
Submitted:
20 September 2024
Posted:
20 September 2024
You are already at the latest version
Abstract
Background/Objectives: Monoclonal antibodies (mAbs) have revolutionized multiple myeloma (MM) treatment. However, post-marketing data on their neuropsychiatric safety is limited. This study aimed to evaluate neuropsychiatric adverse events (AEs) related to mAbs used for MM through a retrospective pharmacovigilance analysis using the Food and Drug Administration (FDA) Adverse Events Reporting System (FAERS) database.
Methods: Individual case safety reports (ICSRs) from 2015 to 2023 with at least one neuropsy-chiatric AE and one of the MM-approved mAbs as the suspect drug (i.e., daratumumab, elo-tuzumab, isatuximab, belantamab mafodotin, teclistamab, elranatamab, and talquentamab) were analyzed using descriptive and disproportionality approaches.
Results: Unknown signals of disproportionate reporting (SDR) included cerebral infarction for daratumumab (n = 45; reporting odds ratio (ROR) = 2.39, 95% confidence interval (CI) = 1.79-3.21; information component (IC) = 1.54, IC025-IC075 = 1.05-1.9), elotuzumab (25; 7.61, 5.13-11.28; 3.03, 2.37-3.51), and isatuximab (10; 2.56, 1.38-4.76; 1.67, 0.59-2.4); mental status changes for daratumumab (40; 2.66, 1.95-3.63; 1.67, 1.14-2.04) and belantamab mafodotin (10; 4.23, 2.28-7.88; 2.3, 1.22-3.03); altered state of consciousness for daratumumab (32; 1.97, 1.39-2.78; 1.32, 0.73-1.74) and belantamab mafodotin (6; 2.35, 1.05-5.23; 1.6, 0.19-2.52); Guil-lain-Barre syndrome (GBS) for daratumumab (23; 6.42, 4.26-9.69; 2.81, 2.11-3.3), isatuximab (8; 10.72, 5.35-21.48; 3.57, 2.35-4.37), and elotuzumab (3; 4.74, 1.53-14.7; 2.59, 0.52-3.8); and orthos-tatic intolerance for daratumumab (10; 12.54, 6.71-23.43; 3.75, 2.67-4.48) and elontuzumab (4; 28.31, 10.58-75.73; 5 , 3.24-6.08).
Conclusions: Our analysis highlighted several previously unacknowledged SDRs for MM-approved mAbs. Given the complex and not entirely understood etiology of some neuropsy-chiatric AEs, including GBS, further investigations are necessary.
Keywords:
Neuropsychiatric Adverse Events
; Multiple Myeloma
; FAERS
; Monoclonal Antibody
; Pharmacovigilance
1. Introduction
Multiple myeloma (MM) is characterized by the abnormal growth of plasma cells, which produce monoclonal immunoglobulins. This proliferation of cells within the bone marrow frequently leads to bone lesions, kidney damage, anemia, and elevated calcium levels [1]. Monoclonal antibodies (mAbs) have transformed MM treatment, offering significant effectiveness in both newly diagnosed MM (NDMM) and relapsed/refractory MM (RRMM) cases, improving survival rates and treatment compliance while reducing toxicity [2,3]. Five-year overall survival (OS) rates for MM have now surpassed 50% [4]. Daratumumab combined with lenalidomide, and dexamethasone extends median OS to 67.6 months compared to 51.8 months with lenalidomide and dexamethasone alone [5]. Elotuzumab improves median progression-free survival (PFS) to 19.4 months [6], while teclistamab shows a median PFS of 11.3 months [7]. By targeting plasma cell antigens, mAbs induce apoptosis through mechanisms such as antibody-dependent cellular cytotoxicity (ADCC), complement-dependent cytotoxicity, inhibition of mitochondrial transfer, and antibody-dependent cellular phagocytosis [8]. MAbs approved by the Food and Drug Administration (FDA) for MM include daratumumab, isatuximab, elotuzumab, belantamab mafodotin (withdrawn from the market), teclistamab, elranatamab, and talquetamab [9,10,11,12,13,14,15].
Although generally well-tolerated, mAbs can cause several adverse events (AEs) [9,10,11,12,13,14,15], including neuropsychiatric ones. While known neuropsychiatric AEs such as neuropathy for daratumumab, elotuzumab, teclistamab, elranatamab, and talquetamab and immune effector cell-associated neurotoxicity syndrome (ICANS) for teclistamab, elranatamab, and talquetamab are documented in the FDA Prescribing Information for these drugs, the literature suggests other undetected potential neuropsychiatric AEs for mAbs. For example, there have been case series reporting leukoencephalopathy and encephalitis with daratumumab [16,17,18], as well as other neurotoxicities, including movement and/or neurocognitive disorders not reported in FDA labels [15,19,20]. However, a comprehensive post-marketing study investigating the neuropsychiatric profile of the new MM therapies is lacking. The present study aims to evaluate and characterize neuropsychiatric AEs related to all mAbs used for MM by analyzing the US FDA Adverse Event Reporting System (FAERS) database to detect new potential neuropsychiatric safety signals.
2. Results
2.1. Selection Process and Descriptive Analysis
After applying the preliminary exclusion criteria and performing the final cleaning of the database, a total of 13,496,241 individual case safety reports (ICSRs) were identified. Among those, 4061 ICSRs met the previously specified inclusion criteria and were classified as cases because they were related to neuropsychiatric AEs and had one of the mAbs approved for MM as suspect drug. Most of these cases (n = 2862; 70.5%) were related to daratumumab, followed by isatuximab (n = 345; 8.5%) and elotuzumab (n = 321; 7.9%) (Figure 1).
Nearly half of the ICSRs were reported for elderly patients (n = 1947; 47.9%). This percentage was significantly higher than that observed in the non-cases (n = 2,895,017; 21.5%). A higher frequency of male patients was also observed in cases compared to non-cases (n = 1849; 45.5% vs. n = 4,670,150; 34.6%) (Table 1). A variation in age frequency was noted when stratifying neuropsychiatric ICSRs by each mAb. Specifically, lower frequencies of elderly patients were shown for teclistamab (n = 86; 39.8%), belantamab mafodotin (n = 69; 28.6%), and talquetamab (n = 13; 27.7%) (Table S1). Neuropsychiatric ICSRs were mainly issued by physicians (n = 2114; 52.1%) and from Europe (n = 1668; 41.1%). In terms of codified outcomes, neuropsychiatric ICSRs were mainly deemed to be linked to AEs of medical importance (n = 1801; 44.4%), followed by AEs leading to or prolonging hospitalization (n = 1397; 34.4%). Additionally, 351 ICSRs (8.6%) reported death as an outcome (Table 1). Considering neuropsychiatric AEs by each mAb, belantamab mafodotin and teclistamab-related ICSRs presented higher frequencies of death (n = 52; 21.6% and n = 42; 19.4%, respectively) (Table S1).
The shortest median (Q1-Q3) time to onset (TTO) for neuropsychiatric AEs was observed with teclistamab at 8 (3-11) days, while the highest median (Q1-Q3) TTO was observed with elranatamab at 72 (18-98) days (Figure 2).
2.2. Disproportionality Analysis
New and previously undetected signals of disproportionate reporting (SDRs) using neuropsychiatric AEs were detected by calculating the Reporting Odds Ratios (ROR) and their 95% confidence intervals (CI). The Bayesian information component (IC) was also computed to gauge the association strength between mAbs and AEs. Unexpected AEs were considered as such if not listed in the FDA Prescribing Information. Further details are provided in the materials and methods section.
Several already acknowledged AEs related to mAbs approved for the treatment of MM emerged as SDRs from our analysis. These included syncope for daratumumab, ICANS for both talquetamab and teclistamab, as well as peripheral neuropathy for both elotuzumab and elranatamab. The entire disproportionality analysis is available in the Table S2. Moreover, some SDRs were linked to other similar known neuropsychiatric AEs. Daratumumab was associated with polyneuropathies, which could include peripheral sensory neuropathy, and encephalopathies possibly linked to the known posterior reversible encephalopathy syndrome. Elranatamab related-ICSRs reported syncope, with a depressed level of consciousness being a known AE. Furthermore, postherpetic neuralgia, possibly tied to herpes zoster infection, was reported for elotuzumab. However, some unknown AEs also emerged as SDRs (Table 2).
Daratumumab had several SDRs which included some unknown nervous system-related AEs as follows: cerebral infarction (n = 45; ROR = 2.39, 95% CI = 1.79-3.21), depressed level of consciousness (42; 1.65, 1.22-2.24), ischaemic stroke (33; 2.24, 1.59-3.15; 1.47, 0.89-1.88), altered state of consciousness (32; 1.97, 1.39-2.78), partial seizures (27; 6.77, 4.63-9.89), spinal cord compression (23; 6.48, 4.29-9.77), Guillain-Barre syndrome (GBS) (23; 6.42, 4.26-9.69), ICANS (18; 5.36, 3.37-8.53), neurotoxicity (17; 1.69, 1.05-2.72), and incoherent (12; 2.61, 1.48-4.61). Considering psychiatric disorders, the AEs not reported in the FDA Prescribing Information for daratumumab were delirium (n = 54; ROR = 2.29, 95% CI = 1.75-2.99), mental status changes (40; 2.66, 1.95-3.63), and body dysmorphic disorder (15; 58.08, 34.3-98.33).
Focusing on belantamab mafodotin, unknown SDRs related to nervous system disorders were neuropathy peripheral (n = 38; ROR = 2.62, 95% CI = 1.90-3.61), altered state of consciousness (6; 2.35, 1.05-5.23), muscle tone disorder (4; 59.56, 22.19-159.81), Bell's palsy (3; 12.77, 4.11-39.68), and neurological decompensation (3; 12.49, 4.02-38.8). Moreover, regarding psychiatric disorders, the only unknown SDR was mental status changes (10; 4.23, 2.28-7.88).
