
Submitted:
27 September 2024
Posted:
27 September 2024
You are already at the latest version
Abstract
Background/Objectives: The burden of hospital-acquired infections (HAIs) is particularly sub-stantial in low- and middle-income countries (LMICs). However, a comprehensive understanding of their prevalence in these regions is lacking. This systematic review aimed to evaluate the prevalence of HAIs in LMICs.
Methods: Major databases, including Scopus, PubMed, and Web of Science, were thoroughly searched for published studies between January 1, 2000, and July 15, 2024. The PRISMA guidelines were followed for a comprehensive and systematic approach. The pooled prevalence of HAIs was estimated using a random-effects model and a 95% confidence interval (CI).
Results: The literature search identified 87 studies reporting HAI prevalence in LMICs. The overall prevalence of HAIs across LMICs was 22% (95% CI: 17-28), with notable regional variations. The South-East Asian Region (SEAR) presented the highest prevalence at 37% (95% CI: 13-62), followed by the African Region at 25% (95% CI: 16-33). The European Region (EUR) had the lowest preva-lence, at 14% (95% CI: 5-23). In terms of income level, low-income countries had the highest prevalence at 37% (95% CI: 23-52), followed by lower-middle income at 22% (15-30) and up-per-middle income at 13% (95% CI: 6-20). Surgical site infections (SSIs) had the highest prevalence among infection types at 27% (95% CI: 23-31), followed by pneumonia at 23% (95% CI: 18-28) and urinary tract infections (UTIs) at 22% (95% CI: 19-26). Gastrointestinal infections (GIs) were less prevalent at 6% (95% CI: 3-9).
Conclusions: This systematic review underscores the high prevalence of HAIs in most LMICs, with variations based on region and income level, emphasizing the need to facilitate the development of targeted prevention and control strategies to mitigate the impact of this critical public health issue, especially in resource-limited settings.
Keywords:
Hospital-acquired infections (HAIs)
; prevalence
; low- and middle-income countries (LMICs)
; hospitalized
; meta-analysis
1. Introduction
Hospital-acquired infections (HAIs) are infections that develop over 48 hours after hospital admission or within 30 days post-discharge [1]. These infections pose considerable global risks to patient safety and well-being [2]. HAIs are the most prevalent adverse events experienced by hospitalized patients, leading to prolonged hospital stays and significant morbidity and mortality [3]. On average, 1 out of every 10 patients affected by an HAI experience mortality associated with the infection [4]. HAIs result in substantial economic burdens, with significant cost discrepancies among healthcare facilities and countries. The worldwide cost of HAIs exceeds $200 billion per year [5]. In the United States, the annual financial impact of HAIs ranges from $28-$45 billion [6], whereas in the European Union, HAI-related costs exceed €7 billion annually [7].
There are differences in the prevalence of HAIs in high-income and low- to middle-income countries. For example, in high-income nations, 7 out of every 100 hospitalized patients develop an HAI, whereas in low- and middle-income countries, this number increases to 15 per 100 patients [4]. In the United States, HAIs impact 3.2% of hospitalized patients [8], whereas in Europe, the prevalence of HAIs in acute care settings is approximately 6.5% [9], which is lower than the reported 9.0% reported in Asia [10] and the estimated 12.8% reported in Africa [11]. However, the true extent of HAIs in low- and middle-income countries (LMICs) remains underestimated or unknown, as there is no comprehensive review that has pooled data on the prevalence of HAIs in these regions. Relying on information from other regions may not accurately reflect the local situation. This review, therefore, aimed to provide insight into the prevalence of HAIs in LMICs.
2. Materials and Methods
2.1. PRISMA Guidelines
We adhered to the requirements provided by Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [12] in order to guarantee a transparent and methodical literature search and evaluation. For the purpose of identifying, screening, and evaluating records, these recommendations offer a detailed list and flow diagram.
2.2. Search Strategy
We extensively searched Scopus, PubMed, and Web of Science for studies published between January 1, 2000, and July 15, 2024, to examine the prevalence of HAIs in LMICs. No language restrictions were applied, and we used Google Translate for non-English studies. The search terms included (“Hospital Acquired Infections” OR “Hospital-Associated Infections” OR “Nosocomial Infections”) AND (“Afghanistan” OR “Korea, Dem. People’s Rep” OR “South Sudan” OR “Burkina Faso” OR “Liberia” OR “Sudan” OR “Burundi” OR “Madagascar” OR “Syrian Arab Republic” OR “Central African Republic” OR “Malawi” OR “Togo” OR “Chad” OR “Mali” OR “Uganda” OR “Congo, Dem. Rep” OR “Mozambique” OR “Yemen, Rep” OR “Eritrea” OR “Niger” OR “Ethiopia” OR “Rwanda” OR “Gambia, The” OR “Sierra Leone” OR “Guinea-Bissau” OR “Somalia” OR “Angola” OR “Honduras” OR “Papua New Guinea” OR “Bangladesh” OR “India” OR “Philippines” OR “Benin” OR “Jordan” OR “Samoa” OR “Bhutan” OR “Kenya” OR “São Tomé and Principe” OR “Bolivia” OR “Kiribati” OR “Senegal” OR “Cabo Verde” OR “Kyrgyz Republic” OR “Solomon Islands” OR “Cambodia” OR “Lao PDR” OR “Sri Lanka” OR “Cameroon” OR “Lebanon” OR “Tajikistan” OR “Comoros” OR “Lesotho” OR “Tanzania” OR “Congo, Rep” OR “Mauritania” OR “Timor-Leste” OR “Côte d’Ivoire” OR “Micronesia, Fed. Sts” OR “Tunisia” OR “Djibouti” OR “Morocco” OR “Uzbekistan” OR “Egypt Arab Rep” OR “Myanmar” OR “Vanuatu” OR “Eswatini” OR “Nepal” OR “Vietnam” OR “Ghana” OR “Nicaragua” OR “West Bank and Gaza” OR “Guinea” OR “Nigeria” OR “Zambia” OR “Zimbabwe” OR “Albania” OR “Equatorial Guinea” OR “Moldova” OR “Algeria” OR “Fiji” OR “Mongolia” OR “Argentina” OR “Gabon” OR “Montenegro” OR “Armenia” OR “Georgia” OR “Namibia” OR “Azerbaijan” OR “Grenada” OR “North Macedonia” OR “Belarus” OR “Guatemala” OR “Paraguay” OR “Belize” OR “Indonesia” OR “Peru” OR “Bosnia and Herzegovina” OR “Iran, Islamic Rep” OR “Serbia” OR “Botswana” OR “Iraq” OR “South Africa” OR “Brazil” OR “Jamaica” OR “St. Lucia” OR “China” OR “Kazakhstan” OR “St. Vincent and the Grenadines” OR “Colombia” OR “Kosovo” OR “Suriname” OR “Costa Rica” OR “Libya” OR “Thailand” OR “Cuba” OR “Malaysia” OR “Tonga” OR “Dominica” OR “Maldives” OR “Türkiye” OR “Dominican Republic” OR “Marshall Islands” OR “Turkmenistan” OR “Ecuador” OR “Mauritius” OR “Tuvalu” OR “El Salvador” OR “Mexico” OR “Ukraine”). We included all relevant studies without restrictions on population groups or outcome measures. Furthermore, we reviewed the reference lists of relevant studies to find additional studies.
2.3. Study Selection
We implemented a two-step screening procedure to find pertinent studies. Initially, we reviewed titles and abstracts to exclude books, case–control studies, commentaries, interventional studies, letters to the editor, reports, and reviews. We subsequently evaluated the full-text of the remaining studies to ascertain their eligibility. The studies were assessed using predetermined inclusion and exclusion criteria. Eligible studies reported the prevalence of HAIs in LMICs, while those conducted outside LMICs or focusing on community-acquired infections were excluded. Studies without patient populations or with inaccuracies in HAI prevalence were also excluded. The screening process involved two independent reviewers who adhered to the criteria, with discrepancies resolved by a third reviewer. To handle the search results and find duplicate studies, we used Mendeley Desktop version 1.19.8.
2.4. Data Extraction
The data from the reviewed studies were organized and managed using Microsoft Excel 2019, version 2406. The extracted information included details from articles such as author(s) and year, the country of the study setting, guidelines used for defining HAIs, study period, patient population, prevalence of HAIs, and types of HAIs. The two reviewers independently employed a data abstraction format, to guarantee accurate data extraction.
