
Preprint
Review
Evaluating Short-Term Intensive Insulin Intervention in Newly Diagnosed Type 2 Diabetes: A Meta-Analysis Perspective
Altmetrics
Downloads
92
Views
89
Comments
0


This version is not peer-reviewed
Medical and Dental Care, Photobiomodulation and Photomedicine
Submitted:
22 September 2024
Posted:
23 September 2024
You are already at the latest version
Alerts
Abstract
Background: Oral hypoglycemic agents are typically the first-line treatment for type 2 diabetes mellitus (T2DM). This study examines the benefits of initiating insulin as the first-line therapy for newly diagnosed T2DM patients. Methods: A PubMed search using keywords ‘Type 2 Diabetes Mellitus’ and ‘Early STIIT’ included RCTs assessing beta cell function, insulin resistance, glycemic control, and lipid profiles. Revman 5.4.1 software was used for meta-analysis, with outcomes represented as mean difference (MD) and 95% confidence intervals (CI). Results: Significant reductions in fasting blood glucose (FBG: MD -4.75, 95% CI -7.07, -2.43), HbA1c (MD -1.84, 95% CI -3.01, -0.68), and postprandial glucose (PPG: MD -9.02, 95% CI -10.48, -7.56) were observed with early STIIT therapy compared to baseline. Beta cell function improved (HOMA-B: MD 53.70, 95% CI 27.78, 79.63) and insulin resistance decreased (HOMA-IR: MD -1.84, 95% CI -3.65, -0.04). Lipid profile improvements included reductions in total cholesterol (TC), triglycerides (TG), and LDL, with no change in HDL. BMI remained stable (MD -0.15, 95% CI -0.82, 0.51). Most patients achieved long-term remission and glycemic control without oral hypoglycemic agents. Conclusion: Early STIIT in newly diagnosed T2DM patients significantly reduces glycemic markers and maintains long-term glycemic control, preserving beta cell function. The therapy also improves lipid profiles, reducing TC, TG, and LDL. Initiating insulin as a first-line treatment shows promising results for glycemic control and overall metabolic health.
Keywords:
Subject: Medicine and Pharmacology - Clinical Medicine
1. Introduction
Diabetes mellitus encompasses a set of metabolic conditions marked by elevated blood glucose levels due to impairments in either the secretion of insulin, its action, or a combination of both factors [1]. According to the IDF Diabetes Atlas (2021), 10.5% of the adult population aged 20-79 years has diabetes, and nearly half of them are unaware of their condition. Projections from the IDF indicate that by 2045, approximately 783 million adults, or 1 in 8, will be living with diabetes [2]. Most diabetes cases can be broadly categorized into two primary etiopathogenetic groups: type 1 diabetes, characterized by a complete deficiency in insulin secretion, and type 2 diabetes, which is much more prevalent and results from a combination of insulin resistance and an insufficient compensatory response in insulin secretion [1]. Type 2 diabetes mellitus (T2DM) arises mainly from insulin resistance, characterized by an inadequate response to the cellular actions mediated by insulin, coupled with a relative insufficiency of pancreatic beta cells [3]. Type 2 diabetes is associated with elevated risks of both macrovascular (heart failure and cardiovascular disease) and microvascular (lower limb amputation, blindness, and kidney failure) complications, with higher glycated hemoglobin (HbA1c) levels linked to increased risks for both [4].
Short-term intensive insulin therapy (STIIT) has emerged as a recent recommendation for managing newly diagnosed type 2 diabetes (T2DM). Short-term intensive insulin therapy can effectively address early T2DM pathophysiological defects, leading to diabetes remission in some cases, by correcting hyperglycemia and laying the groundwork for sustained glycemic control without the need for anti-diabetic medications after insulin discontinuation [5]. Additionally, short-term intensive insulin therapy (STIIT) has offered the potential for diabetes management with reduced chronic stress associated with frequent oral hypoglycemic dosages and a notable decrease in hypoglycemic episodes, which are concerning side effects associated with first-line oral hypoglycemics. Considering the encouraging findings from existing studies and to contribute to the collective knowledge in this area, we conducted a systematic review and meta-analysis to explore the impact of short-term intensive insulin therapy (STIIT) on glycemic control as well as its influence on lipid profile and obesity.
2. Methods
We followed the PRISMA guidelines when conducting this systematic review and meta-analysis. The rules mentioned in the Cochrane Handbook for Systematic Reviews of Interventions were followed in the process.