Undocumented nervous system disorders for isatuximab that emerged as SDRs in our analysis included polyneuropathy (n = 21; ROR = 9.26, 95% CI = 6.03-14.22), transient ischaemic attack (17; 3.37, 2.09-5.42), ischaemic stroke (14; 4.59, 2.71-7.75), peripheral sensory neuropathy (11; 12.23, 6.76-22.13), cerebral infarction (10; 2.56, 1.38-4.76), cerebral ischaemia (9; 12.64, 6.56-24.34), GBS (8; 10.72, 5.35-21.48), haemorrhage intracranial (7; 2.76, 1.31-5.79), basal ganglia infarction (6; 132.39, 58.54-299.42), peripheral motor neuropathy (6; 29.61, 13.25-66.18), and subarachnoid haemorrhage (5; 2.95, 1.23-7.09). The only unknown SDR for psychiatric disorders was acute psychosis (3; 8.8, 2.83-27.34).
Spinal cord compression was the only unknown neuropsychiatric AE for teclistamab (n = 4; ROR = 15.87, 95% CI = 5.94-42.38).
Focusing on elotuzumab, unknown nervous system disorders with SDR included syncope (n = 27; ROR = 1.75; 95% CI = 1.2-2.56), cerebral infarction (25; 7.61, 5.13-11.28), cerebral hemorrhage (12; 2.27, 1.29-4; 1.52, 0.54-2.18), cerebrovascular disorder (4; 16.68, 6.24-44.56), orthostatic intolerance (4; 28.31, 10.58-75.73), VIth nerve paralysis (4; 36.99, 13.81-99.05), GBS (3; 4.74, 1.53-14.7), intention tremor (3; 49.87, 15.97-155.8), monoplegia (3; 4.55, 1.46-14.11), and spinal cord compression (3; 4.78, 1.54-14.83). Considering psychiatric disorders, the only unknown SDR was listlessness (3; 5.28, 1.7-16.38). An association between the drug and all unknown AEs was confirmed by the 95% credibility interval limit being greater than 0 for the IC. Further details are available in Table 2.
3. Discussion
To the best of our knowledge, this is the first study based on mAb-related neuropsychiatric AEs for the treatment of MM using a large-scale spontaneous reporting system database. Focusing on demographic characteristics, we observed a higher frequency of neuropsychiatric ICSRs involving male patients. The different incidence of MM between male and females might be a key factor in interpreting this result. Male sex is a well-recognized risk factor for the onset of MM. Indeed, a population-based study in the US revealed that, from 2000 to 2019, the age-standardized incidence rates of MM per 100,000 people were 8.49 (95% CI 8.43–8.54) for men and 5.58 (95% CI 5.55–5.62) for women [21]. Literature sources have hypothesized that this increased risk might be related genetic factors [22]. Additionally, possible lifestyle-dependent risk factors, more frequent in male patients (such as smoking or obesity), have also been hypothesized to contribute to the onset of monoclonal gammopathy of undetermined significance, a premalignant precursor to MM [23,24,25]. However, no conclusive evidence in MM exists regarding this in MM at present. Elderly patients were the age category with the highest frequency of neuropsychiatric ICSRs. Over 60% of MM diagnoses in the US are made in patients aged 65 years and older [26]. This might be due to early nonspecific symptoms of MM, such as back pain, fatigue, and anemia, which can often be mistaken for age-related issues, leading to delays in MM diagnosis and treatment [27]. Furthermore, elderly patients are known to be more susceptible to the onset of AEs in general [28,29], and age is also considered a risk factor for the development of neuropsychiatric AEs, such as peripheral neuropathy and polyneuropathy, in MM patients [30].
Serious outcomes, including hospitalization and important medical events, were mainly observed in neuropsychiatric ICSRs compared to the non-case group. The line-therapy of mAbs in MM treatment should be considered in this context. Indeed, daratumumab is the only mAb currently approved for NDMM. Thus, a relevant portion of the ICSRs could pertain to patients with RRMM. These patients are typically older, have undergone several lines of previous therapies, and may have disease-related comorbidities [31].
Considering the TTO, elranatamab-related ICSRs exhibited the highest median TTO among all mAbs for neuropsychiatric AEs. Elranatamab-related neuropsychiatric AEs with a longer TTO were mainly associated with alterations in consciousness, such as syncope, depressed level of consciousness, and altered state of consciousness. These manifestations have previously been observed as part of cytokine release syndromes [32]. However, these AEs are mostly reported during the step-up phases of treatment, with randomized controlled trial data highlighting a median (Q1-Q3) TTO 2 (1–9) days [33]. Thus, the observed prolonged TTO might be due to other factors, such as dose delays or interruptions, which could be implemented as mitigation strategies following the onset of previous AEs such as infections or hematologic AEs [33].
The disproportionality analysis highlighted SDRs in vascular disorders involving the central nervous system (CNS). Both cerebral infarction and ischaemic stroke were previously unknown for daratumumab, isatuximab, and elotuzumab. Literature data regarding specific CNS vascular complications in MM patients treated with mAbs is currently lacking. However, pre-marketing safety data for both daratumumab and isatuximab highlighted non relevant effects on the frequency of vascular thromboembolic events (VTE) in general [34,35]. Other factors might play a key role in the onset of these AEs. Indeed, MM patients are frequently characterized by hypercoagulability states, which could facilitate the onset of VTEs [36,37]. Furthermore, the co-administration of mAbs with immunomodulatory drugs, such as lenalidomide and pomalidomide, represents a well-recognized risk factor for VTEs [38]. Additionally, several disproportional haemorrhage-related AEs were observed, such as cerebellar haemorrhage for daratumumab and intracranial haemorrhage for isatuximab. In these cases, disease progression in MM might play a key role in the onset of these AEs. Indeed, MM patients exhibit the highest incidence of thrombocytopenia among those with haematological cancers, which is a significant risk factor for bleeding [39]. Moreover, dysfibrinogenemia, often observed in MM patients due to interactions between MM paraproteins and coagulation proteins, can also lead to bleeding complications [40,41,42].
AEs associated with alterations in the state of consciousness were also identified as unknown SDRs. Specifically, depressed or altered level of consciousness, incoherent state, stupor, and worsening of senile dementia had higher RORs for daratumumab. Alterations in consciousness and mental status were also SDRs for belantamab mafodotin, along with neurological decompensation. Delirium was identified as an SDR for elotuzumab, together with listless. Finally, acute psychotic episodes were unknown SDRs for isatuximab. Altered mental status (AMS) in MM patients is often due to metabolic disturbances such as uremia, hypercalcemia, and hyperviscosity. Elevated levels of serum ammonia have also been reported as a rare but clinically impactful cause of AMS in these patients [43]. Furthermore, a population-based study showed a strong correlation between peripheral neuropathies (PNs) and degradation of cognitive performance, which could lead to AMS in elderly patients [44]. AMS conditions might also result from the co-administration with immunomodulators, which could themselves be related to neurotoxicity [45]. Moreover, AMS might be part of more complex clinical pictures, such as encephalopathies [46], which were disproportionally reported for daratumumab and elotuzumab. The posterior reversible encephalopathy syndrome is an already documented AE for daratumumab. This condition is characterized by reversible vasogenic cerebral edema that manifests acutely with neurological symptoms such as seizures, headaches, and visual disturbances, in addition to AMS [47].
Neuropathies were also identified as SDRs in several mAbs. The onset of PNs was not mentioned in the FDA Prescribing Information for isatuximab and belantamab mafodotin. The neuronal damage that could lead to PNs might theoretically be caused by isatuximab and belantamab mafodotin through mechanisms such as ADCC [48,49] and CDC [50]. However, PNs can also emerge as consequences of worsening MM [30,51] due to deposits of the M-protein produced by myeloma cells on neurons [52]. Furthermore, isatuximab is currently approved only as a third-line treatment, while belantamab mafodotin was approved as a fifth-line therapy before its withdrawn. Thus, compromised patient conditions should be considered as a possible influencing factor [53,54]. Moreover, the concomitant use of pomalidomide and carfilzomib with daratumumab or isatuximab could also be associated with the onset of PNs in MM patients [55,56]. Neuropathies can be associated with both sensory (e.g., numbness, tingling, pain) and motor symptoms (e.g., muscle weakness). In some cases, PNs can also be associated with paralysis [30]. Our data were in line with this, as unknown VIth nerve paralyses were SDRs for daratumumab, belantamab mafodotin, and elotuzumab. Moreover, a rare severe form of PN, characterized by rapidly advancing, symmetrical limb weakness [51,52] and known as GBS, was also disproportionally reported for daratumumab, isatuximab, and elotuzumab [49,50]. The mechanisms underlying the onset of GBS remain unclear; however, the presence of a previous infection is considered an important factor [57]. Although immunodeficiency is a common feature of MM [58,59], both daratumumab and isatuximab-based therapies have been linked to an increased risk of infections [60]. Indeed, the results of a recent meta-analysis showed that among anti-CD38-treated patients, the relative risk for any grade of infection compared with control was 1.27 (95% CI, 1.17–1.37) [61]. This increased susceptibility to infections could potentially trigger the onset of GBS in predisposed individuals.
3.1. Strengths and Limitations
Spontaneous reporting system database-based analyses are among the most widely used methodologies for generating hypotheses about drug safety in pharmacovigilance [62,63]. The large-scale nature of the FAERS database enables the detection of AEs not previously identified in controlled environment studies [64]. However, some limitations inherent to the chosen methodology are present. The absence of a proper denominator prevents us from determining the incidence of the observed AEs [65]. Additionally, pharmacovigilance databases are mainly based on spontaneous reporting, which can lead to underreporting or overreporting of events due to various external factors [66,67]. Another limitation is the potential presence of duplicate ICSRs. To mitigate this issue, we implemented a multi-step control process based on key information fields, as detailed in the materials and methods section. Several additional measures were also implemented to improve data quality, such as eliminating undescriptive AEs and using validated data extraction and processing tools, as well as a standardized drug naming dictionary [68]. Most of the mAbs considered are prescribed as a second or subsequent lines of treatment for patients with RRMM. Therefore, the influence of disease progression on the reporting of neuropsychiatric AEs cannot be excluded. The observed disproportionalities may also have been influenced by the presence of other co-administered drugs, which complicates establishing a causal relationship between the observed AEs and mAbs. Furthermore, the lack of complete patient clinical histories, which are not available in the open FAERS data, limits our ability to conduct a more comprehensive evaluation. Despite these limitations, we believe our study provides valuable insights for oncologists, aiding in the understanding of the neuropsychiatric safety profile of mAbs and assisting in the management of MM patients.
