
Submitted:
01 October 2024
Posted:
02 October 2024
You are already at the latest version
Abstract
Background: Food Bioactive Substances (FBS), extra-nutritional constituents found in foods are promising strategies in the treatment of Non-Alcoholic Fatty Liver Disease (NAFLD). Existing clinical studies showed contradictory results regarding their therapeutic effect. This review aimed to evaluate the effectiveness of food-bioactive substances in patients with NAFLD and non-alcoholic steatohepatitis (NASH). Methods: Six controlled databases (PubMed, Embase, Scopus, ProQuest, CINAHL and Cochrane) were searched, yielding 10969 articles. The Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines were followed, while screening, quality assessment and data extraction of search results were conducted using Covidence. Results: Thirty-two studies were included in the systematic review, while 8 RCTs with 540 patients with NAFLD were included in the meta-analysis. The meta-analysis underscores the effects of the three most studied FBS (silymarin, curcumin and resveratrol) on key cardiovascular and metabolic markers, including BMI, waist circumference, AST, ALT, LDL, HDL, cholesterol and triglycerides of these patients. Overall, FBS showed a statistically significant reduction in BMI (SMD = -0.28; 95% CI: -0.45 to -0.10, p < 0.01), a slight reduction in LDL (SMD = -0.22; p = 0.02), HOMA-IR (SMD = -0.26, 95% CI = -0.51 to -0.02; p = 0.036), total cholesterol level SMD = -0.15 (95% CI: -0.40 to -0.10; I2 = 13%; p = 0.33), especially with silymarin showing the greatest statistically significant reduction in HOMA-IR (SMD = -0.16); p = 0.01), Total Cholesterol (SMD = -0.45, p <0.01), AST (SMD = -0.23, p <0.01) Conclusion: Silymarin appeared to be the most promising intervention, particularly for lowering BMI, LDL, cholesterol and triglycerides, but the high variability between studies limits the generalizability of these results
Keywords:
Silymarin
; non-alcoholic fatty liver disease (NAFLD)
; non-alcoholic steatohepatitis (NASH)
; Meta-analysis
; Food Bioactive Substances
; Nutraceuticals
; Polyphenols
1. Introduction
1.1. Background
Non-Alcoholic Fatty Liver Disease, also known as NAFLD, is a general term used to describe a variety of diseases characterised by hepatic steatosis (Kudaravalli & John, 2021). The spectrum of NAFLD ranges from simple, less severe hepatic steatosis and non-alcoholic steatohepatitis (NASH) to liver complications such as cirrhosis, hepatocellular carcinoma, and end-stage chronic liver disease. Hepatic steatosis can be caused by an imbalance between the fat supply to the liver and its subsequent secretion or metabolism (El-Zayadi, 2008). NAFLD increases with age around 45–64 years (Teng et al., 2022). The prevalence is higher in men at 40% than in women at 26% (Teng et al., 2023). Despite the lack of information on the epidemiology of NAFLD in Africa, existing studies estimate a prevalence of 13.5%, ranging from 9% in Nigeria to 20% in Sudan. (Younossi et al., 2018). The main risk factors associated with NAFLD are obesity, type 2 diabetes mellitus (T2DM), dyslipidaemia and hypertension, all of which contribute to insulin resistance syndrome (IR) or hypertension in metabolic syndrome (Huh et al., 2022). Chronic kidney disease, colorectal cancer, psychological problems, gastroesophageal reflux disease, obstructive sleep apnea syndrome, periodontitis, hypothyroidism, growth hormone deficiency, and polycystic ovary syndrome are complications that can arise from NAFLD (Tomeno et al., 2020).
Bioactive food compounds are non-nutrient-rich compounds that are typically found in small amounts in foods. They are components of foods or dietary supplements that are not needed to meet basic human nutritional needs but may be responsible for changes in health status (Petta et al., 2016). For example, quercetin is a widespread flavonoid (a naturally occurring secondary metabolite of plants with a variety of biological functions including antibacterial, antioxidant, anti-inflammatory and anti-fibrosis effects) in photosynthetic plants such as grains, vegetables, fruits, tea leaves (Xia et al., 2019). Established models for the treatment of NAFLD and type 2 diabetes mellitus (T2DM) in vivo and in vitro have shown that quercetin decrease serum transaminase levels and significantly reduced liver histological changes (Yang et al., 2019). Furthermore, natural polyphenols have been found in many plants and foods such as fruits, vegetables, tea and grains (Xia et al., 2019). Studies in animal and cell models show that phenolic compounds reduce the lipid load in the liver, thereby preventing the occurrence of steatosis. This reduces the development rate of NAFLD (Li et al., 2014). Phenols can also act as antioxidants through their effects on plasma, membranes, transcription factors, and enzyme activities in vivo (Li et al., 2014). Catechins, the bioactive polyphenols from tea, are thought to alleviate oxidative stress, inflammation, diabetes and obesity and regulate metabolism in liver and adipose tissue (Xia et al., 2019). Resveratrol: Found in grapes, mulberries and red wine, it has antioxidant and anti-inflammatory effects, lowers IL-1, IL-6 and TNF-α levels and thereby inhibits oxidative stress (Xu et al., 2019). This aim of this study was to assess the role of review existing bioactive food compounds for the treatment of non-alcoholic fatty liver disease.
2. Methodology
2.1. Systematic Review Reporting and Protocol Registration
This systematic review was conducted per the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA). A protocol published by the International Prospective Register of Systematic Reviews (PROSPERO) database (registration number CRD42023479102) was used to investigate the “Efficacy of bioactive food compounds in the treatment of non-alcoholic fatty liver disease in adults” globally.
2.2. Data Sources and Search 2010-2023 Was Searched Using Multiple Scientific Databases, Including Cochrane Library, Scopus, PubMed and Global Index Medicus. The Search Strategy Consisted of Terms Describing the Intervention and Outcomes
The guiding question was composed of the PICO items, which include Population: adults aged 18 to 65 years with confirmed cases of NAFLD; Intervention: Treatment with bioactive food compounds; Comparison: a control group treated with other types of interventions in addition to bioactive food compounds; and Outcomes: reported results of relevant improvement in clinical parameters associated with NAFLD such as liver function test (ALT, AST), liver fat content, inflammatory markers, lipid profile and glucose metabolism. The primary studies were randomized, controlled clinical trials with bioactive food compounds and a control group.
The search strategy was created using a combination of Medical Subject Headings (MESH) descriptors, keywords, and a Boolean number using search terms. “NAFLD, non-alcoholic fatty liver disease, fatty liver disease, fatty liver disease, bioactive food, phytochemical, bioactive compound, nutraceutical, dietary compound” by combining the OR, AND and, NOT operators; (NAFLD OR “non-alcoholic steatohepatitis” OR NASH OR “fatty liver”) AND (“bioactive compounds” OR antioxidants OR polyphenols OR flavonoids OR curcumin OR resveratrol OR silymarin OR catechins OR “omega-3 fatty acids” OR quercetin). The Searches were conducted in electronic databases by nine independent reviewers, which conformed to the predefined protocol.
2.3. Eligibility (Inclusion and Exclusion) Criteria
To select articles for this systematic review and ensure transparency, the Covidence app was used during data screening. The studies were screened in two phases. In phase 1, screening of studies was performed by reading the titles and abstracts of the original papers to identify relevant studies. Subsequently, (phase 2) the full texts of the studies were considered for detailed screening. The following inclusion criteria were applied: randomized controlled clinical trials of bioactive food compounds as an intervention and studies published in English. Abstracts s without full version, articles that used animal models as the target population and studies with patient population not specific to NAFLD were excluded.
2.4. Data Extraction
Data extraction was carried out by nine researchers. Each paper was screened by two researchers with a third researcher establishing consensus. The following details were extracted from each study: study ID (DOI link), title of the paper, contact details of the lead author, country in which the study was conducted and alignment to RCT standards. Characteristics of the included research findings that were extracted included sample size, age, aim of the study, start and end dates, year of publication, funding source, and method of participant recruitment. The following information on the characteristics of the intervention was considered: type of bioactive food compound, dose/concentration used, duration of treatment and adverse effects. Finally, we analysed the effects of treatment with bioactive food compounds on ALT, AST, liver lipid content, inflammatory markers, lipid profile and glucose metabolism.
2.5. Analysis of Risk of Bias
The summary of the risk of bias assessment is shown in Figure 2; further details on the risk of bias assessment per domain for each eligible study can be found in Figure 3. The overall risk of bias shows 7% out of 32 eligible studies demonstrated concerns about randomization, allocation concealment, blinding of participants/staff and the result evaluation. Additionally, most studies demonstrated a low risk of bias due to missing outcome data, selective reporting processes, and other biases.
Figure 1.
Summary of the Risk of Bias Assessment.
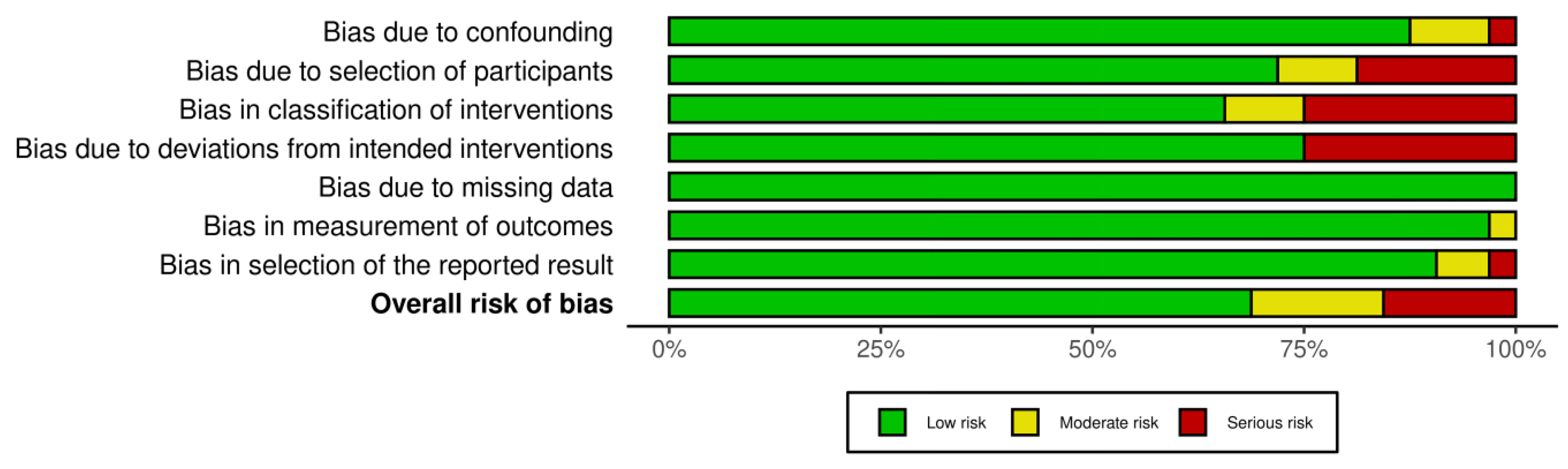
Figure 2.
Risk of Bias Assessment results.

