
Submitted:
25 September 2024
Posted:
25 September 2024
You are already at the latest version
Abstract
This paper presents a comprehensive comparative analysis of head and neck cancer (HNC) biomarkers, a prevalent but molecularly diverse malignancy. We detail the roles of key proteins and genes in tumorigenesis and progression, emphasizing their diagnostic, prognostic, and therapeutic relevance. Our bioinformatic validation reveals crucial genes such as AURKA, HMGA2, MMP1, PLAU, and SERPINE1, along with microRNAs (miRNA) linked to HNC progression. OncomiRs, including hsa-miR-21-5p, hsa-miR-31-5p, hsa-miR-221-3p, hsa-miR-222-3p, hsa-miR-196a-5p, and hsa-miR-200c-3p, drive tumorigenesis, while tumour-suppressive miRNAs like hsa-miR-375 and hsa-miR-145-5p inhibit it. Notably, hsa-miR-155-3p correlates with survival outcomes in addition to genes RAI14, S1PR5, OSBPL10, and METTL6, highlighting its prognostic potential. Future directions focus on leveraging precision medicine, novel therapeutics, and AI integration to advance personalized treatment strategies to optimize patient outcomes in HNC care.
Keywords:
Precision Medicine
; Biomarkers
; Genetic Alterations
; Head and Neck Cancer
; Targeted Therapy
1. Introduction
Head and neck cancer (HNC) is often associated with a malignancy that can be successfully treated, however it still represents a substantial global health challenge due to its high prevalence within society and its significant symptoms. Considering the distinct molecular characteristics of HNC, it is a prime subject for a comparative review. HNC ranks among the top ten cancers globally, affecting critical functions such as speech and swallowing [1]. This cancer's diverse molecular basis and clinical manifestations necessitate a comprehensive understanding at both molecular and clinical levels to help identify unique and shared pathways, allowing for improved diagnosis and clinical management through the development of targeted therapies. Through examination of this cancer potential innovations in treatment strategies, advanced personalized medicine, and improved patient outcomes can be emphasized [2,3].
The global burden of HNC is significant due to its profound impact on mortality and morbidity as essential functions such as breathing, eating, and speaking are impaired. However, the prevalence and outcomes of HNC vary significantly from region to region, influenced by differences in exposure, risk factors, and access to healthcare services [4,5].
HNC is significantly influenced by genetic predispositions and environmental factors, sharing common risk factors such as age and family history [6,7,8]. Susceptibility increases with age, and family history may indicate a genetic link that elevates risk [9]. With an aging global population, the incidence and mortality rates of both cancers are expected to rise. Symptoms commonly appear in advanced stages, complicating optimal cancer treatment and significantly reducing survival rates. This highlights the need for regular screening, heightened awareness, especially for high-risk groups, and the discovery of novel biomarkers to improve both treatment strategies and cure rates. Addressing these challenges requires comprehensive strategies, including prevention, early detection, and tailored treatments [3,10]. (Figure 1)
1.1. The Importance of Molecular Studies in Understanding Head and Neck Cancer
Molecular studies have revolutionized our understanding of HNC, revealing the intricate genetic and molecular landscapes underlying this disease. In HNC, molecular research has shown the central role of viral aetiologies, particularly human papillomavirus (HPV) and Epstein-Barr virus (EBV), in the pathogenesis of these cancers. HPV-positive oropharyngeal cancers, for example, are now recognized as distinct cancers with an improved prognosis and response to treatment compared to HPV-negative cancers. The identification of these viral markers has facilitated the development of targeted therapies and preventive vaccines, such as the HPV vaccine, which has the potential to reduce the incidence of these cancers significantly [11,12].
Molecular profiling of HNC has identified key genetic alterations, including mutations in TP53, NOTCH1, and PIK3CA and amplifications in oncogenes like epidermal growth factor receptor (EGFR). These findings have led to targeted therapies, such as EGFR inhibitors, tailored to each patient's tumour. Understanding HNC molecular pathways has improved patient stratification for personalized treatment, enhancing outcomes and reducing toxicity [13,14]. The insights gained from molecular studies have not only deepened the understanding regarding HNC biology but have also revolutionized the clinical treatment of this condition. By identifying critical genetic and molecular alterations, researchers and clinicians can improve diagnostic accuracy and personalize medicine plans based on more effective, targeted therapies, thus improving treatment outcomes. Among the essential regulators of molecular profiling in head and neck cancer, microRNAs have emerged as pivotal component, influencing gene expression and contributing to the complexity of tumour biology.
1.2. Introduction to miRNAs in Head and Neck Cancer
MicroRNAs (miRNAs) are small (18-25 nucleotides), non-coding RNA molecules that regulate gene expression post-transcriptionally. They are pivotal in various biological processes, including cell proliferation, apoptosis, metastasis, and response to therapy. In addition, the mutual characteristics of oncogenes or tumour suppressors make them invaluable for understanding cancer biology. Their potential as biomarkers for early diagnosis, prognosis, and therapeutic targets highlights their importance in precision medicine. In HNC, miRNAs have emerged as crucial regulators, influencing the molecular landscape, and provides biomarkers as potential targets for diagnosis, prognosis, and therapeutic intervention. Despite advances in treatment, the prognosis for HNC patients remains challenging due to late-stage diagnosis, high recurrence rates, and the development of resistance to conventional therapies [15]. Emphasizing the crucial role of miRNAs in cancer biology presents promising targets for therapeutic intervention. This section provides a comprehensive overview of miRNAs' roles in HNC, underscoring their significance in advancing personalized medicine and improving patient outcomes.
1.3. Introduction to miRNAs in Head and Neck Cancer
Improving diagnostic procedures for HNC involves the study of complex and varied pathways. The route to improving diagnostic procedures for HNC is challenging. For HNC, diagnosis primarily relies on physical examinations as there are no efficient and standardized screening methods, often resulting in late detection when the cancer is more advanced and difficult to treat. These diagnostic limitations have driven the research and substantiation of new biomarkers for increased accuracy and less invasive diagnostic alternatives for cancer. Understanding the molecular intersections of HNC is critical for developing personalized treatment approaches and improving patient outcomes. This review addresses the intricate details of these cancers, highlighting their global prevalence, significance, and the central role of molecular studies in deciphering their complex genetic foundation.
Key risk factors for HNC include tobacco use, alcohol consumption, and infections with oncogenic viruses such as HPV and EBV [16,17,18]. Molecular profiling has identified various genetic alterations, including mutations in tumour suppressor genes such as TP53 and PIK3CA and amplifications in oncogenes such as EGFR. These discoveries have facilitated the development of targeted therapies and improved patient stratification and treatment outcomes [11,12]. Understanding these molecular attributes are critical for developing targeted therapies and improving the precision of treatment strategies [14,19], which are expected to improve patient outcomes in HNC significantly. In HNC, the identification of viral aetiologies and genetic alterations has paved the way for targeted therapies and preventive measures such as the HPV vaccine, which has the potential to reduce cancer incidences significantly (Table 1).
2. Signature Protein/Gene in Head and Neck Cancer
2.1. Literature-Driven Insights
The importance of identifying the pivotal proteins and genes involved in this malignancy has become increasingly apparent to acquiring a greater understanding of HNC. In HNC, human papillomavirus (HPV)oncoproteins E6 and E7 play a crucial role, particularly in oropharyngeal carcinoma, by inactivating the tumour suppressor proteins p53 and retinoblastoma (Rb), respectively [11,12]. In addition, mutations in TP53, CDKN2A, and PIK3CA and amplifications in EGFR are common in HNC and drive tumorigenesis via different pathways.
Several other proteins also play a crucial role in the progression of HNC. Tissue inhibitors of metalloproteinases (TIMPs) are significantly involved in the regulation of extracellular matrix (ECM) remodelling and metastasis through their inhibitory effect on matrix metalloproteinases (MMPs) and thus play a crucial role in the tumour microenvironment [28]. Similarly, galectin-3 (Gal-3) is involved in various aspects of cancer progression, including proliferation, angiogenesis, metastasis, and immune evasion [29].
In head and neck cancer, MMP25 expression correlates with prognosis and degree of immune infiltration, particularly with CD4+ memory T cells, and is involved in oncogenic signalling pathways such as p53 signalling and PI3K/AKT/mTOR signalling. This suggests its crucial role in cancer progression and immune responses [30]. Fibronectin 1 (FN1) is significantly overexpressed in head and neck squamous cell carcinoma (HNSCC) and correlates with higher pathologic stages and poor prognosis. Its downregulation suppresses the proliferation, migration, and invasion of HNSCC cells and inhibits M2 polarization of macrophages in vitro, suggesting its role in promoting HNSCC progression and immune modulation [31]. This indicates the role of fibronectin in modulating post-transcriptional changes that lead to cancer progression [32].
TIMPs, Gal-3, MMPs, and fibronectin are integral to the dynamics of the tumour microenvironment in both head and neck cancer, influencing tumour growth, metastasis, and immune responses. These molecules can potentially serve as biomarkers for diagnosis, prognosis and targets for therapeutic intervention. Understanding their role and interactions is essential for developing personalized treatment approaches and improving treatment outcomes for this cancer (Table 2).
2.2. Database-Driven Insights
To identify datasets from HNC, a dataset search was performed in the Genome Expression Omnibus (GEO). These datasets contain gene expression data for HNC (GSE227919; GSE142083; GSE138206; GSE130605). The most significant differentially expressed genes (DEGs) were identified for HNC cancer. Further analysis identified 37 potential biomarkers for HNC, of which the top 5 DEGs were highlighted. In HNC, the most upregulated genes are MMP1 (matrix metallopeptidase 1), SERPINE1 (serpin family E member 1), PLAU (urokinase-type plasminogen activator), AURKA (Aurora kinase A), and HMGA2 (high mobility group AT-hook 2). Therefore, these genes may serve as biomarkers to distinguish patients with HNC from those without this cancer. This conclusion is supported by literature data from previous studies (Table 3).
