
Submitted:
01 October 2024
Posted:
02 October 2024
You are already at the latest version
Abstract
Interstitial pneumonia is a general term for diseases in which inflammation occurs mainly in the interstitium of the lung. It is also pointed out that interstitial pneumonia reduces alveolar function and makes it difficult to take in oxygen through inspiration, causing symptoms such as dyspnea and coughing, which may eventually lead to respiratory failure. It is At present, there is no effective treatment and only conservative treatment exists. This time, we report that the therapeutic effect was confirmed in patients with interstitial pneumonia who took platinum palladium. In this case, improvement tendencies were observed in patients with Idiopathic pulmonary fibrosis (IPF), but improvement tendencies were also observed in many other lung diseases. In order to explore the mechanism, AMPK was measured at the in vitro level, and blood KL-6 and hydrogen peroxide levels in the patient were measured at the in vivo level. AMPK values were significantly elevated by more than 800%, KL-6 and hydrogen peroxide levels were also significantly decreased by drinking platinum palladium. Platinum palladium exhibits a strong antioxidant effect and is the only substance in the world that can approach all four types of active oxygen. In addition, when it was actually administered to patients, there were cases of dramatic improvement, and it was confirmed that KL-6, a parameter of lung function, decreased in 16 out of 32 patients, and furthermore, oxygen inhalation was completed. patients were also seen. Although the number of cases is expected to increase in the future, the substance is expected to be effective as a drug, although it is currently classified as a soft drink.
Keywords:
Interstitial pneumonia
; COPD
; Platinum-palladium
; functional nutritional food
; KL-6
; AMPK
; Hydrogen peroxide
; Case improvement
; Oxygen inhalation
1. Introduction
Interstitial pneumonia is a general term for diseases in which inflammation occurs mainly in the interstitium of the lungs [1]. Alveoli are roughly divided into parenchyma and interstitium, with the inside of the alveoli being called the parenchyma and the walls and surrounding tissues of the alveoli being called the interstitium. Interstitial pneumonia is called interstitial pneumonia when inflammatory changes occur in the interstitium [2]. Interstitial pneumonia with identifiable causes includes “autoimmune interstitial pneumonia,” “occupational environment interstitial pneumonia,” and “iatrogenic interstitial pneumonia,” [3,4,5] and those with unidentifiable causes are called “idiopathic interstitial pneumonia” [6]. In addition, in the 2013 ATS/ERS classification of interstitial pneumonia, there are nine classifications:
1) Major IIPs
1. Idiopathic pulmonary fibrosis (IPF)
2. Idiopathic nonspecific interstitial pneumonia (idiopathic NSIP)
3. Respiratory bronchiolitis interstitial lung disease (RB-ILD)
4. Desquamative interstitial pneumonia (DIP)
5. Cryptogenic organizing pneumonia (COP)
6. Acute interstitial pneumonia (AIP)
2) Rare IIPs
1. Idiopathic lymphoid interstitial pneumonia (LIP)
2. Idiopathic pleuroparenchymal fibroelastosis (PPFE)
3) Unclassifiable
1. Unclassifiable IIPs [7].
In this study, we investigated the possibility of a new treatment for patients with idiopathic pulmonary fibrosis (IPF). In interstitial pneumonia, inflammation gradually causes fibrosis of the alveolar walls [8], and pulmonary surfactant protein-D (SP-D) levels increase [9,10]. As alveolar function declines, it becomes difficult to take in oxygen through inhalation, leading to respiratory symptoms such as shortness of breath and coughing, and it has been pointed out that this may ultimately lead to respiratory failure1 [11]. At present, there is no effective treatment, and the only symptomatic treatment is immunosuppressants for interstitial lung disease [12].
On the other hand, COPD (Chronic Obstructive Pulmonary Disease) is a type of chronic respiratory disease that causes alveolar destruction and inflammation, resulting in respiratory symptoms such as shortness of breath and progressing irreversibly. Smoking is the biggest risk factor for COPD in many cases, but it has been suggested that it may also be caused by other environmental pollution, etc. [13,14]. As with interstitial pneumonia, there is no established effective treatment for COPD, and the only conservative treatment is oxygen inhalation and maintaining and improving quality of life [16]. Epidemiologically, it is said that by 2030, WHO predicts that COPD will be the third leading cause of death in the world [16]. Epidemiological studies have also suggested that COPD has a high risk of developing lung cancer [17]. Until now, smoking cessation, antioxidants, dietary therapy, and alternative therapies have been the focus for COPD [18], but these have been aimed at