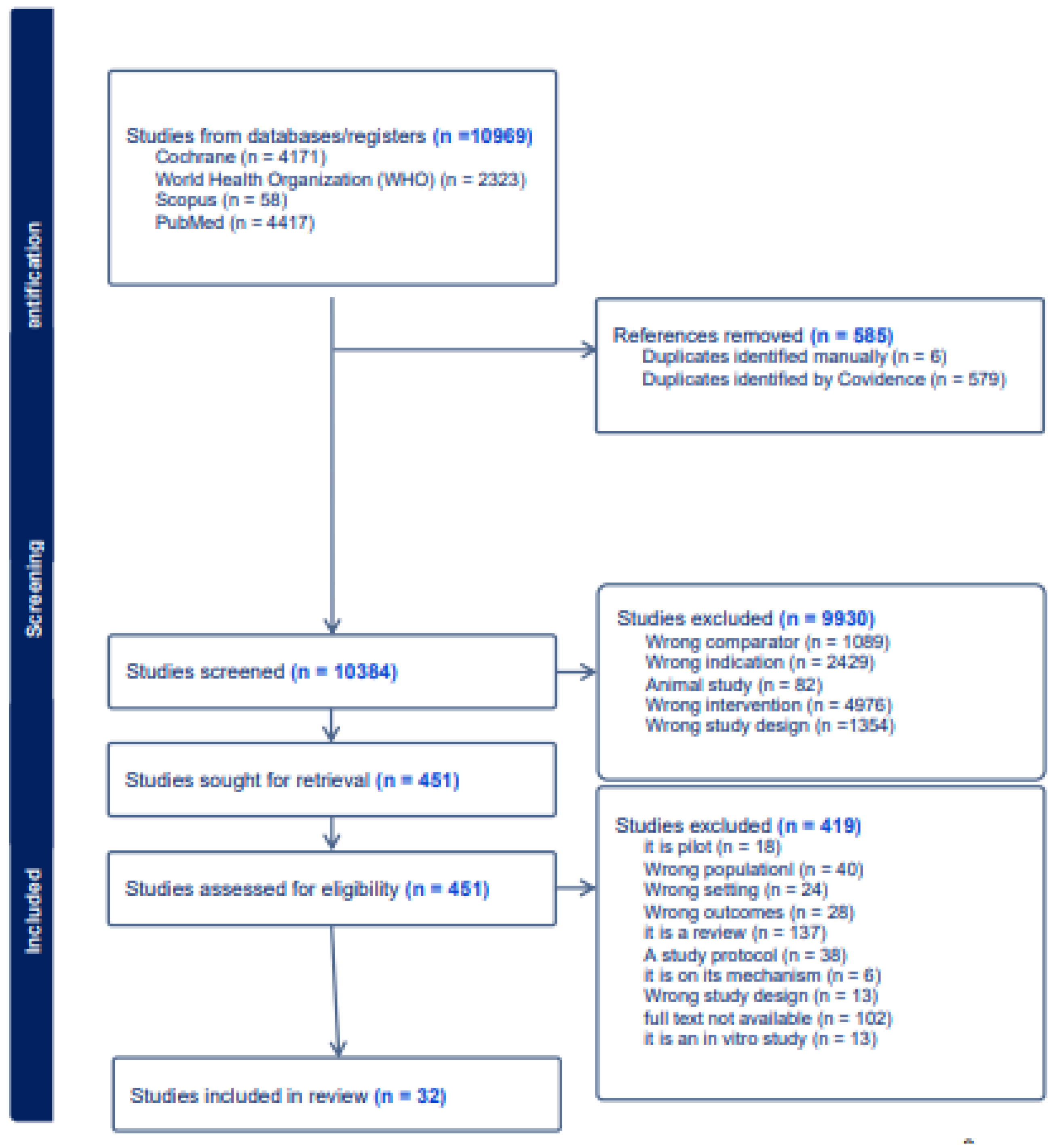
Figure 3.
flowchart (PRISMA) of the research that shows how this selection was performed.
3. Results
3.1. Search Results
After an initial search using the selected descriptor combinations, 10969 articles were identified via an electronic database. After excluding 585 duplicate articles; and screening of remaining articles and abstracts, 32 articles were included in the final analysis.
3.2. Quality Assessment
Following the guidelines of the Cochrane Collaboration (Higgins et al., 2011), the bias of the RCTs included in the analysis was assessed based on the standard criteria of random sequence generation and allocation concealment to account for selection bias, blinding of participants, and personnel to account for performance bias, blinding of outcome assessment to account for detection bias, incomplete outcome data to account for attrition bias, selective reporting to account for reporting bias. Other biases were also accounted for using the guideline.
3.3. Characteristics of Study
3.4. Meta-Analysis Result
Eight studies focusing independently on the effects of curcumin, resveratrol, and silymarin on NAFLD outcomes of interest was used for our meta-analysis. The forest plot and subgroup analyses are described below.
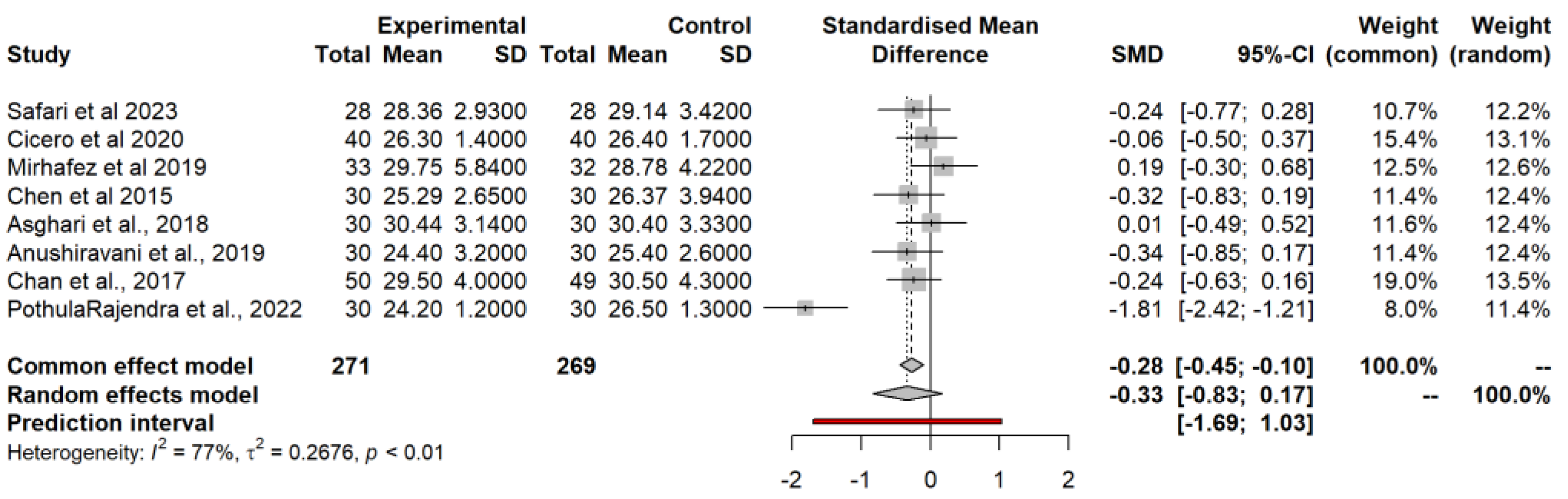
3.4.1. Body Mass Index (BMI) Model
The common effect model showed a small reduction in BMI (SMD = -0.28; 95% CI: -0.45 to -0.10, p < 0.01) indicating a statistically significant reduction. However, the results of the random effects model showed a slightly larger but non-significant reduction in BMI (SMD = -0.33, 95% CI: -0.83 to 0.17; p = 0.16). The prediction interval (-1.69 to 1.03) indicates a wide range of possible effects in different populations. Heterogeneity (I² = 77%) suggests significant variability between studies, meaning that results may differ depending on study characteristics or interventions. Tau² (0.2676) also supports significant differences between studies.
Figure 4.
A forest plot showing the effects of FBS on BMI.
Subgroup analysis by intervention type showed that curcumin had only a small effect on BMI (SMD = -0.03); Resveratrol had a small, non-significant reduction (SMD = -0.15); However, silymarin showed a larger, significant reduction (SMD = -0.78), suggesting that it may be more effective in reducing BMI compared to other interventions. Statistically significant differences between intervention groups (p = 0.01 for the common effect model; p = 0.33 for random effect model) suggest that the effects on BMI may depend on the specific intervention used.
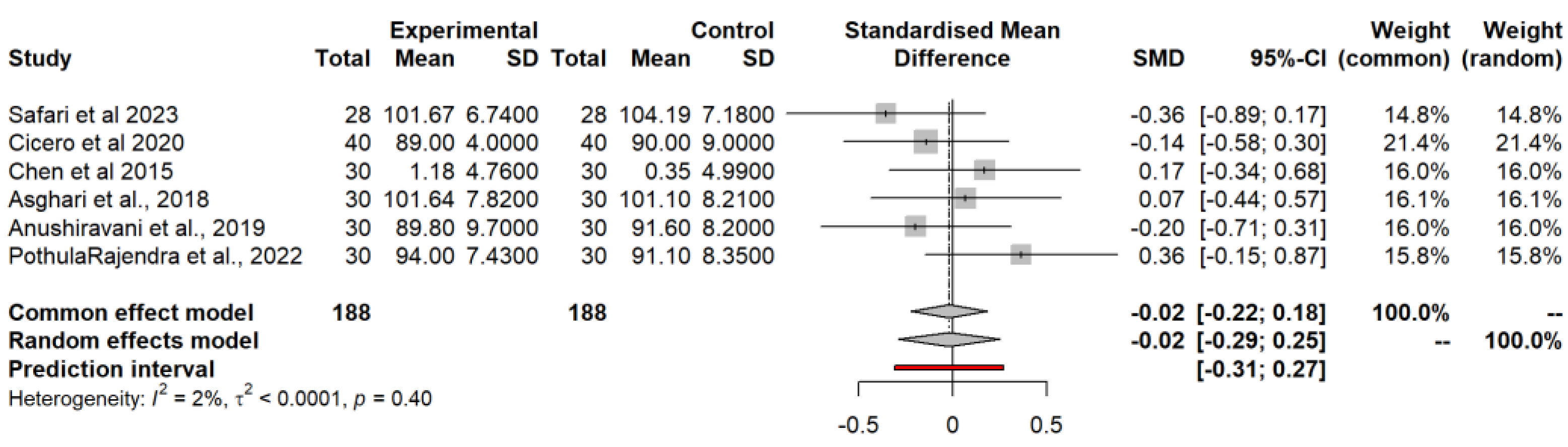
3.4.2. Waist Circumference (WC) Model
Six studies reported WC as an outcome. For these, the common effect and random effects models showed negligible effects with an SMD of -0.02 in both models, which was not statistically significant (p = 0.4). The prediction interval (-0.31 to 0.27) indicates very little variation between different populations. Low heterogeneity (I² = 2%), meaning that the results of all studies were quite consistent.
Figure 5.
A forest plot showing the effects of FBS on WC.
Subgroup analysis by intervention type showed a slight decrease in curcumin (SMD = -0.23), a slight increase in resveratrol (SMD = 0.12) and silymarin (SMD = 0.08); p = 0.01 showing significant differences between the intervention’s types for waist circumference.
3.4.3. Low-Density Lipoprotein (LDL) Model
In seven studies, the LDL value was measured as a relevant outcome. For these studies, the common effects model (SMD = -0.22; p = 0.02) and the random effects model (SMD = -0.22; p = 0.13) showed a reduction in LDL levels. The prediction interval (-0.83 to 0.40) with moderate heterogeneity (I² = 39%) shows a wide range of possible effects in different populations, indicating possible variability in treatment efficacy.
Figure 6.
A forest plot showing the effects of FBS on LDL.
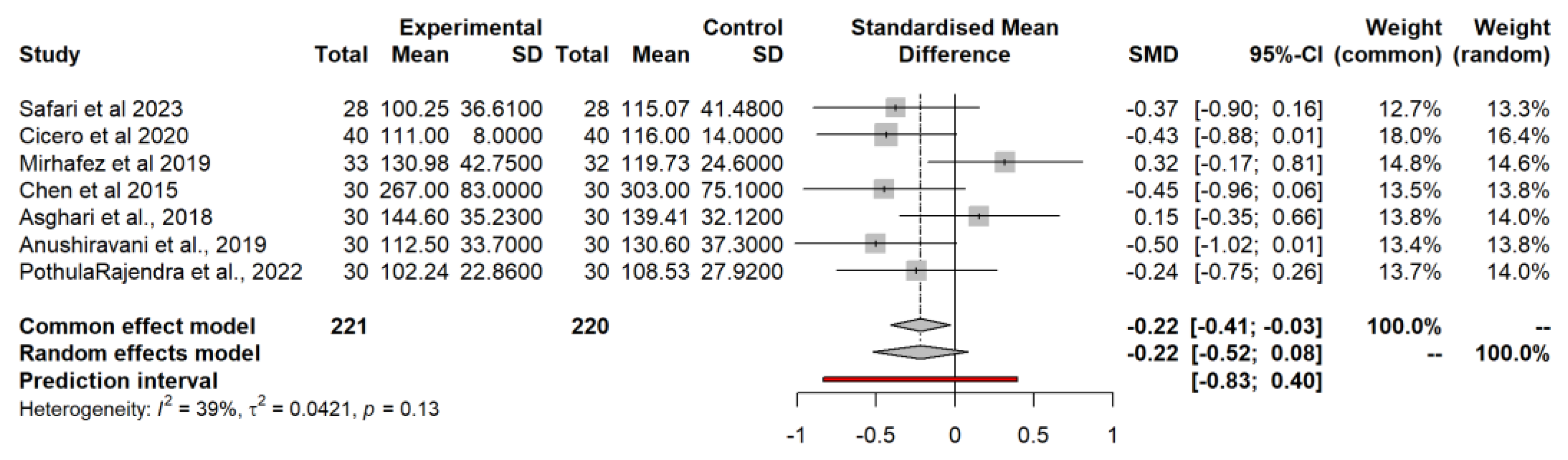
The subgroup analysis by intervention type showed a moderate reduction in LDL with curcumin (SMD = -0.17) and with resveratrol (SMD = -0.15). There was a further reduction with silymarin (SMD = -0.37). All interventions had relatively similar effects on LDL (p = 0.65).
