: Systematic Review of Mechanisms of Resistance, Heteroresistance and In Vivo Emergence of Resistance. Antibiotics (Basel). 2022; 11(6):723. Reference for cefiderocol's affinity for PBP2 in Klebsiella pneumoniae. [CrossRef] [PubMed] [PubMed Central]
- Ong'uti S, Czech M, Robilotti E, Holubar M. Cefiderocol: A New Cephalosporin Stratagem Against Multidrug-Resistant Gram-Negative Bacteria. Clin Infect Dis. 2022; 74(7):1303-1312. Reference for cefiderocol's stability against ESBLs and MBLs. [CrossRef] [PubMed] [PubMed Central]
- Karlowsky, J.A.; Hackel, M.A.; Takemura, M.; Yamano, Y.; Echols, R.; Sahm, D.F. In Vitro Susceptibility of Gram-Negative Pathogens to Cefiderocol in Five Consecutive Annual Multinational SIDERO-WT Surveillance Studies, 2014 to 2019. Antimicrob. Agents Chemother. 2022, 66, e0199021.
- Candel, F.J.; Henriksen, A.S.; Longshaw, C.; Yamano, Y.; Oliver, A. In vitro activity of the novel siderophore cephalosporin, cefiderocol, in Gram-negative pathogens in Europe by site of infection. Clin. Microbiol. Infect. 2022, 28, 447.e1–447.e6.
- Golden, A.R.; Adam, H.J.; Baxter, M.; Walkty, A.; Lagacé-Wiens, P.; Karlowsky, J.A.; Zhanel, G.G. In Vitro Activity of Cefiderocol, a Novel Siderophore Cephalosporin, against Gram-Negative Bacilli Isolated from Patients in Canadian Intensive Care Units. Diagn. Microbiol. Infect. Dis. 2020, 97, 115012.
- Morris, C.P.; Bergman, Y.; Tekle, T.; Fissel, J.A.; Tamma, P.D.; Simner, P.J. Cefiderocol Antimicrobial Susceptibility Testing against Multidrug-Resistant Gram-Negative Bacilli: A Comparison of Disk Diffusion to Broth Microdilution. J. Clin. Microbiol. 2020, 59, e01649-20.
- Mushtaq, S.; Sadouki, Z.; Vickers, A.; Livermore, D.M.; Woodford, N. In Vitro Activity of Cefiderocol, a Siderophore Cephalosporin, against Multidrug-Resistant Gram-Negative Bacteria. Antimicrob. Agents Chemother. 2020, 64, 12.
- E Choby, J.; Ozturk, T.; Satola, S.W.; Jacob, J.T.; Weiss, D.S. Widespread cefiderocol heteroresistance in carbapenem-resistant Gram-negative pathogens. Lancet Infect. Dis. 2021, 21, 597–598.
- Takemura, M.; Yamano, Y.; Matsunaga, Y.; Ariyasu, M.; Echols, R.; Nagata, T.D. 1266. Characterization of Shifts in Minimum Inhibitory Concentrations During Treatment with Cefiderocol or Comparators in the Phase 3 CREDIBLE-CR and APEKS-NP Studies. Open Forum Infect. Dis. 2020, 7, S649–S650.
- Wunderink, R.G.; Matsunaga, Y.; Ariyasu, M.; Clevenbergh, P.; Echols, R.; Kaye, K.S.; Kollef, M.; Menon, A.; Pogue, J.M.; Shorr, A.F.; et al. Cefiderocol versus high-dose, extended-infusion meropenem for the treatment of Gram-negative nosocomial pneumonia (APEKS-NP): A randomised, double-blind, phase 3, non-inferiority trial. Lancet Infect. Dis. 2020, 21, 213–225. [CrossRef]
- Bassetti, M.; Echols, R.; Matsunaga, Y.; Ariyasu, M.; Doi, Y.; Ferrer, R.; Lodise, T.P.; Naas, T.; Niki, Y.; Paterson, D.L.; et al. Efficacy and safety of cefiderocol or best available therapy for the treatment of serious infections caused by carbapenem-resistant Gram-negative bacteria (CREDIBLE-CR): A randomised, open-label, multicentre, pathogen-focused, descriptive, phase 3 trial. Lancet Infect. Dis. 2021, 21, 226–240.
- Klein, S.; Boutin, S.; Kocer, K.; O Fiedler, M.; Störzinger, D.; A Weigand, M.; Tan, B.; Richter, D.; Rupp, C.; Mieth, M.; et al. Rapid Development of Cefiderocol Resistance in Carbapenem-resistant Enterobacter cloacae During Therapy Is Associated With Heterogeneous Mutations in the Catecholate Siderophore Receptor cirA. Clin. Infect. Dis. 2021, 74, 905–908.
- Aoki T, Yoshizawa H, Yamawaki K, Yokoo K, Sato J, Hisakawa S, et al. Cefiderocol (S-649266), A new siderophore cephalosporin exhibiting potent activities against Pseudomonas aeruginosa and other gram-negative pathogens including multi-drug resistant bacteria: Structure activity relationship. Eur J Med Chem 2018; 155:847-68. [CrossRef]
- Sato T, Yamawaki K. Cefiderocol: Discovery, Chemistry, and In Vivo Profiles of a Novel Siderophore Cephalosporin. Clin Infect Dis 2019; 69:S538-S543. [CrossRef]
- Karakonstantis S, Rousaki M, Vassilopoulou L, Kritsotakis EI. Global prevalence of cefiderocol non-susceptibility in Enterobacterales, Pseudomonas aeruginosa, Acinetobacter baumannii, and Stenotrophomonas maltophilia: a systematic review and meta-analysis. Clin Microbiol Infect 2024; 30:178-88. [CrossRef]
- Borde K, Kareem MA, Sharma RM, Dass SM, Ravi V, Mathai D. In vitro activity of cefiderocol against comparators (ceftazidime-avibactam, ceftazidime-avibactam/ aztreonam combination, and colistin) against clinical isolates of meropenem-resistant Klebsiella pneumoniae from India. Microbiol Spectr 2023; 11:e0084723. [CrossRef]
- Gijón D, García-Castillo J, Fernández-López MC, Bou G, Siller M, Calvo-Montes J, et al. In vitro activity of cefiderocol and other newly approved antimicrobials against multi-drug resistant Gram-negative pathogens recovered in intensive care units in Spain and Portugal. Rev Esp Quimioter 2024; 37:69-77. [CrossRef]
- Daoud L, Al-Marzooq F, Ghazawi A, Anes F, Collyns T. High efficacy and enhanced synergistic activity of the novel siderophore-cephalosporin cefiderocol against multidrug-resistant and extensively drug-resistant Klebsiella pneumoniae from inpatients attending a single hospital in the United Arab Emirates. J Infect Public Health 2023; 16 Suppl 1:33-44. [CrossRef]
- Zhao J, Pu D, Li Z, Liu X, Zhang Y, Wu Yet al. In vitro activity of cefiderocol, a siderophore cephalosporin, against carbapenem-resistant hypervirulent Klebsiella pneumoniae in China. Antimicrob Agents Chemother 2023; 67:e0073523. [CrossRef]
- Malisova L, Vrbova I, Pomorska K, Jakubu V, Zemlickova H. In Vitro Activity of Cefiderocol Against Carbapenem-Resistant Enterobacterales and Pseudomonas aeruginosa. Microb Drug Resist 2023; 29:485-91. [CrossRef]
- Khanchandani H, Chaudhury M, Rao MS, Ramakrishna N, Venkataramana B, Chaudhury A. In vitro activity of the newly approved antimicrobial agent Cefiderocol against Carbapenem resistant Gram negative clinical isolates. Indian J Med Microbiol 2024; 48:100556. [CrossRef]
- Saxena S, Aggarwal P, Mitra S, Singh S, Kaim M, Sharma A. In vitro assessment of newer colistin-sparing antimicrobial agents for clinical isolates of carbapenem-resistant organisms. J Infect Chemother 2024: S1341-321X(24)00149-1. [CrossRef]
- Shields RK, Kline EG, Squires KM, Van Tyne D, Doi Y. In vitro activity of cefiderocol against Pseudomonas aeruginosa demonstrating evolved resistance to novel β-lactam/β-lactamase inhibitors. JAC Antimicrob Resist 2023; 5:dlad107. [CrossRef]