slowing down the progression. In our clinical experience, the administration of platinum-palladium to COPD patients has shown a tendency for symptoms to improve in approximately 40-50% of patients. For the above reasons, we expected that the same therapeutic effect would be seen in interstitial pneumonia, so we examined cases. Platinum palladium is generally sold as a soft drink (functional nutritional water) under the name PAPLAL®, which is a colloidal mixture of platinum and palladium (a solution of platinum and palladium mixed at a ratio of 1: 3) (Figure.1, 2) and was invented by Dr. Hideyo Noguchi. It is a completely new functional nutritional water that is expected to have various effects, such as inducing apoptosis in stomach and colon cancer and activating NK cells (unpublished).
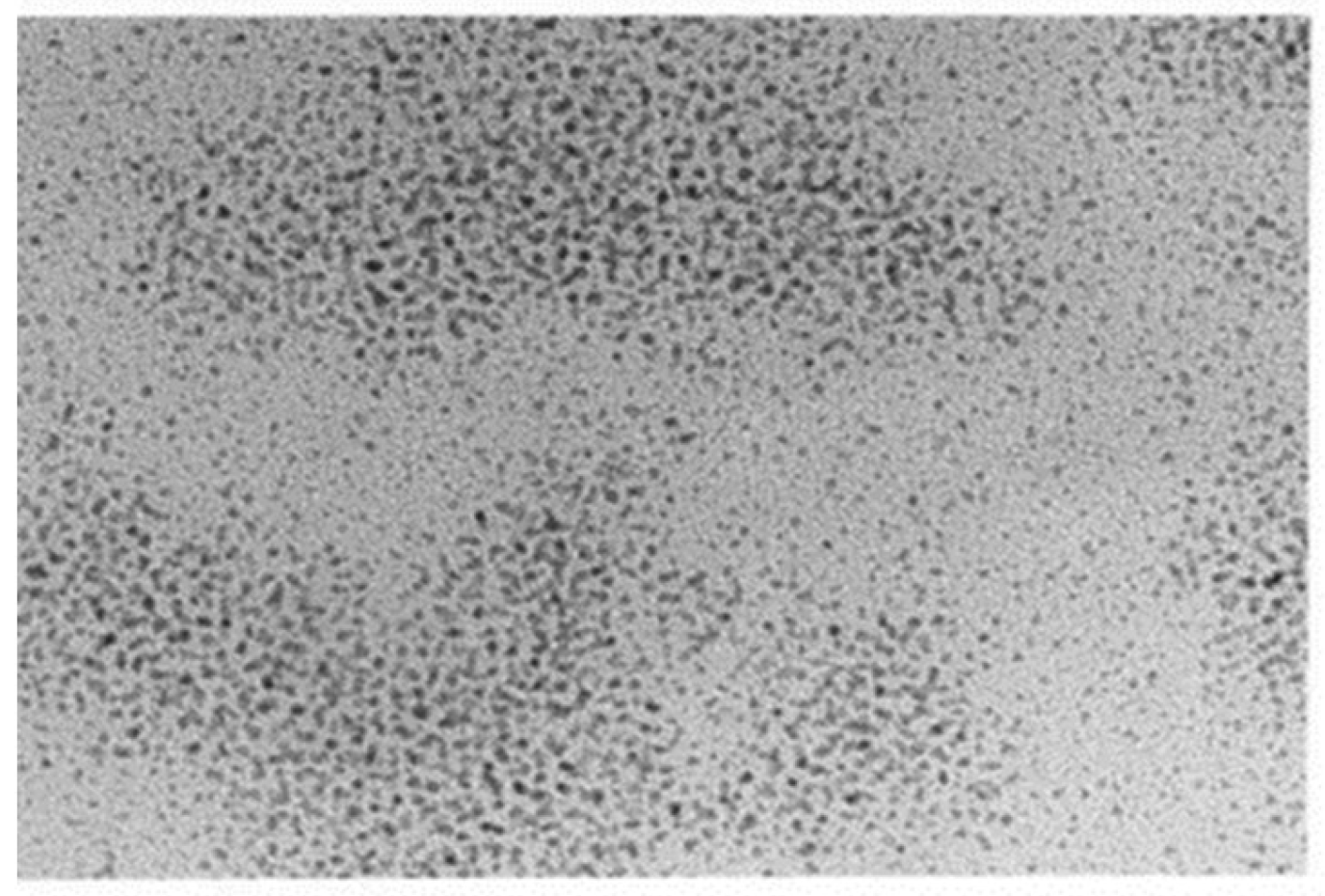
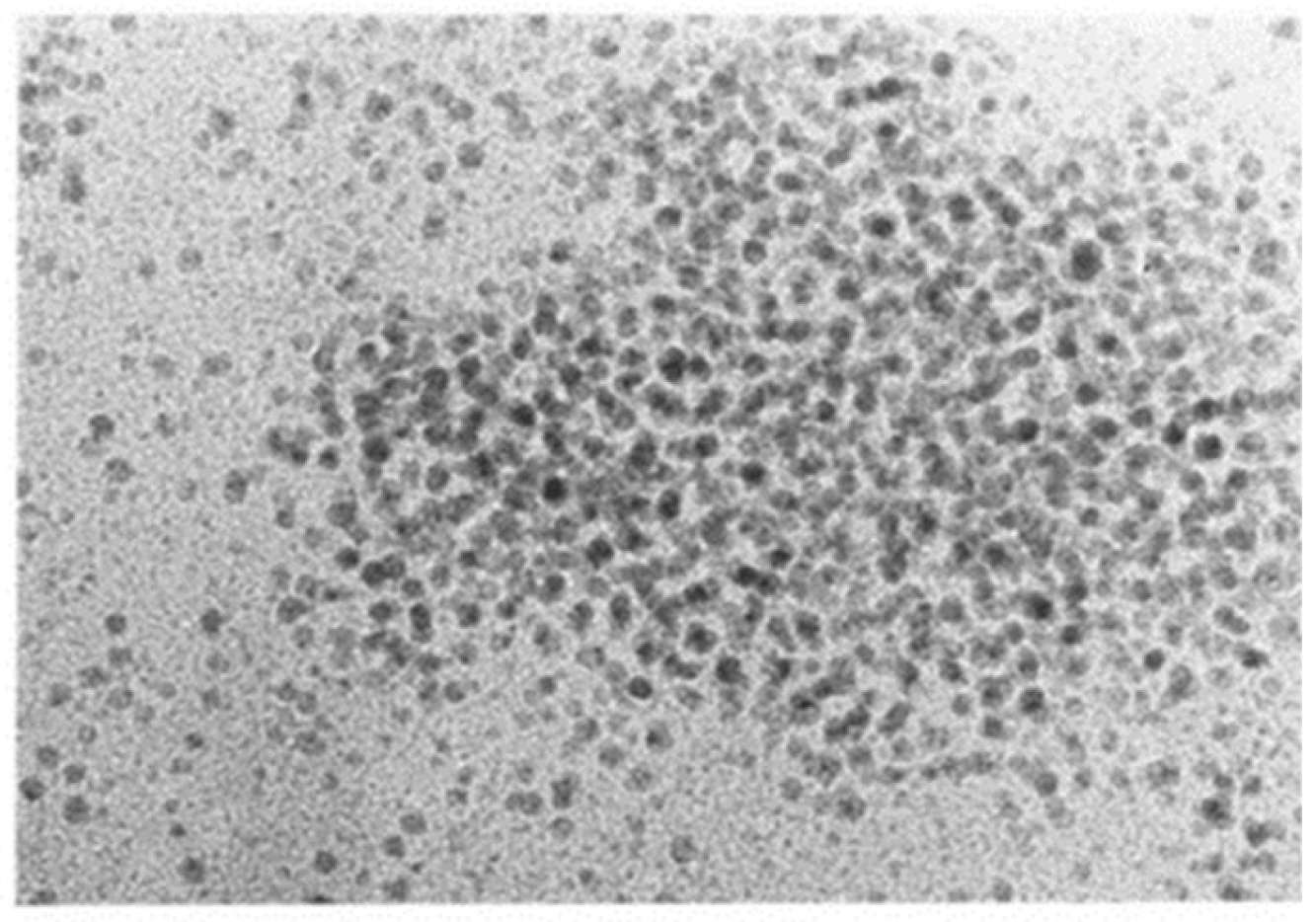
Figure 1.
Platinum colloid.
Figure 2.
Palladium colloid.
Platinum is a chemically very stable element and is used for various purposes. In the medical field, its complexes are used as anticancer drugs [19]. Other uses focusing on the antioxidant properties of platinum have been reported [20]. Palladium is one of the platinum group elements and is widely used as a material for industrial products and dental treatment [21,22]. It has also been reported that palladium has the effect of giving back reducing power to platinum involved in reduction reactions [23], and attempts have been made to use substances that are mixtures of platinum and palladium [24]. Due to the chemical reactions and specificities of the two elements, a mixture of platinum and palladium is expected to be useful as a substance with sustained antioxidant properties compared to platinum alone [24]. Furthermore, it has been found that platinum palladium moderately removes all four types of active oxygen [25]. A literature survey showed that there is no other substance that removes all four types of active oxygen (generally considered to be the four types of superoxide anion radical, hydroxyl radical, hydrogen peroxide, and singlet oxygen [26]. In addition, because platinum-palladium has a low absorption rate in the intestinal tract due to its characteristics [27,28], it is possible that it may act as a catalyst and activate AMPK (AMP-activated protein kinase) at the cellular level in the digestive tract, thereby contributing to the improvement of symptoms and lesions of interstitial pneumonia and COPD. Therefore, in this study, we reported cases and measured the amount of KL-6 [29] and hydrogen peroxide in the blood of patients with interstitial pneumonia and COPD [30]. At the same time, we confirmed whether platinum-palladium activates AMPK at the in vivo and in vitro levels.
2. Materials and Methods
2.1. Case Patient
・89-year-old male.
・Height 172 cm, weight 68 kg, body surface area 1,800 m2.
・Smoking history: None.
・Diagnosis: Interstitial pneumonia.
・Age at onset of interstitial pneumonia: 85 years old (as of 2020)
・Underlying diseases: None.
・Platinum-palladium intake: 18 ml/day (6 ml/1 vial x 3 vials).
・Duration: 32 months.
・Drug treatment: None.
・Oxygen inhalation: None.
2.2. History
In daily life, the patient walked 2-3 km every day to maintain and improve his health. No history of smoking, but alcohol consumption. Suddenly, frequent coughing was confirmed, and although cough suppressants were prescribed, there was no sign of improvement. When the patient was re-examined at a city hospital, chest X-rays and other tests confirmed findings specific to interstitial pneumonia, and he was diagnosed with interstitial pneumonia. The patient was told by her doctor that she had only two years to live. The disease gradually progressed, and she had difficulty breathing even when doing everyday activities such as climbing the stairs or going to the toilet at home, and she would often collapse. She lost the will to move, but by taking platinum-palladium, her respiratory function improved on the 18th day, her coughing almost disappeared, and her breathing difficulties decreased. At the time of her final visit, she had improved enough to resume walking. However, during the period when she stopped taking platinum-palladium, she experienced breathing difficulties again.
3. Measurements at In Vitro and In Vivo Levels
3.1. AMPK Measurement
Study of AMPK Activity by Platinum-Palladium
In this experiment, we used the Cyclex® AMPK Kinase Assay Kit (MEDICAL & BIOLOGICAL LABORATORIES CO., LTD. Tokyo, Japan) as per the usual method, and compared AMPK activity in the platinum-palladium-added group (final concentration 1%) with the PBS-added group as a control, using a purchased human breast cancer cell line (MCF-7). In this kit, the current activity of AMPK was measured 1 hour, 12 hours, and 24 hours after addition. The evaluation was performed using statistical software (IBM SPSS Statistics Ver.26) with the Mann–Whitney U test.
