
Submitted:
02 October 2024
Posted:
03 October 2024
You are already at the latest version
Abstract
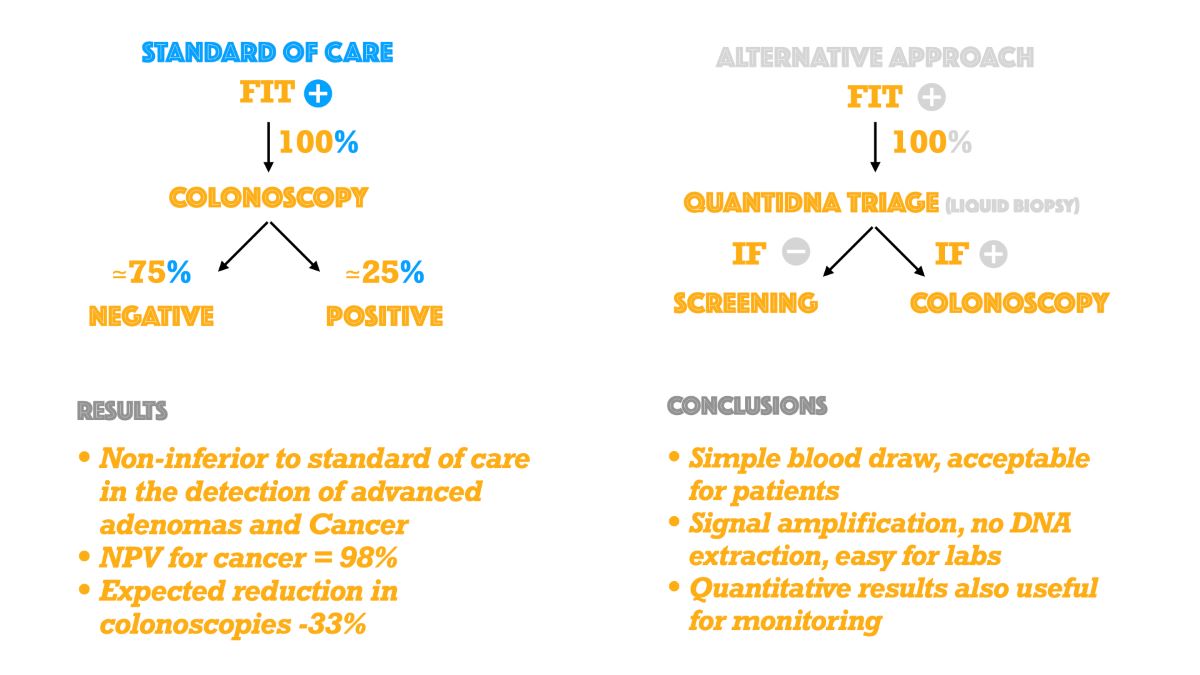
Background: Colorectal Cancer screening programs are effective in reducing incidence and mor-tality. In Europe, every FIT+ patient is referred to colonoscopy. Available data shows that ~75.0% of these patients are negative. It is desirable to select patients at greater risk of having a positive colonoscopy.
Methods: 711 subjects, aged 50-74, attending the screening program of ASL-NA-3-SUD (Na-ples, Italy), were enrolled in a cross-sectional study to evaluate the performance of QuantiDNA™ test and non-inferiority of an alternative approach (AAP). This evaluation is based on FIT+ and QuantiDNA™+ patients referred to colonoscopy, compared to Standard of Care (SOC), colon-oscopy following a FIT+ test alone. A non-inferiority margin for Colorectal Neoplasia (CN) and Advanced Adenomas (AA) was set at -10% and at -3.8% for CRC.
Results: The odds ratio was 1.76 (p-value= 0.009). The detection rate of AAP was 15.9% for colorectal neoplasia (CN), 13.0% for advanced adenoma (AA), and 3.0% for CRC. The risk dif-ference between AAP and SOC was -5.07% (95% C.I -9.23, -0.90) for CN, -4.02% (95% C.I. -7.89, -0.16) for AA, and -1.04% (95% C.I. -3.16, 1.07) for CRC. This data suggests that AAP is non-inferior to SOC for detecting CN, AA, and CRC. The expected decrease in colonoscopies is 33.4%.
Conclusions: The QuantiDNA™ test is straightforward, non-invasive, and well-tolerated. Data from this study indicates it is effective in the reduction of the need for colonoscopy examina-tions (-33.4%) and is non-inferior to SOC in the detection of significant colorectal lesions.
