
Submitted:
22 September 2024
Posted:
23 September 2024
You are already at the latest version
Abstract
Adverse medical events not only harm patients and families, but also cause significant negative impact on healthcare providers, with potential to compromise future professional functioning. These “second victims” may need organizational support and rehabilitation to return to functionality. We analyzed the validity of an adapted tool, the Second Victim Experience and Support Tool (SVEST), to a population in Israel, H-SVEST. The H-SVEST was completed by 172 nurse participants working in a variety of patient care settings. The H-SVEST was assessed for content validity, internal consistency, and construct validity with confirmatory factor analysis (CFA). The CFA run on the initial model with 10 factors and 36 items did not meet criteria for goodness of fit. After removing five items based on their low factor loadings and the correlation, The model fit significantly improved with acceptable CFI, TLI, RMSEA, and SRMR; χ2(389) =626.939, p<.001; χ2/df=1.61; TLI=0.901; CFI=0.917; RMSEA [90% CI]=0.060 [0.051, 0.068]; SRMR=0.064. The final version included 31 items and 10 factors with Cronbach α values ranging from 0.66 to 0.94. The H-SVEST demonstrates robust psychometric properties and valuable insights into the second victim experience in the Israeli context. Comparative analysis with other versions highlights potential cultural influences and areas for further investigation. Implementing this tool and developing evidence-based interventions based on its results can significantly improve well-being and resilience of healthcare providers in Israel and other countries with diverse cultural populations. This study was not registered.
Keywords:
Second Victim Experience and Support Tool
; Confirmatory Factor Analysis
; Validation
1. Introduction
At least one in ten patients in any health care system are affected by an adverse event (AE) [1]. AE is a harmful or negative outcome that occurs during care provision and is caused by medical error, an unexpected adverse event, injury, or even near-miss [2,3,4]. These events are not only distressing for patients and their families, but also cause significant negative physical and emotional impact on healthcare providers (e.g. physicians, nurses, or other medical care providers), with a real potential to compromise future professional functioning [5,6]. Since Wu’s explanation that an AE can have two victims [7] the patient as the main "first victim", the medical provider as "second victim", and, later, that the organization itself as "third victim” [8], the second victim phenomenon (SVP) may also refer to a provider’s emotional response to any negative event in patient care, irrespective of error or harm caused [9]. In 2022, an international group of experts finalized a consensus definition of the second victim as "Any health care worker, directly or indirectly involved in an unanticipated adverse patient event, unintentional healthcare error, or patient injury, and becomes victimized in the sense that also the worker is negatively impacted," [10], p. 6. The prevalence of SVP ranges between 40-90%, depending on the awareness of provider to the phenomenon [11,12,13].
Providers experiencing SVP express difficulty coping with an overflow of negative emotions that may appear immediately after an AE or, after a significant time delay later [8,11,14]. Much research has identified that health care professionals may suffer from a burnout and variety of mental and physical health disorders, alcohol and drug use, and possible suicide attempts as a consequence of SVP [6,8,9,11,15,16,17,18,19,20]. However, some studies have also identified that provision of immediate organizational support may facilitate a quicker return to both well-being and effective work performance, [14,21,22,23] while delaying this support or disregarding the possible trauma of the "second victim", may prevent recovery, and result in defensive or suboptimal treatment [14,17,24,25] and the consideration, or actual, abandonment of the profession [9,14,16,26].
Therefore, many institutions around the world have developed intervention programs [21,27], often applying guidelines developed by United States Agency of Healthcare Research and Quality (AHRQ) [22], but there is still a significant lack in the existence or functionality of these programs to truly resolve the SVP, many health systems do not yet incorporate support in a manner that adequately meet the needs of ‘second victims’ [26,27,28]. Despite the high prevalence and severe manifestations [9,11,12,13,17,23,24,25], this phenomenon is still not well known among health care providers in Israel [29]. Only one quantitative analysis has been conducted in Israel thus far, examining 150 nurses’ responses to suicidal attempts of their patients, to try and determine if this event led to SVP symptoms and could have contributed to nurse absenteeism and turnover, even years after the event [26]. Three qualitative articles found that when the organizational risk management team took a non-blameful approach to errors, more positive second-victim functioning was found [29,30,31]. Additionally, two overarching reviews on physician and nurses' status did suggest that healthcare networks in Israel should create an organized system to proactively manage SVP and not just respond when there is a crisis [32,33].
The summarizing points of these studies demonstrate a need for the Ministry of Health and local healthcare organizations in Israel to recognize the impact of SVP and provide appropriate support. Establishing standardized measures to assess the impact of second victim experiences and the effectiveness of support programs will help institutions better determine the value of these resources. Although some preliminary research of this type has been conducted in Israel [26], no valid and reliable testing instrument is currently available.
The Second Victim Experience and Support Tool (SVEST) developed in 2017 [34], is validated survey instrument developed to assist healthcare organizations implement and track the performance of second victim support resources. The SVEST was originally published in English, and has now been validated in various healthcare settings and translated into Korean (K-SVEST) [35], Chinese (C-SVEST) [36], Italian (IT-SVEST) [37], Turkish (T-SVEST) [38], Spanish [39], Argentinian [40], German [41], Danish [42] and includes additional languages. The questionnaire was tested in several studies, showing internal reliability (Cronbach α) from 0.61-0.89, depending on the dimensions being tested [34,35,36,37,38,42]. It includes 29 items divided into seven dimensions: psychological distress, physical distress, peer support, management support, organizational support, significant family support, and professional self-efficacy. In addition, two outcome variables, work absences and intention to leave work, were also included. Based on this instrument, a revised version (SVEST-R) [2] that includes resilience variables was created in English; this instrument assessing both positive and negative second victim responses, perceptions of support, and employment outcomes.