In HNC, the molecular profile is dominated by critical proteins and genes that drive tumorigenesis, impact patient prognosis, and serve as targets for therapy. AURKA, a member of the Aurora serine/threonine kinase family, plays a role in maintaining chromosome stability and is expressed in many tissues. It is overexpressed in various tumours, including glioblastoma, cervical cancer, and HNC [42,43]. AURKA has been identified as a novel therapeutic target and predictor of overall survival (OS) in HNC [44]. High expression levels of AURKA are associated with the progression of HNC and poor prognosis, especially in HPV-negative tumours. However, AURKA is also known to be upregulated by HPV E7, which increases tumour cell proliferation. Overexpression of AURKA inhibits apoptosis by phosphorylating p73, a protein related to programmed cell death [43]. HMGA2, which belongs to the high mobility group AT-hook (HMGA) gene family, encodes a protein that regulates gene expression, cell replication, and repair. HMGA2 has been identified as an oncogene associated with cancer development when expressed at high levels [45]. Overexpression of HMGA2 is associated with processes related to the progression of HNC, such as significant invasiveness, metastasis, epithelial-mesenchymal transition, dysregulated proliferation and migration of tumour cells [45,46]. The expression of HMGA2 influences OS in HNC, with a high expression indicating a poor prognosis [46,47]. MMP1, a member of the matrix metalloproteinase family, is involved in extracellular matrix (ECM) degradation by cleaving collagen IV and gelatine [48]. MMP1 is overexpressed in HNC, and its expression correlates with T-stage (TNM classification) and cancer progression through tumour-promoting invasion [49]. PLAU, which belongs to the S1 serine peptidase of the plasminogen activator family, encodes a secreted serine protease that converts plasminogen to plasmin [49,50]. This enzyme promotes ECM degradation and facilitates tumour cell invasion and metastasis. In HNC samples, PLAU expression is upregulated and is associated with lower overall survival, poor disease-free survival, and an increased risk of developing HNC [49]. Overexpression of PLAU also leads to upregulation of MMP1. Suppression of PLAU inhibits HNC cells' proliferation, migration, and invasion capacities, while its overexpression has the opposite effect [49]. SERPINE1, a serine protease inhibitor family member, is overexpressed in HNC samples [51,52]. Overexpression of SERPINE1 is associated with the N-stage (TNM classification) and may play a role in tumour angiogenesis and metastasis. Its inhibition is associated with reduced cell proliferation and invasion [53]. SERPINE1 is also a potential prognostic biomarker, as its expression correlates with disease-free survival (DFS) in HNC [52]. Overexpression of SERPINE1 promotes resistance to radiotherapy in HNC patients [51]. These essential proteins and genes play crucial roles in the development and progression of HNC and serve as potential biomarkers for diagnosis, prognosis, and targets for therapeutic intervention. Thus, understanding their functions and interactions is essential for developing personalized treatment approaches and improving treatment outcomes in these cancers.
3. Molecular Pathways Involved in Head and Neck Cancer
As with the genetic landscape, the molecular profiles of HNC have unique features. Dysregulation of signalling pathways such as the EGFR, PI3K/AKT, and RAS-RAF-MEK pathways is critical in HNC, affecting cell cycle regulation, cellular metabolism, and apoptosis. In addition, in oropharyngeal carcinoma, HPV adds a unique viral mechanism to tumour development, mainly through the viral oncoproteins E6 and E7, which affect tumour suppressor pathways such as p53 and Rb [14,54].
Functional enrichment analysis was performed on the string platform using the DEGs identified for HNC (n=37). This analysis aimed to assess the functions of these genes and their association with HNC. The DEGs identified for HNC were associated with the cancer and several signalling pathways and molecular functions related to cancer development and progression, including ERBB and TGF-β signalling, ECM degradation, and focal adhesion. In addition, these genes have been linked to other diseases, such as gastrointestinal and pancreatic cancer and cardiovascular disorders, where they have been found expressed in tissues of the cardiovascular system. ERBB signalling includes elements of the HER family: HER1 (EGFR), HER2 (ErbB2), HER3 (ErbB3) and HER4 (ErbB4) [55,56,57]. EGFR plays an important role in signalling pathways critical to cancer progression, including Ras/Raf/MEK/ERK and PI3K/AKT/mTOR. In HNC, studies indicate that EGFR mutations significantly impact prognosis more than TP53 mutations [57,58]. Other HER family members are also involved in developing HNC and show upregulated expression in patients [57,59]. TGF-β signalling regulates epithelial-to-mesenchymal transition as well as cell differentiation and proliferation in HNC. It plays a dual role by inhibiting dysregulated cell proliferation at early stages while promoting invasion and metastasis at later stages [60].
The ECM is essential for physical interactions with cancer cells and serves as a reservoir for various ligands and growth factors that influence the tumour microenvironment. During cancer progression, focal adhesion is lost, which decreases cellular adhesion and allows cancer cells to permeate the ECM, altering its composition and organization, ultimately leading to degradation. This process is promoted by increased MMP expression in cancer [61]. After degradation of the ECM, the cancer cells enter the bloodstream, invade other tissues and metastasize [62].
As mentioned, HNC shares alterations in the PI3K/AKT/mTOR signalling pathway, highlighting its universal role in cancer progression. Targeted therapies in cancers aim to inhibit this pathway to slow tumour growth and reduce tumour survival [63]. In HNC, targeted agents against EGFR, such as cetuximab, have shown clinical benefits by exploiting abnormal activation of growth factor signalling pathways [4].
Unique to HNC is the influence of viral oncogenes in HPV-associated cancers, necessitating therapeutic strategies that target viral proteins or their effects on cellular mechanisms. Immunotherapy that harnesses the immune system's ability to recognize and destroy cancer cells has shown promise in HNC, particularly PD-1/PD-L1 inhibitors such as Pembrolizumab and Nivolumab [64]. The distinct molecular pathology of HNC emphasizes the need for cancer-specific targeted therapies that reflect their unique molecular basis [65]. Understanding these pathways helps in the development of targeted therapies and the identification of potential biomarkers for better disease management [64,65].
4. Role of Biomarkers in Head and Neck Cancer
Biomarkers are crucial for offering insights into the molecular basis of the disease and providing valuable diagnostic and prognostic information for HNC. Notable biomarkers include DNA methylation patterns, circulating microRNAs, and proteins such as EGFR and HPV oncoproteins (E6 and E7). These markers help detect and assess the cancer's aggressiveness at an early stage, enabling customized therapeutic measures [66,67,68]. Extensive studies have indicated the significant clinical potential of these biomarkers in HNC. Emerging biomarkers, including gene expression profiling in HNC, represent the next frontier in cancer diagnostics [69,70]. These novel biomarkers promise to improve the accuracy of cancer detection, prognosis, and monitoring, and additionally has the potential to revolutionize personalized medicine in oncology. Integrating biomarker testing into clinical practice is expected to significantly improve patient outcomes by enabling earlier detection, more accurate identification of disease stage, and design of optimal personalized therapeutic strategy based on individual tumour characteristics. As part of the collective effort to improve and extend the use of biomarkers in cancer detection and treatment e.g., Filippini et al. (2023) [71] present a systematic review of current data on diagnostic and prognostic molecular biomarkers for head and neck cancer of unknown primary (HNCUP). Using an electronic database and following PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines, they identified 704 articles, of which 23 studies were carefully selected for inclusion. Fourteen studies focused on diagnostic biomarkers for HNCUP, with an emphasis on HPV and EBV, as these are significantly associated with oropharyngeal and nasopharyngeal cancers, respectively [71].
The review underlines the prognostic importance of HPV, which is associated with improved disease-free treatment outcomes and overall survival rates. Currently, HPV and EBV are the only biomarkers for HNCUP used in the clinical setting. Improving molecular characterization and developing accurate tissue of origin classifiers are crucial to advance the diagnosis, accurate identification of disease stage, and treatment of HNCUP patients [71]. The ongoing development and validation of new biomarkers is imperative to improve the precision of cancer treatment, minimize overdiagnosis and overtreatment, and ultimately improve patient survival and quality of life (Table 4).
5. Functional Roles of miRNAs in Head and Neck Cancer
Many research studies have investigated miRNAs' role in HNC. Several miRNAs have been identified as crucial regulators of pathways critical to the pathogenesis of HNC. This review examines recent findings in miRNA studies of HNC and will be discussed based on their role as oncomiR and tumour suppressors.
5.1. OncomiRs in Head and Neck Cancer
As indicated, oncomiRs contribute to cancer progress by targeting tumour suppressor genes. In HNC, several oncomiRs have been identified in tumorigenesis, metastasis, and resistance to therapy [75]. MiR-21 is the first and the most studied oncomiRs in HNC. It is frequently overexpressed in HNC [76,77]. MiR-21 targets tumour suppressor genes such as PTEN/AKT, TPM1, and PDCD4 pathways in HNC [78,79]. Overexpression of miR-21 promotes cell proliferation, invasion, and resistance to apoptosis in HNC [75]. Another oncomiR involved in HNC is miR-155, which targets several genes in cell cycle regulation and apoptosis [80]. For example, the suppressor of cytokine signalling 1 (SOCS1) is one of the targetable genes that negatively regulates the JAK/STAT pathway [81]. MiR-155 elevation downregulates SOCS1 expression, increasing cell growth and cell survival, making it a potential marker for aggressive HNC [82]. Targeting miR-155 expression and overexpression of SOCS1 has a potent antitumor effect on HNC [83,84]. MiR-31 is also upregulated in HNC and plays a significant role in cancer progression, specifically in oral squamous cell carcinoma (OSCC) through regulation of gene expression, cell proliferation, cell cycle regulation, cell survival, signal transduction, and epithelial mesenchyme transition. In OSCC it targets genes such as FIH (factor-inhibiting HIF) and LATS2 (large tumour suppressor kinase 2), involved in hypoxia response and the Hippo signalling pathway, respectively [85]. MiR-31 upregulation contributes to proliferation, invasion, and angiogenesis, leading to more aggressive tumour behaviour in HNC [86]. Another group of miRNAs involved in HNC oncogenesis is the miR-221/222 cluster. These miRNAs target the cyclin-dependent kinase inhibitor p27Kip1 and the pro-apoptotic protein BMF [87]. MiR-221/222 upregulation increases cell cycle progression, reduces apoptosis, and enhances resistance to chemotherapy [88,89]. Ultimately, miR-196a is also overexpressed in HNC and promotes tumour progression, cell proliferation, migration, and invasion, leading to poor prognosis Oncogenic miR-196a directly targets annexin A1 (ANXA1), a gene involved in cell differentiation and apoptosis. ANXA1 protein and mRNA were found to be downregulated in HNC tissues. However, miR-196a functional contribution to HNC development has remained unclear [90]. OncomiRs potentially serve as biomarkers for early detection, prognosis, and monitoring treatment response in HNC [91]. OncomiRs can be targeted by antagomirs (anti-miRNAs) [92] or miRNA sponges to inhibit their oncogenic effects [93]. Clinical trials are exploring the efficacy of such approaches in various cancers, including HNC [94].
