Submitted:
04 October 2024
Posted:
04 October 2024
You are already at the latest version
Abstract
Background/Objectives: Successfully weaning patients with prolonged mechanical ventilation (PMV: ≥21 days) from ventilators is a challenging process, and proper nutritional support is a crucial factor in this process. Previous studies have highlighted the significance of higher albumin levels and increased daily protein intake in predicting successful weaning among PMV patients. However, the importance of calorie intake in patients with PMV has remained unclear. Methods: This retrospective study included 1,038 adult patients (age >18 years) who underwent endotracheal intubation or tracheostomy and required mechanical ventilation for >21 days. Baseline characteristics, nutritional variables, disease severity, management factors and patient outcomes (hospital stay and duration of ventilator use) were analyzed between the weaning-failure and weaning-success sub-cohorts and factors associated with successful weaning were identified. Results: The participants had mean APACHE II score of 18 and a Day 1 SOFA score of 4.9 and the successful weaning rate was 70%. Multivariate logistic regression analysis revealed that higher albumin and hemoglobin levels, the absence of shock, less positive fluid status, and higher calorie intake were associated with a higher successful weaning rate; an average calorie intake higher than 25 kcal/kg/day during respiratory care center (RCC) stay predicted better successful ventilator weaning. Conclusions: Higher daily calorie intake in the RCC is associated with more successful ventilator weaning, and an average intake exceeding 25 kcal/kg/day is recommended for optimizing the weaning process.
Keywords:
calorie intake
; prolonged mechanical ventilation
; ventilator weaning
; respiratory care center
1. Introduction
Prolonged mechanical ventilation (PMV), which is defined as the provision of mechanical ventilation (≥6 h daily) for more than 21 days, is associated with poorer outcomes and higher cost [1,2,3,4]. Successful weaning from mechanical ventilation at hospital discharge reduced the in-hospital and 1-year mortality rates [3]. In patients with PMV, female sex, mechanical power normalized to the lung–thorax compliance, obesity (body mass index ≥30 kg/m2) and hypercapnia constitute potential predictors of weaning failure [5] whereas increased tidal volume/ideal body weight and decreased rapid shallow breathing index (RSBI) independently predicted weaning success [6].
The provision of adequate nutrition is an important contributor for survival and shortens the time to discharge in the critically ill population [7,8]. In inpatients, malnutrition affects lung structure and function and leads to poor respiratory muscle contraction, weakened ventilatory capacity, reduced respiratory endurance, and changes in respiratory mechanisms that prolong the duration of respirator dependence [7,8]. Malnutrition-induced respiratory muscle weakness mainly affects the diaphragm and is potentially related to reduced mitochondrial oxygen consumption [7]. Huang et al. [9] reported that, after 14-day hospitalization, 94% of intensive care unit (ICU) patients were malnourished. Furthermore, malnutrition increased the infection rate, morbidity, mortality, and length of hospital stay of in-patients [10,11]. The 2019 European Society for Parenteral and Enteral Nutrition (ESPEN) guidelines recommended that hypocaloric nutrition (≤70% of energy expenditure) should be administered in the early phase of acute illness and that, after Day 3, caloric delivery can be increased to 80–100% [12]. Weijs et al. found that early energy overfeeding correlated with a higher mortality risk [13]. The 2019 ESPEN guidelines recommended 20–25 kcal/kg/day [12] whereas the American Society for Parenteral and Enteral Nutrition (ASPEN) and the Society of Critical Care Medicine (SCCM) guidelines recommended energy requirements of 25-30 kcal/kg/day [14] caloric intake for critically ill patients. However, no formal nutritional therapy recommendations or guidelines on energy intake are available for the post-ICU hospital stay. Many survivors of critical illness face significant physical and psychological disability following ICU discharge and are frequently malnourished, which is associated with poor outcomes [15,16]. Thus, nutrition remains problematic, particularly in the early phases of ICU recovery. Optimal caloric intake is necessary to enhance recovery and prevent further loss of functional muscle mass. Although nutritional therapy for patients in the early phases of critical illness is well studied [13,17,18], the association of calorie intake with PMV outcomes remains relatively unelucidated.
In this study, we aimed to investigate the impact of calorie intake on weaning from mechanical ventilation in patients with PMV.
2. Materials and Methods
2.1. Study Design and Patient Enrollment
In this retrospective cohort study, we investigated patients who were treated at the respiratory care center (RCC) of Taichung Veterans General Hospital (TCVGH) – a tertiary referral center in Taiwan – from July 2015 to December 2020. In this study, after screening 1282 patients, we enrolled 1038 adult patients (aged ≥18 years) who underwent endotracheal intubation or tracheostomy and required mechanical ventilation for >21 days (Figure 1). We excluded patients with an RCC stay of <3 days, those with multiple admissions, or those without an APACHE II score recorded at the RCC. This study was conducted in accordance with the Declaration of Helsinki and the relevant guidelines and regulations for clinical research and was approved by the Institutional Review Board of Taichung Veterans General Hospital (IRB No. CE23044C). The requirement for informed consent was waived because of the retrospective nature of the study, and the patients’ personal information was deidentified prior to analysis.
The RCC is a specialized unit that is intended for patients with respiratory failure who are recovering from acute decompensated organ failure and cannot be successfully weaned off the ventilator in the ICU for >21 days. In the RCC, patients receive individualized pulmonary rehabilitation and nutritional support to improve their respiratory function, along with standardized weaning protocols to help them gradually transition to spontaneous breathing and eventually discontinue ventilator use.
2.2. Data Collection and Outcome Measures
As the interleukin-6 (IL-6) level is not routinely measured in most ICUs, a modified Nutrition Risk in the Critically Ill (mNUTRIC) score without the IL-6 level was used [19]. Critically ill patients with an mNUTRIC score ≥5 were identified as being at high nutritional risk. Patient characteristics encompassed basic characteristics (age, sex, and Charlson Comorbidity Index [CCI]), nutritional variables (body mass index, mNUTRIC) scores, albumin, hemoglobin), and illness severity and management parameters (Acute Physiology and Chronic Health Evaluation II [APACHE II] scores [20], Day 1 Sequential Organ Failure Assessment (SOFA) score [21], presence of shock, renal replacement therapy, the first 7-day fluid balance, the first 7-day calorie intake and total calorie/BW) in the RCC. Outcome measurements included hospital stay and duration of ventilator use (days). Successful weaning was defined the attainment of spontaneous breathing for ≥48 hours without mechanical ventilator support [22].