Therefore, the objective of this study to develop an Israeli version, Hebrew SVEST (H-SVEST), to address the multicultural needs of Israeli society. Israel's diverse population includes people of various religious backgrounds, ethnicities, geographic locations, and levels of religious observance [43,44]. The H-SVEST will be evaluated and validated to ensure its reliability across different healthcare settings and providers. We hypothesized that the H-SVEST comprises adequate feasibility, face, content, and construct validity as well as reliability.
2. Materials and Methods
Upon receipt of the ethics committee approval of the participating academic institution (#AU-20220409), we conducted a multiple-step approach following the recommendations of the World Health Organization (WHO) [45] for translation: expert evaluation, back translation, and testing of questionnaires (Figure 1).
During the first step, the SVEST was translated into Hebrew by a group of experts (nurses), back and forth translation conducted as part of the study that examined exposure to a suicidal patient, and then the tool was adapted to their research needs [26]. Thereafter, as a second step, results of that study [26] were compared and the SVEST questions were adjusted to the population of Israeli healthcare providers across different healthcare settings. This process was carried out to ensure the accuracy and cultural appropriateness of the translation for face validity, within an expert panel consisting of two nurses and linguistic editor expert. The panel made minor modifications to the questionnaire to improve its clarity and comprehensiveness. Third, a back translation was completed by an English native speaker who was not familiar with the original SVEST or the SVEST-R. In the next step, the results were reevaluated within the expert panel, and pretests and cognitive interviewing were conducted with the support of 20 expert nurses with at least two years of medical expertise. This was done to assess the nurses' understanding of the questionnaire and identify any potential areas of confusion. Based on the feedback from the pretests and cognitive interviews, a few minor revisions were made, and the revised questionnaire was then distributed for validation and reliability testing via social network. The questionnaire was adapted between June and December, 2022 and a pilot study was conducted in January, 2023. Thereafter the larger study was conducted online between January and May, 2023 (Qualtrics, Provo, UT). Participants were recruited from social media platforms in Israel, online forums, and local and regional networks.
Registered nurses working in a wide range of medical organizations and disciplines, including hospitals, geriatrics home care, and community settings, were recruited using a written invitation and information letter. The broad spectrum of healthcare specialties minimized selection bias and low response rates. To achieve the target sample size three rounds of recruitment were conducted within these networks.
Sample size was calculation using Daniel Soper’s A-priori Sample Size Calculator for Structural Equation Modeling [46] with a moderate effect size of 0.30, 10 latent variables, and 36 observed variables. The statistical criteria are a significance level of p<.05, and a power of 1-β >.80. Altogether, such a model requires 128 observations. These calculations are based in part on Westland’s [47] proposal for SEM sample size calculation (see SEM sample size method review) [48]. Moreover, according to Muthén & Muthén [49], simulation studies show that with normally distributed indicator variables and no missing data, a reasonable sample size for a simple CFA model is ~ N = 150. Lastly, the sample size for validation studies a minimum of 50 respondents is recommended, but larger samples over 100 are preferred [50].
The SVEST was used to assess the second victim experience of providers as well as their desired forms of support. The original questionnaire contains 29 items rated on a 5-point Likert scale (1 = strongly disagree, 5 = strongly agree), which yield scores for seven psychosocial factors and two employment-related factors (turnover intentions and absenteeism) associated with the second victim experience. The seven psychosocial factors include psychological distress, physical distress, colleague support, supervisor support, institutional support, nonwork-related support, and professional self-efficacy (Table 1). The two outcome variables were turnover intentions and absenteeism. Items were written to reflect first-person perceptions of each dimension. Seven additional items were included at the end of the questionnaire to assess desired forms of support (e.g., time away from the unit, peaceful location, respected peer to discuss what happened). These items are also rated on a 5-point Likert scale ranging from 1 (strongly do not desire) to 5 (strongly desire) [34].
Data were analyzed using SPSS Software (SPSS Inc, Chicago, IL, v. 28) and R (R software 4.3.3) via “Iavaan” [51]. Descriptive statistics were calculated for demographic characteristics, for each item, and for SVEST scores. The reliability (internal consistency) of SVEST was tested by Cronbach's α coefficient. Cronbach's α coefficient values greater than 0.70 demonstrate an acceptable internal consistency [52,53]. Construct validity to all 36 items was assessed through confirmatory factor analysis (CFA) in order to evaluate model fit. CFA indices considered for the model's goodness of fit were chi-square statistic (χ2; chi-square statistic divided by the degree of freedom <3 is acceptable, root mean square error of approximation (RMSEA; RMSEA<0.08 acceptable, <0.05 excellent), comparative fit index (CFI; CFI>0.90 acceptable, >0.95 excellent), Tucker-Lewis index (TLI; TLI>0.90 acceptable, >0.95 excellent) [54].
3. Results
The study included 172 participants (all nurses) in a variety of therapeutic settings; 62% of them reported experiencing an adverse event within the past year. Most of the participants were female (85%). About 79% (135) were married or in a relationship. Most of them had an academic degree (95%): 43% held Bachelor's degrees, 48% had secondary Master's degrees, and four percent of the sample held PhDs. Most defined their religion as Jewish (89%), and the others were Muslims, Christians, or Druze. Participant ages were between 24 and 67 (M=42.6, SD=9.6), and years of employment ranged from one to 45 years (M=16.6, SD=10.4).