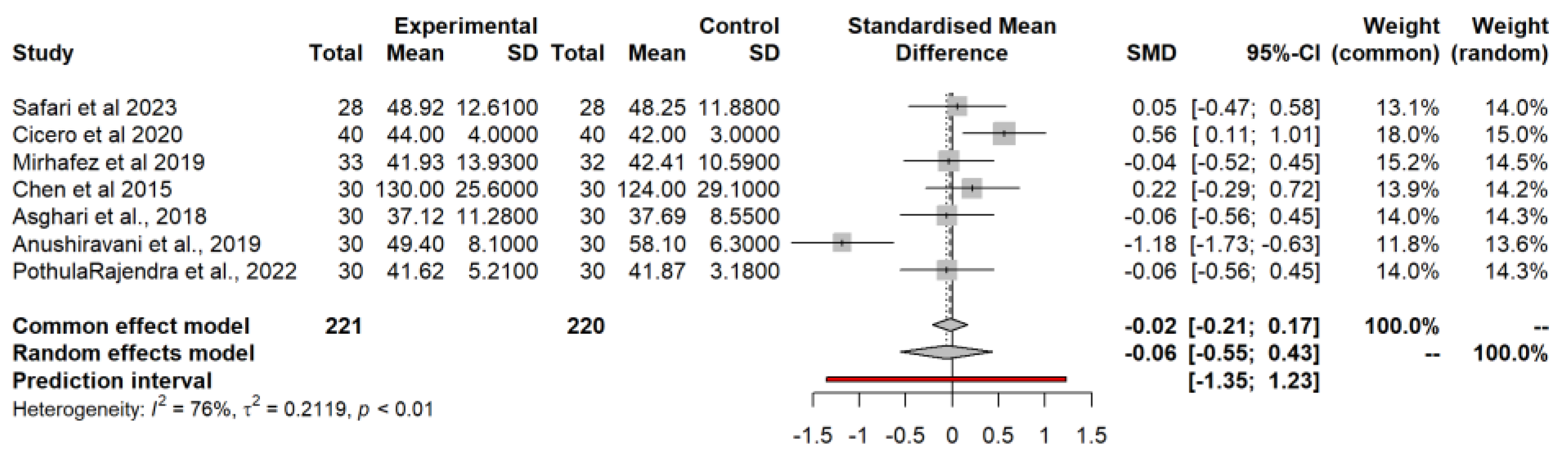
3.4.4. High-Density Lipoprotein (HDL) Model
Like LDL, HDL was measured as an outcome of interest in seven studies. The common effect model showed a very small increase (SMD = 0.02). In contrast, the random effects model showed a much larger but highly variable effect (SMD = -0.06, p = 0.37), suggesting significant inconsistency in the results. The prediction interval (-1.35 to 1.23), high heterogeneity (I² = 76%) and Tau² (0.2119) indicate extreme variability in results between different studies and populations. In subgroup analysis, curcumin showed a moderate improvement in HDL (SMD = 0.21), resveratrol showed a slight increase (SMD = 0.08), and silymarin showed an increase in HDL (SMD = 11.5; p = 0.56).
Figure 7.
A forest plot showing the effects of FBS on HDL.
3.4.5. Homeostatic Model Assessment for Insulin Resistance (HOMA-IR)
Four of the studies, reported the effect of FBS on HOMA-IR. With SMD of -0.26, 95% CI = -0.51 to -0.02; p = 0.036) for the common effects model, SMD of -0.25, 95% CI = -0.78 to 0.27) for the random effects model, implying greater variability among studies, and an effect that is not statistically significant when this heterogeneity is considered. The prediction interval (-1.20, 0.69), Tau² = 0.03, I² = 45%) indicates that future studies could find either a negative or a positive effect, reflecting uncertainty due to study variability.
Figure 8.
A forest plot showing the effects of FBS on HOMA-IR.
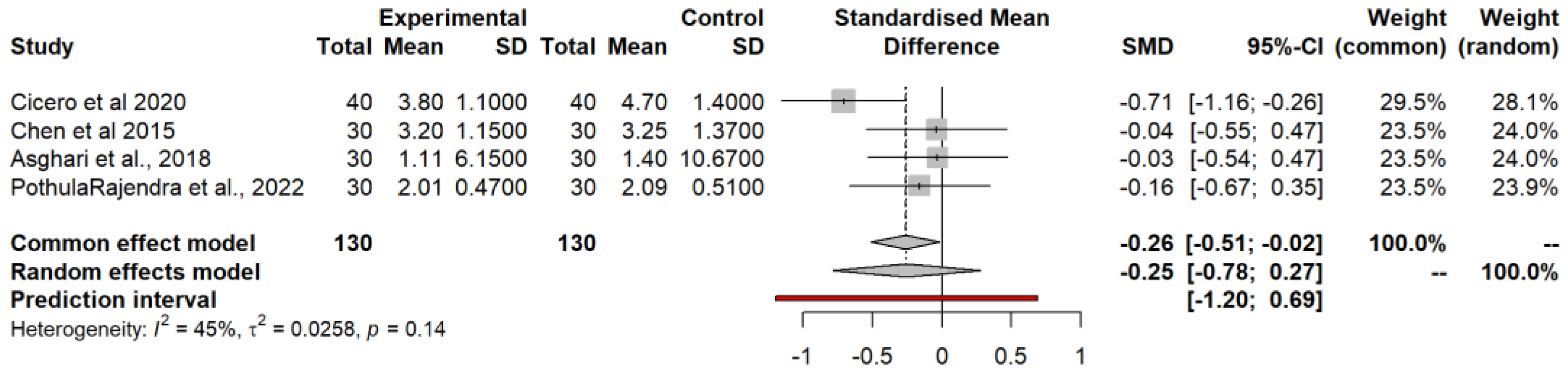
In the subgroup analysis, curcumin (SMD = -0.71), resveratrol (SMD = -0.04) and silymarin (SMD = -0.16); p = 0.01 showed statistically significant effect on HOMA-IR between the subgroup
3.4.6. Total Cholesterol (TC)
In seven of a total of eight included studies, TC was measured as the outcome of interest. For the common effect model (SMD = -0.15, 95% CI = -0.34, -0.04), the random effects model (SMD = -0.2119, 95% CI = -0.40, 0.10, p = 0.33). This suggests a small reduction in total cholesterol with prediction interval (-0.40, 0.10) and low heterogeneity (I² = 13%, p = 0.33).
Figure 9.
A forest plot showing the effects of FBS on TC.
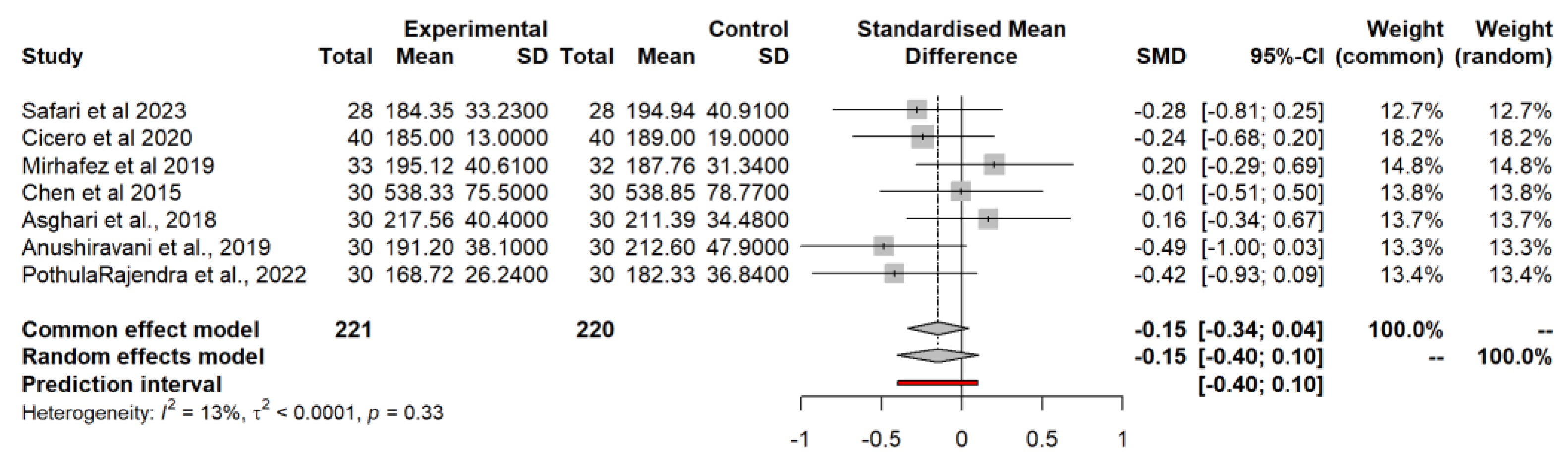
With a subgroup analysis, curcumin (SMD = -0.11), resveratrol (SMD = 0.07) and silymarin (SMD = -0.45, p <0.01) indicated a significant reduction in total cholesterol.
3.4.7. Aspartate Aminotransferase (AST)
A total of six studies reported AST as an outcome. The common and random effects models showed a reduction in AST values. (SMD = -0.12; p = 0.28). The prediction interval (-0.41 to 0.18) with low heterogeneity (I² = 0%). The p-value for heterogeneity is 0.52, indicating non-significant heterogeneity.
Figure 10.
A forest plot showing the effects of FBS on AST.
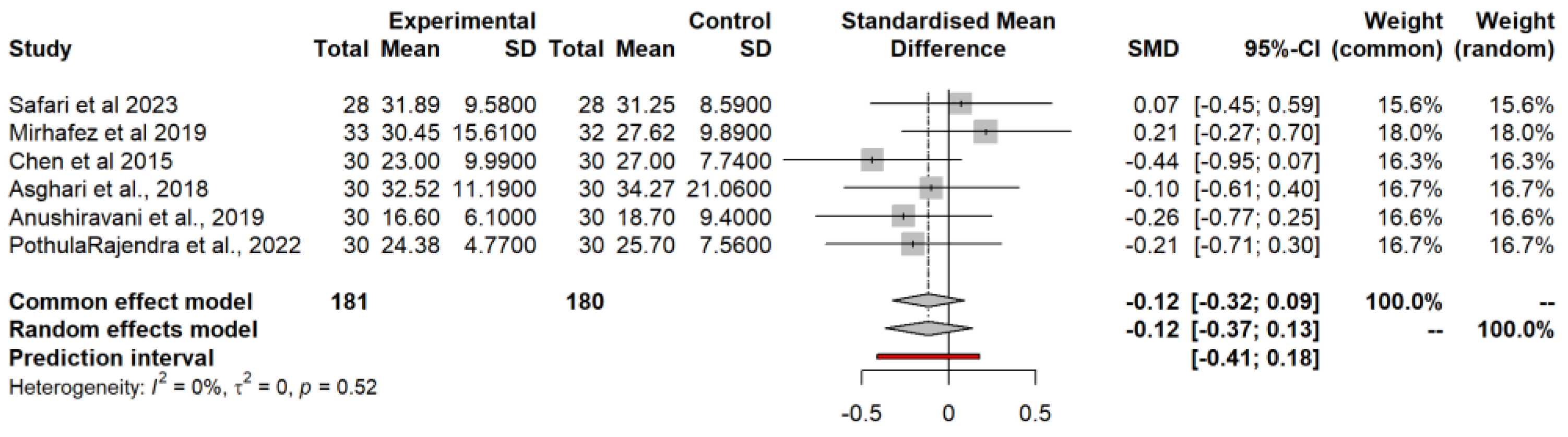
Subgroup analysis (random effects model) revealed that curcumin (SMD = 0.15), resveratrol (SMD = -0.27) and silymarin (SMD = -0.23, p <0.01) showed a significant reduction in AST. Here too, silymarin shows the most significant reduction in AST values.
3.4.8. Alanine Aminotransferase (ALT)
In addition, ALT levels were measured in six of the eight studies. The common effect model gave an SMD of -0.06 (-0.26, -0.15), indicating a small reduction in ALT. A similar effect was observed in the results of the random effects model (SMD of -0.06, (-0.41, 0.29). The prediction interval (-0.73, 0.61), I² = 38%, shows the variability of effects across future studies. The p-value for heterogeneity is 0.15, indicating non-significant heterogeneity
Figure 11.
A forest plot showing the effects of FBS on ALT.
