
Submitted:
27 September 2024
Posted:
30 September 2024
You are already at the latest version
Abstract
The aims of the study were to analyze the relationship between the Mediterranean diet (MD) and arterial stiffness and metabolic syndrome (MetS) and its components in individuals aged over 65, overall and by sex. Subjects were people over 65 years of age with a full record of all variables analyzed from the EVA, MARK and EVIDENT studies. Data from 1,280 subjects with a mean age of 69.52±3.58 years (57.5% men) were analyzed. MD was recorded with the validated 14-item MEDAS questionnaire used in the PREDIMED study. MetS was defined following the guidelines of the joint scientific statement from the Programa Nacional de Educación sobre el Colesterol III. Arterial stiffness was assessed with the VaSera VS-1500® device by measuring the cardio-ankle vascular index (CAVI) and the brachial-ankle pulse wave velocity (baPWV). Results: The mean MEDAS score was 6.00 ± 1.90, (5.92 ± 1.92 in men, 6.11 ± 1.88 in women; p = 0.036). The mean CAVI value was 9.30 ± 1.11 (9.49 ± 1.05 men, 9.03 ± 1.13 women; p = <0.001). The mean baPWV value was 15.82 ± 2.56 (15.75 ± 2.46 men, 15.92 ± 2.68 women; p = <0.001). MetS was found in 51% (49% men, 54% women; p = 0.036). Subjects with MetS had lower MD adherence and higher arterial stiffness values than subjects without MetS. Overall, we found a negative association of MD score with the number of MetS components (β = -0.168), with glycemia (β = -0.007), triglycerides (β = -0.003), waist circumference (β = -0.018), CAVI (β = -0.196) and baPWV (β = -0.065), and a positive association with HDL cholesterol (β = 0.013). By sex, associations followed the same direction but without reaching statistical significance with blood glucose and triglycerides in women and with HDL cholesterol and waist circumference in men. Conclusion: Results indicate that greater adherence to the Mediterranean diet decreases arterial stiffness and the percentage of subjects with MetS, although results differed in the association with MetS components by sex.
Keywords:
Mediterranean diet
; metabolic syndrome
; brachial-ankle pulse wave velocity
; cardio-ankle vascular index
; arterial stiffness
1. Introduction
Nutrition contributes to human health up to the final stages of life [1,2]. The health benefits of the Mediterranean diet (MD) are well supported by scientific evidence, especially in people aged over 65 [3,4,5,6]. The MD is based on the traditional dietary patterns of Mediterranean countries [7,8] and is a pattern is rich in fresh foods such as: fruits, vegetables, legumes, whole grains and nuts, all rich in fiber and antioxidants that improve cellular aging [9,10,11]. In people over 65, consuming MD components as part of a regular dietary pattern contributes to healthy aging [12,13,14] and plays a positive role in muscle function [15], in the prevention of depression [16], cardiovascular diseases (CVD) [17,18,19], type 2 diabetes[20], hypertension [21], obesity [22], in improving the lipid profile [23], in preventing cognitive decline and the risk of Alzheimer's disease [24] and certain types of cancer [25]. It reduces morbidity, mortality [26] and fragility [27], and improves the quality of life [5]. For all these reasons, the MD was proclaimed a UNESCO Intangible Cultural Heritage in 2010 as a way of life that can increase hope and quality of life. [28].
Arterial stiffness (AS) involves the loss of elasticity of the arteries, reducing the arterial wall’s ability to stretch and contract [29,30]. As a risk predictor for cardiovascular disease (CVD), AS is similar to or stronger than other traditional cardiovascular risk factors [31]. Thus, measured non-invasively by oscillometry, with both brachial-ankle pulse wave velocity (baPWV) [32,33] and cardio-ankle vascular index (CAVI) [34,35], AS has shown a positive association with CVD. While AS is mainly determined by age, sex and blood pressure [29,31], the relationship with MD is unclear. Some studies have suggested that MD may not function as an independent risk factor for AS [36], while others have shown that MD may help maintain arterial elasticity and is effective in improving cardiovascular health with clinically relevant reductions in blood pressure and AS [21].
Metabolic syndrome (MetS) is a combination of multiple risk factors for arterial atherosclerosis, such as abdominal obesity, high blood pressure, high fasting plasma glucose (FPG) and atherogenic dyslipidemia [37]. MetS doubles CVD morbidity and mortality and carries a 1.5 times higher risk of all-cause mortality [38,39,40]. Greater fast food consumption, less time spent exercising and increased sedentary behavior during leisure time have led to the growing incidence of MetS [41]. In the over 65s, MetS is more prevalent in women, with figures ranging from 35% to 50%; for men these figures lie between 25% and 40%, and prevalence differs depending on the criteria used to define MetS. This is reflected in several studies [42], among them one carried out in Singapore with 722 adults aged 65 years or over, which found a 41% prevalence of MetS as well as a 50% prevalence in those aged 85 years or older, higher in women than in men. [43]. On the other hand, the ENRICA study [44] found that the Mediterranean lifestyle was linked to a lower frequency of MetS and lower all-cause mortality in Spain, while a further study indicated that participants with MetS have a pro-inflammatory dietary pattern and lower MD adherence, with lower intake of carbohydrates and dried fruits and nuts and a higher intake of protein, saturated fatty acids, cholesterol, red and processed meat products, and use of oils other than olive oil [45]. However, the effect of MD on AS, MetS and each of its components has not been fully established in Caucasians aged over 65. The objectives of this study were therefore: to analyze the relationship of MD with AS, assessed with CAVI and baPWV, and with MetS and its components in Caucasians over 65 years of age, overall and by sex.
2. Materials and Methods
2.1. Type of Study
2.2. Study Population
The three studies were performed in primary care. For the present study, data was used from 1,280 subjects aged over 65 with a full record of all the variables analyzed. The EVA study, in which selection was by random sampling of the urban population of 5 health centers without prior CVD at the start of the study (reference population of 43,946), contributed 135 of its 501 subjects [46]. From the MARK study, where selection was made by random sampling among patients attending primary care consultations in 7 urban health centers and presenting intermediate cardiovascular risk, 948 of its 2511 subjects were incorporated. The EVIDENT study provided 195 of its 1104 subjects. In that study, selection was made following random sampling among patients attending a primary care center. Figure 1 shows the selection of subjects by origin.
2.3. Ethics Committee and Participant Consent
The studies included in this analysis were approved by the Drug Research Ethics Committee of Salamanca on the following dates: the EVA study [46] at the meeting of May 4, 2015, the MARK study [47] at the meeting of December 3, 2013 and the EVIDENT study [48] at the meeting of April 25, 2016. All participants signed written consent before being included in the study. The guidelines of the Declaration of Helsinki [49] and the WHO for observational studies were followed during all phases of the study.
2.4. Variables and Measurement Methods
2.4.1. Mediterranean Diet
MD adherence was assessed using the 14-item MEDAS screener, validated in the Spanish adult population [50]. This questionnaire comprises 12 questions regarding the frequency of food consumption and 2 items on eating habits. The questions were scored with zero or one point. A point was given for daily consumption of (a) ≥ 4 tablespoons of olive oil, (b) ≥ 2 servings of vegetables, (c) ≥ 3 pieces of fruit, (d) < 1 serving of red or processed meat, (e) < 1 serving of animal fat, (f) < 1 cup of sugary carbonated drinks, (g) eating white meat in greater proportion to red meat. A point was also scored for weekly consumption of (a) ≥ 7 glasses of wine, (b) ≥ 3 servings of legumes, (c) ≥ 3 servings of fish, (d) ≥ 3 servings of nuts or dried fruit, (e) ≥ 2 servings of sofrito (a home-made sauce of onions and/or garlic and tomatoes, sautéed in extra-virgin olive oil), and (f) < 2 baked goods. The final score range ranged from 0 to 14 points. We considered MD adherence for scores above 6 points, the median [50].
2.4.2. Metabolic Syndrome
2.4.3. Arterial Stiffness
The CAVI and baPWV stiffness parameters were measured with the VaSera VS-1500 device (Fukuda Denshi Co, Ltd, Tokyo, Japan), following the manufacturer's instructions. Measurements were made with the patient in a supine position, after 5 minutes of rest and not drinking alcohol or smoking in the previous 10 minutes, in a quiet room and without speaking during the duration of the examination. The electrodes were placed on both arms and both legs. A cardiac microphone was placed on the sternum in the second intercostal space, secured with adhesive tape. The device estimated the CAVI value automatically by substituting the stiffness parameters using the following equation: stiffness parameter β=2 ρ×1/(Ps–Pd)×ln (Ps/Pd)×PWV2, where ρ is blood density, Ps and Pd are SBP and DBP in mmHg, and PWV is measured between the aortic valve and the ankle. CAVI measurements were considered valid when at least 3 consecutive heartbeats were obtained [51]. The baPWV was estimated using the following equation: baPWV=((0.5934×height(cm)+14.4724))/tba, where tba is the time interval between arm and ankle waves.
2.4.4. Cardiovascular Risk Factors
Weight was measured twice with approved and calibrated (accuracy ± 0.1 kg) electronic scales (Seca 770; Medical Scales and Measurement Systems, Birmingham, UK), with the participant lightly dressed and barefoot, and the measurement rounded to the nearest 100 g. Height was measured with a portable stadiometer (Seca 222; Medical Scales and Measurement Systems, Birmingham, UK), with the participant standing barefoot and the average of two readings being recorded. The body mass index (BMI) was estimated as weight (kg) divided by height (m) squared. WC was measured following the recommendations of the Spanish Society for the Study of Obesity [52].
Three measurements of systolic blood pressure (SBP) and diastolic blood pressure (DBP) were taken, with the average of the last two recorded, using a validated OMRON model M10-IT sphygmomanometer (Omron Health Care, Kyoto, Japan), following the recommendations of the European Society of Hypertension [53]. Participants were considered to have hypertension if taking antihypertensive medication or had blood pressure levels ≥ 140/90 mmHg, to be diabetic if taking hypoglycemic drugs or having fasting plasma glucose levels ≥ 126 mg/dl or HbA1c levels ≥ 6.5%, and to have dyslipidemia if taking lipid-lowering drugs or having fasting total cholesterol levels ≥ 240 mg/dl, low-density lipoprotein cholesterol (LDL-c) ≥ 160 mg/dl, high-density lipoprotein cholesterol (HDL-c) < 40 mg/dl in men and < 50 mg/dl in women, or triglycerides ≥ 150 mg/dl. Subjects were considered obese if they had BMI levels ≥ 30 kg/m2 [54].
