
Submitted:
09 October 2024
Posted:
10 October 2024
You are already at the latest version
Abstract
The study presents the conceptual development and simulation of a robotic exoskeleton for ankle rehabilitation. The device is designed for ankle rehabilitation in patients with musculoskeletal disorders, injuries, or neurological diseases. The exoskeleton is equipped with three linear electric actuators that provide precise control of joint movements in multiple planes, allowing dorsiflexion and plantar flexion, inversion, and eversion. By utilizing a screw drive, the exoskeleton provides smooth and controlled movements, significantly reducing the risk of re-injury and improving rehabilitation. Simulation of the device and simulation results showed its high compatibility with the biomechanical features of the ankle joint. Virtual testing confirmed that the exoskeleton provides the smooth, controlled movements necessary for effective rehabilitation. Due to its ability to adapt to the individual physical capabilities of the patient, the device can be used in both active and passive forms of movement support. The results of the study demonstrate the potential of the exoskeleton in clinical applications, including its use in rehabilitation centers and at home. Its cost-effectiveness, ease of use, and high accuracy of movement control make this device a promising solution for restoring the functions of the lower extremities in patients with various musculoskeletal disorders.
Keywords:
Exoskeleton
; Rehabilitation
; Ankle joint
; Kinematics
; Linear drives
; Biomechanics
1. Introduction
Increasing life expectancy is one of the most remarkable achievements of humankind. Globally, the number of older persons is growing faster than all other younger age groups. According to the World Health Organization (WHO), by 2030, there will be more older people than children under 10 years of age (1.41 billion and 1.35 billion, respectively). By 2050, the population over 60 years of age will outnumber adolescents and young people aged 10-24 years (2.1 billion and 2.0 billion, respectively). WHO experts predict that in most countries, the share of older people in the total population will increase. In 2017, one in eight people worldwide was over 60 years old. According to forecasts, by 2030, one in six will belong to this age group, and by 2050, one in five [1].
Increasing life expectancy leads to an increase in chronic diseases and disability in the population, which in turn creates new social, economic, and health challenges. These changes highlight the need to develop strategies to maintain health in old age to minimize the negative effects of an aging society. The process of rehabilitation, along with health promotion, disease prevention, treatment, and palliative care, is an important component of comprehensive health coverage. Rehabilitation may become necessary for anyone during their lifetime due to injury, surgery, disease, or age-related loss of functional capacity. It promotes independence not only for older persons but also for children and adults in everyday life, enabling them to participate in educational, vocational, and daily living activities and to fulfill meaningful life roles.
Rehabilitation plays a key role in achieving universal access to health care and is one of the main strategies for achieving the Sustainable Development Goals to ensure healthy lifestyles and well-being for all age groups [2]. Currently, about 2.4 billion people worldwide suffer from diseases that may require rehabilitation interventions. WHO predicts that due to changes in health and demographics, the need for rehabilitation will increase worldwide [3].
Given the increasing number of patients with musculoskeletal disorders, especially among the elderly population, an individualized and precise approach to the rehabilitation process plays a key role. In this case, robotic exoskeletons for lower limb rehabilitation are becoming a hot topic of current research to improve walking function recovery in the population.
Physiotherapy using exoskeleton robots significantly improves the effectiveness of rehabilitation. It provides support and active assistance for patients to regain movement, which is especially important in neurological diseases, injuries, and after surgery. These technologies help improve motor skills and strengthen muscles, which is especially important for patients who are recovering from such events. The use of exoskeletons makes the rehabilitation process more comfortable and customized to the individual needs of patients. They are becoming a particularly relevant topic in modern research focused on personalized medicine.
Robotic systems, such as exoskeletons, allow rehabilitation to be performed with greater precision and consistency, ensuring optimal joint and muscle loading. This approach reduces the risk of overload and injury that can occur with manual therapy, as exoskeletons enable clinicians to fine-tune the device’s parameters for each patient. This improves the quality of recovery and accelerates the rehabilitation process.
A robotic exoskeleton is a mechanical device designed to be worn by a person for a specific purpose. It typically consists of a rigid frame with joints that allow the person to move. Robotic exoskeletons can be wearable and assistive by structure, providing support and technologically augmenting a person’s physical disability.
The rehabilitation of the ankle joint, which is crucial for balance and movement, has received special attention in recent years. According to recent WHO statistics, the population in many countries is aging, and joint diseases are becoming more prevalent. Additionally, athletes and ordinary individuals are experiencing ankle injuries that require treatment. In such cases, rehabilitation devices like exoskeletons play a key role in the effective restoration of ankle joint function, which is especially important for patients with trauma and neurological disorders. Innovative methods for ankle joint treatment and training are being developed and utilized. As a result, there is a growing trend towards new developments in rehabilitation devices, making this field highly relevant.
The authors of this research paper propose a novel exoskeleton for ankle rehabilitation, designed to enhance functionality and support recovery from injuries. The design and modeling of the device are based on modern innovative approaches, making it highly relevant for clinical application. It is expected that this exoskeleton will significantly improve the efficiency of the rehabilitation process.
The proposed design solution for creating a mechanical device intended for ankle joint rehabilitation is based on the use of commercially available materials. This allows for the creation of an effective rehabilitation device with optimal performance characteristics using readily accessible materials.
The use of a screw drive in the proposed design increases the accuracy, smoothness, and safety of exoskeleton movement, which makes it an effective rehabilitation tool.
2. Related Work
Research in this area by various authors demonstrates steady growth over time and is becoming increasingly relevant. The increasing number of scientific publications and studies testifies to the growing attention to the problem of creating rehabilitation exoskeletons for ankle joints, which emphasizes its significance for modern science and clinical practice. Since 2004, about 347 studies have been published in the Scopus database for the keyword “exoskeleton for ankle rehabilitation” ([4]. Information about the dynamics of publications growth on the topic of ankle rehabilitation using exoskeletons (2004-2024) is shown in Figure 1.
The analysis of Figure 1 shows that the rate of publications in this area from 2004 to 2024 exhibits significant growth with some fluctuations. In the early years (2004-2010), there is a slow but steady increase in the number of publications. From 2011 to 2013, the rate decreased slightly, but from 2014 onwards, a consistent upward trend was observed. This indicates a significant increase in interest in this topic within the scientific community. The fluctuations may be related to various factors, such as the funding of scientific projects, shifts in research priorities, or external factors affecting publication activity.
Research published in the Scopus database in the field of exoskeletons for ankle rehabilitation is funded by both national and international scientific foundations, underscoring the global interest in this area. The National Science Foundation (NSF) is a leading research funder, having supported approximately 30 publications, highlighting its crucial role in funding technological innovation in rehabilitation. Similarly, the National Institutes of Health (NIH) has provided significant support, funding nearly 30 papers, indicating its interest in medical and rehabilitation technologies. The National Natural Science Foundation of China funded just over 25 publications during this period, reflecting China’s active support of research focused on developing rehabilitation technologies. The U.S. Department of Health and Human Services supported around 20 publications, demonstrating strong public sector involvement in medical and rehabilitation research. Other organizations, such as the National Institute of Child Health and Human Development, the China Scholarship Council, and the European Commission, have also made substantial contributions to research funding, with each supporting more than 10 publications. These papers cover a wide range of topics related to the development of exoskeletons for restoring ankle joint functionality and aim to improve rehabilitation methods.
Exoskeletons are emerging as an innovative solution to lower limb problems to improve function in older adults and people with joint injuries. As can be known from anatomy the mobility of the foot is defined 3 motions, which are shown as a foot mobility diagram in Figure 2.
Researchers over the world develop different kinds of rehabilitation devices using wide of methods and solutions. A muscle activity-based cost function has been developed in order to improve the efficiency of human ankle support optimization by using optimal combinations of calf muscle activity [5,6]. The authors aim to improve exoskeleton support tuning in various conditions. These results may significantly improve the efficiency of individual adaptation of the ankle exoskeleton to various conditions. In another study, the authors stated that adding real-time step length feedback to ankle support improved walking for people with cerebral palsy more than using the ankle assistance device. Researchers applied a real-time biofeedback mechanism in combination with an adaptive ankle device in order to assess and improve gait performance [7]. A team of researchers studied EMG-based and artificial neural network-based models that can predict ankle joint torques during different movements. In this research EMG-driven model usually predicted ankle torques better than the artificial neural network, especially with specific movement data [8]. However, the EMG-driven model is generally accurate for predicting torques, but the AI can predict much better with the right data. In some studies, the authors have made efforts to develop a rehabilitation robot that can assist stroke patients in different positions. A new rehabilitation device successfully can adjust to different person’s needs and training positions [9]. Many studies have been devoted to the design and testing of ankle joint rehabilitation exoskeletons. Some interesting findings have been stated in the obtained results. Developed prototypes effectively assist ankle movement and rehabilitation with novel design, showing good enough performance [10,11,12,13,14]. The difference between them can be that the authors used different approaches. Another two research works were considered for developing a T-Flex exoskeleton. In these studies, authors state T-FLEX ankle exoskeleton can reduce muscle activity without changing gait parameters or stability, but can not significantly change overall gait [15,16]. Some authors have contributed to the development of a control system for exoskeletons. In [17], the authors presented the effectiveness of a new ankle rehabilitation device controlled by a PD controller and monitored via Arduino IDE. The experimental results show a small error due to the limited resolution of the encoder. Researchers in Japan have developed a robotic self-rehabilitation device that can stretch an affected ankle using the movement of the ankle on the healthy side. The robotic device could allow users to independently rehabilitate an injured ankle using the movements of a healthy ankle, making the process much easier [18]. In addition, many contributions have been devoted to predicting and understanding individual responses to rehabilitation devices. In [19], researchers tested what data can be used to accurately characterize. It was found that mismatch modeling could improve the understanding of ankle exoskeleton responses by analyzing changes in motion. Advances in rehabilitation exoskeletons are significantly improving the mobility and quality of life of people with disabilities.
In recent literature authors propose a novel hybrid ankle rehabilitation robot that combines serial and parallel components, offering enhanced workspace and eliminating singularity for improved rehabilitation motions. The kinematic analysis demonstrates that the robot meets clinical rehabilitation needs, providing a strong basis for future enhancements [20]. In another study authors present an ankle rehabilitation robot for hemiplegic patients, detailing its design, motion mechanisms, and control models using ADAMS and Simulink software [21]. Several studies have been dedicated on ankle rehabilitation devices for stroke and injury recovery. They highlight low-cost, Arduino-controlled systems with positive results and safety features, as well as the growing use of robotics to streamline and enhance rehabilitation, making it more efficient and safer than traditional methods [22,23,24,25,26]. Nowadays, many studies focus on open issues and presenting solutions for new ankle rehabilitation technologies such as a safety-equipped automatic stretching machine that improves ankle flexibility, a precise monitoring device or pressure sensors to track movements [27,28,29]. Another interesting study conducted by the authors [30] to develop a flexible exosuit for ankle rehabilitation demonstrates several significant advantages. The device is lightweight and offers a high degree of mobility and comfort, making it more effective for rehabilitation compared to rigid exoskeletons. Experimental data show that the use of the exosuit reduces the body’s metabolic costs and decreases muscle activity, helping to conserve physical energy. The modular actuator and feedback system ensure accurate tracking of human movements and actively assist ankle joint motion. However, the additional weight of the system can increase energy expenditure, even when the actuator is engaged, which reduces the overall positive effect. The authors’ research [31] on the development of a flexible and lightweight exoskeleton with a high degree of mobility is very promising. It helps reduce muscle activity and metabolic costs during rehabilitation. The device has a modular design and a precise motion control system, which enhances comfort and efficiency in clinical applications. However, the additional weight of the exoskeleton may be associated with increased energy costs for system operation, necessitating further optimization of force transfer and nonlinear system characteristics. Overall, the literature highlights rapid advancements in ankle joint rehabilitation technologies, including innovative devices, low-cost devices and precise monitoring tools that can improve rehabilitation efficiency.
The development of new rehabilitation devices may become a modern requirement of rapidly changing technologies in the world. All the studies discussed above are evidence of the modern trend. Authors around the world develop new technology to improve lifestyle of the humans, by using different approaches and methods. Researchers around the world are developing new technologies to improve human lifestyles using a variety of approaches and methods. Many up-to-date control systems, mechanisms, sensors and etc. have been developed. Many advanced control systems, mechanisms, sensors, etc. have been developed. All the studies can be a good background for developing a new rehabilitation robotic exoskeleton, which is presented in this work. But there are still open problems that have not been covered. This paper presents a new robotic exoskeleton for ankle joint rehabilitation that has 3 DOFs that allow movements around the XYZ axes. The specialty of this research lies in the development of an exoskeleton for ankle joint rehabilitation using three linear electric actuators that provide precise control of joint movements. Unlike traditional rehabilitation devices, the presented design is characterized by ease of use, compactness, and low cost, making it more accessible to a wide range of users. The device adapts to the natural movements of the joint, providing both active and passive motion support in multiple planes, such as dorsal and plantar flexion. This extends its effective application in lower limb rehabilitation processes.
The innovative aspect of the research lies in the use of a screw drive that converts rotary motion into linear motion. The screw drive converts the rotational motion of the motor into linear motion, allowing precise control of the exoskeleton’s movements. It plays a key role in medical and rehabilitation devices where high movement accuracy is required. The helical transmission ensures smooth, jerk-free motion, which is essential for the comfortable use of the exoskeleton by patients. Smooth movements reduce the risk of re-injury and promote effective recovery. Additionally, it allows significant force to be developed with minimal motor power. This enables the exoskeleton to support and move the patient’s limbs without overloading the motors. Particularly noteworthy is the self-locking effect, which helps maintain limb position without the continuous application of motor force.
3. Materials and Methods
This paper proposes a new rehabilitation robotic exoskeleton that can be applied as an additional rehabilitation device. The main objective is to design an exoskeleton for ankle rehabilitation that provides the necessary support and accurate movement using three linear electric actuators.
3.1. Study of Biomechanical Characteristics of the Ankle Joint
The biomechanical features of the ankle joint consist of a set of interrelated characteristics that determine its function and performance. This joint comprises three bony components: the ankle (calcaneus), the bones of the foot (tarsals), and the heel (phalanges), as well as a ligamentous apparatus and muscles, which ensure its stability and mobility.
The ankle joint is a complex mechanical system that includes an axis of rotation, contact surfaces, and the ligaments and muscles that control its motion. The primary types of motion in the joint are dorsiflexion, plantar flexion, and internal and external rotation, allowing a variety of movements to be performed effectively. The functional role of the ankle joint is to support body weight, transfer loads to other joints, and participate in various types of movement. The mechanical behavior of the ankle joint is characterized by its flexibility, elasticity, stability, and ability to adapt to different loads. Its dynamic behavior includes mass-movement properties, energy efficiency, and the temporal characteristics of movement. These parameters are particularly important during high-intensity movements and under changing load conditions. Biomechanical features may also vary between individuals due to genetic factors, anatomical structure differences, and living conditions. Physiological processes that affect joint function include muscle contraction and relaxation, physiological stiffness, and synovial fluid release. These processes play a key role in maintaining normal joint function [32].
