
Submitted:
02 October 2024
Posted:
03 October 2024
You are already at the latest version
Abstract
Background: Kidney transplantation is the therapy of choice for patients with advanced chronic kidney disease; however, predicting graft outcomes remains a significant challenge. Early identification of reliable biomarkers could enhance post-transplant management and improve long-term outcomes. This study aimed to identify metabolomic biomarkers within the first week post-kidney transplantation that predict renal function at six months. Methods: We conducted a prospective study involving 50 adult patients who received deceased donor kidney transplants. Plasma samples collected one-week post-transplant were analyzed using liquid chromatography-mass spectrometry in a semi-targeted metabolomic approach. A Partial Least Squares-Discriminant Analysis (PLS-DA) model identified metabolites associated with serum creatinine >1.5 mg/dL at six months. Metabolites were selected based on a Variable Importance in Projection (VIP) score >1.5, which was used to optimize model performance. Results: The PLS-DA model demonstrated strong predictive performance with an area under the curve (AUC) of 0.958. The metabolites negatively associated with serum creatinine >1.5 mg/dL were 3-methylindole, guaiacol, histidine, 3-indolepropionic acid, and α-lipoic acid. Conversely, metabolites positively associated with worse kidney graft outcomes included homocarnosine, 5-methylcytosine, xanthosine, choline, phenylalanine, kynurenic acid, and L-kynurenine. Conclusions: Early metabolomic profiling post-transplantation shows promise in predicting renal function. Identifying metabolites with antioxidant and anti-inflammatory properties, as well as those that are harmful and could be targeted therapeutically, underscores their potential clinical significance. The link between several metabolites and the tryptophan pathway suggests that further specific evaluation of this pathway is warranted. These biomarkers can enhance patient management and graft survival.
Keywords:
kidney transplant
; metabolomics
; biomarkers
1. Introduction
Chronic kidney disease (CKD) represents a significant global health problem, affecting approximately 12% of the population and leading to high rates of morbidity and mortality that continue to escalate unremittingly [1]. Kidney transplantation is the therapy of choice for patients with advanced CKD. However, predicting graft outcomes remains a major challenge in post-transplant management, highlighting the urgent need for new biomarkers, particularly those that can be identified early in the post-transplant period to predict long-term outcomes.
Metabolomics offers a promising approach for biomarker discovery, encompassing untargeted metabolomics, which provides a comprehensive analysis of all detectable metabolites and has been used in urine samples to monitor and predict graft function [2]; targeted metabolomics, which focuses on the precise quantification of specific metabolites and has been applied to serum samples to assess metabolic profile changes during the first six months post-transplant [3]; and semi-targeted metabolomics, which integrates elements of both approaches to offer a focused yet comprehensive analysis [4], which it has not yet been evaluated for predicting graft evolution in kidney transplantation.
Our objective is to identify reliable biomarkers within the first week following kidney transplantation using a semi-targeted approach with an in-house compound library. These biomarkers should be associated with serum creatinine levels exceeding 1.5 mg/dL at six months, a threshold associated with adverse long-term outcomes in previous studies [5]. By enabling a rapid diagnosis that facilitates early intervention, we aim to improve kidney transplant (KT) outcomes and enhance patient prognosis.
2. Materials and Methods
2.1. Study Design and Participants
This is a prospective, observational, single-center study of 50 adult patients with stage 5 CKD requiring renal replacement therapy who received a deceased donor KT, with a follow-up over six months post-transplant. Inclusion criteria included patients over 18 years old selected to receive a compatible deceased donor KT, while exclusion criteria included patients with advanced CKD not requiring renal replacement therapy, those on immunosuppressive drugs before the transplant, and those receiving combined transplants.
2.2. Data Collection
Clinical variables of the donor and recipient, along with baseline analytical data, were collected pre-transplant (T0). Subsequent clinical outcomes, analytical variables, and metabolomic samples were collected at two time points: T1 (one-week post-transplant) and T2 (six months post-transplant). For T1, samples were specifically collected on either day 7 or day 8 post-transplant to ensure that, in cases where patients required hemodialysis, the samples would be taken before the dialysis session to avoid any potential alterations caused by the hemodialysis process.
Blood samples for metabolomic analysis were collected and processed by centrifugation. The resulting plasma was then stored at -80°C until the completion of the study.
2.3. Metabolomic Analysis
For the metabolomic analysis, 190 μL of cold methanol was added to 10 μL of plasma to precipitate proteins and extract compounds. The mixture was vortexed for 30 seconds and incubated at -20ºC for 30 minutes. Subsequently, the samples underwent double centrifugation at 9,000 rpm for 10 minutes at 4ºC. From the resulting supernatant, 90 μL was transferred to a 96-well plate for liquid chromatography-mass spectrometry and 10 μL of an internal standard mix solution containing phenilanaline-d5, caffeine-d9, reserpine and leucine enkephalin at 20 μM, was added. Quality control (QC) samples were prepared by pooling 5 μL from each serum sample. A blank was prepared by replacing serum with ultrapure water to identify potential artifacts from tubes, reagents, and other materials.
Samples were analyzed on an Ultra-Performance Liquid Chromatography (UPLC) system coupled to a Q-Exactive Plus spectrometer. The chromatographic separation was performed using an Xbridge BEH Amide column (150 × 2 mm, 2.5 μm particle size; Waters). The autosampler was set to 4°C, and a flow rate of 95 μL/min was used with water, 20 mM ammonium acetate, and 20 mM ammonium hydroxide at pH 9.4, as Mobile Phase A and acetonitrile as Mobile Phase B. To minimize intra-batch variability and enhance reproducibility, the samples were injected in a random order, and a QC sample was analyzed every six plasma samples. Blank analyses were conducted at the end of the sequence.
Electrospray ionization was employed in both positive and negative modes, in full mass acquisition, with a resolving power of 140,000 and three events: mass ranges from 70 to 300 Da, 300 to 560 Da and from 350 to 1200. Data were acquired in the centroid mode. Raw data were converted to mzXML format using MSConvert and then processed in EI-MAVEN software (v0.11.0) by using an in-house polar compound library to generate a peak table containing m/z, retention times, and intensities of metabolites detected.
Data quality (reproducibility, stability) was evaluated by means of the internal standard’s stability and the QC’s coefficients of variation (CVs). Molecular features with CVs > 30% were removed from the data matrix. Additionally, a normalization method (LOESS) was used to eliminate intra-batch variability due to technical differences. Data from positive and negative modes were merged and filtered for the statistical analysis.
