
Submitted:
01 October 2024
Posted:
02 October 2024
You are already at the latest version
Abstract
The following systematic and bibliographic review investigates the intersection between the treatment of cognitive impairments and virtual and augmented reality-based game-oriented applications. The review provides a view into the last 12 years of research. The PubMed Database served as the main source for the review. We defined a comprehensive set of investigation variables and classified three main topics: bibliography, medical, and technical. Of a total of 61 identified articles, 19 were included. The findings from these studies indicate the positive effects of using virtual and augmented reality applications to improve cognitive function and depression. There is also a gap in high-quality evidence since clinical trials have been conducted only with a few patients. Preliminary results indicate positive cognitive and physical well-being effects, but the field demands further investigation to determine the effectiveness. Future research needs to focus on larger studies and the quality of the developed applications. Further, it is important to look at scores like Quality of Living and Satisfaction in Daily Activities to create a functioning environment for the patient.
Keywords:
medicine
; cognitive impairment
; dementia
; alzheimer’s
; virtual reality
; augmented reality
; systematic review
1. Introduction
Neurodegenerative diseases are a growing global issue [1]. Most Western societies face an expanding ageing population, while multiple forms of neurodegeneration are taking a strain on the life quality of patients and have an overall impact on mortality [2]. The growth in the number of dementia-related disorders such as Alzheimer’s or Parkinson’s disease creates importance to finding novel approaches to assess, handle and get an understanding of these diseases.
Dementia treatment is based on cognitive and physical stimulation to prevent the fast decline of neurocognitive functions. The argument is that there is a benefit in using virtual reality games and generating an influential immersion and cognitive stimulation in dementia patients [3]. This review project addresses the intersection of the two domains and provides an overview of the current state of research and applied technologies.
1.1. Background
Dementia severely impacts individuals, families, and healthcare systems. Roberts and Knopman define dementia as a progressive decline in cognitive abilities, memory loss, impaired thinking, and behavioural changes [4]. Fifty million people worldwide have dementia, growing by 10 million cases each year; this figure is to triple by 2050. In a total projection, the number of people with dementia is going to reach 82 million in 2030 and 152 million by 2050 [5]. Established pharmacological treatments for dementia are known to have limited success in alleviating symptoms and slowing disease progression. Current pharmaceutical drug development appears slow and without recent promising results, as discovered by Kim et al. [6]. The current research focuses mainly on non-pharmacological interventions, as Meyer et al. find [7].
Traditional treatment includes medication, regular exercise, cognitive stimulation and a healthy diet. Furthermore, having a supportive environment and social interaction is essential, as found in the German S3 guideline for dementia [3]. Video games are interactive electronic experiences. They can influence behaviour, cognition and emotions alike. Research explores topics such as improved attention and better problem-solving, recently thematized by Rodrigo-Aynguas et al. [8] and emotional well-being as discussed by Pallavicini et al. [9].
When a game applies to a context beyond entertainment, we refer to it as a serious game, often used in healthcare or education. When a video game shifts from cognitive to physical domains, we call it an exergame that combines exercise and game, first coined in the early 2000s, as Bogost stated in 2005 [10]. Virtual Reality (VR) and Augmented Reality (AR) technology have become more accessible over the recent years and found their way from professional applications to consumer-grade entertainment products, as stated by Munoz-Saavedra et al. in 2020 [11]. VR immerses users in a wholly digital environment, blocking the real world. AR overlays digital information onto scenes from the real world, intending to enhance the user’s perception of reality. The idea is that video games, in combination with VR and AR, can help treat dementia by enhancing cognitive stimulation and improving exercise and movement.
1.2. Overview
In 2022, Flynn et al. [12] looked at critical stakeholders in using AR and VR solutions for older people with dementia. They took a qualitative approach, collected experiences and perceptions of key stakeholders involved in the care, and used VR and AR solutions. Included in the review were 14 studies that revealed three analytical themes: ’entering virtuality’, ’a virtual world’ and ’returning to reality’. Findings suggested that VR can provide positive experiences for older people with Mild Cognitive impairment (MCI) and that it can have a real-life impact. Another point they make is the importance of designing VR interventions with great sensitivity and involving the critical audience in the design process to ensure helpful technology use in dementia care.
The publication of Yen et al. from 2021 explores the effectiveness of virtual reality exergames in improving cognition and reducing depression in older adults. Eighteen randomized clinical trials have been identified and found to have moderate effects on overall cognitive function and memory but significant effects on depression outcomes. Interestingly, commercial VR games showed a more significant positive effect on depression outcomes than VR-aided exergaming. The review finds that there is potential to positively impact cognition, memory, and depression outcomes in older adults [13].
In the extensive review of 325 initially screened publications, Gates et al. [14] find the comparison of computerized cognitive training with active control interventions to improve cognitive function after a 12-week training period slightly but not sustainable when stopped. The study mentions that the evidence and quality are too low to draw definitive conclusions. There are indicators for a slight improvement in episodic memory but small to no effects on working memory and verbal fluency. Also, current research lacks data on follow-up, quality of life indicators, psychological well-being, daily functioning, and adverse events. Identified issues primarily included imprecision and risk of bias. Higher-quality evidence is necessary to conclude with greater certainty [14].
Research often finds positive outcomes regarding experience, cognitive function, and physical performance. However, outcomes are not strongly evident. Researchers need to conduct more studies on virtual and augmented reality to treat patients with dementia and other neurocognitive diseases, mainly focusing on patient-centric topics such as quality of life, well-being, and daily functioning.
2. Method
Moher et al.’s publication informs the research design. However, the study does not strictly adhere to all elements of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. This is due to the focus of the research question, which has a technical approach, looking at medical and technical variables alike. A visual overview can be seen in Figure 1, and the Workflow is described in the following sections.
2.1. Search Strategy and Identification of Articles
As this review’s primary source of publications, the PubMed database, hosted by the National Library of Medicine in the United States, was utilized [15]. The scope of Dementia and Alzheimer’s disease has been narrowed to video games, computer games, exergames and serious games. This narrowing was done to specifically look at gaming-based approaches and further limited to target mainly the Virtual and Augmented Reality niche, see Appendix B.
The initial query has been translated and refined using the advanced search capabilities provided by PubMed. Boolean operators and medical subject headings (MeSH) were used to find additional articles that explicitly addressed the intersection of dementia, video games, VR, and AR. The expanded query is in the Appendix C. The search was conducted on Wednesday, 30. January 2024 and returned an initial set of 61 results. The search process was aided by the Python library PyMed, which was utilized to interact with the PubMed API.
2.2. Article Screening and Eligibility
After an initial screening of 61 publications, a set of false-positive keywords was identified and transferred into a list of exclusion terms. This enabled the functionality to exclude the terms from the result list automatically. This function has been applied to the title and keywords of the results. The list of false-positive words is included in the publication and can be found in Appendix D. Application of the exclusion terms excluded seven false-positive publications from the result set. Review Articles were not included in the publication. A selection of the most recent reviews was summarized in the Background Section 1.2. In total, 18 reviews were identified and excluded. After removing false positives based on an exclusion list and excluding reviews from the original result set, 36 articles remained and underwent a manual screening process. The eligibility criteria were defined as follows:

Table 1.
Inclusion and Exclusion Criteria for the screening process
| Criteria Type | Description |
|---|---|
| Exclusion Criteria |
|
| Inclusion Criteria |
|
The above-stated eligibility criteria were sufficient for 19 publications. Seventeen publications were excluded.
2.3. Investigation Scope
After the initial review and the application of the eligibility criteria, the 19 remaining publications underwent manual screening and full-text analysis. Within the process, certain Variables were defined and gathered from the publications and their available meta-data.
2.3.1. Bibliographic Variables
Bibliographic variables help to understand basic information about the publication. Two bibliographic variables turned out to be relevant for further investigation and visualization.
Table 2.
Description of Bibliographic Variables
| Variable | Description |
|---|---|
| Year of Publication | Represents the paper’s first publication year. |
| Country of Origin | To create geographical context, the Country of Origin of the publication has been extracted. In the case of multiple authors and affiliations to different organizations, the extracted country is the first affiliation of the first author. |
2.3.2. Medical Variables
In a medical context, variables like the medical condition, advancement of clinical trials, participation in clinical trials and engagement intensity are applied to gain insight into the state of research.
Table 3.
Clinical Research Variables and Descriptions
| Variable | Description |
|---|---|
| Parkinson’s Disease | ICD code G20. |
| Advancement of Clinical Research | Looks into the type of trial conducted and referred to in the assessed publication. |
| Single Case Study | Examination of an individual case to gain in-depth insights into a particular observation. |
| Pilot Study | A small-scale study conducted to evaluate factors like usability, time, cost, and risks. It does not evaluate treatment effects. |
| Feasibility Study | Investigations into the viability of a clinical trial, involving control and randomization groups. Fewer participants than in an RCT but more than in a pilot study. |
| Randomized Clinical Trial (RCT) | Subjects are randomly assigned to intervention groups to evaluate treatment effects and risks compared to a control group. |
| Participation in Clinical Research | Refers to the number of subjects participating in a clinical trial or study. |
| Engagement Intensity | A set of numeric values representing the engagement intensity of applied interventions. |
| Overall period of engagement | Measured in weeks. |
| Number of weekly sessions | The number of weekly sessions administered. |
| Average session duration | Duration of a single session, measured in minutes. |
| Simulator Sickness | Refers to issues of simulator sickness when using AR/VR applications caused by the decoupling of movement and visual signals. |
2.3.3. Technical Variables
The following variables have been defined to be investigated to gain technical insight into the development and state of VR/AR applications.
