
Submitted:
19 September 2024
Posted:
25 September 2024
You are already at the latest version
Abstract
Cervical mesonephric ductal adenocarcinoma (MA) is a HPV-independent adenocarcinoma that originates from remnants of the wolffian duct in the male reproductive system during fetal development and occurs in middle-aged women. MA is a rare disease that accounts for less than 1% of all cervical adenocarcinomas. We report a case of MA in which abdominal radical hysterectomy(ARH) was performed after neoadjuvant chemotherapy (NAC). The patient was a 66-year-old woman with abnormal genital bleeding. A colposcopy examination revealed macroscopic invasive cancer. A pelvic MRI scan revealed a 53 × 26 mm tumor in the cervix, and the histological diagnosis of the cervix was endometrioid carcinoma, with the diagnosis being cervical adenocarcinoma cT1b3N0M0. One course of NAC with paclitaxel-carboplatin (PC) was administered to shrink the tumor and stop the bleeding, and ARH was performed. Postoperative histopathological diagnosis was MA. The surgical margins of the resected specimen were negative, and NAC had been effective, so the patient underwent five courses of PC therapy after surgery. There has been no recurrence 12 months after surgery. There is no established standard treatment, but there are reports that PC therapy is effective. It is necessary to search for effective treatments by following up and accumulating further cases.
Keywords:
Cervical mesonephric adenocarcinoma
; Neoadjuvant chemotherapy
; Adjuvant chemotherapy
1. Introduction
Mesonephric adenocarcinoma (MA) of the cervix is HPV-independent adenocarcinoma [1]. It is currently believed that MA originates from remnants of the Wolffian duct in the male reproductive system during fetal development and occurs in middle-aged women. The average age of patients is 53 years, and it often originates from the lateral wall of the cervix [1]. MA is a rare form of cervical adenocarcinoma, accounting for less than 1% of all cervical adenocarcinomas. In a multicenter collaborative study by Pors J et al. [2], 30 cases of MA and their clinicopathological characteristics were analyzed. Follow-up data revealed that the prognosis of cervical MA was worse than that of HPV-related adenocarcinoma. No standard treatment has been established for cervical MA. We report a case of cervical MA in which radical hysterectomy was performed after neoadjuvant chemotherapy, based on a literature review.
2. Clinical Case
66 years old, G2P2, menopause at 58 years old. Medical history: diabetes.
She had been experiencing abnormal genital bleeding for the past six months, and one month ago she began experiencing daily bleeding, so she visited a local doctor. A cytological examination at a local hospital revealed cervical cytology, AGC, and endometrial cytology class IIIb, and a tumor was found in the cervix. A cervical biopsy was performed, and the patient was diagnosed with endometrioid carcinoma, and referred to our hospital. Colposcopy of the cervix at our hospital revealed a bulky tumor occupying the vagina, and the tumor was diagnosed as macroscopic invasive carcinoma (Figure 1). A transvaginal ultrasound scan revealed a cervical tumor measuring 47 × 22 mm (Figure 2), and a pelvic MRI scan revealed a cervical tumor measuring 53 × 26 mm (Figure 3A). CT scan showed no distant metastasis. Tumor markers were CA125: 13.3 U/ml, CEA: 2.4 U/ml, CA19-9: 6.5 U/L, SCC: 0.5 ng/ml, and no abnormal values were found. A histological diagnosis of the cervix at our hospital also revealed a diagnosis of endometrioid carcinoma. Based on the above, the patient was diagnosed with cervical adenocarcinoma, clinical stage IB3 (cT1b3N0M0). Surgery was scheduled for 40 days later. As the tumor was bulky and bleeding continued, one course of neoadjuvant chemotherapy with paclitaxel-carboplatin (PC) was administered with the aim of reducing the tumor and stopping the bleeding. After one course of PC, the cervical tumor was reduced in size (Figure 3B), and the patient was diagnosed with partial response(PR).