Keywords:
colorectal cancer screning
; colorectal cancer
; genetic testing
| GLOSSARY OF TERMS |
| Sensitivity (True Positive Rate): the proportion of subjects with disease, who have a positive testDetection rate: the proportion of subjects enrolled who have a true positive testOdds ratio (OR): Odds ratio was calculated according to: (TP*TN)/(FP*FN), where TP= True Positives; TN=True Negatives; FN=False Negatives; FP=False PositivesSpecificity (True Negative Rate): the proportion of subjects without disease, who have a negative testPositive Predictive Value (PPV): the proportion of subjects with disease among those with a positive testNegative Predictive Value (NPV): the proportion of subjects without disease among those with a negative testPositivity Rate: the proportion of subjects enrolled who have a positive testNon-Inferiority Margin (NIM): The largest clinically acceptable difference between a new treatment and an active comparator.Triage: The process of prioritizing patients for treatment based on the urgency of their needs.False Positive Rate (1-Specificity): Proportion of subjects without disease, who have a positive testFalse Negative Rate (1-Sensitivity): Proportion of subjects with disease, who have a negative testCN: colorectal neoplasia. (Abnormal growth or mass in the colon or rectum. It includes advanced adenomas, high -risk sessile serrated lesions and colorectal cancers)AA: advanced adenoma.NAA: non-advanced adenoma.CRC: colorectal cancer.SOC: standard of care , or immediate colonoscopy following a FIT+ test.AAP: alternative approach., or colonoscopy iff both FIT+ and QuantiDNA+. |
1. Introduction
Colorectal Cancer (CRC) is the third most common cancer worldwide, accounting for approximately 10% of all cancer cases, is the second leading cause of cancer-related deaths worldwide. Most cases occur in people aged 50 and above and primarily men. In 2020, more than 1.9 million new cases of CRC and more than 930,000 deaths due to CRC were estimated worldwide. (World Health Organization, July 2023) In the recent era of precision medicine advanced CRC patients may benefit from target treatment based on monoclonal antibodies (mAB) against Epidermal Growth Factor Receptor (EGFR) extracellular domain [22]. CRC patients are often diagnosed in an advanced stage, drastically affecting clinical outcome, despite a rapidly evolving scenario of promising target drugs [3]. Organized screening programs have been implemented for the early detection of pre-cancerous lesions in Europe and other parts of the world. Most of them are based on the biennial use of the fecal immunochemical test (FIT) and/or its older version, the fecal occult blood test (FOBT) for people of both genders, aged 50-69 or 50-74 [4]. Screening programs are effective in reducing cancer-related mortality, yet depend largely on participation, which varies between 40-85%, according to different countries. [4] Current screening protocols require immediate referral to colonoscopy, following a FIT positive (Fit+) or FOBT positive (FOBT+) test. However, most of these colonoscopies are negative. [17] For example, in 2021, the Italian CRC screening program screened >2,000,000 individuals and performed about 100,000 colonoscopies, of which some 19.0% were positive for advanced adenomas or worse, and, conversely, >80% were negative [17]. Many colonoscopies are also performed outside the organized screening programs. This may lead to unnecessary discomfort for patients and a work overload for healthcare facilities, not to mention increasing waiting lists. An increased risk of CRC has been observed in association with the number of days to colonoscopy following a FIT+ test (OR = 1.76 for > 180 days of waiting time). [17]
In this scenario, minimally invasive and technically reliable screening tools are currently under investigation. [23] Over the last thirty-five years, the role of circulating cell-free DNA (cfDNA) from liquid biopsy specimens demonstrated a pivotal role for molecular evaluation of CRC patients [1,21] and other neoplastic diseases[2,5]. Particularly, circulating tumor DNA (ctDNA) consisting in a small fraction of cfDNA, is released by tumor cells in blood stream. Plasma is considered a dynamic, reproducible and clinically specific source of nucleic acids capable of integrating tissue-based molecular analysis of predictive biomarkers in clinical practice [23]. Several authors have focused on the detection of mutations in late-stage cancers. In this study we investigated the role of long fragments of cfDNA [1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21]) with a view to establish their utility in the selection of patients at the greatest risk of returning a positive colonoscopy, following a FIT+ (or FOBT+) test adopting QuantiDNA™ test (DiaCarta Inc., Pleasanton (CA), an assay designed to detect total cfDNA and its long fragments in plasma, in the triage of FIT+ patients. This process is commonly known as triage [3], a term widely used in military and emergency medicine and cervical or other screening programs [18] to select those persons of highest priority. In a FIT+ patients triage setting, we aimed to reduce the number of negative colonoscopies, without causing unnecessary harm to the patients, by maximizing the assay sensitivity. We compared two different approaches: 1) SOC, including immediate colonoscopy after a FIT+ (or FOBT+) test; 2) AAP, colonoscopy following both FIT+ (or FOBT+) and cfDNA+ tests.
2. Materials and Methods
2.1. Study Design
During the period 2019-2022, 711 individuals of both genders, aged 50-74 (Table 1 and Table 2; Supplementary Information), participating in a CRC screening program organized by the ASL NA 3 SUD, a public healthcare company operating in the district of Naples (Italy), were enrolled in a cross-sectional study aimed at investigating the possible role of QuantiDNA™ test (DiaCarta Inc., Pleasanton (CA), an assay designed to detect total cfDNA and its long fragments in plasma, in the triage of FIT+ patients.
According to the study protocol, all participants with a FIT+ (or FOBT+) test, willing to sign an informed consent and eligible for the study, received both the QuantiDNA™ test and a colonoscopy. Data analysis strategy ensured a comparison between SOC and AAP. The study was approved by the Ethical Committee in December 2018.
Statistical analysis was conducted internally and independently validated by TechnoSTAT Clinical Services (Israel). The database was provided and held by Mednet, Inc. (MN, USA).
The endoscopy unit of ASL NA 3 SUD served as a recruitment center. The Molecular Pathology Laboratory of the Department of Public Health of the Federico II University of Naples (Naples, Italy) performed whole blood specimens processing. Plasma samples were shipped to the CLIA laboratory of DiaCarta, Inc. (Pleasanton, CA, USA) for final QuantiDNA™ testing.
All colonoscopies were performed by the endoscopy unit of ASL NA 3 SUD, while histopathology for positive colonoscopies was provided by the anatomic pathology laboratory of ASL NA 3 SUD. Patients with a final diagnosis of either cancer or cancerized advanced adenoma were referred to surgery.
