
Submitted:
02 October 2024
Posted:
07 October 2024
You are already at the latest version
Abstract
A major cause of genital discomfort in women around the world is bacterial vaginosis, which results from excessive growth of pathogenic bacteria in the vaginal ecosystem. Current treatment consists of antibiotics and/or probiotics, which show favourable therapeutic effects, but also cause problems such as drug resistance and recurrence. Considering faecal transplantation's success, transplantation of vaginal fluid from healthy donors could provide the most effective treatment for bacterial vaginosis. However, experimental treatments have shown that vaginal microbiome transplantation may not be a one-size-fits-all solution. The present article examines the limitations of current standardized therapy, the advantages of vaginal microbiome transplantation, and presents future novel strategies for treating bacterial vaginosis based on current research findings and clinical trials development worldwide.
Keywords:
bacterial vaginosis
; vaginal microbiota transplantation
; faecal microbiota transplantation
; treatment approaches
; clinical trials development
1. Introduction
Bacterial vaginosis (BV) is a clinically devastating condition associated with vaginal discharge, itching, burning when urinating, increased vaginal pH and fishy odour (Greenbaum et al, 2019). Nevertheless, researchers estimated that up to 50% of women with BV are asymptomatic (DeLong et al, 2019). BV manifests as a shift in the vaginal ecosystem from a dominant Lactobacillus to obligate and facultative anaerobes including Gardnerella, Prevotella and Atopobium vaginae (Vodstrcil et al, 2021). This is one of the most common microbiological vaginal infections in women of childbearing age of 14-49 years (Onderdonk et al, 2016, Javed et al, 2019; Wu et al, 2022,).
Globally, the impact of BV varies considerably from 5 to 70% in women depending upon geography and ethnicity. There is a higher prevalence of this condition in parts of Africa as compared to Europe and Asia that accounting for lower prevalence (Javed et al, 2019). Approximately 17.8% to 63.7% of the adult population in India suffers from this condition, while the prevalence in the United States is about 30%. Infect BV is more prevalent in non-white women accounting for 51% of African American women and around 32% of Mexican American women. (IPPO, 1998; Jain, et al, 2018; Eastment and McClelland, 2018). Although, BV is not a life-threatening condition but it could impose the risk to many gynaecological and obstetric disorders like preterm birth, infertility, vulnerability to sexually transmitted infections and also predispose a greater risk of infections to the upper genital tract (Lev-Sagie, 2019).
The most widely accepted methods of diagnosing BV are Amsel's criteria or Nugent's score. However, the Amsel criteria are mainly used as a diagnostic method due to having high specificity in the clinic setting including pH measurements, inspection of vaginal secretions, visual inspection under microscopy, and the Whiff test. While the Nugent score relies on Gram-stained smear microscopy images of normal flora and is considered more sensitive. To overcome the shortcomings impounded by microscopy and other point-of-care tests (POCTs), DNA sequencing of vaginal fluid has been devised using molecular markers of BV (Coleman and Gaydos, 2018; Wu et al, 2022).
The most widely prescribed antibiotics for treating BV are clindamycin or metronidazole which cure only ~70–85% of women within 1 month and are associated with complications of suboptimal cure (Koumans et al, 2002; Oduyebo et al, 2009). Moreover, there is a significant drawback to these types of treatments, which is high recurrence rates of up to 50% observed within 6 months in most patients (Bradshaw et al, 2006; Sobel et al, 1993,). Other treatment practice of using probiotics which are administered orally or intravaginally to symptomatic patients, however they have shown mixed results. Therefore, researchers suggested using a whole microbiome rather than a single bacteria type to make it more effective to deal with clinical cases (Javed et al, 2019). Further, studies have revealed that organs such as the gut and vagina harbour an array of microbes that play an instrumental role in nutrient extraction, metabolism, and immunity (Flint et al, 2012; Hou et al, 2022; Tibaldi et al, 2009).
Faecal microbiota transplantation (FMT) in recent years has shown promising therapeutic results and is becoming one of the most successful first-line treatments for treating gastrointestinal conditions by rebalancing the intestinal microbiota. The success of faecal microbiota transplantation (FMT) inspired the researchers to take vaginal microbiota transplantation (VMT) as an alternative approach by introducing the microbiome from a healthy donor to a recipient on the basis that both gastrointestinal and vaginal tracts encounter a physiologically similar environment and pathogenesis during microbial dysbiosis (Ma et al, 2019; Wu et al, 2022). Here in this article, we examine therapeutic advancements as well as the inherent pitfalls associated with current methods for the treatment of BV. Furthermore, we also elaborate the promising therapeutic concept of vaginal microbiome transplantation as a new strategy for treating bacterial vaginosis based on recent studies reported by many researchers.
2. Faecal microbiota transplantation as a modern therapeutic tool
The active gut microbial community is considered an emergent system that interacts naturally with the host and directs the physiological functions of the host including digestion to immune homeostasis (Junca et al, 2022; Evans et al, 2013). The imbalance of gut ecosystem homeostasis triggers the pathogenesis of serious gastrointestinal diseases. Therefore, the biological therapy of FMT has attracted much interest and is recommended as the most reliable and promising treatment for refractory gastrointestinal diseases (Baunwall et al, 2020; Ma et al, 2019). FMT is a promising novel therapeutic concept that involves the introduction of a whole microbial community derived from the faecal material of healthy donor into the gastrointestinal tract of patients by using various techniques such as nasogastric tube, upper tract endoscopy, oral capsules, enema, and sigmoidoscopy or colonoscopy to restore gut microbial balance (Gupta et al, 2016; Xiao et al 2020; Greenberg, 2019). An important study revealed that intraduodenal administration of a healthy faecal microbiome caused restoration of healthy microbiota and ward off recurrence as observed in patients suffering from recurrent Clostridium difficile infection (CDI) within 10 weeks of follow-up as compared to other treatment by using antibiotic vancomycin (Zmora et al, 2019). Since then, FMT studies have also been performed in other clinical conditions like cardiometabolic disease and inflammatory bowel disease (IBD) and also show the capability to be applied to other diseases in the future. (Hanssen et al, 2021; Vijay and Valdes, 2022). FMT has proven high success rates of over 85% in preventing CDI recurrences compared to a tapering regimen (35 to 42 days) of vancomycin, which showed the maximum success rate of around 69% in current antibiotic treatment regimens (Yadav D, 2021; Zanella et al, 2014; Terrier MC; Pomares Bascuñana et al, 2021). Comparatively to the standard treatment regime of antibiotics for treating CDI, FMT is generally safe with mild side effects that appear self-resolving. Furthermore, oral capsules showed superior efficacy to other routes of administration, such as colonoscopy and enema. However, severe CDI patients are less responsive to FMT (Greenberg et al, 2018 and Pomares Bascuana et al, 2021). Therefore, more research is highly required to figure out the most appropriate and effective clinical protocols for FMT.
3. Bacterial Vaginosis
In Asian and White women, the vaginal bacteria are mainly prevailed by Lactobacillus species including L. iners and L. crispatus, while L. iners dominates in Black and Hispanic women (Das Purkayastha et al, 2019). Bacterial vaginosis is characterised by a deficiency of lactic acid-producing bacteria and a corresponding increase of anaerobic bacteria diversity of anaerobic including Atopobium, Gardnerella, Megasphera, Prevotella, and Sneathia (Coudray and Madhivanan, 2020; Cheng et al, 2020; Serrano et al, 2019). Interestingly, many studies have demonstrated a strong link between BV symptoms and a change in vaginal bacterial composition.
The Lactobacillus-dominated vaginal microbiome secretes various antimicrobial substances like lactic acid, bacteriocins, and hydrogen peroxide (H2O2), which protect the host against various potential harmful pathogens (Ma et al, 2012; O’Hanlon et al, 2013; Stoyancheva et al, 2014; Vallor et al, 2001). Intriguingly, vaginal fluid contains a lot of glycogen, which is converted by human alpha-amylase into simpler carbohydrates that are turned by Lactobacillus species into lactic acid and helps in maintaining an acidic environment (Amabebe and Anumba, 2018; Wu et al, 2022). Lactobacillus produce bacteriocins viz. IIa, IIc, LF221A, J46, gassericin T, and type-A lantibiotic, which are proteinaceous bacterial substances and known for their antibactericidal properties in the host (Boris and Barbés, 2020; Kalia et al, 2020). Mostly vaginal strains of lactobacilli release H2O2, which maintain a healthy vaginal environment. However, their role is continue under investigation in the context of vaginal bacteria protection. A recent study ascribed the protective and antimicrobial properties to H2O2 rather than lactic acid produced by Lactobacillus spp, (Tachedjian et al, 2018; G. O’Hanlon et al, 2011).
Recent studies have shown that microbiota in the cervical vaginal (CV) space regulates cervical epithelial cell function (Anton et al, 2018 and Anton et al, 2022). Additionally, a CV space microbiota dominated by L. crispatus is correlated with a healthy cervical environment and confers the integrity of the cervical epithelial barrier (Anton, L, Łaniewski, P). In addition, L. crispatus-dominated microbiota is spotted to increase bacterial Immunoglobulin A (IgA) coating known to maintain a healthy intestinal microbiome (Breedveld et al; 2022; Anton et al, 2022). The vaginal fluids in BV exhibit a dramatic loss of lactic acid concentration as well as high levels of acetate, propionate, butyrate, and succinate, increasing vaginal pH by more than 4.5 (Aldunate et al, 2015). Additionally, the breakdown of amino acids into amines such as putrescine and cadaverine contributes to a vaginal fishy odour (Srinivasan et al, 2015). The mucosa layer of the vaginal tract becomes thin due to mucosal protein catabolism and secretes a homogeneous discharge (Srinivasan et al, 2015). Many studies have also confirmed the marked increase in concentration of chemokines and cytokines like IL-1β, TNFα, IL-6, and IL-8 in the vagina of women suffering from BV (Muzny et al, 2020).
4. Current Treatment Regimens for BV
Current treatment options for the BV primarily involve the use of antibiotics such as metronidazole or clindamycin, which target the overgrowth of anaerobic bacteria. While effective in the short term, these treatments often result in high recurrence rates due to the disruption of the vaginal microbiome. Emerging alternatives include probiotics, which aim to restore Lactobacillus dominance, prebiotics to support beneficial bacteria, and novel approaches like phage therapy and biofilm-disruptive agents. These strategies are being explored to achieve more sustainable and long-term management of BV by addressing the underlying microbial imbalance. As depicted in Figure 1.
4.1. Antibiotics
For the initial treatment of BV, antibiotics are usually used for one month and have an efficiency rate between 80% and 90%. However, the cure rate in clinical practice is not higher than 60% after 4 weeks of treatment (Wu et al, 2022; Larsson et al, 2011). The recommended antibiotics for BV with standard course of treatment is outlined in Table 1.
Treatment with antibiotics has the edge in terms of their availability, clinical use, and the fact that patients can directly take them at home as per instructions. Most women suffered with BV are generally cured after a single treatment in a short time frame (Ferris et al, 1995; Oyinlola et al, 2001; Hans et al, 2001). The main complication with current antibiotic treatment is recurrence of BV accounting a rate of 50% to 100% even after a treatment for one year (Wu et al, 2022). Furthermore, the problem of developing high resistance due to Gardnerella vaginalis and Atopobium vaginae, which makes antibiotic treatment less sensitive and use them for further treatment of BV. The oral intake of clindamycin and metronidazole disrupts the healthy gut bacteria, while the risk of vulvovaginal candidiasis increases by local use of antibiotics (Zimmermann and Curtis, 2019; Pilla et al, 2020; Shukla and Sobel, 2019 and Jacob et al, 2018). Therefore, high frustration is shared among clinicians and patients due to the highly complicated nature of vaginal health and limited research in this area. So, it is imperative to explore other treatments that will be more effective and non-harmful to human health.
