Submitted:
08 October 2024
Posted:
09 October 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Parental willingness is a prerequisite for childhood immunization. This study evaluated whether parental vaccination readiness and willingness, measured using the modified Japanese 7C Vaccination Readiness Scale, predicted vaccination behavior. In December 2021, 2 months before the approval of COVID-19 vaccination for children aged 5–11 years in Japan, we asked 1,190 parents of children in this age groups about their intention regarding vaccinating their children against COVID-19 using an online modified 7C Vaccination Readiness Scale, consisting of seven components, namely, Confidence, Complacency, Constraints, Calculation, Collective responsibility, Compliance, and Conspiracy. The modified 7C components were analyzed for model fit and association with parental intention using structural equation modeling. The model fit of the modified 7C scale was good (goodness-of-fit index: 0.98), and the factor loadings and model fit for parental readiness were high (standardized factor loadings: 0.84). In January 2024, we asked the same parents about their children's COVID-19 vaccination status (valid responses: 536). The components of the modified 7C scale were compared with actual vaccination behavior. Parents with a low readiness to vaccinate their children against COVID-19 had a high actual non-vaccination rate. The use of the modified 7C scale may assist in the development of childhood vaccination interventions.
Keywords:
parental intention
; children
; vaccine preparation scale
; vaccination
; specificity
; sensitivity
; vaccine hesitancy
; prevention
1. Introduction
Childhood immunization helps protect children from vaccine-preventable diseases [1,2,3]. As parents decide whether to vaccinate their children, childhood immunization rates depend on parental intention, access to resources, and health-related behavior [4,5]. A psychometrically valid measurement scale allows for a better understanding of parental vaccination readiness, potentially facilitating targeted interventions to increase vaccination rates among children [6].
For adults, intention to be vaccinated has been assessed with the 3C [7] or 5C [8] scales, which are psychological measures that reflect readiness to be vaccinated [9,10,11,12,13,14,15,16,17]. The 3C scale includes Confidence (trust in the safety and efficacy of vaccines, health services, and government), Complacency (tendency to ignore vaccines because of low perceived risk of infectious disease), and Constraints (structural or psychological barriers to vaccination in daily life). The 5C scale includes Calculation (engagement in extensive information searching that indicates a deliberate comparison of the risks of infection and vaccination from which to make an informed decision) and Collective responsibility (the tendency to consider the protection of others in the decision to vaccinate) in addition to the factors included in the 3C scale. During the COVID-19 pandemic, a new 7C Vaccination Readiness Scale (7C) was developed [6] by adding Compliance (support for societal monitoring and sanctioning of people who are not vaccinated), and Conspiracy (conspiracy thinking and belief in fake news related to vaccination) to the 5C scale. The 7C Vaccination Readiness Scale has the following two characteristics: (1) The measure assesses an individual's readiness and willingness to be vaccinated rather than vaccine hesitancy; and (2) it assesses seven psychological components relevant to vaccination readiness [6]. The 7C Vaccination Readiness Scale has been shown to reflect the vaccination intentions of adults [18,19,20]. Vaccination readiness, willingness, and coverage vary by time, type of vaccine, and place [21,22,23,24,25,26,27,28]. Therefore, regional studies are necessary. Machida et al. [29] developed a Japanese version of the 7C for adults. However, until the end of 2021, it was not known whether this scale could be adopted to assess parental readiness to vaccinate their children. In 2021, we modified the Japanese version of the 7C Vaccination Readiness Scale, created by Machida et al. [29], to create a parental version and administered it to parents. In 2024, we reinterviewed the same parents to investigate actual vaccination rates and validated the modified 7C scale.
The purpose of this study was to evaluate whether parental vaccination readiness and willingness using the modified Japanese 7C Vaccination Readiness Scale, predicted vaccination behavior.
2. Materials and Methods
2.1. Survey Respondents and Data Collection
For the baseline survey, we conducted an online survey of adults from December 20 to 22, 2021 [30]. At the time of the survey, COVID-19 vaccines had not yet been approved for use in children aged 5–11 years in Japan; the two-dose regimen had been approved for ages 12 years and older, and booster vaccinations for adults in the general population had not yet been introduced [31]. The respondents were 1190 men and women with children under the age of 11 years who were registered with an online survey company (Macromill, Inc., Tokyo, Japan) [30]. The follow-up survey was conducted in January 26 to 29,2024, two years after the start of the COVID-19 vaccination program in children aged 5–11 years.
2.2. Measurement Methods (Baseline Survey)
Sociodemographic factors measured included sex, age, occupation, residential region, marital status (married or unmarried), presence of children under the age of 11 years in the household, household income category (< 4 million yen, ≥ 4 million yen), level of education (high school, vocational school, or university), and concern about adverse events. We also asked respondents how many doses of COVID-19 vaccine they had received, and whether they had experienced any adverse events, including fever, fatigue, headache, chills, vomiting, diarrhea, muscular pain, arthralgia, or anaphylactic shock.
Parental intention to vaccinate their children against COVID-19 was assessed by their response to the following statement: “When a pediatric vaccine for COVID-19 becomes available, I will have my children vaccinated.” A 5-point Likert scale was used with the following choices: strongly disagree, disagree, neither agree nor disagree, agree, and strongly agree.
Because the Japanese version of the 7C Vaccination Readiness Scale is for adults [6,29,32], we modified the scale by adding “child” or “school”, as described by Geiger et al. [6] and Machida et al. [29] (Table 1). The questions for Compliance and Conspiracy were intentionally left as general, rather than as COVID-19-specific statements, as they were in the original.
Although the original version of the 7 C Vaccination Readiness Scale was scored using a 7-point Likert scale, we used a 5-point Likert scale in this study due to the space limitations of the web-based questionnaire. The scores on the 5-point Likert scale were as follows: strongly disagree = 1 point, disagree = 2 points, neither agree nor disagree = 3 points, agree = 4 points, and strongly agree = 5 points. Scores were assigned in ascending order for Confidence, Complacency, Constraints, Collective responsibility, and Compliance, and in descending order for Calculation and Conspiracy, as in the original study [6]. Higher scores indicated greater vaccination readiness [6].
2.3. Follow-Up Survey
Parents were asked how many doses of COVID-19 vaccine their children aged 5 to 11 years had received, and their response was recorded.