4. Materials and Methods
4.1. Study Design
A retrospective pharmacovigilance study was conducted to identify neuropsychiatric AEs associated with mAbs approved for MM using the FAERS database. The FAERS database, a widely utilized public resource, has consistently demonstrated its reliability as a platform for drug safety evaluation studies [69,70,71,72]. This database aggregates over 20 million ICSRs from patients, healthcare providers, and pharmaceutical companies across the US, Europe, and Asia. Each ICSR includes a primary ID, data related to the individual (e.g., gender, age, and weight), reporting details such as the reporting country and the qualification of primary sources, information on suspected and concomitant drugs – including their indications and administration dates – and suspected AEs classified by the Medical Dictionary for Regulatory Activities (MedDRA®) Preferred Term (PT) [73], along with details on the date of onset and the outcome.
4.2. Selection of Cases
From the zipped ASCII FAERS quarterly data extract files accessible at https://fis.fda.gov/extensions/FPD-QDE-FAERS/FPD-QDE-FAERS.html (accessed on the 29th of January 2024) we downloaded data from the quarter 1 (Q1) of 2015 to the fourth quarter (Q4) of 2023, covering the period since the approval of the first mAbs for MM.
In detail, we retrieved data from each DEMO, DRUG, INDI, OUTC, REAC, and THER files. These files were merged based on the primary ID and the case ID. Information from INDI and THER files was combined with DRUG data to create a comprehensive file named DRUG_ALL. Similarly, OUTC data was merged with DEMO data to generate a file renamed DEMO_ALL. Additionally, the REAC_ALL file contained data exclusively from the REAC file.
Each of these three files —DRUG_ALL, DEMO_ALL, and REAC_ALL— was cleaned by removing all duplicated ICSRs based on primary ID and case ID, as well as key fields including type of AEs, date of onset, gender, age, reporting country, and suspected drug. This process followed FDA recommendations, wherein, in cases with multiple ICSRs sharing the same primary ID, only the most recent case ID version was retained [74].
From the DEMO_ALL file, premarketing ICSRs with supporting literature were excluded. Additionally, for the DRUG_ALL file, we utilized the DiAna dictionary – a dynamic, open-source tool known for its dynamic nature, transparency and adaptability. This dictionary was used to map all drug names in active substances within each ICSR according to the Anatomical Therapeutic Chemical (ATC) classifications [68]. We also excluded ICSRs that contained at least one investigational product, investigational biosimilar, or blinded product. Similarly, from the REAC_ALL file, all cases with the PT “no adverse event” were excluded.
For defining our cases, we selected all ICSRs where one of the following drugs was listed as the primary or secondary suspect: daratumumab, elotuzumab, isatuximab, belantamab mafodotin, teclistamab, elranatamab, and talquentamab. To avoid therapeutic biases, ICSRs with indications other than MM were excluded. Moreover, to analyze neuropsychiatric AEs, we considered all ICSRs containing at least one AE classified under the SOC “nervous system disorders” or “psychiatric disorders”.
4.3. Data Analyses
The demographic and clinical characteristics of FAERS ICSRs were analyzed using a descriptive statistical approach with a case-non-cases comparison. Continuous variables are presented as median with quartiles (Q1–Q3), while categorical variables are shown as absolute values with corresponding percentages. Key variables analyzed include gender, age, the primary source of information, year of reporting, reporting country, and detailed descriptions of AEs, including their outcome and TTO. TTO was calculated as the interval between drug administration (start date) and AE manifestation (event date) and presented as a median (Q1–Q3) for clarity.
A disproportionality analysis was conducted to detect new and previously undetected SDRs for neuropsychiatric PTs, by calculating the ROR and its 95% CI. Statistical significance was determined if the lower limit of the 95% CI for the ROR was greater than one, with a minimum of three ICSRs for each drug-event combination [70].
To reduce the risk of identifying spurious associations and assess the strength of the association between mAbs and AEs, the Bayesian IC was computed. An association between the drug and the AE was indicated by a 95% credibility interval limit greater than 0 (IC025 > 0). AEs not listed in the FDA Full Prescribing Information for each mAb at the time of the study were considered unexpected [9,10,11,12,13,14,15].
5. Conclusions
This study underscores the crucial role of large-scale spontaneous reporting system databases in evaluating AEs. Our findings are consistent with the limited existing literature on neuropsychiatric AEs associated with mAbs used in the treatment of MM. We identified several previously unrecognized neuropsychiatric AEs related to mAbs, including VTE, AMS, and GBS. Further research is needed to better understand and contextualize these tolerability issues. Additionally, our study highlights the importance of ongoing monitoring of MM patients for neuropsychiatric AEs. Timely management of these AEs can enhance patient quality of life and, in some cases, such as alterations in consciousness, may help reduce the impact of associated complications.
Author Contributions
Conceptualization, G.R. and M.A.B.; methodology, G.R. and M.A.B.; software, M.A.B.; validation, M.A.B. and E.S.; formal analysis, G.C., G.R., and M.A.B.; investigation, G.C. and M.A.B; data curation, G.R.; writing—original draft preparation, G.C. and G.R.; writing—review and editing, M.A.B., T.F., M.S., E.S.; visualization, G.C., G.R., V.S., T.F., N.S., M.S., E.S., and M.A.B.; supervision, E.S. and M.A.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study used publicly available safety ICSR data that were provided in an anonymous form and were already compliant with ethical standards. Therefore, no further ethical evaluation was necessary.
Data Availability Statement
This study was entirely based on publicly anonymized data made available by the Food and Drug Administration. The raw data can be downloaded at the following link https://fis.fda.gov/extensions/FPD-QDE-FAERS/FPD-QDE-FAERS.html.
Conflicts of Interest
The authors declare no conflicts of interest.
Appendix – List of Abbreviations
ADCC: antibody-dependent cellular cytotoxicity
AE: adverse event
AMS: altered mental status
ATC: Anatomical Therapeutic Chemical
CI: confidence interval
FAERS: Food and Drug Administration Adverse Events Reporting System
FDA: Food and Drug Administration
GBS: Guillain-Barre syndrome
IC: information component
ICANS: immune effector cell-associated neurotoxicity syndrome
ICSR: Individual Case Safety Report
mAbs: monoclonal antibodies
MedDRA: Medical Dictionary for Regulatory Activities
MM: multiple myeloma
NDMM: newly diagnosed multiple myeloma
PN: peripheral neuropathy
PT: Preferred Term
ROR: Reporting Odds Ratio
RRMM: relapsed/refractory multiple myeloma
SDR: signal of disproportionate reporting
TTO: time to onset
VTE: vascular thromboembolic events
References
- Rajkumar, S.V.; Dimopoulos, M.A.; Palumbo, A.; Blade, J.; Merlini, G.; Mateos, M.-V.; Kumar, S.; Hillengass, J.; Kastritis, E.; Richardson, P.; et al. International Myeloma Working Group Updated Criteria for the Diagnosis of Multiple Myeloma. Lancet Oncol 2014, 15, e538–e548. [Google Scholar] [CrossRef] [PubMed]
- Lapietra, G.; Fazio, F.; Petrucci, M.T. Race for the Cure: From the Oldest to the Newest Monoclonal Antibodies for Multiple Myeloma Treatment. Biomolecules 2022, 12, 1146. [Google Scholar] [CrossRef] [PubMed]
- Wudhikarn, K.; Wills, B.; Lesokhin, A.M. Monoclonal Antibodies in Multiple Myeloma: Current and Emerging Targets and Mechanisms of Action. Best Pract Res Clin Haematol 2020, 33, 101143. [Google Scholar] [CrossRef] [PubMed]
- van de Donk, N.W.C.J.; Pawlyn, C.; Yong, K.L. Multiple Myeloma. Lancet 2021, 397, 410–427. [Google Scholar] [CrossRef] [PubMed]
- Dimopoulos, M.A.; Oriol, A.; Nahi, H.; San-Miguel, J.; Bahlis, N.J.; Usmani, S.Z.; Rabin, N.; Orlowski, R.Z.; Suzuki, K.; Plesner, T.; et al. Overall Survival with Daratumumab, Lenalidomide, and Dexamethasone in Previously Treated Multiple Myeloma (POLLUX): A Randomized, Open-Label, Phase III Trial. Journal of Clinical Oncology 2023, 41, 1590–1599. [Google Scholar] [CrossRef] [PubMed]
- Lonial, S.; Dimopoulos, M.; Palumbo, A.; White, D.; Grosicki, S.; Spicka, I.; Walter-Croneck, A.; Moreau, P.; Mateos, M.-V.; Magen, H.; et al. Elotuzumab Therapy for Relapsed or Refractory Multiple Myeloma. N Engl J Med 2015, 373, 621–631. [Google Scholar] [CrossRef] [PubMed]
- Moreau, P.; Garfall, A.L.; van de Donk, N.W.C.J.; Nahi, H.; San-Miguel, J.F.; Oriol, A.; Nooka, A.K.; Martin, T.; Rosinol, L.; Chari, A.; et al. Teclistamab in Relapsed or Refractory Multiple Myeloma. N Engl J Med 2022, 387, 495. [Google Scholar] [CrossRef]
- Romano, A.; Storti, P.; Marchica, V.; Scandura, G.; Notarfranchi, L.; Craviotto, L.; Di Raimondo, F.; Giuliani, N. Mechanisms of Action of the New Antibodies in Use in Multiple Myeloma. Front Oncol 2021, 11, 684561. [Google Scholar] [CrossRef]
- US Food and Drug Administration Full Prescribing Information Talvey® (Talquetamab-Tgvs) Available online:. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/761342s000lbl.pdf (accessed on 29 April 2024).
- US Food and Drug Administration Full Prescribing Information Elrexfio TM® (Elranatamab Bcmm) Available online:. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/761345Orig1s000lbl.pdf (accessed on 29 April 2024).
