
Submitted:
20 September 2024
Posted:
23 September 2024
You are already at the latest version
Abstract
Background and Objectives: Fifty percent of individuals with borderline personality disorder (BPD) experience Non-Suicidal Self-Injury (NSSI). One of the crucial factors related to NSSI is the feeling of emptiness. Although some inner strengths, such as five precepts, meditation, and equanimity, have been identified as potential buffers against negative mental health outcomes in BPD, their role in mediating the relationship between emptiness and NSSI is not well-documented. This study aimed to explore how these inner strengths mediate the relationship between feelings of emptiness and NSSI in individuals with BPD symptoms. Materials and Methods: A total of 302 participants with BPD symptoms completed several assessments: the SCID-II Personality Disorder (Borderline PD) to assess feelings of emptiness and NSSI, the Inner-Strength-Based Inventory (i-SBI) to evaluate five precepts, meditation, and equanimity, and the Outcome Inventory Depression (OI-Dep) to assess depression. Mediation analysis was performed using IBM SPSS and AMOS, with NSSI as the outcome variable, feelings of emptiness as the predictor, and the inner strengths as mediators. Results: The participants had a mean age of 36.56, with 65.4% being female. The analysis showed that five precepts, meditation, and equanimity significantly mediated the relationship between feelings of emptiness and NSSI, with a standardized coefficient of β = 0.534 (95% CI = 0.417 to 0.647, p < 0.001). The indirect effect of emptiness through these inner strengths was significant (β = 0.034, 95% CI = 0.009 to 0.075, p = 0.005). The mediation model explained 38% of the variance in NSSI with a 3% increase, albeit small but significant. Conclusions: The study highlights a negative mediating role of inner strengths in the relationship between feelings of emptiness and NSSI meaning that as these inner strengths increase, the direct impact of feelings of emptiness on NSSI decreases. This suggests that these inner strengths act as protective factors, reducing the likelihood that someone with feelings of emptiness will resort to NSSI as a coping mechanism. These findings suggest that targeting these inner strengths could be a valuable strategy in developing interventions aimed at reducing NSSI by addressing the underlying emotional challenges associated with BPD.
Keywords:
emptiness
; non-suicidal self-injury
; borderline personality disorder symptoms
; five precepts
; meditation
; equanimity
1. Introduction
Non-suicidal self-injury (NSSI), or self-mutilation, refers to the deliberate, direct destruction or alteration of one's body tissue without conscious suicidal intent. It is common in Borderline Personality Disorder (BPD), a psychiatric condition characterized by unstable interpersonal relationships, fear of abandonment, difficulties in emotion regulation, feelings of emptiness, chronic dysphoria, depression, impulsivity, and heightened risk-taking behaviors. BPD can be understood as stemming from difficulties in early dyadic regulation with primary caregivers, such as early insecure attachment (preoccupied or dismissive), which results in under-regulation of emotions and fear of abandonment [1,2]. In Thailand, the prevalence of BPD among Thai students has been reported as 6.4% [3]. Many patients with BPD exhibit recurring self-injurious or suicidal behavior [4]. Studies discovered that NSSI occurs in 50 to 80% of cases, and is frequently repetitive, with more than 41% of patients engaging in over 50 instances of self-mutilation. The most common form of self-mutilation behavior is cutting. This behavior can relieve negative mood states, reduce distress, elicit care from others, express emotions symbolically, or help patients emerge from dissociation and feel more alive. Despite that, self-mutilation is a significant risk factor for suicide in BPD, with the suicide rate being about twice as high as that of individuals without NSSI. Repetitive self-mutilation may increase dysphoria, leading to greater feelings of depression and hopelessness. Individuals may become more aggressive, display more affective instability, and experience suicidal thoughts more frequently and for longer periods. [5,6,7,8].
Another symptom found in BPD is emptiness, which is more strongly correlated with greater borderline pathology than any other BPD symptoms [9] and is the diagnostic criterion of BPD associated with suicidal and self-injurious behaviors [10].This feeling of emptiness is a complex, negative emotional state that varies among individuals. It may include a physical or bodily component, a sense of aloneness or social disconnectedness, and a deep sense of personal unfulfillment, lack of purpose, dysphoria, boredom, loneliness, and numbness. Research has found that a typical manifestation of emptiness includes a sense of going through life mechanically, purposelessly, and numbly, accompanied by a psychological and bodily inner void, a sense of disconnectedness from others, and a perception[11]. Responses to feelings of emptiness vary[12]. Additionally, findings suggest that emptiness reflects pathological affect and significant psychiatric distress [13]. It contributes to functional impairment, such as lower social functioning, and may help differentiate BPD from other disorders, such as major depressive disorder [14,15]. The feeling of emptiness can lead to non-suicidal self-injury and may also have a significant relationship with suicidality [16]. Higher levels of emptiness predict higher baseline suicide urges; thus, assessing and targeting emptiness may facilitate the reduction of suicide urges in BPD [10]. Evidence has shown that among the individual BPD symptoms, past suicidality, impulsivity, chronic emptiness, and identity disturbance were each significantly and positively associated with a lifetime history of non-suicidal self-injury [17]. BPD patients exhibit deficits in mindfulness, self-compassion, and adaptive emotion-regulation strategies [18]. Non-suicidal self-injury (NSSI) that relates to suicide attempts is related to impulse and emotion dysregulation (cognitive-emotional model), as well as deficits in mindfulness skills, which are also key difficulties in BPD (emotional cascade model, mindfulness deficit theory)[19]. Mindfulness was negatively correlated with NSSI and found to mediate the relationship between depressive symptoms and NSSI partially [20]. A deficit in mindfulness, characterized by difficulty being aware, attentive, and accepting of ongoing experiences, may contribute to the relationship between BPD features and self-injury, as well as overall harmful dysregulated behaviors and suicidal ideation [21,22].