2.1. Search Strategy
A comprehensive search of the existing body of literature was conducted by two independent researchers using the PUBMED database. The primary focus was to investigate the role of early short-term intensive insulin therapy (STIIT) in type 2 Diabetes.” The complete search for PubMed was: (“Insulin” [MeSH] OR “insulin” [Text Word]) AND (“diabetes mellitus, type 2”[MeSH Terms] OR “type 2 diabetes”[Text Word] AND ((“intensive”[Text Word])). To find RCTs that were missed by the online electronic searches, a manual search was also done among the reference lists of all known relevant publications, prior systematic reviews, and review studies. Initial screening was done considering the title and abstract, followed by full-text screening to include eligible studies. Any discrepancies in the study selection process were resolved by the third researcher.
2.2. Study Selection Criteria
The initial search yielded a substantial number of articles, which were subjected to a stringent screening process guided by predefined inclusion and exclusion criteria.
Inclusion criteria:
- 1)
- Studies that included adults aged 18 years or older with newly diagnosed type 2 diabetes mellitus
- 2)
- Studies that studied the effect of short-term intensive insulin therapy on β-cell function (assessed by Homeostasis Model Assessment of β-cell function [HOMA-B]) or insulin resistance (assessed by Homeostasis Model Assessment of Insulin Resistance [HOMA-IR]), or both, reporting means and standard deviations at baseline and after short-term intensive insulin therapy
- 3)
- Assessed patients for glycemic remission after any duration of follow-up.
- 4)
- Assessed patients for lipid profiles before and after STIIT.
- 5)
- Compared glycemic control, HOMA-B, and HOMA-IR in STIIT and OHA (oral hypoglycemic agents) groups.
- 6)
- Compared glycemic control and other outcomes of interest in remission vs. non-remission group of STIIT patients.
Exclusion criteria:
1) Observational, animal, conference, non-English studies, reviews, studies with unreliable data for extraction, studies not reporting on outcomes of interest, and if the full text was unavailable.
The included studies were independently reviewed by two reviewers using a standardized template after meeting the inclusion and exclusion criteria. A third reviewer was consulted to discuss and settle any disagreements.
2.3. Data Extraction
Two investigators independently extracted the data from the included studies in a formatted data extraction sheet that included the following characteristics of the studies: Study first author, study design, study year, sample size, and IIT regimen. IIT duration, baseline characteristics of the patients in each study, including age, sex, body mass index (BMI), and outcomes of interest, including glycemic control indicators. We extracted data on the lipid profiles, glycemic control (HbA1c, FPG, PPG), HOMA-B, HOMA-IR, and Matsuda Index for the meta-analysis. Discussions with another author helped resolve differences in data extraction. A mean and standard deviation were taken from the data for the results.
2.4. Quality and Risk of Bias Assessment
The quality of the included studies was assessed by two authors according to the Cochrane risk of bias (ROB) assessment tool. The tool aims to detect the following biases: selection bias, performance bias, detection bias, attrition bias, reporting bias, and other potential sources of bias. The authors’ judgments are categorized as low, high, or unclear risk of bias. We did not include or exclude the studies because of the risk of bias.
2.5. Data Synthesis
We reported the differences between the mean of the variables like FBG, HbA1c, PPG, HOMA-B, HOMA-IR, Matsuda Index, BMI, and lipid profiles before and after STIIT. Similarly, we calculated the mean differences for the baseline values of the similar variables between the remission and non-remission groups of STIIT. Finally, we presented the mean difference of such variables between the STIIT and OHA groups. Version 5.4.1 of Review Manager for Windows was the program we utilized. A 95% confidence interval (CI) was used in the interval estimation. When there was a lack of heterogeneity predicted by I2 ≤ 50% and p ≥ 0.05, the fixed-effect model was employed to combine the effect values. When there was heterogeneity and I2 ≤ 50% and p < 0.05 suggested this, the random-effect model was applied. The publication bias was assessed by a funnel plot of the effect size against the standard error for each study. The two-tailed Chi-square test was used to test the hypothesis, and ‘tau2’ was estimated using the DerSimonian and Laird methods to verify the heterogeneity. An inverse-variance method was used to calculate the pooled MD, expressed as a 95% confidence interval (CI). For interpretation purposes, forest plots were created. Statistical significance was defined as a P-value of 0.05. A funnel plot symmetry analysis and outlier analysis were used to detect publication bias. We also did a sensitivity analysis to address the heterogeneity in our study.