Understanding these biomechanical features is critical for diagnosing and treating ankle diseases and injuries, as well as for developing rehabilitation devices that create support and correction systems. Analyzing these characteristics provides better insight into the function of the ankle joint and aids in developing effective methods for its support and rehabilitation.
Creating an effective exoskeleton for ankle rehabilitation requires a thorough understanding of the joint’s biomechanics and basic movements. This knowledge is essential for developing a system that not only restores ankle joint functionality but also helps people regain independence and improve their quality of life. Ankle biomechanics analyze movements in three major planes: dorsiflexion and plantarflexion, inversion and eversion, and adduction and abduction. These movements occur in the frontal, sagittal, and transverse planes, helping to maintain joint mobility and proper function during rehabilitation. The exoskeleton simulates these movements to restore a normal gait and improve the functionality of the muscles and ligaments surrounding the ankle joint.
According to Figure 2, plantar flexion movements cover a range from 0 to 50, while dorsiflexion ranges from 0to 30. Inversion/eversion movements range from ±12°, and abduction/adduction movements range from ±10 [33]. These values were obtained in the absence of external loads. Basic ankle joint movements, such as dorsiflexion and plantarflexion, were key parameters in the development of the new ankle rehabilitation device described in this paper.
3.2. Kinematics and Performance of the Exoskeleton System
Important aspects of exoskeleton kinematics include key movements such as dorsiflexion and plantar flexion, which are essential for ankle rehabilitation. The exoskeleton also enables circular movements, expanding the range of rehabilitation exercises and helping to restore the joint’s natural mobility. A notable feature is the device’s adaptability to different levels of load, allowing it to be effectively used by patients with varying degrees of physical fitness and at different stages of rehabilitation.
This research work uses a mixed method of qualitative and quantitative analysis to obtain accurate data. The mathematical model is considered based on the kinematic scheme. The kinematic scheme of a rehabilitation device is presented in Figure 3.
All necessary mathematical data are calculated using the kinematic scheme. The number of degrees of freedom is determined using the Chebyshev equation.
As stated in Equation (1), the degrees of freedom for a planar mechanism are calculated as follows:
n – number of links;
p5 – number of fifth-class couples (single-movement couples);
p6 – number of fifth-class couples (single-movement couples).
According to the scheme in Figure 2, it is calculated as 3. Thus, all these calculations are required as input data for the virtual 3D model of the proposed rehabilitation device.
Figure 3 is a kinematic diagram of the exoskeleton for ankle rehabilitation. The foot platform (1) is used to place the user’s foot and allows movement of the joint. The tibia platform (2) fixes the tibia and is connected to other elements of the device. The actuator (3) is responsible for controlling the movement of the device, varying the length of the actuator (ΔL) to create the desired angle of motion (α). The articulated joint (4) provides mobility between the foot platform and the tibia, allowing smooth rehabilitation movements.
This kinematic scheme allows to calculation of the necessary parameters for building a 3D model and further mathematical modeling of the device, including the definition of degrees of freedom.
Today the market allows us to choose any necessary software to validate the received data and create a virtual prototype. All obtained data from numerical checks and mathematical models can be used to create a virtual 3D prototype. At the same time, such parameters as the prototype dimensions, weight, and mechanical and physical characteristics play a key role in the synchronized operation of the components as a single system. A 3D virtual model of the rehabilitation robotic device is shown in Figure 4. The virtual model of the proposed rehabilitation device in Figure 4 consists of linear actuators, a housing, a foot platform, a ball joint, a controller, EMG sensors, accelerometers, and a monitoring system. Virtual testing of the 3D model is carried out to verify the correct operation of the mechanical system. Therefore, numerical verification, mathematical modeling, and 3D model simulation were used to validate all data before creating a physical prototype.
Figure 4 shows an exploded 3D model of a rehabilitation exoskeleton designed to support and restore ankle joint movements during rehabilitation.
The foot platform (1) is a supporting part of the exoskeleton where the user’s foot is placed. It fixes and supports the foot, providing stability during movements. The shank platform (2) secures the user’s shin and connects it to other elements of the device, maintaining the correct position of the leg. The motor (3) is the main driving element, converting electrical energy into mechanical motion to control the movements of the exoskeleton. The motor holder (4) secures the motor to the structure, ensuring its stable position and the transmission of force to other parts of the exoskeleton. The screw nut (5) works in tandem with the screw shaft, converting rotary motion into linear motion. The screw shaft (6) plays a crucial role in the transmission of movement. It converts the rotary motion of the motor into linear motion. In this case, the helical transmission ensures smooth and controlled movements, which is particularly important for precise control in rehabilitation devices. The ball joint (7) provides freedom of movement in multiple planes, allowing the natural movements of the joint to be replicated. The cylindrical joint (8) allows for rotational movements, which are necessary for the correct functioning of the mechanism.
The screw drive enables smooth, controlled movement, ensuring the exoskeleton is comfortable for patients to use. It also prevents sudden jerks, reducing the risk of re-injury and promoting effective recovery. Due to the self-braking effect of the screw gear, the exoskeleton can hold the limb in the desired position without continuous use of the motor, facilitating rehabilitation and reducing the load on the actuators.
The proposed rehabilitation exoskeleton design is a highly effective solution for ankle joint motor recovery, providing patients with precise motion control and comfort.
Figure 5 is a control schematic for a rehabilitation exoskeleton. This control system for the rehabilitation exoskeleton consists of several key components that interact to ensure the proper operation of the device.
The main control unit is the controller, which processes the input signals from the sensors and determines which commands to send to the motor drives. The Driver controls the motors based on the commands from the controller. It distributes power and control signals to the motors. The monitor displays information about the system operation and helps the operator monitor the parameters in real time. IMU Sensor is an inertial sensor that monitors tilt angles and acceleration. It is used to measure the movement of the exoskeleton. Force Sensor measures the load or force applied to the exoskeleton and sends the data to the controller to adjust the movement. EMG Sensor measures the electrical activity of the user’s muscles, allowing the system to adapt motion support based on muscle activity. Power Supply provides electrical power to all components of the system. Motors (M1, M2, M3) are the actuators that perform the physical movements in the exoskeleton, controlled through the driver and controller.
The block diagram in Figure 6 describes the operation of the motion control system in an exoskeleton with ankle feedback. Data about the position or angle of the ankle joint is fed back to the system. This feedback allows the system to correct movement in real time, providing more accurate and adaptive motion control.
The system dynamically adapts the support of the user’s movements depending on sensor data. IMU, Force, and EMG sensors collect information about movements and loads. The collected data is fed to the controller, which processes the information and determines how the exoskeleton should move. The controller sends commands to the driver, which controls the operation of the motors (M1, M2, M3). The motors create motion based on the commands, which ensures that the exoskeleton moves. During the movement, sensors collect information about the ankle condition and other motion parameters. This data is sent back to the controller, providing feedback that allows the controller to adjust motor operation and tailor the exoskeleton’s movement to the user’s needs. A monitor displays current system performance parameters for operator control.
4. Results
The design process for an ankle rehabilitation exoskeleton combines traditional engineering design methods with modern simulation and analysis technologies. This approach enables the creation of a more efficient and comfortable device that better aligns with the biomechanical characteristics of the ankle joint. To achieve this, the study utilized powerful numerical analysis and simulation software, SolidWorks Simulation Professional, along with a specialized Motion Simulation module to enhance motion analysis capabilities. These tools allow for the analysis of dynamic loads on the rehabilitation device.
A key step in the development of an ankle rehabilitation exoskeleton is achieving dynamic articulation (motion creation) in the simulation. This enables the simulation of natural joint movements and provides insights into load distribution and movement analysis.
Figure 7 shows the three key positions of the exoskeleton for ankle rehabilitation:
(a) dorsiflexion;
(b) neutral position;
(c) plantarflexion.
Figure 6.
Exoskeleton positions for ankle rehabilitation: dorsal flexion (a), neutral position (b) and plantar flexion (c).
Figure 6.
Exoskeleton positions for ankle rehabilitation: dorsal flexion (a), neutral position (b) and plantar flexion (c).
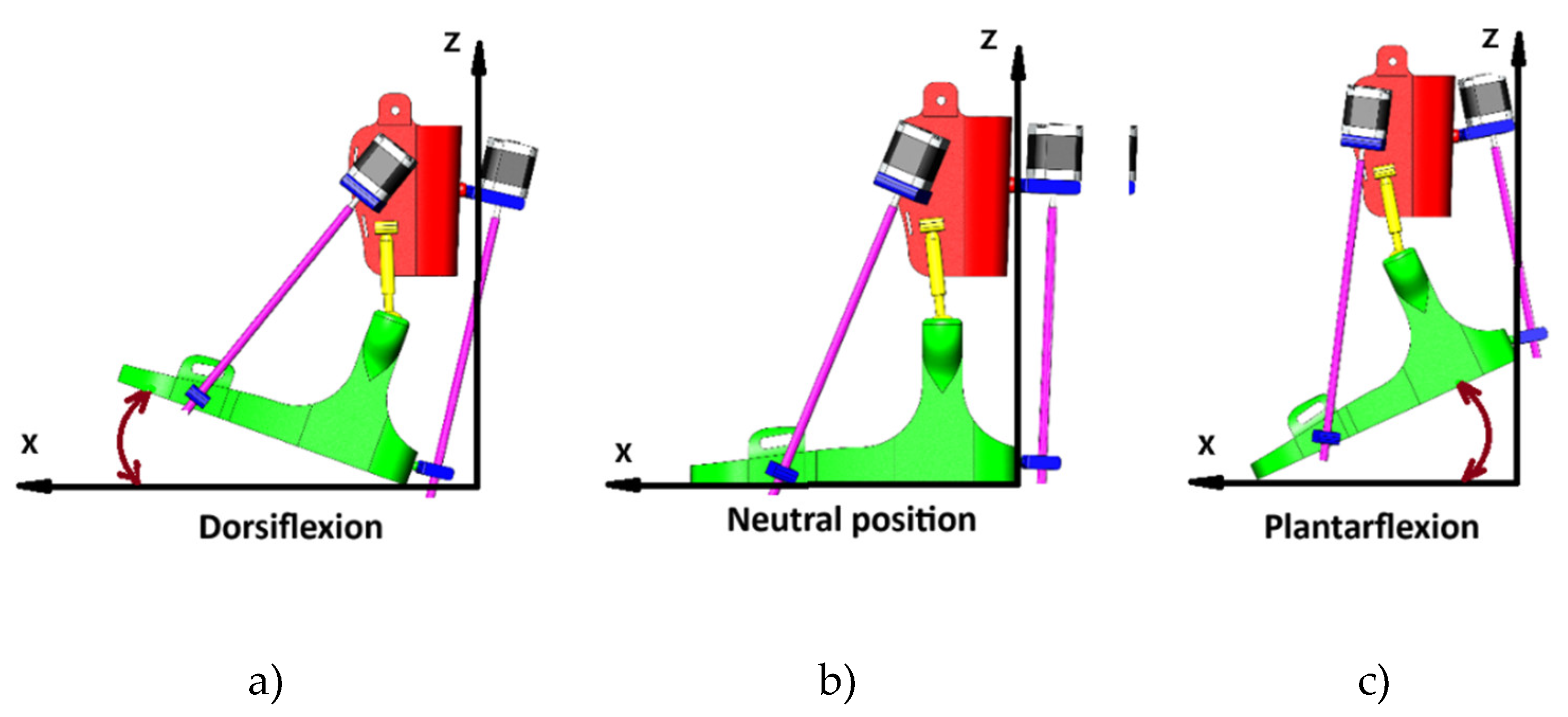
In the dorsiflexion state (a), the foot is lifted upwards by an angle of 15° relative to the X-axis, corresponding to the natural upward motion of the foot during walking. This movement is achieved by adjusting the angles between the exoskeleton components and the active participation of the linear actuators.
The neutral position (b) reflects the starting position, where the ankle joint is at rest at a 90° angle. In this position, the foot is placed perpendicular to the plane of support, providing balance and stability.
In the plantar flexion state (c), the foot is lowered downward at an angle of 20° relative to the X-axis, simulating the motion of the foot pushing off the ground during a stride. This movement is also controlled by the exoskeleton actuators, which ensure the necessary amplitude and precision.
Figure 7 displays the time dependence of exoskeleton drive torque, which shows the exoskeleton motor performance in dynamics, with clear torque fluctuations in response to changing loads and motion cycles.
Figure 7.
Variation of exoskeleton torque during cyclic movements.
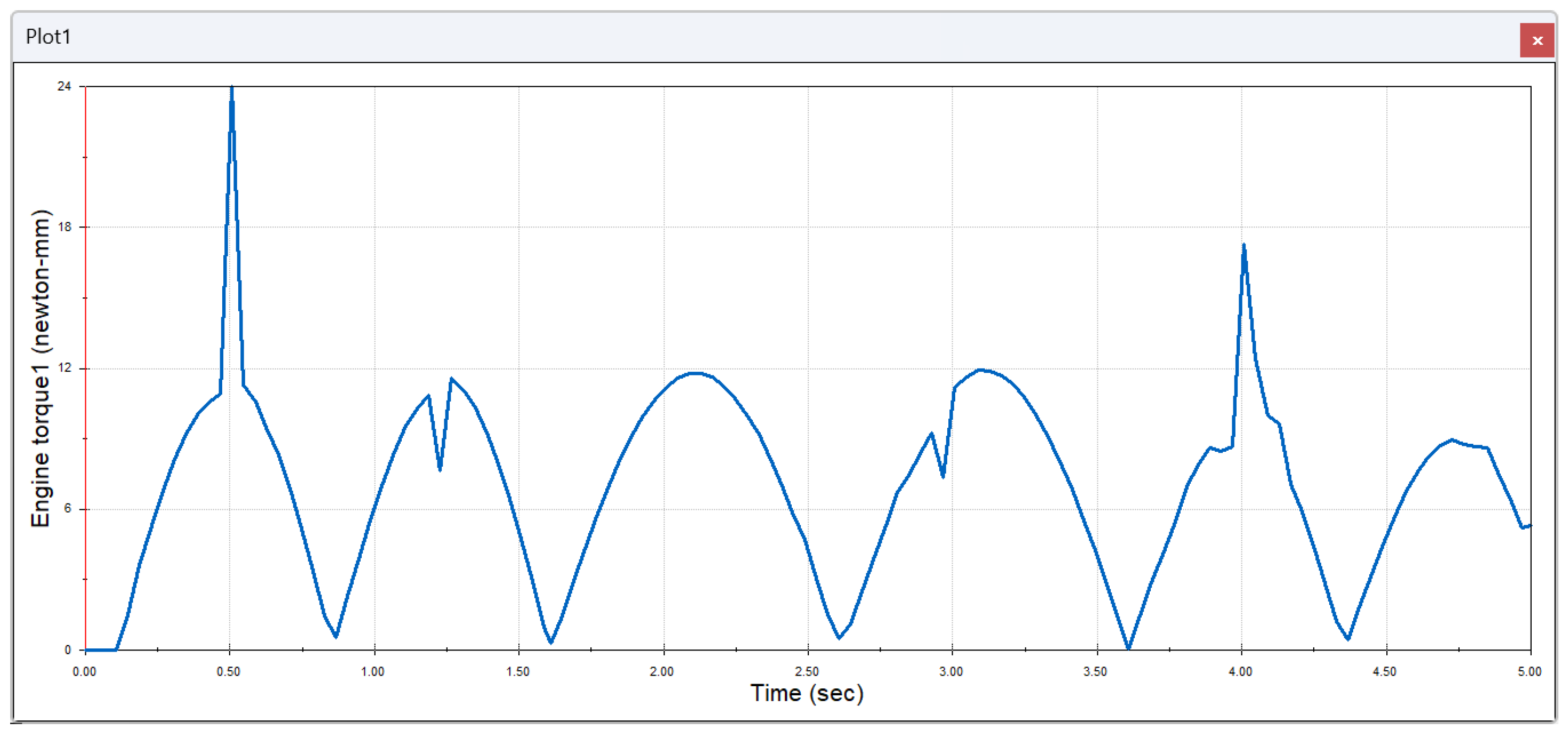
According to Figure 7, at a time mark of about 0.5 seconds, there is a sudden jump in torque to about 24 Newton-millimeters, which may indicate the moment of application of a sudden load on the exoskeleton. After the peak, the torque exhibits cyclic oscillations, with maximum values around 12 Newton-millimeters and minimum values near zero. These oscillations reflect the dynamics of the exoskeleton motor during ankle joint movements such as dorsal and plantar flexion. The graph shows a repeating pattern of oscillations every 0.75 – 1 second, which is related to the cyclic motion of the exoskeleton and the changing actuator loads. At the time mark of about 4 seconds, a second torque peak is observed, slightly lower than the first, which may indicate a change in load level or activation of another phase of exoskeleton motion.