Many studies have supported the effect of meditation or mindfulness on BPD in reducing psychological symptoms and emotional reactivity and improving behavioral regulation [23,24,25].
Mindfulness enhances awareness of emptiness, helps identify related emotions, thoughts, feelings, and experiences, promotes observation through decentering, and improves reflection on cognitive functioning and dysfunctional behaviors[26]. However, a study of the mediators or moderators between emptiness and NSSI is limited.
One study demonstrated that mindfulness and emotion dysregulation mediated the relationship between emptiness and NSSI history. In that, the chronic emptiness had significant indirect effects on self-harm through the mindfulness aspect of strategies, describing, and clarity[19,27]. In addition to mindfulness and emotional regulation, other positive psychological factors are rarely investigated. A related study conducted by Pongpitpitak and colleagues demonstrated that perseverance and meditation were found to be significant moderators for borderline personality disorder symptoms and depression[28].
As the majority of Thais are Buddhists, meditation, which is part of the Ten Perfection, is a significant practice to increase inner strength[29]. However, meditation and mindfulness are not the only practices. Five precepts, which include abstaining from killing, stealing, sexual misconduct, lying, and the consumption of alcohol and other intoxicants, are essential practices along with meditation and found to promote mental health [30,31]. The practice of five precepts has never been explored among borderline individuals. Other than meditation and the five precepts, there are truthfulness, perseverance, wisdom, generosity, patience and endurance, equanimity, determination, and loving-kindness, which are related to positive mental health and a protective factor against mental health problems [29,32]
Along with mindfulness, equanimity, a state of psychological stability and composure that remains undisturbed by emotions, pain, or other circumstances— represents a balanced emotional reaction toward stimuli, accompanied by a tolerant and nonjudgmental attitude toward others [33]. It is a crucial psychological component for enhancing well-being, and meditation techniques exist for cultivating it [34]. Equanimity typically co-occurs with mindfulness. Buddhism emphasizes cultivating equanimity as a virtuous state of mind rooted in freedom [35]. Studies show that equanimity correlates with improved emotional regulation [36,37], decreased anxiety and depression[38], and moderates the relationship between perceived stress, neuroticism, and depressive symptoms [39]. Furthermore, equanimity mediates the impact of perceived social isolation on psychological distress, providing protection against its negative effects [40]. As individuals with BPD have a central problem with emotional regulation, therefore practicing five precepts, meditation, and equanimity may theoretically have a promising impact on BPD symptoms, including the frequency of NSSI, as all these methods promote self-control and emotional stability and regulation. The study’s objective was to investigate these particular strengths, namely, precepts, meditation, and equanimity, to see whether they had a mediating effect on the relationship between feelings of emptiness in patients with BPD symptoms and NSSI among patients attending a psychotherapy clinic. The authors hypothesize that at a high level of precepts, meditation, and equanimity, the effects of feelings of emptiness NSSI should be mitigated. Additionally, since depression is associated with both BPD and NSSI, we will control for depression to avoid confounding factors.
2. Materials and Methods
2.1. Study Design and Sample Size Calculation
This study employed a retrospective cross-sectional design, Using data from the psychotherapy clinic database from November 2011 to August 2022 in Thailand. Estimated Power and Sample Size calculation was carried out for the mediation analysis model [41]. Two parallel mediators with a correlation coefficient of variables (Power (beta) = 0.8 (80%), Correlation coefficient (r) of emptiness, and NSSI = 0.39) yielded a sample size of 96, target power = 0.8 (95% CI = 0.77-0.83), Ethics review and approval were obtained from the Faculty of Medicine, Chiang Mai University, Thailand (study code, PSY-2566-0414; date of approval, 26 December 2023).
