
Submitted:
11 October 2024
Posted:
12 October 2024
You are already at the latest version
Abstract
Exergames (EG) are interactive video games that require physical activity and use gamification to make exercise more engaging. EG interventions have shown various benefits for older adults, such as improved mental health, quality of life, and reduced fall risk. Enhanced cognition is thought to drive these benefits. This review aimed to identify neural correlates underlying cognitive improvements in healthy older adults and those with neurocognitive disorders. We systematically searched major databases and included 13 studies from 2,095 records. Findings revealed that EG interventions led to structural brain changes and improved functional connectivity in healthy adults, Parkinson patients, and those with mild cognitive impairment (MCI). Increased activity in the frontal, temporal, and precuneus regions during rest was specific to adults with neurocognitive disorders. Neuroplastic changes, such as elevated BDNF levels and increased neurovascular coupling, were observed in both groups. However, methodological limitations in some studies highlight the need for further high-quality research.
Keywords:
Exergame
; Older adults
; Neurocognitive disorders
; brain
; aging brain
; EEG
; MRI
; neuroplasticity
; BDNF
1. Introduction
Promoting health through physical activity (PA) has become a worldwide priority due to the well-documented benefits of the regular practice of PA (1). Older adults are particularly concerned, as PA effectively mitigates the consequences of age-related cognitive and functional decline, diseases, and comorbidities (2). Despite this, a significant number of older adults remain inactive (3) because of various personal factors (such as motivation, fear of injuries, and intrinsic capacities) and environmental factors (such as practice locations, transportation difficulties, and infrastructure risks) (4,5). To address these barriers, an emerging research field has identified Exergames (EG) as an effective strategy to engage more older adults in PA (6).
EG are interactive and immersive video games that require the player to be physically active (7). They leverage the benefits of gamification by adding an entertaining dimension, which facilitates greater engagement (8,9). EG often utilizes commercial home video game consoles, such as the Nintendo Wii ® and Xbox Kinect ®, where participants are required to perform some physical tasks to play. Some other formats require participants to step on platforms or floor mats, while responding to visual cues or movement instructions (10–12). Furthermore, there is also the opportunity to use technologies within the Extended Reality (XR) continuum allowing us to model the physical world in a digital immersive environment (13). This has been leveraged for safe PA practice in the form of EG in realistic immersive conditions, thereby limiting the constraints inherent to environmental factors (14–18), particularly in augmented or mixt reality setups (19).
A growing body of evidence supports the notion that EG interventions not only increase older adults' levels of PA but also yield numerous clinical benefits. Recent systematic reviews and meta-analyses reported that healthy older adults who engage in EG interventions improved their quality of life and mental health (20–22), and reduced the risk of fall incidents (12,23,24) and even had lower cognitive impairment cases (25). Moreover, numerous Randomized Controlled Trials (RCT) reported similar effects of EG in reducing falls or improving quality of life as compared to conventional PA interventions (aerobic fitness, resistance training, stretching…) (23,26). These benefits of EG interventions are even more relevant, as the clinical outcomes mentioned above affect most older adults, often imposing a substantial burden on their daily lives.
Moreover, since motor and cognitive functioning progressively decline in both normal and pathological aging (27,28), several studies have investigated whether improvement in such functions would be the principal targets that are responsible for the benefits of EG interventions. Most studies investigated cognitive abilities and demonstrated that EG would lead to improvement in global cognition(17,21,29,30) or in specific domains such as executive functions (31,32) or memory (33). Noteworthy, EG benefits on motor domains are more controversial (17,34) despite existing data on EG-related improved performance in balance or gait evaluations (35,36). Most studies suggest that this might be the result of the intensity of interventions which is insufficient to maximize improvements in motor functions (17,34). Overall, one can understand that improvement in cognitive and motor abilities would be the principal targets of EG interventions. Such improvements can be the result of modifications in several behavioral and physiological mechanisms. Therefore, it appears crucial to identify the underlying mechanisms that give rise to the above-mentioned benefits of EG interventions.
Understanding the underlying mechanisms of EG interventions will enhance our knowledge and help us determine the key factors that could moderate the benefits, thereby optimizing the interventions for maximum efficacy. Given the fact that improvements in cognitive functions are the primary benefits of EG interventions (17,34), one can assume that these gains would be associated with key neural correlates. Interestingly, examining the effects of EG on brain is especially relevant, since the cognitive benefits of PA are believed to be associated with changes in the brain at three levels: structural, functional, and molecular (37,38). Indeed, there is existing evidence of PA (aerobic and resistance training) substantially modifying brain structure by augmenting brain volume in areas such as hippocampus or prefrontal cortex (PFC) (39,40). These effects of PA are supported by other findings suggesting improved resting state functional networks (e.g., Default Mode Network (DMN)) or other specific task-related networks (37,38). Other effects of PA such as elevated levels of neurotrophic factors (e.g., Brain-Derived Neurotrophic Factors (BDNF), Insulin-like Growth Factor (IGF)) (41–43) or enhanced neurovascular coupling (44,45) might further stimulate neuroplastic changes.