Figure 8 illustrates the oscillatory process of linear movement for 5 seconds, with a maximum amplitude of about 300 mm and a minimum amplitude of about 258 mm. These data reflect the cyclic nature of the exoskeleton when performing repetitive movements such as joint flexion and extension. In this case, the amplitude and frequency of movement changes are important parameters for assessing the accuracy and effectiveness of the device in rehabilitation settings.
Figure 9 reflects the cyclic nature of the exoskeleton velocity variation, which increases and decreases over time, with three major velocity peaks. The maximum velocity reaches about 120 mm/sec in the middle of the cycle. Declines in velocity to zero indicate transitions between phases of movement. This graph is used to analyze the accuracy of the exoskeleton and its ability to provide smooth and efficient movements during rehabilitation.
Smooth speed changes with distinct peaks and troughs indicate that the exoskeleton is capable of providing controlled and predictable movements, which are critical for rehabilitation. This demonstrates that the exoskeleton operates with high fidelity, ensuring stable joint support during rehabilitation exercises.
Figure 10 shows smooth and consistent changes in the exoskeleton’s angular motion over 5 seconds, indicating stable device operation. The maximum movement amplitude reaches 110.8 degrees, while the minimum reaches 86.5 degrees, highlighting the cyclic nature of the joint movements. This confirms that the exoskeleton is able to control and maintain movements with high precision, which is essential for effective rehabilitation.
Figure 11 illustrates the exoskeleton’s ability to support lateral movements of the ankle joint, providing restoration of its functionality in different planes of motion, which is critical for complex rehabilitation.
In the adduction position, movement occurs between 0° and 10-15° inward, depending on the design features of the exoskeleton and the physiological characteristics of the patient. This movement is controlled by the exoskeleton’s linear actuators and helps restore lateral joint mobility.
In the neutral position, the foot is perpendicular to the plane of support, corresponding to the initial state where the joint is in equilibrium without lateral deviation.
In the abduction position, the foot moves outward between 0° and 10-15°, simulating the foot’s movement away from the body’s centerline. This movement is important for developing external lateral joint mobility and is also controlled by the exoskeleton’s actuators.
Figure 12 shows predominantly low torque values with periodic peaks, particularly noticeable at the 3.5 and 4.5-second marks when the motor is subjected to a sudden increase in load. The maximum torque reaches 180 Newton-millimeters, corresponding to short-term high-intensity phases of exoskeleton operation. This indicates the motor’s performance under varying load conditions and the transition between movement phases during the rehabilitation cycle.
Figure 13 shows smooth cyclic changes in the linear displacement of the second exoskeleton component. The device works within a small range of movements with a minimum of about 279 mm and a maximum of about 293 mm, which can be important for precise control of movements during rehabilitation. This movement pattern reflects the stable operation of the device with compression and expansion phases.
Figure 14 demonstrates the cyclic nature of the translational velocity of the second exoskeleton component with three major velocity peaks. The maximum speed reaches 110 mm/s at the second peak, which indicates more intense movement in the middle phase. It shows a smooth increase and decrease in speed in each phase, which indicates the controlled and effective operation of the exoskeleton when performing cyclic movements.
Figure 15 shows smooth cyclic changes in the angular displacement of the second exoskeleton component in the range from 94 to 111 degrees. Cycle times are roughly the same, suggesting regular and controlled movements. Smooth transitions between highs and lows indicate stable exoskeleton performance when performing cyclic angular movements, which is important for control accuracy and rehabilitation efficiency.
Figure 16 shows three ankle rehabilitation exoskeleton positions that demonstrate lateral foot movements in different planes:
In the valgus deflection position (a), the foot’s deflection angle can vary between 5° and 15° outward relative to the Y-axis. This movement helps stretch the internal structures of the foot and improve lateral stability. It moves the foot away from the body’s midline, which is important for restoring lateral mobility of the ankle joint.
In the neutral position, the foot’s angle of deviation is 0°, as the foot remains in a neutral state, without inward or outward deviations. This is the starting position used as a baseline to initiate movements and assess joint functionality.
In varus deviation, the angle of deviation of the foot can be 5 °-15 ° inward relative to the Y-axis, which corresponds to the natural movement of the foot when it is brought to the midline. This movement is important to regain control of the internal lateral movements of the joint and ensure the full range of motion.
Figure 17 shows oscillating torque changes with two significant peaks around 6 Newton millimeters at timestamps of 2 and 3.2 seconds, indicating the phase structure of the exoskeleton motor operation. These peaks can correspond to the phases of maximum load or active work of the exoskeleton. Periodic fluctuations between peaks indicate the cyclic nature of the drive over the entire time interval.
Figure 18 shows smooth cyclic changes in the linear movement of the third exoskeleton component ranging from 276 mm to 292 mm. These changes indicate stable operation of the device, providing phase movements between minimum and maximum values. Smooth transitions between phases show precise movement control, which is critical for rehabilitation.
Figure 19 shows cyclic changes in the translational velocity of the third exoskeleton component, with three major velocity peaks. The maximum speed is reached at around 2.5 seconds and is about 50 mm/s. These speed fluctuations reflect the cyclical nature of exoskeleton operation, where the acceleration and deceleration phases alternate, which is important for smooth and controlled movement during rehabilitation.
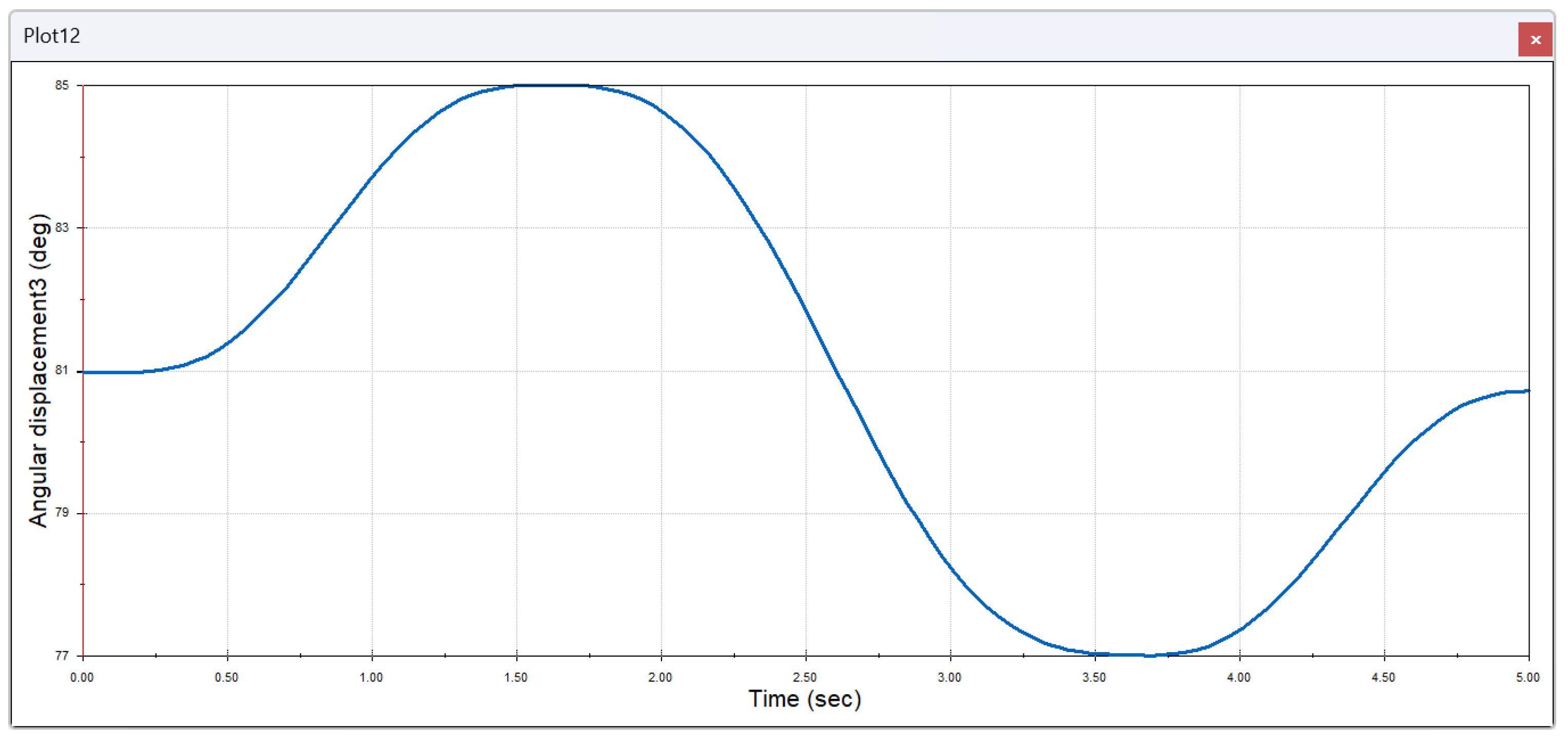
Figure 20 shows cyclic changes in the angular displacement of the third exoskeleton component with a maximum value of about 85 degrees and a minimum of 77 degrees. These smooth transitions between the rising and falling phases of angular displacement show stable operation of the exoskeleton, providing controlled movement within a given range of angles.
Experimental data obtained during the modeling and simulation of the exoskeleton’s operation show that the device provides smooth and controlled movements, which is critical for the rehabilitation of patients with varying degrees of functional impairment. Smooth changes in motor torque and the cyclic nature of the angular movements of the exoskeleton components confirm that the system can adapt to the individual needs of patients, thereby providing optimal recovery conditions. The results for translational velocity and angular displacement demonstrated stability and repeatability throughout testing. This suggests that the exoskeleton not only replicates natural movements but does so with a high degree of accuracy and control, which is essential for the successful recovery of the rehabilitated patient.
One of the main achievements of the study is the demonstrated biomechanical compatibility of the exoskeleton with the ankle. During the tests, the device showed the ability to reproduce natural amplitudes of movement within the physiological range. This is especially important, as accurate reproduction of the natural biomechanics of the joint contributes not only to the restoration of its mobility, but also to reduce the risk of repeated injuries and prevent overload of other joints.
The testing process of the exoskeleton device demonstrated a high degree of adaptability to changing loads and different phases of movement. Controlled fluctuations in torque and linear movement have shown to provide the necessary support at different stages of rehabilitation, which has a positive effect on the recovery rate of patients. Advantages of the design include availability of materials, ease of use, and flexibility in customization, making it an attractive option for use in both clinical and home settings.
5. Conclusions
The proposed exoskeleton model has high potential for clinical application and home use, providing precise motion control, patient comfort and cost-effectiveness, which makes it a promising solution for lower limb function restoration.
In this study, an exoskeleton model for ankle rehabilitation was developed and tested to demonstrate high efficiency in restoring the joint’s motor function. The focus was on the biomechanical compatibility of the device with the natural movements of the ankle joint, allowing for accurate reproduction of movements such as dorsal and plantar flexion, inversion and eversion. This precise motion reduces the risk of re-injury and prevents overloading of other joints, which is especially important for patients with musculoskeletal injuries and diseases.
The innovative use of a screw drive has ensured smooth and controlled movements of the exoskeleton. Smooth and predictable movements without sudden jerks contribute to a comfortable and safe rehabilitation process. Due to the self-locking effect of the screw drive, the exoskeleton can hold the limb in the desired position without constant use of the motor, which reduces the load on the actuators and increases the overall efficiency of the device.
One of the key achievements of the study was the development of a device capable of accurately reproducing natural ankle joint movements, such as dorsiflexion, plantar flexion, inversion, and eversion. This not only helps restore joint mobility but also reduces the risk of re-injury by preventing the overloading of other joints.
An important feature of the exoskeleton is its ability to adapt to different physical conditions of patients. The device provides both active and passive movement support, making it versatile for use at various stages of rehabilitation. This flexibility allows the exoskeleton to be effectively used for the rehabilitation of a wide range of patients, including those with physical disabilities. The simplicity of the design, along with its adaptive capabilities, makes the device easy to use and customize, significantly simplifying the rehabilitation process.
Mathematical modeling and virtual testing have demonstrated the system’s high accuracy in controlling movements. The data obtained confirm that the exoskeleton is capable of providing smooth and controlled movements, which are essential for successful rehabilitation. The smoothness of force moment and angular displacement changes confirmed the high accuracy of control, which is especially important when working with patients who require gradual motor recovery.
The proposed exoskeleton model shows great potential for clinical application due to its compactness, low cost, and ability to adapt to individual patient needs. The device can be used both in specialized rehabilitation centers and at home to support and accelerate the recovery process.
The research emphasizes the significance of employing robotic exoskeletons in the rehabilitation of patients with musculoskeletal injuries and diseases while also showcasing the potential for future advancements in rehabilitation technology. In the future, the development of such devices may contribute to the creation of better, more personalized solutions that will further enhance the effectiveness of rehabilitation processes and improve patients’ quality of life.
Author Contributions
Conceptualization, G.S. and N.Zh.; methodology, G.T.; software, A.U.; validation, Y.N. and A-A.A.; formal analysis, O.A.; investigation, N.Zh.; resources, G.T.; data curation, Y.N.; writing—original draft preparation, G.S.; writing—review and editing, G.T.; visualization, A-A.A.; supervision, G.S.; project administration, G.S.; funding acquisition, G.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Science Committee of the Ministry of Science and Higher Education of the Republic of Kazakhstan, Grant № AP13268857.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- World Health Organization (WHO). Decade of Healthy Ageing: Key Facts. Available online: https://www.who.int/initiatives/decade-of-healthy-ageing (accessed on 14 December 2020).