2.2. Study Population
Subjects with a FIT+ test in the previous 3 months and plans to undergo a colonoscopy within 60 days of signing the informed consent were enrolled (Table 1 and Table 2). The following exclusion criteria applied:
Previous history of colorectal cancer
Overt rectal bleeding within 60 days of enrollment
Personal history of inflammatory bowel disease (IBD), including Crohn’s disease and chronic ulcerative colitis
Personal or family history of familial adenomatous polyposis (FAP)
Personal or family history of hereditary non-polyposis colorectal cancer (HNPCC) or Lynch’s syndrome
Personal history of other hereditary cancer syndromes (see Supplementary Information for details)
Participation in a clinical trial with an investigational medicinal product within the previous 90 days
Pregnancies;
Discontinuation/withdrawal criteria also applied (i.e., personal reasons, loss to follow-up). (Table 1)
2.3. Technical Workflow
All enrolled subjects underwent an eligibility check (subject information, visit information, inclusion/exclusion criteria, demographics, medical history, subject history, substance use, vital signs, family history) (Table 3 -4-5-7-8; Supplementary Information). A total of n=20 ml of entire blood specimens was collected for molecular analysis. In particular, 2 ml of peripheral blood were used for cfDNA evaluation. Whole blood samples were collected in Streck Cell-free DNA BCT® blood collection tubes (La Vista, NE) capable of storing whole blood samples up to 7 days at room temperature. Sample collection took place on the day subjects were undergoing pre-colonoscopy procedures (such as blood coagulation tests). Samples were shipped on the same day of collection to the processing laboratory at the University of Naples where standardized technical procedures to collect and store samples were carried out. Briefly, whole blood samples underwent two centrifugations, first at 1,600 x g and second at 16,000 x g at room temperature for 10 minutes each. Following centrifugation, plasma samples were stored at -80° C. until molecular analysis. Quality checks were also implemented to ensure cfDNA stability and storage at constant temperature. Following enrollment conclusion, the plasma samples were shipped to the DiaCarta, Inc. (Pleasanton, CA) CLIA/CAP-certified laboratory for QuantiDNA™ testing. Sample shipment was arranged by World Courier, a company specializing in international shipments for clinical trials, with confirmed experience in tracking specimens’ temperature during shipment. The plasma samples were stored at -80oC prior to being thawed and tested with the QuantiDNA™ test at the DiaCarta CLIA-certified clinical laboratory. Relative Light Units (RLUs) data were measured by a DiaCarta Luminometer (DiaCarta, Inc., Pleasanton, CA) and converted into ng/ml concentration values using a point-to-point calibration (fig.2). A Receiver Operating Characteristic (ROC) curve was run internally to convert continuous into binary values and indicate presence/absence of disease. As described in the instructions for use, a cut-off of 6.27 ng/ml, previously calculated on a training set, was chosen as an acceptable balance between a sensitivity for CN of 74% and a specificity of 35%.
We analyzed the assay’s performance for odds ratio, detection rates, sensitivity, specificity, PPV, NPV and positivity rate.
2.4. Statistical Analysis
The study pre-specified two sets of hypotheses. The first hypothesis aimed to demonstrate that AAP sensitivity for detecting colorectal neoplasia patients is significantly greater than 50%. The second set of hypotheses aimed to demonstrate that AAP sensitivity is non-inferior to the SOC in detecting colorectal neoplasia, advanced adenomas and colorectal cancer patients, where the non-inferiority margins were set at -10%, -10%, -3.8%, respectively (see “Discussion” section for the justification). The negative sign of the margin reflects the form T - C (Treatment - Control, in this case AAP - SOC). The first hypothesis was tested using exact Binomial distribution; the second set of hypotheses was tested using the Farrington-Manning method with one-sided alpha = 0.025. All tests were one-sided with alpha = 0.025. The sample size for the study was calculated to provide 80% power to demonstrate the first study hypothesis. Assuming sensitivity of 70%, a sample of at least 25 CRC and 100 AA patients was required. To achieve the required number of positive patients, the total sample size was set to 711 patients in total, accounting for dropouts and loss-to-follow-up.
Efficacy analysis was conducted using the efficacy analysis set, as follows:
The primary efficacy analysis, to evaluate the accuracy of QuantiDNA™ test, with a three-stage process:
A. logistic regression was fit to construct the test score.
B. The cut-off was applied to convert the continuous score into positive or negative.
C. Binary accuracy of the test was evaluated, via positivity rate, odds ratio, sensitivity, detection rate, PPV, NPV and specificity.
The secondary efficacy analysis, to repeat the primary analysis using the secondary reference definition.
Covariate analysis in which the following covariates were evaluated: age, gender, body mass index (BMI), smoking and alcohol habits, lesion location, lesion type, cancer grade, cancer stage.
Confidence intervals for sensitivity and specificity were calculated using Clopper-Pearson method
Confidence intervals for PPV and NPV were calculated using the logit transformation, as recommended in Mercaldo et al. (2007).
Confidence intervals for PLR and NLR were calculated using the delta method, as described in Zhou, Obuchowski, and McClish, 2nd ed, 2011 (p. 113).
Model: Anti-logit(0.2045+1.5535*I{Fragment≥6.27})
Primary reference is defined as subject who has the presence of Colorectal Cancer (CRC) or Advanced Adenoma (AA).
The statistical analysis software used were: R-studio® v. 2022.12.0-353 under MacOS® Monterey v.12.4 for internal analysis, and SAS® v. 9.4 under Windows® 2016 Terminal.