4.2. Probiotics
The high abundance of vaginal bacteria such as L. crispatus has been known to maintain healthy vaginal condition, whereas high bacterial communities like L. iners- and non-Lactobacillus strains including the Human papilloma virus and Chlamydia trachomatis spotted as an increased risk for vaginal infections (Coudray et al, 2020; Cheng et al, 2020; Chee et al, 2020). The stabilized colony of Lactobacillus strains in the vagina produces lactic acid and bacteriocins that shield the vagina by inhibiting BV-related pathogens by lowering the vaginal pH and could also expect that this type of environment in vagina also prevents the recurrence phase of BV in the long run. Moreover, the cultivation of single bacterial strains under controlled conditions in large batches is much easier (Wu et al, 2022). Many studies indicated that probiotic treatment in BV for a longer span of 1-3 months is more beneficial in terms of efficacy as compared to short-term treatment (Liu and Yi, 2022). Furthermore, probiotic treatment has been shown to have long-term benefits, such as a high cure rate, and a reduction of recurrence of BV by more than twofold (Nurainiwati et al, 2022; SA Chieng et al, 2022). The probiotic treatment regime for BV is rather safe and shows benefit in both the short and long term. However, many clinical trials and systemic reviews related to probiotic treatment for BV have shown inconclusive results in terms of their efficacy (Wang, 2019).
With probiotics, the major disadvantage is they have strains of beneficial bacteria but lack of other potential benefits as encountered with bacteriophages or prebiotics such as stimulating growth as well as colonization of main beneficial bacteria like Lactobacillus species. Apart from resident vaginal bacteria, there are a lot of factors like level of glucose and lactic acid, hormones level and importantly sexual intercourse which can influence Lactobacillus colonization in the vagina (Antonio et al, 2009; Mirmonsef et al, 2014; Farage et al, 2010). The different make up in terms of the genetic and immunological perspective in human races is another major reason for not success of a single Lactobacillus strain as a probiotic fit for all people due to large variation in the genome of L. crispatus in the vaginal microbiome of different peoples (Zhang et al, 2020 and Duar et al, 2017). Further, it is unclear which strain of bacteria should be selected if a mixture of bacterial strains is to be used in probiotic. Since there is lack of evidence that all mixtures would be suitable for colonization in women having different ethnic and geographical backgrounds. Additionally, there is a lack of a uniform policy that specifies a standardized manufacturing protocol in terms of dose, species, and administration route. Collectively all these factors add further doubt about the results of probiotic treatment in BV (Wu et al, 2022; Kolaček et al, 2017). A previous study concluded that many newly developed vaginal strains proved to have better probiotic properties than current commercial strains flooding the market in different form (Happel et al, 2020). Research on new probiotic strains and uncovering the exact mechanism of probiotics is therefore an important topic for further study. (shown in Figure 2)
4.3. Prebiotics
Another alternative to treat BV is prebiotics which consist of those compounds that provide nutriments as well as stimulate the flourishing of lactobacilli (Menard, 2011). Studies have already shown the beneficial impact of prebiotics on intestinal health (Khangwal and Shukla, 2019; Hill et al, 2014). Therefore, prebiotic compounds such as lactitol, lactulose, raffinose, and oligofructose were assessed whether they could stimulate vaginal lactobacilli (Vieira-Baptista et al, 2022). Various prebiotics used to treat BV are summarized in Table 2. As of now, prebiotics is mainly delivered through vaginal delivery, including pessaries, creams, and douches. Their undesirable side effects, like diarrhoea, bloating, and flatulence, are largely thought to be due to the intestinal osmotic effect.
4.4. Symbiotics
The prebiotics only show their beneficial effect in the presence of a Lactobacilli population, but in vaginal dysbiosis actually the presence of Lactobacilli is completely wiped out. Usually, symbiotics, which are combinations of prebiotics and probiotics, overcome the drawbacks of prebiotics and may improve the efficacy of probiotics by increasing beneficial bacterial in human vaginal ecosystem (Vitali et al, 2016). The use of probiotics and prebiotics, such as bovine lactoferrin, as an adjuvant to metronidazole demonstrated an improvement in outcomes in a randomized controlled trial with 48 women suffering from recurrent BV (Russo et al, 2018).
4.5. pH Modifying Agents
Lactobacilli activity in the vagina causes an acidic pH that helps to maintain vagina health. Acidifying substances in BV suppress potentially infectious bacteria by restoring the low pH in the vagina. Many lactic acid-containing products were extensively used to treat BV, but there is still no evidence that suggests lactic acid-containing products cure or modulate BV (Plummer et al, 2018 and Vieira-Baptista, 2021).
4.6. Phage Therapy
Compared to antibiotics, phage therapy in BV offers many benefits such as self-amplification, high host specificity, high capacity for biofilm degradation, as well as low toxicity (Donlan, 2009 and Bourdin et al, 2014). The vaginal virome in the vagina strongly influences the bacterial community structure (Jakobsen et al, 2020). According to one theory, sexually transmitted phages target Lactobacilli and allow anaerobic bacteria to grow that cause BV. There are proofs that lytic phage can cause dysbiosis in BV by targeting lactobacilli.. Developing specific phage that target the microorganisms causing dysbiosis indicates that this therapy could be the most effective treatment for vaginal dysbiosis in the future. During their lifecycle, bacteriophages produce encoded enzymes called endolysins and show antibacterial activity by degrading the tidoglycan of the target bacterial cell wall (Oliveira et al, 2018). So these isolated enzymes could be employed as potential drugs to target the primary pathogens that causes BV. Now many investigators are researching to form a phage-based therapy for the treatment of BV by selectively targeting Gardnerella. (Vieira-Baptista P). A recently published study showed that novel bacteriophage-derived endolysins offer viable alternatives to antibiotics in treating BV because they neither cause resistance like those associated with antibiotics nor harm beneficial commensal bacteria (Arroyo-Moreno et al. 2022). As well, a recent study found that PM-477 eliminates Gardnerella from cultures of isolated strains as well as from clinically derived samples of natural polymicrobial biofilms with high selectivity and efficacy, and could serve as an alternative to antibiotics in treating patients who frequently experience BV recurrences. (Landlinger et al, 2021).
4.7. Activated Charcoal
According to recent research, activated charcoal is a viable treatment for many ailments and injuries (Vieira-Baptista P). The absorption properties of activated charcoal have made it effective as a scavenger of harmful substances and microbial toxins. Further their non-specific absorption properties could also reduce inflammation and even be effective against viruses. Bacterial infections are generally treated with antibiotics. When activated charcoal is used with antibiotics, significant amounts of antibiotics may be absorbed by charcoal and reduce antibiotic effectiveness. The efficacy of activated charcoal and chloramphenicol for BV was compared in the previous studies. The discharge and malodour were observed to decrease in both groups. An activated charcoal solution in the concentration of 10% has shown maximum efficacy and also significantly lowered pH levels with minimal reductions in lactobacilli (Tominaga et al, 2012). The basic idea for the use of activated charcoal was based on the fact that porous substances tend to exhibit less affinity to bind lactobacilli than other bacteria. A clinical trial on BV patients also showed that activated charcoal decreased the pH of the vagina and only reduced 3.1% lactobacilli (Javed et al, 2018).
4.8. Biofilm Disruptive Agents
TOL-463 is basically a vaginal gel considered safe and effective for BV treatment prepared by using novel boric acid having anti-infective properties and ethylenediaminetetraacetic acid having antibiofilm activity (Marrazzo et al, 2019). A phase II clinical trial conducted on 106 females confirmed that the insert form of TOL-463 showed 59% cure rate, while the gel form had only 50% at 9-12 days. Further studies have shown that the use of boric acid for the treatment of recurrent BV has an advantage over conventional oral metronidazole treatment. (Reichman et al, 2009; Surapaneni et al, 2021). The combination of ethylenediaminetetraacetic with boric acid has been found to enhance the antimicrobial and also increased antibiofilm potency against Candida and G. vaginalis without damaging lactobacilli (Marrazzo et al, 2019). When a proper diagnosis is not feasible, this therapy shows additional benefit by acting not only on biofilms but also on candidiasis in BV.
5. A promising Idea from FMT
The success of FMT as an innovative and safe method for rebalancing the intestinal microbiota over the year motivated American scientists to apply this idea to BV (Biazzo et al, 2022). They assumed that if stool transplants rebalance the intestinal microbiota, vaginal bacteria transplants similarly could also restore a healthy vaginal microbiota. The result of a study conducted on 20 women aged between 25 and 35 years has shown that the presence of a significant amount of Lactobacillus crispatus in the vaginal cavity leads to a higher lactic acid content that keeps acidic pH resulting in protection of the vagina against infectious agents (Delong et al, 2019). Further, research studies found that in the female vaginal wall harbour a large population of Lactobacilli, which metabolise glycogen produced by vaginal epithelial cells under the stimulation of oestrogen into lactic acid for the maintaining an acidic pH of 4.0-4.5 (Smith and Ravel, 2016; Miller et al, 2016). These Lactobacilli also form an epithelial mucosal barrier (bio membrane) in the vagina and act as a first line defence against almost all types of invading pathogens (Amabebe and Anumba, 2018). As yet another key factor for preventing pathogenic organisms including Mycoplasma, Gardnerella, Bacteroides, and Streptococcus from overgrowing is a low pH caused by lactic acid and the production of hydrogen peroxide and bacteriocins antimicrobial substances (Ma et al, 2022). The enrichment of G. vaginalis, Bacteroides and Prevotella in samples taken from BV patients than healthy women (Martinez, 2008; Heinemann and Reid, 2005). An interesting finding revealed by one of study that vaginal microbiota yields lactic acid that shows effective anti-inflammatory and antimicrobial activity properties in cervicovaginal epithelial cells and reduce sexually transmitted infections as well as their transmission (Amabebe and Anumba, 2018; Tachedjian et al, 2018, Delgado-Diaz et al, 2022). Research in the past has also shown that lactic acid is capable of suppressing both the spread of pathogenic bacteria fastened with BV as well as the rate of recurrence of BV. (Boskey et al, 2001; Hay, 2005; Ronnqvist et al, 2006). Interestingly, BV risk in women who lack H2O2-producing lactobacilli was more after taking of antibiotics treatment (Redelinghuys et al. 2015; Onderdonk et al, 2016; Tachedjian et al, 2018). Therefore, a few studies have also recommended introducing exogenous Lactobacilli strains to rebalance vaginal microbiota (Reid et al and Mastromarino et al, 2014).