2.6. Outcomes of Interests
- i)
- Effect of STIIT on glycemic control: fasting plasma glucose (FBG), insulin level, hemoglobin A1c, homeostasis model of assessment-estimated insulin resistance (HOMA-IR), HbA1c, PPG, Matsuda Index.
- ii)
- Effect of STIIT on lipid profile and obesity: triglycerides, total cholesterol, low-density lipoprotein cholesterol (LDL-cholesterol), very low-density lipoprotein cholesterol (VLDL), and BMI
3. Results
3.1. Literature Review
A search of the electronic databases yielded 1543 articles. After removing 97 duplicate articles, 1446 remained. Through screening titles and abstracts, 1144 articles were excluded, and 302 papers were assessed based on inclusion and exclusion criteria. After a full-text assessment for eligibility, 296 articles were excluded. Resolving the conflicts resulted in 6 articles that were included in the meta-analysis, as shown in the PRISMA (Figure 1).
3.2. Study and Patient Characteristics
Quality Assessment and Risk of Bias Result:
For the selected RCTs, the results obtained after assessing the bias risk are shown in Fig. Green is used to indicate low risk, yellow to indicate some concern, blue to indicate no information, and red to indicate severe risk. Two studies had a high risk of bias, four studies had some concerns, and one study had a low risk of bias.
3.3. Outcomes of Interest
3.3.1. Glycemic Control before and after STII Therapy (Figure 2)(Figure3)
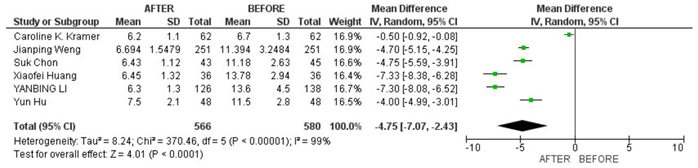
FBG: In the pooled analysis of 6 studies that included 1146 patients, there was a significant reduction in FBG after STIIT as compared to the baseline. MD[CI]: -4.75 [-7.07, -2.43] (Figure 2 Analysis 1.1).
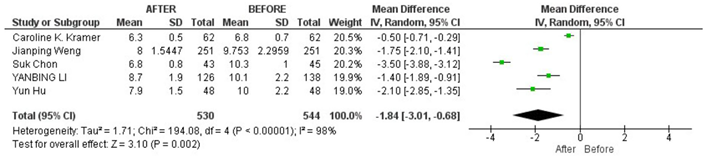
HbA1c: In the pooled analysis of 5 studies including 1074 patients, a significant reduction in HbA1c from baseline was observed after STIIT. MD[CI]: -1.84 [-3.01, -0.68] (Figure 2 Analysis 1.2).
PPG: In the pooled analysis of 3 studies that included 835 patients, a significant reduction from baseline in PPG value was observed after STIIT. -9.02 [-10.48, -7.56] (Figure 2 Analysis 1.3).

HOMA-B: The pooled analysis of 3 studies that included 774 patients showed a significant increase in HOMA-B from baseline after STIIT. 53.70 [27.78, 79.63] (Figure 2 Analysis 1.4).

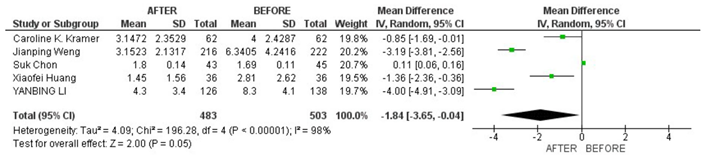
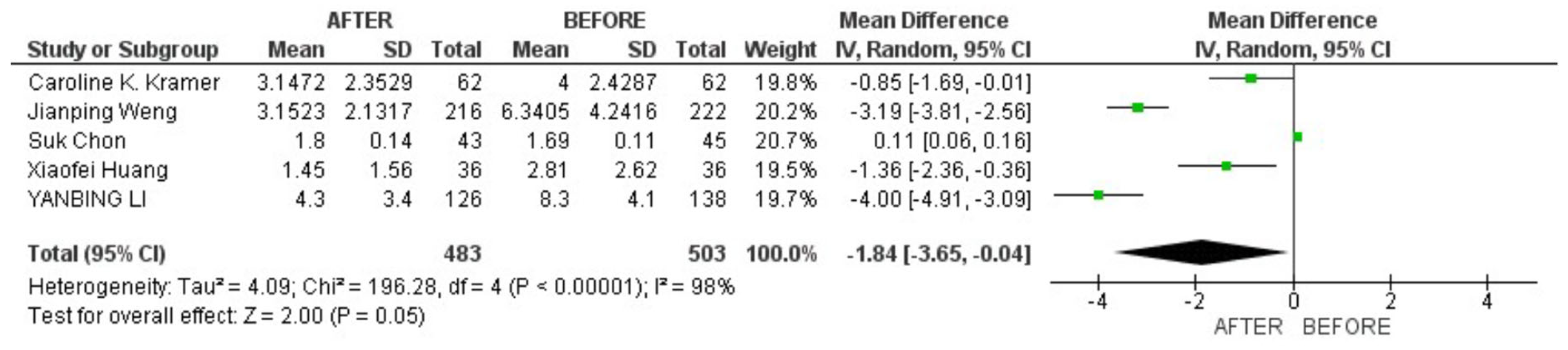
HOMA-IR: The pooled analysis of 986 patients in 5 included studies depicted a significant reduction in HOMA-IR from baseline after STIIT. -1.84 [-3.65, -0.04] (Figure 3 Analysis 1.5).
