
Submitted:
19 September 2024
Posted:
23 September 2024
You are already at the latest version
Abstract
Micro-invasive therapeutic approaches in endodontics differentiate between different modified types of access cavities: occlusal via a smaller occlusal opening (15 ° access angle), medial (via the caries defect) for premolars and molars (30 ° access angle) and cervical with wedge-shaped defects or root caries on anterior teeth and single-rooted premolars (45 ° access angle). Therefore, the aim of this work was (i) to create an in-vitro model for the clinical simulation of these three different modified access types, (ii) to assess the biomechanics of the instrumentation and (iii) to measure the volumetric substance loss of four different preparation systems. Material and Method: Simulated S-shaped root canals with a high degree of obliteration (ISO 10) in acrylic polymer bodies with canal entrance angles of 15 °, 30 ° and 45 ° were shaped with NaOCl (3%) irrigation under clinical simulation at body temperature (37 ° C) in randomized blinded sequences (n = 7) according to manufacturer's instructions: 1. Conventional geometry, not heat treated, up to 35 / .04 (F360, Komet) 2. Conventional geometry, heat-treated, spark-eroded up to 40 / .04 (Hyflex EDM, Coltene Hyflex) 3. Spiral geometry, heat treated, up to 36 / .03 (TruNatomy, DentsplySirona) 4. Distinctive spiral geometry, heat-treated (XP-Endo Shaper, FKG) The vectorization (AutoCAD) of the root canals was performed before and after preparation in the apical, middle and coronal third of the root canal. The volumetric loss of substance in cubic millimeters was recorded and statistically evaluated using an independent two-sided t-test. Clinical demonstrations include three cases of micro-invasive access cavities as final proof of principle of fast and safe root canal treatment. Results The total loss of volume at 15 ° entry angles is significantly lowest with TruNatomy and XP Endo. With an access angle of 30 °, the total loss remains low and increases with F360 and Hyflex .. At a 45 ° access angle, the group differences remain: TruNatomy (6.5 mm3) and XP Endo (6.4 mm3) versus F360 (8.3 mm3) and Hyflex (8.4 mm3). This difference in loss of simulated root dentin is highly significant. Conclusions Conventional instruments achieve optimal shape of apical third of root canals at all entrance angles only with higher substance loss in coronal and middle thirds . In contrast, the spiral instrument geometry contributes to dentin protection and supports the concept of minimally invasive endodontics for lifelong tooth preservation as shown in four clinical cases.
Keywords:
Endodontic instrumentation
; Review
; Angulated access
; Minimally invasive endodontics
; Root canal shaping
; Volume loss
; Clinical consequences
1. Introduction
Any permanent dentition in mammalian animals, including humans, lasts forever in the sense that there is no way to replace permanent teeth. Therefore, the great pioneers of research-oriented dental medicine in the 19th century, W. D. Miller, A. Witzel and G.V. Black were well aware of minimally invasive dental treatments using mainly hand instruments, later foot-driven drills and for centuries the biomaterials for caries treatment silver amalgam, gold foil or gold alloys.
Black`s most famous sentence that a filling, “if it is made well and of material that is durable in the mouth, as gold or amalgam, is invulnerable; it should last a lifetime.” This is still valid, and new adaptable biomaterials could be added, such as composite formulations, hybrid ceramics and newer gold alloys. Unfortunately, this path was lost with the triumphal procession of power drills in the early 20th century culminating in electric turbines destroying any hard tissue in their way by giving up manual sensitivity and most experienced haptic feeling of the dental operator. For nearly one century, the death blow to minimally invasive dental treatment, overusing surgical intervention, misunderstanding Black’s “Extension for prevention” and preparing giant cavities without any use of operating microscopes or even dental loupes.
Therefore, the contemporary trend to microinvasive dentistry and especially endodontics is not at all new; it is just the way back to the roots. It is not aimed at fracture resistance, at less crown or root dentin loss, because in the short-term investigations results remain heterogeneous, with more evidence for no significant increase of fracture resistance (Silva et al. 2020, Rover 2020, Sabeti 2018, Plotino et al. 2017).
The main aim of microinvasive endodontics is indeed to keep as much nonreplaceable dental hard tissues alive or at least in function for many decades. This takes into account the first, second, third, etc. replacement filling and the first, second and eventually third root canal retreatment.
Minimally invasive endodontics will change conventional root canal treatment in adolescents, adults and, especially, in seniors. “Don´t touch too much of sound dentin” means keeping in young teeth most of the coronal and root dentin with tubules and optimal infraction resistance. This means that in old teeth, to keep as much sclerotic coronal and root dentin as possible, infraction and fracture are prone to stabilize the whole tooth as well as all single roots as the most important prerequisites for future secondary and tertiary revisions.
In conventional endodontics, straight line access to the middle third of the root canal is recommended. This often leads to a large loss of hard tissue when preparing the access cavity and straightening the root canal entrance.
In contrast, microinvasive therapeutic approaches differentiate between three modified types of access: occlusal via a smaller opening (15° entrance angle), mesial/distal (via the cavitated caries defect) for premolars and molars (30° entrance angle) and cervical with wedge-shaped defects or root caries on anterior teeth and single-rooted premolars (45° access angle). Therefore, the aim of this work was (i) to create an in vitro model for the clinical simulation of these three different modified access types (Figure 2), (ii) to investigate the biomechanics within the framework of the instrumentation and (iii) to assess the volumetric loss of substance between four different preparation systems.
Recent concepts for endondontic access cavities aim to preserve dental hard tissues while sacrificing the so-called advantages of straight-line access. They range from conservative access cavities to ultraconservative access cavities, which can be divided into micro access and computer-assisted access cavities (Shabbir et al. 2021).
As a result of these microinvasive cavities, the risk for iatrogenic complications such as apical transportation (Alovisi et al. 2017), deviations and instrument fractures (Pedulla et al. 2020, Gluskin et al. 2014) may increase because of non-adequate instrumentation and instrument geometry or missing magnification. Additionally, shortcomings in cleaning the root canal system have been reported (Rover et al. 2017, Silva et al. 2019).
Technological improvements in endodontics, such as better visibility through magnification with dental operating microscopes (Perrin et al. 2013), the increasing preoperative information due to the use of cone-beam computed tomographic imaging (Manigangdan et al. 2020), the availability of various irrigate agitation methods (Azim et al. 2016) and more flexible nickel-titanium instruments with new geometries (Elnaghy et al. 2020), may improve sufficient cleaning and shaping of all anatomical structures of root canal systems.
Instrument systems with off-centered geometry can enhance the preservation of the original anatomical structure of the endodontium with primary and secondary dentin in contrast to instruments with conventional geometry (Kabil et al. 2021, Perez Morales et al. 2020, Oliveira et al. 2019, Bortoluzzi et al. 2015).
However, there are no data available about the effect of different instrument geometries on shaping root canals via defined angles of access cavities.
Therefore, the aim of the present study was to evaluate the performance of four different nickel-titanium preparation systems concerning volumetric substance loss in the coronal, middle and apical third after shaping at three different entrance angles (15°, 30° and 45°) in S-shaped canals. A highly standardized tooth model was selected to perform the clinically simulated treatment in an artificial oral cavity under blinded conditions and body temperature.
For the first time in dental history, endodontics may contribute to the goal of keeping teeth for a lifetime. Therefore, substantial research is needed.
2. Materials and Methods
A new study approach using artificial oral cavity AOC simulating endodontic treatment conditions, including blinded operation, body temperature, file revolutions and forces, video documentation and assessment of dentin loss, was established (Figure 1).