3.2. Measurement of Blood KL-6
Study of KL-6 Fluctuations Due to Platinum-Palladium
The study included 16 subjects (hereafter referred to as subjects) who visited Hino Kosei Clinic and agreed to participate in the study. Each subject was administered platinum-palladium for 28 days (4 weeks). The dosage was 3 vials in the first week, 2 vials in the second week, and 1 vial in the last 2 weeks. KL-6 was measured before and after administration and compared. The evaluation was performed using statistical software (IBM SPSS Statistics Ver.26) with the paired t-test.
3.3. Measurement of Blood Hydrogen Peroxide (Figure 3.)
Study of Changes in Hydrogen Peroxide Due to Platinum-Palladium
The study included 12 subjects (hereafter referred to as subjects) who visited Hino Kosei Clinic and agreed to participate in the study. Each subject was given platinum-palladium for 28 days (4 weeks). The subjects were given 3 vials in the first week, 2 vials in the second week, and 1 vial in the last 2 weeks. Hydrogen peroxide was measured before and after administration and compared. In addition, the results were statistically evaluated using a paired t-test with statistical processing software (IBM SPSS Statistics Ver.26).
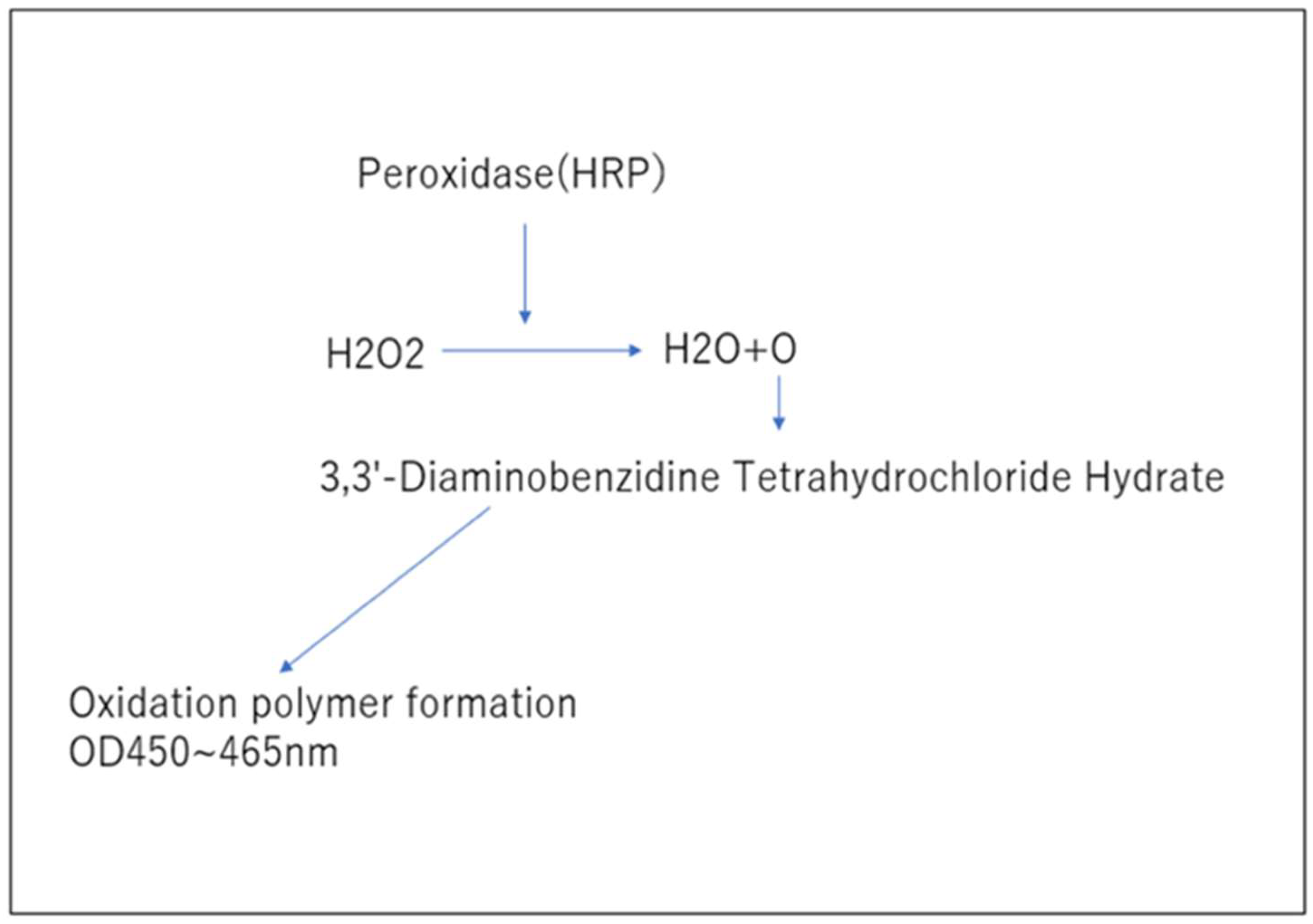
Figure 3.
Hydrogen peroxide measurement principle.
Qualitative measurement of hydrogen peroxide was performed using the peroxidase-diaminobenzidine method.
3.4. Study on the Effect of Platinum-Palladium on Symptom Improvement in Patients with Interstitial Pneumonia
32 patients with interstitial pneumonia were given platinum-palladium for one to three months, 3 vials for the first week, 2 vials for the second week, and 1 vial for the last two weeks, and clinical judgment was made. In this study, the subjects were patients with KL-6>500U/mL, crepitus+ in breath sounds, and + in X-ray reading.
4. Results
4.1. AMPK Measurement
When platinum-palladium was administered to MCF-7 and AMPK activity was measured, it was confirmed that the activity increased significantly in all groups at a significance level of 1% when the control group was taken as 100%. (Table1. 2, Figure 4.)

Table 1.
Absorbance of control and platinum-palladium-added groups 1) Absorbance.
| 1hr | 12hrs | 24hrs | |||
| Cnt | Pt:Pd | Cnt | Pt:Pd | Cnt | Pt:Pd |
| 0.285±0.013 | 2.308±0.223 | 0.352±0.019 | 2.689±0.447 | 0.264±0.034 | 2.341±0.082 |
Table 2.
AMPK activity when compared to the control group (100%) 2) AMPK activity.
| 1hr | 12hrs | 24hrs | |||
| Cnt | Pt:Pd | Cnt | Pt:Pd | Cnt | Pt:Pd |
| 100% | 809.80% | 100% | 763.92% | 100% | 886.74% |
4.2. Measurement of Blood KL-6
In n=16 subjects, a tendency for the KL-6 value to decrease was observed as shown in Table 2 and Figure 2 below. Furthermore, statistical processing revealed a significant decrease at a significance level of 5%. This suggests that the escape of KL-6 from the alveoli is suppressed, suggesting the possibility of improved alveolar function.
4.3. Measurement of Blood Hydrogen Peroxide
When blood hydrogen peroxide levels were measured in n=12 subjects, a de- crease was observed at a significance level of 5%, as shown in Table 3 and Figure 3. Since there is thought to be a relationship between interstitial pneumonia and hydrogen peroxide, these results suggest that interstitial pneumonia caused by hydrogen peroxide may improve.
4.4. Investigation into the Effectiveness of Platinum-Palladium in Improving
symptoms in patients with interstitial pneumonia (Figure 7.)
Thirty-two patients with interstitial pneumonia who visited Hino Kosei Clinic and Kisaragi Soken Clinic took platinum palladium supplement and their progress was monitored. Sixteen of the 32 patients showed a 20% or greater decrease in KL-6 after one month. Ten of them stopped inhaling oxygen after one month, and all ten patients also stopped coughing and sputum. Three of them showed a further 20% decrease in KL-6. Six patients continued to take oxygen after one month, even though their KL-6 had decreased by more than 20%, but three of them stopped taking oxygen and three had their dose reduced after continued intake. This suggests the need to continue taking platinum palladium supplement. Sixteen of the 32 patients showed no decrease in KL-6 after one month, but they were able to stop taking oxygen after three more months of continued intake. Of the patients who stopped drinking the water after one month, three subsequently stopped oxygen inhalation and 10 continued oxygen inhalation; however, this does not mean that the platinum-palladium solution was ineffective, but rather that the patients discontinued the solution due to unavoidable circumstances. Therefore, it is possible that their condition would have improved if they had continued drinking the solution.