- US Food and Drug Administration Full Prescribing Information Texvayli® (Teclistamab-Cqyv) Available online:. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2022/761291s000lbl.pdf (accessed on 30 October 2023).
- US Food and Drug Administration Full Prescribing Information Blenrep® (Belantamab Mafodotin-Blmf). Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/761158s000lbl.pdf (accessed on 30 October 2023).
- US Food and Drug Administration Full Prescribing Information Empliciti® (Elotuzumab) Available online:. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2022/761035s015lbl.pdf (accessed on 30 October 2023).
- US Food and Drug Administration Full Prescribing Information Sarclisa® (Isatuximab-Irfc) Available online:. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/761113s009lbl.pdf (accessed on 30 October 2023).
- US Food and Drug Administration Full Prescribing Information Darzalex® (Daratumumab) Available online:. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/761036s044lbl.pdf (accessed on 30 October 2023).
- Kareem, S.S.; Viswanathan, N.; Sahebjam, S.; Tran, N.D.; Gatewood, T.; Tobon, K.; Baz, R.; Piña, Y.; Shain, K.H.; Mokhtari, S. Leukoencephalopathy During Daratumumab-Based Therapy: A Case Series of Two Patients with Multiple Myeloma. Onco Targets Ther 2022, 15, 953–962. [Google Scholar] [CrossRef]
- Smets, I.; Titulaer, M.J. Antibody Therapies in Autoimmune Encephalitis. Neurotherapeutics 2022, 19, 823–831. [Google Scholar] [CrossRef]
- Ratuszny, D.; Skripuletz, T.; Wegner, F.; Gro?, M.; Falk, C.; Jacobs, R.; Ruschulte, H.; Stangel, M.; S?hs, K.-W.C.R. Daratumumab in a Patient With Severe Refractory Anti-NMDA Receptor Encephalitis. Front Neurol 2020, 11. [Google Scholar] [CrossRef] [PubMed]
- Mohyuddin, G.R.; Banerjee, R.; Alam, Z.; Berger, K.E.; Chakraborty, R. Rethinking Mechanisms of Neurotoxicity with BCMA Directed Therapy. Crit Rev Oncol Hematol 2021, 166, 103453. [Google Scholar] [CrossRef] [PubMed]
- Borrelli, E.P.; McGladrigan, C.G. Differences in Safety Profiles of Newly Approved Medications for Multiple Myeloma in Real-World Settings versus Randomized Controlled Trials. Journal of Oncology Pharmacy Practice 2021, 27, 887–896. [Google Scholar] [CrossRef] [PubMed]
- Mousavi, S.E.; Ilaghi, M.; Aslani, A.; Yekta, Z.; Nejadghaderi, S.A. A Population-Based Study on Incidence Trends of Myeloma in the United States over 2000–2020. Sci Rep 2023, 13, 20705. [Google Scholar] [CrossRef] [PubMed]
- Bird, S.; Cairns, D.; Menzies, T.; Boyd, K.; Davies, F.; Cook, G.; Drayson, M.; Gregory, W.; Jenner, M.; Jones, J.; et al. Sex Differences in Multiple Myeloma Biology but Not Clinical Outcomes: Results from 3894 Patients in the Myeloma XI Trial. Clin Lymphoma Myeloma Leuk 2021, 21, 667–675. [Google Scholar] [CrossRef]
- Lee, D.J.; El-Khoury, H.; Tramontano, A.C.; Alberge, J.-B.; Perry, J.; Davis, M.I.; Horowitz, E.; Redd, R.; Sakrikar, D.; Barnidge, D.; et al. Mass Spectrometry-Detected MGUS Is Associated with Obesity and Other Novel Modifiable Risk Factors in a High-Risk Population. Blood Adv 2024, 8, 1737–1746. [Google Scholar] [CrossRef]
- Muscogiuri, G.; Verde, L.; Vetrani, C.; Barrea, L.; Savastano, S.; Colao, A. Obesity: A Gender-View. J Endocrinol Invest 2023, 47, 299–306. [Google Scholar] [CrossRef]
- U.S. Available online: https://www.cdc.gov/tobacco/data_statistics/fact_sheets/adult_data/cig_smoking/index.htm (accessed on 1 August 2024).
- Padala, S.A.; Barsouk, A.; Barsouk, A.; Rawla, P.; Vakiti, A.; Kolhe, R.; Kota, V.; Ajebo, G.H. Epidemiology, Staging, and Management of Multiple Myeloma. Medical Sciences 2021, 9, 3. [Google Scholar] [CrossRef]
- Boyle, E.M.; Legrand, C.; Demarquette, H.; Guidez, S.; Herbaux, C.; Leleu, X.; Facon, T. Treatment of Elderly Patients with Myeloma. In Handbook of Multiple Myeloma; Springer International Publishing: Cham, 2015; pp. 41–63. [Google Scholar]
- Palumbo, A.; Oliva, S. Latest Advances in the Management of Elderly Patients with Multiple Myeloma. Int J Hematol Oncol 2013, 2, 431–434. [Google Scholar] [CrossRef]
- Palumbo, A.; Bringhen, S.; Ludwig, H.; Dimopoulos, M.A.; Bladé, J.; Mateos, M.V.; Rosiñol, L.; Boccadoro, M.; Cavo, M.; Lokhorst, H.; et al. Personalized Therapy in Multiple Myeloma According to Patient Age and Vulnerability: A Report of the European Myeloma Network (EMN). Blood 2011, 118, 4519–4529. [Google Scholar] [CrossRef]
- Richardson, P.G.; Laubach, J.P.; Schlossman, R.L.; Mitsiades, C.; Anderson, K. Complications of Multiple Myeloma Therapy, Part 1: Risk Reduction and Management of Peripheral Neuropathy and Asthenia. Journal of the National Comprehensive Cancer Network 2010, 8, S–4. [Google Scholar] [CrossRef] [PubMed]
- Pozzi, S.; Bari, A.; Pecherstorfer, M.; Vallet, S. Management of Adverse Events and Supportive Therapy in Relapsed/Refractory Multiple Myeloma. Cancers (Basel) 2021, 13, 4978. [Google Scholar] [CrossRef] [PubMed]
- Shimabukuro-Vornhagen, A.; Gödel, P.; Subklewe, M.; Stemmler, H.J.; Schlößer, H.A.; Schlaak, M.; Kochanek, M.; Böll, B.; von Bergwelt-Baildon, M.S. Cytokine Release Syndrome. J Immunother Cancer 2018, 6, 56. [Google Scholar] [CrossRef] [PubMed]
- Lesokhin, A.M.; Tomasson, M.H.; Arnulf, B.; Bahlis, N.J.; Miles Prince, H.; Niesvizky, R.; Rodrίguez-Otero, P.; Martinez-Lopez, J.; Koehne, G.; Touzeau, C.; et al. Elranatamab in Relapsed or Refractory Multiple Myeloma: Phase 2 MagnetisMM-3 Trial Results. Nat Med 2023, 29, 2259–2267. [Google Scholar] [CrossRef] [PubMed]
- Sborov, D.W.; Baljevic, M.; Reeves, B.; Laubach, J.; Efebera, Y.A.; Rodriguez, C.; Costa, L.J.; Chari, A.; Silbermann, R.; Holstein, S.A.; et al. Daratumumab plus Lenalidomide, Bortezomib and Dexamethasone in Newly Diagnosed Multiple Myeloma: Analysis of Vascular Thrombotic Events in the <scp>GRIFFIN</Scp> Study. Br J Haematol 2022, 199, 355–365. [Google Scholar] [CrossRef]
- Moreau, P.; Dimopoulos, M.-A.; Mikhael, J.; Yong, K.; Capra, M.; Facon, T.; Hajek, R.; Špička, I.; Baker, R.; Kim, K.; et al. Isatuximab, Carfilzomib, and Dexamethasone in Relapsed Multiple Myeloma (IKEMA): A Multicentre, Open-Label, Randomised Phase 3 Trial. The Lancet 2021, 397, 2361–2371. [Google Scholar] [CrossRef]
- Papageorgiou, L.; Alhaj Hussen, K.; Thouroude, S.; Mbemba, E.; Cost, H.; Garderet, L.; Elalamy, I.; Larsen, A.; Van Dreden, P.; Dimopoulos, M.A.; et al. Modelization of Blood-Borne Hypercoagulability in Myeloma: A Tissue-Factor-Bearing Microparticle-Driven Process. TH Open 2019, 03, e340–e347. [Google Scholar] [CrossRef]
- Guo, L.; Tong, D.; Yu, M.; Zhang, Y.; Li, T.; Wang, C.; Zhou, P.; Jin, J.; Li, B.; Liu, Y.; et al. Phosphatidylserine-Exposing Cells Contribute to the Hypercoagulable State in Patients with Multiple Myeloma. Int J Oncol 2018. [Google Scholar] [CrossRef]
- Covut, F.; Sanfilippo, K.M. Mitigating the Risk of Venous Thromboembolism in Patients with Multiple Myeloma Receiving Immunomodulatory-Based Therapy. Hematology 2022, 2022, 363–367. [Google Scholar] [CrossRef]
- Shaw, J.L.; Nielson, C.M.; Park, J.K.; Marongiu, A.; Soff, G.A. The Incidence of Thrombocytopenia in Adult Patients Receiving Chemotherapy for Solid Tumors or Hematologic Malignancies. Eur J Haematol 2021, 106, 662–672. [Google Scholar] [CrossRef]
- Kulkarni, A.; Bazou, D.; Santos-Martinez, M.J. Bleeding and Thrombosis in Multiple Myeloma: Platelets as Key Players during Cell Interactions and Potential Use as Drug Delivery Systems. Int J Mol Sci 2023, 24, 15855. [Google Scholar] [CrossRef] [PubMed]
- Siddiq, N.; Bergstrom, C.; Anderson, L.D.; Nagalla, S. Bleeding Due to Acquired Dysfibrinogenemia as the Initial Presentation of Multiple Myeloma. BMJ Case Rep 2019, 12, e229312. [Google Scholar] [CrossRef] [PubMed]
- Rahman, S.; Veeraballi, S.; Chan, K.H.; Shaaban, H.S. Bleeding Diathesis in Multiple Myeloma: A Rare Presentation of a Dreadful Emergency With Management Nightmare. Cureus 2021. [Google Scholar] [CrossRef]
- Sandhu, G.; Farias, A.A.; Ranade, A.; Meisels, I. Altered Mental Status in a Case of Multiple Myeloma Not Related to a Metabolic Cause. Clin Kidney J 2009, 2, 434–435. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.-J.; Kao, T.-W.; Chen, W.-L. Relationship between Peripheral Neuropathy and Cognitive Performance in the Elderly Population. Medicine 2021, 100, e26071. [Google Scholar] [CrossRef]