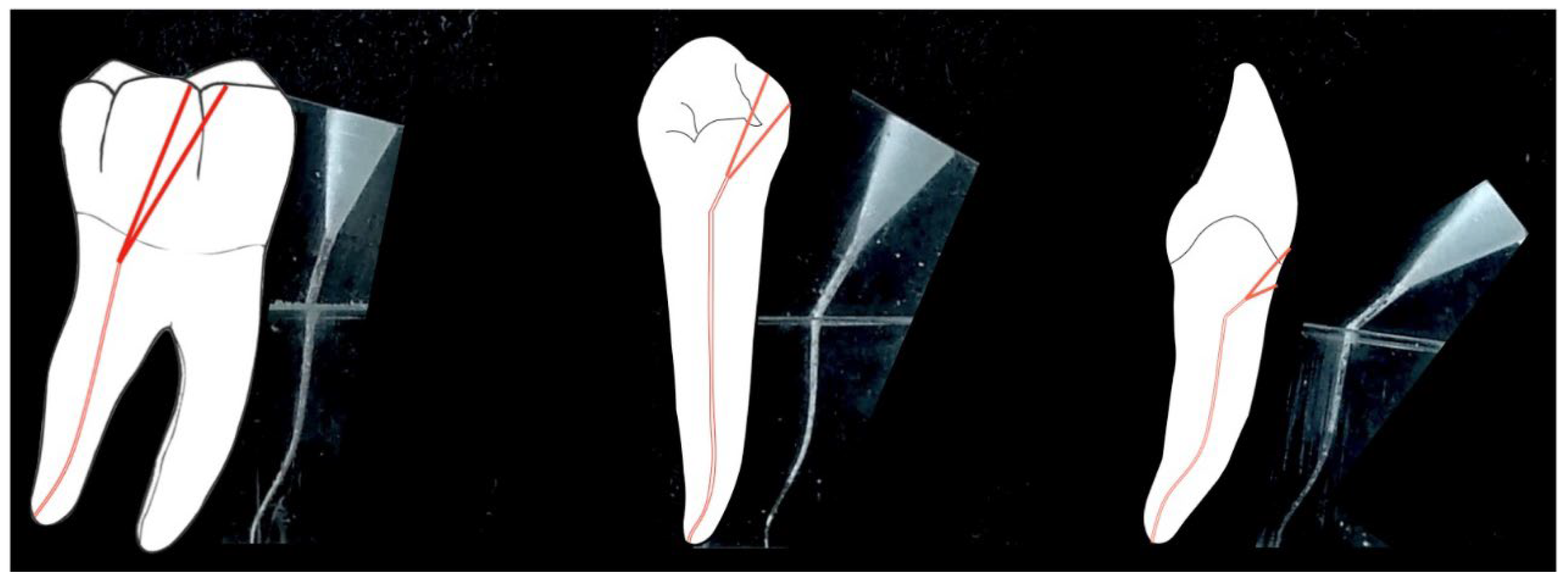
Simulated S-shaped root canals with a high degree of obliteration in acrylic polymer bodies with canal access angles of 15°, 30° and 45° (Figure 2) were randomized and blinded instrumented.
Figure 2.
Clinically simulated root canals and canal access angles of 15°, 30° and 45°.
After manual glide path preparation with Hedstrom files (ISO 15) to working length, the wet shaping of the root canal system with NaOCl (3%) under clinical simulation at body temperature (37 °C) was executed by a single well trained endodontist (V. N.) in a randomized sequence (n = 7) according to the manufacturer`s instructions.
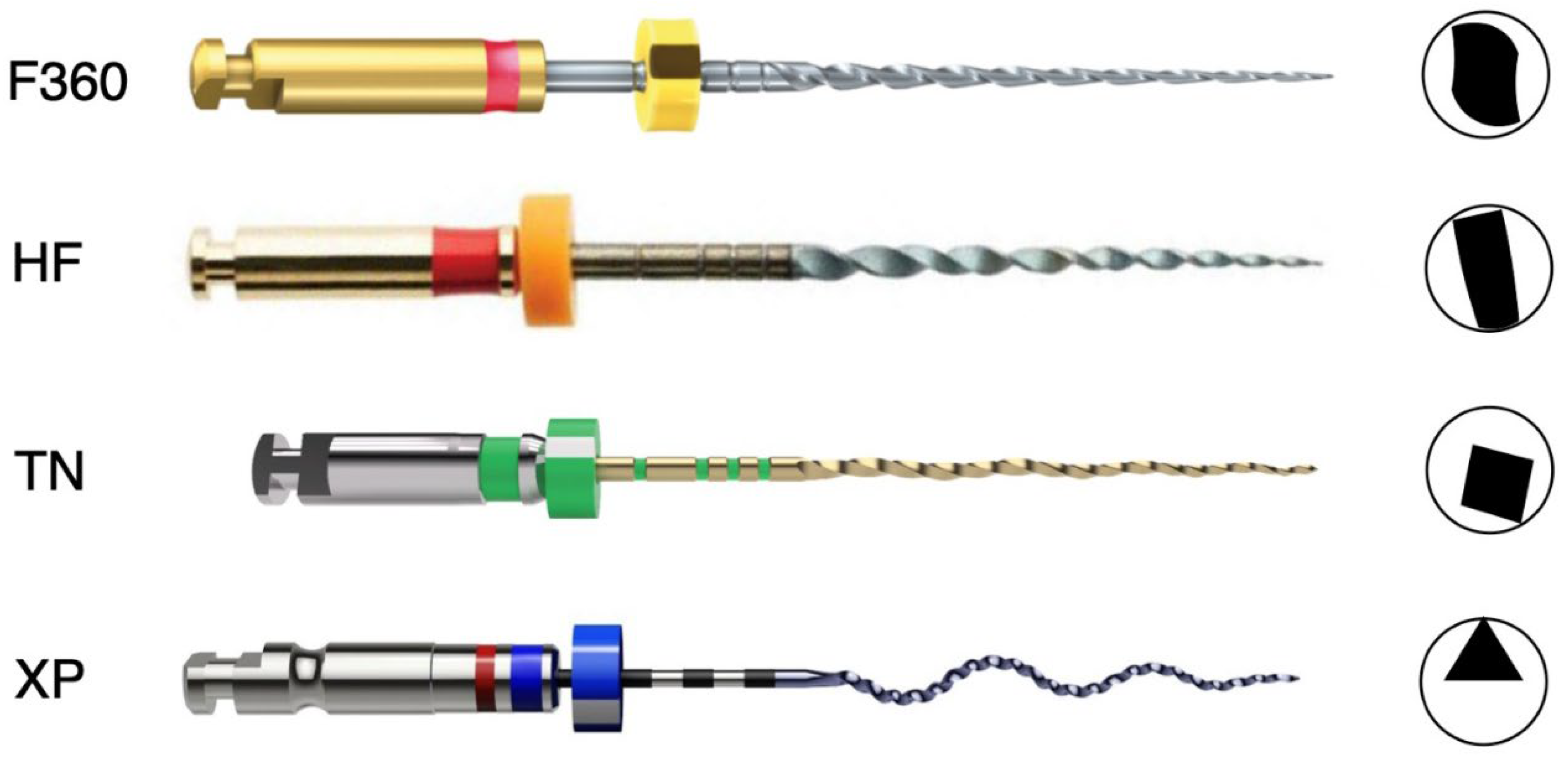
The file systems were selected according to the following criteria (Figure 3):
- (1)
- Conventional cutting geometry, not heat treated, shaping up to 35/.04 (F360, Gebr. Brasseler GmbH & Co. KG, Lemgo, Germany) F360
- (2)
- Conventional cutting geometry, heat-treated, spark-eroded surface, shaping up to 40/.04 (Hyflex EDM, Coltène/Whaledent GmbH + Co. KG, Langenau, Germany) HF
- (3)
- Off-centered geometry, heat treated, shaping up to 36/.03 (TruNatomy, DentsplySirona, Charlotte, USA) TN
- (4)
- Off-centered geometry, heat-treated, shaping up to 30/.04 (XP-Endo Shaper, FKG Dentaire Sàrl, Le Crêt-du-Locle, Switzerland) XP
All simulated S-shaped root canals were photo documented before and after the shaping procedure and vectorized by Auto CAD (Autodesk, San Rafael, USA)
Figure 3.