3. Results
3.1. Study Population
A total of 711 participants were enrolled, of which 671 were included in the final analysis. 40 patients’ data were excluded from analysis due to unavailable colonoscopy data. A total of 27 out of 671 patients were clinically diagnosed as CRC (prevalence 4.0%). Staging information was available only for 19 out of 27 subjects including 8 Stage I, 8 stage IIA, 1 stage IIB, 1 stage IIIB and 1 stage IIIC. A total of 114 out of 671 patients had AA (prevalence 17.0%), for a total number of CN of 141 cases out of 671 (prevalence 21.0%). Lesion distribution was also evaluated according to location, size, histology severity, age, gender, BMI, and smoking status. Of note, 40.0% (56 out of 141) of CN lesions occurred in the 70+ years old group, 39.0% (55 out of 141) in the 60-69 years old group while 21.0% (30 out of 141) of CN were in the 50-59 years old group. As expected, there were more colorectal neoplasia lesions amongst men (57.0%) than women (43.0%). In addition, 53.9% (76 out of 141) of CN lesions were found in the sigmoid colon, 28.3% (40 out of 141) lesions in the ascending colon, 22.7% (32 out of 141) lesions in the rectum and 19.1% (27 out of 141) lesions in the descending colon. 35.1% (40 out of 114) of AA cases displayed High Grade Dysplasia (HGD) , 41.2% (47 out of 114) showed a histological villous pattern ≥ 25%; 36.8% (42 out of 114) had tubular adenoma ≥10 mm and 22.8% (26 out of 114) had a serrated lesion ≥10 mm. Moreover, 53.0% (75 out of 141) of CN cases were found in subjects with a BMI ≥ 27.4 kg/m2 (median), while 47.0% were below this value. 69.0 % (97 out of 141) ) of CN cases were found in non-smokers, 18.0% (25 out of 141) in current smokers and 13.0% (18 out of 141) among former smokers. Alternative Approach shows comparable sensitivities for lesions ≥10 mm. There were 4 lesions ≤ 9 mm with histological features of advanced adenomas and all of them were detected by AAP. 76.3% of AA with size 10-19 mm (61 out of 80), 73.7% with size 20-29 mm (14 out of 19) and 72.7% with size >29 mm (8 out of 11) was detected (Figure 1).
3.2. Clinical Performance
The odds ratio was 1.76 (95% C.I. 1.15, 2.69 p= 0.009). Hence, a subject with a positive cfDNA test had 76.0% greater odds of disease than one with a negative cfDNA test. The detection rate of colorectal neoplasia, advanced adenoma and colorectal cancer is a useful indicator, commonly adopted by European CRC screening programs. Detection Rate for CN was 15.9% (95% C.I. 13.3,18.9), and risk difference with SOC was -5.1% (-9.2, -0.9). DR for AA was 13.0% (10.5, 15.7) and risk difference with SOC was -4.0% (-7.9, -0.2). DR for CRC was 3.0% (1.8, 4.6), and risk difference vs SOC of -1.0% (-3.2, 1.1) (Table 2). Point-estimates and lower bounds of the C.I. for all risk differences were within the non-inferiority margins. This suggests that AAP is non-inferior to SOC in detecting colorectal neoplasia, advanced adenomas and colorectal cancer (Figure 2). PPV and NPV for CRC were 4.5% and 96.9% respectively. There is an expected 33.4% decrease in the need for colonoscopies due to a 66.6% positivity rate. (Table 4)
Sensitivity for CN was 75.9% (95% CI: 68.0, 82.7) (Table 3), which is significantly greater than the 50.0% of the null hypothesis. Specificity was 35.8% (95% CI: 31.8, 40.1), and area under the curve (AUC) was 56% (52.0, 60.0). Sensitivity and specificity for AA were 76.3% and 35.4% respectively, while for CRC they were 74.1% and 33.7%. The assay found 87.5% of CN located in the ascending colon, 87.5% of those found in the rectum, 77.8% in the descending, and 62.4% in the sigmoid colon.
Sensitivity for AA with high-grade dysplasia was 82.5%, while it was 80.8% for serrated lesions, 76% for tubular adenomas, and 74.5% for AAs with a ≥25% villous pattern.
The assay was sensitive towards CN lesions found in former smokers, with a 94.4% sensitivity and significant odds ratio (OR) of 10.6 (1.2, 92.7) vs current smokers. Sensitivity for CN lesions found in non-smokers was 76.3%. The OR of former smoker’s vs non-smokers was 5.28, but not statistically significant (0.7, 41.9).
4. Discussion
Here, we evaluated the role of a liquid biopsy based tool for the triage of FIT+ patients eligible for colonoscopy. Liquid biopsy consists in a versatile, dynamic and minimally invasive diagnostic tool able to assess molecular status of cancer patients. Interestingly, blood specimens are under investigation in early stage setting where a sampling approach capable to overview molecular landscape of tumor cells is required [24]. Particularly, the QuantiDNA™ test assay was calibrated specifically to meet the characteristics of the FIT+ patients’ triage setting. According to SOC, all patients returning a FIT+ test must be referred to colonoscopy. The QuantiDNA™ assay, implemented by the AAP tested in this study, would need to provide reassurance to those patients who are told to forego colonoscopy, while at the same time reducing unnecessary colonoscopies. We chose a cut-off value of 6.27 ng/ml for patient cfDNA concentration, because it appeared to meet both objectives while achieving acceptable sensitivity and specificity values. By applying this cfDNA QuantiDNA™ test assay, the expected decrease in colonoscopies is about 33.4%. NPV for cancer is 97.0%. Non-inferiority analysis suggests that AAP is not unacceptably worse than SOC for all three disease categories (CN, AA, CRC).The clinical test results showed a sensitivity of 75.0% for AA and 74% for CRC (Stage I-II predominantly). We do not have much information about later stages and metastatic cancer (mCRC), because there were only two CRC participants with stage III, while none had stage IV or mCRC. However, the high sensitivity for pre-cancer and early-stage cancers fits well with the purpose of colorectal cancer screening programs.We recognize that a 35.0% specificity is sub-optimal, however, it is important to understand the triage context, bearing in mind that without triage, all FIT+ subjects would inevitably go to colonoscopy examination. Modelling the impact of AAP on 1000 theoretical FIT+ population who would be referred to immediate colonoscopy according to SOC, we would find that AAP would decrease the number of colonoscopies to ~660, applying QuantiDNA™ test’s positivity rate. Furthermore, using AAP’s positive predictive value for CN, negative colonoscopies could decrease by a 36.0% rate. With a NPV of about 97.0% for CRC and non-inferiority in DR for CN, AA and CRC, the model should theoretically provide adequate patient protection. The choice of the non-inferiority margin was challenging due to the absence of guidelines that instead exist for pharmaceutical trials. Our reasoning resulted from some adaptations of the rules set by EMA and FDA (7,8). The assay met the non-inferiority requirements for all of the three disease categories. Interestingly, the AAP showed the highest sensitivity levels for CN lesions located in the ascending colon and the rectum, for high grade dysplasia, and for serrated lesions (87.5%, 87.5%, 82.5% and 80.8% respectively). The assay appears to have a higher sensitivity for CRC Stage II cancers (88.9%), but this will need further confirmation.