Confirmatory Factor Analysis (CFA)
The CFA run on the initial model with 10 factors and 36 items (Table 2) did not meet criteria for goodness fit; χ2(549) =961.563, p<.001; χ2/df=1.75; TLI=0.847; CFI=0.867; RMSEA [90% CI] = 0.066 [0.059, 0.073]; SRMR=0.100. After removing five items based on their low factor loadings and the correlation, Model 2 was created (Table 2). All factor loadings for each item and each model are presented in Table 2. The model fit in Model 2 significantly improved with acceptable CFI, TLI, and RMSEA (Table 2); χ2(389)=626.939, p<.001; χ2/df=1.61; TLI=0.901; CFI=0.917; RMSEA [90% C.I.]=0.060 [0.051, 0.068]; SRMR=0.064. Thus, the final version of the H- SVEST that included 31 items and 10 factors, was more consistent. Additionally, Cronbach α values for each dimension are provided in Table 3.
4. Discussion
Given the deleterious effects of Second Victim Phenomenon (SVP) on healthcare organizations and the well-being of current and prospective patients, there exists a compelling imperative to enhance the identification and delivery of suitable support for providers manifesting symptoms of second victimization. Despite the existence of numerous global support programs for providers [12,21,27], they frequently prove inadequate in addressing the distinctive requirements of diverse cultural populations [26,28,29]. In the case of Israel, the multicultural composition of healthcare organizations exacerbates this deficiency. Culturally sensitive interventions are indispensable for the effective support of providers within this particular milieu. An instrumental stride toward realizing this objective involves the adaptation of the Second Victim Experience and Support Tool (SVEST) to the Hebrew language and contextual considerations.
The objective of this study was to formulate and validate the H-SVEST, a Hebrew-language iteration of the Second Victim Experience and Support Tool (SVEST). The H-SVEST is designed to evaluate the repercussions of adverse events on healthcare providers (second victims) and their perceived need for support. The study adhered to a meticulous methodology encompassing translation, back-translation, pretesting, and confirmatory factor analysis (CFA).
Similar to previous studies on the SVEST [35,36,37,38,40,41] the H-SVEST showed strong psychometric properties with good face validity, content validity, and construct validity. Internal consistency (Cronbach's alpha) for the H-SVEST dimensions ranged from 0.66 - 0.94, indicating good reliability, except for the collegial support dimension (0.58). After subtracting five items, the final version of H-SVEST was comprised of 31 items and 10 factors, providing a comprehensive assessment of the second victim experience.
Comparative analysis with other SVEST versions found that most factors in the H-SVEST demonstrated similar internal consistency to other language versions, with minor deviations. Notably, collegial support (α=0.58 vs. original SVEST 0.61) [34], Non-Work-Related Support (α=0.77 vs. original SVEST 0.84) and absenteeism (α=0.66 vs. original SVEST 0.84 and SVEST-R 0.88) had slightly lower values. At the same time, professional self-efficacy showed a modest increase (α=0.86 vs. SVEST 0.79). The desire for different types of support and mean factor scores were generally similar across most versions, with some exceptions. In contrast with the original SVEST [34], our sample showed institutional support scores were higher, potentially due to active programming efforts. Overall, the H-SVEST demonstrates robust psychometric properties and provides valuable insights into the second victim experience in the Israeli context. Comparative analysis with other versions highlights potential cultural influences and areas for further investigation.
Limitations
While the study sample included a diverse range of nurses, it may not be representative of all healthcare workers in Israel (e.g., doctors, social workers, nurse assistance and more). Further research with larger and more diverse samples is needed to confirm the generalizability of the findings. Moreover, this study focused on cross-sectional data. Longitudinal studies are needed to investigate the long-term effects of adverse events on healthcare providers and the effectiveness of interventions based on the H-SVEST. Future research should examine how organizational culture, support systems, and leadership practices can mitigate the impact of adverse events on healthcare providers.
The objective of this study was not to analyze possible correlations and predictions but rather only to validate this instrument among a Hebrew speaking population. Future larger, and longitudinal, studies applying this instrument among different populations who live in Israel, will be needed to examine this issue in depth and create relevant interventions from those comprehensive results.
5. Conclusions
The H-SVEST is a valuable tool for healthcare organizations in Israel to assess the impact of adverse events on their providers and identify those who may need support. The study highlights the need for increased awareness and support for healthcare providers who experience the second victim phenomenon. Implementing organizational interventions based on the H-SVEST results can help mitigate the negative consequences of adverse events and improve provider well-being and retention.
Overall, this study provides valuable evidence for the validity and reliability of the H-SVEST. Implementing this tool and developing evidence-based interventions based on its results can significantly improve the well-being and resilience of healthcare providers in Israel and other countries with diverse cultural populations.
Public Involvement Statement
There was no public involvement in any aspect of this research.
Guidelines and Standards Statement
This manuscript was drafted against the SQUIRE (Standards for Quality Improvement Reporting Excellence) for intervention research.
Use of Artificial Intelligence
AI or AI-assisted tools were not used in drafting any aspect of this manuscript.