Matsuda Index: The pooled analysis that involved 2 studies did not show a significant difference between baseline and after STIIT Matsuda Index values. 0.23 [-0.11, 0.56] (Figure 3 Analysis 1.6).

(Figure 3 Analysis 1.6):
BMI: There was no significant difference between BMI before and after STIIT in the pooled analysis of 4 studies that included 572 patients. -0.15 [-0.82, 0.51] (Figure 3 Analysis 1.7)
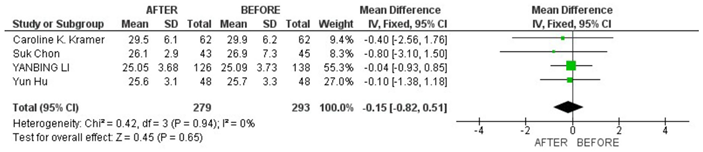
(Figure 3 Analysis 1.7).
3.3.2. Glycemic Control among Remission versus Non-Remission Group (Figure 3 and Figure 4)

Figure 3 (Analysis 1.3):
Forest plot of comparison: 1 Glycemic control before and after STII, outcome: 1.3 PPG After STII in DM.We also analyzed the differences in various baseline variables between remission and non-remission groups to find the patients better fit for STIIT. Four studies included the baseline difference among remission and non-remission groups.
Figure 4 (Analysis 1.4):

Forest plot of comparison: 1 Glycemic control before and after STII, outcome: 1.4 HOMA-B IN STII IN DM.
The remission group had a significantly higher BMI as compared to the non-remission group at baseline. 0.82 [0.24, 1.39]. However, there was no significant difference in FBG, PPG, and HbA1c values at baselines among the remission and non-remission groups. -0.14 [-0.71, 0.44] -0.45 [-1.40, 0.51] -0.01 [-1.02, 1.00]
Interestingly, those who were in remission were younger as compared to the non-remission group during the beginning of STII therapy. -1.91 [-3.76, -0.06]
Moreover, both groups had no significant difference in the time taken to achieve euglycemia. -0.05 [-0.76, 0.65]
3.3.3. Lipid Profile before and after STIIT (Figure 5)
We included 3 studies comprising a total of 849 patients for the pooled analysis of lipid profiles before and after STIIT in diabetic patients.
There was a significant reduction in TC, TG, and LDL values before and after STIIT. However, there was no significant increase in HDL values before and after STIIT.
3.3.4. STIIT versus OHA in Diabetic Patients
Figure 5.
(Analysis 1.5): Forest plot of comparison: 1 Glycemic control before and after STII, outcome.
Figure 5.
(Analysis 1.5): Forest plot of comparison: 1 Glycemic control before and after STII, outcome.
1.5 HOMA-IR IN DM BEFORE AND AFTER STII.
Patients in the STIIT group had a higher FPG as compared to the OHA group in two studies. However, there was no significant difference in the HbA1c and HOMA-IR values among the STIIT and OHA groups.
