
Submitted:
30 September 2024
Posted:
01 October 2024
You are already at the latest version
Abstract
Objectives: The male urethra is a complex structure that plays a critical role in genitourinary health and function. Despite its importance, histological descriptions of the penile urethra, par-ticularly its epithelial components, remain incomplete. This study offers a comprehensive his-tological analysis of the penile urethra, focusing on the epithelium across distinct anatomical regions, including the glans, distal and proximal fossa navicularis, and spongy urethra. Meth-ods: Utilizing four human penile specimens, we employed various staining techniques to eluci-date the structural characteristics of these epithelial tissues. Results: Our findings reveal notable variations in epithelial composition, such as the presence of glycogen-rich cells in the distal fos-sa navicularis and the presence of mucous glands in the spongy urethra and proximal fossa na-vicularis. Additionally, we identified a previously underreported valvule-like structure in the distal fossa navicularis in two of the specimens. Conclusions: This study provides new insights into the histological organization of the penile urethra, offering critical reference data that can enhance our understanding of urethral pathologies and improve the outcomes of surgical inter-ventions, particularly in the context of tissue engineering and reconstructive surgery.
Keywords:
urethra
; epithelium
; fossa navicularis
; glycogen
; gland
1. Introduction
The male urethra can be susceptible to various pathologies, such as hypospadias or stenosis, which often require surgical intervention to restore function [1,2]. Current clinical treatments predominantly rely on the oral mucosa harvested from the inner cheek [3,4]. This tissue is advantageous due to its constant exposure to a humid environment, similar to that of the urethra. However, notable differences exist between oral and urethral mucosa and harvesting oral mucosa can lead to complications at the donor site. Additionally, the limited quantity of tissue that can be harvested may be insufficient in some cases.
In light of these challenges, alternative sources of graftable tissues have been actively pursued, with tissue engineering emerging as a promising solution over the past few decades [5,6]. Tissue engineering enables the reconstruction of tissues in the laboratory, providing potential substitutes for organs or serving as preclinical models [7,8,9]. Regardless of the intended application, a precise understanding of the function and histology of a target tissue is essential.
Histological knowledge of the human male urethra is relatively incomplete. From the prostate to the urinary meatus, the literature generally describes two types of epithelia [10]. However, a few studies have reported additional epithelia types, particularly in specific regions such as the distal Fossa Navicularis. For example, Holstein et al. described a region in the distal Fossa Navicularis containing cells rich in glycogen, which they hypothesized may play a role in protecting against urinary tract infection [11].
To advance our understanding of the human urethral histology, it is crucial to conduct a detailed study of the urethra, defining its distinct regions and transition zones. Such research is particularly important for tissue engineering, where accurately replicating the native urethra is key to ensuring the functionality of engineered substitutes. This study, based on 4 specimens, aims to provide valuable insights for clinicians and researchers alike, offering a comprehensive and up to date reference for the human urethra’s histological organization.
2. Materials and Methods
2.1. Ethic
This study was conducted according to the Declaration of Helsinki and was approved by the institution’s committee for the protection of human participants (Comité d’éthique de la recherche du CHU de Québec-Université Laval, protocol number 2012-1341). All patients provided informed written consent prior to organ collect.
2.2. Organ Collect and Preparation
Four penises were collected following a sex affirming surgery. Prior to the operation, the patients underwent a two-year anti-androgen treatment. After removal, the penises were dissected to remove the two cavernous bodies and the skin, leaving the urethra and the glans intact. The penises were then longitudinally sectioned on the ventral side, leaving the dorsal side untouched (Figure 1). They were then stored in formol to prevent them from degrading until they were embedded in paraffin in preparation for staining.
2.3. Histological Studies
2.3.1. Staining
Four staining were applied for each penis.
The hematoxylin and eosin staining (H&E) uses two dyes to differentiate cellular components. The basic dye (hematoxylin) stains the nuclei of the cells. The acidic dye (eosin) stains the cytoplasm. Muscles cells and collagen fibers can also be seen in dark pink and bright pink, respectively.
The Laidlaw coloration was used to see the reticulin fibers, which are highlighted in black by ammoniacal silver nitrate.
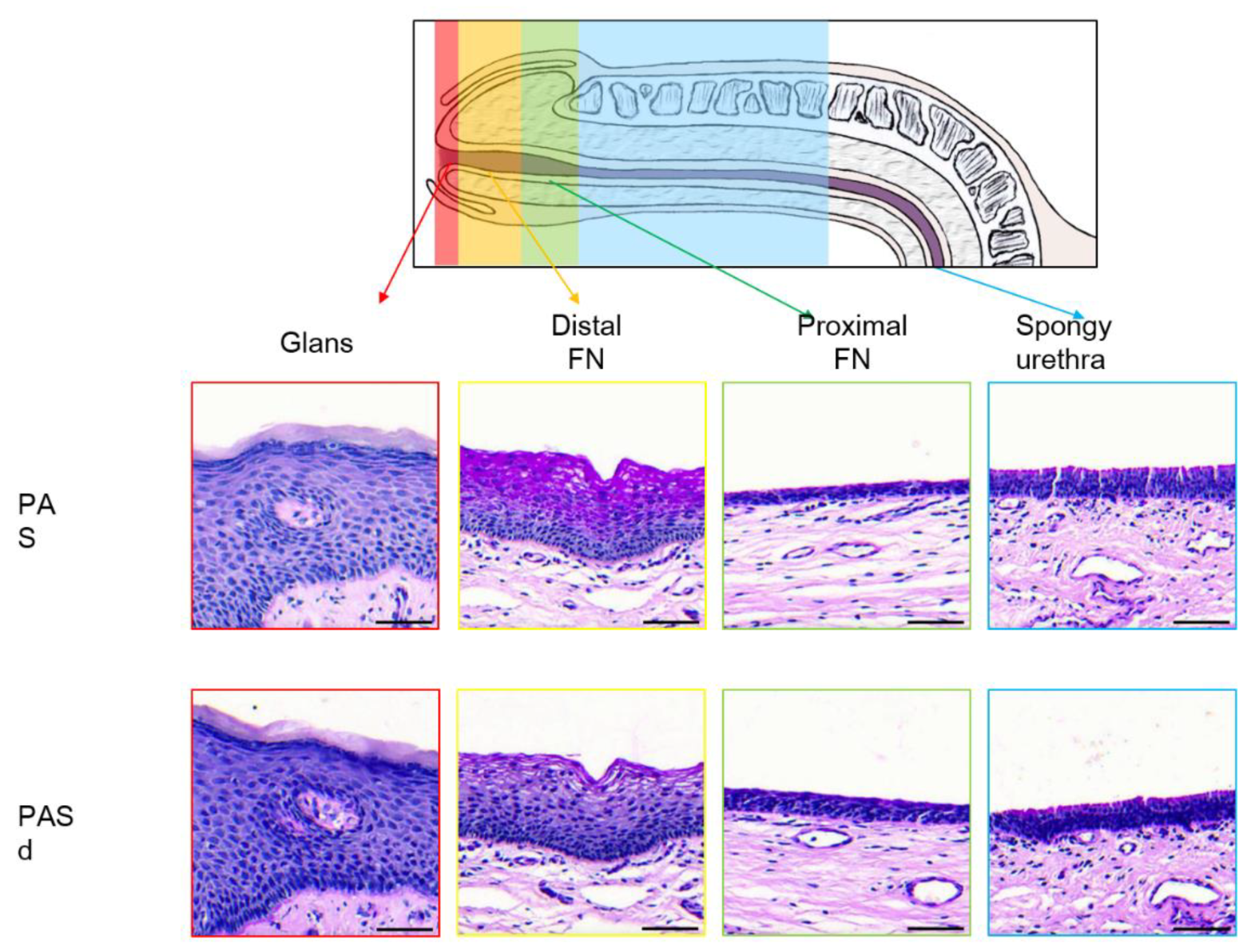
The Periodic Acid Schiff (PAS) was used to highlight the glycogen in the cells of the distal fossa navicularis. The periodic acid colors the glycogen in a bright pink/purple. Since this staining technique targets carbohydrates, mucins were also stained with a similar coloration. As a negative control, an enzymatic solution containing diastase was used to digest the glycogen, which removes the bright pink/purple coloration that is normally seen in the epithelium. The sections were treated with the solution for 60 minutes at 37°C before undergoing standard PAS staining. Since the diastase did not digest the mucins, they remained pink/purple in the PAS-digested (PASd) slides.