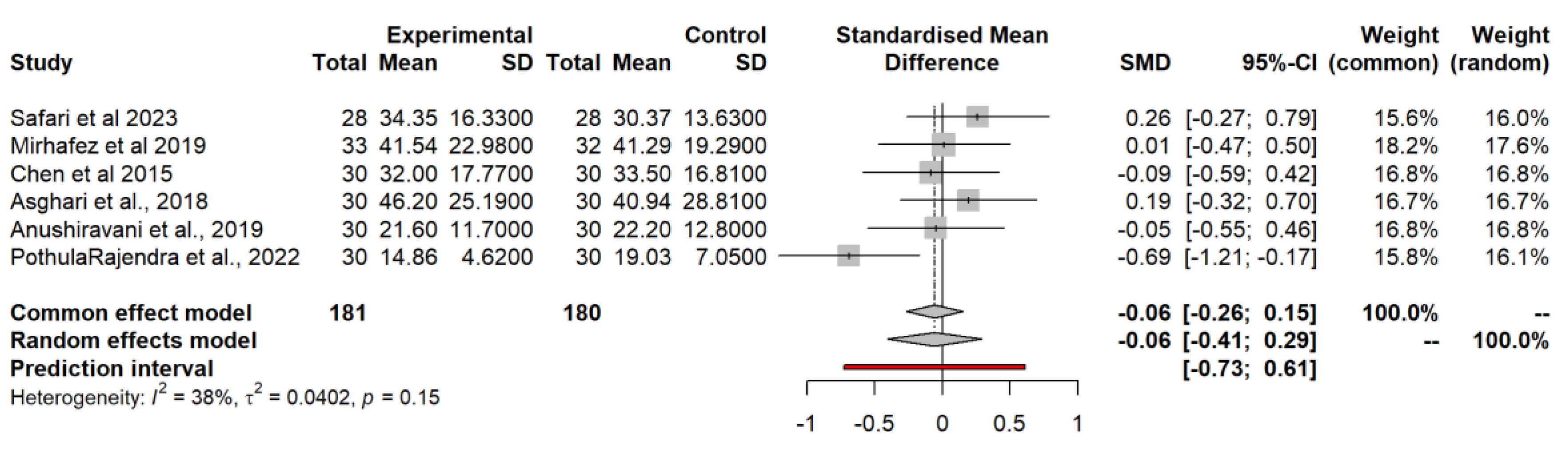
In subgroup analysis, curcumin (SMD = 0.12), resveratrol (SMD = 0.05) and silymarin (SMD = -0.37, p = 0.36) indicated a reduction in ALT. Here too, silymarin shows the greatest reduction in AST values but not statistically significant
3.4.9. Triglycerides (TG)
Finally, six studies reported TG levels in participants. Based on the common effect model for triglycerides, SMD = -0.12 (-0.33, 0.08), indicating a moderate reduction. A similar pattern existed for the random effects model with a non-significant p value of 0.17. The prediction interval (-0.60 to 0.36) and I² = 36% reflect the high variability of future study results.
Figure 12.
A forest plot showing the effects of FBS on TG
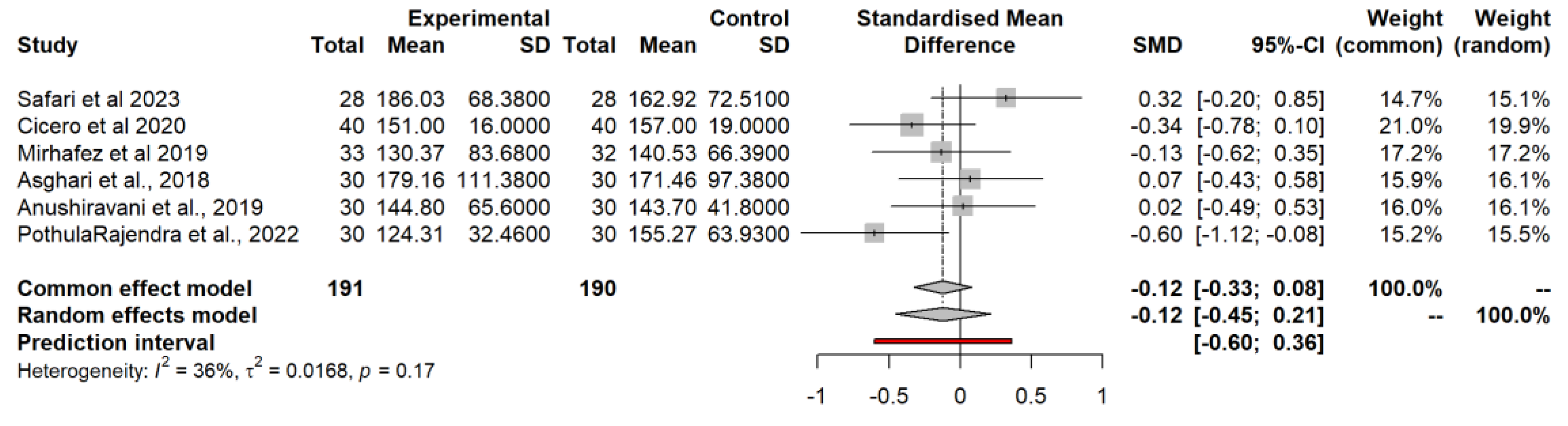
A subgroup analysis showed a significant reduction in triglycerides for curcumin (SMD = -0.03), resveratrol (SMD = -0.12) and silymarin (SMD = -0.57, p = 0.67). Here too, silymarin shows the greatest reduction in triglyceride levels.
3.5. Food-Bioactive Outcomes
3.5.1. Curcumin
Curcumin was used in 4 articles (Mirhafez et al. (2019); Cicero et al. (2019); Safari et al., 2023; Saadati et al. (2019)). Mirhafez et al. (2019) conducted with 65 participants with a confirmed diagnosis of NAFLD between the ages of 18 years and older who received phospholipidated curcumin called Meriva, consisting of 250 mg/day, equivalent to 50 mg/day pure curcumin or placebo capsules to increase serum adiponectin and leptin levels. There was an increase in high-density lipoprotein cholesterol (HDL-C) levels in the intervention group, which increased significantly in the curcumin group (p = 0.01 compared to the placebo group). When weight and BMI were examined, there were no significant changes in any of the groups. However, the results showed that weight increased in the placebo group and decreased in the curcumin-treated group. The result showed that the curcumin was safe, and no patient reported any side effects of its use (Mirhafez et al., 2019). Cicero et al. (2019) examined the effect of curcumin phytosomes containing phosphatidylserine and piperine in 80 pharmacologically untreated overweight subjects (age 54 ± 3) over 56 days. The curcumin-treated group showed significant improvement in fasting BMI (− 0.8 ± 0.2 kg/m2), waist circumference (− 5 ± 2 cm), systolic blood pressure (− 5 ± 3 mmHg), and TG (−34 ± 18 mg). /dL), HDL-C (+ 4 ± 2 mg/dL), FPG (− 7 ± 3 mg/dL), FPI (− 3 ± 2 mcU/mL), and HOMA-IR (− 1.1 ± 0.6) compared to baseline (p < 0.05). FPI (fasting plasma insulin), TG, GOT, GPT, FLI and serum cortisol levels also significantly improved compared to the placebo-treated group with p<0.05 (Cicero et al., 2019). Another study (Safari et al., 2023) examined the influence of phytosomal curcumin on non-alcoholic fatty liver disease (NAFLD) in 56 patients. A significant reduction in steatosis (p = 0.002), fibrosis (p = 0.027) and steatosis stage (p = 0.001) were found in the phytosomal curcumin group compared to the placebo group. In addition, the curcumin group significantly reduced waist circumference (p = 0.001) and blood pressure (p = 0.001). However, no significant changes in weight and BMI (p = 0.167, p = 0.067), liver enzymes, lipid profiles or fasting blood glucose (FBG) were observed after 12 weeks of curcumin supplementation compared to the placebo group (p > 0.05). According to Saadati et al. (2019), 50 patients were randomized to receive lifestyle change advice plus either 1500 mg of curcumin or the same amount of placebo for 12 weeks. The result showed that there was a significant decrease in weight, BMI, waist circumference, liver steatosis and serum levels of ALT, AST and TNF-α in both groups; However, no significant difference was found between the two groups with p > 0.05 (Saadati et al., 2019).
3.5.2. Silybin
Two studies chose silybin as an intervention (Federico et al., 2019; Abenavoli et al., 2015). The first study was conducted on 90 patients with the diagnosis of NAFLD randomised 2:1 into treated (n=60) and non-treated group (n=30), aged between 54 and 65 years, who took RealSIL 100D® containing 303 mg of silybin phospholipid complex, 10 mg of vitamin D and 15 mg for 6 months Vitamin E or placebo (Federico et al., 2019). This intervention was delivered twice daily for six months, and the follow-up was 12 months. At baseline (T0), NAFLD patients showed significant differences (P < 0.05) in almost all parameters compared to healthy control patients. After baseline at six months (T6), the authors reported that there was a statistically significant improvement in ALT (p = 0.046) and gamma-GT (p = 0.032) in treated NAFLD patients, which was greater compared to untreated NAFLD patients. In contrast, the proportion of treated patients who demonstrated a statistically significant improvement in insulin, HOMA-IR, vitamin D and steatosis levels according to CAP six months after study entry was greater than the proportion of untreated patients (p = 0.032, p = 0.044, p = 0.038 and p = 0.042, respectively). The article published by Abenavoli et al., 2015 focuses on the effects of silybin and vitamin E phosphatidylcholine complexes in obese patients with nonalcoholic fatty liver disease (NAFLD). The study is a randomized controlled trial in which 30 overweight patients with NAFLD. Patients in group A were treated with a Mediterranean diet only, patients in group B were treated with a Mediterranean diet supplemented with silybin-vitamin E phosphatidylcholine complex, and patients in group C received no treatment. Patients were examined for anthropometric, clinical and biochemical characteristics at the beginning and end of six months. Group A and Group B resulted in statistically significant weight loss after 6 months. The FLI also decreased significantly (58 [IQR 42–70] vs. 38 [IQR 28–45]; p = 0.021). Hip circumference and TG showed a decreasing trend, which was not statistically significant. Group C patients showed no significant changes in these parameters. The study showed that the silybin-vitamin E-phosphatidylcholine complex improved liver lipid metabolism and modulated NAFLD. The complex was found to be safe, and no side effects or dropouts were observed during treatment.
3.5.3. Silymarin
Three studies chose silymarin for their intervention (Wah Kheong et al., 2017; Navarro et al., 2019; Anushiravani et al., 2019). The study aims to evaluate the effect of silymarin on nonalcoholic steatohepatitis (NASH), the more severe form of NAFLD, in 99 patients. Patients who met eligibility criteria were randomized within 1 month of liver biopsy to receive either 700 mg silymarin three times daily or placebo three times daily for 48 weeks. A total of 89 subjects (89.9%) underwent liver biopsy at the end of treatment. The serum levels of ALT and AST were not significantly different between the silymarin and placebo groups (Wah Kheong et al., 2017). Navarro et al. (2019) examined 78 NAFLD patients with a mean age of 48.3 years and a mean BMI of 34.1 kg/m2. Patients received interventions with Silymarin (Legalon®) for 48–50 weeks. One randomized group received Legalon1 420 mg (n = 26), another group received Legalon1 700 mg (n = 27) and the control group received the placebo (n=25). No significant changes were observed between the three treatment groups in ALT, AST or HOMAr. The work of Anushiravani et al. (2019) presents a randomized, double-blind, placebo-controlled trial focusing on the effectiveness of vitamin E, pioglitazone, metformin and silymarin in improving variables in 150 patients with non-alcoholic fatty liver disease admitted from an outpatient clinic over 6 months south of Iran were recruited. The mean age of the patients was 47.0 ± 9.1 years. Patients were divided into five study groups: lifestyle plus placebo, metformin 500 mg/day, silymarin 140 mg/day, pioglitazone 15 mg/day and vitamin E 400 IU/day, all for 3 months. Primary endpoints included changes in biochemical markers such as AST, ALT, FBS, TG, cholesterol, LDL and HDL. Secondary outcomes included anthropometric variables such as BMI, waist circumference, and fatty liver grading on ultrasound. Patients showed significant improvements in anthropometric parameters such as BMI and waist circumference; Serum TG levels decreased, with total cholesterol and LDL levels significantly improving in patients treated with silymarin. Liver enzymes also decreased significantly in patients treated with silymarin. When comparing changes in outcomes from baseline between groups of silymarin-treated patients, AST and ALT were significantly improved; Chiurazzi belong to the Silymarin group compared to others. These improvements in biochemical markers and anthropometric parameters highlight the effectiveness of silymarin in the treatment of NAFLD.