Investigated instruments with the corresponding cross-sections.
in the apical, middle and coronal third of the root canal. The volumetric loss of dentin in cubic millimeters was recorded and statistically evaluated with an independent two-sided t test.
2.1. Shaping Procedure
Each preparation system was used with full clockwise rotation movement with the endodontic motor X-Smart (DentsplySirona, Charlotte, USA). The artificial pulp chamber was filled with 3% NaOCl throughout the wet instrumentation. Irrigation (3% NaOCl) and recapitulation with a size 10 C-Pilot File (VDW GmbH, Munich, Germany) were performed with standard syringes (Sterican G27 0,4x25 mm, B. Braun SE, Melsungen, Germany) after each canal enlargement step.
2.2. F360 (Komet, Lemgo, Germany)
According to the manufacturer`s instructions, glidepath was performed using Pathglider ISO 15/0.03 (Komet) with the recommended engine settings (300 rpm, 0.5 Ncm), followed by the shaping files ISO 25/0.04, ISO 35/0.04 at 500 rpm and 1.8 Ncm. The instruments were cleaned after every 3 pecking motions until the working length was reached.
2.3. HyFlex EDM (Coltène/Whaledent, Langenau, Germany)
Manual glidepath was prepared with Hyflex EDM Glidepath File ISO 10/0.04 at 300 rpm and 1.8 Ncm), followed by Hyflex EDM One file ISO 25/0.08 and Hyflex ISO 40/0.04. These files were used with the tactile controlled activation technique. The instrument was passively inserted into the canal until maximum frictional resistance was reached. After activation of the motor, the file was gently pushed apically until no further advancement and then removed from the canal. Cleaning of the instrument and irrigation and recapitulation were performed after each stroke until the working length was reached
2.4. TruNatomy (DentsplySirona, York, Pennsylvania, USA)
All instruments were used with 500 rpm and 1.5 Ncm engine settings. The first instrument was the Glider file ISO 17/0.02, moved gently apically 2-3 times with a 2-5 mm amplitude and then removed from the canal. Irrigation and recapitulation were performed before the next instrumentation step. After the Glider file, Prime file ISO 26/0.04 was used in the same way as Glider. If there was no easy apical advancement of the Prime file, after irrigation and recapitulation, the Small file ISO 20/0.04 was used until working length was reached. The shaping procedure was finished after the Prime file and the Medium file ISO 36/0.03 reached the working length.
2.5. XP-Endo Shaper (FKG, La Chaux-de-Fonds, Switzerland)
The XP- Shaper file ISO 15/.01 was used at 800 rpm and 1.0 Ncm engine settings. Gentle apical movements in 5 strokes were performed until working length was reached. Next, 15 gentle apical movements to working length were repeated for the final shape, which should be approximately size 0.30 mm at the tip with taper 0.04 according to the manufacturer`s instructions.
The vectorization of the root canal was assessed before and after preparation using high-resolution macrophotography in the apical, middle and coronal third of the root canal using AutoCAD Software (Autodesk, San Rafael, USA, Figure 2). The volumetric loss of root dentin after shaping procedures in cubic millimeters was recorded for each region.
2.6. Statistical Rationale
The Kolmogorov–Smirnov test (KS test; one sample test) was applied to test the 4 parameters of effectiveness – ‚coronal volume loss‘, ‚middle volume loss‘, ‚apical volume loss‘, and ‚total volume loss‘ – for a normal distribution of loss values. A significance level of α = 0.10 (10%) was used to test this important assumption of arithmetic mean calculation and parametric t-test. As a result, the null hypothesis (H0) of normality was clearly accepted. not rejected for all parameters (exact p values were calculated).
The consequence is that all parameters were analyzed by an in-dependent two-sample t test to assess whether the means of the 4 tested files were significantly different. Application of the t-test was combined with the Levene test. It tests – prior to the t-test – the H0 that the variances of the tested groups or files are equal (homogeneity of variance).
The statistical analyses of different dentin loss values between files kept the basic α-level of p ≤ 0.05 (5%). However, significance values at higher levels (p ≤ 1% and p ≤ 1‰) were also documented.
3. Results
All tested instruments reached the treatment goal of optimal shaping of the apical third with nearly identical volume loss in this region. Instruments F360 and Hyflex reached that goal only with a higher coronal and middle canal third volume loss due to straightening the canal after angulated access with 45°. In contrast, the off-centered geometry of XP-Endo Shaper and TruNatomy exhibits a lower volume loss in the coronal and middle third in the simulated root canals.
The total hard tissue volume loss at 15° entry angles was significantly lowest in the TN and XP Endo groups. With an increased access angle to 30°, the total volume loss remained low in the TN (7.0 mm3) and XP Endo (5.9 mm3) groups but increased in the F360 (9.0 mm3) and Hyflex (7.7 mm3) groups. At a 45° access angle, the following group differences remained: TN (6.5 mm3) and XP Endo (6.4 mm3) on the one hand and F360 (8.3 mm3) and Hyflex (8.4 mm3) on the other hand (Figure 4).
At 45° access angles, the total volume loss between conventional instruments (F360 and HF) was statistically highly significant (p=<0.001) compared to instruments with off-centered geometry (TN and XP) (Table 1). Apical volume loss produced by TN was insignificantly different compared to HF and F360 (Table 1).
4. Discussion
Despite the heterogeneous results (Silva et al. 2020, Rover 2020, Sabeti 2018, Plotino et al. 2017) regarding the effects of minimally invasive access cavities on fracture resistance, the preservation of enamel, crown and root dentin with mostly tubular dentin in juvenile teeth and with many occluded tubules next to carious dentin or sclerotic dentin in senium teeth while performing sufficient shaping and cleaning of the root canal system has undeniable benefits in keeping the tooth in function and for future treatments. Chronic tooth trauma is rather rare in adolescents and young adults; however, it is very common in elderly subjects. Enamel-dentin crown infractions causing dentin crack syndrome ultimately end up in endodontic treatment. Pulp degeneration takes years and decades, and after the loss of primary odontoblasts, only secondary odontoblasts are able to build-up irritation dentin prone to infractions and less prevent the bacterial infection of the partly or total pulp necrosis (Gaengler et al. 2010). Therefore, endodontic treatment has to take into account the completely different structures of young and old dentin, of carious versus noncarious dentin, and, finally, of neural crest-derived odontoblasts secreting secondary dentin versus cellular connective tissue-derived odontoblasts secreting irritation dentin.
Recent studies of microinvasive endodontics have mostly used extracted human teeth in combination with micro-CT evaluation. This is a precise method for the analysis of quantitative and qualitative aspects of root canal instrumentation. The use of extracted teeth has disadvantages concerning the comparability and reproducibility of the entrance angle and the anatomy of the root canal. Micro-CT-based anatomical matching can improve the comparability of selected specimens but still has limitations (De-Deus et al. 2020, Silva et al. 2020). Recent studies, which use mostly mandibular incisors and maxillary premolars with no or less canal curvature, show no significant differences in volumetric loss or percentage of canal wall preparation (Rover 2020, Miranda 2021). Kabil et al. 2021 showed in a micro-CT-based study with mesio-buccal canals in maxillary molars with varying root canal curvatures between 25° and 40° that shaping the root canal with conventional instruments results in significantly more canal transportation in the middle third of the root canal than shaping with off-centered instruments. To overcome the limitation of anatomic variations, the present study evaluated the performance of different instruments on standardized acrylic polymer blocks with defined entrance angles influencing the volumetric loss of simulated dentin in the coronal, middle and apical third of root canals under simulated clinical conditions in an artificial oral cavity at body temperature. The 15° entrance angle simulated occlusal access through a microinvasive occlusal cavity, the 30° entrance angle simulated access via a anterior or posterior cavitated caries lesion , and the 45° entrance angle simulated access through a cervical wedge-shaped defect. All canals with different entrance angles ended up in an S-shaped canal. With these defined, reproducible different root canal settings from light to heavy canal curvature, the effect of the various instrument designs on saving hard tissue depending on the angle of entrance could be better demonstrated with reduced risk of bias. Moreover, the specimens were randomized and blinded to the operator. The highly standardized artificial oral cavity with root dentin simulation allows reproducible outcomes in line with the statistical methodology and, therefore, transferable to clinical conditions and stimulates future biomechanical research and the development of new instruments. We think it contributes to the ongoing discussion of critically reviewing experimental models for studies on human root canal preparation (Huelsmann, 2021).