Healthy vaginal epithelium also plays a vital role in preventing invasive infections (Marrazzo, 2013; Anderson et al, 2014). An influential role that is played by the apical layers of vaginal epithelium is to act as an interface between the host and the environment and provide protection against infection in the vagina (Baroni et al, 2012). The flattened loosely connected dead cornified cells of vagina stratum corneum (SC) lack intracellular organelles, nuclei, DNA, and RNA leading to non-expression of de novo proteins, which recognize and serve defence against pathogenic bacteria. (Eckhart et al, 2013, Wickett and Visscher, 2006). This layer also displays distinct features of permeability to cellular and molecular immunological mediators of immune defence and microbes due to devoid of robust intercellular junctions and complete lipid envelope (Bragulla and Homberger, 2009; Menon et al, 2012). The loose attachment of the cells provides an environment that promotes endogenous vaginal microbiota while preventing foreign bacteria invasion (Anderson et al, 2014). The reproductive tract in females has a mucosal immune system which is uniquely adapted to manage commensal bacteria, sexually transmitted pathogens, allogeneic spermatozoa, and the immunity of the foetus (Ochiel et al, 2008). A previous study has shown that pivotal cells of the innate and adaptive immune systems in the female reproductive tract are antigen-presenting cells and also functionally respond to various antigens in the fallopian tubes, uterus, and cervix. These cells provide protection to neutrophils, macrophages, natural killer cells and epithelial cells through Toll-like receptors by producing chemokines and cytokines that deploy and also activate immunocytes, virucides and bactericides that provide protection specially when sex hormones down regulate adaptive immunity (Wira et al. 2005).. (Wira et al. 2005; Kaushic and Nguyen, 2016).
6. VMT as an emerging concept for BV
Bacteria in the gut and vaginal cavity play an essential role in maintaining physiological and nutritional homeostasis, which is vital to human health. The landscape of gut bacteria in human gut including bacteria, archaea and eukaryotic microorganisms and Lactobacilli in vagina is largely determined by the host genotype, the colonizing history, the host bionomy, and other environmental factors. (Zoetendal et al. 2004 and Mendling, 2016). There are a variety of key roles that gut bacteria play such as digestion, metabolizing drugs, facilitating immunity, competition with pathogens by occupying niches, and promoting intestinal angiogenesis (Lozupone et al, 2012; Maynard et al, 2012; Parekh et al. 2014, Stappenbeck et al; Andriessen et al. 2016). The vaginal cavity also hosts a population of highly diverse microbiota that maintains a balance ecological system by keeping it in good health via physiologic metabolic and immune homeostasis (Petrova et al. 2013; Kim and Park 2017). Vaginal flora exhibits cooperative and competitive interactions with one another, as well as symbiotic relationships with the host tissue and organ. However, all species of microbial are not beneficial and the enrichment of some specific bacteria could be problematic (Dethlefsen et al, 2007; Yazdanbakhsh et al, 2002). The previous study suggested limiting the use of VMT to women who were negative for G vaginalis to avoid risk for BV (Mikamo et al, 2000). Generally, women at any stage of their lives suffer from vaginal infections caused by disrupted gut bacteria (Hao et al. 2011; Dareng et al. 2016; Babu et al. 2017). Surprisingly, the FMT process has shown encouraging results for some diseases resulting from disturbance of whole microbial communities as compared to single or combination forms of probiotics (Robinson et al, 2010). Although many probiotics also have been used for BV, but most of them have shown auxiliary effects with antibiotics but fail when used alone (Vujic et al, 2013). Therefore, VMT could be a very effective treatment for BV or other vaginal infections due to the similarities in physiology and pathogenesis resulting from overgrowth of pathogens in the intestinal tract and vaginal cavity.
6.1. Preconditions Required for VMT
Patient screening, inclusion criteria, exclusion criteria and the consent process for participants for VMT must be meet before to join the trial.
6.1.1. Diagnosis of BV
In order to diagnose BV as per Amsel criteria a minimum of three of these four symptoms or signs such as homogenous, thin, white discharge, a vaginal fluid having pH > 4.5, a fishy odour in vaginal discharge before or after adding 10% potassium hydroxide (the whiff test); and on microscopic examination, >20% of the vaginal epithelium has adherent coccobacilli (clue cells) (Bhujel et al, 2021). While according to Hay-Ison criteria, if the microbiome of an individual is Lactobacillus predominant, it would be classified as normal, while coccid-bacillary dominated or intermediate would be considered positive for BV. (Lev-Sagie et al, 2019).
6.1.2. Main Inclusion Criteria for Recipients
The main inclusion criteria for study candidates are recurrent BV of at least four times in current year in the individual of group of 18-50 years. Further, the individual depend upon antibiotic therapy of twice weekly to keep as symptom free or if they have documented history of prior BV recurrence and now again showing the recurrence in a period of 2-month or less even after following of antibiotics treatment (Lev-Sagie et al, 2019).
6.1.3. Main Exclusion Criteria for Recipients
The key criteria used for study candidates are such as non-pregnant women, free from planned pregnancy in the coming year, free from infection including HIV, hepatitis B, hepatitis C, or syphilis. Study candidates are also free of cervicovaginal infections including Chlamydia trachomatis, Neisseria gonorrhea, Trichomonas vaginalis, and Mycoplasma genitalium confirmed by PCR testing. The study candidates receive standard recommended treatment after confirming positive for these diseases. Study recipient candidates free from human papilloma virus and a cervical cytology screening test (Pap test) confirmed by PCR-based screening. The vaginal cultures of the recipient are free from yeast, bacteria (streptococci groups A, B, C and G), and other tests including urinalysis, urine cultures, and serology analysis for hepatitis A, B and C, HIV, Treponema pallidum, cytomegalovirus (CMV) and herpes viruses (Lev-Sagie et al, 2019).
6.1.4. Main Inclusion Criteria for Donors
Inclusion criteria used for donor selection are having an age from 18 to 50 years, being premenopausal, and having a negative history of vaginal symptoms. Furthermore, they should not be positive for BV and other vaginitis, verified through their history, gynecological examination, PCR test, microscopic examination, and culture of vaginal secretion. If donors are free of potentially serious infections, including group B Streptococcus (GBS) or Streptococcus agalactiae and CMV and also, they did not perform sexual intercourse in the preceding week of vaginal fluid collection (Lev-Sagie et al, 2019).
6.1.5. Main Exclusion Criteria for Donors
Donor candidates are excluded from study if they identified BV positive or even infected with BV in last 5 years or if they have recurrent BV history, and cervico-vaginal sexually transmitted infections, such as M. genitalium, C. trachomatis, T. vaginalis and N. gonorrhoea. Furthermore, study participants are also excluded if individual having recurrent candida vulvovaginitis, and urinary tract infections history and also show the presence of streptococci groups A, C or G and a positive for HPV test. Moreover, if the donor used any antibiotics or systemic medication in the month preceding vaginal fluid collection, used herbal or homeopathic remedies, or used probiotics (orally or vaginally) are also count in exclude criteria. If having history of disease like anogenital dysplasia, anogenital HPV, anogenital herpes, vulvar or vaginal disease, cancer abnormal urinalysis; or infection; pregnancy, seropositivity to hepatitis C, hepatitis B, HIV, syphilis, and have long-term treatment medical and sexual history with clinician (Lev-Sagie et al, 2019).
6.2. Procedure for VMT
The most appropriate time for collecting of vaginal secretions from donors is day seven of the menstrual cycle. The schematic illustration VMT procedure is shown in figure 1. The samples should be taken from the upper vaginal and cervical fornixes and must avoid the cervix region. Importantly, the broad end of a flat Ayre's spatula should be inserted for the collection of vaginal secretion. This spatula has actually a vaginal shape and offers the advantage that it does not absorb vaginal secretion and also does not cause injury to vagina. This technique is also used to collect samples for molecular analysis using the ESwab Multiple Specimen Collection and Transport System (COPAN) and to store samples at -80°C collected as part of VMT sampling. The key instruction of the VMT protocol is that recipients must not engage in sexual activity for one month. Further, the recipient should refrain from bath for at least seven days. Moreover, the recipient should also avoid douching, intra vaginal medication, systemic antibiotics for one month, and probiotics for one year following VMT. After sampling, the collected vaginal discharge must be evaluated for pH and microscopic examination. The vaginal fluid is transferred to the posterior fornix of the recipient vagina after diluting with 1 ml sterile saline without using a speculum within 60 minutes of collection. The transplant procedure can be applied to the recipient at any phase of the menstrual cycle, excluding the menstruation period (Lev-Sagie et al, 2019).
6.3. Follow up Procedure after VMT
At each examination, patients must undergo a gynaecological examination and a microscopic examination of vaginal secretion. If cytology or HPV tests show abnormal results, a colposcopy must be performed before VMT as recommended by American Society for Colposcopy and Cervical Pathology (ASCCP) guidelines. Those patients with normal cytology who have negative HPV test must also be screened again for cytology after one year, as recommended by ASCCP. Generally, the chances of infection become high after VMT, if the recipient maintain sexual relations with their partner. Therefore, these infections could not be attributed to VMT and no need for routine test (Lev-Sagie et al, 2019).
6.4. High throughput 16S rRNA Gene Amplicon Sequencing
Vaginal microbiome samples from donors and recipients must be sequenced with 16S ribosomal DNA (rDNA) sequencing to identify the changes at the genus level. DNA extraction should follow a standard protocol, followed by 500-bp paired-end sequencing (Illumina MiSeq). Amplicons spanning variable region 4 (V4) of the 16S rDNA gene should be generated by using the following barcoded primers: Fwd 515F, AATGATACGGCGACCACCGAGATCTACACTATGGTAATTGTGTGCCAGCMGCCGCGGTAA; Rev 806R, CAAGCAGAAGACGGCATA. Shotgun metagenomic sequencing technique is used for evaluation of samples collected from all donors' and recipients’ to see the changes in vaginal microbiome of BV patients at species-level (Lev-Sagie et al, 2019).
6.5. Microbial Bioinformatics Analysis
Using appropriate software such as QIIME (v1.9.1), sequence data can be analyzed. QC and Trimmomatic should be used to trim and align paired ends, followed by clustering into OTUs (Operational Taxonomic Units) with 97% similarity. The rarefaction method should be used to exclude samples with insufficient read counts. Alpha diversity and beta diversity estimators must be calculated. Principal-coordinate analysis with UniFrac distances can be used to distinguish the microbiomes of the BV patients of from healthy individuals on the basis of different clustering patterns of bacteria. The shift in the micrrobiota composition of recipients prior to and after VMT can be scored by assessing Bray–Curtis (BC) dissimilarity and then correlates with Amsel's criteria. By using BC dissimilarity, the consequences of VMT in the follow-up period can be assessed by comparing the baseline BV configuration of gut bacteria at species level in the patient. The patient’s gut bacteria composition must demonstrate an increase in the abundance of Lactobacillus genus along with depletion of the Bifidobacterium genus specially the Gardnerella genus and other bacteria like Fannyhessea and Prevotella genus on the successful VMT. PCA at species should show samples clustering into BVs, containing mostly samples with Amsel-diagnosed BV features, whereas a healthy cluster will not contain any diagnosed features. Based on the Amsel score, entire samples can be classified into two groups. Accordingly, the first group is designated as samples having zero Amsel criteria and the second group includes samples with more than zero Amsel criteria. A permutational analysis of variance test can be executed on the basis of BC dissimilarity matrix (p< 0.05) to determine whether the groups are distinctly different in the context of gut bacteria. A functional analysis of the microbiome after VMT can be conducted with the Kyoto Encyclopedia of Genes and Genomes (KEGG), which should generally show two noticeable functional clusters that actually separate the BV microbiome from the healthy one (Lev-Sagie et al, 2019).