5.2. Tumor-Suppressive miRNAs in Head and Neck Cancer
As outlined earlier, tumour-suppressive miRNAs inhibit cancer development and progression by targeting oncogenes and other genes involved in cell proliferation, invasion, and survival. In HNC, several tumour-suppressive miRNAs have been identified, playing crucial roles in maintaining cellular homeostasis and preventing malignant transformation. Through analysis of recent findings, the key tumour-suppressive miRNAs in HNC have been documented. MiR-34a is a well-known tumour suppressor miRNA involved in various cancers, including HNC. It targets multiple oncogenes, such as BCL2, MET, and CDK6. MiR-34a induces apoptosis, inhibits cell proliferation, and suppresses metastasis. MiR-34a is considered a novel and highly sensitive biomarker for HNSCC diagnostic applications [75]. MiR-200c is a part of the miR-200 family, known for its role in epithelial-mesenchymal transition (EMT). It was demonstrated that miR-200c expression is significantly down-regulated in OSCC tissues compared with adjacent non-tumour tissues, suggesting that miR-200c might be a potential prognostic biomarker for OSCC [95]. It inhibits ZEB1 and ZEB2, transcription factors that promote EMT and metastasis, thereby reducing invasion and metastasis [96]. MiR-200c-3p is another member of the miR-200 family shown to have a significantly downregulated expression in HNC tissues. In HNC cells, ectopic miR-200c-3p expression inhibits viability, clonogenicity, migration, and invasion [97]. Additionally, miR-375 is highly downregulated in HNC and functions as a tumour suppressor. It targets genes involved in cell cycle regulation, such as insulin-like growth factor 1 receptor (IGF-1R). MiR-375 upregulation inhibits growth and induces cell cycle arrest in G0/G1 phase significantly. It enhances apoptosis and radiosensitivity in HNC [98]. Reduced levels of miR-375 are associated with aggressive tumour behaviour and poor clinical outcomes [99]. MiR-145 is another tumour-suppressive miRNA that is significantly downregulated in HNC. MiR-145 is involved in the p53 signalling pathway. Downregulation of miR-145-5p oncogenes like FSCN1 (fascin actin-bundling protein 1) protein level or SOX2, causing migration, invasion, tumour growth and EMT. Its minimal expression is correlated with advanced disease stages and poor survival rates [80]. Tumour-suppressive miRNAs can serve as biomarkers for early detection, prognosis, and monitoring response to HNC therapy. It could inhibit tumour growth and progression using miRNA or gene therapy approaches. Combining miRNA-based therapies with conventional chemotherapy and radiotherapy may change therapeutic outcomes and overcome resistances [100]. MicroRNAs' unique expression profiles and functional roles make them valuable as diagnostic biomarkers and therapeutic targets for HNC. Further research into these miRNAs' specific mechanisms and interactions in HNC will be essential for developing effective miRNA-based therapies and improving patient outcomes (Figure 2).
5.3. In Silico Validation of miRNAs in Head and Neck Cancer
To validate miRNAs, the OncoMir database (https://oncomir.org/) was utilized. This validation revealed that among the oncomiRs, hsa-miR-21-5p, hsa-miR-31-5p, hsa-miR-221-3p, hsa-miR-222-3p, hsa-miR-196a-5p, and hsa-miR-200c-3p were linked to tumorigenesis in HNSC (Table 5). For tumour-suppressive miRNAs, hsa-miR-375 and hsa-miR-145-5p were also associated with HNSC tumorigenesis (Table 6). Notably, hsa-miR-155-3p was the only miRNA significantly related to survival outcomes in HNSC (Table 7). Additionally, a strong correlation was observed between hsa-miR-155-3p and the genes RAI14, S1PR5, OSBPL10, and METTL6 (Table 8).
6. Recent Studies Profiling miRNA Expression in Head and Neck Cancer Using High-throughput Technologies
Several recent studies have applied high-throughput technologies to profile miRNA expression in HNC. These technologies are advanced and evaluate the comprehensive and large-scale analysis of miRNA molecules. Using these technologies, the roles of miRNAs have been revealed in cancer development, progression, and their potential therapeutic applications. Some of the key high-throughput technologies for miRNA profiling are Next-Generation Sequencing (NGS), RNA-Seq (Total RNA Sequencing), Microarrays, Quantitative Real-Time PCR (qRT-PCR), Digital PCR (dPCR), NanoString nCounter Analysis and Microfluidics-based Platforms. The following are selected examples of recent achievements in finding key miRNAs in HNC using the aforementioned methods. In 2017, Ganci et all., identified 35 miRNAs deregulated in both tumour and peri-tumoral tissues in head and neck squamous cell carcinoma patients using microarray hybridization, reverse transcription of miRNAs and qPCR. This identification of predictive miRNA signature would be crucial for early detection, following up, and treatment strategy for the head and neck squamous cell carcinoma patients [101]. In 2023, three-miRNA panel has identified the potential for the diagnosis of HNSCC from the patients’ plasma. As this research indicates, miR-95-3p and miR-579-5p expression upregulated, and miR-1298-3p downregulated in the plasma of HNSCC patients significantly. This investigation shows a convenient diagnostic and screening tool for head and neck cancer early detection [102]. Another method is dPCR which assists patients with cancer of unknown primary site (CUP). Laprovitera et al., predicted the primary site of 53 CUPs using a molecular assay, based on digital miRNA profiling. Furthermore, HNC with metastases of known origin was assessed in this study and the unknown sites were identified in the CUP patients using dPCR. High-throughput technologies have revolutionized miRNA profiling in HNC. These methods provide comprehensive, sensitive, and quantitative data that are essential for understanding miRNA roles in cancer and developing diagnostic and therapeutic strategies [103]. Each technology has its unique advantages, and the choice of method depends on the specific research question, available resources, and the desired resolution of the miRNA profiling. These unique methodologies have identified numerous miRNAs expressed in various HNC subtypes providing sensitive and precise miRNA profiling for improvement of HNC diagnostic and therapeutic approaches.
Despite all these advancements, HNC is still diagnosed at advanced stages in many cases, generating limited improvements in survival rates. The improvement of miRNA therapeutics in HNC faces several limitations such as: contradictions in study results, miRNAs specificity issues, limited understanding of tumour microenvironment (TME), heterogeneity in molecular subtypes of HNC, lack of effective biomarkers for early detection, resistance of miRNAs to radio and chemo-therapies, HPV-positive vs. HPV-negative HNC, detection and prognostic challenges of miRNAs and epidemiological study limitations [104]. These limitations highlight the need for further research to improve the specificity and reliability of miRNA-based diagnostics and therapeutics in HNC. However, there are several promising fields that the future of profiling miRNA in HNC can be focused on. Investigating the miRNA profiles specific to different anatomical sites of HNC (miRNA signature) is a promising approach that can help identify unique biomarkers and therapeutic targets [105]. In addition, detecting miRNA through liquid biopsies, such as saliva or blood samples is a non-invasive diagnostic and prognostic tools for HNC, potentially allowing for early detection and monitoring of treatment response in HNC [106,107]. Optimization of delivery mechanisms and the stability of miRNA therapeutics are paramount in the progress of wide application of miRNAs in HNC [107]. Moreover, integrating miRNA profiling with comprehensive genomic and transcriptomic data will provide insights into the molecular mechanisms driving HNC. Ultimately, immunotherapy is a very promising approach for the future of HNC treatment. Studying how miRNAs interact with the immune system in HNC and identifying miRNAs that enhance immune response or serve as biomarkers for immunotherapy are fundamental in shaping the future of miRNA therapeutics research in HNC [106].
In summary, research into miRNA profiling in head and neck cancer offers exciting opportunities to improve diagnosis and treatments. By focusing on specific miRNA profiles, integrating with genomic data, and exploring non-invasive diagnostic methods, uncovering new insights and therapeutic targets will be possible. All these efforts ultimately serve enhancing patient care and outcomes.
7. Future Perspectives
Precision medicine in HNC detection and treatment focuses on tailoring treatment to individual genetic profiles. In HNC, identifying specific genetic mutations and viral associations, particularly with HPV, has led to the development of targeted therapies and vaccines designed to improve patient outcomes. For example, the presence of HPV in oropharyngeal cancer has been associated with a better prognosis and response to certain therapies. Targeted treatments, such as those directed against the epidermal growth factor receptor (EGFR), and the use of HPV vaccines are key advances in the precision medicine approach to HNC [10].
The future of precision medicine lies in further integrating genomic, transcriptomic, metabolomic, and proteomic data to enable personalized treatment approaches [108,109]. Combining these different data types allows clinicians to develop more effective, individualized treatment plans that improve patient outcomes and reduce adverse effects. In HNC, research has focused on targeting EGFR with monoclonal antibodies such as cetuximab and exploring the therapeutic potential of inhibiting the PI3K/AKT/mTOR signalling pathway. These signalling pathways are critical for regulating cell growth, survival, and proliferation, and their dysregulation is a hallmark of many cancers. In addition, immunotherapy based on checkpoint inhibitors, such as pembrolizumab and nivolumab, is increasingly recognized as a potential treatment strategy in HNC. These therapies use the patient’s immune system to recognize and destroy cancer cells, offering a new avenue for treatment, especially in cases where conventional therapies have failed [14,110].
Laboratory studies and computer-based data analyses are at the forefront of revolutionizing cancer research and the treatment of HNC. Through use of artificial intelligence (AI) and machine learning (ML) analysis of large data sets can potentially discover new biomarkers, predict treatment outcomes, and personalize treatment plans. These technologies can process and interpret vast amounts of genomic and clinical data, identifying patterns and correlations that may not be apparent using traditional methods. Big data analytics enable the integration of different data types and provide comprehensive insights into cancer biology and treatment responses [111]. In addition, developing digital health tools and wearable technologies for real-time patient monitoring offers new opportunities to improve quality of life and treatment adherence. These tools can track vital signs, medication adherence, and symptom progression, enabling timely interventions and adjustments to treatment plans. Integrating these technologies into clinical practice is expected to accelerate the pace of discoveries in cancer research and change the perspective of cancer care so that treatments become more personalized and responsive to individual patient needs [112].
The future of HNC research and treatment is poised for significant advances through precision medicine, new therapeutic targets, and the integration of technology and data science. These developments promise to improve patient outcomes, personalize cancer treatment, and ultimately change the approach to treating these complex diseases. The continued evolution of precision medicine, driven by genomic, transcriptomic, metabolomic, and proteomic insights, will likely lead to more targeted and effective treatments. The discovery and validation of novel therapeutic targets will expand the arsenal of available treatments. At the same time, advances in AI, ML, and digital health technologies will improve the precision and personalization of cancer care. Integrating these innovative approaches will be instrumental in minimizing overdiagnosis and overtreatment, improving survival rates, and enhancing quality of life for patients with HNC. Collaboration between researchers, clinicians, and technicians will be crucial in realizing the full potential of these advancements and ensuring that each patient receives the most effective and personalized therapy.
8. Conclusions
This review has revealed substantial advancements in deciphering the molecular complexities of HNC. It emphasizes the central role of biomarkers and genetic alterations in the diagnosis and prognosis of these malignancies. Advances in precision medicine, new therapeutic targets, and the integration of technology and data science will revolutionize the treatment strategies for HNC. Identifying specific biomarkers and genetic signatures has not only improved diagnostic accuracy but also facilitated the development of targeted therapeutic interventions. This gives hope for personalized treatment strategies to improve patient outcomes while minimizing toxicity.