- Patel, U.H.; Mir, M.A.; Sivik, J.K.; Raheja, D.; Pandey, M.K.; Talamo, G. Central Neurotoxicity of Immunomodulatory Drugs in Multiple Myeloma. Hematol Rep 2015, 7, 5704. [Google Scholar] [CrossRef] [PubMed]
- Fugate, J.E.; Rabinstein, A.A. Posterior Reversible Encephalopathy Syndrome: Clinical and Radiological Manifestations, Pathophysiology, and Outstanding Questions. Lancet Neurol 2015, 14, 914–925. [Google Scholar] [CrossRef]
- Ghanem, R.; Glaisner, S.; Bobin, A.; Ronchetti, A.-M.; Cereja, S.; Joly, B.; Salanoubat, C.; Fouquet, G. Posterior Reversible Encephalopathy Syndrome (PRES) and Myeloma. Leuk Res Rep 2024, 21, 100407. [Google Scholar] [CrossRef]
- Lonial, S.; Lee, H.C.; Badros, A.; Trudel, S.; Nooka, A.K.; Chari, A.; Abdallah, A.-O.; Callander, N.; Lendvai, N.; Sborov, D.; et al. Belantamab Mafodotin for Relapsed or Refractory Multiple Myeloma (DREAMM-2): A Two-Arm, Randomised, Open-Label, Phase 2 Study. Lancet Oncol 2020, 21, 207–221. [Google Scholar] [CrossRef]
- Tai, Y.-T.; de Weers, M.; Li, X.-F.; Song, W.; Nahar, S.; Bakker, J.M.; Vink, T.; Jacobs, D.; Oomen, L.; Bleeker, W.K.; et al. Daratumumab, a Novel Potent Human Anti-CD38 Monoclonal Antibody, Induces Significant Killing of Human Multiple Myeloma Cells: Therapeutic Implication. Blood 2009, 114, 608–608. [Google Scholar] [CrossRef]
- Markham, A. Belantamab Mafodotin: First Approval. Drugs 2020, 80, 1607–1613. [Google Scholar] [CrossRef] [PubMed]
- Mohty, B.; El-Cheikh, J.; Yakoub-Agha, I.; Moreau, P.; Harousseau, J.-L.; Mohty, M. Peripheral Neuropathy and New Treatments for Multiple Myeloma: Background and Practical Recommendations. Haematologica 2010, 95, 311–319. [Google Scholar] [CrossRef] [PubMed]
- Živković, S.A.; Lacomis, D.; Lentzsch, S. Paraproteinemic Neuropathy. Leuk Lymphoma 2009, 50, 1422–1433. [Google Scholar] [CrossRef] [PubMed]
- Nahi, H.; Walinder, G.; Patel, V.; Qu, Y.; Levine, A.; Majer, I.; Kutikova, L.; Hellqvist Franck, E.; Svensson, M.K.; Hansson, M. Burden of Treatment-Induced Peripheral Neuropathy in Patients with Multiple Myeloma in Sweden. Acta Haematol 2021, 144, 519–527. [Google Scholar] [CrossRef] [PubMed]
- Richardson, P.G.; Delforge, M.; Beksac, M.; Wen, P.; Jongen, J.L.; Sezer, O.; Terpos, E.; Munshi, N.; Palumbo, A.; Rajkumar, S. V; et al. Management of Treatment-Emergent Peripheral Neuropathy in Multiple Myeloma. Leukemia 2012, 26, 595–608. [Google Scholar] [CrossRef] [PubMed]
- Richardson, P.G.; Siegel, D.S.; Vij, R.; Hofmeister, C.C.; Baz, R.; Jagannath, S.; Chen, C.; Lonial, S.; Jakubowiak, A.; Bahlis, N.; et al. Pomalidomide Alone or in Combination with Low-Dose Dexamethasone in Relapsed and Refractory Multiple Myeloma: A Randomized Phase 2 Study. Blood 2014, 123, 1826–1832. [Google Scholar] [CrossRef] [PubMed]
- Siegel, D.S.; Martin, T.; Wang, M.; Vij, R.; Jakubowiak, A.J.; Lonial, S.; Trudel, S.; Kukreti, V.; Bahlis, N.; Alsina, M.; et al. A Phase 2 Study of Single-Agent Carfilzomib (PX-171-003-A1) in Patients with Relapsed and Refractory Multiple Myeloma. Blood 2012, 120, 2817–2825. [Google Scholar] [CrossRef]
- van den Berg, B.; Walgaard, C.; Drenthen, J.; Fokke, C.; Jacobs, B.C.; van Doorn, P.A. Guillain–Barré Syndrome: Pathogenesis, Diagnosis, Treatment and Prognosis. Nat Rev Neurol 2014, 10, 469–482. [Google Scholar] [CrossRef]
- Díaz-Tejedor, A.; Lorenzo-Mohamed, M.; Puig, N.; García-Sanz, R.; Mateos, M.-V.; Garayoa, M.; Paíno, T. Immune System Alterations in Multiple Myeloma: Molecular Mechanisms and Therapeutic Strategies to Reverse Immunosuppression. Cancers (Basel) 2021, 13, 1353. [Google Scholar] [CrossRef]
- Nightingale, B.; Decker, M.; Ryan, R.; Kaczmarczyk, K.; Jandir, P.; Waykole, T.; Ashkar, R.; Harmon, G.; Mathur, A.; Levitt, M. Multiple Myeloma: A Review of the Literature and a Case Report Highlighting the Immunocompromised State of Myeloma Patients. World J Oncol 2024, 15, 348–354. [Google Scholar] [CrossRef]
- Hong, J.; Zhou, B.; Pak, A.; Yang, N.; Barmettler, S. Hypogammaglobulinemia and Risk of Infection Following Daratumumab in Patients with Multiple Myeloma. Journal of Allergy and Clinical Immunology 2024, 153, AB231. [Google Scholar] [CrossRef]
- Vassilopoulos, S.; Vassilopoulos, A.; Kalligeros, M.; Shehadeh, F.; Mylonakis, E. Cumulative Incidence and Relative Risk of Infection in Patients With Multiple Myeloma Treated With Anti-CD38 Monoclonal Antibody-Based Regimens: A Systematic Review and Meta-Analysis. Open Forum Infect Dis 2022, 9. [Google Scholar] [CrossRef] [PubMed]
- Barbieri, M.A.; Sorbara, E.E.; Cicala, G.; Santoro, V.; Cutroneo, P.M.; Franchina, T.; Spina, E. Adverse Drug Reactions with HER2-Positive Breast Cancer Treatment: An Analysis from the Italian Pharmacovigilance Database. Drugs Real World Outcomes 2022, 9, 91–107. [Google Scholar] [CrossRef] [PubMed]
- Barbieri, M.A.; Sorbara, E.E.; Cicala, G.; Santoro, V.; Cutroneo, P.M.; Franchina, T.; Santarpia, M.; Silvestris, N.; Spina, E. Safety Profile of Tyrosine Kinase Inhibitors Used in Non-Small-Cell Lung Cancer: An Analysis from the Italian Pharmacovigilance Database. Front Oncol 2022, 12. [Google Scholar] [CrossRef] [PubMed]
- Celi, L.A.; Moseley, E.; Moses, C.; Ryan, P.; Somai, M.; Stone, D.; Tang, K. From Pharmacovigilance to Clinical Care Optimization. Big Data 2014, 2, 134–141. [Google Scholar] [CrossRef] [PubMed]
- Montastruc, J.; Sommet, A.; Bagheri, H.; Lapeyre-Mestre, M. Benefits and Strengths of the Disproportionality Analysis for Identification of Adverse Drug Reactions in a Pharmacovigilance Database. Br J Clin Pharmacol 2011, 72, 905–908. [Google Scholar] [CrossRef] [PubMed]
- Cicala, G.; de Filippis, R.; Barbieri, M.A.; Cutroneo, P.M.; De Fazio, P.; Schoretsanitis, G.; Spina, E. Tolerability Profile of Paliperidone Palmitate Formulations: A Pharmacovigilance Analysis of the EUDRAVigilance Database. Front Psychiatry 2023, 14. [Google Scholar] [CrossRef]
- Pozsgai, K.; Szűcs, G.; Kőnig-Péter, A.; Balázs, O.; Vajda, P.; Botz, L.; Vida, R.G. Analysis of Pharmacovigilance Databases for Spontaneous Reports of Adverse Drug Reactions Related to Substandard and Falsified Medical Products: A Descriptive Study. Front Pharmacol 2022, 13. [Google Scholar] [CrossRef]
- Fusaroli, M.; Giunchi, V.; Battini, V.; Puligheddu, S.; Khouri, C.; Carnovale, C.; Raschi, E.; Poluzzi, E. Enhancing Transparency in Defining Studied Drugs: The Open-Source Living DiAna Dictionary for Standardizing Drug Names in the FAERS. Drug Saf 2024. [Google Scholar] [CrossRef]
- Barbieri, M.A.; Russo, G.; Sorbara, E.E.; Cicala, G.; Franchina, T.; Santarpia, M.; Speranza, D.; Spina, E.; Silvestris, N. Neuropsychiatric Adverse Drug Reactions with Oral Tyrosine Kinase Inhibitors in Metastatic Colorectal Cancer: An Analysis from the FDA Adverse Event Reporting System. Front Oncol 2023, 13. [Google Scholar] [CrossRef]
- Russo, G.; Barbieri, M.A.; Sorbara, E.E.; Cicala, G.; Franchina, T.; Santarpia, M.; Silvestris, N.; Spina, E. Renal Disorders with Oral Tyrosine Kinase Inhibitors in Metastatic Colorectal Cancer: An Analysis from the FDA Adverse Event Reporting System Database. Biomedicines 2023, 11, 2311. [Google Scholar] [CrossRef] [PubMed]
- Cicala, G.; Barbieri, M.A.; Russo, G.; Salvo, F.; Spina, E. Safety of Dual Orexin Receptor Antagonist Daridorexant: A Disproportionality Analysis of Publicly Available FAERS Data. Pharmaceuticals 2024, 17, 342. [Google Scholar] [CrossRef] [PubMed]
- Raschi, E.; Fusaroli, M.; Giunchi, V.; Repaci, A.; Pelusi, C.; Mollica, V.; Massari, F.; Ardizzoni, A.; Poluzzi, E.; Pagotto, U.; et al. Adrenal Insufficiency with Anticancer Tyrosine Kinase Inhibitors Targeting Vascular Endothelial Growth Factor Receptor: Analysis of the FDA Adverse Event Reporting System. Cancers (Basel) 2022, 14, 4610. [Google Scholar] [CrossRef] [PubMed]
- Brown, E.G.; Wood, L.; Wood, S. The Medical Dictionary for Regulatory Activities (MedDRA). Drug Saf 1999, 20, 109–117. [Google Scholar] [CrossRef] [PubMed]
- Khaleel, M.A.; Khan, A.H.; Ghadzi, S.M.S.; Adnan, A.S.; Abdallah, Q.M. A Standardized Dataset of a Spontaneous Adverse Event Reporting System. Healthcare 2022, 10, 420. [Google Scholar] [CrossRef]
- RStudio Team RStudio: Integrated Development for R 2019.