All NiTi alloys have a unique transformation temperature curve. During the last decade, heat treatment of endodontic instruments became popular to change the stiffness as well as the superelasticity of the instruments, which can negatively influence the torsional resistance as well as the resistance to cyclic fatigue. This heat treatment typically alters the alloy transformation curve. Cardoso et al. (2019) found a negative impact on cyclic fatigue resistance when increasing the temperature from 20 °C to 37 °C in both heat-treated and nonheat-treated instruments. Therefore, the AOC was designed to replicate human body test conditions at 37 °C to address this factor of temperature variability.
Finally, the standardized polymer test blocks simulated the caries-free root dentin of 35- to 54-year-old subjects in wet instrumentation. This means that biomechanical shaping takes place in primary dentin with slightly obliterated tubules, which are not prone to infractions and dentin crack syndrome. The methodological approach represents the typical clinical situation of first-time root canal treatment caused by crown caries progression or acute trauma as an example of minimally invasive endodontics. Future research could focus on the standardized simulation of old sclerotic root dentin with much less open tubules, mostly irritation dentin of secondary odontoblast origin and caused by mainly progressing marginal periodontitis and sometimes by root caries. Because of the expected different biomechanics and shaping behavior, future file development could result in file geometries, flexibility and shaping efficacy for adult endodontics in our case and different senior endodontics for elderly patients with root sclerosis.
The off-centered geometry of TruNatomy files in which the center of mass of the instrument is not aligned with the center of rotation could contribute to a more predictable cone-fit compared to the more extensive off-centered geometry of XP-Endo-Shaper were the final shape could be dependent on the rotation time for full working length. This important clinical aspects should be investigated in future studies.
In conclusion, the shaping of the root canal with off-centered instruments preserves significantly more substances in the coronal and middle third of the root canal than conventionally shaped instruments. This biomechanical revolution in the root canal treatment strategy means that minimally invasive endodontics could go from instrument-oriented biomechanics to tooth-oriented biomechanics. This also means, as part of the discussion, that the endodontic diagnosis should consider not only clinical signs and symptoms as well as the 3D structure of the root canal system but also the quality of primary, secondary and irritation dentin, the individual history of caries lesion progression, the severity of trauma and marginal periodontitis and, finally, the systemic and local host responses to endodontal and periodontal inflammation progression.
It could also be speculated that minimally invasive endodontics are a pacesetter for future personalized dental medicine.
5. Clinical Consequences
All four cases (Figure 5, Figure 6, Figure 7 and Figure 8) demonstrate clearly, that clinical endodontics contribute in general practices as well as in specialized departments to root and crown dentin conservation not because of increasing fracture resistance, what is not very well documented, but to minimizing hard tissue loss because of the minimal invasive instrumentation. This is the most important prerequisite for a second or even third endodontic retreatment caused by progressing apical periodontitis or cyst.
Therefore, the minimal invasive dentistry may result in keeping the human dentition as long as possible and as much teeth as possible in good function. So, the old dream to keep the own natural teeth for lifelong functional action and cosmetic appearance may come through.
Author Contributions
Conceptualization: PG, TL: methodology: TL, AD, IS; performance simulated clinical instrumentation: VN; statistics: KW; clinical endodontic treatment: TL; writing original draft: PG, TL; reviewing draft: PG, TL, VN. All authors have read and agreed to the published version of the manuscript.
Funding
Dentsply Sirona.
Institutional Review Board Statement
Not applicable. The clinical treatment of cases presented here was not study/Review based.
Informed Consent Statement
The four patients gave written informed consent to present the routine clinical outcome in the Review.
Data Availability Statement
Data are available on www.ormed.net.
Conflicts of Interest
The authors declare that there is no conflict of interest.
References
- Alovisi M, Pasqualini D, Musso E, Bobbio E, Giuliano C, Mancino D, Scotti N, Berutti E(2017) Influence of Contracted Endodontic Access on Root Canal Geometry: An in Vitro Study. Journal of Endodontics 44(4), 614-620.
- Azim AA, Aksel H, Zhuang T, Mashtare T, Babu JP, Huang GT (2016) Efficacy of 4 Irrigation Protocols in Killing Bacteria Colonized in Dentinal Tubules Examined by a Novel Confocal Laser Scanning Microscope Analysis. Journal of Endodontics 42(6), 928-34.
- Black G V (1908) A work on operative dentistry in two volumes. Volume 1: the pathology of the hard tissues of the teeth. Chicago (IL): MedicDental Publishing Company.
- Cardoso RM, Alves NCC, de Menezes SE, Batista SM, Vieira TM, Rocha GV, Monteiro GQ, Albuquerque DS (2019) Influence of Temperature on the Cyclic Fatigue of Nickel-Titanium Instruments with Different Heat Treatments on Severely Curved Canals. The Journal of Contemporary Dental Practice, Vol 20, 6.
- De-Deus G, Simões-Carvalho M, Belladonna FG, Versiani MA, Silva EJNL, Cavalcante M, Souza EM, Johnsen GF Haugen HJ, Paciornik S (2020) Creation of well-balanced experimental groups for comparative endodontic laboratory studies: a new proposal based on micro-CT and in silico methods. International Endodontic Journal 53(7), 974-985.
- Elnaghy AM, Elsaka SE, Mandorah AO (2020) In vitro comparison of cyclic fatigue resistance of TruNatomy in single and double curvature canals compared with different nickel-titanium rotary instruments. BMC Oral Health 4, 20(1):38.
- Gluskin AH, Peters CI, Peters OA (2014) Minimally invasive endodontics: challenging prevailing paradigms. British Dental Journal 216(6), 347-53.
- 8. Gaengler P, Hoffmann T, Willershausen B, Schwenzer N, Ehrenfeld N (2010) Konservierende Zahnheilkunde und Parodontologie. [CrossRef]
- Hülsmann M (2021) A critical appraisal of research methods and experimental models for studies on root canal preparation. International Endodontic Journal. Epub ahead of print. [CrossRef]
- Kabil E, Katić M, Anić I, Bago I (2021) Microcomputed Evaluation of Canal Transportation and Centering Ability of 5 Rotary and Reciprocating Systems with Different Metallurgical Properties and Surface Treatments in Curved Root Canals (2021) Journal of Endodontics 47(3), 477-484.
- Manigandan K, Ravishankar P, Sridevi K, Keerthi V, Prashanth P, Pradeep Kumar AR (2020) Impact of dental operating microscope, selective dentin removal and cone beam computed tomography on detection of second mesiobuccal canal in maxillary molars: A clinical study. Indian Journal of Dental Research 31(4), 526-530.
- Miller WD (1898) Lehrbuch der Conservierenden Zahnheilkunde. Zweite umgearbeitete und erweiterte Auflage. Georg Thieme, Leipzig.
- Nagendrababu V, Murray PE, Ordinola-Zapata R, Peters OA, Rôças IN, Siqueira JF Jr, Priya E, Jayaraman J, Pulikkotil S, Camilleri J, Boutsioukis C, Rossi-Fedele G, Dummer PMH (2021) PRILE 2021 guidelines for reporting laboratory studies in Endodontology: A consensus-based development. International Endodontic Journal 54(9), 1482-1490.
