
Submitted:
24 September 2024
Posted:
24 September 2024
You are already at the latest version
Abstract
Alzheimer’s disease (AD) is a progressive, degenerative brain disorder that impairs memory and thinking skills, leading to significant economic and humanistic burdens. It is associated with various neuropsychiatric symptoms (NPSs) such as anxiety, agitation, depression, aggression, apathy, and psychosis. NPSs are common in patients with AD, affecting up to 97% of individuals diagnosed with AD. The severity of NPS is linked to disease progression and cognitive decline. NPS in Alzheimer’s disease leads to increased morbidity, mortality, caregiver burden, earlier nursing home placement, and higher healthcare costs. Despite their significant impact, clinical research on NPS in AD is limited. In clinical settings, accurately distinguishing and diagnosing NPS related to AD remains a challenge. Additionally, conventional treatments for NPS in AD are often ineffective, highlighting the need for new therapies that target these specific symptoms. Understanding these comorbidities can aid in early diagnosis and better management of AD.
In this review, we provide a summary of the various neurological and psychiatric symptoms (NPSs) associated with AD and new candidates under development for the treatment of NPSs based on their therapeutic targets and mechanisms. On top of the conventional NPSs studied far, this review adds recent advancements in the understanding of social functional impairment in AD. This review also provides information that can contribute to the advancement of studies and translational research in this field by emphasizing therapeutic targets and mechanism of action focused on AD-related NPS, rather than conventional mechanisms targeted in AD drug development. Above all, considering the relative lack of research in this new field despite the importance of clinical, medical, and translational research, it may increase interest in NPSs in AD, its pathophysiological mechanisms, and potential therapeutic candidates such as molecules with antioxidant potential.
Keywords:
Alzheimer's disease
; Neuropsychiatric symptoms
; Psychomotor symptoms
; Social function
; Pharmacotherapy
1. Introduction
Alzheimer’s disease (AD) is a progressive neurological disorder that affects cognitive function, primarily memory and thinking skills. It is the most common cause of dementia, accounting for 60-80% of cases.
AD imposes a substantial economic burden on society, encompassing direct (such as medical and non-medical expenses) and indirect costs (related to informal caregiving, lost productivity, and intangible costs). The total societal burden of AD exceeds $958 billion worldwide and is projected to increase significantly by 2050 [1]. Beyond its economic impact, AD also imposes a huge humanistic burden on individuals affected by it, their caregivers, and society. This burden encompasses emotional, psychological, and social challenges such as reduced quality of life, loss of independence, changes in relationships, caregiver stress and burnout, stigma, and overall decline in well-being.
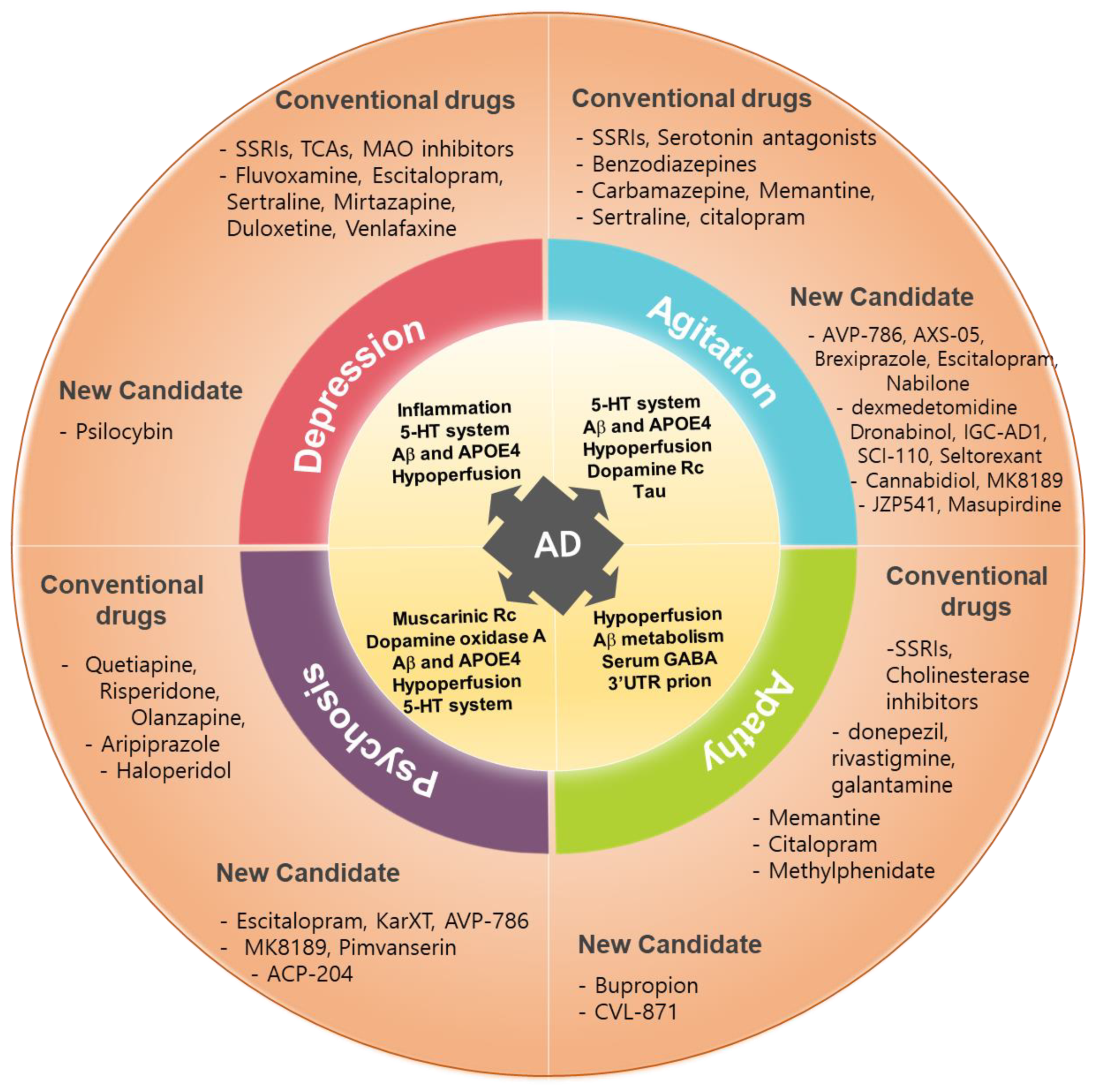
AD has predominantly been researched with a focus on cognitive function and memory decline in terms of diagnosis, management and treatment development. However, over the decades, patients, families, and healthcare providers have recognized that various behavioral, neurological, psychological, and psychiatric symptoms can accompany AD, both before and after its onset. These symptoms include depression, apathy, anxiety, agitation, aggression, personality changes, sleep disturbances, fatigue, psychosis (hallucinations, delusions, and paranoia), sensory impairment, and motor dysfunction. Collectively, these symptoms, which will be defined as neuropsychiatric symptoms (NPS) in this article, are observed in approximately one-third of individuals with dementia residing in the community, and in up to 80% of those in long-term care facilities supervised by nursing staff [2].
Analysis of comorbidities in patients with AD has revealed a combination of neurological, psychiatric, and peripheral disorders [3,4,5] with a significant involvement of reactive oxygen species and anti-oxidative system, inflammation, obesity, and hypertension as determining factors [5,6], and the trajectory of comorbidity could be different from that of the aging population without AD symptoms [7]. A study based on a Spanish cohort over a 6-year period reported a wide range of comorbidities in patients with AD. Approximately 55.1% of patients had 9-12 comorbidities, followed by 32.8% of patients with 5–8 comorbidities [8]. The most common comorbidities include hypertension, neurotic disorders, personality disorders, and other nonpsychotic disorders, as well as metabolic disorders and immune disorders [8].
The occurrence of various comorbidities, especially neuropsychiatric comorbidities, in AD varies depending on disease onset, stage, and pathological state. Sometimes, the presence of a neuropsychiatric condition obscures the detection of AD and vice versa. Therefore, identifying these neurological comorbidities and understanding their characteristics can aid in early diagnosis and treatment of AD. Additionally, the occurrence of these co-symptoms can be influenced by various factors, such as age at disease onset, level of education, and gender. Utilizing this information can help to develop personalized treatment approaches [3,4,7,9]. Furthermore, neurological comorbidities associated with AD are often not well controlled by conventional antidepressants and antipsychotics that are typically used for patients with individual disorders [4]; Ismail and Goodarzi, 2019). This highlights the urgent need for the development of new therapies that can specifically modulate NPS, indicating the presence of disease-specific mechanisms underlying NPS in AD [10]. The new treatment approach may encompass several unconventional and innovative approaches, such as genetic considerations related to AD manifestation and pathophysiology, nonpharmacologic approaches such as psychosocial paradigms, and exploration of alternative therapeutic targets such as 5-HT2A receptor antagonists/inverse agonists and 5-HT6 receptor antagonists for AD-related psychosis [10].
In this review, we aimed to provide a brief summary of the various neurological and psychiatric symptoms associated with AD, followed by a description of candidate compounds for clinical trials aimed at modulating these symptoms and their mechanisms of action. Specifically, we seek to offer information that can contribute to the advancement of research and translational studies in this field by highlighting therapeutic targets and mechanisms focusing on improving AD-related neurological and psychiatric symptoms rather than conventional mechanisms targeted in drug development. Additional attention should also be paid to social interaction deficits in AD and its pathophysiological mechanism, along with potential therapeutic candidates considering the relative scarcity of research in this emerging field, albeit of clinical, medical, and translational importance.
2. NPS in AD

Table 1.
Comparison of each neuropsychiatric symptoms of AD patients and general patients.
| NPS | Category | General patients | AD patients |
|---|---|---|---|
| Depression | Prevalence | 5% ~ 8.3% | 14.8% ~ 40% |
| Symptoms | Feeling sad, irritable, empty, disrupted sleep, hopelessness about the future, poor concentration, weight change, low energy, excessive guilt or low self-worth | Persistent feelings of worthlessness, excessive/inappropriate guilt, a pervasive loss of interest or pleasure in all activities | |
| Treatment | SSRIs (citalopram, fluoxetine, paroxetine, sertraline), SNRIs (duloxetine, vanlafaxine, levomilnacipran), Atypical antidepressants (bupropion, mirtazapine, trazodone, vortioxetine), TCAs (imipramine, desipramine, amitriptyline), MAOIs (selegiline,), | SSRIs (fluoxetine, paroxetine, sertraline, citalopram, escitalopram) | |
| Side effects | Nausea and vomiting, agitation, anxiety, indigestion, diarrhea or constipation, loss of appetite and weight loss, dizziness, blurred vision, dry mouth, excessive sweating, insomnia or drowsiness, headaches, and sexual side effects. | No significant effects | |
| Anxiety | Prevalence | 4% | 39% |
| Symptoms | Trouble concentrating or making decisions, feeling irritable, tense or restless, nausea or abdominal distress, heart palpitations, sweating, trembling or shaking, sleep problem | Excessive worry, fear, restlessness, and irritability | |
| Treatment | Benzodiazepines (alprazolam, diazepam, lorazepam), SSRIs, buspirone, TCAs (imipramine, clomipramine), MAOIs | SSRIs, SNRIs (venlafaxine), serotonergic atypical anxiolytics (buspirone), citalopram | |
| Side effects | Problems with balance and memory, drowsiness, confusion, vision problems, headaches, feeling of depression, dizziness, nausea, constipation, urinary retention, constipation | Abnormal bleeding, seizures, headaches, nausea, sleep trouble | |
| Apathy | Prevalence | 26% ~ 82% | 49% |
| Symptoms | Feeling flat, blunted, or numb emotionally, Lack of emotional reaction, low energy and motivation, lack of goal setting, less interest in pleasure activities, hobbies and relationships, anhedonia, lethargy | A decline in motivation and interest across emotional, goal-directed behavior, and cognitive activity | |
| Treatment | Antidepressants (trazodone, deprenyl, fluvoxamine), psychostimulants (methylphenidate, amphetamine), antipsychotics (risperidone), Acetylcholinesterase inhibitors (donepezil, rivastigmine), NMDA receptor antagonist(memantine) | Cholinesterase inhibitors (donepezil, galantamine, rivastigmine), methylphenidate, Ginkgo biloba, modafinil, and SSRIs | |
| Side effects | Modest weight loss, no change of depression score | Weight loss and increased anxiety, no improvement, high blood pressure, cough and osteoarticular pain | |
| Agitation &Aggression | Prevalence | 1% - 30% | 30% ~ 60% |
| Symptoms | Road rage, child abuse, sexual abuse, and domestic violence, verbally (swearing, shouting or threatening), Physically (hitting, punching, scratching or biting) | Emotional distress, excessive psychomotor activity, aggressive behaviors, disruptive irritability, and disinhibition | |
| Treatment | Haloperidol, aripiprazole, droperidol, olanzapine, | Valproic acid, brexpiprazole, Carbamazepine, SSRIs | |
| Side effects | Dizziness and nausea, paradoxical excitation, constipation, dry mouth, problems sleeping | Hepatotoxicity, GI upset, thrombocytopenia, coagulopathies, metabolic disorders, worsening cognitive dysfunction, agranulocytosis, cardiac arrhythmias | |
| Psychosis | Prevalence | 1.5% ~ 3.5% | 50% |
| Symptoms | Delusions, hallucinations, disorganized thought and behavior, poverty of speech, lack of energy, anhedonia, psychomotor retardation, catatonia | Delusions, hallucinations, disorganized thought and speech | |
| Treatment | Antipsychotics (clozapine and olanzapine), Benzodiazepines | Aripiprazole, risperidone, quetiapine, brexpiprazole | |
| Side effects | Drowsiness, dizziness, dry mouth, blurred vision, tiredness, nausea, constipation, weight gain, trouble sleeping or muscle or nervous system problems (anxiety, agitation, jitteriness, drooling, trouble swallowing, restlessness, shaking or stiffness) | Stroke, myocardial infarction | |
| Sleep disturbances | Prevalence | 20% ~ 41.7% | 45% |
| Symptoms | Excessive daytime sleepiness, irregular breathing or increased movement during sleep, depression, weight gain, lack of concentration, daytime fatigue, irritability, anxiety | Insomnia, excessive daytime sleepiness, nighttime awakenings, and alterations in sleep-wake patterns | |
| Treatment | Melatonin, zolpidem, zaleplon, eszopiclone, ramelteon, suvorexant, lamborexant or doxepin. | Melatonin, trazodone, suvorexant, lemborexant | |
| Side effects | Changes in appetite, constipation or diarrhea, dizziness, headache, daytime drowsiness, heartburn, stomach pain, burning or tingling in the hands, arms, feet or legs, mental impairment | Various results, unclear effects | |
| Social processing | Prevalence | 7% ~ 11% | 30-50%, |
| Symptoms | Difficulty using appropriate greetings, changing language and communication style, telling and understanding stories, engaging in conversation, repairing communication breakdowns, using appropriated verbal and nonverbal signals, interpreting the verbal and nonverbal signals of others, making inferences, and forming and maintaining close relationships | Language problems, personality changes and irritability | |
| Treatment | Behavior interventions, social communication treatments (comic strip conversations), social communication intervention, online speech therapy, social skills strengthening activities | N-acetyl cysteine, BDNF, NGF |
2.1. Depression
Depression in AD is characterized by persistent feelings of worthlessness or excessive/inappropriate guilt, often accompanied by a pervasive loss of interest or pleasure in nearly all activities (American Psychiatric Association, 2013, [14]). This condition significantly diminishes the quality of life, impairs activities of daily living, exacerbates cognitive decline, heightens the likelihood of physical aggression, and may hasten nursing home admission and increase mortality rates among patients with AD [15]. These symptoms serve as prognosticators of worse outcomes in patients with AD, including diminished quality of life, increased risk of self-harm and suicidality, and accelerated cognitive decline. Depressive symptoms are highly prevalent in AD, with a major depression prevalence of 14.8% [16]. Over 40% of individuals diagnosed with AD experience significant depressive symptoms over the course of their disease, a markedly higher proportion compared to the general population, which ranges from 10-15% [17,18]. Conversely, patients with depression have an elevated risk of developing AD among [19]. While the precise reasons for the heightened incidence of depression in AD patients are not been fully elucidated, it is clear that the physical and psychological distress associated with AD progression significantly contributes to the onset of depression.
In sporadic AD, tau protein abnormalities often affect key brain regions early on, including the dorsal raphe nucleus (serotonin) and locus coeruleus (norepinephrine) [20]. The loss of these diffuse systems can manifest as changes in behavior, particularly depression, anxiety, and agitation. There are indications of alterations in the serotonergic system contributing to depression in patients with AD, such as single nucleotide polymorphisms (SNPs) in 5-HT2A and 2C receptors, and the serotonin transporter (SERT), and changes in the expression levels of 5-HT1A, 2A, 2C, and SERT. However, results have been inconsistent and may vary across different brain regions and patients.