Variable: Immersion Level describes how advanced a System is in terms of immersion. Therefore, we rely on Milgram’s taxonomy on Mixed Reality [16]. Who classified the spectrum of AR and VR soft- and hardware under the term mixed reality for reference, see Figure 2
Milgram et al.’s taxonomy is defined by a 3-axis continuum that creates a space for classifying VR and AR technologies.
- Extent of World Knowledge (EWK) (Real World vs. Artificial (modelled) world)
- Reproduction Fidelity (RP) (Modelling Quality: Wireframes vs. 3D Real-time)
- Extend of Presence Metaphor (EP) (Monitor-based vs. Head Mounted Device)
Extended World Knowledge (EWK) is used to classify whether a system is an AR (with limited World Knowledge) or VR (with perfect World Knowledge) system. The EWK axis is not essential to the result and is left out of this publication. The following system was designed to classify the type of immersion.
- Rating of the variables Extend of Presence: Delivery from 1-3 (Low, Medium, High)
- Rating of the variable Extend of Presence: Controls from 1-3 (Low, Medium, High)
- Rating of Reproduction Fidelity from 1-6 (from simple to realistic)
The results on the Extent of Presence Metaphor (EP) were summed up, and Reproduction Fidelity (RP) values were used to create a coordinate plane (x,y) for the immersion classification. Results of this assessment were plotted on a grid as seen in subsection Immersion Level 3.3.4.
Table 4.
Clinical Research Variables and Descriptions: Immersion Assessment
| Variable | Description |
|---|---|
| Extent of Presence: Delivery | Refers to the type of device used to deliver content to the user. |
| Monitor | Standard display attached to a computer to represent 2D and 3D environments. |
| 180° Projector | Curved 180° view to create an immersive experience and project 2D and 3D environments. |
| VR Headset | A virtual reality headset (HMD) that immerses the user in a computer-generated 3D environment. |
| Extent of Presence: Controls | Refers to the type of controllers used to interact with the application. |
| Wireless Remote | A handheld device to track motion and interact with digital spaces. |
| Stationary Bike | A fitness bike enabling stationary but active interaction with the digital environment. |
| Touchscreen | A touch-sensitive screen allows direct digital content interaction. |
| Body Controller | An infrared motion-tracking device (e.g., Microsoft Xbox Kinect) that tracks body movements. |
| Green screen | A film technique to replace the background with computer-generated graphics. |
| Classic Gaming Controller | A handheld controller commonly used with computers or gaming consoles. |
| Hand Motion Tracker | A device to track hand and finger gestures for interaction with the application. |
| Reproduction Fidelity | Assesses and rates the maturity and quality of the application on a scale from 1 to 6. A score of 1 represents simple sounds and graphics, while 6 represents a realistic real-time simulation. |
| Immersion Level | The Extent of Presence Metaphor (EP) and Reproduction Fidelity (RP) values are used to classify immersion levels, plotted on a grid as seen in subsection Immersion Level Section 3.3.4. |
| Autonomy and Guidance | Represents the patient’s autonomy while using the application. |
| Supervised | The patient uses the application under supervision. |
| Unsupervised | The patient uses the application without supervision. |
2.4. Data Presentation
The collected data and variables were visualized using the following visualization techniques: Discrete values are presented as regular bar charts, and more complex sets are visualized by violin and scatter plots. Figures have been created using Python and the following libraries for data-mining and visualization: Pandas, Numpy, Matplotlib, and Seaborn.
3. Results
This section presents the systematic and bibliographic review and the analysis of available publications and data.
3.1. Bibliographic Results
This section presents the Bibliographic Results and features the analysis of the publication year and the corresponding author location.
3.1.1. Timeline of Publications
In total, we are looking at 12 years and 19 publications. The first one was issued in 2012 by Anderson et al. [17]. There was no limit set for the publication date of the papers. After a period of no publications from 2015-2017, they peaked from 2018-2022 with a total of 16 publications within the four years, as seen in figure Figure 3 Timeline of Publications.
In 2023, no work on VR and AR in dementia treatment has been published. As described in Section 2.1, the search query was executed in late January 2024 to cover possible publications from 2023 but returned empty for that year.
3.1.2. Country of Origin
Of the 19 publications, three were conducted in the United States of America, followed by Greece, Netherlands, Canada, and Taiwan, with n=2. The remaining origin countries are spread over the globe with a single publication each. For more details, refer to Table 5 Country of Origin.
3.2. Medical Results
The section focuses on medical results and findings within the publications. The following information has been searched for: advancement of clinical research, participation in clinical research, patient engagement intensity, and simulator sickness.
3.2.1. Advancement of Clinical Research
The size and participation in clinical research activities are good indicators of the maturity of the research field. Publications are classified as Randomized Clinical Trials, Pilot Studies, Feasibility Studies, Design Studies and Single Case Studies, all explained in Section 2.3.2 Medical Variables.
Table 6.
Number of Publications by Study Type
| Study Type | Publications |
|---|---|
| Randomized Clinical Trial (RCT) | 8 |
| Pilot Study | 5 |
| Feasibility Study | 4 |
| Design Study | 1 |
| Single Case Study | 1 |
Considered together with section Participation in Clinical Research 3.2.2, the above metric provides an insight into the maturity of the research field and its ongoing projects.
3.2.2. Participation in Clinical Research
The participation numbers of clinical trials are essential to provide realistic numbers for significance, sample size and reliability. Together with the variable Advancement in Clinical Research, Section 3.2.1, this measurement is represented in Figure 4.
3.2.3. Engagement Intensity
This section describes the Intensity of Engagement that a trial participant experiences. Three elements describe the engagement intensity.
- (1)
- Overall period of engagement with the application. As depicted in Figure 5 Overall duration of engagement.
- (2)
- Number of weekly sessions dispensed, As shown in Figure 6 Number of weekly sessions.
- (3)
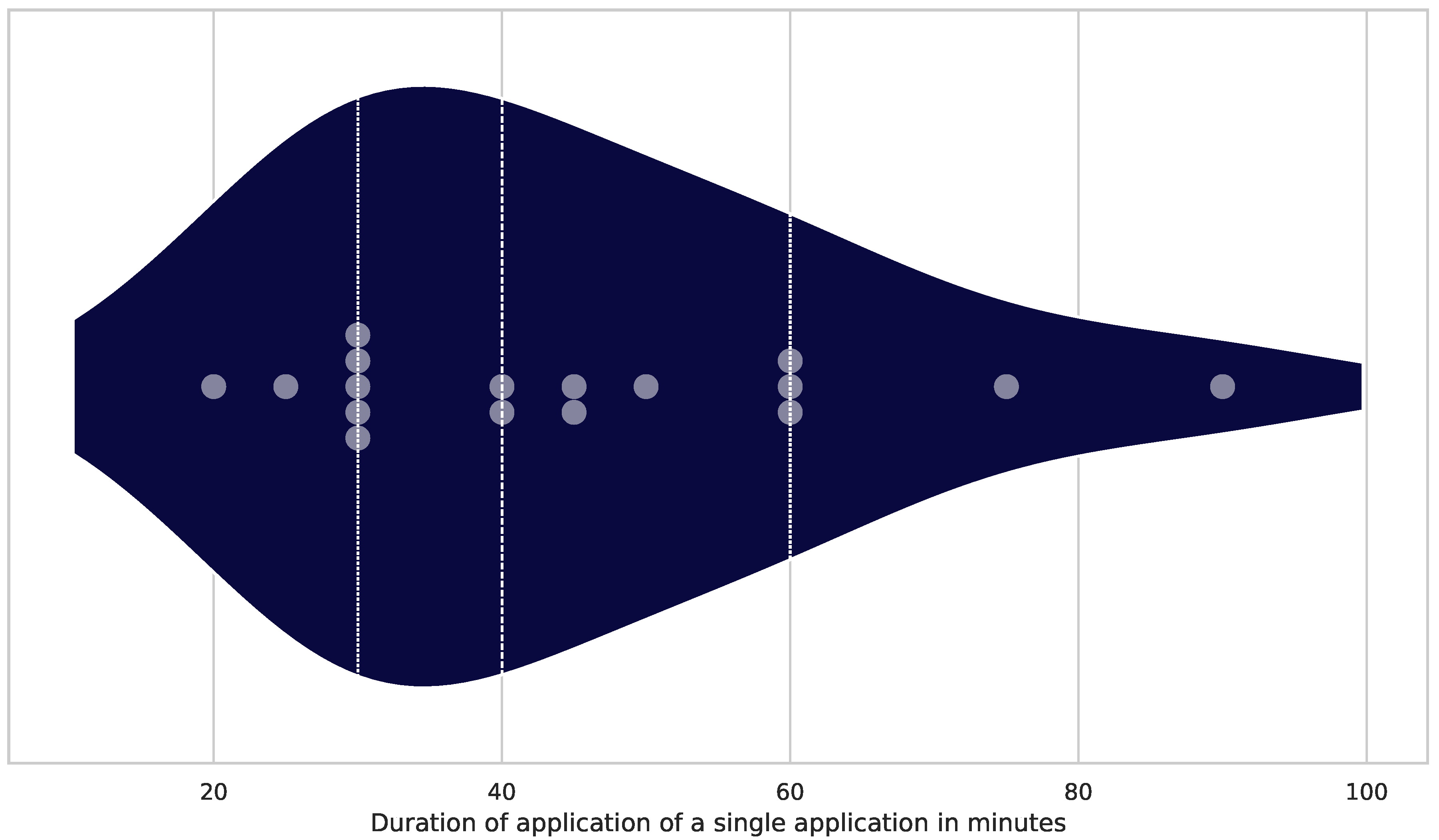
- The average duration of a single session, measured in minutes and visualized in Figure 7 Single session duration.