- Riccobene T, Ai C, Yu KC, Gregory S, Kim B, Debabov D, et al. Real-world in vitro activity of newer antibiotics against Enterobacterales and Pseudomonas aeruginosa, including carbapenem-non-susceptible and multidrug-resistant isolates: a multicenter analysis. Microbiol Spectr 2023; 11:e0312923. [CrossRef]
- Monogue ML, Desai D, Pybus CA, Sanders JM, Clark AE, Greenberg DE. In vitro activity of cefiderocol against Pseudomonas aeruginosa isolated from cystic fibrosis patients. Microbiol Spectr 2023; 11:e0304723. [CrossRef]
- Gill CM, Santini D, Nicolau DP. In vitro activity of cefiderocol against a global collection of carbapenem-resistant Pseudomonas aeruginosa with a high level of carbapenemase diversity. J Antimicrob Chemother 2024; 79:412-6. [CrossRef]
- Santerre Henriksen A, Jeannot K, Oliver A, Perry JD, Pletz MW, Stefani S, et al. In vitro activity of cefiderocol against European Pseudomonas aeruginosa and Acinetobacter spp., including isolates resistant to meropenem and recent β-lactam/β-lactamase inhibitor combinations. Microbiol Spectr 2024; 12:e0383623. [CrossRef]
- Maruri-Aransolo A, López-Causapé C, Hernández-García M, García-Castillo M, Caballero-Pérez JD, Oliver A, et al. In vitro activity of cefiderocol in Pseudomonas aeruginosa isolates from people with cystic fibrosis recovered during three multicentre studies in Spain. J Antimicrob Chemother 2024; 79:1432-40. [CrossRef]
- Valzano F, La Bella G, Lopizzo T, Curci A, Lupo L, Morelli E, et al. Resistance to ceftazidime-avibactam and other new β-lactams in Pseudomonas aeruginosa clinical isolates: a multi-center surveillance study. Microbiol Spectr 2024: e0426623. [CrossRef]
- Huang YS, Chuang YC, Chen PY, Chou PC, Wang JT. In vitro activity of cefiderocol and comparator antibiotics against multidrug-resistant non-fermenting Gram-negative bacilli. JAC Antimicrob Resist 2024; 6:dlae006. [CrossRef]
- Tunney MM, Elborn JS, McLaughlin CS, Longshaw CM. In vitro activity of cefiderocol against Gram-negative pathogens isolated from people with cystic fibrosis and bronchiectasis. J Glob Antimicrob Resist 2024; 36:407-10. [CrossRef]
- Bianco G, Boattini M, Comini S, Iannaccone M, Casale R, Allizond V, et al. Activity of ceftolozane-tazobactam, ceftazidime-avibactam, meropenem-vaborbactam, cefiderocol and comparators against Gram-negative organisms causing bloodstream infections in Northern Italy (2019-2021): emergence of complex resistance phenotypes. J Chemother 2022; 34:302-10. [CrossRef]
- Méndez-Sotelo BJ, Delgado-Beltrán M, Hernández-Durán M, Colín-Castro CA, Esquivel-Bautista J, Ortega-Oliva SA, et al. In vitro activity of ceftazidime/avibactam, cefiderocol, meropenem/vaborbactam and imipenem/relebactam against clinical strains of the Stenotrophomonas maltophilia complex. PLoS One 2024; 19:e0298577. [CrossRef]
- Takemura M, Nakamura R, Ota M, Nakai R, Sahm DF, Hackel MA, et al. In vitro and in vivo activity of cefiderocol against Achromobacter spp. and Burkholderia cepacia complex, including carbapenem-non-susceptible isolates. Antimicrob Agents Chemother 2023; 67:e0034623. [CrossRef]
- Jean-Pierre V, Sorlin P, Pantel A, Chiron R, Lavigne JP, Jeannot K, et al. Cefiderocol susceptibility of Achromobacter spp.: study of an accurately identified collection of 230 strains. Ann Clin Microbiol Antimicrob 2024; 23:54. [CrossRef]
- Jena J, Behera B, Nayak G, Mohanty S, Mahapatra A, Purushotham P, et al. In Vitro Susceptibility of Burkholderia pseudomallei Isolates to Cefiderocol and Ceftazidime/Avibactam from Odisha, India. J Lab Physicians 2023; 15:573-7. [CrossRef]
- Findlay J, Raro OHF, Poirel L, Nordmann P. Molecular analysis of metallo-beta-lactamase-producing Pseudomonas aeruginosa in Switzerland 2022-2023. Eur J Clin Microbiol Infect Dis 2024; 43:551-7. [CrossRef]
- Uskudar-Guclu A, Danyildiz S, Mirza HC, Akcil Ok M, Basustaoglu A. In vitro activity of cefiderocol against carbapenem-resistant Acinetobacter baumannii carrying various β-lactamase encoding genes. Eur J Clin Microbiol Infect Dis 2024; 43:1171-9. [CrossRef]
- Bulens SN, Campbell D, McKay SL, Vlachos N, Burgin A, Burroughs M, et al. Carbapenem-resistant Acinetobacter baumannii complex in the United States-An epidemiological and molecular description of isolates collected through the Emerging Infections Program, 2019. Am J Infect Control 2024: S0196-6553(24)00458-9. [CrossRef]
- Kayama S, Kawakami S, Kondo K, Kitamura N, Yu L, Hayashi W, et al. In vitro activity of cefiderocol against carbapenemase-producing and meropenem-non-susceptible Gram-negative bacteria collected in the Japan Antimicrobial Resistant Bacterial Surveillance. J Glob Antimicrob Resist 2024; 38:12-20. [CrossRef]
- Dahdouh E, Gómez-Marcos L, Cañada-García JE, de Arellano ER, Sánchez-García A, Sánchez-Romero I, et al. Characterizing carbapenemase-producing Escherichia coli isolates from Spain: high genetic heterogeneity and wide geographical spread. Front Cell Infect Microbiol 2024; 14:1390966. [CrossRef]
- to A, Sato T, Ota M, Takemura M, Nishikawa T, Toba S, Kohira N, Miyagawa S, Ishibashi N, Matsumoto S, Nakamura R, Tsuji M, Yamano Y. In Vitro Antibacterial Properties of Cefiderocol, a Novel Siderophore Cephalosporin, against Gram-Negative Bacteria. Antimicrob Agents Chemother. 2017; 62(1):e01454-17. [CrossRef]
- Luscher A, Moynié L, Auguste PS, Bumann D, Mazza L, Pletzer D, Naismith JH, Köhler T. TonB-Dependent Receptor Repertoire of Pseudomonas aeruginosa for Uptake of Siderophore-Drug Conjugates. Antimicrob Agents Chemother. 2018 ;62(6):e00097-18. [CrossRef]
- Gomis-Font MA, Clari MA, López-Causapé C, Navarro D, Oliver A. Emergence of cefiderocol resistance during ceftazidime/avibactam treatment caused by a large genomic deletion, including ampD and piuCD genes, in Pseudomonas aeruginosa. Antimicrob Agents Chemother. 2024; 68(1):e0119223. [CrossRef]
- Streling, A.P.; Al Obaidi, M.M.; Lainhart,W.D.; Zangeneh, T.; Khan, A.; Dinh, A.Q.; Hanson, B.; A Arias, C.; Miller,W.R. Evolution of Cefiderocol Non-Susceptibility in Pseudomonas aeruginosa in a Patient Without Previous Exposure to the Antibiotic. Clin. Infect. Dis. 2021, 73, 4472–4474. [CrossRef]
- Malik S, Kaminski M, Landman D, Quale J. Cefiderocol Resistance in Acinetobacter baumannii: Roles of β-Lactamases, Siderophore Receptors, and Penicillin Binding Protein 3. Antimicrob Agents Chemother. 2020; 64(11):e01221-20. [CrossRef]
- Yamano, Y.; Ishibashi, N.; Kuroiwa, M.; Takemura, M.; Sheng, W.-H.; Hsueh, P.-R. Characterisation of cefiderocol-non-susceptible Acinetobacter baumannii isolates from Taiwan. J. Glob. Antimicrob. Resist. 2021, 28, 120–124.