2.4. Statistical Analysis
Statistical analysis included 1190 parents of children aged 5 to 11 years. The parental characteristics at baseline were analyzed according to their intention to vaccinate their children against COVID-19. Chi-square, Kruskal–Wallis, and Fisher’s exact tests were used to test the characteristics associated with parental intention to vaccinate their children.
To assess the structural validity of the modified scale, a confirmatory factor analysis was conducted according to the method described by Geiger et al. [6]. The model fit was considered acceptable if the goodness-of-fit index (GFI) was ≥ 0.90, Bentler-Bonett Normed Fit Index (NFI) ≥ 0.90, root mean square error of approximation (RMSEA) < 0.08, and standardized root mean squared residual (SRMR) < 0.11 [6,26,29,33].
The modified scale was analyzed for model fit and association with parental intention to vaccinate the children using structural equation modeling. Spearman correlation coefficients (ρ) were calculated for the correlation between parental intention to vaccinate their children and the modified scale. We calculated the percentage of children who had received the COVID-19 vaccine, by each component of the 7C scale. The data were analyzed using SAS version 9.4 (SAS Institute Inc. Cary, NC, USA).
2.5. Ethical Considerations
This study was approved by the Ethics Committee of Saga University (approval number: R2–24; date of approval: November 30, 2020). Respondents were informed that the survey was part of the research and that the results may be published after anonymized processing. Respondents were also informed that the analysis would not affect confidentiality. Respondents answered the survey questions only if they agreed to participate. Respondents were asked to answer each question to avoid missing responses. The responses were stored in a secure password-protected database.
3. Results
3.1. Parental Attributes and Intention Regarding Vaccinating Their Children Against COVID-19
The most common response to the statement about parents' intentions to vaccinate their children prior to the approval of the COVID-19 vaccine was “neither agree nor disagree” (36.5%), indicating that the respondents were undecided, followed by “agree” (34.3%). Parents who indicated the intention to vaccinate their children tended to be older, were less likely to report “concern about adverse events,” and were more likely to have received more than two doses of COVID-19 vaccine (Table 2).
3.2. Measurement Model and Criterion Validity for Parental Readiness to Vaccinate Their Children Against COVID-19
The modified scale g-factor model fit the data well for parental intention to vaccinate their children against COVID-19 (χ2[14]: 83.9, p < 0.001; GFI: 0.980, Bentler-Bonett NFI: 0.948, RMSEA: 0.067, SRMR: 0.040). In the confirmatory factor analysis, the factor saturation (ω) was 0.970, the Akaike information criterion (AIC) was 112 (Figure 1), and Cronbach’s alpha was 0.63.
3.3. Predictors of Parental Intention to Vaccinate Their Children Against COVID-19
3.4. Relationship between Components of the Modified Scale and Parental Intention to Vaccinate Their Children against COVID-19
The bivariate correlation between the components of the modified scale and parental intention is shown in Table 3. Calculation, Compliance, and Conspiracy were found to be less related to the intention to vaccinate than the other four components. In addition, the correlation coefficient for Calculation showed a negative value. Complacency and Constraints were highly correlated with parental intention to vaccinate their children (Table 3).
3.5. Predicted and Observed Vaccination Behavior
In January 2024, approximately 2 years after the initial survey had been conducted, a follow-up survey was conducted of the same parents who participated in the baseline survey, asking about their children's COVID-19 vaccination status (valid responses: 536, follow-up rate = 47.7%). The proportion of children who had not been vaccinated was high (over 80%) among parents who were negative about vaccination (strongly disagreed or disagreed for the five ascending scored components, or strongly agreed or agreed for the two reverse scored components). In contrast, the children’s vaccination rate among parents who were positive about vaccination was 30–58.6%.

Table 4.
Relationship between the modified Japanese version of the 7C Vaccination Readiness Scale (parental component) and child vaccination status.
Table 4.
Relationship between the modified Japanese version of the 7C Vaccination Readiness Scale (parental component) and child vaccination status.
| Vaccinated against COVID-19 | ||
|---|---|---|
| No N = 406 |
Yes N = 130 |
|
| 7C score before vaccine approval, n (%) | ||
| Strongly disagree | 30 (85.7) | 5 (14.3) |
| Disagree | 62 (89.9) | 7 (10.1) |
| Neither agree nor disagree | 184 (78.6) | 50 (21.4) |
| Agree | 114 (66.3) | 58 (33.7) |
| Strongly agree | 16 (61.5) | 10 (38.5) |
| Complacency, n (%) | ||
| Strongly disagree | 20 (80.0) | 5 (20.0) |
| Disagree | 47 (88.7) | 6 (11.3) |
| Neither agree nor disagree | 196 (83.4) | 39 (16.6) |
| Agree | 123 (66.8) | 61 (33.2) |
| Strongly agree | 20 (51.3) | 19 (48.7) |
| Constraints, n (%) | ||
| Strongly disagree | 27 (90.0) | 3 (10.0) |
| Disagree | 71 (91.0) | 7 (9.0) |
| Neither agree nor disagree | 182 (77.4) | 53 (22.6) |
| Agree | 114 (69.5) | 50 (30.5) |
| Strongly agree | 12 (41.4) | 17 (58.6) |
| Calculation, n (%) | 11 (73.3) | |
| Strongly disagree | 4 (26.7) | |
| Disagree | 38 (70.4) | 16 (29.6) |
| Neither agree nor disagree | 159 (79.5) | 41 (20.5) |
| Agree | 151 (72.2) | 58 (27.8) |
| Strongly agree | 47 (81.0) | 11 (19.0) |
| Collective responsibility, n (%) | ||
| Strongly disagree | 18 (85.7) | 3 (14.3) |
| Disagree | 17 (77.3) | 5 (22.7) |
| Neither agree nor disagree | 131 (85.1) | 23 (14.9) |
| Agree | 192 (71.6) | 76 (28.4) |
| Strongly agree | 48 (67.6) | 23 (32.4) |
| Compliance, n (%) | ||
| Strongly disagree | 123 (89.8) | 14 (10.2) |
| Disagree | 113 (76.4) | 35 (23.6) |
| Neither agree nor disagree | 120 (70.2) | 51 (29.8) |
| Agree | 41 (66.1) | 21 (33.9) |
| Strongly agree | 9 (50.0) | 9 (50.0) |
| Conspiracy, n (%) | ||
| Strongly disagree | 14 (70.0) | 6 (30.0) |
| Disagree | 65 (66.3) | 33 (33.7) |
| Neither agree nor disagree | 222 (79.6) | 57 (20.4) |
| Agree | 89 (74.8) | 30 (25.2) |
| Strongly agree | 16 (80.0) | 4 (20.0) |
4. Discussion
Understanding individual differences that determine parental readiness to vaccinate their children may help predict pediatric vaccination rates. We modified the Japanese version of the 7C Vaccination Readiness Scale (for adults), developed by Machida et al. [29], to create an abbreviated version of the Japanese parental vaccination readiness scale to measure parental readiness to vaccinate their children against COVID-19. First, the modified 7C scales were assessed by measuring parental intention to vaccinate their children against COVID-19. The results of the analysis using structural equation modeling showed good model fit between the 7Cs and parents' vaccination intentions. Next, we conducted a follow-up survey and compared the components of the modified 7C scale with actual vaccination behavior. Parents with a low readiness to vaccinate their children had a high rate of non-vaccination with the COVID-19 vaccine. The modified 7C scale had high specificity.