2.3. Statistical Analysis
Data were processed using SPSS (version 22.0; International Business Machines Corp, Armonk, NY, USA). Categorical variables were presented as the frequency and proportion, and intergroup differences were expressed using the chi-square and Fisher’s exact tests. Continuous variables were presented as the mean with standard deviation (SD), and intergroup differences were expressed using the Mann–Whitney U and chi-square tests. Multivariate logistic regression was performed to determine the odds ratio (OR) and 95% confidence interval (CI) for successful weaning. All tests were two-sided, and p<0.05 was considered statistically significant.
3. Results
3.1. Clinicodemographic Characteristics of the Participants
We screened 1282 patients who were treated at the RCC, and enrolled 1038 participants (Figure 1), of whom 726 (69.9%) were weaned successfully, and 312 (30.1%) experienced weaning failure.
The groupwise stratification of the characteristics, including baseline characteristics, nutritional variables, illness severity and management, and outcomes, are summarized in Table 1. In this study cohort (n=1038), the mean age was 68.51 years and 57.32% were male. The participants had mean mNUTRIC, APACHE II, and SOFA scores of 4.1, 18, and 4.9, respectively. Regarding disease severity, 11.08% of patients experienced shock, and this includes those who had norepinephrine-alone use (7.9%) and norepinephrine with other vasopressors use (3.18%). The mean daily calorie intake in the initial 7-day hospital stay was 1151.35 kcal/day and the total calorie/BW intake was 20.68 kcal/kg/day. The durations of hospital stay and ventilator use were 57.87 and 41.16 days, respectively (Table 1).
3.2. Intergroup Differences between the Weaning-Failure and Weaning-Success Sub-Cohorts
Regarding the baseline characteristics and nutritional variables, compared to those in weaning-failure group, patients in the weaning success group were younger (p = 0.001) and had lower CCI and mNUTRIC score but had higher albumin and hemoglobin levels (p<0.001) (Table 1). In disease severity and management factors, the APACHE II score and day 1 SOFA score were lower, and absence of shock (p < 0.001) was higher in the weaning success patients. Use of vasopressors, renal replacement therapy and the first 7-day fluid balance were higher in the weaning failure patients. The average of first 7-day calories intake and total calories/BW intake (p < 0.001) were higher in weaning success group. Regarding to patient outcomes, ventilator day was lower in weaning success group. There was no significant difference in sex, body mass index and hospital stay between the two groups (Table 1).
3.3. Daily Calorie Intake in PMV Patients Stratified by Successful Weaning
To ascertain the association of daily calorie intake with successful weaning in patients with PMV, the daily calorie intake was stratified by weaning status (success or failure). The first 7-day average daily calorie intake was stratified by the enteral nutrition (EN) and parenteral nutrition (PN) routes for patients with weaning success or failure (Table 2). A higher average daily total calorie intake and EN intake were associated with weaning success. In contrast, higher daily PN intakes on days 3, 4, 5, 6, and 7 and the average daily PN intake were associated with weaning failure (Table 2).
3.4. Analysis of Factors Associated with Successful Weaning
In the univariate analysis, age, the CCI, the mNUTRIC score, albumin, hemoglobin, shock status, fluid status, and the initial 7-day average total calorie intake/BW ≥25 kcal/kg/day were significantly correlated with successful weaning (Table 3). In multivariate regression analysis, higher albumin and hemoglobin levels, the absence of shock, less positive initial 7-day fluid status, and a higher initial 7-day average total calorie/BW≥25 kcal/kg/day intake showed independent significant correlations with weaning success (Table 3). Norepinephrine-alone and norepinephrine + other vasopressor use in shock patients were predictors of weaning failure.
3.5. Stratified Analysis of the Association of the Initial 7-day Average Daily Total Calorie Intake/BW ≥25 kcal/kg/day with Successful Weaning
To analyze the effect of stratification of variables on the association of the initial 7-day average daily total calorie intake/BW ≥25 kcal/kg/day with successful weaning, we undertook a stratified analysis for the following variables: age, sex, body mass index, CCI, APACHE II score, mNUTRIC risk, and shock status. Figure 2 shows that age ≥65 years, female sex, BMI ≥18 kg/m2, CCI <3, APACHE II score <26, high mNUTRIC risk, and absence of shock conferred a benefit with regard to the initial 7-day average daily total calorie intake/BW ≥25 kcal/kg/day for weaning success.
4. Discussion
In this retrospective study, we identified the clinical factors of patients with PMV who achieved successful weaning. High albumin and hemoglobin levels, the absence of shock, less positive initial 7-day fluid status, and an initial 7-day average total calorie intake/BW≥25 kcal/kg/day independently and significantly correlated with weaning success (Table 3).
Several previous studies [23,24,25,26] have shown that the serum albumin level is an independent predictor of successful weaning in patients who require PMV, and this was seen in our study’s results. Chao et al. and Mirtallo et al. [23,24] found that patients with albumin concentrations >3.2 g/dL had a 12-fold higher likelihood of successful weaning and that improved nutrition was significantly linked to survival. Wu et al. [25] reported that the serum albumin level was a significant positive predictor of weaning success in patients with PMV who were treated at a hospital-based respiratory care center in Taiwan. Sapijaszko et al. noted that an increased serum albumin level at RCC admission was associated with a 1.3-fold increased probability of weaning success [27]. In a retrospective study conducted by Huang et al. [28], the Δalbumin (difference between the 4th week and baseline serum albumin during RCC stay) level independently and significantly correlated with successful weaning after multivariate regression analysis, but did not correlate with survival.
Previous studies [29,30,31] have shown that an increase in the hemoglobin level is positively associated with weaning success, and this was identified in our study as well (Table 3), wherein the successful weaning group had a hemoglobin level >10 g/dL.
In routine clinical practice, patients in the RCC occasionally developed unstable vital signs because of various causes, such as septic shock. In our study, 11.1% of patients experienced hemodynamic instability, which reflects the real-world clinical status. Vasopressor use, including norepinephrine-alone or norepinephrine with other vasopressors, in shock patients were negative predictors of weaning success. In contrast, in two of the previous nutritional studies [26,28], patients with PMV with vasopressor or inotropic agent use were excluded. Dettmer et al. [4] reported that vasopressor requirement is a poor prognostic factor for long-term mortality in patients with PMV.