2.5. Statistical Analysis
Continuous variables are shown as mean ± standard deviation. Categorical variables are shown as number and percentage. Differences between sexes or between subjects with and without MetS were calculated with the chi-square test for percentages and Student's t test for continuous variables.
To calculate the association between the mean MD score and the number of MetS components (as well as with each component individually) and AS, eight multiple linear regression models were performed (ENTER method), with the MD score as independent variable, and the number of MetS components, SBP and DBP in mmHg, FPG in mg/dl, triglycerides in mg/dl, HDL cholesterol in mg/dl, WC in cm, CAVI and baPWV in m/sec as dependent variables.
To estimate the association between MD adherence and the presence of MetS, its components, CAVI and baPWV, eight logistic regression models were performed. Adherence to MD was the independent variable (encoded as MD adherence = 1, non-adherence = 0). Dependent variables were MetS (yes = 1, no = 0), BP ≥ 130/85 mmHg (yes = 1, no = 0), FPG ≥ 100 mg/dl (yes = 1, no = 0), TGC ≥ 150 mg/dl (yes = 1, no = 0), HDL-C mg/dl < 40 men, < 50 women (yes = 1, no = 0) and WC ≥ 88 cm women, ≥ 102 cm men (yes = 1, no = 0). In all models, age, sex and consumption of antihypertensive drugs (yes = 1, no = 0), hypoglycemic drugs (yes = 1, no = 0) and lipid-lowering drugs (yes = 1, no = 0) were included as adjustment variables.
Analyses were performed overall, by sex, and in subjects with and without MetS. The program used to perform the analysis was SPSS Statistics for Windows, version 28.0 (IBM Corp, Armonk, NY, USA). We used a p value < 0.05 as the limit for statistical significance.
3. Results
3.1. Participant Characteristics
Table 2 shows the variables analyzed overall and differences by sex. The mean MEDAS questionnaire score was 6.00 ± 1.90, (5.92 ± 1.92 men, 6.11 ± 1.88 women; p = 0.036). The mean CAVI value was 9.30 ± 1.11 (9.49 ± 1.05 men, 9.03 ± 1.13 women; p < 0.001). Mean baPWV was 15.82 ± 2.56 (15.75 ± 2.46 men, 15.92 ± 2.68 women; p < 0.001). Mets was found in 51% (49% men, 54% women; p = 0.036). Men had a higher percentage of the following MetS components: blood pressure ≥ 130/85 mmHg (87% vs 81%) and FPG (45% vs 38%) than women. Women presented a higher percentage of the following MetS components: HDL-C (35% vs 16%), WC (76% vs 52%) than men.
Table 3 shows the variables analyzed in subjects with and without MetS, as well as the differences between them. Subjects with MetS had lower MD adherence (35% vs 54%; p = 0.002). Subjects with MetS presented higher baPWV values (16.15 ± 2.58 vs 15.47 ± 2.49; p < 0.001), with no difference in CAVI (p = 0.200).
Table S1 (men) and Table S2 (women) in supplementary material reflect the variables studied in men and women with and without MetS, as well as the differences between them. We found no differences in the percentage of men with MD adherence (p=0.176). Men with MetS presented higher baPWV values (15.96 ± 2.33 vs 15.55 ± 2.38; p = 0.025), with no difference in CAVI (p = 0.486). Women with MetS showed lower MD adherence (33% vs 48%; p < 0.001). Women with MetS presented higher baPWV values (16.39 ± 2.63 vs 15.36 ± 2.64; p < 0.001), with no difference in CAVI (p = 0.077).
Figure 2 shows the number of MetS components, overall (a), in men (b) and in women (c).
Figure 3 shows the difference in MD scores between subjects with and without MetS and the different MetS components, overall and by sex.
3.2. Association between the Mediterranean Diet and Arterial Stiffness and MetS in People over 65 Years of Age
Table 4 shows the association found between the mean MEDAS screener score and the number of components of MetS, the components included in the definition of MetS, and the AS values, overall and by sex. In the overall analysis, the mean MD score showed a negative association with the number of MetS components (β = -0.168, 95% CI: -0.269 to -0.068) and with the following MetS components: FPA (β = -0.007; 95% CI: -0.012 to -0.003), TGC (β = -0.003; 95% CI: -0.005 to -0.002), WC (β = -0.018; 95% CI: -0.028 to -0.008), and with AS values: CAVI (β = -0.196; 95% CI: -0.294 to -0.099) and baPWV (β = -0.065; 95% CI: -0.107 to -0.060), and a positive association with level of HDL-C (β = 0.013; 95% CI: 0.006 to 0.020). In men, the mean MD score was negatively associated with the number of MetS components (β = -0.181, 95% CI: -0.307 to -0.056) and with the following MetS components: FPA (β = -0.011; 95% CI: -0.016 to -0.005), TGC (β = -0.004; 95% CI: -0.006 to -0.002), and with AS values: CAVI (β = -0.230; 95% CI: -0.363 to -0.097) and baPWV (β = -0.099; 95% CI: -0.155 to -0.043). In women, the mean MD score was negatively associated with WC (β = -0.026; 95% CI: -0.040 to -0.012), with the CAVI (β = -0.150; 95% CI: -0.293 to -0.008), and positively associated with levels of HDL-C (β = 0.017; 95% CI: 0.008 to 0.027).
Table 5 presents overall and sex-based logistic regression results. Overall, the adjusted logistic regression models showed that greater MD adherence reduced the likelihood of MetS (OR = 0.675, 95% CI: 0.528 to 0.864) and its components: FPA ≥ 100 mg/dl (OR = 0.640, 95% CI: 0.477 to 0.859); TGC ≥ 150 mg/dl (OR = 0.744, 95% CI: 0.566 to 0.986);
CAVI (OR = 0.835, 95% CI: 0.749 to 0.931), baPWV (OR = 0.939, 95% CI: 0.896 to 0.984), and increased the likelihood of having HDL-C < 40 mg/dl in men or < 50 mg/dl in women (OR = 1.749, 95% CI: 1.305 to 2.326). In men, increased MD adherence reduced the likelihood of TGC ≥ 150 mg/dl (OR = 0.609, 95% CI: 0.417 to 0.891); CAVI (OR = 0.825, 95% CI: 0.711 to 0.957) and baPWV (OR = 0.924, 95% CI: 0.867 to 0.958), and increased the probability of HDL-C < 40 mg/dl (OR = 1.665, 95% CI: 1.082 to 2.563). In women, adjusted logistic regression models showed that higher MD adherence decreased the likelihood of MetS (OR = 0.605, 95% CI: 0.410 to 0.895) and its components: FPA ≥ 100 mg/dl (OR = 0.604, 95% CI: 0.376 to 0.971) and CAVI (OR = 0.841, 95% CI: 0.713 to 0.991) and increased the likelihood of HDL-C < 50 mg/dl (OR = 1.792, 95% CI: 1.221 to 2.632).
4. Discussion
In this study of subjects aged over 65 years, we found that four out of six people adhered to the Mediterranean diet, with a higher MD score in women, and one out of two subjects presented metabolic syndrome, with a higher percentage in women. The association between MD and arterial stiffness and the number of components of MetS and its components was negative, except with the blood pressure figures, for which we found no association, and with HDL-cholesterol, for which the association was positive. Finally, the association differed by sex.
In line with previous studies, MD adherence was higher in women than in men [55,56,57,58]. With regard to metabolic syndrome, the figure diagnosed with MetS was 51%, a result which is lower than that published in Hispanics aged over 60 in the USA (57%) [59] and higher than those published in China, 39% [60], or Iran, 37% [61]. The ENRICA study in Spain [57] analyzed 11,149 people representative of the Spanish population aged over 18, finding a prevalence in those aged 65 or older of 42%. The DARIOS study [58], with 24,670 people between 35 and 74 years of age from ten autonomous communities found a prevalence of MetS in people aged 65 or over of 47%, with a higher percentage of women with MetS than men (49% men, 54% women, p = 0.036). This is in line with other research on people over 65 years of age, such as the ENRICA study [57] (39% men and 44% women) and in the DARIOS study [58] (42% men, 52% women). However, in the USA no differences were found between men and women in this age group [59]. The frequency of MetS components differed in men and women. Men had a higher percentage of the following MetS components: blood pressure ≥ 130/85 mmHg (87% vs 81%) and plasma glucose (45% vs 38%) than women. Women had a higher percentage of HDL-C (35% vs 16%) and WC (76% vs 52%) than men, results which are similar to those published by other authors [57,58,62]. However, it should not be forgotten that the prevalence of MetS varies greatly depending on geographical area, age, sex. Comparing these results therefore has important limitations, and should be read with caution.
In the overall analysis, this study showed a link between MD and MetS and its components, except for blood pressure. These results are consistent in the analyses by both multiple and logistic regression. In the elderly Spanish population, an inverse relationship was found between MD adherence and the prevalence of MetS [63]. In the PREDIMED-PLUS study [45], which involved 5,739 overweight/obese participants aged 55-75 years, it was found that participants with MetS had lower MD adherence. However, in a study of 1,404 adults in Luxembourg, an association of MD with MetS was found when MD was used as a continuous score, but this association disappeared when MD was used as a categorical variable [64]. In Hassani et al. [65], MD adherence was not associated with MetS. However, some prospective studies that have investigated the impact of different interventions analyzing the effect of MD on MetS did find benefits. This was demonstrated, for example, by a clinical trial with a three-month dietary intervention based on salt restriction and MD which achieved a decrease in the prevalence of MetS compared to the control group [66]. Similarly, in a recently published review, Martemucci et al. [67], showed that MD adherence together with increased physical activity were appropriate complementary approaches to preventing the onset of MetS. There are also longitudinal studies which have analyzed the importance of different Mediterranean lifestyle elements measured with MD adherence (MEDLIFE), with a 5-year follow-up of participants in the CORDIOPREV study finding a lower incidence of MetS and a greater likelihood of reversing MetS compared to the group with low adherence to MEDLIFE [68]. At 8.7 years of follow-up in the ENRICA study cohort, a Mediterranean lifestyle assessed with the MEDLIFE index was associated with a lower incidence of MetS [44]. However, these studies did not analyze the individual effect of each item, but rather the combined, and possibly synergistic, effects of several behaviors related to Mediterranean culture. Further prospective studies are therefore needed to study the effect that each MD component has on MetS.
