
Submitted:
01 October 2024
Posted:
02 October 2024
You are already at the latest version
Abstract
Identifying effective and accessible interventions for family caregivers of persons with dementia (PWD) is crucial as the prevalence of dementia increases in Asia. This study investigated the efficacy of a telephone-intervention on reduction of caregiver burden, depressive and anxiety symptoms among family caregivers (FC) of PWD in Malaysia. A single-blinded randomized controlled trial was carried out with 121 FCs of PWD selected from memory or psychiatry clinics in three tertiary hospitals in Malaysia who were randomly allocated into intervention or control group. The intervention group received the psychoeducational intervention delivered by a healthcare staff via telephone for 10 sessions over 12 weeks. The outcome of the intervention was measured by the Malay version of the Zarit Burden Interview and the Hospital Anxiety and Depression Scale at baseline and post-intervention. Intention-to-treat analysis shows that caregiver burden, anxiety symptoms, and psychological distress among FCs in the intervention group decreased by 7.57 units (p<0.001), 2.46 units (p<0.001) and 2.98 units (p=0.011) respectively at post-intervention, compared to the differences from baseline to post-intervention in the control group. Policies aimed at integrating the telephone-intervention into memory/psychiatry clinics in Malaysia may help FCs of PWD to reduce their caregiver burden and stress while caring for a family member with dementia.
Keywords:
Telephone-intervention
; Family caregivers
; Persons with dementia
; Burden
; Anxiety and depression symptoms
1. Introduction
Dementia is a worldwide healthcare challenge encompassing various disorders and conditions affecting cognitive functions particularly in persons aged 65 years and older, posing a significant burden on the person, family and healthcare systems [1]. World Health Organization (WHO) reported that globally more than 55 million people have dementia, with projections of nearly 78 million by 2030 and 139 million in 2050 [2]. Almost 9.9 million new cases of dementia are developed annually, one in every three seconds [3]. Approximately 60% of persons with dementia (PWD) live in low- and middle-income countries (LMIC), which includes Malaysia also.
As longevity increases in many Asian countries due to advancement in healthcare and living standard, individuals are now experiencing longer lifespan compared to previous generations. This development is associated with a higher incidence of dementia [4]. According to the United Nations Development Programme (UNDP) [5], the Asia-Pacific region is one of the fastest aging regions in the world. Recently, the Department of Statistics, Malaysia (DoSM) [6] indicates a rise in the percentage of the population aged 65 years and above, reaching 7.2% in 2022. In 2040, it is estimated that Malaysia’s demographic landscape will have almost equal distribution between young (18.6%) and older population (14.5%) [6].
Subsequently, in Asian countries such as China, Hong Kong, Taiwan and India the prevalence of dementia was reported ranging from 4.2% to 7.4% [7,8,9] while in Malaysia it was 8.5% (almost 260,000 population) in 2018 [10,11]. Family caregivers (FC) often act as informal caregivers, assisting with daily tasks, managing medications, coordinating medical appointments, and advocating for the needs of the PWD [12]. The nature of these caregiving tasks can lead to social isolation, financial strains and disruptions to both personal and family routines, contributing to a higher level of burden [13,14]. Evidence shows that as the severity of dementia increases, the caregiver’s involvement in daily tasks such as bathing, dressing and feeding also increases, resulting in a greater caregiver burden [15,16,17,18]. Similarly, dependency of PWD on daily life activities was found to increase caregiver burden in Malaysia [19].
In addition to the burdens related to caregiver for PWD, FCs also experience depression and anxiety symptoms, with prevalence rates of 14% to 31% and 29% to 32%, respectively [20,21,22,23]. A prospective cohort study by Joling et al. [24] identified an incidence of 37% and 55% for major depressive disorder and anxiety disorder after 24 months of caregiving, and 60% for comorbid depressive and anxiety disorder. In Malaysia, a study found that 30.5% and 20.7% of caregivers to PWD experienced depressive and anxiety symptoms where the majority of them were women [25]. Due to traditional norms, women are often assigned caregiving roles resulting in higher rates of mental health issues compared to male caregivers [26,27].
Cultural and social norms may influence burden and psychological distress among FCs of PWD [28,29]. For instance, in Asian countries, the belief in filial piety is deeply ingrained and widely upheld within the community, promoting positive moral values [29]. Traditionally, a significant proportion of older adults are cared for by their family members to avoid being seen as ungrateful for the sacrifices made by their elders [28]. Thus, it is important for the FCs to receive education about relevant diseases, prognosis, interventions, support groups and other community resources. This can help improve their well-being and enhance the quality of care they provide [30,31].
Interventions for FCs through face-to-face meetings whether in-person or in groups have been carried out in Western countries such as USA [32], Europe [33] and Spain [34] as well as in Asian countries such as Hong Kong [35], Korea [36] and Pakistan [37]. These interventions aim to provide personalized feedback and guidance on coping strategies for FCs. However, some caregivers were hesitant to share sensitive information due to privacy concerns particularly during group discussions [33] and also reported facing challenges relating to transportation and financial constraints [38]. Additionally, internet-based interventions [39,40] and tele-rehabilitation through mobile application [41] have also been implemented. However, the effectiveness of these approaches may be hindered by issues related to sustainability and technical problems, such as poor internet connectivity [42].
Telephone-based interventions have evolved to provide a broader caregiver community with access to support and resources [42,43,44,45]. Telephone-based psychoeducational intervention enables caregivers to increase their knowledge about dementia, develop problem-solving skills, and facilitate social support in a cost-effective manner [46]. Although research on the effectiveness of telephone-delivered intervention in LMIC in Asia is limited [47], existing literature suggests that the individual tailored telephone-intervention can produce favourable outcomes and could be recommended for caregivers of PWD [42,43,44,45].
Like in many Asian countries, FC’s burden and mental health are critical issues in Malaysia [25,48,49]. While empirical evidence of the interventions particularly counselling, in-person and group support have been carried out at the healthcare centre to support the FCs, the demands of caregiving to PWD at home and the cost constraint makes the intervention supports more challenging. Thus, this study aims to address the gaps by evaluating the effect of telephone-delivered psychoeducational interventions to reduce burden, psychological distress and anxiety and depressive symptoms among FCs of PWD in Malaysia.
2. Materials and Methods
This was a parallel group, single-blinded randomized control trial (RCT), where participants were recruited from the registers of PWD at the psychiatry clinic in Sultan Ahmad Shah Medical Centre (SASMEC), Kuantan; psychiatry, memory and neuromedical clinics in Hospital Tengku Ampuan Afzan (HTAA), Kuantan; and geriatric clinic in Universiti Kebangsaan Malaysia Medical Centre (UKMMC), Kuala Lumpur in East and West Malaysia. Research assistants (RA) selected the FCs from the registers of PWD in the hospitals and assessed their eligibility via telephone. The study participants were recruited who met the inclusion criteria includes FCs of clinically diagnosed PWD of any stage (mild, moderate or severe), aged >18 years living at home with the PWD and caring for at least 4 hours/day for >6 months, able to read and understand Malay, being the primary caregiver of a PWD (if there is more than one caregiver), and had access to a telephone. Participants were excluded from the study if they reported any major acute medical illness or had hearing problems, unable to communicate in Malay, or did not complete the entire questionnaire for data collection.
The sample size was calculated using the OpenEpi application. According to Tremont et al., the improvement rate in burden and depressive symptoms as a result of an intervention was 30% [45]. The calculated sample size with a significance level of 5% and power of 80% was 49, but rounded to 50 in each group. An estimated dropout of 20% gives the required sample size of 60 in each intervention and control group, totalling 120 FCs of PWD for the study. At the initial phase of the study, 380 participants were screened for eligibility. A total of 121 participants were included, of them 60 were assigned randomly in the intervention group and the rest in the control group using a computerized randomization program (Figure 1).