7. Need to Further Readdressing of Challenges with Vmt
The therapeutic success of FMT for CDI prompted researchers to examine its feasibility for more prevalent antibiotic-resistant bacterial infections, like VMT. This process involves the transfer of the complete community of vagina microbiome from a healthy donor into the patient for remodelling of the microbial diversity of beneficial bacteria. Research of this kind is complex and presents many unforeseen challenges. First of all, longer phase studies involving a larger cohort of donors and patients as used in FMT has also required in VMT to ascertain the safety of this technique before confirming its efficacy (Quraishi et al, 2017). One study led by Lev-Sagie and colleagues reported that 4 out of 5 individuals having recurrent BV who after receiving microbiome transplantation showed full remission from BV. More importantly, no pharmacologic interventions were required in patients following transplantation, and no side effects were experienced in any patients. In the initial phase, identifying donors who meet all standard criteria may be the biggest challenge. Owing to the unique physiology of vagina in human beings in comparison to other animals, it is not possible to conduct in vivo investigations in the early phases of BV. Since vaginal fluid needs to be administered directly to the patient, a very thorough donor screening is a prerequisite in this technique. Another issue involves the timeline, as in this process investigators collect donor vaginal fluid for a month, during which donors must abstain from sexual activity. Further, a randomized, placebo-controlled trial has to be required for this research work and the enrolment of potential VMT recipients is a very difficult and complicated task. Moreover, a recurrent BV history patient with three or more episodes on record within the previous 12 months is a stringent inclusion criterion. However, women who have a history of recurrent BV for a long time are unlikely to participate in the randomized trial of the placebo group. Even during VMT procedure some patients may be showing the incidents of immunological rejection or infection. Before moving on to VMT, this technique requires genomic sequencing of donor as well as recipient which requires high efforts. In order to perform VMT, both the donor and recipient need genomic sequencing, which requires high effort. Further after VMT, a routine physical exam has to be required to check therapeutic effect on BV and also to ascertain the e health status of individual and finally to know whether the VMT in patient is working effectively or not. In addition, a regular review of the microbiota of vagina in the recipient along with their clinical index is also necessary to ensure that the reinstatement of beneficial vaginal microbiota is accomplished. This regular monitoring is very complex and required for each individual due to having a different immune response and a unique microbiota in the vagina. There are ethical issues with VMT, since people are generally reluctant to accept other people's vaginal microbiota. The main challenge of VMT is social stigma regarding their acceptance in the society. However, the engrafting of microbiota of healthy individuals to patients has broad outcome possibilities. The situation may be such that even after VMT, the recipient comparatively to healthy individuals shows reduced bacterial diversity. A major stumbling block in VMT is its high degree of uncertainty. Hence, regular inspections are essential to check out if the bacterial diversity is actually becoming low or an overabundance of unfavourable bacteria which may cause harm to recipients. The summary of clinical results of recent microbiome transplantation is provided in Table 3
The above discussion after underpinning current evidence concludes that although VMT does not seem to be an obvious standalone remedies for BV. A single study suggests a cure rate of 75% for recurrent BV following VMT. Otherwise, a large number of studies on BV are in pipelines as in clinical trials and will take time to complete. Like the FMT database, human VIRGO (vaginal non-redundant gene catalog) is now available as a central reference database for characterization of the vaginal microbial gene content of individual bacterial species situated in the vagina. Moreover, these alternative treatments still require further research to establish their efficacy. Hence, it is necessary to accelerate the progress of existing clinical trials and conduct more studies on VMT in order to make sure that this treatment is safe and effective.
Conclusions
A significant decline in the expense of microbiome analysis and breakthroughs in technology have caused microbiome research to evolve rapidly in recent years. In fact, a greater understanding of microbiota composition driven by host genetics, host immune response, and environmental factors has contributed to the improvement of the treatment of BV. Consequently, many treatment approaches are in practice for BV. However, probiotics are emerging as an alternative approach to BV treatment alone or in concord with antibiotics despite having the major drawback of lack of sufficient high-quality evidence regarding their long-term results. The main constraint is that unfavourable conditions encountered in BV could not allow the growth of Lactobacilli. This led to the idea of the use of prebiotics and symbiotic as an alternative treatment for BV. Interestingly, even the probiotic approach has proven inadequate, resulting in shifting to a more promising approach known as VMT after proving the high fidelity of FMT in CDI patients. There are, however, a number of reasons why even this novel method does not seem to apply to all types of BV cases. Therefore, the combination of current treatment modalities such as novel antimicrobial agents, probiotics, live bacterial biotherapeutics, biofilm disruptor agents, and VMT has immense potential to treat BV in the future. There is a lack of sufficient solid evidence regarding the full potential of this approach since most of the studies on VMT are in human clinical trials right now. Therefore, it remains unclear what would be the most effective treatment strategy from a variety of approaches for BV in its episodic and recurrent forms, either alone or in combination with antibiotics. As a matter of fact, the current development of VMT indicates that it might be the most effective complementary or optional therapy to replace the traditional treatment regimens for recurrent vaginal problems. Conclusively the importance of a culture of collaboration and partnership in research across the globe is essential for addressing this long-standing problem, especially by accelerating clinical studies of VMT.
Consent for Publication
Not applicable
Conflict of Interest
The authors declare that they have no competing interests.
References
- Antonio, M. A. D., Meyn, L. A., Murray, P. J., Busse, B., Hillier, S. L., 2009. Vaginal colonization by probiotic Lactobacillus crispatus CTV-05 is decreased by sexual activity and endogenous. Lactobacilli. J. Infect. Dis. 199, 1506–1513.
- Aldunate, M.; Srbinovski, D.; Hearps, A.C.; Latham, C.F.; Ramsland, P.A.; Gugasyan, R.; Cone, R.A.; Tachedjian, G. Antimicrobial and immune modulatory effects of lactic acid and short chain fatty acids produced by vaginal microbiota associated with eubiosis and bacterial vaginosis. Front. Physiol. 2015, 6, 164. [CrossRef]
- Andriessen, E.M.; Wilson, A.M.; Mawambo, G.; Dejda, A.; Miloudi, K.; Sennlaub, F.; Sapieha, P. Gut microbiota influences pathological angiogenesis in obesity-driven choroidal neovascularization. EMBO Mol. Med. 2016, 8, 1366–1379. [CrossRef]
- Amabebe, E.; Anumba, D.O.C. The Vaginal Microenvironment: The Physiologic Role of Lactobacilli. Front. Med. 2018, 5, 181. [CrossRef]
- Anton, L.; Sierra, L.-J.; DeVine, A.; Barila, G.; Heiser, L.; Brown, A.G.; Elovitz, M.A. Common Cervicovaginal Microbial Supernatants Alter Cervical Epithelial Function: Mechanisms by Which Lactobacillus crispatus Contributes to Cervical Health. Front. Microbiol. 2018, 9, 2181. [CrossRef]
- Anton, L.; Ferguson, B.; Friedman, E.S.; Gerson, K.D.; Brown, A.G.; Elovitz, M.A. Gardnerella vaginalis alters cervicovaginal epithelial cell function through microbe-specific immune responses. Microbiome 2022, 10, 1–20. [CrossRef]
- Arroyo-Moreno S., Cummings M., Corcoran D.B., Coffey A., McCarthy R.R.,2022. Identification and characterization of novel endolysins targeting Gardnerella vaginalis biofilms to treat bacterial vaginosis. NPJ Biofilms Microbiomes 19, 8(1), 1-12.
- Boris, S.; Barbés, C. Role played by lactobacilli in controlling the population of vaginal pathogens. Microbes Infect. 2000, 2, 543–546. [CrossRef]
- Boskey, E.; Cone, R.; Whaley, K.; Moench, T. Origins of vaginal acidity: high d/l lactate ratio is consistent with bacteria being the primary source. Hum. Reprod. 2001, 16, 1809–1813. [CrossRef]
- Bradshaw, C.S.; Morton, A.N.; Hocking, J.; Garland, S.M.; Morris, M.B.; Moss, L.M.; Horvath, L.B.; Kuzevska, I.; Fairley, C.K. High Recurrence Rates of Bacterial Vaginosis over the Course of 12 Months after Oral Metronidazole Therapy and Factors Associated with Recurrence. J. Infect. Dis. 2006, 193, 1478–1486. [CrossRef]
- Bragulla, H.H.; Homberger, D.G. Structure and functions of keratin proteins in simple, stratified, keratinized and cornified epithelia. Am. J. Anat. 2009, 214, 516–559. [CrossRef]
- Baroni, A.; Buommino, E.; De Gregorio, V.; Ruocco, E.; Ruocco, V.; Wolf, R. Structure and function of the epidermis related to barrier properties. Clin. Dermatol. 2012, 30, 257–262. [CrossRef]
- Bourdin, G.; Navarro, A.; Sarker, S.A.; Pittet, A.; Qadri, F.; Sultana, S.; Cravioto, A.; Talukder, K.A.; Reuteler, G.; Brüssow, H. Coverage of diarrhoea-associated Escherichia coli isolates from different origins with two types of phage cocktails. Microb. Biotechnol. 2014, 7, 165–176. [CrossRef]
- Babu, G., Singaravelu, B.G., Srikumar, R. et al., 2017. Comparative study on the vaginal flora and incidence of asymptomatic vaginosis among healthy women and in women with infertility problems of reproductive age. J Clin Diagn Res, 11(8), DC18-DC22.
