
Submitted:
10 October 2024
Posted:
10 October 2024
You are already at the latest version
Abstract
Silicone mammary implants (SMIs) frequently result in capsular fibrosis, which is marked by the overproduction of fibrous tissue surrounding the implant. This review provides a detailed examination of the molecular and immunological mechanisms driving capsular fibrosis, focusing on the role of foreign body responses (FBR) and microbial biofilm formation. We investigate how microbial adhesion to implant surfaces and biofilm development contribute to persistent inflammation and fibrotic responses. The review critically evaluates antimicrobial strategies, including preoperative antiseptic protocols and antimicrobial-impregnated materials, designed to mitigate infection and biofilm-related complications. Additionally, advancements in material science, such as surface modifications and antibiotic-impregnated meshes, are discussed for their potential to reduce capsular fibrosis and prevent contracture of the capsule. By integrating molecular insights with clinical applications, this review aims to elucidate the current understanding of SMI-related fibrotic responses and highlight knowledge gaps. The synthesis of these findings aims to guide future research directions of improved antimicrobial interventions and implant materials, ultimately advancing the management of capsular fibrosis and enhancing patient outcomes.
Keywords:
silicone mammary implants (SMI)
; capsular fibrosis
; biofilm formation
; antimicrobial strategies
; foreign body response (FBR)
; implant surface modification
; microbial adhesion
; fibrotic response
; antimicrobial-impregnated materials
; surface topography
1. Introduction
The body’s natural wound-healing process plays a central role in medical implant outcomes [1], particularly in individuals receiving silicone mammary implants (SMI). When an SMI is placed, the body initiates a wound-healing response that can lead to implant encapsulation and forming a fibrous capsule around the implant, a condition known as capsular fibrosis [1,2]. While this is part of the body’s attempt to isolate the foreign object and restore tissue integrity, excessive fibrosis can result in complications such as pain, implant deformation, and reduced mobility [3,4]. Moreover, the interaction between biofilm formation on the implant surface and the wound-healing process is believed to exacerbate fibrotic responses [5]. Understanding the fundamentals of wound healing is essential for developing strategies to reduce capsular fibrosis and effectively manage biofilm dynamics in individuals undergoing SMI implantation.
1.1. Foundations of Wound Healing: Implications for Health and Recovery
Wound healing is a crucial biological process fundamental for restoring the integrity and functionality of damaged tissues. It involves a complex series of overlapping phases: hemostasis, inflammation, proliferation, and remodeling, which are aimed at repairing physical damage, preventing complications, and ensuring overall health and recovery.
Hemostasis is the initial response to tissue damage. When the skin is injured, blood vessels constrict to reduce blood loss, followed by the activation of platelets that form a clot. This clot acts as a temporary barrier against pathogens and provides a scaffold for incoming cells. Platelets release growth factors and cytokines that signal the subsequent phases of healing responses [6,7,8]. The clot is eventually reinforced by the conversion of fibrinogen into fibrin, creating a stable thrombus that aids in tissue repair [6,7,8].
The next phase, inflammation, begins shortly after hemostasis. This phase is marked by the recruitment of immune cells to the wound site to prevent infection and clear debris. Neutrophils are the first responders, arriving within the first 24 hours to combat pathogens and release enzymes that help degrade damaged tissue. They are followed by macrophages, which continue the process of debris removal and release cytokines that modulate the inflammatory response [9,10,11,12]. These cells also produce matrix metalloproteinases (MMPs) that degrade extracellular matrix (ECM) components, preparing the wound bed for new tissue formation [10,13]. Macrophages help transition from the inflammatory to the proliferative phase by resolving inflammation and releasing factors that promote tissue repair [14,15].
During the proliferative phase, new tissue is formed to restore the wound area. This includes fibroblast proliferation and ECM deposition, which provide structural support for new tissue. Fibroblasts produce collagen and other ECM components, while endothelial cells contribute to angiogenesis, forming new blood vessels to supply nutrients and oxygen to the growing tissue [16,17,18,19]. Epithelial cells migrate across the wound to re-establish the skin barrier. This phase also involves wound contraction, driven by myofibroblasts, which helps reduce the wound's surface area [20,21,22,23,24,25,26].
The final phase, remodeling, focuses on strengthening and refining the newly formed tissue. During remodeling, collagen fibers are realigned and cross-linked to enhance tensile strength. The ECM undergoes continual remodeling by MMPs and their inhibitors, leading to the maturation of the wound tissue [16,24,27,28,29,30]. This phase can last for months to years, during which time the appearance and functionality of the tissue improve as scar tissue is gradually replaced with more normal tissue architecture.
Effective wound healing is essential for repairing the skin's physical structure and preventing complications such as chronic wounds and pathological scarring, which can lead to persistent pain, impaired function, and increased healthcare costs [9,15]. By ensuring that damaged tissues are effectively repaired, wound healing reduces the risk of further tissue damage and supports the restoration of normal tissue function, ultimately improving outcomes and quality of life for patients.
A key component of wound healing is the prevention of infection. Infections are a common complication in wound care and can significantly impede the healing process, potentially leading to severe health issues [15,31,32,33]. Effective wound healing involves forming a protective barrier through coagulation and subsequent epithelialization, which helps prevent pathogen entry and supports pathogen clearance. This barrier is crucial for minimizing infection risk and promoting a safer, more rapid recovery [15,34].
Another important aspect of effective wound healing is its impact on scar formation. Optimal healing process can reduce excessive scarring, which is vital for both aesthetic and functional reasons [6,7]. Excessive scarring, including hypertrophic scars or keloids, can adversely affect the appearance and function of the repaired tissue. Minimizing scar formation enhances cosmetic outcomes and preserves skin texture and elasticity, which is particularly valuable in surgical and cosmetic procedures [35,36].
Wound healing is also essential for promoting functional recovery. Restoring normal tissue function is crucial for the recovery of movement, sensation, and overall functionality of the affected area [10,37]. In clinical settings, such as after surgery or injury, effective healing ensures that the repaired tissue regains its full functionality, which is critical for enabling patients to return to their normal activities and achieve successful rehabilitation [11].
The overall impact of wound healing extends beyond immediate repair. Chronic wounds or inadequate healing can lead to systemic complications, such as prolonged inflammation, metabolic disturbances, and increased susceptibility to further health issues [29]. Effective wound healing supports overall health by mitigating these risks and reducing the burden on the healthcare system. Promoting rapid and effective repair helps prevent the escalation of health problems and contributes to a more efficient, cost-effective healthcare approach [30].
Advancements in the molecular understanding of wound healing have significantly improved how we approach and manage wounds, leading to notable enhancements in clinical outcomes[20,38]. Key developments include the elucidation of cellular signaling pathways, such as those involving growth factors like Vascular Endothelial Growth Factor (VEGF) and Transforming Growth Factor-beta (TGF-β), as well as cytokines like Interleukin-1 (IL-1) and Tumor Necrosis Factor-alpha (TNF-α) [9,39,40,41]. During wound healing, these pathways regulate crucial processes such as cell proliferation, migration, and differentiation. Understanding these mechanisms has enabled the development of targeted therapies that modulate these pathways to improve healing outcomes.
Research into stem cells has revealed their critical role in wound repair. Mesenchymal stem cells (MSCs) and epithelial stem cells have shown the ability to differentiate into various cell types necessary for tissue regeneration and to secrete factors that promote healing [31]. These advances underscore the potential of stem cell therapies to accelerate wound repair and enhance recovery.
Further progress in understanding the molecular basis of fibrosis has illuminated how excessive scar tissue forms and persists. Key players in this process include fibroblasts, myofibroblasts, and ECM components along with their regulatory proteins [15,33,34]. This knowledge has facilitated the development of strategies to manage and mitigate excessive scar formation, improving the quality of wound healing.
Recent advancements have provided insights into the mechanisms of inflammation resolution, elucidating how the inflammatory response transitions into the proliferative phase of healing [6]. This includes understanding the roles of anti-inflammatory cytokines and the resolution of inflammatory cell infiltration, which has refined approaches to managing chronic inflammation and supporting effective tissue repair.
Genetic and epigenetic research has identified specific genes and regulatory mechanisms influencing wound healing. Changes in gene expression during various healing phases, along with epigenetic modifications affecting cell behavior, have enabled more personalized treatment approaches [7]. Tailoring interventions based on individual genetic profiles can optimize therapeutic efficacy and improve patient outcomes.
Understanding ECM composition and remodeling has also progressed, revealing how the ECM supports cell migration and tissue repair [14,35,36]. These insights have led to the development of novel biomaterials designed to mimic the natural matrix, enhancing the healing environment and promoting better wound repair.
The field has seen significant advancements with the development of biomaterials such as hydrogels, scaffolds, and nanomaterials. These materials interact with cellular and molecular processes to deliver growth factors, support cell growth, and modulate the healing environment, improving the management of complex wounds [10,11].
Molecular diagnostics and personalized medicine have advanced with the use of biomarkers and genomic profiling, enabling more tailored approaches to wound management [31,42]. This personalization allows for the customization of treatments based on genetic and molecular profiles, enhancing the efficacy of interventions and improving patient outcomes.
Finally, research into immune system interactions with wound healing processes has provided valuable insights into the roles of various immune cells in tissue repair and remodeling [14]. Understanding these interactions has improved the management of inflammatory responses and supported effective healing.
1.2. Wound Healing Dynamics, Microbial Biofilms, and Fibrotic Responses in Silicone Mammary Implants
Silicone mammary implants (SMIs) have played a pivotal role in breast surgery since their inception in the early 1960s [43]. Initially developed to meet the demand for cosmetic breast augmentation, these implants quickly became a cornerstone in reconstructive surgery for post-mastectomy patients [44].
Upon the implantation of SMIs, the body initiates an immediate wound response characterized by activation of the innate immune system. Immune cells such as neutrophils, macrophages, and dendritic cells are recruited to the site due to microbial contamination, implant shedding, silicone bleeding, and protein adsorption onto the implant surface [2,45,46,47,48,49,50]. Table 1 provides a comparative overview of these physiological mechanisms and their roles in the wound response to silicone mammary implants.
As the healing progresses, the body forms a fibrous capsule around the implant to isolate the foreign material. This involves the deposition of ECM components such as collagen, leading to the development of a fibrous capsule [46,47,49,51,52]. The extent of fibrosis around silicone mammary implants is shaped by both the initial inflammatory response and the length of chronic inflammation. Persistent inflammation, caused by continuous protein adhesion to the SMI surface and ongoing microbial infiltration, can result in excessive ECM remodeling, increased collagen deposition, and subsequent contracture of the fibrous capsule.
Microbial biofilms that form on the implant surface can persistently stimulate the immune system, leading to prolonged inflammation [53,54,55]. This persistent inflammation is a major factor contributing to excessive ECM remodeling and increased collagen deposition, which exacerbates fibrosis [50,55,56,57]. The continued presence of biofilms intensifies the inflammatory process and promotes the formation of a thick, contracted capsule, ultimately resulting in capsular contracture [58,59,60].
The impact of antimicrobial agents on fibrosis around silicone mammary implants is significant in managing and mitigating fibrotic responses. Antimicrobial treatments, including the use of antimicrobial coatings on implants and systemic antibiotics, aim to prevent or reduce microbial biofilm formation and associated chronic inflammation [61,62,63,64,65].
In examining the management of fibrosis, this review explores the intricate biological pathways involved in the formation and remodeling of fibrous capsules around SMIs. Special attention will be given to how chronic inflammation and excessive ECM remodeling contribute to fibrosis and capsular contracture.
The role of microbial transmission, particularly the formation of biofilms, will be a central focus. Biofilms on implant surfaces can lead to persistent stimulation of the immune system, resulting in prolonged inflammation and exacerbated fibrotic responses. Understanding the relationship between microbial contamination, biofilm formation, and chronic inflammation is essential for developing effective strategies to enhance implant biocompatibility and reduce complications.
Antimicrobial strategies are crucial in controlling infections and improving implant outcomes. Our work assesses current antimicrobial approaches, including antimicrobial coatings and systemic antibiotics, evaluating their effectiveness in preventing or reducing biofilm formation and managing infection. These strategies are vital for reducing the risk of complications and enhancing the long-term success of implants.
Additionally, we discuss novel antiseptic therapies, which offer new opportunities for improving wound healing and reducing infection rates. By examining recent advancements in antiseptic agents, including their mechanisms of action and clinical applications, we aim to identify innovative approaches for enhancing the safety and efficacy of silicone mammary implants.
Through a comprehensive overview of these topics, we want to provide valuable insights into the latest advancements in fibrosis management, infection prevention, and antiseptic therapies. By connecting molecular research with practical clinical applications, we aspire to improve our understanding of these critical factors and their implications in patient care.
2. From Wound to Peri-SMI Capsular Fibrosis
Fibrosis is a pathological condition characterized by the excessive accumulation of ECM components, particularly collagen, leading to scar tissue formation and impaired tissue function [2]. This process is often a consequence of chronic inflammation and injury, where normal wound-healing responses become dysregulated, resulting in persistent fibrosis [2,45,66,67].
2.1. Immediate Inflammatory Response and Early Fibrosis
Acute Inflammatory Response
Upon silicone implant placement, the body’s initial reaction involves an acute inflammatory response. The implant’s surface, whether smooth or textured, acts as a foreign body, triggering a cascade of immune responses. Macrophages are among the first responders, recognizing and attempting to engulf the silicone material. This process, often leading to impaired phagocytosis, results in prolonged inflammation [2,45]. Macrophages release a range of pro-inflammatory cytokines such as tumor necrosis factor-alpha (TNF-α), interleukin-1β (IL-1β), and interleukin-6 (IL-6), which recruit additional immune cells and activate fibroblasts [12,45,66,68,69].
Fibroblasts, in response to inflammatory cytokines, transition from a quiescent to an activated state, characterized by the secretion of matrix metalloproteinases (MMPs) and cytokines that facilitate tissue remodeling [2,66,70]. Early fibrosis begins with the accumulation of fibroblasts around the implant, contributing to the formation of a provisional matrix. This matrix, rich in collagen type III, serves as a scaffold for subsequent repair processes [52].
Early Fibrotic Changes
The transition from acute inflammation to early fibrosis is marked by the differentiation of fibroblasts into myofibroblasts [71,72], cells with contractile properties due to the expression of α-smooth muscle actin (α-SMA) [1,23,73]. These myofibroblasts are integral to the formation of the fibrous capsule, exerting mechanical forces that influence the organization of the ECM [1]. The initial fibrotic response involves a temporary increase in ECM components such as collagen and fibronectin, which are later replaced by more stable collagen types I and III as the fibrosis matures [46,74,75,76,77].
Molecular Signaling Pathways
Key signaling pathways driving early fibrosis include the transforming growth factor-beta (TGF-β) pathway, which plays a crucial role in fibroblast activation and myofibroblast differentiation [78,79,80]. TGF-β stimulates fibroblasts to produce ECM proteins and to adopt a contractile phenotype. Additionally, the nuclear factor-kappa B (NF-κB) pathway is activated in response to inflammatory cytokines, further promoting fibroblast proliferation and ECM deposition [81].
2.2. Chronic Inflammation and Capsular Contracture
Chronic Inflammatory Response
As the inflammatory response persists, chronic inflammation ensues. This phase is characterized by the continued presence of immune cells, particularly macrophages and T cells, which sustain the inflammatory milieu[45]. Macrophages in this stage often differentiate into foreign body giant cells (FBGCs), which are involved in chronic inflammation and fibrosis [69,82,83,84]. Pro-inflammatory cytokines such as TNF-α and IL-1β continue to drive fibroblast activity and ECM deposition[71,72].
Capsular Contracture Formation
The progression to capsular contracture involves a shift from initial fibrosis to a more organized and denser fibrous capsule. This process is marked by increased collagen deposition, particularly collagen type I, and the development of a rigid fibrotic capsule around the implant [76,85]. The contractile activity of myofibroblasts, driven by sustained TGF-β signaling [40,79], contributes significantly to capsule contraction and rigidity [23,29,86].
The Baker classification system, which assesses the severity of capsular contracture, reflects the extent of fibrotic encapsulation and its impact on implant aesthetics and function [87,88,89]. This system categorizes capsular contracture into four distinct grades, reflecting the degree of fibrous tissue formation around the implant and its impact on both the aesthetics and functionality of the breast. In Grade I, the breast appears soft and natural, indicating minimal to no contracture. Grade II describes a breast that is slightly firm but still looks normal, suggesting some fibrous encapsulation is present. Moving to Grade III, the breast becomes firm and may appear abnormal, indicating a significant degree of contracture that can affect the shape and overall appearance. Finally, Grade IV signifies a hard breast with a distorted implant, reflecting severe capsular contracture that often necessitates surgical intervention [87,88,89].
Molecular Signaling Pathways
In chronic inflammation, the persistent activation of TGF-β and NF-κB pathways continues to drive fibroblast activity and ECM remodeling [40,78,79,91]. TGF-β signaling enhances the synthesis of collagen and other ECM proteins [78,79], while NF-κB promotes the expression of inflammatory cytokines and ECM-degrading enzymes like MMPs [81,92]. The interplay between these pathways results in a fibrotic environment that sustains capsule formation and contracture.
Immune Cell Interactions
T cells, particularly CD4+ T helper cells, play a crucial role in chronic inflammation[93]. A predominance of T helper 2 (Th2) and T helper 17 (Th17) cells is associated with increased fibrosis, as these cells secrete cytokines that promote fibrotic responses [94,95]. Regulatory T cells (Tregs) also influence fibrosis, with their presence often inversely proportional to the severity of capsular contracture [93,96,97]. Tregs can modulate the immune response and influence the fibrotic process, though their role can be complex and context-dependent[47].
