
Submitted:
29 September 2024
Posted:
30 September 2024
You are already at the latest version
Abstract
Next-generation sequencing(NGS) for HIV drug resistance(DR) testing has an increasing number of applications for detection of Low-abundance drug resistant variants(LA-DRVs) as its features of quasispecies. However there is less information on detection performance in DR detection with NGS.To determine the feasibility of NGS technology in LA-DRVs detection for HIV-1 pre-treated patients.In this study,80 pre-treated patients’ samples accepted both NGS and Sanger sequencing(SS) in HIV-1 drug resistance testing. The results show that NGS presents higher sensitivity in mutation sites discovery at 5% threshold. NGS shows a satisfactory consistency comparing with SS in both protease inhibitors(PIs) and Integrase inhibitor(INSTIs), more than 90%. But worse consistency in Nucleotide reverse transcriptase inhibitors(NRTIs), only ranging from 61.25%-87.50%. The consistency of Non-nucleotide reverse transcriptase inhibitors(NNRTIs) between NGS and SS was around 85%. NGS shows the highest sensitivity of 91.3% at 5% threshold. The application of NGS technology in HIV-1 genotype resistance detection in different populations infected with HIV needs more documents and to be confirm further.
Keywords:
Next-generation sequencing
; HIV-1 drug resistance
; consistency comparison
1. Introduction
The HIV-1 virus known as quasi-species has a high replication capacity with the high error rate of reverse transcriptase and lack of correction enzymes,leading to a high rate of nucleic acid mismatch, resulting in the production of a variety of homologous variants in infected bodies[1,2,3,4]. HIV drug resistance (HIV DR) has emerged as a major challenge to antiretroviral therapy (ART)[5]. The incredible diversity of HIV within the host and the selective pressure of HIV virions on drugs during ART make HIV resistance a complex and diverse environment[6,7,8].
In China, ART follows the principle of rapid initiation of therapy, and pre-treated monitoring of drug resistance plays a crucial role in ART regimen selection [9,10]. Sanger sequencing(SS) has conventionally been used for HIV drug resistance testing and considered the standard method for HIV-1 drug resistance testing in treatment-naive patients[11]. However, resistance variants below 20% threshold, known as Low-abundance drug resistant variants(LA-DRVs), are not detected by SS[12].LA-DRVs can lead to accumulation of resistance mutations, further increasing the risk of ART failure. It has been proved that individuals had LA-DRVs in the HIV-1 population was correlated with treatment failure[13]. NGS technology improves the sensitivity and quantitatively identify HIV quasi-species detection through its high-throughput, massively parallel sequencing of individual input templates. However, many challenges exist for the generalized adoption of NGS for HIVDR testing including standardized analysis outputs, the selection of threshold[14,15].
In order to clarify the efficiency of NGS detection technology in LA-DRVs detection, the blood samples of HIV-1 infected individuals before treatment were detected genotype resistance detecion using both NGS and SS technologies. Comparing the difference in the mutation rate of resistance sites between results from two technologies to determine the feasibility of the detection method in pre-treated patients.
2. Materials and Methods
2.1. Sample Collection and Ethic Statement
80 HIV-1 newly diagnosed patients were randomly selected accompany with the sentinel survey of men who have sex with men(MSM). This study was approved by the Ethics Committee of Jiangsu Provincial Center for Disease Prevention and Control(SL2023-B015-01).
2.2. Laboratory Detection
200ul plasma was extracted for nucleic acid with QIAsymphony SP/AS Cellfree200_v7 nucleic acid extraction reagent. Genotype resistance detection with SS including amplification of protease and reverse transcriptase regions (PR-RT) and integrase region (Int) were performed repetitively according to the reported research[16]. The amplification products were sent to Shanghai Shenggong Company(Sangon Biotech) for SS. The NGS genotype resistance detection including PR-RT and Int were tested using HIV-1 panel analyses with Thermo Ion Chef™ system and sequenced with Ion S5™[17]. The reads data were processed with buffalo software for drug resistance mutations on threshold 2%, 5%, 10%, 15%, 20% repetitively. The drug resistance sites below the 20% threshold are called Low-abundance drug resistant variants(LA-DRVs).
2.3. Statistical Analysis
Chi-square test was used to analyze statistical differences comparing the results of NGS on 20% or 2% threshold with the results of SS. P<0.05 was considered statistically significant. McNemar's Chi-square test was used to evaluate the consistency between the the two sequencing techniques. Kappa value was used to measure the degree of consistency between the two sequencing methods. If both technologies identify the same mutation in the same individual, or if neither detects any mutation, the resistance characteristics of the two technologies are considered consistent. Conversely, if only resistance mutations are identified by NGS or SS in patients, the two technologies are considered inconsistent. The SS serves as the reference standard. Sensitivity of NGS was defined as its ability to detect mutations in patients identified by SS. Specificity of NGS was defined as its ability to detect mutations in patients in whom SS did not detect mutations.