2.2. Participants and Setting
All 337 participants' data stored in the database were used. These participants were the patients who attended the psychotherapy clinic from November 2011 to August 2022, aged 20 years old and above, able to speak Thai and both genders (other). The exclusion criteria included those without clinical diagnosis (Axis I) and without DSM personality disorder diagnosis (Axis II). Thirty-five participants had incomplete reports; therefore, 302 participants with borderline personality disorder symptoms (BPD symptoms) were used for the final analysis.
2.3. Measurements
2.3.1. Medical Record for Sociodemographic Data Such as Age, Sex, and Axis I (Clinical Disorder)
2.3.2. The SCID-II Personality Disorder (Borderline PD)
The SCID-II Personality Disorder (Borderline PD) had a structured format covering ten standard DSM-IV personality disorders. The Thai version was found to have good and excellent reliability ( The mean trait intraclass correlation coefficient score was 0.90, and the summed score was 0.83) [42]
2.3.3. Inner-Strength-Based Inventory (I-SBI)
The I-SBI measures ten positive behavioral characteristics inspired by the Buddhist ten perfections: generosity, morality, mindfulness, meditation, wisdom, perseverance, patience and endurance, truthfulness, determination, loving-kindness, and equanimity. Each characteristic has multiple-choice responses along a 5-point scale. The scores of I-SBI range from 5 to 50. Higher scores reflect those characteristics, and each subscale can be used separately[29,43]. Items five precepts, meditation, and equanimity were used in this analysis.
2.3.4. Outcome Inventory-21
The OI-21 consists of 21 questions with anxiety, depression, interpersonal difficulties, and somatization subscales. All of these were based on a 5-point Likert scale, including values of 1 (never), 2 (rarely), 3 (sometimes), 4 (frequently), and 5 (almost always). The scores range from 0 to 48. The higher the score, the higher the level of psychopathology.[44]. OI-Depression (OI-Dep) -items 2,5,14,18, and 21 were used in this analysis. Cronbach’s alpha for this study was 0.86.
2.4. Statistical Analysis
Descriptive statistics were used for the demographic data from medical records, such as age, gender, education, and marital status. Mean and standard deviation were used for continuous variables such as age and the score of the Outcome Inventory Depression (OI-Dep). A t-test was used to evaluate the mean differences of the continuous type of variables between the group of NSSI and the group without NSSI. NSSI was obtained from the self-harm items in the SCID-II Personality Disorder of Borderline PD. Chi-square tests were used to test the difference between categorical variables with three or more levels, such as education. Correlation analysis and linear regression analysis were applied to continuous variables. Pearson’s correlation was used to examine the relationships between the Inner-Strength-Based Inventory (I-SBI) and OI-Dep.
Mediation analyses were conducted to examine the significant correlations between feeling emptiness in borderline personality disorder symptoms (X), The five precepts, meditation, and equanimity, were considered M1-M3, and NSSI was the outcome (Y). Both direct and indirect effects of the feeling of emptiness on the outcome were assessed and should be significant. 5000 resampling or bootstrapping methods were applied to produce more accurate mediation analysis results. Standardized regression coefficients (β) and p-values were reported for direct effect coefficients, and bootstrap confidence intervals were reported for conditional indirect effects. Confidence intervals that do not include zero indicate statistical significance. All statistical analyses were performed using the IBM SPSS Program, Version 25.0, and AMOS, Version 24 (IBM Corp., Armonk, NY, USA). The level of significance for all analyses was set at p < 0.05.
3. Results
Among all participants, most were female. The mean and standard deviation of the measurement scores are shown in Table 1. Significant age differences, feelings of emptiness, perceived stress, and Outcome Inventory Depression (OI-Dep) were found between the NSSI and Non-NSSI groups. Feelings of emptiness were higher in the NSSI group.
Table 2 shows the correlation coefficients between each pair of variables. The correlations were as follows: emptiness and NSSI (0.591), Outcome Inventory Depression (OI-Dep) was positively correlated with emptiness, and NSSI (all p < 0.01)
The correlation between emptiness was negatively related to five precepts, meditation, and equanimity (p <0.01). Similarly, NSSI was negatively associated with five precepts, meditation and equanimity (p <0.01).
The standardized regression coefficient for the effect of emptiness on NSSI was β = 0.591 (95% CI = 0.543 to 0.742, p < 0.001). Table 3 shows that when controlling for age and Outcome Inventory Depression (OI-Dep), the regression coefficient for the effect of emptiness on NSSI was reduced to β = 0.565 (95% CI = 0.507 to 0.721, p < 0.001). Even with these controls, the relationship between emptiness and NSSI remained significant. This model explained 35% of the variance in NSSI.
Based on the correlations among variables, we hypothesized a mediation model. Five precepts, meditation and equanimity, were entered as mediators in the relationship between emptiness and non-suicidal self-injury (NSSI), with NSSI as the dependent variable. The analysis assessed the effects of emptiness on NSSI, both directly and indirectly, through the five precepts, meditation, and equanimity—the mediation model controlled for age and Outcome Inventory Depression (OI-Dep). The standardized total effect of emptiness on NSSI was β = 0.568 (95% CI = 0.453 to 0.675, p < 0.001).