S100 Proteins on Inflammation and Fibrosis
S100 proteins are a family of calcium-binding proteins that are implicated in various inflammatory and fibrotic processes[98,99,100]. They are involved in regulating cell motility, differentiation, and inflammatory responses [99,100]. S100A8 and S100A9, for instance, are released by activated macrophages and are known to participate in the inflammatory response by promoting neutrophil chemotaxis and activating other inflammatory cells [100,101].
In the context of silicone implants, S100 proteins can contribute to the pathogenesis of capsular fibrosis. Elevated levels of S100A8 and S100A9 have been associated with chronic inflammation and fibrosis in various tissues, including those surrounding implants [46,47,101]. These proteins interact with receptor RAGE (receptor for advanced glycation end-products) on immune cells, modulating cytokine release and fibroblast activation [101,102]. Their presence in the fibrotic capsule can exacerbate inflammatory responses and promote fibroblast proliferation and ECM deposition, thereby influencing the severity of capsular fibrosis [100].
Figure 1 illustrates the complex sequence of events leading from the immediate inflammatory response to the development of fibrosis and eventual capsular contracture following SMI insertion. This figure emphasizes how initial acute inflammation, triggered by tissue damage and the immune system's response to the foreign body, progresses to chronic inflammation and fibrosis. Over time, these processes contribute to the formation of a dense, fibrotic capsule around the implant, characterized by increased ECM deposition and the activation of fibroblasts and myofibroblasts, ultimately leading to capsular contracture.
2.3. Immediate and Chronic Inflammatory Triggers Following SMI Insertion
Immediate Post-Implantation Response
Upon the insertion of silicone mammary implants (SMIs), the body mounts an acute inflammatory response (Figure 2a) [2,45,46,47,50,103,104]. This is initiated by factors such as tissue damage, contamination by the skin microbiome, and the introduction of damage-associated molecular patterns (DAMPs) and pathogen-associated molecular patterns (PAMPs) [54,55,105]. The immune system rapidly activates, recruiting immune cells like neutrophils and macrophages to clear the damaged tissue and manage the initial microbial contamination [50,55,57,105]. Additionally, microparticulate silicone may shed from the implant, migrating into surrounding tissues and exacerbating the inflammatory response. Microbial attachment to the implant surface, along with the adsorption of wound proteins, triggers further immune activation [50,105]. Inflammatory mediators such as monocyte chemoattractant protein-1 (MCP-1), collagen types I and III (COL1/3), and cellular adhesion markers like CD44 accumulate at the wound site, amplifying the acute response and setting the stage for potential fibrosis [46,50].
Early-Stage Fibrosis (Months Post-Implantation)
As the healing process continues (Figure 2b), a persistent inflammatory state emerges [2,45]. Biofilms can develop on the implant surface, contributing to chronic inflammation due to the ongoing presence of microbial species and their adhesion to the implant [50,105]. This chronic inflammation drives the activation of pro-inflammatory and pro-fibrotic pathways, with these factors becoming incorporated into the developing fibrotic tissue around the implant [46,47]. Over time, the extracellular matrix (ECM) undergoes significant remodeling, marked by the deposition of proteins such as vimentin, decorin, and fibronectin [2,45]. These changes contribute to the formation of a dense fibrotic capsule that surrounds the implant, which is further infiltrated by microbial species, perpetuating the chronic inflammatory state [50]. Ultimately, this sustained inflammation and ECM remodeling lead to the development of capsular fibrosis and contracture around the implant [48,56,58,59,60,106].
2.4. Influence of Surface Characteristics on Inflammation and Fibrotic Pathways
Surface Texture and Inflammation
The surface characteristics of silicone implants, such as texture and roughness, significantly influence the inflammatory and fibrotic responses. Textured surfaces tend to provoke a more robust inflammatory response compared to smooth surfaces. Studies have shown that rougher surfaces increase immune cell activation and cytokine secretion, contributing to heightened fibrosis and contracture [47,50,103,104,107].
Surface texture affects fibroblast behavior, including their attachment, proliferation, and differentiation [104]. Textured surfaces often lead to more pronounced fibroblast activation and increased collagen deposition, while smoother surfaces can result in less severe fibrotic responses [47,104] . This variation in fibrosis is linked to differences in cytokine profiles and immune cell interactions, with rougher surfaces promoting a more aggressive inflammatory environment [47].
Surface Characteristics and Cellular Responses
The impact of implant surface characteristics on cellular responses is mediated through various molecular signaling pathways. For instance, rougher surfaces may enhance the activation of NF-κB and TGF-β pathways, leading to increased fibroblast activity and ECM deposition [47]. Surface roughness also influences macrophage polarization, with smoother surfaces promoting an anti-inflammatory M2 macrophage phenotype and rougher surfaces favoring a pro-inflammatory M1 phenotype [47,108,109].
3. Microbial Adhesion, Colonization, and Biofilm Formation on SMI
Despite rigorous adherence to sterilization and disinfection protocols [110,111,112,113], SMIs can become sites for microbial adhesion, colonization, and biofilm formation. This occurs despite the inert nature of silicone, which itself lacks antimicrobial properties[114]. The body’s immune response to these implants plays a crucial role in managing microbial threats, but it also inadvertently contributes to a conducive environment for bacterial colonization, particularly when biofilms are formed on the implant surface [53,54,55,59,60,115,116].
3.1. Microbial Transmission and Surface Adhesion
During surgical implantation, SMIs may become contaminated through various pathways, including skin microbiota, operating room environments, or surgical instruments. Staphylococcal species, particularly Staphylococcus epidermidis, are commonly implicated due to their ubiquitous presence on human skin and the bacterial ability to adhere to the implant surface [50,58,59]. Once these microbes come into contact with the SMI surface, especially during the acute wound phase (24–120 hours post-operation), they begin the process of adhesion, which is influenced by the surface characteristics of the implant [50].
Surface topography is a critical determinant of microbial adhesion. Rougher surfaces, characterized by higher surface roughness (average roughness Ra 60 µm), provide more surface area and microenvironments conducive to bacterial adherence [50,117]. This is particularly evident in studies where rougher SMI surfaces attracted more bacteria, including S. epidermidis, and facilitated thicker biofilm growth compared to smoother surfaces [50,106,118,119,120,121,122]. The initial phase of microbial adhesion involves reversible attachment, where bacteria adhere to the implant surface through weak van der Waals forces and hydrophobic interactions[123,124]. If conditions are favorable, this progresses to irreversible attachment, where bacteria anchor themselves more securely, often using surface appendages like pili or fimbriae [54,117].
3.2. Colonization and Biofilm Formation
Following successful adhesion, the bacteria begin to proliferate and secrete extracellular polymeric substances (EPS), forming a biofilm [54,117]. Biofilms are complex, structured communities of bacteria encased in a self-produced matrix of EPS, including polysaccharides, proteins, and DNA [54,55,125,126]. This matrix helps bacteria adhere more securely to the implant surface and provides protection from the host immune system and antibiotic treatments [54,125,126,127,128]. Biofilm formation is a key factor in the persistence of bacterial infections associated with SMIs, as bacteria within a biofilm can be up to 1,000 times more resistant to antibiotics than their planktonic (free-floating) counterparts [54,125].
Figure 3 illustrates the sequence of events from initial microbial adhesion to biofilm development, ultimately leading to capsular contracture. The transfer of skin microbiota during implant placement, early bacterial colonization, biofilm formation, and the resulting fibrous capsule formation are critical steps in the pathogenesis of implant-associated infections and complications.
The biofilm development on SMIs is particularly concerning because it can lead to chronic infections that are difficult to detect and treat [53,55,56,57,58,60,116,129]. For example, subclinical infections associated with S. epidermidis are often asymptomatic but can result in significant complications such as capsular contracture[58,59,130,131]. The chronic nature of these infections is partly due to the immune system’s inability to effectively clear biofilms, as the protective EPS matrix inhibits the penetration of immune cells and antimicrobial peptides (AMPs) [50,59].
4. Reducing Capsular Contracture: Antimicrobial Strategies in Breast Implant Surgery
Sterilization and disinfection are crucial components of infection control in healthcare settings, forming the bedrock of patient and healthcare personnel safety [110]. In hospital environments, a multitude of surgical and invasive procedures are performed daily, which inherently introduces the risk of pathogen transmission. The improper sterilization or disinfection of medical instruments can result in severe infection risks, including the transmission of hepatitis B and environmental pathogens [132,133,134,135,136]. To mitigate these risks, healthcare facilities must employ effective decontamination methods for medical devices. Healthcare providers are pivotal in implementing these procedures to reduce and eliminate potential infections [112]. Establishing specific sterilization and disinfection guidelines based on the intended use of medical devices and associated infection risks is mandatory [110]. Given the rise of newly emerging and multidrug-resistant pathogens in healthcare centers, medical professionals need to possess a thorough understanding of these techniques to prevent the spread of infections. The International Organization of Standardization has set standardized definitions and criteria for sterilization, disinfection, and cleaning, with initial guidelines established in 2004 and subsequently updated in 2010 [111,113].
As shown in Figure 2, strategies for reducing capsular contracture in breast implant surgery emphasize the importance of infection control, including sterilization and the use of antimicrobial agents like chlorhexidine gluconate to minimize bacterial contamination. These approaches, combined with surgical techniques like the no-touch method and postoperative care protocols, play a critical role in preventing biofilm formation and ensuring better surgical outcomes.
4.1. Antimicrobial Approaches to Mitigate Postoperative Infections and Biofilm Formation
In the context of aesthetic breast surgery, there has been a noted increase in the rate of postoperative surgical site infections (SSIs). The most commonly identified bacteria in these infections include Staphylococcus epidermidis, Staphylococcus aureus, Escherichia coli, Pseudomonas aeruginosa, Propionibacterium acnes, and Corynebacterium species [59,65,137,138,139]. Preoperative skin antiseptics play a critical role in reducing these postoperative complications. While povidone-iodine and other antimicrobial irrigations have been effective in reducing these complications [140], chlorhexidine gluconate has demonstrated superior efficacy in minimizing biofilm-related capsular contracture compared to povidone-iodine [116].
The relationship between bacterial contamination and implant-related complications was first elucidated by Burkhardt et al. in 1986, highlighting the significant impact of local antimicrobial agents in reducing the incidence of capsular contracture in retromammary implants [141]. Betadine pocket irrigation was once the standard practice for preventing such complications [142]; however, in 2000, the FDA contraindicated its use, prompting the adoption of alternative solutions such as triple antibiotic solution (TAS) [143]. TAS has since been associated with a substantially lower rate of capsular contracture in patients undergoing breast augmentation [57,144,145,146,147]. Although TAS is widely favored, some studies suggest that betadine-containing irrigations may be more effective in certain contexts [146,148].
The timing and duration of irrigation solutions have also been revisited, with evidence suggesting that prolonged exposure times may enhance their efficacy [149,150,151,152]. Surveys conducted among members of the American Society of Plastic Surgeons (ASPS) have highlighted the use of 0.1% polyhexanide as a preferred antimicrobial agent during breast augmentation pocket irrigation. This trend underscores its recognition within the plastic surgery community for its effectiveness in reducing bacterial contamination associated with breast prostheses. Nevertheless, there remains significant variability in the antimicrobial techniques and agents preferred by ASPS members, emphasizing the need for standardized guidelines in breast pocket irrigation and implant soaking.
Recent studies have further examined the anti-biofilm efficacy of various irrigation solutions, comparing hypochlorous acid (HOCl), polyhexanide (Lavasorb®), and octenidine-dihydrochloride/phenoxyethanol using an innovative in-vitro human plasma biofilm model [62]. Their findings revealed that hypochlorous solutions were less effective in eradicating biofilms compared to polyhexanide and octenidine-dihydrochloride/phenoxyethanol, suggesting that HOCl may not be suitable for standalone biofilm eradication [62].
Despite these advances in understanding and technique, staphylococci remain the most common microorganisms in the axillary flora, and antibiotics targeting these bacteria have not significantly impacted the incidence of SSIs [153]. Furthermore, preoperative antibiotic prophylaxis has not markedly reduced SSIs in breast cancer surgery [154,155]. Patient compliance is also critical, as noncompliance with medication regimens can double the risk of infection following breast surgery [156].
The routine application of antimicrobial pocket irrigation, the use of implant soaking agents, and various preventative strategies have been shown to collectively reduce the rates of capsular contracture [157]. However, despite the well-documented association between bacterial contamination and surgical complications, there remains a conspicuous lack of universally accepted, evidence-based guidelines for antimicrobial breast pocket irrigation and perioperative antibiotic administration. Furthermore, the literature provides conflicting evidence regarding the effectiveness of various pocket irrigation solutions, such as HOCl [158], and there is ongoing debate about the role of systemic antibiotics in preventing surgical site infections (SSI), with some studies suggesting a limited impact.
In conclusion, while significant progress has been made in understanding and addressing SSIs and capsular contracture in breast surgery, there remains a critical need for consensus on antimicrobial practices. The establishment of evidence-based guidelines for antimicrobial irrigation in implant-based breast surgery is essential to optimize patient outcomes and reduce the incidence of complications related to bacterial contamination.
4.2. Surgical Techniques for Minimizing Bacterial Contamination
During SMI implantation, minimizing bacterial contamination is crucial for reducing complications such as biofilm-associated fibrotic capsule formation [151,159,160,161]. Effective preoperative preparation plays a vital role in this process. Using electric clippers for hair removal instead of razors minimizes microabrasions and the risk of introducing bacteria into the surgical field [162].
During the surgical procedure, employing a no-touch technique is essential for minimizing the risk of contamination [163]. Devices like Keller funnels facilitate this approach by ensuring that implants are handled in a sterile manner, reducing the chance of bacterial exposure [163].
The technique of implant insertion also plays a significant role in controlling contamination [164]. Using sterile funnels or sleeves during the insertion process limits the implant’s contact with non-sterile surfaces, further reducing bacterial exposure [163,165]. Additionally, the choice of surgical incision is important; the inframammary incision is favored over the periareolar approach due to its lower infection rates and better control over implant exposure to contaminants [164,165,166,167].
Postoperative care is equally critical in minimizing contamination risks. Proper wound care, including keeping the surgical site clean and monitoring for signs of infection, is essential to prevent complications [138,148].
In summary, the choice of surgical incision and careful postoperative care further contribute to minimizing contamination risks and ensuring optimal outcomes.
5. Advances in Implant-Shell-Material and Non-Pharmacological Strategies to Prevent Biofilm-Associated Fibrosis
Fibrotic capsule formation around implanted biomaterials, including breast implants, is a significant clinical issue associated with biofilm formation and microbial colonization. This chapter reviews non-pharmacological strategies that target microbial inhibition and biofilm prevention to mitigate fibrotic responses from a molecular and immunological standpoint.
5.1. Physical Modifications with Antimicrobial Properties
Polyurethane Foam Coatings
Early efforts to modify implant surfaces involved the application of polyurethane foam coatings, which were designed to disrupt the formation of fibrotic tissue by altering the implant's surface characteristics[168,169,170]. Although initial studies indicated a reduction in fibrotic capsule formation, the widespread use of these coatings was curtailed due to concerns over the release of degradation products such as 2,4-toluene diamine, which raised potential toxicity issues [171]. Despite these concerns, newer iterations of polyurethane-coated implants are being investigated for their ability to control microbial adhesion and biofilm formation [169,170,172].
Influence of Surface Topography on Biofilm Dynamics
Surface roughness of SMIs plays a significant role in biofilm formation [106,119]. Implants with rougher surfaces (Ra 60 µm) have been shown to not only attract more bacteria but also support the development of thicker and more mature biofilms compared to smoother implants (Ra 4 µm) [50]. The increased surface area and micro-topographical features of rough implants provide niches that protect bacteria from shear forces and immune surveillance, allowing them to establish robust biofilms [173].
In vitro studies have further demonstrated that SMI surface texture directly influences bacterial behavior. Both Staphylococcus aureus and S. epidermidis, common culprits in implant-related infections, show increased adhesion and biofilm formation on rougher SMI surfaces[50,173]. This is corroborated by electron microscopy, which reveals that biofilms on rough surfaces are more complex and structured than those on smoother surfaces [50,54,55,57,125].
The implications of this are significant for clinical outcomes. Rougher SMIs are more likely to harbor biofilms, which can lead to persistent infections, chronic inflammation, and increased rates of capsular contracture [48,59,106,174]. Moreover, the association between textured implants and breast implant-associated anaplastic large cell lymphoma (BIA-ALCL) is thought to be related to the enhanced likelihood of biofilm formation on these surfaces, which may trigger chronic immune responses and, in some cases, contribute to tumorigenesis [48,174].
5.2. Biological Matrices with Antimicrobial Properties
Antibiotic-Impregnated Meshes
Synthetic and biological matrices impregnated with antibiotics represent a proactive approach to managing microbial contamination [175]. Antibiotic-impregnated meshes, containing agents like minocycline and rifampicin, have been shown to significantly reduce bacterial colonization and biofilm formation around implants [176]. This strategy mitigates the inflammatory and fibrotic responses associated with microbial biofilms by providing sustained antimicrobial activity at the implant site [5,177]. The effectiveness of these meshes highlights the critical role of localized antibiotic delivery in controlling fibrotic reactions.