2.4. Statistical Analysis
Initially, descriptive statistical analyses were performed on the baseline variables of both donors and recipients, as well as on basic laboratory values and clinical outcomes. Subsequently, a statistical analysis was conducted on the metabolomic data obtained at time point T1, using the outcome variable of serum creatinine levels greater than 1.5 mg/dL at six months. The metabolomic dataset comprised 226 molecules from 48 patients (initially 50 patients; one patient was excluded due to early graft loss and another due to a sample error at T1). The categorical response variable (creatinine levels at six months post-transplant) had two levels: 26 patients with creatinine ≤ 1.5 mg/dL and 22 patients with creatinine > 1.5 mg/dL.
For the metabolomic analysis, a Partial Least Squares-Discriminant Analysis (PLS-DA) model was first constructed using all available metabolites. The model utilized seven principal components, and the optimal number of latent variables was selected through Leave-One-Out Cross-Validation (LOOCV) with the aim of minimizing classification error. A Variable Importance in Projection (VIP) score threshold of 1.5 was applied, identifying 22 polar metabolic variables as significant contributors to the initial model.
A second PLS-DA model was then constructed using only the 22 selected variables obtained in the first model. This final model utilized two principal components, with the number of latent variables again optimized using LOOCV to ensure the lowest classification error. Model validation was conducted using permutation testing with 1000 iterations, confirming that the R² coefficient obtained with the original response variable was greater than that obtained with the permuted response variable in 95% of cases. This provided an empirical p-value for model significance, adding robustness to our findings.
Performance metrics of the final model were evaluated based on LOOCV predictions, including the Receiver Operating Characteristic (ROC) curve, Area Under the Curve (AUC), accuracy, sensitivity, and specificity. These metrics provided a comprehensive assessment of model performance. Additionally, coefficients and 95% confidence intervals (CI) for each variable were obtained using the Jack-Knifing resampling technique. Only significant metabolomic variables were proposed as the most relevant for clinical interpretation, highlighting their potential significance in relation to the outcome variable.
3. Results
The study cohort consisted of 50 KT recipients with a mean age of 53.98 years, predominantly male (70%) and Caucasian (94%). Cardiovascular risk factors were prevalent: 82% had hypertension, 70% dyslipidemia, and 28% were classified as obese (Body Mass Index, (BMI)>30). The primary etiologies of CKD were hereditary/familial causes (26%) and unclassified causes (24%).
Regarding renal replacement therapy (RRT) prior to transplantation, 74% were on hemodialysis and 26% were on peritoneal dialysis. The mean duration of RRT was 3.44 years. Most recipients had residual diuresis of less than 500 ml (64%). Sensitization was observed in 18% of recipients, with 6% being highly sensitized (calculated Panel Reactive Antibody (cPRA) >98%). The mean Estimated Post-Transplant Survival (EPTS) score was 41.96%.
Donors had a mean age of 50.58 years, with 70% being female. Most donors were from donation after brain death (DBD) (58%), and 32% were expanded criteria donors (ECD). The mean Kidney Donor Profile Index (KDPI) was 52.66, and the mean cold ischemia time was 17.30 hours. Full demographic and clinical details are summarized in Table 1.
A semi-targeted metabolomic approach identified 226 polar compounds. The results of the final PLS-DA model are visualized in Figure 1. The scores plot (Figure 1A) illustrates the projection of the observations (patients) onto the two components. These two components contributed to the 26.6% of the total X-variance (Component 1: 17.1%; Component 2: 9.5%). The two groups of subjects show robust clustering based on the two creatinine levels, although partially overlapped. Figure 1B shows the representation of loadings explaining the separation of the two groups of patients. The variables used for the PLS-DA model, along with their chemical formula, spectrometric properties, as well as the standardized coefficients, confidence interval, and associated p-values (Jack-Knifing resampling) for the variable Cr >1.5 mg/dl are shown in Table S1 (Supplementary Material). Those metabolites showing a significant p-value have been colored in red in Figure 1B. We found that the following metabolites presented a significant standardized coefficient: 5-Methylcytosine, 3-Indolepropinoic acid, Homocarnosine, Phenylalanine, Choline, Xanthosine, L-Kynurenine, Kynurenic acid, Lipoic Acid, Histidine, Guaiacol and 3-Methylindole.
The model performance metrics after cross-validation are as follows. The model achieved an AUC of 0.958. The overall accuracy was 0.875, with a sensitivity of 0.8636 and a specificity of 0.8846. The model correctly identified 19 true positives and 23 true negatives, while misclassifying 3 false positives and 3 false negatives. The ROC curve, depicted in Figure 1C, further illustrates the model’s performance, with the curve approaching the top left corner.
4. Discussion
The evolution of kidney graft function in the initial months post-transplant correlates with long-term outcomes. Delayed graft function (DGF) and acute rejection are among the most significant, though not isolated, determinants of renal disease progression [6]. Monitoring involves serial assessments of renal function, urine sediment analysis, proteinuria, antibody measurements, and microbiological tests, with renal biopsy being the most accurate but invasive method [7], leading to a growing interest in identifying non-invasive biomarkers that can predict KT outcomes earlier and more reliably.
Omics technologies, particularly metabolomics, have emerged as promising tools for biomarker discover. In KT, omics studies have primarily aimed to diagnose acute rejection [8,9,10]. However, few studies have examined other events like DGF [11] or overall progression [3]. A notable study by Ihsan Yozgat et al. [2] used untargeted metabolomics of urine samples to develop a PLS-DA model, correlating a panel of marker candidates with serum creatinine levels above 1.5 mg/dl one-year post-transplant, achieving an AUC of 0.9 for the one-week post-transplant model. This study highlighted the use of a metabolite panel for better discrimination but noted the challenge of collecting urine samples from DGF patients.
Our study used semi-targeted plasma metabolomics at one-week post-transplant, employing a precise in-house compound library. Employing UPLC system coupled to a Q-Exactive Plus spectrometer and a PLS-DA model for statistical analysis, we achieved excellent performance metrics with an AUC of 0.958 following cross-validation.
We identified five statistically significant metabolites with negative standardized coefficients, indicating their association with better graft function and suggesting a protective role. These metabolites are 3-methylindole (skatole), guaiacol, histidine, 3-indolepropionic acid, and α-lipoic acid.
3-methylindole, or skatole, is a metabolite derived from tryptophan metabolism by the indole pyruvate pathway facilitated by gut microbiota through the enzyme tryptophan dehydrogenase (TrpD) [12] (Figure 2). Sin-Hyoung Hong et al. demonstrated its protective effects by reducing endoplasmic reticulum stress, oxidative stress, lipogenesis, caspase activity, and apoptosis in hepatocytes [13]. Although its direct effect on the kidney is not established, a review suggests potential benefits on CKD through intestinal homeostasis, due to the link between dysbiosis and CKD [14]. However, high concentrations of skatole are associated with colorectal cancer and pneumotoxicity [15], indicating the need for further investigation.