3.3.5. Long-Term Glycemic Remission
Some studies pointed out long-term remission in diabetic patients after STII. Overall, prolonged-term glycemic remission was observed in most patients. In the study by Li during follow-up, the remission rates (percentages of the subjects maintaining near euglycemia on diet alone) at the third, sixth, twelfth, and twenty-fourth months were 72.6% (82 of 113), 67.0% (61 of 91), 47.1% (32 of 68), and 42.3% (11 of 26), respectively. Similarly, in the study by Chon et al., at the end of the study (week 104), subjects treated with IIT had a 52.5% lower risk of failing drug-free glycemic remission compared to subjects treated with COAD after controlling for age, sex, BMI, and DI at the end of IT (p = 0.015; Fig. 4), i.e., subjects who initially underwent the COAD method had a hazard ratio (HR) of 2.1 for the failure of drug-free glycemic remission.
In a study by Weng et al., the remission rate at 1 year was 42·0% (148 of 352) in all patients who achieved glycemic control during the intensive interventions. The remission rate was significantly higher in both insulin groups than in the oral hypoglycemic agents’ group (p = 0·0012). The risk of relapse was reduced by 44% (95% CI 0·40–0·78, p=0·001) with CSII and by 31% (95% CI 0·50–0·97, p=0·032) with MDI compared with oral hypoglycemic agents.
A similar conclusion was seen in the study by Hu et al.: after short-term IT, 21 of 48 newly diagnosed type 2 diabetic patients (44%), comprising 8 CSII, 6 MDI, and 7 OHA subjects, achieved remission for 1 year, and 27 patients (8 in CSII, 12 in MDI, and 7 in the OHA group) had relapsed (no remission).
Discussion
Current practice advocates the use of insulin as a last resort in type 2 diabetes when glycemic targets with other hypoglycemic agents are not reached. However, recent trials have been conducted to determine the role of brief intensive insulin therapy early during type 2 diabetes and have shown promising results. Our Systematic review and metanalysis sought to evaluate the effectiveness of short-term intensive insulin therapy (STIIT) in the management of newly diagnosed type2 Diabetes mellitus.
The analysis included six studies with a total of 1146 patients and demonstrated significant improvements in several key outcomes following STIIT. The primary findings from this review indicate that STIIT significantly reduces fasting blood glucose (FBG), glycated haemoglobin (HbA1c), and postprandial glucose (PPG) levels while improving pancreatic beta-cell function (HOMA-B) and insulin sensitivity (HOMA-IR).
Glycaemic Control:
The pooled analysis revealed substantial reductions in FBG, HbA1c, and PPG values post-STIIT, indicating that this therapy is effective in achieving better glycaemic control. These results underscore the potential of STIIT to correct hyperglycaemia and lay a foundation for sustained glycaemic control.
Pancreatic Function and Insulin Sensitivity:
Improvements in pancreatic beta-cell function and insulin sensitivity were also observed. This suggests that STIIT not only addresses hyperglycaemia but also positively impacts the underlying pathophysiological mechanisms of T2DM, potentially leading to better long-term outcomes.
Impact on Lipid Profile and BMI:
STIIT was associated with significant reductions in total cholesterol (TC), triglycerides (TG), and low-density lipoprotein (LDL) levels, although no significant change was observed in high-density lipoprotein (HDL) levels. The lack of significant change in BMI before and after STIIT suggests that the therapy's benefits on metabolic parameters are independent of weight changes. This finding is particularly important, as it highlights STIIT's role in improving cardiovascular risk factors without necessitating weight loss.
Remission vs. Non-Remission Groups:
An analysis of baseline differences between remission and non-remission groups revealed that patients who achieved remission had a significantly higher BMI and were younger at the onset of STIIT. These findings suggest that younger patients with higher BMI might be more responsive to STIIT, achieving better outcomes in terms of diabetes remission. However, no significant differences were found in baseline FBG, PPG, and HbA1c values between the two groups, indicating that these factors do not predict remission.
Comparison with Oral Hypoglycaemic Agents (OHA):
Comparative analysis between STIIT and OHA groups showed that while the STIIT group had higher fasting plasma glucose (FPG) initially, there was no significant difference in HbA1c and HOMA-IR values between the two groups. This suggests that STIIT might offer additional benefits in the initial control of fasting glucose levels, although long-term outcomes might be comparable to those achieved with oral hypoglycaemic agents.
Long-Term Glycaemic Remission:
The review highlighted the potential for long-term glycaemic remission following STIIT. Various studies reported remission rates ranging from 42% to 72.6% at different follow-up intervals. This long-term remission underscores the potential of STIIT as a valuable strategy in the early management of T2DM, offering patients the possibility of prolonged drug-free periods
The management of diabetes presents a multifaceted challenge, requiring a comprehensive approach that encompasses both lifestyle modifications and pharmacological interventions. Despite the plethora of hypoglycemic agents available, a significant proportion of individuals with diabetes fail to achieve optimal glycemic targets. This failure to attain glycemic control contributes significantly to the onset and progression of devastating complications associated with diabetes, such as cardiovascular disease, nephropathy, retinopathy, and neuropathy.