Author Contributions
Conceptualization, R.C., Y.S., R.N.G.; methodology, R.C., Y.S., R.N.G, O.C.; software, O.C..; validation, R.C., Y.S., R.N.G.; formal analysis, O.C.; investigation, R.C. O.C.; resources, R.C.; data curation, R.C., O.C.; writing—original draft preparation, R.C., Y.S., O.C.; writing—review and editing, R.C., Y.S., R.N.G., O.C.; visualization, R.C.,Y.S., R.N.G., O.C.; supervision, Y.S., R.N.G;. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee) of Ariel University (#AU-20220409) in 2022.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
The authors would like to thank Aviva Yoselis for her editorial assistance.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- de Vries, E.N., Ramrattan. The incidence and nature of in-hospital adverse events: A systematic review. Qual Saf Health Care 2008, 17, 216–223. [Google Scholar] [CrossRef]
- Winning, A.M.; Merandi, J.; Rausch, J.R.; Liao, N.; Hoffman, J.M.; Burlison, J.D.; Gerhardt, C.A. Validation of the Second Victim Experience and Support Tool—Revised in the neonatal intensive care unit. J Patient Saf 2021, 17, 531–540. [Google Scholar] [CrossRef]
- Mitchell, I.; Schuster, A.; Smith, K.; Pronovost, P.; Wu, A. Patient safety incident reporting: a qualitative study of thoughts and perceptions of experts 15 years after ‘To Err is Human’. BMJ Qual Saf 2016, 25, 92–99. [Google Scholar] [CrossRef]
- Lane, M.A.; Newman, B.M.; Taylor, M.Z.; O'Neill, M.; Ghetti, C.; Woltman, R.M.; Waterman, A.D. Supporting clinicians after adverse events: development of a clinician peer support program. Patient Saf 2018, 14, e56–e60. [Google Scholar] [CrossRef]
- Valencia-Martín, J.L. , Vicente-Guijarro, D., San Jose-Saras, P., Moreno-Nunez, P., Pardo-Hernández, A., Aranaz-Andrés, J.A., ESHMAD Director Group and external advisers. Prevalence, characteristics, and impact of Adverse Events in 34 Madrid hospitals. The ESHMAD Study. Eur J Clin Invest 2022, 52, 52. [Google Scholar] [CrossRef]
- Van Gerven, E.; Vander Elst, T.; Vandenbroeck, S.; Dierickx, S.; Euwema, M.; Sermeus, W.; De Witte, H.; Godderis, L. Vanhaecht, K. Increased risk of burnout for physicians and nurses involved in a patient safety incident. Med Care 2016, 54, 937–943. [Google Scholar] [CrossRef]
- Wu, A. Medical error: The second victim. BMJ 2000, 320, 726–727. [Google Scholar] [CrossRef]
- Seys, D.; Wu, A.W.; Van Gerven, E.; Vleugels, A.; Euwema, M.; Panella, M.; Scott, S.D.; Conway, J.; Sermeus, W.; Vanhaecht, K. Health care professionals as second victims after adverse events: A systematic review. Eval Health Prof 2013, 36, 135–162. [Google Scholar] [CrossRef]
- Ganahl, S.; Knaus, M.; Wiesenhuetter, I.; Klemm, V.; Jabinger, E.M.; Strametz, R. Second victims in intensive care-emotional stress and traumatization of intensive care nurses in Western Austria after adverse events during the treatment of patients. Int J Environ Res Public Health 2022, 19, 3611. [Google Scholar] [CrossRef]
- Vanhaecht, K.; Seys, D.; Russott, S.; Strametz, R.; Mira, J.; Sigurgeirsdóttir, S.; Wu, A.W.; Polluste, K.; Popovici, D.G.; Sfetcu, R.; Kurt, S. An evidence and consensus-based definition of second victim: a strategic topic in healthcare quality, patient safety, person-centeredness and human resource management. Int J Environ Res Public Health 2022, 19, 16869. [Google Scholar] [CrossRef]
- Strametz, R.; Fendel, J.C.; Koch, P.; Roesner, H.; Zilezinski, M.; Bushuven, S.; Raspe, M. Prevalence of second victims, risk factors, and support strategies among German nurses (SeViD-II Survey). Int J Environ Res Public Health 2021, 18, 10594. [Google Scholar] [CrossRef]
- Finney, R.E. Implementation of a second victim peer support program in a large anesthesia department. AANA J 2021, 89, 235–244. [Google Scholar]
- Haung, R.; Sun, H.; Chen, G.; Li, Y.; Wang, J. Second-victim experience and support among nurses in mainland China. J Nurs Manag 2021, 30, 260–267. [Google Scholar] [CrossRef]
- Scott, S.D.; Hirschinger, L.E.; Cox, K.R.; McCoig, M.; Brandt, J.; Hall, L.W. The natural history of recovery for the healthcare provider “second victim” after adverse patient events. Qual Saf Health Care 2009, 18, 325–330. [Google Scholar] [CrossRef]
- Garcia, C.L.; Abreu, L.C.; Ramos, J.L.S.; Castro, C.F.; Smiderle, F.R.; Santos, J.A.; Bezerra, I.M. Influence of burnout on patient safety: Systematic review and meta-analysis. Medicina 2019, 55, 553. [Google Scholar] [CrossRef]
- Busch, I.M.; Moretti, F.; Purgato, M.; Barbui, C.; Wu, A.W.; Rimondini, M. Psychological and psychosomatic symptoms of second victims of adverse events: A systematic review and meta-analysis. J Patient Saf 2020, 16, 61–74. [Google Scholar] [CrossRef]
- Sachs, C.J.; Wheaton, N. Second Victim Syndrome. Treasure Island (FL): StatPearls Publishing, 2023.