In this study, we found an association between MD and all the components of MetS, apart from blood pressure. Several studies have analyzed the relationship between MD and the components of MetS, with different results. For example, a logistic regression analysis showed that poor MD adherence was linked to higher WC (OR 1.31) and higher triglyceride levels (OR 2.80) after adjusting for several possible confounding factors [69]. A meta-analysis found that the greater the adherence to MD, the lower the WC (β = -0.20) and the level of triglycerides (β = -0.27) and the higher the level of HDL-C (β = 0.28), without an association with glycemia or blood pressure [70]. On the other hand, of the MD components, higher consumption of vegetables, legumes and nuts were associated with lower all-cause mortality, while higher vegetable intake was associated with lower cardiovascular mortality, and higher red/processed meat intake was associated with higher cardiovascular mortality in participants with MetS [71]. In sum, high MD adherence can improve the different components making up MetS. However, this may differ from one component to another, probably explained by the heterogeneity of the studies in terms of subjects included, analyses performed, associated pathologies or concomitant treatments. Further research in this field is therefore necessary.
In the analysis by sex, we found that MD was associated with glycemia and triglycerides in men, while in women there was an association of MD with HDL-C and WC. These associations differ from other studies, such as the one carried out by Hassani et al. [65], which only demonstrated an association of MD with fasting blood glucose (OR: 0.57) and with abdominal obesity (OR: 0.42) in women. A review of studies on menopausal women concluded that MD had a beneficial effect on women's health, leading to a reduction in weight, blood pressure, triglycerides and total cholesterol [72]. Thus, the association of MD with different MetS components differs by sex, and to date, few studies have analyzed this aspect, so more research is needed to clarify the influence of MD on each of the components by sex.
In the overall analysis we found that a higher score on the MEDAS questionnaire was associated with lower AS assessed with CAVI and baPWV. Similar results have been found in previous studies [73,74]. Along these lines, the NU-AGE clinical trial [35] found that MD decreased AS. The trial conducted by the American College of Physicians concluded that MD could lead to a regression of aortic stiffness [77]. However, the EVasCu study [37] showed that subjects with greater MD adherence had higher AS, although this difference disappeared after adjusting for age. In the RoCAV study [75], which analyzed the association between MD and AS assessed with cfPWV in 2,640 participants without chronic diseases at the time of recruitment, no association was found. Finally, one study found a negative association between MD and increased CAVI at five years [76]. The discrepancies between the results of the different studies may be understood in the sense that as people age, they tend to have more health problems and adopt healthier dietary patterns accordingly. In addition, arteries lose elasticity with age, increasing AS [29,30]. This may lead to a decrease in the age-related benefits of MD. Thus, in older people, age may act as a confounding variable in the association between MD and AS.
In the analysis by sex, the association of MD with baPWV held only in men. Few studies have analyzed such differences between men and women, and different results were found. Thus, the NU-AGE study [21] did not observe any effect of the intervention on cfPWV. These discrepancies between sexes could be explained by the fact that women have higher MD scores than men [55,56,57,58]. In addition, epigenetic and molecular changes cause an increase in AS and reduce adherence, differing according to sex [29,30,77], all of which is combined with the fact that the differences between sexes in AS are influenced by hormonal and non-hormonal factors [78]. For example, the protection of endogenous estrogens until menopause in women is well known. Meanwhile, in men, AS increases linearly from puberty onwards, indicating that women inherently have stiffer main arteries than men, an effect which is mitigated by sexual steroids during reproductive life. Finally, height, body fat and other inflammatory factors differ by sex [78]. Further variation is also due the fact that the stiffness measures used to assess different parts of the vascular tree also different, with baPWV assessing peripheral AS, while CAVI is a measure of central and peripheral AS [79].
Limitations and strengths: This study has important limitations: 1. It is a cross-sectional study, and causality cannot therefore be established; 2. The data analyzed come from three research studies, with different participant characteristics; 3. The origin of the participants from the urban population prevents generalization of results to the rural population; 4. The use of a cut-off point for MD adherence is arbitrary; 5. The data on MD consumption was recorded with questionnaires. Neverthless, the study also has some strengths, which include: the large sample size, the use of a standardized protocol for carrying out measurements, the fact that the researchers who performed them had prior training, and that measurements were made with validated and calibrated devices.
5. Conclusions
The results yielded by this study indicate that greater adherence to the Mediterranean diet decreases AS and the percentage of subjects with MetS, although results differ in the associations found with MetS components according to sex.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Table S1: Characteristics of the subjects included with and without MetS in men; Table S2: Characteristics of the subjects included with and without MetS in women.
Author Contributions
Conceptualization, L.G.-S., M.G.-S., M.A.G.-M. and E.R.-S.; methodology, M.A.G.-M., L.G. O. and E.R.-S., formal analysis, M.A.G.-M. and L.G.-O.; investigation, L.G.-S., M.G.-S., C.L.-S., C.A.-C. and S.G.-S.; data curation, M.A.G.-M. and E.R.-S.; writing—original draft preparation, L.G.-S. and M.G.-S.; writing—review and editing, project administration, M.A.G.-M., L.G.-O. and E.R.-S., funding acquisition, M.A.G.-M. and L.G.-O. All authors have read and agreed to the published version of the manuscript.
Funding
This study was funded by the Regional Health Management of the Junta de Castilla y León through a research project (GRS 1193/B/15), by the Carlos III Health Institute (ISCIII), by project RD21/0016/0010 of the RICAPPS research network (Red de Investigación en Cronicidad, Atención Primaria y Promoción de la Salud), and co-funded by Next Generation EU funds through the ERDF Recovery and Resilience Mechanism (RRM), and through project PI21/00454 funded by the Carlos III Health Institute (ISCIII) and co-funded by the European Union. Human resources were also obtained through the Castilla y León government research program (INT/M/02/17 and INT/M/04/15), from the biomedical research institute of Salamanca (IBSAL) (IBI21/00001) and the Carlos III Health Institute (INT22/00007). None played any role in the study design, data analysis, reporting of results, or the decision to submit the manuscript for publication.
Institutional Review Board Statement
