
Submitted:
09 October 2024
Posted:
10 October 2024
You are already at the latest version
Abstract
Cone-beam computed tomography (CBCT) has become a vital tool in implantology, playing a key role in both pre- and post-surgical phases. Preoperatively, CBCT provides detailed three-dimensional evaluation of anatomical structures, offering precise information on bone quality and quantity, as well as the location of critical structure. This accuracy enhances surgical planning, reducing intra- and postoperative risks and ensuring more precise implant placement. Post-surgically, CBCT is equally important for monitoring osseointegration and detecting potential complications, such as failed integration, infections, or implant misalignment. Its high-resolution imaging capabilities enable clinicians to make accurate therapeutic adjustments, improving treatment outcomes. Overall, CBCT improves decision-making in implantology, offering greater predictability and safety compared to traditional two-dimensional radiography, significantly enhancing the success rates of implant-based oral rehabilitation procedures.
Keywords:
CBCT
; dental implants
; diagnose
Introduction
In recent years, dentistry has experienced significant advances, especially in the digital area, impacting diagnosis, planning and surgical treatment.[1] Radiographic examinations are a fundamental part of this evolution, providing dentists with a detailed view of dental and maxillofacial structures. However, it is essential to obtain patients' informed consent before carrying out these examinations, ensuring that they understand the benefits and potential associated risks.
Conventional radiographs, such as intraoral and extraoral radiographs, are commonly used in clinical practice to aid diagnosis and treatment planning.[2] However, these techniques have limitations, as they only offer a two-dimensional representation of three-dimensional structures.[3,4] This can result in distortions, overlapping images and difficulties in accurately assessing certain anatomical details, such as the relationship between hard and soft tissues.[3,4] To overcome these limitations, advanced imaging techniques have become necessary, with CBCT (Cone Beam Computed Tomography) being one of the main innovations.[3] CBCT was specifically developed for maxillofacial imaging, providing three-dimensional images of high resolution and precision. [5,6]?
Since its introduction in the late 1990s, it has become an essential tool in clinical practice. [7] Compared to two-dimensional radiographs, CBCT offers images without distortion or overlap, allowing an accurate assessment of anatomical structures and significantly improving the predictability of surgical procedures.[8] In oral implantology, CBCT is used in the pre-surgical phase to assess bone quantity and quality, identify the location of vital structures such as the inferior alveolar canal and maxillary sinuses, and define the ideal positioning of implants. [9] This precision facilitates surgical planning and reduces the risk of intra- and post-operative complications. [9]
In addition, CBCT eliminates the need for invasive techniques such as surgical flap elevation, resulting in minimally invasive surgeries with shorter operative times, less post-operative discomfort and faster recovery for the patient.[10] In the post-operative period, CBCT continues to play an important role in monitoring the osseointegration of implants and in the early detection of possible complications, such as infections or failures in bone integration.[10] The ability to generate detailed three-dimensional images allows clinicians to accurately assess the progress of treatment and carry out corrective interventions when necessary [9] In addition, it is possible to monitor bone loss over time, which is crucial for the long-term success of implants.[10]
Despite its advantages, CBCT has some limitations, including higher radiation exposure compared to two-dimensional scans and difficulties in accurately assessing soft tissue.[11] Image artifacts, especially in the presence of metal restorations, can also be a challenge. [11] However, the constant advancement of technology has mitigated many of these limitations, making CBCT increasingly efficient and safe. Given its potential to improve diagnostic and therapeutic accuracy, CBCT has become indispensable in several areas of dentistry, including implantology, oral and maxillofacial surgery, endodontics, orthodontics, and periodontology.[1] Its ability to provide detailed three-dimensional data contributes to more effective and safer treatments, significantly improving clinical results and patients' quality of life.
CBCT: Development, Principles and Clinical Implications
The discovery of X-ray wavelengths by Wilhelm Conrad Röntgen in the 19th century represented a significant milestone in the history of medicine. [12] Since then, diagnostic imaging has evolved considerably, incorporating various technologies. [12] Three-dimensional radiographic images have developed to meet the demands of advanced treatment technologies, driving the emergence of new therapeutic strategies.[12]
Cone Beam Computed Tomography (CBCT) emerged from Computed Tomography, initially developed by Godfrey Hounsfield in 1967. [13] Originally conceived to provide three-dimensional cross-sectional images economically and efficiently for radiotherapy and later for angiography in 1982, CBCT was delayed in commercial availability for around 10 years, being introduced in Europe in 1998 and in the USA in 2001. [13] Columbia Scientific Inc. launched 3D software in 1988, followed by the publication of research on CBCT in 1990. [13] With the adoption of CBCT in dentistry, professionals have been able to deepen their knowledge and obtain a more detailed view of the underlying structures, simplifying the decision-making process and facilitating the identification of bone defects. [13]
Cone Beam Computed Tomography (CBCT) is a radiographic technique that generates precise three-dimensional images of hard tissue structures.[14] The term “cone beam” describes the shape of the beam that examines the patient in a circular motion around the vertical axis of the head. The head retention mechanism is crucial, regardless of the patient's position, and during a 360° examination, the X-ray source and a detector array move simultaneously.[14,15,16,17] The reading software aggregates the axial slice images and, using specific algorithms, reconstructs 3D images in DICOM format, ensuring high spatial resolution.[17,18] A CBCT radiology report should include patient identification, technical details of the examination, radiological findings and diagnostic interpretation. The findings section should address intra-oral and extra-oral observations, such as the condition of the alveolar bone and structures such as the temporomandibular joint. The diagnostic interpretation should provide a differential diagnosis and recommendations for additional examinations, if necessary.[18]
CBCT in Pre-Surgical Evaluation in Implantology
The appropriate choice of preoperative images is crucial for the surgical planning of implants. In all areas of the maxilla and mandible, there are anatomical structures that require detailed three-dimensional analysis, allowing for the selection of implant size and length, as well as assessing the height and width of the alveolar ridge and the proximity of adjacent structures. The American Academy of Oral and Maxillofacial Radiology (AAOMR) recommends the use of cross-sectional images, such as CBCT, for implant surgeries, as this provides benefits that influence surgical planning and results.[10,19]
In recent years, software for surgical planning with CBCT images has been developed, allowing dentists to simulate implants of different sizes to identify the most suitable one.[19]
CBCT also plays an essential role in the creation of drilling guides, increasing accuracy in implant positioning, and facilitating the assessment of bone crest and density, critical factors for implant success and integration. In addition, its use is associated with the maintenance of stable peri-implant tissues, better aesthetic results and reduced risks such as peri-implantitis.[20,21,22]
Anatomy structures
Nasopalatine Canal
The nasopalatine canal (NPC) requires precise evaluation in implantology, and CBCT is an essential tool for this purpose, providing precise and detailed data that helps with surgical planning. CBCT allows the exact measurement of the length and diameters of the canal, as well as morphological classification, identifying important anatomical variations such as single canals, double canals or Y-shaped bifurcations. This information is crucial to avoid complications, such as injuries to the nasopalatine nerve, which can result in sensory disturbances or bleeding.[23,24]
In 2021, Rai et al observed that the majority of individuals had funnel-shaped (38.4%), cylindrical (38.0%), hourglass (19.6%) and fusiform (4.0%) CNP. The most common NPC curvature was inclined (71.3%), followed by 15.6% of curvatures being oblique, 12.3% vertical and 0.8% curved.[24] (Figure 1)
Nasal Fossa
The nasal fossa (NF) is a crucial anatomical structure within the nasal cavity, responsible for respiratory and olfactory functions. It is divided into regions such as the nasal vestibule, the maxilloturbinal region and the ethmoid region. The NF is connected to the pterygopalatine fossa (PPF), which is located posterior to the maxillary sinus and establishes communications with various anatomical areas, including the nasal cavity and the orbit.[28,29,30] (Figure 2)
In implantology, the NF is an important reference point due to its proximity to the maxillary sinus, which can lead to dental implants migrating into the NF, requiring extraction via rhinoscopy. Placing implants in the transnasal bone between the maxillary sinus and the NF allows the use of extralong implants to support full-arch prostheses.[31,32,33]
However, a significant challenge in placing implants in the NF is the risk of perforation, which can be asymptomatic and cause symptoms such as mucopurulent discharge and nasal discomfort. The extension of implants into the nasal cavity is associated with rhinosinusitis and rhinitis.[33,34] (Figure 3).
Canalis Sinuosos
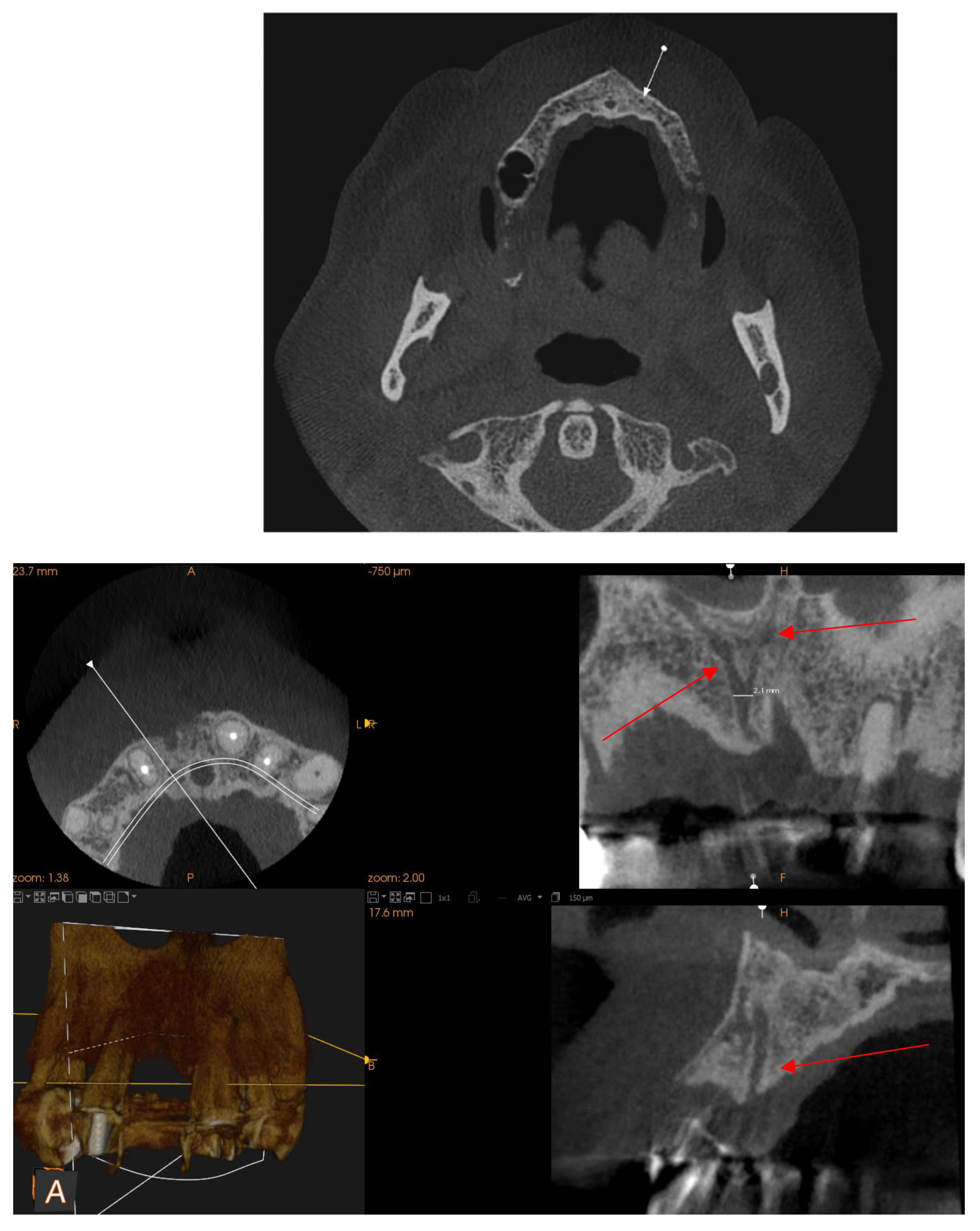
The canalis sinuosus (CS) is a crucial anatomical structure in dental implantology, especially in the anterior maxilla. It is a neurovascular canal that originates from the nerve of the infraorbital canal, through which the superior alveolar nerve passes, sloping medially between the nasal cavity and the maxillary sinus, reaching the premaxilla in the region of the canines and incisors. (Figure 4) CS is usually bilateral, although it can rarely be unilateral.[35]
Its length is little discussed in the literature, with an average of around 55 mm in the maxilla and a vertical distance between the infraorbital foramen and the SC ranging from 0 to 9 mm. [35,36]
The relevance of the SC in the rehabilitation of the anterior maxillary region is evident, especially when using the canine abutment as a support for implants. Contact with the neurovascular bundle of the superior alveolar nerve can compromise osseointegration and induce temporary or permanent paresthesia, as well as bleeding.[37]
Due to its discreet nature on standard radiographs, the SC is often overlooked in implant planning, being identified as a radiolucent image in the periapical region of the canines and maxillary lateral incisors. [38]
Figure 4.