A four-block randomization was performed by an independent statistician who was not involved in the study. The randomization sequence was produced using computer-generated random numbers with a block of four. Each participant was assigned a unique ID number and placed in a sealed opaque envelope, which contained the participant’s treatment group (intervention or control). These envelopes were bundled in groups of four, corresponding to the block size used in the randomization sequence. These envelopes were subsequently sent to the head nurse of the research, who was solely responsible for opening and distributing them to other registered nurses (RN) and occupational therapists (OT) for the delivery of interventions as indicated by the unique ID code on the envelopes. Allocation concealment was maintained by concealing this allocation sequence from those who are involved with the study.
Participants assigned in the intervention group received the psychoeducational intervention delivered by a healthcare staff via telephone over 10 sessions in 12 weeks (Figure 1). Before the intervention the healthcare staff, consisting of five RNs and two OTs, attended a three-day online workshop on FC’s enrolment, psychoeducational intervention module and its implementation strategies. The training was provided by the researchers and clinicians from Karolinska Institutet focusing on active learning by encouraging questions and utilizing participant role-playing. Subsequently, a one-day follow-up training session for the healthcare staff providing the intervention was conducted in Malay to sharpen knowledge before delivering the intervention.
The intervention booklet inspired by the WHO’s iSupport training and support manual for carers of PWD [50] was posted to the caregivers allocated under intervention group by the head nurse once the baseline assessment was completed. The WHO recommends the iSupport program for caregivers of PWD across all the 194 member states. The iSupport program offers various learning opportunities, training modules, support groups [2], and access to web-based resources. The healthcare staff, trained on implementing the intervention, started the initial call, and subsequent follow-up calls were scheduled based on the accessibility and availability of both the healthcare staff and the caregivers. Each call lasted for around 30 minutes and each FC was assigned a specific RN or OT for the whole duration of the intervention. Every session provided by the healthcare staff was ended with a task for the next session. Participants noted the assigned tasks, tips and any issues in their caregiver booklet to discuss in the next session.
The participants completed the baseline survey from August 2022 to February 2023 on caregiver’s burden, psychological distress involving anxiety and depression symptoms through structured questionnaire administered by the trained RA via telephone. The trained RA who assessed the participants was blinded to the treatment group (whether intervention or control). However, blinding was not extended to the nurses responsible for delivering the intervention, nor to the statistician who had knowledge of which participant’s ID received the treatment. Each FC was informed about the research project, psychoeducational intervention, risks and benefits to participate in the study. Only those FCs who gave their voluntary consent was enrolled. In addition, participants in both control and intervention groups received usual care and information which was available at the hospitals or clinics. Post-intervention assessment was carried out at week 14 to assess the outcome measures including caregiver burden, and depressive and anxiety symptoms. Background variables in this study include socioeconomic characteristics such as family caregiver’s age, sex, education (primary, secondary or tertiary), occupation (employed employee, homemaker/unemployed, retired caregiver), monthly household income; caregiving information (length of caregiving, hours of caregiving per day, if the caregiving was shared by other family members, number of family members involved in shared caregiving, caregiver’s relationship with PWD, caregivers perceived social support (family, friends and significant others support); and PWD’s demographic information such as age, sex, and the ability to self-care. Caregivers perceived social support was assessed using validated Malay Version of Multidimensional Scale of Perceived Social Support (MSPSS) which consists of 12-items; family support (4-items), friends’ support (4-items) and significant others support (4-items), scored from 1(very strongly disagree) to 7 (very strongly agree). The total score is between 0 to 84, which higher score indicates higher social support [51]. The internal consistency of the caregiver’s social support for the whole scale and the three subscales was found to have a Cronbach’s alpha between 0.91 to 0.93.
The main end points for the caregivers of PWDs were changes in caregiver burden, psychological distress, anxiety and depressive symptoms between baseline and post-intervention assessment. The Validated Malay version of Zarit Burden Interview (ZBI) was used to measure caregivers’ burden which consists of 22 items, scored from 0 to 4 on each item [52]. The total score is between 0 to 88, where higher score indicates higher level of burden. The reliability and validity of the Malay version of ZBI (MZBI) was verified, whereby a score of 22 represented the optimum cut-off point for 70.8% sensitivity and 69.2% specificity [52]. The internal consistency of MZBI in the original study was assessed using Cronbach’s alpha, which yielded a good internal consistency of 0.90. In our study, the Cronbach’s alpha of MZBI was 0.92 at baseline and 0.93 at post-intervention. The validated Malay version of Hospital Anxiety and Depression Scale (HADS) was used to measure psychological distress [53] which consisted of 14 items, scored from 0 to 3 on each item. The HADS questionnaire consists of two subscales: anxiety (HADS-A) and depressive (HADS-D) symptoms. Each subscale comprises seven items with the total score between 0 to 21, where higher score indicates higher psychological distress, anxiety and depressive symptoms. The scale was developed as a respondent’s verbal response tool [53], and demonstrated good reliability with Cronbach’s alpha 0.88, 0.84, 0.78 at baseline and 0.88, 0.83, 0.82 at post-intervention for psychological distress, anxiety and depressive symptoms.
The data were analyzed using IBM SPSS Statistics version 26.0. Bivariate analyses, i.e., Chi-square or Fisher exact tests, independent t-test, and Mann Whitney U test were done to compare the participants’ baseline characteristics between intervention and control groups. Mixed ANOVA was used to examine the net gain effect of intervention on the outcome variables. Intention to treat (ITT) analysis using linear mixed model for repeated measure adjusted for all possible associated factors was conducted to evaluate the independent effect of the intervention on the outcome variables. Before conducting the ITT analysis, independent t-tests identified the possible baseline characteristics associated with outcome measures. A p-value of <0.05 was considered for statistical significance. An ITT analysis includes all randomized patients (N=121) regardless of subsequent withdrawal from the protocol [54].
The study was approved by the Malaysia Medical Research and Ethics Committee (NMRR ID-22-00137-BUY), IIUM Research and Ethics Committee (IREC 2022-007), Department of Psychiatry and Memory, Hospital Tengku Ampuan Afzan (HTAA) (00137-BUY (2)), Department of Psychiatry, Sultan Ahmad Shah Medical Centre (IIUM/413/013/14/11/2/IISR22-09), and Research Ethics Committee of Universiti Kebangsaan Malaysia (UKMPPI/11/8/JEP-2022-328). Caregivers provided informed consent after receiving comprehensive information about the study's purpose, procedures, risks, and benefits, with the assurance of voluntary participation and the right to withdraw from the study at any time without repercussions. The respondent’s identities were kept confidential, data were collected anonymously, and anonymity was maintained in publishing the data.
3. Results
3.1. Response Rate and Adherence to the Intervention
Among the 121 participants, 16 (13%) dropped out from the study of which 11 (18%) were from the intervention group and 5 (8%) from the control group (Figure 1). The reasons for drop out were time constraint (38%), deceased PWD (25%), participants were unreachable (19%), participants were unwilling to continue in the study (12%), and one PWD went missing (6%) during the study time (Figure 1).
3.2. Baseline Characteristics of the Participants
Baseline socioeconomic and caregiving characteristics of the FCs and demographic characteristics of the PWD were similar between the intervention and control groups, except for participant’s sex and relationship between dyads. About 70% of the FCs were female and 63% were PWD’s own children with significantly higher proportions in the intervention group (p=0.004 and p=0.041, respectively). Mean age of the FCs was 51.6 ( 12.7). Most of them were Muslims, married, had tertiary level of education, and employed with median monthly household income of RM 4,000 (USD 1 = RM 4.7). Moreover, the two groups were similar in their outcome measures at baseline (Table 1). FCs of PWD who dropped out from the study were wealthier (p = 0.031) and had higher years of schooling (p = 0.015). No significant differences were observed on the other baseline characteristics between participants who dropped-out and who remained in the study.