Epidemiological data underscore the magnitude of the problem. According to recent studies, a substantial proportion of individuals with diabetes worldwide fail to meet recommended glycemic targets, with estimates varying across different regions and populations. For example, a meta-analysis conducted by [6] Shaw et al., (2010) reported that only about half of individuals with diabetes achieved target HbA1c levels of less than 7%, indicating a significant gap between clinical guidelines and real-world practice.
Moreover, the failure to achieve glycemic control is associated with a higher risk of developing complications and experiencing adverse outcomes. Epidemiological studies have consistently shown that poor glycemic control is a strong predictor of cardiovascular events, kidney disease progression, diabetic retinopathy, and diabetic neuropathy [7,8]. For instance, the UK Prospective Diabetes Study (UKPDS) demonstrated that every percentage point reduction in HbA1c was associated with a significant reduction in the risk of microvascular complications, emphasizing the critical importance of glycemic control in preventing diabetes-related complications [9].
It is therefore essential to prioritize the advancement of scientific understanding in therapies aimed at enhancing glycemic control.
Type 2 diabetes is characterized by a progressive decline in the functioning of beta cells [10]. In fact, up to 50% of functioning beta cell mass is lost by the time of diagnosis [11]. Progressive decline in the Beta cell functioning mass ultimately results in Beta cell failure, a situation characterized by an inability of the residual functional beta cell mass to maintain Euglycemia [12]. Progressive beta cell dysfunction in type 2 diabetes makes it challenging to achieve glycemic targets, requiring intensified antidiabetic therapy such as adding additional medications.
Various mechanisms have been described to explain the loss of beta cell functioning mass, a few of which include:
Glucotoxicity
Glucotoxicity occurs when high glucose levels impair the function of beta cells [13].
Chronic hyperglycemia leads to defects in beta cells due to the buildup of glucose inside the cells, causing stress in the endoplasmic reticulum (ER) and mitochondria. ER stress triggers a response called the unfolded protein response [14], which can ultimately lead to cell death as shown in a study by [15] where persistent moderate to severe hyperglycemia (540-1080mg/dl) has been shown to cause apoptosis of Beta cells.
Meanwhile, the excess glucose in the mitochondria leads to the overproduction of reactive oxygen species (ROS) [16]. With prolonged hyperglycemia, the integrity of the mitochondrial membrane weakens, allowing cytochrome C to leak into the cytosol, which prompts the apoptosis of beta cells [17].
Lipotoxicity
Lipotoxicity is a condition characterized by inhibition of Beta cell functioning due to lipid overload on the beta cells of the pancreas [18] and occurs via the same pathways as that of glucotoxicity like ER Stress, Oxidative stress, and impaired autophagy [19].
Islet Amyloid
Insulin amyloid polypeptide (IAPP) is a co-molecule secreted by Beta cells of the pancreas along with Insulin [20]. IAPP has the tendency to form amyloid around beta cells of the pancreas. [21] and this amyloid deposition around the beta cells has been shown to induce inflammation and apoptosis of beta cells [22].
All these stressors ultimately lead to Beta cell dysfunction by three models as put forward by Swisa et al. [23], reduced beta cell number, beta cell exhaustion, and loss of beta cell identity.
Short-term intensive insulin therapy is one of the potential ways to preserve beta cell functional mass, which means that it could alter the natural history of type 2 diabetes. Early short-term intensive insulin therapy is defined as short-term insulin administration shortly after the diagnosis of type 2 diabetes for a brief period. It has been shown in various studies to improve beta cell function, insulin sensitivity, remission of hyperglycemia, and the maintenance of normoglycemia without antidiabetic medications. It has shown a profound effect in reversing beta cell dysfunction by preventing the metabolic stress of hyperglycemia, which sets up a vicious cycle as they suppress the beta cells when present chronically.
Various mechanisms have been proposed to elucidate how short-term Intensive Insulin Therapy (STII) plays a role in managing type 2 diabetes (T2D). During the critical period of persistent hyperglycemia around the onset of clinical T2D, beta cells are particularly vulnerable to apoptosis [24].