Guaiacol, or 2-methoxyphenol, is a phenolic compound known for its antioxidant properties, as it can donate electrons and hydrogen atoms to neutralize free radicals and prevent lipid peroxidation [16]. Its antioxidant activity includes reversible inhibition of myeloperoxidase, an enzyme that induces oxidative stress and inflammation, leading to cardiovascular disease complications [17,18]. Although guaiacol’s relationship with renal disease is not well-described, its ability to reduce oxidative stress and inflammation may protect kidney graft function, as suggested by our study.
Histidine is an amino acid with an imidazole side chain that provides proton buffering, metal ion chelation, and antioxidant properties. It scavenges reactive oxygen species (ROS) and reactive nitrogen species (RNS) and sequesters advanced glycation end-products and advanced lipoxidation end-products [19]. Lower levels of histidine are observed in CKD patients [20], and it is used to treat CKD-related anemia [21]. Its protective properties have led to its inclusion in organ preservation solutions like Custodiol®, which is used in our patients.
3-Indolepropionic acid (IPA) is a tryptophan metabolite produced by gut microbiota through the enzyme tryptophanase (TNA) [12] (Figure 2). IPA exhibits potent antioxidant activities, scavenging hydroxyl radicals and improving gut barrier function [22]. It downregulates fibrosis-related genes and inflammatory factors, offering significant renal protection. Additionally, IPA competes with toxic substances like indoxyl sulfate for organic anion transporters, reducing their accumulation in renal tubules and mitigating renal injury [23]. Finally, IPA is recognized as a potential biomarker for protection against CKD [24], and our study associates it with the preventing adverse renal graft outcomes.
α-Lipoic acid is a dithiol compound acting as a cofactor for several enzymes serving as an energy modulator. It exchanges thiol groups with other thiol-containing metabolites, making it a redox modulator and a potent antioxidant by reducing ROS and RNS, chelating metals, and regenerating antioxidants like vitamins C and E. It also has anti-inflammatory activities, targeting NF-κB and decreasing inflammatory cytokines [25]. Its protective effects are documented in various renal diseases, including diabetic nephropathy, sepsis-associated acute kidney failure, nephrotoxicity-induced renal failure, and ischemia-reperfusion (I/R) injury [26]. In I/R injury, α-lipoic acid combats oxidative stress, downregulates Na-K-ATPase and nitric oxide synthase, mitigates neutrophil infiltration, inhibits inflammation, and suppresses endothelin-1 upregulation [27]. It is used as a therapeutic strategy in various solid organ transplants [25] and could serve as a biomarker for protecting against adverse renal graft outcomes.
Conversely, our study revealed seven statistically significant metabolites with positive standardized coefficients, indicating their association with worse kidney graft outcomes. These metabolites are homocarnosine, 5-methylcytosine, xanthosine, choline, phenylalanine, kynurenic acid and L-kynurenine.
Homocarnosine, a dipeptide of gamma-aminobutyric acid and histidine, has been associated with various biological and pathological brain events. Its role in kidney diseases is less studied, though increased levels are observed in diabetic kidney disease compared to those with type 2 diabetes mellitus without nephropathy [28], and in renal tissue after ischemia [29], which may be related to the I/R injury observed in our KT recipients.
5-Methylcytosine (5-mC) is a methylated form of cytosine where a methyl group is attached to carbon at position 5. DNA methylation has been extensively studied in the context of KT and involves adding methyl groups to cytosines in CpG dinucleotides, which cluster in CpG islands, resulting in transcriptional silencing of affected genes [30]. Although methylation is relatively stable, it can be reversed by TET enzymes, converting it to 5-hydroxymethylcytosine in an oxygen-dependent manner. Hypoxia during KT reduces TET activity, leading to 5-mC accumulation and downregulation of genes involved in suppressing kidney fibrosis and injury [31]. This hypermethylation can predict chronic allograft injury [31], as observed in our study, where elevated 5-mC levels predicted worse outcomes at six months.
Xanthosine is a purine nucleoside identified as a prognostic marker for CKD in several studies, often used alongside other metabolites, such as kynurenic acid, kynurenine and choline, which was also found in our study, to estimate CKD progression [32,33,34]. The mechanism by which xanthosine increases CKD risk and its relationship with KT remains unclear. However, purine metabolism dysregulation in CKD, nucleotide breakdown [35] in I/R injury, and the association of other purine metabolites like hypoxanthine as markers of ischemia [36] could be related. An in vitro study showed that hypoxia significantly decreased purine nucleotide phosphorylase activity [37], the enzyme required for converting xanthosine to xanthine, possibly explaining xanthosine accumulation in these patients.
Choline, an essential vitamin found in phospholipids, is involved in methylation reactions like converting homocysteine to methionine via its oxidation to betaine. It is linked to CKD progression through its conversion to trimethylamine-N-oxide, promoting renal fibrosis [34,38]. However, its association with KT appears to be more closely related to I/R injury. Choline is a marker of tissue ischemia linked to phospholipid degradation, exhibiting a biphasic release pattern with a peak immediately following global ischemia and a delayed phase during reperfusion [39]. Lindeman J et al. observed choline uptake in kidney graft recipients from living or deceased donors without DGF, while those with DGF showed choline release, partially masked by its conversion to betaine, potentially associated with the role of betaine in methylation processes occurring in these patients [40]. These findings align with our study, as DGF is related to posterior renal function and the deleterious effects of elevated choline levels on long-term renal function.
Phenylalanine is an essential amino acid that serves as a precursor for various compounds. Its primary metabolic pathway is the conversion to tyrosine, which can then follow multiple metabolic routes, including the synthesis of catecholamines, melanin, and energy metabolism through its deamination and conversion to acetoacetate and fumarate, intermediates of the Krebs cycle. The kidney is the major producer of tyrosine in the body, as it converts phenylalanine to tyrosine via phenylalanine hydroxylation. Consequently, impaired renal function leads to the accumulation of phenylalanine and a deficiency of tyrosine [41], both linked with CKD progression and fibrosis [42] due to their roles in energy metabolism. In KT, I/R injury decreases phenylalanine hydroxylase activity, leading to phenylalanine buildup [43] and poorer graft outcomes.