The Alcian Blue targets acidic substances. In this case, mucins were principally stained with a bright blue. The alcian blue itself is responsible for staining the mucins.
2.3.2. Microscope Observation
The slides were observed with a Zeiss Axioplan microscope and scanned with a Motic EasyScan. ImageJ was then used to create the different figures present in this article. Since the penises were cut on the ventral side, all the observation are from the dorsal part of the penis.
3. Results
3.1. Epithelium of the Glans
The glans is covered by a stratified squamous epithelium topped with a keratinized layer (Figure 2A). Using the Laidlaw staining, the basal membrane can be seen, formed by a layer containing reticulin fibers (Figure 2B). The cells closer to the basal membrane are smaller and have a more cuboidal shape than the ones found in the middle and upper layer, which are more flattened. The cells closer to the lumen undergo deterioration to form the keratinized layer. Excretory ducts can be observed piercing through the epithelium, suggesting the presence of glands in the connective tissue. Dermal papillae, projections of the connective tissue into the epithelium, are seen at the junction between the connective tissue and the epithelium. The comparison between the PAS (Figure 2C) and PASd (Figure 2D) staining shows no presence of glycogen in this epithelium.
3.2. Epithelium of the Distal Fossa Navicularis (DFN)
Dermal papillae which are present near the transition with the glans (Figure 3A,B), are notably absent in the rest of the fossa (Figure 4A).
The DFN is covered by a stratified squamous epithelium, similar to the one of the glans (Figure 4A). However, there are no keratinized layer or excretory ducts. The basal membrane highlighted by the Laidlaw staining is also observed in this part of the urethra (Figure 4B). A comparison between the PAS (Figure 4C) and PASd (Figure 4D) staining reveals the presence of glycogen in the upper section of the epithelium. In the three other stains, the PAS-positive cells exhibit a larger cytoplasm, allowing space for storing extra glycogen (Figure 4D, insert D1).
3.3. Epithelium of the Proximal Fossa Navicularis (PFN)
The PFN is covered by a stratified squamous epithelium, which although similar in structure, has less cells layers than the ones observed in the glans and the DFN (Figure 5A). Unlike the glans and similar to the DFN, the epithelium lacks both the keratin layer and dermal papillae. One distinctive aspect of this epithelium is the presence of mucous glands and excretory ducts, which react to the Alcian Blue staining, suggesting an acidic secretion. As seen in the previous two sections, the basement membrane is also stained in black by the Laidlaw staining (Figure 5B). The comparison between the PAS (Figure 5C) and PASd (Figure 5D) staining reveals that there is no glycogen in this epithelium.
3.4. Epithelium of the Spongy Urethra
The spongy urethra is lined by a rectangular pseudostratified epithelium. Similarly to the one found in the PFN, it has no keratinized layer or dermal papillae (Figure 6A). Within this epithelium, mucous glands are present, similar to those found in the PFN (Figure 6B). However, the ones found in the spongy urethra are often larger in size than the ones in the PFN. They produce a mucoid substance similar to the ones found in the PFN, as the secretory cells are also stained by the Alcian Blue (Figure 7). The basement membrane is still visible when the Laidlaw staining is applied (Figure 6B). The comparison between the PAS (Figure 6C) and PASd (Figure 6D) staining reveals once again that there is no glycogen in this part of the urethra.
3.5. Valvule-Like Structure
In two of the examined penises, a valvule-like structure was identified in the epithelium of the DFN (Figure 8A). This structure causes a noticeable change in the epithelial thickness on either side of the valve. On the distal side (nearest of the glans), the epithelium maintains the characteristics of the DFN (Figure 8A1). However, soon after the valvule and for approximatively 3 millimetres on the proximal side of the valvule (nearest of the prostate), the epithelium becomes thinner, resembling the one found in the PFN. Beyond this 3-millimeter region, the epithelium returns to the typical DFN morphology, continuing until it transitions into the PFN (Figure 8A2). Along with the changes in the epithelium, there are variations in the density of cells beneath the epithelium. On the distal side near the valvule, there is an increase in cell density (Figure 8A1). In contrast, on the proximal side after the valve, the cell density aligns with the more typical pattern observed throughout the rest of the urethra.
4. Discussion
The interest in making this study was to provide pictures of the different epitheliums found in the distal male urethra. Many articles describe with schematic forms what types of epitheliums are present in the urethra, but they often simplify the classification and do not provide pictures to back their observations. For example, an article published in Nature Reviews Urology only described two types of epitheliums in the spongy urethra without any pictures [10], whereas we observed 4 different sections and can provide pictures to back it. Some articles with pictures are available, but they are rare and often old. For example, one of the only article describing the majority of the epitheliums found in the urethra [11], contains few pictures. Also, these pictures were good for the time, but limit the interpretations we can make, notably because they are not colored. These article also do not provide a systematic review of all the epithelium. The authors will select specific regions of interest and ignore the transitions between the different ones.
The epithelial tissues found in the distal male urethra can be categorized into four distinct types (Figure 9). The glans is lined with a stratified squamous epithelium with excretory ducts. It is the only epithelium in the urethra with dermal papillae and a keratin layer. For the distal fossa navicularis, the epithelium is also stratified and squamous but lacks the excretory ducts. Notably, this is the only epithelium in the urethra containing glycogen. Additionally, a valvule was observed in this region of the urethra in two out of the four penises examined. The proximal fossa navicularis features a smaller stratified squamous epithelium with excretory ducts and glands. Finally, the spongy urethra has a rectangular pseudostratified epithelium, also containing glands and excretory ducts. Those observations were consistent with the four penises observed.
Our description of the epithelium lining the glans aligns with that provided by Holstein et al [11] but expends the finding by noting the presence of dermal papillae and excretory ducts that are in this epithelium. The distal fossa navicularis is consistent with the description from both Holstein and Hausmann [12]. In the proximal portion of the fossa navicularis, our observations are similar to those of Hausmann and Holstein, although neither study reported the mucous glands we identified. The epithelium lining the spongy urethra in our observations corresponds with descriptions found in various articles [11,13,14].
The urethra contains various epithelial structures, each serving a distinct function. The keratinized epithelium found in the glans provides a better protection against friction. The dermal papillae, rich in small blood vessels, ensure an adequate vascularisation [15], which is essential since this epithelium has multiple cell layers. The epithelium of the distal fossa navicularis contains glycogen in its upper layers, which provides a substrate for Lactobacillus bacteria, similar to those found in the vagina. These bacteria create an acidic environment that protects the urethra from ascending pathogens [11,16]. These lactobacilli constitute the normal FN microbiota, and can have various roles as demonstrated in FN or vagina: modulate the inflammatory response [17,18], promote wound closure [18] and protect against infections [19]. Protection from microbial, bacterial or viral infections is primarily due to the mucus, which traps microbes, but also to the acidification of the environment through the production of lactic acid [20,21]. There is also production of hydrogen peroxide and bacteriocins [22,23]. Finally, this flora competes directly with pathogens for their adhesion sites. A faster wound healing also limits the entry of pathogens. A decrease in lactobacilli in the FN or vagina correlates with an increase in sexually transmitted infections [19,24,25,26,27,28]. The epithelium in the spongy urethra, which expands through most of the urethra [1], forms an impermeable route for the urine and the sperm to exit the body, while protecting the underlying tissue [29].