Concurrent with our study, Rees et al. [26] developed a parent version of the 7C scale based on the 7C Vaccination Readiness Scale by Geiger et al. [6]. Rees et al. [26] found that the Parental Vaccination Readiness Scale had good psychometric properties and high criterion validity in German and Danish populations, suggesting that this scale may be used as a tool to reflect parental vaccination intentions regarding their children. Among parents of children younger than 12 years, the same age group as the children that were the focus of this study, Constraints, Collective responsibility, and Confidence were the most important correlates of parental vaccination intention. Our results are similar to those of Rees et al. This study confirmed that Complacency, Constraints, and Collective responsibility were related to vaccination behavior. However, the percentage of children who received the COVID-19 vaccine was 58.6% (strongly agree) for the "Constraints" attitude, 38.5% (strongly agree) for the "Confidence" attitude, and 32.4% (strongly agree) for the "Collective responsibility" attitude, indicating that the sensitivity of the 7C scale is limited. However, considering that the overall vaccination rate for Japanese children aged 5 to 11 years during the same period was 24.5% [34], the modified 7C scale was able to predict vaccination behavior.
Although the Calculation component showed negative factor loadings and a negative correlation coefficient with parents' intention to vaccinate their children, in contrast to the findings of Rees et al. [26]. The actual percentage of children who received the COVID-19 vaccine was less than 30% even when parents indicated readiness to vaccinate their children based on the Calculation component (i.e. strongly disagree or disagree because it was a reverse-scored item). One possible reason why the results for the Calculation indicator differed from the results of Rees et al. may be the national character of the Japanese people. Previous studies of COVID-19 vaccination intention among adults in Japan have also shown a weak association between Calculation and vaccination intention [29,30]. In addition, in previous studies of COVID-19 vaccination intention among adults, social norms were most strongly associated with vaccination intentions [30]. A second reason is the ethical consideration regarding children. Acceptance of vaccination is associated with the perceived risk of infection and awareness of adverse events associated with vaccination [35]. The baseline survey was conducted before the Omicron epidemic, and at the time there were reports that children were less likely to develop COVID-19, and that the symptoms were milder in children [27,36,37]. In addition, there were reports of vaccine adverse events, such as myocarditis in young adults [38]. Moreover, some people believe that the risks and benefits of vaccinating healthy children against COVID-19 are unknown [39]. In such cases, experts and clinicians should discuss the ethical considerations involved in vaccinating children to enable parents to develop an informed opinion regarding the benefits and risks of vaccination of their children [25].
When the parental vaccination readiness score is low, the likelihood of not vaccinating children is high, suggesting that the specificity of the 7C vaccine readiness score is high. These findings suggest that COVID-19 vaccination rates among children are higher if parents are “vaccination-ready” according to the 7C scale. Therefore, our modified 7C Vaccination Readiness Scale has the potential to be used to construct effective vaccine policies by looking at responses to each component.
This study has several strengths. First, a follow-up survey was conducted 2 years after the baseline survey, and the modified 7C scale predictions were compared with the children’s COVID-19 vaccination status. Second, the 7C was used to measure readiness to vaccinate children against COVID-19 before the Japanese government approved the vaccination of children aged 5–11 years. As vaccination readiness, willingness, and coverage have been reported to vary by vaccine type and location [21,22,23,24,25,26,27,28], it is useful to determine vaccination intentions for target vaccines in each country. To our knowledge, this is the first report of a readiness scale being used in Japan to assess parental intention to vaccinate their children against COVID-19 prior to the start of COVID-19 vaccination. Third, the sample size was adequate. Finally, respondents were recruited from all parts of Japan, so these results are likely to be generalizable to the country.
However, this study has some limitations: First, the 7C used in this study was a short version. This limited our ability to examine the effects of the intention to vaccinate and the scale specific components in detail. Therefore, when investigating the effect of an intervention on a specific component, the long version should be used, as described by Rees et al. [26]. Second, the 7C responses were obtained using a 5-point Likert scale, which differs from the 7-point scale used with the original tool [6]. A study, comparing the 5-point Likert scale with the 7-point Likert scale using the WatLX scale, reported higher Cronbach alpha values for the 7-point Likert scale [40]. Finally, because this study was an online survey, was limited to individuals with easy access to online resources. Therefore, selection and sampling biases were unavoidable. This needs to be considered when generalizing the results to the Japanese population.
5. Conclusions
In this study, the modified 7C Vaccination Readiness Scale predicted parental intention to vaccinate their children against COVID-19 with high accuracy, based on structural equation modeling and subsequent vaccination rates. The modified 7C scale may be useful in the development of childhood vaccine interventions.
Author Contributions
Conceptualization, M.H., T.N. and Y.H.; methodology, M.H.; validation, M.H.; formal analysis, M.H.; investigation, M.H., Y.F; T.K, resources, M.H; data curation, M.T and M.H; writing, original draft preparation, M.T., and M.H.; writing, review and editing, M.H., and A.M.; Y.F, T.K, visualization, M.H., and A.M; supervision, M.H.; project administration, M.H.; funding acquisition, M.H. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by a research grant for Research on Emerging and Re-emerging Infectious Diseases, Health and Labour Science Research Grants from the Ministry of Health, Labor and Welfare, Japan, grant number R2-SHINKOGYOSEI-SHITEI-003,20HA2001 and 24HA2007.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of Saga University (approval number: R2–24; date of approval: 30 November 2020).