- Baunwall, S.M.D.; Lee, M.M.; Eriksen, M.K.; Mullish, B.H.; Marchesi, J.R.; Dahlerup, J.F.; Hvas, C.L. Faecal microbiota transplantation for recurrent Clostridioides difficile infection: An updated systematic review and meta-analysis. eClinicalMedicine 2020, 29-30, 100642. [CrossRef]
- Bhujel, R.; Mishra, S.K.; Yadav, S.K.; Bista, K.D.; Parajuli, K. Comparative study of Amsel’s criteria and Nugent scoring for diagnosis of bacterial vaginosis in a tertiary care hospital, Nepal. BMC Infect. Dis. 2021, 21, 1–6. [CrossRef]
- Biazzo, M.; Deidda, G. Fecal Microbiota Transplantation as New Therapeutic Avenue for Human Diseases. J. Clin. Med. 2022, 11, 4119. [CrossRef]
- Breedveld, A.C.; Schuster, H.J.; van Houdt, R.; Painter, R.C.; Mebius, R.E.; van der Veer, C.; Bruisten, S.M.; Savelkoul, P.H.M.; van Egmond, M. Enhanced IgA coating of bacteria in women with Lactobacillus crispatus-dominated vaginal microbiota. Microbiome 2022, 10, 1–11. [CrossRef]
- Coste, I.; Judlin, P.; Lepargneur, J.-P.; Bou-Antoun, S. Safety and Efficacy of an Intravaginal Prebiotic Gel in the Prevention of Recurrent Bacterial Vaginosis: A Randomized Double-Blind Study. Obstet. Gynecol. Int. 2012, 2012, 1–7. [CrossRef]
- Chawla, R.; Bhalla, P.; Chadha, S.; Grover, S.; Garg, S. Comparison of Hay’s Criteria with Nugent’s Scoring System for Diagnosis of Bacterial Vaginosis. BioMed Res. Int. 2013, 2013, 1–5. [CrossRef]
- Coleman, J.S.; Gaydos, C.A. Molecular Diagnosis of Bacterial Vaginosis: an Update. J. Clin. Microbiol. 2018, 56. [CrossRef]
- Collins, S.L.; McMillan, A.; Seney, S.; van der Veer, C.; Kort, R.; Sumarah, M.W.; Reid, G. Promising Prebiotic Candidate Established by Evaluation of Lactitol, Lactulose, Raffinose, and Oligofructose for Maintenance of a Lactobacillus-Dominated Vaginal Microbiota. Appl. Environ. Microbiol. 2018, 84, e02200-17. [CrossRef]
- Chee, W.J.Y.; Chew, S.Y.; Than, L.T.L. Vaginal microbiota and the potential of Lactobacillus derivatives in maintaining vaginal health. Microb. Cell Factories 2020, 19, 203. [CrossRef]
- Cheng, L.; Norenhag, J.; Hu, Y.O.O.; Brusselaers, N.; Fransson, E.; Ährlund-Richter, A.; Guðnadóttir, U.; Angelidou, P.; Zha, Y.; Hamsten, M.; et al. Vaginal microbiota and human papillomavirus infection among young Swedish women. npj Biofilms Microbiomes 2020, 6, 1–10. [CrossRef]
- Coudray, M.S.; Madhivanan, P. Bacterial vaginosis—A brief synopsis of the literature. Eur. J. Obstet. Gynecol. Reprod. Biol. 2019, 245, 143–148. [CrossRef]
- Chieng, W.K.; Jalal, M.I.A.; Bedi, J.S.; Zainuddin, A.A.; Mokhtar, M.H.; Abu, M.A.; Chew, K.T.; Azurah, A.G.N. Probiotics, a promising therapy to reduce the recurrence of bacterial vaginosis in women? a systematic review and meta-analysis of randomized controlled trials. Front. Nutr. 2022, 9, 938838. [CrossRef]
- Dethlefsen, L.; McFall-Ngai, M.; Relman, D.A. An ecological and evolutionary perspective on human–microbe mutualism and disease. Nature 2007, 449, 811–818. [CrossRef]
- Dareng, E.O.; Ma, B.; Famooto, A.O.; Akarolo-Anthony, S.N.; Offiong, R.A.; Olaniyan, O.; Dakum, P.S.; Wheeler, C.M.; Fadrosh, D.; Yang, H.; et al. Prevalent high-risk HPV infection and vaginal microbiota in Nigerian women. Epidemiology Infect. 2015, 144, 123–137. [CrossRef]
- Donlan, R.M. Preventing biofilms of clinically relevant organisms using bacteriophage. Trends Microbiol. 2009, 17, 66–72. [CrossRef]
- Duar, R.M.; Lin, X.B.; Zheng, J.; Martino, M.E.; Grenier, T.; Pérez-Muñoz, M.E.; Leulier, F.; Gänzle, M.; Walter, J. Lifestyles in transition: evolution and natural history of the genus Lactobacillus. FEMS Microbiol. Rev. 2017, 41, S27–S48. [CrossRef]
- Das Purkayastha, S.; Bhattacharya, M.K.; Prasad, H.K.; Upadhyaya, H.; Das Lala, S.; Pal, K.; Das, M.; Sharma, G.D.; Bhattacharjee, M.J. Contrasting diversity of vaginal lactobacilli among the females of Northeast India. BMC Microbiol. 2019, 19, 1–10. [CrossRef]
- DeLong, K.; Zulfiqar, F.; Hoffmann, D.E.; Tarzian, A.J.; Ensign, L.M. Vaginal Microbiota Transplantation: The Next Frontier. J. Law, Med. Ethic- 2019, 47, 555–567. [CrossRef]
- Delgado-Diaz, D.J.; Jesaveluk, B.; Hayward, J.A.; Tyssen, D.; Alisoltani, A.; Potgieter, M.; Bell, L.; Ross, E.; Iranzadeh, A.; Allali, I.; et al. Lactic acid from vaginal microbiota enhances cervicovaginal epithelial barrier integrity by promoting tight junction protein expression. Microbiome 2022, 10, 1–16. [CrossRef]
- Dequalinium chloride. Health Canada approved product monograph. Revised Sept, 2021. Health Canada. https://pdf.hres.ca/dpd_pm/00063156.PDF (Accessed 25.10. 2022.).
- Eckhart, L.; Lippens, S.; Tschachler, E.; Declercq, W. Cell death by cornification. Biochim. et Biophys. Acta (BBA) - Mol. Cell Res. 2013, 1833, 3471–3480. [CrossRef]
- Evans, J.M., Morris, L.S., Marchesi, J.R., 2013. The gut microbiome: the role of a virtual organ in the endocrinology of the host. J Endocrinol. 218 (3), R37-R47.
- Eastment, M.C.; McClelland, R.S. Vaginal microbiota and susceptibility to HIV. AIDS 2018, 32, 687–698. [CrossRef]
- Ferris, D.G.; Litaker, M.S.; Woodward, L.; Mathis, D.; Hendrich, J. Treatment of bacterial vaginosis: a comparison of oral metronidazole, metronidazole vaginal gel, and clindamycin vaginal cream.. 1995, 41, 443–9.
- Farage, M.A.; Miller, K.W.; Sobel, J.D. Dynamics of the Vaginal Ecosystem—Hormonal Influences. Infect. Dis. Res. Treat. 2010, 3, IDRT.S3903. [CrossRef]
- Flint, H.J.; Scott, K.P.; Louis, P.; Duncan, S.H. The role of the gut microbiota in nutrition and health. Nat. Rev. Gastroenterol. Hepatol. 2022, 9, 577–589. [CrossRef]
- A Greenberg, S.; Youngster, I.; A Cohen, N.; Livovsky, D.M.; Strahilevitz, J.; Israeli, E.; Melzer, E.; Paz, K.; Fliss-Isakov, N.; Maharshak, N. Five years of fecal microbiota transplantation - an update of the Israeli experience. World J. Gastroenterol. 2018, 24, 5403–5414. [CrossRef]
- Greenbaum, S.; Greenbaum, G.; Moran-Gilad, J.; Weintraub, A.Y. Ecological dynamics of the vaginal microbiome in relation to health and disease. Am. J. Obstet. Gynecol. 2019, 220, 324–335. [CrossRef]
- Gupta, S.; Allen-Vercoe, E.; Petrof, E.O. Fecal microbiota transplantation: in perspective. Ther. Adv. Gastroenterol. 2016, 9, 229–239. [CrossRef]
- Happel, A.-U.; Kullin, B.; Gamieldien, H.; Wentzel, N.; Zauchenberger, C.Z.; Jaspan, H.B.; Dabee, S.; Barnabas, S.L.; Jaumdally, S.Z.; Dietrich, J.; et al. Exploring potential of vaginal Lactobacillus isolates from South African women for enhancing treatment for bacterial vaginosis. PLOS Pathog. 2020, 16, e1008559. [CrossRef]
- Hay, P. Life in the littoral zone: lactobacilli losing the plot. Sex. Transm. Infect. 2005, 81, 100–102. [CrossRef]
- Heinemann, C.; Reid, G. Vaginal microbial diversity among postmenopausal women with and without hormone replacement therapy. Can. J. Microbiol. 2005, 51, 777–781. [CrossRef]
- Hans, V., Rita, V., 2009. Bacterial vaginosis: an update on diagnosis and treatment. Expert Rev. Anti Infect. Ther. 7, 1109–1124.
- Hao, W.; Peng, Y.; Xu, W.; Liao, X.; Li, M.; Luo, S. Diversity of vaginal ecosystem on women in Southern China. 2011 International Conference on Information Science and Technology (ICIST). pp. 1254–1261.
- Hill, C.; Guarner, F.; Reid, G.; Gibson, G.R.; Merenstein, D.J.; Pot, B.; Morelli, L.; Canani, R.B.; Flint, H.J.; Salminen, S.; et al. Expert consensus document: The International Scientific Association for Probiotics and Prebiotics consensus statement on the scope and appropriate use of the term probiotic. Nat. Rev. Gastroenterol. Hepatol. 2014, 11, 506–514. [CrossRef]
- Hanssen, N. M. J., de Vos, W. M., Nieuwdorp, M., 2021. Fecal microbiota transplantation in human metabolic diseases: From a murky past to a bright future? Cell Metabolism. 33(6), 1098–1110.
- Hou, K., Wu, Z.X., Chen, X.Y. et al., 2022. Microbiota in health and diseases. Sig Transduct Target Ther. 7, 1-28.
- Macro, O.R.C., International Institute for Population Sciences (IIPS) 2000. National Family Health Survey (NFHS-2), Mumbai, India. 1998, 99, 307-360.
- Jiang, Z.D., Ajami, N.J., Petrosino, J.F., Jun, G., Hanis, C.L. et al., 2017. Hochman L, Ankoma-Sey V, DuPont AW, Wong MC et al (2017) Randomised clinical trial: faecal microbiota transplantation for recurrent Clostridium difficile infection - fresh, or frozen, or lyophilised microbiota from a small pool of healthy donors delivered by colonoscopy. Aliment Pharmacol Ther. 45,899–908.
- Jacob, L., John, M., Kalder, M. & Kostev, K., 2018. Prevalence of vulvovaginal candidiasis in gynecological practices in Germany: a retrospective study of 954,186 patients. Curr. Med. Mycol. 4, 6–11.
- Jain, J.P.; Bristow, C.C.; Pines, H.A.; Harvey-Vera, A.; Rangel, G.; Staines, H.; Patterson, T.L.; Strathdee, S.A. Factors in the HIV risk environment associated with bacterial vaginosis among HIV-negative female sex workers who inject drugs in the Mexico-United States border region. BMC Public Heal. 2018, 18, 1032. [CrossRef]
- Javed, A., Parvaiz, F., Manzoor, S., 2019. Bacterial vaginosis: An insight into the prevalence, alternative treatments regimen and it's associated resistance patterns. Microb Pathog.127, 21-30.
- Jakobsen, R.R.; Haahr, T.; Humaidan, P.; Jensen, J.S.; Kot, W.P.; Castro-Mejia, J.L.; Deng, L.; Leser, T.D.; Nielsen, D.S. Characterization of the Vaginal DNA Virome in Health and Dysbiosis. Viruses 2020, 12, 1143. [CrossRef]
- Junca, H.; Pieper, D.H.; Medina, E. The emerging potential of microbiome transplantation on human health interventions. Comput. Struct. Biotechnol. J. 2022, 20, 615–627. [CrossRef]
- Koumans, E.H.; Markowitz, L.E.; Hogan, V.; the CDC BV Working Group Indications for Therapy and Treatment Recommendations for Bacterial Vaginosis in Nonpregnant and Pregnant Women: A Synthesis of Data. Clin. Infect. Dis. 2002, 35, S152–S172. [CrossRef]
- Kelly, C.R.; Kahn, S.; Kashyap, P.; Laine, L.; Rubin, D.; Atreja, A.; Moore, T.; Wu, G. Update on Fecal Microbiota Transplantation 2015: Indications, Methodologies, Mechanisms, and Outlook. Gastroenterology 2015, 149, 223–237. Erratum in 2015, 149, 223–237. [CrossRef]
- Kaushic, C., Nguyen, P.V., 2016. Immunology of the female reproductive mucosa. Encyclopedia Immunobiology. 63–72.
