
Submitted:
09 October 2024
Posted:
10 October 2024
You are already at the latest version
Abstract
Objectives: This study focused on the presence or absence of vascular invasion and extrahepatic metastasis in hepatocellular carcinoma (HCC) and examined their impact on systemic treatment outcomes. Methods: We retrospectively analyzed 362 patients with unresectable HCC who received first-line systemic therapy. The prognostic evaluation was based on the presence of vascular invasion and extrahepatic metastasis at the time of treatment initiation. Results: Patients with vascular invasion or extrahepatic metastasis (advanced group) had significantly worse outcomes than those without these features (intermediate group), with median survival times of 434 and 658 days, respectively. Further subdivision of the advanced group into three categories—patients with only extrahepatic metastasis (m group, n = 77), patients with only vascular invasion (v group, n = 78), and patients with both vascular invasion and extrahepatic metastasis (vm group, n = 52)—revealed that the m group had significantly better outcomes than those in the other two groups, with median survival times of 649, 323, and 187 days, respectively. A comparison of the clinical backgrounds among the three groups demonstrated that the m group had significantly better liver function at the time of treatment initiation than that in the other two groups. Multivariate analysis, including performance status, Child–Pugh score, and the use of immune checkpoint inhibitors as first-line therapy, identified the m group as an independent and significant prognostic factor (hazard ratio, 0.50). Conclusions: Unresectable HCC with extrahepatic metastasis and no vascular invasion represents a novel staging category for systemic treatment.
Keywords:
advanced hepatocellular carcinoma
; immune checkpoint inhibitor
; vascular invasion
; extrahepatic metastasis
1. Introduction
Primary liver cancer is the sixth most commonly diagnosed cancer and the third leading cause of cancer-related deaths worldwide. Primary liver cancer includes hepatocellular carcinoma (HCC), which accounts for 75–85% of cases, and intrahepatic cholangiocarcinoma, which accounts for 10–15%, along with other less common types of liver cancer [1]. HCC arises from hepatocytes and typically develops in the presence of chronic liver conditions such as chronic hepatitis B or C infection, alcohol abuse, or metabolic dysfunction-associated steatotic liver disease [2,3,4,5]. Symptoms of HCC include fatigue, abdominal pain or swelling, unexplained weight loss, and jaundice. However, most patients with HCC exhibit no symptoms in the early stages of the disease. Therefore, regular screening tests such as ultrasonography, computed tomography (CT), magnetic resonance imaging (MRI), and blood tests are essential for individuals with chronic liver disease [6,7]. The treatment of HCC depends on the stage of cancer, liver function, and the patient’s overall health status. Treatment options for early-stage HCC include ablation, resection, radiation, transarterial chemoembolization, and liver transplantation. However, the treatment options for advanced-stage HCC are generally limited to systemic therapy [8,9,10].
Advances in systemic treatment have resulted in significant changes in the treatment outcomes of unresectable HCC [11,12,13]. With the advent of immune checkpoint inhibitors and other tyrosine kinase inhibitors, multiple drug treatments have become available, and the indications for each are rapidly evolving [14,15,16,17,18,19]. The Barcelona Clinic Liver Cancer (BCLC) staging system is widely used as a treatment guideline for HCC [20]. In this classification, advanced HCC (BCLC-C) is defined as "patients presenting with vascular invasion or extrahepatic spread who are still relatively fit," with an expected survival period of about 2 years. However, in clinical practice, the prognosis of advanced HCC varies significantly. At the same time, some patients live well beyond 2 years, while many have a prognosis of less than 6 months [21,22,23]. Therefore, a precise subclassification of advanced HCC based on treatment outcomes is highly desirable. In this study, we focused on the presence or absence of vascular invasion and extrahepatic spread when initiating systemic treatment. We identified a simple subclassification associated with treatment outcomes.
2. Materials and Methods
2.1. The Study Population
We retrospectively collected clinical data from patients who received first-line systemic treatment between 2011 and 2024 at the Nagoya University Hospital in Aichi, Japan. Baseline characteristics, including age, sex, underlying liver disease, laboratory data, and tumor-specific factors, such as the duration of drug administration, tumor stage based on the BCLC classification, macrovascular and portal vein invasion, and extrahepatic spread, were retrospectively assessed. This study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of Nagoya University Hospital (No. 2021-0247).
2.2. HCC Diagnosis
HCC was primarily diagnosed using hemodynamic imaging techniques, including contrast-enhanced CT, gadolinium ethoxybenzyl diethylenetriamine pentaacetic acid (Gd-EOB-DTPA)-enhanced MRI, and/or contrast-enhanced ultrasonography with perflubutane [24,25,26]. Pathological diagnosis was performed only in inconclusive cases.