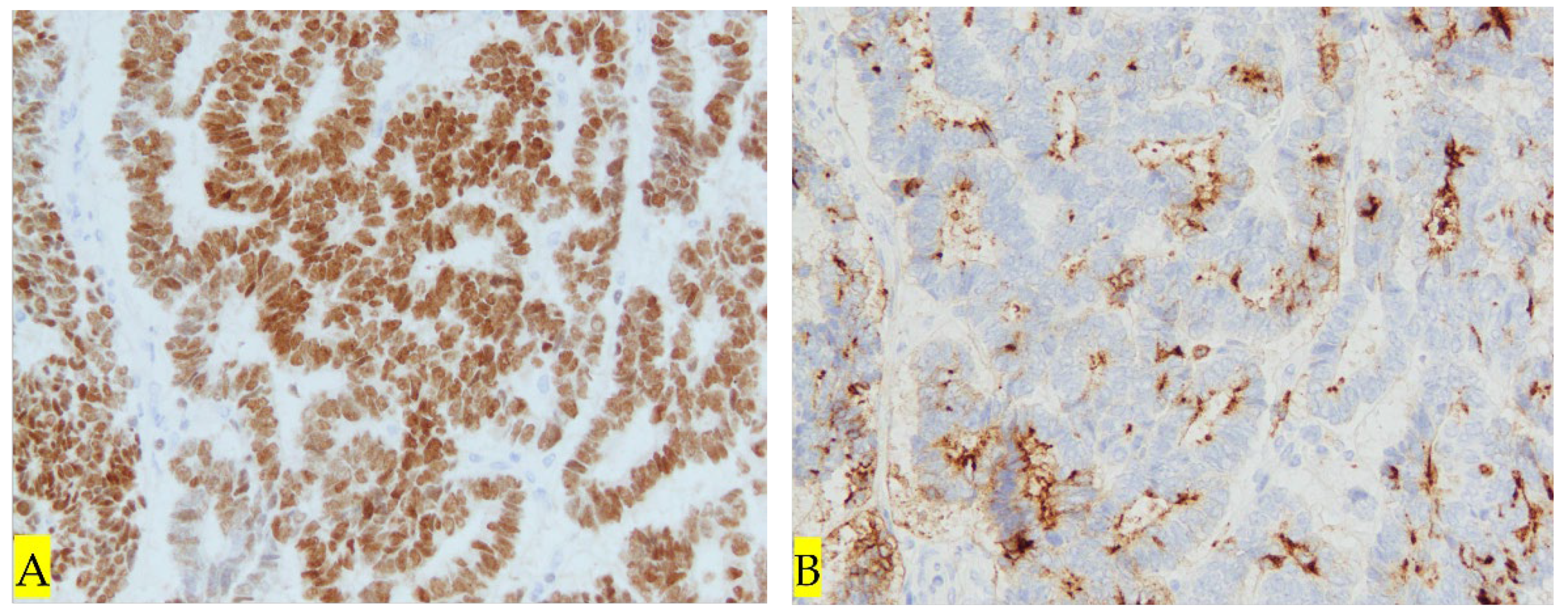
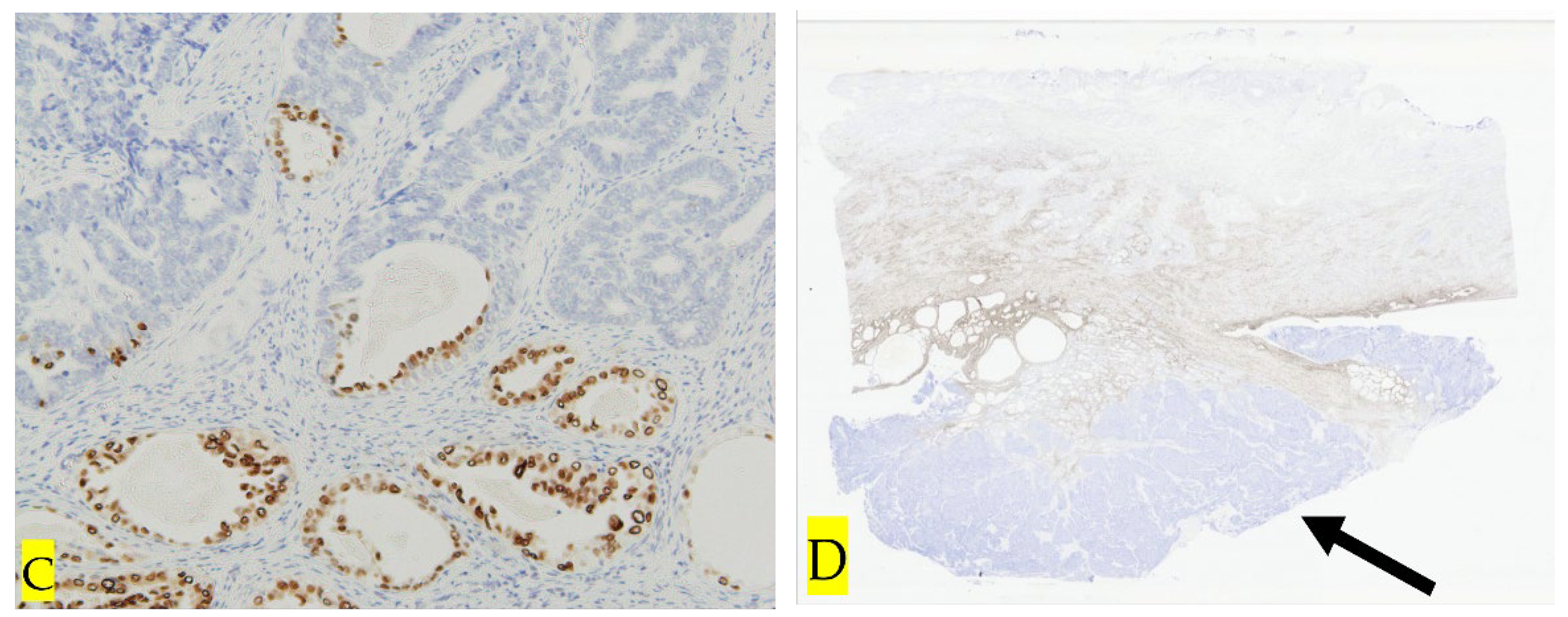
40 days after the initial consultation, an abdominal radical hysterectomy + bilateral salpingo-oophorectomy + pelvic lymphadenectomy (ARH+BSO+PLA) was performed. The operation time was 6 hours and 22 minutes, the blood loss was 905ml, and the postoperative course was uneventful, and the patient was discharged on the 9th day after the operation. Macroscopic findings of the resected specimen showed that the resection margins between the tumor and the parametria were negative, and the resection was diagnosed as complete (Figure4). HE staining revealed that atypical cells proliferated forming a lumen, and the lumen contained eosinophilic protein substances (Figure5A). Morphologically, the tumor resembled endometrioid carcinoma, but remnants of the mesonephric duct are observed (Figure5B). Immunohistochemistry showed that it was transacting T-cell-specific transcription factor GATA-3 (GATA3) (Figure 6A), clusters of differentiation 10 (CD10) (Figure 