4. Discussion
This is a case report in which platinum-palladium improved the pathology of inter stitial pneumonia. In addition to this case, there have been many reports of improvement in other clinics, and many cases of improvement in interstitial pneumonia with platinum-palladium have been confirmed. Therefore, it was suggested that platinum-palladium is an effective treatment method for interstitial pneumonia. Currently, treatment for interstitial pneumonia is mainly conservative, with the aim of preventing the condition from worsening, but improvement is difficult. However, in this case, improvement in daily living activities was observed, so it is possible that lung function may have improved. Although there are still many unknown aspects of the mechanism, we have considered the possibility. Although the cause of interstitial pneumonia is often unknown, it causes inflammation in the interstitium, so the production of reactive oxygen species is thought to be the cause33). Reactive oxygen releases inflammatory cytokines and has a positive aspect as a system to defend the body, but excessive reactive oxygen is known to have a negative effect on normal cells, causing lifestyle-related diseases, aging, and chronic inflammation [34,35]. In this case, platinum-palladium was used, but as mentioned above, platinum-palladium causes moderate antioxidant activity, so it is possible that it did not remove necessary reactive oxygen, but only unnecessary reactive oxygen, which may have led to the improvement of interstitial pneumonia. In addition, when the activity of AMPK by platinum-palladium was confirmed at the in vitro level, AMPK activity was confirmed at a significance level of 1% in all groups. AMPK (AMP-activated protein kinase) is an energy sensor in the body and is a serine/threonine kinase that works to maintain homeostasis of glucose and lipid metabolism [36]. It is said that activation of AMPK regulates energy metabolism and maintains energy homeostasis, and it has attracted attention as a potential therapeutic agent for metabolic diseases including type 2 diabetes and cancer [36]. Energy is essential for human life, and the source of energy is ATP (adenosine triphosphate), which is generated when ATP is hydrolyzed and converted into ADP (adenosine diphosphate) [37]. AMPK regulates ATP levels to maintain homeostasis and is expected to be effective against metabolic diseases such as cancer, type 2 diabetes, and obesity [38,39,40]. It is thought that AMPK regulates metabolism by inhibiting ATP consumption pathways [41,42]. Therefore, AMPK contributes to maintaining health in the body by suppressing chronic inflammation [43,44]. It promotes autophagy [45]. It may increase mitochondrial function [46] and increase intracellular ATP levels by activating mitochondrial biosynthesis [47,48].
In other words, it is thought that increasing AMPK activity can prevent lifestyle-related diseases, including cancer. It is thought that AMPK regulates metabolism by inhibiting ATP consumption pathways. There are reports that AMPK activity reduces abnormal inflammatory responses and cellular aging, leading to the treatment of interstitial pneumonia [49], and it was suggested that this effect could be used to play a role in improving interstitial pneumonia caused by platinum-palladium.
In addition, blood tests were performed on patients at the in vivo level to meas- ure the aforementioned KL-6 and blood hydrogen peroxide levels. KL-6 is a high molecular weight sialylated glycoprotein contained mainly in type II alveolar epithelial cells that is strongly involved in the production and secretion of pulmonary surfactant [50], and is widely used clinically to assess the severity of chronic respiratory diseases because it correlates with the activity (severity) of chronic respiratory diseases [51], and is released into the blood due to inflammatory damage to the alveoli [52,53]. It is strongly correlated with the severity of interstitial pneumonia, but it has also been reported to correlate with the severity of lung cancer and mixed disorders (combined with emphysema) [54], and is used clinically [55].In this experiment, the KL-6 value was significantly reduced, suggesting that the severity had improved. In the future, we plan to investigate what action in the body’s dynamics is suppressing the release of KL-6, but one hypothesis is that this is due to improved alveolar function in patients with interstitial pneumonia. At the same time, hydrogen peroxide (H2O2) was examined. Hydrogen peroxide (H2O2) is one of the representative reactive oxygen species (ROS) [56], and in normal physiological actions, it plays an important role in cell signaling, etc. [57], but on the other hand, it induces oxidative stress in the body and is a factor in cell and tissue damage [58,59]. When glucose is ingested in the body, it enters the TCA cycle through the glycolysis process and then passes through the electron transport system to produce ATP [60], but when glucose cannot be ingested, fat and protein are burned to produce ATP. In other words, ATP is essential for human life support [61]. A large amount of oxygen is required to produce this ATP, and naturally this oxygen is taken in through breathing. Most of it is involved in energy production, but a few percent of it is converted into reactive oxygen species (ROS) [62]. ROS have advantages and disadvantages for the body. One advantage is that ROS play a role in the body’s defense mechanism, destroying bacteria and cancer cells in granules contained in neutrophils [63]. It is known that ROS are related to various lifestyle-related diseases, including malignant neoplasms, and aging [64]. Currently, the following four types of ROS are known to exist: 1) Superoxide (O2-), 2) Hydrogen peroxide (H2O2), 3) Hydroxyl radical (·OH), and 4) Singlet oxygen (1O2) [65]. In recent years, methods for removing ROS have been studied both in Japan and overseas for the purpose of preventing diseases and combating aging [66]. Since aging has been treated as a disease name since ICD-11, [67]it is expected that further research on antioxidants will be conducted in the future. In this context, it has been confirmed that platinum-palladium is the only substance in the world that can remove all four types of reactive oxygen mentioned above [68]. In this study, from the perspective that there may be a possibility that hydrogen peroxide is generated in large amounts in patients with interstitial pneumonia before and after taking platinum-palladium, [69] the plasma hydrogen peroxide level was qualitatively measured, and a significant difference was observed in this experiment, confirming a tendency for hydrogen peroxide to decrease in the body when platinum-palladium was used. Hydrogen peroxide is a type of reactive oxygen species [70], and it is possible that hydrogen peroxide may affect the alveoli in patients with interstitial pneumonia and COPD [71] Therefore, the fact that a decreasing trend was observed in this study indicates that platinum-palladium significantly reduced KL-6 and hydrogen peroxide in patients with interstitial pneumonia. This suggests that platinum-palladium may be effective at the pharmaceutical level not only for interstitial pneumonia but also for COPD by protecting the alveoli in the reduction of KL-6, suppressing the effects of ROS caused by hydrogen peroxide, and increasing mitochondrial activity.
5. Ethical Considerations
This study was conducted with the approval of the Hino Kosei Clinic Ethics Comittee. Ethics Review Numbers HKC_N10023001, HKC_N10023002, HKC_N10023003, HKC_N10023004)
Acknowledgements
We would like to express our sincere gratitude to the university staff and clinic staff who cooperated with in vivo and in vitro research in conducting this study, and to Professor Yoshitaka Fukuzawa of Aichi Medical University and the Center for Preemptive and Integrated Medical Care for his advice.