2.3. Liver Function Assessment
Liver function was assessed using the Child–Pugh classification and the albumin–bilirubin (ALBI) score. In brief, the ALBI score was calculated based on laboratory data using the following formula: ALBI score = log10 bilirubin (µmol/L) × 0.66 + albumin (g/L) × −0.085 [27].
2.4. Systemic Therapy
Patients received systemic therapy until disease progression was confirmed, unacceptable adverse events occurred, consent was withdrawn, or a physician decided to discontinue the treatment based on the patient's condition and clinical data. Sorafenib was administered until February 2018 [14,15], lenvatinib between March 2018 and October 2020 [16], atezolizumab plus bevacizumab from November 2020 [17,18], and tremelimumab plus durvalumab from January 2023 [19]. However, the choice of agent was also influenced by complications. The systemic therapy regimens were as follows: 400 mg sorafenib orally twice daily, 12 mg lenvatinib daily for patients weighing ≥60 kg, or 8 mg daily for those weighing <60 kg; 1200 mg atezolizumab plus 15 mg/kg bevacizumab intravenously every 3 weeks; and 300 mg tremelimumab intravenously once plus 1500 mg durvalumab intravenously every 4 weeks.
2.5. Assessment of Treatment Effects and Adverse Events
Treatment effects were typically assessed every 2–4 months using contrast-enhanced CT or Gd-EOB-DTPA-enhanced MRI, following the RECIST and mRECIST criteria [28]. Tumor markers, such as alpha-fetoprotein and des-γ-carboxy prothrombin, were also evaluated at each patient visit. Adverse events were graded using the Common Terminology Criteria for Adverse Events version 5.0 [29]. Drugs were discontinued or interrupted according to the manufacturer’s instructions.
2.6. Statistical Analysis
Categorical variables, described as numbers, were compared using the chi-square test, and continuous variables, described as means (minimum to maximum), were compared using a one-way analysis of variance. Multiple comparisons were performed using Tukey's multiple comparison test. Overall survival (OS) was analyzed using the Kaplan–Meier method and compared using the log-rank test. Cox proportional hazard models were used to estimate hazard ratios and 95% confidence intervals (CIs). For all tests, statistical significance was set at P < 0.05. GraphPad Prism 9 (GraphPad Software, San Diego, CA, USA), R (version 4.1.2, R Foundation for Statistical Computing, Vienna, Austria; http://www.R-project.org/), and EZR (Saitama Medical Center, Jichi Medical University, Saitama, Japan), a graphical user interface for R, were used for the statistical analyses [30].
3. Results
Approximately, 362 patients with HCC who received first-line systemic therapy were enrolled during the study period. The breakdown of first-line treatments was as follows: sorafenib, 207 cases; lenvatinib, 72 cases; atezolizumab plus bevacizumab, 75 cases; and durvalumab plus tremelimumab, eight cases. By applying the “current” BCLC classification, 207 patients with either vascular invasion or extrahepatic metastasis (advanced group) had significantly worse prognoses than the prognosis of 155 patients without these features (intermediate group), with a median survival of 434 days vs. 658 days (Figure 1a).
Further classification of the advanced group into three subgroups—77 patients with only extrahepatic metastasis (m group), 78 patients with only vascular invasion (v group), and 52 patients with both vascular invasion and extrahepatic metastasis (vm group)—demonstrated that the m group had a significantly better prognosis than the other two groups, with a median survival time of 649 days in the m group, 323 days in the v group, and 187 days in the vm group (Figure 1b). Even among patients with a Child-Pugh score of A for liver function at the initiation of systemic therapy, those in the m group had a significantly better prognosis than those in the other two groups (Figure 1c). These results reveal distinct subgroups of advanced HCC, potentially indicating different prognoses in response to first-line systemic treatments.
A comparison of the clinical backgrounds of the three groups revealed that the m group had significantly better liver function at the time of treatment initiation than the function in the other two groups (Table 1). In addition, intrahepatic lesions were substantially larger in the v group than in the m group. Although no significant differences in progression-free survival among the three groups were observed, the time to treatment failure was significantly longer in the m group than in the other two groups, suggesting better treatment tolerance in the m group (Table 1).
m group, patients with only extrahepatic metastasis; v group, patients with only vascular invasion; vm group, patients with both vascular invasion and extrahepatic metastasis; PS, performance status; SOR, sorafenib; LEN, lenvatinib; AB, atezolizumab DT, durvalumab–tremelimumab PFS, progression-free survival; TTF, time to treatment failure; AFP, alpha-fetoprotein; DCP, des-gamma-carboxy prothrombin; PT-INR, prothrombin time-international normalized ratio; T-bil, total-bilirubin
In a study of 207 patients who received first-line systemic treatment for advanced HCC, those treated with atezolizumab plus bevacizumab had a significantly improved prognosis (Figure 2a). However, in the m group, no significant difference was noted in the prognosis based on the type of initial systemic treatment (Figure 2b). Notably, atezolizumab plus bevacizumab treatment demonstrated significantly better outcomes in the v and vm groups than other systemic treatments (Figure 2c). These results suggest that the improved prognosis following atezolizumab plus bevacizumab treatment in advanced HCC is primarily attributable to the effects of the drugs on the vm and vm groups.