- Oliveira DJF, Leoni GB, Goulart RS (2019) Changes in geometry and transportation of root canals with severe curvature prepared by different heat-treated nickel-titanium instruments: a microcomputed tomographic study. Journal of Endodontics 45, 768–73.
- Pedullà E, La Rosa GRM, Virgillito C, Rapisarda E, Kim HC, Generali L (2020) Cyclic Fatigue Resistance of Nickel-titanium Rotary Instruments according to the Angle of File Access and Radius of Root Canal. Journal of Endodontics 46(3), 431-436.
- Perez Morales MLN, González Sánchez JA, Olivieri Fernández JG, Laperre K, Abella Sans F, Jaramillo DE, Terol FD (2020) TRUShape Versus XP-endo Shaper: A Microcomputed Tomographic Assessment and Comparative Study of the Shaping Ability-An In Vitro Study. Journal of Endodontics 46(2), 271-276.
- Perrin P, Neuhaus KW, Lussi A (2014) The impact of loupes and microscopes on vision in endodontics. International Endodontic Journal 47(5), 425-9.
- Plotino G, Grande NM, Isufi A et al. (2017) Fracture strength of endodontically treated teeth with different access cavity designs. Journal of Endodontics 43, 995–1000.
- Dos Santos Miranda ARL, de Moura JDM, Calefi PHS, Amoroso Silva PA, Marceliano Alves MFV, Lopes RT, Vivan RR, Rodrigues PA (2021) Influence of conservative endodontic access cavities on instrumentation of oval-shaped straight root canals. International Endodontic Journal. 2021 Sep 24. Epub ahead of print. [CrossRef]
- Rover G, Belladonna FG, Bortoluzzi EA, De-Deus G, Silva EJNL, Teixeira CS (2017) Influence of Access Cavity Design on Root Canal Detection, Instrumentation Efficacy, and Fracture Resistance Assessed in Maxillary Molars. Journal of Endodontics 43(10), 1657-1662.
- Rover G, de Lima CO, Belladonna FG, Garcia LFR, Bortoluzzi EA, Silva EJNL, Teixeira CS (2020) Influence of Minimally invasive endodontic access cavities on root canal shaping and filling ability, pulp chamber cleaning and fracture resistance of extracted human mandibular incisors. International Endodontic Journal 53(11), 1530-1539.
- Saber SM, Hayaty DM, Nawar NN, Kim HC (2020) The Effect of Access Cavity Designs and Sizes of Root Canal Preparations on the Biomechanical Behavior of an Endodontically Treated Mandibular First Molar: A Finite Element Analysis. Journal of Endododontics 5, 0099-2399(20)30451-9.
- Sabeti M, Kazem M, Dianat O et al. (2018) Impact of access cavity design and root canal taper on fracture resistance of endodontically treated teeth: an ex vivo investigation. Journal of Endodontics 44, 1402–6.
- Shabbir J, Zehra T, Najmi N, Hasan A, Naz M, Piasecki L, Azim AA (2021) Access Cavity Preparations: Classification and Literature Review of Traditional and Minimally Invasive Endodontic Access Cavity Designs. Journal of Endodontics 47(8), 1229-1244.
- Silva AA, Belladonna FG, Rover G, Lopes RT, Moreira EJL, De-Deus G, Silva EJNL. (2020) Does ultraconservative access affect the efficacy of root canal treatment and the fracture resistance of two-rooted maxillary premolars. International Endodontic Journal 53(2), 265-275.
- Witzel A (1879) Die Antiseptische Behandlung von Pulpakrankheiten des Zahnes mit Beiträgen zur Lehre von den Neubildungen in der Pulpa. C. Ash & Sons Berlin.
Figure 1.
a: Experimental setup with the artificial oral cavity heated to 37 °C and a blinded chamber for the study endodontist with randomly arranged simulated root canals. b: Experimental setup with the artificial oral cavity (access angles 30°, 15°, 45°) from the perspective of the observer; the canal entrances visible to the endodontist do not allow any expectations of the access angle to the canal under treatment.
Figure 1.
a: Experimental setup with the artificial oral cavity heated to 37 °C and a blinded chamber for the study endodontist with randomly arranged simulated root canals. b: Experimental setup with the artificial oral cavity (access angles 30°, 15°, 45°) from the perspective of the observer; the canal entrances visible to the endodontist do not allow any expectations of the access angle to the canal under treatment.
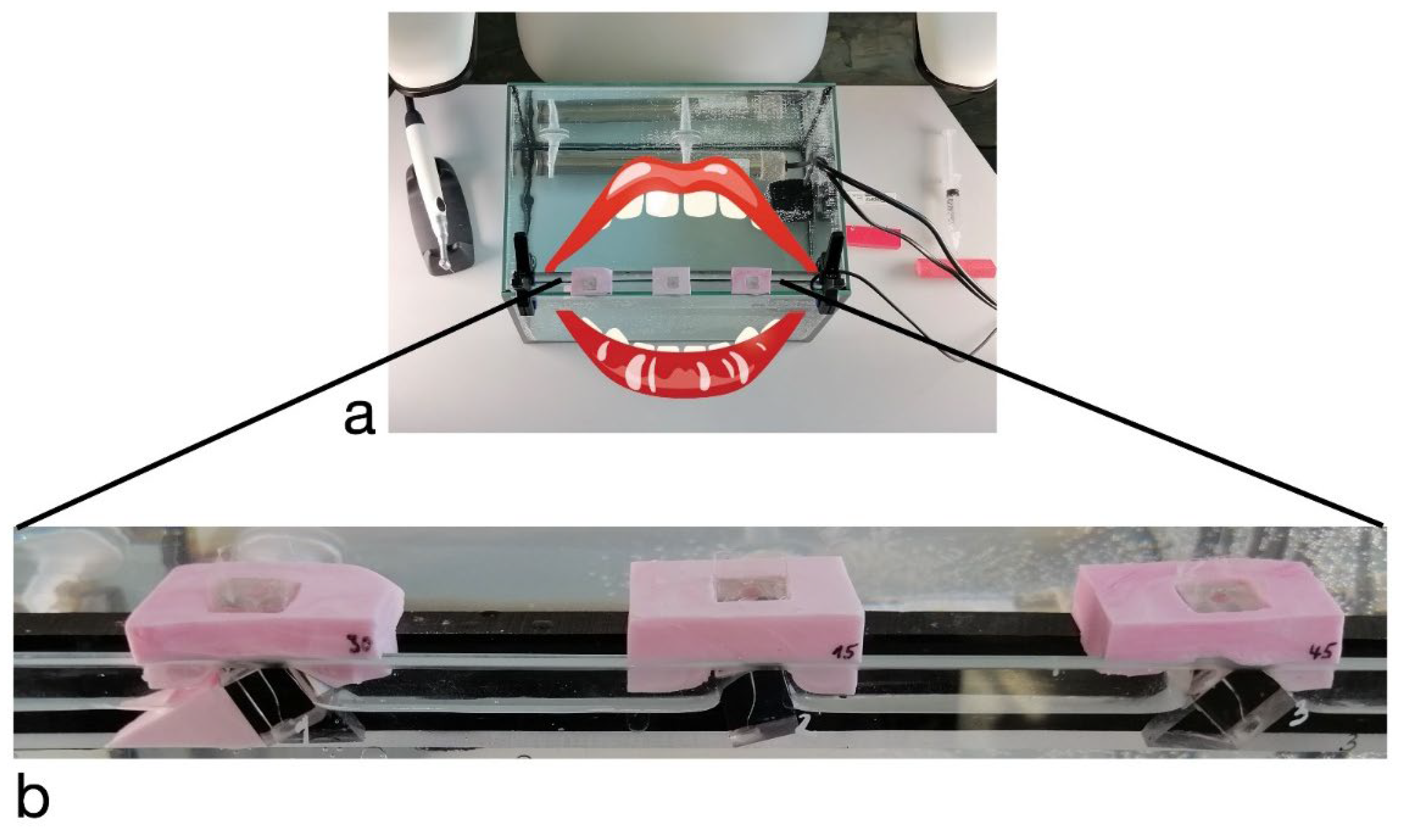
Figure 4.