- World Health Organization (WHO). Rehabilitation: Key Facts. Available online: https://www.who.int/news-room/fact-sheets/detail/rehabilitation (accessed on 22 April 2024).
- World Health Organization (WHO). Rehabilitation 2030 Initiative. Available online: https://iris.who.int/bitstream/handle/10665/376162/9789240087392-eng.pdf?sequence=1 (Meeting report, Geneva, Switzerland, 10 - 11 July 2023).
- https://www.scopus.com/term/analyzer.uri?sort=Analyze+results (accessed on 05 October 2024).
- Han, H., Wang, W., Zhang, F., Li, X., Chen, J., Han, J., & Zhang, J. (2021). Selection of muscle-activity-based cost function in human-in-the-loop optimization of multi-gait ankle exoskeleton assistance. IEEE Transactions on Neural Systems and Rehabilitation Engineering, 29, 944-952. [CrossRef]
- Hu, D., Xiong, C., Wang, T., Zhou, T., Liang, J., & Li, Y. (2022). Modulating energy among foot-ankle complex with an unpowered exoskeleton improves human walking economy. IEEE Transactions on Neural Systems and Rehabilitation Engineering, 30, 1961-1970. [CrossRef]
- Fang, Y., & Lerner, Z. F. (2021). Feasibility of augmenting ankle exoskeleton walking performance with step length biofeedback in individuals with cerebral palsy. IEEE Transactions on Neural Systems and Rehabilitation Engineering, 29, 442-449. [CrossRef]
- Zhang, L., Li, Z., Hu, Y., Smith, C., Farewik, E. M. G., & Wang, R. (2020). Ankle joint torque estimation using an EMG-driven neuromusculoskeletal model and an artificial neural network model. IEEE Transactions on Automation Science and Engineering, 18(2), 564-573.
- Wang, X., Wang, H., Zhang, B., Zheng, D., Yu, H., Cheng, B., & Niu, J. (2024). A Multistage Hemiplegic Lower-Limb Rehabilitation Robot: Design and Gait Trajectory Planning. Sensors, 24(7), 2310. [CrossRef]
- Nursultan, Z., Marco, C., & Balbayev, G. (2023). A Portable Robotic System for Ankle Joint Rehabilitation. Electronics, 12(20), 4271.
- Kubota, S., Kadone, H., Shimizu, Y., Koda, M., Noguchi, H., Takahashi, H., ... & Yamazaki, M. (2022). Development of a new ankle joint hybrid assistive limb. Medicina, 58(3), 395. [CrossRef]
- Racu, C. M., & Doroftei, I. (2015, October). Ankle rehabilitation device with two degrees of freedom and compliant joint. In IOP Conference Series: Materials Science and Engineering (Vol. 95, No. 1, p. 012054). IOP Publishing. [CrossRef]
- Xu, Z. H., Song, C. L., Yu, H. L., Yan, S. J., & Shi, W. B. (2011). Design of an ankle rehabilitation device. Chinese Journal of Tissue Engineering Research, 15(39), 7292. [CrossRef]
- Russo, M., & Ceccarelli, M. (2020). Analysis of a wearable robotic system for ankle rehabilitation. Machines, 8(3), 48.
- Otálora, S., Ballen-Moreno, F., Arciniegas-Mayag, L., Cifuentes, C. A., & Múnera, M. (2022). Biomechanical effects of adding an ankle soft actuation in a unilateral exoskeleton. Biosensors, 12(10), 873. [CrossRef]
- Gomez-Vargas, D., Ballen-Moreno, F., Barria, P., Aguilar, R., Azorín, J. M., Munera, M., & Cifuentes, C. A. (2021). The actuation system of the ankle exoskeleton t-flex: First use experimental validation in people with stroke. Brain sciences, 11(4), 412. [CrossRef]
- Phuoc, P. D., & Tuy, T. X. (2022). Research control for ankle joint rehabilitation device. Journal of Mechanical Engineering and Sciences, 16(1), 8743-8753.
- Toda, H., & Kawamoto, H. (2023). Device Design of Ankle Joint Stretching System Controlled by the Healthy Side Ankle Joint Movement for Self-Rehabilitation. Journal of Robotics and Mechatronics, 35(3), 556-564.
- Ebers, M. R., Rosenberg, M. C., Kutz, J. N., & Steele, K. M. (2023). A machine learning approach to quantify individual gait responses to ankle exoskeletons. Journal of Biomechanics, 157, 111695. [CrossRef]
- Z. Liao, L. Yao, Z. Lu, and J. Zhang. Screw theory based mathematical modeling and kinematic analysis of a novel ankle rehabilitation robot with a constrained 3-PSP mechanism topology. International Journal of Intelligent Robotics and Applications, 2(3):351–360, 2018. [CrossRef]
- Z. Sun et al. Mechanism Design and ADAMS-MATLAB-Simulation of a Novel Ankle Rehabilitation Robot. 2019 IEEE International Conference on Robotics and Biomimetic (ROBIO), pages 425–432, Dali, China, December, 2019. [CrossRef]
- D. Minh Duc, L. T. Thuy Tram, P. Dang Phuoc and T. Xuan Tuy, “Study on Ankle Rehabilitation Device Using Linear Motor,” 2019 International Conference on System Science and Engineering (ICSSE), Dong Hoi, Vietnam, 2019, pp. 573-576. [CrossRef]
- Cazacu, Cristina-Magda & Doroftei, Ioan. (2014). An Overview on Ankle Rehabilitation Devices. Advanced Materials Research. 1036. 781-786. 10.4028/www.scientific.net/AMR.1036.781.
- D.M. Duc, P.D. Phuoc, & T.X. Tuy. (2022). Research control for ankle joint rehabilitation device. Journal of Mechanical Engineering and Sciences, 16(1), 8743–8753. [CrossRef]
- Asaki Akagi, Satoki Tsuichihara, Shinichi Kosugi, Hiroshi Takemura, Development of a Rehabilitation and Training Device Considering the Ankle Degree of Freedom, Journal of Robotics and Mechatronics, 2020, Volume 32, Issue 3, Pages 673-682.
- Ren, Y., Wu, Y. N., Yang, C. Y., Xu, T., Harvey, R. L., & Zhang, L. Q. (2017). Developing a Wearable Ankle Rehabilitation Robotic Device for in-Bed Acute Stroke Rehabilitation. IEEE transactions on neural systems and rehabilitation engineering: a publication of the IEEE Engineering in Medicine and Biology Society, 25(6), 589–596. [CrossRef]
- Shiraishi, Y., Okamoto, S., Yamada, N. et al. Pneumatically-driven stretching machine for ankle dorsiflexion: safety concepts and effectiveness test involving healthy young subjects. Robomech J 7, 10 (2020). [CrossRef]
- Xu, C.; Zhou, Y.; Ji, J.; Wei, C. An Ankle Joint Flexion and Extension Movement-Monitoring Device Based on Pressure Sensors. Micromachines 2023, 14, 2141. [CrossRef]
- Gonçalves, R.S.; Rodrigues, L.A.O.; Humbert, R.; Carbone, G. A User-Friendly Nonmotorized Device for Ankle Rehabilitation. Robotics 2023, 12, 32. [CrossRef]
- He, L.; Xu, C.; Guan, X. Design Methodology and Experimental Study of a Lower Extremity Soft Exosuit. Electronics 2023, 12, 2502. [CrossRef]
- Pan, C.-T.; Lee, M.-C.; Huang, J.-S.; Chang, C.-C.; Hoe, Z.-Y.; Li, K.-M. Active Assistive Design and Multiaxis Self-Tuning Control of a Novel Lower Limb Rehabilitation Exoskeleton. Machines 2022, 10, 318. [CrossRef]
- Meng, Q.; Liu, G.; Xu, X.; Meng, Q.; Yu, H. Design and Analysis of a Supine Ankle Rehabilitation Robot for Early Stroke Recovery. Machines 2023, 11, 787.
- Nursultan, Z., Titov, A., Ceccarelli, M., Balbayev, G. (2022). Design and Performance of a Motion-Assisting Device for Ankle. In: Khang, N.V., Hoang, N.Q., Ceccarelli, M. (eds) Advances in Asian Mechanism and Machine Science. ASIAN MMS 2021. Mechanisms and Machine Science, vol 113. Springer, Cham. [CrossRef]
Figure 1.
Growth dynamics of publications on the topic of ankle rehabilitation using exoskeletons (2004-2024).
Figure 1.
Growth dynamics of publications on the topic of ankle rehabilitation using exoskeletons (2004-2024).
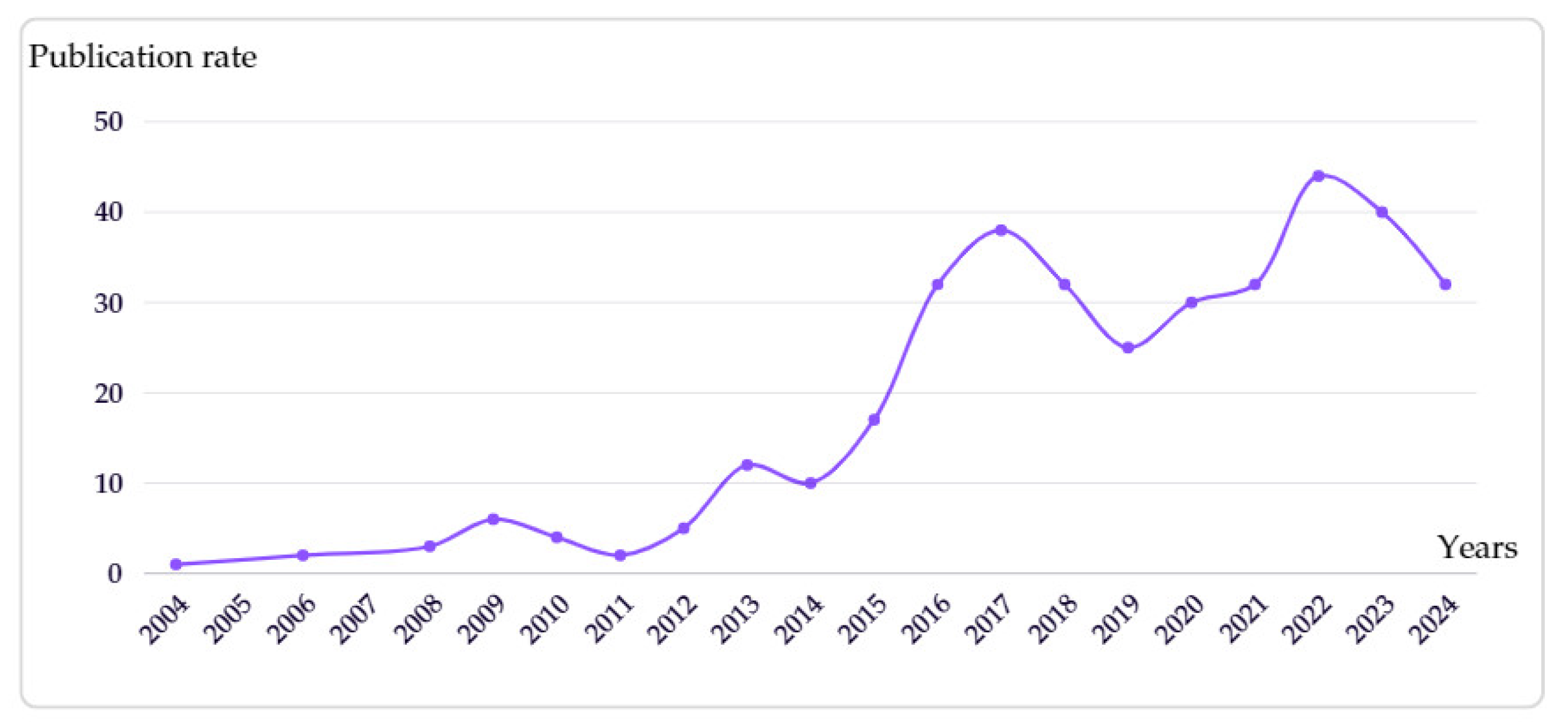
Figure 2.
Foot mobility diagram.
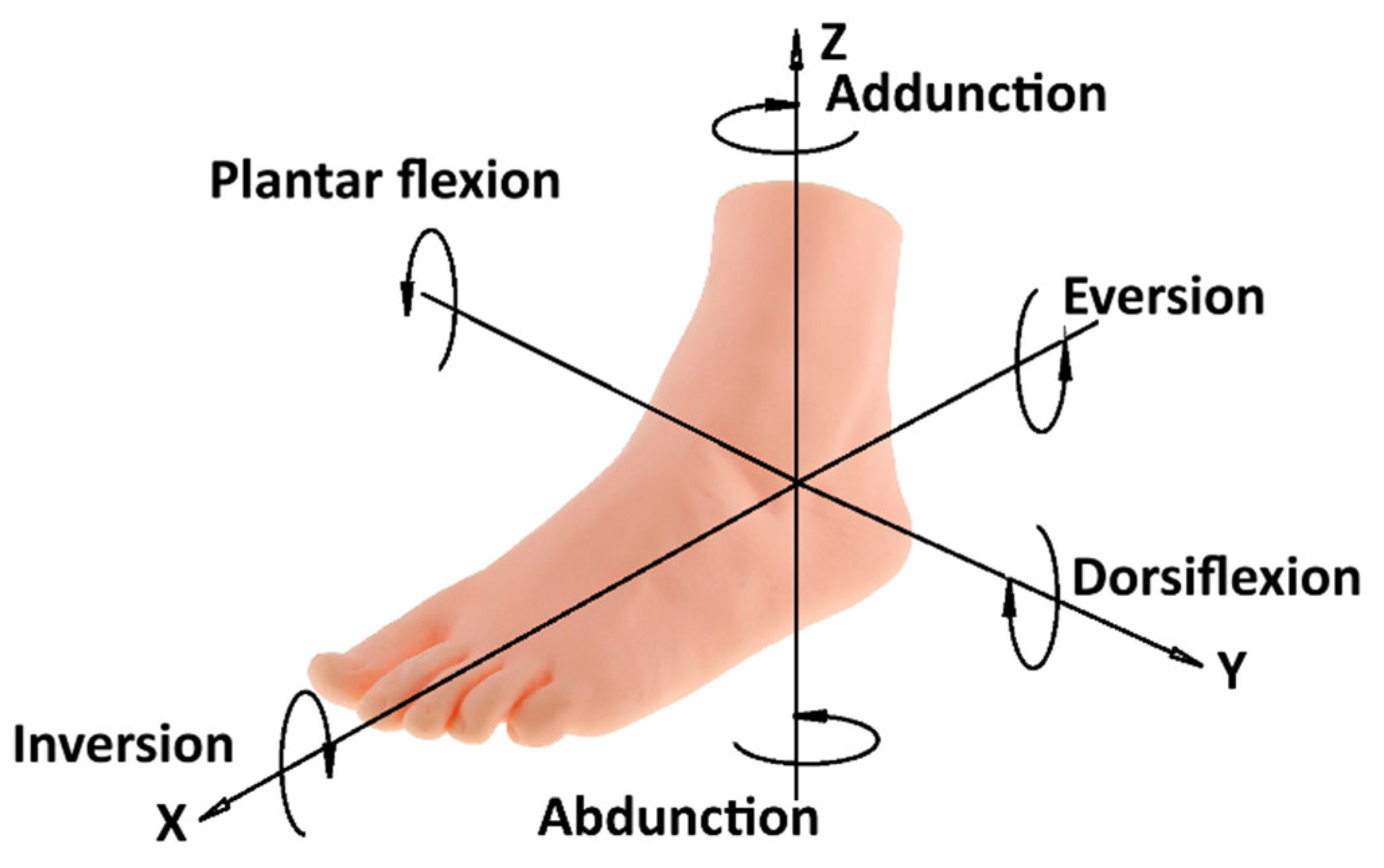
Figure 3.