In the univariate analysis of factors associated with survival, the m group, performance status, Child–Pugh score, and initial treatment with immune checkpoint inhibitors were identified as significant (Table 2). In multivariate analysis, which included these factors, the m group was identified as an independent and significant factor (hazard ratio 0.50, Table 2). Taken together, patients with advanced HCC with only extrahepatic metastases represent a distinct subgroup in terms of prognosis after first-line systemic treatment.
4. Discussion
We focused on the presence or absence of vascular invasion and extrahepatic metastasis at the time of first-line systemic therapy for HCC. We identified that the prognosis could be broadly categorized into three groups. Among these, patients with extrahepatic metastasis but no vascular invasion (group m) had a better prognosis after the introduction of systemic therapy than those in the other two groups. Applying this simple sub-classification at the start of systemic therapy can help guide appropriate treatment decisions.
The prognosis of HCC is significantly influenced not only by the stage of the cancer but also by liver function, performance status, and comorbidities, making individual patient evaluation essential. The BCLC system is commonly used to stage HCC, and each stage provides a general prognostic prediction [20]. For cases classified as BCLC-C with vascular invasion or extrahepatic metastasis, the expected survival time is approximately 2 years, and systemic therapy is recommended. Despite recent advancements in systemic therapy for HCC, leading to trends in prolonged OS, the prognosis for HCC cases classified as BCLC-C varies widely, with many cases having a survival time of less than 6 months [21,22,23].
Recently, new subclassifications such as the Bolondi classification and Kinki criteria have been proposed and widely applied in clinical practice for HCC cases classified as BCLC-B (intermediate HCC) [31,32]. However, investigations into the subclassification of BCLC-C cases are limited. Based on our results, we propose a new subclassification for predicting the prognosis of advanced HCC when introducing systemic therapy, focusing on the presence or absence of vascular invasion and extrahepatic metastasis. Owing to the retrospective study design, we could not determine the underlying cause of the improved prognosis in the m group. However, we speculate that the presence of vascular invasion may aggravate liver function, leading to an insufficient relative dose intensity for systemic therapy and/or reduced capacity for subsequent treatments. As this was a single-center, retrospective observational study, further validation in a multicenter setting is necessary. We hope that this proposal contributes to the reclassification of advanced HCC.
5. Conclusions
Advanced HCC with extrahepatic metastases but no vascular invasion represents a new staging category for the initiation of systemic treatments.
Author Contributions
Conceptualization, N.I.; data curation, N.I., T.Y., K.M., K.Y., T.I., Y.I., T.K., T.H., T.I., and H.K.; writing—original draft preparation, N.I.; supervision, K.T., K.H.; statistical analysis, N.I. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the guidelines of the Declaration of Helsinki and approved by the Institutional Ethics Committee of Nagoya University Hospital (protocol code 2021-0247 and September 2021).
Informed Consent Statement
Patient consent was waived due to the use of opt-out consent for this study.
Data Availability Statement
Research data related to this study will be made available upon request.
Acknowledgments
We sincerely thank all participants for sharing their medical information.
Conflicts of Interest
T. Ito: Honoraria from Chugai and AstraZeneca, Research funding from Chugai; T. Kuzuya: Honoraria from Bayer, Chugai, Eisai, and Eli Lilly, Japan. Research funding was provided by Eisai, Kawashima, and honoraria from Takeda.