Informed Consent Statement
Respondents were informed of the survey’s purpose and requirements, were assured of anonymity and data confidentiality, and submission of responses to the survey was considered indicative of informed consent.
Data Availability Statement
The data presented in this study are available on request from the corresponding author (M.T.). The data are not publicly available due to privacy concerns.
Acknowledgments
We would like to thank all those who participated in the survey, Yasuyuki Maeda and Yusuke Takagi for proofreading the manuscript, and Miyuki Fuchigami for providing administrative support.
Conflicts of Interest
Takashi Nakano receives lecture fees from Daiichi Sankyo Co., Ltd., Sanofi Co., Ltd., and Mitsubishi Tanabe Pharma Corporation. The other authors declare no conflict of interest. The funder had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
References
- Lehmann, B.A.; de Melker, H.E.; Timmermans, D.R.M.; Mollema, L. Informed decision making in the context of childhood immunization. Patient Educ Couns 2017, 100, 2339–2345. [CrossRef]
- Duclos, P.; Okwo-Bele, J. M.; Gacic-Dobo, M.; Cherian T. Global immunization: Status, progress, challenges and future. BMC Int Health Hum Rights 2009, 9 Suppl 1, S2. [CrossRef]
- World Bank. World development report 1993. Oxford University Press, New York: 1993.
- Chen, F.; He, Y.; Shi, Y. Parents' and guardians' willingness to vaccinate their children against COVID-19: A systematic review and meta-analysis. Vaccines (Basel) 2022, 10, 179. [CrossRef]
- Yang, W. Transmission dynamics of and insights from the 2018-2019 measles outbreak in New York City: A modeling study. Sci Adv 2020, 6, eaaz4037. [CrossRef]
- Geiger, M.; Rees, F.; Lilleholt, L.; Santana, A.P.; Zettler, I.; Wilhelm, O.; Betsch, C.; Böhm, R. Measuring the 7Cs of vaccination readiness. Eur J Psych Assess 2021, 38, 261–269. [CrossRef]
- MacDonald, N.E. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [CrossRef]
- Betsch, C.; Schmid, P.; Heinemeier, D.; Korn, L.; Holtmann, C.; Böhm, R. Beyond confidence: Development of a measure assessing the 5c psychological antecedents of vaccination. PLoS One 2018, 13, e0208601.
- Abdou, M.S.; Kheirallah, K.A.; Aly, M.O.; Ramadan, A.; Elhadi, Y.A.M.; Elbarazi, I.; Deghidy, E.A.; El Saeh, H.M.; Salem, K.M.; Ghazy, R.M. The coronavirus disease 2019 (COVID-19) vaccination psychological antecedent assessment using the Arabic 5C validated tool: An online survey in 13 Arab countries. PLoS One 2021, 16, e0260321. [CrossRef]
- Al-Sanafi, M.; Sallam, M. Psychological determinants of COVID-19 vaccine acceptance among healthcare workers in Kuwait: A cross-sectional study using the 5C and vaccine conspiracy beliefs scales. Vaccines 2021, 9, 701. [CrossRef]
- Gallant, A.J.; Nicholls, L.A.; Rasmussen, B.S.; Cogan, N.; Young, D.; Williams, L. Changes in attitudes to vaccination as a result of the COVID-19 pandemic: A longitudinal study of older adults in the UK. PLoS One 2021, 16, e0261844. [CrossRef]
- Kwok, K.O.; Li, K.K.; Wei, W.I.; Tang, A; Wong, S.Y.S.; Lee, S.S. Editor's choice: Influenza vaccine uptake, COVID-19 vaccination intention and vaccine hesitancy among nurses: A survey. Int J Nurs Stud 2021, 114, 103854. [CrossRef]
- Machida, M., Nakamura, I.; Kojima, T.; Saito, R.; Nakaya, T.; Hanibuchi, T.; Takamiya, T.; Odagiri, Y.; Fukushima, N.; Kikuchi, H.; et al. Trends in COVID-19 vaccination intent from pre- to post-COVID-19 vaccine distribution and their associations with the 5C psychological antecedents of vaccination by sex and age in Japan. Hum Vaccin Immunother 2021, 17, 3954–3962. [CrossRef]
- Mercadante, A.R.; Law, A.V. Will they, or won't they? Examining patients' vaccine intention for flu and COVID-19 using the health belief model. Res Social Adm Pharm 2021, 17, 1596–1605. [CrossRef]
- Obohwemu, K.; Christie-de Jong, F.; Ling, J. Parental childhood vaccine hesitancy and predicting uptake of vaccinations: A systematic review. Prim Health Care Res Dev 2022, 23, e68. [CrossRef]
- Wagner, A.; Liberatore, F.; Schmelzer, S.; Dratva, J. Confident and altruistic - parents' motives to vaccinate their children against COVID-19: A cross-sectional online survey in a Swiss vaccination centre." Swiss Med Wkly 2022, 152, w30156. [CrossRef]
- Wismans, A.; Thurik, R.; Baptista, R.; Dejardin, M.; Janssen, F.; Franken, I. Psychological characteristics and the mediating role of the 5C model in explaining students' COVID-19 vaccination intention. PLoS One 2021, 16, e0255382. [CrossRef]
- Cogordan, C.; Fressard, L.; Ramalli, S.; Rebaudet, P.; Malfait, A.; Dutrey-Kaiser, Y.; Attalah, D.; Roy, P.; Berthiaume, A.; Gagneur, A.; Verger, P. Motivational interview-based health mediator interventions increase intent to vaccinate among disadvantaged individuals. Hum Vaccin Immunother 2023, 19, 2261687. [CrossRef]
- Teng, Y.; Hanibuchi, T.; Machida, M.; Nakaya, T. Psychological determinants of COVID-19 vaccine acceptance: A comparison between immigrants and the host population in Japan. Vaccine 2023, 41, 1426–1430. [CrossRef]
- Williams, L.; Gallant, A.; Brown, L.; Corrigan, K.; Crowe, K.; Hendry, E. Barriers and facilitators to the future uptake of regular COVID-19 booster vaccinations among young adults in the UK. Hum Vaccin Immunother 2022, 18, 2129238. [CrossRef]