These diverse epithelial structures found in the urethra highlight the importance of integrating the multiple types of epitheliums observed when reconstructing a urethra for patients with hypospadias. While the urothelium provides an impermeable pathway for the urine and the sperm, the epithelium of the distal fossa navicularis offers protection against infections. Current gold-standard tissue engineering techniques for urethral reconstruction only uses the urothelium [10], but this approach does not utilize the protection offered by the fossa navicularis.
Along the urethra, many glands can be found, either in the epithelium or in the stroma. They are mostly present in the distal part of the spongy urethra and at the proximal end of the proximal fossa navicularis. These glands correspond to Littré’s glands [30]. Two types were described by Krstić. The ones present in the epithelium are small and containing mucus secretive cells. The one in the connective tissue are bigger and have excretory ducts opening into the epithelium [14]. We observed both types in our penises. The mucus secreted by these glands contains glycosaminoglycans, which protects the epithelium from the urine and the pathogens and lubricates the urethra to allow a better passage from the urine and sperm [14,31,32].
Beneath the epithelium lies a dense network of blood vessels, which ensures efficient distribution of nutriments. Since there is no vascularisation in the epithelium, the cells must get their nutriments and get rid of their waste through diffusion, explaining the need of intense vascularisation under the basal membrane.
The two valvules seen in the distal fossa navicularis have previously been described as the lacuna magna or sinus of Guérin [33]. This lacuna is formed by a septum (valve of Guérin), an extension of the ingrowth of the ectoderm that would normally form the distal fossa navicularis [34]. This lacuna may also cause different symptoms, such as dysuria and post-void bloody spotting [35]. Shenoy also describes the valve of Guérin as a “horizontal bar stretched across the roof of the navicular fossa” and documented observing it in 98% of cases. A reason explaining why we only found this valve in 50% of our penises comes from its small size and its localisation varying from one person to another [36].
A limitation in this study comes from the facts that all the patients underwent a minimum of two year of hormonal treatment prior to sex affirmation surgery. Given that estrogen treatments can cause expansion of the distal fossa navicularis [11], it is possible that this area expanded, altering the organisation of the urethra. However, this expansion could be advantageous for these patients. Specifically, if cells from the distal fossa are extracted and harvested, they could be used in tissue engineering to create vaginal-like tissue, which could then be grafted during the surgery. This approach may offer a better alternative to the current gold standard in vaginoplasty, which is penile inversion [36]. Penile inversion has several downsides, including limited tissue availability and the absence of protective vaginal flora. At this moment, the only tissue engineering methods available for vaginoplasty uses buccal mucosa cells [37]. However, this technique takes time and can create morbidity at the donor site [38]. An engineered tissue coming from the patient distal fossa navicularis could provide a better protection against pathogens and HIV [16], while also reducing the need of fetching tissues from other sites [39].
5. Conclusions
To conclude, the epithelium of the penile urethra is composed of at least 4 distinct zones which present a different histological organization adapted to physiological functions. The epithelium of the Fossa Navicularis shows a histology close to that of the vagina with the function of serving as a gate-keeper to prevent the entry of bacteria. The reconstruction of such an area could be considered during reconstruction by tissue engineering, particularly in the case of treatment of hypospadias, in order to limit potential bacterial infection.
Supplementary Materials
The following supporting information can be downloaded at: www.mdpi.com/xxx/s1, Figure S1: title: Representative photographs of Hematoxylin-Eosin staining of the urethra; www.mdpi.com/xxx/s2, Figure S2: title: Representative photographs of Laidlaw coloration of the urethra; www.mdpi.com/xxx/s3, Figure S3: title: Representative photographs of the Periodic-Acid Schiff staining of the urethra; www.mdpi.com/xxx/s4, Figure S4: title Representative photographs of the Periodic-Acid Schiff staining of the urethra after diastase digestion;.
Author Contributions
Concept/design: DB and SC; Data acquisition: MD, DB, SB, and AL; Data analyses/interpretation: MD, DB, SC, and EP; Manuscript drafting: MD; Critical revision: DB, SC and SB; Approval: MD, DB, SC, AL, EP, and SB.
Funding
This study was supported by a New Frontiers Exploration Research fund (NFRFE-2023-00113 ), a Canadian Urological Association scholarship fund and, the Canadian Institutes of Health Research #258229.
Institutional Review Board Statement
This study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Ethics Committee of the CHU de Québec (protocol code 2012-1341, DR-002-1190, approved and renewed annually since December 2013).
Informed Consent Statement
All patients provided informed written consent prior to biopsies.
Data Availability Statement
Data are available upon reasonable request.
Acknowledgments
The authors want to acknowledge the Quebec Cell, Tissue and Gene Therapy Network-ThéCell (a thematic network supported by the FRQS).
Conflicts of Interest
The authors declare no conflict of interest.
References
- Elia E, Caneparo C, McMartin C, Chabaud S and Bolduc S 2024 Tissue Engineering for Penile Reconstruction. Bioengineering (Basel) 11.
- Caneparo C, Brownell D, Chabaud S and Bolduc S 2021 Genitourinary Tissue Engineering: Reconstruction and Research Models. Bioengineering (Basel) 8.
- Dessanti A, Rigamonti W, Merulla V, Falchetti D and Caccia G 1992 Autologous buccal mucosa graft for hypospadias repair: an initial report. J Urol 147 1081–3; discussion 1083-4.
- Cruz-Diaz O, Castellan M and Gosalbez R 2013 Use of buccal mucosa in hypospadias repair. Curr Urol Rep 14 366–72.
- Saad S, Osman N I and Chapple C R 2021 Tissue engineering: recent advances and review of clinical outcome for urethral strictures. Curr Opin Urol 31 498–503.
- Barbagli G, Heidenreich A, Zugor V, Karapanos L and Lazzeri M 2020 Urothelial or oral mucosa cells for tissue-engineered urethroplasty: A critical revision of the clinical outcome. Asian J Urol 7 18–23.
- Bédard P, Gauvin S, Ferland K, Caneparo C, Pellerin È, Chabaud S and Bolduc S 2020 Innovative Human Three-Dimensional Tissue-Engineered Models as an Alternative to Animal Testing. Bioengineering (Basel) 7.
- Saba I, Jakubowska W, Bolduc S and Chabaud S 2018 Engineering Tissues without the Use of a Synthetic Scaffold: A Twenty-Year History of the Self-Assembly Method Biomed Res Int 2018 1–13.
- Roy V, Magne B, Vaillancourt-Audet M, Blais M, Chabaud S, Grammond E, Piquet L, Fradette J, Laverdière I, Moulin V J, Landreville S, Germain L, Auger F A, Gros-Louis F and Bolduc S 2020 Human Organ-Specific 3D Cancer Models Produced by the Stromal Self-Assembly Method of Tissue Engineering for the Study of Solid Tumors. Biomed Res Int 2020 6051210.
- Pederzoli F, Joice G, Salonia A, Bivalacqua T J and Sopko N A 2019 Regenerative and engineered options for urethroplasty Nat Rev Urol 16 453–64.
- Holstein A F, Davidoff M S, Breucker H, Countouris N and Orlandini G 1991 Different epithelia in the distal human male urethra Cell Tissue Res 264 23–32.
- Hausmann R and Schellmann B 1994 Forensic value of the Lugol’s staining method: further studies on glycogenated epithelium in the male urinary tract Int J Legal Med 107 147–51.
- Hossler F E . 2014 Ultrastructure atlas of human tissues.