References
- Lamb YN. Nintedanib: A Review in Fibrotic Interstitial Lung Diseases [published correction appears in Drugs. 2021 Apr 13;:] [published correction appears in Drugs. 2021 Jun;81(9):1133]. Drugs. 2021;81(5):575-586. [CrossRef]
- Renzoni EA, Poletti V, Mackintosh JA. Disease pathology in fibrotic interstitial lung disease: is it all about usual interstitial pneumonia? Lancet. 2021 Oct 16;398(10309):1437-1449. [CrossRef]
- Graney BA, Fischer A. Interstitial Pneumonia with Autoimmune Features. Ann Am Thorac Soc. 2019 May;16(5):525-533. [CrossRef]
- Reynolds C, Feary J, Cullinan P. Occupational Contributions to Interstitial Lung Disease. Clin Chest Med. 2020 Dec;41(4):697-707. [CrossRef]
- Renzoni EA, Poletti V, Mackintosh JA. Disease pathology in fibrotic interstitial lung disease: is it all about usual interstitial pneumonia? Lancet. 2021 Oct 16;398(10309):1437-1449. [CrossRef]
- Belloli EA, Beckford R, Hadley R, Flaherty KR. Idiopathic non-specific interstitial pneumonia. Respirology. 2016 Feb;21(2):259-68. [CrossRef]
- ATS Am J Respir Crit Care Med. 2002;165:277. [CrossRef]
- Maher TM, Wuyts W. Management of Fibrosing Interstitial Lung Diseases. Adv Ther. 2019;36(7):1518-1531. [CrossRef]
- akahashi H, Fujishima T, Koba H, Murakami S, Kurokawa K, Shibuya Y, Shiratori M, Kuroki Y, Abe S. Serum surfactant proteins A and D as prognostic factors in idiopathic pulmonary fibrosis and their relationship to disease extent. Am J Respir Crit Care Med. 2000 Sep;162(3 Pt 1):1109-14. [CrossRef]
- Chiba H, Otsuka M, Takahashi H. Significance of molecular biomarkers in idiopathic pulmonary fibrosis: A mini review. Respir Investig. 2018 Sep;56(5):384-391. [CrossRef]
- Brasch F. Interstitielle Lungenerkrankungen [Interstitial pulmonary diseases]. Pathologe. 2006;27(2):116-132. [CrossRef]
- Wong AW, Ryerson CJ, Guler SA. Progression of fibrosing interstitial lung disease. Respir Res. 2020;21(1):32. Published 2020 Jan 29. [CrossRef]
- GERARD M. TURIN: Natural History and Clinical Management of Emphysema in Patients with and without Alpha1-Antitrypsin Inhibitor Deficiency. Annals of the New York Academy of Sciences. 1991; 624(1), 18-29. [CrossRef]
- D P Tashkin, R Detels, M Simmons, H Liu, A H Coulson, J Sayre, S Rokaw: The UCLA population studies of chronic obstructive respiratory disease. XI. Impact of air pollution and smoking an annual change in forced expiratory volume in one second. Amer J Respir Crit Care Med. 1994; 149(5), 1209-1217. [CrossRef]
- Stoller JK, Panos RJ, Krachman S, Doherty DE, Make B; Long-term Oxygen Treatment Trial Research Group. Oxygen therapy for patients with COPD: current evidence and the long-term oxygen treatment trial. Ches. 2010; 138(1), 179-187. [CrossRef]
- Organization WH. World health statistics 2010. World Health Organization, Geneva, 2010. https://scholar.google.com/scholar?hl=en&q=Organization+WH.+World+health+statistics+2010.+World+Health+Organization%2C+Geneva%2C+2010. Retrieved June 8, 2022.
- R. P. Young, R. J. Hopkins, T. Christmas, P. N. Black, P. Metcalf, G. D. Gamble: COPD prevalence is increased in lung cancer, independent of age, sex and smoking history. European Respiratory Journal. 2009; 34, 380-386. [CrossRef]
- Fischer BM, Voynow JA, Ghio AJ. COPD: balancing oxidants and antioxidants. Int J Chron Obstruct Pulmon Dis. 2015;10:261-276. Published 2015 Feb 2. [CrossRef]
- Alexandra, Moreira-Pais, Rita Ferreira, Rui Gil da Costa: Platinum-induced muscle wasting in cancer chemotherapy: Mechanisms and potential targets for therapeutic intervention. Life Sciences. 2018; 208, 1-9. [CrossRef]
- Malinowska Katarzyna, Szczepanska Anna, Hanna Zielinska-Blizniewska, Majsterek Ireneusz: An Evaluation of the Antioxidant and Anticancer Properties of Complex Compounds of Copper (II), Platinum (II), Palladium (II) and Ruthenium (III) for Use in Cancer Therapy. Mini-Reviews in Medicinal Chemistry. 2018; 18(16), 1373 – 1381. [CrossRef]
- Seung JunLeea, YiseulYua, Hyeon Jin Jung, Shreyanka Shankar Naik, Sanghun Yeon, Myong Yong Choi: Efficient recovery of palladium nanoparticles from industrial wastewater and their catalytic activity toward reduction of 4-nitrophenol. Chemosphere. 2021; 262, 128358. [CrossRef]
- Yurdanur Ucar, William A Brantley, Sreenivas N Bhattiprolu, William M Johnston, Edwin A McGlumphy: Characterization of cast-to implant components from five manufacturers. The Journal of Prosthetic Dentistry. 2009; 102(4), 216-223. [CrossRef]
- Hiroya Okamoto, Kentaro Horii, Akio Fujisawa, Yorihiro Yamamoto: Oxidative deterioration of platinum nanoparticle and its prevention by palladium. Experimental Dermatology. 2012; 21(S1), 5-7. [CrossRef]
- Shuichi Shibuya, Yusuke Ozawa, Kenji Watanabe, Naotaka Izuo, Toshihiko Toda, Koutaro Yokote, Takahiko Shimizu: Palladium and platinum nanoparticles attenuate aging-like skin atrophy via antioxidant activity in mice. PLoS One, 2014; 9(10), e109288. [CrossRef]
- Satoshi Kawakami, Hiroyuki Ichikawa, Tsutomu Sato, Hiroki Kataoka, Takaharu Ide, Hayato Terayama, Kou Sakabe: Antioxidant ability of platinum-palladium -Study using soft drinks containing platinum-palladium-. Journal of the Japan Society for Oral Functional Water. 2021; 22(1), 3-9.
- Bowen Yang, Yu Chen, Jianlin Shi: Reactive Oxygen Species (ROS)-Based Nanomedicine. Chemical Reviews. 2019; 119(8):4881-4985. [CrossRef]
- Binks SP, Dobrota M. Kinetics and mechanism of uptake of platinum-based pharmaceuticals by the rat small intestine. Biochem Pharmacol. 1990; Sep 15;40(6):1329-36. [CrossRef]
- Sable, V., Maindan, K., Kapdi, A. R., Shejwalkar, P. S., & Hara, K: Active Palladium Colloids via Palladacycle Degradation as Efficient Catalysts for Oxidative Homocoupling and Cross-Coupling of Aryl Boronic Acids. ACS omega. 2017; 2(1), 204–217. [CrossRef]
- Lee JS, Lee EY, Ha YJ, Kang EH, Lee YJ, Song YW. Serum KL-6 levels reflect the severity of interstitial lung disease associated with connective tissue disease. Arthritis Res Ther. 2019 ; 21(1):58. [CrossRef]
- Song X, Bai S, He N, Wang R, Xing Y, Lv C, Yu F. Real-Time Evaluation of Hydrogen Peroxide Injuries in Pulmonary Fibrosis Mice Models with a Mitochondria-Targeted Near-Infrared Fluorescent Probe. ACS Sens. 2021; 6(3): 1228-1239. [CrossRef]
- Naoya Sakuraba, Yoko Togami: Fundamental and clinical evaluation of KL—6 measurement by chemiluminescent enzyme immunoassay system “Lumipulse Presto KL—6 Eisai”. Jpn J Med Pharm Sci. 2009; 61(4): 629-635. (in Japanese).