- Szilagyi, P. G.; Shah, M. D.; Delgado, J. R.; Thomas, K.; Vizueta, N.; Cui, Y.; Vangala, S.; Shetgiri, R.; Kapteyn, A. Parents' intentions and perceptions about COVID-19 vaccination for their children: Results from a national survey. Pediatrics 2021, 148, e2021052335. [CrossRef]
- Kezhong, A.; Lu, X.; Wang, J.; Hu, L.; Li, B; Lu, Y. Association between adult vaccine hesitancy and parental acceptance of childhood COVID-19 vaccines: A web-based survey in a northwestern region in China. Vaccines (Basel) 2021, 9, 1088. [CrossRef]
- Almalki, O.S., Alfayez, O.M.; Al Yami, M.S.; Asiri, Y. A.; Almohammed, O.A. Parents' hesitancy to vaccinate their 5-11-year-old children against COVID-19 in Saudi Arabia: Predictors from the health belief model. Front Public Health 2022, 10, 842862. [CrossRef]
- Rane, M.S.; Robertson, M.M.; Westmoreland, D.A.; Teasdale, C.A.; Grov, C.; Nash, D. Intention to vaccinate children against Covid-19 among vaccinated and unvaccinated US parents. JAMA Pediatrics 2022, 176, 201–203. [CrossRef]
- Eberhardt, C.S.; Siegrist, C.A. Is there a role for childhood vaccination against COVID-19? Pediatr Allergy Immunol 2021, 32, 9–16. [CrossRef]
- Rees, F., Geiger, M.; Lilleholt, L.; Zettler, I.; Betsch, C.; Böhm, R.; Wilhelm, O. Measuring parents' readiness to vaccinate themselves and their children against COVID-19. Vaccine 2022, 40, 3825–3834. [CrossRef]
- Swann, O.V.; Holden, K.A.; Turtle, L.; Pollock, L.; Fairfield, C.J.; Drake, T.M.; Seth, S.; Egan, C.; Hardwick, H.E.; Halpin, S.; et al. Clinical characteristics of children and young people admitted to hospital with COVID-19 in United Kingdom: Prospective multicentre observational cohort study. BMJ 2020, 370, m3249. [CrossRef]
- Horiuchi, S.; Sakamoto, H.; Abe, S.K.; Shinohara, R.; Kushima, M.; Otawa, S.; Yui, H.; Akiyama, Y.; Ooka, T.; Kojima, R.; et al. Factors of parental COVID-19 vaccine hesitancy: A cross-sectional study in Japan. PLoS One 2021, 16, e0261121. [CrossRef]
- Machida, M.; Kojima, T.; Popiel, H. A.; Geiger, M.; Odagiri, Y.; Inoue, S. Development, validity, and reliability of the Japanese version of the 7C of vaccination readiness scale. Am J Infect Control 2023, 51, 426–433. [CrossRef]
- Tokiya, M.; Hara, M.; Matsumoto, A.; Ashenagar, M.S.; Nakano; T.; Hirota, Y. Acceptance of booster COVID-19 vaccine and its association with components of vaccination readiness in the general population: A cross-sectional survey for starting booster dose in Japan. Vaccines (Basel) 2022, 10, 1102. [CrossRef]
- Ministry of Health, Labour, and Welfare. About Covid-19 vaccine (shingata korona wakutin ni tuite). https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/vaccine_00184.html. (accessed on 1 October 2024).
- Machida, M.; Kojima, T. H.; Popiel, A.; Geiger, M.; Odagiri, Y.; Inoue. Japanese version of the 7Cs of vaccination readiness. 2021. http://www.tmu-ph.ac/news/data/vaccination-readiness-01.pdf. (accessed on 1 October 2024).
- Goretzko, D.; Siemund, K.; Sterner, P. Evaluating model fit of measurement models in confirmatory factor analysis. Edu Psych Manag 2023, 00131644231163813. [CrossRef]
- Ministry of Health, Labour, and Welfare. Number of doses of the COVID-19 vaccine. 2024. https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/kenkou_iryou/kenkou/kekkaku-kansenshou/yobou-sesshu/syukeihou_00002.html. (accessed on 1 October 2024).
- Nguyen, T., Henningsen, K.H.; Brehaut, J. C.; Hoe, E.; Wilson, K. Acceptance of a pandemic influenza vaccine: A systematic review of surveys of the general public. Infect Drug Resist 2011, 4, 197–207. [CrossRef]
- Götzinger, F.; Santiago-García, B.; Noguera-Julián, A.; Lanaspa, M.; Lancella, L.; Calò Carducci, F. I.; Gabrovska, N.; Velizarova, S.; Prunk, P.; Osterman, V. et al. Covid-19 in children and adolescents in Europe: A multinational, multicentre cohort study." Lancet Child Adolesc Health 2020, 4, 653–661. [CrossRef]
- Rajapakse, N.; Dixit, D. Human and novel coronavirus infections in children: A review. Paediatr Int Child Health 2021, 41, 36–55. [CrossRef]
- Bozkurt, B.; Kamat, I.; Hotez, P.J. Myocarditis with COVID-19 mRNA vaccines. Circulation 2021, 144, 471–484. [CrossRef]
- Zimmermann, P.; Pittet, L.F.; Finn, A.; Pollard, A.J.; Curtis, N. Should children be vaccinated against COVID-19? Arch Dis Child 2022, 107, e1. [CrossRef]
- McMurray, J.; McNeil, H.; Gordon, A.; Elliott, J.; Stolee, P. Psychometric testing of a rehabilitative care patient experience instrument. Arch Phys Med Rehabil 2018, 99, 1840–1847. [CrossRef]
Figure 1.
Confirmatory factor analysis of the modified Japanese version of the 7C Vaccination Readiness Scale for parents. Numbers are estimates of standardized factor loadings. P-values were all < 0.05. χ2(14) = 83.9, p < 0.001, goodness-of-fit index (GFI) = 0.980, Bentler-Bonett Normed Fit Index (NFI) = 0.948, root mean square error of approximation (RMSEA) = 0.067, standardized root mean square residual (SRMR) = 0.040. The factor saturation (ω) = 0.970, and the Akaike information criterion (AIC) = 112.
Figure 1.
Confirmatory factor analysis of the modified Japanese version of the 7C Vaccination Readiness Scale for parents. Numbers are estimates of standardized factor loadings. P-values were all < 0.05. χ2(14) = 83.9, p < 0.001, goodness-of-fit index (GFI) = 0.980, Bentler-Bonett Normed Fit Index (NFI) = 0.948, root mean square error of approximation (RMSEA) = 0.067, standardized root mean square residual (SRMR) = 0.040. The factor saturation (ω) = 0.970, and the Akaike information criterion (AIC) = 112.