The kynurenine pathway (KP) is the main route for tryptophan catabolism, essential for energy metabolism and immune modulation (Figure 2). Excessive activation of this pathway is linked to various kidney diseases, including AKI, CKD, KT progression, I/R injury, infections in KT, and graft rejection. Elevation of these metabolites is linked to inflammation, with pro-inflammatory cytokines like IFN-γ upregulating indoleamine 2,3-dioxygenase (IDO), the rate-limiting enzyme of KP, and downregulate enzymes such as kynureninase and quinolinate phosphoribosyltransferase, leading to the accumulation of KP intermediates and disrupting de novo NAD+ biosynthesis [44,45]. Elevated KP metabolites, such as kynurenine and kynurenic acid (KYNA) correlate with poor renal outcomes and renal fibrosis [34,46]. Notably, kynurenine had the highest score as a biomarker for CKD in a large population analysis [47].
In KT, increased tryptophan degradation and higher kynurenine levels correlate with worse kidney function [48], can predict graft rejection [49], and are associated with infections due to the inflammation present in both conditions, raising questions about their specificity as rejection markers. A study by Dharnidharka et al. [50] found that the serum kynurenine/tryptophan (KYN/TRP) ratio was higher in acute graft rejection. However, peripheral blood CD4-ATP levels were useful in the differential diagnosis, being lower in the infection group. Our study supports the importance of monitoring KP metabolites like Kynurenine and KYNA as potential prognostic biomarkers and therapeutic targets in CKD and KT patients.
This study has several limitations. Firstly, the small sample size, due to the high cost and technical complexity of metabolomic studies, limits the ability to perform subgroup analyses, such as distinguishing between recipients of brain-dead versus cardiac-death donors, with the aim of not losing statistical power. Secondly, metabolomic studies are inherently exploratory and hypothesis-generating, serving as a foundation for future, more comprehensive research that requires validation in larger cohorts. Thirdly, although the long-term evolution of the renal graft has been correlated in other studies with renal function at six months, the short follow-up time in our study does not allow us to ensure this long-term evolution, so further investigation in this aspect would be interesting. Lastly, the use of a semi-targeted approach with an in-house library of compounds to limit irrelevant results and improve their characterization may have limited the discovery of other unknown metabolites.
5. Conclusions
In conclusion, our study reveals the important role of using biomarkers in predicting KT outcomes. We identified five protective metabolites that predominantly exhibit antioxidant and anti-inflammatory properties in other studies, which could be used as therapeutic targets in KT recipients. Additionally, this study highlights the significant relationship between metabolites from tryptophan metabolism and the prediction of KT evolution, paving the way for further research, therapeutic strategies, and improved and earlier patient management.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Table S1: Compounds used for the final PLS-DA model, along with their chemical formula, spectrometric properties, the standardized coefficients, confidence interval, and associated p-values (Jack-Knifing resampling) for the variable Cr >1.5 mg/dl
Author Contributions
Conceptualization, I.V.-B., M. P.-F., I. B.-C. and J. H.-J; methodology, I.V.-B., M.I.R.-M., M.F.-B., M.M.-E., J.L.A and A.B.-T; software, M.I.R.-M, J.L.A and A.B.-T.; validation, M.I.R.-M, J.L.A and A.B.-T; formal analysis, I.V.-B., M.I.R.-M, J.L.A and A.B.-T; investigation, I.V.-B.; writing—original draft preparation, I.V.-B and M. P.-F; writing—review and editing, I.V.-B, M. P.-F, I. B.-C. and J. H.-J; visualization, I.V.-B.; supervision, P. G.-C., J.E.-R., A.V.-G., D.R.-O., M.R.-C. and I.B.-C.; project administration, P. G.-C., J.E.-R., A.V.-G., D.R.-O., M.R.-C. I.B.-C. and J.H.-J. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of La Fe Health Research Institute (protocol code 2022-678-1, approved on 30 September 2022).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data on which the article is based are available as Supplementary Materials.
Acknowledgments
We sincerely thank the patients who participated in this study; their collaboration was essential for the success of this research. We also extend our gratitude to the nursing staff and the Nephrology residents for their unwavering dedication and support throughout the process. Their professionalism and commitment were invaluable. Finally, we thank the Big Data AI and Biostatistics Platform team for their expertise and technical support, which were crucial for the data analysis and the overall success of this study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- GBD Chronic Kidney Disease Collaboration. Global, regional, and national burden of chronic kidney disease, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2020, 395, 709–733. [Google Scholar] [CrossRef]
- Yozgat I, Cakır U, Serdar M.A., et al. Longitudinal non-targeted metabolomic profiling of urine samples for monitoring of kidney transplantation patients. Ren Fail. 2024, 46, 2300736. [Google Scholar] [CrossRef]
- Stanimirova I, Banasik M, Ząbek A, et al. Serum metabolomics approach to monitor the changes in metabolite profiles following renal transplantation. Sci Rep. 2020, 10, 17223. [Google Scholar] [CrossRef]
- Peris-Fernández M, Roca-Marugán M, Amengual JL, et al. Uremic Toxins and Inflammation: Metabolic Pathways Affected in Non-Dialysis-Dependent Stage 5 Chronic Kidney Disease. Biomedicines. 2024, 12, 607. [Google Scholar]
- Hariharan S, Mcbride M.A., Cherikh W.S., Tolleris C.B., Bresnahan BA, Johnson CP. Post-transplant renal function in the first year predicts long-term kidney transplant survival. Kidney International. 2002, 62, 311–318. [Google Scholar] [CrossRef]