References
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, Bray F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021 May;71(3):209-249. Epub 2021 Feb 4. [CrossRef] [PubMed]
- Llovet JM, Kelley RK, Villanueva A, Singal AG, Pikarsky E, Roayaie S, Lencioni R, Koike K, Zucman-Rossi J, Finn RS. Hepatocellular carcinoma. Nat Rev Dis Primers. 2021 Jan 21;7(1):6. Erratum in: Nat Rev Dis Primers. 2024 Feb 12;10(1):10. doi: 10.1038/s41572-024-00500-6. [CrossRef] [PubMed]
- Huang DQ, Mathurin P, Cortez-Pinto H, Loomba R. Global epidemiology of alcohol-associated cirrhosis and HCC: trends, projections and risk factors. Nat Rev Gastroenterol Hepatol. 2023 Jan;20(1):37-49. Epub 2022 Oct 18. [CrossRef] [PubMed] [PubMed Central]
- Shah PA, Patil R, Harrison SA. NAFLD-related hepatocellular carcinoma: The growing challenge. Hepatology. 2023 Jan 1;77(1):323-338. Epub 2022 Nov 8. [CrossRef] [PubMed] [PubMed Central]
- Kawamura Y, Arase Y, Ikeda K, Seko Y, Imai N, Hosaka T, Kobayashi M, Saitoh S, Sezaki H, Akuta N, Suzuki F, Suzuki Y, Ohmoto Y, Amakawa K, Tsuji H, Kumada H. Large-scale long-term follow-up study of Japanese patients with non-alcoholic Fatty liver disease for the onset of hepatocellular carcinoma. Am J Gastroenterol. 2012 Feb;107(2):253-61. Epub 2011 Oct 18. [CrossRef] [PubMed]
- Loomba R, Lim JK, Patton H, El-Serag HB. AGA Clinical Practice Update on Screening and Surveillance for Hepatocellular Carcinoma in Patients With Nonalcoholic Fatty Liver Disease: Expert Review. Gastroenterology. 2020 May;158(6):1822-1830. Epub 2020 Jan 30. [CrossRef] [PubMed] [PubMed Central]
- Ioannou, GN. HCC surveillance after SVR in patients with F3/F4 fibrosis. J Hepatol. 2021 Feb;74(2):458-465. Epub 2020 Dec 7. [CrossRef] [PubMed]
- Forner A, Reig M, Bruix J. Hepatocellular carcinoma. Lancet. 2018 Mar 31;391(10127):1301-1314. Epub 2018 Jan 5. [CrossRef] [PubMed]
- Villanueva A. Hepatocellular Carcinoma. N Engl J Med. 2019 Apr 11;380(15):1450-1462. [CrossRef] [PubMed]
- Brown ZJ, Tsilimigras DI, Ruff SM, Mohseni A, Kamel IR, Cloyd JM, Pawlik TM. Management of Hepatocellular Carcinoma: A Review. JAMA Surg. 2023 Apr 1;158(4):410-420. [CrossRef] [PubMed]
- Kudo M. Recent Advances in Systemic Therapy for Hepatocellular Carcinoma in an Aging Society: 2020 Update. Liver Cancer. 2020 Dec;9(6):640-662. Epub 2020 Nov 17. [CrossRef] [PubMed] [PubMed Central]
- Ganesan P, Kulik LM. Hepatocellular Carcinoma: New Developments. Clin Liver Dis. 2023 Feb;27(1):85-102. Epub 2022 Oct 18. [CrossRef] [PubMed]
- Rossari F, Tada T, Suda G, Shimose S, Kudo M, Yoo C, Cheon J, Finkelmeier F, Lim HY, Presa J, Masi G, Bergamo F, Amadeo E, Vitiello F, Kumada T, Sakamoto N, Iwamoto H, Aoki T, Chon HJ, Himmelsbach V, Iavarone M, Cabibbo G, Montes M, Foschi FG, Vivaldi C, Soldà C, Sho T, Niizeki T, Nishida N, Steup C, Hirooka M, Kariyama K, Tani J, Atsukawa M, Takaguchi K, Itobayashi E, Fukunishi S, Tsuji K, Ishikawa T, Tajiri K, Ochi H, Yasuda S, Toyoda H, Ogawa C, Nishimura T, Hatanaka T, Kakizaki S, Shimada N, Kawata K, Hiraoka A, Tada F, Ohama H, Nouso K, Morishita A, Tsutsui A, Nagano T, Itokawa N, Okubo T, Imai M, Kosaka H, Naganuma A, Koizumi Y, Nakamura S, Kaibori M, Iijima H, Hiasa Y, Persano M, Foti S, Camera S, Stefanini B, Scartozzi M, Cascinu S, Casadei-Gardini A, Rimini M. Disease Etiology Impact on Outcomes of Hepatocellular Carcinoma Patients Treated with Atezolizumab plus Bevacizumab: A Real-World, Multicenter Study. Liver Cancer. 2024 Apr 10;13(5):522-536. [CrossRef] [PubMed] [PubMed Central]
- Llovet JM, Ricci S, Mazzaferro V, Hilgard P, Gane E, Blanc JF, de Oliveira AC, Santoro A, Raoul JL, Forner A, Schwartz M, Porta C, Zeuzem S, Bolondi L, Greten TF, Galle PR, Seitz JF, Borbath I, Häussinger D, Giannaris T, Shan M, Moscovici M, Voliotis D, Bruix J; SHARP Investigators Study Group. Sorafenib in advanced hepatocellular carcinoma. N Engl J Med. 2008 Jul 24;359(4):378-90. [CrossRef] [PubMed]
