
Submitted:
20 September 2024
Posted:
24 September 2024
You are already at the latest version
Abstract
In Belgium, around a quarter of M. genitalium infections are resistant to both macrolides and fluoroquinolones -termed multi-drug-resistant (MDR) infections. It is unclear what the best treatment is for these infections. We report the first two cases of MDR M. genitalium urethritis treated with combination therapy of minocycline, metronidazole, methenamine and pristinamycin. In both cases, this treatment resulted in microbiological and clinical cure.
Keywords:
M. genitalium
; minocycline
; metronidazole
; methenamine
; pristinamycin
; AMR
Background
Mycoplasma genitalium is becoming increasingly resistant to first- and second-line treatments. In Belgium, the prevalence of macrolide resistance in M. genitalium varies between 100% in men who have sex is 100% and 48% in woman [1]. Around a quarter of infections are resistant to both macrolides and fluoroquinolones -termed multi-drug-resistant (MDR) infections [1]. The European IUSTI treatment guidelines suggests trying doxycycline or minocycline 100 mg BID for 14 days (oral) or pristinamycin 1 g QID for 10 days (oral) [2]. Others have suggested a variety of other treatments such as chloramphenicol, sitafloxacin, and metronidazole or sequential tetracycline followed by azithromycin or moxifloxacin . These treatments, however, fail frequently in MDR infections [2]. Monotherapy, even if sequential leads to the further selection of antimicrobial resistance (AMR). To prevent the emergence of this AMR and to improve treatment success, we have attempted combination therapy for MDR M. genitalium infections. We used a regimen of pristinamycin, minocycline, methenamine and metronidazole. Methenamine-amygdalate is a urinary antiseptic that has been successfully been used to prevent recurrent urinary tract infections [3]. It undergoes hydrolysis in the acidic urine where it is converted into formaldehyde, which exhibits antimicrobial activity by denaturing proteins and nucleic acids within bacterial cells [3]. A daily dose of 2 g of methenamine results in a urine concentration of 18–60 μg/mL of formaldehyde, which exceeds the MICs of urinary pathogens [4]. We gave the methenamine at a dose of 1g QID x 4 weeks. It has been shown to be safe for daily use for at least 12 months [3]. Methenamine has not been evaluated for activity against M. genitalium. It is also not active against intracellular bacteria [3] and since M. genitalium is known to reside intracellularly [5], we considered it unlikely that methenamine would be able to eradicate M. genitalium. We therefore added pristinamycin, minocycline and metronidazole to methenamine-amygdalate for the first 14 days of treatment.
Case 1
Our first case was a 27-year-old man who has sex with men and takes HIV PrEP intermittently. He presented with a urethral discharge in October 2021. Genital examination revealed a purulent urethral discharge. Nucleic acid amplification (NAAT) of a first-void urine specimen was negative for Neisseria gonorrhoeae and Chlamydia trachomatis but positive for M. genitalium. He was treated with doxycycline 100mg twice daily for 7 days for non-gonococcal urethritis with only temporary improvement in his symptoms (Table 1). Over the subsequent two and a half years he was treated with multiple courses of doxycycline, minocycline, azithromycin, moxifloxacin, pristinamycin, chloramphenicol and metronidazole with at best temporary resolution of his symptoms (Table 1; Figure 1). In February 2024 he received triple therapy with minocycline, metronidazole and pristinamycin for 14 days with rapid return of his symptoms 1 day following treatment cessation. In March 2024, we commenced quadritherapy with methanamine, minocycline, metronidazole and pristinamycin as detailed in Table 1. His symptoms resolved within 7 days and have not returned. NAAT testing of his urine in July 2024 was negative for M. genitalium.
At the beginning of his infection, his main-partner was found to be negative for M. genitalium. Since June 2022 he has only had sex with a small number of other men. This sex was receptive oral sex without a condom.