3.3. Intervention Effects
Mixed ANOVA (Table 2, Figure 2) showed no significant changes in mean ZBI, HADS-A, HADS-D and HADS-total scores from baseline to post-intervention time points, and between the intervention and control groups. However, interaction between receiving the intervention and time (Figure 2) indicates significant negative net gain scores for all outcome variables except for the HADS-D (Table 2). This indicates that caregiver burden, anxiety symptoms and psychological distress were reduced after receiving the intervention over time. Independent t-test revealed that if caregivers perceived themselves as non-Muslim, had lower monthly household income, and had lower social support reported higher mean score on caregiver burden, depressive and anxiety symptoms, and psychological distress. Additionally, if the PWD were not able to selfcare, the caregivers reported higher caregiver burden while unmarried caregivers exhibited higher mean score of burden, anxiety and psychological distress.
Table 3 shows the results of intention to treat analysis using Linear mixed model for repeated measures and examined the independent effect of intervention on the outcome variables over time while controlling for the possible associated factors, such as caregiver’s religion, monthly household income, marital status, social support and PWD’s ability to selfcare. Except for HADS-D, a significant interaction between receiving the intervention and time was observed on all outcome measures. Caregiver burden among the participants in the intervention group decreased by 7.57 unit on ZBI at T1 (post-intervention) (p<0.001) compared to the difference between T1 and T0 in control group. In terms of psychological outcome, anxiety symptoms and psychological distress scores among participants in the intervention group decreased over time by 2.46 (p<0.001) on HADS-A and 2.98 (p=0.011) on HADS-total compared to the differences from baseline to post-intervention in control group.
4. Discussion
The present study evaluated the effectiveness of a telephone-delivered psychoeducational intervention in reducing FCs’ burden, psychological distress, anxiety and depressive symptoms. The results revealed significant improvements in caregiver burden, psychological distress and anxiety in the intervention group compared to the control group. However, no significant change was observed in depressive symptoms. These outcomes align with previous studies on psychoeducational interventions, which highlight the benefits of educational sessions and problem-solving strategies in reducing caregiver burden and anxiety [46,55,56]. Psychoeducational interventions have been found to be effective in alleviating burden and anxiety while acceptance and commitment therapy is considered more effective for addressing depression [57].
The results suggest that telephone-based intervention significantly reduced caregiver burden of PWD compared to the standard care which is in line with similar results as shown by Kwok et al. [44]. In contrast, Tremont et al. found no intervention effects on caregivers’ burden after 6 months intervention compared to our study which is conducted in 3-month period [45]. Tremont et al. suggests a longer intervention duration for at least 12-months to observe substantial reduction in caregiver’s burden [45]. However, the observed differences shows that the duration of the intervention alone may not fully account for the differences in the outcomes but might be attributed to variations in the specific contents of the interventions. Additionally, Davis et al. shows a reduction in caregiver burden on telephone psychoeducation and skills training [58]. However, as Davis et al. compared with in-home intervention, telephone intervention may take longer time to reduce burden and contribute to higher attrition rate compared to in-home psychoeducation intervention. In-home intervention may be beneficial in terms of personal interaction, but may not be feasible to all FCs of PWD. Conversely, continued research by Chodosh et al. indicates no difference in caregiver burden between telephone approach and in-home plus telephone intervention [59]. It shows that telephone intervention only can be as effective as home visits to achieve the desired outcome variables. Since telephone-based intervention can be seen as doable methods to support FCs of PWD, it requires reliable strategies to enhance engagement and retention.
Significant improvements were also observed in FCs’ psychological distress and anxiety symptoms. This is consistent with an intervention study by Hattink et al. which found significant differences in psychological distress through website portal and telephone consultation after 2 months of intervention compared to standard care [60]. However, there is no improvement in anxiety among FCs of PWD [60]. In contrast to expectations, no statistically significant effect of intervention on depressive symptoms were found in the current study. This is consistent with the results shown by Soylemez et al., where intervention conducted through home visits followed by telephone calls showed no significant reduction in depressive symptoms [61]. Similarly, Martin-Carrasco et al. found no significant reduction in depressive symptoms as a result of an educational intervention program based on coping with caregiving (CWC) [62]. Although some intervention studies have shown the effectiveness of telephone interventions in reducing depressive symptoms [43,45,63], several factors could explain the discrepancies with our results. First, the intervention period in our study was spanned over a three-month period, whereas previous studies showing improvement in depressive symptoms had longer interventions lasting at six-month [45], 15-months [63] and 18-months [43]. Additionally, the mean depression score among participants was 5.5 (SD=4.2), showing the mean score near to lower end of the scale which indicates that the participants in our study have initially lower levels of depressive symptoms compared to burden and anxiety, reducing the likelihood of detecting significant changes in depressive symptoms.
The high level of participant response rate with the current intervention highlighted the caregiver’s evident need for support. However, discontinuing the intervention after the study could lead to potential reduction of the intervention effect [64]. Further investigation is needed to maximize the benefit of the intervention. For instance, Losada et al. suggested to add a few booster sessions as a strategy to maintain the sustainable effect of the interventions [65]. The study also faced limitations, particularly concerning attrition rates among higher income FCs and those with more years of schooling. This subgroup might potentially be influenced by their access to other effective complementary treatment for themselves and their family members with dementia. FCs with advanced levels of schooling may contribute to higher-level reasoning and problem-solving skills that result in better access to information and multiple options of care and treatment, and utilizing the given information in a way to maximize its benefit [66], which is outside our study’s scope. In addition, time constraints were found as the main reason for attrition, suggesting higher income FCs possibly prioritized work commitments. Another limitation is PWD’s stages of severity of dementia were not investigated in this study. The needs of the FC may vary depending on the stage of the person's dementia, from moderate to severe, this in turn impacts on specific needs, coping strategies, and challenges [67].
One of the significant challenges encountered by the healthcare staff during telephone-intervention of the caregivers with the PWD is the necessity to reschedule the intervention sessions due to time limitations. The process of rescheduling intervention sessions may introduce anxiety and stress for both the FCs and the healthcare staff, particularly when arranging suitable call times. Consequently, we offered flexibility to allow caregivers and healthcare staff to schedule the calls at their convenience. Despite these limitations, the study design was a single-blinded randomized control trial which is an appropriate design to measure the efficacy of an intervention. We have used the locally validated instruments to measure the outcomes. The intervention also offered flexibility in terms of the caregiver’s availability and discussion topics which was accessible and convenient for busy caregivers who were employed, homebound or resided in rural areas. Tremont et al. suggests that telephone-based intervention also helps in reducing costs by eliminating the need for physical space and travel expenses [45].
5. Conclusions
This study underscores the potential of telephone-delivered psychoeducational interventions in reducing caregiver burden, psychological distress and anxiety among FCs of PWD. While significant improvements were observed in these areas, the study did not find significant effects on depressive symptoms. This highlights the need for further research to examine the most effective strategy and appropriate treatment duration to address depression effectively. Overall, the support of FCs using telephone-based intervention could be one of the solutions to help the policy makers to implement the intervention model in geriatric and psychiatric clinics or hospitals to improve burden, anxiety and psychological distress of FCs to PWD in the community in Malaysia.
Author Contributions
Hashima E Nasreen (HEN) was the principal investigator of the study and primarily conceptualized the research. Syarifah Amirah Binti Syed Ahmad (SABSA) was responsible for retrieving the data. HEN was responsible for analysing the data. SABSA, HEN, Zarina Nahar Kabir (ZNK), Marie Tyrrell (MT), and Åsa Craftman (AC) participated in interpreting the data in the article. SABSA, HEN, ZNK, MT, and AC critically revised the manuscript for important intellectual content. All authors read and approved the manuscript.
Funding
The study was supported by grants from the Ministry of Higher Education, Malaysia under the Fundamental Research Grant Scheme (IIUM/504/RES/G/14/3/2/1/FRGS21-210-0819).