– a) Presence of SC in CBCT cross-sections in the region of tooth 13.[37] b) Presence of SC and anatomical variation of 2,1mm of diameter in 11.
Figure 4.
– a) Presence of SC in CBCT cross-sections in the region of tooth 13.[37] b) Presence of SC and anatomical variation of 2,1mm of diameter in 11.
Maxillary Sinus
In the context of implantology and the osseointegration process, the maxillary sinus (MS), also known as the Highmore antrum, plays a crucial role. Located in the body of the maxillary bone, the MS is pyramidal in shape, with an average height of approximately 33 mm, a width of 23 mm and an anteroposterior length of around 34 mm. As the largest of the paranasal sinuses, its functions include phonatory resonance, air conditioning and equalization of pressures in the nasal cavity, and it is lined by Schneider's membrane. Sensory innervation is provided by branches of the maxillary nerve, especially the posterior superior alveolar branch.[39,40,41,42]
The anatomical relationship between the SM and the roots of the maxillary posterior teeth is critical in implant placement, as resorption of the alveolar process following tooth loss can lead to pneumatization of the SM, making implant placement difficult and increasing the risk of complications such as perforation of the sinus membrane and sinusitis.[43,44] (Figure 5).
Septa
The maxillary sinus cavity is often subdivided by septa, which are thin walls of cortical bone that protrude from the sinus floor. These septa can be classified as primary, formed during maxillary development, and secondary, which develop after tooth loss and irregular pneumatization of the sinus floor. The prevalence of septa ranges from 10% to 58% in the literature.[48,49] (Figure 6)
Implant planning in the maxilla is challenged by bone atrophy of the alveolar process, especially in the distal region. The reduction in bone height increases the need for elevation of the maxillary sinus floor, which is influenced by the presence of septa, as the adhesive force of the Schneiderian membrane is greater in these areas.[49]
Although septa have been considered clinically insignificant, complications such as perforation of Schneider's membrane have been reported, often associated with their presence. To ensure successful sinus augmentation and avoid complications, assessment of the septa before surgery is crucial. The use of CBCT-based digital implant planning software enables the detection of risks related to maxillary sinus septa.[48,49]
Posterior superior alveolar artery
The posterior superior alveolar artery (PSAA), a branch of the maxillary artery originating from the external carotid artery, supplies blood to the maxillary molars, the maxillary sinus and the surrounding gingival tissues. This artery normally runs along the lateral wall of the MS and can have branches, significantly influencing surgical procedures in the area.[50,51] (Figure 7)
The proximity of the PSAA to the MS and the alveolar ridge is critical when planning the placement of dental implants, as its location can impact surgical techniques, especially in elevations of the MS, where the risk of arterial injury is high. Understanding the anatomy of the PSAA enables safer surgical interventions, minimizing complications such as excessive bleeding.[52,53,54]
The PSAA anastomoses with the infraorbital artery in the oral cavity. In cases of bleeding during osteotomy, it can be controlled by compression or cauterization, with a larger diameter of the compromised vessels resulting in more abundant bleeding.[55]
A study by Hakiem Tawfiew et al. (2023) revealed a higher prevalence of PSAA in women than in men, suggesting a lower risk of hemorrhage in surgical procedures in women.[56]
Mentonian Hole
The mentonian hole (MB) is an anatomical structure located on the anterior surface of the mandible, varying in position both horizontally and vertically. Fishel et al. (1976) observed that 70% of the BM are located between the premolars, while 22% are located in their apical area. Most BM are above the level of the premolar apices, functioning as a channel for the mentonian nerve, which innervates the lower lip, chin and buccal gingiva of the lower incisors.[57,58] (Figure 8)
Correctly determining the position of the BM is crucial to ensure adequate local anesthesia and minimize injuries during surgical procedures. The inferior alveolar nerve often passes a few millimeters in front of the BM, forming the so-called anterior loop, which must be respected when positioning implants.[59]
Complications related to the BM can include lesions of the mentonian nerve, resulting in paresthesia of the lower lip, impacting the patient's quality of life. The anatomy of the BM varies between populations, with an average distance from the midline of the mandible of approximately 25 mm, influenced by age and gender.[59,60]
Sublingual Hole and Canal
Dental implants are currently the main choice for the prosthetic rehabilitation of edentulous patients. However, the placement of implants in the anterior region of the mandible can cause perforation of the lingual cortex, resulting in severe bleeding due to the proximity of the arteries connected to the lingual hole. The lingual hole, located on the inner surface of the mandible, serves as an entrance to the bony canals and is a route for branches of the sublingual and submentonian arteries, increasing the risk of surgical complications.[61]
A descriptive study by Vásquez (2019) analyzed 225 CBCT scans and found that the distance between the lingual hollow and the alveolar ridge was slightly greater in women, while the length of the hollow was greater in men. The course of the lingual canal is upward in most cases, but 28% have a downward course.[61,62]
Mandibular Canal
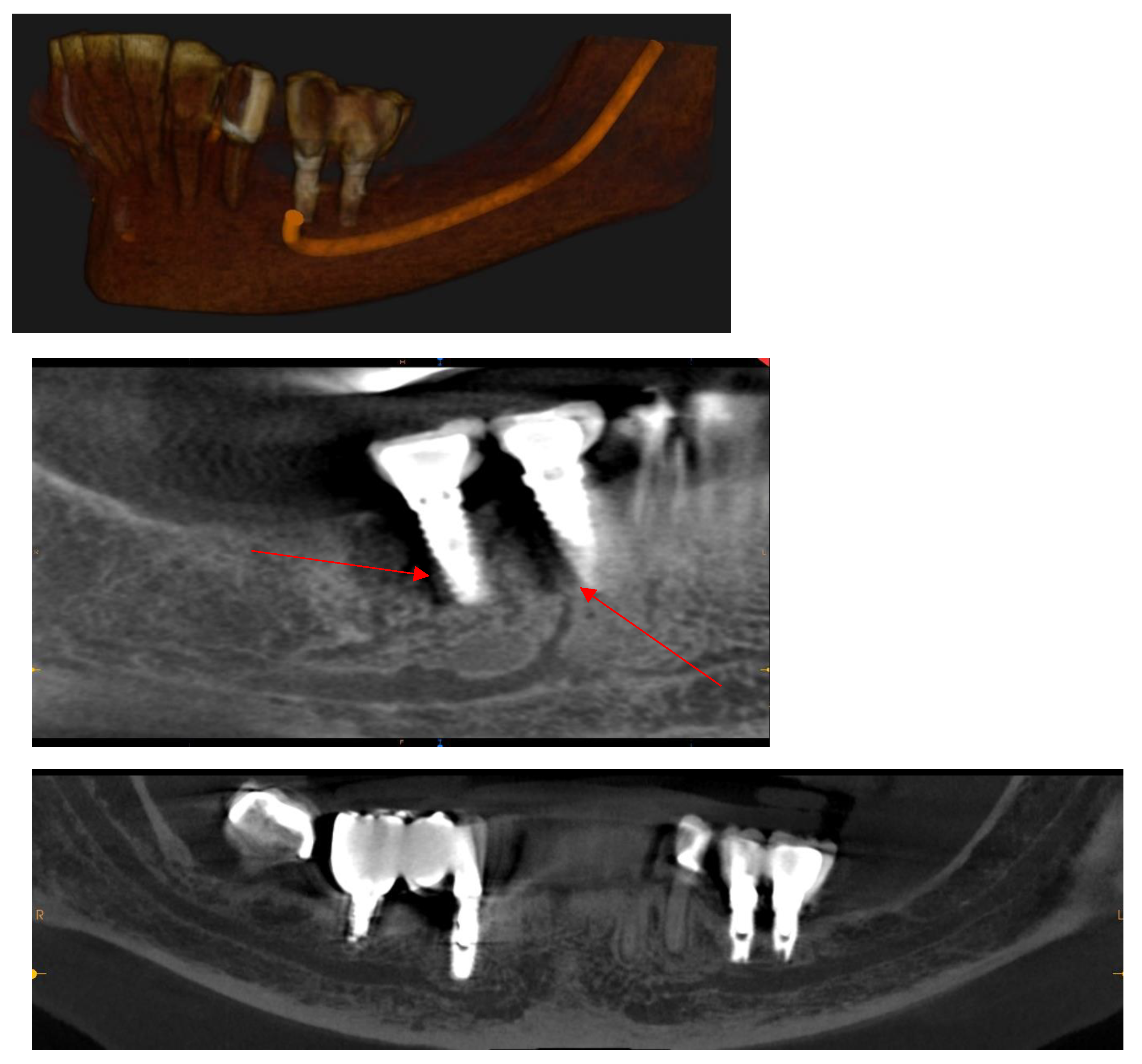
The mandibular canal, also known as the inferior alveolar canal, is a bony canal that houses the inferior alveolar nerve and the inferior alveolar artery, forming the inferior alveolar vasculonervous bundle. It extends from the mandibular pit to the mental pit.[64,65] (Figure 10).