STII addresses the initial glucotoxicity, a detrimental effect on beta cell functioning and survival. However, this alone doesn't fully explain its potential long-term benefits, including glycemic remission. Research by Weng et al. [25] demonstrated that although oral antidiabetic medications immediately achieved glycemic targets, only a minority-maintained remission at one year compared to those on continuous subcutaneous insulin infusion (CSII) or multiple daily injections (MDI), indicating insulin's pleiotropic effects beyond glucotoxicity reversal.
Improvement in beta cell function is a key mechanism. STII has been shown to enhance beta cell function and survival by reversing glucotoxicity. Objective evidence supporting this includes improvements in glycemic control markers (Fasting Blood Glucose, Postprandial Glucose, and HbA1c), lipid profiles (Total Cholesterol, Triglycerides, LDL), along with increased Homeostatic Model Assessment of Beta cell function (HOMA-B) and decreased Homeostatic Model Assessment of Insulin Resistance (HOMA-IR).
5. Strengths and Limitations
Our study includes a robust search strategy using the PubMed database, incorporating RCTs and clinical trials that focus on key outcomes such as beta cell function, insulin resistance, glycemic control, and lipid profiles with broad inclusion criteria without any age, gender, or location restriction.
Limitations
- The reliance on published studies may introduce publication bias, as studies with positive findings are more likely to be published.
- Short-term Follow-up: The duration of follow-up in the included studies might be insufficient to fully capture the long-term effects and sustainability of early STIIT on glycemic control and lipid profiles.
Conclusions
This study demonstrates that initiating early short-term intensive insulin therapy (STIIT) in newly diagnosed type 2 diabetes mellitus (T2DM) patients results in significant improvements in glycemic control, evidenced by reductions in fasting blood glucose (FBG), hemoglobin A1c (HbA1c), and postprandial glucose (PPG). Additionally, STIIT appears to enhance beta cell function and reduce insulin resistance, as indicated by increased HOMA-B and decreased HOMA-IR values. Importantly, this therapeutic approach also leads to favorable changes in lipid profiles, with reductions in total cholesterol (TC), triglycerides (TG), and low-density lipoprotein (LDL), without affecting high-density lipoprotein (HDL) levels. Despite these promising results, the study acknowledges limitations such as potential heterogeneity among included studies, possible publication bias, and the lack of long-term safety data. Nonetheless, the findings support the early use of insulin in newly diagnosed T2DM patients as a viable strategy for achieving durable glycemic control and preserving beta cell function, potentially offering a paradigm shift in diabetes management.
Author Contributions
We the authors are attesting that we have contributed a substantial amount of work to this paper. Mounika Nagarani Tunuguntla- Conceptualisation, manuscript revision, Final approval of the version to be published. Rukesh Yadav- Data analysis. Prashant Obed Reddy Dundi- critical review of important intellectual content. Pranathi Chanti- manuscript initial draft and supervision. Venkata Nitish Reddy Ummadi - manuscript initial draft. Haitham Alhussain - manuscript revision. Akshita Kaushal - manuscript initial draft and supervision. Binay Kumar Panjiyar MBBS GCSRT SOCI – Data analysis Final approval of the version to be published
References
- Diabetes, D. O. F. Diagnosis and classification of diabetes mellitus. Diabetes Care. 2009;32(Suppl. 1). Available from. [CrossRef]
- International Diabetes Federation. Diabetes facts and figures. [Internet]. Available online: https://idf.org/about-diabetes/diabetes-facts-figures/ (accessed on 4 November 2023).
- Mizokami-Stout K, Cree-Green M, Nadeau KJ. Insulin resistance in type 2 diabetic youth. Curr Opin Endocrinol Diabetes Obes. 2012;19(4):255–262. [CrossRef]
- Hippisley-Cox J, Coupland C. Diabetes treatments and risk of amputation, blindness, severe kidney failure, hyperglycemia, and hypoglycemia: Open cohort study in primary care. BMJ (Online). 2016;352. [CrossRef]
- Zheng H, Xing Y, Li F, Ding W, Ye S. Effect of short-term intensive insulin therapy on β-cell function in patients with newly diagnosed type 2 diabetes.