Spider Silk-Based Meshes
Recent advancements include the development of spider silk-based meshes, which leverage the unique properties of spider silk proteins to enhance biocompatibility and reduce biofilm formation [178,179,180,181,182]. These meshes act as barriers to protein and bacterial adhesion, thereby decreasing the risk of fibrotic capsule formation [178,180,182,183,184]. Studies have demonstrated that spider silk-based meshes can inhibit fibroblast proliferation and collagen deposition, which are key processes in fibrotic tissue formation [184]. This approach underscores the potential of biomimetic materials in managing fibrotic responses.
Zwitterionic Polymers
Zwitterionic polymers, characterized by their dual cationic and anionic properties, exhibit superior hydrophilicity and resistance to protein adsorption [185]. These properties make zwitterionic polymers effective in preventing microbial adhesion and biofilm formation [186] Research has shown that zwitterionic hydrogels can prevent the formation of fibrotic capsules by reducing the FBR in animal models [185,187,188,189,190]. The ability of these polymers to resist protein fouling and microbial colonization suggests a promising avenue for mitigating fibrotic responses [189].
6. Pharmacological Strategies to Prevent Biofilm-Associated Fibrosis in Implants
Biofilm-associated fibrosis around implants is a significant clinical challenge, primarily due to microbial infections and the subsequent fibrotic response. This chapter reviews pharmacological strategies with antimicrobial properties aimed at mitigating biofilm-associated fibrosis around implants, focusing on mechanisms of action, drug classes, and specific agents demonstrating efficacy.
6.1. Antibacterial Drugs
Antibacterial drugs play a crucial role in preventing biofilm formation and associated fibrosis. These drugs can be administered in various forms, including systemic, topical, or incorporated into the implant material itself.
Systemic Antibacterials
Systemic antibiotics such as cefazolin and gentamicin are commonly used as prophylactic measures before and during surgery. While cefazolin, a first-generation cephalosporin, is recognized for its effectiveness in reducing infections associated with breast implants [191,192], gentamicin, an aminoglycoside, also demonstrates broad-spectrum activity against both gram-positive and gram-negative bacteria, including those commonly involved in implant infections [191,192]. However, the overall impact of these antibiotics on surgical site infection (SSI) rates continues to be a subject of debate in the literature.
Topical Antibacterials
Topical antibiotics, including bacitracin and chlorhexidine gluconate, are applied directly to the implant or the surgical site. Bacitracin, a peptide antibiotic, is effective against gram-positive bacteria and is used in irrigation solutions to reduce bacterial load [191,193,194,195]. Chlorhexidine gluconate, an antiseptic with broad-spectrum antimicrobial activity, has shown efficacy in reducing microbial contamination and biofilm formation on implant surfaces [196].
Drug Incorporation into Implants
Incorporating antibiotics into the implant material itself can provide sustained antimicrobial effects. Rifampin, a macrocyclic antibiotic, has been incorporated into implant surfaces, showing effectiveness in reducing bacterial colonization and subsequent fibrosis [197]. This approach allows for localized drug delivery, potentially reducing the need for systemic antibiotics and minimizing adverse effects.
6.2. Antifibrotic and Anti-Inflammatory Drugs
Fibrosis, a major consequence of chronic inflammation and infection, can be targeted with antifibrotic and anti-inflammatory drugs.
Pirfenidone
Pirfenidone is an antifibrotic drug with established efficacy in treating idiopathic pulmonary fibrosis. It works by reducing the production of inflammatory mediators and fibroblast proliferation. In preclinical models, pirfenidone administration reduced capsule thickness and fibroblast proliferation around implants [198,199,200,201]. This drug may prove beneficial in mitigating fibrotic responses associated with biofilm infections.
Halofuginone
Halofuginone, originally developed for veterinary use, inhibits collagen type I synthesis and the differentiation of T helper 17 cells. When grafted onto the surface of silicone implants, halofuginone significantly decreased capsule thickness and FBR in animal models [202,203,204,205]. This agent's antifibrotic properties make it a promising candidate for controlling fibrosis related to biofilm infections [206].
Dexamethasone
Dexamethasone, a potent glucocorticoid, reduces inflammation and collagen production by modulating cytokine activity [207]. Its application in implant surgery has been shown to decrease fibrous tissue formation [193,207,208]. The intravenous administration of dexamethasone during the perioperative period may help regulate inflammation and fibrosis surrounding implants, potentially enhancing outcomes for patients susceptible to biofilm-associated fibrosis [193].
6.3. Integration of Antimicrobial Strategies
Effective management of biofilm-associated fibrosis often requires a combination of antimicrobial and antifibrotic approaches. For example, preoperative prophylactic antibiotics combined with local antiseptic irrigation can significantly reduce the risk of infection and biofilm formation[206]. Furthermore, while there is potential in incorporating antifibrotic agents into the implant material or using them adjunctively with antimicrobial strategies to enhance overall efficacy in preventing fibrosis, it is important to note that these strategies have primarily been demonstrated in preclinical and animal studies. There is currently insufficient evidence to support their routine application in clinical practice. [206].
To address biofilm-associated fibrosis around SMI, significant progress has been made through both, material-based and pharmacological strategies. Non-pharmacological approaches, including physical modifications with antimicrobial properties (such as polyurethane coatings and surface topography adjustments) and innovative biological matrices (like antibiotic-impregnated meshes and spider silk-based materials), focus on preventing microbial adhesion and biofilm formation. Concurrently, pharmacological interventions involving systemic and topical antibacterials, as well as antifibrotic agents, provide targeted solutions to manage both infection and fibrosis. The integration of these strategies, as detailed in Table 2, underscores the multifaceted approach needed to effectively mitigate fibrotic responses and improve clinical outcomes related to implant-associated complications.
7. Clinical Implications and Future Directions
The clinical implications of microbial adhesion, colonization, and biofilm formation on SMIs are extensive, influencing both patient outcomes and the effectiveness of treatment strategies. Understanding these processes from a molecular and immunological perspective is crucial for developing improved preventive and therapeutic measures.
Biofilm formation on SMIs is a significant concern due to its impact on implant longevity and patient health. Biofilms, which consist of microorganisms embedded in a self-produced extracellular matrix, offer protection from both host immune responses and antimicrobial treatments [54,125]. This persistent biofilm can lead to chronic inflammation and fibrosis, complicating implant-related conditions. Persistent biofilms exacerbate inflammatory responses, as the biofilm matrix hinders immune cell infiltration and the effectiveness of antimicrobial peptides [54,55,125]. This chronic inflammation often results in a thick fibrous capsule around the implant, potentially leading to complications such as chronic pain, impaired function, and implant failure [53,55,58].
Current strategies to manage these issues include preoperative antimicrobial prophylaxis, antimicrobial coatings, and advanced materials designed to reduce microbial adhesion and biofilm formation. However, the effectiveness of antimicrobial strategies remains limited due to the rise of antimicrobial resistance and variability in clinical practices [57,59,116]. The challenge of biofilm-associated infections underscores the need for more innovative and effective approaches to prevent and manage these complications.
Recent advances in material science and pharmacology offer promising solutions. Antibiotic-impregnated meshes and spider silk-based meshes represent significant progress in preventing microbial adhesion and biofilm formation [175,178]. These materials provide sustained antimicrobial activity or reduce bacterial adhesion through physical and chemical modifications. Additionally, zwitterionic polymers, known for their resistance to protein adsorption and microbial colonization, show potential in mitigating fibrotic responses [185,187]. The integration of antifibrotic and anti-inflammatory agents, such as pirfenidone, halofuginone, and dexamethasone, either incorporated into implant materials or used as adjunctive therapies, further enhances the management of biofilm-associated complications [198,202,207]. These agents can modulate the inflammatory response and reduce fibrosis, offering a targeted approach to managing complications.
Looking forward, several key areas warrant further exploration. Developing targeted antimicrobial strategies that effectively penetrate and disrupt biofilms is crucial. Novel drug delivery systems, such as nanoparticles or localized drug reservoirs, could enhance the efficacy of antimicrobial treatments [197]. Additionally, exploring biomimetic and smart materials that can dynamically respond to microbial threats represents an exciting frontier. These materials could release antimicrobial agents in response to biofilm formation or alter their properties to prevent microbial adhesion [178,185].
Personalized medicine approaches also hold significant promise. Tailoring antimicrobial and antifibrotic treatments based on individual patient factors, such as microbial flora, immune responses, and genetic predispositions, could greatly improve clinical outcomes [198,202]. Moreover, establishing standardized clinical guidelines for antimicrobial prophylaxis, implant coatings, and antifibrotic treatments is essential. Such guidelines would help ensure consistent and effective management of biofilm-associated complications across clinical settings. Ongoing research and clinical trials will be instrumental in developing these guidelines and optimizing patient care [57,59,116].
In summary (Table 3), while advances in understanding microbial contamination and biofilm formation on SMIs have led to improved management strategies, there remains a need for continued innovation and research. By focusing on targeted antimicrobial strategies, exploring novel materials, and standardizing clinical practices, we can enhance patient outcomes and address the challenges associated with biofilm formation and fibrosis.
8. Conclusions
The exploration of microbial adhesion, colonization, and biofilm formation on SMIs highlights a critical area of concern in both the molecular and clinical realms. The persistent challenge of biofilm-associated infections underscores the complexity of managing implant-related complications and the need for continued innovation in both material science and therapeutic strategies.
Biofilm formation on SMIs represents a multifaceted issue, with significant implications for patient health and implant longevity. The inherent protective properties of biofilms, which shield bacteria from both immune responses and antimicrobial treatments, contribute to the chronic nature of infections and the difficulty of eradicating these microbial communities. The extracellular polymeric substances (EPS) that form part of the biofilm matrix play a crucial role in this persistence, effectively hindering the penetration of immune cells and antimicrobial agents. This results in prolonged inflammation and fibrosis, complicating implant-related conditions and impacting patient outcomes.
Recent advancements in material science, such as the development of antimicrobial coatings, antibiotic-impregnated meshes, and spider silk-based materials, offer promising solutions to mitigate biofilm formation and reduce microbial colonization. These innovations aim to enhance the effectiveness of SMIs by either preventing bacterial adhesion or providing sustained antimicrobial activity. Zwitterionic polymers, with their resistance to protein fouling, represent another promising avenue for reducing microbial colonization and associated fibrosis. Incorporating antifibrotic and anti-inflammatory agents into implant materials or using them as adjunctive therapies further supports the management of biofilm-associated complications, providing targeted approaches to control inflammation and fibrosis.
Despite these advancements, several challenges remain. The rise of antimicrobial resistance and variability in clinical practices underscore the need for more effective and standardized approaches to antimicrobial prophylaxis and implant management. The development of targeted drug delivery systems and personalized medicine strategies could significantly improve the efficacy of treatments by tailoring interventions to individual patient factors and specific microbial threats. Additionally, establishing evidence-based guidelines for antimicrobial prophylaxis, implant coatings, and antifibrotic treatments is essential for ensuring consistent and effective management across clinical settings.
Future research should focus on several key areas: enhancing our understanding of biofilm dynamics and microbial interactions with implant surfaces, developing innovative materials that dynamically respond to microbial threats, and optimizing personalized treatment strategies. Continued investigation into novel materials and therapeutic approaches will be instrumental in addressing the challenges associated with biofilm formation and fibrosis. Clinical trials and ongoing research will play a crucial role in refining these strategies and improving patient outcomes.
In conclusion, while significant progress has been made in understanding and addressing microbial contamination and biofilm formation on SMIs, there remains a critical need for continued innovation and research. By focusing on targeted antimicrobial strategies, exploring advanced materials, and establishing standardized clinical practices, we can improve the management of implant-related complications and enhance patient care. The integration of molecular insights with practical clinical approaches will be key to overcoming the challenges posed by biofilm-associated infections and ensuring the long-term success of medical implants.
Author Contributions
Writing—original draft preparation, I.S..; writing—review and editing, M.L. D.C.C.-H., A.A., A.I., S.S., and D.W.; data curation, I.S.; visualization, I.S.; supervision, I.S.. D.W. acquired funding. All authors have read and agreed to the published version of the manuscript.
Funding
Research on this project was funded by Establishment Labs, Costa Rica (ID D152500-015-015) to D.W.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest
References
- Noskovicova, N.; Hinz, B.; Pakshir, P. Implant Fibrosis and the Underappreciated Role of Myofibroblasts in the Foreign Body Reaction. Cells 2021, 10, 1794. [Google Scholar] [CrossRef]
- Wick, G.; Grundtman, C.; Mayerl, C.; Wimpissinger, T.-F.; Feichtinger, J.; Zelger, B.; Sgonc, R.; Wolfram, D. The Immunology of Fibrosis. Annu. Rev. Immunol. 2013, 31, 107–135. [Google Scholar] [CrossRef]
- Wynn, T.A.; Ramalingam, T.R. Mechanisms of fibrosis: therapeutic translation for fibrotic disease. Nat. Med. 2012, 18, 1028–1040. [Google Scholar] [CrossRef] [PubMed]
- Safran, T.; Nepon, H.; Chu, C.K.; Winocour, S.; Murphy, A.M.; Davison, P.G.; Dionisopolos, T.; Vorstenbosch, J. Current Concepts in Capsular Contracture: Pathophysiology, Prevention, and Management. Semin. Plast. Surg. 2021, 35, 189–197. [Google Scholar] [CrossRef] [PubMed]
- Kadirvelu, L.; Sivaramalingam, S.S.; Jothivel, D.; Chithiraiselvan, D.D.; Govindarajan, D.K.; Kandaswamy, K. A review on antimicrobial strategies in mitigating biofilm-associated infections on medical implants. Curr. Res. Microb. Sci. 2024, 6, 100231. [Google Scholar] [CrossRef] [PubMed]
- Pool, J. G. 1977. Normal hemostatic mechanisms: a review. The American journal of medical technology 43.
- Furie, Bruce, and Barbara C Furie. 2008. Mechanisms of thrombus formation. Mechanisms of Disease. The New England journal of medicine 359.