- Leinweber, J.; Creedy, D.K.; Rowe, H.; Gamble, J. Responses to birth trauma and prevalence of posttraumatic stress among Australian midwives. Women Birth 2017, 30, 40–45. [Google Scholar] [CrossRef]
- Baas, M.A.; Scheepstra, K.W.; Stramrood, C.A.; Evers, R.; Dijksman, L.M.; van Pampus, M.G. Work-related adverse events leaving their mark: A cross-sectional study among Dutch gynecologists. BMC Psychiatry 2018, 18, 1–8. [Google Scholar] [CrossRef]
- Dutheil, F.; Aubert, C.; Pereira, B.; Dambrun, M.; Moustafa, F.; Mermillod, M.; Baker, J.S.; Trousselard, M.; Lesage, F.X.; Navel, V. Suicide among physicians and health-care workers: A systematic review and meta-analysis. PLoS ONE 2019, 14, e0226361. [Google Scholar] [CrossRef]
- Seys, D.; Panella, M.; Russotto, S.; Strametz, R.; Joaquín Mira, J.; Van Wilder, A.; Godderis, L.; Vanhaecht, K. In search of an international multidimensional action plan for second victim support: A narrative review. BMC Health Serv Res 2023, 23, 816. [Google Scholar] [CrossRef]
- Hauk, L. Support strategies for health care professionals who are second victims. AORN J 2018, 107, P7–P9. [Google Scholar] [CrossRef]
- Rinaldi, C.; Leigheb, F.; Vanhaecht, K.; Donnarumma, C.; Panella, M. Becoming a “second victim” in health care: Pathway of recovery after adverse event. Rev Calid Asist 2016, 31, 11–19. [Google Scholar] [CrossRef]
- Panella, M.; Rinaldi, C.; Leigheb, F.; Donnarumma, C.; Kul, S.; Vanhaecht, K.; Di Stanislao, F. The determinants of defensive medicine in Italian hospitals: The impact of being a second victim. Rev Calid Asist 2016, 31, 20–25. [Google Scholar] [CrossRef]
- Ozeke, O.; Ozeke, V.; Coskun, O.; Budakoglu, I.I. Second victims in health care: Current perspectives. Adv Med Educ Pract 2019, 10, 593–603. [Google Scholar] [CrossRef]
- Amit Aharon, A.; Fariba, M.; Shoshana, F.; Melnikov, S. Nurses as “second victims” to their patients’ suicidal attempts: A mixed-method study. J Clin Nurs 2021, 30, 3290–3300. [Google Scholar] [CrossRef]
- Busch, I.M.; Moretti, F.; Campagna, I.; Benoni, R.; Tardivo, S.; Wu, A.W.; Rimondini, M. Promoting the psychological well-being of healthcare providers facing the burden of adverse events: A systematic review of second victim support resources. Int J Environ Res Public Health 2021, 18, 5080. [Google Scholar] [CrossRef]
- White, A.A.; Brock, D.M.; McCotter, P.I.; Hofeldt, R.; Edrees, H.H.; Wu, A.W.; Shannon, S.; Gallagher, T.H. Risk managers' descriptions of programs to support second victims after adverse events. J Healthc Risk Manag 2015, 4, 30–40. [Google Scholar] [CrossRef]
- Cohen, R.; Sela, Y.; Nissanholtz-Gannot, R. Addressing the second victim phenomenon in Israeli health care institutions. Isr J Health Policy Res 2023, 12, 30. [Google Scholar] [CrossRef]
- Cohen, R.; Sela, Y.; Halevi Hochwald, I.; Nissanholz-Gannot, R. Nurses' silence: Understanding the impacts of second victim phenomenon among Israeli nurses. Healthcare 2023, 11, 1961. [Google Scholar] [CrossRef]
- Rassin, M.; Kanti, T. The “Second Victim”: Nurses’ coping with medication errors comparison of two decades (2005-2018). J Nur Healthcare 2019, 4, 1–6. [Google Scholar] [CrossRef]
- Shor, *!!! REPLACE !!!*; S, *!!! REPLACE !!!*; Tal, O.; Maymon, R. The second victim: Treating the health care providers. Harefuah, 2017; 156, 38–40. [Google Scholar]
- Cohen, R.; Sela-Vilensky, Y.; Greenberg, K.; Nissanholz-Gannot, R. Nurses’ silence: The second victim phenomenon in Israel. Guf Yeda 2024, 24, 7. [Google Scholar]
- Burlison, J.D.; Scott, S.D.; Browne, E.K.; Thompson, S.G.; Hoffman, J.M. The second victim experience and support tool: validation of an organizational resource for assessing second victim effects and the quality of support resources. J Patient Saf 2017, 13, 93–102. [Google Scholar] [CrossRef]
- Kim, E.M.; Kim, S.A.; Lee, J.R.; Burlison, J.D.; Oh, E.G. Psychometric properties of Korean version of the Second Victim Experience and Support Tool (K-SVEST). J. Patient Saf 2020, 16, 179–186. [Google Scholar] [CrossRef]
- Chen, J.; Yang, Q.; Zhao, Q.; Zheng, S.; Xiao, M. Psychometric validation of the Chinese version of the Second Victim Experience and Support Tool (C-SVEST). J Nurs Manag 2019, 27, 1416–1422. [Google Scholar] [CrossRef]
- Scarpis, E.; Castriotta, L.; Ruscio, E.; Bianchet, B.; Doimo, A.; Moretti, V.; Cocconi, R.; Farneti, F.; Quattrin, R. The Second Victim Experience and Support Tool: A cross-cultural adaptation and psychometric evaluation in Italy (IT-SVEST). J Patient Saf 2022, 18, 88–93. [Google Scholar] [CrossRef]
- Koca, A., Elhan. Validation of the Turkish version of the Second Victim Experience and Support Tool (T-SVEST). Heliyon 2022, 8, e10553. [Google Scholar] [CrossRef]
- Santana-Domínguez, I.; González-de la Torre, H.; Verdú-Soriano, J.; Nolasco, A.; Martín-Martínez, A. Validation and psychometric properties of the Spanish version of the Second Victim Experience and Support Tool Questionnaire. J Patient Saf 2022, 18, 692–701. [Google Scholar] [CrossRef]
- Brunelli, M.V.; Estrada, S.; Celano, C. Cross-cultural adaptation and psychometric evaluation of a Second Victim Experience and Support Tool (SVEST). J Patient Saf 2021, 17, e1401–e1405. [Google Scholar] [CrossRef]
- Strametz, R.; Siebold, B.; Heistermann, P.; Haller, S.; Bushuven, S. Validation of the German version of the Second Victim Experience and Support Tool-Revised. J Patient Saf 2022, 18, 182–192. [Google Scholar] [CrossRef]
- Knudsen, T.; Abrahamsen, C.; Jørgensen, J.S.; Schrøder, K. Validation of the Danish version of the Second Victim Experience and Support Tool. Scand J Public Health 2022, 50, 497–506. [Google Scholar] [CrossRef]
- Keshet, Y.; Popper-Giveon, A. Language practice and policy in Israeli hospitals: the case of the Hebrew and Arabic languages. Isr J Health Policy Res 2019, 8, 58. [Google Scholar] [CrossRef]
- Kalagy, T.; Abu-Kaf, S.; Braun-Lewensohn, O. Effective ways to encourage health-care practices among cultural minorities in Israel during the COVID-19 pandemic. Int J Environ Res Public Health 2021, 18, 9563. [Google Scholar] [CrossRef]
- World Health Organization. Process of Translation and Adaptation of Instruments. WHO Website 2020. Available online: http://www.who.int/substance_abuse/research_tools/translation/en/ (accessed on 14 April 2022).