The following three images show variations in overall publication numbers. The descriptions of the following three figures clarify the total numbers of the datasets.
Figure 5.
Overall duration of study/trial Visualization of the overall duration of the clinical trial in weeks. The three dotted vertical lines represent the lower quartile (4,75 weeks), median (10 weeks) and upper quartile (24 weeks). The grey dots represent the individual trial. The dark blue violin plot visualizes the distribution of publications and weeks (n = 16).
Figure 5.
Overall duration of study/trial Visualization of the overall duration of the clinical trial in weeks. The three dotted vertical lines represent the lower quartile (4,75 weeks), median (10 weeks) and upper quartile (24 weeks). The grey dots represent the individual trial. The dark blue violin plot visualizes the distribution of publications and weeks (n = 16).
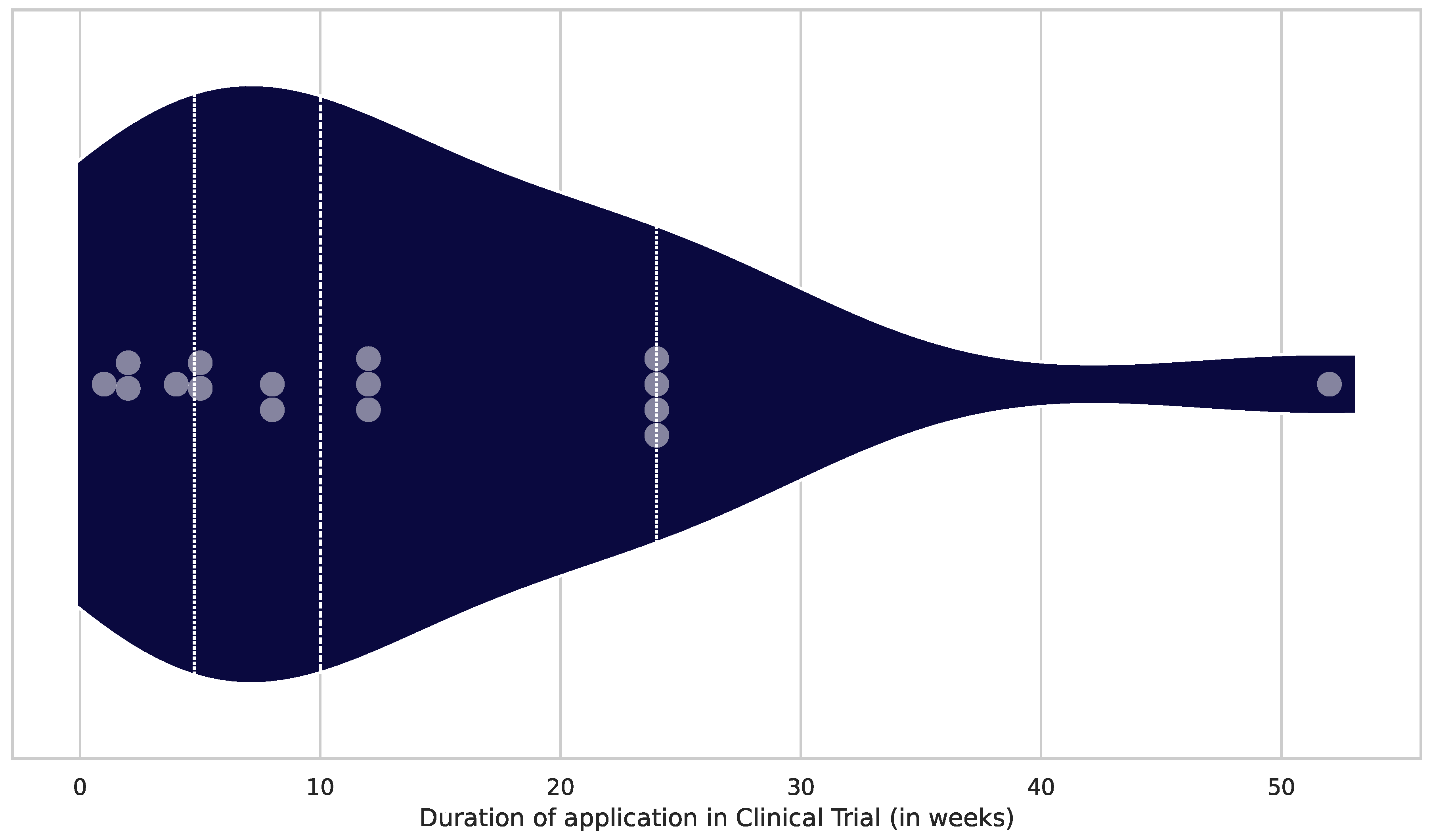
Figure 6.
Number of weekly sessions Weekly number of applied sessions over the total number of weeks. Measured in sessions per week. The three dotted vertical lines represent lower quartile (2 times a week), median (2 times a week) and upper quartile (3 times a week). The grey dots represent the conducted trial. The dark blue violin plot visualizes the distribution of publications and weeks (n = 15).
Figure 6.
Number of weekly sessions Weekly number of applied sessions over the total number of weeks. Measured in sessions per week. The three dotted vertical lines represent lower quartile (2 times a week), median (2 times a week) and upper quartile (3 times a week). The grey dots represent the conducted trial. The dark blue violin plot visualizes the distribution of publications and weeks (n = 15).
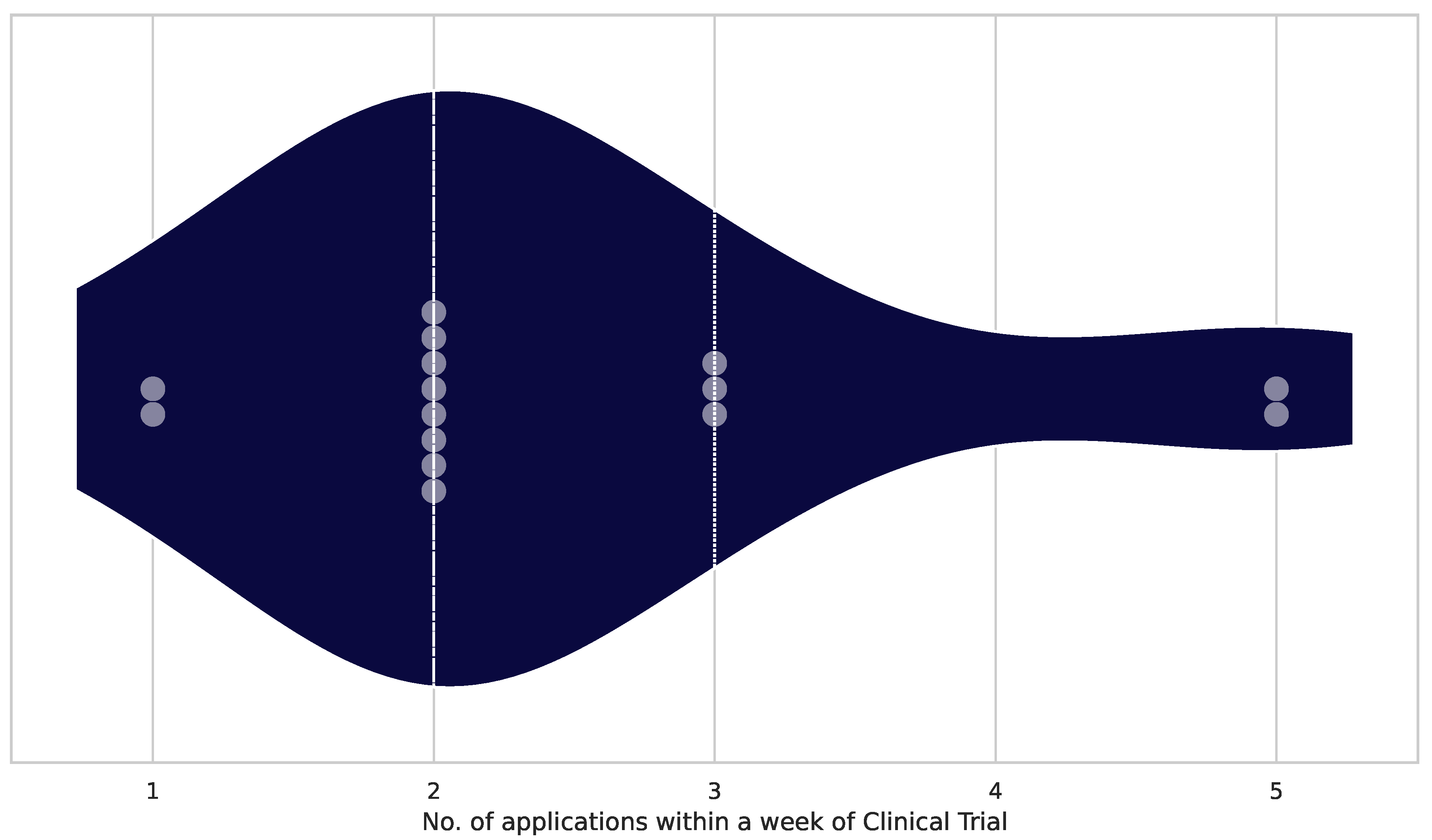
Figure 7.