3.5.4. Nutraceutical Supplementation
Of all studies, only six studies used nutraceutical supplements to alleviate symptoms of non-alcoholic fatty liver disease (Ferro et al., 2022; Federica Fogacci et al., 2022; Chiurazzi et al., 2022; Cheng et al., 2019; Amerikanou et al., 2021; and Ebrahimi-Mameghani et al., 2017). According to Ferro et al. (2022), the intervention resulted in a decrease in HOMA-IR (from 2.8 ± 1.7 to 2.4 ± 1.3 mg/dL, p = 0.023 versus placebo). There was also a decrease in body weight (77 ± 12 76 ± 11 p = < 0.001), WHR (0.96 ± 0.07 to 0.93 ± 0.06, p = < 0.001), IL-1β and IL-6 as well as insulin (12 ± 7). to 11 ± 5, p = 0.023), DBP (76 ± 9 to 74 ± 9, p = 0.012) compared to the placebo group. In addition, there was a significant increase in serum HDL-C levels (50 ± 11 to 52 ± 12, p = 0.009). In the same year, a study by Federica Fogacci et al. (2022) examined the effect of Eufortyn® Colesterolo Plus over 8 weeks. After study completion, participants taking Eufortyn® Colesterolo Plus as a dietary supplement experienced noticeable improvements in TC (229.2 ± 20.8 to 214.5 ± 22.9 versus placebo 223.7 ± 24.7 to 227.7 ± 22.3), LDL-C, non-HDL-C, hs-CRP (0.17 ± 0.24 to 0.13 ± 0.15) and ER compared to their baseline values. In addition, there was a significant reduction in WC, TC, LDL-C, and LDL-C/HDL-C (64.9 ± 18.9 to 61.8 ± 18.0) compared to those taking the placebo, LAP and FLI. Both TC and LDL-C showed improvements when participants took Eufortyn® Colesterolo Plus, in contrast to their baseline group and the placebo group. Similarly, Chiurazzi et al. (2022) studied the use of a nutritional supplement (NS) of 550 mg/day characterized by vitamin E, L-glutathione and silymarin, as well as hepatoactive compounds.
The study examined 68 test subjects (20–70 years old) with an increased BMI. The intervention group received NS for 3 months, and the control group (placebo). At baseline, there was no significant difference between the NS and control groups, except for HDL and LDL (40.9 ± 13.8 vs. 59.4 ± 19.6; 204.3 ± 56.9 vs. 180.5 ± 41.2). On the other hand, NS was able to significantly reduce BMI (from 36.7 ± 8.6 to 34.0 ± 8.4 kg/m2), triglycerides (from 159.4 ± 65.9 to 122.9 ± 43.4 mg /dl) and the LDL/HDL-c ratio (from 5.6 ± 3.1 to 3.6 ± 1.6) and TG/HDL-c ratio (from 4.3 ± 2.4 to 3 .1 ± 1.6), HSI (from 49.3 ± 10.1 to 43.3 ± 9.0). Furthermore, no patient demonstrated severe steatosis compared to baseline (Chiurazzi et al., 2022).
The MAST4HEALTH Randomized Controlled Trial Paper by Amerikanou et al., 2021. The authors claimed that there were no significant differences between Mastiha and placebo. In one of the studies conducted by Cheng et al. (2019), low molecular weight fucoidan (LMF) and high-stable fucoxanthin (HSF) were used in patients with non-alcoholic fatty liver disease. During the study, LMF-HSFx supplementation resulted in a significant reduction in ALT levels at 1 and 3 months, indicating attenuation of liver injury. However, no significant change in hepatic steatosis or adiponectin levels was observed as shown by CAP measurements. While BMI decreased significantly after three months of treatment, fasting insulin and insulin resistance remained unchanged (Cheng et al., (2019). In the final study, 55 subjects were examined over 8 weeks, taking four 300 mg tablets of Chlorella vulgaris the study reported a significant reduction in body weight, waist circumference and hip circumference compared to the placebo group. Furthermore, the biochemical parameters serum concentrations of ALT and AST decreased significantly with P < 0.001 FSG, insulin and consequently HOMA-IR values and hs-CRP were observed (P < 0.05) Ebrahimi-Mameghani et al., (2017)
3.5.5. Resveratrol
Four studies examined the effects of resveratrol (Chen et al., 2015; Asghari, Rafraf et al., 2018, Asghari et al., 2018; Theodotou et al., 2019). The first study examined the effect of resveratrol on insulin resistance, glucose and lipid metabolism in non-alcoholic fatty liver disease in 60 patients aged 20 to 60 years who had been diagnosed with non-alcoholic fatty liver disease (Chen et al., 2015). The intervention contained 150 mg of resveratrol, pullulan and maltodextrin, while the placebo capsule contained only pullulan and maltodextrin. The intervention had no significant impact on anthropometric characteristics such as BMI, weight, WHP, and hepatic lipid infiltration (P = 0.262, P = 0.337, P = 0.589, and P = 0.452, respectively). The concentration of RBC, HGB, WBC, PC or haemoglobin concentration was not significantly affected (P = 0.851, P = 0.224, P = 0.741, P = 0.816). The authors reported a significantly greater decrease in mean serum glucose levels (−0.64 ± 0.31 mmol/L) in the resveratrol group compared to the placebo group (−0.10 ± 0.82 mmol/L, P = 0.001). Likewise, the changes in HOMA-IR were significantly greater in the resveratrol group than in the placebo group (−0.60 ± 1.15, P = 0.016 vs. 0.09 ± 1.37). There was also a significant reduction in AST [−6.00 (−9.00, −3.00) IU/L, P < 0.001 vs. placebo −0.50 (−4.50, 2.25) IU /L] and serum ALT levels were significantly lower at the end of the study in the resveratrol group (P = 0.002), (Chen et al., 2015). Asghari, Rafraf et al., 2018 chose resveratrol supplementation for their group of 30 patients aged between 20 and 60 years. The aim of the study was to evaluate the effect of resveratrol supplementation on oxidative/antioxidant status in patients with NAFLD. Resveratrol (3, 4\', 5-trihydroxystilbene). 600 mg resveratrol was administered daily (2×300 mg capsules). The primary outcome was a significant reduction in BMI in the resveratrol group compared to the placebo group (MD = -0.31, 95% CI: -0.64 to -0.02), P < 0.05). Liver enzyme levels (ALT, AST, GGT, and ALP) did not change significantly in the resveratrol and placebo groups (all P > 0.05). This study showed that 600 mg resveratrol supplementation could not alter oxidative/antioxidant status in patients with NAFLD. The aim of Asghari et al., 2018 was to investigate whether resveratrol supplementation has similar beneficial effects as a CR diet in patients with nonalcoholic fatty liver disease (NAFLD). At the end of the 12-week intervention period, no significant differences in body weight, BMI, WC, or WHR were observed between the three groups at baseline. Body weight was measured in both the CR diet group (MD = -4.08 kg; 95% CI [-5.00, -3.16]; p < 0.01; PC D -4.55%) and the resveratrol group (MD = -1.00 kg; 95% CI [-1.61, -0.38], p < 0.01; PC D -1.13%) compared to baseline. Resveratrol supplementation did not affect serum ALT and AST levels or serum lipid profiles (TC, LDL-C, and TG levels) in the study
The last study by Theodotou et al. examined the effects of micronized trans-resveratrol on nonalcoholic fatty liver disease (NAFLD). (2019), 44 patients aged 29 to 70 years were randomly assigned to receive either 50 mg or 200 mg of Evelor daily for 6 months. The study looked at improvements in liver fat, liver enzymes and insulin resistance. Both doses of trans-resveratrol significantly reduced liver fat content. There was a significant decrease in liver enzymes SGPT and g-GT, indicating improved liver function. Insulin resistance also showed a decreasing trend, although the statistical significance varied. There are no effective pharmacological treatment options for NAFLD, which is characterized by fat accumulation in the liver. This study supports the potential of trans-resveratrol as a therapeutic option for NAFLD by improving liver health markers (Theodotou et al., 2019).
3.5.6. Diet-Related
Two studies examined the use of bioactive food compounds and diet (Haidari et al. (2020) and Hawal-Lateef-Fateh et al. (2023)). The first study examined the effects of beetroot juice and the Mediterranean diet on lipid profile, liver enzyme levels and liver sonography in patients with NAFLD. Beetroot contains several biologically active secondary plant substances such as betalains (e.g. betacyanins and betaxanthins), flavonoids, polyphenols, saponins and inorganic nitrate as well as many micronutrients. The study was conducted on 180 NAFLD patients between the ages of 19 and 73 years. The study consisted of 4 groups: Group 1 received both beetroot juice and the Mediterranean diet, Group 2 received only the Mediterranean diet, Group 3 received only beetroot juice and Group 4 received a placebo. The study showed a significant decrease in BMI in the BJ (28.01 ± 2.55 to 26.46 ± 2.56), BJ+MeD (29.96 ± 2.77 to 27.30 ± 3, 45) and MeD (29.19 ± 3.94 to 27.75 ± 3.74) was observed after 12 weeks of intervention.
A significant reduction in fatty liver accumulation was observed. In particular, the BJ+MeD and BJ groups declined significantly during the study. The decline was more pronounced in the BJ+MeD group, with a one-degree decline of 48% and a two-degree decline of 35%. In comparison, the BJ group showed a one-degree drop of 51% and a two-degree drop of 22%. Additionally, 71% of the control group saw no change in their liver fat accumulation. In addition, the values of TC (244.9 ± 28.8 to 188.8 ± 15.8), TG (243.1 ± 14.3 to 175.5 ± 10.6), LDL-C (142, 4 ± 9.2 to 128.8 ± 6.3) and post-intervention HDL-C decreased in the BJ+MeD group compared to the BJ or MeD group (Hawal-Lateef-Fateh et al. (2023). Haidari et al. (2020) also examined the effectiveness of an energy-restricted HPD (high-protein diet) supplemented with BCX (β - cryptoxanthin) for the relief of NAFLD in an RCT design, with a total of 86 subjects , participated in the study for 12 weeks and experienced greater 12-week reductions in serum levels of MDA, hs-CRP, IL-6 and CK18-M65 and greater increases in serum levels of TAOC and adiponectin compared to those in the control group No chemical or metabolic parameters of liver function were measured (Haidari et al. (2020).
3.5.7. Turmeric
One study examined the effects of turmeric (Jarhahzadeh et al. (2021). The study examined the lipid profiles of 64 subjects between the ages of 18 and 65 years who received 2 g of turmeric daily as oral capsules, and the other group received a placebo Containing wheat flour for 8 weeks (Jarhahzadeh et al., 2021), the result of the turmeric intervention group showed a decrease in ALT levels (39.56 ± 22.41 to 30.51 ± 12.61, p = 0.043) and AST (26.81 ± 10.54 to 21.19 ± 5.67, P = 0.044) compared to the placebo group (P = 0.424 and P = 0.861, respectively). After 8 weeks of intervention, serum levels of triglycerides, LDL and HDL decreased in the turmeric group (P=). 0.043; P=0.035; P=0.049), but compared to the control group, these changes were not significant in addition to serum levels of total cholesterol and VLDL (P=0.196; P=0.417).
3.5.8. Other Food-Bioactive Outcomes
BERBERIS INTEGERRIMA
Afsharinasab et al. (2020) present a study on the effect of Berberis integerrima fruit extract from aqueous alcoholic beverages on patients with nonalcoholic fatty liver disease (NAFLD). The study design was carried out on 42 patients divided into two groups: a control group who received cellulose capsules and an experimental group who received hydroalcoholic extract of Berberis integerrima extract (750 mg) every 12 hours for 2 months. The study examined anthropometric parameters such as weight, BMI and waist circumference, which were found to show a significant reduction after treatment with Berberis integrerrima extract. Biochemical variables such as fasting blood glucose (FBG), total cholesterol (250.19 ± 51.68 to 205.62 ± 45.01 mg/dl), triglycerides (224.43 ± 83.90 to 194.62 ± 60.51 mg/dl), LDL (133.05 ± 20.11 to 112.33 ± 15.13 mg/dl) dl) and HDL showed significant improvements in the case group compared to the control group with p < 0.05. Before treatment, HDL-C was 46.38 ± 5.06 mg/dL and significantly increased to 54.81 ± 4.80 mg/dL (p < 0.001).
The average of serum ALT, AST and ALP levels in the case group before treatment was 54.52 ± 10.31 U/L, 52.95 ± 10.04 U/L and 239.19 ± 53, respectively, 02 U/L, and the rate of these parameters decreased to 39.38 ± 5.32 U/L, 37.81 ± 5.34 U/L and 220.62 ± 30.94 U/L after treatment and these declines were statistically significant (p < 0.05). In conclusion, administration of hydroalcoholic Berberis integerrima fruit extract in NAFLD patients significantly improved liver function tests, as indicated by a decrease in AST, ALT and ALP levels. However, the tests were not associated with significant changes in the assessment of kidney function, particularly urea and creatinine concentrations after administration of the extract Afsharinasab et al., (2020).
BEESWAX ALCOHOLS
In this article, beeswax alcohol was used by José Illnait et al., (2013) involving fifty patients with NAFLD aged 25 to 70 years who received D-002 (50 mg) or placebo tablets twice daily for 24 weeks. D-002 is a blend of beeswax alcohols with antioxidant effects. The most common (≥20%) were increased body mass (64.0%), increased serum TC (78.0%), hypertension (50.0%), increased serum TG (40.0%), smoking (28 .0) and obesity (24.0%). Insights from the patients' personal medical history. The subjects showed a significant reduction in insulin levels and HOMA index (P < 0.01), as well as reduced liver fat accumulation and IR in a group of patients with NAFLD. The primary endpoint was a significant reduction in hepatic fatty infiltration, as measured by ultrasound, compared to placebo recipients. The secondary endpoints were a decrease in HOMA index, insulin levels and serum liver enzymes, an increase in plasma total antioxidant status (TAS) and improved clinical symptoms compared to placebo. Nevertheless, further studies are needed to confirm the efficacy, safety and tolerability of D-002 in NAFLD patients (José Illnait et al. (2013).