All personnel involved in this study were trained before the 445 study began. This study was approved by the ethics committee of the Salamanca Health Area Drug 446 Research Ethics Committee. Informed Consent Statement:.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data supporting the findings of this study are available on ZENODO under the DOI doi: 10.5281/zenodo.12166167. 451.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Rodríguez-Mañas, L.; Moreno-Villares, J.M.; Álvarez Hernández, J.; Romero Secín, A.A.; López Díaz-Ufano, M.L.; Suárez González, F.; Costa-Grille, A.; López-Miranda, J.; Fernández-Garcia, J.M. Awareness and Self-Reported Knowledge and Training on Nutrition in Older People among Primary Care Practitioners. J Frailty Aging 2024, 13, 157–162. [Google Scholar] [CrossRef] [PubMed]
- Chin, S.; Wong, R.; Hirani, V.; O'Leary, F. Nutrition knowledge assessment tools for older adults and their carers: a scoping review. Nutr Res Rev 2023, 36, 216–231. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.; Schupf, N.; Cruz, E.; Stern, Y.; Mayeux, R.P.; Gu, Y. Association Between Mediterranean Diet and Functional Status in Older Adults: A Longitudinal Study Based on the Washington Heights-Inwood Columbia Aging Project. J Gerontol A Biol Sci Med Sci 2022, 77, 1873–1881. [Google Scholar] [CrossRef] [PubMed]
- Coelho-Júnior, H.J.; Trichopoulou, A.; Panza, F. Cross-sectional and longitudinal associations between adherence to Mediterranean diet with physical performance and cognitive function in older adults: A systematic review and meta-analysis. Ageing Res Rev 2021, 70, 101395. [Google Scholar] [CrossRef]
- Apostolaki, I.; Pepa, A.; Vlassopoulos, A.; Kapsokefalou, M. Social Capital and Self-Perceived Quality of Life-Interrelated Predictors of Mediterranean Diet Adherence in Older Adults. Nutrients 2021, 13. [Google Scholar] [CrossRef]
- Zaragoza-Martí, A.; Ferrer-Cascales, R.; Hurtado-Sánchez, J.A.; Laguna-Pérez, A.; Cabañero-Martínez, M.J. Relationship between Adherence to the Mediterranean Diet and Health-Related Quality of Life and Life Satisfaction among Older Adults. J Nutr Health Aging 2018, 22, 89–96. [Google Scholar] [CrossRef]
- Román, G.C.; Jackson, R.E.; Reis, J.; Román, A.N.; Toledo, J.B.; Toledo, E. Extra-virgin olive oil for potential prevention of Alzheimer disease. Rev Neurol (Paris) 2019, 175, 705–723. [Google Scholar] [CrossRef]
- Kiani, A.K.; Medori, M.C.; Bonetti, G.; Aquilanti, B.; Velluti, V.; Matera, G.; Iaconelli, A.; Stuppia, L.; Connelly, S.T.; Herbst, K.L. , et al. Modern vision of the Mediterranean diet. J Prev Med Hyg 2022, 63, E36–e43. [Google Scholar] [CrossRef]
- Trichopoulou, A.; Martinez-Gonzalez, M.A.; Tong, T.Y.; Forouhi, N.G.; Khandelwal, S.; Prabhakaran, D.; Mozaffarian, D.; de Lorgeril, M. Definitions and potential health benefits of the Mediterranean diet: views from experts around the world. BMC Med 2014, 12, 112. [Google Scholar] [CrossRef]
- Martini, D. Health Benefits of Mediterranean Diet. Nutrients 2019, 11. [Google Scholar] [CrossRef]
- Rees, K.; Takeda, A.; Martin, N.; Ellis, L.; Wijesekara, D.; Vepa, A.; Das, A.; Hartley, L.; Stranges, S. Mediterranean-style diet for the primary and secondary prevention of cardiovascular disease. Cochrane Database Syst Rev 2019, 3, Cd009825. [Google Scholar] [CrossRef]
- Dominguez, L.J.; Di Bella, G.; Veronese, N.; Barbagallo, M. Impact of Mediterranean Diet on Chronic Non-Communicable Diseases and Longevity. Nutrients 2021, 13. [Google Scholar] [CrossRef] [PubMed]
- Andreo-López, M.C.; Contreras-Bolívar, V.; Muñoz-Torres, M.; García-Fontana, B.; García-Fontana, C. Influence of the Mediterranean Diet on Healthy Aging. Int J Mol Sci 2023, 24. [Google Scholar] [CrossRef] [PubMed]
- Mazza, E.; Ferro, Y.; Pujia, R.; Mare, R.; Maurotti, S.; Montalcini, T.; Pujia, A. Mediterranean Diet In Healthy Aging. J Nutr Health Aging 2021, 25, 1076–1083. [Google Scholar] [CrossRef] [PubMed]
- Papadopoulou, S.K.; Detopoulou, P.; Voulgaridou, G.; Tsoumana, D.; Spanoudaki, M.; Sadikou, F.; Papadopoulou, V.G.; Zidrou, C.; Chatziprodromidou, I.P.; Giaginis, C. , et al. Mediterranean Diet and Sarcopenia Features in Apparently Healthy Adults over 65 Years: A Systematic Review. Nutrients 2023, 15. [Google Scholar] [CrossRef]
- Rudzińska, A.; Perera, I.; Gryglewska, B.; Gąsowski, J.; Piotrowicz, K. Can the Mediterranean diet decrease the risk of depression in older persons - a systematic review. Psychiatr Pol 2023, 57, 339–354. [Google Scholar] [CrossRef]
- Wermers, J. Mediterranean-style diet for the primary and secondary prevention of cardiovascular disease: Summary of a Cochrane review. Explore (NY) 2020, 16, 201–202. [Google Scholar] [CrossRef]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J. , et al. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil or Nuts. N Engl J Med 2018, 378, e34. [Google Scholar] [CrossRef]
- Rees, K.; Takeda, A.; Martin, N.; Ellis, L.; Wijesekara, D.; Vepa, A.; Das, A.; Hartley, L.; Stranges, S. Mediterranean-Style Diet for the Primary and Secondary Prevention of Cardiovascular Disease: A Cochrane Review. Glob Heart 2020, 15, 56. [Google Scholar] [CrossRef]
- Cabré, J.J.; Barrio, F.; Vizcaíno, J.; Martínez, A.; Mur, T.; Sagarra, R.; Dalmau, S. Results of the implementation of the DP-TRANSFERS project in Catalonia: A translational method to improve diabetes screening and prevention in primary care. Rev Clin Esp (Barc) 2024. [Google Scholar] [CrossRef]
- Jennings, A.; Berendsen, A.M.; de Groot, L.; Feskens, E.J.M.; Brzozowska, A.; Sicinska, E.; Pietruszka, B.; Meunier, N.; Caumon, E.; Malpuech-Brugère, C. , et al. Mediterranean-Style Diet Improves Systolic Blood Pressure and Arterial Stiffness in Older Adults. Hypertension 2019, 73, 578–586. [Google Scholar] [CrossRef] [PubMed]
- Dominguez, L.J.; Veronese, N.; Di Bella, G.; Cusumano, C.; Parisi, A.; Tagliaferri, F.; Ciriminna, S.; Barbagallo, M. Mediterranean diet in the management and prevention of obesity. Exp Gerontol 2023, 174, 112121. [Google Scholar] [CrossRef] [PubMed]
- Tuttolomondo, A.; Simonetta, I.; Daidone, M.; Mogavero, A.; Ortello, A.; Pinto, A. Metabolic and Vascular Effect of the Mediterranean Diet. Int J Mol Sci 2019, 20. [Google Scholar] [CrossRef] [PubMed]
- van den Brink, A.C.; Brouwer-Brolsma, E.M.; Berendsen, A.A.M.; van de Rest, O. The Mediterranean, Dietary Approaches to Stop Hypertension (DASH), and Mediterranean-DASH Intervention for Neurodegenerative Delay (MIND) Diets Are Associated with Less Cognitive Decline and a Lower Risk of Alzheimer's Disease-A Review. Adv Nutr 2019, 10, 1040–1065. [Google Scholar] [CrossRef] [PubMed]
- Mentella, M.C.; Scaldaferri, F.; Ricci, C.; Gasbarrini, A.; Miggiano, G.A.D. Cancer and Mediterranean Diet: A Review. Nutrients 2019, 11. [Google Scholar] [CrossRef]
- Georgoulis, M.; Damigou, E.; Chrysohoou, C.; Barkas, F.; Anastasiou, G.; Kravvariti, E.; Tsioufis, C.; Liberopoulos, E.; Sfikakis, P.P.; Pitsavos, C. , et al. Mediterranean diet trajectories and 20-year incidence of cardiovascular disease: The ATTICA cohort study (2002-2022). Nutr Metab Cardiovasc Dis 2024, 34, 153–166. [Google Scholar] [CrossRef]
- Tanaka, T.; Talegawkar, S.A.; Jin, Y.; Bandinelli, S.; Ferrucci, L. Association of Adherence to the Mediterranean-Style Diet with Lower Frailty Index in Older Adults. Nutrients 2021, 13. [Google Scholar] [CrossRef]
- Di Daniele, N.; Noce, A.; Vidiri, M.F.; Moriconi, E.; Marrone, G.; Annicchiarico-Petruzzelli, M.; D'Urso, G.; Tesauro, M.; Rovella, V.; De Lorenzo, A. Impact of Mediterranean diet on metabolic syndrome, cancer and longevity. Oncotarget 2017, 8, 8947–8979. [Google Scholar] [CrossRef]
- Laurent, S.; Boutouyrie, P.; Cunha, P.G.; Lacolley, P.; Nilsson, P.M. Concept of Extremes in Vascular Aging. Hypertension 2019, 74, 218–228. [Google Scholar] [CrossRef]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A. , et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension: The Task Force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension: The Task Force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension. J Hypertens 2018, 36, 1953–2041. [Google Scholar] [CrossRef]