- Findlay J, Bianco G, Boattini M, Nordmann P. In vivo development of cefiderocol resistance in carbapenem-resistant Acinetobacter baumannii associated with the downregulation of a TonB-dependent siderophore receptor, PiuA. J Antimicrob Chemother. 2024; 79(4):928-930. [CrossRef]
- Huang E, Thompson RN, Moon SH, Keck JM, Lowry MS, Melero J, Jun S-R, Rosenbaum ER, Dare RK. Treatment-emergent cefiderocol resistance in carbapenem-resistant Acinetobacter baumannii is associated with insertion sequence ISAba36 in the siderophore receptor pirA. Antimicrob Agents Chemother. 2024: e0029024. [CrossRef]
- Nurjadi, D.; Kocer, K.; Chanthalangsy, Q.; Klein, S.; Heeg, K.; Boutin, S. New Delhi Metallo-Beta-Lactamase Facilitates the Emergence of Cefiderocol Resistance in Enterobacter cloacae. Antimicrob. Agents Chemother. 2022, 66, 2.
- McElheny, C.L.; Fowler, E.L.; Iovleva, A.; Shields, R.K.; Doi, Y. In Vitro Evolution of Cefiderocol Resistance in an NDM-Producing Klebsiella pneumoniae Due to Functional Loss of CirA. Microbiol. Spectr. 2021, 9, e0177921.
- Price, T.K.; Davar, K.; Contreras, D.;Ward, K.W.; Garner, O.B.; Simner, P.J.; Yang, S.; Chandrasekaran, S. Case Report and Genomic Analysis of Cefiderocol-Resistant Escherichia coli Clinical Isolates. Am. J. Clin. Pathol. 2021, 157, 257–265.
- Lan, P.; Lu, Y.; Chen, Z.;Wu, X.; Hua, X.; Jiang, Y.; Zhou, J.; Yu, Y. Emergence of High-Level Cefiderocol Resistance in Carbapenem-Resistant Klebsiella pneumoniae from Bloodstream Infections in Patients with Hematologic Malignancies in China. Microbiol. Spectr. 2022, 10, e0008422.
- Tascini C, Coppi M, Antonelli A, Niccolai C, Bartolini A, Pecori D, Sartor A, Giani T, Rossolini GM. In vivo evolution to high-level cefiderocol resistance of NDM-1-producing Klebsiella pneumoniae, followed by intra-hospital cross-transmission. Clin Microbiol Infect. 2024; 30(3):398-400. [CrossRef]
- Barker KR, Rebick GW, Fakharuddin K, MacDonald C, Mulvey MR, Mataseje LF. When the Trojan horse is unable to reach inside the city: investigation of the mechanism of resistance behind the first reported cefiderocol-resistant E. coli in Canada. Microbiol Spectr. 2024; 12(5):e0322323. [CrossRef]
- Arcari G, Cecilia F, Oliva A, Polani R, Raponi G, Sacco F, De Francesco A, Pugliese F, Carattoli A. Genotypic Evolution of Klebsiella pneumoniae Sequence Type 512 during Ceftazidime/Avibactam, Meropenem/Vaborbactam, and Cefiderocol Treatment, Italy. Emerg Infect Dis. 2023; 29(11):2266-2274. [CrossRef]
- Yamano, Y., Rio Nakamura, Miki Takemura, Roger Echols, Potential Mechanisms of Cefiderocol MIC Increase in Enterobacterales in In Vitro Resistance Acquisition Studies Open Forum Infectious Diseases Oxford Academic. 2020; 1455: URL https:// academic.oup.com/ofid/article/7/Supplement_1/S730/6057740.
- Padovani M, Bertelli A, Corbellini S, Piccinelli G, Gurrieri F, De Francesco MA. In Vitro Activity of Cefiderocol on Multiresistant Bacterial Strains and Genomic Analysis of Two Cefiderocol Resistant Strains. Antibiotics (Basel). 2023; 12:785. [CrossRef]
- Bao, J.; Xie, L.; Ma, Y.; An, R.; Gu, B.; Wang, C. Proteomic and Transcriptomic Analyses Indicate Reduced Biofilm-Forming Abilities in Cefiderocol-Resistant Klebsiella pneumoniae. Front. Microbiol. 2022, 12, 778190.
- Sato, T.; Ito, A.; Ishioka, Y.; Matsumoto, S.; Rokushima, M.; Kazmierczak, K.M.; Hackel, M.; Sahm, D.F.; Yamano, Y. Escherichia coli strains possessing a four amino acid YRIN insertion in PBP3 identified as part of the SIDERO-WT-2014 surveillance study. JAC-Antimicrob. Resist. 2020, 2, dlaa081.
- Zhang, Q.; Neidig, N.; Chu, T.-Y.; Divoky, C.; Carpenter, J.; Lee-Hsiao, C.; Threatt, H.; Sultana, R.; Bush, K. In vitro antibacterial activity of cefiderocol against recent multidrug-resistant carbapenem-nonsusceptible Enterobacterales isolates. Diagn. Microbiol. Infect. Dis. 2022, 103, 115651.