3. Results
3.1. The Characteristic of Overall Rate of Pre-Treated Drug Resistance (PDR) Mutations in 80 Samples by SS and NGS
The results of NGS showed that PDR gradually decreased with the increase of detection threshold. At the threshold of 2%, the overall PDR rate was 25.0%, which was higher than the results reported by other thresholds of NGS in this study. The PDR rate of PIs resistance, NRTIs resistance, NNRTIs resistance and INSTIs resistance were 6.3%, 5.1%, 10.3% and 6.3%, respectively at the threshold of 2%. Except for NNRTIs, the PDR rate of drugs increased with the decrease of threshold (Table 1).
Compared with the results of NGS, the ability of SS to detect pre-treated patients with resistance to PIs and NRTIs was lower, both of which were 2.5%. By paired chi-square test, when the detection threshold was 20%, there was no significant difference in the ability of NGS to detect PDR compared with SS (P=0.884). But when the detection threshold was reduced to 2%, the ability of NGS to identify PDR of pre-treated patients was significantly higher than that of SS (P<0.001).
From resluts of the resistance levels to drugs, we discovered that the resistance of INSTIs detected by NGS mainly showed low-level resistance to the drugs in first-line ART regimens(EVG and RAL). Under the five thresholds of NGS, there was one new patient was resistant to NFV. The drug resistance of this patient showed high-level resistant at the thresholds of 2%, 10% and 15%, but middle-level resistance at the thresholds of 5% and 20% (Figure 1).
3.2. The analysis of Resistance Mutation Sites Detected by NGS at Different Threshold
Compared to SS, NGS can detect more variant sites at lower thresholds. 52(65%) of the NGS detected subjects had at least one resistance mutation. The mutation sites reported by NGS gradually decreased with the increase of detection threshold. 90, 83, 72, 60, and 50 mutation sites were detected in order of threshold from low to high. At 2% threshold, 32 mutations were detected in 80 sequences with the frequency of 90. 11 mutations were observed in NRTIs. The mutation frequency of S68SG(33.8%,27/80)was the highest in NRTIs at each threshold, but decreased to 10.0%(8/80)with the increase of detection threshold of NGS. The mutation frequency of K219 was the second highest(5.0%,4/80). There were 15 mutation sites associated with NNRTIs, and 29 times were detected. The mutation frequencies of V179E and K103KE were 10.0%(8/80) and 6.3%(5/80), respectively. The mutation frequencies of PIs and INSTIs were much lower. There were 8 mutation sites associated with PIs, and 11 times were detected. F35L was the mutation site with the highest mutation frequency(3.8%,3/80) in PIs. A total of 4 mutation sites were detected for INSTIs , and the highest mutation frequency was E138EA (6.3%, 5/80). (Table 2).
3.3. Comparison of Consistency between SS and NGS
The consistency of drug resistance mutations detected by the two sequencing methods at different thresholds were analyzed (Table 3 and Figure 2). The consistency of drug resistance mutations detected by NGS and SS increased with the increase of detection threshold, while drug resistance mutations detected only by NGS decreased with the increase of threshold. 23 patients were detected mutation sites with SS detection. However, 52, 51, 36, 37 and 34 patients were detected mutation sites with NGS 2 at 10%, 15% and 20% thresholds, respectively. 62.50%-95.00% of the results were identical between the two sequencing methods. The sensitivity and specificity analysis of SS and NGS in detecting drug resistance mutation were used to Assessing consistency. The consistent rates of drug resistance mutations in PIs, NRTIs, NNRTIs, and INSTIs are 92.50% -95.0%, 62.50% -85.00%, 78.75% -87.5%, 90.0% -93.75%, respectively. The majority of research subjects with NRTIs related mutations detected only by NGS were 13.75% -36.25%, with the main mutation site detected being S68SG. Paired chi-square test showed that the difference between the two methods was statistically significant in detecting NRTIs, NNRTIs and overall resistance mutations(Table 4). One more mutation site was both detected at the 2% and 5% threshold. Therefore, at the 5% threshold, the sensitivity of NGS was the highest, which was 91.3%.The Kappa values of the two sequencing techniques for detecting arbitrary mutation sites ranged from 0.2 to 0.4, which was at a general level.
4. Discussion
In this study, we conducted a parallel experiment of genotyping drug resistance detection in pre-treated HIV-1 positive patients, and evaluated the PDR rate of patients at different detection thresholds by comparing the results of SS and NGS. As expected, the detection rate of drug resistance mutations is closely related to the sensitivity of NGS[18]. Specifically, NGS technology recognizes more drug resistance mutations at lower detection thresholds with higher sensitivity. It provides more comprehensive resistance information than SS technology.
