
Submitted:
01 October 2024
Posted:
02 October 2024
You are already at the latest version
Abstract
In vitro tests of cellular activity form part of the diagnostic algorithm of drug hypersensitivity reactions. Because of the wide range of pharmacological mechanisms, clinical symptoms, genetic components and laboratory tests, it is important to know how a particular test performs in the diagnostic procedure. We carried out the detailed retrospective analysis of more than 6,000 measurements of numerous drug compounds tested in the past 6 years. Our cell viability-based lymphocyte transformation had a coefficient of variation of 10% and showed similar performance over the whole range of tested ages. With an adequate number of parallel measurements, the test can identify modest increases in stimulation indices with high confidence. Similar percentages of analytically positive responses were observed for the three most frequently tested drug groups, namely antibiotics, non-steroid anti-inflammatory agents and anesthetics. These results confirm that cell viability tests are suitable alternatives of proliferation assays in drug allergy testing.
Keywords:
drug
; allergy
; lymphocyte transformation
; hypersensitivity
1. Introduction
Medicinal drugs are biologically active molecules introduced into the body with the aim of modulating biochemical events. While drugs are used to prevent or treat malfunctions of the organism, unintended effects may also be induced because of improper dosage, inadequate target specificity, drug interactions, genetic and physiological variability of the human population, temporal variance of physiology and combinations thereof [1,2]. When such adverse drug reactions are caused by the immune system [3,4,5], the term drug hypersensitivity is used, even though the exact mechanism is not necessarily conventional hypersensitivity [6]. If we consider only those adverse drug reactions where the mechanism is true hypersensitivity, the Coombs or modified Coombs categorization can be applied [7,8,9]. As a consequence of increasing medicine usage, the incidence of adverse reactions is on the rise [10].
Even if the clinical symptoms of adverse drug effects are unequivocally related to a single drug – which is less often the case – it is desirable to prove the causality for the diagnosis. Repeated introduction of the drug (drug provocation test) is a straightforward approach but, depending on the nature of symptoms, may impose high risk and require appropriate medical preparedness [11,12]. In vitro diagnostic tests are a possible alternative to provocation; however, it must be emphasized that these tests have limited sensitivity: a sample of blood can never mimic the fate of a drug molecule that is introduced into the body. Yet, if properly chosen, these tests can confirm that immunological mechanisms are responsible for the drug sensitivity [13,14]. Two main classes of tests are in use currently: immediate hypersensitivity reactions are tested for by basophil activation tests (BAT) [15,16]and its alternatives (mast cell tests) [17,18], while delayed type hypersensitivity can be detected by lymphocyte transformation test (LTT) [19,20,21]in general. Suspected drug molecules are mixed with the cells and biological responses are monitored.
LTT utilizes mononuclear cells isolated from peripheral blood by standard methods. Lymphocytes in this fraction of white blood cells are capable of responding to in vitro stimuli during cell culture by expressing activation markers, proliferation, secretion of cytokines [22,23,24,25,26]. Therefore, even though LTT originally referred to the blast transformation of lymphocytes and the measurement of proliferation [27], various techniques can be used to quantify the lymphocyte response [28]. Our laboratory uses a viability test based on enzyme activity [29], similar to those that have been successfully applied for drug allergy testing [30,31] . This approach basically quantifies the effects of a tested drug on the survival of the isolated blood cells; therefore, it gives a combined readout on proliferation and cell death. Since cellular activation is accompanied by the secretion of pro-survival and pro-proliferation factors, with the properly adjusted culture conditions (cell number, culturing time) viability is a useful readout.
The essence of LTT is to recognize when there is a difference between untreated (negative control) and the drug treated culture. This is a matter of statistics where the number of parallels, the expected and measured variance crucially influence the results [32,33]. An important confounding factor is the huge variability of baseline cellular proliferation and responsiveness even within a single individual [32,34]. This can be compensated for by increasing the number of parallel negative control wells.
The result of LTT is an index: the stimulation index (SI), which is the signal ratio of treated versus untreated cultures. For diagnostic purposes either the culture conditions are adjusted so that a given SI value can be used as a cutoff or a diagnostically relevant cutoff SI value is identified by metrology [32,35,36].
Here we show that with the appropriate experimental design cell viability measurements can reveal responsiveness of circulating blood cells towards drugs with high confidence and can therefore serve as an in vitro diagnostics procedure in drug hypersensitivity evaluation.
2. Materials and Methods
2.1. Source of Data
Results of 6 years of drug allergy testing were anonymized and used for this meta-analysis. The dataset included 738 blood samples from individuals (Table 1), who either brought their own medications or ordered the examination of pure active substances.
2.2. Preparation of Drugs for LTT
The tested medicinal drugs were obtained from the subjects who underwent drug allergy testing. Stock solutions were produced by pulverizing if necessary and dissolving the medicine in culture medium or distilled water. The concentrations of stock solutions were based on solubility properties and active substance content of the concerned medicine. Drug solutions were sterile filtered to ensure aseptic conditions.
Pure pharmacologically active drug substances were purchased from Merck KGaA (Darmstadt, Germany). 10 mM stock solutions were prepared with dimethyl sulfoxide (DMSO) for all experiments. The medium with the highest DMSO concentration (0.1%) did not exert any remarkable effect on cell viability and proliferation. The list of applied medicines and drug substances are provided as Supplementary Material. Phytohemagglutinin (PHA) from Phaseolus vulgaris was purchased from Merck KGaA; 1 mg/mL stock solution was prepared with PBS.
2.3. Lymphocyte Transformation Testing
Peripheral blood mononuclear cells (PBMC) were collected by means of Ficoll-Paque separation of whole blood [37]. After a washing step in PBS, PBMCs were transferred to RPMI 1640 media (Gibco) containing 10% Fetal Bovine Serum (FBS, Sigma), 1% sodium piruvate solution (100 mM, Sigma-Aldrich), 1% L-Glutamine (200 mM, Gibco), and 1% MEM Vitamins Solution (Gibco).