- Legendre C, Canaud G, Martinez F. Factors influencing long-term outcome after kidney transplantation. Transpl Int. 2014, 27, 19–27. [Google Scholar] [CrossRef]
- Josephson, MA. Monitoring and Managing Graft Health in the Kidney Transplant Recipient. Clinical Journal of the American Society of Nephrology. 2011, 6, 1774. [Google Scholar] [CrossRef]
- Zhao X, Chen J, Ye L, Xu G. Serum metabolomics study of the acute graft rejection in human renal transplantation based on liquid chromatography-mass spectrometry. J Proteome Res. 2014, 13, 2659–2667. [Google Scholar] [CrossRef]
- Mao Y.Y., Bai J.Q., Chen J.H., et al. A pilot study of GC/MS-based serum metabolic profiling of acute rejection in renal transplantation. Transpl Immunol. 2008, 19, 74–80. [Google Scholar] [CrossRef]
- Blydt-Hansen T.D., Sharma A, Gibson I.W., et al. Urinary Metabolomics for Noninvasive Detection of Antibody-Mediated Rejection in Children After Kidney Transplantation. Transplantation. 2017, 101, 2553–2561. [Google Scholar] [CrossRef]
- Kostidis S, Bank J.R., Soonawala D, et al. Urinary metabolites predict prolonged duration of delayed graft function in DCD kidney transplant recipients. Am J Transplant. 2019, 19, 110–122. [Google Scholar] [CrossRef]
- Paeslack N, Mimmler M, Becker S, et al. Microbiota-derived tryptophan metabolites in vascular inflammation and cardiovascular disease. Amino Acids. 2022, 54, 1339–1356. [Google Scholar] [CrossRef]
- Hong S.H., Hong Y, Lee M, Keum B.R., Kim G.H. Natural Product Skatole Ameliorates Lipotoxicity-Induced Multiple Hepatic Damage under Hyperlipidemic Conditions in Hepatocytes. Nutrients. 2023, 15, 1490. [Google Scholar] [CrossRef]
- Madella A.M., Van Bergenhenegouwen J, Garssen J, Masereeuw R, Overbeek SA. Microbial-Derived Tryptophan Catabolites, Kidney Disease and Gut Inflammation. Toxins. 2022, 14, 645. [Google Scholar] [CrossRef]
- Zgarbová E, Vrzal R. Skatole: A thin red line between its benefits and toxicity. Biochimie. 2023, 208, 1–12. [CrossRef]
- Galano A, León-Carmona J.R., Alvarez-Idaboy J.R. Influence of the Environment on the Protective Effects of Guaiacol Derivatives against Oxidative Stress: Mechanisms, Kinetics, and Relative Antioxidant Activity. J Phys Chem B. 2012, 116, 7129–7137. [Google Scholar] [CrossRef]
- Premkumar J, Sampath P, Sanjay R, Chandrakala A, Rajagopal D. Synthetic Guaiacol Derivatives as Promising Myeloperoxidase Inhibitors Targeting Atherosclerotic Cardiovascular Disease. ChemMedChem. 2020, 15, 1187–1199. [Google Scholar] [CrossRef]
- Aqeel M.T., Rahman N ur, Khan A ullah, et al. Cardioprotective effect of 2-methoxy phenol derivatives against oxidative stress-induced vascular complications: An integrated in vitro, in silico, and in vivo investigation. Biomedicine & Pharmacotherapy 5240, 165, 115240.
- Holeček, M. Histidine in Health and Disease: Metabolism, Physiological Importance, and Use as a Supplement. Nutrients. 2020, 12, 848. [Google Scholar] [CrossRef]
- Watanabe M, Suliman ME, Qureshi A.R., et al. Consequences of low plasma histidine in chronic kidney disease patients: associations with inflammation, oxidative stress, and mortality1. The American Journal of Clinical Nutrition. 2008, 87, 1860–1866. [CrossRef]
- Vera-Aviles M, Vantana E, Kardinasari E, Koh N.L., Latunde-Dada G.O. Protective Role of Histidine Supplementation Against Oxidative Stress Damage in the Management of Anemia of Chronic Kidney Disease. Pharmaceuticals (Basel). 2018, 11, 111. [CrossRef]
- Jiang H, Chen C, Gao J. Extensive Summary of the Important Roles of Indole Propionic Acid, a Gut Microbial Metabolite in Host Health and Disease. Nutrients. 2022, 15, 151. [Google Scholar] [CrossRef]
- Yisireyili M, Takeshita K, Saito S, Murohara T, Niwa T. Indole-3-propionic acid suppresses indoxyl sulfate-induced expression of fibrotic and inflammatory genes in proximal tubular cells. Nagoya J Med Sci. 2017, 79, 477–486. [Google Scholar]
- Sun CY, Lin CJ, Pan HC, et al. Clinical association between the metabolite of healthy gut microbiota, 3-indolepropionic acid and chronic kidney disease. Clinical Nutrition. 2019, 38, 2945–2948. [Google Scholar] [CrossRef]
- Ambrosi N, Guerrieri D, Caro F, et al. Alpha Lipoic Acid: A Therapeutic Strategy that Tend to Limit the Action of Free Radicals in Transplantation. International Journal of Molecular Sciences. 2018, 19, 102. [Google Scholar] [CrossRef]
- Kamt, S.F. , Liu J, Yan L.J. Renal-Protective Roles of Lipoic Acid in Kidney Disease. Nutrients. 2023, 15, 1732. [Google Scholar] [CrossRef]
- Ding Y, Zhang Y, Zhang W, Shang J, Xie Z, Chen C. Effects of Lipoic Acid on Ischemia-Reperfusion Injury. Oxid Med Cell Longev. 2021, 2021, 5093216. [CrossRef]
- Wang J, Zhou C, Zhang Q, Liu Z. Metabolomic profiling of amino acids study reveals a distinct diagnostic model for diabetic kidney disease. Amino Acids. 2023, 55, 1563–1572. [Google Scholar] [CrossRef]
- Fox B.M., Gil H.W., Kirkbride-Romeo L, et al. Metabolomics assessment reveals oxidative stress and altered energy production in the heart after ischemic acute kidney injury in mice. Kidney Int. 2019, 95, 590–610. [CrossRef]
- Xiang X, Zhu J, Dong G, Dong Z. Epigenetic Regulation in Kidney Transplantation. Front Immunol. 2022, 13, 861498. [CrossRef]
- Heylen L, Thienpont B, Naesens M, et al. Ischemia-Induced DNA Hypermethylation during Kidney Transplant Predicts Chronic Allograft Injury. Journal of the American Society of Nephrology. 2018, 29, 1566. [Google Scholar] [CrossRef]
- Chen Y, Zelnick L.R., Wang K, et al. Kidney Clearance of Secretory Solutes Is Associated with Progression of CKD: The CRIC Study. J Am Soc Nephrol. 2020, 31, 817–827. [CrossRef]
- Granda M.L., Zelnick L.R, Prince D.K., Hoofnagle A, Young B.A., Kestenbaum B.R. Tubular Secretion and Estimated GFR Decline in the Jackson Heart Study. Kidney Int Rep. 2022, 7, 2668–2675. [CrossRef]
- Rhee E.P., Clish C.B., Ghorbani A, et al. A Combined Epidemiologic and Metabolomic Approach Improves CKD Prediction. J Am Soc Nephrol. 2013, 24, 1330–1338. [CrossRef]
- Saeb-Parsy K, Martin J.L., Summers D.M., Watson C.J.E, Krieg T, Murphy M.P. Mitochondria as Therapeutic Targets in Transplantation. Trends Mol Med. 2021, 27, 185–198.