In this study, the overall PDR rate resulting from NGS testing increase comparing to SS. The drug resistance rate of other drug categories also increased. Using NGS likewise, Lataillade et al. reported that 30.5%(43/141) of the study subjects detected drug resistance mutations before treatment, and the drug resistance rate related to other drug categories was also higher than those in this study [19]. It is worth to note that NGS in this study did not show an additional advantage in detecting PDR rate of NNRTIs. Even badly happened missing discovered mutation site of K103N and V179E by NGS, but detected by SS in two patients respectively. K103N is a drug resistance site possessing clinical significant, which can decrease the sensitive to NVP and EFV. The methodology of NGS is based on amplification, sequencing and splicing of small fragments. Due to short fragments, there will be a certain error tolerance rate. Therefore, The quality control of NGS for HIV-1 genotype resistance testing is still a challenge and needs to improve[20]. Although there are mutations missed by NGS, NGS still detects more mutation sites and is more sensitive than traditional SS.
This study reveals significant differences between SS and NGS in the detection of drug resistant mutations and drug resistance level. With these differences becoming more pronounced as the threshold level decreases, NGS leads to a sharp increase in detected mutation sites below the 5% threshold. By comparing the consistency of these two sequencing methods in discovering the mutation sites and number of drug resistance mutations in all subjects, we found that there was a high consistency between the two methods in identifying drug resistance mutations associated with PIs and INSTIs, reaching more than 90%. However, the consistency for drug resistance mutations associated with NRTIs was relatively low, ranging from 61.25% to 87.50%. In addition, The proportion of patients with NRTIs drug-related mutations identified only by NGS increased gradually with the decrease of detection threshold, and the proportion of NRTIs drug-related mutations identified by NGS was higher than that of other categories of drug-related mutations. This suggests that resistance mutations associated with NRTIs are more easily detected by NGS with poor accuracy. Although the consistency between resistance profiles of SS and NGS in this study is lower than that reported in previous studies (83%-92%), this may be due to the subjects selection of pre-treated HIV-1 in our study. For those who have received antiviral therapy, under the drug pressure, drug resistance mutations were induced and maintain survival in vivo. These mutation sites are more easily detected both by SS and NGS [21]. Acquisition of genetic material from viruses by their hosts can generate inter-host structural genome variation often occur in vivo. In pre-treated HIV-1 patients, mutations happened more randomly affected by the host[22]. These mutations may be not stable or have no business with drug resistance. However, they can affect the accuracy of test results, especially for highly sensitive methods, NGS. So, it showed a not desired consistency between two methods for genotype drug resistance testing in pre-treated patients. Although there are differences between different studies, it is already recognized that NGS has higher sensitivity than SS, and we proved this in our study. If the efficacy of NGS in different populations and thresholds can be determined, then the results of NGS applied to HIV-1 genotype resistance detection will be more reliable and analyzable[23].
5. Conclusion
Comparing to Sanger sequencing, the sensitivity of next-generation sequencing has been proved higher. NGS is viable for HIV-1 genotype resistance detection in pre-treated patients for PIs and INSTIs, but not a good choice for NRTIs. The application of NGS technology in HIV-1 genotype resistance detection in different populations infected with HIV needs more documents and to be confirm further.
Author Contributions
Ying Zhou and Fei Ouyang, writing—original draft preparation, performing experiments, analyzing data; Xiaoyang Liu, Jing Lu and Haiyang Hu, managing the NGS instruments, consumable material and collecting and keeping samples; Qi Sun, disposing the data; Haitao Yang, giving the advice to the study. All authors have read and agreed to the published version of the manuscript.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Data Availability Statement
Data are contained within the article.
Conflicts of Interest
The authors declare no conflicts of interest.
Ethics Declaration
This study was approved by the Ethics Committee of Jiangsu Provincial Center for Disease Prevention and Control(SL2023-B015-01).