- Locatelli, L.; Colciago, A.; Castiglioni, S.; Maier, J.A. Platelets in Wound Healing: What Happens in Space? Front. Bioeng. Biotechnol. 2021, 9. [Google Scholar] [CrossRef]
- Rodrigues, M.; Kosaric, N.; Bonham, C.A.; Gurtner, G.C. Wound Healing: A Cellular Perspective. Physiol. Rev. 2019, 99, 665–706. [Google Scholar] [CrossRef]
- Su, Y.; Richmond, A. Chemokine Regulation of Neutrophil Infiltration of Skin Wounds. Adv. Wound Care 2015, 4, 631–640. [Google Scholar] [CrossRef]
- He, L.; Marneros, A.G. Macrophages Are Essential for the Early Wound Healing Response and the Formation of a Fibrovascular Scar. Am. J. Pathol. 2013, 182, 2407–2417. [Google Scholar] [CrossRef]
- Koh, T.J.; DiPietro, L.A. Inflammation and wound healing: the role of the macrophage. Expert Rev. Mol. Med. 2011, 13, e23. [Google Scholar] [CrossRef]
- Namas, R.A.; Mi, Q.; Namas, R.; Almahmoud, K.; Zaaqoq, A.M.; Abdul-Malak, O.; Azhar, N.; Day, J.; Abboud, A.; Zamora, R.; et al. Insights into the Role of Chemokines, Damage-Associated Molecular Patterns, and Lymphocyte-Derived Mediators from Computational Models of Trauma-Induced Inflammation. Antioxidants Redox Signal. 2015, 23, 1370–1387. [Google Scholar] [CrossRef] [PubMed]
- Galli, S.J.; Borregaard, N.; Wynn, T.A. Phenotypic and functional plasticity of cells of innate immunity: macrophages, mast cells and neutrophils. Nat. Immunol. 2011, 12, 1035–1044. [Google Scholar] [CrossRef]
- Wilkinson, H.N.; Hardman, M.J. Wound healing: cellular mechanisms and pathological outcomes. Open Biol. 2020, 10. [Google Scholar] [CrossRef] [PubMed]
- Gurtner, G.C.; Werner, S.; Barrandon, Y.; Longaker, M.T. Wound repair and regeneration. Nature 2008, 453, 314–321. [Google Scholar] [CrossRef]
- Eilken, H.M.; Adams, R.H. Dynamics of endothelial cell behavior in sprouting angiogenesis. Curr. Opin. Cell Biol. 2010, 22, 617–625. [Google Scholar] [CrossRef]
- Tonnesen, M.G.; Feng, X.; Clark, R.A. Angiogenesis in Wound Healing. J. Investig. Dermatol. Symp. Proc. 2000, 5, 40–46. [Google Scholar] [CrossRef]
- Li, J.; Zhang, Y.; Kirsner, R.S. Angiogenesis in wound repair: Angiogenic growth factors and the extracellular matrix. Microsc. Res. Tech. 2002, 60, 107–114. [Google Scholar] [CrossRef]
- Mascharak, S.; Desjardins-Park, H.E.; Longaker, M.T. Fibroblast Heterogeneity in Wound Healing: Hurdles to Clinical Translation. Trends Mol. Med. 2020, 26, 1101–1106. [Google Scholar] [CrossRef]
- Kohan, M.; Muro, A.F.; White, E.S.; Berkman, N. EDA-containing cellular fibronectin induces fibroblast differentiation through binding to α4β7integrin receptor and MAPK/Erk 1/2-dependent signaling. FASEB J. 2010, 24, 4503–4512. [Google Scholar] [CrossRef] [PubMed]
- Serini, G.; Bochaton-Piallat, M.-L.; Ropraz, P.; Geinoz, A.; Borsi, L.; Zardi, L.; Gabbiani, G. The Fibronectin Domain ED-A Is Crucial for Myofibroblastic Phenotype Induction by Transforming Growth Factor-β1. J. Cell Biol. 1998, 142, 873–881. [Google Scholar] [CrossRef]
- Shinde, A.V.; Humeres, C.; Frangogiannis, N.G. The role of α-smooth muscle actin in fibroblast-mediated matrix contraction and remodeling. Biochim. et Biophys. Acta (BBA) - Mol. Basis Dis. 2016, 1863, 298–309. [Google Scholar] [CrossRef] [PubMed]
- Darby, I.A.; Laverdet, B.; Bonté, F.; Desmouliere, A. Fibroblasts and myofibroblasts in wound healing. Clin. Cosmet. Investig. Dermatol. 2014, 7, 301–311. [Google Scholar] [CrossRef] [PubMed]
- Thulabandu, V.; Chen, D.; Atit, R.P. Dermal fibroblast in cutaneous development and healing. Wiley Interdiscip. Rev. Dev. Biol. 2017, 7. [Google Scholar] [CrossRef] [PubMed]
- P. , B. Wound healing and the role of fibroblasts. J. Wound Care 2013, 22, 407–412. [Google Scholar] [CrossRef] [PubMed]
- Pakshir, P.; Noskovicova, N.; Lodyga, M.; Son, D.O.; Schuster, R.; Goodwin, A.; Karvonen, H.; Hinz, B. The myofibroblast at a glance. J. Cell Sci. 2020, 133. [Google Scholar] [CrossRef]
- Hinz, B. The role of myofibroblasts in wound healing. Curr. Res. Transl. Med. 2016, 64, 171–177. [Google Scholar] [CrossRef]
- Hinz, B.; McCulloch, C.A.; Coelho, N.M. Mechanical regulation of myofibroblast phenoconversion and collagen contraction. Exp. Cell Res. 2019, 379, 119–128. [Google Scholar] [CrossRef]
- Klingberg, F.; Hinz, B.; White, E.S. The myofibroblast matrix: implications for tissue repair and fibrosis. J. Pathol. 2012, 229, 298–309. [Google Scholar] [CrossRef]
- Lindley, L.E.; Stojadinovic, O.; Pastar, I.; Tomic-Canic, M. Biology and Biomarkers for Wound Healing. Plast. Reconstr. Surg. 2016, 138, 18S–28S. [Google Scholar] [CrossRef]
- Hartman, E.; Wallblom, K.; van der Plas, M.J.A.; Petrlova, J.; Cai, J.; Saleh, K.; Kjellström, S.; Schmidtchen, A. Bioinformatic Analysis of the Wound Peptidome Reveals Potential Biomarkers and Antimicrobial Peptides. Front. Immunol. 2021, 11. [Google Scholar] [CrossRef]
- Han, G.; Ceilley, R. Chronic Wound Healing: A Review of Current Management and Treatments. Adv. Ther. 2017, 34, 599–610. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, A.C.D.O.; Costa, T.F.; de Araújo Andrade, Z.; Medrado, A.R.A.P. Wound Healing—A Literature Review. An. Bras. Dermatol. 2016, 91, 614–620. [Google Scholar] [CrossRef] [PubMed]
- Ng, M.F. The role of mast cells in wound healing. Int. Wound J. 2010, 7, 55–61. [Google Scholar] [CrossRef]
- Komi, D.E.A.; Khomtchouk, K.; Santa Maria, P.L. A Review of the Contribution of Mast Cells in Wound Healing: Involved Molecular and Cellular Mechanisms. Clin. Rev. Allergy Immunol. 2020, 58, 298–312. [Google Scholar] [CrossRef] [PubMed]
- Jiang, D.; Rinkevich, Y. Scars or Regeneration?—Dermal Fibroblasts as Drivers of Diverse Skin Wound Responses. Int. J. Mol. Sci. 2020, 21, 617. [Google Scholar] [CrossRef]
- Cohen, I.K. Lessons from the history of wound healing. Clin. Dermatol. 2007, 25, 3–8. [Google Scholar] [CrossRef]
- Li, H.; Cai, E.; Cheng, H.; Ye, X.; Ma, R.; Zhu, H.; Chang, X. FGA Controls VEGFA Secretion to Promote Angiogenesis by Activating the VEGFR2-FAK Signalling Pathway. Front. Endocrinol. 2022, 13, 791860. [Google Scholar] [CrossRef]
- Margadant, C.; Sonnenberg, A. Integrin–TGF-β crosstalk in fibrosis, cancer and wound healing. Embo Rep. 2010, 11, 97–105. [Google Scholar] [CrossRef]
- Jayaraman, P.; Sada-Ovalle, I.; Nishimura, T.; Anderson, A.C.; Kuchroo, V.K.; Remold, H.G.; Behar, S.M. IL-1β Promotes Antimicrobial Immunity in Macrophages by Regulating TNFR Signaling and Caspase-3 Activation. J. Immunol. 2013, 190, 4196–4204. [Google Scholar] [CrossRef]
- Veves, A. ; Veves; Aristidis; Dsc Discussion: Biology and Biomarkers for Wound Healing. Plast. Reconstr. Surg. 2016, 138, 29S–30S. [Google Scholar] [CrossRef]
- Perry, D.; Frame, J. The history and development of breast implants. Ind. Mark. Manag. 2020, 102, 478–482. [Google Scholar] [CrossRef] [PubMed]
- Ghazal, I.D.; Eleweke, C.; Aladesanwa, F.O.; Onabajo, B.O. Post-mastectomy breast reconstruction: an overview of the state of the art, challenges, and prospects. Int. Surg. J. 2023, 10, 348–354. [Google Scholar] [CrossRef]
- Wick, G.; Backovic, A.; Rabensteiner, E.; Plank, N.; Schwentner, C.; Sgonc, R. The immunology of fibrosis: innate and adaptive responses. Trends Immunol. 2010, 31, 110–119. [Google Scholar] [CrossRef]
- Schoberleitner, I.; Faserl, K.; Sarg, B.; Egle, D.; Brunner, C.; Wolfram, D. Quantitative Proteomic Characterization of Foreign Body Response towards Silicone Breast Implants Identifies Chronological Disease-Relevant Biomarker Dynamics. Biomolecules 2023, 13, 305. [Google Scholar] [CrossRef]
- Schoberleitner, I.; Faserl, K.; Tripp, C.H.; Pechriggl, E.J.; Sigl, S.; Brunner, A.; Zelger, B.; Hermann-Kleiter, N.; Baier, L.; Steinkellner, T.; et al. Silicone implant surface microtopography modulates inflammation and tissue repair in capsular fibrosis. Front. Immunol. 2024, 15, 1342895. [Google Scholar] [CrossRef]
- Mempin, M.; Hu, H.; Chowdhury, D.; Deva, A.; Vickery, K. The A, B and C’s of Silicone Breast Implants: Anaplastic Large Cell Lymphoma, Biofilm and Capsular Contracture. Materials 2018, 11, 2393. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Haddouti, E.-M.; Welle, K.; Burger, C.; Wirtz, D.C.; Schildberg, F.A.; Kabir, K. The Effects of Biomaterial Implant Wear Debris on Osteoblasts. Front. Cell Dev. Biol. 2020, 8, 352. [Google Scholar] [CrossRef] [PubMed]
- Schoberleitner, I.; Baier, L.; Lackner, M.; Zenz, L.-M.; Coraça-Huber, D.C.; Ullmer, W.; Damerum, A.; Faserl, K.; Sigl, S.; Steinkellner, T.; et al. Surface Topography, Microbial Adhesion, and Immune Responses in Silicone Mammary Implant-Associated Capsular Fibrosis. Int. J. Mol. Sci. 2024, 25, 3163. [Google Scholar] [CrossRef]
- Trojanek, J.B.; Michałkiewicz, J.; Grzywa-Czuba, R.; Jańczyk, W.; Gackowska, L.; Kubiszewska, I.; Helmin-Basa, A.; Wierzbicka-Rucińska, A.; Szalecki, M.; Socha, P. Expression of Matrix Metalloproteinases and Their Tissue Inhibitors in Peripheral Blood Leukocytes and Plasma of Children with Nonalcoholic Fatty Liver Disease. Mediat. Inflamm. 2020, 2020, 1–14. [Google Scholar] [CrossRef]
- Singh, D.; Rai, V.; Agrawal, D.K. Regulation of Collagen I and Collagen III in Tissue Injury and Regeneration. Cardiol. Cardiovasc. Med. 2023, 07, 5–16. [Google Scholar] [CrossRef]
- Marcinkiewicz, J.; Strus, M.; Pasich, E. Antibiotic resistance: a “dark side” of biofilm-associated chronic infections. Pol. Arch. Intern. Med. 2013, 123, 309–313. [Google Scholar] [CrossRef]
- Donlan, R.M. Biofilms: Microbial Life on Surfaces. Emerg. Infect. Dis. 2002, 8, 881–890. [Google Scholar] [CrossRef] [PubMed]
- Costerton, J.W.; Stewart, P.S.; Greenberg, E.P. Bacterial Biofilms: A Common Cause of Persistent Infections. Science 1999, 284, 1318–1322. [Google Scholar] [CrossRef] [PubMed]
- Deva, Anand K., and Lionel C. Chang. 1999. Bacterial biofilms: A cause for accelerated capsular contracture? Aesthetic Surgery Journal 19. Mosby Inc.: 130–133. [CrossRef]
- Deva, A.K.; Adams, W.P., Jr.; Vickery, K. The Role of Bacterial Biofilms in Device-Associated Infection. Plast. Reconstr. Surg. 2013, 132, 1319–1328. [Google Scholar] [CrossRef]
- del Pozo, Jose L., and Cristina Auba. 2015. Role of biofilms in breast implant associated infections and capsular contracture. Advances in Experimental Medicine and Biology 831. Springer New York LLC: 53–67. [CrossRef]
- Ajdic, D.; Zoghbi, Y.; Gerth, D.; Panthaki, Z.J.; Thaller, S. The Relationship of Bacterial Biofilms and Capsular Contracture in Breast Implants. Aesthetic Surg. J. 2016, 36, 297–309. [Google Scholar] [CrossRef]
- Rieger, U.M.; Mesina, J.; Kalbermatten, D.F.; Haug, M.; Frey, H.P.; Pico, R.; Frei, R.; Pierer, G.; Lüscher, N.J.; Trampuz, A. Bacterial biofilms and capsular contracture in patients with breast implants. Br. J. Surg. 2013, 100, 768–774. [Google Scholar] [CrossRef]
- Ji, L.; Wang, T.; Tian, L.; Song, H.; Gao, M. Roxatidine inhibits fibrosis by inhibiting NF-κB and MAPK signaling in macrophages sensing breast implant surface materials. Mol. Med. Rep. 2020, 21, 161–172. [Google Scholar] [CrossRef]
- Rembe, J.-D.; Huelsboemer, L.; Plattfaut, I.; Besser, M.; Stuermer, E.K. Antimicrobial Hypochlorous Wound Irrigation Solutions Demonstrate Lower Anti-biofilm Efficacy Against Bacterial Biofilm in a Complex in-vitro Human Plasma Biofilm Model (hpBIOM) Than Common Wound Antimicrobials. Front. Microbiol. 2020, 11, 564513. [Google Scholar] [CrossRef] [PubMed]
- Epps, M.T.; Langsdon, S.B.; Pels, T.K.B.; Lee, T.M.; Thurston, T.; Brzezienski, M.A. Antimicrobial Irrigation and Technique during Breast Augmentation: Survey of Current Practice. Plast. Reconstr. Surg. - Glob. Open 2019, 7, e2310. [Google Scholar] [CrossRef]
- Gofstein-Hayuth, D.; Fliss, E.; Barnea, Y.; Legarda, C.; Bracha, G.; Lerner, A.; Lellouche, J.; Carmeli, Y.; Shani, N.; Arad, E. Comparing the efficacy of antimicrobial pocket-irrigation protocols in an in vivo breast implant infection model. J. Plast. Reconstr. Aesthetic Surg. 2023, 85, 165–173. [Google Scholar] [CrossRef]
- Federica, G.; Tommaso, F.; Alessia, C.; Agostino, C.; Florian, B.; Antonio, G.; Nicola, M.D.; Abdallah, R.; Carmela, S.; Lorenzo, S.; et al. Use of Antimicrobial Irrigation and Incidence of Capsular Contracture in Breast Augmentation and Immediate Implant-Based Breast Reconstruction. Aesthetic Plast. Surg. 2023, 47, 2345–2350. [Google Scholar] [CrossRef] [PubMed]
- Pakshir, P.; Hinz, B. The big five in fibrosis: Macrophages, myofibroblasts, matrix, mechanics, and miscommunication. Matrix Biol. 2018, 68-69, 81–93. [Google Scholar] [CrossRef] [PubMed]
- Mack, M. Inflammation and fibrosis. Matrix Biol. 2018, 68-69, 106–121. [Google Scholar] [CrossRef]
- Moore, Laura Beth, and Themis R. Kyriakides. 2015. Molecular characterization of macrophage-biomaterial interactions. Advances in Experimental Medicine and Biology 865. Springer New York LLC: 109–122. [CrossRef]
- Sheikh, Z.; Brooks, P.J.; Barzilay, O.; Fine, N.; Glogauer, M. Macrophages, Foreign Body Giant Cells and Their Response to Implantable Biomaterials. Materials 2015, 8, 5671–5701. [Google Scholar] [CrossRef] [PubMed]
- Sakar, M.S.; Eyckmans, J.; Pieters, R.; Eberli, D.; Nelson, B.J.; Chen, C.S. Cellular forces and matrix assembly coordinate fibrous tissue repair. Nat. Commun. 2016, 7, 11036. [Google Scholar] [CrossRef]
- Schuster, R.; Rockel, J.S.; Kapoor, M.; Hinz, B. The inflammatory speech of fibroblasts. Immunol. Rev. 2021, 302, 126–146. [Google Scholar] [CrossRef]
- Witherel, C.E.; Abebayehu, D.; Barker, T.H.; Spiller, K.L. Macrophage and Fibroblast Interactions in Biomaterial-Mediated Fibrosis. Adv. Heal. Mater. 2019, 8, e1801451. [Google Scholar] [CrossRef]
- Hinz, B.; Celetta, G.; Tomasek, J.J.; Gabbiani, G.; Chaponnier, C. Alpha-Smooth Muscle Actin Expression Upregulates Fibroblast Contractile Activity. Mol. Biol. Cell 2001, 12, 2730–2741. [Google Scholar] [CrossRef]
- Moyer, K.E.M.; Ehrlich, H.P. Capsular Contracture after Breast Reconstruction. Plast. Reconstr. Surg. 2013, 131, 680–685. [Google Scholar] [CrossRef]
- Cheung, D.T.; Benya, P.D.; Perelman, N.; Dicesare, P.E.; Nimni, M.E. A Highly Specific and Quantitative Method for Determining Type III/I Collagen Ratios in Tissues. Matrix 1990, 10, 164–171. [Google Scholar] [CrossRef]
- Akilbekova, D.; Bratlie, K.M. Quantitative Characterization of Collagen in the Fibrotic Capsule Surrounding Implanted Polymeric Microparticles through Second Harmonic Generation Imaging. PLOS ONE 2015, 10, e0130386. [Google Scholar] [CrossRef] [PubMed]