- Gill, C.M.; Abdelraouf, K.; Oota, M.; Nakamura, R.; Kuroiwa, M.; Gahara, Y.; Takemura, M.; Yamano, Y.; Nicolau, D.P. Discrepancy in sustained efficacy and resistance emergence under human-simulated exposure of cefiderocol against Stenotrophomonas maltophilia between in vitro chemostat and in vivo murine infection models. J. Antimicrob. Chemother. 2021, 76, 2615–2621.
- Werth, B.J.; Ashford, N.K.; Penewit, K.; Waalkes, A.; Holmes, E.A.; Bryan, A.; Salipante, S.J. Evolution of cefiderocol resistance in Stenotrophomonas maltophilia using in vitro serial passage techniques. JAC-Antimicrob. Resist. 2022, 4, dlac011.
- Bianco G, Gaibani P, Comini S, Boattini M, Banche G, Costa C, Cavallo R, Nordmann P. Synergistic Effect of Clinically Available Beta-Lactamase Inhibitors Combined with Cefiderocol against Carbapenemase-Producing Gram-Negative Organisms. Antibiotics (Basel). 2022; 11:1681. [CrossRef]
- Kohira, N.; Hackel, M.A.; Ishioka, Y.; Kuroiwa, M.; Sahm, D.F.; Sato, T.; Maki, H.; Yamano, Y. Reduced susceptibility mechanism to cefiderocol, a siderophore cephalosporin, among clinical isolates from a global surveillance programme (SIDERO-WT-2014). J. Glob. Antimicrob. Resist. 2020, 22, 738–41.
- Poirel, L.; Sadek, M.; Nordmann, P. Contribution of PER-Type and NDM-Type _-Lactamases to Cefiderocol Resistance in Acinetobacter baumannii. Antimicrob. Agents Chemother. 2021, 65, e0087721.
- Poirel, L.; de la Rosa, J.-M.O.; Sadek, M.; Nordmann, P. Impact of Acquired Broad-Spectrum _-Lactamases on Susceptibility to Cefiderocol and Newly Developed _-Lactam/_-Lactamase Inhibitor Combinations in Escherichia coli and Pseudomonas aeruginosa. Antimicrob. Agents Chemother. 2022, 66, e0003922.
- Fröhlich C, Sørum V, Tokuriki N, Johnsen PJ, Samuelsen Ø. Evolution of β-lactamase-mediated cefiderocol resistance. J Antimicrob Chemother. 2022; 77:2429-36. [CrossRef]
- Mezcord V, Traglia GM, Pasteran F, Escalante J, Lopez C, Wong O, Rojas L, Marshall SH, Tolmasky ME, Bonomo RA, Ramirez MS. Characterisation of cefiderocol-resistant spontaneous mutant variants of Klebsiella pneumoniae-producing NDM-5 with a single mutation in cirA. Int J Antimicrob Agents. 2024; 63:107131. [CrossRef]
- Simner, P.J.; Mostafa, H.H.; Bergman, Y.; Ante, M.; Tekle, T.; Adebayo, A.; Beisken, S.; Dzintars, K.; Tamma, P.D. Progressive Development of Cefiderocol Resistance in Escherichia coli during Therapy is Associated With an Increase in blaNDM-5 Copy Number and Gene Expression. Clin. Infect. Dis. 2021, ciab888.
- Bianco G, Boattini M, Comini S, Iannaccone M, Bondi A, Cavallo R, Costa C. In vitro activity of cefiderocol against ceftazidime-avibactam susceptible and resistant KPC-producing Enterobacterales: cross-resistance and synergistic effects. Eur J Clin Microbiol Infect Dis. 2022; 41(1):63-70. [CrossRef]
- Hobson CA, Cointe A, Jacquier H, Choudhury A, Magnan M, Courroux C, Tenaillon O, Bonacorsi S, Birgy A. Cross-resistance to cefiderocol and ceftazidime-avibactam in KPC β-lactamase mutants and the inoculum effect. Clin Microbiol Infect. 2021 Aug;27(8):1172.e7-1172.e10. [CrossRef]
- Poirel L, Sadek M, Kusaksizoglu A, Nordmann P. Co-resistance to ceftazidime-avibactam and cefiderocol in clinical isolates producing KPC variants. Eur J Clin Microbiol Infect Dis. 2022; 41:677-80. [CrossRef]
- Gaibani P, Amadesi S, Lazzarotto T, Ambretti S. Genome characterization of a Klebsiella pneumoniae co-producing OXA-181 and KPC-121 resistant to ceftazidime/avibactam, meropenem/vaborbactam, imipenem/relebactam and cefiderocol isolated from a critically ill patient. J Glob Antimicrob Resist. 2022; 30:262-4. [CrossRef]
- Di Pilato V, Codda G, Niccolai C, Willison E, Wong JLC, Coppo E, Frankel G, Marchese A, Rossolini GM. Functional features of KPC-109, a novel 270-loop KPC-3 mutant mediating resistance to avibactam-based β-lactamase inhibitor combinations and cefiderocol. Int J Antimicrob Agents. 2024; 63:107030. [CrossRef]
- Amadesi S, Bianco G, Secci B, Fasciana T, Boattini M, Costa C, Gaibani P. Complete Genome Sequence of a Klebsiella pneumoniae Strain Carrying Novel Variant blaKPC-203, Cross-Resistant to Ceftazidime/Avibactam and Cefiderocol, but Susceptible to Carbapenems, Isolated in Italy, 2023. Pathogens. 2024; 13:507. [CrossRef]
- Giufrè M, Errico G, Del Grosso M, Pagnotta M, Palazzotti B, Ballardini M, Pantosti A, Meledandri M, Monaco M. Detection of KPC-216, a Novel KPC-3 Variant, in a Clinical Isolate of Klebsiella pneumoniae ST101 Co-Resistant to Ceftazidime-Avibactam and Cefiderocol. Antibiotics (Basel). 2024; 13:507. [CrossRef]
- Jacob AS, Chong GL, Lagrou K, Depypere M, Desmet S. No in vitro activity of cefiderocol against OXA-427-producing Enterobacterales. J Antimicrob Chemother. 2021; 76:3317-8. [CrossRef]
- Shields RK, Iovleva A, Kline EG, Kawai A, McElheny CL, Doi Y. Clinical Evolution of AmpC-Mediated Ceftazidime-Avibactam and Cefiderocol Resistance in Enterobacter cloacae Complex Following Exposure to Cefepime. Clin Infect Dis. 2020; 71:2713-6. [CrossRef]
- Kawai A, Shropshire WC, Suzuki M, Borjan J, Aitken SL, Bachman WC, McElheny CL, Bhatti MM, Shields RK, Shelburne SA, Doi Y. Structural insights into the molecular mechanism of high-level ceftazidime-avibactam resistance conferred by CMY-185. mBio. 2024; 15:e0287423. [CrossRef]
- Amadesi S, Gatti M, Rinaldi M, Pea F, Viale P, Gaibani P. Novel CMY-186 variant conferring cross-resistance to cefiderocol and ceftazidime/avibactam in Klebsiella pneumoniae from a critically ill patient during cefiderocol and ceftazidime/avibactam treatment. Int J Antimicrob Agents. 2024; 63(4):107107. [CrossRef]
- Simner, P.J.; Beisken, S.; Bergman, Y.; E Posch, A.; E Cosgrove, S.; Tamma, P.D. Cefiderocol Activity Against Clinical Pseudomonas aeruginosa Isolates Exhibiting Ceftolozane-Tazobactam Resistance. Open Forum Infect. Dis. 2021, 8, ofab311.