PBMCs were cultured in the absence (negative control) or presence of the drug of interest, and in the presence of mitogen (positive control) for 72 hours and the viability of cells was then assessed using an MTT assay [29]. Cells were seeded onto 96-well microplates at a density of 150,000 cells/well. The wells were filled with medium containing the test compounds prior to the seeding. Untreated cells served as negative control while PHA was used as positive control in all experiments. Samples were incubated at 37⁰C in humidified air containing 5% CO2. After 72 hours, 3-(4,5-Dimethylthiazol-2-yl)-2,5-Diphenyltetrazolium Bromide (MTT) solution (5 mg/mL) was added to each well. After 4 hours, formazan crystals formed by the living cells were solubilized in Hydrogen chloride – 2-propanol solution and measured by spectrophotometry. Negative control wells were comprised of ten parallels, other measurements were performed with five parallel wells.
2.4. Meta-Analysis, Statistical Methods
10 parallel measurements of negative control wells with no stimulant were used for the accurate estimation of background signals and for the calculation of the variance of the method. 5 parallel wells were used for positive control and test substance measurements. The number of parallel measurements required for distinguishing SI values with >95% confidence was defined by the equation:
where r is the number of replicates, CV is the percentage of coefficient of variation, D is the difference required to detect as percent of mean, t1 is tabular value from T-test with specified significance for Type I error, t2 is tabular value from T-test with specified significance for Type II error. Images were created with Scimago Graphica 1.0.45.
3. Results
3.1. Variance of Negative Control
The results of LTT are expressed as the stimulation index: the ratio of the signal in the treated group to that in the untreated group. This unitless quantity is 1 in the absence of stimulation, increases upon stimulation of cells and decreases if the cells die. Reliable discrimination of deviance from 1 requires statistics that characterize random, accidental deviation from 1 in the absence of stimulus. We characterized this property by the analysis of signals of parallel negative control wells. The coefficient of variation (CV%=standard deviation*100/mean optical density) characterizes that deviation and was found to be statistically identical in women (n=560) and men (n=178) (Figure 1a).
Next, we examined the distribution of SI values from all the tests. The expected average of SI values if all tested substances were non-stimulatory would be 1 with an SD value of 0.1, corresponding to the 10% CV of the measurement. The histogram of obtained SI values however shows a distribution that is skewed towards greater SI values (Figure 1b). This skew is the result of stimulatory effects of some of the tested substances in responsive individuals. Observations beyond the normal distribution are non-negative results statistically. A sample with the lower limit of positivity SI=1.4 has a normal distribution with the lowest SI values of its distribution overlapping with the negative test distribution (Figure 1B). These histograms demonstrate the behavior of the cut-off values that we had been using for classification of results: negative SI<1.3, equivocal 1.3=<SI<1.4, positive SI=>1.4.
3.2. Effects of Age and Sex
The immune system changes throughout life, gradually transforming towards a memory cell-based protection with the accumulation of immunological experience. To confirm that a viability measurement is applicable throughout adult life, we tested whether age has an effect on the variance of the background proliferative responses as reflected by the standard deviation of signals in parallel wells. Age had no effect on the SD values of negative control measurements, irrespective of the individual’s sex (Figure 2a). Age did influence, however, the responsiveness to the mitogen PHA that is used as positive control (Figure 2b). In spite of this age-dependent decrease in PHA responses, we did not observe age-dependent responsiveness to the tested substances (Figure 2c).
3.3. Adjustment of Cut-Off for SI
Since cell cultures were set up in parallels to increase the precision of the measurement, the average of these parallels needs to be computed for the calculation of SI. Arithmetic mean and median are the usual choices for averaging in LTT tests. We compared the effect of using these values for SI calculations (Figure 3a). The result of tests with SI values below or above the cut-off values by both calculations is unambiguous (lower left and upper right quadrants). A small percentage of the tests are only above the cut-off with either mean-based or median-based SI calculation (upper left and lower right quadrants). These tests should be examined with regard to the values of the parallel wells and decision be made considering all potential confounding factors in the measurement.
When all the blood cells in culture are quiescent (resting lymphocytes), a lower signal for the negative control wells is expected, while increased cellular activity (blast formation, proliferation) due to ongoing immune responses increases this background signal. To examine the effect of background signals we analyzed the relationship between the median OD values of negative controls and the SI of tested substances (Figure 3b). Increase in background signals was associated with a diminishing frequency of positive test outcome.
3.4. Frequencies and Relationships of Positive Responses
We sorted the tested drugs according to their pharmaceutical effects and created categories from the three most frequently tested groups (antibiotics, anesthetics and non-steroid anti-inflammatory agents) and a miscellaneous group. The proportions of equivocal and positive results were comparable for the three major categories (Figure 4).
Next we sorted the tested drugs according to the number of patient blood samples in which they have been examined. Amoxicillin, which is generally used in combination with the beta-lactamase inhibitor clavulanic acid, was the most frequently tested substance, in agreement with the common need of confirming penicillin allergy. The median values of the percentage of negative, equivocal and positive results for the most frequently examined drugs were 81.8%, 9.0% and 9.5% respectively (Table 2). While specific drugs showed notable deviations from these values, the tendency was the comparable precentage of equivocal and positive results, supporting the right-skewed distribution of SI values shown in Figure 1.
4. Discussion
LTTs are traditionally based on the measurement of proliferation using radioactive thymidine incorporation onto dividing cells. When the aim of the test is the assessment of lymphocyte reactivity towards potentially allergenic small molecules, other readouts are also possible and reasonable with current technologies. The viability test we employ has small variability when an adequate number of parallels are used (Figure 1). Therefore, a modest increase in SI value, as a result of increased cellular survival by direct (proliferation) or indirect (cytokines, chemokines) effect of responding cells, can be confidently distinguished from the absence of response. Even though mitogen-triggered responses decline with age, the responses triggered by the tested substances showed no such decline (Figure 2). The likely reason is the distinct mechanism of action: whereas PHA is a lectin that binds cell surface glycans and triggers agglutination and finally mitosis [38,39], drugs mostly act as a bridge between MHC and TCR molecules [40,41,42].