- Visseren, F.L.J.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.M.; Capodanno, D. , et al. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice. Eur Heart J 2021, 42, 3227–3337. [Google Scholar] [CrossRef] [PubMed]
- Ohkuma, T.; Ninomiya, T.; Tomiyama, H.; Kario, K.; Hoshide, S.; Kita, Y.; Inoguchi, T.; Maeda, Y.; Kohara, K.; Tabara, Y. , et al. Brachial-Ankle Pulse Wave Velocity and the Risk Prediction of Cardiovascular Disease: An Individual Participant Data Meta-Analysis. Hypertension 2017, 69, 1045–1052. [Google Scholar] [CrossRef] [PubMed]
- Yasuharu, T.; Setoh, K.; Kawaguchi, T.; Nakayama, T.; Matsuda, F. Brachial-ankle pulse wave velocity and cardio-ankle vascular index are associated with future cardiovascular events in a general population: The Nagahama Study. J Clin Hypertens (Greenwich) 2021, 23, 1390–1398. [Google Scholar] [CrossRef] [PubMed]
- Matsushita, K.; Ding, N.; Kim, E.D.; Budoff, M.; Chirinos, J.A.; Fernhall, B.; Hamburg, N.M.; Kario, K.; Miyoshi, T.; Tanaka, H. , et al. Cardio-ankle vascular index and cardiovascular disease: Systematic review and meta-analysis of prospective and cross-sectional studies. J Clin Hypertens (Greenwich) 2019, 21, 16–24. [Google Scholar] [CrossRef]
- Miyoshi, T.; Ito, H.; Shirai, K.; Horinaka, S.; Higaki, J.; Yamamura, S.; Saiki, A.; Takahashi, M.; Masaki, M.; Okura, T. , et al. Predictive Value of the Cardio-Ankle Vascular Index for Cardiovascular Events in Patients at Cardiovascular Risk. J Am Heart Assoc 2021, 10, e020103. [Google Scholar] [CrossRef]
- Liese, A.D.; Couch, S.C.; The, N.S.; Crandell, J.L.; Lawrence, J.M.; Crume, T.L.; Mayer-Davis, E.J.; Zhong, V.W.; Urbina, E.M. Association between diet quality indices and arterial stiffness in youth with type 1 diabetes: SEARCH for Diabetes in Youth Nutrition Ancillary Study. J Diabetes Complications 2020, 34, 107709. [Google Scholar] [CrossRef]
- Alberti, K.G.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.; Loria, C.M.; Smith, S.C., Jr. Harmonizing the metabolic syndrome: a joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [CrossRef]
- Mottillo, S.; Filion, K.B.; Genest, J.; Joseph, L.; Pilote, L.; Poirier, P.; Rinfret, S.; Schiffrin, E.L.; Eisenberg, M.J. The metabolic syndrome and cardiovascular risk a systematic review and meta-analysis. J Am Coll Cardiol 2010, 56, 1113–1132. [Google Scholar] [CrossRef]
- Kotani, K.; Satoh-Asahara, N.; Nakakuki, T.; Yamakage, H.; Shimatsu, A.; Tsukahara, T. Association between metabolic syndrome and multiple lesions of intracranial atherothrombotic stroke: a hospital-based study. Cardiovasc Diabetol 2015, 14, 108. [Google Scholar] [CrossRef] [PubMed]
- Jiang, B.; Li, B.; Wang, Y.; Han, B.; Wang, N.; Li, Q.; Yang, W.; Huang, G.; Wang, J.; Chen, Y. , et al. The nine-year changes of the incidence and characteristics of metabolic syndrome in China: longitudinal comparisons of the two cross-sectional surveys in a newly formed urban community. Cardiovasc Diabetol 2016, 15, 84. [Google Scholar] [CrossRef]
- Saklayen, M.G. The Global Epidemic of the Metabolic Syndrome. Curr Hypertens Rep 2018, 20, 12. [Google Scholar] [CrossRef] [PubMed]
- Cornier, M.A.; Dabelea, D.; Hernandez, T.L.; Lindstrom, R.C.; Steig, A.J.; Stob, N.R.; Van Pelt, R.E.; Wang, H.; Eckel, R.H. The metabolic syndrome. Endocr Rev 2008, 29, 777–822. [Google Scholar] [CrossRef]
- Merchant, R.A.; Chan, Y.H.; Lim, J.Y.; Morley, J.E. Prevalence of Metabolic Syndrome and Association with Grip Strength in Older Adults: Findings from the HOPE Study. Diabetes Metab Syndr Obes 2020, 13, 2677–2686. [Google Scholar] [CrossRef] [PubMed]
- Sotos-Prieto, M.; Ortolá, R.; Ruiz-Canela, M.; Garcia-Esquinas, E.; Martínez-Gómez, D.; Lopez-Garcia, E.; Martínez-González, M.; Rodriguez-Artalejo, F. Association between the Mediterranean lifestyle, metabolic syndrome and mortality: a whole-country cohort in Spain. Cardiovasc Diabetol 2021, 20, 5. [Google Scholar] [CrossRef] [PubMed]
- Gallardo-Alfaro, L.; Bibiloni, M.D.M.; Mascaró, C.M.; Montemayor, S.; Ruiz-Canela, M.; Salas-Salvadó, J.; Corella, D.; Fitó, M.; Romaguera, D.; Vioque, J. , et al. Leisure-Time Physical Activity, Sedentary Behaviour and Diet Quality are Associated with Metabolic Syndrome Severity: The PREDIMED-Plus Study. Nutrients 2020, 12. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Marcos, M.A.; Martinez-Salgado, C.; Gonzalez-Sarmiento, R.; Hernandez-Rivas, J.M.; Sanchez-Fernandez, P.L.; Recio-Rodriguez, J.I.; Rodriguez-Sanchez, E.; García-Ortiz, L. Association between different risk factors and vascular accelerated ageing (EVA study): study protocol for a cross-sectional, descriptive observational study. BMJ Open 2016, 6, e011031. [Google Scholar] [CrossRef]
- Martí, R.; Parramon, D.; García-Ortiz, L.; Rigo, F.; Gómez-Marcos, M.A.; Sempere, I.; García-Regalado, N.; Recio-Rodriguez, J.I.; Agudo-Conde, C.; Feuerbach, N. , et al. Improving interMediAte risk management. MARK study. BMC Cardiovasc Disord 2011, 11, 61. [Google Scholar] [CrossRef]
- Recio-Rodríguez, J.I.; Martín-Cantera, C.; González-Viejo, N.; Gómez-Arranz, A.; Arietaleanizbeascoa, M.S.; Schmolling-Guinovart, Y.; Maderuelo-Fernandez, J.A.; Pérez-Arechaederra, D.; Rodriguez-Sanchez, E.; Gómez-Marcos, M.A. , et al. Effectiveness of a smartphone application for improving healthy lifestyles, a randomized clinical trial (EVIDENT II): study protocol. BMC Public Health 2014, 14, 254. [Google Scholar] [CrossRef]
- World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. Jama 2013, 310, 2191–2194. [CrossRef]
- Schröder, H.; Fitó, M.; Estruch, R.; Martínez-González, M.A.; Corella, D.; Salas-Salvadó, J.; Lamuela-Raventós, R.; Ros, E.; Salaverría, I.; Fiol, M. , et al. A short screener is valid for assessing Mediterranean diet adherence among older Spanish men and women. J Nutr 2011, 141, 1140–1145. [Google Scholar] [CrossRef]
- Shirai, K.; Hiruta, N.; Song, M.; Kurosu, T.; Suzuki, J.; Tomaru, T.; Miyashita, Y.; Saiki, A.; Takahashi, M.; Suzuki, K. , et al. Cardio-ankle vascular index (CAVI) as a novel indicator of arterial stiffness: theory, evidence and perspectives. J Atheroscler Thromb 2011, 18, 924–938. [Google Scholar] [CrossRef] [PubMed]
- Salas-Salvadó, J.; Rubio, M.A.; Barbany, M.; Moreno, B. [SEEDO 2007 Consensus for the evaluation of overweight and obesity and the establishment of therapeutic intervention criteria]. Med Clin (Barc) 2007, 128, 184–196. [Google Scholar] [CrossRef]
- O'Brien, E.; Asmar, R.; Beilin, L.; Imai, Y.; Mancia, G.; Mengden, T.; Myers, M.; Padfield, P.; Palatini, P.; Parati, G. , et al. Practice guidelines of the European Society of Hypertension for clinic, ambulatory and self blood pressure measurement. J Hypertens 2005, 23, 697–701. [Google Scholar] [CrossRef]
- 2013 Practice guidelines for the management of arterial hypertension of the European Society of Hypertension (ESH) and the European Society of Cardiology (ESC): ESH/ESC Task Force for the Management of Arterial Hypertension. J Hypertens 2013, 31, 1925–1938. [CrossRef] [PubMed]
- GómezSánchez, M.; Gómez Sánchez, L.; Patino-Alonso, M.C.; Alonso-Domínguez, R.; Sánchez-Aguadero, N.; Lugones-Sánchez, C.; Rodríguez Sánchez, E.; García Ortiz, L.; Gómez-Marcos, M.A. Adherence to the Mediterranean Diet in Spanish Population and Its Relationship with Early Vascular Aging according to Sex and Age: EVA Study. Nutrients 2020, 12. [Google Scholar] [CrossRef] [PubMed]
- Caparello, G.; Galluccio, A.; Giordano, C.; Lofaro, D.; Barone, I.; Morelli, C.; Sisci, D.; Catalano, S.; Andò, S.; Bonofiglio, D. Adherence to the Mediterranean diet pattern among university staff: a cross-sectional web-based epidemiological study in Southern Italy. Int J Food Sci Nutr 2020, 71, 581–592. [Google Scholar] [CrossRef]