- Cheng AL, Kang YK, Chen Z, Tsao CJ, Qin S, Kim JS, Luo R, Feng J, Ye S, Yang TS, Xu J, Sun Y, Liang H, Liu J, Wang J, Tak WY, Pan H, Burock K, Zou J, Voliotis D, Guan Z. Efficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: a phase III randomised, double-blind, placebo-controlled trial. Lancet Oncol. 2009 Jan;10(1):25-34. Epub 2008 Dec 16. [CrossRef] [PubMed]
- Kudo M, Finn RS, Qin S, Han KH, Ikeda K, Piscaglia F, Baron A, Park JW, Han G, Jassem J, Blanc JF, Vogel A, Komov D, Evans TRJ, Lopez C, Dutcus C, Guo M, Saito K, Kraljevic S, Tamai T, Ren M, Cheng AL. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: a randomised phase 3 non-inferiority trial. Lancet. 2018 Mar 24;391(10126):1163-1173. [CrossRef] [PubMed]
- Finn RS, Qin S, Ikeda M, Galle PR, Ducreux M, Kim TY, Kudo M, Breder V, Merle P, Kaseb AO, Li D, Verret W, Xu DZ, Hernandez S, Liu J, Huang C, Mulla S, Wang Y, Lim HY, Zhu AX, Cheng AL; IMbrave150 Investigators. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N Engl J Med. 2020 May 14;382(20):1894-1905. [CrossRef] [PubMed]
- Cheng AL, Qin S, Ikeda M, Galle PR, Ducreux M, Kim TY, Lim HY, Kudo M, Breder V, Merle P, Kaseb AO, Li D, Verret W, Ma N, Nicholas A, Wang Y, Li L, Zhu AX, Finn RS. Updated efficacy and safety data from IMbrave150: Atezolizumab plus bevacizumab vs. sorafenib for unresectable hepatocellular carcinoma. J Hepatol. 2022 Apr;76(4):862-873. Epub 2021 Dec 11. [CrossRef] [PubMed]
- Abou-Alfa GK, Lau G, Kudo M, Chan SL, Kelley RK, Furuse J, Sukeepaisarnjaroen W, Kang YK, Van Dao T, De Toni EN, Rimassa L, Breder V, Vasilyev A, Heurgué A, Tam VC, Mody K, Thungappa SC, Ostapenko Y, Yau T, Azevedo S, Varela M, Cheng AL, Qin S, Galle PR, Ali S, Marcovitz M, Makowsky M, He P, Kurland JF, Negro A, Sangro B. Tremelimumab plus Durvalumab in Unresectable Hepatocellular Carcinoma. NEJM Evid. 2022 Aug;1(8):EVIDoa2100070. Epub 2022 Jun 6. [CrossRef] [PubMed]
- Reig M, Forner A, Rimola J, Ferrer-Fàbrega J, Burrel M, Garcia-Criado Á, Kelley RK, Galle PR, Mazzaferro V, Salem R, Sangro B, Singal AG, Vogel A, Fuster J, Ayuso C, Bruix J. BCLC strategy for prognosis prediction and treatment recommendation: The 2022 update. J Hepatol. 2022 Mar;76(3):681-693. Epub 2021 Nov 19. [CrossRef] [PubMed] [PubMed Central]
- Mizuno K, Imai N, Yamamoto T, Yokoyama S, Yamamoto K, Ito T, Ishizu Y, Honda T, Kuzuya T, Ishigami M, Kawashima H. Pretreatment Proteinuria Predicts the Prognosis of Patients Receiving Systemic Therapy for Unresectable Hepatocellular Carcinoma. Cancers (Basel). 2023 May 21;15(10):2853. [CrossRef] [PubMed] [PubMed Central]
- Kuzuya T, Ishigami M, Ito T, Ishizu Y, Honda T, Ishikawa T, Fujishiro M. Sorafenib vs. Lenvatinib as First-line Therapy for Advanced Hepatocellular Carcinoma With Portal Vein Tumor Thrombosis. Anticancer Res. 2020 Apr;40(4):2283-2290. [CrossRef] [PubMed]
- Yamamoto T, Imai N, Kuzuya T, Yokoyama S, Yamamoto K, Ito T, Ishizu Y, Honda T, Ishigami M. Changes in Body Composition Predict the Time to Treatment Failure of Lenvatinib in Patients with Advanced Hepatocellular Carcinoma: A Pilot Retrospective Study. Nutr Cancer. 2022;74(9):3118-3127. Epub 2022 Mar 12. [CrossRef] [PubMed]
- Shah A, Tang A, Santillan C, Sirlin C. Cirrhotic liver: What's that nodule? The LI-RADS approach. J Magn Reson Imaging. 2016 Feb;43(2):281-94. Epub 2015 May 21. [CrossRef] [PubMed]
- Terzi E, Giamperoli A, Iavarone M, Leoni S, De Bonis L, Granito A, Forgione A, Tovoli F, Piscaglia F. Prognosis of Single Early-Stage Hepatocellular Carcinoma (HCC) with CEUS Inconclusive Imaging (LI-RADS LR-3 and LR-4) Is No Better than Typical HCC (LR-5). Cancers (Basel). 2022 Jan 11;14(2):336. [CrossRef] [PubMed] [PubMed Central]