- Krstić R V. 1991 Urogenital Apparatus Human Microscopic Anatomy (Berlin, Heidelberg: Springer Berlin Heidelberg) pp 295–437.
- Barbieri J S, Wanat K and Seykora J 2014 Skin: Basic Structure and Function Pathobiology of Human Disease (Elsevier) pp 1134–44.
- Saba I, Barat C, Chabaud S, Reyjon N, Leclerc M, Jakubowska W, Orabi H, Lachhab A, Pelletier M, Tremblay M J and Bolduc S 2021 Immunocompetent Human 3D Organ-Specific Hormone-Responding Vaginal Mucosa Model of HIV-1 Infection Tissue Eng Part C Methods 27 152–66.
- Mohtashami M, Mohamadi M, Azimi-Nezhad M, Saeidi J, Nia FF, Ghasemi A. Lactobacillus bulgaricus and Lactobacillus plantarum improve diabetic wound healing through modulating inflammatory factors. Biotechnol Appl Biochem. 2021 Dec;68(6):1421-1431.
- Takada K, Komine-Aizawa S, Kuramochi T, Ito S, Trinh QD, Pham NTK, Sasano M, Hayakawa S. Lactobacillus crispatus accelerates re-epithelialization in vaginal epithelial cell line MS74. Am J Reprod Immunol. 2018 Sep;80(3):e13027.
- Bowie WR, Pollock HM, Forsyth PS, Floyd JF, Alexander ER, Wang SP, Holmes KK. Bacteriology of the urethra in normal men and men with nongonococcal urethritis. J Clin Microbiol. 1977 Nov;6(5):482-8.
- O’Hanlon DE, Moench TR, Cone RA. Vaginal pH and microbicidal lactic acid when lactobacilli dominate the microbiota. PLoS One. 2013 Nov 6;8(11):e80074.
- Aldunate M, Tyssen D, Johnson A, Zakir T, Sonza S, Moench T, Cone R, Tachedjian G. Vaginal concentrations of lactic acid potently inactivate HIV. J Antimicrob Chemother. 2013 Sep;68(9):2015-25.
- Atassi F, Servin AL. Individual and co-operative roles of lactic acid and hydrogen peroxide in the killing activity of enteric strain Lactobacillus johnsonii NCC933 and vaginal strain Lactobacillus gasseri KS120.1 against enteric, uropathogenic and vaginosis-associated pathogens. FEMS Microbiol Lett. 2010 Mar;304(1):29-38.
- Spurbeck RR, Arvidson CG. Lactobacilli at the front line of defense against vaginally acquired infections. Future Microbiol. 2011 May;6(5):567-82.
- Unemo M, Bradshaw CS, Hocking JS, de Vries HJC, Francis SC, Mabey D, Marrazzo JM, Sonder GJB, Schwebke JR, Hoornenborg E, Peeling RW, Philip SS, Low N, Fairley CK. Sexually transmitted infections: challenges ahead. Lancet Infect Dis. 2017 Aug;17(8):e235-e279.
- Petrova MI, van den Broek M, Balzarini J, Vanderleyden J, Lebeer S. Vaginal microbiota and its role in HIV transmission and infection. FEMS Microbiol Rev. 2013 Sep;37(5):762-92.
- Martin, DH. The microbiota of the vagina and its influence on women’s health and disease. Am J Med Sci. 2012 Jan;343(1):2-9.
- Schwebke, JR. Abnormal vaginal flora as a biological risk factor for acquisition of HIV infection and sexually transmitted diseases. J Infect Dis. 2005 Oct 15;192(8):1315-7.
- Schwebke JR, Desmond R. A randomized trial of metronidazole in asymptomatic bacterial vaginosis to prevent the acquisition of sexually transmitted diseases. Am J Obstet Gynecol. 2007 Jun;196(6):517.e1-6.
- Caneparo C, Chabaud S and Bolduc S 2021 Reconstruction of Vascular and Urologic Tubular Grafts by Tissue Engineering Processes 9 513.
- Dictionnaire médical de l’Académie de Médecine.
- Isola M, CossuM, DeLisa A, Isola R, Massa D, Casti A, Solinas P and Lantini M S 2010 Oxytocin Immunoreactivity in the Human Urethral (Littre’s) Glands Journal of Reproduction and Development 56 94–7.
- Zechhi-Orlandini S, Gulisano M, Orlandini G E and Holstein A F 2009 Scanning Electron Microscopic Observations on the Epithelium of the Human Spongy Urethra Andrologia 20 132–7.
- Serbanoiu A, Ion R T, Filipoiu F, Tulin A and Enyedi M 2024 Dissection of the Male Urethra Demonstrating Its Topographical Specificity. Cureus 16 e65946.
- Kajbafzadeh A 2005 Congenital Urethral Anomalies in Boys. Part II Urol J 2 125–31.
- Shenoy S P, Marla P K, Venugopal P, Adappa K K, Tantry T P, Shankar M and Rai G D 2011 An Endoscopic Study of the Lacuna Magna and Reappraisal of Its Clinical Significance in Contemporary Urological Practice Urology 78 1009–15.
- Pariser J J and Kim N 2019 Transgender vaginoplasty: Techniques and outcomes Transl Androl Urol 8 241–7.
- Dessy L A, Mazzocchi M, Corrias F, Ceccarelli S, Marchese C and Scuderi N 2014 The use of cultured autologous oral epithelial cells for vaginoplasty in male-to-female transsexuals: A feasibility, safety, and advantageousness clinical pilot study Plast Reconstr Surg 133 158–61.
- Sueters J, Groenman F A, Bouman M-B, Roovers J P W, de Vries R, Smit T H and Huirne J A F 2023 Tissue Engineering Neovagina for Vaginoplasty in Mayer–Rokitansky–Küster–Hauser Syndrome and Gender Dysphoria Patients: A Systematic Review Tissue Eng Part B Rev 29 28–46.
- Bustos S S, Bustos V P, Mascaro A, Ciudad P, Forte A J, Del Corral G and Manrique O J 2021 Complications and Patient-reported Outcomes in Transfemale Vaginoplasty: An Updated Systematic Review and Meta-analysis Plast Reconstr Surg Glob Open 9 e3510.
Figure 1.
Urethra collection from male-to-female vaginoplasty surgery. A schematic representation of the region collected from the penis, A. A representative photo of a specimen, B. Puncture wounds are seen in the distal fossa (red circle). This specimen presented a macroscopically visible valvule (black circle).
Figure 1.
Urethra collection from male-to-female vaginoplasty surgery. A schematic representation of the region collected from the penis, A. A representative photo of a specimen, B. Puncture wounds are seen in the distal fossa (red circle). This specimen presented a macroscopically visible valvule (black circle).