- Foundation for Statistical Computing, R. R: A Language and Environment for Statistical Computing Available online: https://www.R-project.org/.
Figure 1.
Database Cleaning and Cases Selection Flowchart. AE = adverse event; ICSR = individual case safety report; MM = multiple myeloma; PT = Preferred Term.
Figure 1.
Database Cleaning and Cases Selection Flowchart. AE = adverse event; ICSR = individual case safety report; MM = multiple myeloma; PT = Preferred Term.
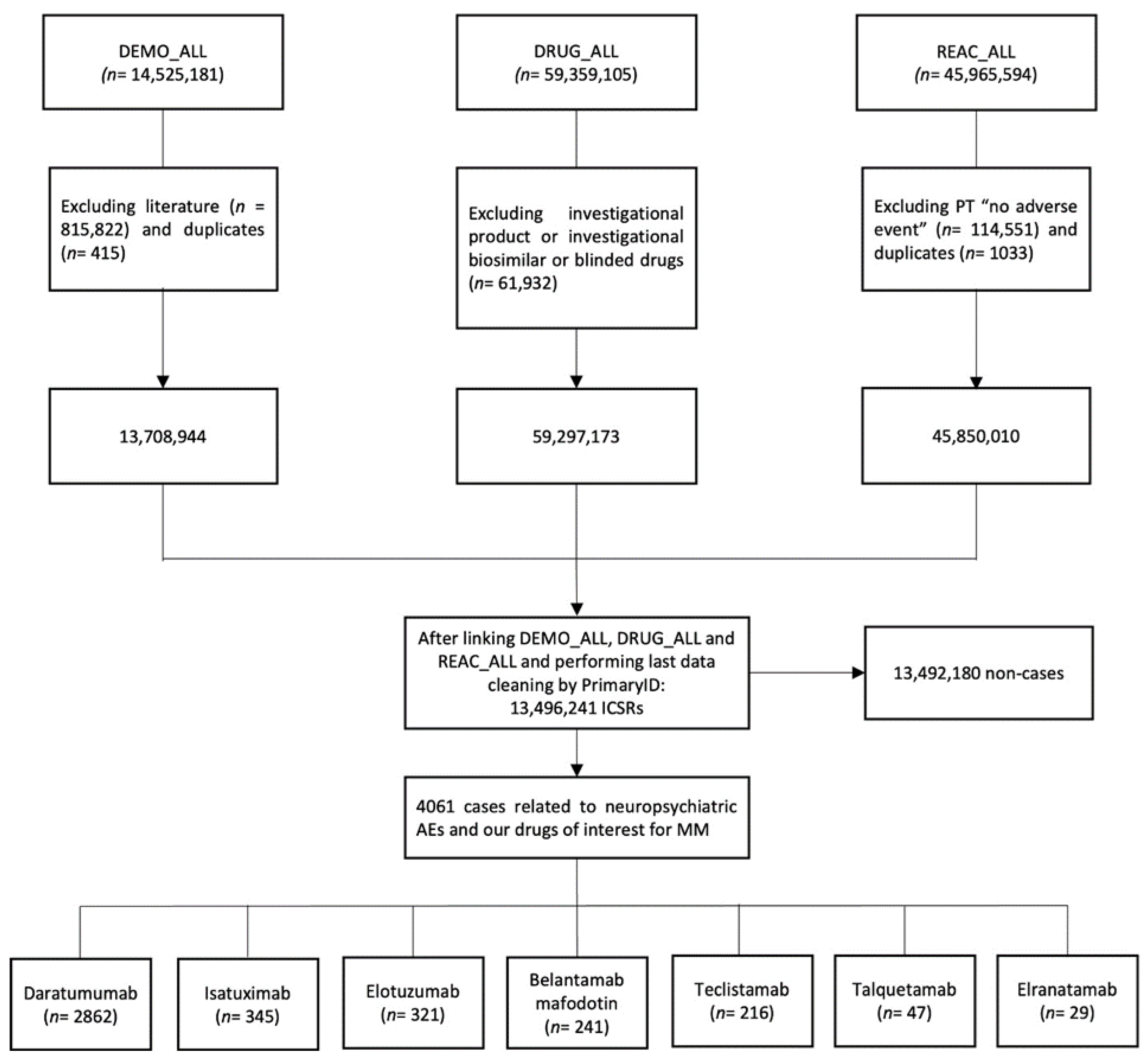
Figure 2.
Time to onset of neuropsychiatric AEs. The data are sorted in descending order of frequency and presented as a box plot, with the box extending from the first quartile (Q1) to the third quartile (Q3), and a horizontal line in the middle representing the median time to onset (TTO).
Figure 2.
Time to onset of neuropsychiatric AEs. The data are sorted in descending order of frequency and presented as a box plot, with the box extending from the first quartile (Q1) to the third quartile (Q3), and a horizontal line in the middle representing the median time to onset (TTO).
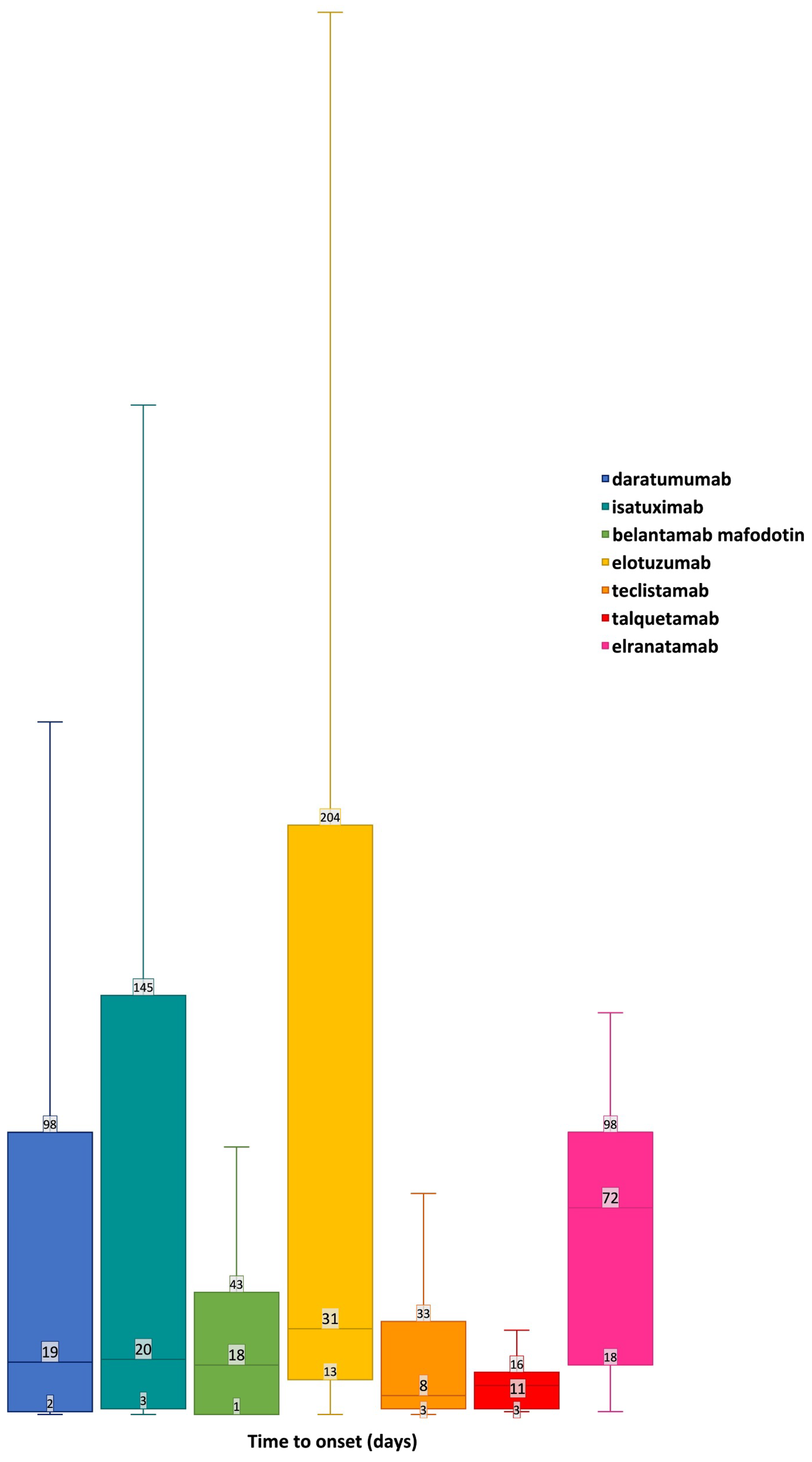

Table 1.