Informed Consent Statement
All subjects gave their informed consents for inclusion before they participated in the study. The study protocol was approved by Malaysia Medical Research and Ethics Committee (NMRR ID-22-00137-BUY), IIUM Research and Ethics Committee (IREC 2022-007), Department of Psychiatry and Memory, Hospital Tengku Ampuan Afzan (HTAA) (00137-BUY (2)), Department of Psychiatry, Sultan Ahmad Shah Medical Centre (IIUM/413/013/14/11/2/IISR22-09), and Research Ethics Committee of Universiti Kebangsaan Malaysia (UKMPPI/11/8/JEP-2022-328).
Data Availability Statement
The dataset generated and analysed during the current study are not publicly available due to confidentiality issues but are available from the principal investigator on reasonable request.
Acknowledgments
We thank all clinic nurses and research assistants involved in helping data collection, family caregivers to PWD who participated in the study, the authors who clarified questions or provided additional information about their studies.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Aranda, M. P.; Kremer, I. N.; Hinton, L.; Zissimopoulos, J.; Whitmer, R. A.; Hummel, C. H.; Trejo, L.; Fabius, C. Impact of Dementia: Health Disparities, Population Trends, Care Interventions, and Economic Costs. J Am Geriatr Soc 2021;69(7):1774–83. [CrossRef]
- World Health Organization. Global Status Report on the Public Health Response to Dementia. Geneva: World Health Organization. 2021;251p.
- Pot, A.; Gallagher-Thompson, D Xiao, L. D., Willemse, B. M., Rosier, I., Mehta, K. ISupport: A WHO Global Online Intervention for Informal Caregivers of People with Dementia. Wiley Online Library. AM Pot, D Gallagher-Thompson, LD Xiao, BM Willemse, I Rosier, KM Mehta, D Zandi, T DuaWorld Psychiatry, 2019. Wiley Online Library 2019;18, 3. [CrossRef]
- Alzheimer’s Disease International. World Alzheimer Report 2015. The Global Impact of Dementia an Analysis of Prevalence, Incidence, Cost and Trends. 2015.
- UNDP Regional Bureau for Asia and the Pacific. 2016.
- Department of Statistics Malaysia. https://www.dosm.gov.my/portal-main/release-content/current-population-estimates-malaysia-2022 (accessed 2024-07-22).
- Qi, S.; Yin, P.; Zhang, H.; Zhang, Q.; Xiao, Y.; Deng, Y.; Dong, Z.; Shi, Y.; Meng, J.; Peng, D.; Wang, Z. Prevalence of Dementia in China in 2015: A Nationwide Community-Based Study. Front Public Health 2021, 9. [CrossRef]
- Wu, Y.-T.; Ali, G.-C.; Lenn Guerchet, M.; Prina, A. M.; Chan, K. Y.; Prince, M.; Brayne, C. Prevalence of Dementia in Mainland China, Hong Kong and Taiwan: An Updated Systematic Review and Meta-Analysis. academic.oup.comYT Wu, GC Ali, M Guerchet, AM Prina, KY Chan, M Prince, C BrayneInternational Journal of Epidemiology, 2018, academic.oup.com. [CrossRef]
- Lee, J.; Meijer, E.; Langa, K. M.; Ganguli, M.; Varghese, M.; Banerjee, J.; Khobragade, P.; Angrisani, M.; Kurup, R.; Chakrabarti, S. S.; Singh Gambhir, I.; Koul, P. A.; Goswami, D.; Talukdar, A.; Ranjan Mohanty, R.; Yadati, R. S.; Padmaja, M.; Sankhe, L.; Rajguru, C.; Gupta, M.; Kumar, G.; Dhar, M.; Chatterjee, P.; Singhal, S.; Bansal, R.; Bajpai, S.; Desai, G.; Rao, A. R.; Sivakumar, P. T.; Muliyala, K. P.; Crimmins, E. M.; Dey, A. B. Prevalence of Dementia in India: National and State Estimates from a Nationwide Study. Alzheimer’s & Dementia, 2023, 19 (7), 2898–2912. [CrossRef]
- Ganapathy, S. S.; Sooryanarayana, R.; Ahmad, N. A.; Jamaluddin, R.; Abd Razak, M. A.; Tan, M. P.; Mohd Sidik, S.; Mohamad Zahir, S.; Sandanasamy, K. S.; Ibrahim, N. Prevalence of Dementia and Quality of Life of Caregivers of People Living with Dementia in Malaysia. Geriatr Gerontol Int 2020, 20 (S2), 16–20. [CrossRef]
- National Health and Morbidity Survey Elderly Health, 2018. https://iku.moh.gov.my/images/IKU/Document/REPORT/NHMS2018/NHMS2018ElderlyHealthVolume1.pdf.
- Teti, M.; Benson, J.; … K. W.-J. of A.; 2023, undefined. “Each Day We Lose a Little More”: Visual Depictions of Family Caregiving for Persons with Dementia. Journal of Applied Gerontology, 2023, 42 (7), 1642–1650. [CrossRef]
- Lee, J.; Baik, S.; Becker, T. D.; Cheon, J. H. Themes Describing Social Isolation in Family Caregivers of People Living with Dementia: A Scoping Review. 2021, 21 (2), 701–721. [CrossRef]
- Ku, L. J. E.; Chang, S. M.; Pai, M. C.; Hsieh, H. M. Predictors of Caregiver Burden and Care Costs for Older Persons with Dementia in Taiwan. Int Psychogeriatr 2019, 31 (6), 885–894. [CrossRef]
- Kim, B.; Kim, J.; Na, H.; Lee, K.; Chae, K.; geriatrics, S. K.-B. Factors Influencing Caregiver Burden by Dementia Severity Based on an Online Database from Seoul Dementia Management Project in Korea.BMC geriatrics,2021, 21 (1). [CrossRef]
- Xu, L.; Liu, Y.; He, H.; Fields, N.; Ivey, D.; and Kan, C. Caregiving Intensity and Caregiver Burden among Caregivers of People with Dementia: The Moderating Roles of Social Support. Elsevier 2021. [CrossRef]
- Kawaharada, R.; Sugimoto, T.; Matsuda, N.; Tsuboi, Y.; Sakurai, T.; Ono, R. Impact of Loss of Independence in Basic Activities of Daily Living on Caregiver Burden in Patients with Alzheimer’s Disease: A Retrospective Cohort Study. Geriatr Gerontol Int 2019, 19 (12), 1243–1247. [CrossRef]
- Reed, C.; Belger, M.; Andrews, J. S.; Tockhorn-Heidenreich, A.; Jones, R. W.; Wimo, A.; Dodel, R.; Haro, J. M. Factors Associated with Long-Term Impact on Informal Caregivers during Alzheimer’s Disease Dementia Progression: 36-Month Results from GERAS. International psychogeriatrics, 2019. [CrossRef]
- Wahab, P.; Talib, N.; Hatta, N. N. K. N. M., Saidi, S., Mulud, Z. A., Wahab, M. N. A., & Pairoh. The Caregiving Burden of Older People with Functional Deficits and Associated Factors on Malaysian Family Caregivers. Malaysian Journal of Medical Sciences: MJMS, 2024, ncbi.nlm.nih.gov. [CrossRef]
- Collins, R. N.; Kishita, N. Prevalence of Depression and Burden among Informal Care-Givers of People with Dementia: A Meta-Analysis. Ageing Soc 2020, 40 (11), 2355–2392. [CrossRef]
- Alfakhri, A. S.; Alshudukhi, A. W.; Alqahtani, A. A.; Alhumaid, A. M.; Alhathlol, O. A.; Almojali, A. I.; Alotaibi, M. A.; Alaqeel, M. K. Depression among Caregivers of Patients with Dementia. journals.sagepub.comAS Alfakhri, AW Alshudukhi, AA Alqahtani, AM Alhumaid, OA Alhathlol, AI AlmojaliINQUIRY: The Journal of Health Care Organization, 2018, 55, 1–6. [CrossRef]
- Kaddour, L.; and, Kishita, N. Anxiety in Informal Dementia Carers: A Meta-Analysis of Prevalence. Journal of Geriatric Psychiatry and Neurology, 2020, 33 (3), 161–172. [CrossRef]
- Liang, X.; Guo, Q.; Luo, J.; Li, F.; Ding, D.; Zhao, Q.; neurology, Z. H.-B.; 2016, undefined. Anxiety and Depression Symptoms among Caregivers of Care-Recipients with Subjective Cognitive Decline and Cognitive Impairment. Springer 2016, 16 (1). [CrossRef]
- Joling, K.; Marwijk, H. Van; Veldhuijzen A.E, van der Horst H. E.; Scheltens P; Smit F. The Two-Year Incidence of Depression and Anxiety Disorders in Spousal Caregivers of Persons with Dementia: Who Is at the Greatest Risk? Elsevier, 2015.