Single session duration Duration of a single session. Measured in minutes. The three dotted vertical lines represent lower quartile (30 min), median (40 min) and upper quartile (60 min). The grey dots represent the conducted trial, and the dark blue violin plot visualizes the distribution of publications and administered minutes for the individual trial (n = 16).
Figure 7.
Single session duration Duration of a single session. Measured in minutes. The three dotted vertical lines represent lower quartile (30 min), median (40 min) and upper quartile (60 min). The grey dots represent the conducted trial, and the dark blue violin plot visualizes the distribution of publications and administered minutes for the individual trial (n = 16).
3.2.4. Simulator Sickness
Of the 19 publications, 14 contained no information on the topic. Three publications mention that no simulator sickness was reported during the clinical trial.
Zhu et al. are applying an HMD to the Virtual Supermarket Application report of one patient who reported simulator sickness, but it went away after the fifth session [18]. The team of the GRAIL System, a 180°walking simulator published by Amaefule et al. in 2022 [19], identified 1 out of 13 subjects had problems with Simulator Sickness.
In summary, the average clinical trial in VR and AR gaming in preventing dementia over the last 12 years includes 23,5 subjects, follows a protocol lasting ten weeks, has an average of 2 sessions per week, and is 40 minutes long per session. Simulator Sickness is either not present or not reported.
3.3. Technical Results
The Technical Results section considers Device Type, Device Controls, and Immersion Level variables. A first look at Autonomy and Guidance will give insight into whether a patient needs guidance and supervision during use.
3.3.1. Extend of Presence: Delivery
The variable of how the virtual world is delivered to the patient is partly defined by the Computer Output Device. Milgram et al. describe the delivery Method as the Extend of Presence (EP)[16] suggests. The regular TV screen has a lower score, and more advanced VR and AR systems result in a higher score on the EP axis. EP forms the y-axis above in the Figure 8.
Table 7.
Number of Publications by Display Type
| Display Type | Publications |
|---|---|
| TV Screen | 11 |
| HMD (Head-Mounted Display) | 6 |
| 180° Screen | 1 |
| Tablet | 1 |
The German researchers Amaefule et al. built a walking simulator featuring a 180°Field of View provided by a projector in front of an extra-wide treadmill [19]. This is to be seen as the first applied to VR and AR research in dementia treatment. The benefits are ease of use for the patient and great immersion without relying on HMDs to generate the immersion. Through the walking speed, the surrounding 3D environment can be controlled.
3.3.2. Extend of Presence - Controls
This variable, which influences the Extent of Presence in the virtual world, focuses on the controls used to interact with the environment. A versatile controller can significantly improve the user experience and create a more profound sense of immersion, while a poorly chosen controller can ruin it.
Table 8 shows the controllers used within the publications and their distribution.
Table 8.
Number of Publications by Controller Type
| Controller Type | Publications |
|---|---|
| Stationary Bike | 5 |
| Wireless Remote | 4 |
| Classic Gaming Controller | 2 |
| Body Controller | 2 |
| Treadmill | 2 |
| Greenscreen | 1 |
| Hand Motion Tracker | 1 |
| Driving Simulator | 1 |
| Touchscreen | 1 |
The stationary bike is the main used input controller and appears in 5 publications. This is followed by the wireless remote, which has been used four times, and applications where the body is used as an input device (e.g., Mircosoft Xbox Kinect). Other publications use treadmills (n=2), green screens, classic controllers, hand-motion trackers, driving simulators, and touch screens. (n=19) That makes choosing the suitable controller in line with the user’s interaction needs in the environment is essential. This selection ensures users comfortable interaction and navigation within the digital realm and improves comfort and the feeling of immersion.
3.3.3. Reproduction Fidelity
The Reproduction Fidelity (RP), as proposed by Milgram’s taxonomy [16], distinguishes certain levels of quality of how virtual entities are modelled and rendered within the VR and AR environment. Minimalist graphic and sound environments score low (1), and most advanced real-time realistic audio and video productions score high (6). Most applications feature a mediocre quality in terms of Reproduction fidelity. Ten publications have an average rating of 3. Only 5 of 19 publications delivered a state-of-the-art audiovisual experience. Four of the 19 were ranked below average. The total results are displayed in Table 9.
3.3.4. Immersion Level
The Immersion Level is essential to the application’s acceptance and effect. A combination of Extend of Presence (EP) and Reproduction Fidelity (RP) visualizes the publication’s location on the grid.
The combination of Extent of Presence (EP) and Reproduction Fidelity (RP) influences the combined Immersion Level of an AR/VR application. The Immersion Level is a key factor in how convincing the technology is for users. It reflects how much a person feels like they are part of the virtual world.
In Figure 8, you can see how the Immersion Level is mapped out, with RP on the x-axis and EP on the y-axis, ranging from 1 to 6. The visualization shows where different studies fall on the scale of immersion, with those positioned towards the upper right corner being studies that demonstrate high levels of both presence and fidelity.
In short, achieving a high level of immersion is all about getting the right mix of delivery methods, control systems, and how the environment is reproduced.
3.3.5. Autonomy and Guidance
The Autonomy and Guidance section answers whether supervision is needed during an application. Ideally, a patient could use the application without help and oversight, resulting in redacted care and treatment costs. The benefit of supervised solutions is that immediate assistance can be given to guide the patient to a secure and ideal applied performance of the exercise. Progress and feedback on inventions and applications can be provided in real-time. Furthermore, the patient might benefit from social interaction with the supervisor. The autonomic approach improves skills of independence and interaction without constant monitoring and feedback. When an application is used, a patient gains flexibility in the conduction, timing, and intensity levels.
Table 10.
Number of Publications by Supervision Status
| Supervision Status | Publications |
|---|---|
| Supervised | 16 |
| Not Supervised | 3 |
The majority of reviewed publications use a supervision approach. Only three publications (n=19) used autonomous interaction with the patient.
Two of the three publications are conducted by Anderson-Hanley et al. and feature a 2D cycling simulator that can also be used at home, see [19,20]. The third unsupervised application from van der Kolk et al. also features a cycling simulator called Cybercycle, which can be ridden autonomously [21].
4. Discussion
This systematic review explored VR and AR technologies as new intervention methods for neurodegenerative diseases.
4.1. Principal Findings
The publication timeline suggests that during the COVID-19 outbreak, research in VR, AR, and neurodegenerative disease slowed down drastically but picked up in recent years. This can be explained by the difficulty of conducting a clinical trial under those circumstances. There were no publications in the field in 2023, and it will be interesting to follow recent trends and publications for 2024. Most publications were conducted by research teams in the United States and Greece, but the sample size is too small to create further conclusions. The most researched conditions were dementia and MCI, whereas MCI can be seen as a general term for a spectrum of conditions. There were some instances of specialization for Parkinson’s and Alzheimer’s in the data, but they are rare. The number of randomized clinical trials was higher than that of Pilot and Feasibility studies. This suggests that this area of research is slowly maturing into an appliance. The number of participants in the clinical trials, including the control groups, averaged 23 subjects. This size is not very large to create reliable evidence, but it is a step in the right direction. There were almost no reports of Simulator Sickness. Only five of 19 publications contained information on Simulator Sickness, and none reported severe problems. Due to the complexity of VR and AR Settings and state-of-the-art technology, ease of use is often not effortless. There is a clear tendency towards supervised interventions. While the field is still young, this will become easier to handle with advanced technology, and we might see a trend towards unsupervised applications.
The results for immersion of a patient in the application were very average. Utilizing the MR continuum by Milgram et al. [16], the results showed that only a handful of applications could reach the upper right sector, creating a convincing immersion for the patient. Fixing this could directly result in immediate better results for the patient’s quality of life and also help to improve testing scores.
4.2. Strength and Limitations
Better information was extracted through the manual screening process and application analysis, in contrast to text mining approaches and the sole analysis of meta-data. Through the manual analysis and screening process, there is an improbable chance of individual bias of the analyzing author. However, it also highlights the demand for a meticulous review process, possibly with multiple reviewers checking, to lessen the chance of personal bias and understand a complete picture of the applications in use.
4.3. Conclusion
This text provides a perspective on the last 12 years of research on the cross-section of Cognitive Impairment and VR and AR Games used as treatments. Using VR and AR Games to treat patients with cognitive impairment is beneficial. However, the evidence is still fragile, and it is necessary to improve the engineering side of the applications and conduct more trials to gain a better insight into how and if said application can work. With more powerful hardware and software development, VR and AR technology will integrate better into existing treatments and workflows, creating opportunities for patients, doctors, and healthcare professionals to increase the quality of life for all involved.
Author Contributions
Conceptualization, M.E. and G.H.; methodology, M.E. and G.H.; software, M.E.; validation, M.E., G.H. and J.E.; formal analysis, M.E.; investigation, M.E. and T.O.; resources, M.E., T.O., J.E.; data curation, M.E.; writing—original draft preparation, M.E.; writing—review and editing, M.E., T.O. J.E. and G.H.; visualization, M.E.; supervision, T.O., J.E. and G.H.; project administration, G.H.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding
Institutional Review Board Statement
Not applicable
Informed Consent Statement
Not applicable
Conflicts of Interest
The authors declare no conflicts of interest
Abbreviations
The following abbreviations are used in this manuscript:
| API | Application Programming Interface |
| AR | Augmented Reality |
| EP | Extent of Presence |
| HMD | Head-Mounted Display |
| ICD | International Classification of Diseases |
| MCI | Mild Cognitive Impairment |
| MeSH | Medical Subject Headings |
| OSF | Open Science Framework |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| RCT | Randomized Clinical Trial |
| RP | Reproduction Fidelity |
| VR | Virtual Reality |
Appendix A. Table of included publications
Table A1.