- Dolores, W.; Christian, R.; Harald, N.; Hildegunde, P.; Georg, W. Cellular and molecular composition of fibrous capsules formed around silicone breast implants with special focus on local immune reactions. J. Autoimmun. 2004, 23, 81–91. [Google Scholar] [CrossRef] [PubMed]
- Biernacka, A.; Dobaczewski, M.; Frangogiannis, N.G. TGF-β signaling in fibrosis. Growth Factors 2011, 29, 196–202. [Google Scholar] [CrossRef] [PubMed]
- Meng, X.-M.; Nikolic-Paterson, D.J.; Lan, H.Y. TGF-β: the master regulator of fibrosis. Nat. Rev. Nephrol. 2016, 12, 325–338. [Google Scholar] [CrossRef] [PubMed]
- Hu, H.-H.; Chen, D.-Q.; Wang, Y.-N.; Feng, Y.-L.; Cao, G.; Vaziri, N.D.; Zhao, Y.-Y. New insights into TGF-β/Smad signaling in tissue fibrosis. Chem. Interactions 2018, 292, 76–83. [Google Scholar] [CrossRef]
- Liu, T.; Zhang, L.; Joo, D.; Sun, S.-C. NF-κB signaling in inflammation. Signal Transduct. Target. Ther. 2017, 2, 17023. [Google Scholar] [CrossRef]
- Dondossola, E.; Holzapfel, B.M.; Alexander, S.; Filippini, S.; Hutmacher, D.W.; Friedl, P. Examination of the foreign body response to biomaterials by nonlinear intravital microscopy. Nat. Biomed. Eng. 2016, 1, 1–10. [Google Scholar] [CrossRef]
- Miron, R.J.; Bosshardt, D.D. Multinucleated Giant Cells: Good Guys or Bad Guys? Tissue Eng. Part B Rev. 2018, 24, 53–65. [Google Scholar] [CrossRef]
- McNally, A.K.; Anderson, J.M. Phenotypic expression in human monocyte-derived interleukin-4-induced foreign body giant cells and macrophagesin vitro: Dependence on material surface properties. J. Biomed. Mater. Res. Part A 2014, 103, 1380–1390. [Google Scholar] [CrossRef]
- Volk, S.W.; Wang, Y.; Mauldin, E.A.; Liechty, K.W.; Adams, S.L. Diminished Type III Collagen Promotes Myofibroblast Differentiation and Increases Scar Deposition in Cutaneous Wound Healing. Cells Tissues Organs 2011, 194, 25–37. [Google Scholar] [CrossRef]
- Desmoulière, A.; Chaponnier, C.; Gabbiani, G. Perspective Article: Tissue repair, contraction, and the myofibroblast. Wound Repair Regen. 2005, 13, 7–12. [Google Scholar] [CrossRef] [PubMed]
- de Bakker, E.; Rots, M.; Buncamper, M.E.; Niessen, F.B.; Smit, J.M.; Winters, H.A.H.; Özer, M.; de Vet, H.C.W.; Mullender, M.G. The Baker Classification for Capsular Contracture in Breast Implant Surgery Is Unreliable as a Diagnostic Tool. Plast. Reconstr. Surg. 2020, 146, 956–962. [Google Scholar] [CrossRef] [PubMed]
- Spear, S.L.; Baker, J.L. Classification of capsular contracture after prosthetic breast reconstruction. . 1995, 96, 1119. [Google Scholar] [PubMed]
- Hall-Findlay, E.J.; Findlay, H.; J. , E. Discussion: The Baker Classification for Capsular Contracture in Breast Implant Surgery Is Unreliable as a Diagnostic Tool. Plast. Reconstr. Surg. 2020, 146, 963–963. [Google Scholar] [CrossRef]
- Bachour, Y.; Verweij, S.P.; Gibbs, S.; Ket, J.C.; Ritt, M.J.; Niessen, F.B.; Mullender, M.G. The aetiopathogenesis of capsular contracture: A systematic review of the literature. J. Plast. Reconstr. Aesthetic Surg. 2018, 71, 307–317. [Google Scholar] [CrossRef]
- Lan, H.Y. Diverse Roles of TGF-β/Smads in Renal Fibrosis and Inflammation. Int. J. Biol. Sci. 2011, 7, 1056–1067. [Google Scholar] [CrossRef]
- Mirastschijski, U.; Schnabel, R.; Claes, J.; Schneider, W.; Ågren, M.S.; Haaksma, C.; Tomasek, J.J. Matrix metalloproteinase inhibition delays wound healing and blocks the latent transforming growth factor-β1-promoted myofibroblast formation and function. Wound Repair Regen. 2010, 18, 223–234. [Google Scholar] [CrossRef]
- Zhang, M.; Zhang, S. T Cells in Fibrosis and Fibrotic Diseases. Front. Immunol. 2020, 11, 1142. [Google Scholar] [CrossRef]
- Iwanaga, N.; Kolls, J.K. Updates on T helper type 17 immunity in respiratory disease. Immunology 2018, 156, 3–8. [Google Scholar] [CrossRef]
- Zhang, S. The role of transforming growth factor β in T helper 17 differentiation. Immunology 2018, 155, 24–35. [Google Scholar] [CrossRef]
- Sakaguchi, S.; Mikami, N.; Wing, J.B.; Tanaka, A.; Ichiyama, K.; Ohkura, N. Regulatory T Cells and Human Disease. Annu. Rev. Immunol. 2020, 38, 541–566. [Google Scholar] [CrossRef] [PubMed]
- Wolfram, D.; Rabensteiner, E.; Grundtman, C.; Böck, G.; Mayerl, C.; Parson, W.; Almanzar, G.; Hasenöhrl, C.; Piza-Katzer, H.; Wick, G. T Regulatory Cells and TH17 Cells in Peri–Silicone Implant Capsular Fibrosis. Plast. Reconstr. Surg. 2012, 129, 327e–337e. [Google Scholar] [CrossRef] [PubMed]
- Singh, P.; Ali, S.A. Multifunctional Role of S100 Protein Family in the Immune System: An Update. Cells 2022, 11, 2274. [Google Scholar] [CrossRef]
- Gonzalez, L.L.; Garrie, K.; Turner, M.D. Role of S100 proteins in health and disease. Biochim. et Biophys. Acta (BBA) - Mol. Cell Res. 2020, 1867, 118677. [Google Scholar] [CrossRef]
- Sreejit, Gopalkrishna, Michelle C. Flynn, Mallikarjun Patil, Prasanna Krishnamurthy, Andrew J. Murphy, and Prabhakara R. Nagareddy. 2020. S100 family proteins in inflammation and beyond. Advances in Clinical Chemistry 98. Elsevier: 173–231. [CrossRef]
- Araki, K.; Kinoshita, R.; Tomonobu, N.; Gohara, Y.; Tomida, S.; Takahashi, Y.; Senoo, S.; Taniguchi, A.; Itano, J.; Yamamoto, K.-I.; et al. The heterodimer S100A8/A9 is a potent therapeutic target for idiopathic pulmonary fibrosis. J. Mol. Med. 2020, 99, 131–145. [Google Scholar] [CrossRef] [PubMed]
- Darby, Ian A., and Tim D. Hewitson. 2007. Fibroblast Differentiation in Wound Healing and Fibrosis. International Review of Cytology 257: 143–179. [CrossRef]
- Cappellano, G.; Ploner, C.; Lobenwein, S.; Sopper, S.; Hoertnagl, P.; Mayerl, C.; Wick, N.; Pierer, G.; Wick, G.; Wolfram, D. Immunophenotypic characterization of human T cells after in vitro exposure to different silicone breast implant surfaces. PLOS ONE 2018, 13, e0192108. [Google Scholar] [CrossRef]
- Doloff, J.C.; Veiseh, O.; de Mezerville, R.; Sforza, M.; Perry, T.A.; Haupt, J.; Jamiel, M.; Chambers, C.; Nash, A.; Aghlara-Fotovat, S.; et al. The surface topography of silicone breast implants mediates the foreign body response in mice, rabbits and humans. Nat. Biomed. Eng. 2021, 5, 1115–1130. [Google Scholar] [CrossRef]
- Bizjak, M.; Selmi, C.; Praprotnik, S.; Bruck, O.; Perricone, C.; Ehrenfeld, M.; Shoenfeld, Y. Silicone implants and lymphoma: The role of inflammation. J. Autoimmun. 2015, 65, 64–73. [Google Scholar] [CrossRef]
- Brauman, D. Rough Textured Silicone Implants, Bacterial Biofilms, and Capsular Contracture. 2019, 144, 322E–323E. [CrossRef]
- Schoberleitner, I.; Augustin, A.; Egle, D.; Brunner, C.; Amort, B.; Zelger, B.; Brunner, A.; Wolfram, D. Is It All about Surface Topography? An Intra-Individual Clinical Outcome Analysis of Two Different Implant Surfaces in Breast Reconstruction. J. Clin. Med. 2023, 12, 1315. [Google Scholar] [CrossRef]
- Abaricia, J.O.; Farzad, N.; Heath, T.J.; Simmons, J.; Morandini, L.; Olivares-Navarrete, R. Control of innate immune response by biomaterial surface topography, energy, and stiffness. Acta Biomater. 2021, 133, 58–73. [Google Scholar] [CrossRef]
- Love, R.J.; Jones, K.S. The recognition of biomaterials: Pattern recognition of medical polymers and their adsorbed biomolecules. J. Biomed. Mater. Res. Part A 2013, 101A, 2740–2752. [Google Scholar] [CrossRef] [PubMed]
- Mohapatra, S. 2017. Sterilization and Disinfection. Essentials of Neuroanesthesia. Elsevier: 929. [CrossRef]
- Belay, E.D.; Schonberger, L.B.; Brown, P.; Priola, S.A.; Chesebro, B.; Will, R.G.; Asher, D.M. Disinfection and Sterilization of Prion-Contaminated Medical Instruments. Infect. Control. Hosp. Epidemiology 2010, 31, 1304–1306. [Google Scholar] [CrossRef] [PubMed]
- Rutala, W. New Disinfection and Sterilization Methods. Emerg. Infect. Dis. 2001, 7, 348–353. [Google Scholar] [CrossRef]
- Rutala, W.A.; Weber, D.J. Guideline for Disinfection and Sterilization of Prion-Contaminated Medical Instruments. Infect. Control. Hosp. Epidemiol. 2010, 31, 107–117. [Google Scholar] [CrossRef]
- Lam, M.; Migonney, V.; Falentin-Daudre, C. Review of silicone surface modification techniques and coatings for antibacterial/antimicrobial applications to improve breast implant surfaces. Acta Biomater. 2020, 121, 68–88. [Google Scholar] [CrossRef]
- Dapunt, U.; Prior, B.; Kretzer, J.P.; Giese, T.; Zhao, Y. Bacterial Biofilm Components Induce an Enhanced Inflammatory Response Against Metal Wear Particles. Ther. Clin. Risk Manag. 2020, ume 16, 1203–1212. [Google Scholar] [CrossRef]
- Carvajal, J.; Carvajal, M.; Chavez, D.; Hernandez, G. Back to Basics: Could the Preoperative Skin Antiseptic Agent Help Prevent Biofilm-Related Capsular Contracture? Aesthetic Surg. J. 2018, 39, 848–859. [Google Scholar] [CrossRef]
- Rezende-Pereira, G.; Albuquerque, J.P.; Souza, M.C.; A Nogueira, B.; Silva, M.G.; Hirata, R.; Mattos-Guaraldi, A.L.; Duarte, R.S.; Neves, F.P.G. Biofilm Formation on Breast Implant Surfaces by Major Gram-Positive Bacterial Pathogens. Aesthetic Surg. J. 2020, 41, 1144–1151. [Google Scholar] [CrossRef]
- Mu, Minchen, Shuhao Liu, William DeFlorio, Li Hao, Xunhao Wang, Karla Solis Salazar, Matthew Taylor, et al. 2023. Influence of Surface Roughness, Nanostructure, and Wetting on Bacterial Adhesion. Langmuir 39. American Chemical Society: 5426–5439. [CrossRef]
- James, G.A.; Boegli, L.; Hancock, J.; Bowersock, L.; Parker, A.; Kinney, B.M. Bacterial Adhesion and Biofilm Formation on Textured Breast Implant Shell Materials. Aesthetic Plast. Surg. 2018, 43, 490–497. [Google Scholar] [CrossRef] [PubMed]
- Josse, J.; Laurent, F.; Diot, A. Staphylococcal Adhesion and Host Cell Invasion: Fibronectin-Binding and Other Mechanisms. Front. Microbiol. 2017, 8, 2433. [Google Scholar] [CrossRef]
- Yoda, I.; Koseki, H.; Tomita, M.; Shida, T.; Horiuchi, H.; Sakoda, H.; Osaki, M. Effect of surface roughness of biomaterials on Staphylococcus epidermidis adhesion. BMC Microbiol. 2014, 14, 234. [Google Scholar] [CrossRef] [PubMed]
- Arciola, C.R.; Baldassarri, L.; Montanaro, L. In catheter infections by Staphylococcus epidermidis the intercellular adhesion (ica) locus is a molecular marker of the virulent slime-producing strains. J. Biomed. Mater. Res. 2001, 59, 557–562. [Google Scholar] [CrossRef] [PubMed]
- Berne, C.; Ellison, C.K.; Ducret, A.; Brun, Y.V. Bacterial adhesion at the single-cell level. Nat. Rev. Microbiol. 2018, 16, 616–627. [Google Scholar] [CrossRef] [PubMed]
- Boks, N.P.; Norde, W.; van der Mei, H.C.; Busscher, H.J. Forces involved in bacterial adhesion to hydrophilic and hydrophobic surfaces. Microbiology 2008, 154, 3122–3133. [Google Scholar] [CrossRef]
- Høiby, N.; Ciofu, O.; Johansen, H.K.; Song, Z.-J.; Moser, C.; Jensen, P.Ø.; Molin, S.; Givskov, M.; Tolker-Nielsen, T.; Bjarnsholt, T. The clinical impact of bacterial biofilms. Int. J. Oral Sci. 2011, 3, 55–65. [Google Scholar] [CrossRef]
- Arciola, C.R.; Campoccia, D.; Ravaioli, S.; Montanaro, L. Polysaccharide intercellular adhesin in biofilm: structural and regulatory aspects. Front. Cell. Infect. Microbiol. 2015, 5, 7–7. [Google Scholar] [CrossRef]
- Rumbaugh, K.P. , and K. Sauer. 2020. Biofilm dispersion. Nat Rev Microbiol 18: 571–586.
- Costerton, J.W.; Stewart, P.S.; Greenberg, E.P. Bacterial Biofilms: A Common Cause of Persistent Infections. Science 1999, 284, 1318–1322. [Google Scholar] [CrossRef]
- Vestby, L.K.; Grønseth, T.; Simm, R.; Nesse, L.L. Bacterial Biofilm and its Role in the Pathogenesis of Disease. Antibiotics 2020, 9, 59. [Google Scholar] [CrossRef]
- Fey, P.D.; Olson, M.E. Current concepts in biofilm formation of Staphylococcus epidermidis. Futur. Microbiol. 2010, 5, 917–933. [Google Scholar] [CrossRef] [PubMed]
- Pajkos, A.; Deva, A.K.; Vickery, K.; Cope, C.; Chang, L.; Cossart, Y.E. Detection of Subclinical Infection in Significant Breast Implant Capsules. Plast. Reconstr. Surg. 2003, 111, 1605–1611. [Google Scholar] [CrossRef]
- Sopwith, W.; Hart, T.; Garner, P. Preventing infection from reusable medical equipment: a systematic review. BMC Infect. Dis. 2002, 2, 4–4. [Google Scholar] [CrossRef] [PubMed]
- Biron, F.; Verrier, B.; Peyramond, D. Transmission of the Human Immunodeficiency Virus and the Hepatitis C Virus. New Engl. J. Med. 1997, 337, 348–349. [Google Scholar] [CrossRef] [PubMed]
- Gillespie, T.; Hogg, L.; Budge, E.; Duncan, A.; Coia, J. Mycobacterium chelonae isolated from rinse water within an endoscope washer–disinfector. J. Hosp. Infect. 2000, 45, 332–334. [Google Scholar] [CrossRef]
- Schelenz, S.; French, G. An outbreak of multidrug-resistant Pseudomonas aeruginosa infection associated with contamination of bronchoscopes and an endoscope washer-disinfector. J. Hosp. Infect. 2000, 46, 23–30. [Google Scholar] [CrossRef]
- Srinivasan, A.; Wolfenden, L.L.; Song, X.; Mackie, K.; Hartsell, T.L.; Jones, H.D.; Diette, G.B.; Orens, J.B.; Yung, R.C.; Ross, T.L.; et al. An Outbreak ofPseudomonas aeruginosaInfections Associated with Flexible Bronchoscopes. New Engl. J. Med. 2003, 348, 221–227. [Google Scholar] [CrossRef]
- Cohen, J.B.; Carroll, C.; Tenenbaum, M.M.; Myckatyn, T.M. Breast Implant–Associated Infections. Plast. Reconstr. Surg. 2015, 136, 921–929. [Google Scholar] [CrossRef] [PubMed]
- Palubicka, A.; Jaworski, R.; Wekwejt, M.; Swieczko-Zurek, B.; Pikula, M.; Jaskiewicz, J.; Zielinski, J. Surgical Site Infection after Breast Surgery: A Retrospective Analysis of 5-Year Postoperative Data from a Single Center in Poland. Medicina 2019, 55, 512. [Google Scholar] [CrossRef]
- Prantl, L.; Momeni, A.; Brebant, V.; Kuehlmann, B.; Heine, N.; Biermann, N.; Brix, E. Recommendations for the Use of Antibiotics in Primary and Secondary Esthetic Breast Surgery. Plast. Reconstr. Surg. - Glob. Open 2020, 8, e2590. [Google Scholar] [CrossRef]
- Yalanis, G.C.; Liu, E.-W.; Cheng, H.-T. Efficacy and Safety of Povidone-Iodine Irrigation in Reducing the Risk of Capsular Contracture in Aesthetic Breast Augmentation. Plast. Reconstr. Surg. 2015, 136, 687–698. [Google Scholar] [CrossRef]
- Burkhardt, B.R.; Dempsey, P.D.; Schnur, P.L.; Tofield, J.J. Capsular Contracture. Plast. Reconstr. Surg. 1986, 77, 919–930. [Google Scholar] [CrossRef]
- Brandon, H.; Brandon, D.H.J.; Young, V.L.; Jerina, D.K.L.; Wolf, C.J.; Adams, J.W.P.; Watson, M.E. Mechanical analysis of explanted saline-filled breast implants exposed to betadine pocket irrigation. Aesthetic Surg. J. 2002, 22, 438–445. [Google Scholar] [CrossRef] [PubMed]
- U.S. Food and Drug Administration (2017). 2023. Premarket Approval (PMA). https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfpma/pma.cfm?ID=402786. Accessed October 30.