Currently, selective serotonin reuptake inhibitors (SSRIs) are the primary pharmacological treatment for depression in patients with AD owing to their relatively low side-effect profiles. However, large-scale studies and meta-analyses of carefully conducted clinical trials have revealed no significant therapeutic effects of SSRIs compared to placebo [21,22]. This lack of efficacy may be attributed to the challenges in applying common psychiatric diagnostic criteria and clinical features to a population with neurodegenerative diseases [23]. These findings underscore the pressing need to investigate the precise pathophysiological mechanisms of depression in AD and to develop more targeted medications.
2.2. Anxiety
Anxiety in AD is characterized by excessive worry, fear, restlessness, and irritability. These symptoms can exacerbate cognitive decline, hinder social interactions, and increase caregiver burden. Anxiety is distressing and common among individuals with AD, with a meta-analysis conducted in 2021 revealing a pooled prevalence of up to 39% [24]. Similar to depression, anxiety has been linked to a heightened risk of dementia and cognitive impairment [25,26].
Because of the potential for adverse effects in the elderly population, benzodiazepines are not recommended as the preferred treatment method. Currently, selective serotonin reuptake inhibitors (SSRIs), serotonin-norepinephrine reuptake inhibitors (SNRIs) such as venlafaxine, and serotonergic atypical anxiolytics such as buspirone are commonly prescribed to treat anxiety in AD patients. Recent meta-analytical studies have indicated significant therapeutic effects of certain drugs, such as citalopram, compared to control groups [27]. However, concerns persist regarding the relative efficacy and overall advantage of these drugs, considering their common side effects, particularly gastrointestinal and neurological side effects, which are more prevalent in elderly patients.
2.3. Apathy
Apathy in AD is characterized by a decline in motivation and interest across emotional, goal-directed behavior, and cognitive activity domains. Managing and supporting patients with apathy can significantly increase caregiver burden and service utilization, as individuals may struggle to make decisions or pursue life-sustaining goals. Apathy is the most common NPS in AD, with a prevalence exceeding 49%, is often linked with functional impairment, and has become a focal point for treatment interventions [28,29]. Importantly, apathy can persist throughout the disease progression [30,31]. However, distinguishing between apathy and depression poses a challenge. While apathy and depression may coexist or be mistaken for one another, antidepressants have not demonstrated efficacy in treating apathy, and may even exacerbate it. Regrettably, evidence from treatment studies is generally of low quality, largely because of the variability in the measurement tools employed. Secondary analyses have shown potential effectiveness of cholinesterase inhibitors, but not of memantine, although prospective studies remain limited. Based on a recent Cochrane review, the most compelling evidence thus far supports the use of methylphenidate at a daily dose of 20 mg, making it the recommended first-line agent in cases where cholinesterase inhibitors are not used [32]. Various other interventions, such as Ginkgo biloba, modafinil, and SSRIs, have been investigated the treatment of apathy in AD, but their efficacy varies, and some may be associated with side effects or offer limited benefits [15]. Apathy represents a critical aspect of NPS in AD, highlighting the urgent need for novel treatment targets and therapeutic advancements in this area.
2.4. Agitation and Aggression
Agitation and aggression are prevalent in AD, and their frequency escalates as the disease advances, thereby augmenting the economic burden and challenges in caregiving. Aggression occurs in approximately 30% of AD patients, and may increase to 60% among AD patients living in long-term care facilities [15,33,34]. Agitation, a nonspecific symptom, leads to variability in the study population. While definitions may vary across studies, manifestations of agitation and aggression in patients with AD include restlessness, excessive fidgeting, verbal abuse, shouting, and even physical violence. Recently, the International Psychogeriatric Association (IPA) introduced a syndromic definition, categorizing agitation into excessive motor activity, verbal aggression, and physical aggression [35]. Antipsychotics and benzodiazepines have been used to address these symptoms, albeit with heightened risks of adverse reactions, such as falls, cognitive decline, and delirium, particularly among the elderly. Furthermore, discontinuing antipsychotic treatment abruptly can exacerbate agitation and aggression, thereby establishing an unfavorable cycle [36].
Likewise, the utilization of mood stabilizers such as valproic acid is linked to diverse adverse effects and varying degrees of effectiveness [37]. Brexpiprazole, an atypical antipsychotic, was approved by the FDA specifically for treating agitation symptoms in AD based on comparative clinical trials that demonstrated its superiority over other antipsychotics in alleviating these symptoms [38]. Considering the pharmacological mechanism of brexpiprazole, which entails partial agonism of serotonin 5-HT1A and dopamine D2 receptors and antagonism of serotonin 5-HT2A receptors, further investigation is warranted to ascertain whether its specific pharmacology confers superior therapeutic potential in this particular patient cohort.
2.5. Psychosis
Psychosis, characterized by delusions, hallucinations, and disorganized thought and speech, typically worsens as AD progresses and isoften accompanied by agitation and aggression in affected patients. Psychosis in AD leads to confusion, fear, distress, paranoia, mistrust, and behavioral disturbances, impacting communication, caregiving, relationships, and patient management. Moreover, psychosis in AD is associated with poor clinical outcomes, including accelerated cognitive decline. It is estimated that up to 50% of patients with AD will experience some form of psychosis during the disease course, usually in later stages, although its severity and duration vary among individuals [39]. Despite being relatively less investigated, AD patients with aphasia and psychosis may exhibit further challenges due to disorganized thought and speech, complicating social functioning as the disease advances [40].
When evaluating evidence for the treatment of agitation and psychosis in dementia, it is crucial to recognize that different assessment measures may vary in capturing symptoms and response to treatment. Similar to agitation, the IPA and the International Society to Advance Alzheimer’s Research and Treatment NPS Professional Interest Area are in the process of developing a revised syndromic definition for psychosis in dementia [41].
There have been mixed outcomes with both traditional and newer versions of antipsychotics such as aripiprazole, risperidone, quetiapine, brexpiprazole, and anticonvulsants (Ismail and Goodarzi, 2019). Similar to other medications used for NPS, the administration of antipsychotics should be meticulously determined and monitored because of the wide range of potential adverse reactions associated with this class of medication, including, but not limited to, increased sedation, cognitive decline, extrapyramidal side effects, and cardiovascular risks.
Numerous new agents are currently under investigation for managing agitation and psychosis in patients with AD. Dextromethorphan-quinidine has demonstrated efficacy in treating pseudobulbar affect and is currently being explored for its potential in AD treatment [42]. Dextromethorphan acts as a sigma-1 and mu opioid receptor agonist, inhibits serotonin and norepinephrine transporters, and also exhibits antagonist properties at NMDA and nicotinic α3β4 receptors. When combined with quinidine, it extends its half-life, which would otherwise be too short. Additionally, pimavanserin, which is already approved for treating psychosis in individuals with Parkinson’s disease, is also undergoing investigation for its application in AD [43].
2.6. Sleep Disturbances
Most patients with AD typically encounter various sleep difficulties, including insomnia, excessive daytime sleepiness, nighttime awakenings, and alterations in sleep-wake patterns. Research suggests that approximately 45% of AD patients experience some form of sleep disturbance [44,45]. Recent meta-analyses have highlighted that insomnia is associated with an increased risk of cardiovascular and mental disorders, including AD [46].
While changes in sleep architecture and physiology are common in normal aging, pronounced sleep issues in AD not only disrupt the patients’ and caregivers’ quality of life but also significantly impact the disease’s pathophysiology and progression. Sleep disruption, including sleep apnea, is recognized as a prominent factor contributing to the onset of AD [47,48]. Studies indicate that sleep deprivation in animals mirrors the behaviors observed in AD patients [49] and can elevate amyloid beta levels in the cerebrospinal fluid after just one day of sleep disturbance in middle-aged men [50]. Reduced sleep may lead to prolonged neural activity, resulting in increased amyloid beta production, reduced clearance, and subsequent plaque formation, thereby perpetuating a cycle of sleep deficits [47].
Polysomnographic studies reveal that AD patients exhibit various sleep abnormalities compared to healthy individuals, including decreased total sleep time, reduced sleep efficiency, alterations in slow-wave sleep (SWS) and rapid eye movement (REM) sleep, as well as increased sleep latency, wake time after sleep onset, number of awakenings, and REM latency [45]. Although evidence supporting alterations in sleep EEG frequency components and sleep spindles in AD is limited, these changes have also been noted [45].
Given reports suggesting the potential impact of sleep management on AD pathology and functional performance, understanding the characteristics of sleep deprivation in AD patients and its underlying mechanisms is vital for developing more effective and safe treatment methods [51,52]. Common pharmacological treatments for sleep disturbances in AD include melatonin and its receptor activators (e.g., ramelteon), antidepressants (such as trazodone), and orexin antagonists (like suvorexant and lemborexant) [51]. However, clinical trials assessing the efficacy of these medications on sleep disturbances in AD patients have shown varying results, with some indicating only modest improvements and significant individual differences in response. In many of these clinical trials, it remains uncertain whether there’s improvement in certain aspects of sleep architecture, such as the frequency of nighttime awakenings, compared to more obvious parameters like total sleep duration and the onset time to fall asleep. Non-pharmacological interventions, including behavioral strategies, environmental adjustments, and cognitive-behavioral therapy for insomnia, are often preferred by researchers and physicians due to their lower risk of side effects and drug interactions [53]. This highlights the need for the development of more effective therapeutic approaches to address this unmet medical need.
2.7. Social Processing
Social interaction plays a crucial role in the pathophysiology of AD. AD patients often exhibit reduced social engagement [54,55]. Disease-related phenotypes, such as language problems, personality changes and irritability, may contribute to this reduced social processing as well as the neurobiological changes hampering the proper functioning of brain circuits responsible for regulating social interaction [56]. Active and prolonged social participation may reduce the risk of developing dementia by 30-50%, although the exact causality remains unclear. It is postulated that social engagement enhances cognitive reserve and promotes brain maintenance, potentially through stress reduction and improved cerebrovascular health [57]. While interventions targeting social participation have demonstrated improvements in cognition, long-term studies specifically addressing dementia risk reduction are rare with short term comparative studies did not consistently provided positive results [57].
The link between social behaviors and cognitive deficits in animal models of AD has been extensively investigated. Social isolation exacerbates cognitive impairment [58], although the precise neurobiological mechanisms remain elusive [58,59]. Possible mechanisms include increased production of Aβ peptide, tau protein phosphorylation [60,61], elevated oxidative stress, inflammatory reactions [62], impaired anti-inflammatory responses [63], altered synaptic plasticity (reduction in brain-derived neurotrophic factors (BDNF) [64,65], and myelination changes [66]. Ali et al. investigated the role of social isolation as a risk factor for AD development in animal models by isolating rats for 4 weeks [58]. Prolonged social isolation led to neurological damage in the brain, evidenced by significant increases in markers such as Aβ, AChE, MDA, TNF-α, and IL-1β, along with decreases in SOD, TAC, BDNF, and monoamines. These findings have been corroborated by histopathological changes observed in various brain regions, which is more pronounced in AD models. Isolation also enhanced DNA fragmentation induced by AD, providing insights into the impact of social relationships on cognitive health [58].
In line with the results described above, N-acetyl cysteine administration has been reported to decrease cognitive impairment in socially isolated mice [67]. Increased social interaction has also been associated with the normalization of memory and cognitive function deficits in an AD animal model, achieved through elevated expression of BDNF. Interestingly, BDNF, which plays a crucial role in synaptic plasticity and regulation of cognitive function, can be epigenetically influenced by social interactions [61,68]. Early life-time social enrichment, such as the communal nest paradigm in mice, leads to higher NGF and BDNF levels in the brain. Adult mice exposed to this enrichment exhibit greater social propensity and achieve a more prompt social dominance behavioral profile which demonstrates how early social enrichment can influence social behavior and neurotrophic factor levels in the brain, highlighting the importance of social interactions in normal brain functioning [69].
Given these mechanisms, enhancing social interaction may contribute to better disease outcomes in human AD patients. However, further research is needed to fully investigate this possibility.
Among the six domains of neurological function outlined by the Research Domain Criteria (RDoC) of the NIH, only the aspect concerning the “multi-dimensional modulation of social processing” remains resistant to clinicopharmacological modulation. As a result, cognitive-behavioral modulation and social support programs emerge as the sole viable options for enhancing social interaction in AD patients at the moment. The development of drugs aimed at improving sociability, similar to social enhancement therapeutics used for conditions like autism spectrum disorder, may hold promise for modulating social impairments in AD patients, which could be the crucial step to determine whether enhancing sociability positively impacts the course of AD.
2.8. Implication from the NPS in AD
There are several implications arising from the aforementioned studies examining the relationship between NPS and AD, as well as AD-related dementia. Firstly, the comorbidity of NPS in AD is influenced by co-existing variables such as disease onset time, disease stage, gender, socio-economic status, family history, and so forth. Secondly, the presence of NPS not only affects the care and management of AD patients but also influences the pathophysiology and prognosis of AD. Thirdly, AD neuropathology correlates with the severity of NPS in general, with varying degrees of correlation among different symptoms. Certain NPS are more common in specific subsets of AD-related disorders (ADRD). For example, hallucinations were more frequent in individuals with both AD and Lewy body disease (LBD) neuropathology compared to LBD alone. Apathy and disinhibition were common in individuals with behavioral variant frontotemporal lobar degeneration and hippocampal sclerosis.
Lastly, commonly used medications, while generally effective, do not consistently provide sufficient therapeutic efficacy or safety profiles for AD patients. This phenomenon cannot be solely explained by the age profile of AD patients, indicating that sophisticated mechanisms are at play in modulating specific neurobehavioral, neurobiological, and neurochemical determinants underlying the regulation of specific NPS. For example, Consentino et al. suggested that social cognition in AD patients is separable construct from general cognition [70]. It is evident that neuronal death, synaptic degeneration, and functional deficits may work in concert with neurochemical and neurobiological deficits secondary to changes occurring in specific regions of the AD brain. Carefully designed and conducted clinical trials sometimes yield promising therapeutic effects against certain NPS in the AD population, suggesting that it might be possible to target specific neurobiological mechanisms relevant to NPS in AD patients.
3. Treatment Pipelines, Targets, and Mechanism of Actions
Table 2.
Candidates and mechanism of action under development for the treatment of AD-related neuropsychiatric symptoms.
Table 2.