References
- Perelson, A.S.; Neumann, A.U.; Markowitz, M.; Leonard, J.M.; Ho, D.D. HIV-1 Dynamics in Vivo: Virion Clearance Rate, Infected Cell Life-Span, and Viral Generation Time. Science 1996, 271, 1582–1586. [Google Scholar] [CrossRef] [PubMed]
- Drake, J.W.; Holland, J.J. Mutation rates among RNA viruses. Proceedings of the National Academy of Sciences of the United States of America 1999, 96, 13910–13913. [Google Scholar] [CrossRef] [PubMed]
- Duffy, S.; Shackelton, L.A.; Holmes, E.C. Rates of evolutionary change in viruses: patterns and determinants. Nat. Rev. Genet. 2008, 9, 267–276. [Google Scholar] [CrossRef] [PubMed]
- Jiao, L.Y.; Liu, Y.J.; Guo, D.X.; et al. Comparison of two HIV-1 drug resistance quasispecies analysis methods. Proceedings of Academy of Military Medical Sciences 2010, 34, 261–264. [Google Scholar]
- Cao, W.; Hsieh, E.; Li, T. Optimizing Treatment for Adults with HIV/AIDS in China: Successes over Two Decades and Remaining Challenges. Curr. HIV/AIDS Rep. 2020, 17, 26–34. [Google Scholar] [CrossRef]
- Johnson, J.A.; Li, J.F.; Wei, X.; et al. Minority HIV-1 drug resistance mutations are present in antiretroviral treatment-naïve populations and associate with reduced treatment efficacy. PLoS medicine 2008, 5, e158. [Google Scholar] [CrossRef]
- HIV infection. Nat. Rev. Dis. Prim. 2015, 1, 15060. [CrossRef]
- Ji, H.; Enns, E.; Brumme, C.J.; Parkin, N.; Howison, M.; Lee, E.R.; Capina, R.; Marinier, E.; Avila-Rios, S.; Sandstrom, P.; et al. Bioinformatic data processing pipelines in support of next-generation sequencing-based HIV drug resistance testing: the Winnipeg Consensus. J. Int. AIDS Soc. 2018, 21, e25193. [Google Scholar] [CrossRef]
- World Health Organization. Global Action Plan. on HIV Drug Resistance 2017-2021; World Health Organization: Geneva, Switzerland, 2017; ISBN 9789241512848. [Google Scholar]
- Dai, L.L.; Chen, R.F.; Chen, Y.K.; et al. Expert consensus on rapid initiation of HIV/AIDS antiviral therapy. China Journal of AIDS and Sexually Transmitted Diseases 2023, 29, 737–744. [Google Scholar]
- Alidjinou, E.K.; Deldalle, J.; Hallaert, C.; Robineau, O.; Ajana, F.; Choisy, P.; Hober, D.; Bocket, L. RNA and DNA Sanger sequencing versus next-generation sequencing for HIV-1 drug resistance testing in treatment-naive patients. J. Antimicrob. Chemother. 2017, 72, 2823–2830. [Google Scholar] [CrossRef]
- McCluskey, S.M.; Siedner, M.J.; Marconi, V.C. Management of Virologic Failure and HIV Drug Resistance. Infect. Dis. Clin. North Am. 2019, 33, 707–742. [Google Scholar] [CrossRef] [PubMed]
- Kyeyune, F.; Gibson, R.M.; Nankya, I.; Venner, C.; Metha, S.; Akao, J.; Ndashimye, E.; Kityo, C.M.; Salata, R.A.; Mugyenyi, P.; et al. Low-Frequency Drug Resistance in HIV-Infected Ugandans on Antiretroviral Treatment Is Associated with Regimen Failure. Antimicrob. Agents Chemother. 2016, 60, 3380–3397. [Google Scholar] [CrossRef]
- Ouyang, F.; Yuan, D.; Zhai, W.; Liu, S.; Zhou, Y.; Yang, H. HIV-1 Drug Resistance Detected by Next-Generation Sequencing among ART-Naïve Individuals: A Systematic Review and Meta-Analysis. Viruses 2024, 16, 239. [Google Scholar] [CrossRef]
- Ávila-Ríos, S.; Parkin, N.; Swanstrom, R.; Paredes, R.; Shafer, R.; Ji, H.; Kantor, R. Next-Generation Sequencing for HIV Drug Resistance Testing: Laboratory, Clinical, and Implementation Considerations. Viruses 2020, 12, 617. [Google Scholar] [CrossRef]
- Jingna, X.; Rong, C.; Jun, C.; Hongxia, W.; Ronghui, X.; Zhenyan, W.; Qi, T.; Ren, F.; Li, L.; Hongzhou, L. [Investigation on drug resistance of HIV-infected people before antiviral therapy in three cities in Chinese]. Chinese journal of HIV and STD 2020, 26, 805–808. [Google Scholar] [CrossRef]
- Pyne, M.T.; Simmon, K.E.; Mallory, M.A.; Hymas, W.C.; Stevenson, J.; Barker, A.P.; Hillyard, D.R. HIV-1 Drug Resistance Assay Using Ion Torrent Next Generation Sequencing and On-Instrument End-to-End Analysis Software. J. Clin. Microbiol. 2022, 60, e0025322. [Google Scholar] [CrossRef]
- Lee, E.R.; Parkin, N.; Jennings, C.; Brumme, C.J.; Enns, E.; Casadellà, M.; Howison, M.; Coetzer, M.; Avila-Rios, S.; Capina, R.; et al. Performance comparison of next generation sequencing analysis pipelines for HIV-1 drug resistance testing. Sci. Rep. 2020, 10, 1–10. [Google Scholar] [CrossRef]
- Yuan, D.F. Epidemiological study of HIV-1 subtypes and drug resistance mutations in HIV-1 infected persons under treatment in Jiangsu Province; Southeast University: Jiangsu, 2022. [Google Scholar]
- Teo, C.H.Y.; Norhisham, N.H.B.; Lee, O.F.; Png, S.; Chai, C.N.; Yan, G.; Tang, J.W.-T.; Lee, C.K. Towards Next-Generation Sequencing for HIV-1 Drug Resistance Testing in a Clinical Setting. Viruses 2022, 14, 2208. [Google Scholar] [CrossRef]
- Lataillade, M.; Chiarella, J.; Yang, R.; Schnittman, S.; Wirtz, V.; Uy, J.; Seekins, D.; Krystal, M.; Mancini, M.; McGrath, D.; et al. Prevalence and Clinical Significance of HIV Drug Resistance Mutations by Ultra-Deep Sequencing in Antiretroviral-Naïve Subjects in the CASTLE Study. PLOS ONE 2010, 5, e10952. [Google Scholar] [CrossRef]
- Kojima, S.; Kamada, A.J.; Parrish, N.F. Virus-derived variation in diverse human genomes. PLOS Genet. 2021, 17, e1009324. [Google Scholar] [CrossRef]
- Capina, R.; Li, K.; Kearney, L.; Vandamme, A.-M.; Harrigan, P.R.; Van Laethem, K. Quality Control of Next-Generation Sequencing-Based HIV-1 Drug Resistance Data in Clinical Laboratory Information Systems Framework. Viruses 2020, 12, 645. [Google Scholar] [CrossRef] [PubMed]
- Novitsky, V.; Nyandiko, W.; Vreeman, R.; DeLong, A.K.; Manne, A.; Scanlon, M.; Ngeresa, A.; Aluoch, J.; Sang, F.; Ashimosi, C.; et al. Added Value of Next Generation over Sanger Sequencing in Kenyan Youth with Extensive HIV-1 Drug Resistance. Microbiol. Spectr. 2022, 10, e0345422. [Google Scholar] [CrossRef]
Figure 1.