- Ogihara T, Hirano K, Morinobu T, Ogawa S, Hiroi M, Ban R, Ogihara H, Tamai H. KL-6, a mucinous glycoprotein, as an indicator of chronic lung disease of the newborn. J Pediatr. 2000 Aug;137(2):280-2. [CrossRef]
- Wei-Zheng Zhang, Kylie Venardos, Jaye Chin-Dusting, David M Kaye: Adverse effects of cigarette smoke on NO bioavailability: role of arginine metabolism and oxidative stress. Hypertension. 2006; 48(2), 278-285. [CrossRef]
- RonMittler: ROS Are Good. Trends in Plant Science. 2017; 22(1),11-19. [CrossRef]
- Ilaria Liguori, Gennaro Russo, Francesco Curcio, Giulia Bulli, Luisa Aran, David Della-Morte, Gaetano Gargiulo, Gianluca Testa, Francesco Cacciatore, Domenico Bonaduce, Pasquale Abete: Oxidative stress, aging, and diseases, Clinical Interventions in Aging. 2018; 13: 757–772. [CrossRef]
- David Carling: AMPK signalling in health and disease. Current Opinion in Cell Biology. 2017; 45, 31-37. [CrossRef]
- P.D. Boyer, B. Chance, L. Ernster, P. Mitchell, E. Racker, E.C. Slater: Oxidative phosphorylation and photophosphorylation. Annual Review of Biochemistry. 1977; 46, 955-1026. [CrossRef]
- Barbara Cool, Bradley Zinker, William Chiou, Lemma Kifle, Ning Cao, Matthew Perham, Robert Dickinson, Andrew Adler, Gerard Gagne, Rajesh Iyengar, Gang Zhao, Kennan Marsh, Philip Kym, Paul Jung, Heidi S Camp, Ernst Frevert: Identification and characterization of a small molecule AMPK activator that treats key components of type 2 diabetes and the metabolic syndrome. Cell Metabolism. 2006; 3(6), 403-416. [CrossRef]
- Fabrizio Giordanetto, David Karis: Direct AMP-activated protein kinase activators: a review of evidence from the patent literature. Expert Opinion on Therapeutic Patents. 2012; 22(12), 1467-77. [CrossRef]
- Bing Xiao, Matthew J. Sanders, David Carmena, Nicola J. Bright, Lesley F. Haire, Elizabeth Underwood, Bhakti R. Patel, Richard B. Heath, Philip A. Walker, Stefan Hallen, Fabrizio Giordanetto, Stephen R. Martin, David Carling & Steven J. Gamblin: Structural basis of AMPK regulation by small molecule activators. Nature Communications. 2013; 4, 3017. [CrossRef]
- Herzig S, Shaw RJ. AMPK: guardian of metabolism and mitochondrial homeostasis. Nat Rev Mol Cell Biol. 2018;19(2), 121-135. [CrossRef]
- Mihaylova MM, Shaw RJ. The AMPK signalling pathway coordinates cell growth, autophagy and metabolism. Nature cell biology. 2011; 13, 1016–1023. [CrossRef]
- Russell FM, Hardie DG. AMP-Activated Protein Kinase: Do We Need Activators or Inhibitors to Treat or Prevent Cancer?. Int J Mol Sci. 2020;22(1), 186. [CrossRef]
- Wu S, Zou MH. AMPK, Mitochondrial Function, and Cardiovascular Disease. Int J Mol Sci. 2020;21(14), 4987. [CrossRef]
- Zhang D, Wang W, Sun X, et al. AMPK regulates autophagy by phosphorylating BECN1 at threonine 388. Autophagy. 2016;12(9):1447-1459. [CrossRef]
- Bergeron R, et al. Chronic activation of AMP kinase results in NRF-1 activation and mitochondrial biogenesis. Am J Physiol Endocrinol Metab. 2001; 281, E1340–E1346. [CrossRef]
- Hwang, Jung Hwan et al.: Enhanced Production of Adenosine Triphosphate by Pharmacological Activation of Adenosine Monophosphate-Activated Protein Kinase Ameliorates Acetaminophen-Induced Liver Injury. Molecules and cells. 2015; 38(10), 843-50. [CrossRef]
- Hardie D.G., Schaffer B.E., Brunet A. AMPK: an energy-sensing pathway with multiple inputs and out-puts. Trends Cell Biol. 2016;26(3), 190–201. [CrossRef]
- Xiao-Yu Cheng, Yang-Yang Li, Cheng Huang, Jun Li, Hong-Wei Yao: AMP-activated protein kinase reduces inflammatory responses and cellular senescence in pulmonary emphysema. Oncotarget. 2017; 8(14), 22513-22523. [CrossRef]
- Osaka A, Yanagihara K, Yamada Y, Hasegawa H, Inokuchi N, Hayashi T, Komoda M, Nakamura S, Aoyama M, Sawada T, Kamihira S. Elevation of serum KL-6 glycoprotein or surfactant protein-D in adult T-cell leukemia with distinct pulmonary complications. Tohoku J Exp Med. 2009;218(2):99-105. [CrossRef]
- Okamoto T, Fujii M, Furusawa H, Tsuchiya K, Miyazaki Y, Inase N. The usefulness of KL-6 and SP-D for the diagnosis and management of chronic hypersensitivity pneumonitis. Respir Med. 2015;109(12):1576-81. [CrossRef]
- Kubota M, Haruta T. The role of serum KL-6 measurement in common pediatric respiratory infections. J Infect Chemother. 2006 ;12(1):22-4. [CrossRef]
- Zhang Y, Kaminski N. Biomarkers in idiopathic pulmonary fibrosis. Curr Opin Pulm Med. 2012 ;18(5):441-6. [CrossRef]
- d’Alessandro M, Bergantini L, Cameli P, Pieroni M, Refini RM, Sestini P, Bargagli E. Serum Concentrations of KL-6 in Patients with IPF and Lung Cancer and Serial Measurements of KL-6 in IPF Patients Treated with Antifibrotic Therapy. Cancers (Basel). 2021;13(4):689. [CrossRef]
- Miyazaki K, Kurishima K, Kagohashi K, Kawaguchi M, Ishikawa H, Satoh H, Hizawa N. Serum KL-6 levels in lung cancer patients with or without interstitial lung disease. J Clin Lab Anal. 2010;24(5):295-9. [CrossRef]
- Knaus UG. Oxidants in Physiological Processes. Handb Exp Pharmacol. 2021;264:27-47. [CrossRef]
- Sies H. Hydrogen peroxide as a central redox signaling molecule in physiological oxidative stress: Oxidative eustress. Redox Biol. 20171; 11, 613-619. [CrossRef]
- Watt BE, Proudfoot AT, Vale JA. Hydrogen peroxide poisoning. Toxicol Rev. 2004;23(1):51-7. [CrossRef]
- van der Vliet A, Janssen-Heininger YM. Hydrogen peroxide as a damage signal in tissue injury and inflammation: murderer, mediator, or messenger? J Cell Biochem. 2014 ;115(3):427-35. [CrossRef]
- Tang BL. Glucose, glycolysis, and neurodegenerative diseases. J Cell Physiol. 2020 Nov;235(11):7653-7662. [CrossRef]
- Judge A, Dodd MS. Metabolism. Essays Biochem. 2020 Oct 8;64(4):607-647. [CrossRef]
- Ministry of Health , Labour and Welfare, Reactive oxygen species and oxidative stress. https://www.e-healthnet.mhlw.go.jp/information/food/e-04-003.html (Accessed April 28, 2023) (in Japanese).
- Beck-Schimmer B, Bonvini JM. Bronchoaspiration: incidence, consequences and management. Eur J Anaesthesiol. 2011 ;28(2):78-84. [CrossRef]
- Singh A, Kukreti R, Saso L, Kukreti S. Oxidative Stress: Role and Response of Short Guanine Tracts at Genomic Locations. Int J Mol Sci. 2019;20(17):4258. [CrossRef]
- Madreiter-Sokolowski CT, Thomas C, Ristow M. Interrelation between ROS and Ca in aging and age-related diseases. Redox Biol. 2020 ;36:101678. [CrossRef]
- Moore MN. Autophagy as a second level protective process in conferring resistance to environmentally-induced oxidative stress. Autophagy. 2008;4(2):254-6. [CrossRef]
- Calimport SRG, Bentley BL. Aging Classified as a Cause of Disease in ICD-11. Rejuvenation Res. 2019 Aug;22(4):281. [CrossRef]
- Satoshi Kawakami, Hiroyuki Ichikawa, Tsutomu Sato, Hiroki Kataoka, Takaharu Ide, Hayato Terayama, Kou Sakabe: Antioxidant ability of platinum-palladium -Study using soft drinks containing platinum-palladium-, J Jpn Soc Oral Funct Water, 2021;22,3-10. (in Japanese).
- Nagaraja C, Shashibhushan BL, Sagar, Asif M, Manjunath PH. Hydrogen peroxide in exhaled breath condensate: A clinical study. Lung India. 2012;29(2):123-7. [CrossRef]
- Brand MD. Mitochondrial generation of superoxide and hydrogen peroxide as the source of mitochondrial redox signaling. Free Radic Biol Med. 2016;100:14-31. [CrossRef]
- Ramírez-Prieto MT, García-Río F, Villamor J. Papel del estrés oxidativo en las enfermedades respiratorias y su monitorización [Role of oxidative stress in respiratory diseases and its monitoring]. Med Clin (Barc). 2006;127(10):386-96. [CrossRef]
Figure 4.
AMPK activity in platinum-palladium compared to the control group (100%) (Mann-Whitney U test. P<0.01).
Figure 4.