2.5. Quality Assessment
The study quality was assessed using the JBI manual of Evidence Synthesis for prevalence studies [13]. This tool comprises 9 questions, each answered with “Y” for YES, “N” for NO, or “U” for Unclear. Studies scoring 50% or less were deemed “high risk of bias” or low quality, those between 50% and 70% were considered “moderate risk of bias” or medium quality, and those above 70% were labelled “low risk of bias” or high quality. A third reviewer arbitrated differences between the two independent reviewers who carried out the quality evaluation (Table S3).
2.6. Statistical Analysis
The meta and metafor packages in the R software (version 4.3.1) were used to perform statistical data analyses. The pooled prevalence of HAIs was estimated using a random-effects model, which generated an effect size with a 95% confidence interval (CI). Forest plots were used to visualize the meta-analysis results. The I2 test quantified statistical heterogeneity, with a p value <0.05 considered significant. A funnel plot was used to illustrate the assessment of publication bias through Egger’s test. Subgroup analyses were performed to address variability in estimates on the basis of regional differences and income levels.
3. Results
3.1. Search Results
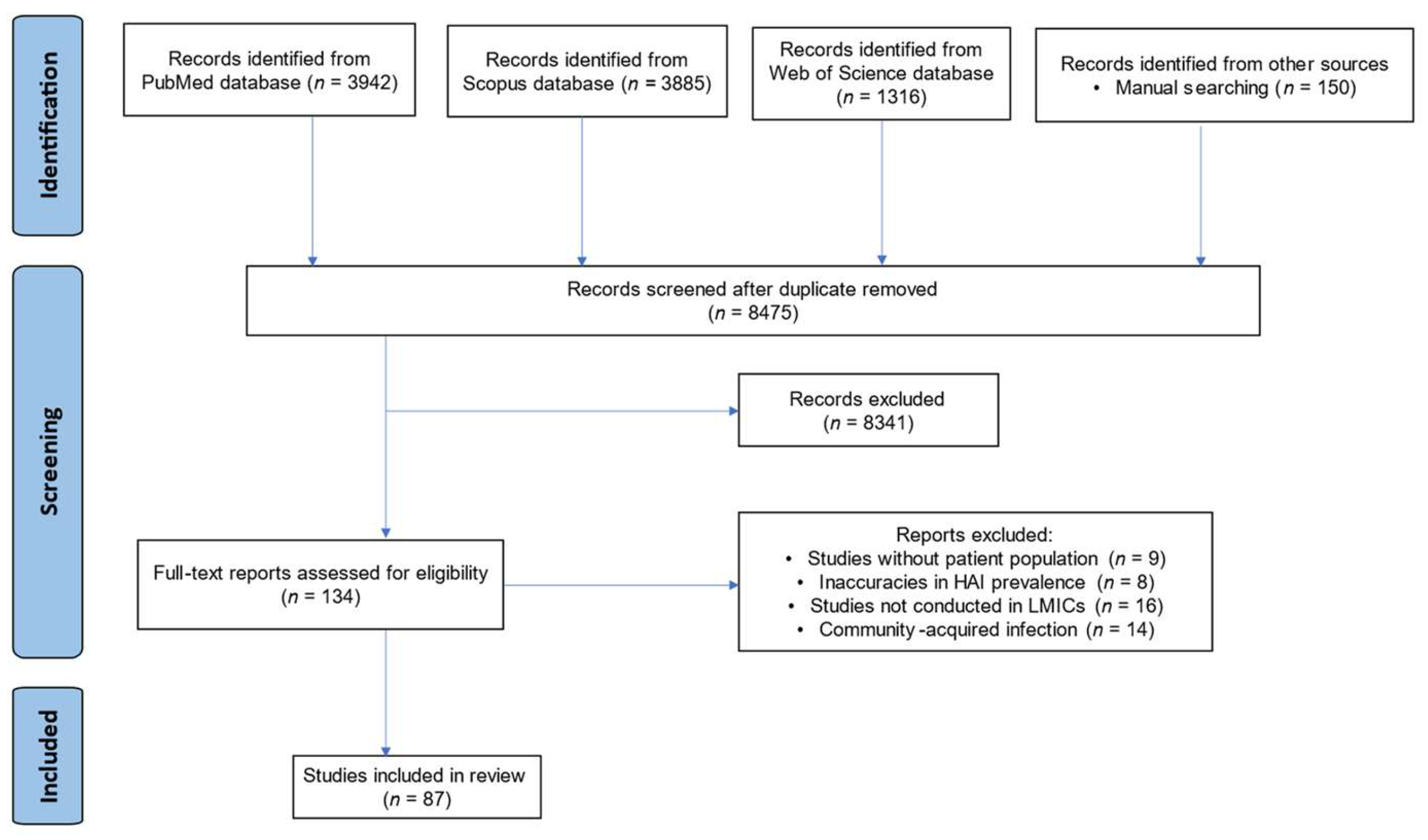
The initial database search on platforms such as PubMed (n = 3942), Scopus (n = 3885), and Web of Science (n = 1316) produced a total of 9143 publications. An additional 150 articles were identified through manual searches, resulting in a total of 9293. After removing duplicates (n = 818), 8475 records remained and were screened on the basis of their titles and abstracts. After excluding 8341 articles that failed to meet the inclusion criteria, 134 full-text articles were assessed for eligibility. Of these, 87 articles met the criteria and were included in the review.
Figure 1.
PRISMA flow diagram for articles screening.
3.2. Study Distribution
These 87 articles [14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100] presented data on the prevalence of HAIs in LMICs (Table S1). According to the WHO region classification, 35 studies were from the African Region (AFR), 17 from the Eastern Mediterranean Region (EMR), 11 from the South East Asian Region (SEAR), 7 from the European Region (EUR), 9 from the Western Pacific Region (WPR), 6 from the Region of the Americas (AMR), and 2 were unclassified.
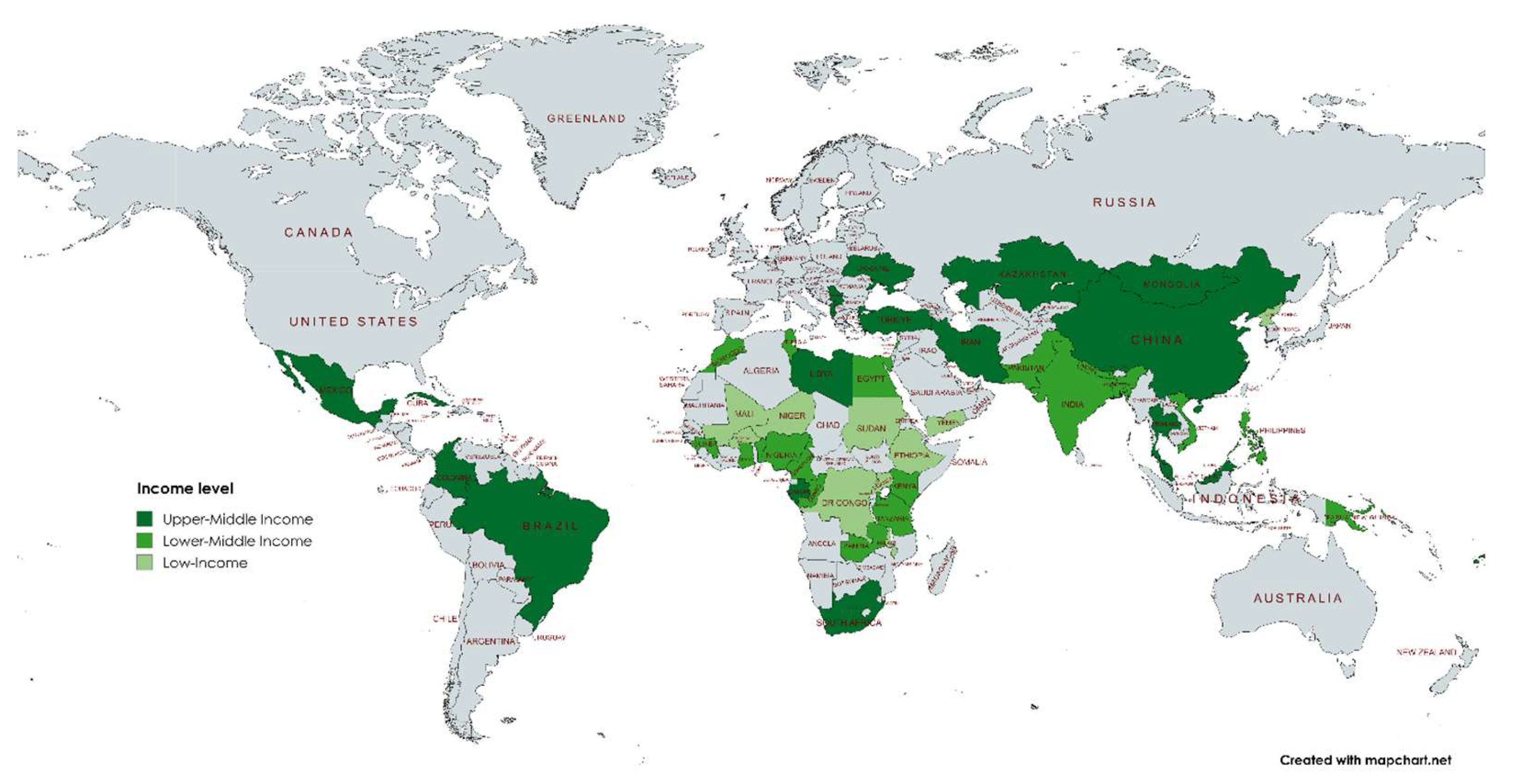
Concerning the income level of the countries based on the World Bank income level for 2024-2025 [101], 20 studies were from low-income countries, 36 were from lower-middle-income countries, and 31 were from upper-middle-income countries.