Radiographically, the canal appears as a well-defined radiotransparent line, delimited by radiopaque lines. The location of the mandibular canal is crucial for dental implant surgery, as damage to the inferior alveolar nerve can result in temporary or permanent paralysis, with an incidence of between 6.5% and 37%. Inadequate bone length assessments and the use of very long implants increase this risk. Therefore, accurate assessment of the canal position prior to implant placement is essential.[66]
Implants in the posterior region of the mandible face challenges, especially in cases of bone atrophy. The reduced vertical distance between the alveolar crest and the roof of the canal requires the vertical safety distance to be at least 6 mm to avoid nerve damage. Chavarry (2019) suggests that implants vestibular to the mandibular canal may be an effective alternative for rehabilitating posterior atrophic ridge.[67]
Assessment, Planning and Prevention in the Surgical Context
CBCT is a fundamental technology in the assessment of bone density in implantology, allowing a precise three-dimensional analysis of the quantity and quality of bone available for the placement of dental implants. This tool provides a detailed visualization of bone structures and their anatomical relationships and is essential for pre-surgical planning and predictable results.[68]
Studies show that high bone density is associated with a higher success rate and primary stability of implants.[69] Lekholm and Zarb (1985) classified bone density into four types based on the proportion of cortical and trabecular bone, with implants in type I, II and III bone having a higher survival rate compared to type IV bone.[70]
Bone density, measured in Hounsfield Units (HU) in conventional tomography, can also be assessed by gray values in CBCT, helping to determine the quality of the bone and influencing surgical planning.[71,72]
CBCT improves all aspects of implantology, from diagnosis to surgical execution and post-operative follow-up. A study by Buser et al. (2013) revealed that the use of CBCT in early implants resulted in stability of the peri-implant tissues and a reduced risk of mucosal recession, with successful maintenance of the facial bone wall in 95% of patients. Detailed analysis of adjacent anatomical structures, such as the residual alveolar ridge, maxillary sinus and mandibular canal, is crucial to avoid complications such as neurosensory lesions or perforation of the sinus membrane.[19,73]
CBCT offers a 3D analysis that makes it possible to determine the height, width and quality of the bone, identify important anatomical structures and fabricate surgical guides. Studies by Suomalainen et al. (2008) indicate that CBCT measurements are reliable and accurate for implant planning. In addition, the AAOMR reinforces the importance of accurate diagnoses to ensure implant success.[19]
In the context of preventing surgical complications, CBCT also plays a role in detailed pre-surgical analysis, complemented by assessment of the medical and dental history. Patients with diseases such as diabetes or who take specific medications, such as bisphosphonates, may be at greater risk of complications, requiring an adapted approach.[74,75]
In addition, smoking cessation and oral hygiene education are crucial to prevent conditions such as peri-implantitis and increase implant longevity.[76],
Informed consent is vital to ensure that patients understand the risks and benefits of the procedure.[77]
CBCT in the Post-Surgical Phase: Assessment of Bone Loss and Post-Operative Surgical Complications
Cone Beam Computed Tomography (CBCT) plays a crucial role in the post-surgical phase of dental implants, especially in the assessment of peri-implantitis. This imaging modality makes it possible to monitor the condition of the bone graft and the position of the implant, facilitating effective planning and ensuring correct positioning in relation to critical anatomical structures, such as the inferior alveolar nerve.[21,78]
Assessing the success of implants involves clinical and radiographic examinations. Although 2D intraoral radiographs are useful, they have limitations, such as image overlap, while CBCT excels in detecting peri-implant defects, especially in assessing bone loss related to peri-implantitis. CBCT is recommended in cases of persistent pain or the need for bone augmentation, allowing for a more precise analysis of bone morphology.[10]
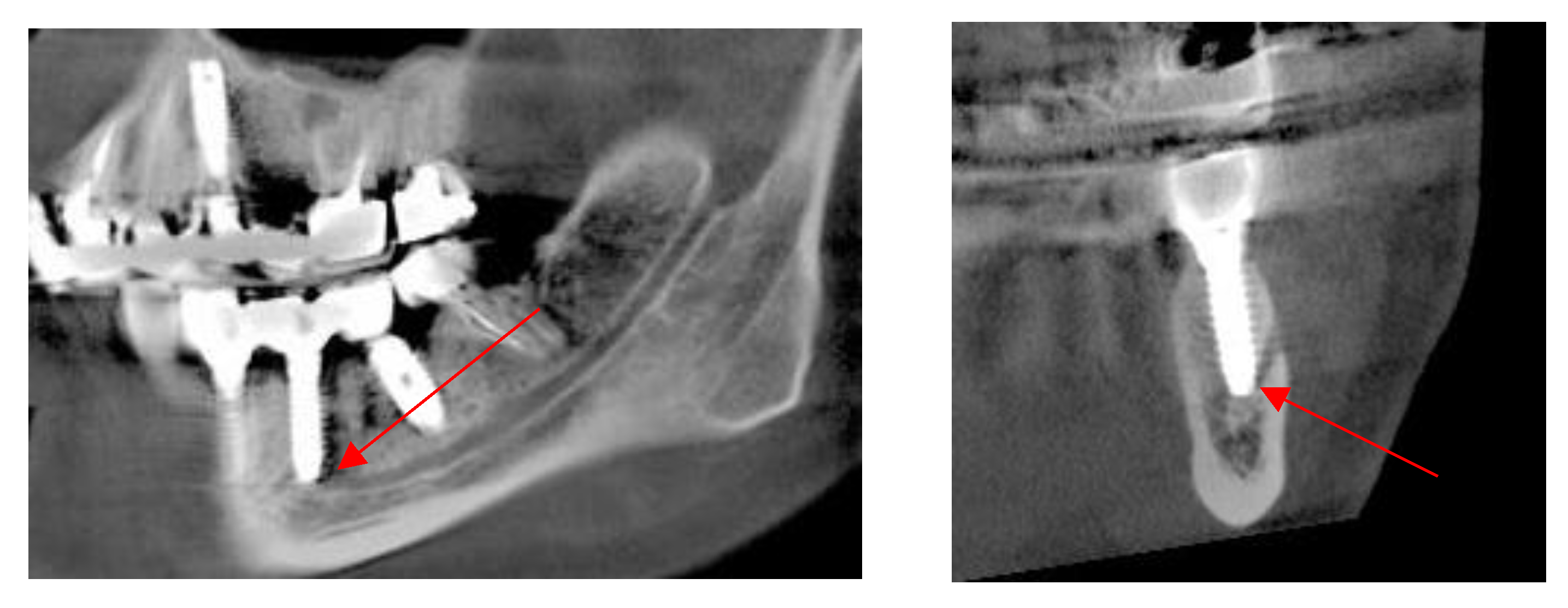
Figure 11.
– Implant in contact with mandibular canal.
3D CBCT images offer a better morphological assessment and volumetric data on bone, which is particularly relevant in the context of bone healing and monitoring peri-implantitis. Studies indicate that early detection of marginal bone loss, often associated with peri-implantitis, is essential for the long-term success of implants.[10,79]
In the post-operative phase, CBCT is essential for assessing complications such as lesions in neurovascular structures and peri-implant bone loss. Initial crestal bone loss is common and can be influenced by factors such as surgical trauma and microgap, with direct implications for peri-implant health.[80,81]
The ability of CBCT to identify the extent of bone loss and classify peri-implant bone defects allows for more effective treatment planning for peri-implantitis. In addition, the assessment of peri-implantitis is crucial for maintaining implant health. CBCT has shown high accuracy in the early detection of marginal bone loss, compared to intraoral radiographs, with a sensitivity of 100% compared to 69-63% for radiographs.[82]
This underlines the importance of CBCT in the assessment and management of peri-implantitis. Complications such as nerve damage can occur after implant placement, resulting in paresthesia, which is often painless.[83]
Infection is a common cause of implant placement failure, requiring adequate antibiotic prophylaxis, now recommended for a maximum of three days after surgery.[84,85]
Finally, the presence of bruising after surgery is a normal condition that should be communicated to patients.[86]
The combination of CBCT with rigorous clinical follow-up is fundamental to the long-term success of implant treatments, especially with regard to the management of peri-implantitis.
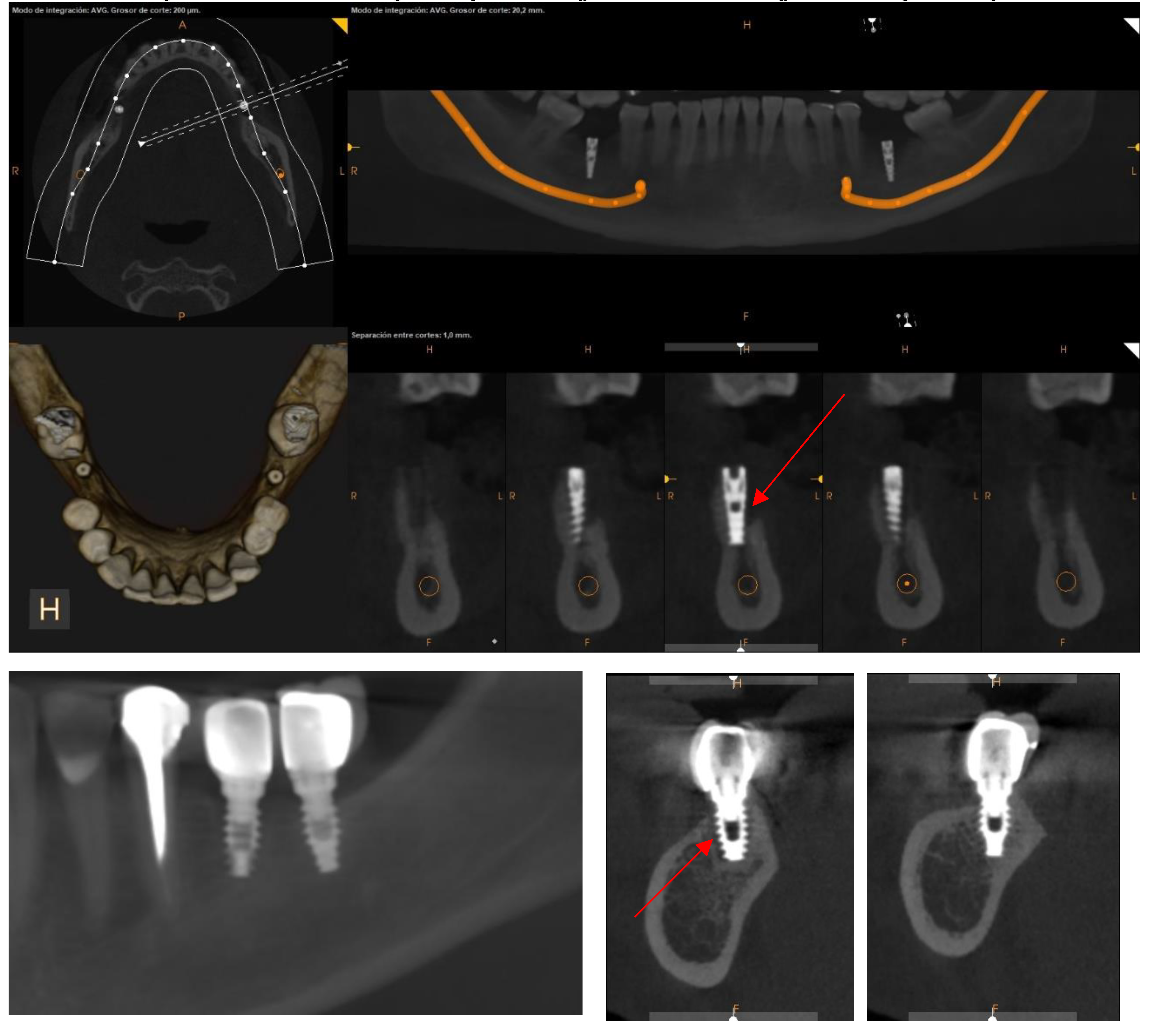
Figure 12.