- Ballesté-Delpierre, C.; Ramírez, Á.; Muñoz, L.; Longshaw, C.; Roca, I.; Vila, J. Assessment of In Vitro Cefiderocol Susceptibility and Comparators against an Epidemiologically Diverse Collection of Acinetobacter baumannii Clinical Isolates. Antibiotics 2022, 11, 187.
- Liu C, Yi J, Lu M, Yang P, Du C, Jiang F, Du P, Shen N. Dynamic within-host cefiderocol heteroresistance caused by blaSHV-12 amplification in pandrug-resistant and hypervirulent Klebsiella pneumoniae sequence type 11. Drug Resist Updat. 2024; 73:101038. [CrossRef]
- Nordmann, P.; Shields, R.K.; Doi, Y.; Takemura, M.; Echols, R.; Matsunaga, Y.; Yamano, Y. Mechanisms of Reduced Susceptibility to Cefiderocol Among Isolates from the CREDIBLE-CR and APEKS-NP Clinical Trials. Microb. Drug Resist. 2022, 28, 398–407.
- Rolston KVI, Gerges B, Shelburne S, Aitken SL, Raad I, Prince RA. Activity of Cefiderocol and Comparators against Isolates from Cancer Patients. Antimicrob Agents Chemother. 2020; 64:e01955-19. [CrossRef]
- Simner, P.J.; Beisken, S.; Bergman, Y.; Ante, M.; Posch, A.E.; Tamma, P.D. Defining Baseline Mechanisms of Cefiderocol Resistancein the Enterobacterales. Microb. Drug Resist. 2022, 28, 161–170.
- Ito, A.; Nishikawa, T.; Ishii, R.; Kuroiwa, M.; Ishioka, Y.; Kurihara, N.; Sakikawa, I.; Ota, T.; Rokushima, M.; Tsuji, M.; et al. 696. Mechanism of Cefiderocol high MIC mutants obtained in non-clinical FoR studies. Open Forum Infect. Dis. 2018, 5, S251.
- Magallon, A.; Amoureux, L.; Garrigos, T.; Sonois, M.; Varin, V.; Neuwirth, C.; Bador, J. Role of AxyABM overexpression in acquired resistance in Achromobacter xylosoxidans. J. Antimicrob. Chemother. 2022, 77, 926–929.
- Bilal M, El Tabei L, Büsker S, Krauss C, Fuhr U, Taubert M. Clinical Pharmacokinetics and Pharmacodynamics of Cefiderocol. Clin Pharmacokinet. 2021; 60(12):1495-1508. [CrossRef] [PubMed] [PubMed Central]
- Katsube T, Echols R, Wajima T. Pharmacokinetic and Pharmacodynamic Profiles of Cefiderocol, a Novel Siderophore Cephalosporin. Clin Infect Dis. 2019; 69(Suppl 7):S552-S558. [CrossRef] [PubMed] [PubMed Central]
- Chen IH, Kidd JM, Abdelraouf K, Nicolau DP. Comparative <i>In Vivo</i> Antibacterial Activity of Human-Simulated Exposures of Cefiderocol and Ceftazidime against <i>Stenotrophomonas maltophilia</i> in the Murine Thigh Model. Antimicrob Agents Chemother. 2019; 63(12):e01558-19. [CrossRef] [PubMed] [PubMed Central]
- Monogue ML, Tsuji M, Yamano Y, Echols R, Nicolau DP. Efficacy of Humanized Exposures of Cefiderocol (S-649266) against a Diverse Population of Gram-Negative Bacteria in a Murine Thigh Infection Model. Antimicrob Agents Chemother. 2017; 61(11):e01022-17. [CrossRef] [PubMed] [PubMed Central]
- Ghazi IM, Monogue ML, Tsuji M, Nicolau DP. Pharmacodynamics of cefiderocol, a novel siderophore cephalosporin, in a Pseudomonas aeruginosa neutropenic murine thigh model. Int J Antimicrob Agents. 2018; 51(2):206-212. [CrossRef] [PubMed]
- Stainton SM, Monogue ML, Tsuji M, Yamano Y, Echols R, Nicolau DP. Efficacy of Humanized Cefiderocol Exposures over 72 Hours against a Diverse Group of Gram-Negative Isolates in the Neutropenic Murine Thigh Infection Model. Antimicrob Agents Chemother. 2019; 63(2):e01040-18. [CrossRef] [PubMed] [PubMed Central]
- Nakamura R, Ito-Horiyama T, Takemura M, Toba S, Matsumoto S, Ikehara T, Tsuji M, Sato T, Yamano Y. <i>In Vivo</i> Pharmacodynamic Study of Cefiderocol, a Novel Parenteral Siderophore Cephalosporin, in Murine Thigh and Lung Infection Models. Antimicrob Agents Chemother. 2019; 63(9):e02031-18. [CrossRef] [PubMed] [PubMed Central]
- Sumi CD, Heffernan AJ, Lipman J, Roberts JA, Sime FB. What Antibiotic Exposures Are Required to Suppress the Emergence of Resistance for Gram-Negative Bacteria? A Systematic Review. Clin Pharmacokinet. 2019; 58(11):1407-1443. [CrossRef] [PubMed]
- Gatti M, Cojutti PG, Pea F. Impact of attaining aggressive vs. conservative PK/PD target on the clinical efficacy of beta-lactams for the treatment of Gram-negative infections in the critically ill patients: a systematic review and meta-analysis. Crit Care. 2024; 28(1):123. [CrossRef] [PubMed] [PubMed Central]
- Gatti M, Bartoletti M, Cojutti PG, Gaibani P, Conti M, Giannella M, Viale P, Pea F. A descriptive case series of pharmacokinetic/pharmacodynamic target attainment and microbiological outcome in critically ill patients with documented severe extensively drug-resistant Acinetobacter baumannii bloodstream infection and/or ventilator-associated pneumonia treated with cefiderocol. J Glob Antimicrob Resist. 2021; 27:294-298. [CrossRef] [PubMed]
- Mornese Pinna S, Corcione S, De Nicolò A, Montrucchio G, Scabini S, Vita D, De Benedetto I, Lupia T, Mula J, Di Perri G, D'Avolio A, De Rosa FG. Pharmacokinetic of Cefiderocol in Critically Ill Patients Receiving Renal Replacement Therapy: A Case Series. Antibiotics (Basel). 2022; 11(12):1830. [CrossRef] [PubMed] [PubMed Central]
- Gatti M, Giannella M, Rinaldi M, Gaibani P, Viale P, Pea F. Pharmacokinetic/Pharmacodynamic Analysis of Continuous-Infusion Fosfomycin in Combination with Extended-Infusion Cefiderocol or Continuous-Infusion Ceftazidime-Avibactam in a Case Series of Difficult-to-Treat Resistant <i>Pseudomonas aeruginosa</i> Bloodstream Infections and/or Hospital-Acquired Pneumonia. Antibiotics (Basel). 2022; 11(12):1739. [CrossRef] [PubMed] [PubMed Central]