Characteristic of cases related to neuropsychiatric adverse events of monoclonal antibodies approved for multiple myeloma compared to non-cases.
Table 1.
Characteristic of cases related to neuropsychiatric adverse events of monoclonal antibodies approved for multiple myeloma compared to non-cases.
| Characteristic | Neuropsychiatric cases (n= 4061) |
Non-cases (n= 13,492,180) |
Total (n=13,496,241) |
|---|---|---|---|
| Age group, n (%) | |||
| Neonate | 3 (<0.1%) | 39,379 (0.3%) | 39,382 (0.3%) |
| Infants | 15,400 (0.1%) | 15,400 (0.1%) | |
| Child | 7 (0.2%) | 150,436 (1.1%) | 150,443 (1.1%) |
| Adolescent | 10 (0.3%) | 196,410 (1.5%) | 196,420 (1.5%) |
| Adult | 1006 (24.8%) | 4,157,969 (30.8%) | 4,158,975 (30.8%) |
| Elderly | 1947 (47.9%) | 2,895,017 (21.5%) | 2,896,964 (21.5%) |
| Not available | 1088 (26.8%) | 6,037,569 (44.8%) | 6,038,657 (44.7%) |
| Sex, n (%) | |||
| Female | 1588 (39.1%) | 7,145,404 (53.0%) | 7,146,992 (53.0%) |
| Male | 1849 (45.5%) | 4,670,150 (34.6%) | 4,671,999 (34.6%) |
| Not available | 624 (15.4%) | 1,676,626 (12.4%) | 1,677,250 (12.4%) |
| Primary source qualification, n (%) | |||
| Consumers | 580 (14.3%) | 6,659,308 (49.4%) | 6,659,888 (49.4%) |
| Health professional | 685 (16.9%) | 1,185,741 (8.8%) | 1,186,426 (8.8%) |
| Physician | 2114 (52.1%) | 2,801,856 (20.8%) | 2,803,970 (20.8%) |
| Other health-professional | 352 (8.7%) | 1,140,098 (8.5%) | 1,140,450 (8.5%) |
| Pharmacist | 312 (7.7%) | 884,427 (6.6%) | 884,739 (6.6%) |
| Lawyer | 502,463 (3.7%) | 502,463 (3.7%) | |
| Not available | 18 (0.4%) | 318,287 (2.4%) | 318,305 (2.4%) |
| Outcome codification, n (%) | |||
| Death | 351 (8.6%) | 780,158 (5.8%) | 780,509 (5.8%) |
| Disability | 69 (1.7%) | 147,322 (1.1%) | 147,391 (1.1%) |
| Hospitalization - Initial or prolonged | 1397 (34.4%) | 2,090,657 (15.5%) | 2,092,054 (15.5%) |
| Life-threatening | 112 (2.8%) | 143,135 (1.1%) | 143,247 (1.1%) |
| Other serious (Important Medical Event) | 1801 (44.4%) | 4,233,022 (31.4%) | 4,234,823 (31.4%) |
| Required intervention to prevent permanent impairment/damage | 5 (0.1%) | 12,674 (0.1%) | 12,679 (0.1%) |
| Congenital anomaly | 21,535 (0.2%) | 21,535 (0.2%) | |
| Not available | 326 (8.0%) | 6,063,677 (44.9%) | 6,064,003 (44.9%) |
| Reporter Country, n (%) | |||
| Africa | 19 (0.5%) | 37,622 (0.3%) | 37,641 (0.3%) |
| Asia | 635 (15.6%) | 667,858 (5.0%) | 668,493 (5.0%) |
| Central America | 18 (0.4%) | 28,633 (0.2%) | 28,651 (0.2%) |
| Europe | 1668 (41.1%) | 1,749,620 (13.0%) | 1,751,288 (13.0%) |
| North America | 1414 (34.8%) | 10,100,868 (74.9%) | 10,102,282 (74.9%) |
| Oceania | 77 (1.9%) | 95,927 (0.7%) | 96,004 (0.7%) |
| South America | 172 (4.2%) | 227,114 (1.7%) | 227,286 (1.7%) |
| Not available | 58 (1.4%) | 584,538 (4.3%) | 584,596 (4.3%) |
| Year of reporting, n (%) | |||
| 2015 | 17 (0.4%) | 1,239,483 (9.2%) | 1,239,500 (9.2%) |
| 2016 | 251 (6.2%) | 1,300,142 (9.6%) | 1,300,393 (9.6%) |
| 2017 | 250 (6.2%) | 1,356,259 (10.1%) | 1,356,509 (10.1%) |
| 2018 | 414 (10.2%) | 1,616,069 (12.0%) | 1,616,483 (12.0%) |
| 2019 | 471 (11.6%) | 1,628,852 (12.1%) | 1,629,323 (12.1%) |
| 2020 | 469 (11.6%) | 1,681,724 (12.5%) | 1,682,193 (12.5%) |
| 2021 | 535 (13.2%) | 1,706,194 (12.7%) | 1,706,729 (12.7%) |
| 2022 | 748 (18.4%) | 1,628,953 (12.1%) | 1,629,701 (12.1%) |
| 2023 | 906 (22.3%) | 1,334,504 (9.9%) | 1,335,410 (9.9%) |
| Median age (Q1–Q3), years | 69 (61 - 75) | 60 (44 - 71) | 60 (44 - 71) |
| Median weights (Q1–Q3), Kgs | 70 (60 - 85) | 73 (60 - 88) | 73 (60 - 88) |
Table 2.
Disproportionality analyses and notoriety evaluations based on Food and Drug Administration Prescribing Information for neuropsychiatric adverse events related to monoclonal antibodies approved for multiple myeloma.
Table 2.
Disproportionality analyses and notoriety evaluations based on Food and Drug Administration Prescribing Information for neuropsychiatric adverse events related to monoclonal antibodies approved for multiple myeloma.
| Daratumumab | |||||
|---|---|---|---|---|---|
| SOC | PT | N | ROR (95%CI) | IC (IC025-IC075) | Expected in FDA Prescribing Information |
| Nervous system disorders | Neuropathy peripheral | 533 | 5.89 (5.4-6.42) | 2.64 (2.49-2.74) | Uk (peripheral sensory neuropathy) |
| Polyneuropathy | 189 | 17.74 (15.34-20.5) | 4.15 (3.91-4.32) | Uk (peripheral sensory neuropathy) | |
| Syncope | 145 | 1.66 (1.41-1.95) | 1.11 (0.83-1.31) | Yes | |
| Encephalopathy | 71 | 5.07 (4.01-6.41) | 2.48 (2.08-2.76) | Uk (posterior reversible encephalopathy syndrome) | |
| Peripheral sensory neuropathy | 45 | 10.49 (7.81-14.08) | 3.45 (2.96-3.81) | Yes | |
| Cerebral infarction | 45 | 2.39 (1.79-3.21) | 1.54 (1.05-1.9) | No | |
| Depressed level of consciousness | 42 | 1.65 (1.22-2.24) | 1.12 (0.6-1.48) | No | |
| Ischaemic stroke | 33 | 2.24 (1.59-3.15) | 1.47 (0.89-1.88) | No | |
| Altered state of consciousness | 32 | 1.97 (1.39-2.78) | 1.32 (0.73-1.74) | No | |
| Presyncope | 32 | 1.42 (1-2.01) | 0.96 (0.37-1.37) | Yes | |
| Posterior reversible encephalopathy syndrome | 29 | 6.13 (4.25-8.84) | 2.74 (2.12-3.18) | Yes | |
| Nervous system disorder | 28 | 1.69 (1.16-2.45) | 1.15 (0.52-1.59) | Yes | |
| Partial seizures | 27 | 6.77 (4.63-9.89) | 2.87 (2.23-3.33) | No | |
| Leukoencephalopathy | 26 | 14.8 (10.04-21.84) | 3.93 (3.28-4.4) | Uk (posterior reversible encephalopathy syndrome) | |
| Spinal cord compression | 23 | 6.48 (4.29-9.77) | 2.82 (2.12-3.31) | No | |
| Guillain-Barre syndrome | 23 | 6.42 (4.26-9.69) | 2.81 (2.11-3.3) | No | |
| Brain oedema | 20 | 2.51 (1.62-3.9) | 1.62 (0.87-2.14) | Uk (peripheral oedema) | |
| Facial paralysis | 19 | 1.6 (1.02-2.52) | 1.1 (0.33-1.64) | Uk (peripheral sensory neuropathy) | |
| Peripheral sensorimotor neuropathy | 18 | 22.42 (14.02-35.85) | 4.51 (3.72-5.07) | Uk (peripheral sensory neuropathy) | |
| ICANS | 18 | 5.36 (3.37-8.53) | 2.58 (1.79-3.13) | No | |
| Neurotoxicity | 17 | 1.69 (1.05-2.72) | 1.16 (0.35-1.73) | No | |
| Peripheral motor neuropathy | 14 | 14.48 (8.53-24.58) | 3.93 (3.02-4.55) | Uk (peripheral sensory neuropathy) | |
| Incoherent | 12 | 2.61 (1.48-4.61) | 1.68 (0.71-2.35) | No | |
| Orthostatic intolerance | 10 | 12.54 (6.71-23.43) | 3.75 (2.67-4.48) | No | |
| Stupor | 8 | 4.48 (2.23-8.98) | 2.39 (1.18-3.19) | No | |
| Senile dementia | 6 | 10.24 (4.57-22.93) | 3.52 (2.1-4.43) | No | |
| Intracranial mass | 6 | 4.61 (2.07-10.3) | 2.45 (1.04-3.36) | No | |
| Cytotoxic oedema | 5 | 41.17 (16.71-101.45) | 5.44 (3.88-6.42) | Uk (peripheral oedema) | |
| Allodynia | 5 | 8.64 (3.57-20.86) | 3.31 (1.74-4.29) | Uk (nerve damage causing tingling, numbness or pain) | |