Finally, blood sample collection was accepted and well tolerated by most patients. Laboratory procedures also proved acceptable. The bDNA technology and signal amplification appear to provide consistent detection of cfDNA directly in plasma, without the DNA extraction step which is known to lose variable amounts of genetic material. Thus, using the QuantiDNA™ test could generate opportunities for reliable patient cfDNA monitoring. The study presented here has some limitations. First of all, the study conducted only allowed for single-site enrollment. This was due to considerations pertaining to disease prevalence in different regions of Italy and the probability of finding a significant number of pre-cancers and cancers without enrolling an overwhelming number of subjects. ASL NA 3 SUD has been implementing a CRC screening program for less than 10 years, and appears to meet this enrollment requirement. Secondly, the choice of a cross-sectional design to compare two interventions does not provide the same level of evidence of a fully randomized, interventional study. Notably, the comparison between the two approaches was made possible by the data analysis strategy.
5. Conclusions
This study showed promising results in the triage of FIT positive patients. Further studies are needed to confirm this data in clinical practice and will improve our knowledge of liquid biopsy, cfDNA and its potential contribution to the prevention of colorectal cancer.
Ethics approval statement
provided by the Ethical Committee of ASL NA 3 SUD (Protocol DIA-001).
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Figure S1: title; Table S1: title; Video S1: title.
Contributorship Statement: Conceptualisation: MS, FP, UM, GT, MB. Methodology: all authors. Software: S.S, S.E, Y.G. Validation: all authors. Formal analysis: all authors. Investigation: all au-thors. Resources: all authors. Data curation: all authors. Writing—original draft preparation: MS, FP. Writing—review and editing: all authors. Visualisation: all authors. Supervision: UM, MB, GT and AI. Project administration: UM and GT. Funding acquisition: MS
Funding
the study was funded by DiaCarta, Inc.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
data supporting the conclusions of this article will be made available by the authors on request.Data of the study is in sponsor’s possession and available upon request.
Conflicts of Interest
The following authors have a collaboration contract with the sponsor: M.S, S.S, R.C, H.Tanaka, M.Sh, D.C, S.Sh. F.P. has received personal fees (as consultant and/or speaker bureau) from Menarini unrelated to the current work. U.M. has received personal fees (as con-sultant and/or speaker bureau) from Boehringer Ingelheim, Roche, MSD, Amgen, Thermo Fisher Scientifics, Eli Lilly, Diaceutics, GSK, Merck and AstraZeneca, Janssen, Diatech, Novartis and Hede-ra unrelated to the current work. G.T. reports personal fees (as speaker bureau or advisor) from Roche, MSD, Pfizer, Boehringer Ingelheim, Eli Lilly, BMS, GSK, Menarini, AstraZeneca, Amgen and Bayer, unrelated to the current work.
References
- Xin Wang, Xia-Qing Shi, Peng-Wei Zeng, Fong-Ming Mo, Zi-Hua Chen. Circulating cell free DNA as the diagnostic marker for colorectal cancer: a systematic review and meta-analysis. Oncotarget, 2018, Vol.9, No.36, pp: 24514-24524.
- Paul Okunieff, Natalie A. Lockney, Randal H. Henderson, Steven G. Swarts, Zhenhuan Zhang, Bingrong Zhang, Jennifer Li, Robert A. Zlotecki, Cristopher G. Morris, Katherine A. Casey-Sawicki. Measuring Radiation Toxicity Using Circulating Cell-free DNA in Prostate Cancer Patients. IJPT, 2021.
- Scimia M, Du J, Pepe F, Bianco MA, Russo Spena S, Patell-Socha F, Sun Q, Powell MJ, Malapelle U, Troncone G. Evaluation of a novel liquid biopsy-based ColoScape assay for mutational analysis of colorectal neoplasia and triage of FIT+ patients: a pilot study. J Chin Pathol, 2018; 0: 1-4.
- Carlo Senore, Partha Basu, Ahti Anttila, Antonio Ponti, Mariano Tomatis, Diama Bhadra Vale, Guglielmo Ronco, Isabelle Soerjomataram, Maja Primic-Zakelj, Emilia Riggi, Joakim Dillner, Miriam Klara Elfstrom, Stefan Lonnberg, Rengaswamy Sankaranarayanan, Nereo Segnan. Performance of colorectal cancer screening in the European Union Member States: data from the second European screening report. Gut 2018; 0: 1-13.
- Chen Qian, Shaoqing Ju, Jing Qi, Jianmei Zhao, Xianjuan Shen, Rongrong Jing, Juan Yu, Li Li, Yingjuan Shi, Lurong Zhang, Zhiwei Wang, Hui Kong. Alu–based cell-free DNA: a novel biomarker for screening of gastric cancer. Oncotarget, advance publications 2016.
- Maria Antonia Bianco, Gianluca Rotondano, Maria Lucia Garofano, Livio Cipolletta. Discovering a magnified world. Superficial neoplastic lesions… and beyond. Area Qualità, first published September 2005.