-a)Implant with periimplantitis. b)panoramic reconstruction with 2 implants in 36 y 37 c &d) same implants of b) showing periimplantitis (arrow) in 36 and normality in 37.
Figure 12.
-a)Implant with periimplantitis. b)panoramic reconstruction with 2 implants in 36 y 37 c &d) same implants of b) showing periimplantitis (arrow) in 36 and normality in 37.
Conclusion
Implantology has transformed oral rehabilitation by offering long-lasting and aesthetic solutions to tooth loss. The advancement of implant techniques is linked to the evolution of imaging technologies, with CBCT being an essential tool in today's practice. In the pre-surgical phase, CBCT provides a detailed three-dimensional view of bone and soft tissue structures, allowing the analysis of bone quality and quantity, and the identification of anatomical limitations. This results in more precise surgical planning, reducing risks and increasing the predictability of results. After surgery, CBCT is crucial in monitoring healing and assessing results, ensuring the correct position of the implant. In conclusion, it is essential to improve students' knowledge of CBCT by dedicating more curricular time to this advanced imaging modality, which is becoming standard in various dental specialties.
References
- Gaêta-Araujo, H.; Alzoubi, T.; Vasconcelos, K.D.F.; Orhan, K.; Pauwels, R.; Casselman, J.W.; Jacobs, R. Cone beam computed tomography in dentomaxillofacial radiology: A two-decade overview. Dentomaxillofacial Radiology 2020, 49, 20200145. [Google Scholar] [CrossRef] [PubMed]
- Du Bois, A.; Kardachi, B.; Bartold, P. Is there a role for the use of volumetric cone beam computed tomography in periodontics? Australian Dental Journal 2012, 57, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Davidopoulou, S.; Karakostas, P.; Batas, L.; Barmpalexis, P.; Assimopoulou, A.; Angelopoulos, C.; Tsalikis, L. Multidimensional 3D-Printed Scaffolds and Regeneration of Intrabony Periodontal Defects: A Systematic Review. Journal of Functional Biomaterials 2024, 15, 44. [Google Scholar] [CrossRef] [PubMed]
- Shah, N. Recent advances in imaging technologies in dentistry. World Journal of Radiology 2014, 6, 794. [Google Scholar] [CrossRef] [PubMed]
- Mandelaris, G.A.; Scheyer, E.T.; Evans, M.; Kim, D.; McAllister, B.; Nevins, M.L.; Rios, H.F.; Sarment, D. American Academy of Periodontology Best Evidence Consensus Statement on Selected Oral Applications for Cone-Beam Computed Tomography. Journal of Periodontology 2017, 88, 939–945. [Google Scholar] [CrossRef]
- Ludlow, J.B.; Timothy, R.; Walker, C.; Hunter, R.; Benavides, E.; Samuelson, D.B.; Scheske, M.J. Effective dose of dental CBCT—a meta analysis of published data and additional data for nine CBCT units. Dentomaxillofacial Radiology 2015, 44, 20140197. [Google Scholar] [CrossRef]
- Lindfors, N.; Ekestubbe, A.; Frisk, F.; Lund, H. Is cone-beam computed tomography (CBCT) an alternative to plain radiography in assessments of dental disease? A study of method agreement in a medically compromised patient population. Clinical Oral Investigations 2024, 28, 127. [Google Scholar] [CrossRef] [PubMed]
- De Faria Vasconcelos, K.; Evangelista, K.; Rodrigues, C.; Estrela, C.; De Sousa, T.; Silva, M. Detection of periodontal bone loss using cone beam CT and intraoral radiography. Dentomaxillofacial Radiology 2012, 41, 64–69. [Google Scholar] [CrossRef]
- Jain, S.; Choudhary, K.; Nagi, R.; Shukla, S.; Kaur, N.; Grover, D. New evolution of cone-beam computed tomography in dentistry: Combining digital technologies. Imaging Science in Dentistry 2019, 49, 179. [Google Scholar] [CrossRef]
- Weiss, R.; Read-Fuller, A. Cone Beam Computed Tomography in Oral and Maxillofacial Surgery: An Evidence-Based Review. Dentistry Journal 2019, 7, 52. [Google Scholar] [CrossRef]
- Kamburoğlu, K. Use of dentomaxillofacial cone beam computed tomography in dentistry. World Journal of Radiology 2015, 7, 128. [Google Scholar] [CrossRef] [PubMed]
- Venkatesh, E.; Venkatesh Elluru, S. (2017). CONE BEAM COMPUTED TOMOGRAPHY: BASICS AND APPLICATIONS IN DENTISTRY. Journal of Istanbul University Faculty of Dentistry, 51. [CrossRef]
- Shukla, S.; Chug, A.; Afrashtehfar, K. Role of cone beam computed tomography in diagnosis and treatment planning in dentistry: An update. Journal of International Society of Preventive and Community Dentistry 2017, 7, 125. [Google Scholar] [CrossRef]
- Kumar, M.; Shanavas, M.; Sidappa, A.; Kiran, M. (2015). Cone Beam Computed Tomography—Know its Secrets. Cone Beam Computed Tomography.
- Abramovitch, K.; Rice, D.D. Basic Principles of Cone Beam Computed Tomography. Dental Clinics of North America 2014, 58, 463–484. [Google Scholar] [CrossRef] [PubMed]
- Scarfe, W.C.; Farman, A.G. What is Cone-Beam CT and How Does it Work? Dental Clinics of North America 2008, 52, 707–730. [Google Scholar] [CrossRef]
- Howerton, W.B.; Mora, M.A. Advancements in Digital Imaging. The Journal of the American Dental Association 2008, 139, S20–S24. [Google Scholar] [CrossRef]
- Heller, Z.A.; Hogge, M.; Ragan, M.R.; Portnof, J.E. Applications of Cone Beam Computed Tomography Scans in Dental Medicine and Potential Medicolegal Issues. Dental Clinics of North America 2024, 68, 55–65. [Google Scholar] [CrossRef] [PubMed]
- Hussaini, S.; Glogauer, M.; Sheikh, Z.; Al-Waeli, H. CBCT in Dental Implantology: A Key Tool for Preventing Peri-Implantitis and Enhancing Patient Outcomes. Dentistry Journal 2024, 12, 196. [Google Scholar] [CrossRef]
- Jha, S.; Pathi, J.; Sangamesh, N.C.; Singh, D.K.; Sikdar, A.; Dash, M. (2022). Marginal Bone Level and Bone Quality Evaluation Using CBCT after Functional Loading around Dental Implant in the Population of Bhubaneswar, Odisha: A Longitudinal Study. Journal of Pharmaceutical Research International, 6–13. [CrossRef]
- Meer Rownaq Ali, A.B.; Khanam, K.G.K.K.; Mathew, A. CBCT- A Boon for Implant Dentistry. Saudi Journal of Oral and Dental Research 2019, 04, 691–699. [Google Scholar] [CrossRef]
- Zewail, A.M.; Abdullah, A.B.; Aboelhasan, M.F.; El-Ashmawy, M.M.; Ibrahim, A.G. Qualitative Analysis of Maxillary Sinus after Guided Lateral Sinus Lift Procedure with Simultaneous Implant Placement. Al-Azhar Assiut Dental Journal 2024, 7, 103–111. [Google Scholar] [CrossRef]
- Fernández Bodereau, E.; Flores, V.Y.; Naldini, P.; Torassa, D.; Tortolini, P. Clinical Evaluation of the Nasopalatine Canal in Implant-Prosthetic Treatment: A Pilot Study. Dentistry Journal 2020, 8, 30. [Google Scholar] [CrossRef]
- Rai, S.; Misra, D.; Misra, A.; Khatri, M.; Kidwai, S.; Bisla, S.; Jain, P. Significance of morphometric and anatomic variations of nasopalatine canal on cone-beam computed tomography in anterior functional zone—A retrospective study. Annals of Maxillofacial Surgery 2021, 11, 108. [Google Scholar] [CrossRef] [PubMed]
- Fokas, G.; Vaughn, V.M.; Scarfe, W.C.; Bornstein, M.M. Accuracy of linear measurements on CBCT images related to presurgical implant treatment planning: A systematic review. Clinical Oral Implants Research 2018, 29, 393–415. [Google Scholar] [CrossRef]
- Guerrero, M.E.; Noriega, J.; Jacobs, R. Preoperative implant planning considering alveolar bone grafting needs and complication prediction using panoramic versus CBCT images. Imaging Science in Dentistry 2014, 44, 213. [Google Scholar] [CrossRef]
- Singhal, M.; Dandriyal, R.; Aggarwal, A.; Agarwal, A.; Yadav, S.; Baranwal, P. Implant placement into the nasopalatine foramen: Considerations from anatomical and surgical point of view. Annals of Maxillofacial Surgery 2018, 8, 347. [Google Scholar] [CrossRef]
- Battaglia, P.; Turri–Zanoni, M.; Lepera, D.; Sica, E.; Karligkiotis, A.; Dallan, I.; Castelnuovo, P. (2016). Endoscopic transnasal approaches to pterygopalatine fossa tumors. Head & Neck, 38. [CrossRef]
- Omura, K.; Nomura, K.; Mori, R.; Ishii, Y.; Tanaka, Y.; Otori, N.; Kojima, H. Advanced Endoscopic Endonasal Approach to the Pterygopalatine Fossa and Orbit: The Endoscopic Tri-port Approach. Journal of Neurological Surgery Part B: Skull Base 2021, 82, 437–442. [Google Scholar] [CrossRef] [PubMed]
- Ranslow, A.N.; Richter, J.P.; Neuberger, T.; Van Valkenburgh, B.; Rumple, C.R.; Quigley, A.P.; Pang, B.; Krane, M.H.; Craven, B.A. Reconstruction and Morphometric Analysis of the Nasal Airway of the White-Tailed Deer ( Odocoileus virginianus ) and Implications Regarding Respiratory and Olfactory Airflow. The Anatomical Record 2014, 297, 2138–2147. [Google Scholar] [CrossRef]
- Oh, S.; Zelig, D.; Aalam, A.A.; Kurtzman, G.M. (2023). Case report: Utilization of Z-Point fixture “Trans-nasal” implants. Annals of Medicine & Surgery. [CrossRef]
- Sanchis, J.; Díaz, J. (2021). Accidental migration of dental implant into the nasal cavity: Spontaneous expulsion through the nose. Journal of Clinical and Experimental Dentistry, 1060; e1057–e1060. [Google Scholar] [CrossRef]
- Yeom, H.-G.; Huh, K.-H.; Yi, W.-J.; Heo, M.-S.; Lee, S.-S.; Choi, S.-C.; Kim, J.-E. Nasal cavity perforation by implant fixtures: Case series with emphasis on panoramic imaging of nasal cavity extending posteriorly. Head & Face Medicine 2023, 19, 37. [Google Scholar] [CrossRef]
- Biafora, M.; Bertazzoni, G.; Trimarchi, M. Maxillary Sinusitis Caused by Dental Implants Extending into the Maxillary Sinus and the Nasal Cavities. Journal of Prosthodontics 2014, 23, 227–231. [Google Scholar] [CrossRef]
- Arruda, J.A.; Silva, P.; Silva, L.; Álvares, P.; Silva, L.; Zavanelli, R.; Rodrigues, C.; Gerbi, M.; Sobral, A.P.; Silveira, M. Dental Implant in the Canalis Sinuosus: A Case Report and Review of the Literature. Case Reports in Dentistry 2017, 2017, 1–5. [Google Scholar] [CrossRef]
- Von Arx, T.; Lozanoff, S.; Sendi, P.; Bornstein, M.M. Assessment of bone channels other than the nasopalatine canal in the anterior maxilla using limited cone beam computed tomography. Surgical and Radiologic Anatomy 2013, 35, 783–790. [Google Scholar] [CrossRef]
- Manhães Júnior, L.R.C.; Villaça-Carvalho, M.F.L.; Moraes, M.E.L.; Lopes, S.L.P.D.C.; Silva, M.B.F.; Junqueira, J.L.C. (2016). Location and classification of Canalis sinuosus for cone beam computed tomography: Avoiding misdiagnosis. Brazilian Oral Research, 30. [CrossRef]
- Shelley, A.; Rushton, V.; Horner, K. Canalis sinuosus mimicking a periapical inflammatory lesion. British Dental Journal 1999, 186, 378–379. [Google Scholar] [CrossRef] [PubMed]
- de Sousa, F.O.; Kassis, E.N.; Manzini, R. (2022). Molecular, cellular and surgical processes of osseointegration for dental implants: A systematic review. 3.