- Gatti M, Rinaldi M, Tonetti T, Gaibani P, Siniscalchi A, Viale P, Pea F. Pharmacokinetics/pharmacodynamics of cefiderocol administered by continuous infusion in a case series of critically ill patients with carbapenem-resistant Acinetobacter baumannii infections undergoing continuous venovenous haemodiafiltration (CVVHDF). Int J Antimicrob Agents. 2023; 62(2):106852. [CrossRef] [PubMed]
- Pea F, Viale P. The antimicrobial therapy puzzle: could pharmacokinetic- pharmacodynamic relationships be helpful in addressing the issue of appropriate pneumonia treatment in critically ill patients? Clin Infect Dis. 2006; 42(12):1764-71. [CrossRef] [PubMed]
- Katsube T, Nicolau DP, Rodvold KA, Wunderink RG, Echols R, Matsunaga Y, Menon A, Portsmouth S, Wajima T. Intrapulmonary pharmacokinetic profile of cefiderocol in mechanically ventilated patients with pneumonia. J Antimicrob Chemother. 2021; 76(11):2902-2905. doi: 10.1093/jac/dkab280. Erratum in: J Antimicrob Chemother. 2021 ;76(11):3069. [CrossRef] [PubMed] [PubMed Central]
- Kawaguchi N, Katsube T, Echols R, Wajima T, Nicolau DP. Intrapulmonary Pharmacokinetic Modeling and Simulation of Cefiderocol, a Parenteral Siderophore Cephalosporin, in Patients With Pneumonia and Healthy Subjects. J Clin Pharmacol. 2022; 62(5):670-680. [CrossRef] [PubMed] [PubMed Central]
- From the American Association of Neurological Surgeons (AANS), American Society of Neuroradiology (ASNR), Cardiovascular and Interventional Radiology Society of Europe (CIRSE), Canadian Interventional Radiology Association (CIRA), Congress of Neurological Surgeons (CNS), European Society of Minimally Invasive Neurological Therapy (ESMINT), European Society of Neuroradiology (ESNR), European Stroke Organization (ESO), Society for Cardiovascular Angiography and Interventions (SCAI), Society of Interventional Radiology (SIR), Society of NeuroInterventional Surgery (SNIS), and World Stroke Organization (WSO); Sacks D, Baxter B, Campbell BCV, Carpenter JS, Cognard C, Dippel D, Eesa M, Fischer U, Hausegger K, Hirsch JA, Shazam Hussain M, Jansen O, Jayaraman MV, Khalessi AA, Kluck BW, Lavine S, Meyers PM, Ramee S, Rüfenacht DA, Schirmer CM, Vorwerk D. Multisociety Consensus Quality Improvement Revised Consensus Statement for Endovascular Therapy of Acute Ischemic Stroke. Int J Stroke. 2018; 13(6):612-632. [CrossRef] [PubMed]
- Möhlmann JE, van Luin M, Uijtendaal EV, Zahr N, Sikma MA. Continuous infusion of cefiderocol in a critically ill patient with continuous venovenous haemofiltration. Br J Clin Pharmacol. 2023; 89(12):3753-3757. [CrossRef] [PubMed]
- Gatti M, Pea F. Jumping into the future: overcoming pharmacokinetic/pharmacodynamic hurdles to optimize the treatment of severe difficult to treat-Gram-negative infections with novel beta-lactams. Expert Rev Anti Infect Ther. 2023; 21(2):149-166. [CrossRef] [PubMed]
- 117 Naseer S, Weinstein EA, Rubin DB, Suvarna K, Wei X, Higgins K, Goodwin A, Jang SH, Iarikov D, Farley J, Nambiar S. US Food and Drug Administration (FDA): Benefit-Risk Considerations for Cefiderocol (Fetroja®). Clin Infect Dis. 2021; 72(12):e1103-e1111. [CrossRef] [PubMed]
- Bassetti M, Echols R, Matsunaga Y et al. Efficacy and safety of cefiderocol or best available therapy for the treatment of serious infections caused by carbapenem-resistant Gram-negative bacteria (CREDIBLE-CR): a randomised, open-label, multicentre, pathogen focused, descriptive, phase 3 trial. Lancet Infect Dis 2021; 21: 226–40. [CrossRef]
- Portsmouth S., van Veenhuyzen D., Echols R., et al 2017. Cefiderocol compared with imipenem/cirastatin in the treatment of adults with complicated urinary tract infections with or without pyelonephritis or acute uncomplicated pyelonephritis: results from a multicenter, double-blind, randomized study, abstr OS0250D. Abstr 27th Eur Congr Clin Microbiol Infect Dis.
- EMA, 2020. Fetcroja. European Medicines Agency. URL https://www.ema.europa.eu/en/medicines/human/EPAR/fetcroja.
- World Health Organization Regional Office for Europe, European Centre for Disease Prevention and Control. 2022. Antimicrobial resistance surveillance Europe. https://www.ecdc.europa.eu/sites/default/files/documents/Joint-WHO-ECDC-AMR-report-2022.pdf.
- Satlin MJ, Simner PJ, Slover CM, et al Cefiderocol Treatment for Patients with Multidrug- and Carbapenem-Resistant Pseudomonas aeruginosa Infections in the Compassionate Use Program. Antimicrob Agents Chemother. 2023; 67(7):e0019423. [CrossRef] [PubMed]
- de la Fuente C, Rodríguez M, Merino N, et al. Real-life use of cefiderocol for salvage therapy of severe infections due to carbapenem-resistant Gram-negative bacteria, International Journal of Antimicrobial Agents, 2023; 62(1): 106818, ISSN 0924-8579. [CrossRef]
- Gavaghan V, Miller JL, Dela-Pena J. Case series of cefiderocol for salvage therapy in carbapenem-resistant Gram-negative infections. Infection. 2023; 51(2):475-482. [CrossRef] [PubMed] [PubMed Central]
- Vacheron, CH., Kaas, A., Rasigade, JP. et al. Correction: Cefiderocol in Difficult-to-Treat Nf-GNB in ICU Settings. Ann. Intensive Care 2024; 14, 81 . [CrossRef]
- Ramirez P et al. Real-world effectiveness and safety of cefiderocol in patients with Gram-negative bacterial infections in the early access programme in Spain: results of the PERSEUS study. Abstract. ECCMID 2024.