The use of multiple identical measurements (parallels) is necessary for increasing the precision of the method, but it also raises the question of how to average the observed individual signals. When the SI values calculated from the arithmetic means and the medians of parallel wells give discordant results (Figure 3a), we suggest to examine the distribution of signals. A single outlier value can be reasonably excluded from evaluation, while a cluster of two outliers suggests non-random but true biological effects. In this latter case the use of the mean value of all parallels better reflects biological events.
The clinical diagnostic accuracy of LTTs for drug allergy is very difficult, if possible at all, to establish. Each substance may act via distinct mechanisms and each individual may respond in different ways to distinct substances. The analytical (metrological) sensitivity and specificity can be established, however, and may provide a cue about the reliability of the measurement method. We designed our assay so as the number of parallel measurements is suitable for distinguishing SI values above the cut-off with high confidence. Our analysis shows that indeed the analytical specificity is high, 99% of the measurements above the lower cut-off value are predicted to be true cellular responses (Figure 1b). Accordingly, we assume that the diagnostic specificity of the test is also high. However, the diagnostic sensitivity of the test is assumed to be low, simply because an in vitro test cannot reproduce in vivo effects of a drug. For this reason the LTT is not suitable for excluding drug sensitivity, but only for confirming hypersensitivity and comparing the reactivity of related drug substances.
Analysis of particular substances (Table 2) suggests that the observations are not due to random noise (observed positivity is more frequent) but less than what would be a general stimulatory effect (when the majority of measurements would be positive). These measurements can therefore be good correlates but yet cannot explain the molecular nature of the cellular response and immunological consequences in the body. These tests can therefore only provide support for the diagnosis of drug hypersensitivity and should not be interpreted without consideration of clinical data.
A critical aspect of testing of cells is the variability of an individual’s responsiveness, that may be modulated by general health, ongoing immunological processes, time of latency from last allergic symptoms. Our results highlight that increased background activity is associated with decreased incidence of positive results, pointing towards decreased sensitivity (Figure 3b). These results suggest that the test should ideally be repeated in case the background signal is high and the clinical symptoms were strongly suggestive of allergic reactions.
From the theoretical points of view LTTs are suited for detecting cellular responses of delayed type hypersensitivity. Nevertheless, IgE-mediated immediate allergic reactions may also be identified by the test, because antigen specific T helper cells are involved and can be stimulated in vitro. LTT can be combined with other in vitro allergy tests, such as a basophil activation test [12], in order to broaden the range of immunological mechanisms behind drug reactions that can be detected.
5. Conclusions
The in vitro testing of potentially allergenic drugs and drug components is feasible using viability tests as a readout for LTT. Our results confirm that the method is applicable throughout adulthood and highlight that increased background, potentially caused by ongoing immune responses, can decrease testing sensitivity. Most frequently tested substances (antibiotics, NSAIDs and anesthetics) were comparable regarding the percentage of positive results, confirming that the widespread use of drugs is accompanied by a range of adverse drug reactions.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org; Table S1: LTT-results; Table S2: list-of-tested-drugs.
Author Contributions
“Conceptualization, A.G. and J.P.; methodology, G.M.; software, K.P.; validation, J.P.; formal analysis, A.G. and K.P.; investigation, A.G.; resources, J.P.; data curation, K.P.; writing—original draft preparation, A.G. and J.P.; writing—review and editing, J.P.; visualization, A.G.; supervision, J.P.; project administration, A.G.; funding acquisition, J.P. All authors have read and agreed to the published version of the manuscript.”
Funding
Support from the National Office for Research, Development and Innovation (NKFIH) in the form of research grant VEKOP-2.1.1.-15-2016-00098 is acknowledged.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data supporting reported results is provided as Supplementary Material.
Acknowledgments
The authors wish to thank Edina Garaczi for continued consultations on the indications and interpretations of LTT in drug allergy testing. The development of LTT in the laboratory was initiated by Klára Rásky, Zoltán Hérincs and Hajna Péterfy, whose efforts are greatly appreciated by the authors.
Conflicts of Interest
The authors are employed by a company that provides allergy testing services.