Several previous studies [32,33,34,35] have shown that a positive fluid balance in the initial 3-day ICU stay prior to weaning is associated with worse outcomes after extubation [32] and high hospital mortality [relative risk 2.15 (95% CI, 1.51–3.07)] [35]. Positive fluid balance at 24, 48, and 72 h, as well as the cumulative balance from hospitalization prior to weaning, were significantly higher in the weaning-failure group compared to the weaning-success group. Additionally, a negative cumulative fluid balance at 24 h prior to spontaneous breathing trials (OR=2.9) and a negative cumulative fluid balance from admission (OR=3.4) were independently associated with successful weaning on the first day [32]. In our study, a less positive initial 7-day fluid status independently and significantly correlated with weaning success. Besides, Wang et al. [36] reported that the cumulative fluid balance on days 1–3 and 4–7 with a per 1-L increment (HR: 1.047 and 1.094; 95% CI 1.037–1.058 and 1.080–1.108, respectively) were independently associated with high long-term mortality in critically ill patients.
Enteral feeding intolerance occurs frequently (incidence: 30.5%) in critically ill patients receiving mechanical ventilation in ICUs and is associated with malnutrition, reduced ventilator-free days, extended hospital stay, and increased mortality [37]. In our study, the weaning-success group had a higher average daily calorie and calories/BW than the weaning-failure group (weaning-success group:1192.85 ± 309.33 kcal and 21.33 ± 6.92 kcal/kg, weaning-failure group: 1054.76 ± 338.10 kcal and 19.17 ± 7.77 kcal/kg, respectively; p<0.001; Table 1) and the average initial 7-day total calorie intake/BW ≥25 kcal/kg/day was associated with weaning success in patients with PMV (Table 3). Chiang et al. [38] reported that the average daily calorie and calories/BW intake in the weaning-success group were significantly higher than that in the weaning-failure group (1722.1 ± 240.6 kcal and 31.0 ± 8.2 kcal/kg vs 1597.4 ± 167.9 kcal and 30.2 ± 8.3 kcal/kg, respectively, p<0.05), which our results support. In contrast, Lo et al. [26] found no significant differences in calorie intake between the weaning-success and -failure groups (27.8 ± 9.1 vs 25.6 ± 7.5 kcal/kg/day, p=0.199) but demonstrated that patients with PMV who received a higher calorie and protein intake during ventilator weaning had favorable weaning success, better survival, and lower mortality, and thereby suggested nutritional intervention for 25–30 kcal/kg/day and >1.2 g/kg/day protein intakes for better outcomes in patients with PMV. In another retrospective study conducted by Huang et al. [28], the daily calorie intake was significantly higher in the successfully weaned patients than in the weaning-failure patients (28.04 ± 6.18 vs 19.9 ± 5.83 kcal/kg/day, p<0.0001) and a daily calorie intake ≥24.48 kcal/kg/day positively and significantly correlated with successful weaning in the univariate, but not in the multivariate, analysis. Nonetheless, the trend shows that sufficient calorie intake may contribute to successful weaning. Similarly, our findings in both univariate and multivariate analyses show that the average initial 7-day total calorie intake/BW ≥25 kcal/kg/day was associated with weaning success. More patients with higher APACHE II score (average: 18.05) and hemodynamic instability required vasopressors (11.1%) in our study than those with lower APACHE II score (average: 16.76) and without hemodynamic instability required vasopressors in Huang’s study [28], and this could have contributed to the different results between the two studies.
The 2019 ESPEN guidelines [12] recommended that hypocaloric nutrition (not exceeding 70% of energy expenditure) should be administered in the early phase of acute illness and that, after Day 3, calorie delivery can be increased up to 80–100%. The 2022 ASPEN updated guidelines [39] showed no significant difference in clinical outcomes, including ICU or hospital mortality, length of stay, mean ventilator days and risk of any infection, between ICU patients with higher and lower levels of energy intake, and thereby recommended 12–25 kcal/kg as the nutrition goal in the first 7–10 days of ICU stay. However, the calorie intake of patients with subacute critical illness and PMV was not defined in either the ASPEN [39] or ESPEN [12] guidelines. Adequate calorie intake play a significant role in successful weaning, and achievement of a higher calorie intake with protein consumption is crucial for patients with PMV during the post-ICU phase [40]. In our study, higher average daily total calories and EN intakes were significantly associated with weaning success (Table 2) and the initial 7-day average total calorie intake/BW≥25 kcal/kg/day was independently and significantly correlated with weaning success in multivariate analysis (Table 3). Furthermore, we found a higher mNUTRIC score in the weaning-failure group as compared to the weaning-success group (weaning-failure group: 4.74±1.87 vs weaning success group: 3.82±1.80, respectively; p<0.001; Table 1) and patients with high nutrition risk could benefit from average total calories/BW≥25 kcal/kg/day intake in successful weaning (odds ratio [95% CI] 1.76 [1.02–3.01]; Figure 2). Patients with high nutritional risk are often malnourished, and this is associated with reduced ventilator-free days and increased mortality [37]. The 2016 ASPEN guidelines [14] suggested that patients who were at high nutritional risk and accepted >80% of their estimated or calculated target energy and protein within 48–72 h ICU stay showed significantly reduced mortality risk. Doley et al. [41] suggested that a chronically and severely ill patient on prolonged mechanical ventilator use should be given at least 20–30 kcal/kg/day calorie intake. Calorie deficiency leads to decreased respiratory epithelial regeneration and loss of lean muscle mass, with consequent respiratory muscle weakness and prolonged mechanical ventilation [11]. Among critically ill patients in the acute phase of ICU stay, muscle wasting occurs early and rapidly. Diaphragmatic dysfunction occurs in a significant number of critically ill patients and is linked to higher rates of morbidity and mortality [42]. In these individuals, diaphragmatic weakness could arise from disuse caused by inactivity related to mechanical ventilation, as well as the impact of systemic inflammation, such as that in sepsis. The diaphragmatic dysfunction acquired during critical illness hampers the respiratory system’s ability to manage increased respiratory demands due to lung injury and fluid overload, and this results in prolonged respiratory failure and potentially death [42] . In the subacute phase of ICU care, it is important to provide higher calorie targets, ideally alongside pulmonary rehabilitation, to prevent additional loss of muscle mass and function. A large prospective randomized controlled trial will be needed to determine the ventilator weaning impact of average total calorie intake/BW≥25 kcal/kg/day in patients with high nutrition risk.
As this was a retrospective observational study, there were some limitations. First, we had no protein intake data for the RCC patients. Second, our study evaluated nutritional intake based on actual body weight instead of indirect calorimetry [12], which might provide a more accurate reflection of the patients’ nutritional needs.
5. Conclusions
Higher daily calorie intake in the RCC predicted successful ventilator weaning, with an average intake exceeding 25 kcal/kg/day recommended for optimizing the weaning process. Patients with high nutritional risk could benefit from an average intake ≥25 kcal/kg/day for successful weaning from ventilator.