- Paez JG, Costa S. Risk factors associated with mortality of infections caused by Stenotrophomonas maltophilia: a systematic review. J Hosp Infect. 2008; 70(2):101–108. [CrossRef]
- Cai B, Nguyen ST, Copeland JD, Song HJ, Slover CM. 2751. Cefiderocol Use in Treating Patients with Confirmed Stenotrophomonas maltophilia Infections in US Hospitals During January 2020 - June 2022. Open Forum Infect Dis. 2023; 10(Suppl 2):ofad500.2362. [CrossRef]
- Timsit JF, Paul M, Shields RK, et al. Cefiderocol for the Treatment of Infections Due to Metallo-B-lactamase-Producing Pathogens in the CREDIBLE-CR and APEKS-NP Phase 3 Randomized Studies. Clin Infect Dis. 2022; 75(6):1081-1084. [CrossRef]
- Falcone M, Tiseo G. Cefiderocol for the Treatment of Metallo-β-Lactamases Producing Gram-Negative Bacilli: Lights and Shadows From the Literature. Clin Infect Dis. 2022; 75(6):1085-1087. [CrossRef]
- Isler, B., Vatansever, C., Özer, B., et al Higher rates of cefiderocol resistance among NDM producing Klebsiella bloodstream isolates applying EUCAST over CLSI breakpoints. Infectious Diseases, 2023; 55(9), 607–613. [CrossRef]
- Bavaro, D.F.; Belati, A.; Diella, L.; et al. Cefiderocol- Based Combination Therapy for “Difficult-to-Treat” Gram-Negative Severe Infections: Real-Life Case Series and Future Perspectives. Antibiotics 2021, 10, 652. [CrossRef]
- Marco Falcone, Giusy Tiseo, Manuela Nicastro, et al Cefiderocol as Rescue Therapy for Acinetobacter baumannii and Other Carbapenem-resistant Gram-negative Infections in Intensive Care Unit Patients, Clinical Infectious Diseases, 2021; 72(11): 2021–2024. [CrossRef]
- Bavaro, D.F., Papagni, R., Belati, A. et al. Cefiderocol Versus Colistin for the Treatment of Carbapenem-Resistant Acinetobacter baumannii Complex Bloodstream Infections: A Retrospective, Propensity-Score Adjusted, Monocentric Cohort Study. Infect Dis Ther 2023; 12, 2147–2163 . [CrossRef]
- Dalfino, L.; Stufano, M.; Bavaro, D.F.; et al. Effectiveness of First-Line Therapy with Old and Novel Antibiotics in Ventilator-Associated Pneumonia Caused by Carbapenem-Resistant Acinetobacter baumannii: A Real Life, Prospective, Observational, Single-Center Study. Antibiotics 2023, 12, 1048. [CrossRef]
- Emanuele Rando, Salvatore Lucio Cutuli, Flavio Sangiorgi, et al, Cefiderocol-containing regimens for the treatment of carbapenem-resistant A. baumannii ventilator-associated pneumonia: a propensity-weighted cohort study, JAC-Antimicrobial Resistance, 2023; 5(4) dlad085. [CrossRef]
- Russo A, Bruni A, Gullì S, Bet al. Efficacy of cefiderocol- vs colistin-containing regimen for treatment of bacteraemic ventilator-associated pneumonia caused by carbapenem-resistant Acinetobacter baumannii in patients with COVID-19. Int J Antimicrob Agents. 2023; 62(1):106825. [CrossRef]
- Oliva A, Liguori L, Covino S, et al. Clinical effectiveness of cefiderocol for the treatment of bloodstream infections due to carbapenem-resistant Acinetobacter baumannii during the COVID-19 era: a single center, observational study. Eur J Clin Microbiol Infect Dis. 2024; 43(6):1149-1160. [CrossRef]
- Renato Pascale, Zeno Pasquini, Michele Bartoletti, et al. Cefiderocol treatment for carbapenem-resistant Acinetobacter baumannii infection in the ICU during the COVID-19 pandemic: a multicentre cohort study, JAC-Antimicrobial Resistance, 2021; 3(4): dlab174. [CrossRef]
- Maddalena Giannella, Stefano Verardi, Andreas Karas, et al , Carbapenem-Resistant Acinetobacter spp Infection in Critically Ill Patients With Limited Treatment Options: A Descriptive Study of Cefiderocol Therapy During the COVID-19 Pandemic, Open Forum Infectious Diseases, 2023; 10(7): ofad329. [CrossRef]
- Pranita D. Tamma, Emily L. Heil, Julie Ann Justo et al Infectious Diseases Society of America Antimicrobial-Resistant Treatment Guidance: Gram-Negative Bacterial Infections. Infectious Diseases Society of America 2024; Version 4.0. Available at https://www.idsociety.org/practice-guideline/amr-guidance/].
- Marino, A.; Stracquadanio, S.; Campanella, E.; et al Intravenous Fosfomycin: A Potential Good Partner for Cefiderocol. Clinical Experience and Considerations. Antibiotics 2023, 12,49. [CrossRef]
- Paranos P, Vourli S, Pournaras S, Meletiadis J. Assessing Clinical Potential of Old Antibiotics against Severe Infections by Multi-Drug-Resistant Gram-Negative Bacteria Using In Silico Modelling. Pharmaceuticals (Basel). 2022; 15(12):1501. [CrossRef] [PubMed] [PubMed Central]
- Simner PJ, Beisken S, Bergman Y, Ante M, Posch AE, Tamma PD. Defining Baseline Mechanisms of Cefiderocol Resistance in the Enterobacterales. Microb Drug Resist. 2022; 28(2):161-170. [CrossRef] [PubMed] [PubMed Central]
- Mezcord, V.; Escalante, J.; Nishimura, B.; et al. Induced Heteroresistance inCarbapenem-Resistant Acinetobacter baumannii (CRAB) via Exposure to Human Pleural Fluid (HPF) and Its Impact on Cefiderocol Susceptibility. Int. J. Mol. Sci. 2023, 24, 11752. [CrossRef]
- Amadesi S, Amedeo A, Rinaldi M, Palombo M, Giannella M, Gaibani P. In vivo emergence of cefiderocol and ceftazidime/avibactam cross-resistance in KPC- producing Klebsiella pneumoniae following ceftazidime/avibactam -based therapies. Diagn Microbiol Infect Dis. 2024; 110(1):116372. [CrossRef]
- Bovo F, Amadesi S, Palombo M, Lazzarotto T, Ambretti S, Gaibani P. Clonal dissemination of Klebsiella pneumoniae resistant to cefiderocol, ceftazidime/avibactam, meropenem/vaborbactam and imipenem/relebactam co- producing KPC and OXA-181 carbapenemase. JAC Antimicrob Resist. 2023; 5(4):dlad099. [CrossRef]
- Lewis RE, Palombo M, Diani E, Secci B, Gibellini D, Gaibani P. Synergistic Activity of Cefiderocol in Combination with Avibactam, Sulbactam or Tazobactam against Carbapenem-Resistant Gram-Negative Bacteria. Cells. 2024; 13(16):1315. [CrossRef]
Figure 1.
Two-dimensional representation of cefiderocol. Structure activity relationship on Gram-negative bacteria highlighted by the violet dotted circles.
Figure 1.
Two-dimensional representation of cefiderocol. Structure activity relationship on Gram-negative bacteria highlighted by the violet dotted circles.