The molecular understanding of HNC has contributed significantly to cancer therapy development. By deciphering the genetic and epigenetic changes underlying these cancers, researchers have identified key pathways and targets for intervention. These molecular insights are crucial for developing more effective, less harmful treatments and overcoming resistance to current therapies. They mark the transition from a one-size-fits-all approach to a more nuanced, patient-specific strategy in cancer treatment and emphasizes the need for comprehensive molecular diagnosis as the cornerstone of effective cancer management. Considering these advances, there is a critical need for continued research and collaboration within the oncology community. Multidisciplinary efforts that combine the expertise of molecular biologists, clinicians, data scientists, and patient advocates are essential to further unravel the complexities of HNC. Such collaborative efforts will not only accelerate the discovery of new biomarkers and therapeutic targets, but also ensure the rapid translation of these findings into clinical practice, ultimately improving patient care. These collective efforts are vital to overcoming the remaining challenges in the treatment of HNC, including drug resistance, metastasis and recurrence. The oncology community is therefore called upon to foster an environment of innovation, collaboration, and shared knowledge with the ultimate goal of defeating these formidable diseases. Although significant progress has been made in the molecular characterization and treatment of HNC, the path forward requires sustained research, innovation, and collaboration. As we continue to explore the molecular basis of these cancers, the oncology community can look forward to a future where cancer treatment is not only effective but also personalized, transforming the prognosis for patients worldwide. Advances in precision medicine, the exploration of novel therapeutic targets, the integration of cutting-edge technology, and data science will collectively drive this transformation and ensure that each patient receives the most effective and personalized care and treatment.
Authors contributions
Conceptualization: RV, SG; Writing – original draft preparation: SV, ABB, MJL, JM, RWRV; Formal analysis and investigation: RV, AF, AE, SG; Writing – review and editing: MJ, RV, AF, SG, RW.
Acknowledgments
This work was supported within the scope of the national funds through FCT - Portuguese Foundation for Science and Technology, under by iBiMED (UIDB/04501/2020 and POCI-01-0145-FEDER-007628), and by Cardiovascular R&D Center – UnIC (UIDB/00051/2020 and UIDP/00051/2020) (RV) and Grant number: BNW-1-044/K/3/B (JM).
Conflicts of Interest
The authors declare no conflict of interest.
Informed Consent Statement
Not applicable.
Institutional Review Board Statement
Not applicable.
Data Availability Statement
Not applicable.
References
- Mody, M.D.; Rocco, J.W.; Yom, S.S.; Haddad, R.I.; Saba, N.F. Head and neck cancer. Lancet 2021, 398, 2289–2299. [Google Scholar] [CrossRef]
- Rawla, P. Epidemiology of Prostate Cancer. World J Oncol 2019, 10, 63–89. [Google Scholar] [CrossRef]
- Rebello, R.J.; Oing, C.; Knudsen, K.E.; Loeb, S.; Johnson, D.C.; Reiter, R.E.; Gillessen, S.; Van der Kwast, T.; Bristow, R.G. Prostate cancer. Nature reviews. Disease primers 2021, 7, 9. [CrossRef]
- Guo, K.; Xiao, W.; Chen, X.; Zhao, Z.; Lin, Y.; Chen, G. Epidemiological Trends of Head and Neck Cancer: A Population-Based Study. BioMed research international 2021, 2021, 1738932. [Google Scholar] [CrossRef]
- Cohen, N.; Fedewa, S.; Chen, A.Y. Epidemiology and Demographics of the Head and Neck Cancer Population. Oral Maxillofac Surg Clin North Am 2018, 30, 381–395. [Google Scholar] [CrossRef]
- Chulam, T.C.; Bertonha, F.B.; Villacis, R.A.R.; Filho, J.G.; Kowalski, L.P.; Rogatto, S.R. Epidemiological, Clinical, and Genomic Profile in Head and Neck Cancer Patients and Their Families. Biomedicines 2022, 10. [Google Scholar] [CrossRef]
- Hopkins, J.; Cescon, D.W.; Tse, D.; Bradbury, P.; Xu, W.; Ma, C.; Wheatley-Price, P.; Waldron, J.; Goldstein, D.; Meyer, F.; et al. Genetic polymorphisms and head and neck cancer outcomes: a review. Cancer epidemiology, biomarkers & prevention : a publication of the American Association for Cancer Research, cosponsored by the American Society of Preventive Oncology 2008, 17, 490–499. [Google Scholar] [CrossRef]
- Ferraguti, G.; Terracina, S.; Petrella, C.; Greco, A.; Minni, A.; Lucarelli, M.; Agostinelli, E.; Ralli, M.; de Vincentiis, M.; Raponi, G.; et al. Alcohol and Head and Neck Cancer: Updates on the Role of Oxidative Stress, Genetic, Epigenetics, Oral Microbiota, Antioxidants, and Alkylating Agents. Antioxidants (Basel, Switzerland) 2022, 11. [CrossRef]
- Pilleron, S.; Sarfati, D.; Janssen-Heijnen, M.; Vignat, J.; Ferlay, J.; Bray, F.; Soerjomataram, I. Global cancer incidence in older adults, 2012 and 2035: A population-based study. International journal of cancer 2019, 144, 49–58. [Google Scholar] [CrossRef]
- Leemans, C.R.; Snijders, P.J.F.; Brakenhoff, R.H. The molecular landscape of head and neck cancer. Nat Rev Cancer 2018, 18, 269–282. [Google Scholar] [CrossRef]
- Mirza, A.H.; Thomas, G.; Ottensmeier, C.H.; King, E.V. Importance of the immune system in head and neck cancer. Head & neck 2019, 41, 2789–2800. [Google Scholar] [CrossRef]
- Schoenfeld, J.D. Immunity in head and neck cancer. Cancer immunology research 2015, 3, 12–17. [Google Scholar] [CrossRef]
- Jiang, X.; Ye, J.; Dong, Z.; Hu, S.; Xiao, M. Novel genetic alterations and their impact on target therapy response in head and neck squamous cell carcinoma. Cancer management and research 2019, 11, 1321–1336. [Google Scholar] [CrossRef]
- Arora, K.; Barbieri, C.E. Molecular Subtypes of Prostate Cancer. Curr Oncol Rep 2018, 20, 58. [Google Scholar] [CrossRef]
- Kowalski, L.P.; Coletta, R.D.; Salo, T.; Maschietto, M.; Chojniak, R.; Lima, J.M.; Mlynarek, A.; Hier, M.P.; Alaoui-Jamali, M.A.; Silva, S.D. Head and neck cancer: Emerging concepts in biomarker discovery and opportunities for clinical translation. Clin Transl Med 2020, 10, e209. [Google Scholar] [CrossRef]
- Kumar, R.; Rai, A.K.; Das, D.; Das, R.; Kumar, R.S.; Sarma, A.; Sharma, S.; Kataki, A.C.; Ramteke, A. Alcohol and Tobacco Increases Risk of High Risk HPV Infection in Head and Neck Cancer Patients: Study from North-East Region of India. PloS one 2015, 10, e0140700. [Google Scholar] [CrossRef]
- Singhania, N.; Mishra, A. Alcohol Consumption, Tobacco Use, and Viral Infections: A Multifactorial Approach to Understanding Head and Neck Cancer Risk. International Journal of Applied Health Care Analytics 2024, 9, 44–57. [Google Scholar]
- Smith, E.M.; Rubenstein, L.M.; Haugen, T.H.; Hamsikova, E.; Turek, L.P. Tobacco and alcohol use increases the risk of both HPV-associated and HPV-independent head and neck cancers. Cancer Causes Control 2010, 21, 1369–1378. [Google Scholar] [CrossRef]
- The Molecular Taxonomy of Primary Prostate Cancer. Cell 2015, 163, 1011–1025. [CrossRef]
- Soares, P.C.; Abdelhay, E.S.; Thuler, L.C.S.; Soares, B.M.; Demachki, S.; Ferro, G.V.R.; Assumpção, P.P.; Lamarão, L.M.; Ribeiro Pinto, L.F.; Burbano, R.M.R. HPV positive, wild type TP53, and p16 overexpression correlate with the absence of residual tumors after chemoradiotherapy in anal squamous cell carcinoma. BMC Gastroenterol 2018, 18, 30. [Google Scholar] [CrossRef]
- Levva, S.; Kotoula, V.; Kostopoulos, I.; Manousou, K.; Papadimitriou, C.; Papadopoulou, K.; Lakis, S.; Koukoulias, K.; Karavasilis, V.; Pentheroudakis, G.; et al. Prognostic Evaluation of Epidermal Growth Factor Receptor (EGFR) Genotype and Phenotype Parameters in Triple-negative Breast Cancers. Cancer genomics & proteomics 2017, 14, 181–195. [Google Scholar] [CrossRef]