Author Contributions
Conceptualization: J.L.W. and C.Y.W.; Data curation: C.J.C.and W.C.Y.; Formal analysis: S.H.J.; Investigation: C.J.C.; Methodology: C.Y.W.; Project administration: J.L.W.; Supervision: C.Y.W.; Writing—original draft: C.C.H.; Writing—review and editing: C.Y.W. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by grants from the TCVGH-1134101E.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki and the relevant guidelines and regulations for clinical research and was approved by the Institutional Review Board of Taichung Veterans General Hospital (IRB No. CE23044C).
Informed Consent Statement
Patient consent was waived because of the retrospective nature of the study, and as the patients’ personal information was deidentified prior to analysis.
Data Availability Statement
All the generated data from the present study is presented in this published article. The data used for this study are not available publicly due to data protection policy.
Acknowledgments
This study was based in part on data from the Taichung Veterans General Hospital Research Database, which is managed by the Clinical Informatics Research and Development Center of Taichung Veterans General Hospital .
Conflicts of Interest
The authors declare no competing financial interest and also declare no conflict of interest.
References
- Cox, C.E.; Carson, S.S.; Govert, J.A.; Chelluri, L.; Sanders, G.D. An economic evaluation of prolonged mechanical ventilation. Crit Care Med 2007, 35, 1918–1927. [Google Scholar] [CrossRef]
- Cox, C.E.; Carson, S.S.; Lindquist, J.H.; Olsen, M.K.; Govert, J.A.; Chelluri, L. Differences in one-year health outcomes and resource utilization by definition of prolonged mechanical ventilation: a prospective cohort study. Crit Care 2007, 11, R9. [Google Scholar] [CrossRef]
- Damuth, E.; Mitchell, J.A.; Bartock, J.L.; Roberts, B.W.; Trzeciak, S. Long-term survival of critically ill patients treated with prolonged mechanical ventilation: a systematic review and meta-analysis. Lancet Respir Med 2015, 3, 544–553. [Google Scholar] [CrossRef]
- Dettmer, M.R.; Damuth, E.; Zarbiv, S.; Mitchell, J.A.; Bartock, J.L.; Trzeciak, S. Prognostic Factors for Long-Term Mortality in Critically Ill Patients Treated With Prolonged Mechanical Ventilation: A Systematic Review. Crit Care Med 2017, 45, 69–74. [Google Scholar] [CrossRef]
- Ghiani, A.; Paderewska, J.; Sainis, A.; Crispin, A.; Walcher, S.; Neurohr, C. Variables predicting weaning outcome in prolonged mechanically ventilated tracheotomized patients: a retrospective study. J Intensive Care 2020, 8, 19. [Google Scholar] [CrossRef]
- Leonov, Y.; Kisil, I.; Perlov, A.; Stoichev, V.; Ginzburg, Y.; Nazarenko, A.; Gimelfarb, Y. Predictors of successful weaning in patients requiring extremely prolonged mechanical ventilation. Adv Respir Med 2020, 88, 477–484. [Google Scholar] [CrossRef]
- Arora, N.S.; Rochester, D.F. Respiratory muscle strength and maximal voluntary ventilation in undernourished patients. Am Rev Respir Dis 1982, 126, 5–8. [Google Scholar] [CrossRef]
- McWhirter, J.P.; Pennington, C.R. Incidence and recognition of malnutrition in hospital. Bmj 1994, 308, 945–948. [Google Scholar] [CrossRef]
- Huang, Y.C.; Yen, C.E.; Cheng, C.H.; Jih, K.S.; Kan, M.N. Nutritional status of mechanically ventilated critically ill patients: comparison of different types of nutritional support. Clin Nutr 2000, 19, 101–107. [Google Scholar] [CrossRef]
- Kan, M.N.; Chang, H.H.; Sheu, W.F.; Cheng, C.H.; Lee, B.J.; Huang, Y.C. Estimation of energy requirements for mechanically ventilated, critically ill patients using nutritional status. Crit Care 2003, 7, R108–R115. [Google Scholar] [CrossRef]
- Barr, J.; Hecht, M.; Flavin, K.E.; Khorana, A.; Gould, M.K. Outcomes in critically ill patients before and after the implementation of an evidence-based nutritional management protocol. Chest 2004, 125, 1446–1457. [Google Scholar] [CrossRef]
- Singer, P.; Blaser, A.R.; Berger, M.M.; Alhazzani, W.; Calder, P.C.; Casaer, M.P.; Hiesmayr, M.; Mayer, K.; Montejo, J.C.; Pichard, C.; et al. ESPEN guideline on clinical nutrition in the intensive care unit. Clin Nutr 2019, 38, 48–79. [Google Scholar] [CrossRef]
- Weijs, P.J.; Looijaard, W.G.; Beishuizen, A.; Girbes, A.R.; Oudemans-van Straaten, H.M. Early high protein intake is associated with low mortality and energy overfeeding with high mortality in non-septic mechanically ventilated critically ill patients. Crit Care 2014, 18, 701. [Google Scholar] [CrossRef]
- McClave, S.A.; Taylor, B.E.; Martindale, R.G.; Warren, M.M.; Johnson, D.R.; Braunschweig, C.; McCarthy, M.S.; Davanos, E.; Rice, T.W.; Cresci, G.A.; et al. Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Adult Critically Ill Patient: Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.). JPEN J Parenter Enteral Nutr 2016, 40, 159–211. [Google Scholar] [CrossRef]
- Azoulay, E.; Vincent, J.L.; Angus, D.C.; Arabi, Y.M.; Brochard, L.; Brett, S.J.; Citerio, G.; Cook, D.J.; Curtis, J.R.; Dos Santos, C.C.; et al. Recovery after critical illness: putting the puzzle together-a consensus of 29. Crit Care 2017, 21, 296. [Google Scholar] [CrossRef]
- Herridge, M.S.; Chu, L.M.; Matte, A.; Tomlinson, G.; Chan, L.; Thomas, C.; Friedrich, J.O.; Mehta, S.; Lamontagne, F.; Levasseur, M.; et al. The RECOVER Program: Disability Risk Groups and 1-Year Outcome after 7 or More Days of Mechanical Ventilation. Am J Respir Crit Care Med 2016, 194, 831–844. [Google Scholar] [CrossRef]
- Reignier, J.; Boisrame-Helms, J.; Brisard, L.; Lascarrou, J.B.; Ait Hssain, A.; Anguel, N.; Argaud, L.; Asehnoune, K.; Asfar, P.; Bellec, F.; et al. Enteral versus parenteral early nutrition in ventilated adults with shock: a randomised, controlled, multicentre, open-label, parallel-group study (NUTRIREA-2). Lancet 2018, 391, 133–143. [Google Scholar] [CrossRef]