- Hamdy, R.M. (2013). Three-dimensional linear and volumetric analysis of maxillary sinus pneumatization.
- Iwanaga, J.; Wilson, C.; Lachkar, S.; Tomaszewski, K.A.; Walocha, J.A.; Tubbs, R.S. (2018). Clinical anatomy of the maxillary sinus: Application to sinus floor augmentation.
- Whyte, A.; Boeddinghaus, R. (2019). The maxillary sinus: Physiology, development and imaging anatomy. The Maxillary Sinus.
- Li, L.; Fu, Y.; Huang, S.; Lai, Z.; Ge, J. (2020). An Analysis of The Relationship between The Maxillary Molars and The maxillary sinus oor in Adult Patient Using Cone-beam Computed Tomography.
- Nogami, S.; Yamauchi, K.; Tanuma, Y.; Odashima, K.; Matsui, A.; Tanaka, K.; Takahashi, T. (2016). Removal of dental implant displaced into maxillary sinus by combination of endoscopically assisted and bone repositioning techniques: A case report.
- Çam, K.; Zengi̇N, A.Z. (2024). Evaluation of the Localization of Posterior Superi̇or Alveolar Artery and Infraorbital Foramen Originating From the Same Source by Using Conic Beam Computed Tomography. [CrossRef]
- Khalighi Sigaroudi, A.; Dalili Kajan, Z.; Rastgar, S.; Neshandar Asli, H. Frequency of different maxillary sinus septal patterns found on cone-beam computed tomography and predicting the associated risk of sinus membrane perforation during sinus lifting. Imaging Science in Dentistry 2017, 47, 261. [Google Scholar] [CrossRef] [PubMed]
- Raghav, M.; Karjodkar, F.; Sontakke, S.; Sansare, K. Prevalence of incidental maxillary sinus pathologies in dental patients on cone-beam computed tomographic images. Contemporary Clinical Dentistry 2014, 5, 361. [Google Scholar] [CrossRef]
- Assari, A.; Alotaibi, N.; Alajaji, M.A.; Alqarni, A.; Ali Alarishi, M. Characteristics of Maxillary Sinus Septa: A Cone-Beam Computed Tomography Evaluation. International Journal of Dentistry 2022, 2022, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Hungerbühler, A.; Rostetter, C.; Lübbers, H.-T.; Rücker, M.; Stadlinger, B. Anatomical characteristics of maxillary sinus septa visualized by cone beam computed tomography. International Journal of Oral and Maxillofacial Surgery 2019, 48, 382–387. [Google Scholar] [CrossRef]
- Dworski, K.; Mazurek, M.; Domański, J. Posterior superior alveolar artery – an anatomical and clinical case report. Medical Journal of Cell Biology 2023, 11, 93–97. [Google Scholar] [CrossRef]
- Tofangchiha, M.; Hematzadeh, S.; Vali, M.E.; Ghonche, M.R.A.; Mirzadeh, M.; Reda, R.; Testarelli, L. Anatomical localization of posterior superior alveolar artery: A retrospective study by cone-beam computed tomography. Dental and Medical Problems 2022, 59, 407–412. [Google Scholar] [CrossRef]
- McDaniel, C.R.; Johnson, T.M.; Stancoven, B.W.; Lincicum, A.R. Distribution of the intraosseous branch of the posterior superior alveolar artery relative to the posterior maxillary teeth. Imaging Science in Dentistry 2024, 54, 121. [Google Scholar] [CrossRef]
- Radmand, F.; Razi, T.; Baseri, M.; Gavgani, L.F.; Salehnia, F.; Faramarzi, M. Anatomic evaluation of the posterior superior alveolar artery using cone-beam computed tomography: A systematic review and meta-analysis. Imaging Science in Dentistry 2023, 53, 177. [Google Scholar] [CrossRef]
- Tehranchi, M.; Taleghani, F.; Shahab, S.; Nouri, A. Prevalence and location of the posterior superior alveolar artery using cone-beam computed tomography. Imaging Science in Dentistry 2017, 47, 39. [Google Scholar] [CrossRef]
- Mardinger, O.; Abba, M.; Hirshberg, A.; Schwartz-Arad, D. Prevalence, diameter and course of the maxillary intraosseous vascular canal with relation to sinus augmentation procedure: A radiographic study. International Journal of Oral and Maxillofacial Surgery 2007, 36, 735–738. [Google Scholar] [CrossRef] [PubMed]
- Hakiem Tawfieq, A.; Ali Hasan, H.; Abd Alrazaq Hassan, M.; Salah Khlfi, M. Localization of the position of vital anatomical structures in the lateral wall of maxillary sinus during different surgical intervention using cone beam computed tomography. Diyala Journal of Medicine 2023, 25, 61–71. [Google Scholar] [CrossRef]
- Al-Mahalawy, H.; Al-Aithan, H.; Al-Kari, B.; Al-Jandan, B.; Shujaat, S. Determination of the position of mental foramen and frequency of anterior loop in Saudi population. A retrospective CBCT study. The Saudi Dental Journal 2017, 29, 29–35. [Google Scholar] [CrossRef]
- Fishel, D.; Buchner, A.; Hershkowith, A.; Kaffe, I. Roentgenologic study of the mental foramen. Oral Surgery, Oral Medicine, Oral Pathology 1976, 41, 682–686. [Google Scholar] [CrossRef]
- Juodzbalys, G.; Wang, H.-L.; Sabalys, G. (2010). Anatomy of Mandibular Vital Structures. Part I: Mandibular Canal and Inferior Alveolar Neurovascular Bundle in Relation with Dental Implantology. Journal of Oral and Maxillofacial Research, 1. [CrossRef]
- Parnia, F.; Moslehifard, E.; Hafezeqoran, A.; Mahboub, F.; Mojaver-Kahnamoui, H. (2012). Characteristics of anatomical landmarks in the mandibular interforaminal region: A cone-beam computed tomography study. Medicina Oral Patología Oral y Cirugia Bucal, e420–e425. [CrossRef]
- Vásquez, C.A.P. (2019). Tesis para optar el título de Especialista en Radiología Bucal y Maxilofacial.
- Hidalgo, R.; Alejandro; San Pedro, V. ; Jaime. Relación del Foramen Lingual con Espinas Mentonianas y Evaluación del Conducto Lingual Mediante Radiografías Periapicales y Extraorales. International journal of odontostomatology 2010, 4, 295–302. [Google Scholar] [CrossRef]
- Pérez-Vásquez, A.; Vilma, R. CARACTERIZACIÓN DEL FORAMEN LINGUAL MANDIBULAR MEDIANTE TOMOGRAFÍA COMPUTARIZADA DE HAZ CÓNICO. Odontología Activa Revista Científica 2019, 4, 1–8. [Google Scholar] [CrossRef]
- Okumuş, Ö.; Dumlu, A. Prevalence of bifid mandibular canal according to gender, type and side. Journal of Dental Sciences 2019, 14, 126–133. [Google Scholar] [CrossRef] [PubMed]
- Vendruscolo, F.S.; Alegre, P. (2013). VARIAÇÕES NA ANATOMIA DA MANDÍBULA: BIFURCAÇÃO DO CANAL MANDIBULAR E DO DEFEITO ÓSSEO DE STAFNE.