Table of the included trials, containing the number of subjects, year of publication, sorted by number of included subjects.
Table A1.
Table of the included trials, containing the number of subjects, year of publication, sorted by number of included subjects.
| Publication Title | Subjects | Year |
|---|---|---|
| Effectiveness of home-based and remotely supervised aerobic exercise in Parkinson’s disease: a double-blind, randomised controlled trial. [21] | 125 | 2019 |
| Exergaming as a Physical Exercise Strategy Reduces Frailty in People With Dementia: A Randomized Controlled Trial. [22] | 115 | 2019 |
| The Aerobic and Cognitive Exercise Study (ACES) for Community-Dwelling Older Adults With or At-Risk for Mild Cognitive Impairment (MCI): Neuropsychological, Neurobiological and Neuroimaging Outcomes of a Randomized Clinical Trial. [20] | 111 | 2018 |
| Exergaming and older adult cognition: a cluster randomized clinical trial.[17] | 102 | 2012 |
| A Comparison of Traditional and Serious Game-Based Digital Markers of Cognition in Older Adults with Mild Cognitive Impairment and Healthy Controls. [23] | 76 | 2021 |
| The Effectiveness of a Virtual Reality-Based Intervention on Cognitive Functions in Older Adults with Mild Cognitive Impairment: A Single-Blind, Randomized Controlled Trial. [24] | 60 | 2020 |
| The Effectiveness of a Virtual Reality-Based Tai Chi Exercise on Cognitive and Physical Function in Older Adults with Cognitive Impairment. [25] | 60 | 2018 |
| Immersive Virtual Reality-Based Cognitive Intervention for the Improvement of Cognitive Function, Depression, and Perceived Stress in Older Adults With Mild Cognitive Impairment and Mild Dementia: Pilot Pre-Post Study. [18] | 31 | 2022 |
| Effects of virtual reality-based cognitive training in older adults living without and with mild dementia: a pretest-posttest design pilot study. [26] | 27 | 2019 |
| The Long-term Effects of Immersive Virtual Reality Reminiscence in People With Dementia: Longitudinal Observational Study. [27] | 20 | 2022 |
| A Virtual Reality App for Physical and Cognitive Training of Older People With Mild Cognitive Impairment: Mixed Methods Feasibility Study. [28] | 20 | 2021 |
| 2D Virtual Reality-Based Exercise Improves Spatial Navigation in Institutionalized Non-robust Older Persons: A Preliminary Data Report of a Single-Blind, Randomized, and Controlled Study. [29] | 14 | 2021 |
| Effect of Spatial Disorientation in a Virtual Environment on Gait and Vital Features in Patients with Dementia: Pilot Single-Blind Randomized Control Trial. [19] | 13 | 2020 |
| Does Practicing with a Virtual Reality Driving Simulator Improve Spatial Cognition in Older Adults? A Pilot Study. [30] | 11 | 2020 |
| Cognitive Training Using Fully Immersive, Enriched Environment Virtual Reality for Patients With Mild Cognitive Impairment and Mild Dementia: Feasibility and Usability Study. [31] | 11 | 2020 |
| A pilot study and brief overview of rehabilitation via virtual environment in patients suffering from dementia. [32] | 10 | 2018 |
| Feasibility study of the BrightBrainer™ integrative cognitive rehabilitation system for elderly with dementia. [33] | 10 | 2015 |
| Tele-Rehabilitation with Virtual Reality: A Case Report on the Simultaneous, Remote Training of Two Patients with Parkinson Disease. [34] | 2 | 2021 |
| Two-week virtual reality training for dementia: Single case feasibility study. [35] | 1 | 2014 |
Appendix B. Initial Search Query
((dementia) OR (alzheimers disease)) AND ((video games) OR (computer games) OR (exergames) OR (serious games))AND ((augmented reality) OR (virtual reality))
Appendix C. Extended Search Query
(" dementia "[ MeSH Terms] OR " dementia "[ All Fields] OR " dementias "[ All Fields] OR " dementia s"[ All Fields] OR (" alzheimer disease "[ MeSH Terms] OR (" alzheimer "[ All Fields] AND " disease "[ All Fields ]) OR (" alzheimer disease "[ All Fields] OR (" alzheimer s"[ All Fields] AND " disease "[ All Fields ]) OR " alzheimer s disease "[ All Fields ])) AND (" video games "[ MeSH Terms] OR (" video "[ All Fields] AND " games "[ All Fields ]) OR " video games "[ All Fields] OR (" video games "[ MeSH Terms] OR (" video "[ All Fields] AND " games "[ All Fields ]) OR " video games "[ All Fields] OR (" computer "[ All Fields] AND " games "[ All Fields ]) OR " computer games "[ All Fields]) OR (" exergamers "[ All Fields] OR " exergaming "[ MeSH Terms] OR " exergaming "[ All Fields] OR " exergame "[ All Fields] OR " exergames "[ All Fields ]))
Appendix D. Exclusion Terms
1 stroke 2 cancer 3 tumor 4 glaucoma 5 bipolar 6 corona 7 covid 8 panic disorder 9 athlete 10 autism 11 eating disorder 12 adhd 13 schizophrenia 14 chronic pain 15 multiple sclerosis 16 traumatic brain injury 17 spinal cord 18 anesthesia 19 robot 20 robotics 21 posttraumatic 22 screening 23 detecting 24 amblyopia 25 alcohol 26 small vessel disease 27 sex 28 cirrho 29 spectroscopy 30 health care provider 31 schizophrenia 32 remission 33 intensive care 34 drug abusers 35 preoperative 36 heart failure 37 phantom limb pain 38 psychosis 39 loss of control eating 40 sway disturbance 41 spastic 42 falls 43 child 44 biochemical 45 borderline 46 phantom 47 hand 48 limb 49 ptsd 50 nanocluster
References
- Crimmins, E.M.; Kim, J.K.; Langa, K.M.; Weir, D.R. Assessment of Cognition Using Surveys and Neuropsychological Assessment: The Health and Retirement Study and the Aging, Demographics, and Memory Study. The Journals of Gerontology Series B: Psychological Sciences and Social Sciences 2011, 66B, i162–i171. [Google Scholar] [CrossRef]
- Park, M.J.; Kim, D.J.; Lee, U.; Na, E.J.; Jeon, H.J. A Literature Overview of Virtual Reality (VR) in Treatment of Psychiatric Disorders: Recent Advances and Limitations. Frontiers in Psychiatry 2019, 10, 505. [Google Scholar] [CrossRef]
- DGPPN – DGN., Ed. S3-Leitlinie Demenzen; Springer Berlin Heidelberg: Berlin, Heidelberg, 2017. [CrossRef]
- Roberts, R.; Knopman, D.S. Classification and Epidemiology of MCI. Clinics in Geriatric Medicine 2013, 29, 753–772. [Google Scholar] [CrossRef]
- World Health Organization. Risk reduction of cognitive decline and dementia: WHO guidelines; World Health Organization: Geneva, 2019. [Google Scholar]
- Kim, C.K.; Lee, Y.R.; Ong, L.; Gold, M.; Kalali, A.; Sarkar, J. Alzheimer’s Disease: Key Insights from Two Decades of Clinical Trial Failures. Journal of Alzheimer’s Disease 2022, 87, 83–100. [Google Scholar] [CrossRef]
- Meyer, C.; O’Keefe, F. Non-pharmacological interventions for people with dementia: A review of reviews. Dementia 2020, 19, 1927–1954. [Google Scholar] [CrossRef]
- Rodrigo-Yanguas, M.; González-Tardón, C.; Bella-Fernández, M.; Blasco-Fontecilla, H. Serious Video Games: Angels or Demons in Patients With Attention-Deficit Hyperactivity Disorder? A Quasi-Systematic Review. Frontiers in Psychiatry 2022, 13, 798480. [Google Scholar] [CrossRef]
- Pallavicini, F.; Pepe, A.; Mantovani, F. Commercial Off-The-Shelf Video Games for Reducing Stress and Anxiety: Systematic Review. JMIR Mental Health 2021, 8, e28150. [Google Scholar] [CrossRef]
- Bogost, I. The rhetoric of exergaming. Proceedings of the Digital Arts and Cultures (DAC) 2005, 51. [Google Scholar]
- Muñoz-Saavedra, L.; Miró-Amarante, L.; Domínguez-Morales, M. Augmented and Virtual Reality Evolution and Future Tendency. Applied Sciences 2020, 10, 322. [Google Scholar] [CrossRef]
- Flynn, A.; Healy, D.; Barry, M.; Brennan, A.; Redfern, S.; Houghton, C.; Casey, D. Key Stakeholders’ Experiences and Perceptions of Virtual Reality for Older Adults Living With Dementia: Systematic Review and Thematic Synthesis. JMIR serious games 2022, 10, e37228. [Google Scholar] [CrossRef]
- Yen, H.Y.; Chiu, H.L. Virtual Reality Exergames for Improving Older Adults’ Cognition and Depression: A Systematic Review and Meta-Analysis of Randomized Control Trials. Journal of the American Medical Directors Association 2021, 22, 995–1002. [Google Scholar] [CrossRef]
- Gates, N.J.; Rutjes, A.W.; Di Nisio, M.; Karim, S.; Chong, L.Y.; March, E.; Martínez, G.; Vernooij, R.W. Computerised cognitive training for 12 or more weeks for maintaining cognitive function in cognitively healthy people in late life. The Cochrane Database of Systematic Reviews 2020, 2, CD012277. [Google Scholar] [CrossRef]
- PubMed Database.