A kinematic scheme of an ankle rehabilitation exoskeleton: 1 – Foot platform; 2 – Shank platform; 3 – motor; 4 – spherical joint.
Figure 3.
A kinematic scheme of an ankle rehabilitation exoskeleton: 1 – Foot platform; 2 – Shank platform; 3 – motor; 4 – spherical joint.
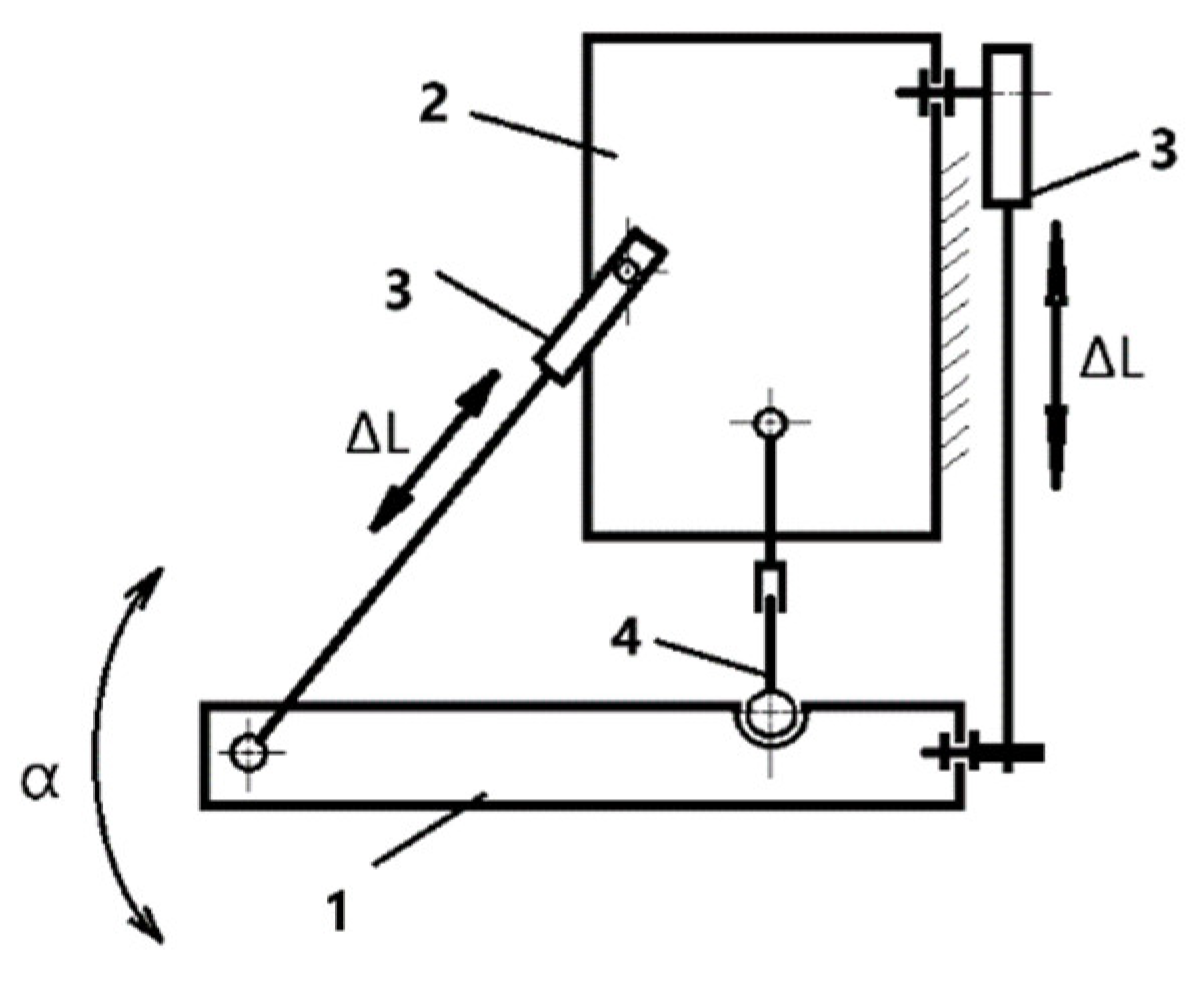
Figure 4.
Exploded 3D model of a rehabilitation exoskeleton: 1- foot platform; 2- shank platform; 3- motor; 4- motor holder; 5- screw nut; 6 – screw shaft; 7 – ball joint; 8 – cylindrical joint.
Figure 4.
Exploded 3D model of a rehabilitation exoskeleton: 1- foot platform; 2- shank platform; 3- motor; 4- motor holder; 5- screw nut; 6 – screw shaft; 7 – ball joint; 8 – cylindrical joint.
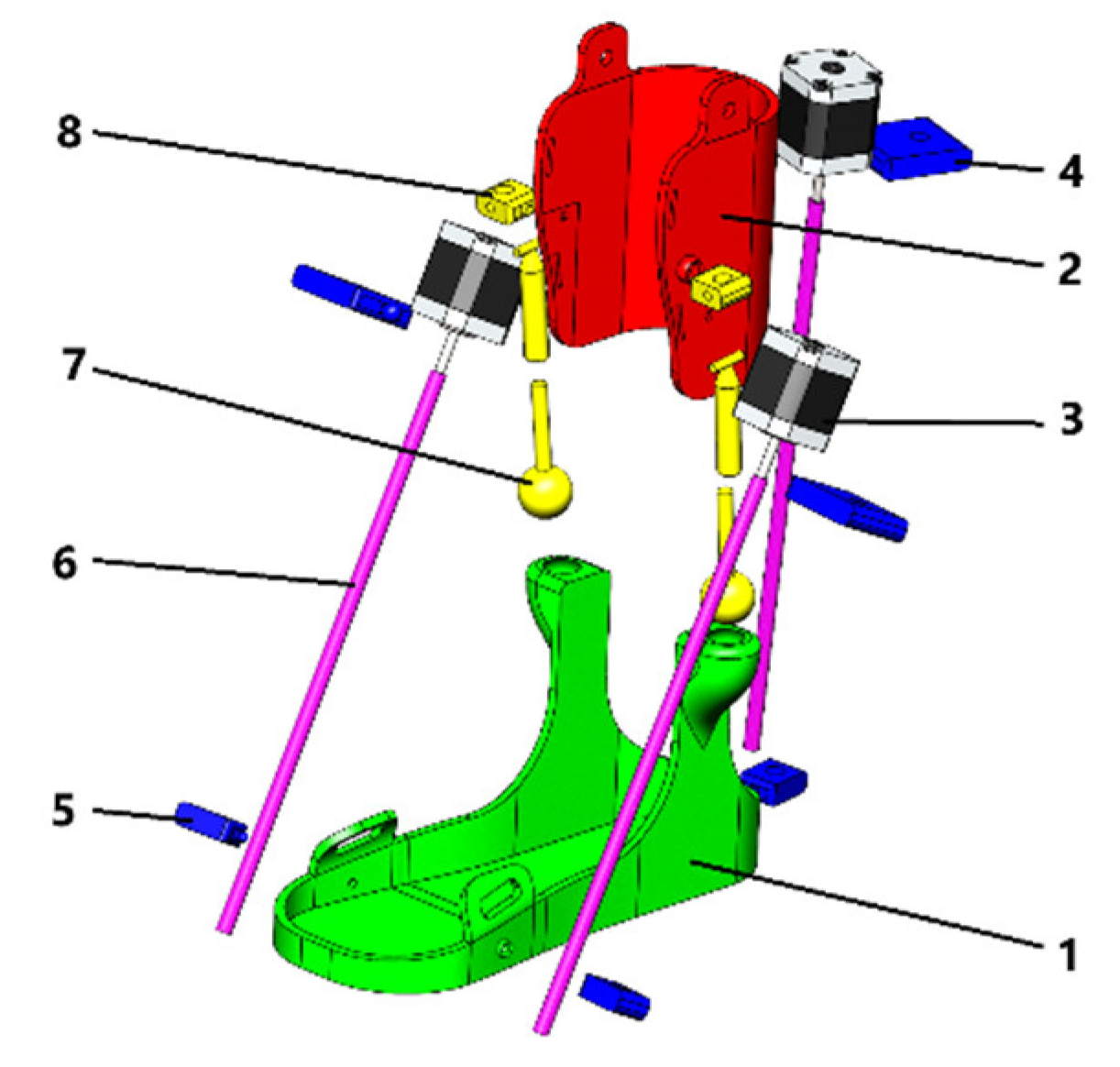
Figure 5.
A conceptual design diagram.
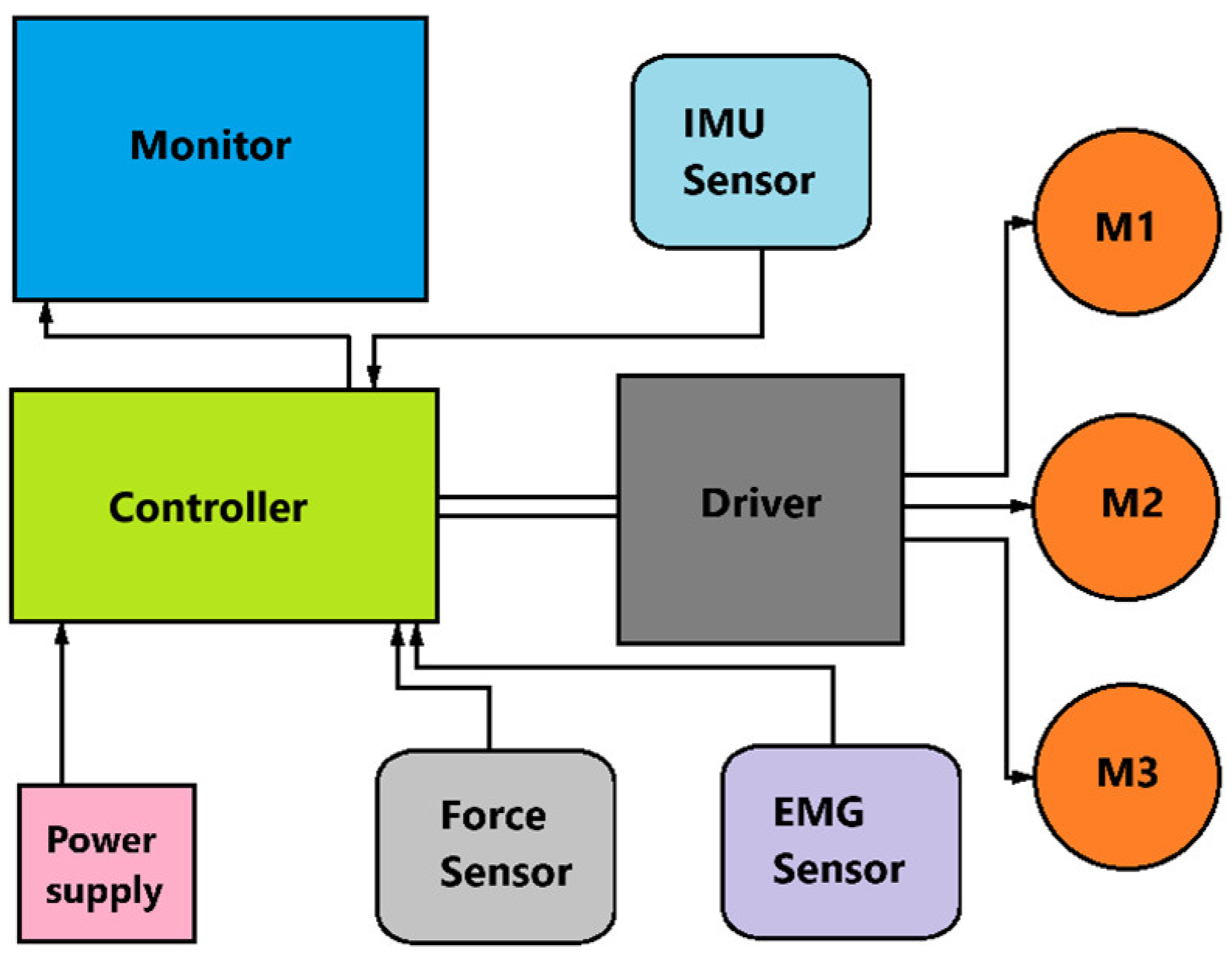
Figure 6.
A scheme for control design for the proposed exoskeleton.
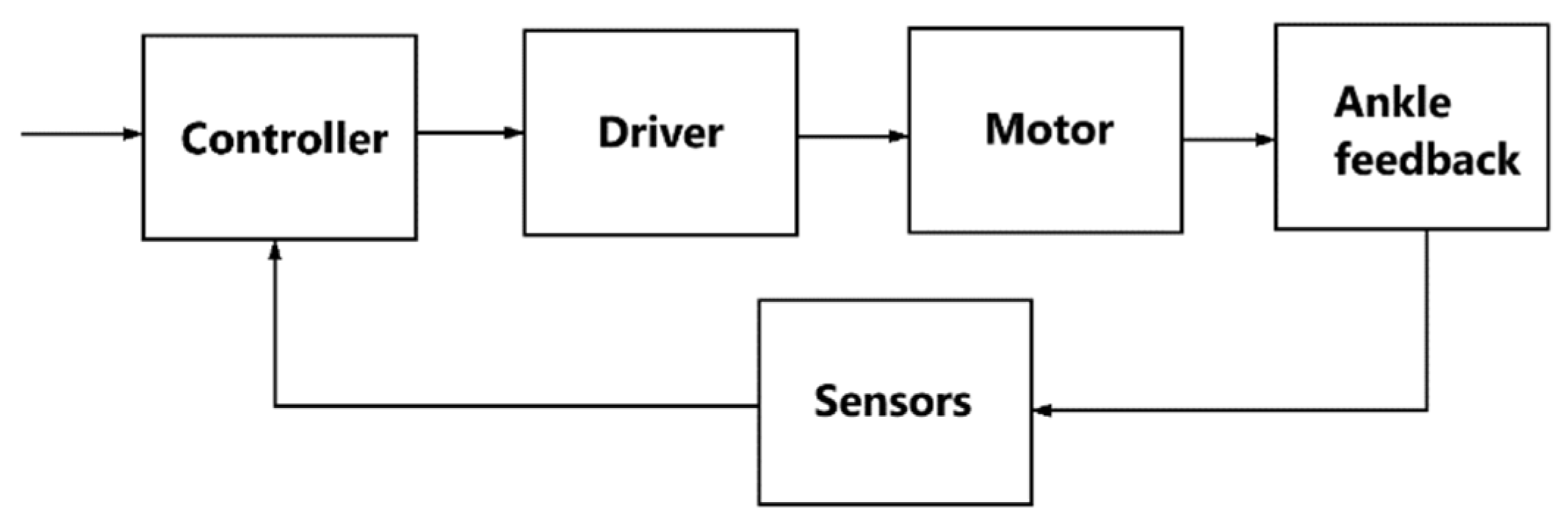
Figure 8.