AMPK activity in platinum-palladium compared to the control group (100%) (Mann-Whitney U test. P<0.01).
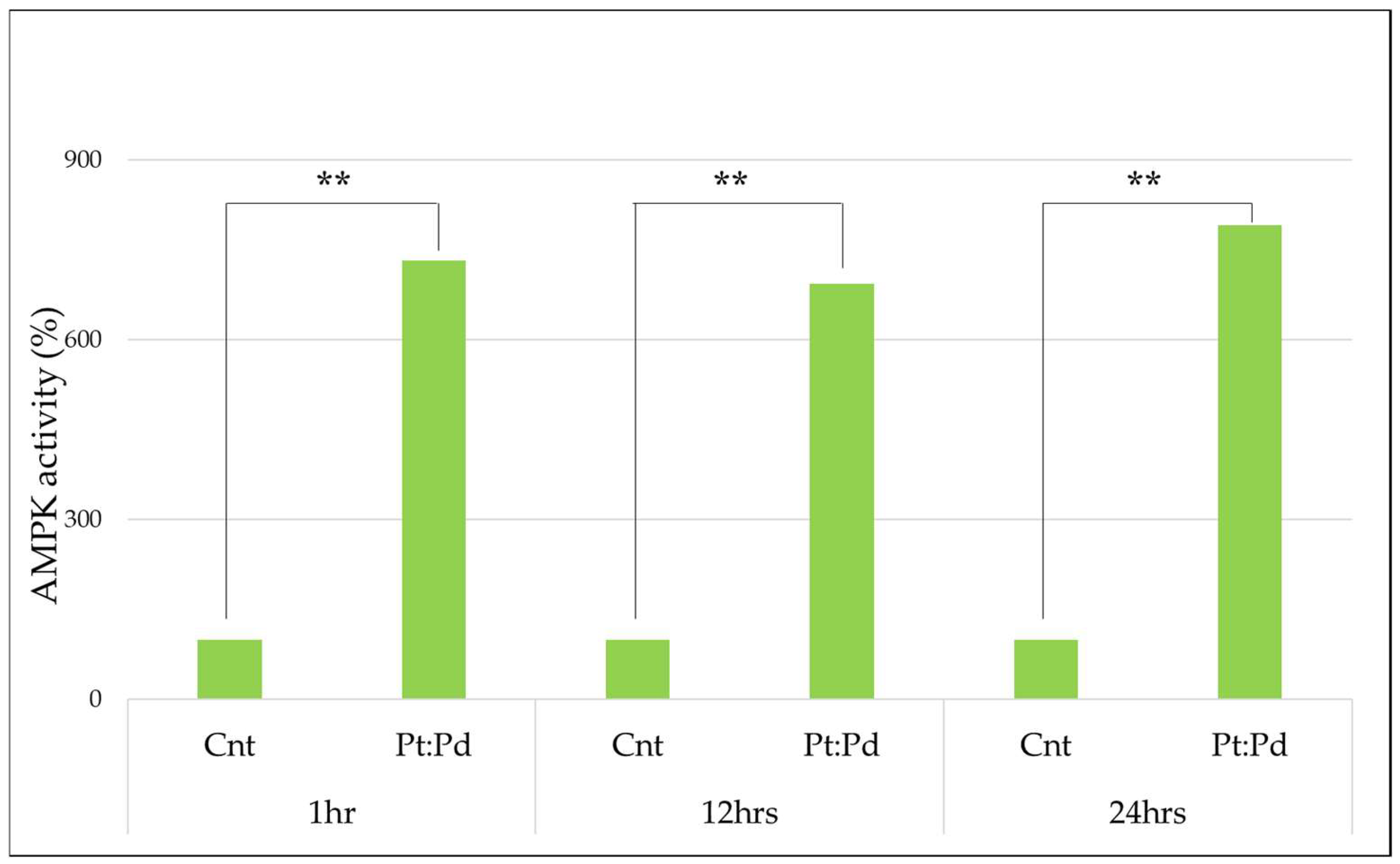
Figure 5.
Changes in KL-6 before and after platinum-palladium administration (Paired-samples t-test. P<0.05) .
Figure 5.
Changes in KL-6 before and after platinum-palladium administration (Paired-samples t-test. P<0.05) .
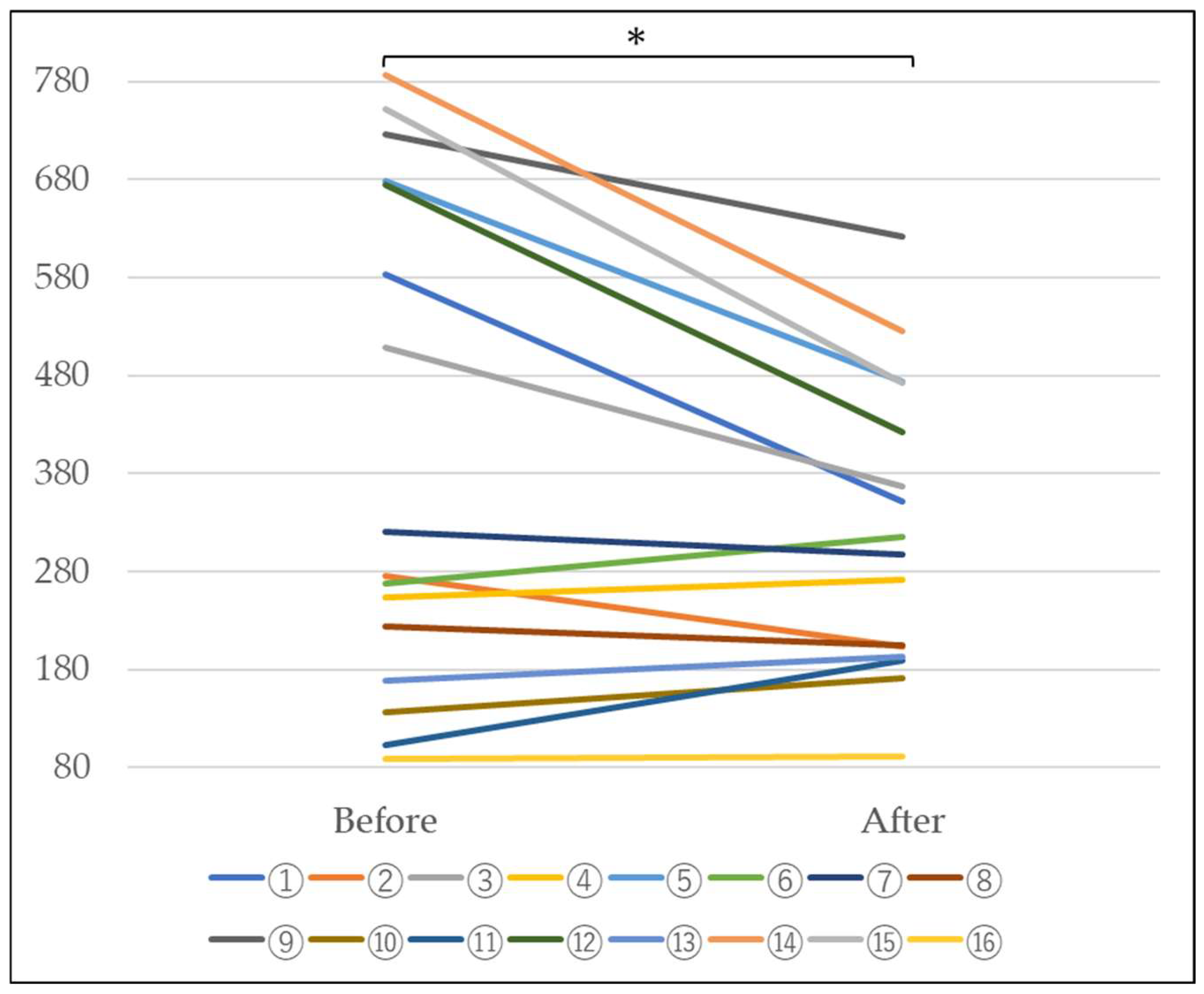
Figure 6.
Changes in blood hydrogen peroxide levels before and after administration of platinum-palladium (Paired-samples t-test. P<0.05) .
Figure 6.