- Milgram, P.; Takemura, H.; Utsumi, A.; Kishino, F. Augmented reality: a class of displays on the reality-virtuality continuum; , 1995; pp. 282–292. [CrossRef]
- Anderson-Hanley, C.; Arciero, P.J.; Brickman, A.M.; Nimon, J.P.; Okuma, N.; Westen, S.C.; Merz, M.E.; Pence, B.D.; Woods, J.A.; Kramer, A.F.; Zimmerman, E.A. Exergaming and older adult cognition: a cluster randomized clinical trial. American Journal of Preventive Medicine 2012, 42, 109–119. [Google Scholar] [CrossRef]
- Zhu, K.; Zhang, Q.; He, B.; Huang, M.; Lin, R.; Li, H. Immersive Virtual Reality-Based Cognitive Intervention for the Improvement of Cognitive Function, Depression, and Perceived Stress in Older Adults With Mild Cognitive Impairment and Mild Dementia: Pilot Pre-Post Study. JMIR serious games 2022, 10, e32117. [Google Scholar] [CrossRef]
- Amaefule, C.O.; Lüdtke, S.; Kirste, T.; Teipel, S.J. Effect of Spatial Disorientation in a Virtual Environment on Gait and Vital Features in Patients with Dementia: Pilot Single-Blind Randomized Control Trial. JMIR serious games 2020, 8, e18455. [Google Scholar] [CrossRef]
- Anderson-Hanley, C.; Barcelos, N.M.; Zimmerman, E.A.; Gillen, R.W.; Dunnam, M.; Cohen, B.D.; Yerokhin, V.; Miller, K.E.; Hayes, D.J.; Arciero, P.J.; Maloney, M.; Kramer, A.F. The Aerobic and Cognitive Exercise Study (ACES) for Community-Dwelling Older Adults With or At-Risk for Mild Cognitive Impairment (MCI): Neuropsychological, Neurobiological and Neuroimaging Outcomes of a Randomized Clinical Trial. Frontiers in Aging Neuroscience 2018, 10, 76. [Google Scholar] [CrossRef]
- van der Kolk, N.M.; de Vries, N.M.; Kessels, R.P.C.; Joosten, H.; Zwinderman, A.H.; Post, B.; Bloem, B.R. Effectiveness of home-based and remotely supervised aerobic exercise in Parkinson’s disease: a double-blind, randomised controlled trial. The Lancet. Neurology 2019, 18, 998–1008. [Google Scholar] [CrossRef]
- Karssemeijer, E.G.A.; Bossers, W.J.R.; Aaronson, J.A.; Sanders, L.M.J.; Kessels, R.P.C.; Olde Rikkert, M.G.M. Exergaming as a Physical Exercise Strategy Reduces Frailty in People With Dementia: A Randomized Controlled Trial. Journal of the American Medical Directors Association 2019, 20, 1502–1508. [Google Scholar] [CrossRef]
- Iliadou, P.; Paliokas, I.; Zygouris, S.; Lazarou, E.; Votis, K.; Tzovaras, D.; Tsolaki, M. A Comparison of Traditional and Serious Game-Based Digital Markers of Cognition in Older Adults with Mild Cognitive Impairment and Healthy Controls. Journal of Alzheimer’s disease: JAD 2021, 79, 1747–1759. [Google Scholar] [CrossRef]
- Torpil, B.; Şahin, S.; Pekçetin, S.; Uyanık, M. The Effectiveness of a Virtual Reality-Based Intervention on Cognitive Functions in Older Adults with Mild Cognitive Impairment: A Single-Blind, Randomized Controlled Trial. Games for Health Journal 2021, 10, 109–114. [Google Scholar] [CrossRef]
- Hsieh, C.C.; Lin, P.S.; Hsu, W.C.; Wang, J.S.; Huang, Y.C.; Lim, A.Y.; Hsu, Y.C. The Effectiveness of a Virtual Reality-Based Tai Chi Exercise on Cognitive and Physical Function in Older Adults with Cognitive Impairment. Dementia and Geriatric Cognitive Disorders 2018, 46, 358–370. [Google Scholar] [CrossRef]
- Zając-Lamparska, L.; Wiłkość-Dębczyńska, M.; Wojciechowski, A.; Podhorecka, M.; Polak-Szabela, A.; Warchol, L.; Kędziora-Kornatowska, K.; Araszkiewicz, A.; Izdebski, P. Effects of virtual reality-based cognitive training in older adults living without and with mild dementia: a pretest-posttest design pilot study. BMC research notes 2019, 12, 776. [Google Scholar] [CrossRef]
- Huang, L.C.; Yang, Y.H. The Long-term Effects of Immersive Virtual Reality Reminiscence in People With Dementia: Longitudinal Observational Study. JMIR serious games 2022, 10, e36720. [Google Scholar] [CrossRef]
- Hassandra, M.; Galanis, E.; Hatzigeorgiadis, A.; Goudas, M.; Mouzakidis, C.; Karathanasi, E.M.; Petridou, N.; Tsolaki, M.; Zikas, P.; Evangelou, G.; Papagiannakis, G.; Bellis, G.; Kokkotis, C.; Panagiotopoulos, S.R.; Giakas, G.; Theodorakis, Y. A Virtual Reality App for Physical and Cognitive Training of Older People With Mild Cognitive Impairment: Mixed Methods Feasibility Study. JMIR serious games 2021, 9, e24170. [Google Scholar] [CrossRef]
- Oliveira, L.M.; Evangelista E Souza, E.H.; Alves, M.R.; Carneiro, L.S.F.; Fagundes, D.F.; de Paula, A.M.B.; Engedal, K.; Nascimento, O.J.M.; Monteiro-Junior, R.S. 2D Virtual Reality-Based Exercise Improves Spatial Navigation in Institutionalized Non-robust Older Persons: A Preliminary Data Report of a Single-Blind, Randomized, and Controlled Study. Frontiers in Neurology 2020, 11, 609988. [Google Scholar] [CrossRef]
- Masoumzadeh, S.; Moussavi, Z. Does Practicing with a Virtual Reality Driving Simulator Improve Spatial Cognition in Older Adults? A Pilot Study. Neuroscience Insights 2020, 15, 2633105520967930. [Google Scholar] [CrossRef]
- Yun, S.J.; Kang, M.G.; Yang, D.; Choi, Y.; Kim, H.; Oh, B.M.; Seo, H.G. Cognitive Training Using Fully Immersive, Enriched Environment Virtual Reality for Patients With Mild Cognitive Impairment and Mild Dementia: Feasibility and Usability Study. JMIR serious games 2020, 8, e18127. [Google Scholar] [CrossRef]
- Fasilis, T.; Patrikelis, P.; Siatouni, A.; Alexoudi, A.; Veretzioti, A.; Zachou, L.; Gatzonis, S.S. A pilot study and brief overview of rehabilitation via virtual environment in patients suffering from dementia. Psychiatrike = Psychiatriki 2018, 29, 42–51. [Google Scholar] [CrossRef]
- Burdea, G.; Polistico, K.; Krishnamoorthy, A.; House, G.; Rethage, D.; Hundal, J.; Damiani, F.; Pollack, S. Feasibility study of the BrightBrainer™ integrative cognitive rehabilitation system for elderly with dementia. Disability and Rehabilitation. Assistive Technology 2015, 10, 421–432. [Google Scholar] [CrossRef]
- Cornejo Thumm, P.; Giladi, N.; Hausdorff, J.M.; Mirelman, A. Tele-Rehabilitation with Virtual Reality: A Case Report on the Simultaneous, Remote Training of Two Patients with Parkinson Disease. American Journal of Physical Medicine & Rehabilitation 2021, 100, 435–438. [Google Scholar] [CrossRef]
- McEwen, D.; Taillon-Hobson, A.; Bilodeau, M.; Sveistrup, H.; Finestone, H. Two-week virtual reality training for dementia: Single case feasibility study. Journal of Rehabilitation Research and Development 2014, 51, 1069–1076. [Google Scholar] [CrossRef]
Figure 1.
Exclusion Workflow Visual representation of conducted stages, visualizing the individual steps and numbers of excluded publications in each stage.
Figure 1.
Exclusion Workflow Visual representation of conducted stages, visualizing the individual steps and numbers of excluded publications in each stage.