- EMA Guideline on the choice of the non-inferiority margin. Doc. Ref. EMEA/CPMP/EWP/2158/99.
- FDA Non-inferiority clinical trials to establish effectiveness. Guidance for Industry.
- Jack Cuzick, Peter Sasieni. Interpreting the results of non-inferiority trials — a review. British Journal of Cancer, 2022; 127:1755-1759.
- Thomas F Imperiale, David F Ransohoff, Steven H. Itzkowitz, Theodore R Levin, Philip Lavin, Graham P Midgard, David A. Ahlquist, Barry M. Berger. Multitarget Stool DNA Testing for Colorectal-Cancer Screening. The New England Journal of Medicine, 2014.
- Liang Huang, Yue Hu, Shan Liu, Bo Jin, Bin Lu. The analysis of multilevel factors affecting adenoma detection rates for colonoscopies: a large-scale retrospective study. BMC Gastroenterology, 2021; 21; 403.
- Hayato Yamaguchi, Masakatsu Fukuzawa, Hirohito Minami, Tadashi Ichimiya, Hiroshi Takahashi, Yubu Matsue, Mitsuyoshi Honjo, Yasutake Hirayama, Daisuke Nutahara, Junichi Taira, Hironori Nakamura, Takashi Kawai, Takao Itoi. The relationship between Post-colonoscopy Colorectal Cancer and Quality Indicators of Colonoscopy: The Latest Single-centre Cohort Study with a Review of the Literature. Intern. Med., 2020; 59: 141-1488.
- Manuel Zorzi, Giulio Antonelli, Claudio Barbiellini Amidei, Jessica Battagello, Bastianello Germanà, Flavio Valiante, Stefano Benvenuti, Alberto Tringali, Francesco Bortoluzzi, Erica Cervellin, Davide Giacomin, Tamara Meggiato, Erik Rosa-Rizzotto, Diego Fregonese, Manuela Dinca, Gianluca Baldassarre, Paola Scalon, Maurizio Pantalena, Luisa Milan, Gianmarco Bulighin, Daniele Di Piramo, Maurizio Azzurro, Armando Gabrielli, Alessandro Repici, Douglas K Rex, Massimo Rugge, Cesare Hassan, Veneto Screening Endoscopists Working Group, Anna Giacomin, Andrea Buda, Deborah Costa, Davide Checchin, Renato Marin, Elisabetta Patarnello, Aldo Ceriani, Ennio Guido, Perla Bertomoro, Nicoletta Merlini, Francesca Murer, Ephrem Ntakirutimana, Luca Benamato, Maria Cristina Conti Bellocchi. Adenoma detection rate and colorectal cancer risk in fecal immunochemical test screening programs: an observational cohort study. Ann Intern Med. 2023; 176:303-310.
- Michael Greenspan, Kumar Bharat Rajan, Adil Baig, Todd Beck, Sohrab Mobarhan, Joshua Melson. Advanced adenoma detection rate is independent of nonadvanced adenoma detection rate. Am J Gastroenterol. 2013;108:1286-92.
- Aasma Shaukat, Amy A. Gravely, Adam S Kim, Jeffery Rank, Timothy R Church, John I Allen. Rates of Detection of Adenoma, Sessile Serrated Adenoma, and Advanced Adenoma Are Stable Over Time and Modifiable. Gastroenterology AGA, Brief communication. Volume 156, Issue 3, P816-817, 2019.
- Aasma Shaukat, Jennifer Holub, Irving M Pike, Mark Pochapin, David Greenwald, Colleen Schmitt, Glenn Eisen. Benchmarking Adenoma Detection Rates for Colonoscopy: Results from a US-Based Registry. Am J Gastroenterol. 2021 1; 116: 1946-1949.
- Manuel Zorzi. Giscor Survey of Italian Colorectal cancer screening programs 2022-2023. www.giscor.it.
- Mark Schiffman, Diane Solomon. Findings to date from the ASCUS-LSIL Triage Study (ALTS). Arch Pathol Lab Med. 2003;127:946-9.
- Efrat L Amitay, Katarina Cuk, Tobias Niedermaier, Korbinian Weigl, Hermann Brenner. Factors associated with false-positive fecal immunochemical tests in a large German colorectal cancer screening study. Int J Cancer. 2019 15;144:2419-2427.
- Gregory J Tsongalis. Branched DNA technology in molecular diagnostics. Am J Clin Pathol. 2006; 126:448-53.
- T B Hao, W Shi, X J Shen, J Qi, X H Wu, Y Wu, Y Y Tang, S Q Ju. Circulating cell-free DNA in serum as a biomarker for the diagnosis and prognostic prediction of CRC. BJC, 2014, 111, 1482–1489;
- <i>22. </i>V. Heinemann, J.Y. V. Heinemann, J.Y. Douillard, M. Ducreux, M. Peeters. Targeted therapy in Metastatic Colorectal Cancer - An example of personalised medicine in action. Cancer Treatment Reviews, 2013, vol.39: 592-601.
- Matthew, G. Krebs, Umberto Malapelle, Fabrice Andrè, Luis Paz-Ares, Martin Schuler, David M. Thomas, Gilad Vainer, Takayuki Yoshino, Christian Rolfo. Practical Considerations for the Use of Circulating tumor DNA in the Treatment of Patients with Cancer: a Narrative Review. JAMA Oncology, 2022.
- Umberto Malapelle, Pasquale Pisapia, Francesco Pepe, Gianluca Russo, Mauro Buono, Alessandro Russo, Jorge Gomez, Ola Khorshid, Philip C. Mack, Christian Rolfo, Giancarlo Troncone. The Evolving role of Liquid Biopsy in Lung Cancer. Lung Cancer, 2022, 172: 53-64.
Figure 1.