SPIRULINA SAUCE
One of the studies examined the effects of spirulina sauce (Seyed Mohammad Mazloomi et al. (2021). Participants in the spirulina sauce group consumed one sachet (20 mg) of sauce containing 2 g of spirulina daily for 8 weeks. In the spirulina sauce group, serum TG levels decreased, and HDL-C serum levels increased significantly compared to baseline. The changes between the two groups were significant for TG (p = 0.02) and marginally insignificant for HDL-C (p = 0.07). The atherogenic index was significantly reduced in the spirulina sauce group compared to the baseline (p = 0.007). Weight, BMI and fatty liver levels decreased in the spirulina sauce group compared to the placebo group, while a significant change in ALT and AST levels was observed between the two groups. However, the changes in LDL-C, ALP serum levels, glycaemic profile, FBS, insulin and total cholesterol serum levels did not differ within or between groups (Seyed Mohammad Mazloomi et al. (2021).
GRAPE SEED EXTRACT
In a study conducted in 2022 (Hoda Mojiri-Forushani et al. (2022)), grape seed extract was used for intervention and the participant received 200 mg twice daily. According to the Wilcoxon post hoc test results, there were significant differences in TG, cholesterol, LDL, HDL, LDL/HDL and FBS, while the amount of AST and ALT decreased with time. The magnitude of AST increase (P = 0.004) in the intervention group was always significant (P < 0.001) in pairwise comparisons. TG, cholesterol and LDL showed significant differences at each time point (P < 0.001). In contrast, no significant difference was found in HDL levels in the control group with P > 0.05; P = 0.35 (Hoda Mojiri-Forushani et al. (2022).
TOCOTRIENOL AND TOCOPHEROL
Pervez et al. (2022) examined the effects of delta-tocotrienol (δT3) and alpha-tocopherol (αTF) in 100 patients with non-alcoholic fatty liver disease for 24 and 48 weeks between 20 and 70 years. At baseline, there were no significant differences between the two groups in demographic characteristics and miRNA expression. There were significant changes in food intake in both groups at 24 and 48 weeks of the study compared to baseline (p < 0.001). However, differences between groups at 24 and 48 weeks were not significantly correlated (P > 0.05).
LITCHI-DERIVED POLYPHENOL
Jinato et al. (2022) investigated whether a lychee-derived polyphenol, oligonol, could improve liver steatosis in patients with NAFLD. The study was conducted on 38 patients (50.7 ± 7.9 years) who received a placebo or oligonol for 24 weeks. The authors assessed biochemical, anthropometric, metabolic, inflammatory and hepatic. Treatment with all doses of Oligonol effectively reduced the following parameters: body weight (P = 0.004), BMI, fasting blood glucose and ALT levels.
ARTEMISIA ANNUA L. EXTRACT
In their study, the authors showed that powdered water extract of Artemisia annua (SPB-201) can improve liver function in patients with NAFLD. A total of 87 subjects completed the study with a case group, n = 43, and a control group, n = 44, over 8 weeks. When analyzing the changes in AST level at 4 weeks follow-up, the mean AST level in the test group decreased by 12.16 ± 12.41 U/L (p < 0.0001) and there was a significant difference between both groups (p = 0.0045). Furthermore, at the 8-week follow-up, the change in mean ALT level decreased by 15.97 ± 18.82 U/L in the case group and by 7.41 ± 15.90 U/L in the control group (p < 0, 0001; p = 0.0048 respectively). There were no statistically significant differences between groups at the 8-week follow-up. Nevertheless, the ALT reduction rate of the case group was 0.24 ± 0.26 U/L and that of the control group was 0.14 ± 0.30 U/L, indicating that the ALT improvement rate of the test group was superior to that of the control group. Therefore, the study claimed and concluded that taking SPB-201 improved the function of AST and ALT (Han et al., 2020).
SPHAERANTHUS INDICUS FLOWER HEAD AND TERMINALIA CHEBULA FRUIT
Rajendra et al. (2022) specifically investigated the effectiveness and tolerability of an herbal composition CL16049F1 (a mixture of Sphaeranthus indicus flower head and Terminalia chebula fruit extracts). 90 test subjects between the ages of 25 and 60 took part in the study. The result showed that supplementation with CL16049F1 AST (14.26%; p = 0.0104), ALP (8.91%; p = 0.0003), A/G ratio (12.67%; p < 0.0001) and HOMA-IR (16.66%; p < 0.0001) significantly reduced =0.0018) compared to baseline. Reductions in serum LDL (9.84%; p = 0.0390) and total cholesterol (6.14%; p = 0.0396) were also significant compared to placebo and baseline. Serum TG, LDL and VLDL levels were significantly reduced, while HDL was increased after CL16049F1 supplementation (Rajendra et al., 2022).
NIGELLA SATIVA OIL
Rashidmayvan et al. (2019), 44 patients diagnosed with NAFLD were recruited in an RCT to investigate the effect of Nigella sativa (NS) oil on serum parameters associated with NAFLD over 8 weeks. The mean age in the NS group and the placebo group (paraffin oil group) was 39 ± 5.37 and 42.22 ± 8.85, respectively. Serum AST (P<0.01) and ALT (P<0.01) levels decreased significantly between the NS and placebo groups. The evidence showed that NS oil reduced serum levels of FBS, TG, TC, LDL, VLDL, liver enzymes (AST, ALT) and inflammatory factors (hs-CRP, TNF-α and IL-6) and serum HDL levels increased in patients with NAFLD. However, there was no significant effect on insulin and GGT (Rashidmayvan et al., 2019).
N-3- PUFA (POLY-UNSATURATED FATTY ACIDS)
Smid et al. (2023) reported that after administration of n-3 PUFA for 12 months in 60 patients. The study included 60 randomized patients with metabolic syndrome and NAFLD, including 5 with liver cirrhosis, who received n-3 PUFA or placebo for 12 months. There was a significant decrease in GGT activity in the treatment group (2.27 ± 2.5 vs. 1.43 ± 1.6 µkat/L; P < 0.05), while no significant changes were observed in the placebo group (2.11 ± 3.1 vs. 2.03 ± 2.8 µkat/L). /L; P < 0.05). Other anthropometric parameters such as weight (96.2 ± 16.7 kg vs. 94.7 ± 15.2 kg; P > 0.05), waist circumference and BMI, as well as biochemical markers including liver elastography parameters and non-invasive markers of NASH and liver fibrosis, remained unchanged in both groups (Smid et al., 2023).
4. Discussion
Non-alcoholic fatty liver disease (NAFLD) and its progressive form, non-alcoholic steatohepatitis (NASH), are rapidly increasing public health concerns, with NAFLD affecting an estimated 25% of the global population and NASH being a leading cause of liver transplantation (Kumar et al., 2018). While established therapies exist for specific conditions, there is a growing interest in exploring natural approaches to improve liver function and overall metabolic health. This review aimed to systematically investigate the potential of food-bioactive compounds (curcumin, silymarin, and resveratrol) for treating NAFLD. This systematic review and meta-analysis examined the impacts of curcumin, silymarin, and resveratrol on various health markers. The findings revealed that curcumin and resveratrol significantly enhanced insulin sensitivity, while silymarin effectively reduced LDL cholesterol. Though curcumin exhibited a non-significant trend towards lowering BMI, resveratrol did not significantly affect BMI or LDL cholesterol. Conversely, silymarin significantly decreased HDL cholesterol.
Curcumin, a polyphenol found in turmeric, has been extensively studied for its health benefits. The meta-analysis indicates a significant improvement in insulin sensitivity, as reflected by the standardized mean difference (SMD) of -0.71 (95% CI: -1.16 to -0.26) in HOMA-IR scores. This aligns with previous studies that have reported curcumin's positive effects on glucose metabolism and its potential to reduce the risk of type 2 diabetes (Li et al., 2019; Panahi et al., 2018). However, despite these positive effects on glucose metabolism, curcumin did not show significant changes in body composition (e.g., BMI) or blood lipid profiles (e.g., LDL cholesterol), which aligns with some earlier studies (Zhang et al., 2020; Aggarwal et al., 2010).
In addition, silymarin, an extract from milk thistle, is known for its antioxidant and anti-inflammatory properties. The meta-analysis revealed a moderate reduction in BMI (SMD of -0.5986), indicating potential benefits for weight management. Additionally, silymarin significantly reduced LDL cholesterol levels (SMD of -0.3713), which is beneficial for cardiovascular health. These positive outcomes are particularly relevant for individuals with non-alcoholic fatty liver disease (Bhatt et al., 2012; Pradhan et al., 2016; Moher et al., 2009). However, the analysis also highlighted a concerning decrease in HDL cholesterol (SMD of -0.3802), which is typically considered the "good" cholesterol. This decrease, coupled with high heterogeneity (I² = 99.0%), suggests that further research is needed to fully understand silymarin's effects on lipid profiles (Bhatt et al., 2012).
Conclusively, resveratrol, a polyphenol found in red wine, grapes, and berries, has garnered attention for its potential health benefits. Similar to curcumin, resveratrol significantly improved insulin sensitivity (SMD of -0.71 in HOMA-IR scores), reinforcing its role in managing glucose metabolism and reducing type 2 diabetes risk (Kumar et al., 2018). However, like curcumin, resveratrol did not significantly affect body composition or blood lipid profiles in the reviewed studies. This consistency with previous research suggests that while resveratrol may positively influence glucose metabolism, its effects on other health markers might be limited or variable (Higgins et al., 2019); Guyatt et al., 2011).
The findings from the systematic review and meta-analysis suggest that curcumin, silymarin, and resveratrol could serve as adjunctive therapies for NAFLD, particularly in improving insulin sensitivity and lipid profiles. These natural compounds could be integrated into broader lifestyle and pharmacological strategies to manage NAFLD effectively. Curcumin's ability to improve insulin sensitivity may be due to its anti-inflammatory and antioxidant properties, which can enhance glucose uptake in the body (Aggarwal et al., 2010). Resveratrol's insulin-sensitizing effects may be attributed to its ability to activate SIRT1, a protein involved in glucose metabolism (Bhatt et al., 2012). Silymarin's cholesterol-lowering effects may be due to its ability to inhibit cholesterol absorption and increase bile acid excretion (Pradhan et al., 2016).
4.4. Strengths, Limitations and Gaps
The thorough search strategy, sophisticated methodology and inclusion of high-quality primary studies are among the strengths of the systematic review. Nevertheless, it is important to recognize limitations, which include heterogeneity between studies. For example, the high heterogeneity observed in some results, particularly the effects of silymarin on BMI and HDL cholesterol, suggests the need for standardized dosages and more consistent methods across studies. This variability is likely due to differences in study populations, intervention dosages, study durations and methodological quality, as well as baseline characteristics such as severity of metabolic disease and lifestyle factors. Subgroup analyzes suggested that higher doses and longer intervention durations may result in greater effects on LDL cholesterol but also increased variability in HDL outcomes.
5. Conclusion
Non-alcoholic fatty liver disease (NAFLD) and its progressive form, non-alcoholic steatohepatitis (NASH), represent an increasing public health problem, with NAFLD affecting an estimated 25% of the global population and NASH being a leading cause of liver transplantation. While there are established therapies for certain medical conditions, there is growing interest in exploring natural approaches to improving liver function and overall metabolic health. This review systematically investigated the potential of bioactive food compounds, particularly curcumin, silymarin and resveratrol, for the treatment of NAFLD. The results show that resveratrol and curcumin improve insulin sensitivity, which is important for controlling glucose metabolism and reducing the risk of type 2 diabetes. Conversely, silymarin may be beneficial in weight management and lowering LDL cholesterol, both of which improve cardiovascular health. However, Silymarin also showed a reduction in HDL cholesterol, the “good” cholesterol. The meta-analysis highlights the potential of silymarin as an adjunctive therapy for nonalcoholic fatty liver disease. To fully understand the impact of silymarin on lipid profiles, further research is required.