- Guallar-Castillón, P.; Pérez, R.F.; López García, E.; León-Muñoz, L.M.; Aguilera, M.T.; Graciani, A.; Gutiérrez-Fisac, J.L.; Banegas, J.R.; Rodríguez-Artalejo, F. Magnitude and management of metabolic syndrome in Spain in 2008-2010: the ENRICA study. Rev Esp Cardiol (Engl Ed) 2014, 67, 367–373. [Google Scholar] [CrossRef]
- Fernández-Bergés, D.; Cabrera de León, A.; Sanz, H.; Elosua, R.; Guembe, M.J.; Alzamora, M.; Vega-Alonso, T.; Félix-Redondo, F.J.; Ortiz-Marrón, H.; Rigo, F. , et al. Metabolic syndrome in Spain: prevalence and coronary risk associated with harmonized definition and WHO proposal. DARIOS study. Rev Esp Cardiol (Engl Ed) 2012, 65, 241–248. [Google Scholar] [CrossRef]
- Hirode, G.; Wong, R.J. Trends in the Prevalence of Metabolic Syndrome in the United States, 2011-2016. Jama 2020, 323, 2526–2528. [Google Scholar] [CrossRef]
- Ma, K.; Liu, H.; Guo, L.; Li, J.; Lei, Y.; Li, X.; Sun, L.; Yang, L.; Yuan, T.; Wang, C. , et al. Comparison of metabolic syndrome prevalence and characteristics using five different definitions in China: a population-based retrospective study. Front Public Health 2024, 12, 1333910. [Google Scholar] [CrossRef]
- Jahangiry, L.; Khosravi-Far, L.; Sarbakhsh, P.; Kousha, A.; EntezarMahdi, R.; Ponnet, K. Prevalence of metabolic syndrome and its determinants among Iranian adults: evidence of IraPEN survey on a bi-ethnic population. Sci Rep 2019, 9, 7937. [Google Scholar] [CrossRef] [PubMed]
- Alipour, P.; Azizi, Z.; Raparelli, V.; Norris, C.M.; Kautzky-Willer, A.; Kublickiene, K.; Herrero, M.T.; Emam, K.E.; Vollenweider, P.; Preisig, M. , et al. Role of sex and gender-related variables in development of metabolic syndrome: A prospective cohort study. Eur J Intern Med 2024, 121, 63–75. [Google Scholar] [CrossRef] [PubMed]
- Cubas-Basterrechea, G.; Elío, I.; Alonso, G.; Otero, L.; Gutiérrez-Bardeci, L.; Puente, J.; Muñoz-Cacho, P. Adherence to the Mediterranean Diet Is Inversely Associated with the Prevalence of Metabolic Syndrome in Older People from the North of Spain. Nutrients 2022, 14. [Google Scholar] [CrossRef]
- Al Kudsee, K.; Vahid, F.; Bohn, T. High adherence to the Mediterranean diet and Alternative Healthy Eating Index are associated with reduced odds of metabolic syndrome and its components in participants of the ORISCAV-LUX2 study. Front Nutr 2022, 9, 1087985. [Google Scholar] [CrossRef]
- Hassani Zadeh, S.; Salehi-Abargouei, A.; Mirzaei, M.; Nadjarzadeh, A.; Hosseinzadeh, M. The association between dietary approaches to stop hypertension diet and mediterranean diet with metabolic syndrome in a large sample of Iranian adults: YaHS and TAMYZ Studies. Food Sci Nutr 2021, 9, 3932–3941. [Google Scholar] [CrossRef]
- Filippou, C.D.; Thomopoulos, C.G.; Konstantinidis, D.G.; Dimitriadis, K.S.; Chrysochoou, C.A.; Tatakis, F.A.; Siafi, E.P.; Tousoulis, D.M.; Nihoyannopoulos, P.I.; Panagiotakos, D.B. , et al. Effect of DASH vs. mediterranean diet accompanied by a salt restriction on metabolic syndrome and cardiometabolic risk factors in adults with high normal blood pressure or grade 1 hypertension: secondary analyses of a randomized controlled trial. Hellenic J Cardiol 2024. [Google Scholar] [CrossRef] [PubMed]
- Martemucci, G.; Khalil, M.; Di Luca, A.; Abdallah, H.; D'Alessandro, A.G. Comprehensive Strategies for Metabolic Syndrome: How Nutrition, Dietary Polyphenols, Physical Activity, and Lifestyle Modifications Address Diabesity, Cardiovascular Diseases, and Neurodegenerative Conditions. Metabolites 2024, 14. [Google Scholar] [CrossRef]
- Romero-Cabrera, J.L.; García-Ríos, A.; Sotos-Prieto, M.; Quintana-Navarro, G.; Alcalá-Díaz, J.F.; Martín-Piedra, L.; Torres-Peña, J.D.; Luque, R.M.; Yubero-Serrano, E.M.; Delgado-Lista, J. , et al. Adherence to a Mediterranean lifestyle improves metabolic status in coronary heart disease patients: A prospective analysis from the CORDIOPREV study. J Intern Med 2023, 293, 574–588. [Google Scholar] [CrossRef]
- George, E.S.; Gavrili, S.; Itsiopoulos, C.; Manios, Y.; Moschonis, G. Poor adherence to the Mediterranean diet is associated with increased likelihood of metabolic syndrome components in children: the Healthy Growth Study. Public Health Nutr 2021, 24, 2823–2833. [Google Scholar] [CrossRef]
- Bakaloudi, D.R.; Chrysoula, L.; Kotzakioulafi, E.; Theodoridis, X.; Chourdakis, M. Impact of the Level of Adherence to Mediterranean Diet on the Parameters of Metabolic Syndrome: A Systematic Review and Meta-Analysis of Observational Studies. Nutrients 2021, 13. [Google Scholar] [CrossRef]
- Fan, H.; Wang, Y.; Ren, Z.; Liu, X.; Zhao, J.; Yuan, Y.; Fei, X.; Song, X.; Wang, F.; Liang, B. Mediterranean diet lowers all-cause and cardiovascular mortality for patients with metabolic syndrome. Diabetol Metab Syndr 2023, 15, 107. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, C.; Moreira, H.; Santos, R. Systematic review of mediterranean diet interventions in menopausal women. AIMS Public Health 2024, 11, 110–129. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Sánchez, L.; Rodríguez-Sánchez, E.; Ramos, R.; Marti-Lluch, R.; Gómez-Sánchez, M.; Lugones-Sánchez, C.; Tamayo-Morales, O.; Llamas-Ramos, I.; Rigo, F.; García-Ortiz, L. , et al. The Association of Dietary Intake with Arterial Stiffness and Vascular Ageing in a Population with Intermediate Cardiovascular Risk-A MARK Study. Nutrients 2022, 14. [Google Scholar] [CrossRef] [PubMed]
- Cobos-Palacios, L.; Ruiz-Moreno, M.I.; Muñoz-Ubeda, M.; López-Sampalo, A.; Vilches-Perez, A.; Vargas-Candela, A.; Benitez-Porres, J.; Navarro-Sanz, A.; Pérez-Belmonte, L.M.; Lopez-Carmona, M.D. , et al. A healthy lifestyle is associated with lower arterial stiffness in a metabolically healthy elderly population with overweight or obesity. J Hypertens 2022, 40, 1808–1814. [Google Scholar] [CrossRef]
- Lasalvia, P.; Gianfagna, F.; Veronesi, G.; Franchin, M.; Tozzi, M.; Castelli, P.; Grandi, A.M.; Zambon, A.; Iacoviello, L.; Ferrario, M.M. Identification of dietary patterns in a general population of North Italian adults and their association with arterial stiffness. The RoCAV study. Nutr Metab Cardiovasc Dis 2021, 31, 44–51. [Google Scholar] [CrossRef]
- Navarro Cáceres, A.; Navarro-Matías, E.; Gómez-Sánchez, M.; Tamayo-Morales, O.; Lugones-Sánchez, C.; González-Sánchez, S.; Rodríguez-Sánchez, E.; García-Ortiz, L.; Gómez-Sánchez, L.; Gómez-Marcos, M.A. , et al. Increase in Vascular Function Parameters According to Lifestyles in a Spanish Population without Previous Cardiovascular Disease-EVA Follow-Up Study. Nutrients 2023, 15. [Google Scholar] [CrossRef]
- Palombo, C.; Kozakova, M. Arterial stiffness, atherosclerosis and cardiovascular risk: Pathophysiologic mechanisms and emerging clinical indications. Vascul Pharmacol 2016, 77, 1–7. [Google Scholar] [CrossRef]
- Rossi, P.; Francès, Y.; Kingwell, B.A.; Ahimastos, A.A. Gender differences in artery wall biomechanical properties throughout life. J Hypertens 2011, 29, 1023–1033. [Google Scholar] [CrossRef]
- Chester, R.; Sander, G.; Fernandez, C.; Chen, W.; Berenson, G.; Giles, T. Women have significantly greater difference between central and peripheral arterial pressure compared with men: the Bogalusa Heart Study. J Am Soc Hypertens 2013, 7, 379–385. [Google Scholar] [CrossRef]
Figure 1.
Number of those included and excluded, and their origin.
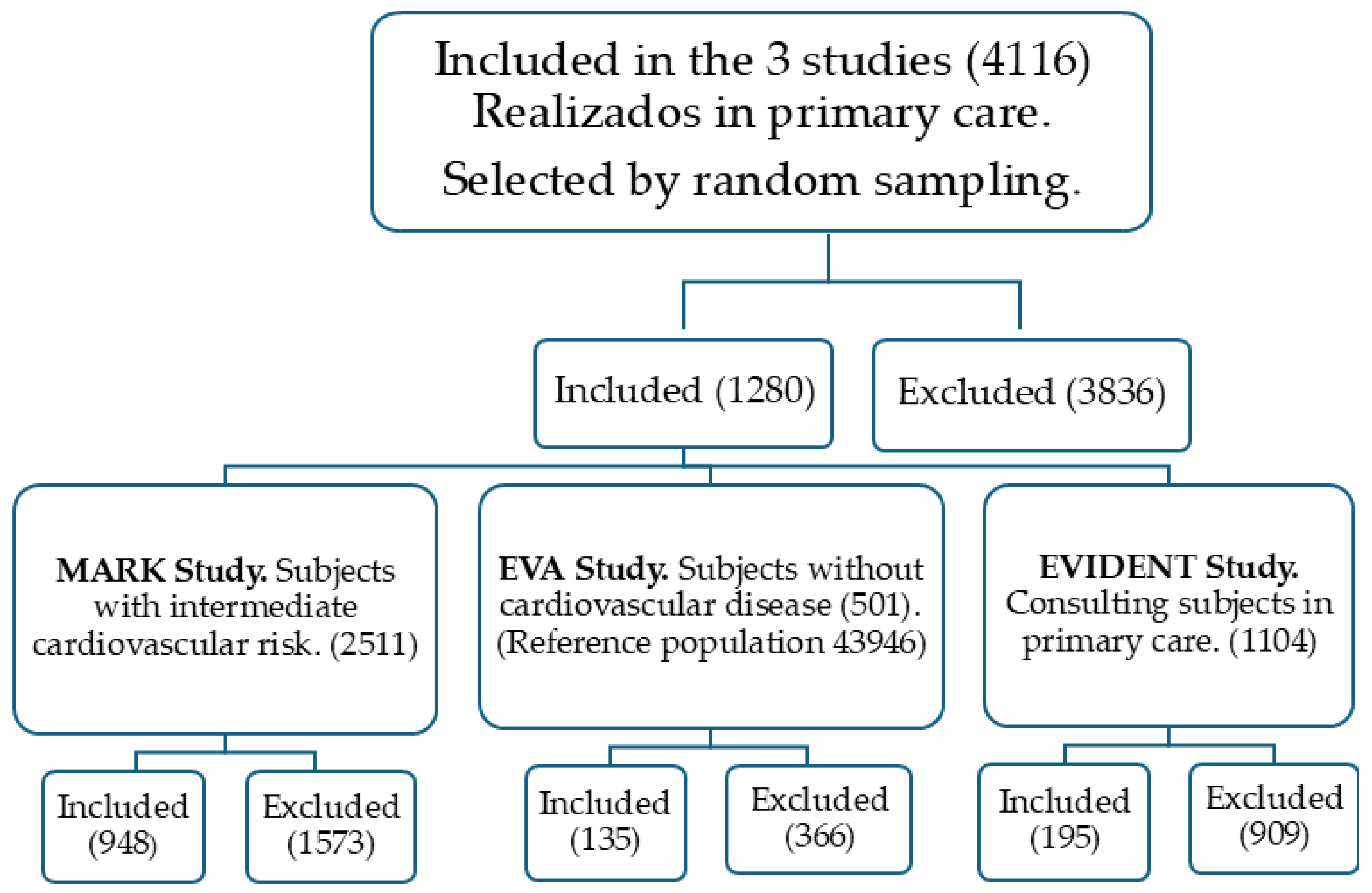
Figure 2.
Percentage of participants according to the number of MetS components overall and by sex. MetS: Metabolic syndrome; MD: Mediterranean diet.
Figure 2.
Percentage of participants according to the number of MetS components overall and by sex. MetS: Metabolic syndrome; MD: Mediterranean diet.
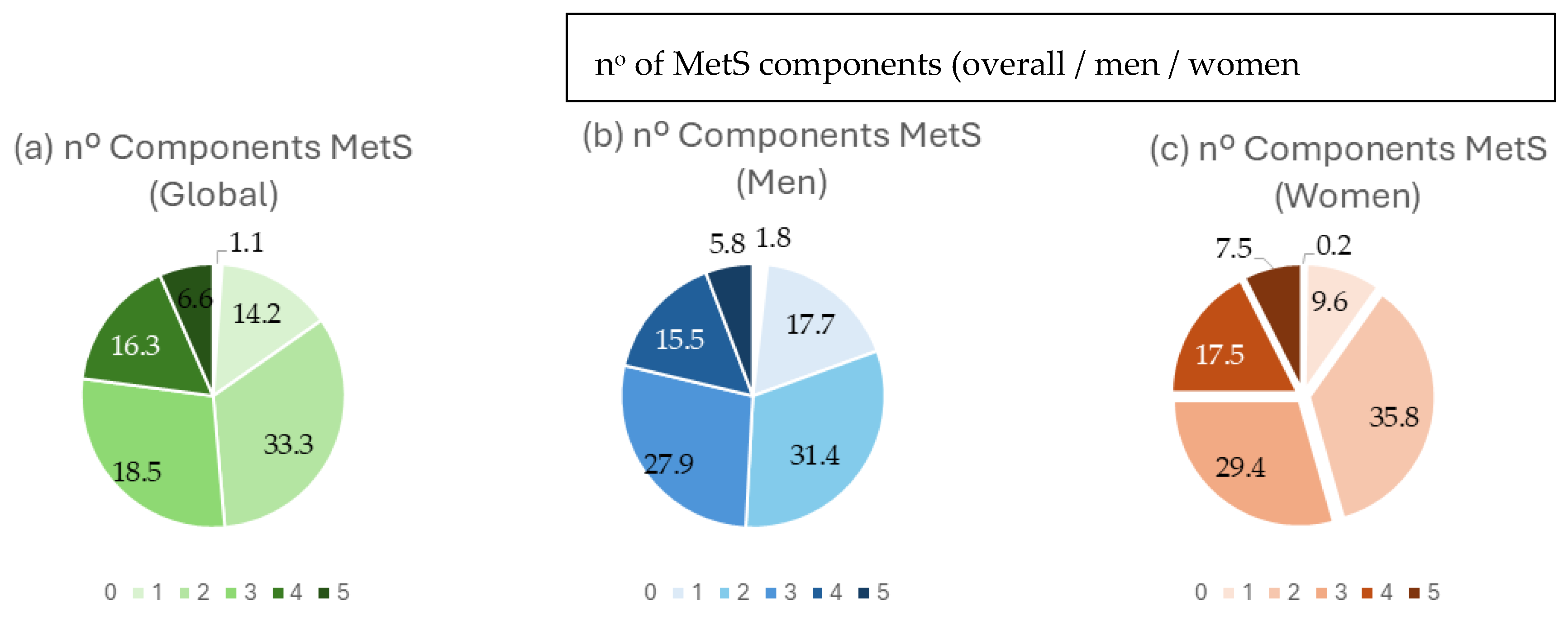
Figure 3.