- Hsu, J.-T.; Huang, H.-L.; Fuh, L.-J.; Li, R.-W.; Wu, J.; Tsai, M.-T.; Shen, Y.-W.; Tu, M.-G. Location of the Mandibular Canal and Thickness of the Occlusal Cortical Bone at Dental Implant Sites in the Lower Second Premolar and First Molar. Computational and Mathematical Methods in Medicine 2013, 2013, 1–8. [Google Scholar] [CrossRef]
- Chavarry, N.G.M. Dental implants placed buccally to the mandibular canal in molar regions with severe vertical bone loss: Case reports. Rio de Janeiro Dental Journal (Revista Científica Do CRO-RJ) 2019, 4, 107–113. [Google Scholar] [CrossRef]
- Angelopoulos, C.; Aghaloo, T. Imaging Technology in Implant Diagnosis. Dental Clinics of North America 2011, 55, 141–158. [Google Scholar] [CrossRef]
- Silva, I.M.D.C.C.; Freitas, D.Q.D.; Ambrosano, G.M.B.; Bóscolo, F.N.; Almeida, S.M. Bone density: Comparative evaluation of Hounsfield units in multislice and cone-beam computed tomography. Brazilian Oral Research 2012, 26, 550–556. [Google Scholar] [CrossRef] [PubMed]
- Chugh, T.; Jain, A.K.; Jaiswal, R.K.; Mehrotra, P.; Mehrotra, R. Bone density and its importance in orthodontics. Journal of Oral Biology and Craniofacial Research 2013, 3, 92–97. [Google Scholar] [CrossRef] [PubMed]
- Cassetta, M.; Stefanelli, L.V.; Pacifici, A.; Pacifici, L.; Barbato, E. How Accurate Is CBCT in Measuring Bone Density? A Comparative CBCT-CT In Vitro Study. Clinical Implant Dentistry and Related Research 2014, 16, 471–478. [Google Scholar] [CrossRef] [PubMed]
- Köseoğlu Seçgin, C.; Karslıoğlu, H. ; Özemre, Mö.; Orhan, K. (2021). Gray value measurement for the evaluation of local alveolar bone density around impacted maxillary canine teeth using cone beam computed tomography. Medicina Oral Patología Oral y Cirugia Bucal, e669–e675. [CrossRef]
- Genç, T.; Duruel, O.; Kutlu, H.; Dursun, E.; Karabulut, E.; Tözüm, T. Evaluation of anatomical structures and variations in the maxilla and the mandible before dental implant treatment. Dental and Medical Problems 2018, 55, 233–240. [Google Scholar] [CrossRef]
- Javed, F.; Romanos, G.E. Impact of Diabetes Mellitus and Glycemic Control on the Osseointegration of Dental Implants: A Systematic Literature Review. Journal of Periodontology 2009, 80, 1719–1730. [Google Scholar] [CrossRef]
- Madrid, C.; Sanz, M. (2009). What impact do systemically administrated bisphosphonates have on oral implant therapy? A systematic review. Clinical Oral Implants Research, 20, 87–95. [CrossRef]
- Ismail, A.; Shaddox, L.; Santamaria, M.; Sabbagh, M. (2022). Peri-implantitis: A Review to Simplify a Mystifying Disease. Medical Research Archives, 10. [CrossRef]
- Esau, T.; Puryer, J.; McNally, L.; O’Sullivan, D. Patient understanding and recall of risks and complications of dental implant treatment following informed consent. Faculty Dental Journal 2016, 7, 16–21. [Google Scholar] [CrossRef]
- Khongkhunthian, P.; Jomjunyong, K.; Reichart, A.P. Accuracy of Cone Beam Computed Tomography for Dental Implant Treatment Planning. Chiang Mai University Journal of Natural Sciences 2017, 16. [Google Scholar] [CrossRef]
- Jacobs, R.; Salmon, B.; Codari, M.; Hassan, B.; Bornstein, M.M. Cone beam computed tomography in implant dentistry: Recommendations for clinical use. BMC Oral Health 2018, 18, 88. [Google Scholar] [CrossRef]
- Oh, T.; Yoon, J.; Misch, C.E.; Wang, H. The Causes of Early Implant Bone Loss: Myth or Science? Journal of Periodontology 2002, 73, 322–333. [Google Scholar] [CrossRef]
- Arai, Y.; Takashima, M.; Matsuzaki, N.; Takada, S. (2024). Marginal bone loss in dental implants: A literature review of risk factors and treatment strategies for prevention. Journal of Prosthodontic Research, JPR_D_23_00223. [CrossRef]
- Song, D.; Shujaat, S.; De Faria Vasconcelos, K.; Huang, Y.; Politis, C.; Lambrichts, I.; Jacobs, R. Diagnostic accuracy of CBCT versus intraoral imaging for assessment of peri-implant bone defects. BMC Medical Imaging 2021, 21, 23. [Google Scholar] [CrossRef]
- Rydholm, H.; Von Corswant, C.; Denison, H.; Jensen, J.M.; Lehmann, A.; Ruth, M.; Söderlind, E.; Aurell-Holmberg, A. Reducing Adverse Effects During Drug Development: The Example of Lesogaberan and Paresthesia. Clinical Therapeutics 2016, 38, 946–960. [Google Scholar] [CrossRef] [PubMed]
- Esposito, M.; Grusovin, M.G.; Worthington, H.V. (2013). Interventions for replacing missing teeth: Antibiotics at dental implant placement to prevent complications. Cochrane Database of Systematic Reviews, 2019. [CrossRef]
- Hossein, K.; Dahlin, C.; Bengt, A. Influence of Different Prophylactic Antibiotic Regimens on Implant Survival Rate: A Retrospective Clinical Study. Clinical Implant Dentistry and Related Research 2005, 7, 32–35. [Google Scholar] [CrossRef] [PubMed]
- Goodacre, C.J.; Bernal, G.; Rungcharassaeng, K. ; Kan. (2004). Common complications with implants and implant prostheses: What complications are associated with dental implants? Evidence-Based Dentistry, 5, 70–71. [CrossRef]
Figure 1.
- CBCT image in the sagittal plane, showing the different shapes of the nasopalatine canal: cylindrical, fusiform, hourglass and funnel-shaped.[24].
Figure 1.
- CBCT image in the sagittal plane, showing the different shapes of the nasopalatine canal: cylindrical, fusiform, hourglass and funnel-shaped.[24].
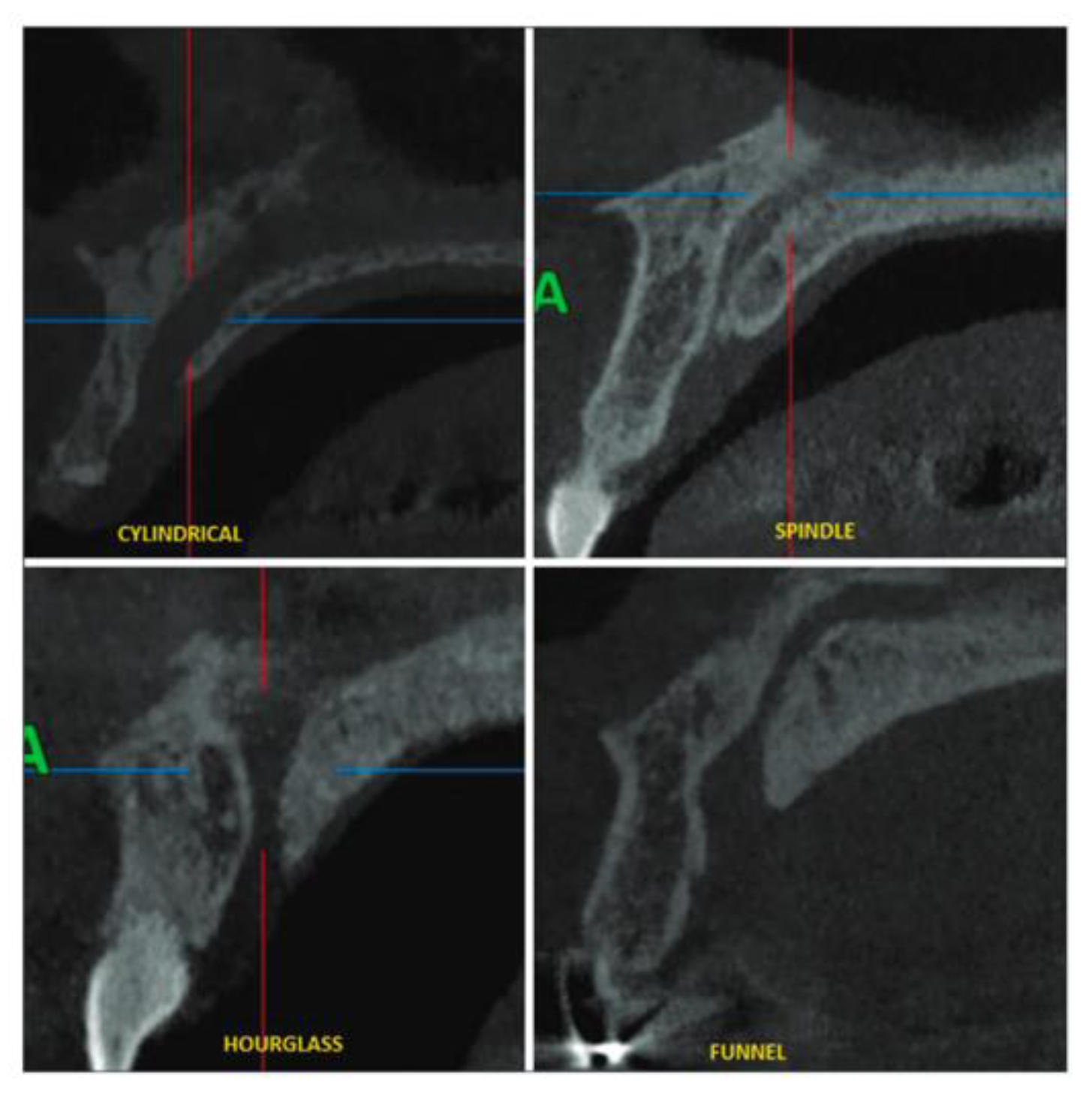
Figure 2.
- Nasal cavities with soft tissue.
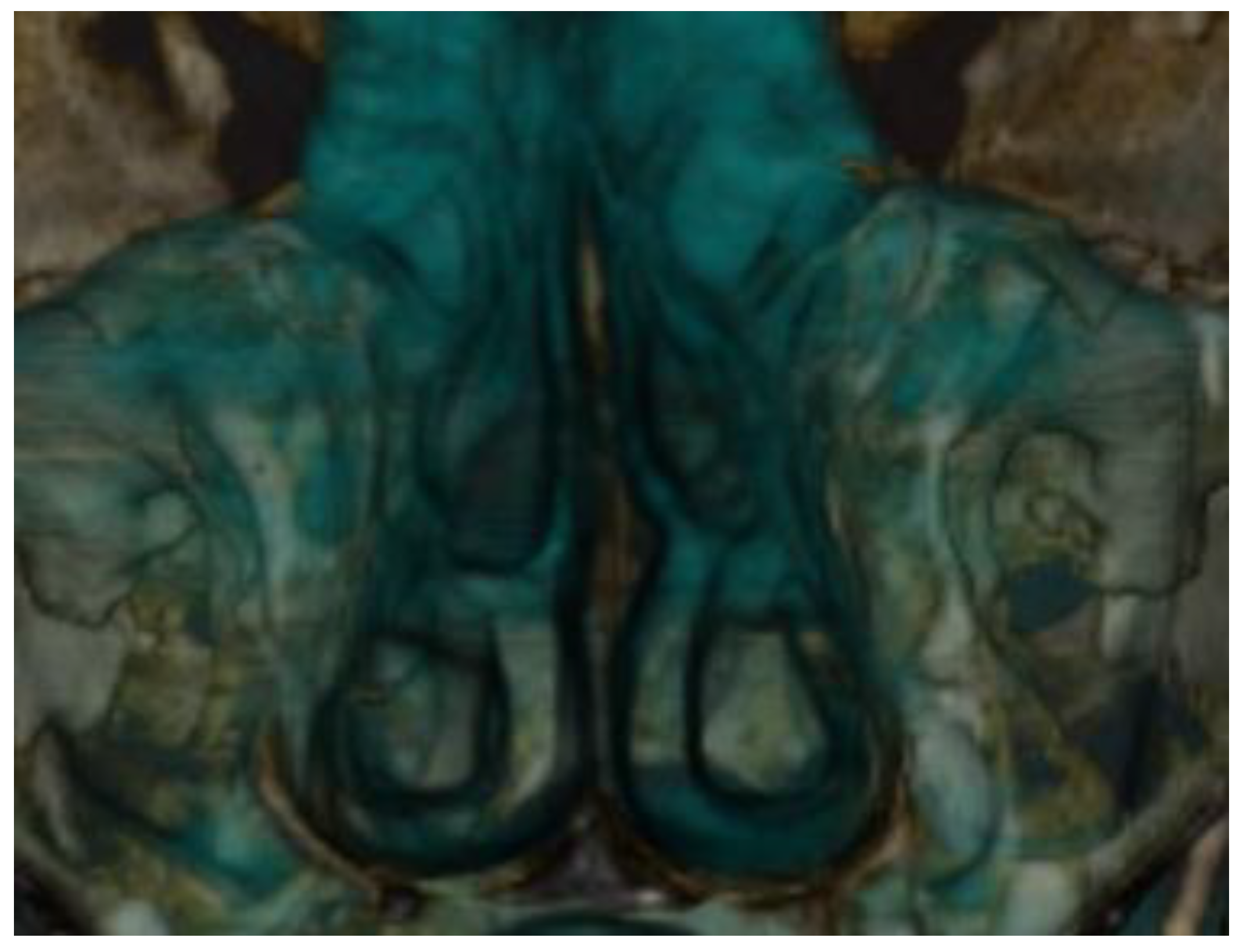
Figure 3.
– Placement with exposure of the implant in the nasal fossa.[31].
Figure 3.
– Placement with exposure of the implant in the nasal fossa.[31].