The patients number with low level or above resistance to drugs detected by SS and NGS.
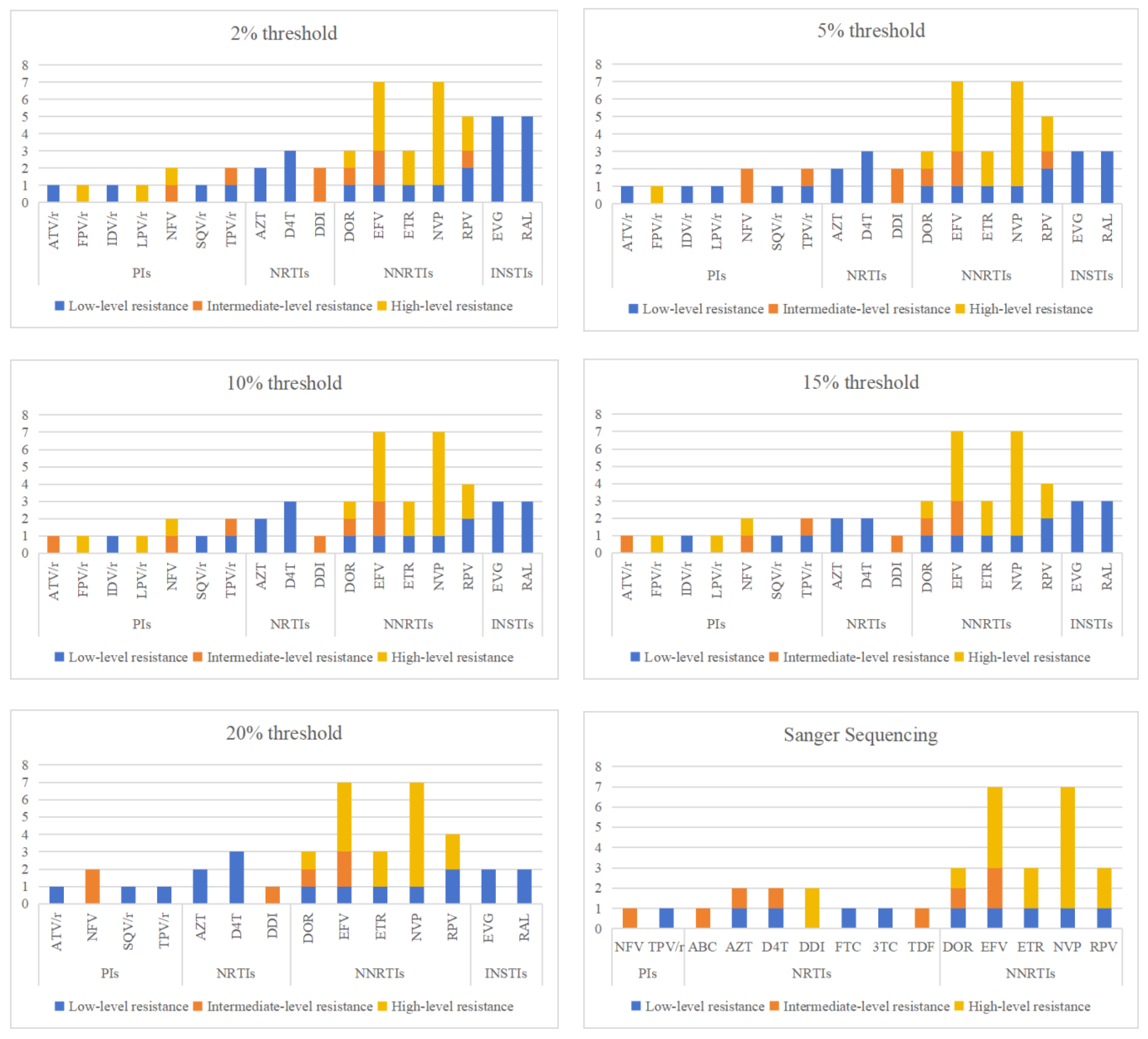
Figure 2.