Case 2
The second case was a 56-year-old man who has sex with men and women and takes HIV PrEP intermittently. He presented in January 2024 with dysuria and a purulent urethral discharge. Nucleic acid amplification of a urine specimen was positive for M. genitalium (xx) and negative for Neisseria gonorrhoeae and Chlamydia trachomatis (xx) (Table 2). Various courses of doxycycline, azithromycin, moxifloxacin were administered over the course of the subsequent 6 six months with only temporary symptomatic improvement. Molecular testing confirmed mutations known to cause resistance to macrolides and fluoroquinolones ().
In July 2024 he commenced the same quadritherapy regimen as case one, with resolution of his symptoms within 10 days. A urine NAAT conducted 4 weeks post treatment cessation was negative for M. genitalium. His female main-partner was asymptomatic but her urine tested positive for M. genitalium in January 2024. Resistance testing was not performed. She was treated with sequential azithromycin (500mg day one then 250mg days 2 to 5) and then moxifloxacin 500mg BID x 7 days. A NAAT test performed 1 month after treatment cessation was negative for M. genitalium.
Discussion
In both cases, quadritherapy was associated with the rapid cessation of symptoms and microbiological cure. Both cases had confirmed M. genitalium infections that were resistant to macrolides and fluoroquinolones. Both individuals had tried multiple courses of antimicrobials without success. In the second case, the quadritherapy involved two new treatments – pristinamycin and methenamine – which could have been responsible for treatment success. The only treatment not used prior to quadritherapy in case one was methenamine. The inclusion of methenamine may thus have been important in treatment success for both cases.
Our findings are however based on two case reports and due caution is therefore required. It is possible that the clearance of M. genitalium was due to natural clearance of the infection, due to the sequential antimicrobial therapies or some other factor. Randomized controlled trials are urgently required to build an evidence base for the optimal treatment of MDR M. genitalium. In vitro evaluations of the antimicrobial susceptibility of these agents alone and in combination would also be useful. A key problem here is that methenamine is only active in an acidic milieu [3]. This acidic milieu is however toxic to most of the cell lines used to cultivate M. genitalium [6].
References
- De Baetselier I, Smet H, Kehoe K, Loosen I, Reynders M, Mansoor I, et al. Estimation of antimicrobial resistance of Mycoplasma genitalium, Belgium, 2022. Eurosurveillance. 2024;29(7):2300318.
- Jensen J, Cusini M, Gomberg M, Moi H, Wilson J, Unemo M. 2021 European guideline on the management of Mycoplasma genitalium infections. Journal of the European Academy of Dermatology and Venereology. 2022;36(5):641-50.
- Li JM, Cosler LE, Harausz EP, Myers CE, Kufel WD. Methenamine for urinary tract infection prophylaxis: a systematic review. Pharmacotherapy: The Journal of Human Pharmacology and Drug Therapy. 2024;44(2):197-206.
- Petri, W. Sulfonamides, trimethoprim, sulfamethoxazole, quinolones, and agents for urinary tract infections. Goodman & Gilman’s the pharmacological basis of therapeutics New York (NY): McGraw Hill. 2006:1111-25.
- McGowin CL, Popov VL, Pyles RB. Intracellular Mycoplasma genitalium infection of human vaginal and cervical epithelial cells elicits distinct patterns of inflammatory cytokine secretion and provides a possible survival niche against macrophage-mediated killing. BMC microbiology. 2009;9:1-11.
- Pitt R, Boampong D, Day M, Jensen JS, Cole M. Challenges of in vitro propagation and antimicrobial susceptibility testing of Mycoplasma genitalium. Journal of Antimicrobial Chemotherapy. 2022;77(11):2901-7.
Figure 1.
Time of symptoms, M. genitalium detection and treatments given to case 1.