- Kim, J.-M.; Park, Y.J. Probiotics in the Prevention and Treatment of Postmenopausal Vaginal Infections: Review Article. J. Menopausal Med. 2017, 23, 139–145. [CrossRef]
- Kolaček, S., et al., 2017. Commercial probiotic products: a call for improved quality control. A position paper by the ESPGHAN working group for probiotics and prebiotics. J. Pediatr. Gastroenterol. Nutr. 65 (1), 117–124.
- Khangwal, I.; Shukla, P. Prospecting prebiotics, innovative evaluation methods, and their health applications: a review. 3 Biotech 2019, 9, 1–7. [CrossRef]
- Kalia, N.; Singh, J.; Kaur, M. Microbiota in vaginal health and pathogenesis of recurrent vulvovaginal infections: a critical review. Ann. Clin. Microbiol. Antimicrob. 2020, 19, 1–19. [CrossRef]
- Larsson, P.-G.; Brandsborg, E.; Forsum, U.; Pendharkar, S.; Andersen, K.K.; Nasic, S.; Hammarström, L.; Marcotte, H. Extended antimicrobial treatment of bacterial vaginosis combined with human lactobacilli to find the best treatment and minimize the risk of relapses. BMC Infect. Dis. 2011, 11, 223–223. [CrossRef]
- Lozupone, C.A.; Stombaugh, J.I.; Gordon, J.I.; Jansson, J.K.; Knight, R. Diversity, stability and resilience of the human gut microbiota. Nature 2012, 489, 220–230. [CrossRef]
- Lev-Sagie, A.; Goldman-Wohl, D.; Cohen, Y.; Dori-Bachash, M.; Leshem, A.; Mor, U.; Strahilevitz, J.; Moses, A.E.; Shapiro, H.; Yagel, S.; et al. Vaginal microbiome transplantation in women with intractable bacterial vaginosis. Nat. Med. 2019, 25, 1500–1504. [CrossRef]
- Landlinger, C.; Tisakova, L.; Oberbauer, V.; Schwebs, T.; Muhammad, A.; Latka, A.; Van Simaey, L.; Vaneechoutte, M.; Guschin, A.; Resch, G.; et al. Engineered Phage Endolysin Eliminates Gardnerella Biofilm without Damaging Beneficial Bacteria in Bacterial Vaginosis Ex Vivo. Pathogens 2021, 10, 54. [CrossRef]
- Liu, H.-F.; Yi, N. A systematic review and meta-analysis on the efficacy of probiotics for bacterial vaginosis. 2022, 26, 90–98. [CrossRef]
- Mikamo, H., Sato., Hayasaki, Y. et al., 2000. Vaginal microflora in healthy women with Gardnerella vaginalis. J Infect Chemother. 6(3), 173–177.
- Martinez, R.C.R.; Franceschini, S.A.; Patta, M.C.; Quintana, S.M.; Nunes, A.C.; Moreira, J.L.S.; Anukam, K.C.; Reid, G.; De Martinis, E.C.P. Analysis of Vaginal Lactobacilli from Healthy and Infected Brazilian Women. Appl. Environ. Microbiol. 2008, 74, 4539–4542. [CrossRef]
- Menard, J.-P. Antibacterial treatment of bacterial vaginosis: current and emerging therapies. Int. J. Women's Heal. 2011, 3, 295–305. [CrossRef]
- Ma, B.; Forney, L.J.; Ravel, J. Vaginal Microbiome: Rethinking Health and Disease. Annu. Rev. Microbiol. 2012, 66, 371–389. [CrossRef]
- Maynard, C.L.; Elson, C.O.; Hatton, R.D.; Weaver, C.T. Reciprocal interactions of the intestinal microbiota and immune system. Nature 2012, 489, 231–241. [CrossRef]
- Menon, G.K.; Cleary, G.W.; Lane, M.E. The structure and function of the stratum corneum. Int. J. Pharm. 2012, 435, 3–9. [CrossRef]
- Mastromarino, P.; Hemalatha, R.; Barbonetti, A.; Cinque, B.; Cifone, M.; Tammaro, F.; Francavilla, F. Biological control of vaginosis to improve reproductive health. 2014, 140, S91–S97.
- Mendling, W., 2016. Vaginal Microbiota. Advances in experimental medicine and biology. 902, 83–93.
- Miller, E.A.; Beasley, D.E.; Dunn, R.R.; Archie, E.A. Lactobacilli Dominance and Vaginal pH: Why Is the Human Vaginal Microbiome Unique?. Front. Microbiol. 2016, 7, 1936. [CrossRef]
- Myles, I. A., Earland, N. J., Anderson, E. D., Moore, I. N. et al., 2019. First-in-human topical microbiome transplantation with Roseomonas mucosa for atopic dermatitis. JCI insight, 3(9), e120608. Ma D, Chen Y, Chen T. Vaginal microbiota transplantation for the treatment of bacterial vaginosis: a conceptual analysis. FEMS Microbiol Lett. 366(4), 1-13. [CrossRef]
- Marrazzo, J.M.; Dombrowski, J.C.; Wierzbicki, M.R.; Perlowski, C.; Pontius, A.; Dithmer, D.; Schwebke, J. Safety and Efficacy of a Novel Vaginal Anti-infective, TOL-463, in the Treatment of Bacterial Vaginosis and Vulvovaginal Candidiasis: A Randomized, Single-blind, Phase 2, Controlled Trial. Clin. Infect. Dis. 2019, 68, 803–809. [CrossRef]
- Muzny, C.A.; Łaniewski, P.; Schwebke, J.R.; Herbst-Kralovetz, M.M. Host–vaginal microbiota interactions in the pathogenesis of bacterial vaginosis. Curr. Opin. Infect. Dis. 2020, 33, 59–65. [CrossRef]
- Muzny, C.A.M.; Kardas, P. A Narrative Review of Current Challenges in the Diagnosis and Management of Bacterial Vaginosis. Sex. Transm. Dis. 2020, 47, 441–446. [CrossRef]
- Nurainiwati, S.A.; Ma'Roef, M.; Pravitasari, D.N.; Putra, P.Y.P. Effectivity and efficacy probiotics for Bacterial Vaginosis treatments: Meta-analysis. Infect. Dis. Model. 2022, 7, 597–604. [CrossRef]
- Ochiel, D.O.; Fahey, J.V.; Ghosh, M.; Haddad, S.N.; Wira, C.R. Innate Immunity in the Female Reproductive Tract: Role of Sex Hormones in Regulating Uterine Epithelial Cell Protection Against Pathogens. Curr. Women s Heal. Rev. 2008, 4, 102–117. [CrossRef]
- Oduyebo, O.; I Anorlu, R.; Ogunsola, F.T. The effects of antimicrobial therapy on bacterial vaginosis in non-pregnant women. Cochrane Database Syst. Rev. 2009, CD006055. [CrossRef]
- Oyinlola, O. O., Rose, I. A., Folasade, T. O., 2009. The effects of antimicrobial therapy on bacterial vaginosis in non-pregnant women. Cochrane Database Syst. Rev. 8, CD006055.
- E O'Hanlon, D.; Moench, T.R.; A Cone, R. In vaginal fluid, bacteria associated with bacterial vaginosis can be suppressed with lactic acid but not hydrogen peroxide. BMC Infect. Dis. 2011, 11, 200–200. [CrossRef]
- O’hanlon, D.E.; Moench, T.R.; Cone, R.A. Vaginal pH and Microbicidal Lactic Acid When Lactobacilli Dominate the Microbiota. PLOS ONE 2011, 8, e80074. [CrossRef]
- Onderdonk, A.B.; Delaney, M.L.; Fichorova, R.N. The Human Microbiome during Bacterial Vaginosis. Clin. Microbiol. Rev. 2016, 29, 223–238. [CrossRef]
- Otsuki, K.; Imai, N. Effects of lactoferrin in 6 patients with refractory bacterial vaginosis. Biochem. Cell Biol. 2017, 95, 31–33. [CrossRef]
- Oliveira, H.; São-José, C.; Azeredo, J. Phage-Derived Peptidoglycan Degrading Enzymes: Challenges and Future Prospects for In Vivo Therapy. Viruses 2018, 10, 292. [CrossRef]
- Petrova, M.I., Marianne, V.D.B., Jan, B. et al., 2013. Vaginal microbiota and its role in HIV transmission and infection. Fems Microbiol Rev, 37:762–92.
- Pilla, R.; Gaschen, F.P.; Barr, J.W.; Olson, E.; Honneffer, J.; Guard, B.C.; Blake, A.B.; Villanueva, D.; Khattab, M.R.; AlShawaqfeh, M.K.; et al. Effects of metronidazole on the fecal microbiome and metabolome in healthy dogs. J. Veter- Intern. Med. 2020, 34, 1853–1866. [CrossRef]
- Plummer, E.L.; Bradshaw, C.S.; Doyle, M.; Fairley, C.K.; Murray, G.L.; Bateson, D.; Masson, L.; Slifirski, J.; Tachedjian, G.; Vodstrcil, L.A. Lactic acid-containing products for bacterial vaginosis and their impact on the vaginal microbiota: A systematic review. PLOS ONE 2021, 16, e0246953. [CrossRef]
- Bascuñana, R.P.; Veses, V.; Sheth, C. Effectiveness of fecal microbiota transplant for the treatment of Clostridioides difficile diarrhea: a systematic review and meta-analysis. Lett. Appl. Microbiol. 2021, 73, 149–158. [CrossRef]
- Quraishi, M.N.; Widlak, M.; Bhala, N.; Moore, D.; Price, M.; Sharma, N.; Iqbal, T.H. Systematic review with meta-analysis: the efficacy of faecal microbiota transplantation for the treatment of recurrent and refractory Clostridium difficile infection. Aliment. Pharmacol. Ther. 2017, 46, 479–493. [CrossRef]
- Reid, G., Charbonneau, D., Erb, J. et al., 2003. Oral use of Lactobacillus rhamnosus GR-1 and L. fermentum RC-14 significantly alters vaginal flora: randomized, placebo-controlled trial in 64 healthy women. Fems Immunol Med Mic. 35 (2), 131–134.
- Rousseau, V.; Lepargneur, J.; Roques, C.; Remaud-Simeon, M.; Paul, F. Prebiotic effects of oligosaccharides on selected vaginal lactobacilli and pathogenic microorganisms. Anaerobe 2005, 11, 145–153. [CrossRef]
- Rönnqvist, P.D.J.; Forsgren-Brusk, U.B.; Grahn-Håkansson, E.E. Lactobacilli in the female genital tract in relation to other genital microbes and vaginal pH. Acta Obstet. et Gynecol. Scand. 2006, 85, 726–735. [CrossRef]
- Reichman, O.; Akins, R.; Sobel, J.D. Boric Acid Addition to Suppressive Antimicrobial Therapy for Recurrent Bacterial Vaginosis. Sex. Transm. Dis. 2009, 36, 732–734. [CrossRef]
- Robinson, C.J.; Bohannan, B.J.M.; Young, V.B. From Structure to Function: the Ecology of Host-Associated Microbial Communities. Microbiol. Mol. Biol. Rev. 2010, 74, 453–476. [CrossRef]
- Raybardhan, S.; Ng, W.; Tomassi, J.; Katz, K. Self-stool banking as a source for fecal microbiota transplantation: A pilot study. Off. J. Assoc. Med Microbiol. Infect. Dis. Can. 2017, 2, 9–14. [CrossRef]
- Redelinghuys, M.J.; Ehlers, M.M.; Dreyer, A.W.; Kock, M.M. Normal flora and bacterial vaginosis in pregnancy: an overview. Crit. Rev. Microbiol. 2016, 42, 1–12. [CrossRef]
- Russo, R., Karadja, E., & De Seta, F., 2019. Evidence-based mixture containing Lactobacillus strains and lactoferrin to prevent recurrent bacterial vaginosis: a double blind, placebo controlled, randomised clinical trial. Beneficial microbes. 10 (1), 19–26.