- Cai WJ, Ying M, Zheng RQ, Liao J, Luo B, Tang L, Cheng W, Yang H, Wei A, Yang Y, Wang H, Luo YC, Liu C, Zhong H, Yang Q, Yu J, Liang P. Contrast-Enhanced Ultrasound Liver Imaging Reporting and Data System in Hepatocellular Carcinoma ≤5 cm: Biological Characteristics and Patient Outcomes. Liver Cancer. 2023 Jan 24;12(4):356-371. [CrossRef] [PubMed] [PubMed Central]
- Hiraoka A, Michitaka K, Kumada T, Izumi N, Kadoya M, Kokudo N, Kubo S, Matsuyama Y, Nakashima O, Sakamoto M, Takayama T, Kokudo T, Kashiwabara K, Kudo M. Validation and Potential of Albumin-Bilirubin Grade and Prognostication in a Nationwide Survey of 46,681 Hepatocellular Carcinoma Patients in Japan: The Need for a More Detailed Evaluation of Hepatic Function. Liver Cancer. 2017 Nov;6(4):325-336. Epub 2017 Sep 22. [CrossRef] [PubMed] [PubMed Central]
- Eisenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sargent D, Ford R, Dancey J, Arbuck S, Gwyther S, Mooney M, Rubinstein L, Shankar L, Dodd L, Kaplan R, Lacombe D, Verweij J. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009 Jan;45(2):228-47. [CrossRef] [PubMed]
- US Department of Health and Human Services. Common Terminology Criteria for Adverse Events (CTCAE) US Department of Health and Human Services; Washington, DC, USA: 2017. Version 5.0.
- Kanda, Y. Investigation of the freely available easy-to-use software 'EZR' for medical statistics. Bone Marrow Transplant. 2013 Mar;48(3):452-8. Epub 2012 Dec 3. [CrossRef] [PubMed] [PubMed Central]
- Bolondi L, Burroughs A, Dufour JF, Galle PR, Mazzaferro V, Piscaglia F, Raoul JL, Sangro B. Heterogeneity of patients with intermediate (BCLC B) Hepatocellular Carcinoma: proposal for a subclassification to facilitate treatment decisions. Semin Liver Dis. 2012 Nov;32(4):348-59. Epub 2013 Feb 8. [CrossRef] [PubMed]
- Kudo M, Arizumi T, Ueshima K, Sakurai T, Kitano M, Nishida N. Subclassification of BCLC B Stage Hepatocellular Carcinoma and Treatment Strategies: Proposal of Modified Bolondi's Subclassification (Kinki Criteria). Dig Dis. 2015 Oct;33(6):751-8. Epub 2015 Oct 21. [CrossRef] [PubMed]
Figure 1.
Comparison of the current and proposed classifications for advanced hepatocellular carcinoma undergoing systemic treatment. After first-line systemic treatment, overall survival (OS) was analyzed using the Kaplan–Meier method and compared using the log-rank test. Figure 1a illustrates the comparison of OS between the 207 patients with vascular invasion or extrahepatic metastasis (advanced group) and 155 patients without these features (intermediate group). Figure 1b presents an OS comparison based on the proposed classification as follows: 77 patients with extrahepatic metastasis only (m group), 78 patients with vascular invasion only (v group), and 52 patients with both vascular invasion and extrahepatic metastasis (vm group). Figure 1c compares OS among patients with a Child–Pugh score of A across the three groups.
Figure 1.
Comparison of the current and proposed classifications for advanced hepatocellular carcinoma undergoing systemic treatment. After first-line systemic treatment, overall survival (OS) was analyzed using the Kaplan–Meier method and compared using the log-rank test. Figure 1a illustrates the comparison of OS between the 207 patients with vascular invasion or extrahepatic metastasis (advanced group) and 155 patients without these features (intermediate group). Figure 1b presents an OS comparison based on the proposed classification as follows: 77 patients with extrahepatic metastasis only (m group), 78 patients with vascular invasion only (v group), and 52 patients with both vascular invasion and extrahepatic metastasis (vm group). Figure 1c compares OS among patients with a Child–Pugh score of A across the three groups.