- Farthing D.E., Farthing C.A., Xi L.Inosine and hypoxanthine as novel biomarkers for cardiac ischemia: From bench to point-of-care. Exp Biol Med (Maywood). 2015, 240, 821–831. [CrossRef]
- Rivera-Pérez C, Gaxiola-Robles R, Olguín-Monroy N.O., et al.Effect of hypoxia on purine metabolism in human skeletal muscle cells. Biotecnia. 2021, 23, 141–148.
- Zhang W, Miikeda A, Zuckerman J, et al. Inhibition of microbiota-dependent TMAO production attenuates chronic kidney disease in mice. Sci Rep. 2021, 11, 518. [Google Scholar] [CrossRef]
- Brühl A, Hafner G, Löffelholz K. Release of choline in the isolated heart, an indicator of ischemic phospholipid degradation and its protection by ischemic preconditioning: no evidence for a role of phospholipase D. Life Sci. 2004, 75, 1609–1620. [Google Scholar] [CrossRef]
- Lindeman J.H., Wijermars L.G., Kostidis S, et al.Results of an explorative clinical evaluation suggest immediate and persistent post-reperfusion metabolic paralysis drives kidney ischemia reperfusion injury. Kidney Int. 2020, 98, 1476–1488. [CrossRef]
- Møller N, Meek S, Bigelow M, Andrews J, Nair K.S. The kidney is an important site for in vivo phenylalanine-to-tyrosine conversion in adult humans: A metabolic role of the kidney. Proceedings of the National Academy of Sciences. 2000, 97, 1242–1246. [CrossRef]
- Kopple, J.D. Phenylalanine and tyrosine metabolism in chronic kidney failure. J Nutr. 2007, 137 (6 Suppl 1), 1586S-1590S; discussion 1597S-1598S. [Google Scholar] [CrossRef]
- Supavekin S, Zhang W, Kucherlapati R, Kaskel F.J, Moore L.C., Devarajan P. Differential gene expression following early renal ischemia/reperfusion. Kidney Int. 2003, 63, 1714–1724. [CrossRef]
- Wee H.N., Liu J.J., Ching J, Kovalik J.P., Lim S.C. The Kynurenine Pathway in Acute Kidney Injury and Chronic Kidney Disease. Am J Nephrol. 2021, 52, 771–787. [CrossRef]
- Zulpaite R, Miknevicius P, Leber B, Strupas K, Stiegler P, Schemmer P. Tryptophan Metabolism via Kynurenine Pathway: Role in Solid Organ Transplantation. International Journal of Molecular Sciences. 2021, 22, 1921. [Google Scholar] [CrossRef]
- Goek O.N., Prehn C, Sekula P, et al. Metabolites associate with kidney function decline and incident chronic kidney disease in the general population. Nephrol Dial Transplant. 2013, 28, 2131–2138. [CrossRef]
- Silva, R.E., Baldim J.L., Chagas-Paula D.A., et al. Predictive metabolomic signatures of end-stage renal disease: A multivariate analysis of population-based data. Biochimie.
- Vavrincova-Yaghi D, Seelen M.A., Kema I.P., et al. Early Posttransplant Tryptophan Metabolism Predicts Long-term Outcome of Human Kidney Transplantation. Transplantation. 2015, 99, e97–e104. [CrossRef]
- Lahdou I, Sadeghi M, Daniel V, et al. Increased pretransplantation plasma kynurenine levels do not protect from but predict acute kidney allograft rejection. Hum Immunol. 2010, 71, 1067–1072. [Google Scholar] [CrossRef]
- Dharnidharka, V.R, Al Khasawneh E, Gupta S, et al. Verification of association of elevated serum IDO enzyme activity with acute rejection and low CD4-ATP levels with infection. Transplantation. 2013, 96, 567–572. [CrossRef]
Figure 1.
Scores plot of PLS-DA based on metabolomics. (A). The samples are colored based on the two levels, with grey representing creatinine ≤1.5 mg/dl and black representing creatinine >1.5 mg/dl. The ellipses around each cluster represent the 95% confidence regions, indicating the spread and overlap of each group. (B) Loading plot of PLS-DA showing the contribution of the 22 selected metabolites (whose VIP scores were over 1.5 in the first PLS-DA model) to the two categories. Each point represents a metabolite, and its position indicates its influence on the two components. Red points indicate significant p-values for the variable (Cr >1.5 mg/dl). (C) Receiver Operating Characteristics (ROC) curve illustrating the performance of the LOOCV of the PLS-DA model in distinguishing patients with Creatinine ≤ 1.5 mg/dl or >1.5 mg/dl six months after the KT. The diagonal dashed line represents the baseline performance of a random classifier. Dot point shows the optimal cut off point based on the maximal specificity and sensibility, which corresponds to 0.5.
Figure 1.
Scores plot of PLS-DA based on metabolomics. (A). The samples are colored based on the two levels, with grey representing creatinine ≤1.5 mg/dl and black representing creatinine >1.5 mg/dl. The ellipses around each cluster represent the 95% confidence regions, indicating the spread and overlap of each group. (B) Loading plot of PLS-DA showing the contribution of the 22 selected metabolites (whose VIP scores were over 1.5 in the first PLS-DA model) to the two categories. Each point represents a metabolite, and its position indicates its influence on the two components. Red points indicate significant p-values for the variable (Cr >1.5 mg/dl). (C) Receiver Operating Characteristics (ROC) curve illustrating the performance of the LOOCV of the PLS-DA model in distinguishing patients with Creatinine ≤ 1.5 mg/dl or >1.5 mg/dl six months after the KT. The diagonal dashed line represents the baseline performance of a random classifier. Dot point shows the optimal cut off point based on the maximal specificity and sensibility, which corresponds to 0.5.