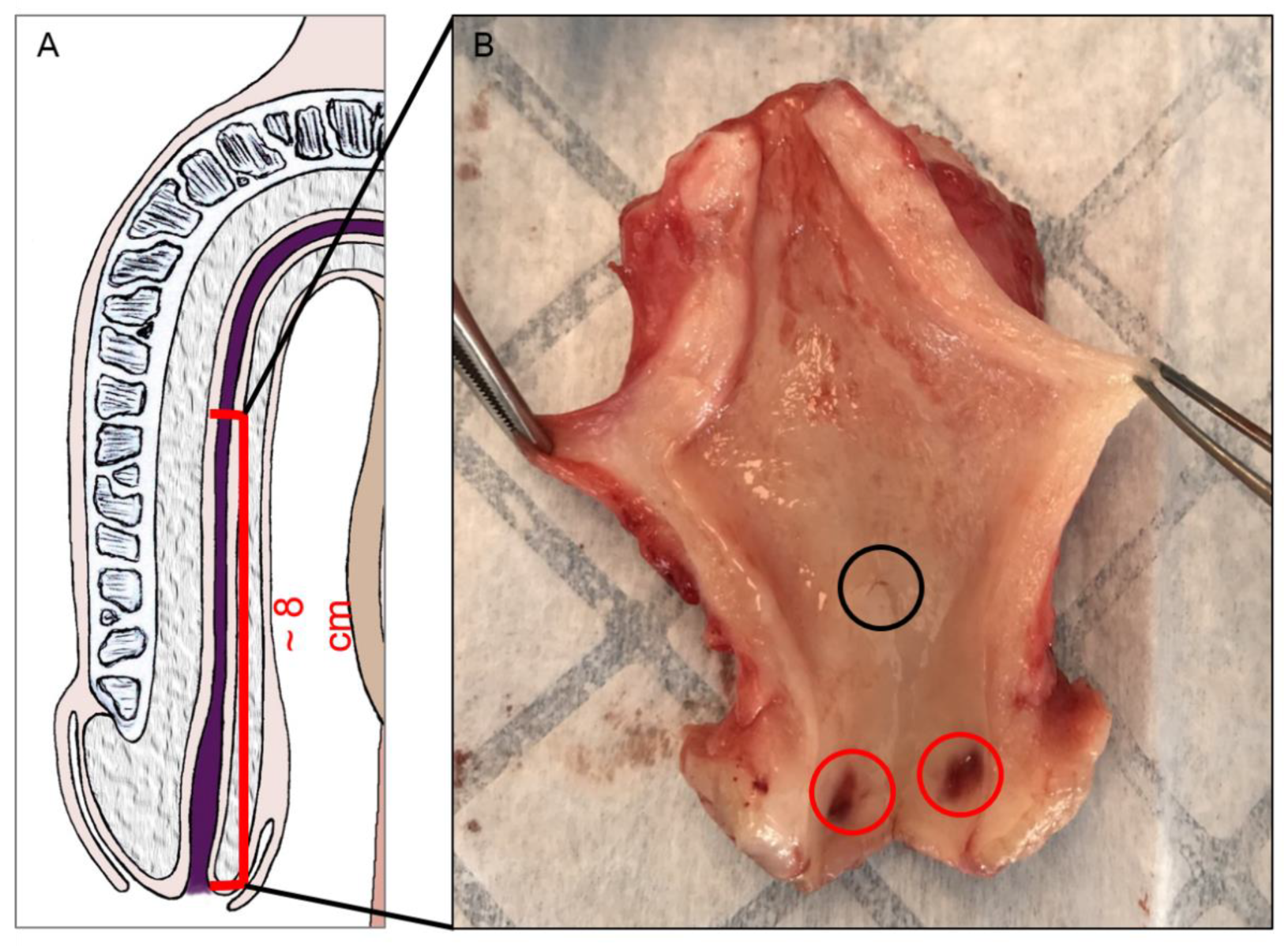
Figure 2.
The glandular urethra. H&E (A), Laidlaw (B), PAS (C), and PASd (D) staining of the glandular urethra. Blue arrows highlight the keratin layer. Excretory ducts are pointed to by black triangles. Dermal papillae are labelled with yellow arrows. The basal membrane marked by a yellow star. Scale bars represent 100µm.
Figure 2.
The glandular urethra. H&E (A), Laidlaw (B), PAS (C), and PASd (D) staining of the glandular urethra. Blue arrows highlight the keratin layer. Excretory ducts are pointed to by black triangles. Dermal papillae are labelled with yellow arrows. The basal membrane marked by a yellow star. Scale bars represent 100µm.
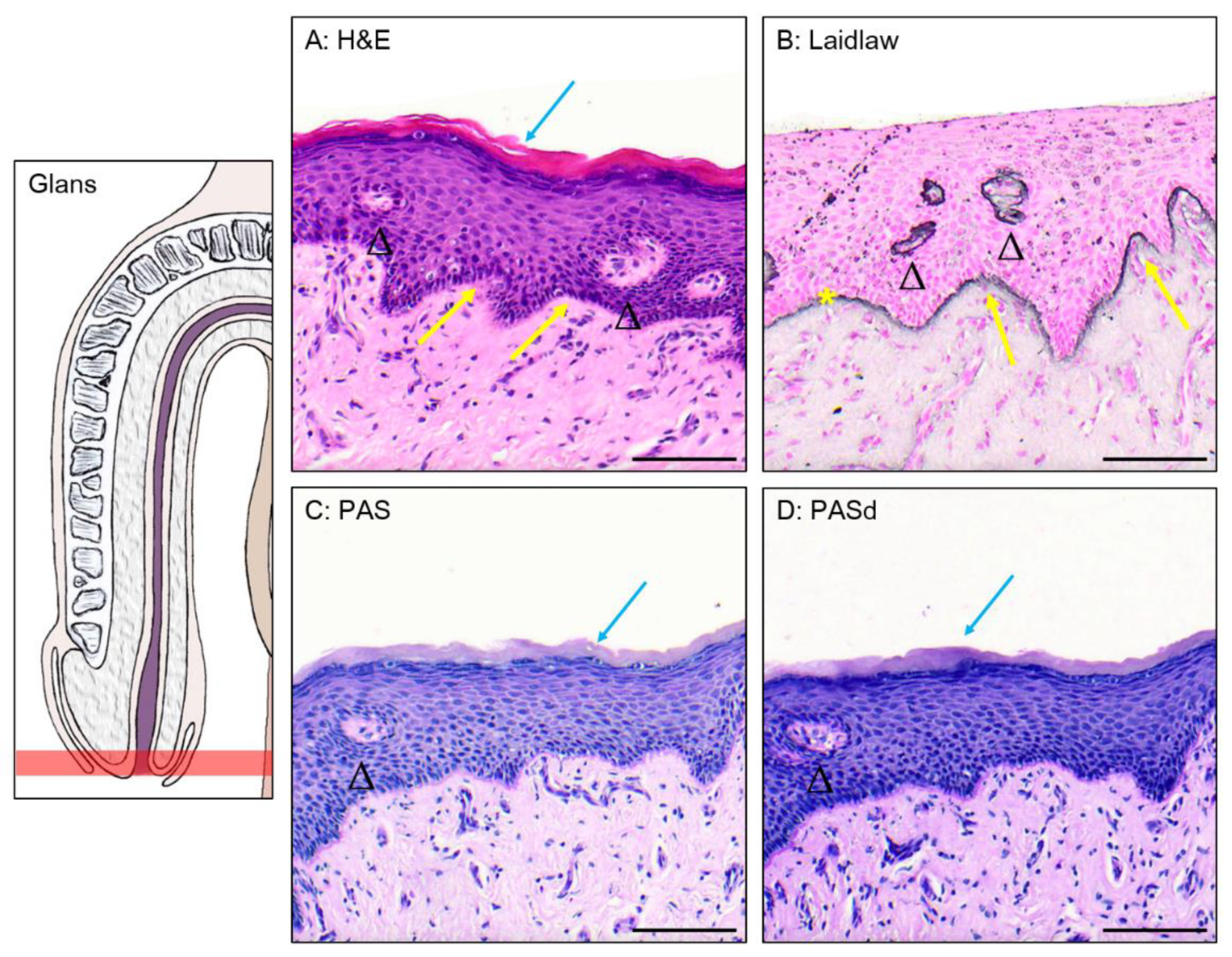
Figure 3.
The glans-FN epithelial transition. PAS (A) and PASd (B) staining of the glans-FN epithelial transition. Glycogen apparition is pointed to by white arrows. Excretory ducts are labelled by black triangles. Dermal papillae are labeled with yellow arrows. Scale bars represent 500 µm.
Figure 3.