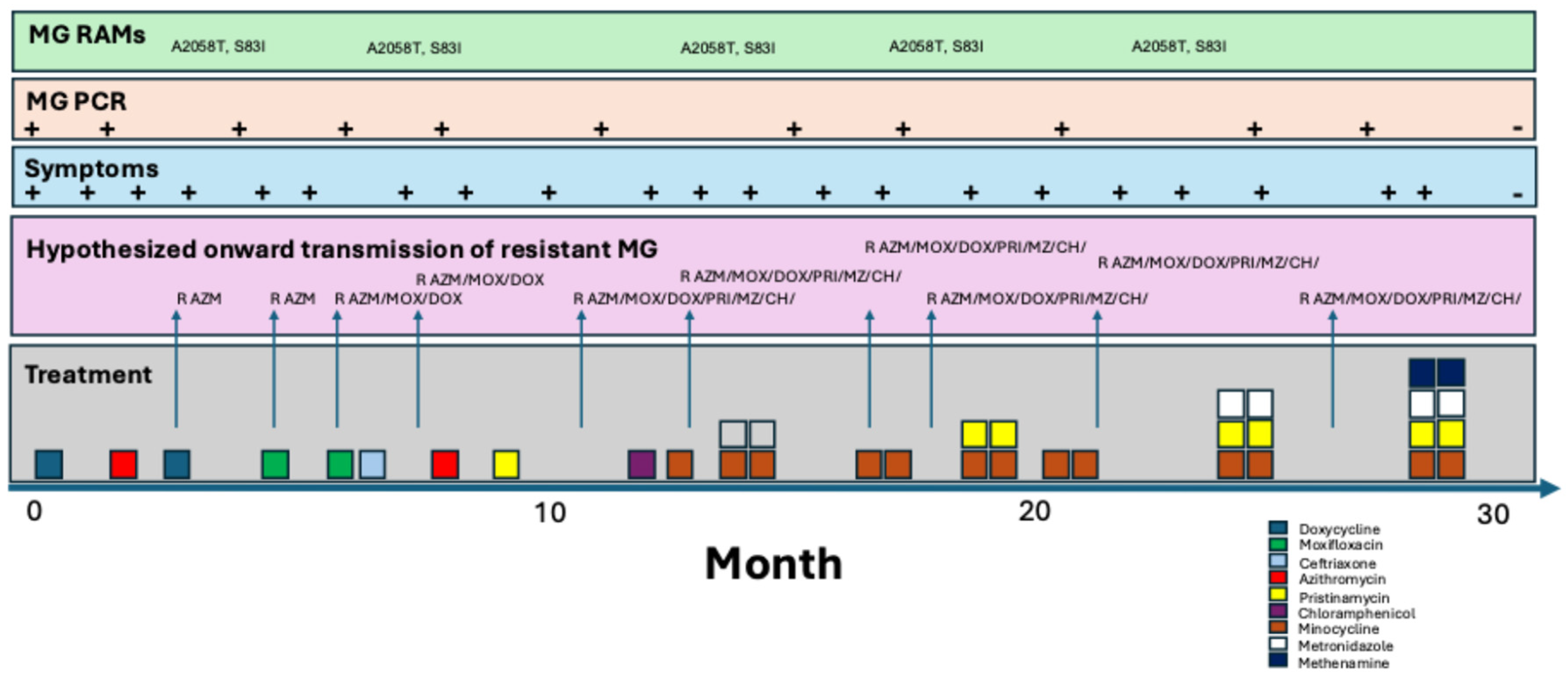

Table 1.
Summary of symptoms, M. genitalium molecular test results and antimicrobial treatments of case 1.
Table 1.
Summary of symptoms, M. genitalium molecular test results and antimicrobial treatments of case 1.