- Ang, J. P. ; K. ; Koh, E. B. Y. ; Pang, N. T. P. ; Mat Saher, Z.; Pin Tan, K.; Kiat Ang, J.; Boon, E.; Koh, Y.; Tze, N.; Pang, P.; Saher, Z. M. Relationship of Psychological Flexibility and Mindfulness to Caregiver Burden, and Depressive and Anxiety Symptoms in Caregivers of People with Dementia. International Journal of Environmental Research and Public Health, 2023•mdpi.com 2023. [CrossRef]
- Wang, Q.; Xiao, X.; Zhang, J.; Jiang, D.; Wilson, A.; Qian, B.; Song, P.; Yang, Q. The Experiences of East Asian Dementia Caregivers in Filial Culture: A Systematic Review and Meta-Analysis. Front Psychiatry 2023, 14. [CrossRef]
- Whitten, L. Informal Caregiving for People with Dementia and Women’s Health: A Gender-Based Assessment of Studies on Resilience. Current Women’s Health Reviews, 2022. [CrossRef]
- Ng, H. Y.; Griva, K.; Lim, H. A.; Tan, J. Y. S.; Mahendran, R. The Burden of Filial Piety: A Qualitative Study on Caregiving Motivations amongst Family Caregivers of Patients with Cancer in Singapore. Psychol Health 2016, 31 (11), 1293–1310. [CrossRef]
- Pan, Y.; Chen, R.; Nursing, D. Y.-G. The Relationship between Filial Piety and Caregiver Burden among Adult Children: A Systematic Review and Meta-Analysis. Elsevier, 2022. [CrossRef]
- Durepos, P.; Sussman, T.; Ploeg, J.; Akhtar-Danesh, N.; Punia, H.; Kaasalainen, S. What Does Death Preparedness Mean for Family Caregivers of Persons with Dementia? Journal of Hospice and Palliative Medicine, 2019, 36 (5), 436–446. [CrossRef]
- Gabbard, J.; Johnson, D.; Russell, G.; Spencer, S.; Williamson, J. D.; Mclouth, L. E.; Ferris, K. G.; Sink, K.; Brenes, G.; Yang, M. Prognostic Awareness, Disease and Palliative Understanding among Caregivers of Patients with Dementia 2020, 37 (9), 683–691. [CrossRef]
- Guest, G.; Namey, E.; O’Regan, A.; Godwin, C.; Taylor, J. Comparing Interview and Focus Group Data Collected in Person and Online. 2023.
- Joling, K. J.; van Marwijk, H. W. J.; Smit, F.; van der Horst, H. E.; Scheltens, P.; van de Ven, P. M.; Mittelman, M. S.; van Hout, H. P. J. Does a Family Meetings Intervention Prevent Depression and Anxiety in Family Caregivers of Dementia Patients? A Randomized Trial. PLoS One 2012, 7 (1), e30936. [CrossRef]
- Losada, A.; Márquez-González, M.; Romero-Moreno, R.; Mausbach, B. T.; López, J.; Fernández-Fernández, V.; and Nogales-González, C. Cognitive–Behavioral Therapy (CBT) versus Acceptance and Commitment Therapy (ACT) for Dementia Family Caregivers with Significant Depressive Symptoms. Journal of consulting and clinical psychology, 2015.
- Cheung, K. S. L.; Lau, B. H. P.; Wong, P. W. C.; Leung, A. Y. M.; Lou, V. W. Q.; Chan, G. M. Y.; Schulz, R. Multicomponent Intervention on Enhancing Dementia Caregiver Well-Being and Reducing Behavioral Problems among Hong Kong Chinese: A Translational Study Based on REACH II. Int J Geriatr Psychiatry 2015, 30 (5), 460–469. [CrossRef]
- Kim, H. What Is the Effect of a Support Program for Female Family Caregivers of Dementia on Depression? 1. International Journal of Bio-Science and Bio-Technology 2013, 5 (5), 39–46. [CrossRef]
- Ali, S.; and Bokharey, I. Z. Efficacy of Cognitive Behavior Therapy among Caregivers of Dementia: An Outcome Study. Pakistan Journal of Psychological Research, 2015, 30 (2), 249–269.
- Bayly, M.; Morgan, D.; Chow, A. F.; Kosteniuk, J.; Elliot, V. Dementia-Related Education and Support Service Availability, Accessibility, and Use in Rural Areas: Barriers and Solutions. Journal on Aging/La Revue Canadienne Du Vieillissement, 2020. [CrossRef]
- Kajiyama, B.; Thompson, L. W.; Eto-Iwase, T.; Yamashita, M.; Di Mario, J.; Marian Tzuang, Y.; Gallagher-Thompson, D. Exploring the Effectiveness of an Internet-Based Program for Reducing Caregiver Distress Using the ICare Stress Management e-Training Program. Aging Ment Health 2013, 17 (5), 544–554. [CrossRef]
- Kwok, T.; Au, A.; Wong, B.; Ip, I.; Mak, V; Ho, F. Effectiveness of Online Cognitive Behavioral Therapy on Family Caregivers of People with Dementia. Clinical Interventions in Aging, 2014, 9, 631–636. [CrossRef]
- Park, E.; Park, H.; Kim, E. K. The Effect of a Comprehensive Mobile Application Program (CMAP) for Family Caregivers of Home-Dwelling Patients with Dementia: A Preliminary Research. Japan Journal of Nursing Science 2020, 17 (4). [CrossRef]
- Jackson, D.; Roberts, G.; Wu, M. L.; Ford, R.; and Doyle, C. A Systematic Review of the Effect of Telephone, Internet or Combined Support for Carers of People Living with Alzheimer’s, Vascular or Mixed Dementia in the Community. Elsevier, 2016.