- Koekkoek, W.; van Setten, C.H.C.; Olthof, L.E.; Kars, J.; van Zanten, A.R.H. Timing of PROTein INtake and clinical outcomes of adult critically ill patients on prolonged mechanical VENTilation: The PROTINVENT retrospective study. Clin Nutr 2019, 38, 883–890. [Google Scholar] [CrossRef]
- Rahman, A.; Hasan, R.M.; Agarwala, R.; Martin, C.; Day, A.G.; Heyland, D.K. Identifying critically-ill patients who will benefit most from nutritional therapy: Further validation of the “modified NUTRIC” nutritional risk assessment tool. Clin Nutr 2016, 35, 158–162. [Google Scholar] [CrossRef]
- Knaus, W.A.; Draper, E.A.; Wagner, D.P.; Zimmerman, J.E. APACHE II: a severity of disease classification system. Crit Care Med 1985, 13, 818–829. [Google Scholar] [CrossRef]
- Vincent, J.L.; Moreno, R.; Takala, J.; Willatts, S.; De Mendonça, A.; Bruining, H.; Reinhart, C.K.; Suter, P.M.; Thijs, L.G. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med 1996, 22, 707–710. [Google Scholar] [CrossRef]
- Boles, J.M.; Bion, J.; Connors, A.; Herridge, M.; Marsh, B.; Melot, C.; Pearl, R.; Silverman, H.; Stanchina, M.; Vieillard-Baron, A.; et al. Weaning from mechanical ventilation. Eur Respir J 2007, 29, 1033–1056. [Google Scholar] [CrossRef]
- Mirtallo, J.M. Assessing the nutritional needs of the critically ill patient. DICP 1990, 24, S20–S23. [Google Scholar]
- Chao, D.C.; Scheinhorn, D.J.; Stearn-Hassenpflug, M. Impact of renal dysfunction on weaning from prolonged mechanical ventilation. Crit Care 1997, 1, 101–104. [Google Scholar] [CrossRef]
- Wu, Y.K.; Kao, K.C.; Hsu, K.H.; Hsieh, M.J.; Tsai, Y.H. Predictors of successful weaning from prolonged mechanical ventilation in Taiwan. Respir Med 2009, 103, 1189–1195. [Google Scholar] [CrossRef]
- Lo, S.C.; Ma, K.S.; Li, Y.R.; Li, Z.Y.; Lin, C.H.; Lin, H.C.; Yang, S.F. Nutritional support for successful weaning in patients undergoing prolonged mechanical ventilation. Sci Rep 2022, 12, 12044. [Google Scholar] [CrossRef]
- Sapijaszko, M.J.; Brant, R.; Sandham, D.; Berthiaume, Y. Nonrespiratory predictor of mechanical ventilation dependency in intensive care unit patients. Crit Care Med 1996, 24, 601–607. [Google Scholar] [CrossRef]
- Huang, S.W.; Lin, H.C.; Chou, Y.F.; Lin, T.Y.; Lo, C.Y.; Huang, H.Y.; Fang, Y.F.; Hsieh, M.H.; Lin, S.M.; Lo, Y.L.; et al. The Impact of Higher Protein Intake in Patients with Prolonged Mechanical Ventilation. Nutrients 2022, 14. [Google Scholar] [CrossRef]
- El Hadidy, S.; Saad, M.; El Hossany, R.; El Gohary, T.; El Ghobashy, M. Coinciding Changes in B Lines Patterns, Haemoglobin and Hematocrit Values Can Predict Outcomes of Weaning from Mechanical Ventilation. Open Access Maced J Med Sci 2019, 7, 4010–4014. [Google Scholar] [CrossRef]
- Chen-Roetling, J.; Ma, S.K.; Cao, Y.; Shah, A.; Regan, R.F. Hemopexin increases the neurotoxicity of hemoglobin when haptoglobin is absent. J Neurochem 2018, 145, 464–473. [Google Scholar] [CrossRef]
- Lai, Y.C.; Ruan, S.Y.; Huang, C.T.; Kuo, P.H.; Yu, C.J. Hemoglobin levels and weaning outcome of mechanical ventilation in difficult-to-wean patients: a retrospective cohort study. PLoS One 2013, 8, e73743. [Google Scholar] [CrossRef]
- Upadya, A.; Tilluckdharry, L.; Muralidharan, V.; Amoateng-Adjepong, Y.; Manthous, C.A. Fluid balance and weaning outcomes. Intensive Care Med 2005, 31, 1643–1647. [Google Scholar] [CrossRef]
- Frutos-Vivar, F.; Ferguson, N.D.; Esteban, A.; Epstein, S.K.; Arabi, Y.; Apezteguia, C.; Gonzalez, M.; Hill, N.S.; Nava, S.; D’Empaire, G.; et al. Risk factors for extubation failure in patients following a successful spontaneous breathing trial. Chest 2006, 130, 1664–1671. [Google Scholar] [CrossRef]
- Maezawa, S.; Kudo, D.; Miyagawa, N.; Yamanouchi, S.; Kushimoto, S. Association of Body Weight Change and Fluid Balance With Extubation Failure in Intensive Care Unit Patients: A Single-Center Observational Study. J Intensive Care Med 2021, 36, 175–181. [Google Scholar] [CrossRef]
- Messmer, A.S.; Zingg, C.; Muller, M.; Gerber, J.L.; Schefold, J.C.; Pfortmueller, C.A. Fluid Overload and Mortality in Adult Critical Care Patients-A Systematic Review and Meta-Analysis of Observational Studies. Crit Care Med 2020, 48, 1862–1870. [Google Scholar] [CrossRef]
- Wang, T.J.; Pai, K.C.; Huang, C.T.; Wong, L.T.; Wang, M.S.; Lai, C.M.; Chen, C.H.; Wu, C.L.; Chao, W.C. A Positive Fluid Balance in the First Week Was Associated With Increased Long-Term Mortality in Critically Ill Patients: A Retrospective Cohort Study. Front Med (Lausanne) 2022, 9, 727103. [Google Scholar] [CrossRef]
- Gungabissoon, U.; Hacquoil, K.; Bains, C.; Irizarry, M.; Dukes, G.; Williamson, R.; Deane, A.M.; Heyland, D.K. Prevalence, risk factors, clinical consequences, and treatment of enteral feed intolerance during critical illness. JPEN J Parenter Enteral Nutr 2015, 39, 441–448. [Google Scholar] [CrossRef]
- Chiang, C.Y.; Lan, C.C.; Yang, C.H.; Hou, Y.C. Investigating the differences in nutritional status between successfully weaned and unsuccessfully weaned respirator patients. Sci Rep 2023, 13, 7144. [Google Scholar] [CrossRef]
- Compher, C.; Bingham, A.L.; McCall, M.; Patel, J.; Rice, T.W.; Braunschweig, C.; McKeever, L. Guidelines for the provision of nutrition support therapy in the adult critically ill patient: The American Society for Parenteral and Enteral Nutrition. JPEN J Parenter Enteral Nutr 2022, 46, 12–41. [Google Scholar] [CrossRef]
- van Zanten, A.R.H.; De Waele, E.; Wischmeyer, P.E. Nutrition therapy and critical illness: practical guidance for the ICU, post-ICU, and long-term convalescence phases. Crit Care 2019, 23, 368. [Google Scholar] [CrossRef]
- Doley, J.; Mallampalli, A.; Sandberg, M. Nutrition management for the patient requiring prolonged mechanical ventilation. Nutr Clin Pract 2011, 26, 232–241. [Google Scholar] [CrossRef]
- Supinski, G.S.; Morris, P.E.; Dhar, S.; Callahan, L.A. Diaphragm Dysfunction in Critical Illness. Chest 2018, 153, 1040–1051. [Google Scholar] [CrossRef]
Figure 1.