Candidates and mechanism of action under development for the treatment of AD-related neuropsychiatric symptoms.
| Candidate drugs | Target | Mechanism of Action | Target NPS | Disease stage of AD | Clinical status | References |
|---|---|---|---|---|---|---|
| Lumateperone (Caplyta) | Neurotransmitter receptors | A 5-HT2A antagonist, a SERT inhibitor, DRD2 antagonist, a GluN2B modulator | Depression | [71,72,73,74] | ||
| Psilocybin | Neurotransmitter receptors | A modulator of 5-HT1A, 5-HT2A and 5-HT2C receptors | Prodormal/Prodromal-Mild | Phase 1 | [75,76,77] | |
| Cannabidiol | Neurotransmitter receptors | Cannabinoid, An agonist against 5-HT1A, A2A and TRP-V1 receptors, Anti-inflammatory action |
Anxiety | Mild-Moderate dementia Prodormal/Prodromal-Mild |
Phase 1 Phase 2 |
[78,79] |
| Dextromethorphan | Neurotransmitter receptors | NMDA receptor antagonist; σ-1 receptor agonist A SERT and NET inhibitor A nicotinic σ3β4 receptor antagonist |
Agitation | [11,80,81,82,83,84] | ||
| AVP-923 (Neudexta) | Neurotransmitter receptors | dextromethorphan/ quinidine |
Mild-Moderate dementia Severe dementia |
[83,85,86] | ||
| AXS-05 | Neurotransmitter receptors | dextromethorphan/ bupropion NMDA receptor antagonist; σ-1 receptor agonist A SERT and NET inhibitor |
Mild-Moderate dementia Severe dementia |
Phase 3 | [87,88,89] | |
| Nabilone | Cannabinoid receptor | A partial agonist against CB1 and CB2 receptor | Mild-Moderate dementia Severe dementia |
Phase 3 | [90,91] | |
| Brexpiprazole | Neurotransmitter receptors | A partial agonist against D2, D3 receptor and 5-HT1A. A serotonin and dopamine modulator |
Mild-Moderate dementia Severe dementia |
[38,92,93] | ||
| AVP-786 | Neurotransmitter receptors | NMDA receptor antagonist; σ-1 receptor agonist A SERT and NET inhibitor |
Mild-Moderate dementia Severe dementia |
Phase 3 | [12,94] | |
| Dexmedetomidine | Neurotransmitter receptors | An α2 adrenergic agonist | Mild-Moderate dementia Severe dementia |
Phase 3 | [95,96,97] | |
| JZP541 | Cannabinoid receptor | An agonist against CB1 and CB2 receptor | Mild-Moderate dementia Severe dementia |
Phase 2 | [12] | |
| Dronabinol | Cannabinoid receptor | A weak partial agonist against CB1 and CB2 receptor | Mild-Moderate dementia | Phase 2 | [98,99,100] | |
| IGC-AD1 | Cannabinoid receptor | Cannabinoid, A partial agonist against CB1 receptor |
Mild-Moderate dementia Severe dementia |
Phase 2 | [12,79] | |
| Prazosin | Neurotransmitter receptors | An α1 adrenergic antagonist | Phase 2b | [101,102] | ||
| SCI-110 | Neurotransmitter receptors | Tetrahydrocannabinol and palmitoylethanolamide | Mild-Moderate dementia | Phase 2 | [103,104] | |
| THC-Free CBD | Cannabinoid receptor | An agonist against CB1 and CB2 receptor | Mild-Moderate dementia Severe dementia |
Phase 2 | [105,106] | |
| Masupirdine | Neurotransmitter receptors | A 5-HT6 receptor antagonist | Mild-Moderate dementia | Phase 3 | [107,108,109,110] | |
| MK-8189 | Phosphodiesterase | A PDE10a inhibitor | Mild-Moderate dementia | phase 1 | [111] | |
| Pimvanserin | Neurotransmitter receptors | A selective inverse agonist of the serotonin 5-HT2A receptor | Psychosis | Phase 3 | [43,112,113] | |
| ACP-204 | Neurotransmitter receptors | A potent and selective antagonist/inverse agonist of 5-HT2A receptor | Mild-Moderate dementia Severe dementia |
Phase 2 Phase 3 |
[11,12,79,114] | |
| KarXT | Cholinergic modulator | A dual M1/M4 muscarinic acetylcholine receptor agonist | Mild-Moderate dementia | Phase 3 | [115,116,117,118,119] | |
| Seltorexant | Orexin system | A selective antagonist of the orexin-2 receptor | Sleep disturbances | Mild-Moderate dementia | Phase 2 | [120,121] |
| SLV | Neurotransmitter receptors | A selective 5-HT6 receptor antagonist | Social processing | [122] | ||
| N-acetyl cysteine | Redox system | An antioxidant and glutathione inducer | [67] | |||
| BDNF | Neurotrophic factor | A member of the neurotrophin family, TrkB activation | [61,68,69] | |||
| Oxytocin | Endocrine system | a nonapeptide hormone, oxytocin receptor activation | [123,124,125] |
3.1. An Antagonist of NMDA Receptor Dextromethorphan
Recently, dextromethorphan has gained attention as a candidate substance for treating AD and NPS accompanied to AD. Previously used as a cough suppressant, its protective mechanisms are known to reduce brain cell damage and suppress inflammation. These properties have drawn the interest of researchers as they might help inhibit neuronal degeneration and delay the progression of the disease in AD patients. Chen et al. reported that individuals who used dextromethorphan had a lower risk of developing dementia compared to those who did not use it, even after adjusting the age and other variables [80]. Notably, dextromethorphan not only reduces the onset of AD in proportion to its amount of usage but also significantly decreases dementia onset caused by various risk factors for AD, including liver and kidney diseases, diabetes, and cardiovascular diseases [80]. This suggests broad potential for dextromethorphan in mitigating dementia risk across different health conditions.
In addition to its neuroprotective effects, dextromethorphan possesses pharmacological profiles as an NMDA receptor antagonist, σ-1 receptor agonist, serotonin and norepinephrine transporter inhibitor, and nicotinic σ3β4 receptor antagonist, all of which has been implicated in the modulation of neurological disorders, although the efficacy is relatively weak. For example, modulation of σ-1 receptor has been implicated in regulating symptoms and disease progression in various neurodegenerative and neurodevelopmental disorders. While the precise mechanisms are not yet clearly demonstrated, they appear to be a pleiotropic. These mechanisms include calcium shuttling into mitochondria, increased ATP production, trafficking of NMDA receptors, modulation of synaptic transmission through SK channels, and regulation of channels such as L-type Ca2+ channels, voltage-gated Na+ channels, and A-type K+ channels etc [81]. By acting as a σ-1 receptor agonist, dextromethorphan inhibits presynaptic glutamate release, potentially contributing to the modulation of synaptic transmission and providing a neuroprotective mechanism [82]. In addition to neurochemical and neurophysiological changes, dextromethorphan also modulates glial survival and inflammatory activation. It reduces microglia-mediated dopaminergic neuron degeneration, inhibits NOX-2 transcription, and decreases the production of TNF-α, NO and superoxide anion. Madeira et al. suggests that dextromethorphan reduces lesion size and neuronal cell death, possibly by lowering microglial activation. Furthermore, it promotes oligodendrocyte and progenitor cell proliferation and differentiation, affecting myelination processes [11].
One drawback of dextromethorphan as a CNS drug candidate is its poor brain penetration and the side effects of both the drug itself and its metabolite [126]. Dextromethorphan is commonly abused due to its euphoric, hallucinogenic, and dissociative properties, especially at high concentrations (Raiborde et al., 2022). Additionally, dextromethorphan may lead to various adverse events, including hypertension, seizures, tachycardia, psychosis, and rhabdomyolysis, depending on the amount ingested.
Due to the strong metabolism of dextromethorphan by the cytochrome P450 (CYP) liver enzyme CYP2D6, it exhibits high first-pass metabolism and low bioavailability, along with substantial individual variation in pharmacokinetic parameters. To enhance its effectiveness, a pharmacological approach combines dextromethorphan with another drug to prevent its metabolism, thereby increasing its bioavailability in the brain. Co-administration of a small dose of quinidine with dextromethorphan decreases the latter’s metabolism, resulting in a 25-fold increase in the concentration of free dextromethorphan. This allows free dextromethorphan to effectively reach the brain and exert its neurological and psychiatric effects [83,84].
3.1.1. AVP-923
An incrementally modified drug combination of dextromethorphan and quinidine has demonstrated significant efficacy in reducing agitation and aggression of AD patients compared to placebo [35,127]. The combination of dextromethorphan and quinidine sulfate, administered at a dose of 20 mg/10 mg twice daily (Neudexta or AVP-923), is approved for treating pseudobulbar affect in the United States and European Union. Evidence suggesting a potential effect of dextromethorphan/quinidine for agitation in dementia comes from controlled clinical trial data in non-demented patients with pseudobulbar affect [83]. However, subsequent studies yielded a mixed result.
3.1.2. AVP-786
Following successful findings in the phase 2 trial with AVP-923, the FDA granted a fast-track designation to the deuterated sister compound, AVP-786, for direct investigation in phase 3 trials targeting agitation in AD [128]. Deuteration of dextromethorphan was shown to reduce the amount of quinidine needed to achieve an effective plasma concentration of free dextromethorphan, thereby minimizing drug-drug interaction and cardiac side effects typically associated with quinidine. Apart from the pharmacokinetic alteration, deuteration of dextromethorphan did not show to affect the selectivity and affinity for brain receptors implicated in neuropsychiatric effects. The two completed phase 3 trials with AVP-786, sponsored by Avanir Pharmaceuticals (TRIAD-1 (NCT02442765) and TRIAD-2 (NCT02442778)), yielded contradictory findings, potentially due to differences in clinical study design - one study adopted a sequential parallel comparison design, while the other followed a more conventional study approach, highlighting the need for large-scale confirmatory clinical trials [94].
3.1.3. AXS-05
Another combination, dextromethorphan/bupropion, is FDA-approved for treating major depression in adults. This combination demonstrated promising results in a Phase 2 trial for agitation in dementia and also in a couple of Phase 3 trials [87]. Bupropion is a norepinephrine and dopamine reuptake inhibitor commonly used as an antidepressant, which serves to increase the bioavailability of dextromethorphan by acting as a strong CYP2D6 inhibitor. It was reported that add on treatment of dextromethorphan with bupropion XL leads to rapid-acting antidepressant effects within 48 hours in treatment-resistant depression [88,89]. In the multicenter, double-blind, placebo-controlled phase 2/3 study (ADVANCE-1) using dextromethorphan/bupropion (AXS-05) in 366 AD patients with agitation, the dextromethorphan/bupropion combination showed better efficacy compared to bupropion alone and placebo. This combination has received FDA designation for breakthrough therapy. More recent results from the AXS-05 phase 3 trial (ACCORD study, ClinicalTrials.gov Identifier: NCT04797715), which composed of an open-label period followed by a randomized placebo-controlled study period in patients with a diagnosis of probable AD and clinically meaningful agitation associated with the disease, demonstrated significant delay and reduction of AD-related agitation relapse.
3.2. An Inverse Agonist and Antagonist 5-HT2A Receptor
3.2.1. Pimavanserin
Another actively investigated candidates for NPS in AD is pimavanserin, an atypical antipsychotic. Pimavanserin acts an inverse agonist and antagonist at serotonin 5-HT2A receptors, with lesser potency at 5-HT2C receptors and almost negligible affinity against dopamine receptor. It has been approved for treating psychosis associated with PD, sold under the brand name Nuplazid, and is actively being studied for a similar indication in patients with AD [43,112,113]. However, a phase 3 randomized controlled trial (RCT) examining the effect and safety of 20 mg and 34 mg of pimavanserin treatment on the relapse of hallucinations and delusions associated with dementia-related psychosis (NCT03325556) revealed only marginal efficacy of pimavanserin over placebo for this indication. Nonetheless, it demonstrated an excellent safety profile in another phase 3b trials [129], which necessitates further carefully designed studies.
3.2.2. ACP-204
ACP-204 is an inverse agonist and potent antagonist at the 5-HT2A receptor, developed by Acadia Pharmaceuticals for the treatment of hallucinations and delusions associated with AD’s psychosis (ADP) [12]. Currently, ACP-204 is under clinical development in both phase 2 and phase 3 for ADP (NCT06159673, NCT06194799).
3.3. A Partial Agonist of Dopamine D2 Receptor and 5-HT1A Receptor
3.3.1. Brexpiprazole
Brexpiprazole (Rexulti), developed by Otsuka and Lundbeck, grained the FDA approval in July 2015. It’s an atypical antipsychotic medication used to treat major depressive disorder, schizophrenia, and agitation associated with dementia due to AD [38,92]. Brexpiprazole targets noradrenergic, serotonergic, and dopaminergic neurotransmitter systems. It is a partial agonist of dopamine D2/D3 receptor and 5-HT1A receptor, which is known as a serotonin-dopamine activity modulator (SDAM) [93]. Notably, Brexpiprazole is the first treatment approved by FDA for agitation associated with dementia due to AD (Ajenikoko, 2023).
3.4. An Antagonist of 5-HT2A and Dopamine (D1, D2 and D4) Receptor
3.4.1. Lumateperone
Lumateperone (ITI-007, ITI-722) received its initial approval from the FDA in the USA in December 2019 for treating schizophrenia in adults. Its therapeutic efficacy is under investigation for bipolar depression, behavioral disorders linked to AD and dementia, sleep disorders, and major depressive disorders [71,72]. Pharmacodynamically, lumateperone exhibits potent antagonistic activity at serotonin 5-HT2A receptors and is a serotonin transport (SERT) inhibitor. Additionally, it functions as a presynaptic partial agonist and a postsynaptic antagonist at dopamine D2 receptors, along with being a dopamine D1 receptor-dependent indirect modulator of GluN2B receptors [73]. Given this multi-target activity, lumateperone has the potential to modulate depressive symptoms and irritability by attenuating overt neural activity, although direct clinical evidence is needed in the future.
3.5. Glutamate Receptor Modulator and an Inositol Monophosphatase Inhibitor
3.5.1. Lithium
Another candidate for modulation of NPS in AD is lithium, which is clinically used for bipolar disorders and manic psychosis. Although the exact mechanism of action of lithium as a mood stabilizer is unknown, it has been shown to modulate glutamate receptors (especially GluR3) and inhibit inositol monophosphase [130]. In a four-site randomized clinical trial, low-dose lithium failed to significantly alleviate agitation in AD patient but was associated with global clinical improvement and was generally considered safe [131].
3.6. Norepinephrine Modulators
3.6.1. Prazosin
It has been theorized that norepinephrine is functionally overactive compared to other prominent neuromodulators such as dopamine and serotonin in AD, which suggests novel combinations of pharmacological agents to counteract AD [101]. Phase IIb clinical trials using the α1 adrenergic antagonist prazosin to assess efficacy against agitation in AD patients have been completed, albeit with reduced participant sizes due to the COVID pandemic, and await final report. Similarly, maintaining adequate level of norepinephrine is proposed to be pivotal in maintaining proper neural function. Therefore, the use of norepinephrine-modulating drugs is suggested as an interesting alternative therapeutic option for AD. [102]. Targeting the noradrenergic system in preclinical models using norepinephrine reuptake inhibitors, monoamine oxidase inhibitors, α2 adrenergic antagonists, L-DOPS, tyrosine hydroxylase potentiation, and direct locus coeruleus stimulation has been shown to modulate AD pathophysiology and memory impairment. These mechanisms include reduced inflammation, diminished amyloid burden, neuroprotection, glial modulation, and regulation of neurotrophic factors [102].
3.7. Cannabinoid Receptors
Medical cannabis containing CBD and THC, such as Epidiolex and Sativex, has been approved and used for several neurological conditions, such as epilepsy associated with Lennox Gastaut syndrome, Dravet syndrome, Tuberous sclerosis as well as multiple sclerosis [132]. Additionally, various formulations and synthetic varieties of these compounds are actively being investigated for their potential effects on NPS in AD.
3.7.1. Nabilone
A synthetic cannabinoid, is used as an antiemetic in patients undergoing cancer treatment. It acts as a partial agonist at CB1 and CB2 receptors, similar to tetrahydrocannabinol (THC). Nabilone produces dose-dependent mood elevation and psychomotor inhibition comparable to 10 or 20 mg of oral dronabinol (THC). Although nabilone has been implicated in alleviating the symptoms in fibromyalgia, neuropathic pain, and multiple sclerosis, there are reports of postoperative pain aggravation. In a 14-week clinical trial with a crossover design (including a 1-week washout period between nabilone and placebo), nabilone improved agitation, overall behavior, and caregiver distress compared to placebo. While sedation was more pronounced in the nabilone treatment group, it did not significantly limit treatment efficacy [90,91]. Ongoing research includes a phase 3 interventional study with a larger participant group (112) and a phase 2 study investigating agitation in frontotemporal dementia (NCT05742698). Although nabilone is argued to effectively reduce agitation in AD patients, it may impair cognitive functions in healthy adults.
3.7.2. Dronabinol,
the (-)-trans-enantiomer of THC, improves anorexia induced by HIV and alleviates chemotherapy-induced nausea and vomiting. As early as 1997, dronabinol was suggested to have a beneficial effect on anorexia and disturbed behavior in AD patients [98], and ongoing clinical trials explore its impact on agitation in dementia and AD [99,100].
3.7.3. JZP541
is a botanical cannabinoid drug product containing cannabidiol (CBD), cannabichrome (CBC) and delta-9-tetrahydrocannabinol (THC). JZP541, developed by Jazz Pharmaceuticals, has undergone a phase 2 clinical trial to evaluate its efficacy and safety as a treatment for irritability associated with Autism Spectrum Disorder (ASD). Recently, JZP541 is ongoing phase 2 trials to evaluate the safety and therapeutic efficacy for managing agitation in AD patients (CALM-IT, NCT06014424).
3.7.4. IGC-AD1
is a natural THC-based formulation administered in micro doses. It combines a CB1 receptor partial agonist with anti-neuroinflammatory properties and an inflammasome inhibitor targeting the upregulation of inflammasome-3. Although not yet published, it has been argued IGC-AD1 demonstrated safety and tolerability in a phase 1 clinical trial. Interim phase 2 results suggest a clinically and statistically significant reduction in agitation among patients with AD compared to placebo (NCT05543681). These findings appear more favorable than those for brexpiprazole, but further verification is needed in final, larger-scale trials. The combination of the inflammasome inhibitor is proposed to reduce amyloid-beta plaque buildup and promote mitochondrial function, potentially restoring spatial memory based on in vitro and in vivo preclinical studies.
3.7.5. SCI
-110, previously known as THX-110, is another candidate for addressing NPS in AD. SCI-110 is a combination of THC and palmitoylethanolamide (PEA), administered separately as pills. A completed phase 2 open-label trial (NCT05239390) examined the safety, tolerability, and efficacy trend of SCI -110 in AD patients with agitation. However, a larger study is needed in the future. Recently, the sponsor of SCX-110 initiated clinical trials of SCI-110 for treating Tourette syndrome. Palmitoylethanolamide (PEA) is an endogenous fatty acid amide and lipid modulator. It exerts pleiotropic effects on PPAR-alpha and other nuclear receptors, as well as cannabinoid-like G-coupled receptors GPR55 and GPR119. Although PEA does not directly bind to CB1 and CB2 receptors, it is argued to enhance the activity of anandamide [103,104]. PEA is metabolized by cellular enzymes, including fatty acid amide hydrolase (FAAH) and N-acylethanolamine acid amide hydrolase (NAAA), which play a role in the degradation of endocannabinoids.