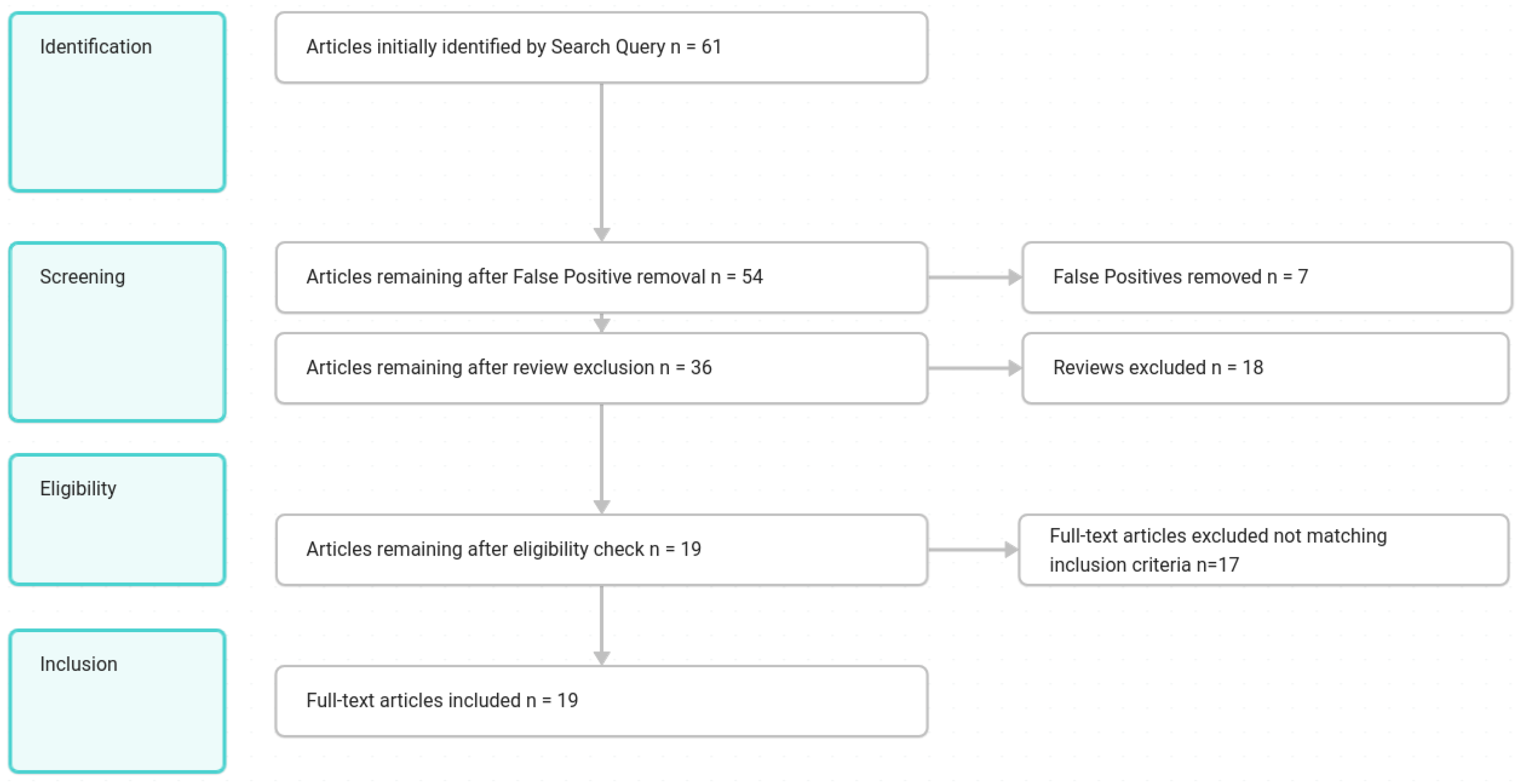
Figure 2.
Reality-Virtuality (RV Continuum) Figure from Milgram et al. [16] detailing the domain of Mixed Reality. The left represents our real environment, and the right side represents a fully virtual environment. In between is a spectrum of Virtual and Augmented Reality.
Figure 2.
Reality-Virtuality (RV Continuum) Figure from Milgram et al. [16] detailing the domain of Mixed Reality. The left represents our real environment, and the right side represents a fully virtual environment. In between is a spectrum of Virtual and Augmented Reality.
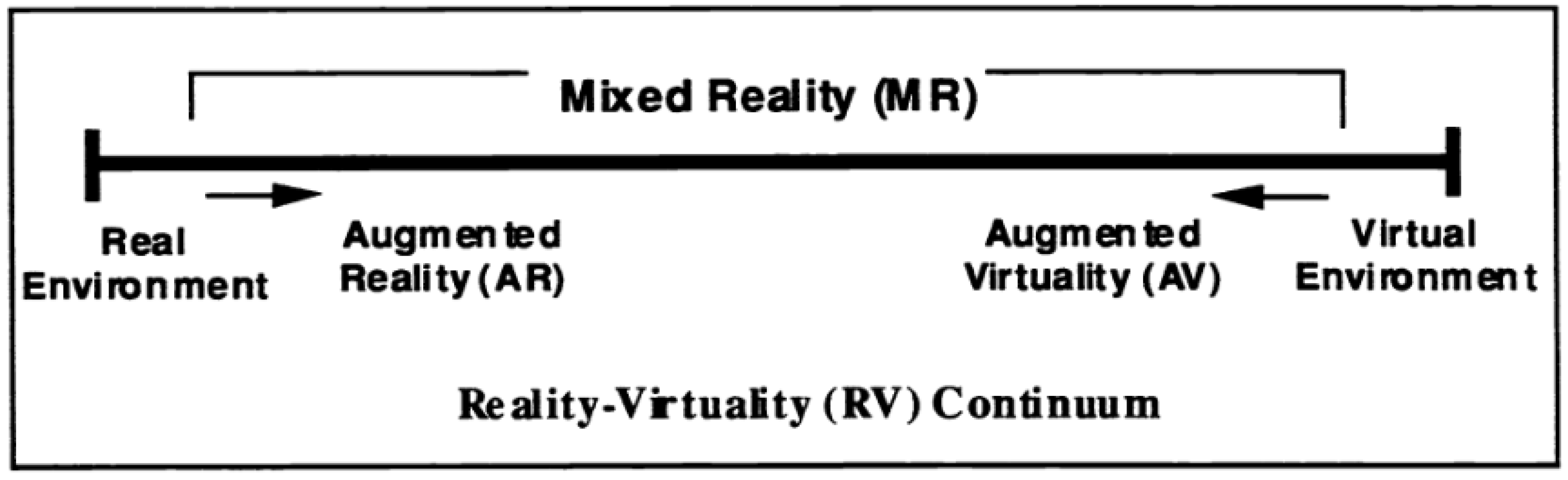
Figure 3.
Timeline of Publications The bars show the number of publications for the specific year. The years range from 2012 to 2023. There are clear gaps visible from 2015 to 2018 and from 2022 onward.
Figure 3.
Timeline of Publications The bars show the number of publications for the specific year. The years range from 2012 to 2023. There are clear gaps visible from 2015 to 2018 and from 2022 onward.
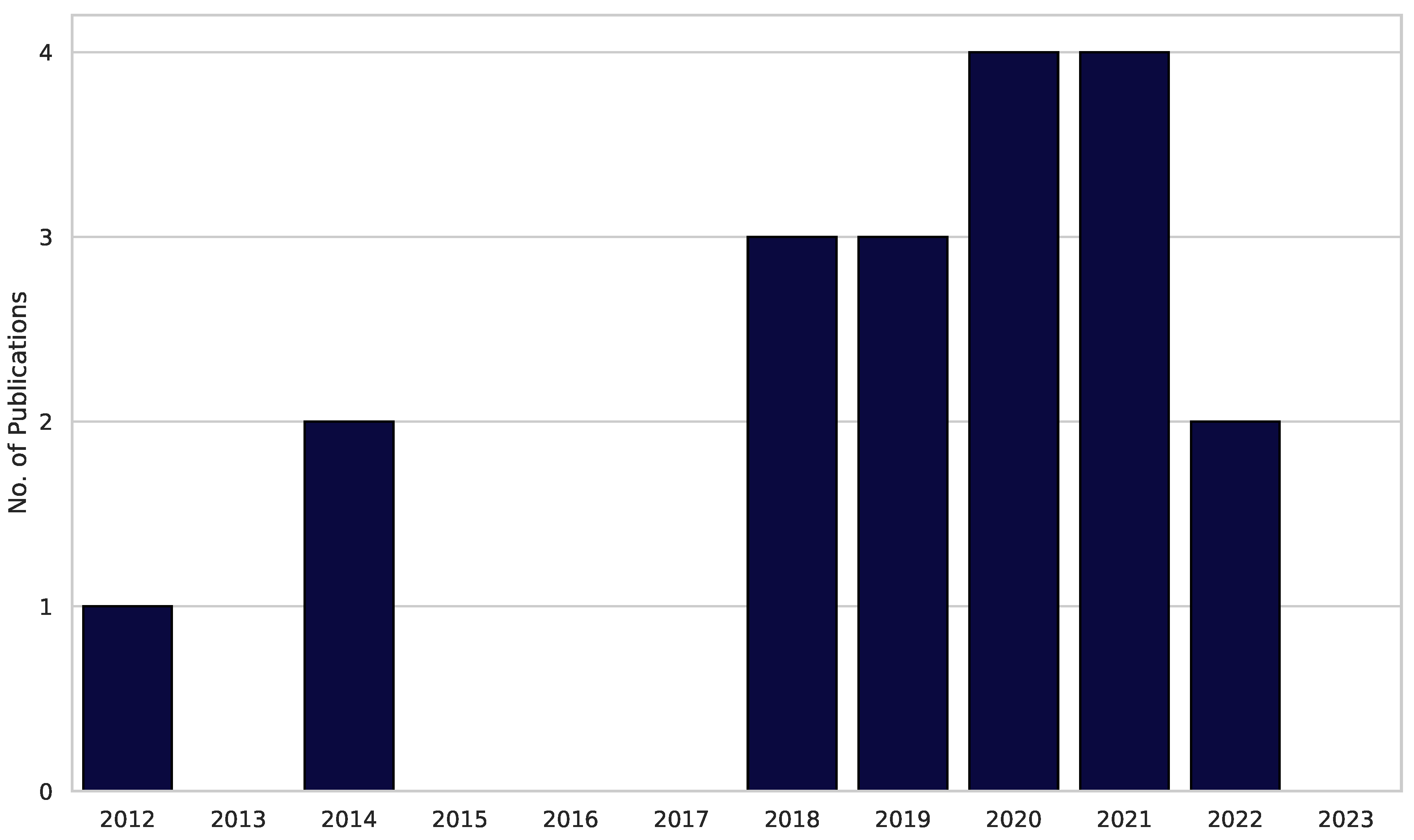
Figure 4.