6B) and thyroid transcription factor 1 (TTF-1) positive (Figure 6C)and estrogen receptor (ER) negative, (Figure 6D) and the tumor was diagnosed as HPV-independent mesonephric adenocarcinoma. The surgical margins of the resected specimen were negative, and the tumor was sufficiently separated from the lesion. As preoperative chemotherapy was effective, the patient underwent five courses of PC therapy after surgery. There has been no recurrence as of 12 months after surgery.
Figure 3.
A Pelvic MRI T2 weighted image : A cervical tumor measuring 53 × 26 mm. Before chemotherapy. Figure 3B Pelvic MRI T2 weighted image : After one course of neoadjuvant chemotherapy with paclitaxel-carboplatin (PC) . A cervical tumor measuring 43×23 mm. The tumor shrank and PR was diagnosed.
Figure 3.
A Pelvic MRI T2 weighted image : A cervical tumor measuring 53 × 26 mm. Before chemotherapy. Figure 3B Pelvic MRI T2 weighted image : After one course of neoadjuvant chemotherapy with paclitaxel-carboplatin (PC) . A cervical tumor measuring 43×23 mm. The tumor shrank and PR was diagnosed.

Figure 4.
Macroscopic findings of the resected specimen showed that the resection margins between the tumor and the parametria were negative, and the resection was diagnosed as complete. ① → Cervical tumor ② → Tumor that has fallen off from the cervical tumor.
Figure 4.
Macroscopic findings of the resected specimen showed that the resection margins between the tumor and the parametria were negative, and the resection was diagnosed as complete. ① → Cervical tumor ② → Tumor that has fallen off from the cervical tumor.
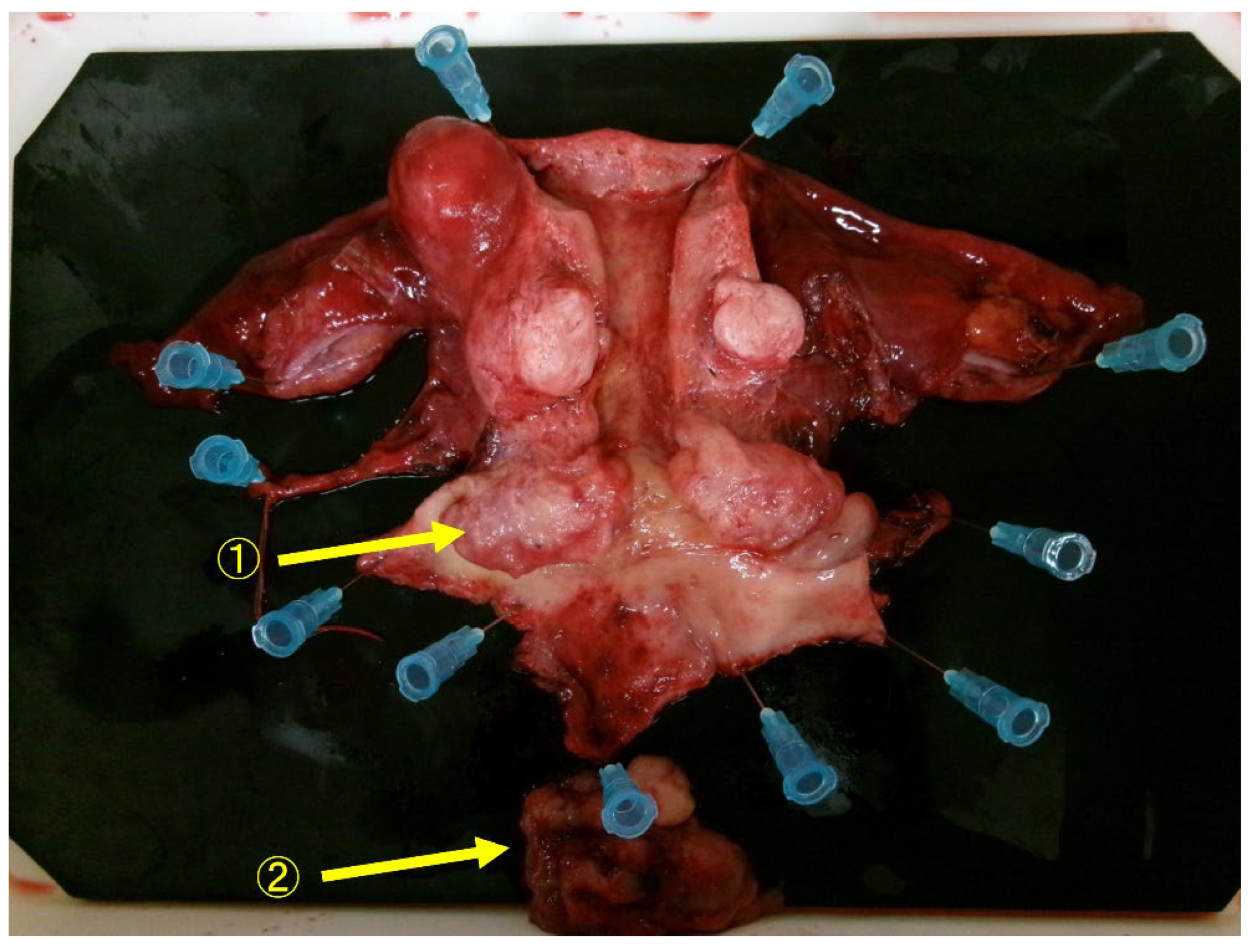
Figure 5.
A HE staining 100×. Atypical cells proliferate and form a lumen that contains eosinophilic protein material. Figure5B HE staining 100×. Remnants of the mesonephric duct are observed (→).
Figure 5.
A HE staining 100×. Atypical cells proliferate and form a lumen that contains eosinophilic protein material. Figure5B HE staining 100×. Remnants of the mesonephric duct are observed (→).
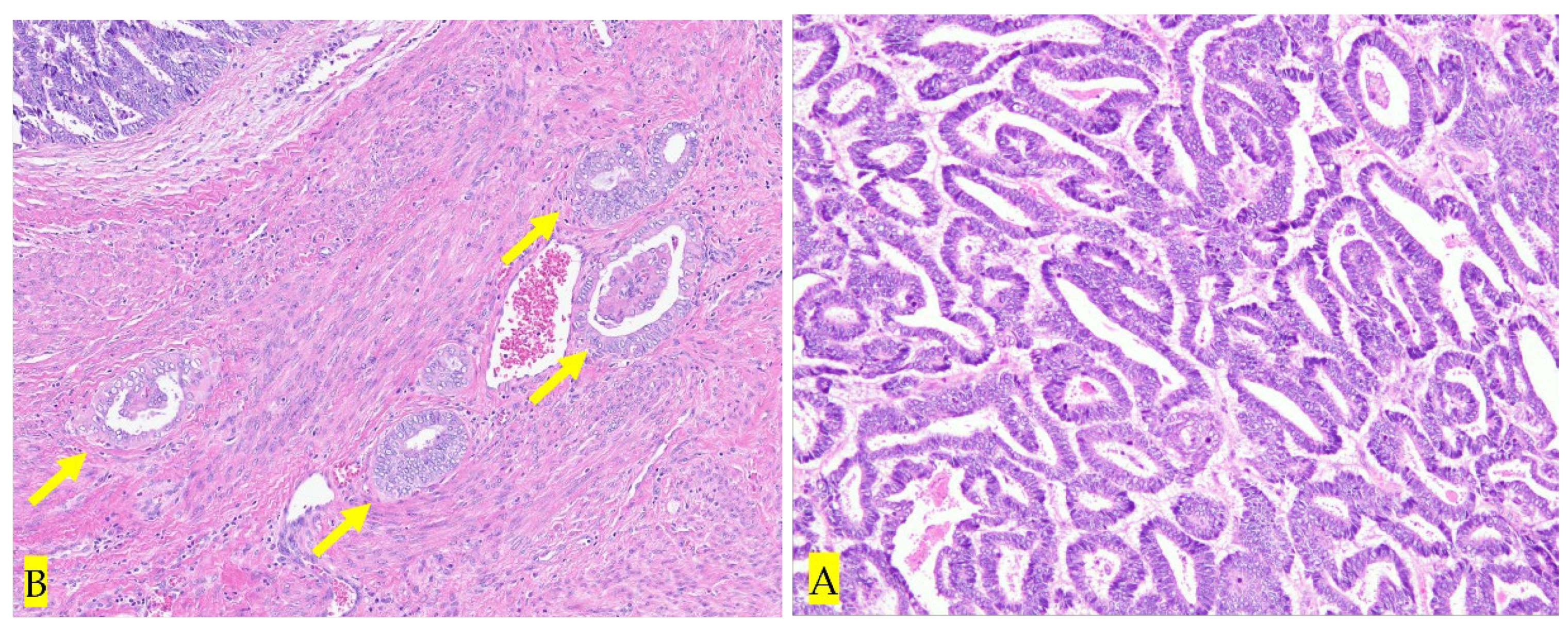
Figure 6.