3.7.6. While Cannabidiol (CBD)
does not directly bind to classical CB1 and CB2 receptor, its efficacy against AD and related NPS is actively under investigation. In an animal model of AD, CBD treatment enhanced cognitive function and protected against Aβ42-induced neurotoxicity [78]. These effects may be related to CBD’s anti-inflammatory action and its engagement with multiple targets, including 5-HT1A, A2A and TRP-V1 receptors [133]. However, the detailed mechanism should be verified in future studies. An ongoing open-label subchronic clinical trial is evaluating sublingual CBD solution for treating clinically significant anxiety and agitation in individuals with mild cognitive impairment or mild to moderate AD (NCT04075435). This trial may provide further evidence regarding CBD’s effectiveness in AD and NPS associated with AD.
3.8. Cholinergic Modulators
3.8.1. KarXT
is a novel dual-action agent that combines Xanomeline and Trospium. It selectively targets the M1/M4 muscarinic acetylcholine receptors in the CNS as a partial agonist. Although ligand binding analysis suggests nearly identical binding affinity for all five different muscarinic receptors, KarXT has shown promising results in clinical trials targeting schizophrenia [115]. Notably, it even addresses cognitive impairment observed in these patients [116,117]. Ongoing phase 3 clinical trials are evaluating KarXT’s efficacy against NPS in AD (NCT05511363). KarXT’s primary therapeutic principle is xanomeline, combined with the peripherally restricted muscarinic receptor antagonist trospium chloride. This combination aims to mitigate xanomeline-related adverse events associated with peripheral muscarinic receptors. Given xanomeline’s muscarinic action, it is anticipated that KarXT will mitigate cognitive impairment in AD. Moreover, the therapeutic efficacy of KarXT not only makes it feasible for targeting schizophrenia with cholinergic modulators but also for intervening in NPS associated with AD [118,119].
3.9. 5-HT6 Receptor Antagonists
The 5-HT6 receptor has recently gained attention as a potential therapeutic option in AD. However, in phase 2 clinical trials evaluating the efficacy and safety of the 5-HT6 receptor antagonist masupirdine as adjunct treatment for patients with moderate AD (concomitantly treated with donepezil and memantine), no significance was observed compared to the placebo group [107]. The 5-HT6 receptor is selectively expressed in the CNS, specifically on GABAergic interneuron, contributing to the tonic inhibition of neurotransmitter release. Selective blockade of the 5-HT6 receptor may improve learning and memory, possibly by increasing acetylcholine and glutamate output [134]. Consequently, 5-HT6 receptor antagonists hold promise as novel therapeutic candidate for addressing memory deficits in AD [109,110]. Based on subgroup analysis showing improvement in the agitation/aggression domain of the Neuropsychiatric Inventory scores during the phase 2 study, masupirdine is now undergoing phase 3 clinical trials for treating NPS in AD [108].
3.10. Orexin-2 Receptor Antagonists
Seltorexant is a selective antagonist of the human orexin-2 receptor. The neuropeptide orexin regulates wakefulness, and inhibiting orexin receptor signaling promotes sleep. The orexin system also modulates aggressive behaviors, motor behavior, reactivity to stress, anxiety, reward processing, and addictive behaviors. Seltorexant has completed phase 2 clinical trials in probable AD patients with clinically significant agitation and aggression (NCT05307692). Additionally, seltorexant is in advanced clinical development for treating depression, where its effectiveness is thought to be related to improving sleep. Given that sleep deprivation plays a critical role in the pathogenesis of AD, there is a mechanistic rationale for using an orexin antagonist to improve symptoms associated with AD. Seltorexant is being investigated as a potential treatment for agitation and aggression in people with AD [120,121].
3.11. An Agonist of Alpha 2 Adrenergic Receptor
Dexmedetomidine is an agonist of α2-adrenergic receptors having sedative, anxiolytic, hypnotic, analgesic and sympatholytic properties, inhibiting the release of norepinephrine. It has anti-inflammatory effects and cognitive enhancing effects [95,96]. It was approved by FDA for the treatment of agitation in schizophrenia and bipolar disorder in 2022 [97]. Recently, BioXcel Therapeutics conducted a phase 3 clinical trial to evaluate the safety and efficacy of BXCL501, an oral formulation of dexmedetomidine, as a treatment for agitation associated with dementia including Alzheimer’s disease (TRANQUILITY II, NCT05271552).
3.12. PDE10 Inhibitors
Among various subtypes of phosphodiesterase enzymes that degrade cAMP and cGMP, Phosphodiesterase type 10 (PDE10) is expressed in the brain, particularly within the striatum, medium spiny neurons, nucleus accumbens, and olfactory tubercle. PDE10 emerges as a potential candidate against psychiatric and neurological disorders. Reduced activation of dopamine D1 receptor signaling may contribute to negative symptoms in schizophrenia, and PDE10A, which modulates both dopamine D2- and D1-dependent signaling, is a clinical candidate aimed at improving cognitive and negative symptoms associated with schizophrenia. Additionally, PDE10 is being investigated as a promising therapeutic strategy for psychiatric and neurodegenerative diseases, based on its efficacy in animal models of schizophrenia, Parkinson’s, Huntington’s, and AD [135,136]. While negative results regarding the effect of a PDE10 inhibitor on reward-based effortful behavior and reward learning indices have been published [137], another PDE10a inhibitor, MK-8189, is currently undergoing phase 1 clinical trials in participants with AD with agitation-aggression and/or psychosis [111].
3.13. Psychedelic Compounds
3.13.1. Psilocybin
Psilocybin, is a naturally occurring psychedelic compound found in certain mushroom species, has garnered significant interest for its potential use in treating various psychiatric and neurological disorders, including treatment-resistant depression, obsessive compulsive disorders, addiction, and PTSD. Numerous preclinical and clinical studies have explored its effects [75,76,77]. The hallucinogenic and neurological effects of psilocybin are linked to its modulation of serotonergic receptors, particularly 5-HT1A, 5-HT2A and 5-HT2C. However, the therapeutic mechanism remains unclear. In the context of NPS in AD, psilocybin is being investigated in an open-label pilot clinical trial for depression in individuals with MCI or early AD (NCT04123314).
3.14. Antioxidants and Anti-Inflammatory Drugs
Oxidative stress and inflammation have long been studied as key therapeutic targets, and are recognized as pathophysiological features of neurodegenerative diseases like AD and neuropsychiatric disorders such as depression, psychosis, and aggression. High levels of reactive oxygen species (ROS) are driven by stress response, neuroinflammation, and imbalances in neurotransmitter function, and disruptions in synaptic plasticity. Many studies have demonstrated that oxidative stress is elevated in the brains of AD patients, and that the levels of antioxidants such as glutathione (GSH) are lower in the plasma of schizophrenia patients with psychotic behavior [138,139]. Studies have found a link between depressive symptoms and lower intake of antioxidants, including selenium, and vitamins (A, C, E B6, folate, and B12) [140]. Recently, findings indicate that in cases of excessive aggression coupled with depression, oxidative stress and inflammation increase along with mitochondrial dysfunction, potentially leading to reduced synaptic function and worsening depressive symptoms [141,142,143]. Additionally, research has reported that cognitive decline in socially isolated mice was mitigated by the administration of the antioxidant N-acetyl-cysteine, while anxiety and aberrant socialization were exacerbated by social defeat stress. This increase in ROS in the brain may ultimately lead to greater social impairment and depressive behavior. These findings suggest that antioxidants like N-acetyl-cysteine could help alleviate anxiety, aggression, and social deficits caused by social defeat stress [58,144]. Thus, elevated ROS activity is implicated in neuropsychiatric symptoms, including anxiety, depression, and aggression, and ROS scavenging agents have the potential to restore normal behavior by promoting neurochemical homeostasis. Notably, several antioxidant and anti-inflammatory agents, such as DHA (NCT036138844), Flos gossypii flavonoids (NCT05269173), quercetine (NCT05422885), edravone (NCT05323812), and PrimeC (NCT06185543)[12] are currently in clinical trials for AD treatment in 2024. Although these compounds are primarily being tested as disease-modifying drugs, those with antioxidative properties may emerge as promising treatments for AD-related NPSs.
3.15. Social Deficits in AD
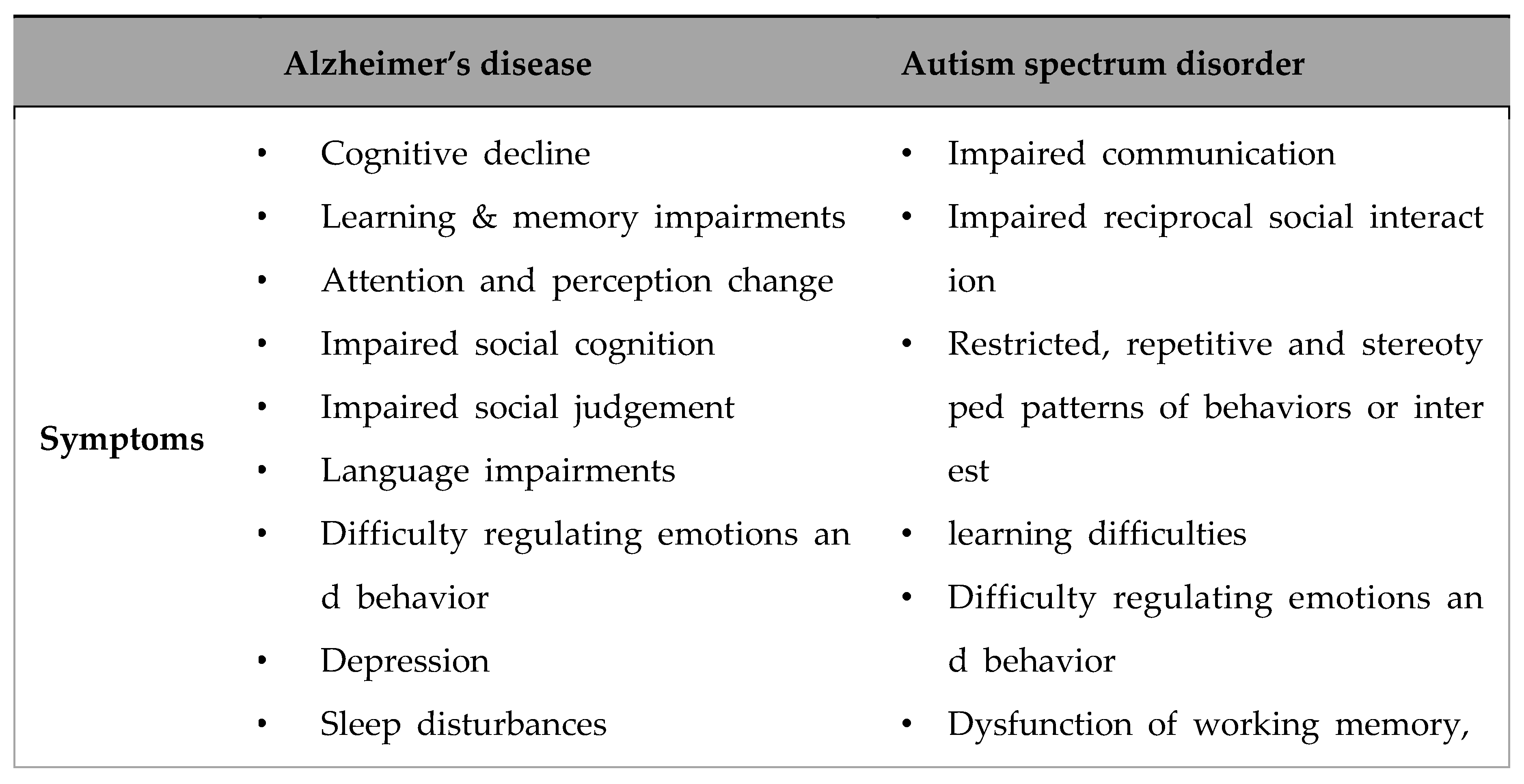
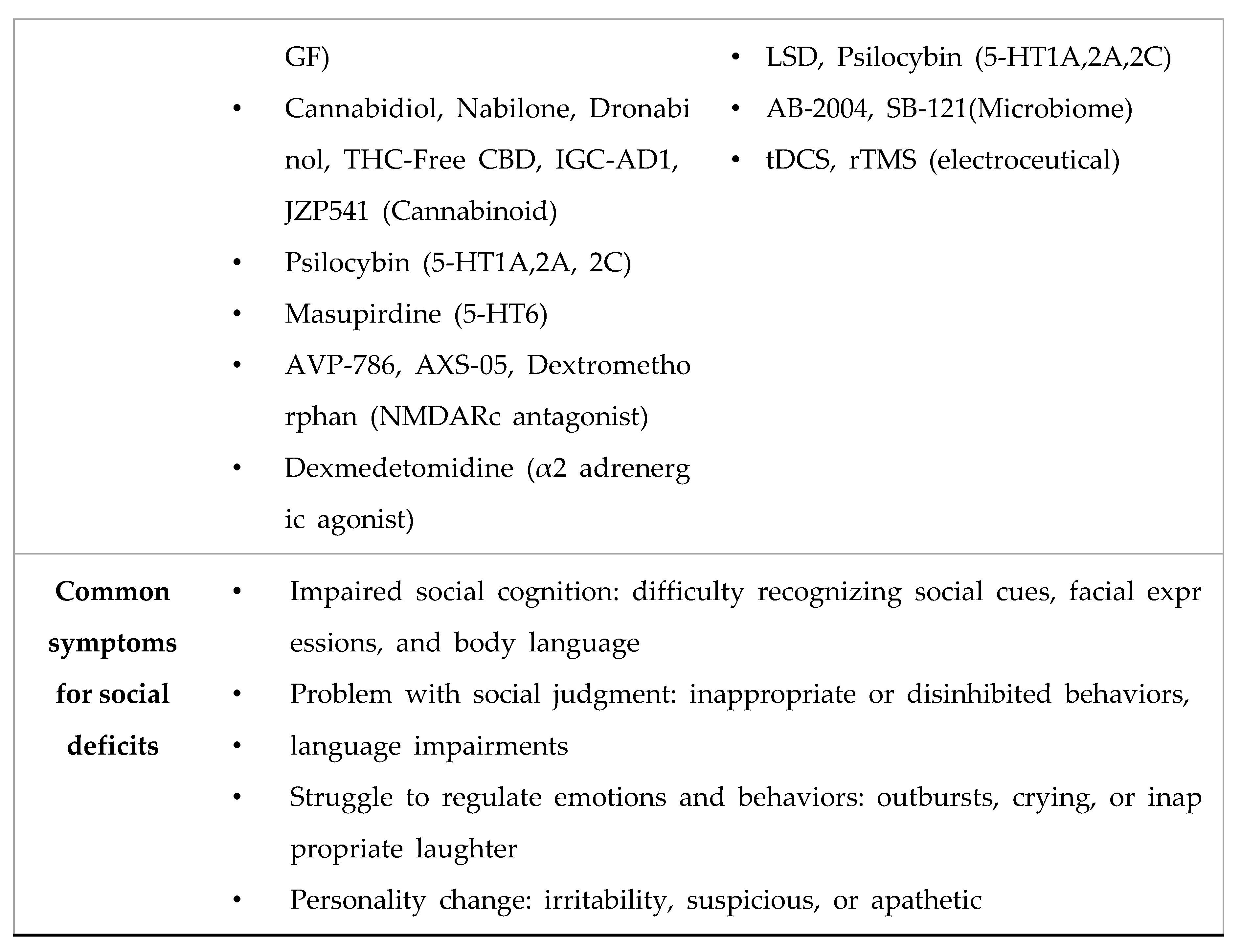
In addition to the agitation/aggression, depression, anxiety, sleep dysregulation, psychosis and apathy, AD significantly impacts social behavior in affected individuals [54,145,146,147,148,149]. Social deficits and dysregulation of social interactions are common NPS associated with AD. These challenges arise from cognitive decline and changes in brain function during the disease’s pathological process, affecting patient’s ability to engage in and navigate social situations. Caregivers also face enormous challenge in managing these behaviors. AD patients often exhibit impaired social cognition, including difficulty recognizing social cues, facial expressions, and body language, which are critical for understanding others’ emotions and intentions. It also results in problems with social judgment, leading to inappropriate or disinhibited behaviors in social settings. Due to the language impairments including trouble finding the right words, following conversations, and understanding what others are saying, using the pragmatic language as well as repetitive questioning or conversation, AD patients find social engagements and communication to be stressful and difficult. Due to the challenges faced during social interactions, individuals with AD may withdraw from social engagements, leading to isolation and exacerbating social difficulties. AD patients often struggle to regulate emotions and behaviors appropriately in social contexts, leading to outbursts, crying, or inappropriate laughter-similar to what is observed in other psychiatric disorders, including schizophrenia. Shifts in personality traits and other NPS in AD, such as increased irritability, suspicious, or apathetic, further affect social functioning. Recent meta-analysis revealed facial expression recognition deficits in FTD and AD with overall emotion recognition being most frequently impaired, followed by recognition of anger in FTD and by fear in AD [150]. Additionally, patients with behavioral variant AD (bvAD) exhibit greater impairments in social cognition and divergent eye movement patterns compared to patients with typical AD and the severity of social problems is comparable in many senses behavioral variant FTD (bvFTD) [151]. Conversely, social isolation and loneliness is regarded as risk factors for AD and can adversely affects cognitive well-being and AD manifestation in both humans and animals [58,152,153,154,155]. A recent study estimates that prevalence of as much as 4% can be reduced with the prevention of social isolation in later life [156].