Box plots of total volume loss (mm3) for the four test groups (TN: TruNatomy; XP: XP-Endo Shaper; F360: Komet F360 and HF: HyFlex EDM) compared to the canal entrance angles of 15°, 30° and 45°).
Figure 4.
Box plots of total volume loss (mm3) for the four test groups (TN: TruNatomy; XP: XP-Endo Shaper; F360: Komet F360 and HF: HyFlex EDM) compared to the canal entrance angles of 15°, 30° and 45°).
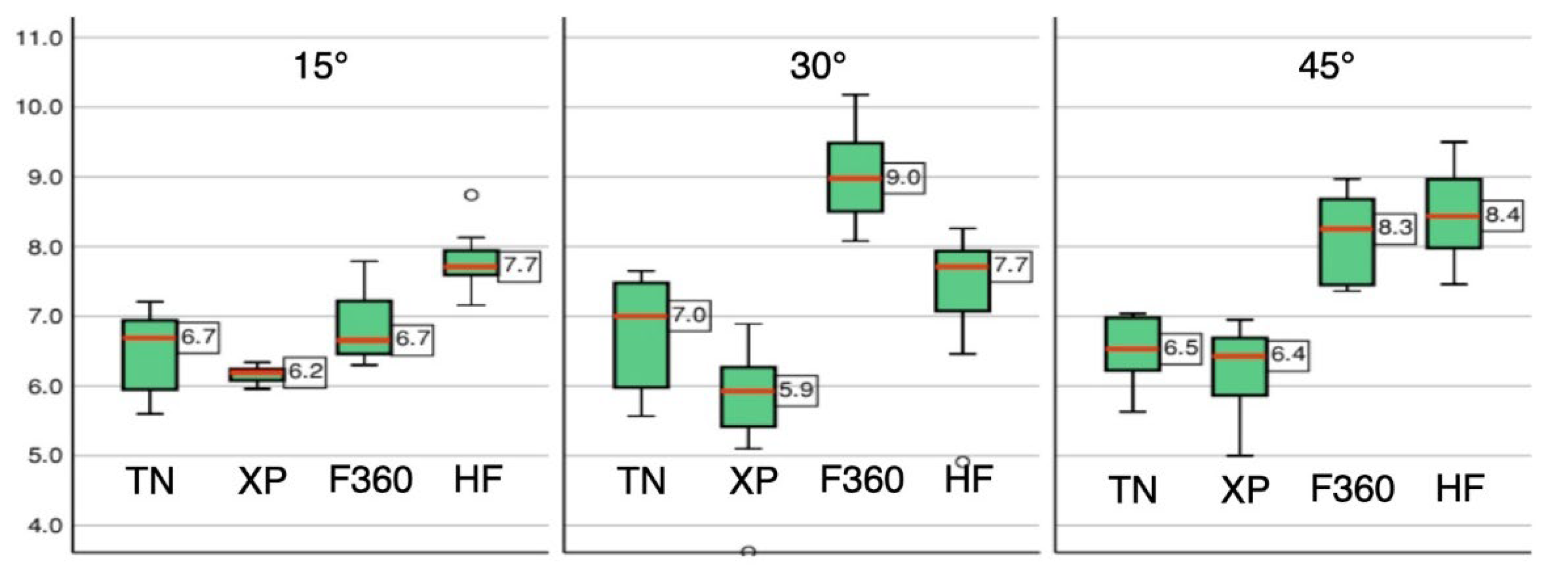
Figure 5.
Tooth anomaly of mandibular permanent incisor with dilaceration due to trauma at age of 6 years, consequently obliterated pulp chamber and outer half root canal. A: Baseline X-ray with posterior profound caries lesion and apical periodontitis. B: final X-ray after root canal treatment and fiber post stabilization. C+D: Planning of approximal access cavity with CBCT imaging (blue line).
Figure 5.
Tooth anomaly of mandibular permanent incisor with dilaceration due to trauma at age of 6 years, consequently obliterated pulp chamber and outer half root canal. A: Baseline X-ray with posterior profound caries lesion and apical periodontitis. B: final X-ray after root canal treatment and fiber post stabilization. C+D: Planning of approximal access cavity with CBCT imaging (blue line).
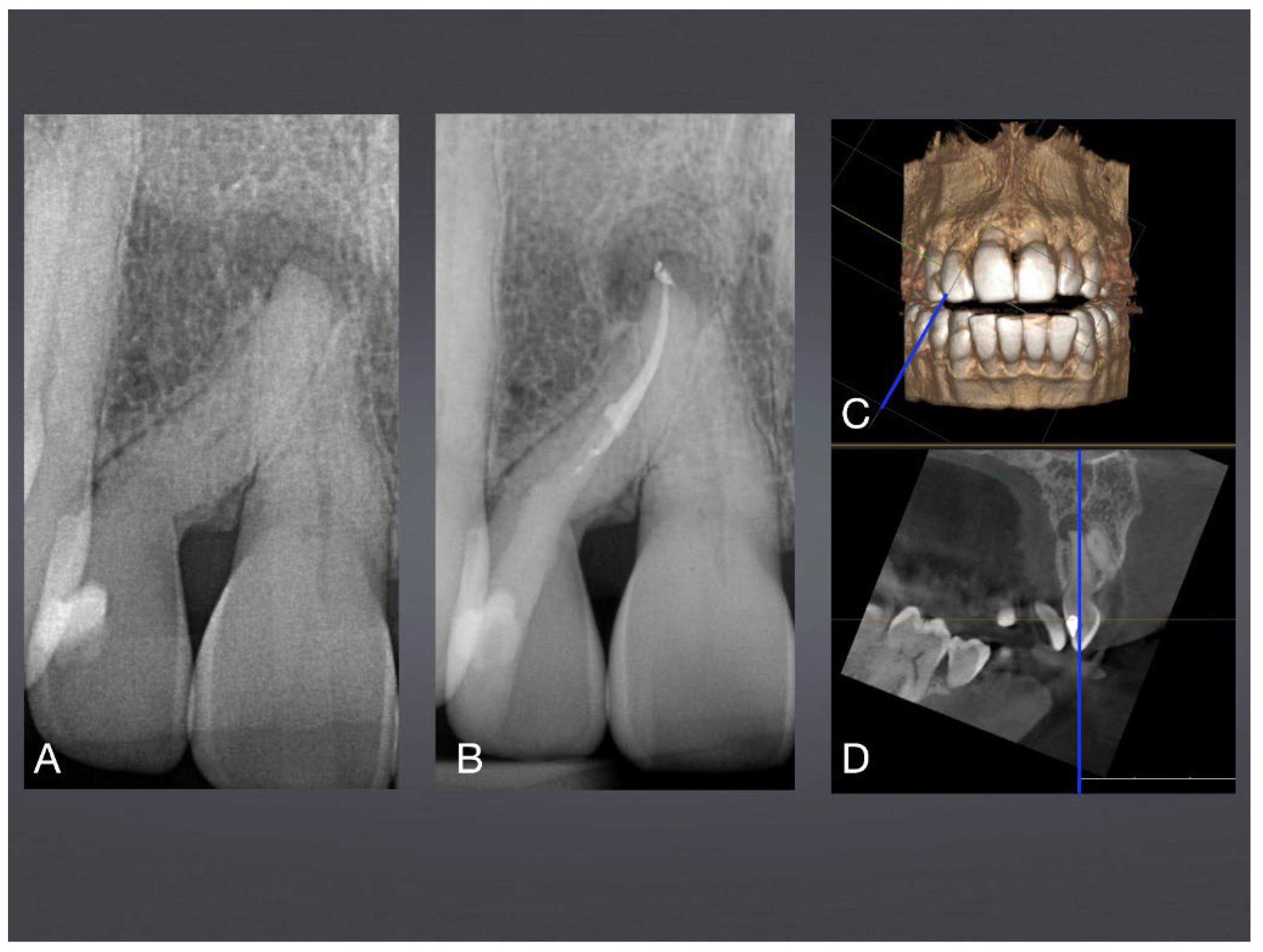
Figure 6.