- Sobel, J.D.; Schmitt, C.; Meriwether, C. Long-Term Follow-Up of Patients with Bacterial Vaginosis Treated with Oral Metronidazole and Topical Clindamycin. J. Infect. Dis. 1993, 167, 783–784. [CrossRef]
- Stappenbeck, T.S.; Hooper, L.V.; Gordon, J.I. Developmental regulation of intestinal angiogenesis by indigenous microbes via Paneth cells. Proc. Natl. Acad. Sci. 2002, 99, 15451–15455. [CrossRef]
- Stoyancheva, G.; Marzotto, M.; Dellaglio, F.; Torriani, S. Bacteriocin production and gene sequencing analysis from vaginal Lactobacillus strains. Arch. Microbiol. 2014, 196, 645–653. [CrossRef]
- Srinivasan, S.; Morgan, M.T.; Fiedler, T.L.; Djukovic, D.; Hoffman, N.G.; Raftery, D.; Marrazzo, J.M.; Fredricks, D.N. Metabolic Signatures of Bacterial Vaginosis. mBio 2015, 6, e00204-15. [CrossRef]
- Smith, S.B.; Ravel, J. The vaginal microbiota, host defence and reproductive physiology. J. Physiol. 2016, 595, 451–463. [CrossRef]
- Serrano, M.G.; Parikh, H.I.; Edwards, D.J.; Arodz, T.J.; Edupuganti, L.; Huang, B.; Girerd, P.H.; Bokhari, Y.A.; Bradley, S.P.; Brooks, J.L.; et al. Racioethnic diversity in the dynamics of the vaginal microbiome during pregnancy. Nat. Med. 2019, 25, 1001–1011. [CrossRef]
- Shukla, A.; Sobel, J.D. Vulvovaginitis Caused by Candida Species Following Antibiotic Exposure. Curr. Infect. Dis. Rep. 2019, 21, 44. [CrossRef]
- Secnidasole oral granules. US Food and Drug Administration (FDA) approved product information. Revised September 2017. US National Library of Medicine. Available at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2021/209363s015lbl.pdf (Accessed on June 17.06. 2021).
- Surapaneni, S.; Akins, R.; Sobel, J.D. Recurrent Bacterial Vaginosis: An Unmet Therapeutic Challenge. Experience With a Combination Pharmacotherapy Long-Term Suppressive Regimen. Sex. Transm. Dis. 2021, 48, 761–765. [CrossRef]
- Tibaldi, C.; Cappello, N.; Latino, M.; Masuelli, G.; Marini, S.; Benedetto, C. Vaginal and endocervical microorganisms in symptomatic and asymptomatic non-pregnant females: risk factors and rates of occurrence. Clin. Microbiol. Infect. 2009, 15, 670–679. [CrossRef]
- Tominaga, K.; Sato, S.; Hayashi, M. Activated charcoal as an effective treatment for bacterial vaginosis. Pers. Med. Universe 2012, 1, 54–57. [CrossRef]
- Tachedjian, G.; O’hanlon, D.E.; Ravel, J. The implausible “in vivo” role of hydrogen peroxide as an antimicrobial factor produced by vaginal microbiota. Microbiome 2018, 6, 29. [CrossRef]
- Tinidazole tablet. US Food and Drug Administration (FDA) approved product information. Revised Dec, 2019. US National Library of Medicine. Available at: https://dailymed.nlm.nih.gov/dailymed/ (Accessed on 30.04.2021).
- Vallor, A.C.; Antonio, M.A.D.; Hawes, S.E.; Hillier, S.L. Factors Associated with Acquisition of, or Persistent Colonization by, Vaginal Lactobacilli: Role of Hydrogen Peroxide Production. J. Infect. Dis. 2001, 184, 1431–1436. [CrossRef]
- Vodstrcil, L.A.; Muzny, C.A.; Plummer, E.L.; Sobel, J.D.; Bradshaw, C.S. Bacterial vaginosis: drivers of recurrence and challenges and opportunities in partner treatment. BMC Med. 2021, 19, 1–12. [CrossRef]
- Vieira-Baptista, P.; De Seta, F.; Verstraelen, H.; Ventolini, G.M.; Lonnee-Hoffmann, R.; Lev-Sagie, A. The Vaginal Microbiome: V. Therapeutic Modalities of Vaginal Microbiome Engineering and Research Challenges. J. Low. Genit. Tract Dis. 2022, 26, 99–104. [CrossRef]
- Vitali, B.; Abruzzo, A.; Parolin, C.; Palomino, R.A..; Dalena, F.; Bigucci, F.; Cerchiara, T.; Luppi, B. Association of Lactobacillus crispatus with fructo-oligosaccharides and ascorbic acid in hydroxypropyl methylcellulose vaginal insert. Carbohydr. Polym. 2016, 136, 1161–1169. [CrossRef]
- Vijay, A., & Valdes, A. M., 2022. Role of the gut microbiome in chronic diseases: a narrative review. European journal of clinical nutrition. 76(4), 489–501.
- Wira, C.R.; Fahey, J.V.; Sentman, C.L.; Pioli, P.A.; Shen, L. Innate and adaptive immunity in female genital tract: cellular responses and interactions. Immunol. Rev. 2005, 206, 306–335. [CrossRef]
- Baroni, A.; Buommino, E.; De Gregorio, V.; Ruocco, E.; Ruocco, V.; Wolf, R. Structure and function of the epidermis related to barrier properties. Clin. Dermatol. 2012, 30, 257–262. [CrossRef]
- Wang, Z.; He, Y.; Zheng, Y. Probiotics for the Treatment of Bacterial Vaginosis: A Meta-Analysis. Int. J. Environ. Res. Public Health 2019, 16, 3859. [CrossRef]
- Wu, S.; Hugerth, L.W.; Schuppe-Koistinen, I.; Du, J. The right bug in the right place: opportunities for bacterial vaginosis treatment. npj Biofilms Microbiomes 2022, 8, 1–11. [CrossRef]
- Xiao, Y.; Angulo, M.T.; Lao, S.; Weiss, S.T.; Liu, Y.-Y. An ecological framework to understand the efficacy of fecal microbiota transplantation. Nat. Commun. 2020, 11, 1–17. [CrossRef]
- Yazdanbakhsh, M., Kremsner, P. G., van Ree, R., 2002. Allergy, parasites, and the hygiene hypothesis. Science (New York, N.Y.). 296 (5567), 490–494.
- Youngster, I.; Mahabamunuge, J.; Systrom, H.K.; Sauk, J.; Khalili, H.; Levin, J.; Kaplan, J.L.; Hohmann, E.L. Oral, frozen fecal microbiota transplant (FMT) capsules for recurrent Clostridium difficile infection. BMC Med. 2016, 14, 1–4. [CrossRef]
- Yadav, D., Khanna, S., 2021. Safety of fecal microbiota transplantation for Clostridioides difficile infection focusing on pathobionts and SARS-CoV-2. Therapeutic advances in gastroenterology. 14, 1-11.
- Zoetendal, E.G.; Cheng, B.; Koike, S.; I Mackie, R. Molecular microbial ecology of the gastrointestinal tract: from phylogeny to function.. 2004, 5, 31–47.
- Zeng, Z.-M.; Liao, Q.-P.; Yao, C.; Geng, L.; Feng, L.-H.; Shi, H.-R.; Xin, X.-Y.; Li, P.; Wang, H.-L.; Pang, Y.-C.; et al. Directed shift of vaginal flora after topical application of sucrose gel in a phase III clinical trial: a novel treatment for bacterial vaginosis. Chinese medical journal 2010, 123, 2051–7.
- Terrier, M.-C.Z.; Frossard, J.-L.; Simonet, M.L. [Recurrent Clostridium difficile infections: the importance of the intestinal microbiota]. World journal of gastroenterology 2014, 9, 1898, 1900–4.
- Zimmermann, P.; Curtis, N. The effect of antibiotics on the composition of the intestinal microbiota - a systematic review. J. Infect. 2019, 79, 471–489. [CrossRef]
- Zmora, N.; Soffer, E.; Elinav, E. Transforming medicine with the microbiome. Sci. Transl. Med. 2019, 11, eaaw1815. [CrossRef]
- Zhang, Q.; Zhang, L.; Ross, P.; Zhao, J.; Zhang, H.; Chen, W. Comparative Genomics of Lactobacillus crispatus from the Gut and Vagina Reveals Genetic Diversity and Lifestyle Adaptation. Genes 2020, 11, 360. [CrossRef]
- Sadhu, S.; Rizvi, Z.A.; Pandey, R.P.; Dalal, R.; Rathore, D.K.; Kumar, B.; Pandey, M.; Kumar, Y.; Goel, R.; Maiti, T.K.; et al. Gefitinib Results in Robust Host-Directed Immunity Against Salmonella Infection Through Proteo-Metabolomic Reprogramming. Front. Immunol. 2021, 12. [CrossRef]
- Pandey RP, Kumar S, Ahmad S, Vibhuti A, Raj VS, Verma AK, Sharma P, Leal E. Use Chou's 5-steps rule to evaluate protective efficacy induced by antigenic proteins of Mycobacterium tuberculosis encapsulated in chitosan nanoparticles. Life Sci. 2020 Sep 1;256:117961.
- Kumar, S., Singh, M. P., Bharti, V. K., & Pandey, R. P. (2018). Quality control ofvaccines-A journey from classical approach to 3Rs. Microbiology: CurrentResearch, 2(3), 45-61.
- Pandey, R.P.; Mukherjee, R.; Chang, C.-M. Emerging Concern with Imminent Therapeutic Strategies for Treating Resistance in Biofilm. Antibiotics 2022, 11, 476. [CrossRef]
- Pandey, R.P.; Mukherjee, R.; Priyadarshini, A.; Gupta, A.; Vibhuti, A.; Leal, E.; Sengupta, U.; Katoch, V.M.; Sharma, P.; Moore, C.E.; et al. Potential of nanoparticles encapsulated drugs for possible inhibition of the antimicrobial resistance development. Biomed. Pharmacother. 2021, 141, 111943. [CrossRef]
Figure 1.
Treatment options for BV.