- Soper, D. A-priori Sample Size Calculator for Structural Equation Models [stats calculator website]. 14 April. Available online: https://www.danielsoper.com/statcalc/calculator.aspx?id=89 (accessed on 14 April 2022).
- Westland, J.C. Lower bounds on sample size in structural equation modeling. Electron Commer Res Appl 2010, 9, 476–487. [Google Scholar] [CrossRef]
- Ranatunga, R.V.S.P.K.; Priyanath, H.M.S.; Megama, R.G.N. Methods and rule-of-thumbs in the determination of minimum sample size when applying Structural Equation Modelling: A review. JSSR 2020, 15, 102–109. [Google Scholar] [CrossRef]
- Muthén, B.O.; Muthén, L.K. How to use a Monte Carlo study to decide on sample size and determine power. Struct Equ Modeling 2002, 9, 599–620. [Google Scholar] [CrossRef]
- de Vet, H.C.W. , Mokking, L.B., Knol, D.L. Measurement in medicine: A practical guide. Cambridge: Cambridge University Press, 2011.
- Rosseel, Y. Iavaan: An R package for structural equation modeling. J Stat Softw 2012, 48, 1–36. [Google Scholar] [CrossRef]
- Bland, M.; Altman, D.G. Cronbach's alpha. BMJ 1997, 314, 572. [Google Scholar] [CrossRef]
- Tavakol, M.; Dennick, R. Making sense of Cronbach's alpha. Int J Med Educ 2011, 2, 53–55. [Google Scholar] [CrossRef]
- Xia, Y. , Yang, Y. RMSEA, CFI, and TLI in structural equation modeling with ordered categorical data: The story they tell depends on the estimation methods. Behav Re Methods 2019, 51, 409–428. [Google Scholar] [CrossRef]
Figure 1.
Translation and adaptation process of the H-SVEST.
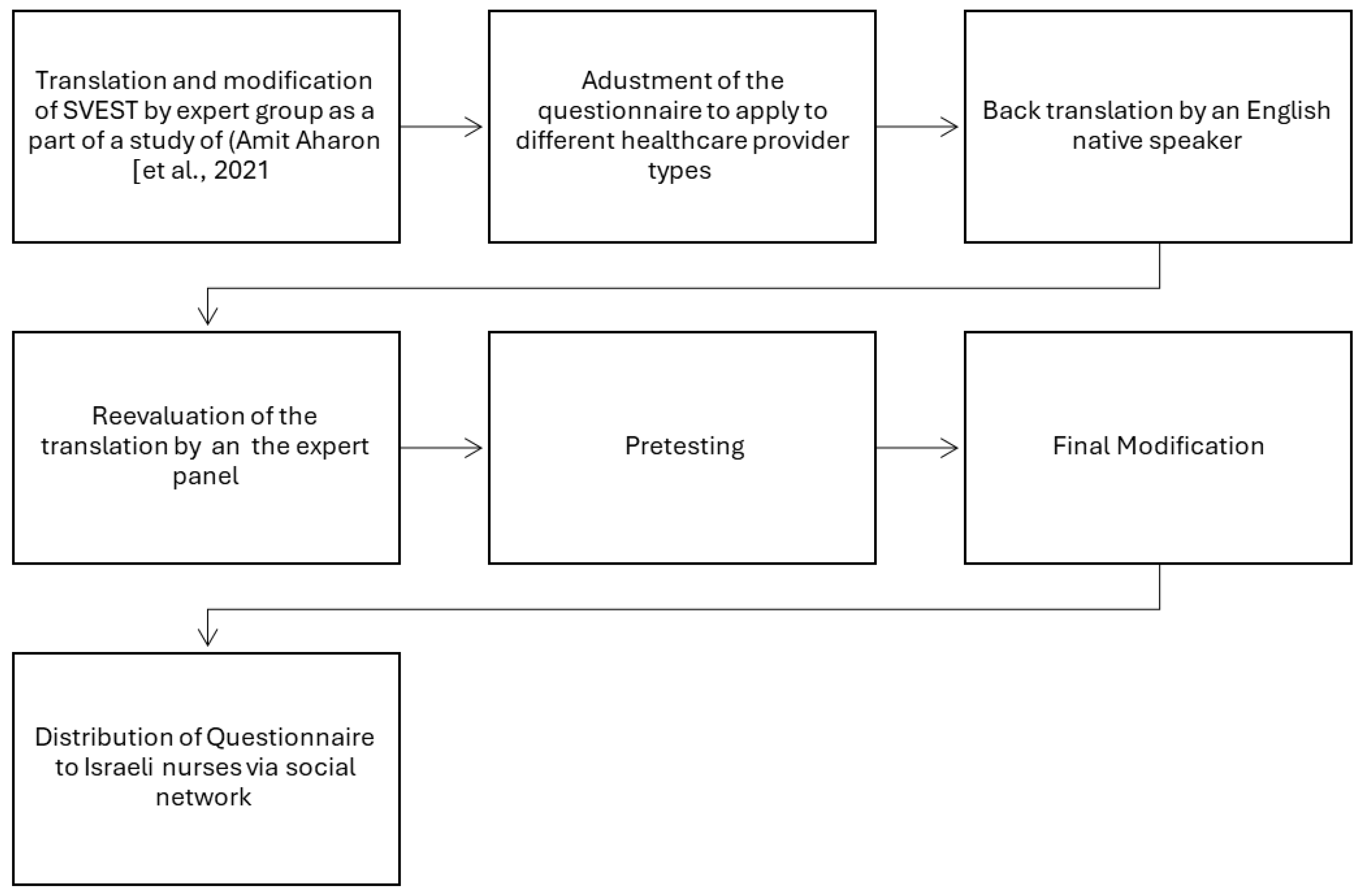

Table 1.