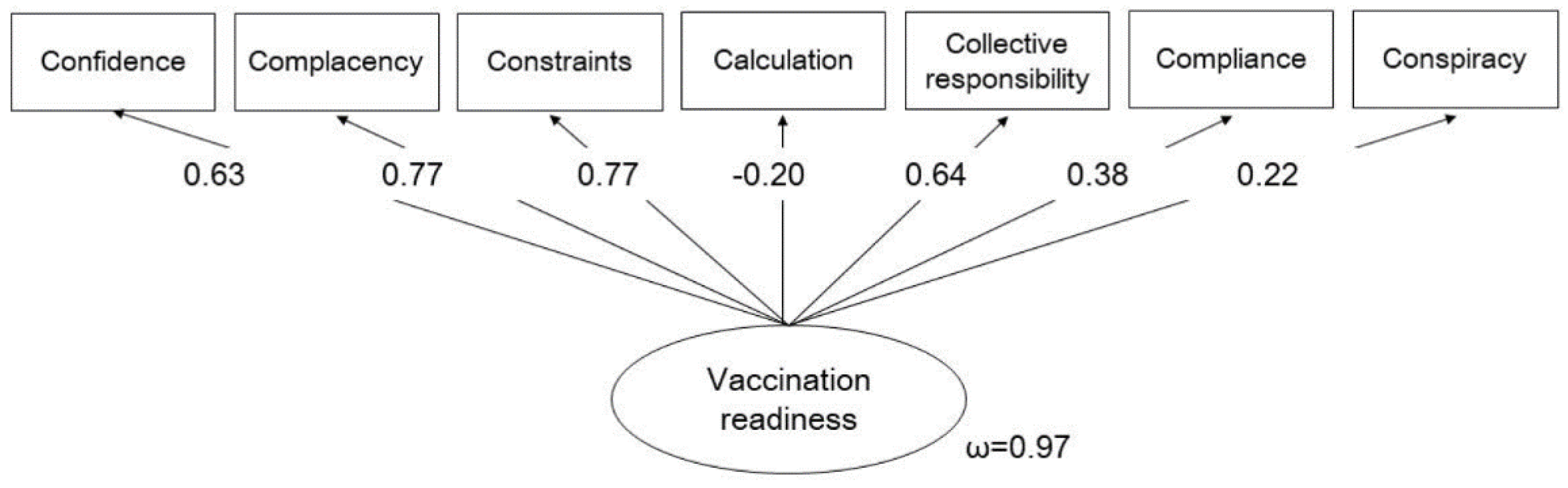
Figure 2.
Predicting parental intentions regarding having their children vaccinated against COVID-19. The numbers are estimates of standardized factor loadings. P-values were all < 0.05. The r-square of the multiple correlation coefficient for "Parental intention to vaccinate their children" was 0.70. χ2[14] = 89.5, p < 0.001, goodness-of-fit index (GFI) = 0.981, Bentler-Bonett Normed Fit Index (NFI) = 0.966, root mean square error of approximation (RMSEA) = 0.057, standardized root mean square residual (SRMR) = 0.035. The factor saturation (ω) = 0.969, and the Akaike information criterion (AIC) = 124.
Figure 2.
Predicting parental intentions regarding having their children vaccinated against COVID-19. The numbers are estimates of standardized factor loadings. P-values were all < 0.05. The r-square of the multiple correlation coefficient for "Parental intention to vaccinate their children" was 0.70. χ2[14] = 89.5, p < 0.001, goodness-of-fit index (GFI) = 0.981, Bentler-Bonett Normed Fit Index (NFI) = 0.966, root mean square error of approximation (RMSEA) = 0.057, standardized root mean square residual (SRMR) = 0.035. The factor saturation (ω) = 0.969, and the Akaike information criterion (AIC) = 124.
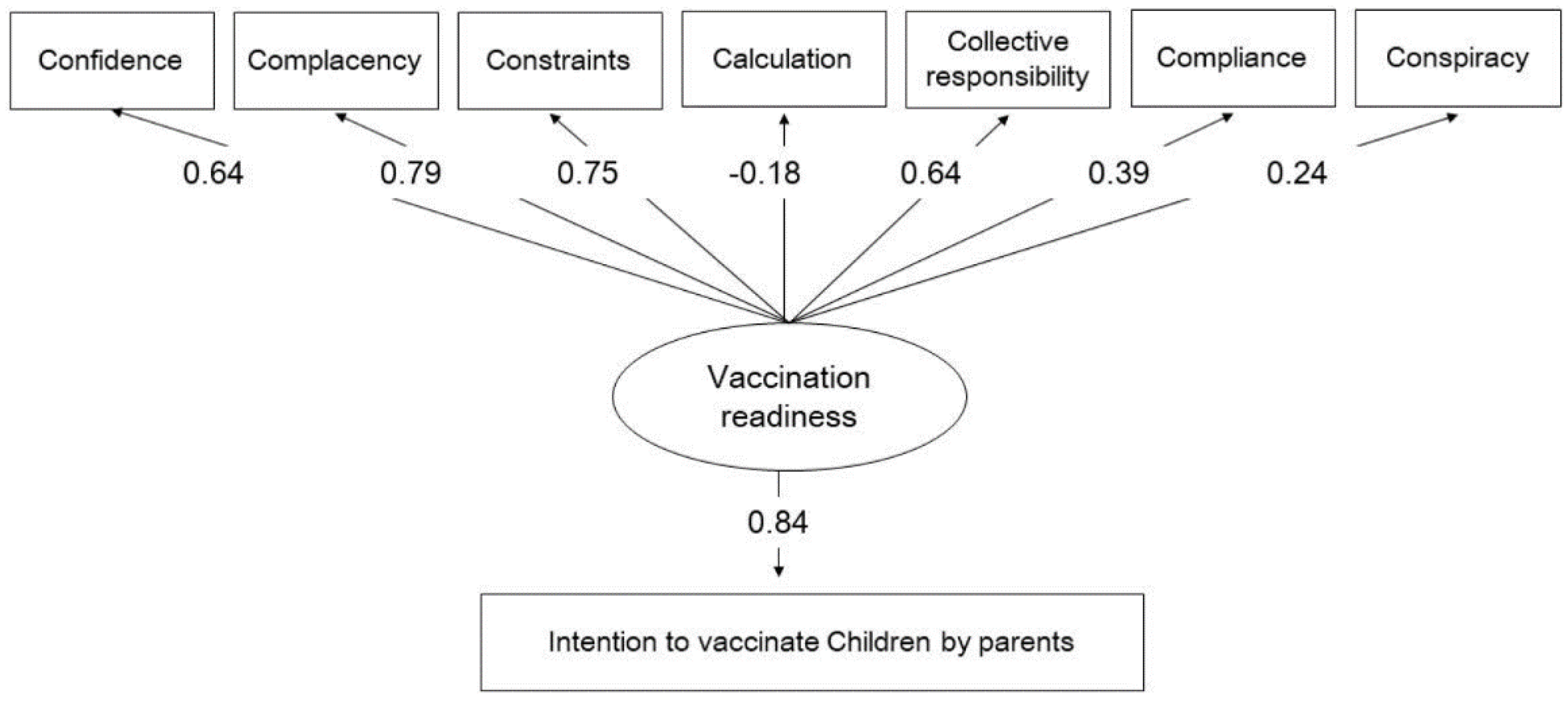
Table 1.