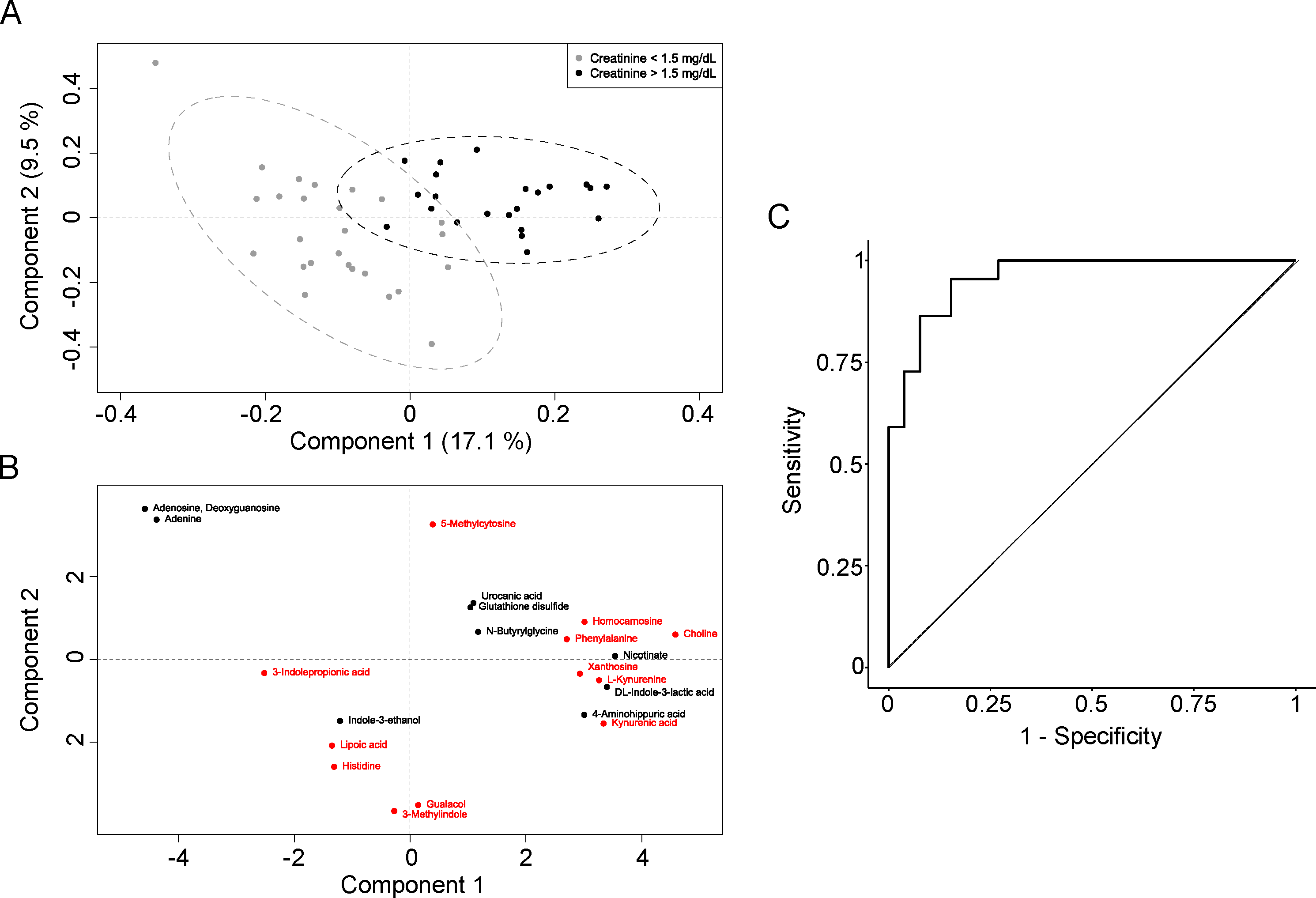
Figure 2.
Tryptophan Metabolism Pathways and Associated Metabolites with Post-Transplant Renal Function. This diagram illustrates the key pathways of tryptophan metabolism: the Kynurenine Pathway, Indole Pyruvate Pathway, and Serotonin Pathway. Metabolites marked in red are associated with an increased risk of having a serum creatinine level greater than 1.5 mg/dL at six months post-transplant. Metabolites marked in blue are associated with a reduced risk (protective effect) of having a serum creatinine level greater than 1.5 mg/dL at six months post-transplant. Metabolites marked with an asterisk (*) denote statistically significant associations. ArAT: Aromatic amino acid transaminase, IDO: Indolamine-2,3-dioxygenase, TDO: Tryptophan 2,3-Dioxygenase, TNA: Tryptophanase, TpH1: Tryptophan hydroxylase 1, TrpD: Tryptophan dehydrogenase.
Figure 2.
Tryptophan Metabolism Pathways and Associated Metabolites with Post-Transplant Renal Function. This diagram illustrates the key pathways of tryptophan metabolism: the Kynurenine Pathway, Indole Pyruvate Pathway, and Serotonin Pathway. Metabolites marked in red are associated with an increased risk of having a serum creatinine level greater than 1.5 mg/dL at six months post-transplant. Metabolites marked in blue are associated with a reduced risk (protective effect) of having a serum creatinine level greater than 1.5 mg/dL at six months post-transplant. Metabolites marked with an asterisk (*) denote statistically significant associations. ArAT: Aromatic amino acid transaminase, IDO: Indolamine-2,3-dioxygenase, TDO: Tryptophan 2,3-Dioxygenase, TNA: Tryptophanase, TpH1: Tryptophan hydroxylase 1, TrpD: Tryptophan dehydrogenase.
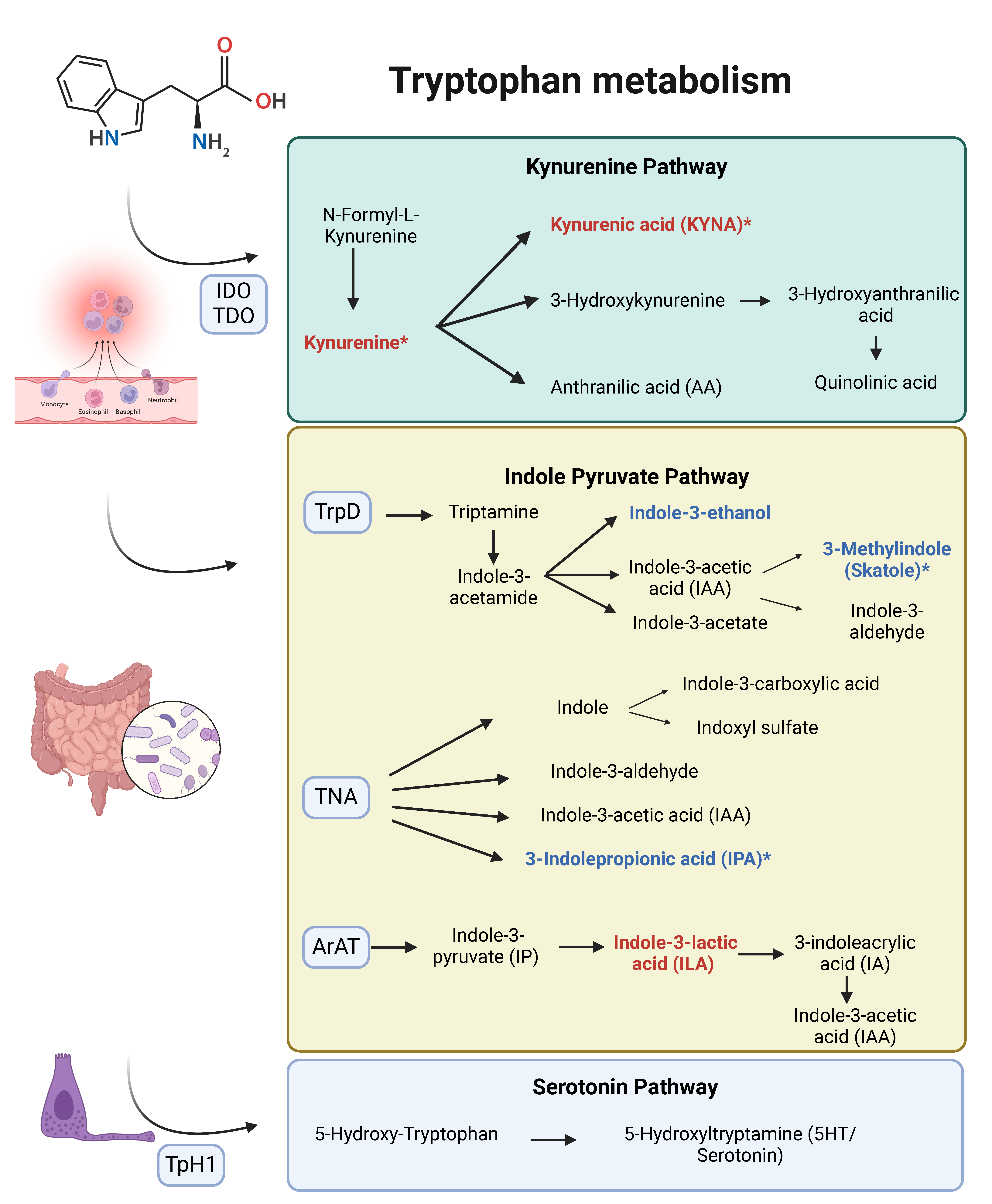

Table 1.