Figure 1 shows the standardized estimation coefficients for the direct effects of emptiness on NSSI. The direct impact of emptiness was reduced from β = 0.565 (95% CI = 0.507 to 0.721, p < 0.001) to β = 0.534 (95% CI = 0.417 to 0.647, p < 0.001) when controlling for the mediators. The predictors in the mediation model explained 38% of the variance in NSSI.
Table 4 shows the direct effects of emptiness on the five precepts, meditation, equanimity, and NSSI. It also presents the direct effects of the five precepts, meditation, and equanimity on NSSI. The indirect effect of emptiness on NSSI was β = 0.034 (95% CI = 0.009 to 0.075, p = 0.005) (Table 5). For each variable of inner strength, meditation was correlated with the five precepts (r = 0.35) and equanimity (r = 0.10).
4. Discussion
This study investigated how the five precepts, meditation, and equanimity mediate the relationship between emptiness and NSSI. The findings highlight the significantly indirect effect of the feeling of emptiness on NSSI through these inner strengths among individuals with BPD symptoms. A negative mediating role suggested that as these inner strengths increase, the direct impact of feelings of emptiness on NSSI decreases. In other words, more potent inner resources—like adherence to five precepts, regular meditation, and equanimity—weaken the connection between feeling empty and engaging in NSSI. This suggests that these inner strengths may act as protective factors, reducing the likelihood that someone feeling emptiness will resort to NSSI as a coping mechanism. In this context, inner strengths help buffer or diminish emotional emptiness's impact on the likelihood of engaging in NSSI.
The fact that meditation and precepts may help individuals become more aware and attentive and control their negative experiences, as found in individuals with BPD symptoms[21]. Though no direct study can be referred to, the related studies have demonstrated that meditation and the five precepts on the relationship between secure attachment and resilience [31]. Additionally, the five precepts are associated with higher levels of happiness [30], and is negatively related to aggression, neuroticism, and sensation-seeking [32], whereas equanimity was linked to decreased anxiety and depression, and it mitigates the effects of perceived stress on depression [38,39]. All inner strengths combined demonstrated the significant indirect effect of the feeling of emptiness on NSSI. Regarding the relationship between feelings of emptiness and NSSI, the findings are consistent with the related studies[9,17].
Implication of the Study and Future Research
Inner strength—encompassing the five precepts, meditation, and equanimity—that can help prevent NSSI may be developed through various methods. Often, patients learn to cultivate these strengths on many occasions in their daily lives, with a focus on promoting equanimity in individuals with BPD. Five precepts and equanimity ( a part of four immeasurables) are common practices along with meditation in Thailand, which are considered methods to enhance mental well-being.
In a clinical setting, these activities can be suggested. Patients with BPD symptoms may be encouraged to engage in meditation practices and follow the five precepts (which include abstaining from killing, stealing, sexual misconduct, lying, and the consumption of alcohol) as part of supplementary activities of psychotherapeutic intervention.
Future research should be encouraged among individuals with BPD in different cultures, as inner strength is considered a universal concept. More robust research should be conducted on proving whether providing training in equanimity, the five precepts, and meditation among patients with BPD symptoms, particularly those experiencing feelings of emptiness, can help prevent NSSI behavior.
Strengths and Limitation
To the best of our knowledge, this study is one of the first to demonstrate the beneficial role of five precepts, meditation, and equanimity in relation to NSSI among individuals with BPD symptoms experiencing feelings of emptiness. However, there are several limitations that should be addressed. Firstly, the patients with BPD symptoms populations were categorized using the SCID-II Personality Disorder (Borderline PD) rather than clinical diagnoses, which may lead to false-positive cases. Secondly, social desirability bias in self-reports may be unavoidable, and thus the interpretation of the results should be cautiously approached. Thirdly, our data cannot exclude participants who are currently receiving psychological treatment, which may have influenced reductions in NSSI and increases in inner strength due to therapy. Fourthly, this study was conducted in Thailand, and cultural factors might have influenced the outcomes, particularly those related to inner strength. Therefore, replication studies in other countries are warranted. Finally, due to the retrospective cross-sectional design of this study, causal inferences cannot be confirmed; a longitudinal design would be more appropriate for establishing causality.
5. Conclusions
The present study has demonstrated a positive correlation between feelings of emptiness and non-suicidal self-injury (NSSI). Conversely, inner strength, the five precepts, meditation, and equanimity significantly mediate the relationship between feelings of emptiness in individuals with borderline personality disorder symptoms (BPD symptoms) and NSSI, showing a negative association. This novel evidence provides guidance for helping individuals with BPD symptoms who experience feelings of emptiness manage NSSI more effectively.