Figure 2.
Distribution of studies according to WHO region.
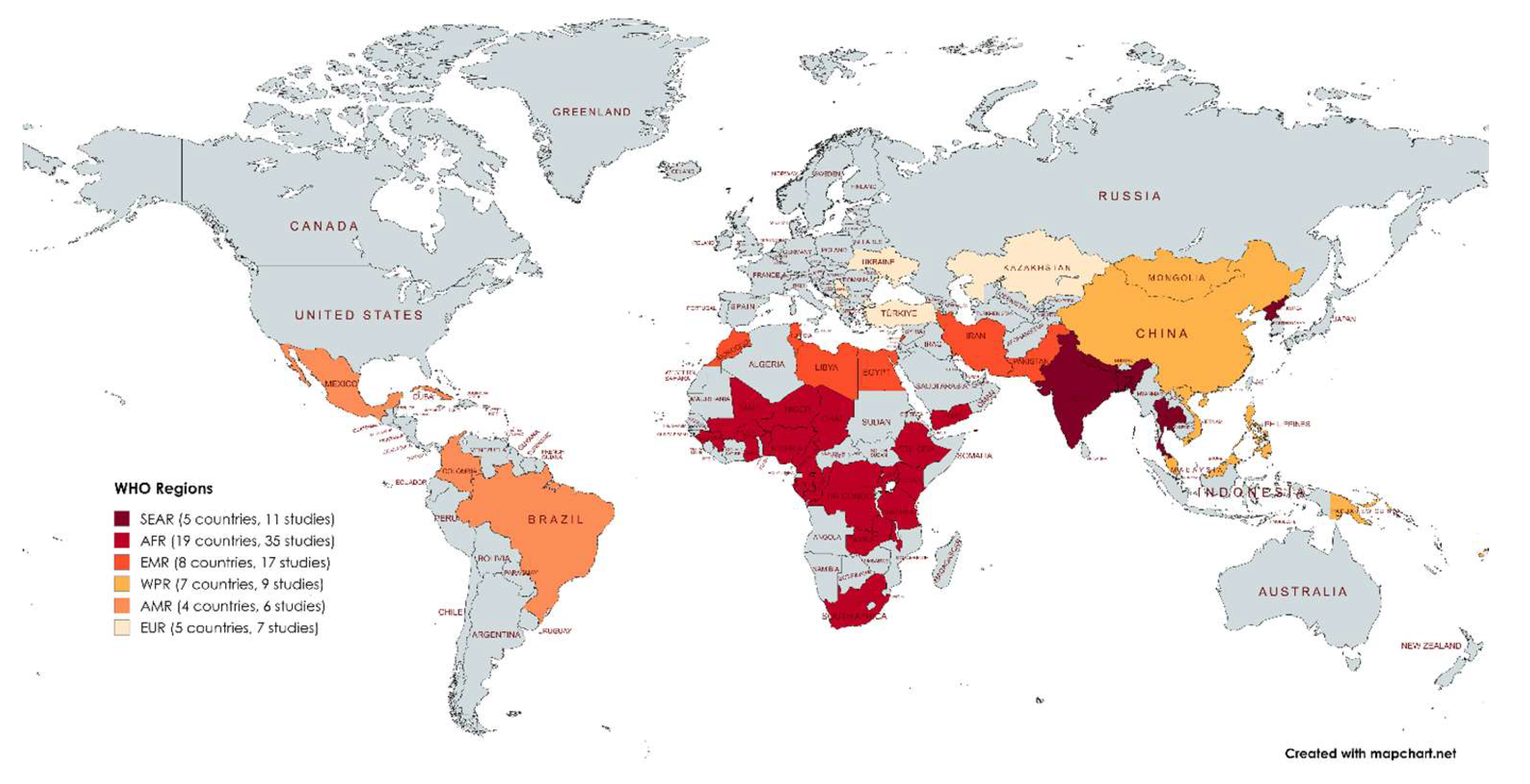
Figure 3.
Distribution of studies according to income level.
3.2. Pool Prevalence of HAIs in LMICs
In the studies reviewed, out of 17,221,026 hospitalized patients, 246,190 cases were identified as HAIs. The meta-analysis estimated that the overall prevalence of HAIs in LMICs was 22% (95% CI: 17-28) (Figure 4). Subgroup analysis by WHO region revealed a prevalence of 14% (95% CI: 5-23) in the European Region (EUR) and 37% (95% CI:13-62) in the Southeast Asian Region (SEAR). In terms of income levels, low-income countries had a prevalence of 37% (95% CI: 23-52), whereas upper-middle-income countries presented a lower prevalence of 13% (95% CI: 6-20) (Table 1).
3.3. HAI Type
Among the 246,190 HAI cases analysed, surgical site infections (SSIs) had the highest prevalence at 27% (95% CI: 23-31), followed by pneumonia at 0.23 (95% CI: 18-28) and urinary tract infections (UTIs) at 22% (95% CI: 19-26). Gastrointestinal infections (GIs) had the lowest number of cases at 174, with a prevalence of 6% (95% CI: 3-9) (Table 2). Notably, UTIs were predominant, identified in 77 studies across 46 countries, whereas bloodstream infections (BSIs) were documented in 65 studies across 40 countries. In contrast, gastrointestinal infections (GIs) were observed in only 19 studies across 16 countries.
3.4. Quality of the Studies
After the JBI critical appraisal questions were assessed, only 3 studies (3.4%) were identified as medium quality or moderate risk of bias. In contrast, the majority, comprising 84 studies (96.6%), were classified as high quality or low risk of bias (Table S3).
4. Discussion
HAIs impose a significant burden on healthcare systems globally, with varying prevalence and types across regions. This review examines HAIs in LMICs, highlighting major infection types. The review involved 17,273,166 hospitalized patients, with an overall HAI prevalence of 22% (95% CI: 17-28) in LMICs, which is significantly greater than that reported in high-income countries. In Europe, the prevalence was 6.5% [102], and in the United States, it was 4.0% [103]. The prevalence of HAIs varied across WHO regions, with LMICs in the Southeast Asian Region (SEAR) having the highest at 37% (95% CI: 13-62), followed by those in the African Region at 25% (95% CI: 16-33). This contrasts with a global study where the African Region had the highest prevalence, followed by the Southeast Asian Region (SEAR) [104]. The estimated prevalence reported in this review surpasses that reported in previous reviews in LMICs across different regions. For example, a systematic review in 2015 reported a prevalence of 9.0% in Southeast Asia [10], whereas a recent study by Goh et al. [105] reported a prevalence of 21.6% in the same region. In Africa, the prevalence was 12.8% in 2022 [11], whereas a recent review reported a prevalence of 15% [106]. These trends suggest a growing prevalence of HAIs, supported by the increasing prevalence observed in LMICs in this review. Compared with upper-middle-income countries, low-income countries presented a greater prevalence, which aligns with the findings of a global study by Raoofi et al. [104]. Low-income countries, primarily in the Southeast Asian Region (SEAR) and the African Region (AFR), often face challenges such as limited healthcare infrastructure, fewer healthcare facilities, and a shortage of healthcare professionals. These factors can contribute to higher rates of HAIs due to inadequate infection control measures and overcrowding hospitals.