A Immunostaining: GATA 200×. GATA positive in tumor tissue. Figure6B Immunostaining: CD10 100×. CD10 positivity found in the stroma. Figure6C Immunostaining: TTF-1 200×. TTF-1 positive in some tumor tissues. Figure6D Immunostaining: ER 1×. ER negative in tumor tissue (→).
Figure 6.
A Immunostaining: GATA 200×. GATA positive in tumor tissue. Figure6B Immunostaining: CD10 100×. CD10 positivity found in the stroma. Figure6C Immunostaining: TTF-1 200×. TTF-1 positive in some tumor tissues. Figure6D Immunostaining: ER 1×. ER negative in tumor tissue (→).
3. Discussion
The mesonephric duct, also known as the Wolffian duct, runs parallel to the paramesonephric duct (Mullerian duct) during early pregnancy, and in men it develops and differentiates into the male internal genital organs (epididymis and vas deferens) under the action of testosterone.
In women, unlike men, the paramesonephric ducts (Mullerian ducts) develop and differentiate to form the female internal genital organs (uterus, fallopian tubes, and upper one-third of the vagina [3]. In women, the mesonephric duct regresses, but residual tissue may be found around the ovary, within the broad ligament, uterus, and vagina [4]. Cervical mesonephric adenocarcinoma (MA) has been reported to arise mostly from the mesonephric duct located deep within the lateral wall of the cervix, but it can also arise from remnants of the mesonephric duct in the uterine body [5].
The initial symptom of cervical MA is often abnormal genital bleeding [5], and in this case, the diagnosis was made based on abnormal genital bleeding. It has been reported that the detection rate of abnormal cells in cytology is as low as 10% [5], but in this case, a solid tumor was already occupying the vagina at the time of initial diagnosis, and cervical cytology showed that AGC was diagnosed. Cervical MA has a wide variety of histological findings, and the preoperative diagnostic rate in biopsy tissue is reported to be 20% [6]. Therefore, it has been reported that it may be confused with other more common adenocarcinomas, such as serous, clear cell, or endometrial adenocarcinoma [7]. The classic histopathological pattern is the proliferation of columnar cells forming lumina containing acidophilic hyaline secretions [1]. In this case, preoperative pathological diagnosis showed that atypical cells had a glandular structure, and the case was diagnosed as cervical endometrioid carcinoma. In addition to morphological features, immunostaining is effective in diagnosing cervical MA. In tumor tissue, GATA-3, paired box 8 (PAX8), and CD10 were positive, and ER was negative. TTF-1 is rarely positive, p16 is not distributed, and HPV is usually not detected [1]. In this case, columnar cells proliferated and formed a lumen containing acidophilic hyaline-like secretions, and immunohistochemistry was positive for GATA3, PAX8, CD10, TTF-1, and negative for ER. The preoperative diagnosis was endometrioid carcinoma, but the final pathological diagnosis was MA..
There are few comprehensive reports on the prognosis of cervical MA, but Pors et al. reported the clinical characteristics in a multi-institutional study [2]. Of 30 cases of cervical MA, 25 were available for analysis; 10 cases (20%) were FIGO Stage I, and 15 cases (60%) were FIGO Stage II to IV. Lymph node metastasis was observed in 28% (4/14), and the recurrence rate was 50% (12/24), with the most common site of metastasis being the lungs 2). The 5-year progression-free survival rate was 60%, and the overall survival rate was 74%. Multivariate analysis revealed that the disease progression-free survival rate was associated with advanced stage (P value 0.04), but no association was observed with age, tumor size, or lymph node metastasis [2]. In a two-year follow-up study of cervical MA, HPV-dependent adenocarcinoma, and HPV-independent adenocarcinoma, the PFS of HPV-dependent adenocarcinoma was favorable (P value <0.01), while no significant difference in PFS was observed between cervical MA and HPV-independent adenocarcinoma [2]. Based on these facts, cervical MA has a poorer prognosis than HPV-dependent cervical cancer, and is a pathological condition that is prone to distant metastasis, especially lung metastasis, but it is a rare disease and there is no evidence regarding treatment. There is a lack of standard treatment, and no standard treatment has been established.