Flowchart depicting participant enrolment and allocation in the study. RCC: respiratory care center.
Figure 1.
Flowchart depicting participant enrolment and allocation in the study. RCC: respiratory care center.
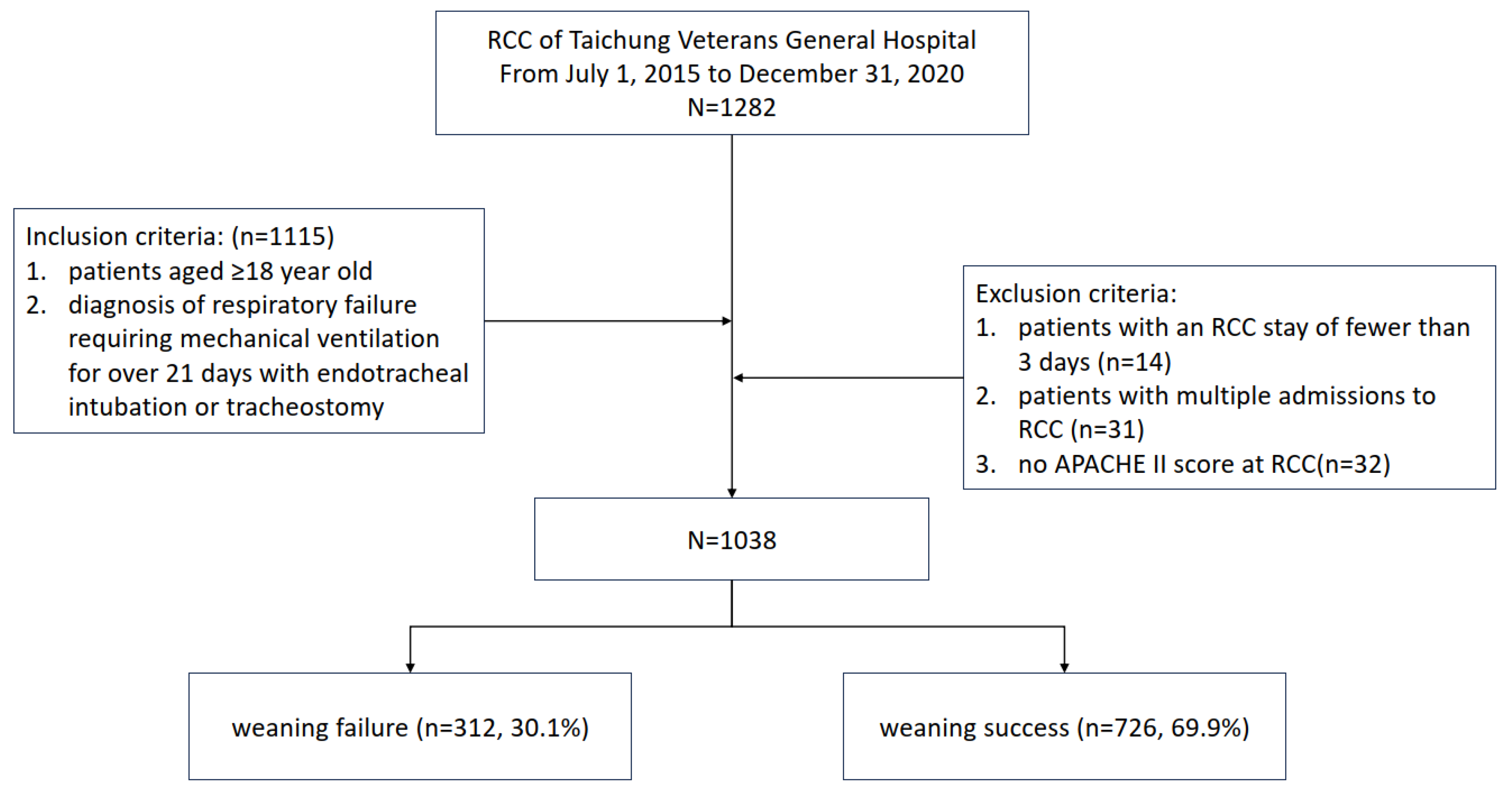
Figure 2.
Logistic regression analysis of the effect-stratified modification of variables related to the association of total calories/BW ≥25 kcal/kg/day (days 1–7, average) with successful weaning. APACHE: Acute Physiology and Chronic Health Evaluation; CI: confidence interval; NUTRIC: Nutrition Risk in Critically ill; OR: odds ratio. Logistic regression. *p<0.05, **p<0.01.
Figure 2.
Logistic regression analysis of the effect-stratified modification of variables related to the association of total calories/BW ≥25 kcal/kg/day (days 1–7, average) with successful weaning. APACHE: Acute Physiology and Chronic Health Evaluation; CI: confidence interval; NUTRIC: Nutrition Risk in Critically ill; OR: odds ratio. Logistic regression. *p<0.05, **p<0.01.