List of final 36 survey items and ten psychosocial and employment factors.
| Survey Items | Dimensions & Outcome Variables |
|---|---|
| I have experienced embarrassment from these instances. | Psychological Distress |
| My involvement in these types of instances has made me fearful of future occurrences. | |
| My experiences have made me feel miserable. | |
| I feel deep remorse for my past involvements in these types of events. | |
| The mental weight of my experience is exhausting. | Physical Distress |
| My experience with these occurrences can make it hard to sleep regularly. | |
| The stress from these situations has made me feel queasy or nauseous. | |
| Thinking about these situations can make it difficult to have an appetite. | |
| I appreciate my coworkers’ attempts to support me, but their efforts can come at the wrong time. | Colleague Support |
| Discussing what happened with my colleagues provides me with a sense of relief. | |
| My colleagues can be indifferent to the impact these situations have had on me. | |
| My colleagues help me feel that I am still a good healthcare provider despite any mistakes I have made. | |
| I feel that my supervisor treats me appropriately after these occasions. | Supervisor Support |
| My supervisor’s responses are fair. | |
| My supervisor blames individuals. | |
| I feel that my supervisor evaluates these situations in a manner that considers the complexity of patient care practices. | |
| My organization understands that those involved may need help to process and resolve any effects they may have on care providers. | Institutional Support |
| My organization offers a variety of resources to help me get over the effects of involvement with these instances. | |
| The concept of concern for the well-being of those involved in these situations is not strong at my organization. | |
| I look to close friends and family for emotional support after one of these situations happens. | Non-Work-Related Support |
| The love from my closest friends and family helps me get over these occurrences. | |
| Following my involvement, I experienced feelings of inadequacy regarding my patient care abilities. | Professional Self-Efficacy |
| My experience makes me wonder if I am not really a good healthcare provider. | |
| After my experience, I became afraid to attempt difficult or high-risk procedures. | |
| These situations do not make me question my professional abilities. | |
| My experience with these events has led to a desire to take a position outside of patient care. | Turnover Intentions |
| Sometimes the stress from being involved with these situations makes me want to quit my job. | |
| My experience with an adverse patient event or medical error has resulted in me taking a mental health day. | Absenteeism |
| I have taken time off after one of these instances occurs. | |
| The ability to immediately take time away from my unit for a little while. | Desired Forms of Support |
| A specified peaceful location that is available to recover and recompose after one of these types of events. | |
| A respected peer to discuss the details of what happened. | |
| An employee assistance program that can provide free counseling to employees outside of work. | |
| A discussion with my manager or supervisor about the incident. | |
| The opportunity to schedule a time with a counselor at my hospital to discuss the event. | |
| A confidential way to get in touch with someone 24 hours a day to discuss how my experience may be affecting me. |
Table 2.
Factor loadings for each item of H-SVEST for Models 1 and 2.
| Standardized Factor Loadings | ||||||
|---|---|---|---|---|---|---|
| Factors / Items | Min | Max | M | SD | Model 1 | Model 2 |
| Psychological Distress | 1.00 | 5.00 | 3.46 | 1.22 | ||
| 1. I have felt embarrassment from these events. | 1.00 | 5.00 | 3.44 | 1.51 | .694 | .698 |
| 2. My involvement in these types of events has made me fearful of future occurrences. | 1.00 | 5.00 | 3.67 | 1.48 | .734 | .733 |
| 3. My experiences have made me feel miserable. | 1.00 | 5.00 | 3.12 | 1.50 | .792 | .791 |
| 4. I feel deep remorse for my past involvement in these types of events. | 1.00 | 5.00 | 3.65 | 1.40 | .824 | .823 |
| Physical Distress | 1.00 | 5.00 | 3.16 | 1.20 | ||
| 5. The mental weight of my experience is exhausting. | 1.00 | 5.00 | 3.38 | 1.35 | .866 | .861 |
| 6. My experience with these occurrences can make it difficult to sleep regularly. | 1.00 | 5.00 | 3.13 | 1.49 | .786 | .790 |
| 7. The stress from these situations has made me feel queasy or nauseated. | 1.00 | 5.00 | 3.46 | 1.42 | .758 | .761 |
| 8. Thinking about these situations has sometimes affected my appetite. | 1.00 | 5.00 | 2.65 | 1.43 | .676 | .677 |
| Colleague Support | 1.00 | 5.00 | 3.65 | 1.01 | ||
| 9. I appreciate my coworkers’ attempts to console me, but their efforts can come at the wrong time. | 1.00 | 5.00 | 2.94 | 1.24 | NA | |
| 10. Discussing what happened with my colleagues provides me with a sense of relief. | 1.00 | 5.00 | 3.54 | 1.23 | NA | .749 |