Dependence of exoskeleton linear displacement on time during cyclic motion.
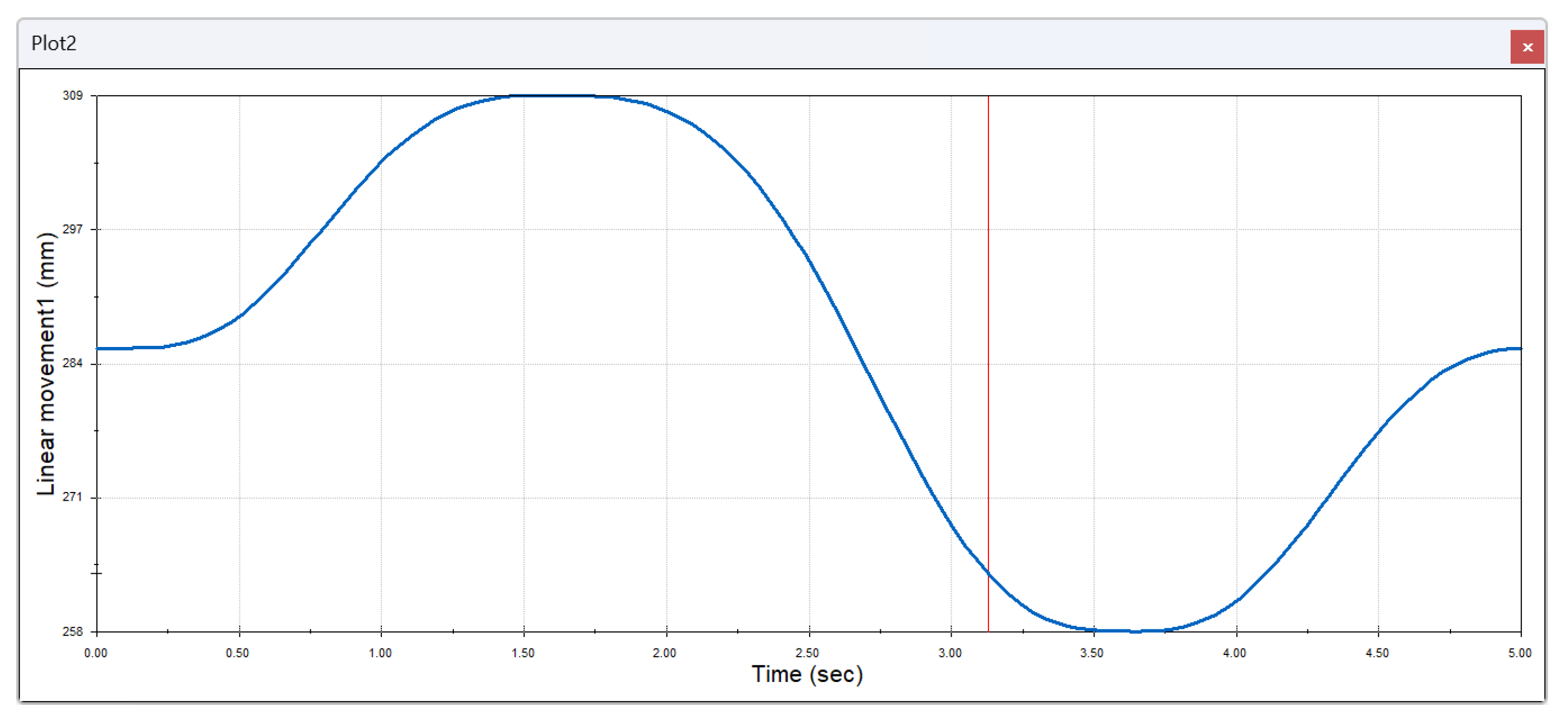
Figure 9.
Variation of exoskeleton movement velocity in time during cyclic motion.
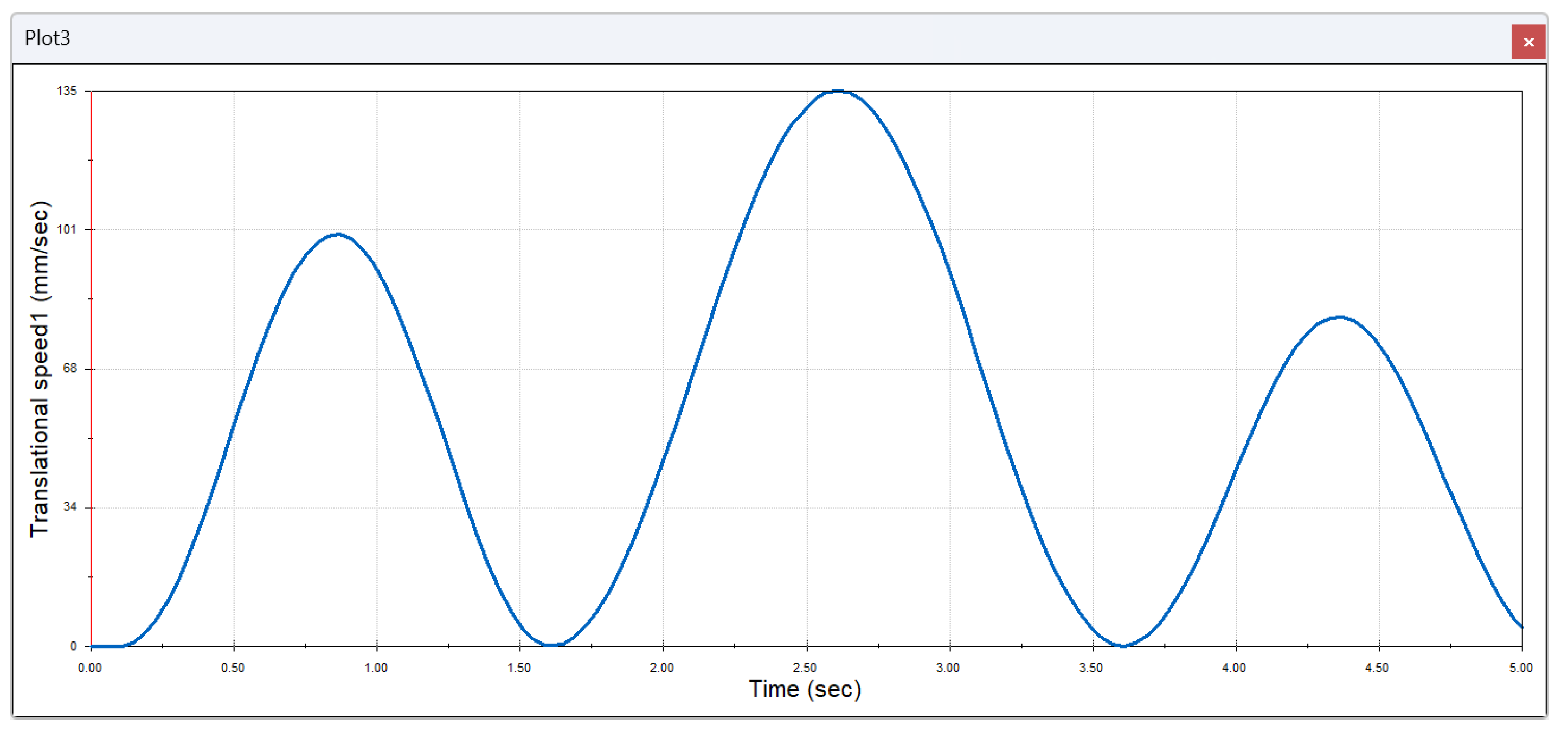
Figure 10.
Dynamics of exoskeleton angular displacement in time.
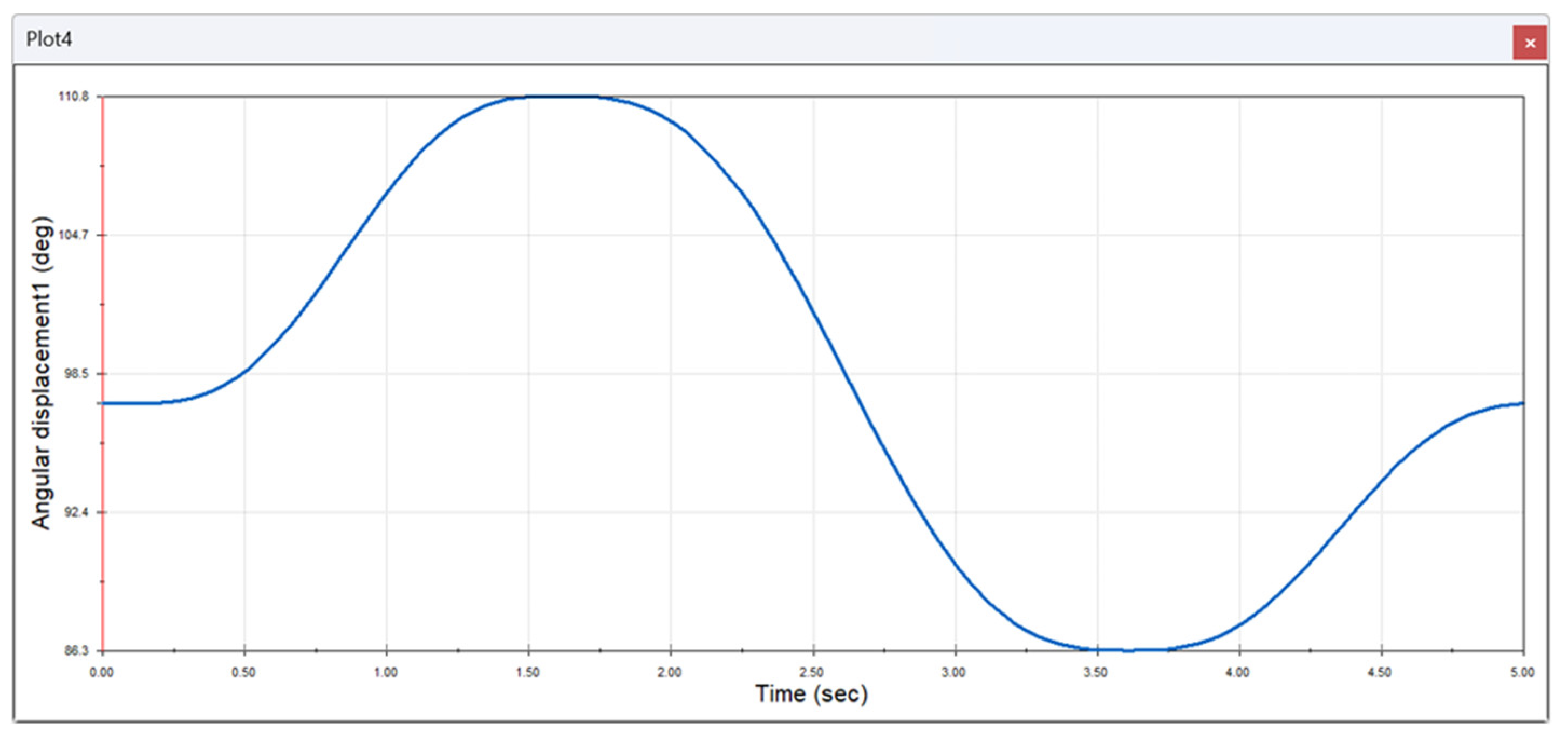
Figure 11.
Position of the exoskeleton in different phases of lateral movement of the foot.
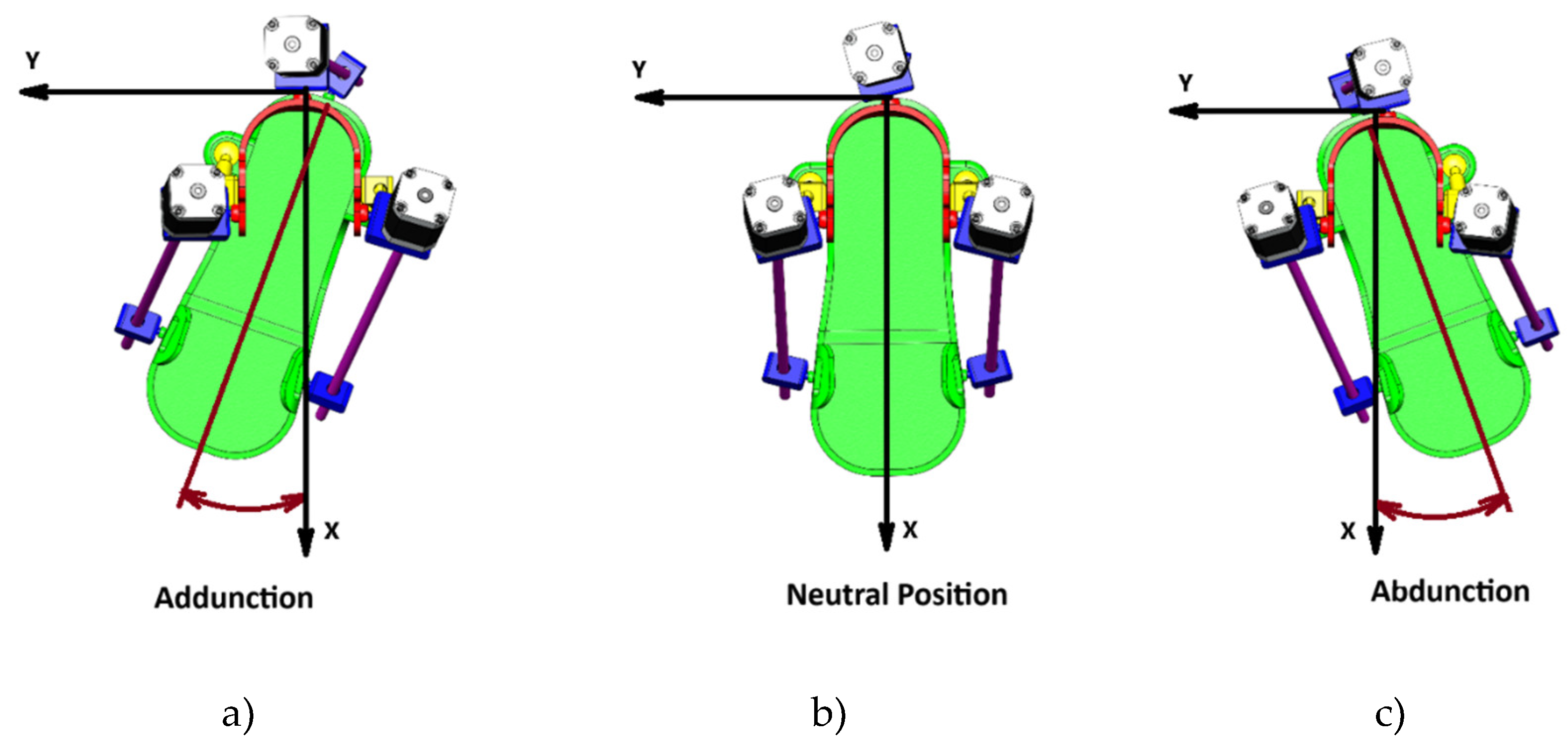
Figure 12.