- Kuo, L.-M.; Huang, H.-L.; Liang, J.; Kwok, Y.-T.; Hsu, W.-C.; Su, P.-L.; Yea-Ing, &; Shyu, L.; Assistant, R. A Randomized Controlled Trial of a Home-based Training Programme to Decrease Depression in Family Caregivers of Persons with Dementia. Journal of Advanced Nursing, 2017, 73 (3), 585–598. [CrossRef]
- Kwok, T.; Wong, B.; Ip, I.; Chui, K.; Young, D.; Ho, F. Telephone-Delivered Psychoeducational Intervention for Hong Kong Chinese Dementia Caregivers: A Single-Blinded Randomized Controlled Trial. Clinical Interventions in Aging, 2013, 8, 1191–1197. [CrossRef]
- Tremont, G.; Davis J.D; Papandonatos ,G.D; Ott, B.R; Fortinsky, R.H; Gozalo, P; Yue, M.S. Psychosocial Telephone Intervention for Dementia Caregivers: A Randomized, Controlled Trial. Elsevier, 2015. [CrossRef]
- Frias, C. E.; Garcia-Pascual, M.; Montoro, M.; Ribas, N.; Risco, E.; Zabalegui, A. Effectiveness of a Psychoeducational Intervention for Caregivers of People With Dementia with Regard to Burden, Anxiety and Depression: A Systematic Review. J Adv Nurs 2020, 76 (3), 787–802. [CrossRef]
- Hinton, L.; Tran, D.; Nguyen, T.; Ho, J.; and Gitlin, L. Interventions to Support Family Caregivers of People Living with Dementia in High, Middle and Low-Income Countries in Asia: A Scoping Review. BMJ Global Health, 2019, 4, 1830. [CrossRef]
- Nasreen, H.E.; Tyrrell, M.; Vikström, S.; Craftman, Å.; Ahmad, S.A.B.S.; Zin, N.M.; Abd Aziz, K.H.; Tohit, N.B.M.; Aris, M.A.M. and Kabir, Z.N. Caregiver Burden, Mental Health, Quality of Life and Self- Efficacy of Family Caregivers of Persons with Dementia in Malaysia: Baseline Results of a Psychoeducational Intervention Study. 2023. [CrossRef]
- Minhat, H.; Afiah, N.; Zulkefli, M.; Ahmad, N.; Amatullah, T.; Mohd, M. T.; Amirah, N.; Razi, M.; Minhat, H. S.; Jaafar, H. A Systematic Review on Caregiver’s Burden Among Caregivers of Dementia Patients in Malaysia. Journal of Medicine & Health Sciences, 2023, 19 (1), 254–262. [CrossRef]
- World Health Organization. ISupport for Dementia: Training and Support Manual for Carers of People with Dementia; 2018.
- Ng, C.G; Nurasikin M.S; Loh H.S; HA A.Y; Zainal, N.Z. Factorial Validation of the Malay Version of Multidimensional Scale of Perceived Social Support Among a Group of Psychiatric Patients : Malaysian Journal Of Psychiatry. 2012 1;21(2):17-26. https://journals.lww.com/mjp/_layouts/15/oaks.journals/downloadpdf.aspx?an=02076098-201221020-00004 (accessed 2024-08-02).
- Shim, V.; Ng, C.; and Drahman, I. Validation of the Malay Version of Zarit Burden Interview (MZBI). 2017.
- Yahya, F.; and Othman. Validation of the Malay Version of Hospital Anxiety and Depression Scale (HADS) in Hospital Universiti Sains Malaysia. Int Med J, 2015, 22 (2), 80–82.
- Fisher, L.D.; Dixon, D.O.; Herson, J.; Frankowski, R.K.; Hearron, M.S.; Peace, K.E.; Intention to treat in clinical trials Statistical issues in drug research and development. 1990 New York Marcel Dekker:331–50.
- Gonyea, J.; López, L.; and Velásquez, E. H. The Effectiveness of a Culturally Sensitive Cognitive Behavioral Group Intervention for Latino Alzheimer’s Caregivers. The Gerontologist, 2016, 56 (2), 292–302. [CrossRef]
- Lessing, S.; Deck, R.; Research, M. B.-B. H. S.; 2023, undefined. Telephone-Based Aftercare Groups for Family Carers of People with Dementia–Results of a Mixed-Methods Process Evaluation of a Randomized Controlled Trial. BMC Health Services Research, 2023, 23 (1), 643. [CrossRef]
- Sun, Y.; Ji, M.; Leng, M.; Li, X.; Zhang, X.; Wand, Z. Comparative Efficacy of 11 Non-Pharmacological Interventions on Depression, Anxiety, Quality of Life, and Caregiver Burden for Informal Caregivers of People With. International journal of nursing studies, 2022. [CrossRef]
- Davis, L.; Burgio, L.; and Buckwalter, K.C. A Comparison of In-Home and Telephone-Based Skill Training Interventions with Caregivers of Persons with Dementia. Journal of Mental Health and Aging, 2004.
- Chodosh, J.; Colaiaco, B. A.; Connor, K. I.; Cope, D. W.; Liu, H.; Ganz, D. A.; Richman, M. J.; Cherry, D. L.; Blank, J. M.; Carbone, R. D. P.; Wolf, S. M.; Vickrey, B. G. Dementia Care Management in an Underserved Community. 2015, 27 (5), 864–893. [CrossRef]
- Hattink, B.; Meiland, F.; Roest, H. van der; Kevern, P.; Abiuso, F.; Bengtsson, J.; Giuliano, A.; Duca, A. Web-Based STAR E-Learning Course Increases Empathy and Understanding in Dementia Caregivers: Results from a Randomized Controlled Trial in The. Journal of Medical Internet Research, 2015. [CrossRef]
- Söylemez, B. A.; Küçükgüçlü, Ö.; Buckwalter, K. C. Application of the Progressively Lowered Stress Threshold Model with Community-Based Caregivers: A Randomized Controlled Trial. J Gerontol Nurs 2016, 42 (7), 44–54. [CrossRef]
- Martín-Carrasco, M., Domínguez-Panchón, A.I., González-Fraile, E., Muñoz-Hermoso, P., Ballesteros, J. and EDUCA group. Effectiveness of a Psychoeducational Intervention Group Program in the Reduction of the Burden Experienced by Caregivers of Patients with Dementia: The EDUCA-II. Alzheimer Disease & Associated Disorders, 2014, 28(1), pp.79-87.
- Losada, A.; Márquez-González, M.; Romero-Moreno, R. Mechanisms of Action of a Psychological Intervention for Dementia Caregivers: Effects of Behavioral Activation and Modification of Dysfunctional Thoughts. Int J Geriatr Psychiatry 2011, 26 (11), 1119–1127. [CrossRef]
- Pinquart, M.; and Sorenson, S. Helping Caregivers of Persons with Dementia: Which Interventions Work and How Large Are Their Effects? International psychogeriatrics, 2006.
- Losada, A.; Márquez-González, Romero-Moreno, R.; Mausbach, B.T.; López, J.; Journal. Cognitive–Behavioural Therapy (CBT) versus Acceptance and Commitment Therapy (ACT) for Dementia Family Caregivers with Significant Depressive Symptoms. Journal of consulting and clinical psychology, 2015.
- Brown, A. F.; Vassar, S. D.; Connor, K. I.; Vickrey, B. G. Collaborative Care Management Reduces Disparities in Dementia Care Quality for Caregivers with Less Education. J Am Geriatr Soc 2013, 61 (2), 243–251. [CrossRef]
- Schumann, C.; Alexopoulos, P.; Perneczky, R. Determinants of Self- and Carer-Rated Quality of Life and Caregiver Burden in Alzheimer Disease. Int J Geriatr Psychiatry 2019, 34 (10), 1378–1385. [CrossRef]
Figure 1.
Flowchart of participants enrolment.