Consistency of PDR mutation sites identified by SS and NGS.
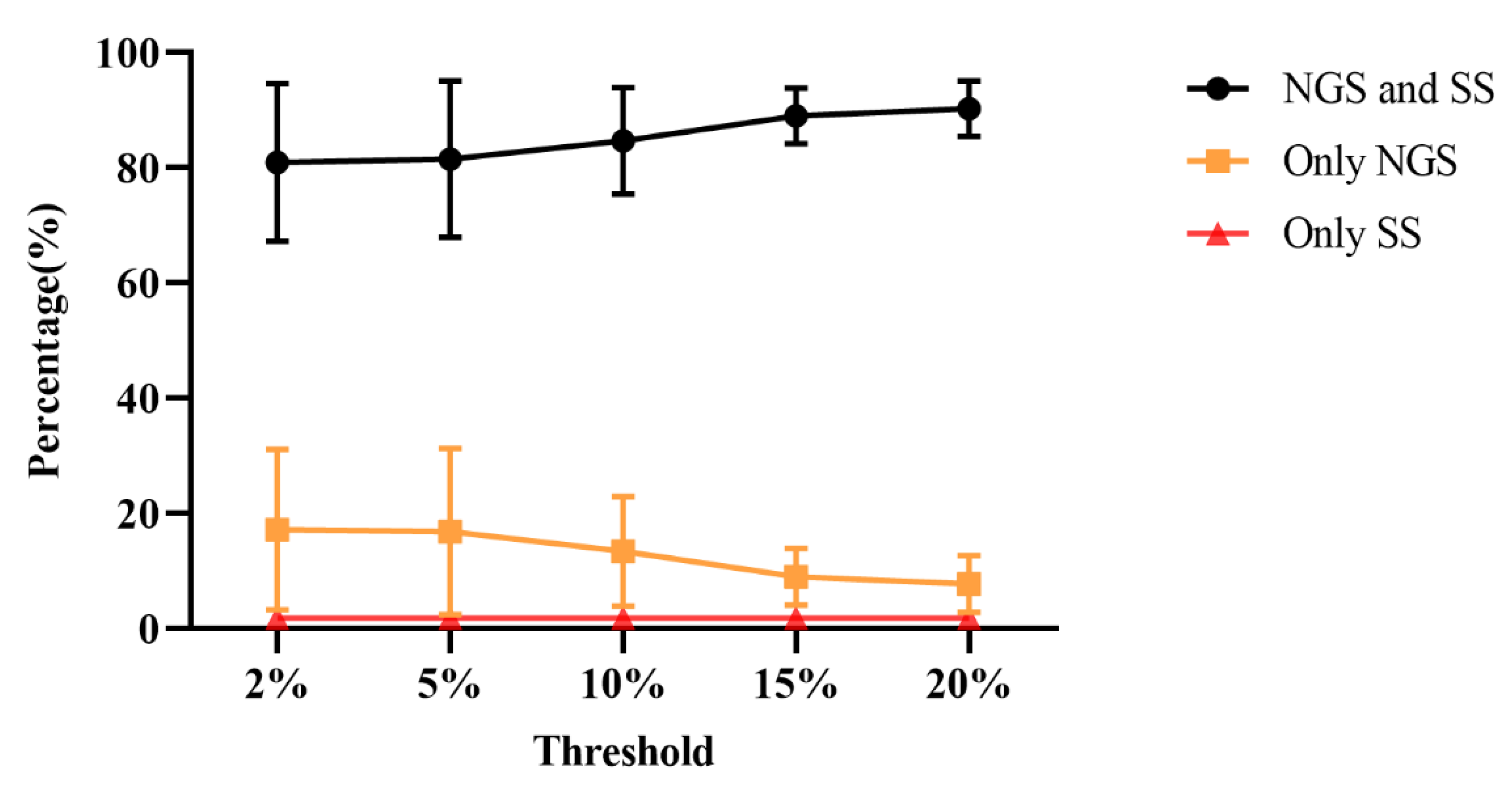

Table 1.