| Date | Symptoms | Micro. (PMN/HPF) | PCR MG | RAMs | Treatment | Outcome |
|---|---|---|---|---|---|---|
| 10/2021 | Subtle DC, dysuria | + | Doxycycline 100mg BID x 7d | Initial improvement but symptoms return 2 days post treatment | ||
| 02/2022 | Subtle DC, dysuria | 5-10 | + | Azithromycin 500mg d1 and 250mg d2-5 | No improvement | |
| 06/2022 | DC, dysuria | + | A2058T, S83I | Doxycycline 100mg BID x 21d | No improvement | |
| 07/2022 | DC, dysuria | + | A2058T, S83I | Moxifloxacin 500mg BID x 10d | Symptoms return 10days post treatment | |
| 08/2022 | DC, dysuria | + | A2058T, S83I | Moxifloxacin 500mg BID x 10d + ceftriaxone 1g IMI (partner had NG) | No improvement | |
| 09/2022 | DC, dysuria | + | Azithromycin 500mg d1 and 250mg d2-5 +BPG 2.4mu (partner had syphilis) | No improvement | ||
| 10/2022 | DC, dysuria | + | A2058T, S83I | Pristinamycin 1g QID x 10d | Symptoms return 21 days post treatment | |
| 12/2022 | DC, dysuria | + | A2058T, S83I | None | ||
| 02/2023 | DC, dysuria | + | Ibuprofen for pain | |||
| 03/2023 | DC, dysuria | 8 | + | Chloramphenicol 1g QID x 14d | ||
| 04/2023 | DC, dysuria | 4 | + | Minocycline 100mg BID x 14d | Symptoms return 20 days post treatment | |
| 05/2023 | DC, dysuria | 10 | + | A2058T, S83I | Minocycline 100mg BID x 14d then metronidazole 500mg TID x 14d | All symptoms resolve except light dysuria x 30 days |
| 08/2023 | DC, dysuria | + | Minocycline 100mg BID x 14d then Pristinamycin 1g QID x 10d | No response | ||
| 11/2023 | DC, dysuria | + | Minocycline 100mg BID x 14d | |||
| 01/2024 | Dysuria | + | Minocycline 100mg BID x 14d | |||
| 02/2024 | DC, dysuria | + | Minocycline 100mg BID x 14d + metronidazole 500mg TID x 14d + Pristinamycin 1g QID x 14d | Symptoms return 1 day post treatment | ||
| 03/2024 | DC, dysuria | + | Minocycline 100mg BID x 14d + metronidazole 500mg TID x 14d + Pristinamycin 1g QID x 14d + methenamine-amygdalate 1g QID x 28d | Symptoms resolve within one week | ||
| 07/2024 | None | 0 | Neg | No symptoms | ||
| 09/2024 | None | No symptoms |
DC – urethral discharge; BID -twice daily; TID -three times daily; QID -four times daily;.
Table 2.
Summary of symptoms, M. genitalium molecular test results and antimicrobial treatments of case 2.
Table 2.
Summary of symptoms, M. genitalium molecular test results and antimicrobial treatments of case 2.
| Date | Symptoms | Micro. (PMN/HPF) | PCR MG | RAMs | Treatment | Outcome |
|---|---|---|---|---|---|---|
| 01/2024 | DC, dysuria | 15+ | + | Doxycycline 100mg BID x 7d then azithromycin 500mg d1 and 250mg d2-5 | No improvement | |
| 02/2024 | DC, dysuria | 5-10 | + | Doxycycline 100mg BID x 21d, then then Moxifloxacin 500mg BID x 7d | Symptoms return 1 day post treatment | |
| 03/2024 | DC, dysuria | + | Azithromycin 2.5g over 4d then Moxifloxacin 500mg BID x 7d | No improvement | ||
| 04/2024 | DC, dysuria | Doxycycline 100mg BID x 7d then Moxifloxacin 500mg BID x 10d | Symptoms return 10 days post treatment | |||
| 05/2024 | DC, dysuria | + | Doxycycline 100mg BID x 14d then Azithromycin 500mg d1 and 250mg d2-5 then metronidazole 500mg TID x 7d | No improvement | ||
| 06/2024 | DC, dysuria | + | Doxycycline 100mg BID x 28d | No improvement | ||
| 07/2024 | DC, dysuria | + | Minocycline 100mg BID x 14d + metronidazole 500mg TID x 14d + Pristinamycin 1g QID x 14d + methenamine-amygdalate 1g QID x 28d | Symptoms resolve within 10days of starting treatment | ||
| 09/2024 | None | 0 | - | None | No symptoms |
DC – urethral discharge; BID -twice daily; TID -three times daily; QID -four times daily;.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