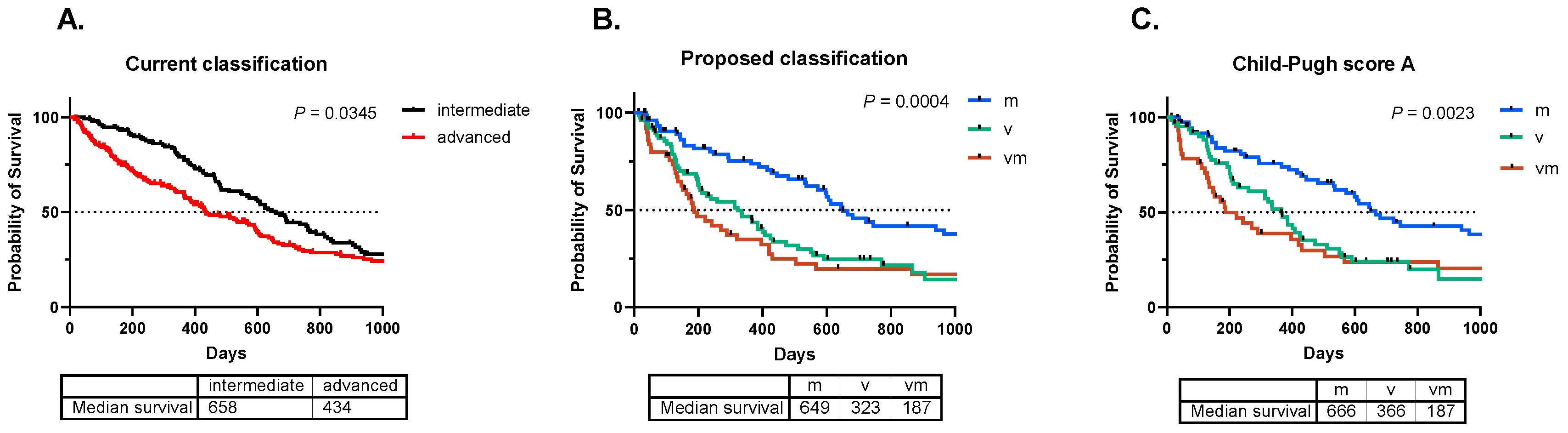
Figure 2.
Comparison of initial systemic treatment regimens for advanced hepatocellular carcinoma. Overall survival (OS) following first-line systemic treatment among 207 patients with either vascular invasion or extrahepatic metastasis (advanced group) was analyzed using the Kaplan–Meier method and compared using the log-rank test. Figure 2a displays the OS comparison between 126 patients treated with sorafenib, 35 patients treated with lenvatinib, 40 patients treated with atezolizumab plus bevacizumab, and six patients treated with durvalumab plus tremelimumab. Figure 2b illustrates the OS comparison based on the initial systemic treatment among the 77 patients with only extrahepatic metastasis (m group). Figure 2c illustrates the OS comparison based on the initial systemic treatment among 78 patients with only vascular invasion (v group) and 52 patients with both vascular invasion and extrahepatic metastasis (vm group).
Figure 2.
Comparison of initial systemic treatment regimens for advanced hepatocellular carcinoma. Overall survival (OS) following first-line systemic treatment among 207 patients with either vascular invasion or extrahepatic metastasis (advanced group) was analyzed using the Kaplan–Meier method and compared using the log-rank test. Figure 2a displays the OS comparison between 126 patients treated with sorafenib, 35 patients treated with lenvatinib, 40 patients treated with atezolizumab plus bevacizumab, and six patients treated with durvalumab plus tremelimumab. Figure 2b illustrates the OS comparison based on the initial systemic treatment among the 77 patients with only extrahepatic metastasis (m group). Figure 2c illustrates the OS comparison based on the initial systemic treatment among 78 patients with only vascular invasion (v group) and 52 patients with both vascular invasion and extrahepatic metastasis (vm group).
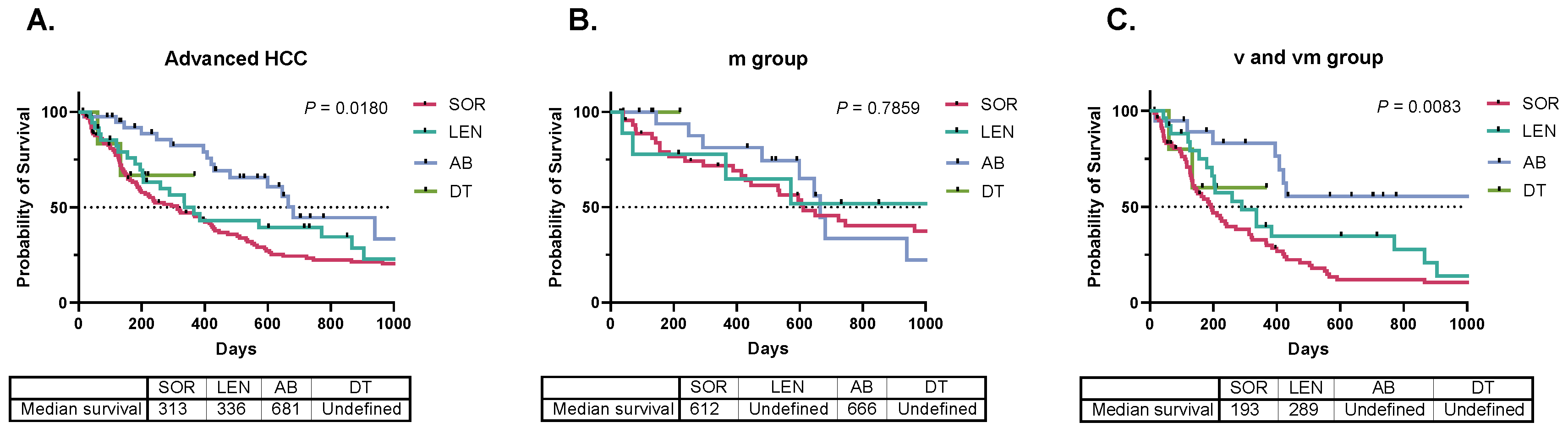

Table 1.