Molecular and cellular mechanism underlying the social deficits in AD is also under active investigation as well as identifying targets for more precise therapeutic intervention. In the Tg2576 mouse model of AD, social memory deficits are associated with a decreased presence of the extracellular matrix perineuronal net (PNN) around parvalbumin-positive interneurons (PV) and dysregulated long-term synaptic plasticity in the CA2 area of the hippocampus [157]. Furthermore, direct application of growth factor neuregulin-1 (NRG1) in the affected area, sufficiently restored both PV/PNN levels and social memory performance of these mice, again exemplifying the importance of the regulation of neural activity in the brain regions involved in social behaviors [157]. A group of researchers focused on the serotonergic modulation to improve memory and social deficits in AD. In a study using Wistar rat, selective 5-HT6 receptor antagonist SLV was administered to rats reared in isolation, which showed positive effects on memory performance in an object recognition test (ORT). In prenatally valproic acid-exposed rat offspring, a commonly used rodent model mimicking ASD-like symptoms such as social deficits and repetitive behaviors, SLV mitigated the behavioral deficits. Additionally, SLV fully reversed MK-801-induced deficits in the ORT and scopolamine-induced memory deficits, although it did not show beneficial effects on the cognitive performance of 12-month-old Tg2576 mice [122]. In addition to the serotonergic modulators, administration of the dopamine D1 receptor positive allosteric modulator DETQ improves cognition and social interaction in aged mice, regardless of the treatment period. The effect may be related to the increased acetylcholine efflux in cortical and hippocampal regions [158].
Table 3.
Comparison of mechanisms, symptoms, and therapeutic candidates of Autism spectrum disorder and Alzheimer’s disease for Social Deficits.
Table 3.
Comparison of mechanisms, symptoms, and therapeutic candidates of Autism spectrum disorder and Alzheimer’s disease for Social Deficits.
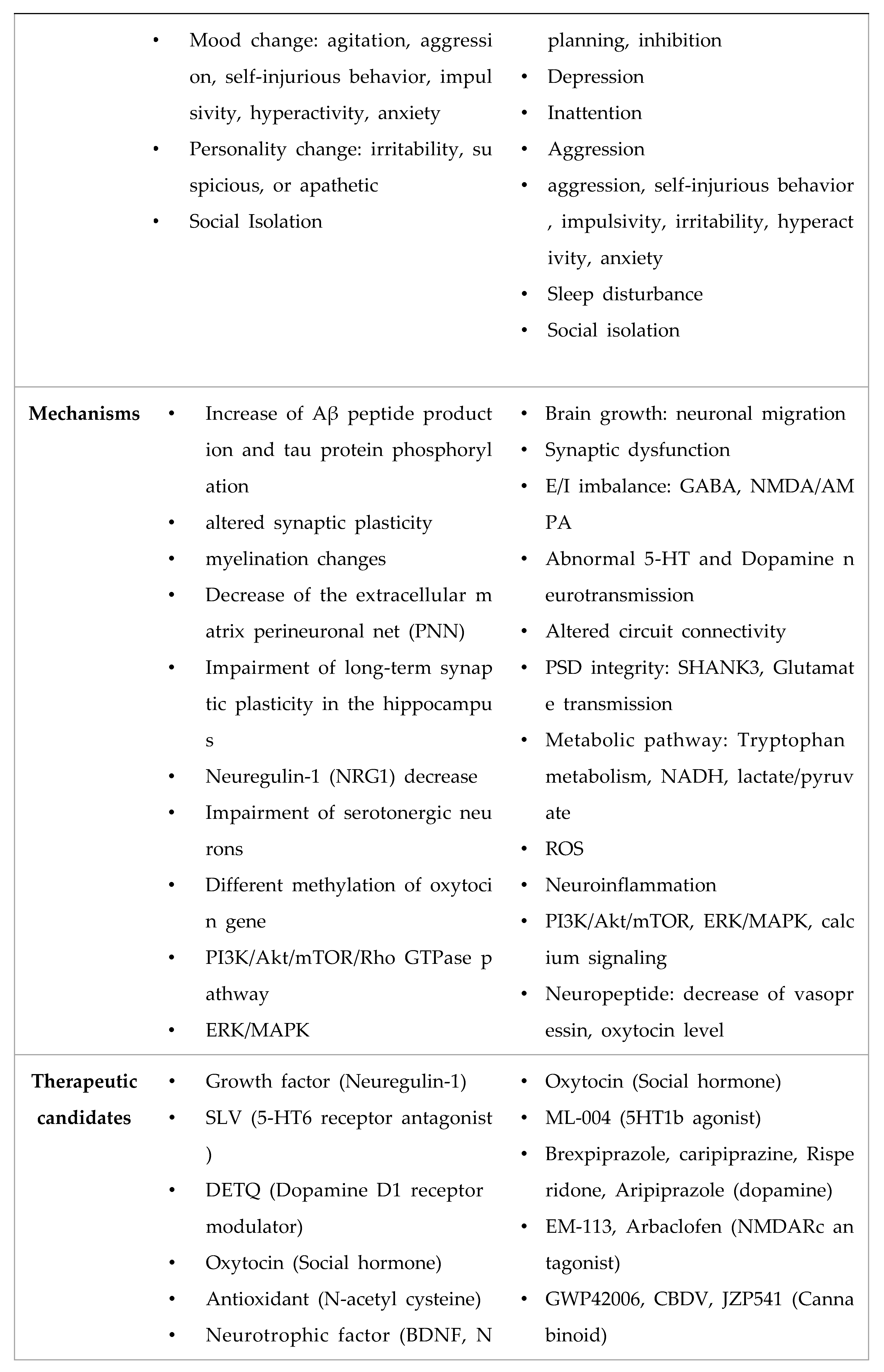
Oxytocin, released from the hypothalamus, is one of the well-known “social hormone”, along with vasopressin. It plays an important role in other brain functions, such as stress regulation, appetite control, lactation and associative learning. Based on the finding that the gene encoding for oxytocin, oxt, is differentially methylated in the brain and blood of AD patients [123,124], it is speculated that oxytocin may modulate memory loss in AD [125]. Interestingly, low dose of long-term (42 days) intranasal oxytocin treatment mitigates spatial and working memory deficits in female APP/PS1 mice, suggesting the potential therapeutic effects of oxytocin against AD [125]. As expected, APP/PS1 mice showed decreased sociability in the social interaction test, but surprisingly enough, oxytocin further deteriorated social interaction in the experimental animals [125]. Further studies might be needed to underscore the mechanism of social deficits in AD and develop better therapeutic tools for the intervention of this specific domain of NPS in AD. On the contrary, a pilot randomized, double-blind, placebo-controlled crossover trial using intranasal oxytocin treatment revealed moderate-to-large effect size improvements in participant health outcomes and core social cognitive functions, as well as a reduction in caregiver burden. However, no positive effects were associated with participant outcomes related to social cognition itself [159].
Due to the seemingly similar nature of social interaction deficits in AD and ASD, as well as the developmental and degenerative nature of these disorders, some researchers have focused on the possible common etiology, pathological mechanisms, and association between the two especially focusing on the role of APP, Aβ and secretase [160,161,162,163,164,165]. Studies using conditional APP/APLP1/APLP2 triple KO (cTKO) mice, which lack the APP family in excitatory forebrain neurons from embryonic day 11.5 onwards [161], have demonstrated agenesis of the corpus callosum and disrupted hippocampal lamination – phenotypes often observed in ASD model mice. These cTKO mice also exhibit dysregulated synaptic structure and function, impairments in learning and memory, repetitive behaviors (such as rearing and climbing), impaired social communication, and deficits in social interaction, which are core symptoms of ASD. These findings underscore the essential role of APP in regulating synaptic development, which is crucial for cognitive function and social behaviors [161]. Aberrations in the APP pathway, whether increased or decreased direction, have been associated with ASD-like phenotypes in experimental animals as well as in clinical samples suggesting a common etiological mechanism understanding both ASD and the social deficits observed in AD. For instance, mechanisms involving ERK receptor activation on the PI3K/Akt/mTOR/Rho GTPase pathway have been implicated [161,162,163,166,167].
Recently, it has been reported that CNTNAP2, one of the key proteins implicated in the manifestation of ASD, can be processed by γ-secretase. Similar to the situation where the amyloid-β precursor protein (APP) undergoes successive cleavage by β- and γ-secretases to generate the amyloid β protein (Aβ), the secreted APP (sAPP), and the APP intracellular domain (AICD) acting on nuclear transcription of target genes, a motif within the transmembrane domain of CNTNAP2 was postulated to be a target of γ-secretase because it is highly homologous to the γ-secretase cleavage site of APP. Like AICD and notch intracellular domain (NICD) production and activation, CNTNAP2 is cleaved by γ-secretase to produce the CNTNAP2 intracellular domain (CICD), which can translocate into the nucleus to modulate gene expression. Moreover, viral delivery of CICD to the medial prefrontal cortex (mPFC) in Cntnap2-deficient (Cntnap2-/-) mice normalized social deficits of the knockout (KO) mice, suggesting the essential role of CICD in the modulation of social behavior [164]. Interestingly, intermittent hypoxia for 14 days in reduced oxygen concentration (8%) enhanced sociability and working memory C57BL/6J mice, which has been associated with the up-regulation of CNTNAP2 expression [165].
Overall, these results suggest a common etiological mechanism of social deficits observed in both AD and ASD as well as the feasibility of identifying and validating new targets for more precise control of symptoms in both disorders. The input obtained from either field of neurological disorders into another may facilitate breakthrough findings in the regulating these seemingly formidable neuropsychiatric symptoms.
4. Conclusion
Alzheimer’s disease (AD), along with cognitive decline, is a major type of dementia, showing high prevalence rates worldwide due to the aging population and societal progress, with patients increasing over time. Numerous studies have been conducted to diagnose and treat AD, focusing on target discovery and drug development. Not only global big pharma but also startup venture companies worldwide are actively developing pipelines for AD. Currently, AD treatment pipelines are being developed based on disease-modifying drugs, cognitive enhancing drugs, and neuropsychiatric symptom treatment.
Traditionally, AD therapeutic development has focused on pathology-based targets, aiming to address cognitive impairment and prevent neuronal cell death. Acetylcholinesterase inhibitors like donepezil, galantamine, and rivastigmine are currently used for cognitive impairment in AD. Recently, the US FDA approved AD therapies targeting amyloid beta clearance, including aducanumab in 2021, lecanemab in 2023, and donanemab in 2024. Additionally, clinical trials are underway for tau pathology and neuronal cell death inhibition.
Beyond cognitive impairment, neuropsychiatric symptoms such as agitation, aggression, apathy, psychosis, sleep disturbances, and social deficits significantly impact AD patients and caregivers. In this review, the pipelines for NPS treatment were discussed, focusing on drugs targeting neurotransmitter receptors such as NMDA receptors, cannabinoids, sigma receptors, and adrenergic receptors. These drugs include cannabidiol, THC-Free CBD, masupirdine, dronabidol, hallucinogens like psilocybin, and antioxidant molecules such as DHA, which are currently undergoing clinical trials.
In particular, symptoms such as agitation, anxiety, aggression, and social deficits observed in AD patients are similar to those seen in Autism Spectrum Disorder (ASD). As a result, drugs that were previously tested as ASD treatments are now being investigated in clinical trials as potential NPS therapies for AD.
This potential trend extends from ASD, which exhibits social processing dysfunction based on the Research Domain Criteria (RDoC), to other neurological disorders such as depression and Parkinson’s disease.
Successful NPS treatment of AD is not only applicable for the sophisticated management of AD but may also have potential applications, and help mechanistic understanding of other neurological disorders, such as depression, bipolar disorders, anxiety, schizophrenia, ASD and Parkinson’s disease.
Acknowledgments
This work was supported by the Basic Science Research Program (2022R1A2C1005917) through the National Research Foundation (NRF) of Korea funded by the Ministry of Science, ICT & Future Planning.