- Adams, W.P.; Conner, W.C.H.; Barton, F.E.; Rohrich, R.J. Optimizing Breast-Pocket Irrigation: The Post-Betadine Era. Plast. Reconstr. Surg. 2001, 107, 1596–1601. [Google Scholar] [CrossRef] [PubMed]
- Jewell, M.L.; Adams, W.P. Betadine and Breast Implants. Aesthetic Surg. J. 2018, 38, 623–626. [Google Scholar] [CrossRef] [PubMed]
- Adams, W.P. Commentary on: Surgical Site Irrigation in Plastic Surgery: What is Essential? Aesthetic Surg. J. 2017, 38, 276–278. [Google Scholar] [CrossRef]
- Viola, G.M.; Rolston, K.V.; Butler, C.; Selber, J.; Reece, G.; Clemens, M.; Villa, M.; Raad, I.I.; Baumann, D. Evaluation of Current Perioperative Antimicrobial Regimens for the Prevention of Surgical Site Infections in Breast Implant-based Reconstructive Surgeries. Plast. Reconstr. Surg. - Glob. Open 2019, 7, e2342. [Google Scholar] [CrossRef]
- Zhadan, O.; Becker, H. Surgical Site Irrigation in Plastic Surgery. Aesthetic Surg. J. 2017, 38, 265–273. [Google Scholar] [CrossRef]
- McKinnon, P.S.; Davis, S.L. Pharmacokinetic and Pharmacodynamic Issues in the Treatment of Bacterial Infectious Diseases. Eur. J. Clin. Microbiol. Infect. Dis. 2004, 23, 271–288. [Google Scholar] [CrossRef] [PubMed]
- Scuderi, N.; Mazzocchi, M.; Fioramonti, P.; Bistoni, G. The Effects of Zafirlukast on Capsular Contracture: Preliminary Report. Aesthetic Plast. Surg. 2006, 30, 513–520. [Google Scholar] [CrossRef]
- Rubino, C.; Brongo, S.; Pagliara, D.; Cuomo, R.; Abbinante, G.; Campitiello, N.; Santanelli, F.; Chessa, D. Infections in breast implants: a review with a focus on developing countries. J. Infect. Dev. Ctries. 2014, 8, 1089–1095. [Google Scholar] [CrossRef]
- Jianu, D.M.; Săndulescu, O.; Berciu, I.; Blidaru, A.; Filipescu, M.; Vartic, M.; Cobani, O.; Jianu. A.; Tălăpan, D.; Dorobăț, O.; et al. Microbiologic Safety of the Transareolar Approach in Breast Augmentation. Aesthetic Surg. J. 2015, 36, 51–57. [Google Scholar] [CrossRef]
- Zhang, H.; Wang, Y.; Yang, S.; Zhang, Y. Peri-Operative Antibiotic Prophylaxis Does Not Reduce Surgical Site Infection in Breast Cancer. Surg. Infect. 2020, 21, 268–274. [Google Scholar] [CrossRef] [PubMed]
- Monroig, K.B.; Ghosh, K.B.; Marquez, J.E.M.; Medrano, C.B.; Marmor, W.A.B.; McAuliffe, P.B.; Ferrier, A.B.; Kapadia, K.; Rogoff, H.B.; Huston, T.M.; et al. Do Postoperative Prophylactic Antibiotics Reduce Highly Virulent Infections? Ann. Plast. Surg. 2020, 85, S50–S53. [Google Scholar] [CrossRef] [PubMed]
- Gil Conesa, M.; Martínez, N.C.; Luque, J.D.M.; Poveda, M.D.; Villar, D.R.; Caravaca, G.R. Evaluation of compliance with the antibiotic prophylaxis protocol in breast surgery and its effect on the incidence of surgical infection. An. del Sist. Sanit. de Navar. 2019, 42, 139–146. [Google Scholar] [CrossRef]
- Doherty, C.; McClure, J.A.; Baxter, N.N.; Brackstone, M. Complications From Postmastectomy Radiation Therapy in Patients Undergoing Immediate Breast Reconstruction: A Population-Based Study. Adv. Radiat. Oncol. 2022, 8, 101104. [Google Scholar] [CrossRef]
- Adams, W.P.; Culbertson, E.J.; Deva, A.K.; Magnusson, M.R.; Layt, C.; Jewell, M.L.; Mallucci, P.; Hedén, P. Macrotextured Breast Implants with Defined Steps to Minimize Bacterial Contamination around the Device: Experience in 42,000 Implants. Plast. Reconstr. Surg. 2017, 140, 427–431. [Google Scholar] [CrossRef]
- Hu, H.; Sleiman, J.; Johani, K.; Vickery, K. Hypochlorous Acid Versus Povidone-Iodine Containing Irrigants: Which Antiseptic is More Effective for Breast Implant Pocket Irrigation? Aesthetic Surg. J. 2018, 38, 723–727. [Google Scholar] [CrossRef]
- Brody, G.S. On the Safety of Breast Implants. Plast. Reconstr. Surg. 1997, 100, 1314–1321. [Google Scholar] [CrossRef]
- Steiert, A.; Sorg, H.; Boyce, M. Capsular contracture by silicone breast implants: possible causes, biocompatibility, and prophylactic strategies. Med Devices: Évid. Res. 2013, 6, 211–8. [Google Scholar] [CrossRef]
- Risks and Complications of Breast Implants | FDA. 2022. https://www.fda.gov/medical-devices/breast-implants/risks-and-complications-breast-implants. Accessed November 21.
- Jewell, M.L.; Bengtson, B.P.; Smither, K.; Nuti, G.; Perry, T. Physical Properties of Silicone Gel Breast Implants. Aesthetic Surg. J. 2018, 39, 264–275. [Google Scholar] [CrossRef]
- Henriksen, T.F.; Fryzek, J.P.; Hölmich, L.R.; McLaughlin, J.K.; Kjøller, K.; Høyer, A.P.; Olsen, J.H.; Friis, S. Surgical Intervention and Capsular Contracture After Breast Augmentation. Ann. Plast. Surg. 2005, 54, 343–351. [Google Scholar] [CrossRef]
- Namnoum, J.D.; Largent, J.; Kaplan, H.M.; Oefelein, M.G.; Brown, M.H. Primary breast augmentation clinical trial outcomes stratified by surgical incision, anatomical placement and implant device type. J. Plast. Reconstr. Aesthetic Surg. 2013, 66, 1165–1172. [Google Scholar] [CrossRef] [PubMed]
- Moyer, HR, B Ghazi, A Losken - Plastic and Reconstructive Surgery, and undefined 2011. 2024. Sterility in breast implant placement: the Keller funnel and the “no touch” technique. journals.lww.comHR Moyer, B Ghazi, A LoskenPlastic and Reconstructive Surgery, 2011•journals.lww.com. https://journals.lww.com/plasreconsurg/fulltext/2011/10001/Capsular_Contracture_Rate_in_Low_Risk_Population.14.aspx. Accessed August 27.
- Vazquez, B.; Given, K.S.; Houston, G.C. Breast augmentation: A review of subglandular and submuscular implantation. Aesthetic Plast. Surg. 1987, 11, 101–105. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.-H.; Samuel, M.; Tan, B.-K.; Song, C. Capsular Contracture in Subglandular Breast Augmentation with Textured versus Smooth Breast Implants: A Systematic Review. Plast. Reconstr. Surg. 2006, 118, 1224–1236. [Google Scholar] [CrossRef]
- Khandwekar, A.; Rho, C.K. Modulation of cellular responses on engineered polyurethane implants. J. Biomed. Mater. Res. Part A 2012, 100A, 2211–2222. [Google Scholar] [CrossRef]
- Manav, S.; Ayhan, M.S.; Deniz, E.; Özkoçer, E.; Elmas. ; Yalinay, M.; Şahin, E. Capsular contracture around silicone miniimplants following bacterial contamination: an in vivo comparative experimental study between textured and polyurethane implants. J. Plast. Reconstr. Aesthetic Surg. 2020, 73, 1747–1757. [Google Scholar] [CrossRef]
- Duxbury, P.J.; Harvey, J.R. Systematic review of the effectiveness of polyurethane-coated compared with textured silicone implants in breast surgery. J. Plast. Reconstr. Aesthetic Surg. 2016, 69, 452–460. [Google Scholar] [CrossRef]
- Daka, J.N.; Chawl, A.S. Release of Chemicals from Polyurethane Foam in the Meme Breast Implant. Biomater. Artif. Cells Immobil. Biotechnol. 1993, 21, 23–46. [Google Scholar] [CrossRef] [PubMed]
- Harmeling, J.X.; Cinca, K.P.; Andrinopoulou, E.-R.; Corten, E.M.L.; A Mureau, M. Long-term outcomes of two-stage, immediate and delayed breast reconstruction with polyurethane-covered versus textured implants: protocol of a prospective, multicentre randomised controlled trial (TIPI trial). BMJ Open 2021, 11, e044219. [Google Scholar] [CrossRef]
- Encinas, N.; Yang, C.-Y.; Geyer, F.; Kaltbeitzel, A.; Baumli, P.; Reinholz, J.; Mailänder, V.; Butt, H.-J.; Vollmer, D. Submicrometer-Sized Roughness Suppresses Bacteria Adhesion. ACS Appl. Mater. Interfaces 2020, 12, 21192–21200. [Google Scholar] [CrossRef]
- Alessandri-Bonetti, M.; Jeong, T.; Vaienti, L.; De La Cruz, C.; Gimbel, M.L.; Nguyen, V.T.; Egro, F.M. The Role of Microorganisms in the Development of Breast Implant-Associated Anaplastic Large Cell Lymphoma. Pathogens 2023, 12, 313. [Google Scholar] [CrossRef]
- Rolph, R.; Farhadi, J. The use of meshes and matrices in breast reconstruction. Br. J. Hosp. Med. 2018, 79, 454–459. [Google Scholar] [CrossRef] [PubMed]
- Jacombs, A.; Allan, J.; Hu, H.; Valente, P.M.; Wessels, W.L.F.; Deva, A.K.; Vickery, K. Prevention of Biofilm-Induced Capsular Contracture With Antibiotic-Impregnated Mesh in a Porcine Model. Aesthetic Surg. J. 2012, 32, 886–891. [Google Scholar] [CrossRef]
- Ruff, E.S.; Hirase, T.; Rude, M.J. Evaluation of Antibiotic-Impregnated Mesh in Preventing the Recurrence of Capsular Contracture. Aesthetic Surg. J. 2018, 39, 509–515. [Google Scholar] [CrossRef] [PubMed]
- Borkner, C.B.; Wohlrab, S.; Möller, E.; Lang, G.; Scheibel, T. Surface Modification of Polymeric Biomaterials Using Recombinant Spider Silk Proteins. ACS Biomater. Sci. Eng. 2016, 3, 767–775. [Google Scholar] [CrossRef]
- Weiss, A.C.G.; Herold, H.M.; Lentz, S.; Faria, M.; Besford, Q.A.; Ang, C.-S.; Caruso, F.; Scheibel, T. Surface Modification of Spider Silk Particles to Direct Biomolecular Corona Formation. ACS Appl. Mater. Interfaces 2020, 12, 24635–24643. [Google Scholar] [CrossRef]
- Salehi, S.; Koeck, K.; Scheibel, T. Spider Silk for Tissue Engineering Applications. Molecules 2020, 25, 737. [Google Scholar] [CrossRef] [PubMed]
- Scheibel, T. Spider silks: recombinant synthesis, assembly, spinning, and engineering of synthetic proteins. Microb. Cell Factories 2004, 3, 14–14. [Google Scholar] [CrossRef]
- Kumari, S.; Lang, G.; DeSimone, E.; Spengler, C.; Trossmann, V.T.; Lücker, S.; Hudel, M.; Jacobs, K.; Krämer, N.; Scheibel, T. Engineered spider silk-based 2D and 3D materials prevent microbial infestation. 2020, 41, 21–33. [CrossRef]
- Kumari, S.; Bargel, H.; Scheibel, T. Recombinant Spider Silk–Silica Hybrid Scaffolds with Drug-Releasing Properties for Tissue Engineering Applications. Macromol. Rapid Commun. 2019, 41, e1900426. [Google Scholar] [CrossRef]
- Zeplin, P.H.; Maksimovikj, N.C.; Jordan, M.C.; Nickel, J.; Lang, G.; Leimer, A.H.; Römer, L.; Scheibel, T. Spider Silk Coatings as a Bioshield to Reduce Periprosthetic Fibrous Capsule Formation. Adv. Funct. Mater. 2014, 24, 2658–2666. [Google Scholar] [CrossRef]
- Erathodiyil, N.; Chan, H.-M.; Wu, H.; Ying, J.Y. Zwitterionic polymers and hydrogels for antibiofouling applications in implantable devices. Mater. Today 2020, 38, 84–98. [Google Scholar] [CrossRef]
- Mi, L.; Jiang, S. Integrated Antimicrobial and Nonfouling Zwitterionic Polymers. Angew. Chem. Int. Ed. 2014, 53, 1746–1754. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Yuan, Z.; Jain, P.; Hung, H.-C.; He, Y.; Lin, X.; McMullen, P.; Jiang, S. De novo design of functional zwitterionic biomimetic material for immunomodulation. Sci. Adv. 2020, 6, eaba0754. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Cao, Z.; Bai, T.; Carr, L.; Ella-Menye, J.-R.; Irvin, C.; Ratner, B.D.; Jiang, S. Zwitterionic hydrogels implanted in mice resist the foreign-body reaction. Nat. Biotechnol. 2013, 31, 553–556. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Jain, P.; Ma, J.; Smith, J.K.; Yuan, Z.; Hung, H.-C.; He, Y.; Lin, X.; Wu, K.; Pfaendtner, J.; et al. Trimethylamine N -oxide–derived zwitterionic polymers: A new class of ultralow fouling bioinspired materials. Sci. Adv. 2019, 5, eaaw9562. [Google Scholar] [CrossRef] [PubMed]
- Jansen, L.E.; Amer, L.D.; Chen, E.Y.-T.; Nguyen, T.V.; Saleh, L.S.; Emrick, T.; Liu, W.F.; Bryant, S.J.; Peyton, S.R. Zwitterionic PEG-PC Hydrogels Modulate the Foreign Body Response in a Modulus-Dependent Manner. Biomacromolecules 2018, 19, 2880–2888. [Google Scholar] [CrossRef]
- Adams, W.P., Jr.; Rios, J.L.; Smith, S.J. Enhancing Patient Outcomes in Aesthetic and Reconstructive Breast Surgery Using Triple Antibiotic Breast Irrigation: Six-Year Prospective Clinical Study. Plast. Reconstr. Surg. 2006, 118, 46S–52S. [Google Scholar] [CrossRef]
- Giordano, S.; Peltoniemi, H.; Lilius, P.; Salmi, A. Povidone-Iodine Combined With Antibiotic Topical Irrigation to Reduce Capsular Contracture in Cosmetic Breast Augmentation. Aesthetic Surg. J. 2013, 33, 675–680. [Google Scholar] [CrossRef]
- Drinane, J.J.; Bergman, R.S.; Folkers, B.L.; Kortes, M.J. Revisiting Triple Antibiotic Irrigation of Breast Implant Pockets. Plast. Reconstr. Surg. - Glob. Open 2013, 1, e55–e55. [Google Scholar] [CrossRef]
- Jewell, M.L.; Hariri, S.; E Lantz, E.; Jewell, H.L.; Strickland, A.D.; Leung, B.K. In Vitro Evaluation of Common Antimicrobial Solutions Used for Breast Implant Soaking and Breast Pocket Irrigation—Part 1: Efficacy Against Planktonic Bacteria. Aesthetic Surg. J. 2020, 41, 1242–1251. [Google Scholar] [CrossRef]
- Baker, J.E.; Seitz, A.P.; Boudreau, R.M.; Skinner, M.J.B.; Beydoun, A.B.; Kaval, N.; Caldwell, C.C.; Gulbins, E.M.; Edwards, M.J.; Gobble, R.M. Doxycycline-Coated Silicone Breast Implants Reduce Acute Surgical-Site Infection and Inflammation. Plast. Reconstr. Surg. 2020, 146, 1029–1041. [Google Scholar] [CrossRef]
- Nguyen, L.; Afshari, A.; Green, J.; Joseph, J.; Yao, J.; Perdikis, G.; Higdon, K.K. Post-Mastectomy Surgical Pocket Irrigation With Triple Antibiotic Solution vs Chlorhexidine Gluconate: A Randomized Controlled Trial Assessing Surgical Site Infections in Immediate Tissue Expander Breast Reconstruction. Aesthetic Surg. J. 2021, 41, NP1521–NP1528. [Google Scholar] [CrossRef] [PubMed]
- Unlu, R.E.; Yilmaz, A.D.; Orbay, H.; Can, B.; Tekdemir, I.; Sensoz, O. Influence of Rifampin on Capsule Formation Around Silicone Implants in a Rat Model. Aesthetic Plast. Surg. 2007, 31, 358–364. [Google Scholar] [CrossRef] [PubMed]
- Gancedo, M.; Ruiz-Corro, L.; Salazar-Montes, A.; Rincón, A.R.; Armendáriz-Borunda, J. Pirfenidone Prevents Capsular Contracture After Mammary Implantation. Aesthetic Plast. Surg. 2007, 32, 32–40. [Google Scholar] [CrossRef] [PubMed]
- Schaefer, C.J.; Ruhrmund, D.W.; Pan, L.; Seiwert, S.D.; Kossen, K. Antifibrotic activities of pirfenidone in animal models. Eur. Respir. Rev. 2011, 20, 85–97. [Google Scholar] [CrossRef] [PubMed]
- Fayzullin, A.; Churbanov, S.; Ignatieva, N.; Zakharkina, O.; Tokarev, M.; Mudryak, D.; Khristidis, Y.; Balyasin, M.; Kurkov, A.; Golubeva, E.N.; et al. Local Delivery of Pirfenidone by PLA Implants Modifies Foreign Body Reaction and Prevents Fibrosis. Biomedicines 2021, 9, 853. [Google Scholar] [CrossRef] [PubMed]
- Grattendick, K.; Nakashima, J.; Feng, L.; Giri, S.; Margolin, S. Effects of three anti-TNF-α drugs: Etanercept, infliximab and pirfenidone on release of TNF-α in medium and TNF-α associated with the cell in vitro. Int. Immunopharmacol. 2008, 8, 679–687. [Google Scholar] [CrossRef]
- Zeplin, P.H.; Larena-Avellaneda, A.; Schmidt, K. Surface Modification of Silicone Breast Implants by Binding the Antifibrotic Drug Halofuginone Reduces Capsular Fibrosis. Plast. Reconstr. Surg. 2010, 126, 266–274. [Google Scholar] [CrossRef]
- Pines, M.; Nagler, A. Halofuginone: A Novel Antifibrotic Therapy. Gen. Pharmacol. Vasc. Syst. 1998, 30, 445–450. [Google Scholar] [CrossRef]
- Granot, I.; Halevy, O.; Hurwitz, S.; Pines, M. Halofuginone: An inhibitor of collagen type I synthesis. Biochim. et Biophys. Acta (BBA) - Gen. Subj. 1993, 1156, 107–112. [Google Scholar] [CrossRef]
- McGaha, T.L.; Bona, C.; Phelps, R.G.; Spiera, H. Halofuginone, an Inhibitor of Type-I Collagen Synthesis and Skin Sclerosis, Blocks Transforming-Growth-Factor-β-Mediated Smad3 Activation in Fibroblasts. J. Investig. Dermatol. 2002, 118, 461–470. [Google Scholar] [CrossRef]
- Guimier, E.; Carson, L.; David, B.; Lambert, J.M.; Heery, E.; Malcolm, R.K. Pharmacological Approaches for the Prevention of Breast Implant Capsular Contracture. J. Surg. Res. 2022, 280, 129–150. [Google Scholar] [CrossRef] [PubMed]
- Colak, O.; Ozer, K.; Dikmen, A.; Ozakinci, H.; Ozkaya, O. Evaluation of Safe Systemic Immunosuppression Created with Dexamethasone in Prevention of Capsular Contracture: A Glance to Distinct Perspectives with Toll-Like Receptors. Aesthetic Plast. Surg. 2018, 42, 1133–1143. [Google Scholar] [CrossRef] [PubMed]
- Wilk, M.; Hessler, R.; Mugridge, K.; Jolly, C.; Fehr, M.; Lenarz, T.; Scheper, V. Impedance Changes and Fibrous Tissue Growth after Cochlear Implantation Are Correlated and Can Be Reduced Using a Dexamethasone Eluting Electrode. PLOS ONE 2016, 11, e0147552. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Stages of the inflammatory and fibrotic response SMI insertion, illustrating the transition from immediate post-implantation inflammation to long-term fibrosis and implant encapsulation, with a detailed schematic of the cellular and molecular events driving these processes. Schematic representation of the cellular and molecular events involved in the inflammatory and fibrotic processes: (1.) Lymphocyte Activation: CD4+ T cells are activated by dendritic cells (DC) presenting antigens through major histocompatibility complex (MHC) molecules. Heat shock proteins (HSP60) and other danger-associated molecular patterns (DAMPs) interact with pattern recognition receptors (PRR) and toll-like receptors (TLR), initiating the immune response.(2.) Th1/Th17 Immune Response: Activated T cells differentiate into Th1 and Th17 subsets, secreting pro-inflammatory cytokines (IL-1β, IFN-γ, TNF-α, IL-17), which drive the inflammatory response while suppressing regulatory T cells (Treg). (3) Macrophage Activation: M1 macrophages, stimulated by the inflammatory environment, contribute to chronic inflammation. Over time, there may be a transition to M2 macrophages, associated with tissue repair and fibrosis. (4.) Fibrogenesis: Myofibroblasts arise from fibroblasts under the influence of cytokines like TGF-β, leading to the production of ECM components and the development of fibrotic tissue. (5.) ECM Remodeling: The ECM undergoes significant changes, with increased production of proteins such as COL1<3, vimentin, and decorin. Matrix metalloproteinases (MMP2, MMP8) are involved in the remodeling process, regulated by factors like HSP60. (6.) Implant Encapsulation: The final outcome is the encapsulation of the implant by fibrotic tissue, forming a dense fibrous capsule around the implant due to the accumulation and remodeling of ECM components.