| 11. My colleagues can be indifferent to the impact these situations have had on me. | 1.00 | 5.00 | 3.00 | 1.26 | NA | |
| 12. My colleagues help me feel that I am still a good healthcare provider despite any mistakes I have made. | 1.00 | 5.00 | 3.76 | 1.17 | NA | .549 |
| Supervisor Support | 1.00 | 5.00 | 3.29 | 1.19 | ||
| 13. I feel that my supervisor treats me appropriately after these occasions. | 1.00 | 5.00 | 3.33 | 1.38 | .893 | .897 |
| 14. My supervisor’s responses are fair. | 1.00 | 5.00 | 3.29 | 1.40 | .959 | .954 |
| 15. My supervisor blames individuals. | 1.00 | 5.00 | 3.33 | 1.47 | .687 | .687 |
| 16. I feel that my supervisor evaluates these situations in a manner that considers the complexity of patient care practices. | 1.00 | 5.00 | 3.20 | 1.34 | .658 | .661 |
| Institutional Support | 1.00 | 5.00 | 2.36 | 1.05 | ||
| 17. My organization understands that those involved may need help to process and resolve any effects they may have on care providers. | 1.00 | 5.00 | 2.45 | 1.30 | .832 | .833 |
| 18. My organization offers a variety of resources to help me get over the effects of involvement with these instances. | 1.00 | 5.00 | 1.96 | 1.10 | .802 | .802 |
| 19. The concept of concern for the well-being of those involved in these situations is not strong at my organization. | 1.00 | 5.00 | 2.67 | 1.39 | .585 | .584 |
| Non-Work-Related Support | 1.00 | 5.00 | 3.68 | 1.12 | ||
| 20. I look to close friends and family for emotional support after one of these situations happens. | 1.00 | 5.00 | 3.44 | 1.27 | 1.038 | .834 |
| 21. The love from my closest friends and family helps me recover from these occurrences. | 1.00 | 5.00 | 3.91 | 1.21 | .607 | .756 |
| Professional Self-Efficacy | 1.00 | 5.00 | 2.41 | 1.24 | ||
| 22. Following my involvement, I experienced feelings of inadequacy regarding my patient care abilities. | 1.00 | 5.00 | 2.17 | 1.32 | .858 | .857 |
| 23. My experience makes me wonder if I am not really a good healthcare provider. | 1.00 | 5.00 | 2.46 | 1.39 | .846 | .848 |
| 24. After my experience, I became afraid to attempt difficult or high-risk procedures. | 1.00 | 5.00 | 2.61 | 1.46 | .786 | .786 |
| 25. These situations do not make me question my professional abilities. | 1.00 | 5.00 | 2.48 | 1.42 | -.002 | |
| Turnover Intentions | 1.00 | 5.00 | 2.60 | 1.45 | ||
| 26. My experience with these events has led to a desire to take a position outside of patient care. | 1.00 | 5.00 | 2.53 | 1.48 | .939 | .941 |
| 27. Sometimes the stress from being involved with these situations makes me want to quit my job. | 1.00 | 5.00 | 2.66 | 1.51 | .945 | .944 |
| Absenteeism | 1.00 | 5.00 | 2.42 | 1.26 | ||
| 28. My experience with an adverse patient event or medical error has resulted in me taking a mental health day. | 1.00 | 5.00 | 1.96 | 1.39 | .552 | .558 |
| 29. I have taken time off after one of these instances occurs. | 1.00 | 5.00 | 2.89 | 1.52 | .903 | .894 |
| Desired Forms of Support | 1.00 | 5.00 | 3.98 | 0.99 | ||
| 30. The ability to immediately take time away from my unit for a little while | 1.00 | 5.00 | 3.36 | 1.45 | .498 | |
| 31. A specified peaceful location that is available to recover and recompose after one of these types of events | 1.00 | 5.00 | 3.55 | 1.40 | .588 | .567 |
| 32. A respected peer to discuss the details of what happened | 1.00 | 5.00 | 4.18 | 1.10 | .707 | .706 |
| 33. An employee assistance program that can provide free counseling to employees outside of work | 1.00 | 5.00 | 4.01 | 1.28 | .864 | .865 |
| 34. A discussion with my manager or supervisor about the incident | 1.00 | 5.00 | 3.77 | 1.36 | .431 | |
| 35. The opportunity to schedule a time with a counselor at my hospital to discuss the event | 1.00 | 5.00 | 4.01 | 1.23 | .839 | .843 |
| 36. A confidential way to get in touch with someone 24 hours a day to discuss how my experience may be affecting me | 1.00 | 5.00 | 4.20 | 1.20 | .672 | .683 |
Table 3.
Internal consistency of the dimension of the H-SVEST as compared with other SVEST versions.
Table 3.
Internal consistency of the dimension of the H-SVEST as compared with other SVEST versions.
| This study | ||||||||
|---|---|---|---|---|---|---|---|---|
| Factors | Model 1 | Model 2 | Original | Turkish | Italian | Korean | Chinese | Argentinian |
| Psychological Distress | .85 | .85 | .83 | .86 | .72 | .83 | .83 | .74 |
| Physical Distress | .86 | .86 | .87 | .83 | .69 | .87 | .92 | .70 |
| Colleague Support | .27 | .58 | .61 | .78 | .73 | .61 | .59 | .56 |
| Supervisor Support | .87 | .87 | .87 | .86 | .77 | .87 | .80 | .44 |
| Institutional Support | .76 | .76 | .64 | .88 | .75 | .64 | .60 | .79 |
| Non-Work-Related Support | .77 | .77 | .84 | .87 | .74 | .84 | .84 | .84 |
| Professional Self-Efficacy | .66 | .86 | .79 | .84 | .71 | .79 | .61 | .85 |
| Turnover Intentions | .94 | .94 | .89 | .89 | .74 | .81 | .92 | .71 |
| Absenteeism | .66 | .66 | .86 | .86 | .73 | .88 | .88 | .73 |
| Desired Forms of Support | .84 | .84 | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