The overall PDR Rate Based on NGS and SS.
| resistance patterns | Sanger sequencing | Next-generation sequencing | ||||
|---|---|---|---|---|---|---|
| 20% threshold | 15% threshold | 10% threshold | 5% threshold | 2% threshold | ||
| Any drug resistance, n (%) | 11 (13.8) | 14 (17.9) | 16 (20.5) | 17 (21.8) | 19 (23.8) | 20 (25.0) |
| PIs resistance, n (%) | 2 (2.5) | 3 (3.8) | 5 (6.3) | 5 (6.3) | 5 (6.3) | 5 (6.3) |
| NRTIs resistance, n (%) | 2 (2.5) | 2 (2.6) | 2 (2.6) | 3 (3.8) | 4 (5.1) | 4 (5.1) |
| NNRTIs class resistance, n (%) | 8 (10.0) | 8 (10.3) | 8 (10.3) | 8 (10.3) | 8 (10.3) | 8 (10.3) |
| INSTIs resistance, n (%) | 0 | 2 (2.6) | 3 (3.8) | 3 (300.8) | 3 (3.8) | 5 (6.3) |
Table 2.
Resistance mutations statistics at different thresholds detected by SS and NGS.
| drug classes | mutation site | Next-generation sequencing detection threshold | Sanger sequencing |
||||
|---|---|---|---|---|---|---|---|
| 2% | 5% | 10% | 15% | 20% | |||
| PIs | L33F | 3 | 3 | 3 | 3 | 3 | 3 |
| M46I | 1 | 1 | 1 | 1 | 1 | 1 | |
| M46L | 1 | 0 | 1 | 1 | 0 | 0 | |
| M46V | 0 | 0 | 0 | 0 | 1 | 0 | |
| I47AV | 1 | 1 | 1 | 1 | 0 | 0 | |
| F53L | 3 | 3 | 3 | 3 | 1 | 0 | |
| Q58E | 1 | 1 | 1 | 1 | 1 | 1 | |
| L89LMV | 1 | 1 | 1 | 1 | 1 | 0 | |
| total | 11 | 10 | 11 | 11 | 9 | 5 | |
| NRTIs | E40F | 0 | 1 | 1 | 1 | 1 | 0 |
| M41L | 1 | 1 | 1 | 1 | 1 | 1 | |
| E44EDV | 0 | 1 | 0 | 0 | 0 | 0 | |
| S68SG | 27 | 27 | 20 | 12 | 8 | 0 | |
| S68G | 2 | 2 | 2 | 2 | 2 | 3 | |
| D67N | 1 | 1 | 1 | 1 | 1 | 1 | |
| T69D | 1 | 1 | 1 | 1 | 1 | 1 | |
| D67del | 0 | 0 | 0 | 0 | 0 | 1 | |
| T69TADN | 1 | 1 | 0 | 0 | 0 | 0 | |
| F77FL | 1 | 0 | 0 | 0 | 0 | 0 | |
| T215TS | 1 | 1 | 1 | 0 | 0 | 0 | |
| K219KN | 2 | 2 | 2 | 2 | 1 | 0 | |
| K219KQ | 1 | 1 | 0 | 0 | 0 | 0 | |
| K219KR | 1 | 1 | 0 | 0 | 0 | 0 | |
| total | 39 | 40 | 29 | 20 | 15 | 7 | |
| NNRTIs | K101E | 1 | 1 | 1 | 1 | 1 | 1 |
| K103KE | 5 | 5 | 5 | 2 | 1 | 0 | |
| K103N | 2 | 2 | 3 | 3 | 3 | 4 | |
| K103NS | 1 | 1 | 0 | 0 | 0 | 0 | |
| K103S | 1 | 1 | 1 | 1 | 1 | 1 | |
| V106VI | 1 | 0 | 0 | 0 | 0 | 0 | |
| E138EA | 1 | 1 | 1 | 1 | 1 | 0 | |
| E138EG | 1 | 1 | 1 | 1 | 1 | 1 | |
| E138EK | 1 | 1 | 0 | 0 | 0 | 0 | |
| V179D | 3 | 3 | 3 | 3 | 3 | 1 | |
| V179E | 8 | 8 | 8 | 8 | 7 | 5 | |
| Y181C | 1 | 1 | 1 | 1 | 1 | 1 | |
| Y181V | 1 | 1 | 1 | 1 | 1 | 1 | |
| G190S | 1 | 1 | 1 | 1 | 1 | 1 | |
| P225PH | 1 | 1 | 1 | 1 | 1 | 1 | |
| total | 29 | 28 | 27 | 24 | 22 | 17 | |
| INSTIs | T66A | 0 | 0 | 1 | 0 | 0 | 0 |
| E138EA | 5 | 3 | 2 | 3 | 2 | 0 | |
| A128AT | 1 | 0 | 0 | 0 | 0 | 1 | |
| S153A | 4 | 1 | 1 | 1 | 1 | 1 | |
| D232N | 1 | 1 | 1 | 1 | 1 | 0 | |
| total | 11 | 5 | 5 | 5 | 4 | 2 | |
Table 3.