Author Contributions
Conceptualization, P.S., T.W., and N.W.; methodology, P.S., T.W., and N.W.; software, T.W.; validation, T.W., and N.W.; formal analysis, P.S. and T.W.; investigation, P.S.; resources, T.W. and N.W.; data curation, P.S.; writing—original draft preparation, P.S.; writing—review and editing, T.W. and N.W.; visualization, P.S.; supervision, T.W. and N.W.; project administration, T.W. and N.W.; funding acquisition, P.S. All authors have read and agreed to the polished version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was approved by the research ethics committee of the Faculty of Medicine, Chiang Mai University (protocol code PSY-2566-0414 and date of approval 26 December 2023).
Informed Consent Statement
Patient consent was waived due to the study being a retrospective cross-sectional analysis.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Acknowledgments
We are grateful to all the patients who attended the psychotherapy clinic and participated in this study. The authors also thanked their research assistants.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Mosquera, D., A. Gonzalez, and A.M. Leeds, Early experience, structural dissociation, and emotional dysregulation in borderline personality disorder: the role of insecure and disorganized attachment.
- van Dijke, A. and J.D. Ford, Adult attachment and emotion dysregulation in borderline personality and somatoform disorders.
- Lohanan, T., et al., Development and validation of a screening instrument for borderline personality disorder (SI-Bord) for use among university students. BMC Psychiatry, 2020. 20(1): p. 479. [CrossRef]
- Brüne, M., Borderline Personality Disorder: Why 'fast and furious'? Evol Med Public Health, 2016. 2016(1): p. 52-66. [CrossRef]
- Urnes, O., [Self-harm and personality disorders]. Tidsskr Nor Laegeforen, 2009. 129(9): p. 872-6. [CrossRef]
- Nitkowski, D. and F. Petermann, [Non-suicidal self-injury and comorbid mental disorders: a review]. Fortschr Neurol Psychiatr, 2011. 79(1): p. 9-20. [CrossRef]
- Oumaya, M., et al., [Borderline personality disorder, self-mutilation and suicide: literature review]. Encephale, 2008. 34(5): p. 452-8. [CrossRef]
- Reichl, C. and M. Kaess, Self-harm in the context of borderline personality disorder. Curr Opin Psychol, 2021. 37: p. 139-144. [CrossRef]
- Martin, J.A. and K.N. Levy, Chronic feelings of emptiness in a large undergraduate sample: Starting to fill the void. Personal Ment Health, 2022. 16(3): p. 190-203. [CrossRef]
- Fulham, L., J. Forsythe, and S. Fitzpatrick, The relationship between emptiness and suicide and self-injury urges in borderline personality disorder. Suicide Life Threat Behav, 2023. 53(3): p. 362-371. [CrossRef]
- Herron, S.J. and F. Sani, Understanding the typical presentation of emptiness: a study of lived-experience. J Ment Health, 2022. 31(2): p. 188-195. [CrossRef]
- Miller, C.E., M.L. Townsend, and B.F.S. Grenyer, Understanding chronic feelings of emptiness in borderline personality disorder: a qualitative study. Borderline Personal Disord Emot Dysregul, 2021. 8(1): p. 24. [CrossRef]
- Klonsky, E.D., What is emptiness? Clarifying the 7th criterion for borderline personality disorder. J Pers Disord, 2008. 22(4): p. 418-26. [CrossRef]
- Elsner, D., J.H. Broadbear, and S. Rao, What is the clinical significance of chronic emptiness in borderline personality disorder? Australas Psychiatry, 2018. 26(1): p. 88-91. [CrossRef]
- Miller, C.E., et al., Measuring the shadows: A systematic review of chronic emptiness in borderline personality disorder. PLoS One, 2020. 15(7): p. e0233970. [CrossRef]
- D'Agostino, A., et al., The Feeling of Emptiness: A Review of a Complex Subjective Experience. Harv Rev Psychiatry, 2020. 28(5): p. 287-295. [CrossRef]
- Brickman, L.J., et al., The relationship between non-suicidal self-injury and borderline personality disorder symptoms in a college sample. Borderline Personality Disorder and Emotion Dysregulation, 2014. 1(1): p. 14. [CrossRef]
- Salgó, E., et al., Emotion regulation, mindfulness, and self-compassion among patients with borderline personality disorder, compared to healthy control subjects. PLoS One, 2021. 16(3): p. e0248409. [CrossRef]
- Kresznerits, S., Á. Zinner-Gérecz, and D. Perczel-Forintos, [Borderline personality disorder and non-suicidal self-injury: the role of mindfulness training in risk reduction]. Psychiatr Hung, 2023. 38(2): p. 142-152.