Urinary tract infections (UTIs), surgical site infections (SSIs), and bloodstream infections (BSIs), and were the most commonly reported HAIs in more than 74% of the studies included in our review. SSIs had the highest prevalence, which is consistent with findings in the African review [11]. In contrast, the study in the United States by Magill et al. [103] identified pneumonia as the most prevalent HAI. Other significant HAIs included pneumonia, UTIs, and BSIs, whereas gastrointestinal infections were less common. Rigorous hand hygiene among healthcare workers likely reduces the transmission of gastrointestinal pathogens, often resulting from inadequate food handling and hygiene practices, thereby contributing to a lower prevalence. SSIs, which are particularly prevalent in low-resource settings, may result from inadequate hygiene practices before, during, and after surgery. The incidence of SSIs varies from 3% to 15% across different surgical procedures and is influenced by patient health and surgery type [107]. Factors such as high air contamination in operating rooms, frequent door openings and crowded surgery settings increase the risk of SSI [108,109]. The reported SSI rates in studies may underestimate the actual rates, as some infections occur post discharge. Establishing a surveillance system with active follow-up post discharge is essential to identify SSIs that develop after hospital stays.
HAIs present a global concern, with LMICs imposing a disproportionate burden, as outlined in this review. The ECDC suggests that up to 50% of HAIs are preventable [110]. Several studies have indicated that relying solely on manual cleaning is insufficient to completely eliminate contamination and ensure the safety of patients and medical staff [111,112,113]. To improve outcomes and reduce infection rates, a comprehensive infection control strategy that integrates automated disinfection methods such as UV-C light and hydrogen peroxide vapour with manual cleaning techniques is crucial [114,115]. Active surveillance is essential for gathering data on HAI incidence, identifying risk factors, evaluating the effectiveness of infection control programs, and highlighting areas requiring further interventions and resources. However, information on surveillance activities for HAI prevention and control in LMICs is limited. Critical care medicine in LMICs is still in its early stages compared with that in more developed countries with established systems. Surveillance systems such as the European Center for Disease Prevention and Control (ECDC) in Europe [110] and the National Health Safety Network (NHSN) in the United States [116] continuously monitor HAIs. Most of the studies in our review followed the criteria of these established surveillance systems for identifying and classifying HAIs. However, some studies used criteria set by the authors, which may not accurately determine HAIs.
It is important to acknowledge some limitations of our review. This review focused primarily on quantitative data, limiting the exploration of qualitative factors contributing to HAIs in LMICs. The analysis included studies from only 50 out of the total 132 LMICs defined by the World Bank, representing approximately 17.4% of the entire LMIC population with available HAI prevalence data. Encouraging studies in countries without existing HAI research is vital. Variations in study designs and methodologies may lead to disparities in results. While some studies have used single-center and retrospective designs, prospective active surveillance is considered the preferred method for accurate data collection and analysis. Future studies in LMICs should involve multiple centers and adopt a prospective approach to address this limitation.
5. Conclusions
The review revealed that HAIs pose a significant issue in LMICs, with prevalence rates varying across regions and income levels. Surgical site infections and pneumonia had the highest prevalence, whereas urinary tract infections were the most commonly reported HAIs. These results emphasize the importance of implementing specific interventions and infection control strategies to address HAIs in LMICs.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Figure S1: title; Table S1: title; Video S1: title.
Author Contributions
Conceptualization, E.S.D., and A.O.; methodology, A.O., PBT-Q., and E.S.D.; validation, A.O., PBT-Q., and E.S.D.; formal analysis, A.O., PBT-Q., and E.S.D.; investigation, A.O., PBT-Q., and E.S.D.; resources, A.O., PBT-Q., and E.S.D.; data curation, A.O., PBT-Q., and E.S.D.; writing—original draft preparation, A.O., PBT-Q., and E.S.D.; writing—review and editing, A.O., PBT-Q., and E.S.D.; visualization, A.O., PBT-Q., and E.S.D.; supervision, E.S.D., and PBT-Q; project administration, E.S.D., PBT-Q., and A.O.; funding acquisition, E.S.D. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
The data supporting the findings of this study are available within the article or supplementary file.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Haque M, Sartelli M, McKimm J, Abu Bakar M. Health care-associated infections - an overview. Infect Drug Resist 2018, 11, 2321–2333. [Google Scholar] [CrossRef] [PubMed]
- Alamer A, Alharbi F, Aldhilan A, Almushayti Z, Alghofaily K, Elbehiry A, et al. Healthcare-Associated Infections (HAIs): Challenges and Measures Taken by the Radiology Department to Control Infection Transmission. Vaccines (Basel) 2022, 10, 2060. [Google Scholar] [CrossRef] [PubMed]
- Maki G, Zervos M. Health Care-Acquired Infections in Low- and Middle-Income Countries and the Role of Infection Prevention and Control. Infect Dis Clin North Am 2021, 35, 827–839. [Google Scholar] [CrossRef] [PubMed]
- WHO launches first ever global report on infection prevention and control. Available online: https://www.who.int/news/item/06-05-2022-who-launches-first-ever-global-report-on-infection-prevention-and-control (accessed on 7 August 2024).
- Scott RD, Culler SD, Rask KJ. Understanding the Economic Impact of Health Care-Associated Infections: A Cost Perspective Analysis. Journal of Infusion Nursing. 2019, 42, 61–69. [Google Scholar] [CrossRef]
- Stone, PW. Economic burden of healthcare-associated infections: an American perspective. Expert Rev Pharmacoecon Outcomes Res. 2009, 9, 417–422. [Google Scholar] [CrossRef]
- Report on the Burden of Endemic Health Care-Associated Infection Worldwide Clean Care is Safer Care. 2011. Available online: www.who.int (accessed on 6 August 2024).
- Magill SS, O’Leary E, Janelle SJ, Thompson DL, Dumyati G, Nadle J, et al. Changes in Prevalence of Health Care–Associated Infections in U.S. Hospitals. New England Journal of Medicine. 2018, 379, 1732–1744.
- Suetens C, Latour K, Kärki T, Ricchizzi E, Kinross P, Moro ML, et al. Prevalence of healthcare-associated infections, estimated incidence and composite antimicrobial resistance index in acute care hospitals and long-term care facilities: results from two European point prevalence surveys, 2016 to 2017. Euro Surveill 2018, 23, 1800516. [Google Scholar]
- Ling ML, Apisarnthanarak A, Madriaga G. The Burden of Healthcare-Associated Infections in Southeast Asia: A Systematic Literature Review and Meta-analysis. Clinical Infectious Diseases 2015, 60, 1690–1699. [Google Scholar] [CrossRef]
- Abubakar U, Amir O, Rodríguez-Baño J. Healthcare-associated infections in Africa: a systematic review and meta-analysis of point prevalence studies. J Pharm Policy Pract 2022, 15, 99. [Google Scholar] [CrossRef]
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021, n71. [CrossRef]
- Munn Z, Moola S, Lisy K, Riitano D, Tufanaru C. Methodological guidance for systematic reviews of observational epidemiological studies reporting prevalence and cumulative incidence data. Int J Evid Based Healthc. 2015, 13, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Newman, MJ. Nosocomial and Community Acquired Infections in Korle Bu Teaching Hospital, Accra. West Afr J Med 2010, 28. [Google Scholar] [CrossRef] [PubMed]
- Iwuafor AA, Ogunsola FT, Oladele RO, Oduyebo OO, Desalu I, Egwuatu CC, et al. Incidence, Clinical Outcome and Risk Factors of Intensive Care Unit Infections in the Lagos University Teaching Hospital (LUTH), Lagos, Nigeria. PLoS One 2016, 11, e0165242–e0165242. [Google Scholar] [CrossRef] [PubMed]
- Dayyab FM, Iliyasu G, Aminu A, Habib ZG, Tiamiyu AB, Tambuwal SH, et al. A prospective study of hospital-acquired infections among adults in a tertiary hospital in north-western Nigeria. Trans R Soc Trop Med Hyg 2018, 112, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Labi AK, Obeng-Nkrumah N, Owusu E, Bjerrum S, Bediako-Bowan A, Sunkwa-Mills G, et al. Multi-centre point-prevalence survey of hospital-acquired infections in Ghana. Journal of Hospital Infection 2019, 101, 60–68. [Google Scholar] [CrossRef]
- Abubakar, U. Point-prevalence survey of hospital acquired infections in three acute care hospitals in Northern Nigeria. Antimicrob Resist Infect Control 2020, 9, 63. [Google Scholar] [CrossRef]
- Andersen CT, Langendorf C, Garba S, Sayinzonga-Makombe N, Mambula C, Mouniaman I, et al. Risk of community- and hospital-acquired bacteremia and profile of antibiotic resistance in children hospitalized with severe acute malnutrition in Niger. International Journal of Infectious Diseases 2022, 119, 163–171. [Google Scholar] [CrossRef]
- Ige OK, Adesanmi AA, Asuzu MC. Hospital-acquired infections in a Nigerian tertiary health facility: An audit of surveillance reports. Niger Med J 2011, 52, 239–243. [Google Scholar] [CrossRef]
- Onuzo CN, Sefogah PE, Nuamah MA, Ntumy M, Osei MM, Nkyekyer K. Surgical site infections following caesarean sections in the largest teaching hospital in Ghana. Infection prevention in practice 2022, 4, 100203. [Google Scholar] [CrossRef]
- Iliyasu G, Dayyab FM, Abubakar S, Inuwa S, Tambuwal SH, Tiamiyu AB, et al. Laboratory-confirmed hospital-acquired infections: An analysis of a hospital’s surveillance data in Nigeria. Heliyon. 2018, 4, e00720. [Google Scholar] [CrossRef]
- Olawale KO, Fadiora SO, Taiwo SS. Prevalence of hospital-acquired enterococci infections in two primary-care hospitals in osogbo, southwestern Nigeria. Afr J Infect Dis 2011, 5, 40–46. [Google Scholar]
- Ahoyo TA, Bankolé HS, Adéoti FM, Gbohoun AA, Assavèdo S, Amoussou-Guénou M, et al. Prevalence of nosocomial infections and anti-infective therapy in Benin: results of the first nationwide survey in 2012. Antimicrob Resist Infect Control 2014, 3, 17. [Google Scholar] [CrossRef] [PubMed]
- Hien H, Drabo KM, Ouédraogo L, Konfé S, Zeba S, Sangaré L, et al. Healthcare-associated infection in Burkina Faso: an assessment in a district hospital. J Public Health Afr 2012, 3, e29–e29. [Google Scholar] [CrossRef]
- Ngolet LO, Fortuné A, Liboko B, Roland B, Ibara O, Dokekias AE. Hospital acquired infection in a department of hematology-oncology care in the Congo. Am J Blood Res 2021, 11, 191–198. Available online: www.AJBlood.us/ (accessed on 14 April 2024).