- American Diabetes Association. Standards of medical care in diabetes--2010. Diabetes Care. 2010 Jan;33(Suppl 1): S11-61. Erratum in: Diabetes Care. 2010 Mar;33(3):692. [CrossRef] [PubMed]
- Stratton IM, Adler AI, Neil HA, Matthews DR, Manley SE, Cull CA, et al. Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): Prospective observational study. BMJ. 2000;321(7258):405–412. [CrossRef]
- ACCORD Study Group, Buse JB, Bigger JT, Byington RP, Cooper LS, Cushman WC, et al. Action to Control Cardiovascular Risk in Diabetes (ACCORD) trial: Design and methods. Am J Cardiol. 2007;99(12A):21i–33i. [CrossRef]
- King P, Peacock I, Donnelly R. The UK prospective diabetes study (UKPDS): Clinical and therapeutic implications for type 2 diabetes. Br J Clin Pharmacol. 1999;48(5):643–648. [CrossRef]
- Wysham C, Shubrook J. Beta-cell failure in type 2 diabetes: Mechanisms, markers, and clinical implications. Postgrad Med. 2020;132(8):676–686.
- Sun T, Han X. Death versus dedifferentiation: The molecular bases of beta cell mass reduction in type 2 diabetes. Semin Cell Dev Biol. 2020;103:76–82. [CrossRef]
- Ikegami H, Babaya N, Noso S. β-Cell failure in diabetes: Common susceptibility and mechanisms shared between type 1 and type 2 diabetes. J Diabetes Investig. 2021;12(9):1526–1539. [CrossRef]
- Kawahito S, Kitahata H, Oshita S. Problems associated with glucose toxicity: Role of hyperglycemia-induced oxidative stress. World J Gastroenterol. 2009;15(33):4137–4142. [CrossRef]
- Haeri M, Knox BE. Endoplasmic reticulum stress and unfolded protein response pathways: Potential for treating age-related retinal degeneration. J Ophthalmic Vis Res. 2012;7(1):45–59. [PubMed]
- Cai Z, Liu S, Nie Y, Dong B, Li C, Zhang J, et al. Decreased Sirt3 contributes to cyclic production of reactive oxygen species and islet β-cell apoptosis in high glucose conditions. Mol Biol Rep. 2022;49(11):10479–10488. [CrossRef]
- Yu T, Robotham JL, Yoon Y. Increased production of reactive oxygen species in hyperglycemic conditions requires dynamic change of mitochondrial morphology. Proc Natl Acad Sci U S A. 2006;103(8):2653–2658. [CrossRef]
- Tomita, T. Apoptosis in pancreatic β-islet cells in type 2 diabetes. Bosn J Basic Med Sci. 2016;16(3):162–179. [CrossRef]
- Oh YS, Bae GD, Baek DJ, Park EY, Jun HS. Fatty acid-induced lipotoxicity in pancreatic beta-cells during development of type 2 diabetes. Front Endocrinol (Lausanne). 2018;9:384. [CrossRef]
- Lytrivi M, Castell A, Poitout V, Cnop M. Recent insights into mechanisms of β-cell lipo- and glucolipotoxicity in type 2 diabetes. J Mol Biol. 2020;432(5):1514-1534. [CrossRef]
- Kanatsuka A, Kou S, Makino H. IAPP/amylin and β-cell failure: Implication of the risk factors of type 2 diabetes. Diabetol Int. 2018;9(3):143–157. [CrossRef]
- Akter R, Cao P, Noor H, Ridgway Z, Tu LH, Wang H, et al. Islet amyloid polypeptide: Structure, function, and pathophysiology. J Diabetes Res. 2016;2016:2798269. [CrossRef]
- Böni-Schnetzler M, Meier DT. Islet inflammation in type 2 diabetes. Semin Immunopathol. 2019;41(4):501–513. [CrossRef]
- Swisa A, Glaser B, Dor Y. Metabolic stress and compromised identity of pancreatic beta cells. Front Genet. 2017;8:21. [CrossRef]
- Tabák AG, Jokela M, Akbaraly TN, Brunner EJ, Kivimäki M, Witte DR. Trajectories of glycaemia, insulin sensitivity, and insulin secretion before diagnosis of type 2 diabetes: An analysis from the Whitehall II study. Lancet. 2009;373(9682):2215–2221. [CrossRef]
- Weng J, Li Y, Xu W, et al. Effect of intensive insulin therapy on beta-cell function and glycaemic control in patients with newly diagnosed type 2 diabetes: a multicentre randomised parallel-group trial. Lancet. 2008;371(9626):1753-60. [CrossRef]
Figure 1.
.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



MDPI Initiatives
Important Links
© 2024 MDPI (Basel, Switzerland) unless otherwise stated