A bar chart describing the test’s sensitivity for disease type, subdivided by polyp size.
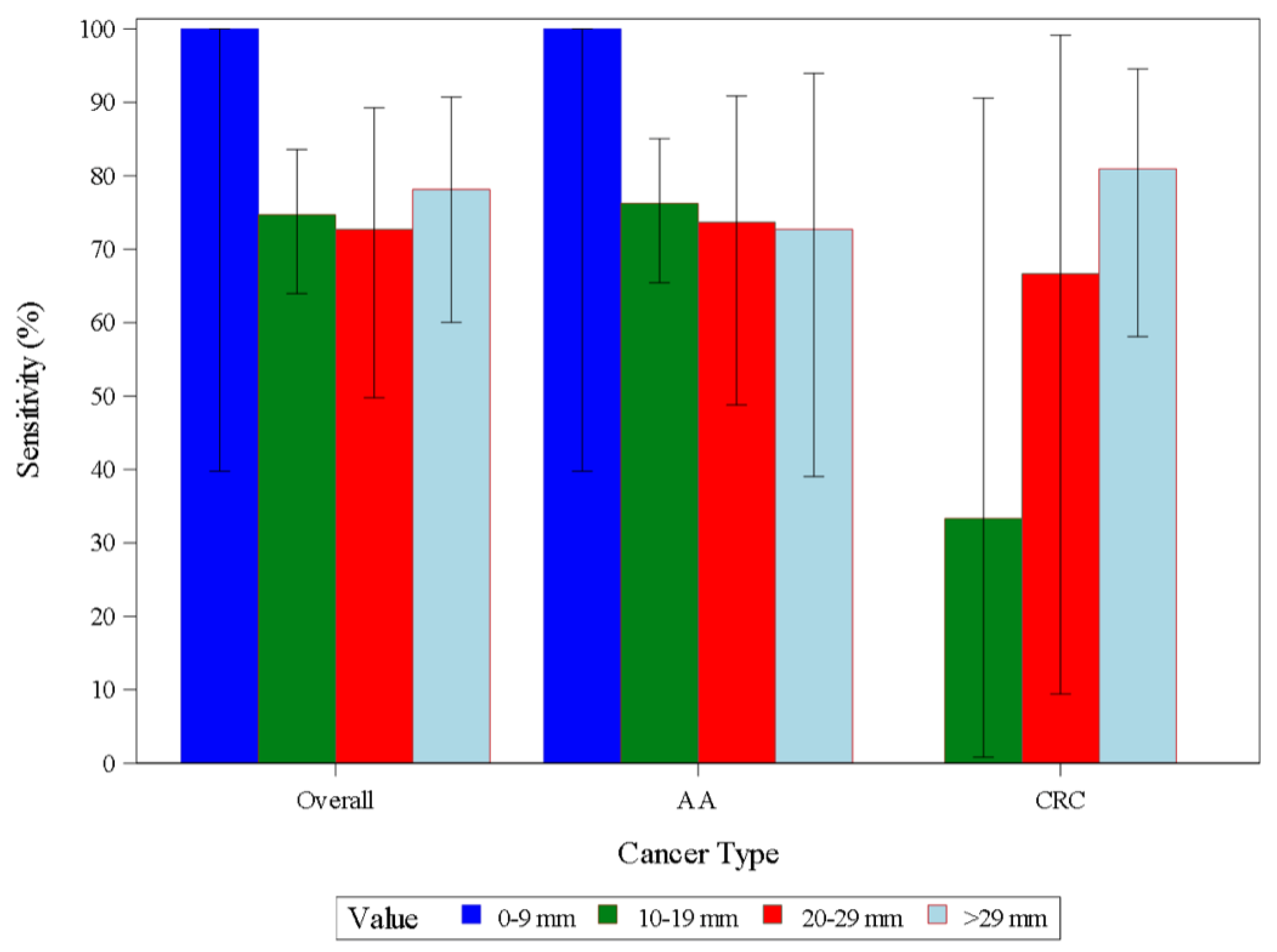
Figure 2.
Graphs of the non-inferiority analysis of AAP vs SOC.
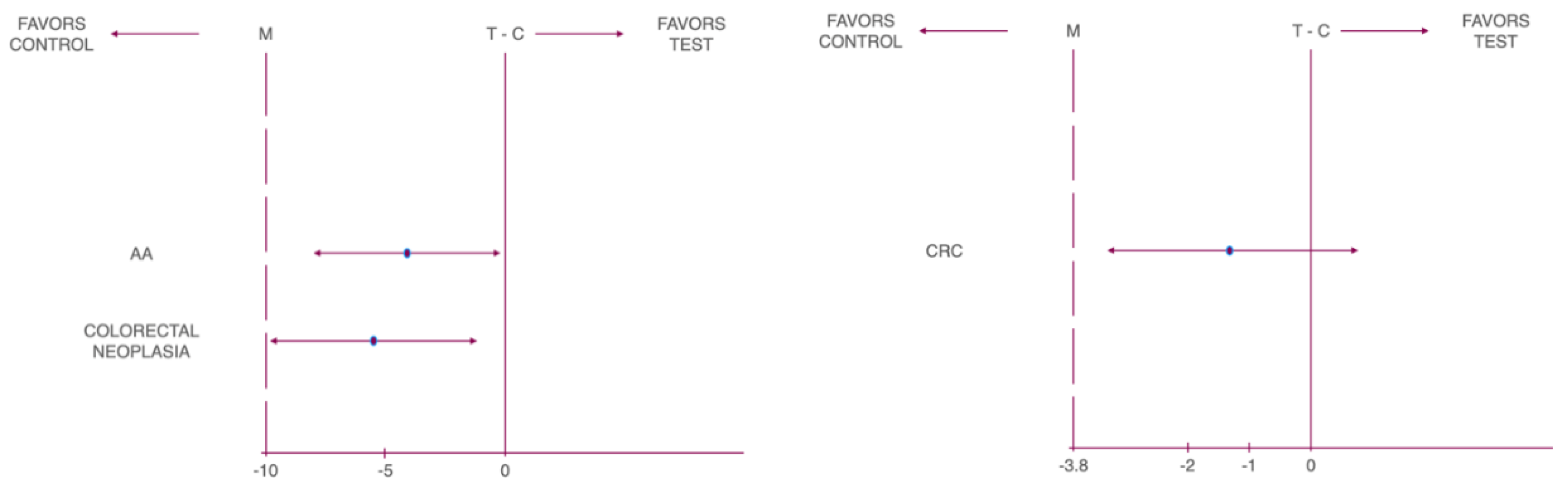

Table 1.