- Hassan R, El-Gilany AH, Abd Elaal AM, El-Mashad N, Azim DA. An overview of healthcare-associated infections in a tertiary care hospital in Egypt. Infection prevention in practice 2020, 2, 100059. [Google Scholar] [CrossRef]
- See I, Lessa FC, ElAta OA, Hafez S, Samy K, El-Kholy A, et al. Incidence and pathogen distribution of healthcare-associated infections in pilot hospitals in Egypt. Infect Control Hosp Epidemiol 2013, 34, 1281–1288. [Google Scholar] [CrossRef]
- Hamam S, Sakr A, Zahran W, Kholy R, Kasemy Z, Ibrahem R, et al. Health care-associated infections at an Egyptian tertiary care hospital: a 2-year prospective study. Menoufia Medical Journal. 2021, 34, 514. [Google Scholar] [CrossRef]
- Scherbaum M, Kösters K, Mürbeth RE, Ngoa UA, Kremsner PG, Lell B, et al. Incidence, pathogens and resistance patterns of nosocomial infections at a rural hospital in Gabon. BMC Infect Dis 2014, 14, 124. [Google Scholar]
- Keita AK, Doumbouya N, Sow MS, Konaté B, Dabo Y, Panzo DA, et al. Prévalence des infections nosocomiales dans deux hôpitaux de Conakry (Guinée). Sante Publique (Paris) 2016, 28, 251–255. [Google Scholar] [CrossRef]
- Kalagouda R, Kabera B, Muia CK, Ale BM. Hospital acquired infections in a private paediatric hospital in Kenya: a retrospective cross-sectional study. Pan African Medical Journal. 2022, 41.
- Bunduki GK, Feasey N, Henrion MYR, Noah P, Musaya J. Healthcare-associated infections and antimicrobial use in surgical wards of a large urban central hospital in Blantyre, Malawi: a point prevalence survey. Infection prevention in practice 2021, 3, 100163. [Google Scholar] [CrossRef] [PubMed]
- Jroundi I, Khoudri I, Azzouzi A, Zeggwagh AA, Benbrahim NF, Hassouni F, et al. Prevalence of hospital-acquired infection in a Moroccan university hospital. Am J Infect Control 2007, 35, 412–416. Available online: https://pubmed.ncbi.nlm.nih.gov/17660013/ (accessed on 14 April 2024). [CrossRef] [PubMed]
- Kallel H, Bahoul M, Ksibi H, Dammak H, Chelly H, Hamida CB, et al. Prevalence of hospital-acquired infection in a Tunisian hospital. Journal of Hospital Infection 2005, 59, 343–347. [Google Scholar] [CrossRef] [PubMed]
- Ginawi I, Saleem M, Sigh M, Vaish AK, Ahmad I, Srivastava VK, et al. Hospital acquired infections among patients admitted in the medical and surgical wards of a non-teaching secondary care hospital in northern India. J Clin Diagn Res 2014/02/03. 2014, 8, 81–83. [Google Scholar]
- Nair V, Sahni AK, Sharma D, Grover N, Shankar S, Chakravarty A, et al. Point prevalence & risk factor assessment for hospital-acquired infections in a tertiary care hospital in Pune, India. Indian J Med Res 2017, 145, 824–832. [Google Scholar]
- Vergeire-Dalmacion GR, Itable JR, Baja ES. Hospital-acquired infection in public hospital buildings in the Philippines: Is the type of ventilation increasing the risk? The Journal of Infection in Developing Countries 2016, 10, 1236–1242. [Google Scholar] [CrossRef]
- Viderman D, Khamzina Y, Kaligozhin Z, Khudaibergenova M, Zhumadilov A, Crape B, et al. An observational case study of hospital associated infections in a critical care unit in Astana, Kazakhstan. Antimicrob Resist Infect Control 2018, 7, 57. [Google Scholar] [CrossRef]
- Askarian M, Yadollahi M, Assadian O. Point prevalence and risk factors of hospital acquired infections in a cluster of university-affiliated hospitals in Shiraz, Iran. J Infect Public Health 2012, 5, 169–176. [Google Scholar] [CrossRef]
- Le NK, HF W, Vu PD, Khu DTK, Le HT, Hoang BTN, et al. High prevalence of hospital-acquired infections caused by gram-negative carbapenem resistant strains in Vietnamese pediatric ICUs. Medicine. 2016, 95, e4099. [Google Scholar] [CrossRef]
- Phu VD, Wertheim HFL, Larsson M, Nadjm B, Dinh QD, Nilsson LE, et al. Burden of Hospital Acquired Infections and Antimicrobial Use in Vietnamese Adult Intensive Care Units. PLoS One. 2016, 11, e0147544. [Google Scholar]
- Arif S, Sadeeqa S, Saleem Z, Latif S, Sharif M. The burden of healthcare-associated infections among pediatrics: a repeated point prevalence survey from Pakistan. Hosp Pract 2020, 49, 34–40. [Google Scholar] [CrossRef]
- Saleem Z, Hassali MA, Godman B, Hashmi FK, Saleem F. A multicenter point prevalence survey of healthcare–associated infections in Pakistan: Findings and implications. Am J Infect Control 2019, 47, 421–424. [Google Scholar] [CrossRef] [PubMed]
- Shrestha SK, Shrestha S, Ingnam S. Point prevalence of healthcare-associated infections and antibiotic use in a tertiary care teaching hospital in Nepal: A cross-sectional study. J Infect Prev 2022, 23, 29–32. Available online: https://pubmed.ncbi.nlm.nih.gov/35126679 (accessed on 29 August 2021). [CrossRef] [PubMed]
- Shrestha SK, Trotter A, Shrestha PK. Epidemiology and Risk Factors of Healthcare-Associated Infections in Critically Ill Patients in a Tertiary Care Teaching Hospital in Nepal: A Prospective Cohort Study. Infect Dis 2022, 15, 11786337211071120–11786337211071120. [Google Scholar]
- Loftus MJ, Curtis SJ, Naidu R, Cheng AC, Jenney AWJ, Mitchell BG, et al. Prevalence of healthcare-associated infections and antimicrobial use among inpatients in a tertiary hospital in Fiji: a point prevalence survey. Antimicrob Resist Infect Control 2020, 9, 146. [Google Scholar] [CrossRef]
- Braga IA, Campos PA, Gontijo-Filho PP, Ribas RM. Multi-hospital point prevalence study of healthcare-associated infections in 28 adult intensive care units in Brazil. Journal of Hospital Infection 2018, 99, 318–324. [Google Scholar] [CrossRef]
- Oliveira AC de, Kovner CT, Silva RS da. Nosocomial Infection in an Intensive Care Unit in a Brazilian University Hospital. Rev Lat Am Enfermagem 2010, 18, 233–239. [Google Scholar] [CrossRef]
- Ferreira GB, Donadello JCS, Mulinari LA. Healthcare-Associated Infections in a Cardiac Surgery Service in Brazil. Braz J Cardiovasc Surg 2020, 35, 614–618. [Google Scholar]
- Salmanov A, Vozianov S, Kryzhevsky V, Litus O, Drozdova A, Vlasenko I. Prevalence of healthcare-associated infections and antimicrobial resistance in acute care hospitals in Kyiv, Ukraine. Journal of Hospital Infection. 2019, 102, 431–437. [Google Scholar] [CrossRef]
- Hema A, Arsène Some S, Kaboré O, Sanou S, Poda A, Meda C, et al. Risk and outcomes of healthcare-associated infections in three hospitals in Bobo Dioulasso, 2 2022 (Burkina Faso): a longitudinal study Authors’ contributions. medRxiv 2024. [CrossRef]
- Yallew WW, Kumie A, Yehuala FM. Point prevalence of hospital-acquired infections in two teaching hospitals of Amhara region in Ethiopia. Drug Healthc Patient Saf 2016, 8, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Tassew SG, Alebachew Woldu M, Amogne Degu W, Shibeshi W. Management of hospital-acquired infections among patients hospitalized at Zewditu memorial hospital, Addis Ababa, Ethiopia: A prospective cross-sectional study. PLoS One 2020, 15, e0231949–e0231949. [Google Scholar] [CrossRef] [PubMed]
- Sahiledengle B, Seyoum F, Abebe D, Geleta EN, Negash G, Kalu A, et al. Incidence and risk factors for hospital-acquired infection among paediatric patients in a teaching hospital: a prospective study in southeast Ethiopia. BMJ Open 2020, 10, e037997–e037997. [Google Scholar] [CrossRef] [PubMed]