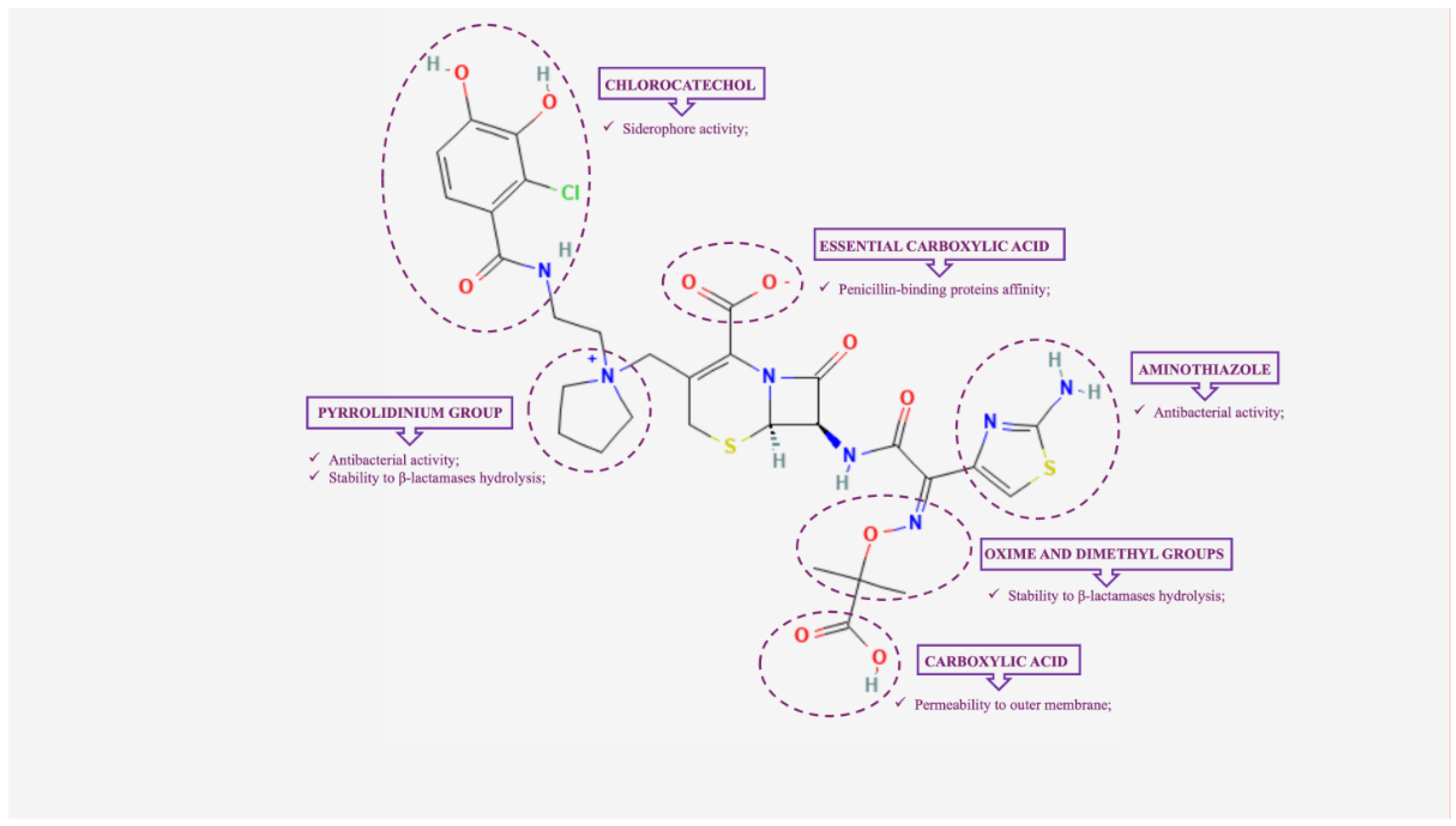
Figure 2.
Mechanisms of action of cefiderocol on Gram-negative bacteria. Cefiderocol enters bacteria by both passive and active transport via the bacteria's own TonB iron transport system.
Figure 2.
Mechanisms of action of cefiderocol on Gram-negative bacteria. Cefiderocol enters bacteria by both passive and active transport via the bacteria's own TonB iron transport system.


Table 1.
In vitro activity of cefiderocol against major Gram-negative bacilli collections according to EUCAST breakpoints.
Table 1.
In vitro activity of cefiderocol against major Gram-negative bacilli collections according to EUCAST breakpoints.
| Cefiderocol susceptibility % | Study remarks | Country | Reference | |||||||||||||
| Carbapenemase-producing strains | Carbapenem-non-susceptible strains | Overall | ||||||||||||||
| BURK | BURK | |||||||||||||||
| ACB | PA | EB | ACHR | ACB | PA | EB | ACHR | STEMA | ACB | PA | EB | |||||
| 55.3-59.1 | 77.1-98.2 | 61.2-75.1 | 86.8 | 96.5 | 87.6 | 99.6 | 91.2 | 98.6 | 97 | Meta-analysis | Worldwide | [3] | ||||
| 80.6 | 82.3 | K. pneumoniae | India | [4]* | ||||||||||||
| 100 | 98.4 | 100 | 99.5 | Spain, Portugal | [5]* | |||||||||||
| 93.3 | 97.9 | K. pneumoniae | UAE | [6]* | ||||||||||||
| 86-90 | 90.3 | 95.6 | K. pneumoniae | China | [7]* | |||||||||||
| 84 | 82 | Czech Republic | [8] | |||||||||||||
| 100 | 95.2 | 93.3 | India | [9]* | ||||||||||||
| 93.4 | 100 | 97.2 | India | [10]* | ||||||||||||
| 93.8 | USA | [11]* | ||||||||||||||
| 93.3 | 95.6 | USA | [12]* | |||||||||||||
| 63 | 80.7 | CFP | USA | [13]* | ||||||||||||
| 69-100 | 95 | Worldwide | [14] | |||||||||||||
| 85 | 97.8 | 92.4 | 98.9 | Europe | [15] | |||||||||||
| 70.6 | 91.5 | CFP | Spain | [16] | ||||||||||||
| 95.8 | Italy | [17] | ||||||||||||||
| 100 | 100 | 97.9 | 94.4 | Taiwan | [18]* | |||||||||||
| 70.7 | 87.8 | 86.2 | CFP | UK | [19] | |||||||||||
| 83.4-87.5 | 97.2 | 96 | 100 | Italy | [20] | |||||||||||
| 95.1 | Mexico | [21]* | ||||||||||||||
| 92.9 | 88.5 | 94.8 | 96.7 | Worldwide | [22] | |||||||||||
| 96.3 | 99.1 | CFP | France, Denmark | [23] | ||||||||||||
| 100 | India | [24]* | ||||||||||||||
| 79.5 | MBL | Switzerland | [25] | |||||||||||||
| 59.6 | Turkey | [26] | ||||||||||||||
| 97.9 | 96.9 | USA | [27]* | |||||||||||||
| 91.2 | 100 | 83.3-100 | Japan | [28]* | ||||||||||||
| 92.2 | E. coli | Spain | [29] | |||||||||||||
Grey shading indicates cefiderocol activity <90%. * According CLSI clinical breakpoints. Abbreviations: EB: Enterobacterales; PA: Pseudomonas aeruginosa; ACB: Acinetobacter baumannii complex; STEMA: Stenotrophomonas maltophilia; ACHR: Achromobacter species; BURK: Burkholderia species; MBL: metallo-β-lactamase; Cystic fibrosis patients, CFP.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