Participation in Clinical Trials The three dotted vertical lines represent lower quartile (11 subjects), median (23,5 subjects) and upper quartile (72 subjects). The grey dots represent the individual trial. The dark blue violin plot visualizes the distribution of overall subjects (n = 18).
Figure 4.
Participation in Clinical Trials The three dotted vertical lines represent lower quartile (11 subjects), median (23,5 subjects) and upper quartile (72 subjects). The grey dots represent the individual trial. The dark blue violin plot visualizes the distribution of overall subjects (n = 18).
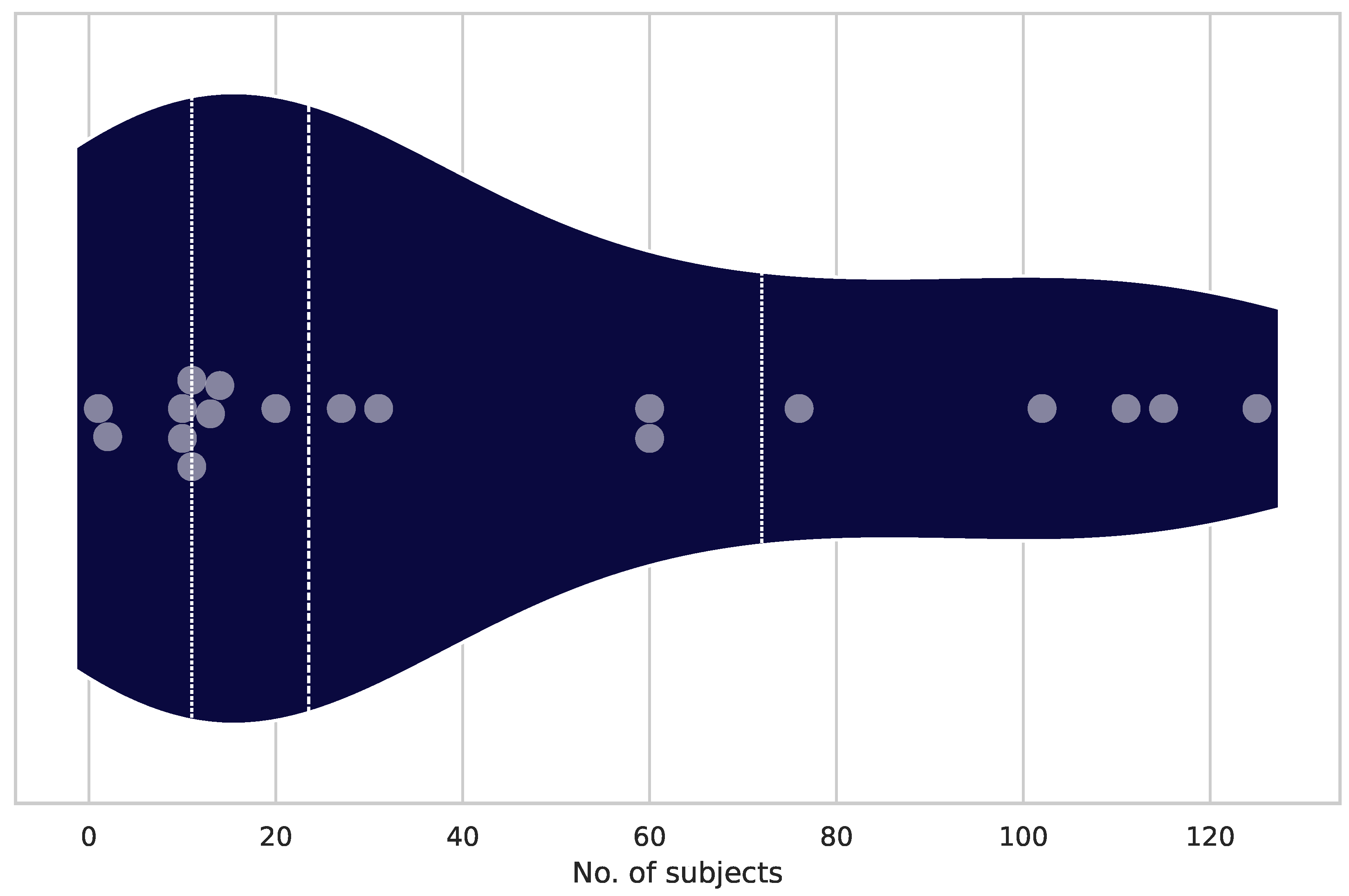
Figure 8.
Immersion Level Reproduction Fidelity (RP) is set on the x-axis, with a range from 1 to 6 as an indicator for graphical and auditive modelling quality. The Extend of Presence on the y-axis represents user engagement and immersion in the VR and AR worlds, ranging from 1 to 6 (n=19).
Figure 8.
Immersion Level Reproduction Fidelity (RP) is set on the x-axis, with a range from 1 to 6 as an indicator for graphical and auditive modelling quality. The Extend of Presence on the y-axis represents user engagement and immersion in the VR and AR worlds, ranging from 1 to 6 (n=19).
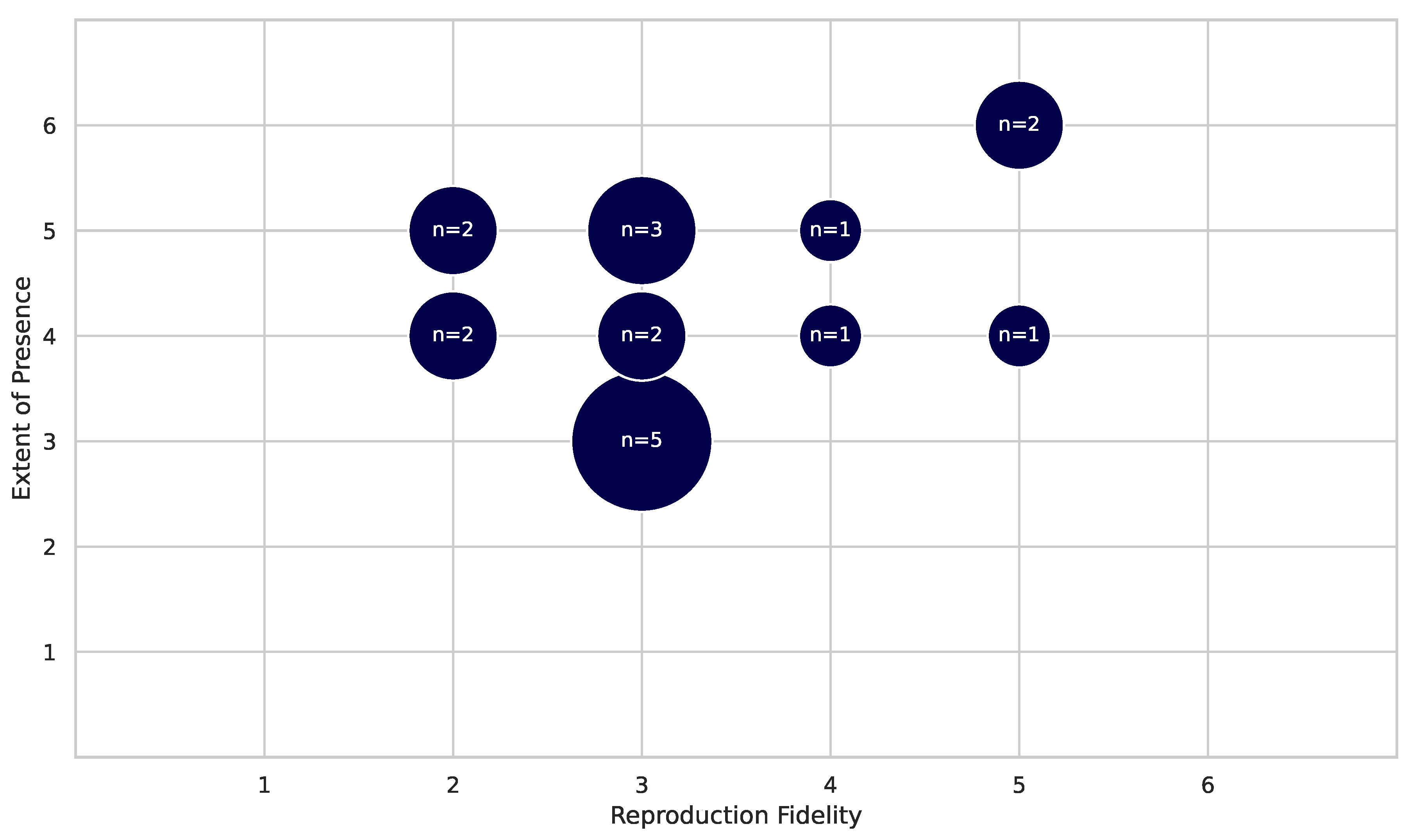
Table 5.
Number of Publications by Country (Sorted by Publications and Country)
| Country | Publications | Country | Publications | Country | Publications |
|---|---|---|---|---|---|
| Greece | 3 | Taiwan | 2 | Israel | 1 |
| USA | 3 | Brazil | 1 | Korea | 1 |
| Canada | 2 | China | 1 | Poland | 1 |
| Netherlands | 2 | Germany | 1 | Turkey | 1 |
Table 9.
Aggregated Reproduction Fidelity (RP) Scores
| RP Score | Number of Publications |
|---|---|
| 1 | 0 |
| 2 | 5 |
| 3 | 9 |
| 4 | 2 |
| 5 | 3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