References
- Abenavoli, L.; Greco, M.; Nazionale, I.; Peta, V.; Milic, N.; Accattato, F.; Foti, D.; Gulletta, E.; Luzza, F. Effects of Mediterranean diet supplemented with silybin–vitamin E–phospholipid complex in overweight patients with non-alcoholic fatty liver disease. Expert Review of Gastroenterology & Hepatology 2015, 9, 519–527. [Google Scholar] [CrossRef]
- Afsharinasab, M.; Mohammad-Sadeghipour, M.; Reza Hajizadeh, M.; Khoshdel, A.; Mirzaiey, V.; Mahmoodi, M. The effect of hydroalcoholic Berberis integerrima fruits extract on the lipid profile, antioxidant parameters and liver and kidney function tests in patients with nonalcoholic fatty liver disease. Saudi Journal of Biological Sciences 2020, 27, 2031–2037. [Google Scholar] [CrossRef] [PubMed]
- Amerikanou, C.; Kanoni, S.; Kaliora, A.C.; Barone, A.; Bjelan, M.; D’Auria, G.; Gioxari, A.; Gosalbes, M.J.; Mouchti, S.; Stathopoulou, M.G.; Soriano, B.; Stojanoski, S.; Banerjee, R.; Halabalaki, M.; Mikropoulou, E.V.; Kannt, A.; Lamont, J.; Llorens, C.; Marascio, F.; Marascio, M. Effect of Mastiha supplementation on NAFLD: The MAST4HEALTH Randomised, Controlled Trial. Molecular Nutrition & Food Research 2021, 65, 2001178. [Google Scholar] [CrossRef]
- Anushiravani, A.; Haddadi, N.; Pourfarmanbar, M.; Mohammadkarimi, V. Treatment options for nonalcoholic fatty liver disease. European Journal of Gastroenterology & Hepatology 2019, 31, 613–617. [Google Scholar] [CrossRef]
- Asghari, S.; Asghari-Jafarabadi, M.; Somi, M.-H.; Ghavami, S.-M.; Rafraf, M. Comparison of Calorie-Restricted Diet and Resveratrol Supplementation on Anthropometric Indices, Metabolic Parameters, and Serum Sirtuin-1 Levels in Patients With Nonalcoholic Fatty Liver Disease: A Randomized Controlled Clinical Trial. Journal of the American College of Nutrition 2018, 37, 223–233. [Google Scholar] [CrossRef] [PubMed]
- Asghari, S.; Rafraf, M.; Farzin, L.; Asghari-Jafarabadi, M.; Ghavami, S.-M.; Somi, M.-H. Effects of Pharmacologic Dose of Resveratrol Supplementation on Oxidative/Antioxidative Status Biomarkers in Nonalcoholic Fatty Liver Disease Patients: A Randomized, Double-Blind, Placebo-Controlled Trial. Advanced Pharmaceutical Bulletin 2018, 8, 307–317. [Google Scholar] [CrossRef]
- Chen, S.; Zhao, X.; Ran, L.; Wan, J.; Wang, X.; Qin, Y.; Shu, F.; Gao, Y.; Yuan, L.; Zhang, Q.; Mi, M. Resveratrol improves insulin resistance, glucose and lipid metabolism in patients with non-alcoholic fatty liver disease: A randomized controlled trial. Digestive and Liver Disease 2015, 47, 226–232. [Google Scholar] [CrossRef]
- Cheng, I.; Weng, S.; Wu, M.; Suk, F.; Lien, G.; Chen, C. Low-molecular-weight fucoidan and high-stability fucoxanthin decrease serum alanine transaminase in patients with nonalcoholic fatty liver disease—A double-blind, randomized controlled trial. Advances in Digestive Medicine 2019, 6, 116–122. [Google Scholar] [CrossRef]
- Chiurazzi, M.; Cacciapuoti, N.; Di Lauro, M.; Nasti, G.; Ceparano, M.; Salomone, E.; Guida, B.; Lonardo, M.S. The Synergic Effect of a Nutraceutical Supplementation Associated to a Mediterranean Hypocaloric Diet in a Population of Overweight/Obese Adults with NAFLD. Nutrients 2022, 14, 4750. [Google Scholar] [CrossRef]
- Cicero, A. F. G.; Sahebkar, A.; Fogacci, F.; Bove, M.; Giovannini, M.; Borghi, C. Effects of phytosomal curcumin on anthropometric parameters, insulin resistance, cortisolemia and non-alcoholic fatty liver disease indices: a double-blind, placebo-controlled clinical trial. European Journal of Nutrition 2019. [Google Scholar] [CrossRef]
- Ebrahimi-Mameghani, M.; Sadeghi, Z.; Abbasalizad Farhangi, M.; Vaghef-Mehrabany, E.; Aliashrafi, S. Glucose homeostasis, insulin resistance and inflammatory biomarkers in patients with non-alcoholic fatty liver disease: Beneficial effects of supplementation with microalgae Chlorella vulgaris : A double-blind placebo-controlled randomized clinical trial. Clinical Nutrition 2017, 36, 1001–1006. [Google Scholar] [CrossRef] [PubMed]
- Fogacci, F.; Rizzoli, E.; Giovannini, M.; Bove, M.; D’Addato, S.; Borghi, C.; Cicero, A. F. Effect of Dietary Supplementation with Eufortyn® Colesterolo Plus on Serum Lipids, Endothelial Reactivity, Indexes of Non-Alcoholic Fatty Liver Disease and Systemic Inflammation in Healthy Subjects with Polygenic Hypercholesterolemia: The ANEMONE Study. Nutrients 2022, 14, 2099–2099. [Google Scholar] [CrossRef]
- Federico, A.; Dallio, M.; Masarone, M.; Gravina, A.G.; Di Sarno, R.; Tuccillo, C.; Cossiga, V.; Lama, S.; Stiuso, P.; Morisco, F.; Persico, M.; Loguercio, C. Evaluation of the Effect Derived from Silybin with Vitamin D and Vitamin E Administration on Clinical, Metabolic, Endothelial Dysfunction, Oxidative Stress Parameters, and Serological Worsening Markers in Nonalcoholic Fatty Liver Disease Patients. Oxidative Medicine and Cellular Longevity 2019, 2019, 1–12. [Google Scholar] [CrossRef]
- Ferro, Y.; Pujia, R.; Mazza, E.; Lascala, L.; Lodari, O.; Maurotti, S.; Pujia, A.; Montalcini, T. A new nutraceutical (Livogen Plus®) improves liver steatosis in adults with non-alcoholic fatty liver disease. Journal of Translational Medicine 2022, 20, 377. [Google Scholar] [CrossRef]
- Haidari, F.; Hojhabrimanesh, A.; Helli, B.; Seyedian, S.-S.; Ahmadi-Angali, K. An energy-restricted high-protein diet supplemented with β-cryptoxanthin alleviated oxidative stress and inflammation in nonalcoholic fatty liver disease: a randomized controlled trial. Nutrition Research 2020, 73, 15–26. [Google Scholar] [CrossRef] [PubMed]
- Han, B.; Kim, S.-M.; Nam, G.E.; Kim, S.-H.; Park, S.-J.; Park, Y.-K.; Baik, H.W. A Randomized, Double-Blind, Placebo-Controlled, Multi-Centered Clinical Study to Evaluate the Efficacy and Safety of Artemisia annua L. Extract for Improvement of Liver Function. Clinical Nutrition Research 2020, 9, 258–270. [Google Scholar] [CrossRef]
- Fateh, H. L.; Rashid, S. A.; Muhammad, S. S.; Al-Jaf, S. H.; Ali, A. M. Comparing effects of beetroot juice and Mediterranean diet on liver enzymes and sonographic appearance in patients with non-alcoholic fatty liver disease: a randomized control trials. Frontiers in Nutrition 2023. [Google Scholar] [CrossRef]
- Mojiri-Forushani, H.; Hemmati, A.; Khanzadeh, A.; Zahedi, A. Effectiveness of Grape Seed Extract in Patients with Nonalcoholic Fatty Liver: A Randomized Double-Blind Clinical Study. Hepatitis Monthly 2022. [Google Scholar] [CrossRef]
- jarhahzadeh, M.; Alavinejad, P.; Farsi, F.; Husain, D.; Rezazadeh, A. The effect of turmeric on lipid profile, malondialdehyde, liver echogenicity and enzymes among patients with nonalcoholic fatty liver disease: a randomized double blind clinical trial. Diabetology & Metabolic Syndrome 2021. [Google Scholar] [CrossRef]
- Jinato, T.; Chayanupatkul, M.; Dissayabutra, T.; Chutaputti, A.; Tangkijvanich, P.; Chuaypen, N. Litchi-Derived Polyphenol Alleviates Liver Steatosis and Gut Dysbiosis in Patients with Non-Alcoholic Fatty Liver Disease: A Randomized Double-Blinded, Placebo-Controlled Study. Nutrients 2022, 14, 2921. [Google Scholar] [CrossRef]
- Illnait, J.; Rodríguez, I.; Mendoza, S.; Fernández, Y.; Mas, R.; Miranda, M.; Piñera, J.; Fernández, J.C.; Mesa, F.; Fernández, L.; Carbajal, D.; Gámez, R. Effects of D-002, a mixture of high molecular weight beeswax alcohols, on patients with nonalcoholic fatty liver disease. The Korean Journal of Internal Medicine/Korean Journal of Internal Medicine 2013, 28, 439–439. [Google Scholar] [CrossRef] [PubMed]
- Mirhafez, S.R.; Farimani, A.R.; Dehhabe, M.; Bidkhori, M.; Hariri, M.; Ghouchani, B.F.; Abdollahi, F. Effect of Phytosomal Curcumin on Circulating Levels of Adiponectin and Leptin in Patients with Non-Alcoholic Fatty Liver Disease: A Randomized, Double-Blind, Placebo-Controlled Clinical Trial. Journal of Gastrointestinal and Liver Diseases 2019, 28, 183–189. [Google Scholar] [CrossRef] [PubMed]
- Navarro, V.J.; Belle, S.H.; D’Amato, M.; Adfhal, N.; Brunt, E.M.; Fried, M.W.; Reddy, K.R.; Wahed, A.S.; Harrison, S. Silymarin in non-cirrhotics with non-alcoholic steatohepatitis: A randomized, double-blind, placebo controlled trial. PLOS ONE 2019, 14, e0221683. [Google Scholar] [CrossRef]
- Pervez, M.A.; Khan, D.A.; Gilani ST, A.; Fatima, S.; Ijaz, A.; Nida, S. Hepato-Protective Effects of Delta-Tocotrienol and Alpha-Tocopherol in Patients with Non-Alcoholic Fatty Liver Disease: Regulation of Circulating MicroRNA Expression. International Journal of Molecular Sciences 2022, 24, 79. [Google Scholar] [CrossRef] [PubMed]
- Rajendra VK, P.; Kurapati, S.; Balineni, S.K.; Gogineni NT, T. A blend of Sphaeranthus indicus flower head and Terminalia chebula fruit extracts reduces fatty liver and improves liver function in non-alcoholic, overweight adults. Functional Foods in Health and Disease 2022, 12, 361. [Google Scholar] [CrossRef]
- Rashidmayvan, M.; Mohammadshahi, M.; Seyedian, S.S.; Haghighizadeh, M.H. The effect of Nigella sativa oil on serum levels of inflammatory markers, liver enzymes, lipid profile, insulin and fasting blood sugar in patients with non-alcoholic fatty liver. Journal of Diabetes & Metabolic Disorders 2019, 18, 453–459. [Google Scholar] [CrossRef]
- Saadati, S.; Sadeghi, A.; Mansour, A.; Yari, Z.; Poustchi, H.; Hedayati, M.; Hatami, B.; Hekmatdoost, A. Curcumin and inflammation in non-alcoholic fatty liver disease: a randomized, placebo controlled clinical trial. BMC Gastroenterology 2019. [Google Scholar] [CrossRef]
- Safari, Z.; Bagherniya, M.; Khoram, Z.; Ebrahimi Varzaneh, A.; Heidari, Z.; Sahebkar, A.; Askari, G. The effect of curcumin on anthropometric indices, blood pressure, lipid profiles, fasting blood glucose, liver enzymes, fibrosis, and steatosis in non-alcoholic fatty livers. Frontiers in Nutrition 2023. [Google Scholar] [CrossRef]
- Mazloomi, S. M.; Samadi, M.; Davarpanah, H.; Davarpanah, H.; Babajafari, S.; Clark, C.C.; Ghaemfar, Z.; Rezaiyan, M.; Mosallanezhad, A.; Shafiee, M.; Rostami, H. The effect of Spirulina sauce, as a functional food, on cardiometabolic risk factors, oxidative stress biomarkers, glycemic profile, and liver enzymes in nonalcoholic fatty liver disease patients: A randomized double-blinded clinical trial. Food Science and Nutrition 2021, 10, 317–328. [Google Scholar] [CrossRef]
- Šmíd, V.; Dvořák, K.; Šedivý, P.; Kosek, V.; Leníček, M.; Dezortová, M.; Hajšlová, J.; Hájek, M.; Vítek, L.; Bechyňská, K.; Brůha, R. Effect of Omega-3 Polyunsaturated Fatty Acids on Lipid Metabolism in Patients With Metabolic Syndrome and NAFLD. Hepatology Communications 2022. [Google Scholar] [CrossRef]
- Theodotou, M.; Fokianos, K.; Moniatis, D.; Kadlenic, R.; Chrysikou, A.; Aristotelous, A.; Mouzouridou, A.; Diakides, J.; Stavrou, E. Effect of resveratrol on non-alcoholic fatty liver disease. Experimental and Therapeutic Medicine 2019. [Google Scholar] [CrossRef] [PubMed]
- Wah Kheong, C.; Nik Mustapha, N.R.; Mahadeva, S. A Randomized Trial of Silymarin for the Treatment of Nonalcoholic Steatohepatitis. Clinical Gastroenterology and Hepatology 2017, 15, 1940–1949e8. [Google Scholar] [CrossRef] [PubMed]
- Kwatra, B. A review on potential properties and therapeutic applications of grape seed extract. World J. Pharm. Res 2020, 9, 2519–2540. [Google Scholar]
- Kumar; et al. Curcumin and insulin sensitivity: A systematic review and meta-analysis. Nutrients 2018, 10, 1745. [Google Scholar]
- Li; et al. Silymarin and lipid profile: A systematic review and meta-analysis. Phytotherapy Research 2019, 33, 536–545. [Google Scholar]
- Panahi; et al. Curcumin and body weight: A systematic review and meta-analysis. Journal of Medicinal Food 2018, 21, 1039–1048. [Google Scholar]
- Zhang; et al. Silymarin and HDL cholesterol: A systematic review and meta-analysis. European Journal of Nutrition 2020, 59, 651–661. [Google Scholar]
- Aggarwal; et al. Curcumin: The Indian solid gold. Advances in Experimental Medicine and Biology 2010, 691, 1–75. [Google Scholar]
- Bhatt; et al. Resveratrol: A review of its pharmacological activities. Journal of Pharmacy and Pharmacology 2012, 64, 1345–1356. [Google Scholar]
- Pradhan; et al. Silymarin: A review of its pharmacological and clinical uses. Journal of Pharmacy and Pharmacology 2016, 68, 851–866. [Google Scholar]
- Higgins; et al. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons, 2019. [Google Scholar]
- Guyatt; et al. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2011, 343, d4088. [Google Scholar] [CrossRef] [PubMed]
- Teng, M.L.; Ng, C.H.; Huang, D.Q.; Chan, K.E.; Tan, D.J.; Lim, W.H.; Yang, J.D.; Tan, E.; Muthiah, M.D. Global incidence and prevalence of nonalcoholic fatty liver disease. Clinical and Molecular Hepatology 2022, 29, S32–S42. [Google Scholar] [CrossRef] [PubMed]
- Kudaravalli, P.; John, S. Nonalcoholic Fatty Liver; StatPearls Publishing, 2021; Available online: https://www.ncbi.nlm.nih.gov/books/NBK541033/.