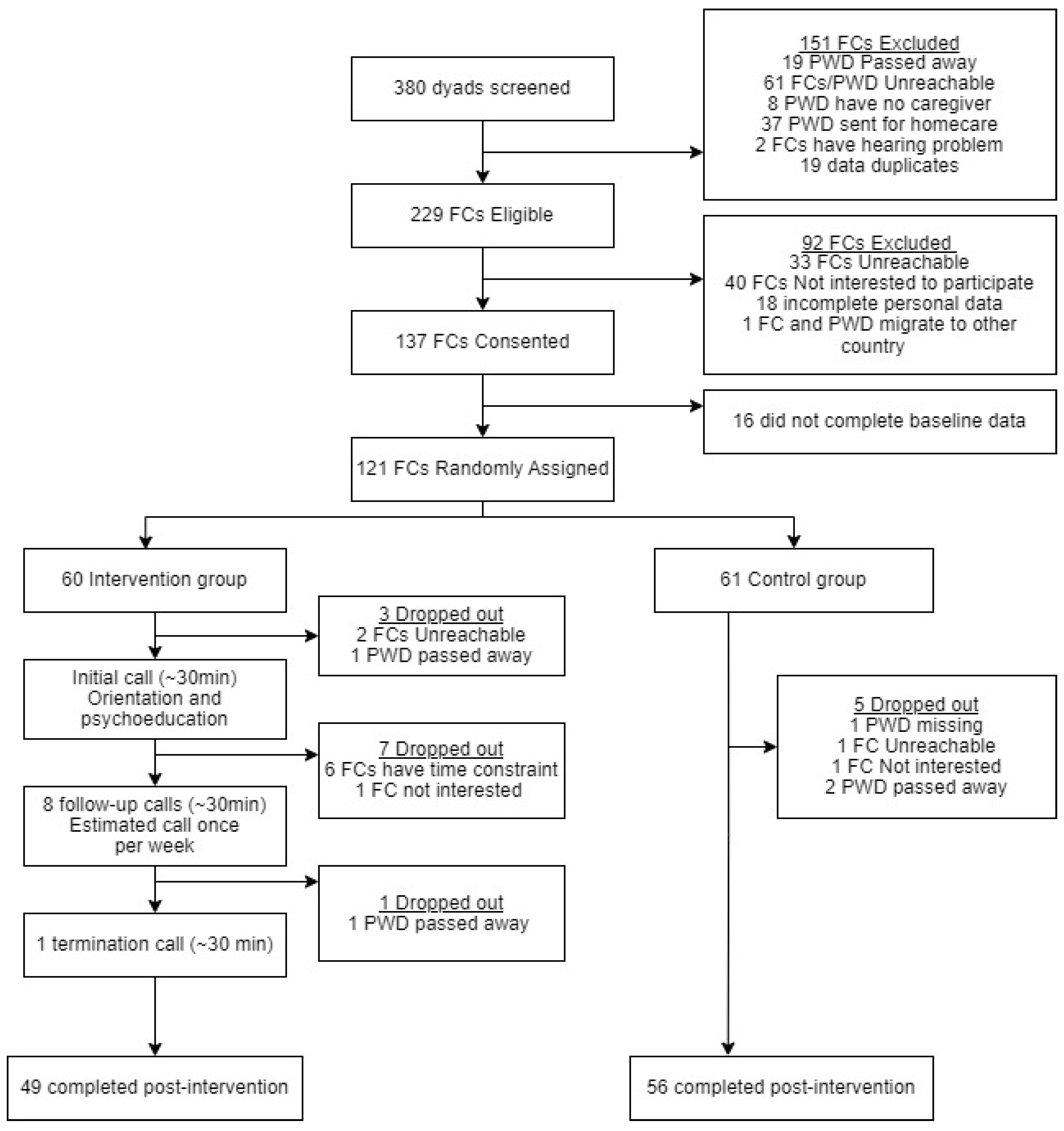
Figure 2.
Interaction between time and intervention on outcome variables: (a) caregiving burden (ZBI); (b) anxiety symptoms (HADS-A); (c) depressive symptoms (HADS-D); (d) psychological distress (HADS-Total).
Figure 2.
Interaction between time and intervention on outcome variables: (a) caregiving burden (ZBI); (b) anxiety symptoms (HADS-A); (c) depressive symptoms (HADS-D); (d) psychological distress (HADS-Total).
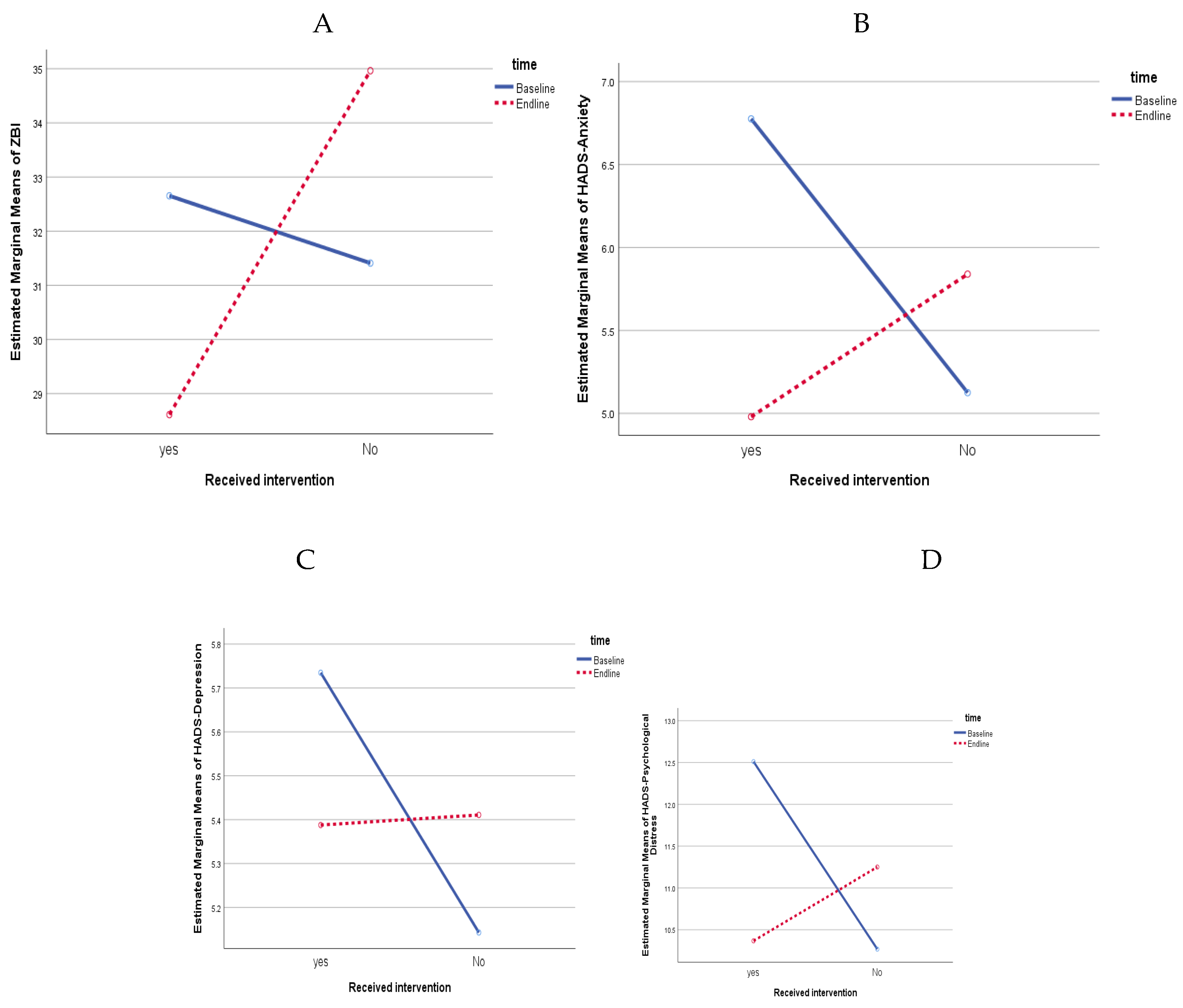

Table 1.