- Ali S, Birhane M, Bekele S, Kibru G, Teshager L, Yilma Y, et al. Healthcare associated infection and its risk factors among patients admitted to a tertiary hospital in Ethiopia: longitudinal study. Antimicrob Resist Infect Control 2018, 7, 2. [Google Scholar] [CrossRef] [PubMed]
- Endalafer N, Gebre-Selassie S, Kotiso B. Nosocomial bacterial infections in a tertiary hospital in Ethiopia. J Infect Prev 2010, 12, 38–43. [Google Scholar] [CrossRef]
- Atalay YA, Gebeyehu NA, Gelaw KA. The prevalence of hospital acquired infection and associated factors among patients admitted at Wolaita Sodo University Comprehensive Specialized Hospital, in Ethiopia. IP Journal of Nutrition, Metabolism and Health Science 2024, 7, 43–50. [CrossRef]
- Coulibaly Y, Kone O, Amadou I, Diop THM, Coulibaly O, Doumbia A, et al. Hospital Acquired Infections at the Service of Pediatric Surgery in Gabriel Touré Academic Hospital, Bamako, Mali. Open J Pediatr 2020, 10, 185–193. [Google Scholar] [CrossRef]
- Aminata M, Alioune BS, Yacouba C, Agaly DO, Bassirou D, Abdoulaye T, et al. Multidrug resistant bacteria isolated from nosocomial infections at University Teaching Hospital of Point-G, Bamako, Mali. African Journal of Bacteriology Research 2023, 15, 1–7. Available online: https://academicjournals.org/journal/JBR/article-abstract/39116BE70184 (accessed on 7 August 2024).
- Bocoum A, Fané S, Traoré Y, Sanogo SA, Kanté I, Kouma A, et al. Bacteriology of Healthcare-Associated Infections in the Gynecology and Obstetrics Department of CHU Gabriel Touré. Open J Obstet Gynecol 2019, 09, 1336–1346. [Google Scholar] [CrossRef]
- Kim EJ, Kwak YG, Kwak SH, Ko SH, Kweon OM, Kim ES, et al. Korean National Healthcare-associated Infections Surveillance System, Intensive Care Unit Module Report: Summary of Data from July 2019 through June 2020. Korean Journal of Healthcare-Associated Infection Control and Prevention 2021, 26, 115–128. [Google Scholar] [CrossRef]
- Kim EJ, Kwak YG, Kwak SH, Ko SH, Kweon OM, Kim ES, et al. Korean National Healthcare-associated Infections Surveillance System, Intensive Care Unit Module Report: Summary of Data from July 2020 through June 2021. Korean Journal of Healthcare-Associated Infection Control and Prevention 2023, 28, 64–77. [Google Scholar] [CrossRef]
- Kim EJ, Kwak YG, Kwak SH, Ko SH, Kim JH, Kim ES, et al. Korean National Healthcare-associated Infections Surveillance System, Intensive Care Unit Module Report: Summary of Data from July 2018 to June 2019. Korean J healthc assoc Infect Control Prev 2020, 25, 115–127. [Google Scholar] [CrossRef]
- Osman, T. Prevalence of Intensive Care Unit-Acquired Infections in different Hospitals in Khartoum State-Sudan. American Journal of PharmTech Research 2019, 9, 176–186. [Google Scholar] [CrossRef]
- Greco D, Magombe I. Hospital acquired infections in a large north Ugandan hospital. J Prev Med Hyg 2011, 52, 55–58. [Google Scholar]
- Al-Shami HZ, Al-Haimi MA. Nosocomial Infections in Six Major Hospitals in Sana’a Capital City and in Some Governorates in Yemen. Applied Microbiology: Open Access 2018, 4. [CrossRef]
- Mukomena PN, Munsaka S, Simunza M, Kwenda G, Yamba K, Kabwe J, et al. Nosocomial infections and associated risk factors at two tertiary healthcare facilities in Lusaka and Copperbelt Provinces, Zambia. Sci Afr 2023, 20, e01644. [Google Scholar] [CrossRef]
- Afroz H, Fakruddin M, Masud MR, Islam K. Incidence of and risk factors for Hospital Acquired Infection in a Tertiary Care Hospital of Dhaka, Bangladesh. Bangladesh Journal of Medical Science 2017, 16, 358–369. [Google Scholar] [CrossRef]
- Amin ZA, Nahar N. Hospital Acquired Infection in a Tertiary Military Hospital in Dhaka, Bangladesh. International Journal of Infectious Diseases and Therapy 2017, 2, 35–39. [Google Scholar]
- Nouetchognou JS, Ateudjieu J, Jemea B, Mesumbe EN, Mbanya D. Surveillance of nosocomial infections in the Yaounde University Teaching Hospital, Cameroon. BMC Res Notes 2016, 9, 505. [Google Scholar]
- Kakupa DK, Muenze PK, Byl B, Wilmet MD. Study of the prevalence of nosocomial infections and associated factors in the two university hospitals of Lubumbashi, Democratic Republic of Congo. Pan Afr Med J 2016, 24, 275. [Google Scholar]
- Razine R, Azzouzi A, Barkat A, Khoudri I, Hassouni F, Chefchaouni AC, et al. Prevalence of hospital-acquired infections in the university medical center of Rabat, Morocco. Int Arch Med 2012, 5, 26. [Google Scholar] [CrossRef] [PubMed]
- Curtis SJ, Barnabas R, Cairns KA, Cameron D, Coghlan B, Jones R, et al. Healthcare-associated infections and antimicrobial use at a major referral hospital in Papua New Guinea: a point prevalence survey. Lancet Reg Health West Pac. 2024, 48, 101120. [Google Scholar]
- Gosling R, Mbatia R, Savage A, Mulligan JA, Reyburn H. Prevalence of hospital-acquired infections in a tertiary referral hospital in northern Tanzania. Annals of Tropical Medicine & Parasitology 2003, 97, 69–73. [Google Scholar] [CrossRef]
- Ider BE, Clements A, Adams J, Whitby M, Muugolog T. Prevalence of hospital-acquired infections and antibiotic use in two tertiary Mongolian hospitals. Journal of Hospital Infection 2010, 75, 214–219. [Google Scholar] [CrossRef]
- Aiesh BM, Qashou R, Shemmessian G, Swaileh MW, Abutaha SA, Sabateen A, et al. Nosocomial infections in the surgical intensive care unit: an observational retrospective study from a large tertiary hospital in Palestine. BMC Infect Dis 2023, 23, 686. [Google Scholar]
- Faria S, Sodano L, Gjata A, Dauri M, Sabato AF, Bilaj A, et al. The first prevalence survey of nosocomial infections in the University Hospital Centre ‘Mother Teresa’ of Tirana, Albania. Journal of Hospital Infection 2007, 65, 244–250. [Google Scholar] [CrossRef]
- Tao XB, Qian LH, Li Y, Wu Q, Ruan JJ, Cai DZ, et al. Hospital-acquired infection rate in a tertiary care teaching hospital in China: a cross-sectional survey involving 2434 inpatients. International Journal of Infectious Diseases 2014, 27, 7–9. [Google Scholar] [CrossRef]
- Huang G, Huang Q, Zhang G, Jiang H, Lin Z. Point-prevalence surveys of hospital-acquired infections in a Chinese cancer hospital: From 2014 to 2018. J Infect Public Health 2020, 13, 1981–1987. [Google Scholar] [CrossRef]
- Wintaco LM, Quintero-Lesmes DC, Vargas-Soler JA, Barrera DM, Palacio LN, Granados U, et al. Analysis of Healthcare-associated Infections before and during the COVID-19 pandemic in a Colombian hospital. Revista Cuidarte 2024. [CrossRef]
- Izquierdo-Cubas F, Zambrano A, Frómeta I, Gutiérrez A, Bastanzuri M, Guanche H, et al. National Prevalence of Nosocomial Infections. Cuba 2004. Journal of Hospital Infection 2008, 68, 234–240. [Google Scholar] [CrossRef]
- Tabatabaei SM, Behmanesh Pour F, Osmani S. Epidemiology of Hospital-Acquired Infections and Related Anti-Microbial Resistance Patterns in a Tertiary-Care Teaching Hospital in Zahedan, Southeast Iran. International Journal of Infection 2015, 2. [Google Scholar] [CrossRef]
- Eshrati B, Masoumi Asl H, Afhami S, Pezeshki Z, Seifi A. Health care-associated infections in Iran: A national update for the year 2015. Am J Infect Control 2018, 46, 663–667. [Google Scholar] [CrossRef] [PubMed]
- Masoudifar M, Gouya M, Pezeshki Z, Eshrati B, Afhami S, Farzami M, et al. Health care-associated infections, including device-associated infections, and antimicrobial resistance in Iran: The national update for 2018. J Prev Med Hyg. 2022, 62, E943–9.