Consistency of PDR mutation sites identified by SS and NGS.
| detection threshold | drug resistance mutation sites | PIs | NRTIs | NNRTIs | INSTIs |
|---|---|---|---|---|---|
| 2% | Only detected by NGS | 6.25% | 36.25% | 18.75% | 7.50% |
| Only detected by SS | 1.25% | 1.25% | 2.50% | 2.50% | |
| Consistency | 92.50% | 62.50% | 78.75% | 90.00% | |
| 5% | Only detected by NGS | 6.25% | 37.50% | 16.25% | 7.50% |
| Only detected by SS | 1.25% | 1.25% | 2.50% | 2.50% | |
| Consistency | 92.50% | 62.50% | 81.25% | 90.00% | |
| 10% | Only detected by NGS | 6.25% | 26.25% | 15.00% | 6.25% |
| Only detected by SS | 1.25% | 1.25% | 2.50% | 2.50% | |
| Consistency | 92.50% | 72.5% | 82.50% | 91.25% | |
| 15% | Only detected by NGS | 5.00% | 15.00% | 11.25% | 5.00% |
| Only detected by SS | 1.25% | 1.25% | 2.50% | 2.50% | |
| Consistency | 93.75% | 83.75% | 86.25% | 92.50% | |
| 20% | Only detected by NGS | 3.75% | 13.75% | 10.00% | 3.75% |
| Only detected by SS | 1.25% | 1.25% | 2.50% | 2.50% | |
| Consistency | 95.00% | 85.00% | 87.50% | 93.75% |
Table 4.
Sensitivity and specificity comparison with SS and NGS in PDR mutation sites detection.
| NGS | SS | Sensitiv-ity | Specifi-city | P | Kappa value | 95%CI | ||
|---|---|---|---|---|---|---|---|---|
| Detected | Not detected | |||||||
| PIs | ||||||||
| 2%/5%/10% | Detected | 4 | 5 | 80.0% | 93.3% | 0.109 | 0.534 | 0.211-0.857 |
| Not detected | 1 | 70 | ||||||
| 15% | Detected | 4 | 4 | 80.0% | 94.6% | 0.109 | 0.583 | 0.257-0.810 |
| Not detected | 1 | 71 | ||||||
| 20% | Detected | 4 | 3 | 80.0% | 96.0% | 0.109 | 0.640 | 0.315-0.965 |
| Not detected | 1 | 72 | ||||||
| NRTIs | ||||||||
| 2% | Detected | 3 | 29 | 75.0% | 61.8% | <0.001 | 0.085 | -0.042-0.212 |
| Not detected | 1 | 47 | ||||||
| 5% | Detected | 3 | 30 | 75.0% | 60.5% | <0.001 | 0.080 | -0.042-0.202 |
| Not detected | 1 | 46 | ||||||
| 10% | Detected | 3 | 21 | 75.0% | 72.4% | <0.001 | 0.141 | -0.033-0.315 |
| Not detected | 1 | 55 | ||||||
| 15% | Detected | 3 | 12 | 75.0% | 84.2% | 0.003 | 0.257 | -0.004-0.518 |
| Not detected | 1 | 64 | ||||||
| 20% | Detected | 2 | 11 | 50.0% | 86.8% | 0.006 | 0.278 | 0.004-0.552 |
| Not detected | 1 | 66 | ||||||
| NNRTIs | ||||||||
| 2% | Detected | 11 | 10 | 84.6% | 85.1% | 0.019 | 0.558 | 0.342-0.774 |
| Not detected | 2 | 57 | ||||||
| 5% | Detected | 11 | 8 | 84.6% | 88.1% | <0.001 | 0.409 | 0.168-0.650 |
| Not detected | 2 | 59 | ||||||
| 10% | Detected | 11 | 9 | 84.6% | 86.6% | 0.033 | 0.585 | 0.369-0.801 |
| Not detected | 2 | 58 | ||||||
| 15% | detected | 11 | 8 | 84.6% | 88.1% | 0.055 | 0.613 | 0.399-0.823 |
| Not detected | 2 | 59 | ||||||
| 20% | Detected | 11 | 7 | 84.6% | 89.6% | <0.001 | 0.599 | 0.322-0.796 |
| Not detected | 2 | 60 | ||||||
| Any mutation | ||||||||
| 2% | Detected | 20 | 32 | 87.0% | 43.9% | <0.001 | 0.224 | 0.071-0.377 |
| Not detected | 3 | 25 | ||||||
| 5% | Detected | 21 | 30 | 91.3% | 47.4% | <0.001 | 0.284 | 0.131-0.437 |
| Not detected | 2 | 27 | ||||||
| 10% | Detected | 19 | 25 | 82.6% | 56.1% | <0.001 | 0.305 | 0.129-0.481 |
| Not detected | 4 | 32 | ||||||
| 15% | Detected | 19 | 18 | 82.6% | 68.4% | <0.001 | 0.417 | 0.231-0.603 |
| Not detected | 4 | 39 | ||||||
| 20% | Detected | 17 | 19 | 81.0% | 67.8% | <0.001 | 0.396 | 0.206-0.586 |
| Not detected | 4 | 40 | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