Baseline characteristics of family caregivers and persons with dementia (PWD).
| Total sample n = 121 |
Intervention n = 60 |
Control n = 61 |
p-value | |
|---|---|---|---|---|
| Family caregivers’ socioeconomic characteristics | ||||
| Age (years), Mean (SD) | 51.6 (12.7) | 50.1 (12.4) | 53.1 (12.9) | .185 |
| Sex (%) Male Female |
30.6 69.4 |
18.3 81.7 |
42.6 57.4 |
.004 |
| Religion (%) Muslim Hindu/Buddhist/Christian |
66.9 33.1 |
75.0 25.0 |
59.0 41.7 |
.057 |
| Education (%) Primary Secondary Tertiary |
13.2 39.7 47.1 |
15.0 33.3 51.7 |
11.5 45.9 42.6 |
.365 |
| Years of schooling, Mean (SD) | 12.9 (3.4) | 12.9 (3.5) | 13.0 (3.3) | .935 |
| Marital status (%) Unmarried Married Divorced/widowed |
18.2 73.6 8.2 |
18.3 71.7 10.0 |
18.0 75.4 6.6 |
.553 |
| Occupation (%) Employed Homemaker/unemployed Retired |
54.5 35.5 10.0 |
45.0 43.3 11.7 |
63.9 27.9 8.2 |
.111 |
| Monthly HH income (RM), Median (IQR) | 4,000 (69,500) | 4,000 (69,250) | 4,000 (29,500) | .977 |
| Caregiving information | ||||
| Length of caregiving (months), Mean (SD) | 47.9 (42.8) | 40.7 (34.3) | 55.1 (49.0) | .064 |
| Hours of caregiving/day, Mean (SD) | 18.6 (6.9) | 18.8 (6.9) | 18.4 (7.1) | .800 |
| Shared caregiving by other family members (%) | 60.3 | 56.7 | 63.9 | .414 |
| Number of persons involved in shared caregiving, Mean (SD) | 1.3 (1.5) | 1.4 (1.7) | 1.3 (1.3) | .890 |
| Relationship with person with dementia (%) Spouse Adult child In-laws |
27.3 62.8 9.9 |
21.7 73.3 5.0 |
32.8 52.5 14.8 |
.041 |
| Social support, Mean (SD) | ||||
| Social support (total) | 59.3 (17.1) | 58.6 (16.8) | 59.9 (17.6) | .682 |
| Family support | 21.2 (6.4) | 21.3 (6.0) | 21.5 (6.7) | .891 |
| Friend support | 16.1 (7.3) | 16.0 (7.5) | 16.3 (7.2) | .844 |
| Significant other support | 21.7 (6.5) | 21.3 (6.9) | 22.2 (6.1) | .466 |
| Zarit Burden Interview (ZBI), Mean (SD) | 32.9 (18.4) | 34.0 (18.5) | 31.8 (18.2) | .510 |
| HADS, Mean (SD) | ||||
| HADS-total score | 11.7 (8.2) | 12.6 (8.1) | 10.8 (8.2) | .227 |
| HADS-D score | 5.5 (4.2) | 5.7 (4.3) | 5.4 (4.2) | .693 |
| HADS-A score | 6.2 (4.6) | 6.9 (4.3) | 5.5 (4.9) | .090 |
| PWD’s demographic information | ||||
| Age (year), Mean (SD) | 75.2 (10.1) | 74.8 (10.2) | 75.6 (9.9) | .661 |
| Sex (%) Male Female |
37.2 62.8 |
38.3 61.7 |
36.1 63.9 |
.796 |
| Able to self-care (%) | 56.2 | 50.0 | 62.3 | .173 |
Table 2.
Mean scores and gain scores on ZBI and HADS by intervention groups (N=105).
| Mean score (SD) | Gain score | p-value | Net gain score (95% CI) |
p-value | Effect size (partial η2) |
|||
|---|---|---|---|---|---|---|---|---|
| T0 (Baseline) | T1 (post-intervention) | |||||||
| ZBI | Intervention | 32.65 (19.00) | 28.61 (18.14) | -4.04 | 0.787 |
-7.59 (-11.16- -4.03) |
<0.001 | 0.148 |
| Control | 31.41 (18.50) | 34.96 (19.67) | 3.55 | |||||
| Difference | 1.24 | -6.35 | ||||||
| p-value | 0.992 | |||||||
| HADS-A | Intervention | 6.78 (4.18) | 4.98 (3.78) | -1.80 | 0.111 |
-2.51 (-3.84- -1.18) |
<0.001 | 0.119 |
| Control | 5.13 (4.76) | 5.84 (4.94) | 0.71 | |||||
| Difference | 1.65 | -0.86 | ||||||
| p-value | 0.201 | |||||||
| HADS-D | Intervention | 5.73 (4.42) | 5.39 (4.89) | -0.35 | 0.909 |
-0.62 (-1.97- 0.75) |
0.373 | 0.008 |
| Control | 5.14 (4.03) | 5.41 (4.25) | 0.27 | |||||
| Difference | 0.59 | -0.02 | ||||||
| p-value | 0.956 | |||||||
| HADS-total: Psychological Distress | Intervention | 12.51 (8.08) | 10.37 (7.97) | -2.14 | 0.319 |
-3.13 (-5.42- -0.83) |
0.008 | 0.065 |
| Control | 10.27 (8.10) | 11.25 (8.25) | 0.98 | |||||
| Difference | 2.24 | -0.88 | ||||||
| p-value | 0.426 | |||||||
* Gain score= post-intervention score – baseline score; *Net gain score= gain score (intervention)- gain score (control); partial η2: small effect (η2=0.01 to 0.06), moderate effect (η2>0.06 to 0.14), large effect (η2>0.14) (Richardson, 2011).
Table 3.
Linear mixed model for repeated measures showing the effects of intervention on caregiving burden and psychological distress of family caregivers to persons with dementia (N=121).
Table 3.
Linear mixed model for repeated measures showing the effects of intervention on caregiving burden and psychological distress of family caregivers to persons with dementia (N=121).
| Unadjusted | Adjusted | |||||||
|---|---|---|---|---|---|---|---|---|
| β | Std. error | 95% CI | p-value | β | Std. error | 95% CI | p-value | |
| ZBI | ||||||||
| IG (ref: CG) | 2.18 | 3.37 | 4.49 – 8.51 | .519 | 1.38 | 3.11 | -4.78 – 7.54 | .657 |
| T1 (ref: T0) | 3.50 | 1.22 | 1.08 – 5.93 | .005 | 3.47 | 1.22 | 1.05 – 5.89 | .005 |
| IG T1 (ref: CG T0) | -7.71 | 1.79 | -11.25 – -4.17 | <.001 | -7.57 | 1.78 | -11.11 – -4.03 | <.001 |
| HADS-A | ||||||||
| IG (ref: CG) | 1.54 | 0.82 | -0.09 – 3.17 | .063 | 1.44 | 0.76 | -0.07 – 2.95 | .061 |
| T1 (ref: T0) | 0.64 | 0.45 | -0.27 – 1.54 | .167 | 0.62 | 0.46 | -0.29 – 1.52 | .179 |
| IG T1 (ref: CG T0) | -2.48 | 0.67 | -3.80 – -1 .16 | <.001 | -2.46 | 0.67 | -3.78 – -1.14 | <.001 |
| HADS-D | ||||||||
| IG (ref: CG) | 0.26 | 0.80 | -1.32 – 1.84 | .749 | 0.36 | 0.75 | -1.13 – 1.86 | .630 |
| T1 (ref: T0) | 0.18 | 0.46 | -0.75 – 1.10 | .704 | 0.16 | 0.47 | -0.77 – 1.08 | .738 |
| IG T1 (ref: CG T0) | -0.51 | 0.67 | -1.86 – 0.84 | .456 | -0.53 | 0.68 | -1.88 – 0.82 | .439 |
| HADS-total: psychological distress | ||||||||
| IG (ref: CG) | 1.80 | 1.48 | -1.13 – 4.72 | .227 | 1.74 | 1.35 | -0.94 – 4.41 | .201 |
| T1 (ref: T0) | 0.84 | 0.78 | -0.73 – 2.40 | .291 | 0.79 | 0.78 | -0.77 – 2.35 | .317 |
| IG T1 (ref: CG T0) | -3.01 | 1.14 | -5.29 – -0.73 | .010 | -2.98 | 1.14 | -5.26 – -0.70 | .011 |
* IG: Intervention group, CG: Control group; * T0: Baseline, T1: Post-intervention; Models were adjusted for FC’s religion, monthly household income, marital status, social support, and PWD’s ability to selfcare.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