References
- Coleman, J.J.; Pontefract, S.K. Adverse drug reactions. Clin. Med. 2016, 16, 481–485. [Google Scholar] [CrossRef] [PubMed]
- Gomes, E.R.; Marques, M.L.; Regateiro, F. Epidemiology and risk factors for severe delayed drug hypersensitivity reactions. Curr. Pharm. Des. 2019. [Google Scholar] [CrossRef] [PubMed]
- Illing, P.T.; Mifsud, N.A.; Ardern-Jones, M.R.; Trubiano, J. Editorial: The immunology of adverse drug reactions. Front. Immunol. 2022, 13, 863414. [Google Scholar] [CrossRef] [PubMed]
- Chu, M.-T.; Chang, W.-C.; Pao, S.-C.; Hung, S.-I. Delayed drug hypersensitivity reactions: Molecular recognition, genetic susceptibility, and immune mediators. Biomedicines 2023, 11. [Google Scholar] [CrossRef]
- Pichler, W.J.; Adam, J.; Watkins, S.; Wuillemin, N.; Yun, J.; Yerly, D. Drug Hypersensitivity: How Drugs Stimulate T Cells via Pharmacological Interaction with Immune Receptors. Int. Arch. Allergy Immunol. 2015, 168, 13–24. [Google Scholar] [CrossRef]
- Zhang, B.; Li, Q.; Shi, C.; Zhang, X. Drug-Induced Pseudoallergy: A Review of the Causes and Mechanisms. Pharmacology 2018, 101, 104–110. [Google Scholar] [CrossRef]
- Redwood, A.J.; Pavlos, R.K.; White, K.D.; Phillips, E.J. HLAs: Key regulators of T-cell-mediated drug hypersensitivity. HLA 2018, 91, 3–16. [Google Scholar] [CrossRef]
- Pichler, W.J. Delayed drug hypersensitivity reactions. Ann. Intern. Med. 2003, 139, 683–693. [Google Scholar] [CrossRef]
- Schrijvers, R.; Gilissen, L.; Chiriac, A.M.; Demoly, P. Pathogenesis and diagnosis of delayed-type drug hypersensitivity reactions, from bedside to bench and back. Clin. Transl. Allergy 2015, 5, 31. [Google Scholar] [CrossRef]
- Doña, I.; Torres, M.J.; Celik, G.; Phillips, E.; Tanno, L.K.; Castells, M. Changing patterns in the epidemiology of drug allergy. Allergy 2024, 79, 613–628. [Google Scholar] [CrossRef]
- Torres, M.J.; Romano, A.; Celik, G.; Demoly, P.; Khan, D.A.; Macy, E.; Park, M.; Blumenthal, K.; Aberer, W.; Castells, M.; Barbaud, A.; Mayorga, C.; Bonadonna, P. Approach to the diagnosis of drug hypersensitivity reactions: Similarities and differences between Europe and North America. Clin. Transl. Allergy 2017, 7, 7. [Google Scholar] [CrossRef]
- Srinoulprasert, Y.; Rerkpattanapipat, T.; Sompornrattanaphan, M.; Wongsa, C.; Kanistanon, D. Clinical value of in vitro tests for the management of severe drug hypersensitivity reactions. Asia Pac. Allergy 2020, 10, e44. [Google Scholar] [CrossRef]
- Mayorga, C.; Celik, G.; Rouzaire, P.; Whitaker, P.; Bonadonna, P.; Rodrigues-Cernadas, J.; Vultaggio, A.; Brockow, K.; Caubet, J.C.; Makowska, J.; Nakonechna, A.; Romano, A.; Montañez, M.I.; Laguna, J.J.; Zanoni, G.; Gueant, J.L.; Oude Elberink, H.; Fernandez, J.; Viel, S.; Demoly, P.; Torres, M.J. In vitro tests for Drug Allergy Task Force of EAACI Drug Interest Group In vitro tests for drug hypersensitivity reactions: An ENDA/EAACI Drug Allergy Interest Group position paper. Allergy 2016, 71, 1103–1134. [Google Scholar] [CrossRef]
- Saretta, F.; Mori, F.; Cardinale, F.; Liotti, L.; Franceschini, F.; Crisafulli, G.; Caimmi, S.; Bottau, P.; Bernardini, R.; Caffarelli, C. Pediatric drug hypersensitivity: Which diagnostic tests? Acta Biomed 2019, 90, 94–107. [Google Scholar] [CrossRef]
- Steiner, M.; Harrer, A.; Himly, M. Basophil Reactivity as Biomarker in Immediate Drug Hypersensitivity Reactions-Potential and Limitations. Front. Pharmacol. 2016, 7, 171. [Google Scholar] [CrossRef]
- Cabrera, C.M.; Clarcast, M.; Palacios-Cañas, A. Clinical validation of the basophil activation test in immediate hypersensitivity reactions to gadolinium-based contrast agents. Int. Immunopharmacol. 2023, 117, 110000. [Google Scholar] [CrossRef]
- Bahri, R.; Custovic, A.; Korosec, P.; Tsoumani, M.; Barron, M.; Wu, J.; Sayers, R.; Weimann, A.; Ruiz-Garcia, M.; Patel, N.; Robb, A.; Shamji, M.H.; Fontanella, S.; Silar, M.; Mills, E.N.C.; Simpson, A.; Turner, P.J.; Bulfone-Paus, S. Mast cell activation test in the diagnosis of allergic disease and anaphylaxis. J. Allergy Clin. Immunol. 2018, 142, 485–496.e16. [Google Scholar] [CrossRef]
- Ebo, D.G.; De Puysseleyr, L.P.; Van Gasse, A.L.; Elst, J.; Poorten, M.-L. van der; Faber, M.A.; Mertens, C.; Van Houdt, M.; Hagendorens, M.M.; Sermeus, L.; Vitte, J.; Moise, M.; Garvey, L.H.; Castells, M.C.; Tacquard, C.; Mertes, P.-M.; Schwartz, L.B.; Sabato, V. Mast cell activation during suspected perioperative hypersensitivity: A need for paired samples analysis. J. Allergy Clin. Immunol. Pract. 2021, 9, 3051–3059.e1. [Google Scholar] [CrossRef]
- Fatangare, A.; Glässner, A.; Sachs, B.; Sickmann, A. Future perspectives on in-vitro diagnosis of drug allergy by the lymphocyte transformation test. J. Immunol. Methods 2021, 495, 113072. [Google Scholar] [CrossRef]
- Glässner, A.; Dubrall, D.; Weinhold, L.; Schmid, M.; Sachs, B. Lymphocyte transformation test for drug allergy detection: When does it work? Ann. Allergy Asthma Immunol. 2022, 129, 497–506.e3. [Google Scholar] [CrossRef]
- Pichler, W.J.; Tilch, J. The lymphocyte transformation test in the diagnosis of drug hypersensitivity. Allergy 2004, 59, 809–820. [Google Scholar] [CrossRef]