Clinical parameters of enrolled patients.
| Demographic Characteristics | Number * | % | |
|---|---|---|---|
| Gender | Female | 348 | 51.9 |
| Male | 323 | 48.1 | |
| Total | 671 | 100.0 | |
| Race | Caucasian | 668 | 99.6 |
| Black or African | 0 | 0.0 | |
| Middle Eastern or North African | 0 | 0.0 | |
| South Asian | 0 | 0.0 | |
| East Asian | 0 | 0.0 | |
| Eastern European | 2 | 0.3 | |
| Western European | 1 | 0.1 | |
| Southeast Asian or Pacific Islander | 0 | 0.0 | |
| Other | 0 | 0.0 | |
| Total | 671 | 100.0 |
Table 2.
Non-Inferiority Analysis on Detection Rate (DR) by Lesion Type (Fragment Efficacy Analysis Set).
Table 2.
Non-Inferiority Analysis on Detection Rate (DR) by Lesion Type (Fragment Efficacy Analysis Set).
| Cancer Type | Non-inferiority Margin (%) | Risk Difference (%) | Lower 95% CL | Upper 95% CL | P-Value |
|---|---|---|---|---|---|
| CN | -10 | -5.07 | -9.23 | -0.90 | 0.010 |
| AA | -10 | -4.02 | -7.89 | -0.16 | 0.001 |
| CRC | -3.8 | -1.04 | -3.16 | 1.07 | 0.005 |
Table 3.
Accuracy Parameters by Logistic Regression Model as Derived from Pilot Study – Primary Reference Definition.
Table 3.
Accuracy Parameters by Logistic Regression Model as Derived from Pilot Study – Primary Reference Definition.
| CN | Parameter | Total N | True Outcome | Estimate (%) | Lower 95% CL | Upper 95% CL | |
| Sensitivity | 141 | 107 | 75.9 | 68.0 | 82.7 | ||
| Specificity | 530 | 190 | 35.8 | 31.8 | 40.1 | ||
| PPV | 447 | 107 | 23.9 | 21.9 | 26.0 | ||
| NPV | 224 | 190 | 84.8 | 80.3 | 88.4 | ||
| DR | 671 | 107 | 15.9 | 13.3 | 18.9 | ||
| PR | 671 | 447 | 66.6 | 62.9 | 70.2 | ||
| NLR | 0.67 | 0.49 | 0.92 | ||||
| PLR | 1.18 | 1.06 | 1.32 | ||||
| OR | 1.76 | 1.15 | 2.69 | ||||
| Youden's J statistic | 0.117 | ||||||
| AA | Sensitivity | 114 | 87 | 76.3 | 67.4 | 83.8 | |
| Specificity | 557 | 197 | 35.4 | 31.4 | 39.5 | ||
| PPV | 447 | 87 | 19.5 | 17.7 | 21.4 | ||
| NPV | 224 | 197 | 87.9 | 83.7 | 91.2 | ||
| DR | 671 | 87 | 13.0 | 10.5 | 15.7 | ||
| PR | 671 | 447 | 66.6 | 62.9 | 70.2 | ||
| NLR | 0.67 | 0.47 | 0.95 | ||||
| PLR | 1.18 | 1.05 | 1.33 | ||||
| OR | 1.76 | 1.11 | 2.81 | 0.017 | |||
| Youden's J statistic | 0.117 | ||||||
| CRC | Sensitivity | 27 | 20 | 74.1 | 53.7 | 88.9 | |
| Specificity | 644 | 217 | 33.7 | 30.0 | 37.5 | ||
| PPV | 447 | 20 | 4.5 | 3.6 | 5.6 | ||
| NPV | 224 | 217 | 96.9 | 94.2 | 98.3 | ||
| DR | 671 | 20 | 3.0 | 1.8 | 4.6 | ||
| PR | 671 | 447 | 66.6 | 62.9 | 70.2 | ||
| NLR | 0.77 | 0.40 | 1.47 | ||||
| PLR | 1.12 | 0.89 | 1.41 | ||||
| OR | 1.45 | 0.60 | 3.49 | 0.404 | |||
| Youden's J statistic | 0.078 |
Table 4.
Accuracy Parameters by Logistic Regression Model as Derived from Pilot Study for CRC Cases – Primary Reference Definition.
Table 4.
Accuracy Parameters by Logistic Regression Model as Derived from Pilot Study for CRC Cases – Primary Reference Definition.
| Parameter | Total N | True Outcome | Estimate (%) | Lower 95% CL | Upper 95% CL |
| Sensitivity | 27 | 20 | 74.1 | 53.7 | 88.9 |
| PPV | 447 | 20 | 4.5 | 3.6 | 5.6 |
| NPV | 224 | 217 | 96.9 | 94.2 | 98.3 |
| DR | 671 | 20 | 3.0 | 1.8 | 4.6 |
| PR | 671 | 447 | 66.6 | 62.9 | 70.2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