- Rajabi M, Abdar ME, Rafiei H, Aflatoonia MR, Abdar ZE. Nosocomial Infections and Epidemiology of Antibiotic Resistance in Teaching Hospitals in South East of Iran. Glob J Health Sci 2015, 8, 190–197. [Google Scholar]
- Choobdar F, Vahedi Z, Khosravi N, Khalesi N, Javid A, Shojaee S. Nosocomial Infection in an Iranian Neonatal Intensive Care Unit: Hospital Epidemiology and Risk Factors. Arch Pediatr Infect Dis 2020, 8. [Google Scholar] [CrossRef]
- Raka L, Spahija G, Gashi-Gecaj A, Hamza A, Haxhiu E, Rashiti A, et al. Point prevalence survey of healthcare-associated infections and antimicrobial use in Kosovo hospitals. Infect Dis Rep 2019, 11, 7975. [Google Scholar] [CrossRef]
- Azzam R, Dramaix M. A one-day prevalence survey of hospital-acquired infections in Lebanon. Journal of Hospital Infection 2001, 49, 74–78. [Google Scholar] [CrossRef]
- Daw MA, Mahamat MH, Wareg SE, El-Bouzedi AH, Ahmed MO. Epidemiological manifestations and impact of healthcare-associated infections in Libyan national hospitals. Antimicrob Resist Infect Control 2023, 12, 122. [Google Scholar] [CrossRef]
- Hughes AJ, Ariffin N, Huat TL, Molok HA, Hashim S, Sarijo J, et al. Prevalence of Nosocomial Infection and Antibiotic Use at a University Medical Center in Malaysia. Infection Control & Hospital Epidemiology 2005, 26, 100–104. [Google Scholar] [CrossRef]
- Hernández Orozco H, Lucas Resendiz E, Luis Castañeda J, De Colsa A, Ramirez Mayans J, Johnson KM, et al. Surveillance of Healthcare Associated Infections in Pediatric Cancer Patients Between 2004 and 2009 in a Public Pediatric Hospital in Mexico City, Mexico. J Pediatr Hematol Oncol 2014, 36, 96–98. [Google Scholar] [CrossRef]
- Ćirković I, Marković-Denić L, Bajčetić M, Dragovac G, Đorđević Z, Mioljević V, et al. Microbiology of Healthcare-Associated Infections: Results of a Fourth National Point Prevalence Survey in Serbia. Antibiotics (Basel) 2022, 11, 1161. [Google Scholar]
- Šuljagić V, Bajčetić M, Mioljević V, Dragovac G, Mijović B, Janićijević I, et al. A nationwide assessment of the burden of healthcare-associated infections and antimicrobial use among surgical patients: results from Serbian point prevalence survey, 2017. Antimicrob Resist Infect Control 2021, 10, 47. [Google Scholar] [CrossRef] [PubMed]
- Ilic M, Markovic-Denic L. Nosocomial infections prevalence study in a Serbian university hospital. Vojnosanit Pregl 2009, 66, 868–875. [Google Scholar] [CrossRef] [PubMed]
- Olivier C, Kunneke H, O’Connell N, Von Delft E, Wates M, Dramowski A. Healthcare-associated infections in paediatric and neonatal wards: A point prevalence survey at four South African hospitals. South African Medical Journal 2018, 108, 418. [Google Scholar] [CrossRef]
- Nair A, Steinberg WJ, Habib T, Saeed H, Raubenheimer JE. Prevalence of healthcare-associated infection at a tertiary hospital in the Northern Cape Province, South Africa. South African Family Practice 2018, 60, 162–167. [Google Scholar] [CrossRef]
- Manosuthi W, Thientong V, Moolasart V, Rongrungrueng Y, Sangsajja C, Danchaivijitr S. HEALTHCARE-ASSOCIATED INFECTIONS AT SELECTED HOSPITALS IN THAILAND. Southeast Asian J Trop Med Public Health 2017, 48, 204–212. Available online: https://pubmed.ncbi.nlm.nih.gov/29644841/ (accessed on 14 April 2024).
- Moolasart V, Srijareonvijit C, Charoenpong L, Kongdejsakda W, Anugulruengkitt S, Kulthanmanusorn A, et al. Prevalence and Risk Factors of Healthcare-Associated Infections among Hospitalized Pediatric Patients: Point Prevalence Survey in Thailand 2021. Children (Basel) 2024, 11, 738. [Google Scholar]
- Kepenekli E, Soysal A, Yalindag-Ozturk N, Ozgur O, Ozcan I, Devrim I, et al. Healthcare-Associated Infections in Pediatric Intensive Care Units in Turkey: a National Point-Prevalence Survey. Jpn J Infect Dis 2015, 68, 381–386. [Google Scholar] [CrossRef]
- World Bank country classifications by income level for 2024-2025. Available online: https://blogs.worldbank.org/en/opendata/world-bank-country-classifications-by-income-level-for-2024-2025 (accessed on 8 August 2024).