Demographic and clinical characteristics of the sample.
| Kidney transplant recipient | |
|---|---|
| Variable | Mean/Frequency |
| Age (years) (mean ± SD) | 53.98 ± 10.94 |
| Gender, n (%) | Male: 35 (70%) Female: 15 (30%) |
| Race, n (%) | Caucasian: 47 (94%) African American: 3 (6%) |
| Blood type, n (%) | 0+: 18 (36%) 0-: 1 (2%) A+: 19 (38%) A-: 6 (12%) B+: 5 (10%) B- 0 (0%). AB+: 1 (2%) AB-: 0 (0%) |
| Hypertension, n (%) | 41 (82%) |
| Type 2-diabetes, n (%) | 8 (16%) |
| Dyslipidemia, n (%) | 35 (70%) |
| BMI (mean ± SD) | 26.58 (3.89) |
| Obesity, n (%) | Underweight: 0 (0%) Normal weight: 18 (36%) Overweight: 18 (36%) Obesity: 14 (28%) |
| Hyperuricemia, n (%) | 17 (34%) |
| Smoking status, n (%) | Non-smoker: 21 (42%) Former smoker: 20 (40%) Current smoker: 9 (18%) |
| Physical activity, n (%) | Sedentary: 39 (78%) Moderately active: 5 (10%) Very active: 6 (12%) |
| Etiology of chronic kidney disease, n (%) | Glomerulonephritis: 5 (10%) Chronic pyelonephritis/tubulointerstitial: 7 (14%) Diabetes mellitus: 6 (12%) Hypertension/vascular diseases: 3 (6%) Hereditary/familial: 13 (26%) Systemic diseases: 4 (8%) Unclassified: 12 (24%) |
| Renal replacement therapy, n (%) | Hemodialysis: 37 (74%) Peritoneal dialysis: 13 (26%) |
| Time on dialysis (years), (mean ± SD) | 3.44 ± 2.32 |
| Residual diuresis, n (%) | <500 ml: 32 (64%) 500-1000 ml: 7 (14%) >1000 ml: 11 (22%) |
| Heart failure, n (%) | 2 (4%) |
| Coronary artery disease, n (%) | 7 (14%) |
| Vascular disease, n (%) | 4 (18%) |
| Previous transplant, n (%) | 6 (12%) |
| Transfusions history, n (%) | 17 (34%) |
| Pregnancy history, n (%) | 12 (24%) |
| Sensitization, n (%) | No: 41 (82%) < 98% PRAc: 6 (12%) >98% PRAc (PATHI): 3 (6%) |
| EPTS, (mean ± SD) | 41.96 ± 26.94 |
| Kidney Donor | |
| Variable | Mean/Frequency |
| Age, (mean ± SD) | 50.58 ± 16.30 |
| Gender, n (%) | Male: 15 (30%) Female: 35 (70%) |
| Donor type, n (%) | DBD: 29 (58%) DCD: 21 (42%) |
| Hypertension, n (%) | 14 (28%) |
| Diabetes mellitus, n (%) | 9 (18%) |
| BMI, (mean ± SD) | 26.29 ± 5.85 |
| Donor AKI, n (%) | 2 (4%) |
| Expanded criteria donor (EC), n (%) | 16 (32%) |
| KDPI, (mean ± SD) | 52.66 ± 28.72 |
| Transplant process | |
| Variable | Mean/Frequency |
| Cold ischemia time, (mean ± SD) | 17.30 ± 4.58 |
| Mismatch 6/6, (mean ± SD) | 4.3 ± 1.18 |
| Mismatch 10/10, (mean ± SD) | 7.2 ± 1.82 |
| One-week events | |
| Variable | Mean/Frequency |
| Overdose of calcineurin inhibitor, n (%) | 30 (60%) |
| Urinary infection, n (%) | 11 (22%) |
| Graft rejection, n (%) | 3 (6%) |
| Graft function, n (%) | Immediate graft function: 10 (20%) Slow graft function: 13 (26%) Delayed graft function: 27 (54%) |
| Six-month post-transplant events (Excluding week 1) | |
| Variable | Mean/Frequency |
| Graft rejection, n (%) | 1 (2%) |
| Urinary infection, n (%) | 18 (36%) |
| CMV infection, n (%) | 3 (6%) |
| BK infection, n (%) | Yes (viremia): 5 (10%) Nephropathy: 0 (0%) |
| MACE | 6 (12%) |
AKI: Acute Kidney Injury. BMI: Body Mass Index. cPRA: calculated Panel Reactive Antibody. EPTS (Estimated Post Transplant Survival). KDPI: Kidney Donor Risk Index. MACE: Major Adverse Cardiovascular Events. PATHI: National Plan for Access to Kidney Transplantation for Highly Sensitized Patients. SD: Standard Deviation.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