We reviewed literature reporting on the treatment of cervical MA over the past 10 years from 2014 to 2024 (Table1). Neoadjuvant chemotherapy (NAC) was administered to 3 patients, including this case, and all were partial responded, and radical hysterectomy was subsequently performed. The initial treatment for all 12 patients was total hysterectomy, and as postoperative adjuvant therapy., 4 patients underwent CCRT and 1 patient received radiation therapy alone. Chemotherapy was administered in 3 patients, and no post-treatment was administered in 4 patients. The effect of NAC in improving prognosis in stage I-II cervical cancer is unclear [17]. However, NAC is being considered as an option for patients undergoing elective treatment for cervical cancer during the COVID-19 pandemic, according to the International Gynecologic Cancer Society (IGCS) and the European Society of Gynecological Oncology (ESGO) [18]. In this case, the preoperative pathological diagnosis was endometrioid carcinoma, which is HPV-independent, and radiation therapy may have been ineffective. In addition, the bulky tumor occupied the vagina and there was a lot of bleeding, so early treatment was necessary. Therefore, PC therapy was administered as NAC, and since the tumor were partial responded and bleeding decreased, a radical hysterectomy was performed after one course of chemotherapy was completed. Although the number of cases of NAC is limited, all three reported cases were successful, and therefore we believe that NAC should also be considered for cervical MA. Concerning postoperative adjuvant therapy for cervical cancer, CCRT is recommended for cases at risk of recurrence [19]. On the other hand, in a clinical trial investigating the effectiveness of radiation alone, CCRT, and chemotherapy as postoperative therapy for stage IB-II cervical adenocarcinoma, it was reported that there was no difference in survival rate among the three groups, and chemotherapy may also be effective as a postoperative adjuvant therapy [20]. Although no clear standard chemotherapy has been established for cervical MA, there have been reported cases in which PC therapy was effective in recurrent cases [21]. Considering these circumstances, in this case, because NAC had been effective and the tumor resection margins were adequately secured, chemotherapy with PC therapy was selected as postoperative adjuvant therapy.

Table 1.
Literature reporting on the treatment of cervical MA over the past 10 years from 2014 to 2024.
Table 1.
Literature reporting on the treatment of cervical MA over the past 10 years from 2014 to 2024.
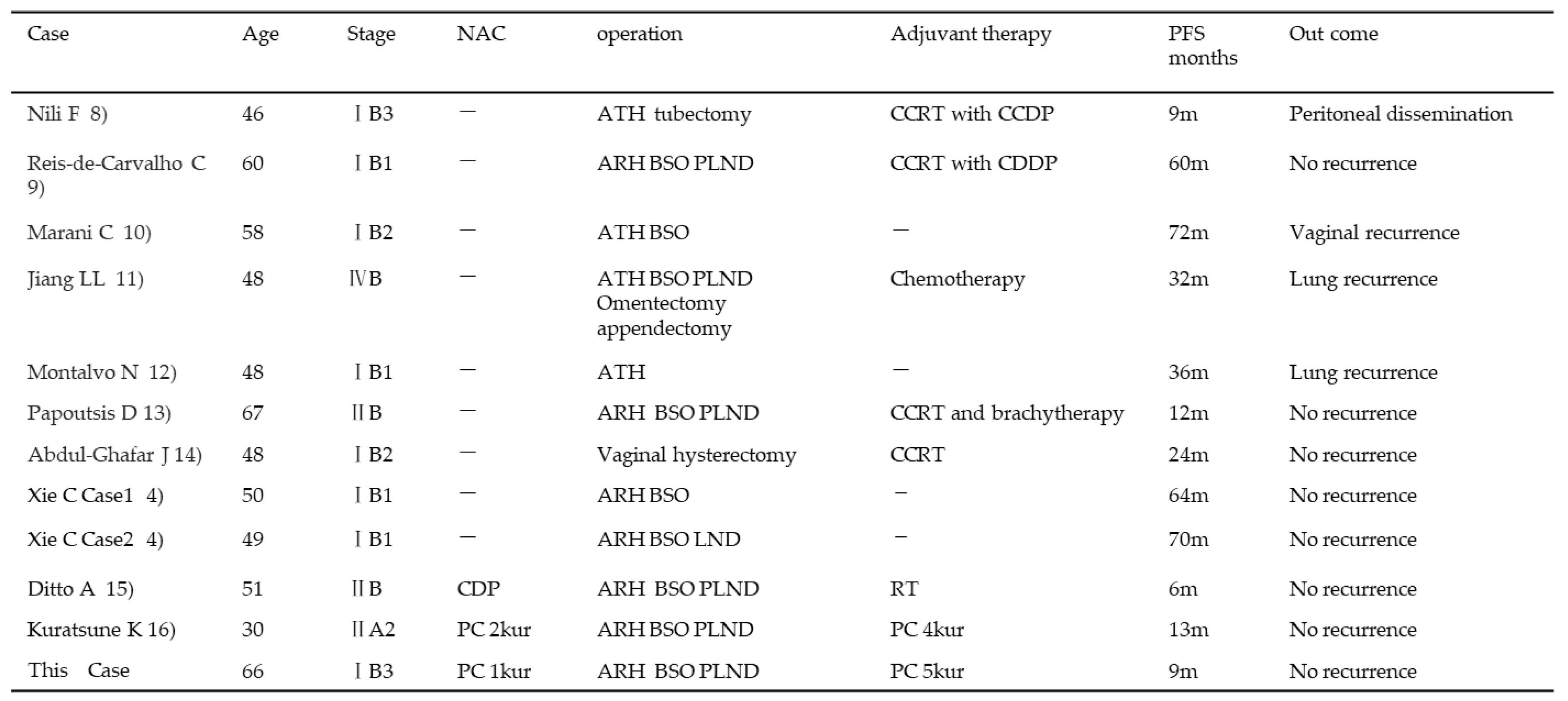 |
ATH : Abdominal total hysterectomy, CCRT : Concurrent chemoradiotherapy, CDDP : Cisplatin, ARH : Abdominal radical hysterectomy, BSO: Bilateral salpingo-oophorectomy, PLND : Pelvic lymphadenectomy, LND : Lymph node dissection, CDP: Cisplatin Doxorubicin Paclitaxel, PC : Paclitaxel Carboplatin.