The change in the torque of the second engine of the exoskeleton over time is analyzed in the following section.
Figure 12.
The change in the torque of the second engine of the exoskeleton over time is analyzed in the following section.
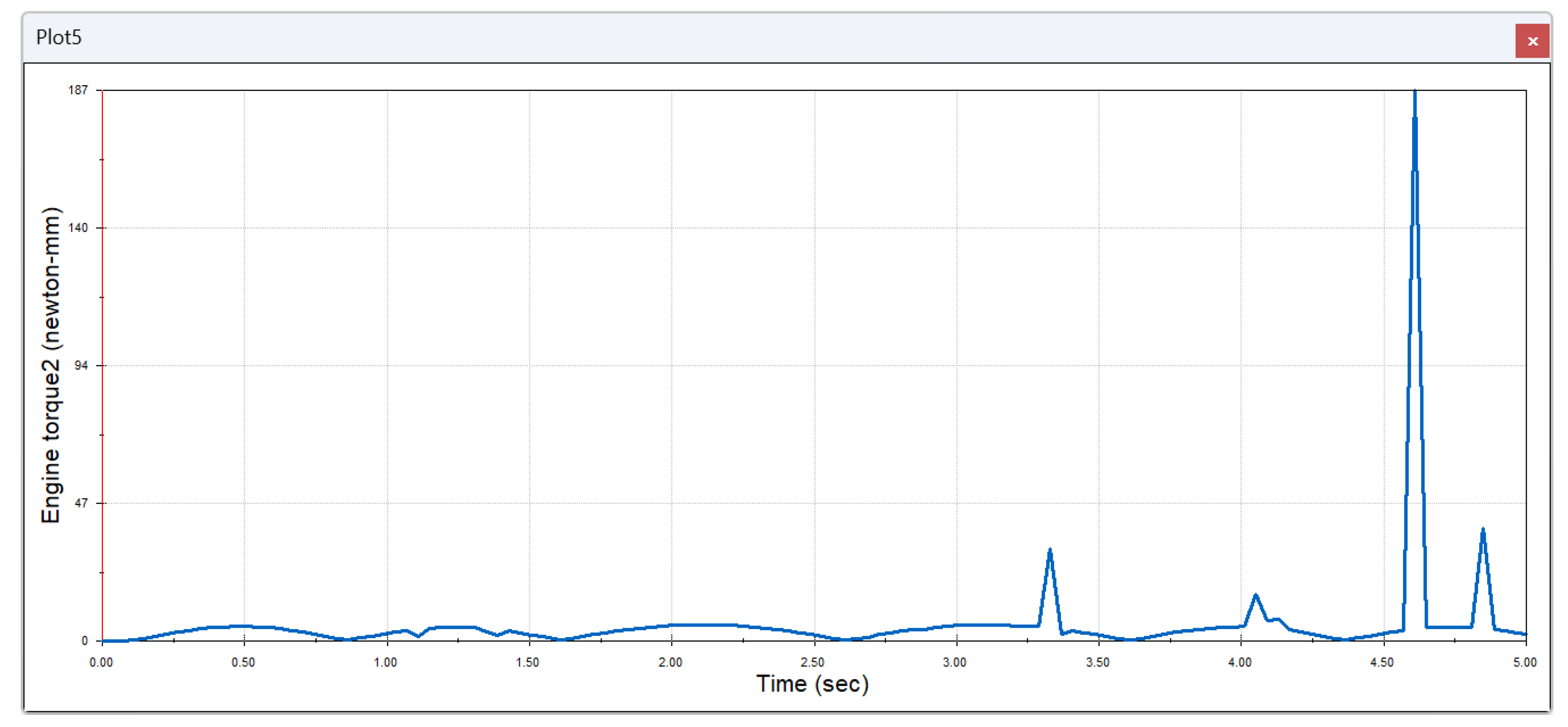
Figure 13.
Change in linear movement of the second exoskeleton component over time.
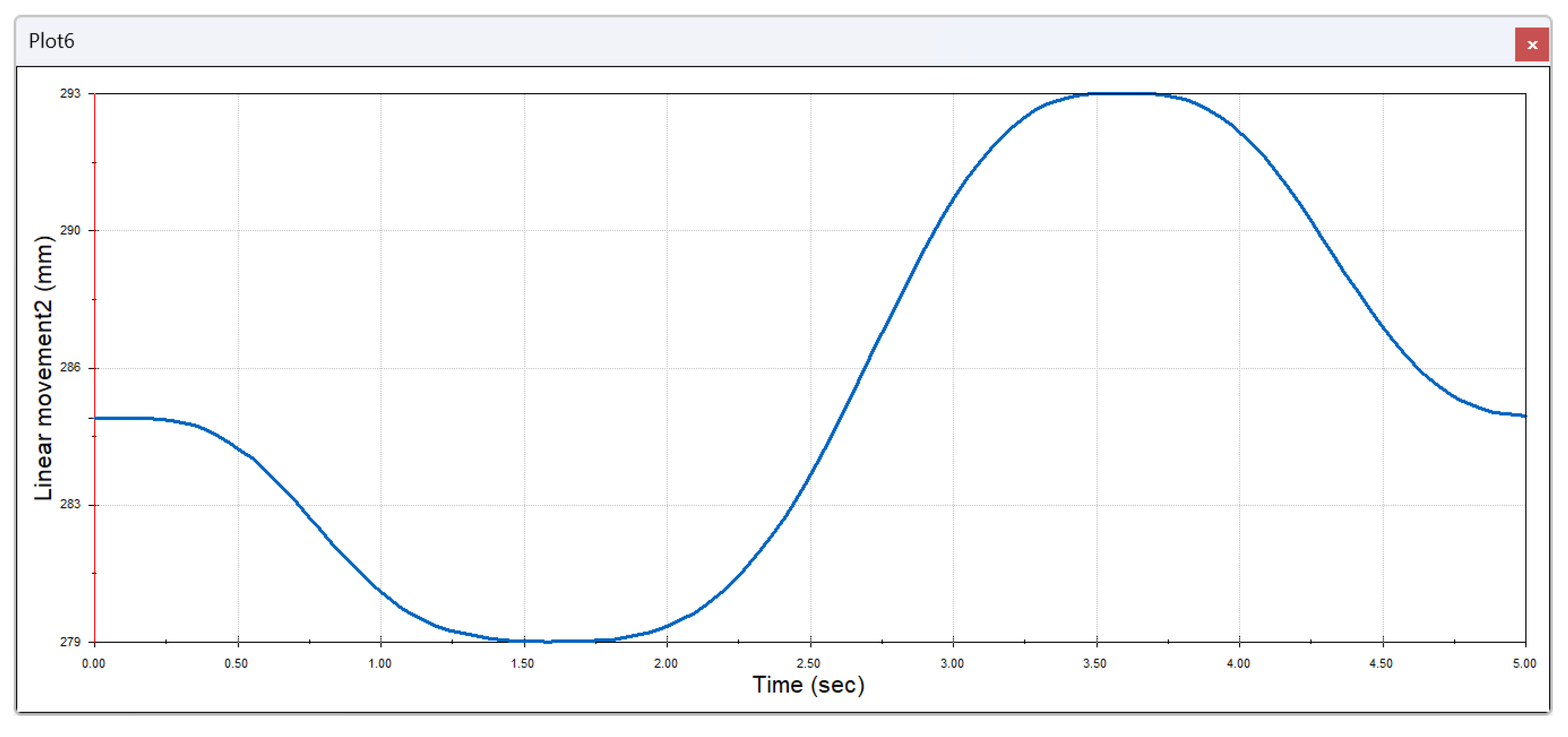
Figure 14.
Change in translational velocity of the second exoskeleton component over time.
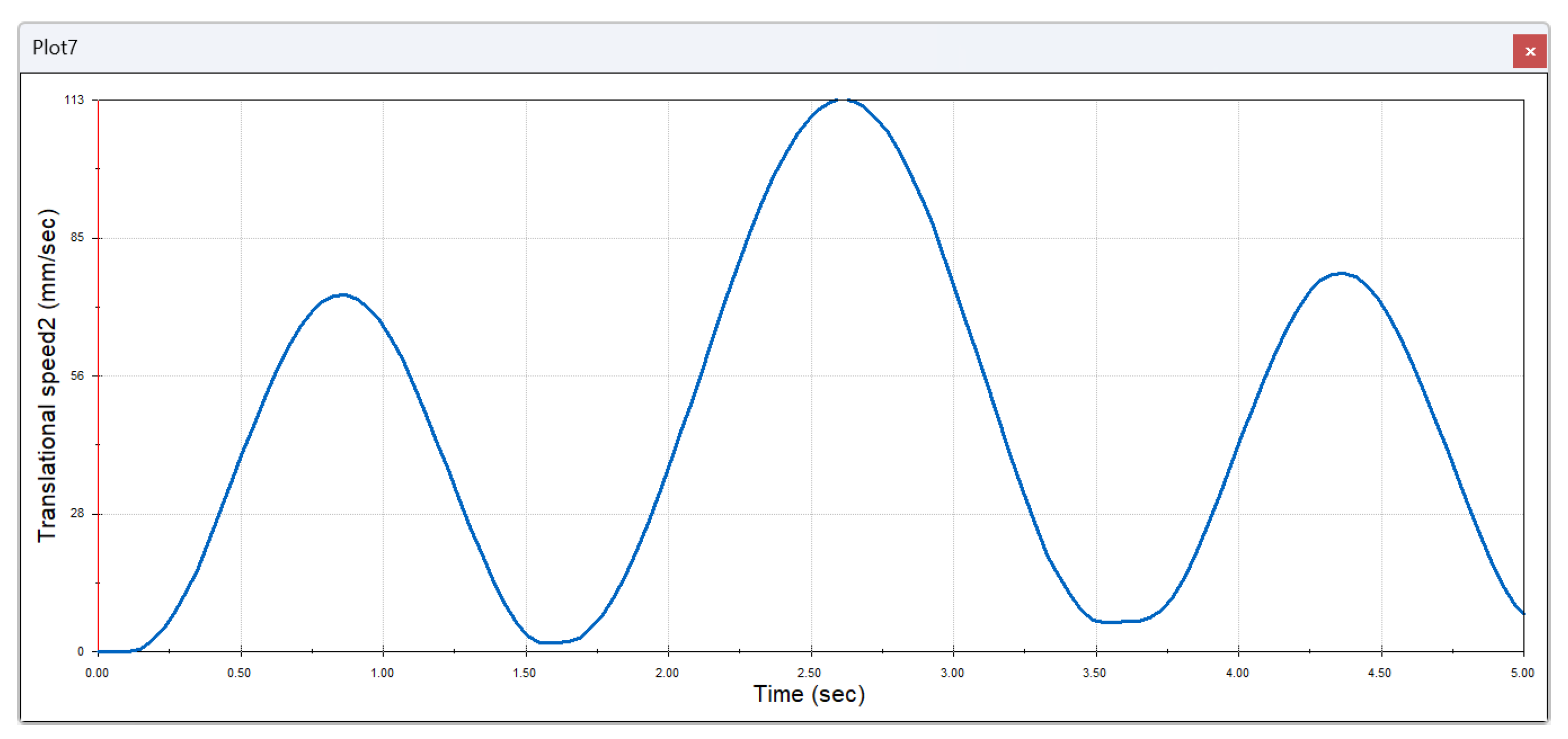
Figure 15.
Change in angular displacement of the second exoskeleton component over time.
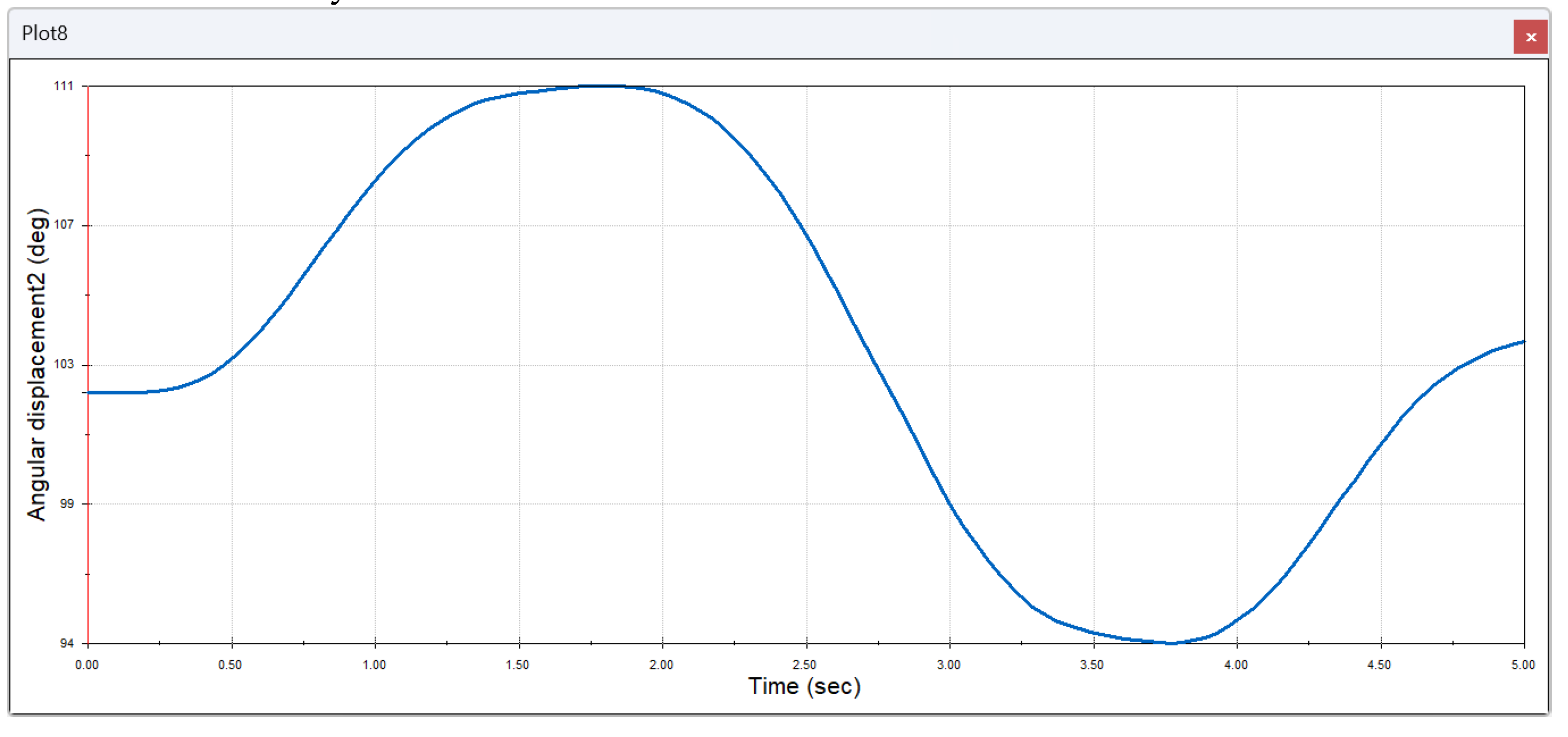
Figure 16.