Modification of the Japanese version of the 7C Vaccination Readiness Scale (short version for parents).
Table 1.
Modification of the Japanese version of the 7C Vaccination Readiness Scale (short version for parents).
| 7C scale original version Short version |
Modified 7C scale original version |
Modified 7C scale Japanese version | |
|---|---|---|---|
| Confidence | I am convinced the appropriate authorities do only allow effective and safe vaccines. | I am convinced the appropriate authorities do only allow effective and safe vaccines for children. | 政府関係機関が小児に対して効果的で安全なワクチンのみを許可すると確信している. |
| Complacency | I get vaccinated because it is too risky to get infected. | I get my child vaccinated because it is too risky for children to get infected. | 小児が感染すると非常に危険なので,子どもに予防接種を受けさせる. |
| Constraints | Vaccinations are so important to me that I prioritize getting vaccinated over other things. | Vaccinations are so important for my child that I prioritize getting them vaccinated over other things. | 予防接種は子どもにとってとても大切なので,他のことよりも優先する. |
| Calculation | I only get vaccinated when the benefits clearly outweigh the risks. (R) | I only get my child vaccinated when the benefits clearly outweigh the risks. (R) | 利益が危険性より明らかに上回る場合にのみ,予防接種を受けさせる.(R) |
| Collective responsibility | I see vaccination as a collective task against the spread of diseases. | I see vaccinations as a collective task against the spread of disease in schools. | 予防接種は学校での病気の蔓延を防ぐための集団行動だと思う. |
| Compliance | It should be possible to sanction people who do not follow the vaccination recommendations by health authorities. | It should be possible to sanction parents who do not follow the vaccination recommendations by health authorities. | 保健機関による予防接種の推奨に従わない人には,制裁を加えることができるようにすべきだ. |
| Conspiracy | Vaccinations cause diseases and allergies that are more serious than the diseases they ought to protect from. (R) | Vaccinations cause diseases and allergies that are more serious than the diseases they ought to protect from. (R) | ワクチンの接種は,それが本来防ぐ病気よりも,もっと深刻な病気やアレルギーを引き起こす.(R) |
The original abbreviated version of the "Parental Readiness Scale for Vaccinating Children" and the abbreviated Japanese version developed for this project. The underlined text indicates statements that have been added. ‘R’ marks items scored in a descending order.
Table 2.
Parental intention to have their children vaccinated against COVID-19 according to parental characteristics.
Table 2.
Parental intention to have their children vaccinated against COVID-19 according to parental characteristics.
| When a pediatric vaccine for COVID-19 becomes available, I will vaccinate my children | P-valuea | |||||
|---|---|---|---|---|---|---|
| Characteristic | Strongly disagree (N = 88) n (%) |
Disagree (N = 154) n (%) |
Undecided (N = 430) n (%) |
Agree (N = 405) n (%) |
Strongly agree (N = 113) n (%) |
|
| Percent of responses | (7.4%) | (12.9%) | (36.1%) | (34.0%) | (9.5%) | |
| Sex | 0.009 | |||||
| Male | 36 (40.9) | 58 (37.7) | 171 (39.8) | 178 (44.0) | 65 (57.5) | |
| Female | 52 (59.1) | 96 (62.3) | 259 (60.2) | 227 (56.1) | 48 (42.5) | |
| Age (years), mean ± SD | 37.5 ± 6.5 | 36.5 ± 6.6 | 37.6 ± 7.8 | 40.3 ± 9.0 | 39.8 ± 9.0 | <0.001b |
| Residential region | 0.544 | |||||
| Hokkaido | 4 (4.6) | 7 (4.6) | 22 (5.1) | 19 (4.7) | 6 (5.3) | |
| Tohoku | 6 (6.8) | 5 (3.3) | 19 (4.4) | 22(5.4) | 7 (6.2) | |
| Kanto | 22 (25.0) | 37 (24.0) | 136 (31.6) | 131 (32.4) | 43 (38.1) | |
| Chubu | 14 (15.9) | 36 (23.4) | 83 (19.3) | 80 (19.8) | 17 (15.0) | |
| Kinki | 22 (25.0) | 30 (19.5) | 82 (19.1) | 74 (18.3) | 24 (21.2) | |
| Chugoku | 6 (6.8) | 7 (4.6) | 26 (6.1) | 27 (6.7) | 5 (4.4) | |
| Shikoku | 3 (3.4) | 2 (1.3) | 12 (2.8) | 12 (2.9) | 2 (1.8) | |
| Kyusyu | 11 (12.5) | 30 (19.5) | 50 (11.6) | 40 (9.9) | 9 (8.0) | |
| Marital status | 0.017 | |||||
| Unmarried | 7 (8.0) | 9 (5.8) | 36 (8.4) | 13 (3.2) | 4 (3.5) | |
| Married | 81 (92.1) | 145 (94.2) | 394 (91.6) | 392 (96.8) | 109 (96.5) | |
| Household income | 0.365 | |||||
| <4 million yen | 16 (18.2) | 15 (9.7) | 65 (15.1) | 61 (15.1) | 12 (10.6) | |
| ≥4 million yen | 54 (61.4) | 107 (69.5) | 278 (64.7) | 268 (66.2) | 85 (75.2) | |