- Jørgensen, C.L.T.; Forsare, C.; Bendahl, P.O.; Falck, A.K.; Fernö, M.; Lövgren, K.; Aaltonen, K.; Rydén, L. Expression of epithelial-mesenchymal transition-related markers and phenotypes during breast cancer progression. Breast cancer research and treatment 2020, 181, 369–381. [Google Scholar] [CrossRef]
- Das, T.; Zhong, R.; Spiotto, M.T. Notch Signaling and Human Papillomavirus-Associated Oral Tumorigenesis. Advances in experimental medicine and biology 2021, 1287, 105–122. [Google Scholar] [CrossRef] [PubMed]
- Montalto, F.I.; De Amicis, F. Cyclin D1 in Cancer: A Molecular Connection for Cell Cycle Control, Adhesion and Invasion in Tumor and Stroma. Cells 2020, 9. [Google Scholar] [CrossRef]
- Tang, Q.; Chen, Y.; Li, X.; Long, S.; Shi, Y.; Yu, Y.; Wu, W.; Han, L.; Wang, S. The role of PD-1/PD-L1 and application of immune-checkpoint inhibitors in human cancers. Frontiers in Immunology 2022, 13. [Google Scholar] [CrossRef]
- Akanji, M.A.; Rotimi, D.; Adeyemi, O.S. Hypoxia-Inducible Factors as an Alternative Source of Treatment Strategy for Cancer. Oxid Med Cell Longev 2019, 2019, 8547846. [Google Scholar] [CrossRef] [PubMed]
- Burns, J.S.; Manda, G. Metabolic Pathways of the Warburg Effect in Health and Disease: Perspectives of Choice, Chain or Chance. International journal of molecular sciences 2017, 18. [Google Scholar] [CrossRef]
- Groblewska, M.; Siewko, M.; Mroczko, B.; Szmitkowski, M. The role of matrix metalloproteinases (MMPs) and their inhibitors (TIMPs) in the development of esophageal cancer. Folia Histochem Cytobiol 2012, 50, 12–19. [Google Scholar]
- Méndez-Huergo, S.P.; Blidner, A.G.; Rabinovich, G.A. Galectins: emerging regulatory checkpoints linking tumor immunity and angiogenesis. Curr Opin Immunol 2017, 45, 8–15. [Google Scholar] [CrossRef]
- Liang, Y.; Guan, C.; Li, K.; Zheng, G.; Wang, T.; Zhang, S.; Liao, G. MMP25 Regulates Immune Infiltration Level and Survival Outcome in Head and Neck Cancer Patients. Frontiers in oncology 2020, 10, 1088. [Google Scholar] [CrossRef]
- Zhou, W.H.; Du, W.D.; Li, Y.F.; Al-Aroomi, M.A.; Yan, C.; Wang, Y.; Zhang, Z.Y.; Liu, F.Y.; Sun, C.F. The Overexpression of Fibronectin 1 Promotes Cancer Progression and Associated with M2 Macrophages Polarization in Head and Neck Squamous Cell Carcinoma Patients. Int J Gen Med 2022, 15, 5027–5042. [Google Scholar] [CrossRef]
- Martinucci, B.; Cucielo, M.S.; Minatel, B.C.; Cury, S.S.; Caxali, G.H.; Aal, M.C.E.; Felisbino, S.L.; Pinhal, D.; Carvalho, R.F.; Delella, F.K. Fibronectin Modulates the Expression of miRNAs in Prostate Cancer Cell Lines. Front Vet Sci 2022, 9, 879997. [Google Scholar] [CrossRef]
- Cosper, P.F.; Bradley, S.; Luo, L.; Kimple, R.J. Biology of HPV Mediated Carcinogenesis and Tumor Progression. Semin Radiat Oncol 2021, 31, 265–273. [Google Scholar] [CrossRef] [PubMed]
- Byeon, H.K.; Ku, M.; Yang, J. Beyond EGFR inhibition: multilateral combat strategies to stop the progression of head and neck cancer. Exp Mol Med 2019, 51, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Zhang, T.; Su, W.; Dou, Z.; Zhao, D.; Jin, X.; Lei, H.; Wang, J.; Xie, X.; Cheng, B.; et al. Mutant p53 in cancer: from molecular mechanism to therapeutic modulation. Cell death & disease 2022, 13, 974. [Google Scholar] [CrossRef]
- Chen, Z.; Guo, Y.; Zhao, D.; Zou, Q.; Yu, F.; Zhang, L.; Xu, L. Comprehensive Analysis Revealed that CDKN2A is a Biomarker for Immune Infiltrates in Multiple Cancers. Frontiers in cell and developmental biology 2021, 9, 808208. [Google Scholar] [CrossRef]
- Sirico, M.; D'Angelo, A.; Gianni, C.; Casadei, C.; Merloni, F.; De Giorgi, U. Current State and Future Challenges for PI3K Inhibitors in Cancer Therapy. Cancers 2023, 15. [Google Scholar] [CrossRef]
- Cabral-Pacheco, G.A.; Garza-Veloz, I.; Castruita-De la Rosa, C.; Ramirez-Acuña, J.M.; Perez-Romero, B.A.; Guerrero-Rodriguez, J.F.; Martinez-Avila, N.; Martinez-Fierro, M.L. The Roles of Matrix Metalloproteinases and Their Inhibitors in Human Diseases. International journal of molecular sciences 2020, 21. [Google Scholar] [CrossRef]
- Farhad, M.; Rolig, A.S.; Redmond, W.L. The role of Galectin-3 in modulating tumor growth and immunosuppression within the tumor microenvironment. Oncoimmunology 2018, 7, e1434467. [Google Scholar] [CrossRef]
- Gonzalez-Avila, G.; Sommer, B.; Mendoza-Posada, D.A.; Ramos, C.; Garcia-Hernandez, A.A.; Falfan-Valencia, R. Matrix metalloproteinases participation in the metastatic process and their diagnostic and therapeutic applications in cancer. Critical Reviews in Oncology/Hematology 2019, 137, 57–83. [Google Scholar] [CrossRef]
- Wu, J.-L.; Xu, C.-F.; Yang, X.-H.; Wang, M.-S. Fibronectin promotes tumor progression through integrin αvβ3/PI3K/AKT/SOX2 signaling in non-small cell lung cancer. Heliyon 2023, 9, e20185. [Google Scholar] [CrossRef]
- Huang, C.; Chen, L.; Zhang, Y.; Wang, L.; Zheng, W.; Peng, F.; Xu, Y. Predicting AURKA as a novel therapeutic target for NPC: A comprehensive analysis based on bioinformatics and validation. Frontiers in genetics 2022, 13, 926546. [Google Scholar] [CrossRef]
- Shaikh, M.H.; Idris, A.; Johnson, N.W.; Fallaha, S.; Clarke, D.T.W.; Martin, D.; Morgan, I.M.; Gabrielli, B.; McMillan, N.A.J. Aurora kinases are a novel therapeutic target for HPV-positive head and neck cancers. Oral oncology 2018, 86, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Ren, X.; Song, L.J.; Zhang, M.; Zhang, W.; Lin, K.; He, H. Identification of Prognostic Markers for Head and NeckSquamous Cell Carcinoma Based on Glycolysis-Related Genes. Evid Based Complement Alternat Med 2022, 2022, 2762595. [Google Scholar] [CrossRef] [PubMed]
- Binabaj, M.M.; Soleimani, A.; Rahmani, F.; Avan, A.; Khazaei, M.; Fiuji, H.; Soleimanpour, S.; Ryzhikov, M.; Ferns, G.A.; Bahrami, A.; et al. Prognostic value of high mobility group protein A2 (HMGA2) over-expression in cancer progression. Gene 2019, 706, 131–139. [Google Scholar] [CrossRef]
- Okano, L.M.; Fonseca, L.; Erthal, I.D.; Malta, T.M. Epigenomic integrative analysis pinpoint master regulator transcription factors associated with tumorigenesis in squamous cell carcinoma of oral tongue. Genet Mol Biol 2023, 46, e20220358. [Google Scholar] [CrossRef]
- Alajez, N.M.; Shi, W.; Wong, D.; Lenarduzzi, M.; Waldron, J.; Weinreb, I.; Liu, F.F. Lin28b promotes head and neck cancer progression via modulation of the insulin-like growth factor survival pathway. Oncotarget 2012, 3, 1641–1652. [Google Scholar] [CrossRef]
- Reis, S.T.; Antunes, A.A.; Pontes-Junior, J.; Sousa-Canavez, J.M.; Dall'Oglio, M.F.; Piantino, C.B.; Cruz, J.A.; Morais, D.R.; Srougi, M.; Leite, K.R. Underexpression of MMP-2 and its regulators, TIMP2, MT1-MMP and IL-8, is associated with prostate cancer. Int Braz J Urol 2012, 38, 167–174. [Google Scholar] [CrossRef]
- Wu, K.; Mao, Y.Y.; Han, N.N.; Wu, H.; Zhang, S. PLAU1 Facilitated Proliferation, Invasion, and Metastasis via Interaction With MMP1 in Head and Neck Squamous Carcinoma. Frontiers in oncology 2021, 11, 574260. [Google Scholar] [CrossRef]
- Cui, X.; Sun, H.; Liu, X.; Bai, Y.; Bai, Y.; Cui, Y.; Wang, B.; Zhang, S.; Li, X. PLAU promotes cell proliferation and migration of head and neck cancer via STAT3 signaling pathway. Experimental cell research 2024, 438, 114056. [Google Scholar] [CrossRef]
- Barbosa, S.; Laureano, N.K.; Hadiwikarta, W.W.; Visioli, F.; Bonrouhi, M.; Pajdzik, K.; Conde-Lopez, C.; Herold-Mende, C.; Eidt, G.; Langie, R.; et al. The Role of SOX2 and SOX9 in Radioresistance and Tumor Recurrence. Cancers 2024, 16. [Google Scholar] [CrossRef]
- Doescher, J.; von Witzleben, A.; Boukas, K.; Weissinger, S.E.; Thomas, G.J.; Laban, S.; Thomas, J.; Hoffmann, T.K.; Ottensmeier, C.H. Changes in Gene Expression Patterns in the Tumor Microenvironment of Head and Neck Squamous Cell Carcinoma Under Chemoradiotherapy Depend on Response. Frontiers in oncology 2022, 12, 862694. [Google Scholar] [CrossRef]