References
- Tahami Monfared, A.A.; Byrnes, M.J.; White, L.A.; Zhang, Q. The Humanistic and Economic Burden of Alzheimer’s Disease. Neurol Ther 2022, 11, 525–551. [Google Scholar] [CrossRef] [PubMed]
- Lyketsos, C.G.; Steinberg, M.; Tschanz, J.T.; Norton, M.C.; Steffens, D.C.; Breitner, J.C. Mental and behavioral disturbances in dementia: findings from the Cache County Study on Memory in Aging. Am J Psychiatry 2000, 157, 708–714. [Google Scholar] [CrossRef] [PubMed]
- Jost, B.C.; Grossberg, G.T. The evolution of psychiatric symptoms in Alzheimer’s disease: a natural history study. J Am Geriatr Soc 1996, 44, 1078–1081. [Google Scholar] [CrossRef] [PubMed]
- Lyketsos, C.G.; Carrillo, M.C.; Ryan, J.M.; Khachaturian, A.S.; Trzepacz, P.; Amatniek, J.; Cedarbaum, J.; Brashear, R.; Miller, D.S. Neuropsychiatric symptoms in Alzheimer’s disease. Alzheimers Dement 2011, 7, 532–539. [Google Scholar] [CrossRef]
- Avitan, I.; Halperin, Y.; Saha, T.; Bloch, N.; Atrahimovich, D.; Polis, B.; Samson, A.O.; Braitbard, O. Towards a Consensus on Alzheimer’s Disease Comorbidity? J Clin Med 2021, 10. [Google Scholar] [CrossRef]
- Sinyor, B.; Mineo, J.; Ochner, C. Alzheimer’s Disease, Inflammation, and the Role of Antioxidants. J Alzheimers Dis Rep 2020, 4, 175–183. [Google Scholar] [CrossRef]
- Butler, L.M.; Houghton, R.; Abraham, A.; Vassilaki, M.; Duran-Pacheco, G. Comorbidity Trajectories Associated With Alzheimer’s Disease: A Matched Case-Control Study in a United States Claims Database. Front Neurosci 2021, 15, 749305. [Google Scholar] [CrossRef]
- Olazaran, J.; Carnero-Pardo, C.; Fortea, J.; Sanchez-Juan, P.; Garcia-Ribas, G.; Vinuela, F.; Martinez-Lage, P.; Boada, M. Prevalence of treated patients with Alzheimer’s disease: current trends and COVID-19 impact. Alzheimers Res Ther 2023, 15, 130. [Google Scholar] [CrossRef] [PubMed]
- Ehrenberg, A.J.; Suemoto, C.K.; Franca Resende, E.P.; Petersen, C.; Leite, R.E.P.; Rodriguez, R.D.; Ferretti-Rebustini, R.E.L.; You, M.; Oh, J.; Nitrini, R.; et al. Neuropathologic Correlates of Psychiatric Symptoms in Alzheimer’s Disease. J Alzheimers Dis 2018, 66, 115–126. [Google Scholar] [CrossRef]
- Lanctot, K.L.; Amatniek, J.; Ancoli-Israel, S.; Arnold, S.E.; Ballard, C.; Cohen-Mansfield, J.; Ismail, Z.; Lyketsos, C.; Miller, D.S.; Musiek, E.; et al. Neuropsychiatric signs and symptoms of Alzheimer’s disease: New treatment paradigms. Alzheimers Dement (N Y) 2017, 3, 440–449. [Google Scholar] [CrossRef]
- Ajenikoko, M.K.; Ajagbe, A.O.; Onigbinde, O.A.; Okesina, A.A.; Tijani, A.A. Review of Alzheimer’s disease drugs and their relationship with neuron-glia interaction. IBRO Neurosci Rep 2023, 14, 64–76. [Google Scholar] [CrossRef] [PubMed]
- Cummings, J.; Zhou, Y.; Lee, G.; Zhong, K.; Fonseca, J.; Cheng, F. Alzheimer’s disease drug development pipeline: 2024. Alzheimers Dement (N Y) 2024, 10, e12465. [Google Scholar] [CrossRef] [PubMed]
- Li, X.L.; Hu, N.; Tan, M.S.; Yu, J.T.; Tan, L. Behavioral and psychological symptoms in Alzheimer’s disease. Biomed Res Int 2014, 2014, 927804. [Google Scholar] [CrossRef] [PubMed]
- Evans-Lacko, S.; Aguilar-Gaxiola, S.; Al-Hamzawi, A.; Alonso, J.; Benjet, C.; Bruffaerts, R.; Chiu, W.T.; Florescu, S.; de Girolamo, G.; Gureje, O.; et al. Socio-economic variations in the mental health treatment gap for people with anxiety, mood, and substance use disorders: results from the WHO World Mental Health (WMH) surveys. Psychol Med 2018, 48, 1560–1571. [Google Scholar] [CrossRef]
- Pless, A.; Ware, D.; Saggu, S.; Rehman, H.; Morgan, J.; Wang, Q. Understanding neuropsychiatric symptoms in Alzheimer’s disease: challenges and advances in diagnosis and treatment. Front Neurosci 2023, 17, 1263771. [Google Scholar] [CrossRef]
- Asmer, M.S.; Kirkham, J.; Newton, H.; Ismail, Z.; Elbayoumi, H.; Leung, R.H.; Seitz, D.P. Meta-Analysis of the Prevalence of Major Depressive Disorder Among Older Adults With Dementia. J Clin Psychiatry 2018, 79. [Google Scholar] [CrossRef] [PubMed]
- Chi, S.; Wang, C.; Jiang, T.; Zhu, X.C.; Yu, J.T.; Tan, L. The prevalence of depression in Alzheimer’s disease: a systematic review and meta-analysis. Curr Alzheimer Res 2015, 12, 189–198. [Google Scholar] [CrossRef]
- Daly, M.; Sutin, A.R.; Robinson, E. Depression reported by US adults in 2017-2018 and March and April 2020. J Affect Disord 2021, 278, 131–135. [Google Scholar] [CrossRef]
- Wang, J.; Yu, J.T.; Wang, H.F.; Meng, X.F.; Wang, C.; Tan, C.C.; Tan, L. Pharmacological treatment of neuropsychiatric symptoms in Alzheimer’s disease: a systematic review and meta-analysis. J Neurol Neurosurg Psychiatry 2015, 86, 101–109. [Google Scholar] [CrossRef]
- Simic, G.; Babic Leko, M.; Wray, S.; Harrington, C.R.; Delalle, I.; Jovanov-Milosevic, N.; Bazadona, D.; Buee, L.; de Silva, R.; Di Giovanni, G.; et al. Monoaminergic neuropathology in Alzheimer’s disease. Prog Neurobiol 2017, 151, 101–138. [Google Scholar] [CrossRef]
- Orgeta, V.; Tabet, N.; Nilforooshan, R.; Howard, R. Efficacy of Antidepressants for Depression in Alzheimer’s Disease: Systematic Review and Meta-Analysis. J Alzheimers Dis 2017, 58, 725–733. [Google Scholar] [CrossRef] [PubMed]
- Dudas, R.; Malouf, R.; McCleery, J.; Dening, T. Antidepressants for treating depression in dementia. Cochrane Database Syst Rev 2018, 8, CD003944. [Google Scholar] [CrossRef] [PubMed]
- Ismail, Z.; Gatchel, J.; Bateman, D.R.; Barcelos-Ferreira, R.; Cantillon, M.; Jaeger, J.; Donovan, N.J.; Mortby, M.E. Affective and emotional dysregulation as pre-dementia risk markers: exploring the mild behavioral impairment symptoms of depression, anxiety, irritability, and euphoria. Int Psychogeriatr 2018, 30, 185–196. [Google Scholar] [CrossRef] [PubMed]
- Mendez, M.F. The Relationship Between Anxiety and Alzheimer’s Disease. J Alzheimers Dis Rep 2021, 5, 171–177. [Google Scholar] [CrossRef] [PubMed]
- Gulpers, B.; Ramakers, I.; Hamel, R.; Kohler, S.; Oude Voshaar, R.; Verhey, F. Anxiety as a Predictor for Cognitive Decline and Dementia: A Systematic Review and Meta-Analysis. Am J Geriatr Psychiatry 2016, 24, 823–842. [Google Scholar] [CrossRef]
- Santabarbara, J.; Lipnicki, D.M.; Olaya, B.; Villagrasa, B.; Bueno-Notivol, J.; Nuez, L.; Lopez-Anton, R.; Gracia-Garcia, P. Does Anxiety Increase the Risk of All-Cause Dementia? An Updated Meta-Analysis of Prospective Cohort Studies. J Clin Med 2020, 9. [Google Scholar] [CrossRef]
- Chen, L.; Sun, Y.; Li, J.; Liu, S.; Ding, H.; Wang, G.; Li, X. Assessing Cannabidiol as a Therapeutic Agent for Preventing and Alleviating Alzheimer’s Disease Neurodegeneration. Cells 2023, 12. [Google Scholar] [CrossRef]
- Drijgers, R.L.; Aalten, P.; Winogrodzka, A.; Verhey, F.R.; Leentjens, A.F. Pharmacological treatment of apathy in neurodegenerative diseases: a systematic review. Dement Geriatr Cogn Disord 2009, 28, 13–22. [Google Scholar] [CrossRef]
- Wolinsky, D.; Drake, K.; Bostwick, J. Diagnosis and Management of Neuropsychiatric Symptoms in Alzheimer’s Disease. Curr Psychiatry Rep 2018, 20, 117. [Google Scholar] [CrossRef]
- Costello, H.; Husain, M.; Roiser, J.P. Apathy and Motivation: Biological Basis and Drug Treatment. Annu Rev Pharmacol Toxicol 2024, 64, 313–338. [Google Scholar] [CrossRef]
- Fahed, M.; Steffens, D.C. Apathy: Neurobiology, Assessment and Treatment. Clin Psychopharmacol Neurosci 2021, 19, 181–189. [Google Scholar] [CrossRef] [PubMed]
- Ruthirakuhan, M.T.; Herrmann, N.; Abraham, E.H.; Chan, S.; Lanctot, K.L. Pharmacological interventions for apathy in Alzheimer’s disease. Cochrane Database Syst Rev 2018, 5, CD012197. [Google Scholar] [CrossRef]
- Kverno, K.S.; Rabins, P.V.; Blass, D.M.; Hicks, K.L.; Black, B.S. Prevalence and treatment of neuropsychiatric symptoms in advanced dementia. J Gerontol Nurs 2008, 34, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Ravyts, S.G.; Perez, E.; Donovan, E.K.; Soto, P.; Dzierzewski, J.M. Measurement of aggression in older adults. Aggress Violent Behav 2021, 57. [Google Scholar] [CrossRef]
- Cummings, J.; Mintzer, J.; Brodaty, H.; Sano, M.; Banerjee, S.; Devanand, D.P.; Gauthier, S.; Howard, R.; Lanctot, K.; Lyketsos, C.G.; et al. Agitation in cognitive disorders: International Psychogeriatric Association provisional consensus clinical and research definition. Int Psychogeriatr 2015, 27, 7–17. [Google Scholar] [CrossRef]
- Ballard, C.; Orrell, M.; YongZhong, S.; Moniz-Cook, E.; Stafford, J.; Whittaker, R.; Woods, B.; Corbett, A.; Garrod, L.; Khan, Z.; et al. Impact of Antipsychotic Review and Nonpharmacological Intervention on Antipsychotic Use, Neuropsychiatric Symptoms, and Mortality in People With Dementia Living in Nursing Homes: A Factorial Cluster-Randomized Controlled Trial by the Well-Being and Health for People With Dementia (WHELD) Program. Am J Psychiatry 2016, 173, 252–262. [Google Scholar] [CrossRef]
- Safdar, A.; Ismail, F. A comprehensive review on pharmacological applications and drug-induced toxicity of valproic acid. Saudi Pharm J 2023, 31, 265–278. [Google Scholar] [CrossRef]
- Lee, D.; Slomkowski, M.; Hefting, N.; Chen, D.; Larsen, K.G.; Kohegyi, E.; Hobart, M.; Cummings, J.L.; Grossberg, G.T. Brexpiprazole for the Treatment of Agitation in Alzheimer Dementia: A Randomized Clinical Trial. JAMA Neurol 2023, 80, 1307–1316. [Google Scholar] [CrossRef]
- Murray, P.S.; Kumar, S.; Demichele-Sweet, M.A.; Sweet, R.A. Psychosis in Alzheimer’s disease. Biol Psychiatry 2014, 75, 542–552. [Google Scholar] [CrossRef]
- Woodward, M. Aspects of communication in Alzheimer’s disease: clinical features and treatment options. Int Psychogeriatr 2013, 25, 877–885. [Google Scholar] [CrossRef]
- Ismail, Z.; Creese, B.; Aarsland, D.; Kales, H.C.; Lyketsos, C.G.; Sweet, R.A.; Ballard, C. Psychosis in Alzheimer disease - mechanisms, genetics and therapeutic opportunities. Nat Rev Neurol 2022, 18, 131–144. [Google Scholar] [CrossRef]
- Khoury, R.; Marx, C.; Mirgati, S.; Velury, D.; Chakkamparambil, B.; Grossberg, G.T. AVP-786 as a promising treatment option for Alzheimer’s Disease including agitation. Expert Opin Pharmacother 2021, 22, 783–795. [Google Scholar] [CrossRef]
- Kurhan, F.; Akin, M. A New Hope in Alzheimer’s Disease Psychosis: Pimavanserin. Curr Alzheimer Res 2023, 20, 403–408. [Google Scholar] [CrossRef]
- Shi, L.; Chen, S.J.; Ma, M.Y.; Bao, Y.P.; Han, Y.; Wang, Y.M.; Shi, J.; Vitiello, M.V.; Lu, L. Sleep disturbances increase the risk of dementia: A systematic review and meta-analysis. Sleep Med Rev 2018, 40, 4–16. [Google Scholar] [CrossRef]
- Zhang, Y.; Ren, R.; Yang, L.; Zhang, H.; Shi, Y.; Okhravi, H.R.; Vitiello, M.V.; Sanford, L.D.; Tang, X. Sleep in Alzheimer’s disease: a systematic review and meta-analysis of polysomnographic findings. Transl Psychiatry 2022, 12, 136. [Google Scholar] [CrossRef]
- Wu, T.T.; Zou, Y.L.; Xu, K.D.; Jiang, X.R.; Zhou, M.M.; Zhang, S.B.; Song, C.H. Insomnia and multiple health outcomes: umbrella review of meta-analyses of prospective cohort studies. Public Health 2023, 215, 66–74. [Google Scholar] [CrossRef]
- Ju, Y.E.; Lucey, B.P.; Holtzman, D.M. Sleep and Alzheimer disease pathology--a bidirectional relationship. Nat Rev Neurol 2014, 10, 115–119. [Google Scholar] [CrossRef]
- Jiang, X.; Wang, Z.; Hu, N.; Yang, Y.; Xiong, R.; Fu, Z. Cognition effectiveness of continuous positive airway pressure treatment in obstructive sleep apnea syndrome patients with cognitive impairment: a meta-analysis. Exp Brain Res 2021, 239, 3537–3552. [Google Scholar] [CrossRef]
- Di Meco, A.; Joshi, Y.B.; Pratico, D. Sleep deprivation impairs memory, tau metabolism, and synaptic integrity of a mouse model of Alzheimer’s disease with plaques and tangles. Neurobiol Aging 2014, 35, 1813–1820. [Google Scholar] [CrossRef]
- Ooms, S.; Overeem, S.; Besse, K.; Rikkert, M.O.; Verbeek, M.; Claassen, J.A. Effect of 1 night of total sleep deprivation on cerebrospinal fluid beta-amyloid 42 in healthy middle-aged men: a randomized clinical trial. JAMA Neurol 2014, 71, 971–977. [Google Scholar] [CrossRef]
- McCurry, S.M.; Reynolds, C.F.; Ancoli-Israel, S.; Teri, L.; Vitiello, M.V. Treatment of sleep disturbance in Alzheimer’s disease. Sleep Med Rev 2000, 4, 603–628. [Google Scholar] [CrossRef]
- Burke, S.L.; Hu, T.; Spadola, C.E.; Burgess, A.; Li, T.; Cadet, T. Treatment of Sleep Disturbance May Reduce the Risk of Future Probable Alzheimer’s Disease. J Aging Health 2019, 31, 322–342. [Google Scholar] [CrossRef] [PubMed]
- McCleery, J.; Sharpley, A.L. Pharmacotherapies for sleep disturbances in dementia. Cochrane Database Syst Rev 2020, 11, CD009178. [Google Scholar] [CrossRef] [PubMed]
- Bediou, B.; Ryff, I.; Mercier, B.; Milliery, M.; Henaff, M.A.; D’Amato, T.; Bonnefoy, M.; Vighetto, A.; Krolak-Salmon, P. Impaired social cognition in mild Alzheimer disease. J Geriatr Psychiatry Neurol 2009, 22, 130–140. [Google Scholar] [CrossRef]
- Moreau, N.; Rauzy, S.; Viallet, F.; Champagne-Lavau, M. Theory of mind in Alzheimer disease: Evidence of authentic impairment during social interaction. Neuropsychology 2016, 30, 312–321. [Google Scholar] [CrossRef] [PubMed]
- Ellis Weismer, S.; Tomblin, J.B.; Durkin, M.S.; Bolt, D.; Palta, M. A preliminary epidemiologic study of social (pragmatic) communication disorder in the context of developmental language disorder. Int J Lang Commun Disord 2021, 56, 1235–1248. [Google Scholar] [CrossRef]
- Sommerlad, A.; Kivimaki, M.; Larson, E.B.; Rohr, S.; Shirai, K.; Singh-Manoux, A.; Livingston, G. Social participation and risk of developing dementia. Nat Aging 2023, 3, 532–545. [Google Scholar] [CrossRef]
- Hsiao, Y.H.; Chang, C.H.; Gean, P.W. Impact of social relationships on Alzheimer’s memory impairment: mechanistic studies. J Biomed Sci 2018, 25, 3. [Google Scholar] [CrossRef]
- Leser, N.; Wagner, S. The effects of acute social isolation on long-term social recognition memory. Neurobiol Learn Mem 2015, 124, 97–103. [Google Scholar] [CrossRef]
- Huang, H.; Wang, L.; Cao, M.; Marshall, C.; Gao, J.; Xiao, N.; Hu, G.; Xiao, M. Isolation Housing Exacerbates Alzheimer’s Disease-Like Pathophysiology in Aged APP/PS1 Mice. Int J Neuropsychopharmacol 2015, 18, pyu116. [Google Scholar] [CrossRef]
- Hsiao, Y.H.; Hung, H.C.; Yu, Y.J.; Su, C.L.; Chen, S.H.; Gean, P.W. Co-housing reverses memory decline by epigenetic regulation of brain-derived neurotrophic factor expression in an animal model of Alzheimer’s disease. Neurobiol Learn Mem 2017, 141, 1–8. [Google Scholar] [CrossRef]
- Powell, N.D.; Sloan, E.K.; Bailey, M.T.; Arevalo, J.M.; Miller, G.E.; Chen, E.; Kobor, M.S.; Reader, B.F.; Sheridan, J.F.; Cole, S.W. Social stress up-regulates inflammatory gene expression in the leukocyte transcriptome via beta-adrenergic induction of myelopoiesis. Proc Natl Acad Sci U S A 2013, 110, 16574–16579. [Google Scholar] [CrossRef]
- Azzinnari, D.; Sigrist, H.; Staehli, S.; Palme, R.; Hildebrandt, T.; Leparc, G.; Hengerer, B.; Seifritz, E.; Pryce, C.R. Mouse social stress induces increased fear conditioning, helplessness and fatigue to physical challenge together with markers of altered immune and dopamine function. Neuropharmacology 2014, 85, 328–341. [Google Scholar] [CrossRef]
- Djordjevic, A.; Adzic, M.; Djordjevic, J.; Radojcic, M.B. Chronic social isolation is related to both upregulation of plasticity genes and initiation of proapoptotic signaling in Wistar rat hippocampus. J Neural Transm (Vienna) 2009, 116, 1579–1589. [Google Scholar] [CrossRef]
- Murinova, J.; Hlavacova, N.; Chmelova, M.; Riecansky, I. The Evidence for Altered BDNF Expression in the Brain of Rats Reared or Housed in Social Isolation: A Systematic Review. Front Behav Neurosci 2017, 11, 101. [Google Scholar] [CrossRef]