4. Conclusions
We report a case of cervical mesonephric adenocarcinoma in which preoperative chemotherapy was effective. Cervical MA is very rare, and preoperative diagnosis is difficult. Because it is a rare disease, there is currently no established standard treatment, but it has been suggested that PC therapy may be effective. This disease is characterized by a high incidence of distant metastasis to the lungs and other organs, and it is necessary to conduct long-term follow-up and accumulate more cases to find effective treatments.
Author Contributions
Conceptualisation: H.I., H.E.; methodology: H.I.,M.M., M.N.; validation: H.I., A.T.; formal analysis: H.I.; investigation: H.I., R.W., and N.H. ; resources: H.I., R.W., and N.H., ;data curation: H.I, M.M, H.E. and M.N.; writing—original draft preparation: H.I.;writing—review and editing: H.I.; visualisation: H.I., M.N., and N.H.; supervision: N.H., A.T. ; project administration: H,I. All authors have read and agreed to the published version of the manuscript.Conceptualisation: H.I.,
Funding
This research received no external funding.
Informed Consent Statement
Informed consent has been obtained from the patient(s) to publish this paper.
Data Availability Statement
Datasets generated and/or analysed during the current study are available from the corresponding author upon reasonable request.
Acknowledgments
Editage has provided English proofreading.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of this study; in the collection, analysis, or interpretation of the data; in the writing of the manuscript; or in the decision to publish the results.
References
- WHO Classification of Tumours Female Genital Tumours[M] (5th ed.), Lyon: IARC Press (2020), pp. 378-379.
- Pors, J.; Segura, S.; Chiu, D.S.; Almadani, N.; Ren, H.; Fix, D.J.; Howitt, B.E.; Kolin, D.; McCluggage, W.G.; Mirkovic, J.; Gilks, B.; Park, K.J.; Hoang, L. Clinicopathologic Characteristics of Mesonephric Adenocarcinomas and Mesonephric-like Adenocarcinomas in the Gynecologic Tract: A Multi-institutional Study. Am J Surg Pathol. 2021, 45, 498–506. [Google Scholar] [CrossRef] [PubMed]
- Howitt, B.E.; Nucci, M.R. Mesonephric proliferations of the female genital tract. Pathology. 2018, 50, 141–150, Epub 2017 Dec 19. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Zhang, L.; Cao, W.; Hu, Y.; Liu, Y. Mesonephric adenocarcinoma of the uterine corpus. Int J Clin Exp Pathol. 2014, 7, 7012–7019. [Google Scholar] [PubMed]
- Xie, C.; Chen, Q.; Shen, Y. Mesonephric adenocarcinomas in female genital tract: A case series. Medicine (Baltimore). 2021, 100, e27174. [Google Scholar] [CrossRef] [PubMed]
- McFarland, M.; Quick, C.M.; McCluggage, W.G. Hormone receptor-negative, thyroid transcription factor 1-positive uterine and ovarian adenocarcinomas: report of a series of mesonephric-like adenocarcinomas. Histopathology. 2016, 68, 1013–1020, Epub 2016 Jan 4. [Google Scholar] [CrossRef] [PubMed]
- Secosan, C.; Balint, O.; Ilian, A.; Balan, L.; Balulescu, L.; Motoc, A.; Zahoi, D.; Grigoras, D.; Pirtea, L. New Insights in the Diagnosis of Rare Adenocarcinoma Variants of the Cervix-Case Report and Review of Literature. Healthcare (Basel). 2022, 10, 1410. [Google Scholar] [CrossRef] [PubMed]
- Nili, F.; Salarvand, S.; Saffar, H.; Kalaghchi, B.; Ghalehtaki, R. Mesonephric Adenocarcinoma of Uterine Cervix: A Case Report and Review of the Literature. Iran J Pathol. 2021, 16, 227–231, Epub 2020 Dec 21. [Google Scholar] [CrossRef] [PubMed]
- Reis-de-Carvalho, C.; Vaz-de-Macedo, C.; Ortiz, S.; Colaço, A.; Calhaz-Jorge, C. Cervical Mesonephric Adenocarcinoma: A Case Report of a Rare Gynecological Tumor from Embryological Remains of the Female Genital Tract. Rev Bras Ginecol Obstet. 2021, 43, 329–333, Epub 2021 Mar 30. [Google Scholar] [CrossRef] [PubMed]