The glans-FN epithelial transition. PAS (A) and PASd (B) staining of the glans-FN epithelial transition. Glycogen apparition is pointed to by white arrows. Excretory ducts are labelled by black triangles. Dermal papillae are labeled with yellow arrows. Scale bars represent 500 µm.
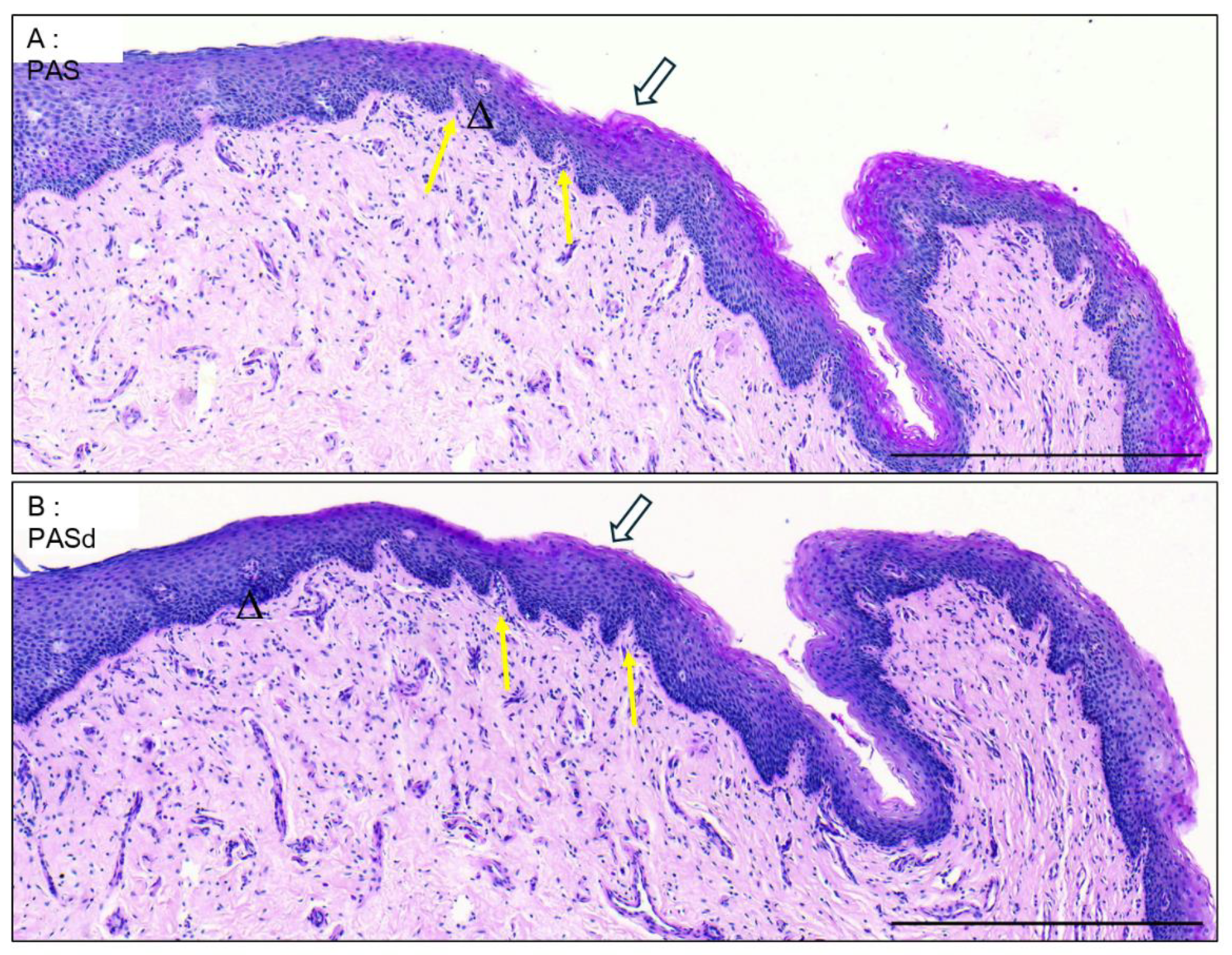
Figure 4.
The distal fossa navicularis. H&E (A), Laidlaw (B), PAS (C), and PASd (D) staining were performed. The basal membrane is marked by a yellow star. Some glycogenated cells are labelled with white arrows. D1 shows a zoom of the epithelium. Scale bars are 100µm for A,B,C,D and 50µm for D1.
Figure 4.
The distal fossa navicularis. H&E (A), Laidlaw (B), PAS (C), and PASd (D) staining were performed. The basal membrane is marked by a yellow star. Some glycogenated cells are labelled with white arrows. D1 shows a zoom of the epithelium. Scale bars are 100µm for A,B,C,D and 50µm for D1.
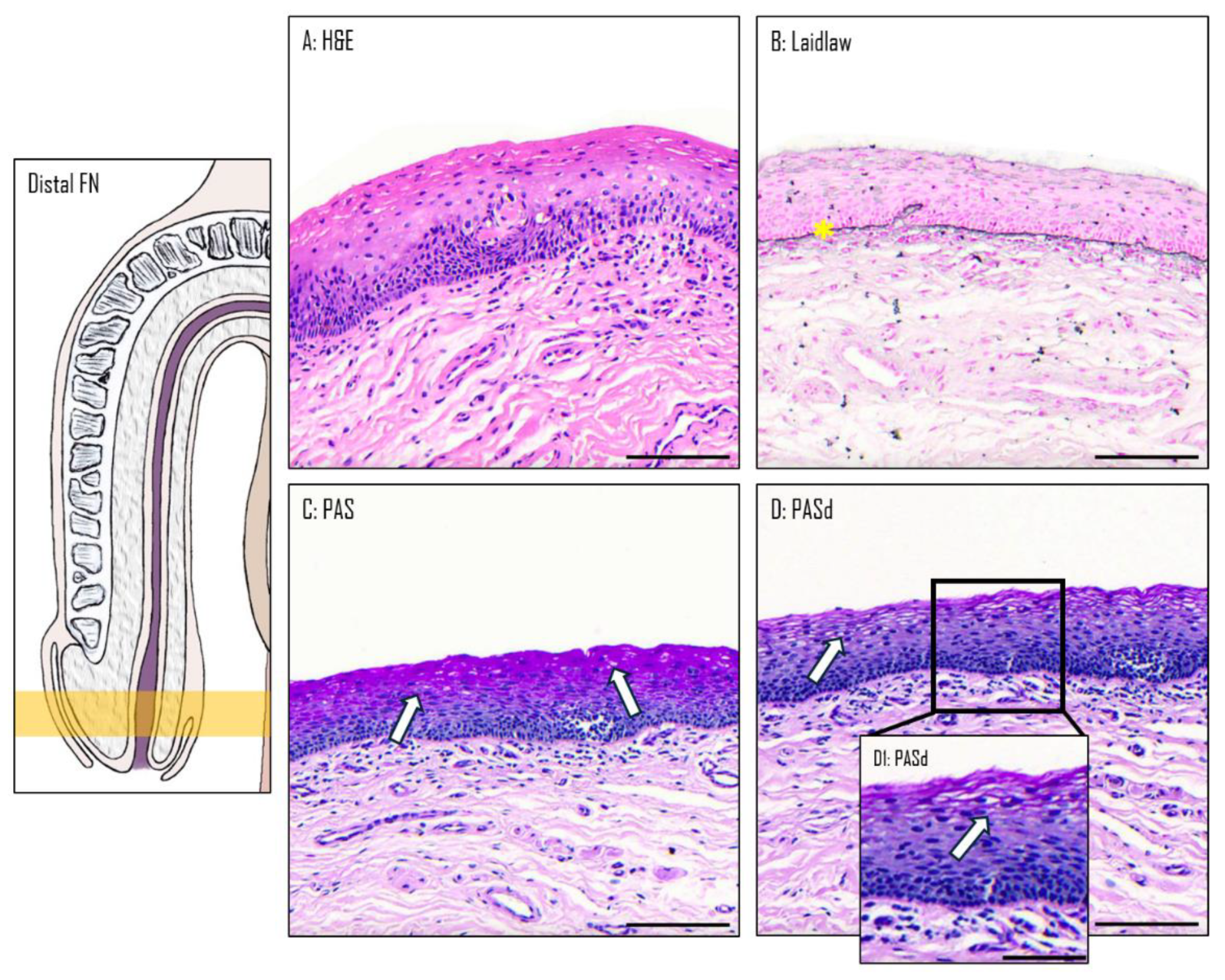
Figure 5.