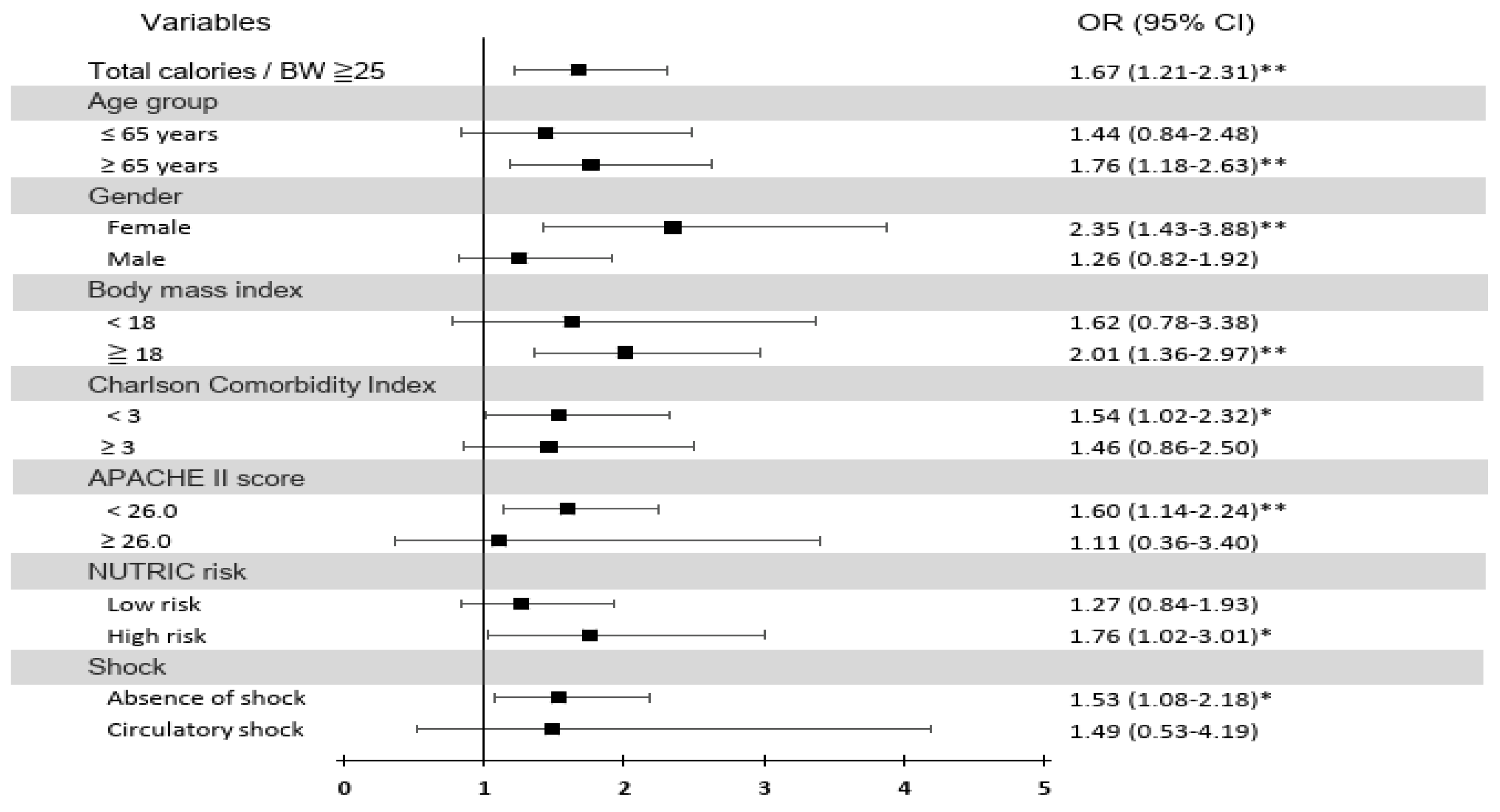

Table 1.
Patient characteristics stratified by successfully weaning.
| All (n=1038) | successful weaning for 48 hrs | p-value | ||
|---|---|---|---|---|
| Weaning failure (n=312) | Weaning success (n=726) | |||
| Mean±SD | Mean±SD | Mean±SD | ||
| Basic characteristics | ||||
| Age, years | 68.51±16.01 | 71.04±15.06 | 67.42±16.30 | 0.001** |
| Sex-Male, n (%) | 595 (57.32%) | 187 (59.94%) | 408 (56.20%) | 0.264 |
| Charlson Comorbidity Index | 2.30±1.56 | 2.71±1.59 | 2.12±1.51 | <0.001** |
| Nutrition relevant variables | ||||
| Body mass index | 22.59±4.44 | 22.55±4.50 | 22.61±4.42 | 0.951 |
| mNUTRIC score(ICU) | 4.10±1.87 | 4.74±1.87 | 3.82±1.80 | <0.001** |
| Albumin (g/dL) | 3.03±0.47 | 2.89±0.46 | 3.09±0.46 | <0.001** |
| Hemoglobin (g/dL) | 9.86±1.45 | 9.37±1.41 | 10.07±1.42 | <0.001** |
| Disease severityand managements | ||||
| APACHE II score (in the RCC) | 18.05±5.51 | 19.85±5.86 | 17.27±5.16 | <0.001** |
| SOFA score on Day 1 | 4.85±2.54 | 5.37±2.84 | 4.63±2.37 | <0.001** |
| Presence of shock, n (%) | ||||
| Absence of shock, n (%) | 923 (88.92%) | 231 (74.04%) | 692 (95.32%) | |
| Norepinephrine-alone, n (%) | 82 (7.90%) | 55 (17.63%) | 27 (3.72%) | |
| Norepinephrine and other vasopressors, n (%) | 33 (3.18%) | 26 (8.33%) | 7 (0.96%) | |
| Renal replacement therapy (RRT), n (%) | 52 (5.01%) | 22 (7.05%) | 30 (4.13%) | 0.048* |
| Fluid balance, day 1-7 | 1167.79±2995.60 | 1768.93±3344.02 | 909.45±2795.74 | <0.001** |
| Calorie intake, days 1–7 (kcal/day) | 1151.35±324.33 | 1054.76±338.10 | 1192.85±309.33 | <0.001** |
| Total calories/BW, days 1–7 (kcal/kg/day) | 20.68±7.25 | 19.17±7.77 | 21.33±6.92 | <0.001** |
| Outcomes | ||||
| Duration of hospital stay, days | 57.87±47.21 | 61.61±68.16 | 56.27±34.44 | 0.096 |
| Ventilator-use duration, days | 41.16±21.15 | 52.78±25.80 | 36.17±16.47 | <0.001** |
Results of the Mann–Whitney U test and the chi-square test. *p<0.05, **p<0.01. Data are presented as the mean ± standard deviation; APACHE II: Acute Physiology and Chronic Health Evaluation II; BW: body weight; ICU: intensive care unit; mNUTRIC: modified Nutrition Risk in the Critically Ill; SOFA: Sequential Organ Failure Assessment; RCC: respiratory care center..*p<0.05, **p<0.001.