- Kärki T, Plachouras D, Cassini A, Suetens C. Burden of healthcare-associated infections in European acute care hospitals. Wien Med Wochenschr 2019, 169 (Suppl. 1), 3–5. Available online: https://pubmed.ncbi.nlm.nih.gov/30680486/. [CrossRef]
- Magill SS, Edwards JR, Bamberg W, Beldavs ZG, Dumyati G, Kainer MA, et al. Multistate point-prevalence survey of health care-associated infections. N Engl J Med 2014, 370, 1198–1208. [Google Scholar] [CrossRef]
- Raoofi S, Pashazadeh Kan F, Rafiei S, Hosseinipalangi Z, Noorani Mejareh Z, Khani S, et al. Global prevalence of nosocomial infection: A systematic review and meta-analysis. PLoS One. 2023, 18, e0274248. [Google Scholar]
- Goh LPW, Marbawi H, Goh SM, Bin Abdul Asis AK, Gansau JA. The prevalence of hospital-acquired infections in Southeast Asia (1990-2022). The Journal of Infection in Developing Countries 2023, 17, 139–146. [Google Scholar] [CrossRef] [PubMed]
- Bunduki GK, Masoamphambe E, Fox T, Musaya J, Musicha P, Feasey N. Prevalence, risk factors, and antimicrobial resistance of endemic healthcare-associated infections in Africa: a systematic review and meta-analysis. BMC Infect Dis. 2024, 24, 158. [Google Scholar]
- Gomaa K, Abdelraheim AR, El Gelany S, Khalifa EM, Yousef AM, Hassan H. Incidence, risk factors and management of post cesarean section surgical site infection (SSI) in a tertiary hospital in Egypt: a five year retrospective study. BMC Pregnancy Childbirth 2021, 21. Available online: /pmc/articles/PMC8449867/. (accessed on 15 April 2024). [Google Scholar]
- Lansing SS, Moley JP, McGrath MS, Stoodley P, Chaudhari AMW, Quatman CE. High Number of Door Openings Increases the Bacterial Load of the Operating Room. Surg Infect (Larchmt) 2020/12/23. 2021, 22, 684–689. [Google Scholar] [CrossRef]
- Romano F, Milani S, Gustén J, Joppolo CM. Surgical Smoke and Airborne Microbial Contamination in Operating Theatres: Influence of Ventilation and Surgical Phases. Int J Environ Res Public Health 2020, 17, 5395. [Google Scholar] [CrossRef]
- Healthcare-associated infections. Available online: https://www.ecdc.europa.eu/en/healthcare-associated-infections (accessed on 6 August 2024).
- Leistner R, Kohlmorgen B, Brodzinski A, Schwab F, Lemke E, Zakonsky G, et al. Environmental cleaning to prevent hospital-acquired infections on non-intensive care units: a pragmatic, single-centre, cluster randomized controlled, crossover trial comparing soap-based, disinfection and probiotic cleaning. EClinicalMedicine. 2023, 59, 101958. [Google Scholar] [CrossRef]
- Dancer, SJ. Cleaning and decontamination of the healthcare environment. In Decontamination in Hospitals and Healthcare; Elsevier: Amsterdam, The Netherlands, 2014; pp. 370–97. [Google Scholar]
- Umscheid CA, Mitchell MD, Doshi JA, Agarwal R, Williams K, Brennan PJ. Estimating the Proportion of Healthcare-Associated Infections That Are Reasonably Preventable and the Related Mortality and Costs. Infect Control Hosp Epidemiol. 2011, 32, 101–114. [Google Scholar] [CrossRef]
- Boyce, JM. Modern technologies for improving cleaning and disinfection of environmental surfaces in hospitals. Antimicrob Resist Infect Control. 2016, 5, 10. [Google Scholar] [CrossRef]
- Kubde D, Badge AK, Ugemuge S, Shahu S. Importance of Hospital Infection Control. Cureus 2023. [Google Scholar]
- NHSN | CDC. Available online: https://www.cdc.gov/nhsn/index.html (accessed on 6 August 2024).
Figure 4.
Pooled prevalence of HAIs in LMICs.
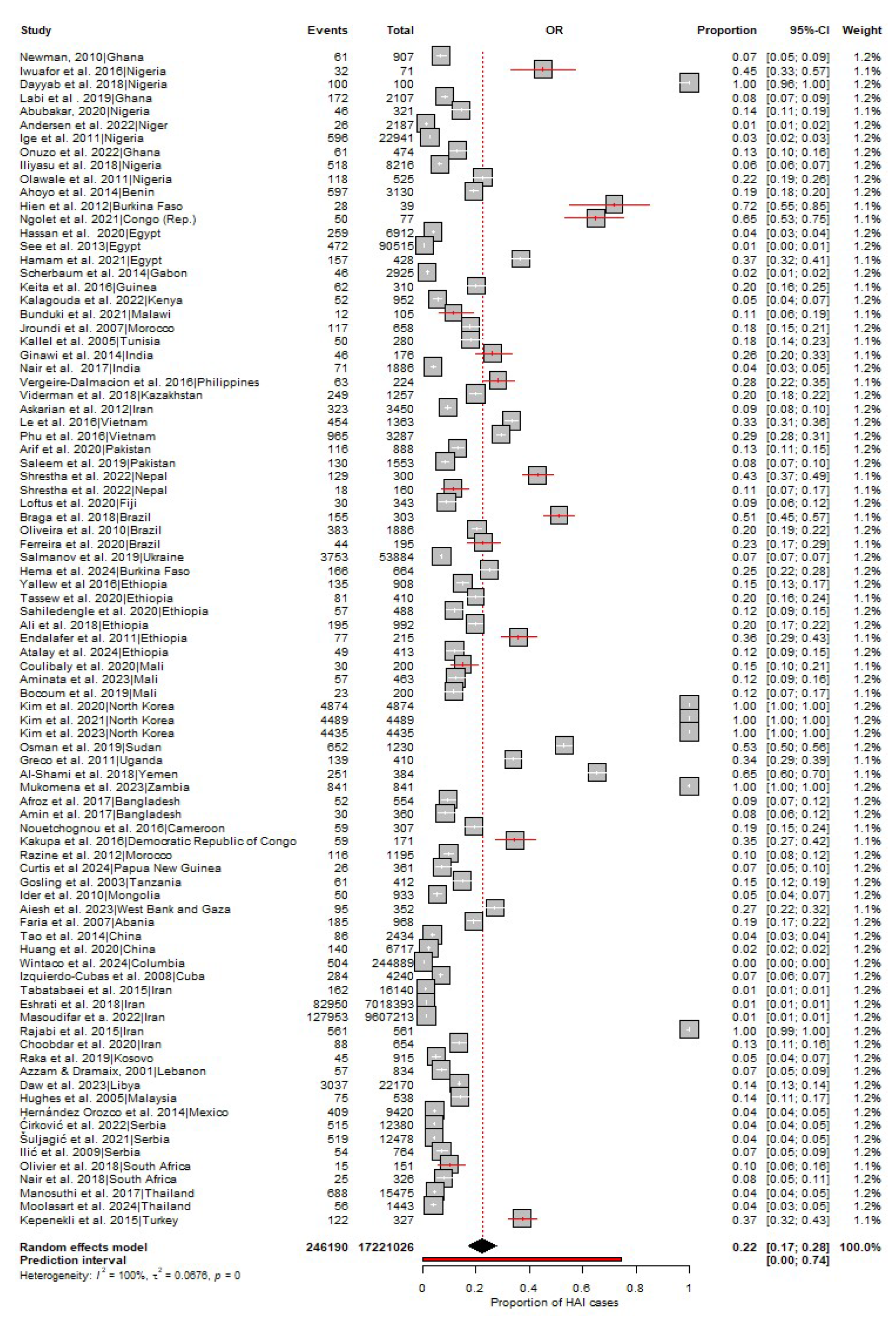

Table 1.
Subgroup analysis according to WHO region and World Bank income level (2024/2025).
| Variable | Prevalence (95% CI) | I2 | p value |
|---|---|---|---|
| WHO region | |||
| SEAR | 37% (13-62) | 100% | 0 |
| AFR | 25% (16-33) | 100% | 0 |
| EMR | 19% (6-31) | 100% | 0 |
| AMR | 17% (3-32) | 100% | 0 |
| WPR | 15% (7-23) | 100% | 0 |
| EUR | 14 % (5-23) | 99% | <0.01 |
| World Bank income level (2024/2025) | |||
| Low-Income | 37% (23-52) | 100% | 0 |
| Lower-Middle Income | 22% (15-30) | 100% | 0 |
| Upper-Middle Income | 13% (6-20) | 100% | 0 |
Table 2.
Subgroup analysis according to HAI type.
| HAI | No. of countries | No. of studies | No. of cases | Prevalence (95% CI) | I2 | p- value |
|---|---|---|---|---|---|---|
| SSIs | 43 | 70 | 44312 | 27% (23-31) | 99% | 0 |
| Pneumonia | 27 | 41 | 62633 | 23% (18-28) | 99% | 0 |
| UTIs | 46 | 77 | 65505 | 22% (19-26) | 99% | 0 |
| BSIs | 40 | 65 | 33731 | 21% (16-25) | 99% | 0 |
| LRTIs | 20 | 26 | 1211 | 19% (13-25) | 98% | <0.01 |
| SSTIs | 24 | 33 | 812 | 10% (6-13) | 95% | <0.01 |
| GIs | 16 | 19 | 174 | 6% (3-9) | 88% | <0.01 |
lower respiratory tract infections (LRTIs), skin and soft tissue infections (SSTIs).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