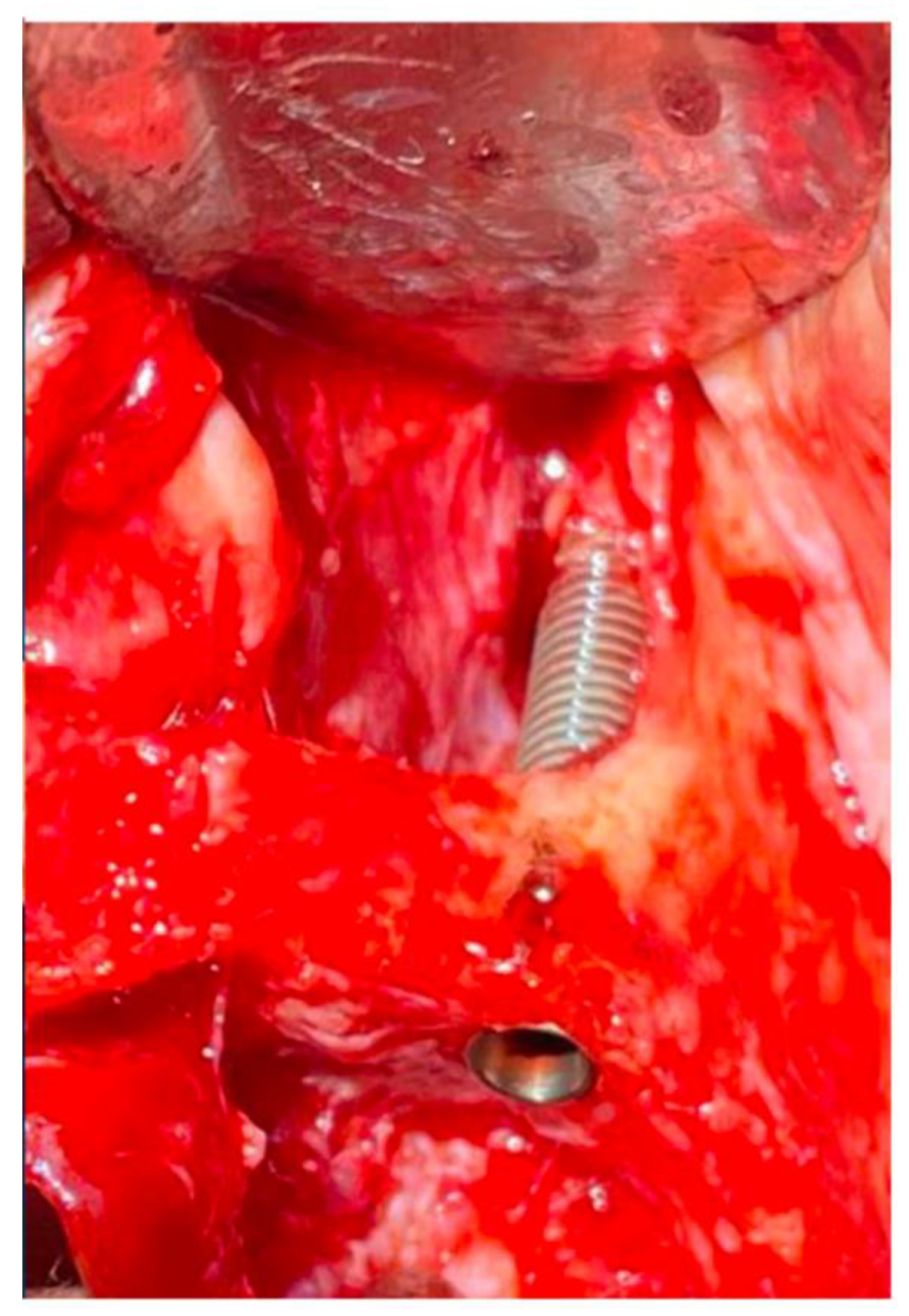
Figure 5.
- Image of an oblique sagittal section showing the relationship between the healthy maxillary sinus and the roots of the posterior teeth.
Figure 5.
- Image of an oblique sagittal section showing the relationship between the healthy maxillary sinus and the roots of the posterior teeth.
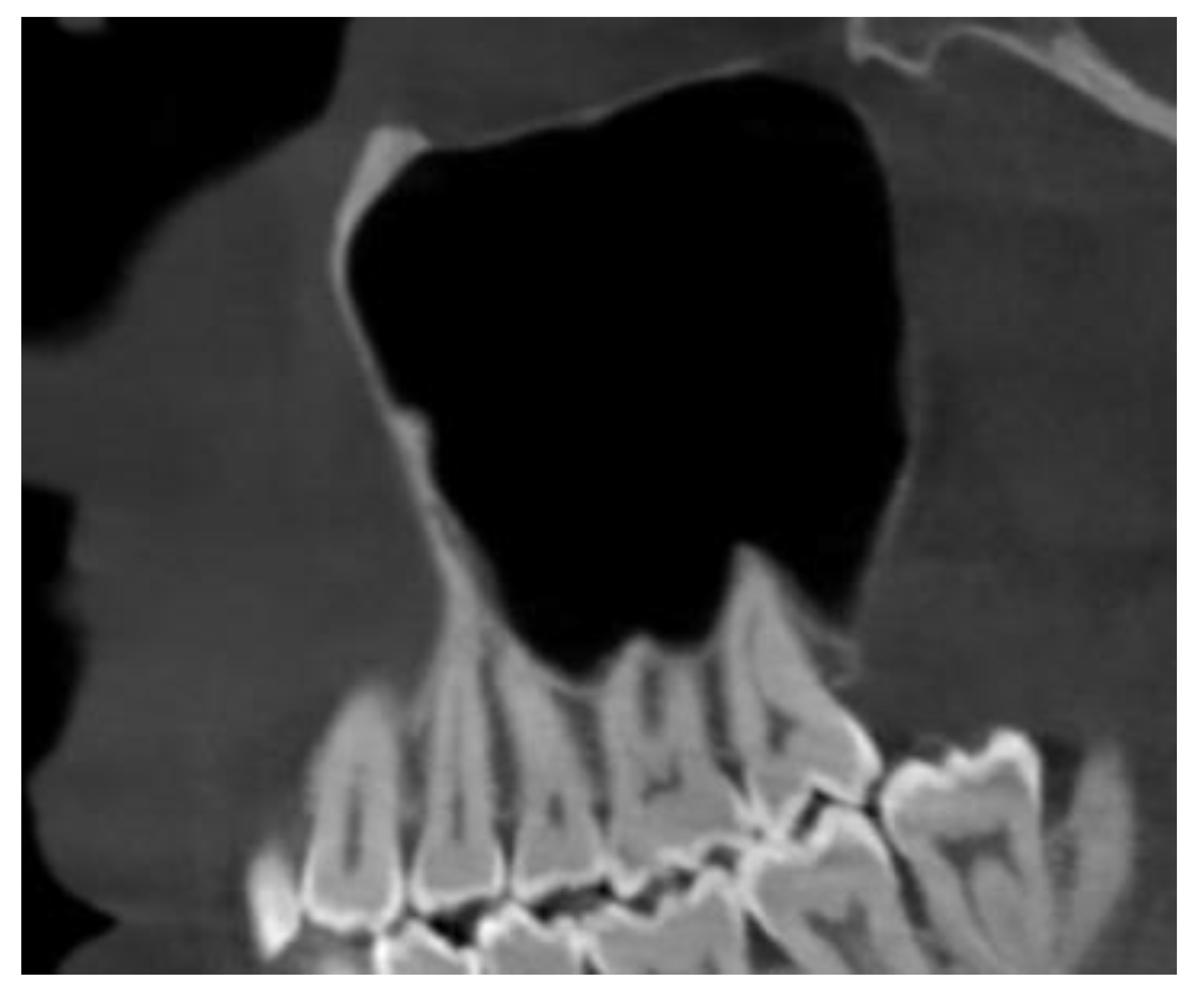
Figure 6.
- Orientation of septa on CBCT: (1) sagittal, (2) coronal, (3) transverse.[49].
Figure 6.
- Orientation of septa on CBCT: (1) sagittal, (2) coronal, (3) transverse.[49].
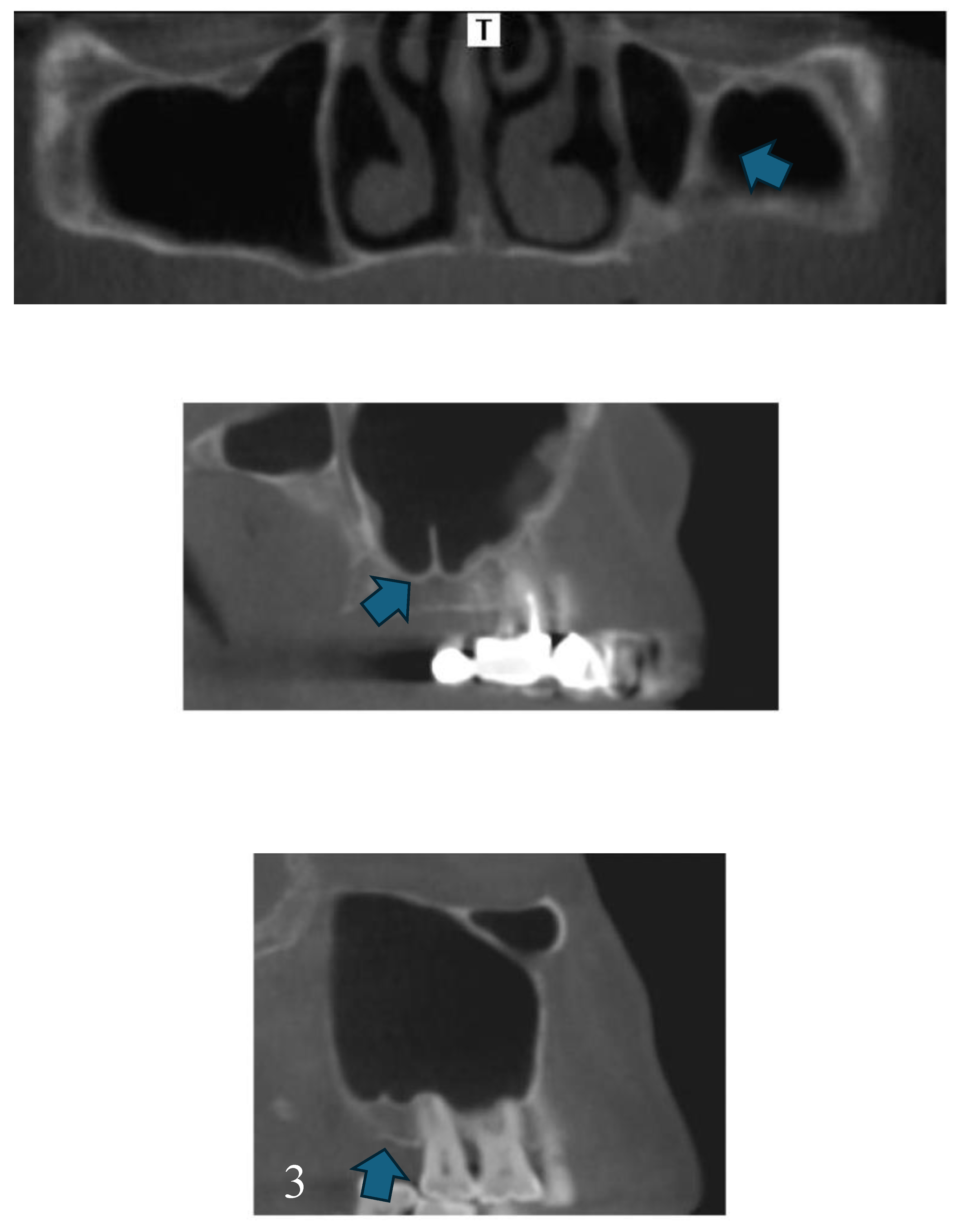
Figure 7.