- Guo, X.; Sun, Z.; Chen, H.; Ling, J.; Zhao, H.; Chang, A.; Zhuo, X. SERPINE1 as an Independent Prognostic Marker and Therapeutic Target for Nicotine-Related Oral Carcinoma. Clinical and experimental otorhinolaryngology 2023, 16, 75–86. [Google Scholar] [CrossRef]
- Jou, A.; Hess, J. Epidemiology and Molecular Biology of Head and Neck Cancer. Oncol Res Treat 2017, 40, 328–332. [Google Scholar] [CrossRef]
- Roskoski, R., Jr. The ErbB/HER family of protein-tyrosine kinases and cancer. Pharmacological research 2014, 79, 34–74. [Google Scholar] [CrossRef]
- El-Gamal, M.I.; Mewafi, N.H.; Abdelmotteleb, N.E.; Emara, M.A.; Tarazi, H.; Sbenati, R.M.; Madkour, M.M.; Zaraei, S.O.; Shahin, A.I.; Anbar, H.S. A Review of HER4 (ErbB4) Kinase, Its Impact on Cancer, and Its Inhibitors. Molecules 2021, 26. [Google Scholar] [CrossRef]
- Zhang, J.; Saba, N.F.; Chen, G.Z.; Shin, D.M. Targeting HER (ERBB) signaling in head and neck cancer: An essential update. Mol Aspects Med 2015, 45, 74–86. [Google Scholar] [CrossRef]
- Etienne, M.C.; Pivot, X.; Formento, J.L.; Bensadoun, R.J.; Formento, P.; Dassonville, O.; Francoual, M.; Poissonnet, G.; Fontana, X.; Schneider, M.; et al. A multifactorial approach including tumoural epidermal growth factor receptor, p53, thymidylate synthase and dihydropyrimidine dehydrogenase to predict treatment outcome in head and neck cancer patients receiving 5-fluorouracil. British journal of cancer 1999, 79, 1864–1869. [Google Scholar] [CrossRef]
- Pollock, N.I.; Grandis, J.R. HER2 as a therapeutic target in head and neck squamous cell carcinoma. Clinical cancer research : an official journal of the American Association for Cancer Research 2015, 21, 526–533. [Google Scholar] [CrossRef]
- Mehra, R.; Serebriiskii, I.G.; Dunbrack, R.L., Jr.; Robinson, M.K.; Burtness, B.; Golemis, E.A. Protein-intrinsic and signaling network-based sources of resistance to EGFR- and ErbB family-targeted therapies in head and neck cancer. Drug Resist Updat 2011, 14, 260–279. [Google Scholar] [CrossRef]
- Pereira, A.L.; Veras, S.S.; Silveira, E.J.; Seabra, F.R.; Pinto, L.P.; Souza, L.B.; Freitas, R.A. The role of matrix extracellular proteins and metalloproteinases in head and neck carcinomas: an updated review. Braz J Otorhinolaryngol 2005, 71, 81–86. [Google Scholar] [CrossRef]
- Rao, V.U.; Arakeri, G.; Subash, A.; Bagadia, R.K.; Thakur, S.; Kudpaje, A.S.; Nayar, R.; Patil, S.; Paiva Fonseca, F.; Gomez, R.S.; et al. Circulating tumour cells in head and neck cancers: Biological insights. Journal of oral pathology & medicine : official publication of the International Association of Oral Pathologists and the American Academy of Oral Pathology 2020, 49, 842–848. [Google Scholar] [CrossRef]
- Weiss, F.; Lauffenburger, D.; Friedl, P. Towards targeting of shared mechanisms of cancer metastasis and therapy resistance. Nature reviews. Cancer 2022, 22, 157–173. [Google Scholar] [CrossRef]
- Nisa, L.; Barras, D.; Medová, M.; Aebersold, D.M.; Medo, M.; Poliaková, M.; Koch, J.; Bojaxhiu, B.; Eliçin, O.; Dettmer, M.S.; et al. Comprehensive Genomic Profiling of Patient-matched Head and Neck Cancer Cells: A Preclinical Pipeline for Metastatic and Recurrent Disease. Molecular cancer research : MCR 2018, 16, 1912–1926. [Google Scholar] [CrossRef]
- Lozano, R.; Castro, E.; Aragón, I.M.; Cendón, Y.; Cattrini, C.; López-Casas, P.P.; Olmos, D. Genetic aberrations in DNA repair pathways: a cornerstone of precision oncology in prostate cancer. British journal of cancer 2021, 124, 552–563. [Google Scholar] [CrossRef]
- Konings, H.; Stappers, S.; Geens, M.; De Winter, B.Y.; Lamote, K.; van Meerbeeck, J.P.; Specenier, P.; Vanderveken, O.M.; Ledeganck, K.J. A Literature Review of the Potential Diagnostic Biomarkers of Head and Neck Neoplasms. Frontiers in oncology 2020, 10, 1020. [Google Scholar] [CrossRef]
- Mishra, V.; Singh, A.; Chen, X.; Rosenberg, A.J.; Pearson, A.T.; Zhavoronkov, A.; Savage, P.A.; Lingen, M.W.; Agrawal, N.; Izumchenko, E. Application of liquid biopsy as multi-functional biomarkers in head and neck cancer. British journal of cancer 2022, 126, 361–370. [Google Scholar] [CrossRef]
- Rapado-González, Ó.; Martínez-Reglero, C.; Salgado-Barreira, Á.; Muinelo-Romay, L.; Muinelo-Lorenzo, J.; López-López, R.; Díaz-Lagares, Á.; Suárez-Cunqueiro, M.M. Salivary DNA Methylation as an Epigenetic Biomarker for Head and Neck Cancer. Part I: A Diagnostic Accuracy Meta-Analysis. Journal of personalized medicine 2021, 11. [CrossRef]
- Patel, A.; Patel, S.; Patel, P.; Tanavde, V. Saliva Based Liquid Biopsies in Head and Neck Cancer: How Far Are We From the Clinic? Frontiers in oncology 2022, 12, 828434. [Google Scholar] [CrossRef]
- Gattuso, G.; Crimi, S.; Lavoro, A.; Rizzo, R.; Musumarra, G.; Gallo, S.; Facciponte, F.; Paratore, S.; Russo, A.; Bordonaro, R.; et al. Liquid Biopsy and Circulating Biomarkers for the Diagnosis of Precancerous and Cancerous Oral Lesions. Noncoding RNA 2022, 8. [Google Scholar] [CrossRef]
- Filippini, D.M.; Broseghini, E.; Carosi, F.; Molin, D.D.; Riefolo, M.; Fabbri, L.; Abeshi, A.; Fernandez, I.J.; Ferracin, M. A Systematic Review of Diagnostic and Prognostic Biomarkers for Head and Neck Cancer of Unknown Primary: An Unmet Clinical Need. Diagnostics (Basel, Switzerland) 2023, 13. [CrossRef]
- Lechner, M.; Liu, J.; Masterson, L.; Fenton, T.R. HPV-associated oropharyngeal cancer: epidemiology, molecular biology and clinical management. Nat Rev Clin Oncol 2022, 19, 306–327. [Google Scholar] [CrossRef]
- Halder, S.; Basu, S.; Lall, S.P.; Ganti, A.K.; Batra, S.K.; Seshacharyulu, P. Targeting the EGFR signaling pathway in cancer therapy: What's new in 2023? Expert Opin Ther Targets 2023, 27, 305–324. [Google Scholar] [CrossRef]
- Krsek, A.; Baticic, L.; Sotosek, V.; Braut, T. The Role of Biomarkers in HPV-Positive Head and Neck Squamous Cell Carcinoma: Towards Precision Medicine. Diagnostics 2024, 14, 1448. [Google Scholar] [CrossRef]
- Thomaidou, A.C.; Batsaki, P.; Adamaki, M.; Goulielmaki, M.; Baxevanis, C.N.; Zoumpourlis, V.; Fortis, S.P. Promising Biomarkers in Head and Neck Cancer: The Most Clinically Important miRNAs. Int J Mol Sci 2022, 23. [Google Scholar] [CrossRef]
- Chang, S.S.; Jiang, W.W.; Smith, I.; Poeta, L.M.; Begum, S.; Glazer, C.; Shan, S.; Westra, W.; Sidransky, D.; Califano, J.A. MicroRNA alterations in head and neck squamous cell carcinoma. Int J Cancer 2008, 123, 2791–2797. [Google Scholar] [CrossRef]
- Sheng, S.; Su, W.; Mao, D.; Li, C.; Hu, X.; Deng, W.; Yao, Y.; Ji, Y. MicroRNA-21 induces cisplatin resistance in head and neck squamous cell carcinoma. PLoS One 2022, 17, e0267017. [Google Scholar] [CrossRef]
- Ou, H.; Li, Y.; Kang, M. Activation of miR-21 by STAT3 induces proliferation and suppresses apoptosis in nasopharyngeal carcinoma by targeting PTEN gene. PLoS One 2014, 9, e109929. [Google Scholar] [CrossRef]
- Irimie-Aghiorghiesei, A.I.; Pop-Bica, C.; Pintea, S.; Braicu, C.; Cojocneanu, R.; Zimța, A.A.; Gulei, D.; Slabý, O.; Berindan-Neagoe, I. Prognostic Value of MiR-21: An Updated Meta-Analysis in Head and Neck Squamous Cell Carcinoma (HNSCC). J Clin Med 2019, 8. [Google Scholar] [CrossRef] [PubMed]
- Vahabi, M.; Blandino, G.; Di Agostino, S. MicroRNAs in head and neck squamous cell carcinoma: a possible challenge as biomarkers, determinants for the choice of therapy and targets for personalized molecular therapies. Transl Cancer Res 2021, 10, 3090–3110. [Google Scholar] [CrossRef]
- Sobah, M.L.; Liongue, C.; Ward, A.C. SOCS Proteins in Immunity, Inflammatory Diseases, and Immune-Related Cancer. Front Med (Lausanne) 2021, 8, 727987. [Google Scholar] [CrossRef]
- Gao, G.; Gay, H.A.; Chernock, R.D.; Zhang, T.R.; Luo, J.; Thorstad, W.L.; Lewis, J.S., Jr.; Wang, X. A microRNA expression signature for the prognosis of oropharyngeal squamous cell carcinoma. Cancer 2013, 119, 72–80. [Google Scholar] [CrossRef]