Figure 1.
Stages of the inflammatory and fibrotic response SMI insertion, illustrating the transition from immediate post-implantation inflammation to long-term fibrosis and implant encapsulation, with a detailed schematic of the cellular and molecular events driving these processes. Schematic representation of the cellular and molecular events involved in the inflammatory and fibrotic processes: (1.) Lymphocyte Activation: CD4+ T cells are activated by dendritic cells (DC) presenting antigens through major histocompatibility complex (MHC) molecules. Heat shock proteins (HSP60) and other danger-associated molecular patterns (DAMPs) interact with pattern recognition receptors (PRR) and toll-like receptors (TLR), initiating the immune response.(2.) Th1/Th17 Immune Response: Activated T cells differentiate into Th1 and Th17 subsets, secreting pro-inflammatory cytokines (IL-1β, IFN-γ, TNF-α, IL-17), which drive the inflammatory response while suppressing regulatory T cells (Treg). (3) Macrophage Activation: M1 macrophages, stimulated by the inflammatory environment, contribute to chronic inflammation. Over time, there may be a transition to M2 macrophages, associated with tissue repair and fibrosis. (4.) Fibrogenesis: Myofibroblasts arise from fibroblasts under the influence of cytokines like TGF-β, leading to the production of ECM components and the development of fibrotic tissue. (5.) ECM Remodeling: The ECM undergoes significant changes, with increased production of proteins such as COL1<3, vimentin, and decorin. Matrix metalloproteinases (MMP2, MMP8) are involved in the remodeling process, regulated by factors like HSP60. (6.) Implant Encapsulation: The final outcome is the encapsulation of the implant by fibrotic tissue, forming a dense fibrous capsule around the implant due to the accumulation and remodeling of ECM components.
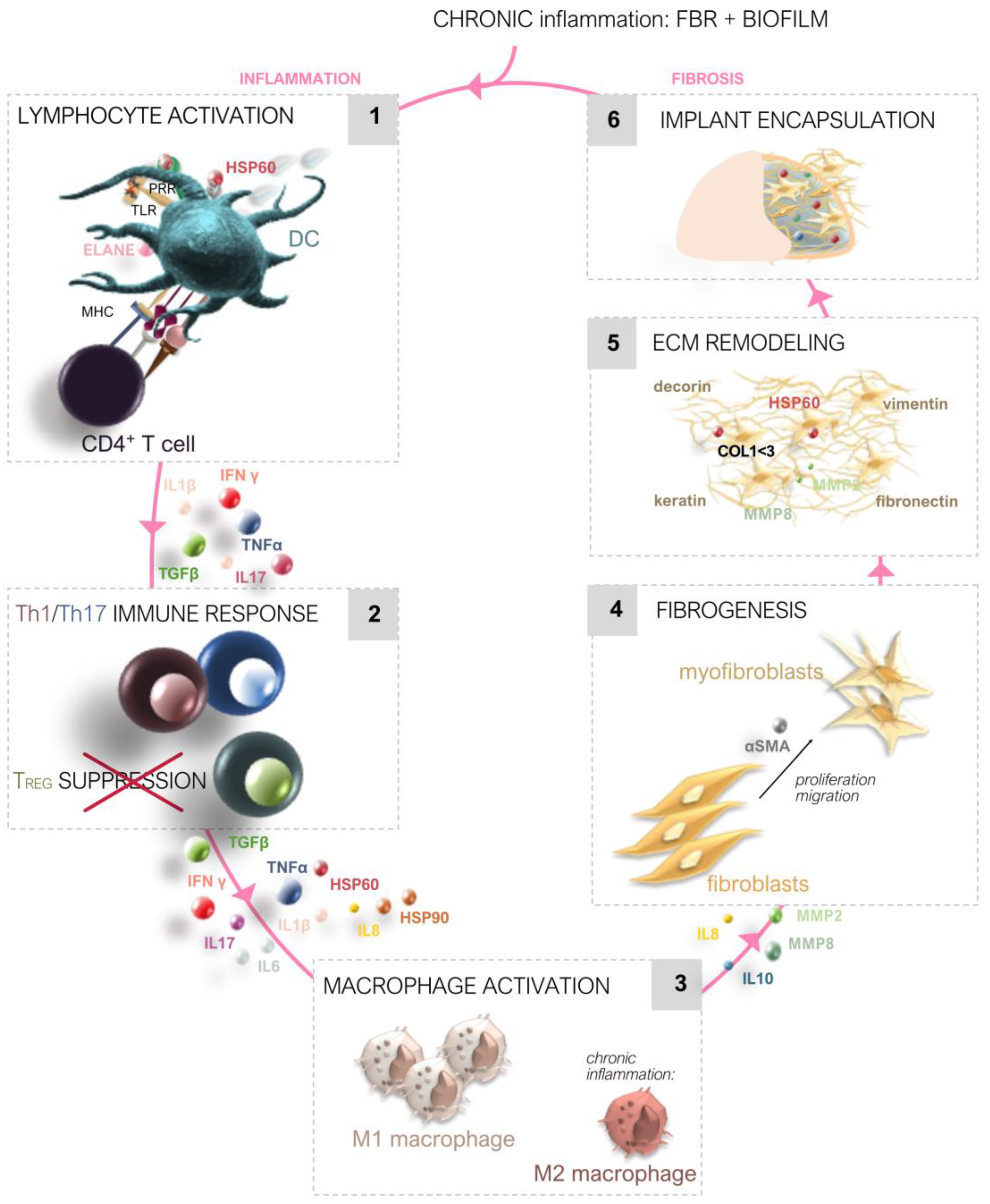
Figure 2.
Mechanisms triggering immediate and chronic inflammation in response to silicone mammary implants. (a) Immediate Inflammatory Triggers Post-Implantation: The acute inflammatory response is initiated immediately after silicone mammary implant (SMI) insertion due to tissue damage, skin microbiome contamination, and the introduction of DAMPs and PAMPs. Silicone microparticle shedding, microbial attachment, and protein adsorption on the implant surface further intensify the inflammatory response, with mediators like MCP-1, collagen (COL1/3), and CD44 accumulating in the wound environment. (b) Chronic Inflammatory Triggers and Early-Stage Fibrosis: Months after implantation, persistent inflammation is driven by biofilm formation on the implant surface and the adhesion of proinflammatory and profibrotic factors. Microbial infiltration into fibrotic tissue and extensive ECM remodeling, involving vimentin, decorin, and fibronectin, result in the development of a dense fibrotic capsule.
Figure 2.
Mechanisms triggering immediate and chronic inflammation in response to silicone mammary implants. (a) Immediate Inflammatory Triggers Post-Implantation: The acute inflammatory response is initiated immediately after silicone mammary implant (SMI) insertion due to tissue damage, skin microbiome contamination, and the introduction of DAMPs and PAMPs. Silicone microparticle shedding, microbial attachment, and protein adsorption on the implant surface further intensify the inflammatory response, with mediators like MCP-1, collagen (COL1/3), and CD44 accumulating in the wound environment. (b) Chronic Inflammatory Triggers and Early-Stage Fibrosis: Months after implantation, persistent inflammation is driven by biofilm formation on the implant surface and the adhesion of proinflammatory and profibrotic factors. Microbial infiltration into fibrotic tissue and extensive ECM remodeling, involving vimentin, decorin, and fibronectin, result in the development of a dense fibrotic capsule.
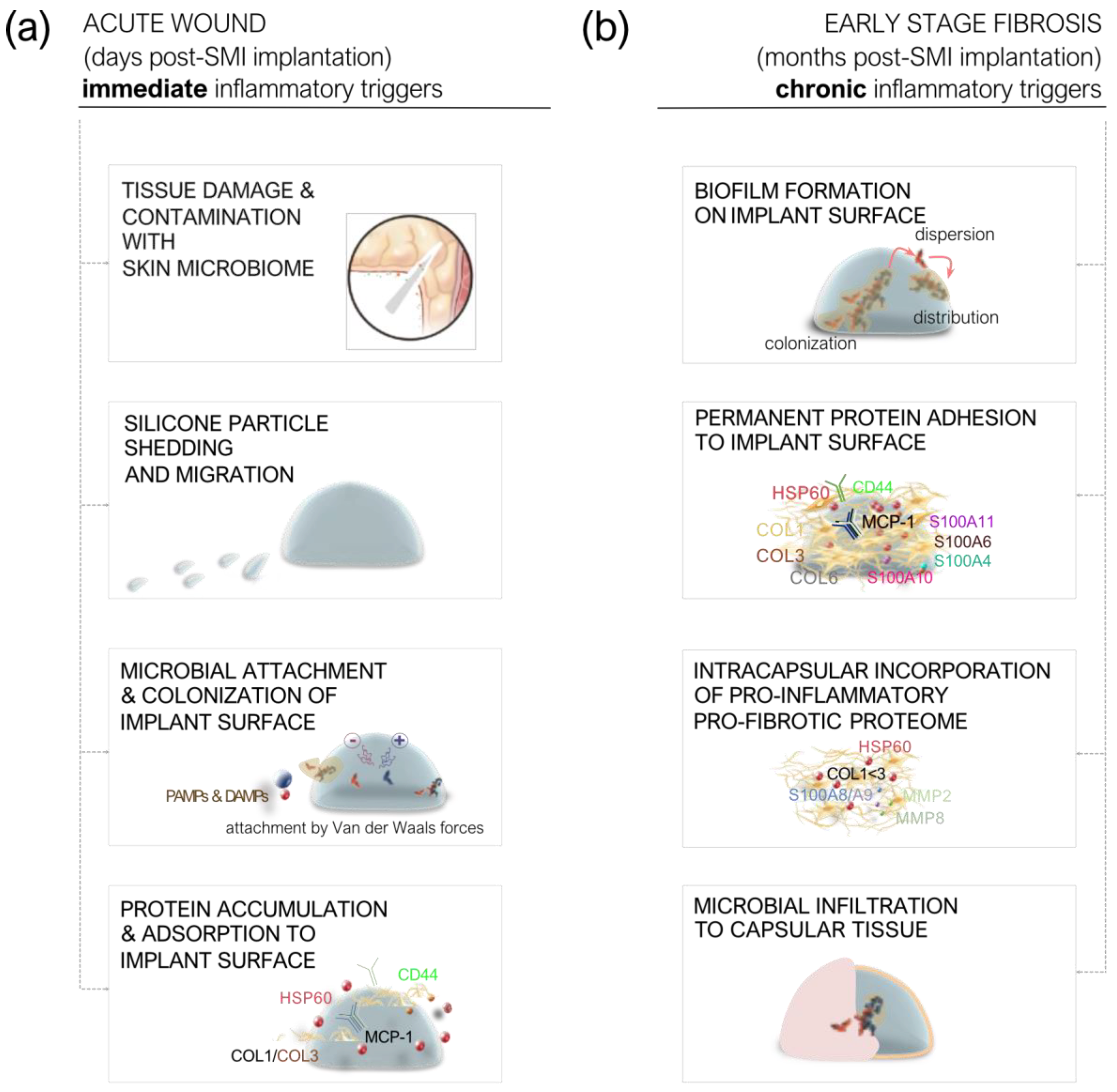
Figure 3.
Bacterial contamination and biofilm development contribute to capsular contracture. Microbial colonization during implant placement begins with the transfer of the skin microbiome to the implant surface through surgical tools and incision, embedding the implant into the lower tissue layers. Microbial Proliferation in the Acute Wound: The patient’s skin microbiome is transferred to the implant surface during surgery, via the scalpel, incision, and implant placement. Reversible Phase: In this early stage, planktonic bacteria adhere to the implant surface and the adhesive proteome through electrostatic and hydrophobic forces. At this point, the bacterial adhesion is reversible, and appropriate interventions can still prevent colonization. Irreversible Phase: As time progresses, bacteria establish a firm attachment to the surface, proliferating and forming a biofilm. The biofilm matrix shields the bacteria from the host's immune system and antimicrobial treatments, promoting a persistent infection. Capsule Formation and Contracture: The persistent presence of biofilms triggers ongoing antimicrobial inflammatory reaction, contributing to the development of a fibrous capsule around the implant. This process can result in capsular contracture, where the capsule thickens and tightens, causing complications.
Figure 3.
Bacterial contamination and biofilm development contribute to capsular contracture. Microbial colonization during implant placement begins with the transfer of the skin microbiome to the implant surface through surgical tools and incision, embedding the implant into the lower tissue layers. Microbial Proliferation in the Acute Wound: The patient’s skin microbiome is transferred to the implant surface during surgery, via the scalpel, incision, and implant placement. Reversible Phase: In this early stage, planktonic bacteria adhere to the implant surface and the adhesive proteome through electrostatic and hydrophobic forces. At this point, the bacterial adhesion is reversible, and appropriate interventions can still prevent colonization. Irreversible Phase: As time progresses, bacteria establish a firm attachment to the surface, proliferating and forming a biofilm. The biofilm matrix shields the bacteria from the host's immune system and antimicrobial treatments, promoting a persistent infection. Capsule Formation and Contracture: The persistent presence of biofilms triggers ongoing antimicrobial inflammatory reaction, contributing to the development of a fibrous capsule around the implant. This process can result in capsular contracture, where the capsule thickens and tightens, causing complications.