Ankle exoskeleton positions: valgus (a), neutral (b), and varus (c).
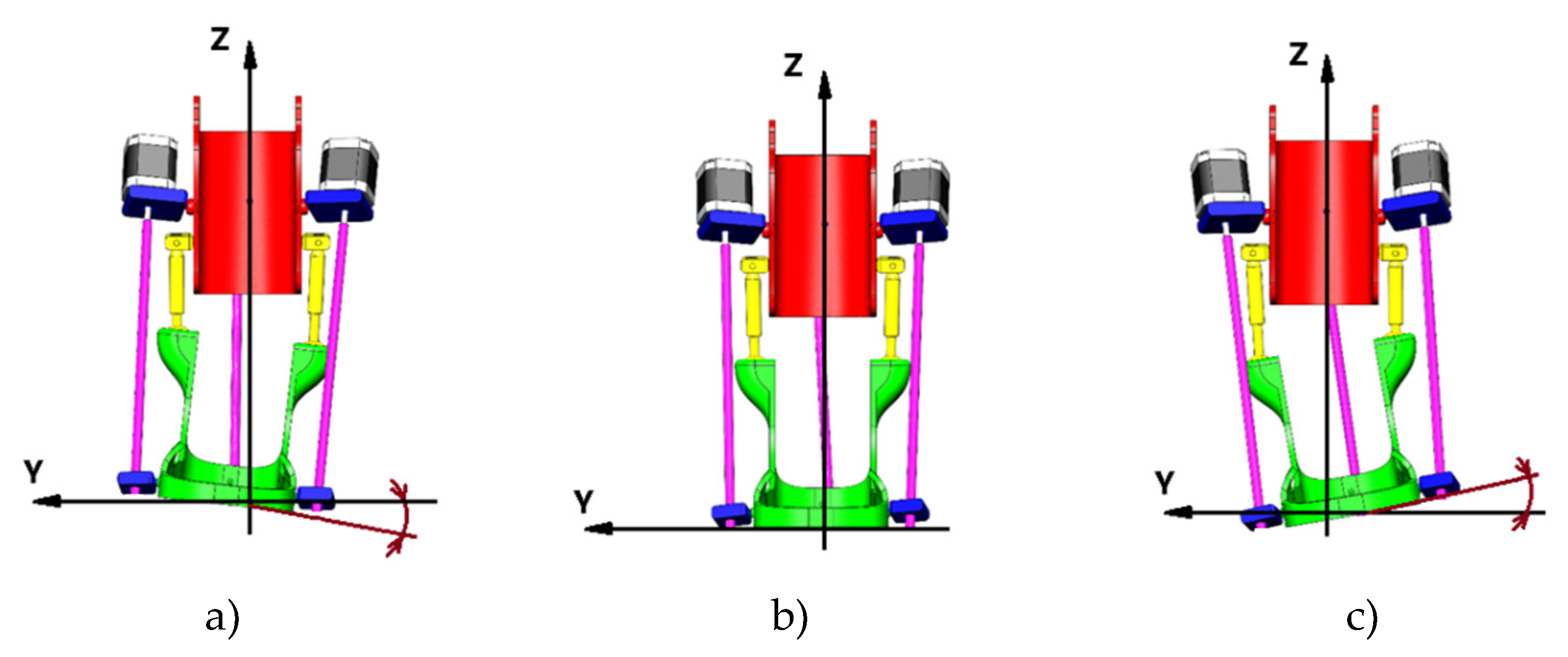
Figure 17.
Change of torque of the third drive of exoskeleton in time.
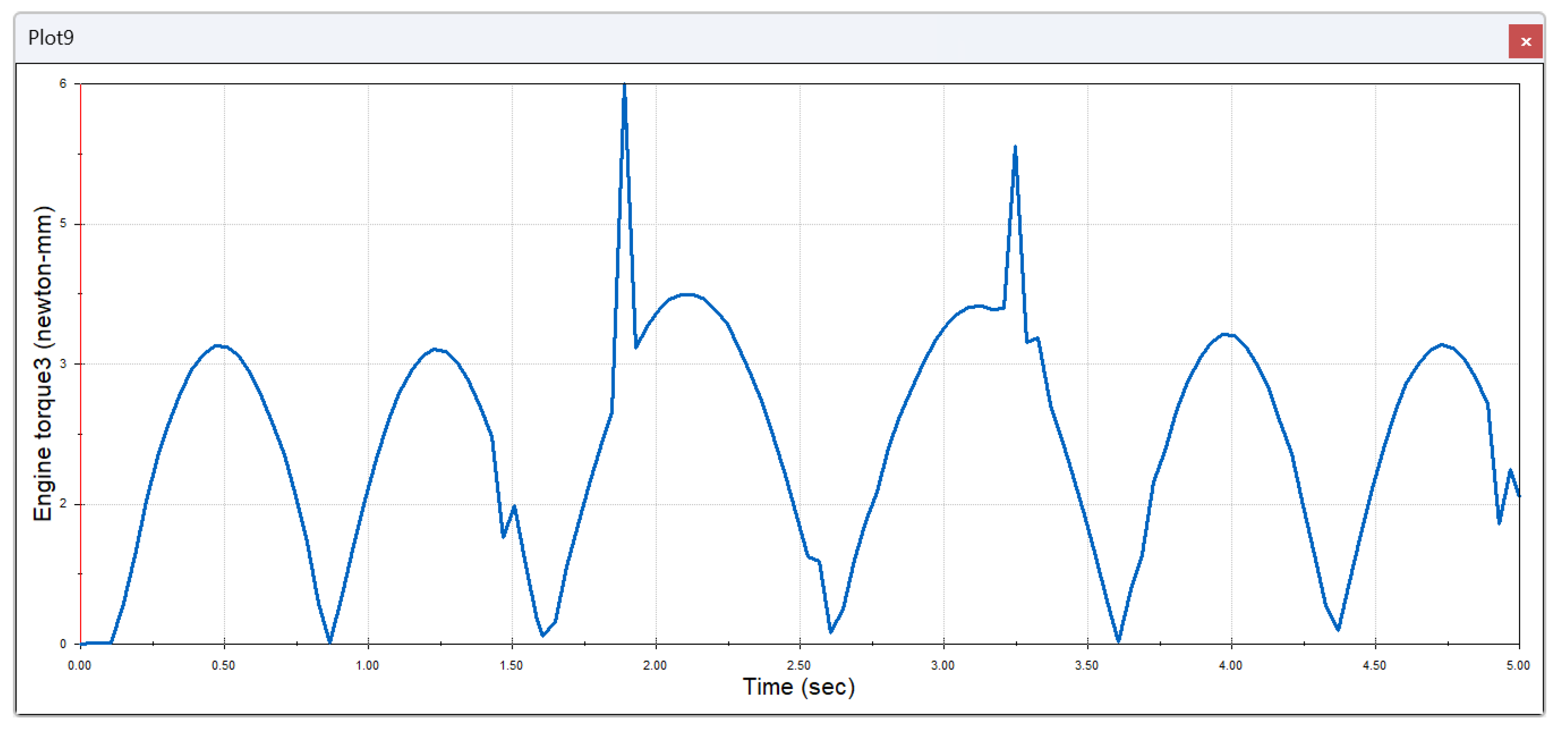
Figure 18.
Change in linear movement of the third exoskeleton component over time.
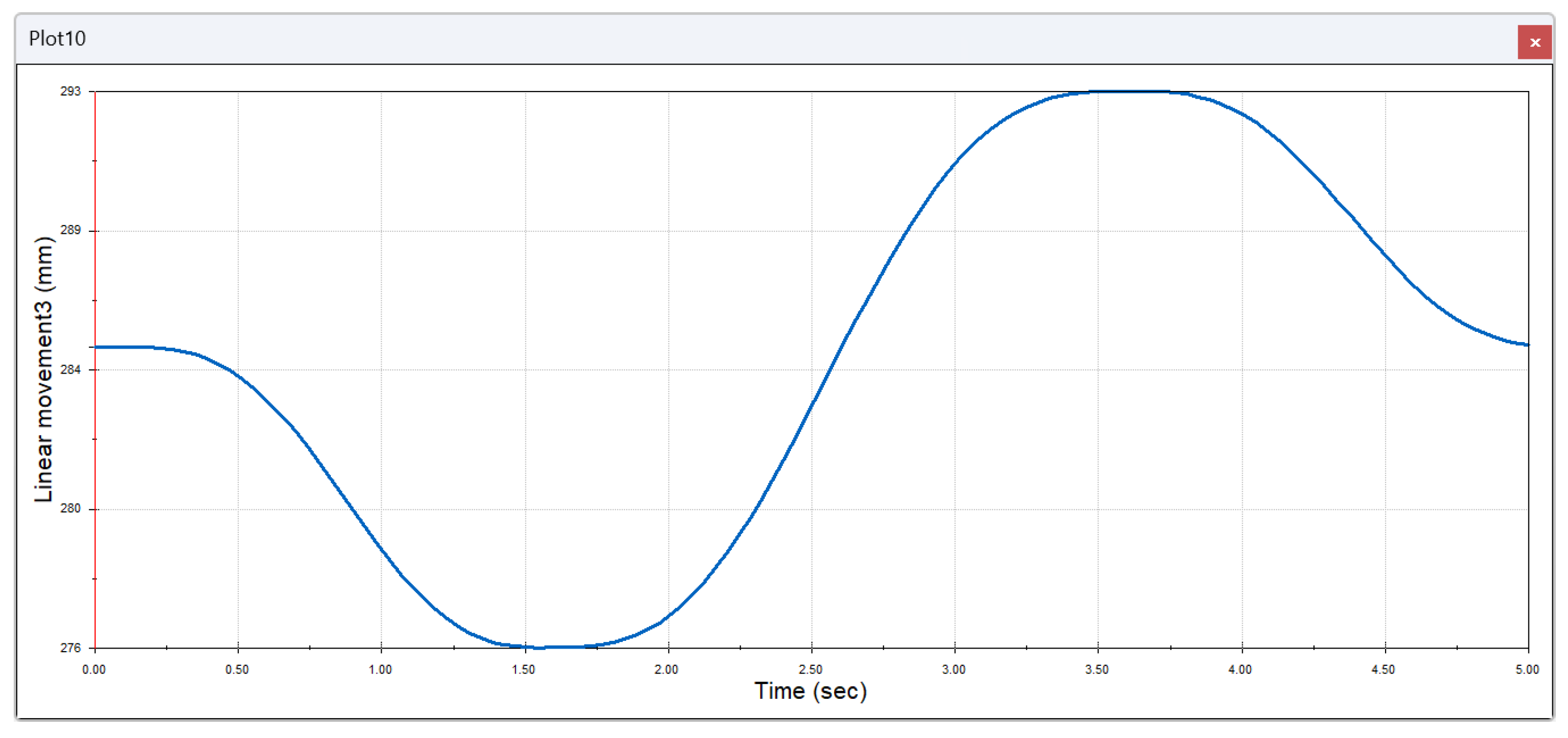
Figure 19.
Change in translational velocity of the third exoskeleton component over time.
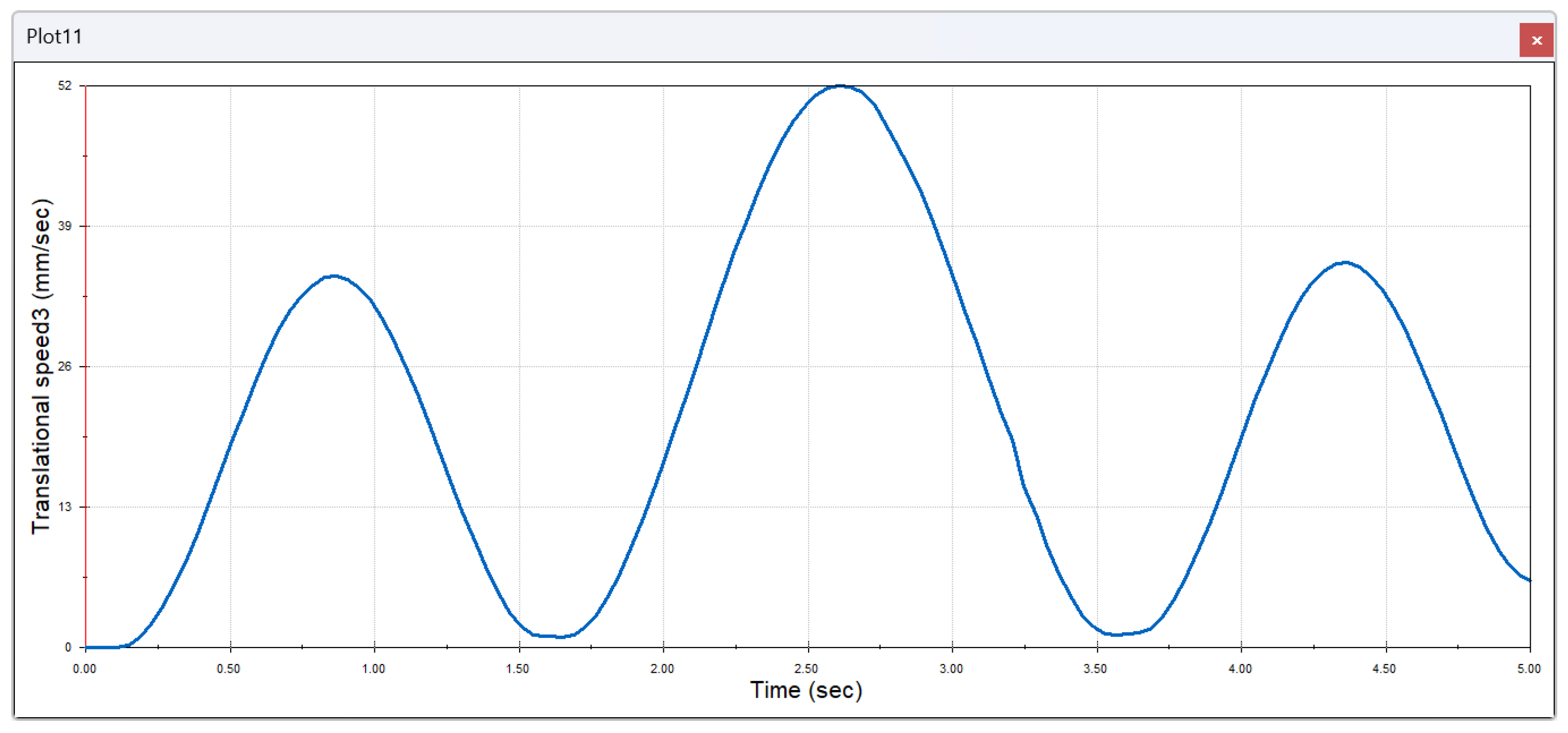
Figure 20.
Change in angular displacement of the third exoskeleton component over time.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