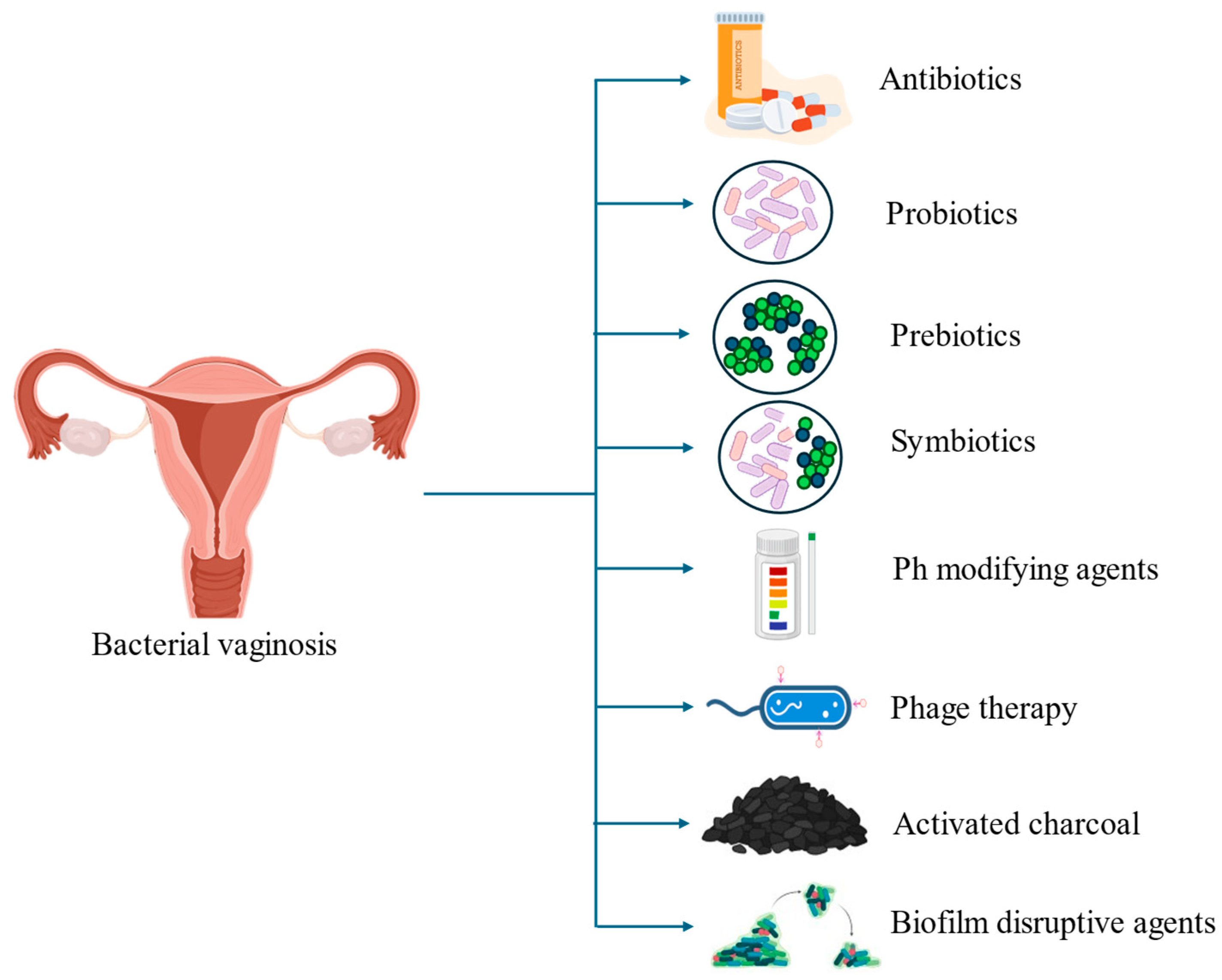
Figure 2.
Pathological changes in the vaginal microbiome during BV, where overgrowth of anaerobic bacteria leads to mucosal breakdown, discharge, and a fishy Odor. This imbalance reduces Lactobacillus dominance, increasing infection risk. Treatment restores balance by reintroducing Lactobacillus through antibiotics, pH-modifying agents, or probiotics, reducing harmful bacteria and promoting a healthy vaginal environment.
Figure 2.
Pathological changes in the vaginal microbiome during BV, where overgrowth of anaerobic bacteria leads to mucosal breakdown, discharge, and a fishy Odor. This imbalance reduces Lactobacillus dominance, increasing infection risk. Treatment restores balance by reintroducing Lactobacillus through antibiotics, pH-modifying agents, or probiotics, reducing harmful bacteria and promoting a healthy vaginal environment.
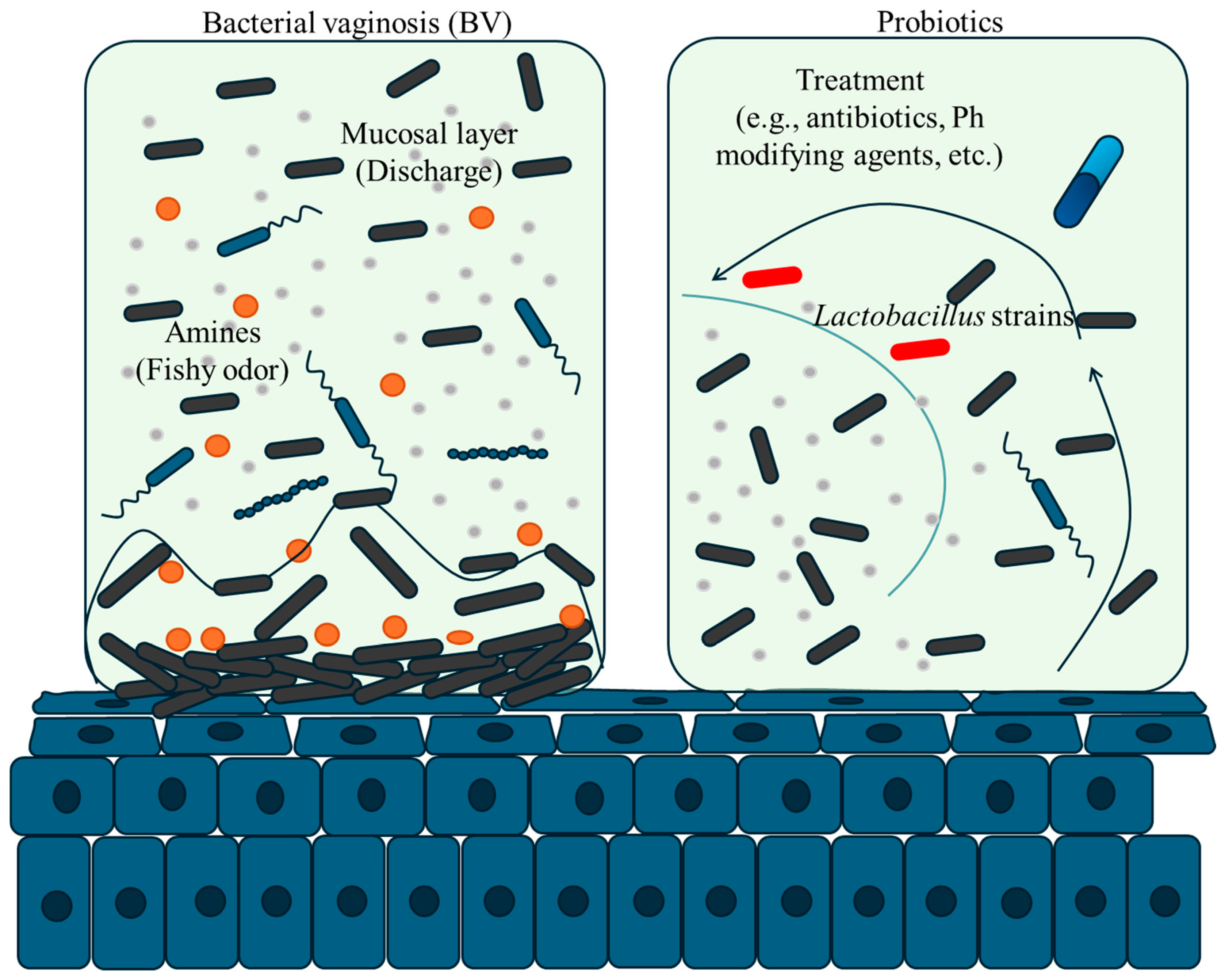

Table 1.
Treatment options for BV (non-pregnant females or persons with a vagina).
| S. No | Therapies | Dose | Duration | Adverse effects | References |
| 1. | Metronidazole | 400 mg orally for every 12 hours or 0.75% gel 5 g once daily | 5-7 days 5 days |
Metallic taste, nausea, and transient neutropenia | Muzny and Kardas, 2020 |
| 2. | Clindamycin | 300 mg orally every 12 hours or 100 mg intravaginally once daily |
7 days 3 days |
Vulvovaginal candidiasis and gastrointestinal side effects. |
https://dailymed.nlm.nih.gov/dailymed/ (Accessed 28, 06.2021). |
| 3. | Tinidazole | 2 g orally once daily 1 g orally once daily |
2 days 5 days |
Metallic/bitter taste, nausea, and weakness or fatigue | https://dailymed.nlm.nih.gov/dailymed/ (Accessed 30.04.2021 |
| 4. | Secnidazole | 2 g packet (orally) once | Vulvovaginal candidiasis. Headache, nausea, diarrhoea and abdominal pain | https://www.accessdata.fda.gov/drugsatfda_docs/label/2021/209363s015lbl.pdf (Accessed 17.06. 2021 | |
| 5. | Dequalinium chloride | 10 mg tablet intra vaginally | 6 nights | Product use is limited |
https://pdf.hres.ca/dpd_pm/00063156.PDF (Accessed 25.08. 2022). |
Table 2.
Effect of prebiotics treatment in BV.
| S. No. | Prebiotics | Beneficial effects | Adverse effect | References |
| 1. | Oligosaccharides | Selectively help in promoting the enrichment of lactobacilli Increase lactic acid production Prevent the growth of anaerobic bacteria by inhibiting adhesion and replication through the secretion of antibacterial substances. |
Not observed | Rousseau et al, 2005 |
| 2. | Vaginal sucrose gel (5g) for 5 continuous days as twice daily | Therapeutic cure rate was 61% after 21–35 days treatment At 5-7 days, the Nugent score showed significantly higher levels of lactobacilli in the sucrose gel group treatment as versus the metronidazole group. |
Promote the development of candidiasis | Zeng et al, 2010 |
| 3. | Disaccharide lactulose | Promote the enrichment of vaginal lactobacilli including L. crispatus and non-stimulating of C. albicans and other harmful bacteria spotted in BV. | Not observed | Collins et al, 2018 |
| 4 | Trifolium pratense (red clover) extract and Galacto-oligosaccharides | Nugent score ≤ 3 | Not observed | Coste et al, 2012 |
| 5. | Lactoferrin treatment for 1 month | Improved the BV by gradual increasing of lactobacilli | Not observed | Otsuki and Imai, 2017 |
Table 3.
Summary of clinical results of recent microbiome transplantation studies.
| Citations ClinicalTrials.gov Identifier | Population | Study Focus | Primary cure rate |
| Kelly et al, 2015 | N=46 | FMT vs Antibiotic | 91% |
| Youngster et al, 2016 | N=180 | FMT Delivery Method | 82% |
| Jiang e al, 2017 | N=72 | FMT Material Processing | 100% |
| Myles et al, 2018 | N=15 | Topical Microbiome Transplant | 75% |
| Lev-Sagie et al, 2019 | N=5 | VMT for Recurrent Bacterial Vaginosis | 75% |
| NCT04046900 | N=134 | VMT for Recurrent Bacterial Vaginosis | Primary completion on December 2024 |
| NCT04517487 | N=100 | Biological: Vaginal Microbiome Transplantation | Primary completion on December 2024 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