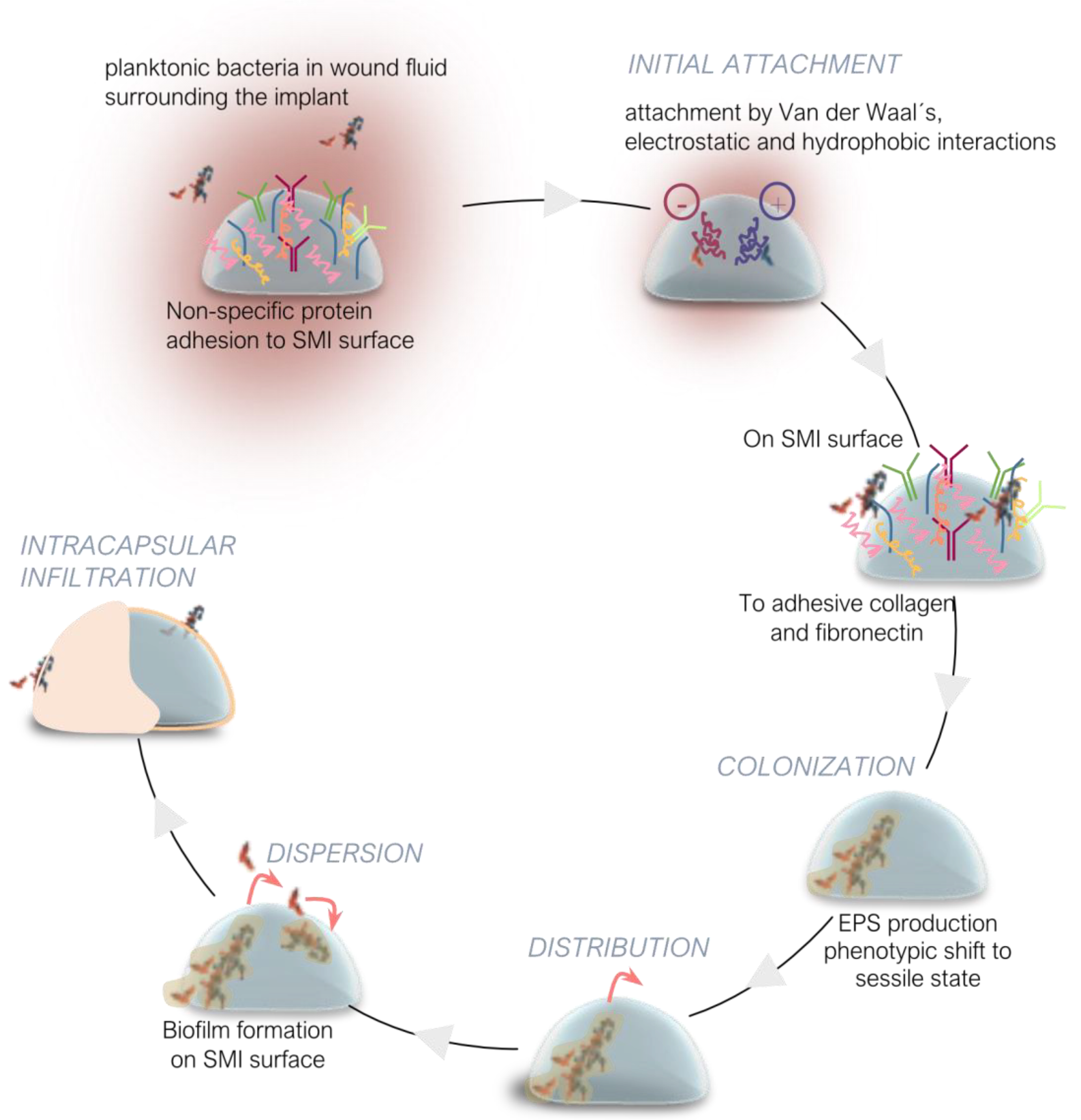
Figure 4.
Figure 4. Strategies for Reducing Capsular Contracture in Breast Implant Surgery. Infection Control and Sterilization: Proper sterilization and disinfection of medical instruments are emphasized to prevent pathogen transmission in healthcare settings [109,131,132,133,134,135]. Guidelines tailored to the specific use of medical devices and associated infection risks are critical for avoiding severe infections [109]. Antimicrobial Approaches: The effectiveness of preoperative antiseptics, including chlorhexidine gluconate and povidone-iodine, is compared, with a focus on their role in reducing biofilm-related capsular contracture [115,139]. The use of irrigation solutions such as Triple Antibiotic Solution (TAS), polyhexanide, and hypochlorous acid is also explored for biofilm eradication [54,59,60,143,144,145,146]. Surgical Techniques: Preoperative preparation, including antisepsis methods and hair removal techniques, is combined with intraoperative strategies like the no-touch technique and antimicrobial pocket irrigation to reduce bacterial exposure [161,162,165,166,167,168]. The use of sterile devices like Keller funnels and the selection of specific incision types, such as inframammary incisions, are recommended to minimize contamination risks. Postoperative Care: Proper wound management, including keeping the surgical site clean and monitoring for infections, is crucial for preventing complications and ensuring optimal surgical outcomes [137,147].
Figure 4.
Figure 4. Strategies for Reducing Capsular Contracture in Breast Implant Surgery. Infection Control and Sterilization: Proper sterilization and disinfection of medical instruments are emphasized to prevent pathogen transmission in healthcare settings [109,131,132,133,134,135]. Guidelines tailored to the specific use of medical devices and associated infection risks are critical for avoiding severe infections [109]. Antimicrobial Approaches: The effectiveness of preoperative antiseptics, including chlorhexidine gluconate and povidone-iodine, is compared, with a focus on their role in reducing biofilm-related capsular contracture [115,139]. The use of irrigation solutions such as Triple Antibiotic Solution (TAS), polyhexanide, and hypochlorous acid is also explored for biofilm eradication [54,59,60,143,144,145,146]. Surgical Techniques: Preoperative preparation, including antisepsis methods and hair removal techniques, is combined with intraoperative strategies like the no-touch technique and antimicrobial pocket irrigation to reduce bacterial exposure [161,162,165,166,167,168]. The use of sterile devices like Keller funnels and the selection of specific incision types, such as inframammary incisions, are recommended to minimize contamination risks. Postoperative Care: Proper wound management, including keeping the surgical site clean and monitoring for infections, is crucial for preventing complications and ensuring optimal surgical outcomes [137,147].
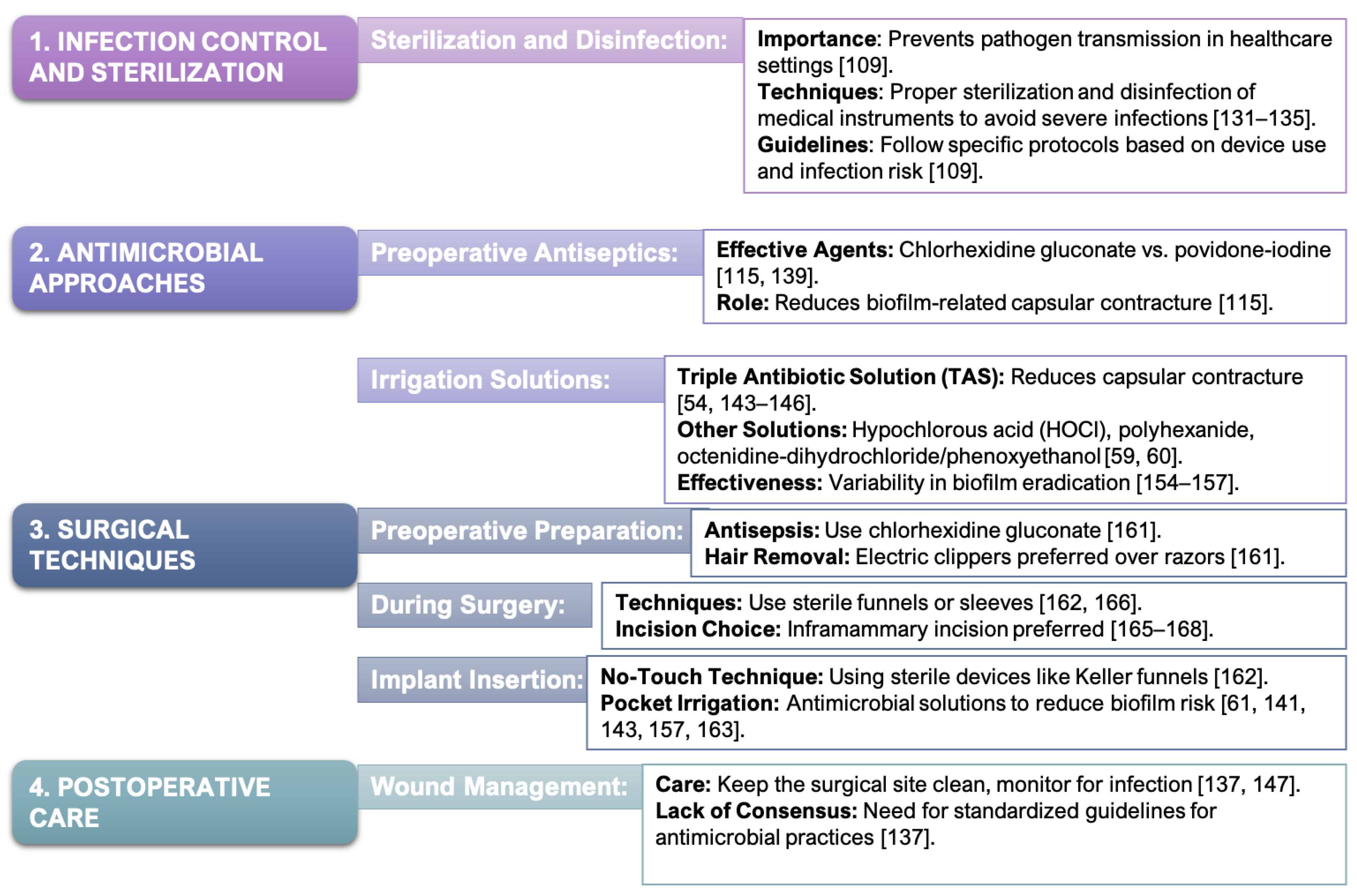

Table 1.
Key physiological processes and their impact on wound healing around silicone mammary implants.
Table 1.
Key physiological processes and their impact on wound healing around silicone mammary implants.
| Biological Mechanisms | Wound Healing Dynamics | Fibrotic Responses in SMI |
| Pathophysiological Process | Restoration of tissue integrity and function through hemostasis, inflammation, proliferation, and remodeling. | Formation of a fibrous capsule around implants due to inflammatory response and biofilm formation. |
| Initial Response | Hemostasis: Constriction of blood vessels, platelet activation, clot formation to prevent blood loss and provide a scaffold for healing. | Immediate Immune Response: Activation of innate immune system, recruitment of immune cells (neutrophils, macrophages) due to microbial contamination and protein adsorption. |
| Molecular Components | Platelets, Fibrinogen, Fibrin: Form a clot that acts as a barrier and temporary scaffold. | Microorganisms, Proteins: Microbial biofilm formation on the implant surface, leading to persistent immune stimulation. |
| Inflammatory Phase | Neutrophils and Macrophages: Clear debris, combat infection, release cytokines and MMPs to modulate the inflammatory response. | Chronic Inflammation: Persistent inflammation due to biofilm, leading to prolonged immune response and ongoing ECM remodeling. |
| Proliferation Phase | Fibroblast Proliferation, ECM Deposition, Angiogenesis, Epithelialization: Formation of new tissue, collagen production, and blood vessel formation. | Fibrous Capsule Formation: Collagen and ECM deposition around the implant, leading to capsule formation. |
| Remodeling Phase | Collagen Realignment, Cross-Linking, Continual ECM Remodeling: Strengthening of new tissue and refinement of the wound architecture. | Capsular Contracture: Excessive collagen deposition and ECM remodeling leading to a contracted and thickened fibrous capsule. |
| Impact on Healing | Prevention of Infection, Scar Formation: Effective healing reduces infection risk, minimizes scar formation, and restores tissue function. | Infection Risk: Biofilms create a persistent infection risk that complicates healing and exacerbates fibrosis. |
Table 2.
Non-pharmacological and pharmacological strategies to prevent biofilm-associated fibrosis in implants.
Table 2.
Non-pharmacological and pharmacological strategies to prevent biofilm-associated fibrosis in implants.
| Category | Strategy | Mechanism | Key Points |
|
Physical Modifications with Antimicrobial Properties |
Polyurethane Foam Coatings | Surface modification to disrupt fibrotic tissue formation | Initial reduction in fibrotic capsule formation, concerns over toxicity from degradation products [169,170,171,172]. |
|
Surface Topography |
Rough surfaces increase biofilm formation | Rougher surfaces (Ra 60 µm) enhance bacterial adhesion and biofilm maturity, leading to infections and capsular contracture [45,47,105,175]. | |
|
Biological Matrices with Antimicrobial Properties |
Antibiotic- Impregnated Meshes |
Localized antibiotic delivery to reduce biofilm formation | Effective in reducing bacterial colonization and biofilm formation with sustained antimicrobial activity [176,177,178,179]. |
|
Spider Silk- Based Meshes |
Inhibits bacterial adhesion and fibrotic tissue formation | Biocompatible, reduces fibroblast proliferation, and collagen deposition [180,181,182,183,184,185,186]. | |
|
Zwitterionic Polymers |
Superior hydrophilicity, preventing protein adsorption and microbial adhesion | Resistant to microbial colonization, preventing foreign body response and fibrotic capsules [187,188,189,190,191]. | |
|
Pharmacological Strategies |
Systemic Antibacterials (Cefazolin, Gentamicin) |
Prophylactic antibiotics to prevent infections before and during surgery | Effective against gram-positive and gram-negative bacteria in breast implant surgeries [192,193]. |
|
Topical Antibacterials (Bacitracin, Chlorhexidine) |
Direct application to reduce bacterial load and biofilm formation | Applied during surgery to prevent contamination and infection [192,194,195,196]. | |
|
Drug Incorporation into Implants (Rifampin) |
Localized, sustained antimicrobial effect from drug-coated implant surfaces | Reduces bacterial colonization and biofilm formation directly at the implant site [197]. | |
| Antifibrotic and Anti-inflammatory Drugs | Pirfenidone | Reduces inflammation and fibroblast activity | Shown to reduce capsule thickness in preclinical models, potential use in biofilm-associated fibrosis [198,199,200,201]. |
| Halofuginone | Inhibits collagen synthesis and T helper 17 cell differentiation | Reduces fibrosis and capsule formation around implants, promising antifibrotic properties [202,203,204,205]. | |
| Dexamethasone | Reduces inflammation and collagen production by modulating cytokine activity | Decreases fibrous tissue formation and inflammation, improving implant surgery outcomes [194,207,208]. | |
|
Integration of Antimicrobial and Antifibrotic Strategies |
Combined Approaches |
Use of both antimicrobial and antifibrotic strategies to prevent biofilm formation and fibrosis | Combining antibiotics with local antiseptic irrigation and antifibrotic agents enhances efficacy in preventing biofilm-associated fibrosis. |
Table 3.
Challenges, current strategies, and future directions for improving the clinical management of biofilm-associated complications in SMI-based breast surgery.
Table 3.
Challenges, current strategies, and future directions for improving the clinical management of biofilm-associated complications in SMI-based breast surgery.
| Clinical Aspect | Challenges | Current Strategies | Future Directions |
|
Biofilm Formation on SMIs |
Persistent biofilms protect bacteria from immune responses and antimicrobials, leading to chronic inflammation and fibrosis. | Antimicrobial prophylaxis, antimicrobial coatings, and advanced material surfaces designed to reduce biofilm formation. | Develop targeted antimicrobial strategies that penetrate biofilms. Biomimetic materials that release antimicrobials in response to biofilm formation. |
|
Chronic Inflammation and Fibrosis |
Biofilm matrix limits immune cell infiltration and antimicrobial effectiveness, leading to thick fibrous capsules. | Anti-inflammatory and antifibrotic agents (pirfenidone, halofuginone, dexamethasone) to reduce fibrosis. | Incorporate anti-inflammatory and antifibrotic agents into implant materials. Personalized treatment approaches based on patient immune responses. |
| Antimicrobial Resistance | Resistance to traditional antimicrobial treatments is rising, making it difficult to manage biofilm infections. | Preoperative prophylaxis with systemic antibiotics; antimicrobial materials such as antibiotic-impregnated meshes. | Novel drug delivery systems (e.g., nanoparticles or localized reservoirs) that enhance antimicrobial efficacy and overcome resistance. |
|
Advanced Materials |
Existing materials may not fully prevent microbial adhesion or fibrosis. | Antibiotic-impregnated and spider silk-based meshes, zwitterionic polymers. | Development of smart materials that dynamically respond to microbial threats, change surface properties, or release antimicrobials. |
|
Clinical Guidelines and Practice |
Variability in practices and lack of standardized guidelines lead to inconsistent management of biofilm complications. | General antimicrobial prophylaxis and surface modifications for reducing biofilm risk. | Standardized clinical guidelines for antimicrobial prophylaxis, coatings, and antifibrotic treatments across clinical settings. |
| Personalized Medicine | Generalized treatments may not consider individual patient factors, leading to suboptimal outcomes. | Uniform antibiotic and antifibrotic regimens based on general risk profiles. | Personalized treatments tailored to patient-specific factors (microbial flora, immune responses, genetic predisposition). |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