- Kajiyama, T.; Serada, S.; Fujimoto, M.; Ohkawara, T.; Komori, M.; Hyodo, M.; Naka, T. SOCS1 Gene Therapy for Head and Neck Cancers: An Experimental Study. Anticancer Res 2022, 42, 3361–3372. [Google Scholar] [CrossRef]
- Zeng, Q.; Tao, X.; Huang, F.; Wu, T.; Wang, J.; Jiang, X.; Kuang, Z.; Cheng, B. Overexpression of miR-155 promotes the proliferation and invasion of oral squamous carcinoma cells by regulating BCL6/cyclin D2. Int J Mol Med 2016, 37, 1274–1280. [Google Scholar] [CrossRef]
- Kavitha, M.; Jayachandran, D.; Aishwarya, S.Y.; Md. Younus, P.; Venugopal, A.; Suresh Babu, H.W.; Ajay, E.; Sanjana, M.; Arul, N.; Balachandar, V. A new insight into the diverse facets of microRNA-31 in oral squamous cell carcinoma. Egyptian Journal of Medical Human Genetics 2022, 23, 149. [CrossRef]
- Hammouz, R.Y.; Kołat, D.; Kałuzińska, Ż.; Płuciennik, E.; Bednarek, A.K. MicroRNAs: Their Role in Metastasis, Angiogenesis, and the Potential for Biomarker Utility in Bladder Carcinomas. Cancers (Basel) 2021, 13. [Google Scholar] [CrossRef]
- Ghafouri-Fard, S.; Gholipour, M.; Taheri, M.; Shirvani Farsani, Z. MicroRNA profile in the squamous cell carcinoma: prognostic and diagnostic roles. Heliyon 2020, 6, e05436. [Google Scholar] [CrossRef] [PubMed]
- Song, J.; Ouyang, Y.; Che, J.; Li, X.; Zhao, Y.; Yang, K.; Zhao, X.; Chen, Y.; Fan, C.; Yuan, W. Potential Value of miR-221/222 as Diagnostic, Prognostic, and Therapeutic Biomarkers for Diseases. Front Immunol 2017, 8, 56. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.Q.; Ahmed, E.I.; Elareer, N.R.; Junejo, K.; Steinhoff, M.; Uddin, S. Role of miRNA-Regulated Cancer Stem Cells in the Pathogenesis of Human Malignancies. Cells 2019, 8. [Google Scholar] [CrossRef]
- Raulf, N.; Lucarelli, P.; Thavaraj, S.; Brown, S.; Vicencio, J.M.; Sauter, T.; Tavassoli, M. Annexin A1 regulates EGFR activity and alters EGFR-containing tumour-derived exosomes in head and neck cancers. Eur J Cancer 2018, 102, 52–68. [Google Scholar] [CrossRef]
- Sharma, P.C.; Gupta, A. MicroRNAs: potential biomarkers for diagnosis and prognosis of different cancers. Transl Cancer Res 2020, 9, 5798–5818. [Google Scholar] [CrossRef]
- Malumbres, M. miRNAs and cancer: an epigenetics view. Mol Aspects Med 2013, 34, 863–874. [Google Scholar] [CrossRef]
- Singh, S.; Sinha, T.; Panda, A.C. Regulation of microRNA by circular RNA. Wiley Interdisciplinary Reviews: RNA 2024, 15, e1820. [Google Scholar]
- Li, Q.; Tie, Y.; Alu, A.; Ma, X.; Shi, H. Targeted therapy for head and neck cancer: signaling pathways and clinical studies. Signal Transduct Target Ther 2023, 8, 31. [Google Scholar] [CrossRef]
- Song, J.; Zhang, N.; Cao, L.; Xiao, D.; Ye, X.; Luo, E.; Zhang, Z. Down-regulation of miR-200c associates with poor prognosis of oral squamous cell carcinoma. Int J Clin Oncol 2020, 25, 1072–1078. [Google Scholar] [CrossRef]
- Perdigão-Henriques, R.; Petrocca, F.; Altschuler, G.; Thomas, M.P.; Le, M.T.; Tan, S.M.; Hide, W.; Lieberman, J. miR-200 promotes the mesenchymal to epithelial transition by suppressing multiple members of the Zeb2 and Snail1 transcriptional repressor complexes. Oncogene 2016, 35, 158–172. [Google Scholar] [CrossRef] [PubMed]
- Sanli, F.; Tatar, A.; Gundogdu, B.; Karatas, O.F. IP3R1 dysregulation via mir-200c-3p/SSFA2 axis contributes to taxol resistance in head and neck cancer. Eur J Pharmacol 2024, 973, 176592. [Google Scholar] [CrossRef] [PubMed]
- Zhang, B.; Li, Y.; Hou, D.; Shi, Q.; Yang, S.; Li, Q. MicroRNA-375 Inhibits Growth and Enhances Radiosensitivity in Oral Squamous Cell Carcinoma by Targeting Insulin Like Growth Factor 1 Receptor. Cell Physiol Biochem 2017, 42, 2105–2117. [Google Scholar] [CrossRef] [PubMed]
- Kozłowska-Masłoń, J.; Guglas, K.; Kolenda, T.; Lamperska, K.; Makałowska, I. miRNA in head and neck squamous cell carcinomas: promising but still distant future of personalized oncology. Rep Pract Oncol Radiother 2023, 28, 681–697. [Google Scholar] [CrossRef]
- Seo, H.A.; Moeng, S.; Sim, S.; Kuh, H.J.; Choi, S.Y.; Park, J.K. MicroRNA-Based Combinatorial Cancer Therapy: Effects of MicroRNAs on the Efficacy of Anti-Cancer Therapies. Cells 2019, 9. [Google Scholar] [CrossRef]
- Ganci, F.; Sacconi, A.; Manciocco, V.; Covello, R.; Benevolo, M.; Rollo, F.; Strano, S.; Valsoni, S.; Bicciato, S.; Spriano, G.; et al. Altered peritumoral microRNA expression predicts head and neck cancer patients with a high risk of recurrence. Mod Pathol 2017, 30, 1387–1401. [Google Scholar] [CrossRef]
- Liu, W.; Liu, Y.; Li, P.; Chen, J.; Liu, J.; Shi, Z.; Liu, H.; Ye, J. Identification of candidate plasma miRNA biomarkers for the diagnosis of head and neck squamous cell carcinoma. Future Sci OA 2024, 10, Fso928. [Google Scholar] [CrossRef]
- Laprovitera, N.; Riefolo, M.; Porcellini, E.; Durante, G.; Garajova, I.; Vasuri, F.; Aigelsreiter, A.; Dandachi, N.; Benvenuto, G.; Agostinis, F.; et al. MicroRNA expression profiling with a droplet digital PCR assay enables molecular diagnosis and prognosis of cancers of unknown primary. Mol Oncol 2021, 15, 2732–2751. [Google Scholar] [CrossRef]
- Kumarasamy, C.; Madhav, M.R.; Sabarimurugan, S.; Krishnan, S.; Baxi, S.; Gupta, A.; Gothandam, K.M.; Jayaraj, R. Prognostic Value of miRNAs in Head and Neck Cancers: A Comprehensive Systematic and Meta-Analysis. Cells 2019, 8, 772. [Google Scholar] [CrossRef]
- Yerukala Sathipati, S.; Ho, S.Y. Survival associated miRNA signature in patients with head and neck carcinomas. Heliyon 2023, 9, e17218. [Google Scholar] [CrossRef]
- Kabzinski, J.; Maczynska, M.; Majsterek, I. MicroRNA as a Novel Biomarker in the Diagnosis of Head and Neck Cancer. Biomolecules 2021, 11. [Google Scholar] [CrossRef]
- Bhattacharjee, B.; Syeda, A.F.; Rynjah, D.; Hussain, S.M.; Chandra Bora, S.; Pegu, P.; Sahu, R.K.; Khan, J. Pharmacological impact of microRNAs in head and neck squamous cell carcinoma: Prevailing insights on molecular pathways, diagnosis, and nanomedicine treatment. Front Pharmacol 2023, 14, 1174330. [Google Scholar] [CrossRef]
- Weissman, S.M. Personalized medicine: a new horizon for medical therapy. Precis Clin Med 2018, 1, 1–2. [Google Scholar] [CrossRef]
- Emwas, A.H.; Szczepski, K.; Al-Younis, I.; Lachowicz, J.I.; Jaremko, M. Fluxomics - New Metabolomics Approaches to Monitor Metabolic Pathways. Front Pharmacol 2022, 13, 805782. [Google Scholar] [CrossRef]
- Shtivelman, E.; Beer, T.M.; Evans, C.P. Molecular pathways and targets in prostate cancer. Oncotarget 2014, 5, 7217–7259. [Google Scholar] [CrossRef]
- Filella, X.; Fernández-Galan, E.; Fernández Bonifacio, R.; Foj, L. Emerging biomarkers in the diagnosis of prostate cancer. Pharmgenomics Pers Med 2018, 11, 83–94. [Google Scholar] [CrossRef]
- Solomon, B.; Young, R.J.; Rischin, D. Head and neck squamous cell carcinoma: Genomics and emerging biomarkers for immunomodulatory cancer treatments. Semin Cancer Biol 2018, 52, 228–240. [Google Scholar] [CrossRef]
Figure 1.
Epidemiological Aspect of Head and Neck Cancer (Created with BioRender.com).
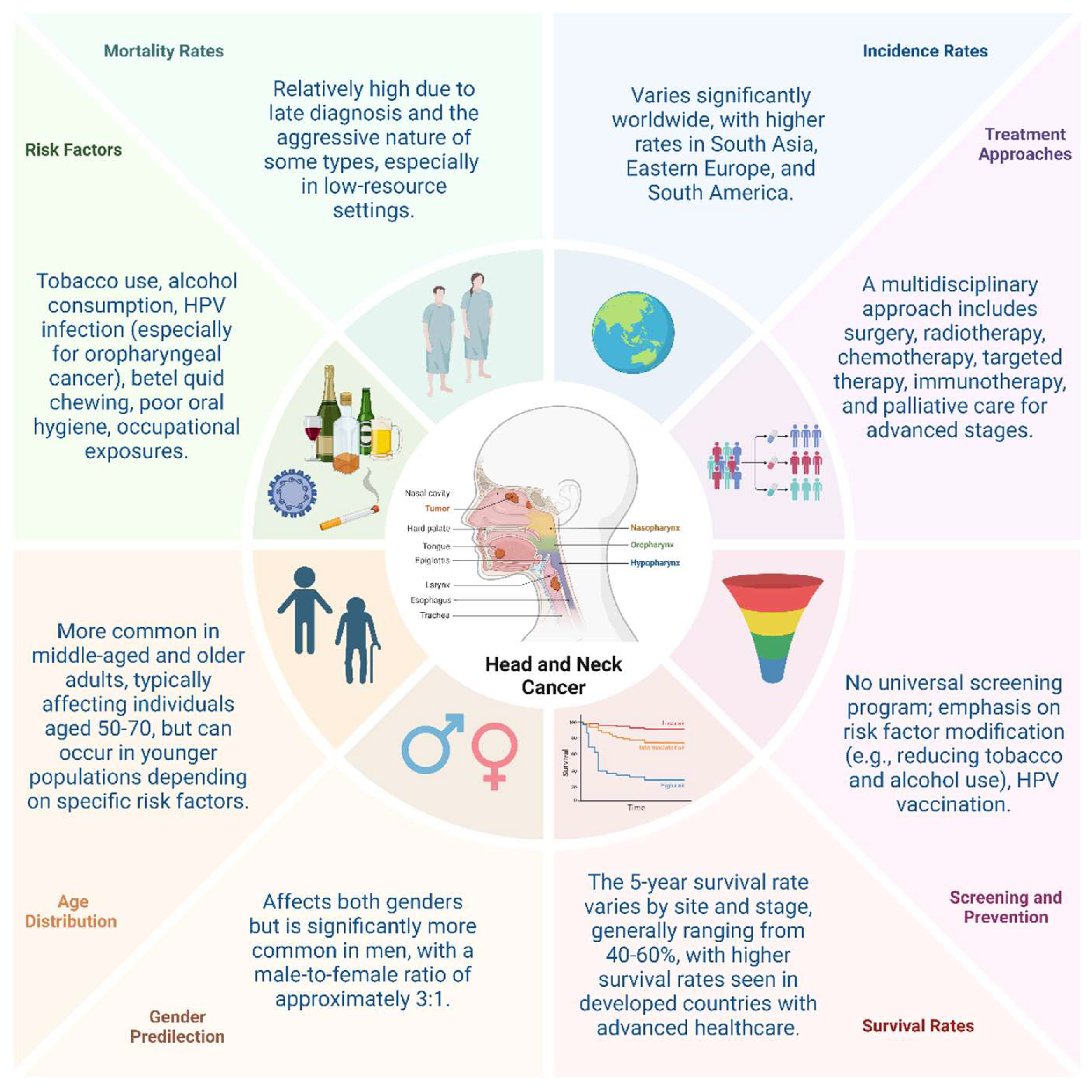
Figure 2.
OncomiRs and Tumour-Suppressive miRNAs: Key Regulators in Head and Neck Cancer Progression. This figure illustrates the dual roles of oncomiRs and tumour-suppressive miRNAs in head and neck cancer. OncomiRs promote tumour growth and metastasis, while tumour-suppressive miRNAs inhibit cancer progression. Together, these miRNAs orchestrate molecular pathways in cell proliferation, apoptosis, and angiogenesis. (Created with BioRender.com).
Figure 2.
OncomiRs and Tumour-Suppressive miRNAs: Key Regulators in Head and Neck Cancer Progression. This figure illustrates the dual roles of oncomiRs and tumour-suppressive miRNAs in head and neck cancer. OncomiRs promote tumour growth and metastasis, while tumour-suppressive miRNAs inhibit cancer progression. Together, these miRNAs orchestrate molecular pathways in cell proliferation, apoptosis, and angiogenesis. (Created with BioRender.com).