The proximal fossa navicularis. H&E (A), Laidlaw (B), PAS (C), and PASd (D) staining were performed. A gland in the epithelium is labelled with a black triangle. The basal membrane is marked with a yellow star. Scale bars represent 100µm.
Figure 5.
The proximal fossa navicularis. H&E (A), Laidlaw (B), PAS (C), and PASd (D) staining were performed. A gland in the epithelium is labelled with a black triangle. The basal membrane is marked with a yellow star. Scale bars represent 100µm.

Figure 6.
The spongy urethra. H&E (A), Laidlaw (B), PAS (C), and PASd (D) staining were performed. Glands are labelled with black triangles. The basal membrane is labelled with yellow star. Scale bars represent 100µm.
Figure 6.
The spongy urethra. H&E (A), Laidlaw (B), PAS (C), and PASd (D) staining were performed. Glands are labelled with black triangles. The basal membrane is labelled with yellow star. Scale bars represent 100µm.
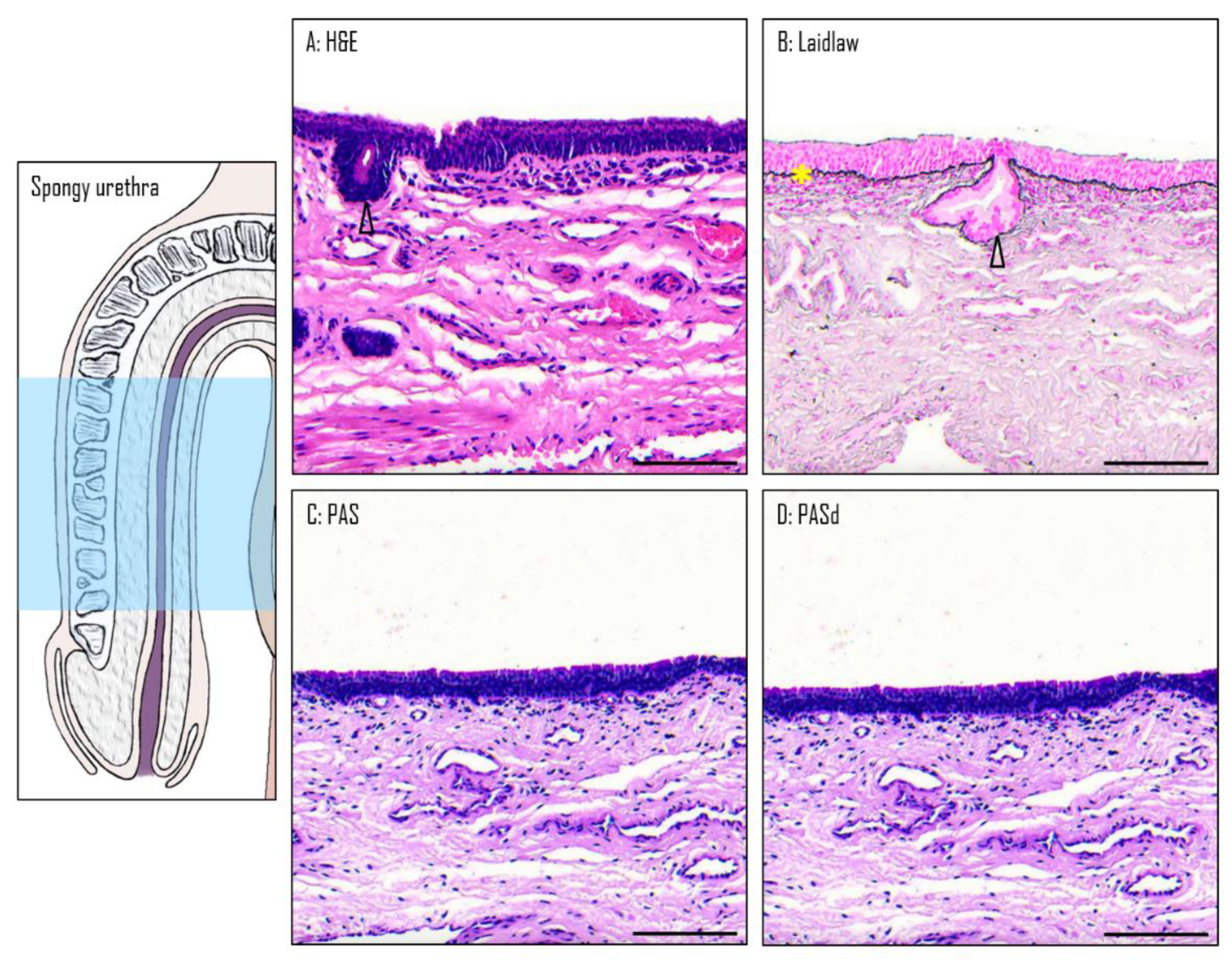
Figure 7.
Glands in the spongy urethra. Alcian Blue staining reveals large glandular structures (A). Details are seen in A1. Scale bars are 500 µm for A and 350 µm for A1.
Figure 7.
Glands in the spongy urethra. Alcian Blue staining reveals large glandular structures (A). Details are seen in A1. Scale bars are 500 µm for A and 350 µm for A1.