- Liu, J.; Dietz, K.; DeLoyht, J.M.; Pedre, X.; Kelkar, D.; Kaur, J.; Vialou, V.; Lobo, M.K.; Dietz, D.M.; Nestler, E.J.; et al. Impaired adult myelination in the prefrontal cortex of socially isolated mice. Nat Neurosci 2012, 15, 1621–1623. [Google Scholar] [CrossRef] [PubMed]
- Hsiao, Y.H.; Kuo, J.R.; Chen, S.H.; Gean, P.W. Amelioration of social isolation-triggered onset of early Alzheimer’s disease-related cognitive deficit by N-acetylcysteine in a transgenic mouse model. Neurobiol Dis 2012, 45, 1111–1120. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Du, W.; Shao, F.; Wang, W. Cognitive dysfunction and epigenetic alterations of the BDNF gene are induced by social isolation during early adolescence. Behav Brain Res 2016, 313, 177–183. [Google Scholar] [CrossRef] [PubMed]
- Branchi, I.; D’Andrea, I.; Fiore, M.; Di Fausto, V.; Aloe, L.; Alleva, E. Early social enrichment shapes social behavior and nerve growth factor and brain-derived neurotrophic factor levels in the adult mouse brain. Biol Psychiatry 2006, 60, 690–696. [Google Scholar] [CrossRef]
- Cosentino, S.; Zahodne, L.B.; Brandt, J.; Blacker, D.; Albert, M.; Dubois, B.; Stern, Y. Social cognition in Alzheimer’s disease: a separate construct contributing to dependence. Alzheimers Dement 2014, 10, 818–826. [Google Scholar] [CrossRef]
- Blair, H.A. Lumateperone: First Approval. Drugs 2020, 80, 417–423. [Google Scholar] [CrossRef] [PubMed]
- Mazza, M.; Marano, G.; Traversi, G.; Sani, G.; Janiri, L. Evidence on the New Drug Lumateperone (ITI-007) for Psychiatric and Neurological Disorders. CNS Neurol Disord Drug Targets 2020, 19, 243–247. [Google Scholar] [CrossRef] [PubMed]
- Vanover, K.E.; Davis, R.E.; Zhou, Y.; Ye, W.; Brasic, J.R.; Gapasin, L.; Saillard, J.; Weingart, M.; Litman, R.E.; Mates, S.; et al. Dopamine D(2) receptor occupancy of lumateperone (ITI-007): a Positron Emission Tomography Study in patients with schizophrenia. Neuropsychopharmacology 2019, 44, 598–605. [Google Scholar] [CrossRef] [PubMed]
- Vyas, P.; Hwang, B.J.; Brasic, J.R. An evaluation of lumateperone tosylate for the treatment of schizophrenia. Expert Opin Pharmacother 2020, 21, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Gattuso, J.J.; Wilson, C.; Hannan, A.J.; Renoir, T. Psilocybin as a lead candidate molecule in preclinical therapeutic studies of psychiatric disorders: A systematic review. J Neurochem 2023. [Google Scholar] [CrossRef]
- Kozak, Z.; Johnson, M.W.; Aaronson, S.T. Assessing potential of psilocybin for depressive disorders. Expert Opin Investig Drugs 2023, 32, 887–900. [Google Scholar] [CrossRef]
- Sharma, P.; Nguyen, Q.A.; Matthews, S.J.; Carpenter, E.; Mathews, D.B.; Patten, C.A.; Hammond, C.J. Psilocybin history, action and reaction: A narrative clinical review. J Psychopharmacol 2023, 37, 849–865. [Google Scholar] [CrossRef]
- Chen, K.; Li, H.; Yang, L.; Jiang, Y.; Wang, Q.; Zhang, J.; He, J. Comparative efficacy and safety of antidepressant therapy for the agitation of dementia: A systematic review and network meta-analysis. Front Aging Neurosci 2023, 15, 1103039. [Google Scholar] [CrossRef]
- Cummings, J.; Zhou, Y.; Lee, G.; Zhong, K.; Fonseca, J.; Cheng, F. Alzheimer’s disease drug development pipeline: 2023. Alzheimers Dement (N Y) 2023, 9, e12385. [Google Scholar] [CrossRef]
- Chen, C.Y.; Chung, C.H.; Chien, W.C.; Chen, H.C. The Association Between Dextromethorphan Use and the Risk of Dementia. Am J Alzheimers Dis Other Demen 2022, 37, 15333175221124952. [Google Scholar] [CrossRef]
- Malar, D.S.; Thitilertdecha, P.; Ruckvongacheep, K.S.; Brimson, S.; Tencomnao, T.; Brimson, J.M. Targeting Sigma Receptors for the Treatment of Neurodegenerative and Neurodevelopmental Disorders. CNS Drugs 2023, 37, 399–440. [Google Scholar] [CrossRef]
- Ohi, Y.; Tsunekawa, S.; Haji, A. Dextromethorphan inhibits the glutamatergic synaptic transmission in the nucleus tractus solitarius of guinea pigs. J Pharmacol Sci 2011, 116, 54–62. [Google Scholar] [CrossRef]
- Pioro, E.P.; Brooks, B.R.; Cummings, J.; Schiffer, R.; Thisted, R.A.; Wynn, D.; Hepner, A.; Kaye, R.; Safety, T.; Efficacy Results Trial of, A.V.P.i.P.B.A.I. Dextromethorphan plus ultra low-dose quinidine reduces pseudobulbar affect. Ann Neurol 2010, 68, 693–702. [Google Scholar] [CrossRef]
- Taylor, C.P.; Traynelis, S.F.; Siffert, J.; Pope, L.E.; Matsumoto, R.R. Pharmacology of dextromethorphan: Relevance to dextromethorphan/quinidine (Nuedexta(R)) clinical use. Pharmacol Ther 2016, 164, 170–182. [Google Scholar] [CrossRef]
- Chez, M.; Kile, S.; Lepage, C.; Parise, C.; Benabides, B.; Hankins, A. A Randomized, Placebo-Controlled, Blinded, Crossover, Pilot Study of the Effects of Dextromethorphan/Quinidine for the Treatment of Neurobehavioral Symptoms in Adults with Autism. J Autism Dev Disord 2020, 50, 1532–1538. [Google Scholar] [CrossRef]
- Cummings, J.L.; Lyketsos, C.G.; Peskind, E.R.; Porsteinsson, A.P.; Mintzer, J.E.; Scharre, D.W.; De La Gandara, J.E.; Agronin, M.; Davis, C.S.; Nguyen, U.; et al. Effect of Dextromethorphan-Quinidine on Agitation in Patients With Alzheimer Disease Dementia: A Randomized Clinical Trial. JAMA 2015, 314, 1242–1254. [Google Scholar] [CrossRef]
- Devanand, D.P. Management of neuropsychiatric symptoms in dementia. Curr Opin Neurol 2023, 36, 498–503. [Google Scholar] [CrossRef]
- Lauterbach, E.C. Treatment Resistant Depression with Loss of Antidepressant Response: Rapid-Acting Antidepressant Action of Dextromethorphan, A Possible Treatment Bridging Molecule. Psychopharmacol Bull 2016, 46, 53–58. [Google Scholar]
- Willett, K.C.; Bond, L.R.; Morrill, A.M.; Lorena, D.; Petru, I. Dextromethorphan/Bupropion: A Novel Treatment for Patients With Major Depressive Disorder. Am J Ther 2024, 31, e24–e29. [Google Scholar] [CrossRef] [PubMed]
- Herrmann, N.; Ruthirakuhan, M.; Gallagher, D.; Verhoeff, N.; Kiss, A.; Black, S.E.; Lanctot, K.L. Randomized Placebo-Controlled Trial of Nabilone for Agitation in Alzheimer’s Disease. Am J Geriatr Psychiatry 2019, 27, 1161–1173. [Google Scholar] [CrossRef]
- Ruthirakuhan, M.; Herrmann, N.; Andreazza, A.C.; Verhoeff, N.; Gallagher, D.; Black, S.E.; Kiss, A.; Lanctot, K.L. Agitation, Oxidative Stress, and Cytokines in Alzheimer Disease: Biomarker Analyses From a Clinical Trial With Nabilone for Agitation. J Geriatr Psychiatry Neurol 2020, 33, 175–184. [Google Scholar] [CrossRef] [PubMed]
- Diefenderfer, L.A.; Iuppa, C. Brexpiprazole: A review of a new treatment option for schizophrenia and major depressive disorder. Ment Health Clin 2017, 7, 207–212. [Google Scholar] [CrossRef] [PubMed]
- Eaves, S.; Rey, J.A. Brexpiprazole (Rexulti): A New Monotherapy for Schizophrenia and Adjunctive Therapy for Major Depressive Disorder. P T 2016, 41, 418–422. [Google Scholar] [PubMed]
- Khoury, R. Deuterated dextromethorphan/quinidine for agitation in Alzheimer’s disease. Neural Regen Res 2022, 17, 1013–1014. [Google Scholar] [CrossRef] [PubMed]
- Luo, S.M.; Li, L.Y.; Guo, L.Z.; Wang, L.; Wang, Y.F.; Chen, N.; Wang, E. Dexmedetomidine exerts an anti-inflammatory effect via alpha2 adrenoceptors to alleviate cognitive dysfunction in 5xFAD mice. Front Aging Neurosci 2022, 14, 978768. [Google Scholar] [CrossRef]
- Deiner, S.; Luo, X.; Lin, H.M.; Sessler, D.I.; Saager, L.; Sieber, F.E.; Lee, H.B.; Sano, M.; and the Dexlirium Writing, G.; Jankowski, C.; et al. Intraoperative Infusion of Dexmedetomidine for Prevention of Postoperative Delirium and Cognitive Dysfunction in Elderly Patients Undergoing Major Elective Noncardiac Surgery: A Randomized Clinical Trial. JAMA Surg 2017, 152, e171505. [Google Scholar] [CrossRef]
- Preskorn, S.H.; Zeller, S.; Citrome, L.; Finman, J.; Goldberg, J.F.; Fava, M.; Kakar, R.; De Vivo, M.; Yocca, F.D.; Risinger, R. Effect of Sublingual Dexmedetomidine vs Placebo on Acute Agitation Associated With Bipolar Disorder: A Randomized Clinical Trial. JAMA 2022, 327, 727–736. [Google Scholar] [CrossRef]
- Volicer, L.; Stelly, M.; Morris, J.; McLaughlin, J.; Volicer, B.J. Effects of dronabinol on anorexia and disturbed behavior in patients with Alzheimer’s disease. Int J Geriatr Psychiatry 1997, 12, 913–919. [Google Scholar] [CrossRef]
- Woodward, M.R.; Harper, D.G.; Stolyar, A.; Forester, B.P.; Ellison, J.M. Dronabinol for the treatment of agitation and aggressive behavior in acutely hospitalized severely demented patients with noncognitive behavioral symptoms. Am J Geriatr Psychiatry 2014, 22, 415–419. [Google Scholar] [CrossRef]
- Cohen, L.M.; Ash, E.; Outen, J.D.; Vandrey, R.; Amjad, H.; Agronin, M.; Burhanullah, M.H.; Walsh, P.; Wilkins, J.M.; Leoutsakos, J.M.; et al. Study rationale and baseline data for pilot trial of dronabinol adjunctive treatment of agitation in Alzheimer’s dementia (THC-AD). Int Psychogeriatr 2021. [Google Scholar] [CrossRef]
- Fitzgerald, P.J. Norepinephrine May Oppose Other Neuromodulators to Impact Alzheimer’s Disease. Int J Mol Sci 2021, 22. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez, I.L.; Dello Russo, C.; Novellino, F.; Caso, J.R.; Garcia-Bueno, B.; Leza, J.C.; Madrigal, J.L.M. Noradrenaline in Alzheimer’s Disease: A New Potential Therapeutic Target. Int J Mol Sci 2022, 23. [Google Scholar] [CrossRef] [PubMed]
- Di Marzo, V.; Melck, D.; Orlando, P.; Bisogno, T.; Zagoory, O.; Bifulco, M.; Vogel, Z.; De Petrocellis, L. Palmitoylethanolamide inhibits the expression of fatty acid amide hydrolase and enhances the anti-proliferative effect of anandamide in human breast cancer cells. Biochem J 2001, 358, 249–255. [Google Scholar] [CrossRef]
- Jonsson, K.O.; Vandevoorde, S.; Lambert, D.M.; Tiger, G.; Fowler, C.J. Effects of homologues and analogues of palmitoylethanolamide upon the inactivation of the endocannabinoid anandamide. Br J Pharmacol 2001, 133, 1263–1275. [Google Scholar] [CrossRef]
- Outen, J.D.; Burhanullah, M.H.; Vandrey, R.; Amjad, H.; Harper, D.G.; Patrick, R.E.; May, R.L.; Agronin, M.E.; Forester, B.P.; Rosenberg, P.B. Cannabinoids for Agitation in Alzheimer’s Disease. Am J Geriatr Psychiatry 2021, 29, 1253–1263. [Google Scholar] [CrossRef] [PubMed]
- Goveas, J.S. Commentary on “Cannabinoids for Agitation in Alzheimer’s Disease”. Am J Geriatr Psychiatry 2021, 29, 1264–1266. [Google Scholar] [CrossRef] [PubMed]
- Nirogi, R.; Ieni, J.; Goyal, V.K.; Ravula, J.; Jetta, S.; Shinde, A.; Jayarajan, P.; Benade, V.; Palacharla, V.R.C.; Dogiparti, D.K.; et al. Effect of masupirdine (SUVN-502) on cognition in patients with moderate Alzheimer’s disease: A randomized, double-blind, phase 2, proof-of-concept study. Alzheimers Dement (N Y) 2022, 8, e12307. [Google Scholar] [CrossRef]
- Nirogi, R.; Jayarajan, P.; Benade, V.; Shinde, A.; Goyal, V.K.; Jetta, S.; Ravula, J.; Abraham, R.; Grandhi, V.R.; Subramanian, R.; et al. Potential beneficial effects of masupirdine (SUVN-502) on agitation/aggression and psychosis in patients with moderate Alzheimer’s disease: Exploratory post hoc analyses. Int J Geriatr Psychiatry 2022, 37. [Google Scholar] [CrossRef]
- de Jong, I.E.M.; Mork, A. Antagonism of the 5-HT(6) receptor - Preclinical rationale for the treatment of Alzheimer’s disease. Neuropharmacology 2017, 125, 50–63. [Google Scholar] [CrossRef]
- Ferrero, H.; Solas, M.; Francis, P.T.; Ramirez, M.J. Serotonin 5-HT(6) Receptor Antagonists in Alzheimer’s Disease: Therapeutic Rationale and Current Development Status. CNS Drugs 2017, 31, 19–32. [Google Scholar] [CrossRef]
- Tomaszewski, M.R.; Meng, X.; Haley, H.D.; Harrell, C.M.; McDonald, T.P.; Miller, C.O.; Smith, S.M. Magnetic resonance imaging detects white adipose tissue beiging in mice following PDE10A inhibitor treatment. J Lipid Res 2023, 64, 100408. [Google Scholar] [CrossRef] [PubMed]
- Baker, M.; Song, W.; Fusick, A. Pimavanserin Use in Lewy Body Dementia: A Case Report Demonstrating the Medication’s Efficacy. Cureus 2023, 15, e46356. [Google Scholar] [CrossRef] [PubMed]
- Tariot, P.N.; Ballard, C.; Devanand, D.P.; Cummings, J.L.; Sultzer, D.L. Pimavanserin and dementia-related psychosis. Lancet Neurol 2022, 21, 114–115. [Google Scholar] [CrossRef]
- Ballard, C.; O’Brien, J.; Coope, B.; Fairbairn, A.; Abid, F.; Wilcock, G. A prospective study of psychotic symptoms in dementia sufferers: psychosis in dementia. Int Psychogeriatr 1997, 9, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Thorn, C.A.; Moon, J.; Bourbonais, C.A.; Harms, J.; Edgerton, J.R.; Stark, E.; Steyn, S.J.; Butter, C.R.; Lazzaro, J.T.; O’Connor, R.E.; et al. Striatal, Hippocampal, and Cortical Networks Are Differentially Responsive to the M4- and M1-Muscarinic Acetylcholine Receptor Mediated Effects of Xanomeline. ACS Chem Neurosci 2019, 10, 1753–1764. [Google Scholar] [CrossRef] [PubMed]
- Kaul, I.; Sawchak, S.; Correll, C.U.; Kakar, R.; Breier, A.; Zhu, H.; Miller, A.C.; Paul, S.M.; Brannan, S.K. Efficacy and safety of the muscarinic receptor agonist KarXT (xanomeline-trospium) in schizophrenia (EMERGENT-2) in the USA: results from a randomised, double-blind, placebo-controlled, flexible-dose phase 3 trial. Lancet 2024, 403, 160–170. [Google Scholar] [CrossRef]
- Sauder, C.; Allen, L.A.; Baker, E.; Miller, A.C.; Paul, S.M.; Brannan, S.K. Effectiveness of KarXT (xanomeline-trospium) for cognitive impairment in schizophrenia: post hoc analyses from a randomised, double-blind, placebo-controlled phase 2 study. Transl Psychiatry 2022, 12, 491. [Google Scholar] [CrossRef]
- Kidambi, N.; Elsayed, O.H.; El-Mallakh, R.S. Xanomeline-Trospium and Muscarinic Involvement in Schizophrenia. Neuropsychiatr Dis Treat 2023, 19, 1145–1151. [Google Scholar] [CrossRef]
- Leber, A.; Ramachandra, R.; Ceban, F.; Kwan, A.T.H.; Rhee, T.G.; Wu, J.; Cao, B.; Jawad, M.Y.; Teopiz, K.M.; Ho, R.; et al. Efficacy, safety, and tolerability of xanomeline for schizophrenia spectrum disorders: a systematic review. Expert Opin Pharmacother 2024. [Google Scholar] [CrossRef]
- Bergamini, G.; Coloma, P.; Massinet, H.; Steiner, M.A. What evidence is there for implicating the brain orexin system in neuropsychiatric symptoms in dementia? Front Psychiatry 2022, 13, 1052233. [Google Scholar] [CrossRef]
- Kron, J.O.J.; Keenan, R.J.; Hoyer, D.; Jacobson, L.H. Orexin Receptor Antagonism: Normalizing Sleep Architecture in Old Age and Disease. Annu Rev Pharmacol Toxicol 2024, 64, 359–386. [Google Scholar] [CrossRef] [PubMed]
- de Bruin, N.; van Loevezijn, A.; Wicke, K.M.; de Haan, M.; Venhorst, J.; Lange, J.H.M.; de Groote, L.; van der Neut, M.A.W.; Prickaerts, J.; Andriambeloson, E.; et al. The selective 5-HT6 receptor antagonist SLV has putative cognitive- and social interaction enhancing properties in rodent models of cognitive impairment. Neurobiol Learn Mem 2016, 133, 100–117. [Google Scholar] [CrossRef] [PubMed]
- Lardenoije, R.; Roubroeks, J.A.Y.; Pishva, E.; Leber, M.; Wagner, H.; Iatrou, A.; Smith, A.R.; Smith, R.G.; Eijssen, L.M.T.; Kleineidam, L.; et al. Alzheimer’s disease-associated (hydroxy)methylomic changes in the brain and blood. Clin Epigenetics 2019, 11, 164. [Google Scholar] [CrossRef] [PubMed]
- Watson, C.T.; Roussos, P.; Garg, P.; Ho, D.J.; Azam, N.; Katsel, P.L.; Haroutunian, V.; Sharp, A.J. Genome-wide DNA methylation profiling in the superior temporal gyrus reveals epigenetic signatures associated with Alzheimer’s disease. Genome Med 2016, 8, 5. [Google Scholar] [CrossRef]
- Koulousakis, P.; Willems, E.; Schepers, M.; Rombaut, B.; Prickaerts, J.; Vanmierlo, T.; van den Hove, D. Exogenous Oxytocin Administration Restores Memory in Female APP/PS1 Mice. J Alzheimers Dis 2023, 96, 1207–1219. [Google Scholar] [CrossRef]
- Journey, J.D.; Agrawal, S.; Stern, E. Dextromethorphan Toxicity. In StatPearls, Treasure Island (FL) ineligible companies. Disclosure: Suneil Agrawal declares no relevant financial relationships with ineligible companies. Disclosure: Evan Stern declares no relevant financial relationships with ineligible companies., 2024.