- Porebski, G.; Piotrowicz-Wojcik, K.; Spiewak, R. ELISpot assay as a diagnostic tool in drug hypersensitivity reactions. J. Immunol. Methods 2021, 495, 113062. [Google Scholar] [CrossRef]
- Copaescu, A.M.; Ben-Shoshan, M.; Trubiano, J.A. Tools to improve the diagnosis and management of T-cell mediated adverse drug reactions. Front Med (Lausanne) 2022, 9, 923991. [Google Scholar] [CrossRef]
- Drygala, S.; Rdzanek, E.; Porebski, G.; Dubiela, P. In Vitro Assays for Diagnosis of Drug-Induced Nonsevere Exanthemas: A Systematic Review and Meta-Analysis. J. Immunol. Res. 2022, 2022, 2386654. [Google Scholar] [CrossRef]
- Copaescu, A.; Gibson, A.; Li, Y.; Trubiano, J.A.; Phillips, E.J. An updated review of the diagnostic methods in delayed drug hypersensitivity. Front. Pharmacol. 2020, 11, 573573. [Google Scholar] [CrossRef]
- Dobozy, A.; Hunyadi, J.; Simon, N. Lymphocyte-transformation test in detection of drug hypersensitivity. Lancet 1972, 2, 1319. [Google Scholar] [CrossRef]
- Sachs, B.; Fatangare, A.; Sickmann, A.; Glässner, A. Lymphocyte transformation test: History and current approaches. J. Immunol. Methods 2021, 493, 113036. [Google Scholar] [CrossRef]
- Ganesan, N.; Ronsmans, S.; Hoet, P. Methods to assess proliferation of stimulated human lymphocytes in vitro: A narrative review. Cells 2023, 12. [Google Scholar] [CrossRef]
- Mosmann, T. Rapid colorimetric assay for cellular growth and survival: Application to proliferation and cytotoxicity assays. J. Immunol. Methods 1983, 65, 55–63. [Google Scholar] [CrossRef]
- Szabó, I.; Gonda, A.; Bakos, B.; Tóth, K.; Hunyadi, J. [Lymphoblast transformation colorimetry in the diagnosis of drug hypersensitivity]. Orv. Hetil. 1998, 139, 2379–2382. [Google Scholar]
- Weir, C.; Li, J.; Fulton, R.; Fernando, S.L. Development and initial validation of a modified lymphocyte transformation test (LTT) assay in patients with DRESS and AGEP. Allergy Asthma Clin. Immunol. 2022, 18, 90. [Google Scholar] [CrossRef]
- Di Blasi, D.; Claessen, I.; Turksma, A.W.; van Beek, J.; Ten Brinke, A. Guidelines for analysis of low-frequency antigen-specific T cell results: Dye-based proliferation assay vs 3H-thymidine incorporation. J. Immunol. Methods 2020, 487, 112907. [Google Scholar] [CrossRef] [PubMed]
- Karami, Z.; Mesdaghi, M.; Karimzadeh, P.; Mansouri, M.; Taghdiri, M.M.; Kayhanidoost, Z.; Jebelli, B.; Shekarriz Foumani, R.; Babaie, D.; Chavoshzadeh, Z. Evaluation of Lymphocyte Transformation Test Results in Patients with Delayed Hypersensitivity Reactions following the Use of Anticonvulsant Drugs. Int. Arch. Allergy Immunol. 2016, 170, 158–162. [Google Scholar] [CrossRef] [PubMed]
- Alsalamah, M.; Vong, L.; Cimpean, L.; Dadi, H. Establishing reference ranges for lymphocyte proliferation responses to phytohemagglutinin in patients with T cell dysfunction. LymphoSign Journal 2019, 6, 26–30. [Google Scholar] [CrossRef]
- Frome, E.L.; Smith, M.H.; Littlefield, L.G.; Neubert, R.L.; Colyer, S.P. Statistical methods for the blood beryllium lymphocyte proliferation test. Environ. Health Perspect. 1996, 104 Suppl 5, 957–968. [Google Scholar] [CrossRef]
- Mascarenhas, R.E.; Brodskyn, C.; Barbosa, G.; Clarêncio, J.; Andrade-Filho, A.S.; Figueiroa, F.; Galvão-Castro, B.; Grassi, F. Peripheral blood mononuclear cells from individuals infected with human T-cell lymphotropic virus type 1 have a reduced capacity to respond to recall antigens. Clin. Vaccine Immunol. 2006, 13, 547–552. [Google Scholar] [CrossRef] [PubMed]
- Jaatinen, T.; Laine, J. Isolation of mononuclear cells from human cord blood by Ficoll-Paque density gradient. Curr. Protoc. Stem Cell Biol. 2007, 1, 2A. 1.1–2A. 1.4. [Google Scholar] [CrossRef]
- Nowell, P.C. Phytohemagglutinin: An initiator of mitosis in cultures of normal human leukocytes. Cancer Res. 1960, 20, 462–466. [Google Scholar]
- Sharon, N.; Lis, H. History of lectins: From hemagglutinins to biological recognition molecules. Glycobiology 2004, 14, 53R–62R. [Google Scholar] [CrossRef]
- Depta, J.P.H.; Altznauer, F.; Gamerdinger, K.; Burkhart, C.; Weltzien, H.U.; Pichler, W.J. Drug interaction with T-cell receptors: T-cell receptor density determines degree of cross-reactivity. J. Allergy Clin. Immunol. 2004, 113, 519–527. [Google Scholar] [CrossRef]
- Gerber, B.O.; Pichler, W.J. Noncovalent interactions of drugs with immune receptors may mediate drug-induced hypersensitivity reactions. AAPS J. 2006, 8, E160–5. [Google Scholar] [CrossRef]
- Adam, J.; Pichler, W.J.; Yerly, D. Delayed drug hypersensitivity: Models of T-cell stimulation. Br. J. Clin. Pharmacol. 2011, 71, 701–707. [Google Scholar] [CrossRef]
Figure 1.
Variance of signals and distribution of SI values. The distribution of CV% values is shown for women and men (a). Assuming a normal distribution for random signals and 10% CV, the percentage of truly increased events can be calculated (b).
Figure 1.
Variance of signals and distribution of SI values. The distribution of CV% values is shown for women and men (a). Assuming a normal distribution for random signals and 10% CV, the percentage of truly increased events can be calculated (b).