- Marani, C.; Akaev, I.; Yeoh, C.C.; Walsh, E.; Rahimi, S. Cervical malignant mixed mesonephric tumour: A case report with local recurrence after six-years and next-generation sequencing analysis with particular reference to the ataxia telangiectasia mutated gene. Exp Ther Med. 2021, 21, 394, Epub 2021 Feb 24. [Google Scholar] [CrossRef] [PubMed]
- Jiang, L.L.; Tong, D.M.; Feng, Z.Y.; Liu, K.R. Mesonephric adenocarcinoma of the uterine cervix with rare lung metastases: A case report and review of the literature. World J Clin Cases. 2020, 8, 1735–1744. [Google Scholar] [CrossRef] [PubMed]
- Montalvo, N.; Redrobán, L.; Galarza, D. Mesonephric adenocarcinoma of the cervix: a case report with a three-year follow-up, lung metastases, and next-generation sequencing analysis. Diagn Pathol. 2019, 14, 71. [Google Scholar] [CrossRef] [PubMed]
- Papoutsis, D.; Sahu, B.; Kelly, J.; Antonakou, A. Perivascular epithelioid cell tumour and mesonephric adenocarcinoma of the uterine cervix: an unknown co-existence. Oxf Med Case Reports. 2019, 2019, omy115. [Google Scholar] [CrossRef] [PubMed]
- Abdul-Ghafar, J.; Chong, Y.; Han, H.D.; Cha, D.S.; Eom, M. Mesonephric Adenocarcinoma of the Uterine Cervix Associated with Florid Mesonephric Hyperplasia: A Case Report. J Lifestyle Med. 2013, 3, 117–120, Epub 2013 Sep 30. [Google Scholar]
- Ditto, A.; Martinelli, F.; Bogani, G.; Gasparri, M.L.; Donato, V.D.; Paolini, B.; Carcangiu, M.L.; Lorusso, D.; Raspagliesi, F. Bulky mesonephric adenocarcinoma of the uterine cervix treated with neoadjuvant chemotherapy and radical surgery: report of the first case. Tumori. 2016, 102 (Suppl. 2). [Google Scholar] [CrossRef] [PubMed]
- Kuratsune, K.; Ueda, T.; Tajiri, R.; Tohyama, A.; Hoshino, K.; Harada, H.; Kurita, T.; Kubo, C.; Komatsu, K.; Shiba, E.; Matsuura, Y.; Yoshino, K. [A Case of Adenocarcinoma, HPV-independent, Mesonephric Type with Significant Response to Neoadjuvant Chemotherapy]. J UOEH. 2024, 46, 45–51, Japanese. [Google Scholar] [CrossRef] [PubMed]
- Zhao, H.; He, Y.; Yang, S.L.; Zhao, Q.; Wu, Y.M. Neoadjuvant chemotherapy with radical surgery vs radical surgery alone for cervical cancer: a systematic review and meta-analysis. Onco Targets Ther 2019, 12, 1881–1891. [Google Scholar] [CrossRef] [PubMed]
- Ramirez, P.T.; Chiva, L.; Eriksson, A.G.Z.; Frumovitz, M.; Fagotti, A.; Gonzalez Martin, A.; Jhingran, A.; Pareja, R. COVID-19 Global Pandemic: Options for Management of Gynecologic Cancers. Int J Gynecol Cancer. 2020, 30, 561–563, Epub 2020 Mar 27. [Google Scholar] [CrossRef] [PubMed]
- Rosa, D.D.; Medeiros, L.R.; Edelweiss, M.I.; Pohlmann, P.R.; Stein, A.T. Adjuvant platinum-based chemotherapy for early stage cervical cancer. Cochrane Database Syst Rev. 2012, 6, CD005342, Update in: Cochrane Database Syst Rev. 2016 Nov 22;11:CD005342. [Google Scholar] [CrossRef] [PubMed]
- Shimada, M.; Nishimura, R.; Hatae, M.; Hiura, M.; Takehara, K.; Tase, T.; Yamada, H.; Kurachis, H.; Sugiyama, T.; Kigawa, J. Comparison of adjuvant chemotherapy and radiotherapy in patients with cervical adenocarcinoma of the uterus after radical hysterectomy: SGSG/TGCU Intergroup surveillance. Eur J Gynaecol Oncol. 2013, 34, 425–428. [Google Scholar] [PubMed]
- Montagut, C.; Mármol, M.; Rey, V.; Ordi, J.; Pahissa, J.; Rovirosa, A.; Gascón, P.; Mellado, B. Activity of chemotherapy with carboplatin plus paclitaxel in a recurrent mesonephric adenocarcinoma of the uterine corpus. Gynecol Oncol. 2003, 90, 458–461. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