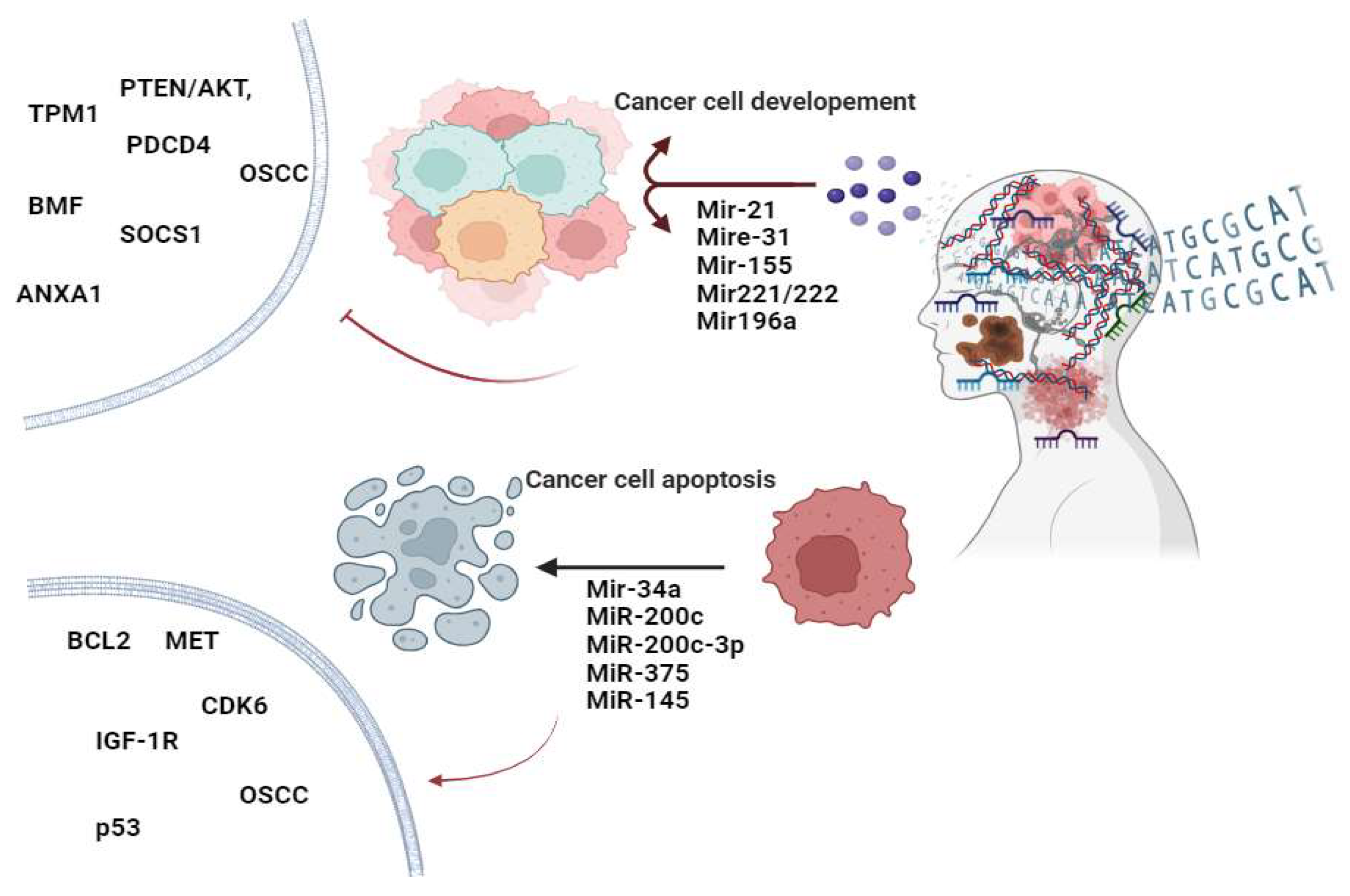

Table 1.
Molecular Subtypes of Head and Neck Cancer: Characteristics and Clinical Implications.
| Molecular Subtype | Characteristic Features | Clinical Implications | References |
|---|---|---|---|
| HPV-positive |
Presence of HPV DNA, overexpression of p16, and absence of TP53 mutations. | Better response to treatment and prognosis compared to HPV-negative tumours. | [20] |
| Basal |
High expression of basal cell markers, EGFR amplification, and TP53 mutations. | Poor differentiation and worse prognosis. | [21] |
| Mesenchymal |
Features of epithelial-to-mesenchymal transition, expression of mesenchymal markers. | Resistance to chemotherapy and radiation therapy. | [22] |
| Atypical |
Mutations in NOTCH1, low HPV, and p16 expression. | Diverse prognosis, potential sensitivity to NOTCH inhibitors. | [23] |
| Classical |
High expression of genes involved in cell cycle regulation, notably cyclin D1 and CDK6. | Aggressive behaviour, potential targets for cell cycle inhibitors. | [24] |
| Immune-Related |
High infiltration of immune cells and expression of immune checkpoint molecules such as PD-L1. | Potential responsiveness to immunotherapy, particularly immune checkpoint inhibitors. | [25] |
| Hypoxic |
Overexpression of hypoxia-inducible factors (HIFs), adaptation to low oxygen environments. | Poor prognosis, potential targets for therapies aimed at hypoxic conditions. | [26] |
| Metabolic |
Alterations in metabolic pathways, increased glycolysis (Warburg effect), overexpression of GLUT1. | Potential for targeting metabolic pathways, implications for metabolic inhibitors. | [27] |
Table 2.
Key Proteins and Genes in Head and Neck (HNC).
| Key Protein/Gene | Role in Cancer | Clinical Relevance | Ref |
|---|---|---|---|
| HPV E6/E7 |
Oncogenic viral proteins that inactivate p53 and Rb, promoting cell cycle progression. | HPV status is a critical prognostic marker and determines treatment strategies. | [33] |
| EGFR |
Overexpressed in many HNCs, leading to increased cell proliferation. | Targeted by EGFR inhibitors like cetuximab, it predicts responsiveness to therapy. | [34] |
| TP53 |
Mutations lead to loss of tumour suppressor function, contributing to carcinogenesis. | Associated with poor prognosis and aggressive disease; potential target for therapy. | [35] |
| CDKN2A (p16) |
Tumour suppressor gene, loss contributes to cell cycle deregulation. | Frequently mutated or deleted in HNC, indicative of poor prognosis. | [36] |
| PIK3CA | Mutation activates the PI3K/AKT pathway, promoting tumorigenesis. | Target for PI3K inhibitors associated with therapeutic resistance. | [37] |
| TIMPs (Tissue Inhibitors of Metalloproteinases) | Regulate ECM remodelling and metastasis by inhibiting MMPs, potentially suppressing tumour progression. | Targets for therapy and markers for disease progression and response to treatment. | [38] |
| Gal-3 (Galectin-3) |
Involved in cell adhesion, migration, and tumour progression. | Potential marker for prognosis and therapeutic targeting. | [39] |
| MMPs (Matrix Metalloproteinases) | Facilitate tumour invasion and metastasis through ECM degradation. | Biomarkers for invasive potential and therapeutic targets. | [40] |
| Fibronectin |
Contributes to cell adhesion and migration, influencing tumour growth and metastasis. | Insights into tumour progression and potential therapeutic implications. | [41] |
Table 3.
Characterization of Top DEGs Identified for HNC.
| Gene | Role in Cancer Identified in Previous Studies | Reference |
|---|---|---|
| AURKA |
High expression is associated with cancer progression, dysregulated proliferation, and inhibition of apoptosis. It is a good predictor of OS, with overexpression representing a poor prognosis. | [42,43,44] |
| HMGA2 |
Overexpression increases tumour cell proliferation, migration, invasion, and metastasis. A good predictor of OS, with high levels indicating poor prognosis. | [45,46,47] |
| MMP1 |
Upregulation is associated with ECM degradation and consequent cancer-promoting invasiveness. Its expression correlates with T stage (TNM classification) and cancer progression. | [48,49] |
| PLAU |
Overexpression is associated with ECM degradation, an increased risk of developing HNC, and an upregulation of MMP1. Knockdown inhibits proliferation, invasion, and metastasis. | [49,50] |
| SERPINE1 |
Overexpression is associated with N stage (TNM classification), poor DFS, and the promotion of radiotherapy resistance. Inhibition leads to decreased cell proliferation and invasion. | [4,51,52] |
Table 4.
Diagnostic and Prognostic Biomarkers in HNC: Effectiveness Overview.
| Biomarker | Diagnostic Use | Prognostic Use | Potential Effectiveness |
Ref |
|---|---|---|---|---|
| HPV DNA |
Identifies HPV-associated HNC | Indicates better prognosis and response to treatment in HPV-positive cases | Highly effective for subclassification and prognosis | [72] |
| EGFR |
Used for identifying tumours with EGFR overexpression | Associated with poor response to radiation and certain chemotherapies | Effective in selecting candidates for EGFR-targeted therapies | [73] |
| p16 |
Surrogate marker for HPV oncogenic activity | Suggests improved outcomes in HPV-positive HNC | Widely used, offers good prognostic value | [74] |
Table 5.
miRNAs associated with tumorigenesis of HNSC.
| miRNA name | P-value T-Test | FDR T-Test | Upregulated in | Tumor Log2 Mean Expression | Normal Log2Mean Expression |
|---|---|---|---|---|---|
| hsa-miR-21-5p | 8.64E-15 | 6.65E-13 | Tumour | 0 | 0 |
| hsa-miR-31-5p | 1.12E-07 | 8.23E-07 | Tumour | 0 | 0 |
| hsa-miR-221-3p | 1.14E-03 | 3.09E-03 | Tumour | 0 | 0 |
| hsa-miR-222-3p | 2.07E-06 | 1.02E-05 | Tumour | 0 | 0 |
| hsa-miR-196a-5p | 2.44E-17 | 8.45E-15 | Tumour | 0 | 0 |
| hsa-miR-200c-3p | 1.44E-02 | 3.12E-02 | Tumour | 0 | 0 |
| hsa-miR-375 | 1.77E-11 | 3.60E-10 | Normal | 0 | 0 |
| hsa-miR-145-5p | 2.44E-04 | 7.54E-04 | Normal | 0 | 0 |
Table 6.
miRNAs significantly associated with survival in HNSC.
| miRNA name | Log Rank P-value |
Log Rank FDR |
Z-score | Upregulated in | Deceased Log2 Mean Expression |
Living Log2 Mean Expression |
T-Test P-value |
T-Test FDR |
|---|---|---|---|---|---|---|---|---|
| hsa-miR-155-3p | 3.46E-02 | 3.77E-01 | 1.985 | Living | 0.52 | 0.65 | 3.33E-01 | 5.94E-01 |
Table 7.
hsa-miR-155-3p -Target Correlation in HNSC.
| Gene | Gene Description | Correlation | Correlation P-value | Correlation FDR | miRDB Score |
|---|---|---|---|---|---|
| RAI14 | Retinoic acid-induced 14 | -0.106 | 1.73E-02 | 5.67E-01 | 82 |
| S1PR5 | Sphingosine-1-phosphate receptor 5 | -0.0983 | 2.73E-02 | 5.67E-01 | 76 |
| OSBPL10 | Oxysterol binding protein-like 10 | -0.0961 | 3.09E-02 | 5.67E-01 | 90 |
| METTL6 | Methyltransferase like 6 | -0.0876 | 4.93E-02 | 5.79E-01 | 63 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