Table 2.
Daily calorie intake in patients on PMV in subgroups stratified by successful weaning.
| All (n=1038) | RCC successful weaning for 48 h | p-value | |||||
|---|---|---|---|---|---|---|---|
| Weaning failure (n=312) | Weaning success (n=726) | ||||||
| Mean±SD | Mean±SD | Mean±SD | |||||
| Total calories (kcal/day) | |||||||
| Day 1 | 1178.95±361.14 | 1117.01±369.86 | 1205.57±354.26 | <0.001** | |||
| Day 2 | 1174.71±362.98 | 1100.20±374.50 | 1206.73±353.38 | <0.001** | |||
| Day 3 | 1172.30±356.20 | 1084.94±371.50 | 1209.85±342.89 | <0.001** | |||
| Day 4 | 1156.08±374.54 | 1055.76±395.00 | 1199.20±357.11 | <0.001** | |||
| Day 5 | 1142.30±390.71 | 1036.26±425.54 | 1187.87±365.72 | <0.001** | |||
| Day 6 | 1135.44±414.54 | 994.85±454.96 | 1195.86±380.59 | <0.001** | |||
| Day 7 | 1099.64±440.15 | 994.33±473.09 | 1144.90±417.45 | <0.001** | |||
| Days 1–7 | 1151.35±324.33 | 1054.76±338.10 | 1192.85±309.33 | <0.001** | |||
| Enteral Nutrition | |||||||
| Day 1 | 1137.95±387.02 | 1059.90±406.42 | 1171.50±373.68 | <0.001** | |||
| Day 2 | 1135.42±389.69 | 1043.87±419.09 | 1174.77±369.74 | <0.001** | |||
| Day 3 | 1135.49±382.30 | 1032.00±409.63 | 1179.96±361.22 | <0.001** | |||
| Day 4 | 1119.67±397.82 | 1001.29±425.34 | 1170.54±374.36 | <0.001** | |||
| Day 5 | 1106.70±413.83 | 982.21±454.49 | 1160.20±383.17 | <0.001** | |||
| Day 6 | 1097.95±433.70 | 936.23±478.97 | 1167.46±393.11 | <0.001** | |||
| Day 7 | 1066.22±455.45 | 941.69±494.17 | 1119.74±427.08 | <0.001** | |||
| Days 1–7 | 1114.20±350.87 | 999.60±378.17 | 1163.45±326.59 | <0.001** | |||
| Parenteral Nutrition | |||||||
| Day 1 | 41.00±116.78 | 57.11±166.05 | 34.07±86.71 | 0.108 | |||
| Day 2 | 39.29±112.43 | 56.33±154.86 | 31.96±87.26 | 0.205 | |||
| Day 3 | 36.82±105.34 | 52.93±137.09 | 29.89±87.46 | 0.004** | |||
| Day 4 | 36.41±114.02 | 54.47±154.27 | 28.65±90.48 | 0.001** | |||
| Day 5 | 35.60±110.16 | 54.05±146.67 | 27.67±89.00 | 0.002** | |||
| Day 6 | 37.49±134.49 | 58.63±175.66 | 28.40±111.17 | 0.001** | |||
| Day 7 | 33.42±117.31 | 52.64±167.44 | 25.16±86.19 | 0.003** | |||
| Days 1–7 | 37.15±95.15 | 55.17±123.72 | 29.40±78.63 | <0.001** | |||
PMV: prolonged mechanical ventilation; RCC: respiratory care center; Mann–Whitney U test and chi-square test. *p<0.05, **p<0.001. PMV: prolonged mechanical ventilation; RCC: respiratory care center.
Table 3.
Factors associated with successful weaning identified on univariate and multivariate analyses.
Table 3.
Factors associated with successful weaning identified on univariate and multivariate analyses.
| Characteristics | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|
| OR (95% CI) | p-value | OR (95% CI) | p-value | |||
| Age, per year increment | 0.99 (0.98–0.99) | 0.001** | 0.99 (0.98–1.01) | 0.341 | ||
| Sex (male) | 0.86 (0.65–1.12) | 0.264 | ||||
| CCI, per 1 score increment | 0.79 (0.72–0.86) | <0.001** | 0.91 (0.82–1.00) | 0.060 | ||
| BMI, per 1 kg/m2 increment | 1.00 (0.97–1.03) | 0.833 | ||||
| NUTRIC score, high risk (≥5) | 0.43 (0.33–0.57) | <0.001** | 0.76 (0.49–1.17) | 0.210 | ||
| Albumin, per 1 g/dL increment | 2.63 (1.94–3.56) | <0.001** | 1.93 (1.35–2.75) | <0.001** | ||
| Hemoglobin, per 1 g/dL increment | 1.44 (1.30–1.60) | <0.001** | 1.20 (1.07–1.36) | 0.003** | ||
| APACHE II score, per 1 score increment | 0.92 (0.90–0.94) | <0.001** | 0.99 (0.95–1.03) | 0.596 | ||
| Absence of shock | 1.00 | |||||
| Norepinephrine-alone | 0.16 (0.10–0.27) | <0.001** | 0.27 (0.16–0.46) | <0.001** | ||
| Norepinephrine and other vasopressors | 0.09 (0.04–0.21) | <0.001** | 0.15 (0.06–0.37) | <0.001** | ||
| RRT during RCC | 0.57 (0.32–1.00) | 0.051 | ||||
| Fluid balance, days 1–7, per liter | 0.91 (0.86–0.95) | <0.001** | 0.87 (0.83–0.92) | <0.001** | ||
| Calories intake, days 1–7, per kcal | 1.21 (1.14–1.29) | <0.001** | ||||
| Total calories/BW ≥25 kcal/kg/day (days 1–7) | 1.67 (1.21–2.31) | 0.002** | 1.50 (1.05–2.15) | 0.026* | ||
APACHE II: Acute Physiology and Chronic Health Evaluation II; BMI: body mass index; CCI: Charlson Comorbidity Index; mNUTRIC: modified Nutrition Risk in the Critically Ill; OR: odds ratio; Logistic regression. *p<0.05, **p<0.01.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