Comparison of patient characteristics across the three groups.
| m | v | vm | |||||
| Number of patients | 77 | 78 | 52 | Chi-square test P value | |||
| Sex (M/F) | 64 / 13 | 62 / 16 | 43 / 9 | 0.5318 | |||
| Etiology (B/C/NBNC) | 17 / 21 /39 | 16 / 22 / 40 | 11 / 16 / 25 | 0.6178 | |||
| PS (0/1/2) | 59 / 17 / 1 | 56 / 19 / 3 | 33 / 18 / 1 | 0.0489 | |||
| Medication (SOR/LEN/AB/DT) | 47 / 9 / 20 / 1 | 44 / 18 / 12 / 4 | 35 / 8 / 8 / 1 | 0.0032 | |||
| Turkey's test P value | |||||||
| one-way ANOVA P value | m vs. v | m vs. vm | v vs. vm | ||||
| Age (year) | 72 (34 - 91) | 69 (40 - 92) | 67 (37 - 87) | 0.1654 | - | - | - |
| PFS (day) | 117 (13 - 2704) | 95 (14 - 2129) | 56 (7 - 966) | 0.0503 | - | - | - |
| TTF (day) | 216 (4 - 4071) | 119 (6 - 1146) | 88 (7 - 2370) | 0.0024 | 0.0067 | 0.0108 | 0.9850 |
| AFP (U/mL) | 22 (1 - 382175) | 289 (2 - 656984) | 1413 (2 - 3610200) | 0.1088 | - | - | - |
| DCP (mAU/mL) | 160 (0 - 603470) | 2392 (0 - 500000) | 1431 (10 - 490380) | 0.1410 | - | - | - |
| PT-INR (ratio) | 1.05 (0.91 - 1.33) | 1.08 (0.93 - 1.57) | 1.08 (0.96 - 1.31) | 0.1361 | - | - | - |
| T-bil (mg/dL) | 0.7 (0.4 - 1.6) | 0.9 (0.3 - 5.1) | 0.9 (0.4 - 4.3) | 0.0485 | 0.0529 | 0.0079 | 0.6243 |
| Alb (g/dL) | 3.8 (2.6 - 4.8) | 3.5 (2.2 - 4.4) | 3.6 (2.4 - 4.5) | 0.0040 | 0.0048 | 0.0449 | 0.8924 |
| ALBI | -2.42 (-3.24 - -1.51) | -2.20 (-2.93 - -1.16) | -2.21 (-3.21 - -1.15) | 0.0004 | 0.0009 | 0.0060 | 0.9789 |
| CPS | 5 (5 - 7) | 6 (5 - 8) | 6 (5 - 9) | 0.0030 | 0.0076 | 0.0140 | 0.9940 |
| HCC size (mm) | 23 (0 - 170) | 33 (5 - 182) | 23 (5 - 180) | 0.0075 | 0.0050 | 0.3731 | 0.3006 |
Table 2.
Univariate and multivariate analysis of overall survival following first-line systemic treatment for hepatocellular carcinoma.
Table 2.
Univariate and multivariate analysis of overall survival following first-line systemic treatment for hepatocellular carcinoma.
| Univariate analysis | Multivariate analysis | ||||||
|---|---|---|---|---|---|---|---|
| Parameter | Hazard ratio | 95% CI | P value | Hazard ratio | 95% CI | P value | |
| m group | 0.50 | 0.35 - 0.71 | 0.0001 | 0.50 | 0.34 - 0.74 | 0.0004 | |
| PS | 2.59 | 1.91 - 3.51 | < 0.0001 | 2.05 | 1.46 - 2.88 | < 0.0001 | |
| CPS | 1.56 | 1.28 - 1.90 | < 0.0001 | 1.31 | 1.02 - 1.68 | 0.0294 | |
| ICI | 0.47 | 0.29 - 0.79 | 0.0038 | 0.71 | 0.42 - 1.21 | 0.2133 | |
P-values were calculated using the Cox proportional hazard model. m group, patients with only extrahepatic metastasis; PS, performance status; CPS, Child–Pugh score; ICI, initial treatment with immune checkpoint inhibitors.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