Mandibular premolar with 3 S-shaped roots with 20° root canal access access angle. A: final X-ray after root canal treatment via occlusal surface, see preserved peri-cervical dentin (red line), characterizing microinvasive endodontics. B: Access cavity planning with SICAT-Endo guiding software. C: Occlusal access via preexisting crown restoration.
Figure 6.
Mandibular premolar with 3 S-shaped roots with 20° root canal access access angle. A: final X-ray after root canal treatment via occlusal surface, see preserved peri-cervical dentin (red line), characterizing microinvasive endodontics. B: Access cavity planning with SICAT-Endo guiding software. C: Occlusal access via preexisting crown restoration.
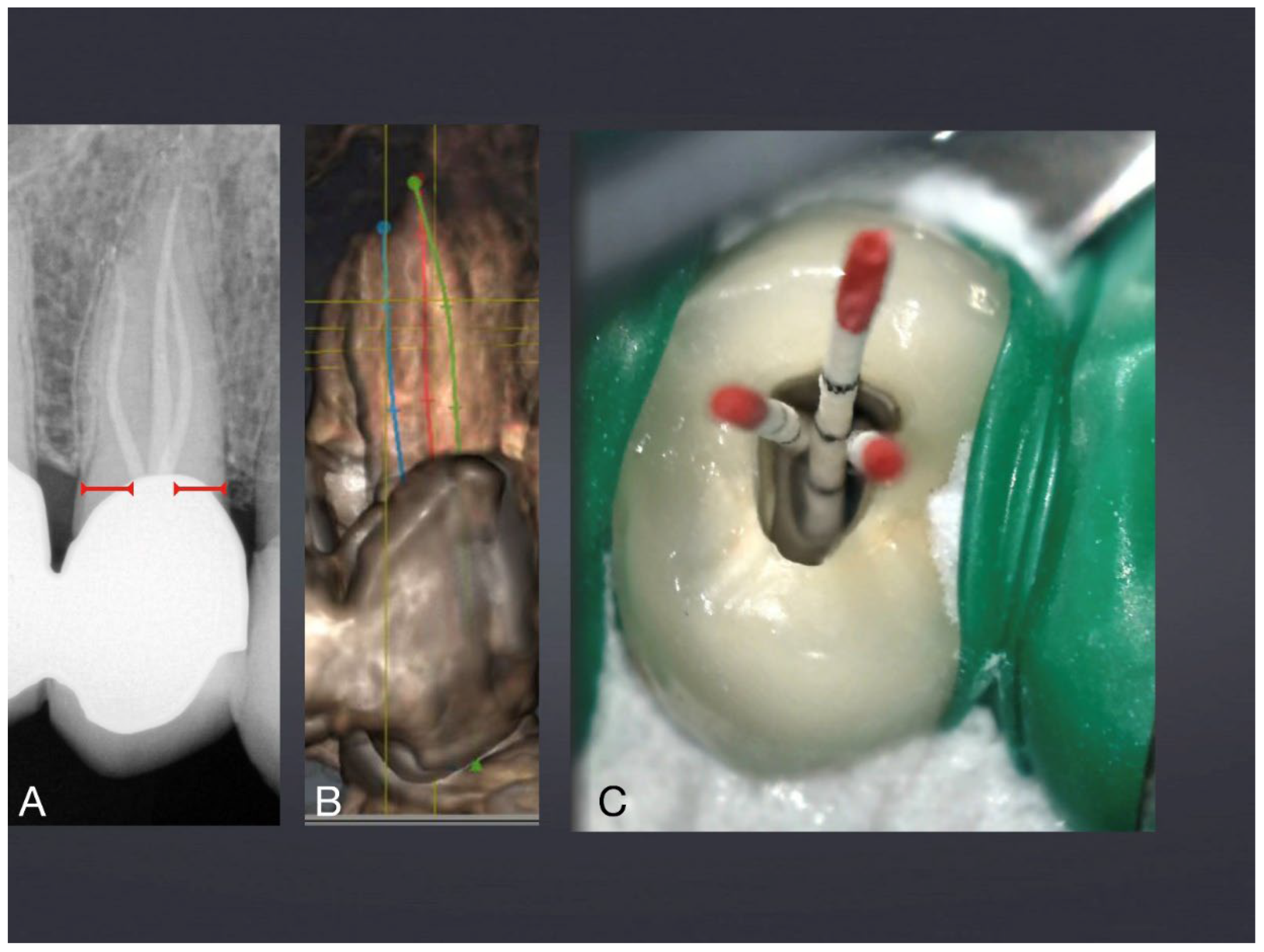
Figure 7.
Maxillary incisor with root canal obliteration. A: final X-ray after root canal treatment. B: Magnification of C: Access cavity via incisal edge and dentin abrasion facete. D: Access opening in comparison to 1 mm syringe, typical for microinvasive endodontics.
Figure 7.
Maxillary incisor with root canal obliteration. A: final X-ray after root canal treatment. B: Magnification of C: Access cavity via incisal edge and dentin abrasion facete. D: Access opening in comparison to 1 mm syringe, typical for microinvasive endodontics.
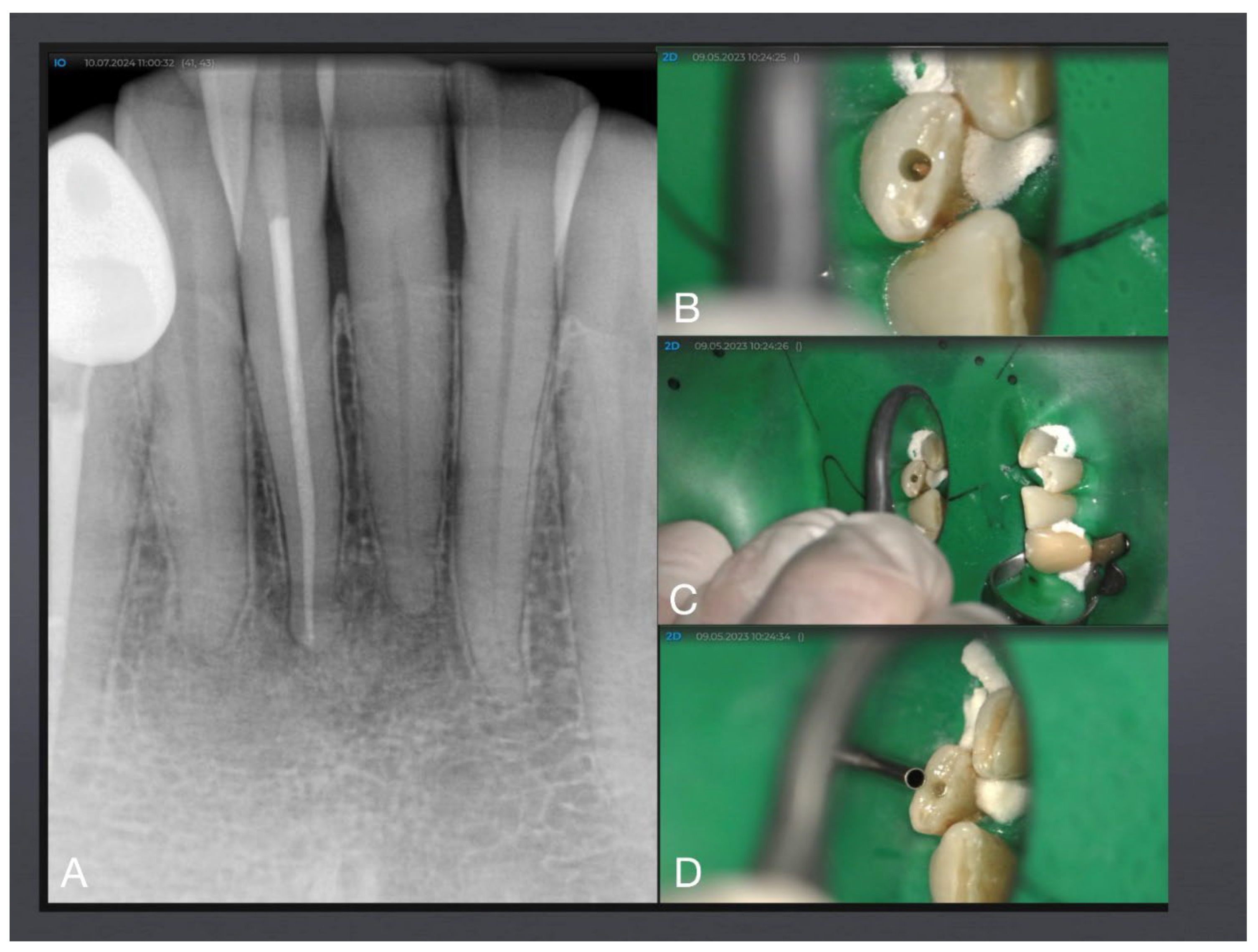
Figure 8.