Changes in blood hydrogen peroxide levels before and after administration of platinum-palladium (Paired-samples t-test. P<0.05) .
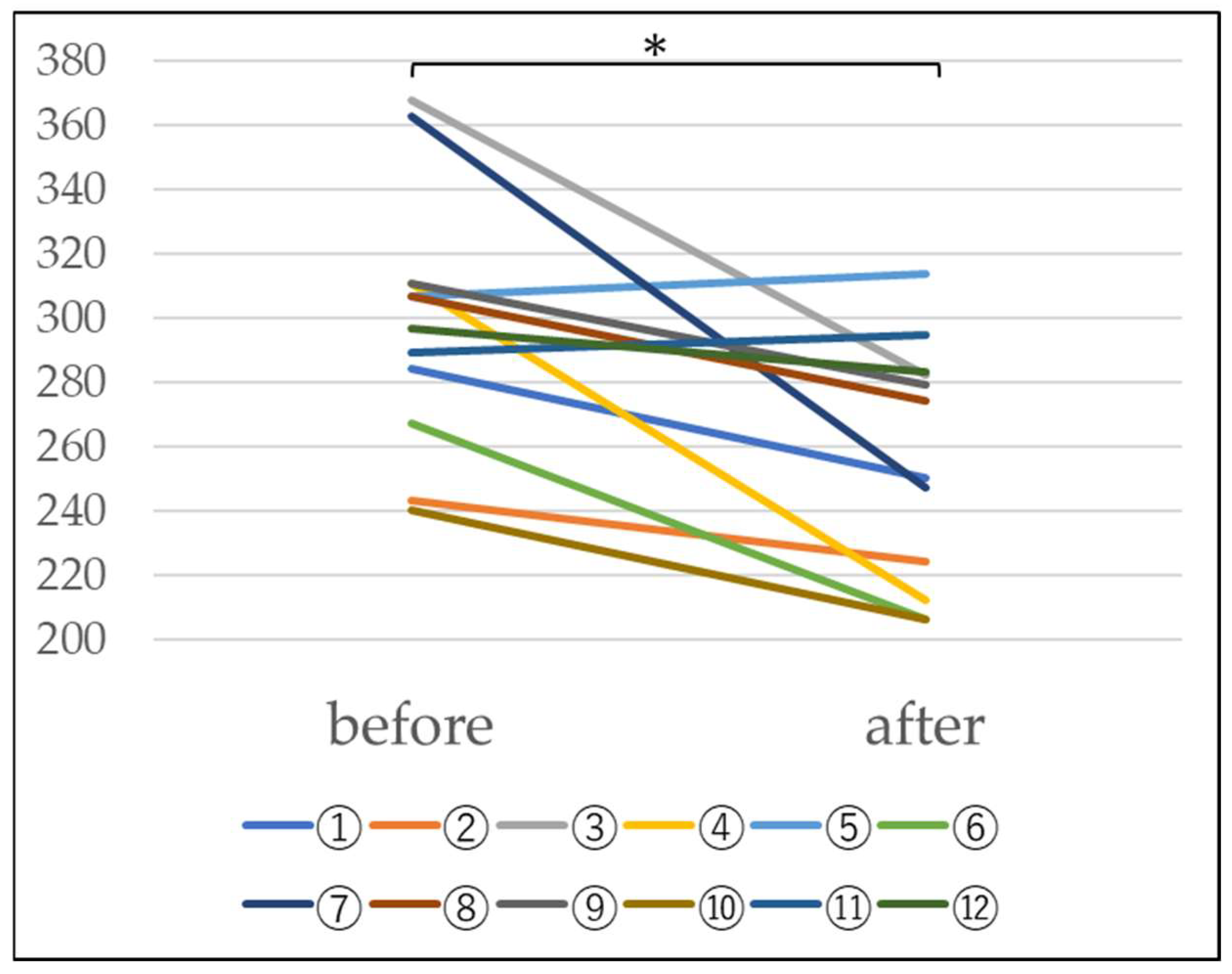
Figure 7.
Changes after drinking platinum-palladium.
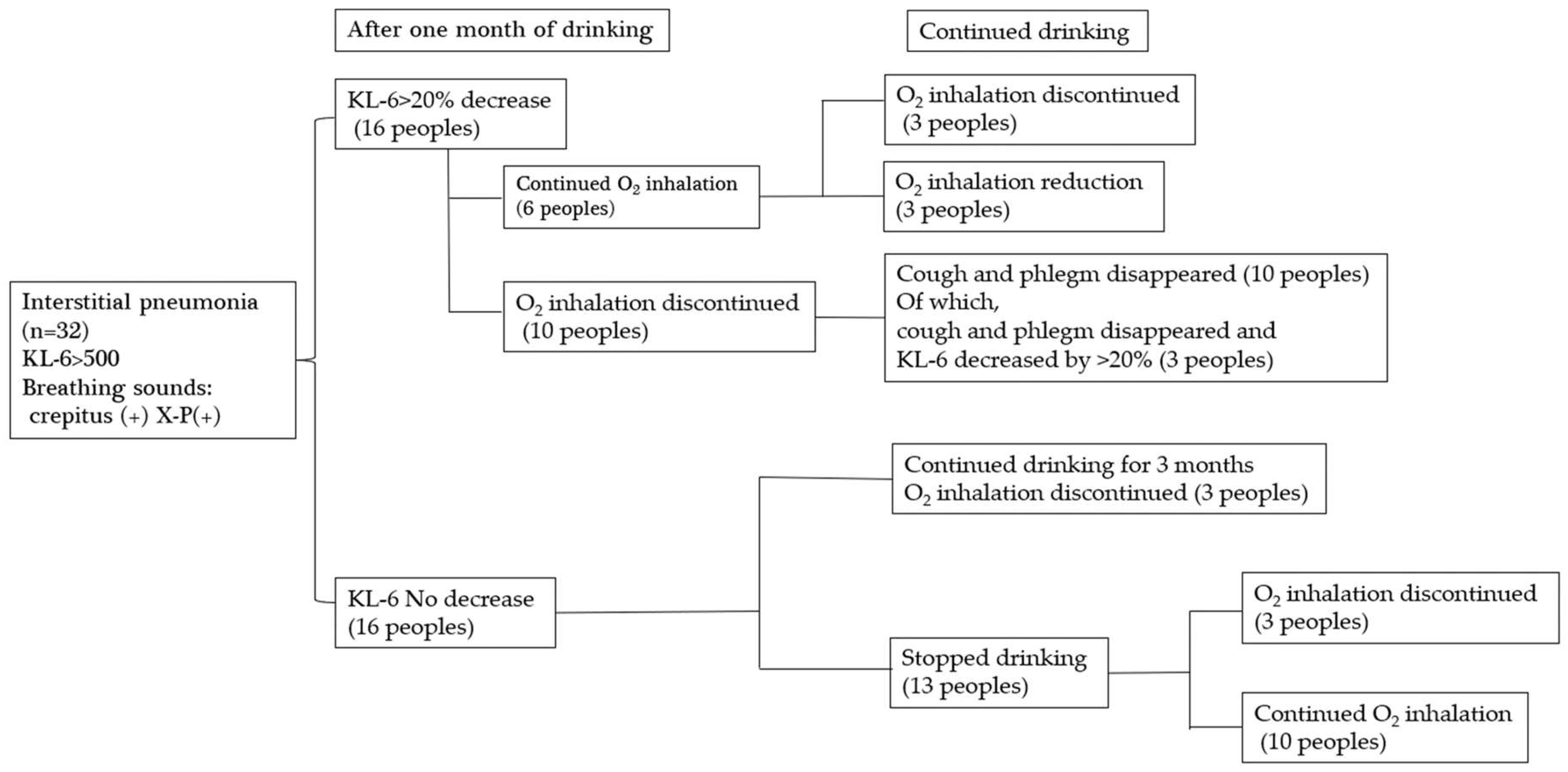
Table 3.
Comparison of KL-6 before and after administration of platinum-palladium (n=16) KL-6 (IU/ml).
Table 3.
Comparison of KL-6 before and after administration of platinum-palladium (n=16) KL-6 (IU/ml).
 |
Table 4.
Changes in blood hydrogen peroxide levels due to platinum-palladium (U).
 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