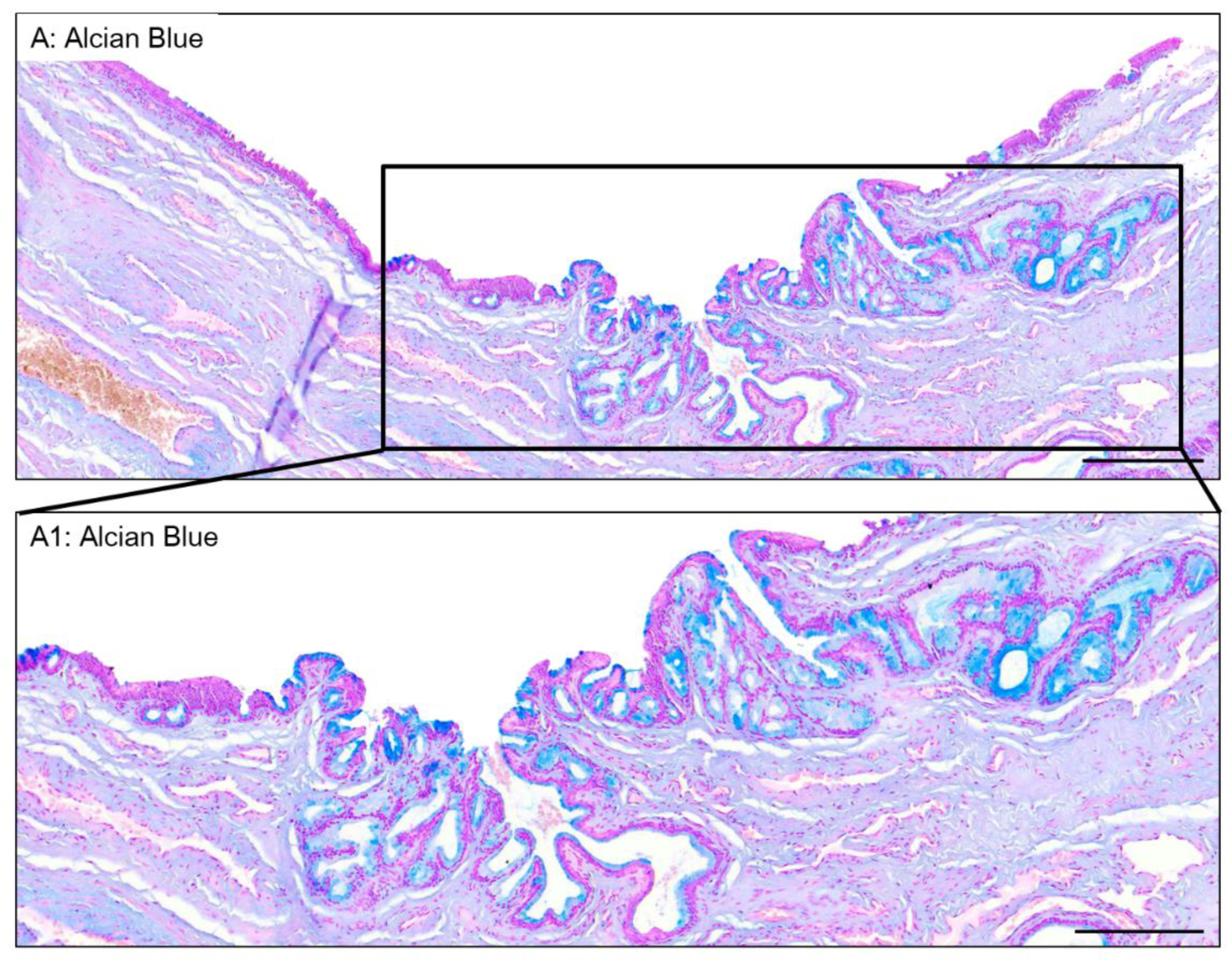
Figure 8.
The urethral valvule. H&E staining of the distal FN (A). The tissue is oriented with the glans to the left and the prostate to the right. A1 shows a zoom of the valvule. A2 shows a transition from a thin to a thick epithelium. High density stromal cells are pointed out with a black star. Glycogen containing cells are shown with a white arrow. Scale bars are 700 µm for A and 400 µm for A1 and A2.
Figure 8.
The urethral valvule. H&E staining of the distal FN (A). The tissue is oriented with the glans to the left and the prostate to the right. A1 shows a zoom of the valvule. A2 shows a transition from a thin to a thick epithelium. High density stromal cells are pointed out with a black star. Glycogen containing cells are shown with a white arrow. Scale bars are 700 µm for A and 400 µm for A1 and A2.
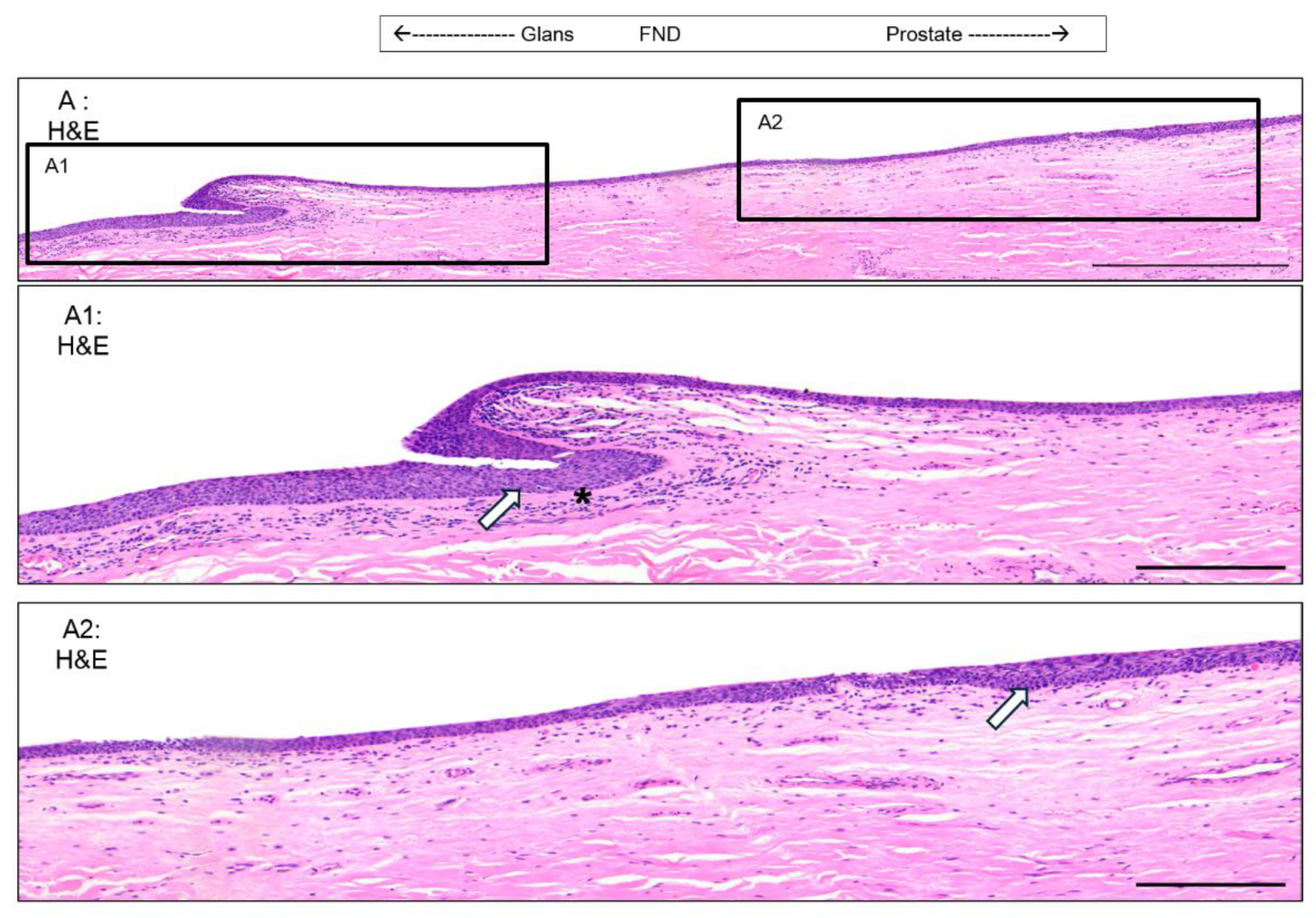
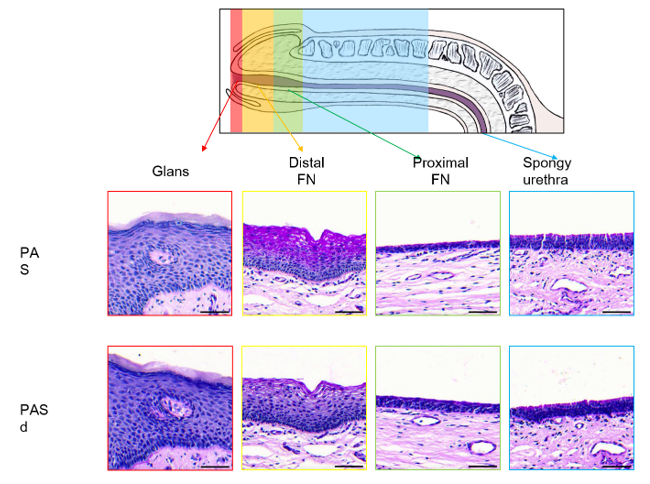
Figure 9.
Summary of the urethral epithelial histology from the gland to spongy urethra.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