- Tampi, R.R.; Joshi, P.; Marpuri, P.; Tampi, D.J. Evidence for using dextromethorphan-quinidine for the treatment of agitation in dementia. World J Psychiatry 2020, 10, 29–33. [Google Scholar] [CrossRef]
- Garay, R.P.; Grossberg, G.T. AVP-786 for the treatment of agitation in dementia of the Alzheimer’s type. Expert Opin Investig Drugs 2017, 26, 121–132. [Google Scholar] [CrossRef]
- Alva, G.; Cubala, W.J.; Berrio, A.; Coate, B.; Abler, V.; Pathak, S. Safety Profile of Pimavanserin Therapy in Elderly Patients with Neurodegenerative Disease-Related Neuropsychiatric Symptoms: A Phase 3B Study. J Alzheimers Dis 2024, 98, 265–274. [Google Scholar] [CrossRef]
- Quiroz, J.A.; Machado-Vieira, R.; Zarate, C.A., Jr.; Manji, H.K. Novel insights into lithium’s mechanism of action: neurotrophic and neuroprotective effects. Neuropsychobiology 2010, 62, 50–60. [Google Scholar] [CrossRef]
- Devanand, D.P.; Crocco, E.; Forester, B.P.; Husain, M.M.; Lee, S.; Vahia, I.V.; Andrews, H.; Simon-Pearson, L.; Imran, N.; Luca, L.; et al. Low Dose Lithium Treatment of Behavioral Complications in Alzheimer’s Disease: Lit-AD Randomized Clinical Trial. Am J Geriatr Psychiatry 2022, 30, 32–42. [Google Scholar] [CrossRef]
- Hidding, U.; Mainka, T.; Buhmann, C. Therapeutic use of medical Cannabis in neurological diseases: a clinical update. J Neural Transm (Vienna) 2024, 131, 117–126. [Google Scholar] [CrossRef] [PubMed]
- Xiong, Y.; Lim, C.S. Understanding the Modulatory Effects of Cannabidiol on Alzheimer’s Disease. Brain Sci 2021, 11. [Google Scholar] [CrossRef]
- Dawson, L.A. The central role of 5-HT6 receptors in modulating brain neurochemistry. Int Rev Neurobiol 2011, 96, 1–26. [Google Scholar] [CrossRef]
- Zagorska, A.; Partyka, A.; Bucki, A.; Gawalskax, A.; Czopek, A.; Pawlowski, M. Phosphodiesterase 10 Inhibitors - Novel Perspectives for Psychiatric and Neurodegenerative Drug Discovery. Curr Med Chem 2018, 25, 3455–3481. [Google Scholar] [CrossRef] [PubMed]
- Layton, M.E.; Kern, J.C.; Hartingh, T.J.; Shipe, W.D.; Raheem, I.; Kandebo, M.; Hayes, R.P.; Huszar, S.; Eddins, D.; Ma, B.; et al. Discovery of MK-8189, a Highly Potent and Selective PDE10A Inhibitor for the Treatment of Schizophrenia. J Med Chem 2023, 66, 1157–1171. [Google Scholar] [CrossRef]
- Umbricht, D.; Abt, M.; Tamburri, P.; Chatham, C.; Holiga, S.; Frank, M.J.; Collins, A.G.E.; Walling, D.P.; Mofsen, R.; Gruener, D.; et al. Proof-of-Mechanism Study of the Phosphodiesterase 10 Inhibitor RG7203 in Patients With Schizophrenia and Negative Symptoms. Biol Psychiatry Glob Open Sci 2021, 1, 70–77. [Google Scholar] [CrossRef]
- Murray, A.J.; Rogers, J.C.; Katshu, M.; Liddle, P.F.; Upthegrove, R. Oxidative Stress and the Pathophysiology and Symptom Profile of Schizophrenia Spectrum Disorders. Front Psychiatry 2021, 12, 703452. [Google Scholar] [CrossRef]
- Forman, H.J.; Zhang, H. Targeting oxidative stress in disease: promise and limitations of antioxidant therapy. Nat Rev Drug Discov 2021, 20, 689–709. [Google Scholar] [CrossRef] [PubMed]
- Correia, A.S.; Cardoso, A.; Vale, N. Oxidative Stress in Depression: The Link with the Stress Response, Neuroinflammation, Serotonin, Neurogenesis and Synaptic Plasticity. Antioxidants (Basel) 2023, 12. [Google Scholar] [CrossRef]
- Klinedinst, N.J.; Regenold, W.T. A mitochondrial bioenergetic basis of depression. J Bioenerg Biomembr 2015, 47, 155–171. [Google Scholar] [CrossRef]
- Fries, G.R.; Saldana, V.A.; Finnstein, J.; Rein, T. Molecular pathways of major depressive disorder converge on the synapse. Mol Psychiatry 2023, 28, 284–297. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, S.; Nagappa, A.N.; Patil, C.R. Role of oxidative stress in depression. Drug Discov Today 2020, 25, 1270–1276. [Google Scholar] [CrossRef] [PubMed]
- Lehmann, M.L.; Weigel, T.K.; Poffenberger, C.N.; Herkenham, M. The Behavioral Sequelae of Social Defeat Require Microglia and Are Driven by Oxidative Stress in Mice. J Neurosci 2019, 39, 5594–5605. [Google Scholar] [CrossRef]
- Elamin, M.; Pender, N.; Hardiman, O.; Abrahams, S. Social cognition in neurodegenerative disorders: a systematic review. J Neurol Neurosurg Psychiatry 2012, 83, 1071–1079. [Google Scholar] [CrossRef] [PubMed]
- Dos Santos, T.; de Carvalho, R.L.S.; Nogueira, M.; Baptista, M.A.T.; Kimura, N.; Lacerda, I.B.; Dourado, M.C.N. The Relationship between Social Cognition and Executive Functions in Alzheimer’s Disease: A Systematic Review. Curr Alzheimer Res 2020, 17, 487–497. [Google Scholar] [CrossRef] [PubMed]
- Setien-Suero, E.; Murillo-Garcia, N.; Sevilla-Ramos, M.; Abreu-Fernandez, G.; Pozueta, A.; Ayesa-Arriola, R. Exploring the Relationship Between Deficits in Social Cognition and Neurodegenerative Dementia: A Systematic Review. Front Aging Neurosci 2022, 14, 778093. [Google Scholar] [CrossRef]
- Saris, I.M.J.; Aghajani, M.; Jongs, N.; Reus, L.M.; van der Wee, N.J.A.; Bilderbeck, A.C.; Winter van Rossum, I.; Arango, C.; de la Torre-Luque, A.; Malik, A.; et al. Cross-disorder and disorder-specific deficits in social functioning among schizophrenia and alzheimer’s disease patients. PLoS One 2022, 17, e0263769. [Google Scholar] [CrossRef]
- Legaz, A.; Prado, P.; Moguilner, S.; Baez, S.; Santamaria-Garcia, H.; Birba, A.; Barttfeld, P.; Garcia, A.M.; Fittipaldi, S.; Ibanez, A. Social and non-social working memory in neurodegeneration. Neurobiol Dis 2023, 183, 106171. [Google Scholar] [CrossRef]
- Stam, D.; Rosseel, S.; De Winter, F.L.; Van den Bossche, M.J.A.; Vandenbulcke, M.; Van den Stock, J. Facial expression recognition deficits in frontotemporal dementia and Alzheimer’s disease: a meta-analytic investigation of effects of phenotypic variant, task modality, geographical region and symptomatic specificity. J Neurol 2023, 270, 5731–5755. [Google Scholar] [CrossRef]
- Singleton, E.H.; Fieldhouse, J.L.P.; van ‘t Hooft, J.J.; Scarioni, M.; van Engelen, M.E.; Sikkes, S.A.M.; de Boer, C.; Bocancea, D.I.; van den Berg, E.; Scheltens, P.; et al. Social cognition deficits and biometric signatures in the behavioural variant of Alzheimer’s disease. Brain 2023, 146, 2163–2174. [Google Scholar] [CrossRef]
- Goldberg, T.E.; Choi, J.; Lee, S.; Gurland, B.; Devanand, D.P. Effects of restriction of activities and social isolation on risk of dementia in the community. Int Psychogeriatr 2021, 33, 1207–1215. [Google Scholar] [CrossRef] [PubMed]
- Drinkwater, E.; Davies, C.; Spires-Jones, T.L. Potential neurobiological links between social isolation and Alzheimer’s disease risk. Eur J Neurosci 2022, 56, 5397–5412. [Google Scholar] [CrossRef] [PubMed]
- Ren, Y.; Savadlou, A.; Park, S.; Siska, P.; Epp, J.R.; Sargin, D. The impact of loneliness and social isolation on the development of cognitive decline and Alzheimer’s Disease. Front Neuroendocrinol 2023, 69, 101061. [Google Scholar] [CrossRef] [PubMed]
- Joshi, P.; Hendrie, K.; Jester, D.J.; Dasarathy, D.; Lavretsky, H.; Ku, B.S.; Leutwyler, H.; Torous, J.; Jeste, D.V.; Tampi, R.R. Social connections as determinants of cognitive health and as targets for social interventions in persons with or at risk of Alzheimer’s disease and related disorders: a scoping review. Int Psychogeriatr 2024, 36, 92–118. [Google Scholar] [CrossRef]
- Livingston, G.; Huntley, J.; Sommerlad, A.; Ames, D.; Ballard, C.; Banerjee, S.; Brayne, C.; Burns, A.; Cohen-Mansfield, J.; Cooper, C.; et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet 2020, 396, 413–446. [Google Scholar] [CrossRef]
- Rey, C.C.; Robert, V.; Bouisset, G.; Loisy, M.; Lopez, S.; Cattaud, V.; Lejards, C.; Piskorowski, R.A.; Rampon, C.; Chevaleyre, V.; et al. Altered inhibitory function in hippocampal CA2 contributes in social memory deficits in Alzheimer’s mouse model. iScience 2022, 25, 103895. [Google Scholar] [CrossRef]
- Rajagopal, L.; Huang, M.; Mahjour, S.; Ryan, C.; Elzokaky, A.; Svensson, K.A.; Meltzer, H.Y. The dopamine D1 receptor positive allosteric modulator, DETQ, improves cognition and social interaction in aged mice and enhances cortical and hippocampal acetylcholine efflux. Behav Brain Res 2024, 459, 114766. [Google Scholar] [CrossRef]
- Michaelian, J.C.; McCade, D.; Hoyos, C.M.; Brodaty, H.; Harrison, F.; Henry, J.D.; Guastella, A.J.; Naismith, S.L. Pilot Randomized, Double-Blind, Placebo-Controlled Crossover Trial Evaluating the Feasibility of an Intranasal Oxytocin in Improving Social Cognition in Individuals Living with Alzheimer’s Disease. J Alzheimers Dis Rep 2023, 7, 715–729. [Google Scholar] [CrossRef]
- Nadeem, M.S.; Hosawi, S.; Alshehri, S.; Ghoneim, M.M.; Imam, S.S.; Murtaza, B.N.; Kazmi, I. Symptomatic, Genetic, and Mechanistic Overlaps between Autism and Alzheimer’s Disease. Biomolecules 2021, 11. [Google Scholar] [CrossRef]
- Steubler, V.; Erdinger, S.; Back, M.K.; Ludewig, S.; Fassler, D.; Richter, M.; Han, K.; Slomianka, L.; Amrein, I.; von Engelhardt, J.; et al. Loss of all three APP family members during development impairs synaptic function and plasticity, disrupts learning, and causes an autism-like phenotype. EMBO J 2021, 40, e107471. [Google Scholar] [CrossRef]
- Sokol, D.K.; Lahiri, D.K. APPlications of amyloid-beta precursor protein metabolites in macrocephaly and autism spectrum disorder. Front Mol Neurosci 2023, 16, 1201744. [Google Scholar] [CrossRef] [PubMed]
- Sokol, D.K.; Lahiri, D.K. Neurodevelopmental disorders and microcephaly: how apoptosis, the cell cycle, tau and amyloid-beta precursor protein APPly. Front Mol Neurosci 2023, 16, 1201723. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Cai, F.; Lu, R.; Xing, X.; Xu, L.; Wu, K.; Gong, Z.; Zhang, Q.; Zhang, Y.; Xing, M.; et al. CNTNAP2 intracellular domain (CICD) generated by gamma-secretase cleavage improves autism-related behaviors. Signal Transduct Target Ther 2023, 8, 219. [Google Scholar] [CrossRef]
- Zhang, Q.; Xu, L.; Bai, Y.; Chen, P.; Xing, M.; Cai, F.; Wu, Y.; Song, W. Intermittent hypoxia-induced enhancement of sociability and working memory associates with CNTNAP2 upregulation. Front Mol Neurosci 2023, 16, 1155047. [Google Scholar] [CrossRef] [PubMed]
- Lahiri, D.K.; Sokol, D.K.; Erickson, C.; Ray, B.; Ho, C.Y.; Maloney, B. Autism as early neurodevelopmental disorder: evidence for an sAPPalpha-mediated anabolic pathway. Front Cell Neurosci 2013, 7, 94. [Google Scholar] [CrossRef]
- Ray, B.; Sokol, D.K.; Maloney, B.; Lahiri, D.K. Finding novel distinctions between the sAPPalpha-mediated anabolic biochemical pathways in Autism Spectrum Disorder and Fragile X Syndrome plasma and brain tissue. Sci Rep 2016, 6, 26052. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