Difference in MD scores between subjects with and without MetS and MetS components, overall and by sex. MetS: Metabolic syndrome; MD: Mediterranean diet; BP: blood pressure; FPG: fasting plasma glucose; TGC: triglycerides; HDH-C: high–density lipoprotein cholesterol; WC: waist circumference.
Figure 3.
Difference in MD scores between subjects with and without MetS and MetS components, overall and by sex. MetS: Metabolic syndrome; MD: Mediterranean diet; BP: blood pressure; FPG: fasting plasma glucose; TGC: triglycerides; HDH-C: high–density lipoprotein cholesterol; WC: waist circumference.
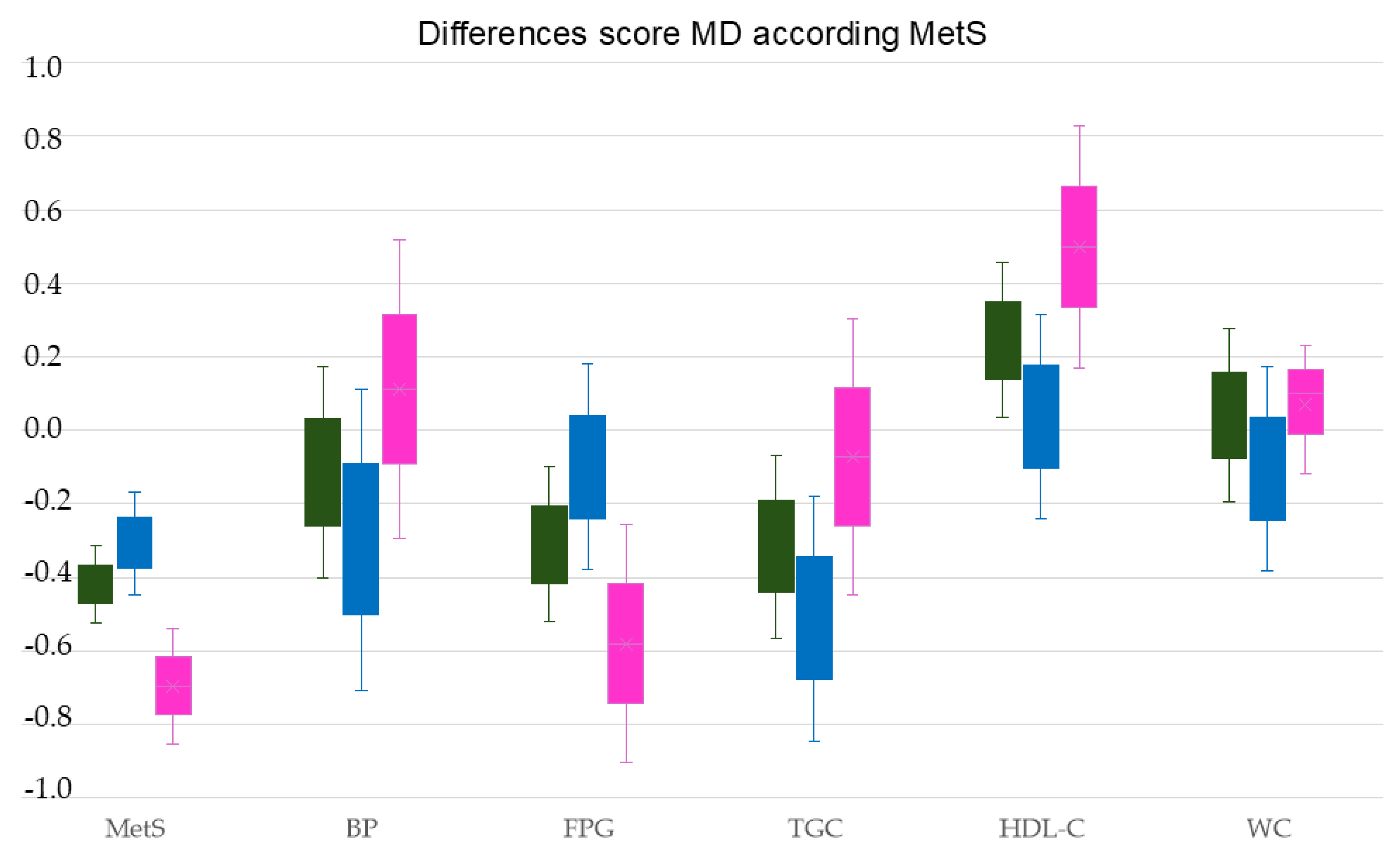

Table 1.
Diagnostic criteria for MetS.
| Blood pressure | BP figures ≥130/85 mmHg or treatment with antihypertensives |
|---|---|
| Glycemia | FBG ≥ 100 mg/dl or treatment with hypoglycemic medication |
| Triglycerides | TGC ≥ 150 mg/dl or lipid-lowering medication |
| HDL-cholesterol | HDL-C < 40 mg/dl in men or < 50mg/dl in women |
| Waist circumference | WC ≥ 88 cm in women or WC ≥ 102 cm in men |
MetS: Metabolic syndrome, BP: blood pressure; FBG: fasting plasma glucose, TGC: triglycerides, HDL-C: high–density lipoprotein cholesterol, WC: waist circumference. Adapted from International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity [37].
Table 2.
Characteristics of the study participants.
| Overall (n=1,280) | Men (n=736) | Women (n=544) |
p value | ||||||
| Mediterranean diet | Mean or nº | SD or (%) | Mean or nº | SD or (%) | Mean or nº | SD or (%) | |||
| MD (total score) | 6.00 | 1.90 | 5.92 | 1.92 | 6.11 | 1.88 | 0.036 | ||
| MD adherence, n (%) | 504 | (39) | 288 | (40) | 216 | (40) | 0.440 | ||
| Conventional risk factors | |||||||||
| Age, (years) | 69.52 | 3.58 | 69.47 | 3.51 | 69.58 | 3.67 | 0.286 | ||
| SBP, (mmHg) | 136.81 | 17.95 | 138.86 | 17.42 | 134.03 | 18.31 | <0.001 | ||
| DBP, (mmHg) | 80.15 | 10.06 | 80.96 | 9.67 | 79.04 | 10.48 | <0.001 | ||
| Hypertension, n (%) | 947 | (74) | 548 | (74%) | 399 | (73%) | 0.350 | ||
| Antihypertensive drugs, n (%) | 739 | (58) | 410 | (56) | 329 | (61) | 0.049 | ||
| HDL cholesterol, (mg/dl) | 54.10 | 14.79 | 50.96 | 12.79 | 58.33 | 16.20 | <0.001 | ||
| Triglycerides, (mg/dl) | 121.43 | 57.56 | 120.87 | 60.49 | 122.18 | 53.38 | 0.344 | ||
| Dyslipidemia, n (%) | 1042 | (81) | 564 | (77) | 478 | (88) | <0.001 | ||
| Lipid–lowering drugs, n (%) | 463 | (36) | 240 | (33) | 223 | (41) | 0.001 | ||
| FPG, (mg/dl) | 103.04 | 28.91 | 104.37 | 28.61 | 101.23 | 29.23 | 0.028 | ||
| Diabetes mellitus, n (%) | 298 | (23) | 180 | (25) | 118 | (22) | 0.142 | ||
| Hypoglycemic drugs, n (%) | 261 | (20) | 155 | (21) | 106 | (19) | 0.268 | ||
| WC, cm | 99.61 | 10.94 | 102.59 | 9.42 | 95.57 | 11.55 | <0.001 | ||
| Obesity, n (%) | 391 | (30) | 206 | (28) | 185 | (34) | 0.012 | ||
| Arterial stiffness | |||||||||
| CAVI | 9.30 | 1.11 | 9.49 | 1.05 | 9.03 | 1.13 | <0.001 | ||
| baPWV, m/sec | 15.82 | 2.56 | 15.75 | 2.46 | 15.92 | 2.68 | <0.001 | ||
| MetS and its components | |||||||||
| Number of MetS components | 2.64 | 1.14 | 2.55 | 1.17 | 2.77 | 1.09 | 0.129 | ||
| Mets, n (%) | 658 | (51) | 362 | (49) | 296 | (54) | 0.036 | ||
| BP ≥ 130/85 mmHg, n (%) | 1082 | (84) | 639 | (87) | 443 | (81) | 0.005 | ||
| FPG ≥ 100 mg/dL, n (%) | 541 | (42) | 334 | (45) | 207 | (38) | 0.005 | ||
| TGC ≥150 mg/dL, n (%) | 289 | (23) | 162 | (22) | 127 | (23) | 0.303 | ||
| HDL-C mg/dL < 40 men, < 50 women, n (%) | 308 | (24) | 119 | (16) | 189 | (35) | <0.001 | ||
| WC ≥88 cm women, ≥102 cm men, n (%) | 798 | (62) | 385 | (52) | 413 | (76) | <0.001 | ||
Values are means and standard deviations for continuous data, and number and proportions for categorical data. MetS: Metabolic syndrome; MD: Mediterranean diet; SBP: systolic blood pressure; DBP: diastolic blood pressure; HDL-C: high–density lipoprotein cholesterol; FPG: fasting plasma glucose; WC: waist circumference; BP: blood pressure; TGC: triglycerides; CAVI: cardio-ankle vascular index; baPWV: brachial-ankle pulse wave velocity; p value: differences between men and women.
Table 3.