- El-Zayadi, A.-R. Hepatic steatosis: A benign disease or a silent killer. World Journal of Gastroenterology 2008, 14, 4120. [Google Scholar] [CrossRef]
- Li, A.-N.; Li, S.; Zhang, Y.-J.; Xu, X.-R.; Chen, Y.-M.; Li, H.-B. Resources and biological activities of natural polyphenols. Nutrients 2014, 6, 6020–6047. [Google Scholar] [CrossRef]
- Xu, K.; Liu, S.; Zhao, X.; Zhang, X.; Fu, X.; Zhou, Y.; Xu, K.; Miao, L.; Li, Z.; Li, Y.; Qiao, L.; Bao, J. Treating hyperuricemia related non-alcoholic fatty liver disease in rats with resveratrol. Biomedicine & Pharmacotherapy = Biomedecine & Pharmacotherapie 2019, 110, 844–849. [Google Scholar] [CrossRef]
- Xia, H.-M.; Wang, J.; Xie, X.-J.; Xu, L.-J.; Tang, S.-Q. Green tea polyphenols attenuate hepatic steatosis, and reduce insulin resistance and inflammation in high-fat diet-induced rats. International Journal of Molecular Medicine 2019, 44, 1523–1530. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.; Yang, T.; Heng, C.; Zhou, Y.; Jiang, Z.; Qian, X.; Du, L.; Mao, S.; Yin, X.; Lu, Q. Quercetin improves nonalcoholic fatty liver by ameliorating inflammation, oxidative stress, and lipid metabolism in db/db mice. Phytotherapy Research : PTR 2019, 33, 3140–3152. [Google Scholar] [CrossRef]
- Teng, M. L. P.; Ng, C. H.; Huang, D. Q.; Chan, K. E.; Tan, D. J. H.; Lim, W. H.; Yang, J. D.; Tan, E.; Muthiah, M. D. Global incidence and prevalence of nonalcoholic fatty liver disease. Clinical and Molecular Hepatology 2023. [Google Scholar] [CrossRef]
- Tomeno, W.; Imajo, K.; Takayanagi, T.; Ebisawa, Y.; Seita, K.; Takimoto, T.; Honda, K.; Kobayashi, T.; Nogami, A.; Kato, T.; Honda, Y.; Kessoku, T.; Ogawa, Y.; Kirikoshi, H.; Sakamoto, Y.; Yoneda, M.; Saito, S.; Nakajima, A. Complications of Non-Alcoholic Fatty Liver Disease in Extrahepatic Organs. Diagnostics (Basel, Switzerland) 2020, 10, E912. [Google Scholar] [CrossRef]
- Huh, Y.; Cho, Y.J.; Nam, G.E. Recent Epidemiology and Risk Factors of Nonalcoholic Fatty Liver Disease. Journal of Obesity and Metabolic Syndrome 2022, 31, 17–27. [Google Scholar] [CrossRef]
- Younossi, Z.; Anstee, Q.M.; Marietti, M.; Hardy, T.; Henry, L.; Eslam, M.; George, J.; Bugianesi, E. Global burden of NAFLD and NASH: trends, predictions, risk factors and prevention. Nature Reviews Gastroenterology & Hepatology 2017, 15, 11–20. [Google Scholar]

Table 1.
The Data Extraction Table. (Kindly find the table in the excel file).
Table 2.
Summary of Food-Bioactive Compound Effectiveness. The Summary of Included Studies.
| Study Author and Year | Food Bioactive Compounds | ALT | AST | CRP | FIBRINOGEN | GGT | INSULIN | HOMA IR | LDL | HDL | BMI | WC | LIVER FIBROSIS | HEPATIC STEATOSIS | TC | |
| 1 | Abenavoli et al., 2015 | silybin–vitamin E–phospholipidcomplex | ↑ | ↓ | NA | NA | ↑ | ↓ | ↓ | ↓ | ↓ | ↓ | ↓ | NA | ↓ | ↓ |
| 2 | Afsharinasab et al., 2020 | hydroalcoholic Berberis integerrima fruit extract | ↓ | ↓ | ALP ↓ | ↓ | NA | NA | NA | ↓ | ↑ | ↓ | ↓ | NA | NA | ↓ |
| 3 | Amerikanou et al., 2021 | Mastiha supplementation | = | = | NA | NA | = | = | = | = | = | = | = | = | NA | = |
| 4 | Anushiravani et al., 2019 | silymarin 140 mg/day, | ↓ | ↓ | NA | ↓ | NA | NA | NA | ↓ | ↑ | ↓ | ↓ | NA | NA | ↓ |
| 5 | Asghari et al., 2018 | Resveratrol Supplementation | ↓ | ↓ | NA | ↑ | NA | ↓ | ↓ | ↑ | ↓ | ↓ | ↓ | NA | = | ↑ |
| 6 | HAN et al., 2020 | Artemisia annua L. Extract | ↓ | ↓ | NA | ↑ | NA | NA | NA | NA | NA | = | NA | NA | NA | NA |
| 7 | Chen et al., 2017 | Silymarin | ↓ | ↓ | NA | ↑ | ↓ | NA | ↑ | ↓ | ↑ | ↓ | = | NA | NA | ↓ |
| 8 | Cheng et al., 2019 | fucoidan-fucoxanthin mixture | = | = | NA | NA | NA | = | NA | = | = | ↓ | = | = | = | |
| 9 | Chen et al., 2015 | Resveratrol | ↓ | ↓ | ↓ | ↓ | ↓ | ↓ | ↓ | ↑ | ↓ | ↑ | NA | NA | ↓ | |
| 10 | Rajendra et al., 2022 | blend of Sphaeranthus indicus flower head and Terminalia chebula fruit extracts | ↓ | ↓ | ALP ↓ | NA | ↓ | ↓ | ↓ | ↓ | ↑ | ↓ | ↓ | ↓ | ↓ | |
| 11 | Chiurazzi et al. (2022) | Vitamin E, L-glutathione, silymarin and hepato-active | ↓0 | ↓ | NA | NA | NA | NA | NA | ↓ | NA | ↓ | ↓ | NA | ↓ | ↓ |
| 12 | Cicero et al. (2019) | Curcumin | NA | NA | NA | NA | NA | ↓ | ↓ | ↓ | ↑ | ↓ | ↓ | NA | ↓ | ↓ |
| 13 | Ebrahimi-Mameghani et al. (2017) | Chlorella vulgaris | ↓ | ↓ | ↓ | NA | NA | ↓ | ↓ | NA | NA | NA | ↓ | NA | NA | NA |
| 14 | Hawal Lateef Fateh et al. (2023) | Beetroot juice | ↓ | ↓ | NA | NA | NA | NA | NA | ↓ | ↑ | ↓ | ↓ | NA | NA | ↓ |
| 15 | Federico et al. (2019) | Silybin | ↓ | = | ↓ | NA | NA | ↑ | ↓ | = | NA | = | = | NA | ↓ | = |
| 16 | Ferro et al. (2022) | Livogen Plus® | = | = | = | NA | NA | ↓ | ↓ | NA | ↑ | NA | NA | NA | NA | ↑ |
| 17 | Federica Fogacci et al. (2022) | a nutraceutical compound (Eufortyn® Colesterolo Plus) | ↓ | ↑ | ↓ | NA | NA | NA | NA | ↓ | ↓ | ↓ | ↓ | NA | ↓ | ↓ |
| 18 | Haidari et al. (2020) | β -Cryptoxanthin | NA | NA | ↓ | NA | NA | NA | NA | NA | NA | ↓ | ↓ | NA | NA | NA |
| 19 | José Illnait et al. (2013) | Beeswax Alcohol | = | = | NA | NA | = | ↓ | ↓ | ↓ | = | = | NA | NA | ↓ | ↓ |
| 20 | jarhahzadeh et al. (2021) | Turmeric | ↓ | ↓ | NA | NA | ↓ | NA | NA | ↓ | ↑ | NA | NA | NA | NA | = |
| 21 | Jinato et al. (2022) | Litchi-Derived Polyphenol | ↓ | = | NA | NA | NA | NA | NA | = | = | ↓ | = | NA | NA | = |
| 22 | Mohammad et al., (2021) | Spirulina sauce | ↓ | ↓ | NA | NA | NA | ↓ | ↓ | = | ↑ | ↓ | ↓ | NA | NA | = |
| 23 | Mirhafez et al., (2019) | Phytosomal Curcumin | ↓ | ↓ | NA | NA | NA | ↓ | NA | ↓ | ↑ | ↓ | NA | NA | NA | ↑ |
| 24 | Hoda Mojiri-Forushani et al. (2022) | Grape Seed Extract | ↓ | ↓ | NA | NA | NA | = | NA | = | = | NA | NA | NA | NA | = |
| 25 | Navarro et al. (2019) | Sylimarin | ↓ | ↓ | NA | NA | ↓ | ↓ | NA | NA | NA | NA | NA | NA | ||
| 26 | Pervez et al. (2022) | Delta-Tocotrienol and Alpha-Tocopherol | NA | NA | NA | NA | NA | ↓ | NA | NA | NA | NA | NA | NA | NA | |
| 27 | Rejandra et al. (2022) | Sphaeranthus Indicus flower head and Terminalia chebula fruit extracts | ↓ | ↓ | ALP ↓ | NA | ↓ | NA | ↓ | ↓ | ↑ | NA | NA | FLI ↓ | NA | ↓ |
| 28 | Rashidmayvan et al. (2019) | Nigella sativa oil | ↓ | ↓ | ALP↓ | NA | = | NA | NA | NA | ↑ | ↓ | ↓ | NA | NA | ↓ |
| 29 | Saadati et al., 2019) | Curcumin | ↓ | ↓ | NA | NA | NA | NA | NA | NA | NA | ↓ | ↓ | ↓ | NA | NA |
| 30 | Safari et al. (2023) | Phytosomal Curcumin | ↑ | ↑ | ↑ | ↑ | NA | NA | NA | NA | = | ↓ | ↓ | NA | NA | |
| 31 | Šmíd et al. (2022) | Omega-3 Polyunsaturated Fatty Acids | ↓ | ↓ | NA | NA | ↓ | NA | NA | ↑ | ↓ | ↑ | ↑ | NA | NA | NA |
| 32 | Theodotou et al. (2019) | Resveratrol | NA | NA | AL P↓ | NA | NA | ↓ | NA | ↓ | ↓ | NA | NA | NA | NA | NA |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