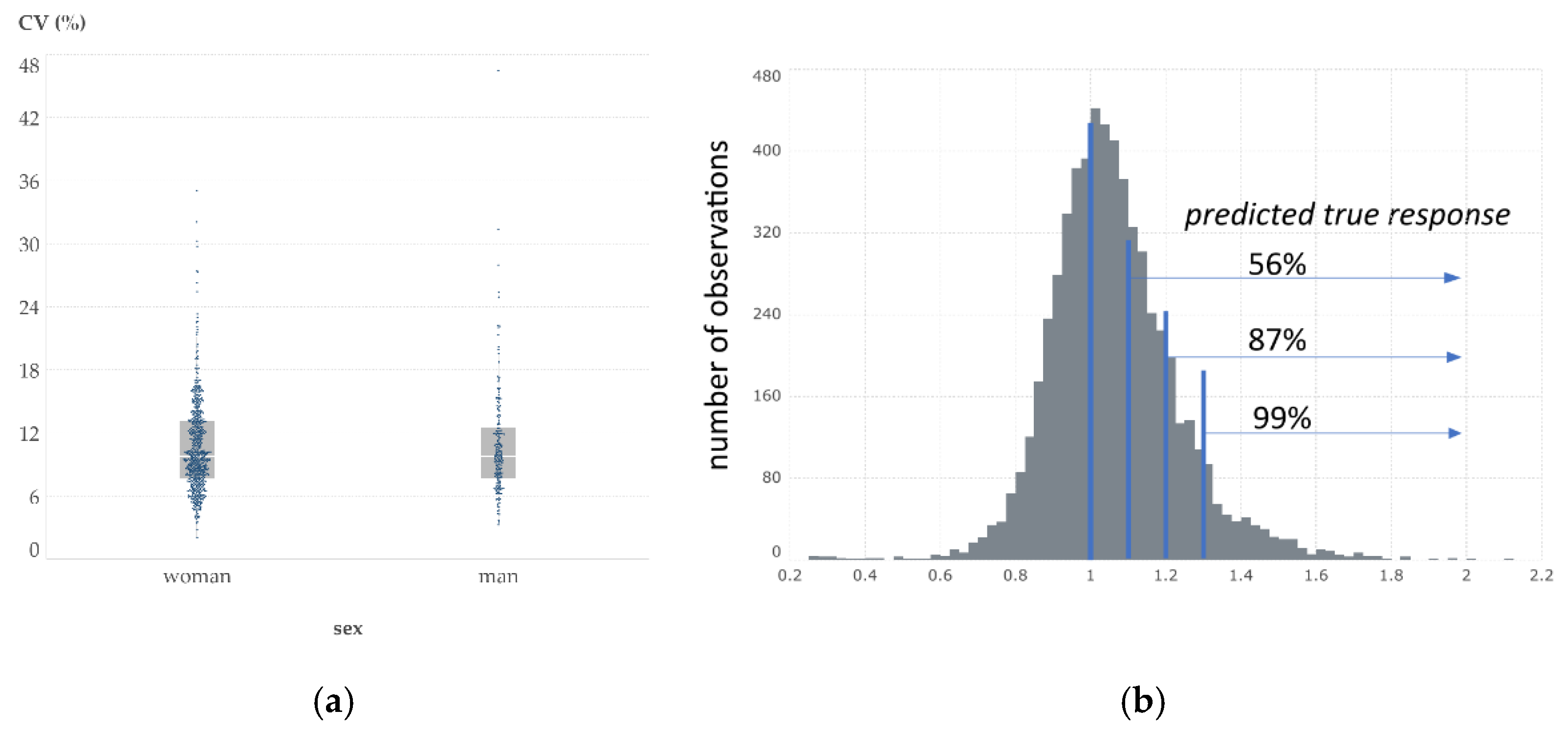
Figure 2.
Effects of age and sex on test performance. (a) SD of negative controls; (b) SI of positive controls; and (c) SI of tested substances as a function of age are shown. Lines stand for linear regression lines of the respective sexes.
Figure 2.
Effects of age and sex on test performance. (a) SD of negative controls; (b) SI of positive controls; and (c) SI of tested substances as a function of age are shown. Lines stand for linear regression lines of the respective sexes.
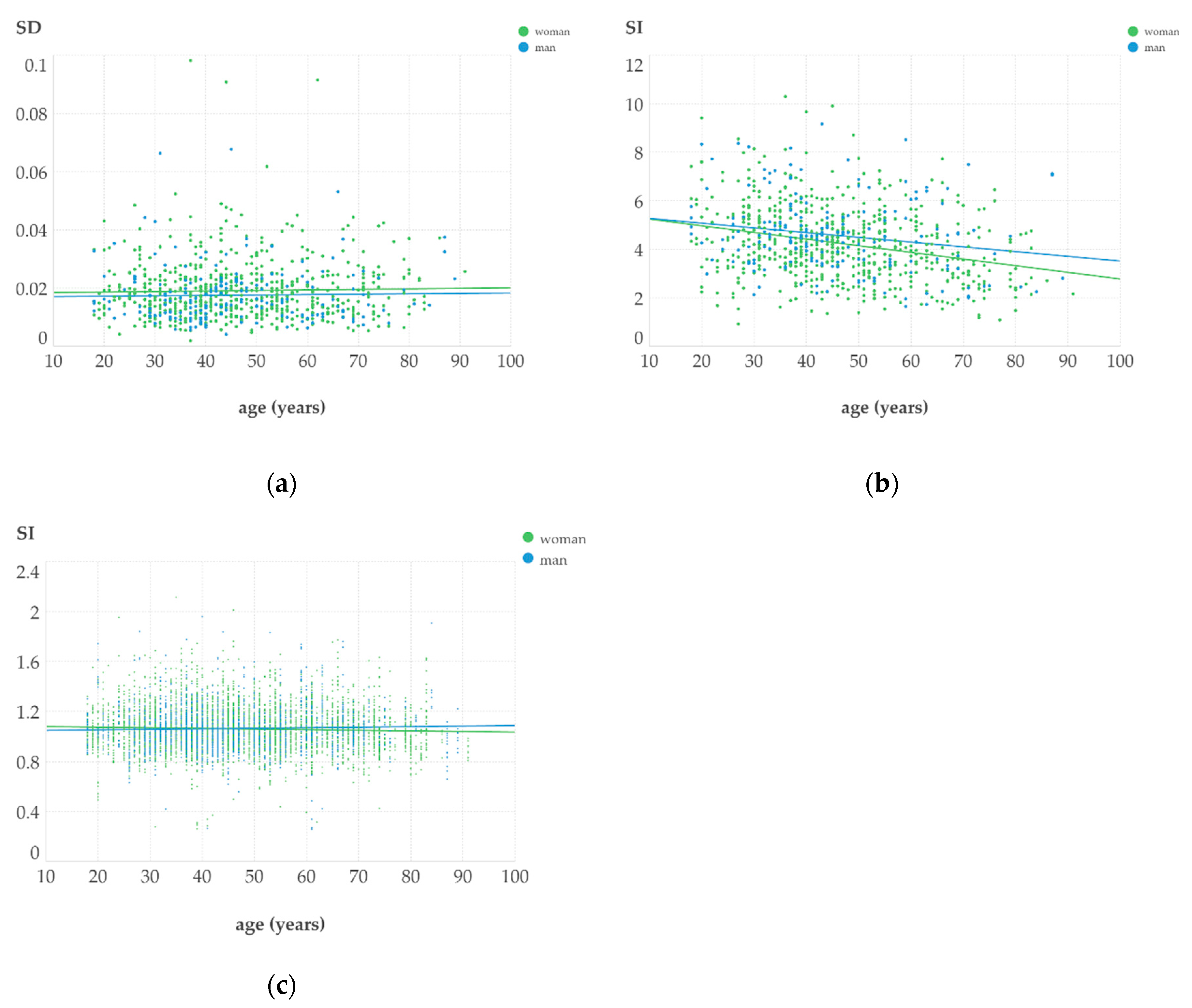
Figure 3.