- Heath, N.L., et al., The Relationship Between Mindfulness, Depressive Symptoms, and Non-Suicidal Self-Injury Amongst Adolescents. Arch Suicide Res, 2016. 20(4): p. 635-49. [CrossRef]
- Wupperman, P., et al., Borderline personality features and harmful dysregulated behavior: the mediational effect of mindfulness. J Clin Psychol, 2013. 69(9): p. 903-11. [CrossRef]
- Shorey, R.C., et al., The relationship between dispositional mindfulness, borderline personality features, and suicidal ideation in a sample of women in residential substance use treatment. Psychiatry Res, 2016. 238: p. 122-128. [CrossRef]
- Feliu-Soler, A., et al., Fostering Self-Compassion and Loving-Kindness in Patients With Borderline Personality Disorder: A Randomized Pilot Study. Clin Psychol Psychother, 2017. 24(1): p. 278-286. [CrossRef]
- Keng, S.L. and J.X. Tan, Effects of brief mindful breathing and loving-kindness meditation on shame and social problem solving abilities among individuals with high borderline personality traits. Behav Res Ther, 2017. 97: p. 43-51. [CrossRef]
- Tortella-Feliu, M., et al., Relationship between effortful control and facets of mindfulness in meditators, non-meditators and individuals with borderline personality disorder. Personal Ment Health, 2018. 12(3): p. 265-278. [CrossRef]
- Didonna, F.a.G.Y., Mindfulness and Feelings of Emptiness. 2009. 125-151.
- Natividad, A., et al., What aspects of mindfulness and emotion regulation underpin self-harm in individuals with borderline personality disorder? J Ment Health, 2024. 33(2): p. 141-149. [CrossRef]
- Pongpitpitak, N., et al., Buffering Effect of Perseverance and Meditation on Depression among Medical Students Experiencing Negative Family Climate. Healthcare (Basel), 2022. 10(10). [CrossRef]
- Wongpakaran, N., T. Wongpakaran, and P. Kuntawong, Development and Validation of the inner Strength-Based Inventory (SBI). Mental Health, Religion & Culture, 2020. 23(3-4): p. 263-273. [CrossRef]
- Winzer, L., B. Samutachak, and R. Gray, Religiosity, Spirituality, and Happiness in Thailand from the Perspective of Buddhism. Journal of Population and Social Studies, 2018. 26: p. 332-343. [CrossRef]
- DeMaranville, J., et al., Meditation and Five Precepts Mediate the Relationship between Attachment and Resilience. Children (Basel), 2022. 9(3). [CrossRef]
- Kövi, Z., et al., Relationship between Personality Traits and the Inner Strengths. Psychiatr Danub, 2021. 33(Suppl 4): p. 844-849.
- Thavaro, V., Handbook of meditation practice. 1982, Chuanpim Bangkok, Thailand:.
- Desbordes, G., et al., Moving beyond Mindfulness: Defining Equanimity as an Outcome Measure in Meditation and Contemplative Research. Mindfulness (N Y), 2014. 2014(January): p. 356-72. [CrossRef]
- Maurer, B.T., Evaluating the patient with a measure of equanimity. JAAPA, 2009. 22(12): p. 56.
- Giluk, T.L., Mindfulness, Big Five personality, and affect: A meta-analysis. Personality and Individual Differences, 2009. 47(8): p. 805-811. [CrossRef]
- Ostafin, B.D., M.D. Robinson, and B.P. Meier, Introduction: The science of mindfulness and self-regulation. Handbook of mindfulness and self-regulation, 2015: p. 1-6. [CrossRef]
- Kwok, J.Y.Y., et al., Effects of Mindfulness Yoga vs Stretching and Resistance Training Exercises on Anxiety and Depression for People With Parkinson Disease: A Randomized Clinical Trial. JAMA Neurol, 2019. 76(7): p. 755-763. [CrossRef]
- Wongpakaran, N., et al., Role of Equanimity on the Mediation Model of Neuroticism, Perceived Stress and Depressive Symptoms. Healthcare (Basel), 2021. 9(10). [CrossRef]
- Mann, L.M. and B.R. Walker, The role of equanimity in mediating the relationship between psychological distress and social isolation during COVID-19. J Affect Disord, 2022. 296: p. 370-379. [CrossRef]
- Schoemann, A., A. Boulton, and S. Short, Determining Power and Sample Size for Simple and Complex Mediation Models. Social Psychological and Personality Science, 2017. 8: p. 194855061771506. [CrossRef]
- Wongpakaran, T., et al., Interrater reliability of Thai version of the Structured Clinical Interview for DSM-IV Axis II Personality Disorders (T-SCID II). J Med Assoc Thai, 2012. 95(2): p. 264-9.
- Wongpakaran, N., et al., Moderating role of observing the five precepts of Buddhism on neuroticism, perceived stress, and depressive symptoms. PLOS ONE, 2022. 17(11): p. e0277351. [CrossRef]
- Wongpakaran, N., T. Wongpakaran, and Z. Kövi, Development and validation of 21-item outcome inventory (OI-21). Heliyon, 2022. 8(6): p. e09682. [CrossRef]
Figure 1.