Mandibular molar with 15° root canal access cavity angle next to the anterior caries lesion. A: Baseline X-ray with anterior filled caries lesion and apical periodontitis. B: Access planning with SICAT-Endo guiding software. C: Dried root canals after instrumentation and disinfection. D: Root canals after filling (photographed through water). E: final X-ray after microinvasive root canal treatment via occlusal surface demonstrating preserved peri-cervical dentin (red line).
Figure 8.
Mandibular molar with 15° root canal access cavity angle next to the anterior caries lesion. A: Baseline X-ray with anterior filled caries lesion and apical periodontitis. B: Access planning with SICAT-Endo guiding software. C: Dried root canals after instrumentation and disinfection. D: Root canals after filling (photographed through water). E: final X-ray after microinvasive root canal treatment via occlusal surface demonstrating preserved peri-cervical dentin (red line).
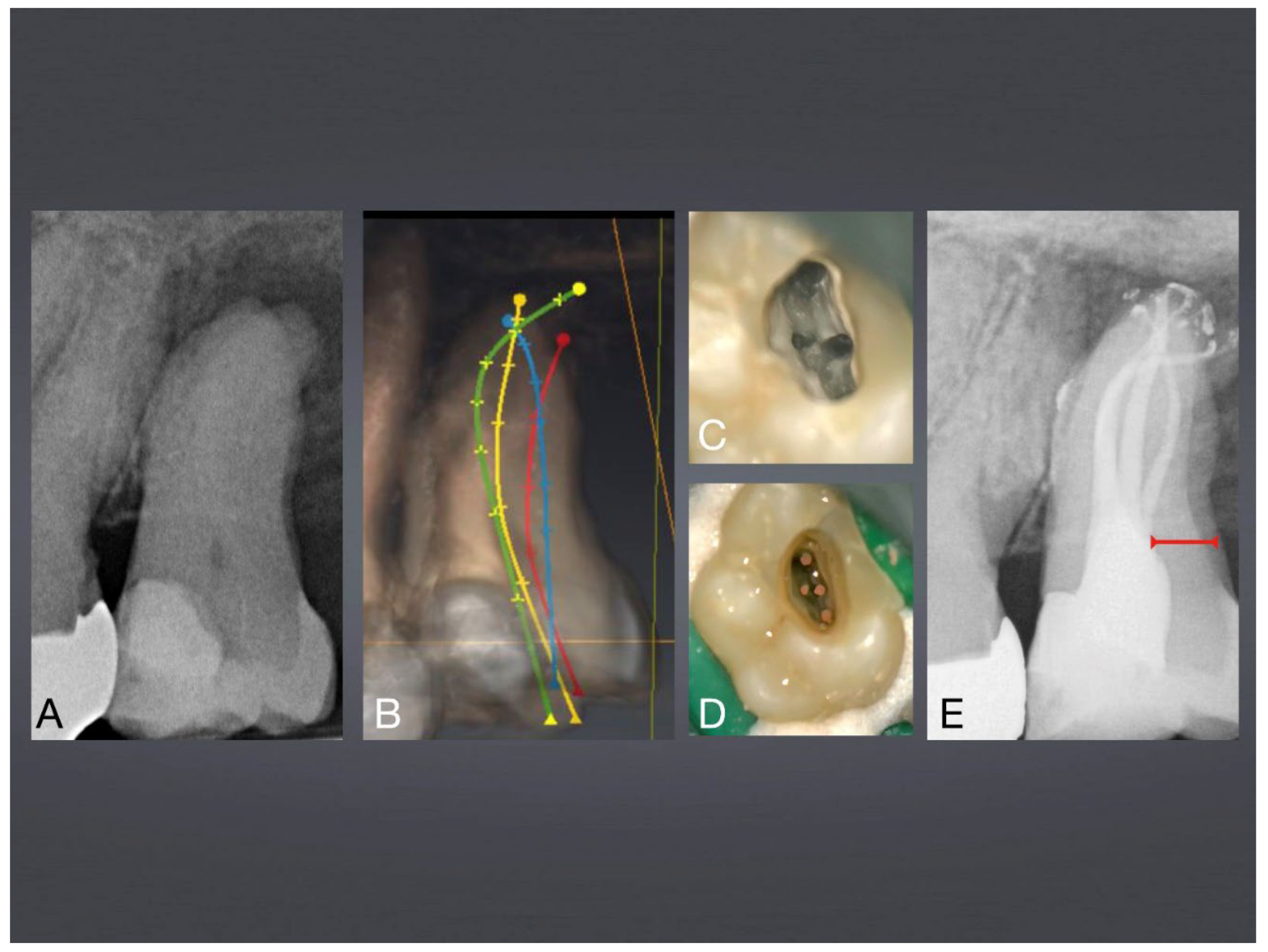

Table 1.
Results of t-test of parameter volume loss (VL) in the coronal, middle and apical thirds of the root canal and the total volume loss at 45° canal entrance angles between the different preparation systems. TruNatomy and XP-Endo files are significantly less aggressive concerning dentin loss than the two conventional file systems (yellow: not significant after Bonferroni correction).
Table 1.
Results of t-test of parameter volume loss (VL) in the coronal, middle and apical thirds of the root canal and the total volume loss at 45° canal entrance angles between the different preparation systems. TruNatomy and XP-Endo files are significantly less aggressive concerning dentin loss than the two conventional file systems (yellow: not significant after Bonferroni correction).
|
Comparison 45° |
Segment | Statistics | |||
| t | df | p | Mean difference |
||
|
XP-Endo Shaper vs. F360 |
Coronal VL | -1.900 | 11 | 0.084 | -0.434 |
| Middle VL | -5.737*** | 11 | 0.000 | -1.218 | |
| Apical VL | -4.724*** | 11 | 0.001 | -0.295 | |
| Total VL | -5.075*** | 11 | 0.000 | -1.947 | |
| XP-Endo Shaper vs. HyFlex EDM |
Coronal VL | -2.018 | 12 | 0.066 | -0.677 |
| Middle VL | -7.267*** | 12 | 0.000 | -1.281 | |
| Apikales VL | -6.490*** | 12 | 0.000 | -0.299 | |
| Total VL | -5.732*** | 12 | 0.000 | -2.257 | |
| F360 vs. HyFlex EDM |
Coronal VL | -0.836 | 7.461 | 0.429 | -0.243 |
| Middle VL | -0.407 | 11 | 0.692 | -0.063 | |
| Apikales VL | -0.049 | 11 | 0.961 | -0.003 | |
| Total VL | -0.760 | 11 | 0.463 | -0.310 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