- Types of PSAA: A- Intrasinusoidal; B- Intraosseous; C- Superficial. [51].
Figure 7.
- Types of PSAA: A- Intrasinusoidal; B- Intraosseous; C- Superficial. [51].
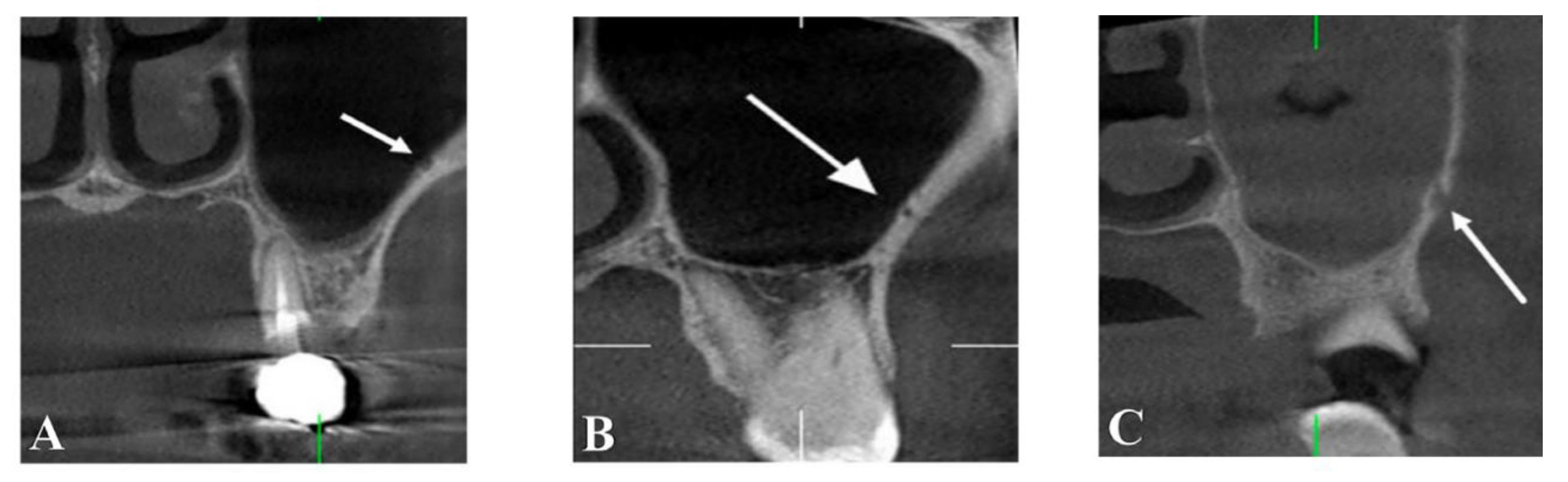
Figure 8.
A) 3D reconstruction of the mentonian hole on the right side; B) 3D reconstruction of the mentonian hole bilaterally.
Figure 8.
A) 3D reconstruction of the mentonian hole on the right side; B) 3D reconstruction of the mentonian hole bilaterally.
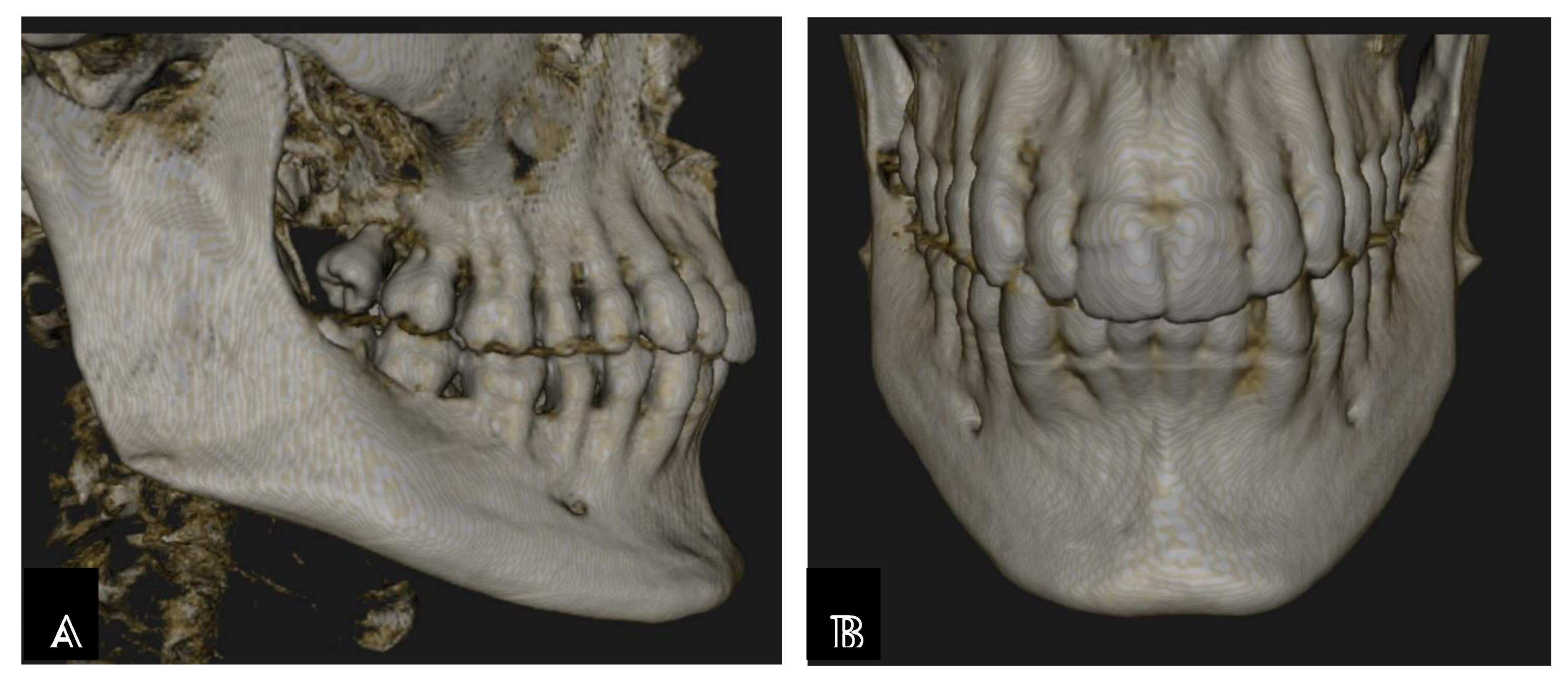
Figure 9.
– a) Implant in contact with the lingual canal; b) Implant not in contact with the lingual canal.[63].
Figure 9.
– a) Implant in contact with the lingual canal; b) Implant not in contact with the lingual canal.[63].
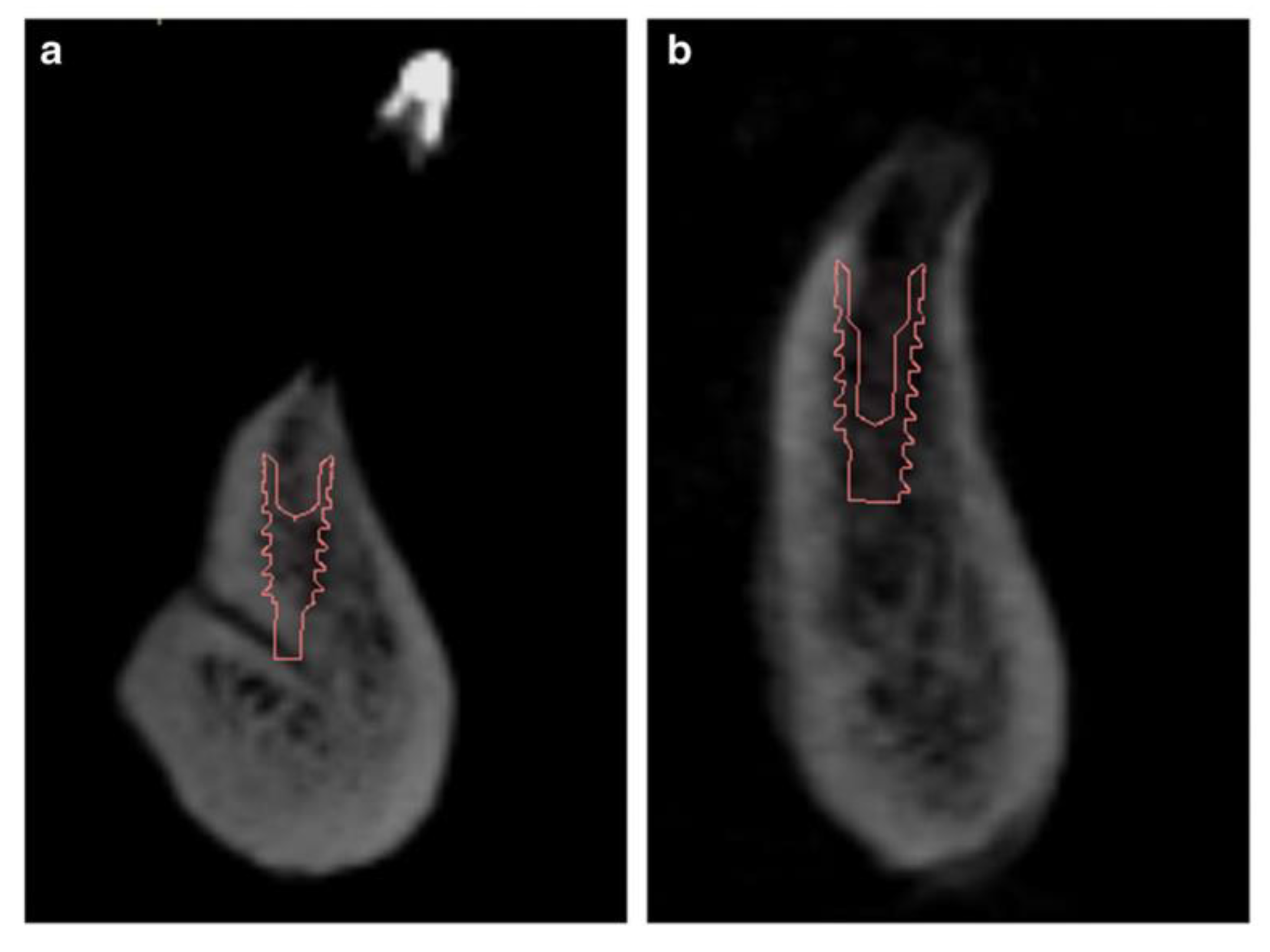
Figure 10.
- Mandibular canal a) 3D reconstruction b) Secundary canals in contact with implants c) Panoramic reconstruction showing bilateral incisal and mandibular canals.
Figure 10.
- Mandibular canal a) 3D reconstruction b) Secundary canals in contact with implants c) Panoramic reconstruction showing bilateral incisal and mandibular canals.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