| Hyperammonaemic encephalopathy | 5 | 7.57 (3.13-18.26) | 3.13 (1.57-4.11) | Uk (posterior reversible encephalopathy syndrome) | |
| Paraparesis | 5 | 3.69 (1.53-8.89) | 2.18 (0.62-3.17) | Uk (peripheral sensory neuropathy) | |
| Pleocytosis | 4 | 11.42 (4.25-30.68) | 3.72 (1.95-4.8) | No | |
| VIth nerve paralysis | 4 | 6.48 (2.42-17.35) | 2.95 (1.19-4.03) | Uk (nerve damage causing tingling, numbness or pain) | |
| Cerebellar haemorrhage | 4 | 3.04 (1.14-8.11) | 1.97 (0.2-3.04) | No | |
| Loss of proprioception | 3 | 12.5 (3.99-39.14) | 3.89 (1.82-5.1) | No | |
| Cerebellar haematoma | 3 | 11.42 (3.65-35.74) | 3.77 (1.7-4.98) | No | |
| Toxic neuropathy | 3 | 10.67 (3.41-33.38) | 3.68 (1.61-4.88) | Uk (peripheral sensory neuropathy) | |
| Autonomic neuropathy | 3 | 3.93 (1.26-12.21) | 2.34 (0.27-3.55) | Uk (peripheral sensory neuropathy) | |
| Psychiatric disorders | Delirium | 54 | 2.29 (1.75-2.99) | 1.49 (1.04-1.81) | No |
| Mental status changes | 40 | 2.66 (1.95-3.63) | 1.67 (1.14-2.04) | No | |
| Body dysmorphic disorder | 15 | 58.08 (34.3-98.33) | 5.81 (4.94-6.41) | No | |
| Anxiety disorder | 12 | 3.6 (2.04-6.35) | 2.08 (1.1-2.75) | Yes | |
| Belantamab Mafodotin | |||||
| SOC | PT | N | ROR (95%CI) | IC (IC025-IC075) | Expected in FDA Prescribing Information |
| Nervous system disorders | Neuropathy peripheral | 38 | 2.62 (1.9-3.61) | 1.65 (1.11-2.03) | No |
| Altered state of consciousness | 6 | 2.35 (1.05-5.23) | 1.6 (0.19-2.52) | No | |
| Muscle tone disorder | 4 | 59.56 (22.19-159.81) | 6.06 (4.29-7.14) | No | |
| Bell's palsy | 3 | 12.77 (4.11-39.68) | 3.94 (1.87-5.15) | No | |
| Neurological decompensation | 3 | 12.49 (4.02-38.8) | 3.91 (1.84-5.12) | No | |
| Psychiatric disorders | Mental status changes | 10 | 4.23 (2.28-7.88) | 2.3 (1.22-3.03) | No |
| Elranatamab | |||||
| SOC | PT | N | ROR (95%CI) | IC (IC025-IC075) | Expected in FDA Prescribing Information |
| Nervous system disorders | Altered state of consciousness | 3 | 20.7 (6.61-64.83) | 4.6 (2.53-5.81) | Yes |
| Syncope | 3 | 3.82 (1.22-11.98) | 2.29 (0.22-3.5) | Uk (depressed level of consciousness) | |
| Neuropathy peripheral | 3 | 3.6 (1.15-11.28) | 2.22 (0.15-3.42) | Yes | |
| Isatuximab | |||||
| SOC | PT | N | ROR (95%CI) | IC (IC025-IC075) | Expected in FDA Prescribing Information |
| Nervous system disorders | Polyneuropathy | 21 | 9.26 (6.03-14.22) | 3.31 (2.58-3.82) | No |
| Transient ischaemic attack | 17 | 3.37 (2.09-5.42) | 1.98 (1.17-2.55) | No | |
| Ischaemic stroke | 14 | 4.59 (2.71-7.75) | 2.39 (1.48-3.01) | No | |
| Peripheral sensory neuropathy | 11 | 12.23 (6.76-22.13) | 3.72 (2.7-4.42) | No | |
| Cerebral infarction | 10 | 2.56 (1.38-4.76) | 1.67 (0.59-2.4) | No | |
| Cerebral ischaemia | 9 | 12.64 (6.56-24.34) | 3.78 (2.64-4.54) | No | |
| Guillain-Barre syndrome | 8 | 10.72 (5.35-21.48) | 3.57 (2.35-4.37) | No | |
| Haemorrhage intracranial | 7 | 2.76 (1.31-5.79) | 1.79 (0.48-2.64) | No | |
| Basal ganglia infarction | 6 | 132.39 (58.54-299.42) | 7.11 (5.7-8.02) | No | |
| Peripheral motor neuropathy | 6 | 29.61 (13.25-66.18) | 5.01 (3.6-5.92) | No | |
| Subarachnoid haemorrhage | 5 | 2.95 (1.23-7.09) | 1.9 (0.34-2.89) | No | |
| Acute motor-sensory axonal neuropathy | 4 | 93.02 (34.43-251.26) | 6.68 (4.91-7.76) | No | |
| Meningoradiculitis | 3 | 179.87 (56.31-574.58) | 7.64 (5.57-8.85) | No | |
| Chronic inflammatory demyelinating polyradiculoneuropathy | 3 | 11.95 (3.84-37.14) | 3.85 (1.78-5.05) | No | |
| Psychiatric disorders | Acute psychosis | 3 | 8.8 (2.83-27.34) | 3.42 (1.36-4.63) | No |
| Talquetamab | |||||
| SOC | PT | N | ROR (95%CI) | IC (IC025-IC075) | Expected in FDA Prescribing Information |
| Nervous system disorders | Dysgeusia | 13 | 17.71 (10.11-31.02) | 4.16 (3.22-4.8) | Yes |
| ICANS | 7 | 185.55 (87.3-394.35) | 7.59 (6.29-8.44) | Yes | |
| Taste disorder | 7 | 26.81 (12.63-56.93) | 4.82 (3.52-5.68) | Yes | |
| Ageusia | 5 | 18.81 (7.75-45.66) | 4.37 (2.81-5.36) | Yes | |
| Neurotoxicity | 3 | 26.11 (8.35-81.62) | 4.93 (2.86-6.14) | Yes | |
| Teclistamab | |||||
| SOC | PT | N | ROR (95%CI) | IC (IC025-IC075) | Expected in FDA Prescribing Information |
| Nervous system disorders | ICANS | 96 | 450.7 (364.76-556.89) | 8.66 (8.32-8.9) | Yes |
| Neurotoxicity | 22 | 31.49 (20.65-48.02) | 5 (4.29-5.51) | Yes | |
| Polyneuropathy | 5 | 6.45 (2.68-15.53) | 2.92 (1.36-3.91) | Yes | |
| Nervous system disorder | 5 | 4.27 (1.78-10.28) | 2.37 (0.81-3.36) | Yes | |
| Depressed level of consciousness | 5 | 2.79 (1.16-6.71) | 1.83 (0.27-2.82) | Yes | |
| Spinal cord compression | 4 | 15.87 (5.94-42.38) | 4.19 (2.43-5.27) | No | |
| Encephalopathy | 4 | 4.02 (1.51-10.72) | 2.32 (0.56-3.4) | Yes | |
| Unresponsive to stimuli | 4 | 3.44 (1.29-9.19) | 2.13 (0.36-3.21) | Uk (depressed level of consciousness) | |
| Psychiatric disorders | Mental status changes | 5 | 4.7 (1.95-11.31) | 2.5 (0.94-3.48) | Yes |
| Elotuzumab | |||||
| SOC | PT | N | ROR (95%CI) | IC (IC025-IC075) | Expected in FDA Prescribing Information |
| Nervous system disorders | Neuropathy peripheral | 41 | 2.52 (1.85-3.43) | 1.6 (1.08-1.97) | Yes |
| Syncope | 27 | 1.75 (1.2-2.56) | 1.19 (0.55-1.64) | No | |
| Cerebral infarction | 25 | 7.61 (5.13-11.28) | 3.03 (2.37-3.51) | No | |
| Cerebral haemorrhage | 12 | 2.27 (1.29-4) | 1.52 (0.54-2.18) | No | |
| Cerebrovascular disorder | 4 | 16.68 (6.24-44.56) | 4.26 (2.5-5.34) | No | |
| Clumsiness | 4 | 7.82 (2.93-20.86) | 3.21 (1.45-4.29) | Uk (peripheral motor neuropathy) | |
| Orthostatic intolerance | 4 | 28.31 (10.58-75.73) | 5 (3.24-6.08) | No | |
| VIth nerve paralysis | 4 | 36.99 (13.81-99.05) | 5.38 (3.62-6.46) | No | |
| Guillain-Barre syndrome | 3 | 4.74 (1.53-14.7) | 2.59 (0.52-3.8) | No | |
| Intention tremor | 3 | 49.87 (15.97-155.8) | 5.86 (3.79-7.06) | No | |
| Monoplegia | 3 | 4.55 (1.46-14.11) | 2.54 (0.47-3.74) | No | |
| Post herpetic neuralgia | 3 | 11.39 (3.67-35.39) | 3.78 (1.71-4.99) | Uk (herpes zoster) | |
| Spinal cord compression | 3 | 4.78 (1.54-14.83) | 2.6 (0.53-3.81) | No | |
| Toxic encephalopathy | 3 | 6.51 (2.1-20.22) | 3.01 (0.95-4.22) | No | |
| Psychiatric disorders | Delirium | 15 | 3.63 (2.18-6.02) | 2.08 (1.21-2.68) | Uk (mood altered) |
| Listless | 3 | 5.28 (1.7-16.38) | 2.73 (0.66-3.94) | No | |
CI = Confidence Interval; FDA = Food and Drug Administration; IC = Information Component; ICANS = Immune effector Cell-Associated Neurotoxicity Syndrome; PT = Preferred Term; ROR = Reporting Odds Ratio; SOC = System Organ Class; Uk= Unknown.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