Mediation model of feeling of emptiness in patients with borderline personality disorder symptoms (BPD symptoms), with five precepts, meditation, equanimity and non-suicidal self-injury (NSSI), adjusted for age and OI-Depression. X=Predictor; M1, M2, M3= Mediator; Y= Outcome; a1, a2, a3, b1, b2, b3, c, c’ = Path coefficients; c= Total direct effect of emptiness on NSSI; c’ = Direct effect of emptiness on NSSI mediating by five precepts, meditation, equanimity. Value for NSSI (Y) are the R-square. NSSI = non-suicidal self-injury. * p<0.05, ** p<0.01, ***p<0.001.
Figure 1.
Mediation model of feeling of emptiness in patients with borderline personality disorder symptoms (BPD symptoms), with five precepts, meditation, equanimity and non-suicidal self-injury (NSSI), adjusted for age and OI-Depression. X=Predictor; M1, M2, M3= Mediator; Y= Outcome; a1, a2, a3, b1, b2, b3, c, c’ = Path coefficients; c= Total direct effect of emptiness on NSSI; c’ = Direct effect of emptiness on NSSI mediating by five precepts, meditation, equanimity. Value for NSSI (Y) are the R-square. NSSI = non-suicidal self-injury. * p<0.05, ** p<0.01, ***p<0.001.
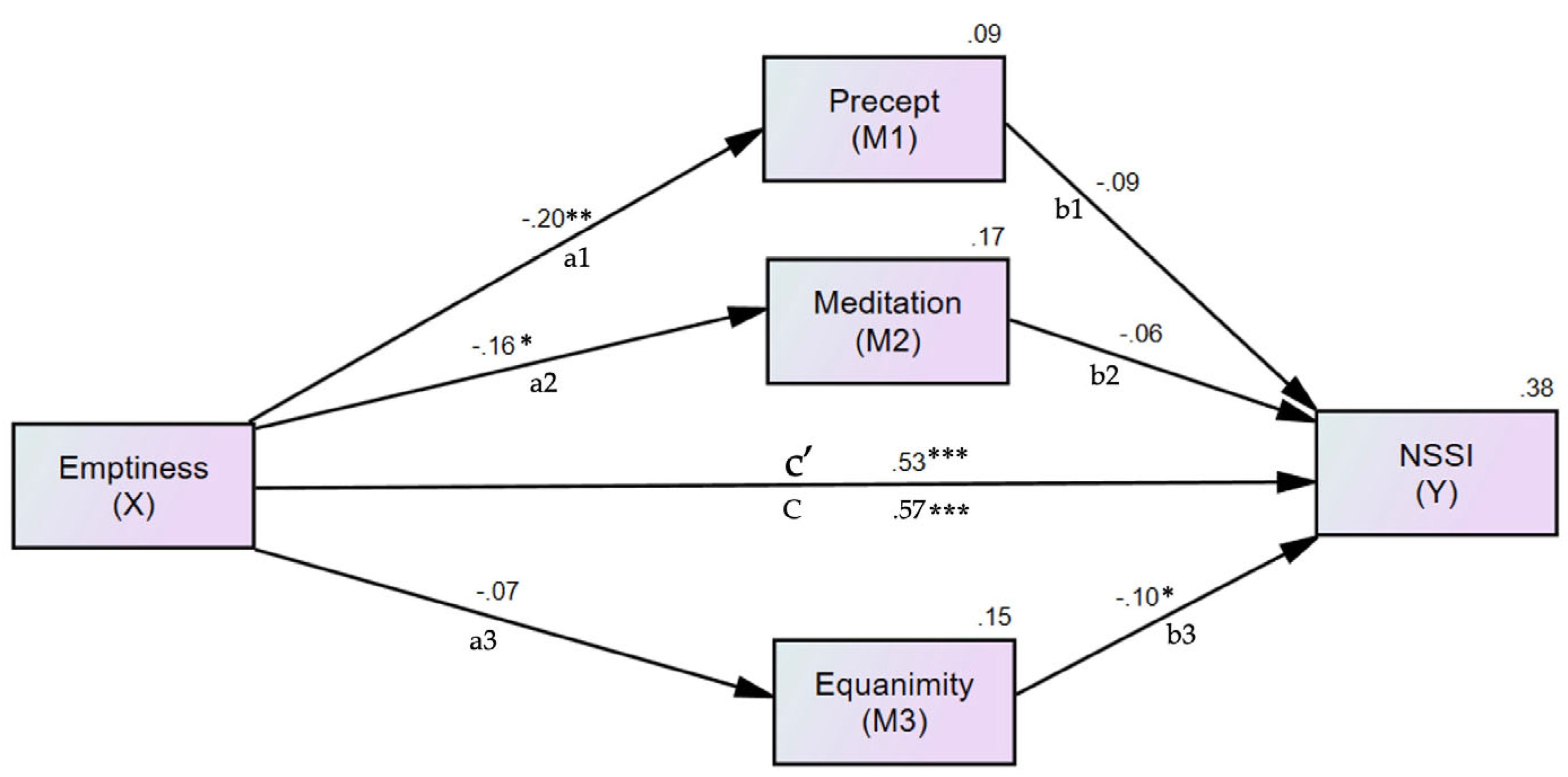

Table 1.