| Unknown | 18 (20.5) | 32 (20.8) | 87 (20.2) | 76 (18.8) | 16 (14.2) | |
| Level of education | 0.140 | |||||
| ≤ High school | 15 (17.1) | 35 (22.7) | 109 (25.4) | 84 (20.7) | 18 (15.9) | |
| > High school | 73 (83.0) | 119 (77.3) | 321 (74.7) | 321 (79.3) | 95(84.1) | |
| Concerns about adverse events | ||||||
| Strongly disagree | 6 (6.8) | 5 (3.3) | 5 (1.2) | 1 (0.3) | 2 (1.8) | <0.001 |
| Disagree | 4 (4.6) | 15 (9.7) | 25 (5.8) | 14 (3.5) | 12 (10.6) | |
| Not sure | 2 (2.3) | 18 (11.7) | 91 (21.2) | 58 (14.3) | 24 (21.2) | |
| Agree | 10 (11.4) | 47 (30.5) | 148 (34.4) | 209 (51.6) | 35 (31.0) | |
| Strongly agree | 66 (75.0) | 69 (44.8) | 161 (37.4) | 123 (30.4) | 40 (35.4) | |
| Parental vaccination for COVID-19 | ||||||
| None | 40 (45.5) | 32 (20.8) | 49 (11.4) | 13 (3.2) | 4 (3.5) | <0.001 |
| Once | 1 (1.1) | 2 (1.3) | 9 (2.1) | 7 (1.7) | 1 (0.9) | |
| Twice | 47 (53.4) | 116 (75.3) | 364 (84.7) | 375 (92.6) | 106 (93.8) | |
| Three times | 0 (0.0) | 4 (2.6) | 8 (1.9) | 10 (2.5) | 2 (1.8) | |
| Number of valid responses | N = 48 | N = 122 | N = 381 | N = 392 | N = 109 | |
| Experienced any adverse eventsc | ||||||
| Fever | 26 (54.2) | 66 (54.1) | 234 (61.4) | 210 (53.6) | 62 (56.9) | 0.238d |
| Fatigue | 27 (56.3) | 70(57.4) | 240 (63.0) | 226 (57.7) | 60(55.1) | 0.429d |
| Headache | 17 (35.4) | 41 (33.6) | 140 (36.8) | 119 (30.4) | 35 (32.1) | 0.443d |
| Chill | 13 (27.1) | 20 (16.4) | 78 (20.5) | 69 (17.6) | 23 (21.1) | 0.421d |
| Vomiting | 0 (0.0) | 0 (0.0) | 11 (2.9) | 5 (1.3) | 3 (2.8) | 0.159d |
| Diarrhea | 1 (2.1) | 2 (1.6) | 7 (1.8) | 14 (3.6) | 4 (3.7) | 0.508d |
| Muscular pain | 15 (31.3) | 36 (29.5) | 102 (26.8) | 104 (26.5) | 32 (29.4) | 0.882d |
| Arthralgia | 5 (10.4) | 25 (20.5) | 58 (15.2) | 64 (16.3) | 21 (19.3) | 0.444d |
| Anaphylactic shock | 0 (0.0) | 1 (0.8) | 1 (0.3) | 1 (0.3) | 0 (0.0) | 0.702d |
a. The chi-square test was used to test the characteristics associated with parental intention to vaccinate their children. b. The Kruskal–Wallis test was used to test the characteristics associated with parental intention to vaccinate their children. P-values of ‘a’ &’b’ with significance level as <0.05/20 = 0.003. c. The number of respondents is shown, excluding missing values. d. Fisher’s exact test was used.
Table 3.
Correlation between the "modified Japanese version of the 7C Vaccination Readiness Scale for parents" component and parental intention to vaccinate their children against COVID-19.
Table 3.
Correlation between the "modified Japanese version of the 7C Vaccination Readiness Scale for parents" component and parental intention to vaccinate their children against COVID-19.
| Component | When a pediatric vaccine for COVID-19 becomes available, I will vaccinate my children | ρ | P-value | ||||
|---|---|---|---|---|---|---|---|
| Strongly disagree (Mean ± SD) |
Disagree (Mean ± SD) |
Neither agree nor disagree (Mean ± SD) |
Agree (Mean ± SD) |
Strongly Agree (Mean ± SD) |
|||
| Confidence | 1.91 ± 1.06 | 2.58 ± 0.88 | 3.03 ± 0.74 | 3.49 ± 0.78 | 3.91 ± 0.87 | 0.513 | <0.001 |
| Complacency | 1.82 ± 1.07 | 2.56 ± 0.75 | 3.06 ± 0.56 | 3.74 ± 0.67 | 4.27 ± 0.90 | 0.667 | <0.001 |
| Constraints | 1.98 ±1.10 | 2.40 ± 0.79 | 2.97 ± 0.69 | 3.58 ± 0.69 | 4.14 ± 0.85 | 0.610 | <0.001 |
| Calculation | 3.16 ± 1.42 | 2.69 ± 0.96 | 2.58 ± 0.78 | 2.50 ± 0.85 | 2.50 ± 1.13 | −0.127 | <0.001 |
| Collective responsibility | 2.44 ± 1.26 | 3.09 ± 0.86 | 3.43 ± 0.76 | 3.99 ± 0.61 | 4.43 ± 0.79 | 0.549 | <0.001 |
| Compliance | 1.56 ± 0.96 | 1.93 ± 0.92 | 2.39 ± 0.94 | 2.55 ± 1.05 | 2.88 ± 1.27 | 0.278 | <0.001 |
| Conspiracy | 2.33 ± 1.15 | 2.90 ± 0.88 | 2.98 ± 0.69 | 3.03 ± 0.76 | 3.20 ± 1.15 | 0.170 | <0.001 |
| Total vaccination readiness | 15.19 ± 4.50 | 18.16 ± 2.62 | 20.45 ± 2.35 | 22.87 ± 2.36 | 25.35 ± 3.14 | 0.678 | <0.001 |
Spearman correlation coefficient values (ρ) are shown for parents' intention to vaccinate their children against COVID-19 and the score of each component and overall score on the Japanese version of the Vaccination Readiness Scale short scale. The total vaccination readiness score was the sum of the scores for the seven components.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