Characteristics of the subjects included with and without Mets.
| With MetS (n=658) | Without MetS (n=622) | p value | |||
| Mediterranean Diet | Mean or N | SD or (%) | Mean or N | SD or (%) | |
| MD (total score) | 5.85 | 1.81 | 6.16 | 1.98 | 0.003 |
| MD adherence, n (%) | 232 | (35.3) | 272 | (54.0) | 0.002 |
| Conventional risk factors | |||||
| Men, n (%) | 362 | (51) | 374 | (49) | 0.236 |
| Women, n (%) | 296 | (54) | 248 | (46) | 0.036 |
| Age, (years) | 69.46 | 3.31 | 69.58 | 3.84 | 0.534 |
| SBP, (mmHg) | 139.08 | 16.38 | 134.41 | 19.21 | <0.001 |
| DBP, (mmHg) | 81.16 | 9.85 | 79.07 | 10.18 | <0.001 |
| Hypertension, n (%) | 562 | (85) | 385 | (62) | <0.001 |
| Antihypertensive drugs, n (%) | 447 | (68) | 292 | (47) | <0.001 |
| HDL cholesterol, (mg/dl) | 47.78 | 11.23 | 60.79 | 15.17 | <0.001 |
| Triglycerides, (mg/dl) | 146.26 | 64.78 | 95.12 | 32.17 | <0.001 |
| Dyslipidemia, n (%) | 534 | (82) | 508 | (81) | 0.411 |
| Lipid–lowering drugs, n (%) | 268 | (41) | 195 | (31) | <0.001 |
| FPG, (mg/dl) | 114.28 | 32.28 | 91.16 | 18.55 | <0.001 |
| Diabetes mellitus, n (%) | 248 | (38) | 50 | (8) | <0.001 |
| Hypoglycemic drugs, n (%) | 222 | (34) | 39 | (6) | <0.001 |
| WC, cm | 103.37 | 10.83 | 95.64 | 9.56 | <0.001 |
| Obesity, n (%) | 291 | (44) | 100 | (26) | <0.001 |
| Arterial stiffness | |||||
| CAVI | 9.33 | 1.12 | 9.25 | 1.10 | 0.200 |
| baPWV, m sec | 16.15 | 2.58 | 15.47 | 2.49 | <0.001 |
| MetS and its components | |||||
| Number of MetS components | 3.57 | 0.71 | 1.66 | 0.52 | <0.001 |
| BP ≥ 130/85 mmHg, n (%) | 621 | (94) | 461 | (74) | <0.001 |
| FPG ≥ 100 mg/dL, n (%) | 445 | (68) | 95 | (15) | <0.001 |
| TGC ≥ 150 mg/dL, n (%) | 270 | (41) | 19 | (7) | <0.001 |
| HDL-C mg/dL < 40 men, < 50 women, n (%) | 268 | (40) | 40 | (13) | <0.001 |
| WC ≥88 cm women, ≥102 cm men, n (%) | 517 | (78) | 281 | (35) | <0.001 |
Values are means and standard deviations for continuous data, and number and proportions for categorical data. MetS: metabolic syndrome; MD: Mediterranean diet; SBP: systolic blood pressure; DBP: diastolic blood pressure; HDL-C: high–density lipoprotein cholesterol; FPG: fasting plasma glucose; WC: waist circumference; BP: blood pressure; TGC: triglycerides; CAVI: cardio-ankle vascular index; baPWV: brachial-ankle pulse wave velocity; p value: differences between subjects with and without MetS.
Table 4.
Association of the Mediterranean diet with arterial stiffness and with the number and components of the metabolic syndrome, overall and by sex. Multiple regression analysis.
Table 4.
Association of the Mediterranean diet with arterial stiffness and with the number and components of the metabolic syndrome, overall and by sex. Multiple regression analysis.
| Global | β | (95% | CI) | R2 | p |
|---|---|---|---|---|---|
| Number of MetS components | -0.168 | (-0.269 | to -0.068) | 3.30 | 0.001 |
| SBP, (mmHg) | 0.001 | (-0.005 | to 0.007) | 2.90 | 0.669 |
| DBP, (mmHg) | -0.005 | (-0.015 | to 0.006) | 3.00 | 0.402 |
| FPG, (mg/dl) | -0.007 | (-0.012 | to -0.003) | 3.70 | 0.001 |
| Triglycerides, (mg/dl) | -0.003 | (-0.005 | to -0.002) | 3.90 | <0.001 |
| HDL cholesterol, (mg/dl) | 0.013 | (0.006 | to 0.020) | 3.90 | <0.001 |
| WC, cm | -0.018 | -(0.028 | to -0.008) | 3.90 | <0.001 |
| CAVI | -0.196 | (-0.294 | to -0.099) | 4.00 | <0.001 |
| baPWV, m/sec | -0.065 | (-0.107 | to -0.060) | 3.30 | 0.002 |
| Women | |||||
| Number of MetS components | -0.115 | (-0.282 | to 0.051) | 5.20 | 0.174 |
| SBP, (mmHg) | 0.004 | (-0.004 | to 0.013) | 5.00 | 0.329 |
| DBP, (mmHg) | -0.012 | (-0.027 | to 0.002) | 4.90 | 0.099 |
| FPG, (mg/dl) | -0.001 | (-0.009 | to 0.006) | 4.00 | 0.681 |
| Triglycerides, (mg/dl) | -0.002 | (-0.005 | to 0.001) | 5.00 | 0.302 |
| HDL cholesterol, (mg/dl) | 0.017 | (0.008 | to 0.027) | 7.10 | 0.001 |
| WC, cm | -0.026 | (-0.040 | to -0.012) | 6.40 | <0.001 |
| CAVI | -0.150 | (-0.293 | to -0.008) | 5.50 | 0.038 |
| baPWV, m/sec | -0.021 | (-0.082 | to 0.040) | 4.00 | 0.499 |
| Men | |||||
| Number of MetS components | -0.181 | -0.307 | to -0.056 | 4.50 | 0.005 |
| SBP, (mmHg) | -0.002 | -0.009 | to 0.006 | 3.50 | 0.702 |
| DBP, (mmHg) | 0.003 | -0.012 | to 0.018 | 3.80 | 0.663 |
| FPG, (mg/dl) | -0.011 | -0.016 | to -0.005 | 4.50 | <0.001 |
| Triglycerides, (mg/dl) | -0.004 | -0.006 | to -0.002 | 5.10 | <0.001 |
| HDL cholesterol, (mg/dl) | 0.006 | -0.005 | to 0.017 | 3.70 | 0.281 |
| WC, cm | -0.009 | -0.024 | to 0.006 | 3.00 | 0.230 |
| CAVI | -0.230 | -0.363 | to -0.097 | 4.80 | 0.001 |
| baPWV, m/sec | -0.099 | -0.155 | to -0.043 | 4.30 | 0.001 |
Multiple regression analysis using as dependent variables: arterial stiffness, number of components, SBP, DBP, FPG, triglycerides, HDL cholesterol and WC; Mediterranean diet score was the independent variable; adjustment variables: age, sex, and use of antihypertensive drugs, hypoglycemic and lipid-lowering agents. MetS: metabolic syndrome; MD: Mediterranean diet; SBP: systolic blood pressure; DBP: diastolic blood pressure; HDL: high-density lipoprotein; FPG: fasting plasma glucose; WC: waist circumference; CAVI: cardio-ankle vascular index; baPWV: brachial-ankle pulse wave velocity.
Table 5.
Association of Mediterranean diet adherence with arterial stiffness and metabolic syndrome and its components, overall and by sex. Logistic regression analysis.
Table 5.
Association of Mediterranean diet adherence with arterial stiffness and metabolic syndrome and its components, overall and by sex. Logistic regression analysis.
| Global. | OR | (95% | CI) | R2 | p |
|---|---|---|---|---|---|
| MetS | 0.675 | (0.528 | to 0.864) | 2.50 | 0.002 |
| BP ≥ 130/85 mmHg | 0.932 | (0.651 | to 1.335) | 1.50 | 0.701 |
| FPG ≥ 100 mg/dl | 0.640 | (0.477 | to 0.859) | 2.40 | 0.003 |
| Triglycerides ≥ 150 mg/dl | 0.747 | (0.566 | to 0.986) | 1.90 | 0.040 |
| HDL-C mg/dl < 40 men, <50 mg/dl women | 1.749 | (1.315 | to 2.326) | 3.10 | <0.001 |
| WC ≥ 88 cm women, ≥102 cm men | 0.815 | (0.645 | to 1.553) | 1.50 | 0.088 |
| CAVI | 0.835 | (0.749 | to 0.931) | 2.50 | 0.001 |
| baPWV, m/sec | 0.939 | (0.896 | to 0.984) | 2.10 | 0.008 |
| Women | |||||
| MetS | 0.605 | (0.410 | to 0.895) | 6.00 | 0.012 |
| BP ≥ 130/85 mmHg | 1.347 | (0.770 | to 2.356) | 4.70 | 0.296 |
| FPG ≥ 100 mg/dl | 0.604 | (0.376 | to 0.971) | 5.50 | 0.033 |
| Triglycerides ≥ 150 mg/dl | 1.035 | (0.681 | to 1.573) | 4.50 | 0.873 |
| HDL-C mg/dl < 40 men, < 50 women | 1.792 | (1.221 | to 2.632) | 6.70 | 0.003 |
| WC ≥ 88 cm women, ≥ 102 cm men | 0.751 | (0.495 | to 1.140) | 4.50 | 0.178 |
| CAVI | 0.841 | (0.713 | to 0.991) | 5.30 | 0.038 |
| baPWV, m/sec | 0.952 | (0.887 | to 1.022) | 4.70 | 0.171 |
| Men | |||||
| MetS | 0.760 | (0.552 | to 1.046) | 3.20 | 0.093 |
| BP ≥ 130/85 mmHg | 0.685 | (0.423 | to 1.109) | 3.10 | 0.124 |
| FPG ≥ 100 mg/dl | 0.696 | (0.477 | to 1.015) | 3.30 | 0.060 |
| Triglycerides ≥ 150 mg/dl | 0.609 | (0.417 | to 0.891) | 3.90 | 0.011 |
| HDL-C mg/dl < 40 men, < 50 women | 1.665 | (1.082 | to 2.563) | 3.70 | 0.020 |
| WC ≥ 88 cm women, ≥102 cm men | 0.840 | (0.622 | to 1.134) | 2.90 | 0.255 |
| CAVI | 0.825 | (0.711 | to 0.957) | 3.70 | 0.011 |
| baPWV, m/sec | 0.924 | (0.867 | to 0.985) | 3.60 | 0.015 |
Logistic regression analysis using as dependent variables MetS and its components, as independent variable Mediterranean diet score ≥ 7, and as adjustment variables age, sex, and use of antihypertensive drugs, hypoglycemic and lipid-lowering agents. MD, Mediterranean diet; MetS, metabolic syndrome; BP, blood pressure ≥ 130/85 mmHg; FPG, fasting plasma glucose ≥ 100 mg/dL, TGC, triglycerides ≥ 150 mg/dL; HDL-C, high–density lipoprotein < 40 men mg/dL, < 50 mg/dL women; WC, waist circumference WC ≥ 88 cm women, ≥ 102 cm men.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