The effects of calculation and of background signals on SI values. (a) Mean and median values of parallels are strongly correlated but result in slightly different classification in the grey zone; (b) density map of SI values as a function of negative control absorbance representing the background cellular activity. Black lines represent the upper cut-off value (SI=1.3) of a negative result.
Figure 3.
The effects of calculation and of background signals on SI values. (a) Mean and median values of parallels are strongly correlated but result in slightly different classification in the grey zone; (b) density map of SI values as a function of negative control absorbance representing the background cellular activity. Black lines represent the upper cut-off value (SI=1.3) of a negative result.
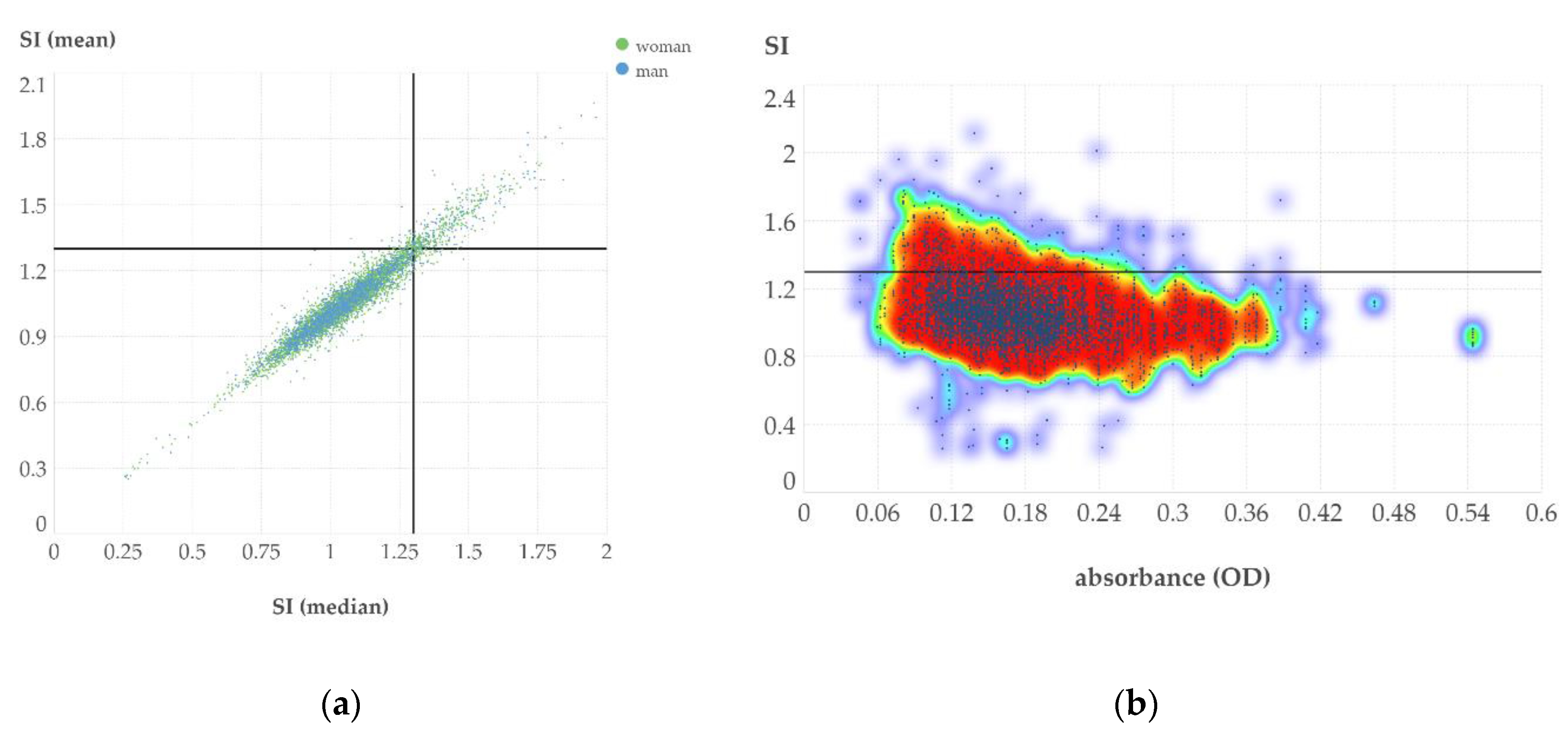
Figure 4.
Number of patients with negative, equivocal and positive results in the four tested drug categories. Note that the same patient may have been tested for several drug categories.
Figure 4.
Number of patients with negative, equivocal and positive results in the four tested drug categories. Note that the same patient may have been tested for several drug categories.