Sociodemographic.
| Variables | All (n=302) |
NSSI1 | Non-NSSI1 | Test Difference |
|---|---|---|---|---|
| Age (year) | 36.56 ±17.17 | 34.92 ±17.10 | 41.35 ±16.60 | t (296) = -2.85, p = 0.005 |
| Sex, female | 195 (65.4%) | 146 (65.8%) | 49 (64.5%) | χ2 (1) = 0.042, p = 0.838 |
| Education Lower Bachelor or higher |
135 (45.3%) 163 (54.7%) |
99 (44.6%) 123 (55.4%) |
36 (47.4%) 40 (52.6%) |
χ2 (1) = 0.176, p = 0.675 |
| Marital status Together Alone |
120 (40.3%) 178 (59.7%) |
91 (41%) 131 (59%) |
29 (38.2%) 47 (61.8%) |
χ2 (1) = 0.189, p = 0.664 |
| Emptiness | 242 (80.1%) | 212 (93.8%) | 30 (23.3%) | χ2 (1) = 105.45, p <0.001 |
| OI-Depress2 | 13.46 ±5.37 | 14.24 ±5.41 | 11.14 ±4.54 | t (300) = 4.48, p <0.001 |
1 NSSI = non-suicidal self-injury, 2 OI-Dep = Outcome inventory Depression.
Table 2.
The correlation coefficients between emptiness, NSSI, OI-Dep, five precepts, meditation, and equanimity.
Table 2.
The correlation coefficients between emptiness, NSSI, OI-Dep, five precepts, meditation, and equanimity.
| Variables | N(%) or mean SD | Emptiness | NSSI1 | OI-Dep2 | Precepts | Meditation | Equanimity |
|---|---|---|---|---|---|---|---|
| Emptiness | 242 (80.1%) | . | |||||
| NSSI1 | 226 (74.8%) | 0.591** | . | ||||
| OI-Dep2 | 13.46 ±5.4 | 0.309** | 0.251** | . | |||
| Precepts | 2.83 ±1.2 | -0.236** | -0.240** | -0.081 | . | ||
| Meditation | 1.72 ±1.0 | -0.250** | -0.240** | -0.162** | 0.420** | . | |
| Equanimity | 2.90 ±1.2 | -0.188** | -0.232** | -0.380** | 0.096 | 0.158** | . |
1 NSSI = non-suicidal self-injury, 2 OI-Dep = Outcome inventory Depression, * p<0.05, ** p<0.01, ***p<0.001.
Table 3.
Regression model of emptiness predicting NSSI.
| Antecedent | Coeff. 1 | 95%CI | p-value |
|---|---|---|---|
| X (emptiness) | 0.565 | 0.507, 0.721 | <0.001 |
| Age | 0.002 | -0.002, 0.003 | 0.64 |
| OI-Dep2 | 0.080 | -0.002, 0.015 | 0.118 |
| R2= 0.35 | |||
1 coeff. = standardized coefficient, 2 OI-Dep = Outcome inventory Depression.
Table 4.
The direct effect of emptiness, five precepts, meditation, and equanimity on NSSI.
| Coeff. 1 ( 95%CI), p-value | ||||
|---|---|---|---|---|
| Antecedent | M1 (Precept) | M2 (Meditation) | M3 (Equanimity) | Y (NSSI2) |
| X (emptiness) | -0.200 (-0.319, -0.073), 0.001 | -0.164 (-0.303, 0.028), 0.018 | -0.071(-0.182, 0.039), 0.210 | 0.534, (0.417, 0.647), <0.001 |
| Precept | -0.085 (-0.179, 0.009), 0.077 | |||
| Meditation | -0.060 (-0.179, 0.055), 0.304 | |||
| Equanimity | -0.103 (-0.194, 0-.017), 0.016 | |||
| R2= 0.09 | R2= 0.17 | R2= 0.15 | R2= 0.38 | |
1 coeff. = standardized coefficient, 2 NSSI = non-suicidal self-injury.
Table 5.
Indirect effect of emptiness on NSSI.
| Antecedent | Effect | 95%CI | p-value |
|---|---|---|---|
| Emptiness | 0.034 | 0.009, 0.075 | 0.005 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