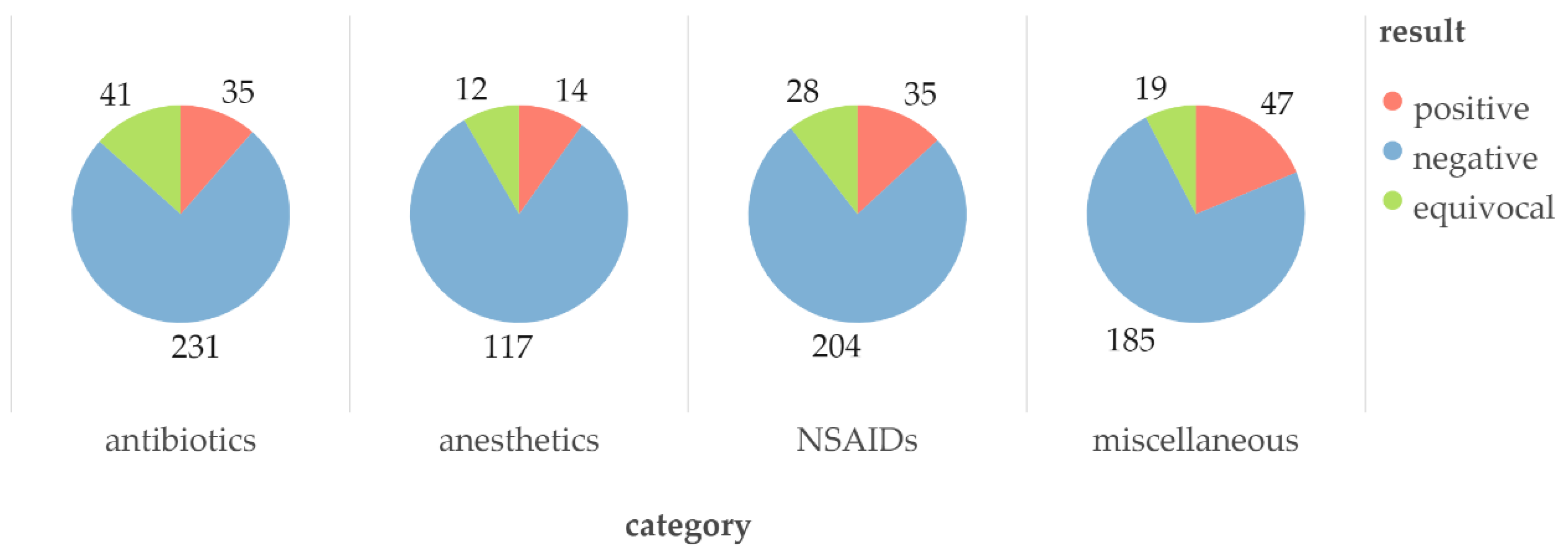

Table 1.
Patient characteristics.
| Parameters | Man | Woman |
|---|---|---|
| patient number | 178 | 560 |
| age (mean ± SD, years) | 45.3 ± 15.1 | 47.1 ± 15.3 |
| age range (years) | 18 - 89 | 18 - 91 |
Table 2.
Results of most frequently examined medicines and substances. The data represent the number and percentage of observed cellular responses (-, negative; +/-, equivocal; +, positive) for the listed investigated substances and medicines, containing these active substances alone or in combination.
Table 2.
Results of most frequently examined medicines and substances. The data represent the number and percentage of observed cellular responses (-, negative; +/-, equivocal; +, positive) for the listed investigated substances and medicines, containing these active substances alone or in combination.
| Medicine/substance | n patient | - | +/- | + | - (%) | +/- (%) | + (%) |
|---|---|---|---|---|---|---|---|
| amoxicillin | 201 | 166 | 18 | 17 | 82.6 | 9.0 | 8.5 |
| clavulanic acid | 173 | 149 | 13 | 11 | 86.1 | 7.5 | 6.4 |
| lidocaine | 119 | 104 | 6 | 9 | 87.4 | 5.0 | 7.6 |
| clavulanic acid* alone | 96 | 89 | 3 | 4 | 92.7 | 3.1 | 4.2 |
| metamizole | 92 | 72 | 11 | 9 | 78.3 | 12.0 | 9.8 |
| articaine | 90 | 74 | 9 | 7 | 82.2 | 10.0 | 7.8 |
| diclofenac | 85 | 78 | 0 | 7 | 91.8 | 0.0 | 8.2 |
| paracetamol | 81 | 70 | 4 | 7 | 86.4 | 4.9 | 8.6 |
| phenoxymethylpenicillin | 78 | 71 | 5 | 2 | 91.0 | 6.4 | 2.6 |
| acetylsalicylic acid | 72 | 53 | 9 | 10 | 73.6 | 12.5 | 13.9 |
| ibuprofen | 69 | 55 | 7 | 7 | 79.7 | 10.1 | 10.1 |
| cefuroxime | 32 | 25 | 3 | 4 | 78.1 | 9.4 | 12.5 |
| benzylpenicillin | 27 | 22 | 3 | 2 | 81.5 | 11.1 | 7.4 |
| sulfamethoxazole & trimethoprim | 24 | 19 | 2 | 3 | 79.2 | 8.3 | 12.5 |
| ciprofloxacin | 22 | 18 | 1 | 3 | 81.8 | 4.5 | 13.6 |
| azithromycin | 21 | 17 | 2 | 2 | 81.0 | 9.5 | 9.5 |
| levofloxacin | 19 | 13 | 4 | 2 | 68.4 | 21.1 | 10.5 |
| tolperisone | 17 | 14 | 0 | 3 | 82.4 | 0.0 | 17.6 |
| perindopril | 17 | 15 | 1 | 1 | 88.2 | 5.9 | 5.9 |
| levothyroxine | 13 | 6 | 3 | 4 | 46.2 | 23.1 | 30.8 |
| enoxaparin | 10 | 7 | 2 | 1 | 70.0 | 20.0 | 10.0 |
*Pure drug substance.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