Thus, recent review studies have investigated the effects of EG interventions on brain functions (46–48). The results suggest neuroplastic changes that include augmented levels of BDNF and improved activity within neural networks during the processing of cognitive tasks (e.g., attention, working memory). This effect on neural networks was measured using functional Near-Infrared Spectroscopy (fNIRS) or scalp Electroencephalogram (EEG), with results suggesting higher recruitment of specialized neural networks and reduced reliance on compensatory networks. This is particularly interesting considering the model of scaffolding theory of aging and cognition which explains how different brain variables, both structural and functional, are related to cognitive functions (49). Indeed, the CRUNCH hypothesis of this model may explain the benefits of EG interventions, particularly by suggesting that older adults, when relying on compensatory networks, recruit additional neural resources and display hyperactivation during low-demand tasks to meet performance demand (50,51). Overall, current evidence suggests that the cognitive behavioral benefits of EG interventions can be associated with the neurobiological aspects of age-related functional decline.
Nevertheless, some aspects of the effects of EG interventions on brain structures and functions were not covered in these previous review studies (46–48). First, there is a lack of studies investigating all three levels—structural, functional, and molecular of the effects on the brain. Additionally, since technologies for conducting EG continue to advance rapidly, there is a need for updated research and literature that examines these emerging tools and their impact on neural correlates. Most importantly, the previous review studies only considered healthy older adults while studying neural correlates. However, it is demonstrated that EG interventions can also benefit older adults with neurocognitive disorders(10,18,25,32,33,52,53). In addition, it is well established that neurocognitive disorders are progressive, affecting cerebral bases across all three levels—structural, functional, and molecular. Thus, it is particularly relevant to consider this population to investigate whether EG can trigger brain modifications that are relevant to neurocognitive disorders.
In the present study, our objective was two-fold. First, we aimed to expand on previous review studies by examining recent studies that shed light on the neural correlates of EG interventions in aging, focusing on changes in the brain structure, functional networks and molecular markers. Second, we extended the range of our population of interest to include older adults with a neurocognitive disorder, assessing whether EG interventions impacted neural correlates relevant to these diseases.
2. Methods
2.1. Search Strategy
The research question of the present review was designed using the PICO framework as follows: Population (Older adults with or without a neurocognitive disorder), Intervention (Exergame), Control (One-arm study, passive (no activity, usual activity, education), or active (physical or cognitive)), Outcome (neural correlates: gray-matter volume, connectivity, neuroplasticity biomarkers). The search was conducted in accordance with updated PRISMA guidelines (Page et al., 2021), in June 2024 across the following electronic registries: PubMed, Cochrane Library, Embase, Science Direct, and Scopus. The search strings included terms combined with "OR" and "AND" operators as follows: (older adults OR elder OR elderly OR seniors OR aging OR ageing) AND (Exergame OR Exergaming OR Virtual Reality OR Mixed Reality OR Augmented Reality OR Extended Reality OR Wii OR Kinect OR PlayStation OR Interactive Videogame OR Active Video Game) AND (Neurobiology OR Neurophysiology OR Neural OR Brain).
2.2. Eligibility Criteria
The screening (duplicates, titles and abstracts, and full texts) was conducted by two independent researchers with a consensual meeting for conflict resolution afterwards. After the duplicate removals and the title and abstracts screening, the remaining reports were retrieved for full-text screening to determine eligibility for inclusion. Full-text articles were eligible for inclusion in this review study if they met the following criteria: 1) published in peer-reviewed scientific journals, 2) written in English, 3) included healthy older adults (mean age 60 or older), or older adults with a neurocognitive disorder, 4) examined the effects of an EG intervention in at least one group, and 5) performed a noninvasive measurement of neural correlates (brain structure or activity) was the primary or secondary outcome investigated in the study. Moreover, the studies with the following intervention were not considered: technology-assisted PA without a gamified dimension, additional interventions alongside EG within a multidomain approach.
2.3. Data Extraction and Quality Assessment
For each article included, the following elements were independently extracted by two researchers, with a consensual meeting for conflict resolution afterwards. They reported the following items: 1) Metadata (Authors, year of publication country), 2) Characteristics of the study population, 3) intervention settings (design, duration, intensity), 4) type of EG 5) type of setup used for the measurement of neural correlates, and 5) main findings. Finally, the methodological quality was assessed through the risk of bias tool provided by Cochrane Collaboration (Higgins et al., 2011).
3. Results
3.1. Study Selection
We identified 2,095 records following the initial search. After removals of duplicates (n =375) and the title and abstract screening (n = 1676 removed), we searched for the full texts of 44 reports that were screened for eligibility criteria resulting in 31 additional removals (see Figure 1). Therefore, we included 13 studies in the present systematic review that investigated the neural correlates of EG interventions in older adults with or without a neurocognitive disorder. Tables 1 and 2 summarize the characteristics and findings of the included studies based on the items extracted as presented in the method section.
3.2. Study Participants, Design and Interventions
Ten studies included healthy older adults (mean age = 72 years), while the remaining three involved participants with a neurocognitive disorder: Parkinson's disease (n=1; mean age = 66 years) and MCI (n=2; mean age 75 years). The studies were conducted worldwide, including in the USA, Europe, South America, and Asia. Most studies (n=10) utilized a randomized controlled approach, one was non-randomized and the remaining two were one-arm where all participants performed the EG intervention.
The interventions lasted between 4 to 24 weeks (mean duration = 10 weeks), averaging three sessions per week which lasted 20-100 minutes. Most of the studies (n=8) indicated that a moderate to vigorous intensity was applied for the tasks, while the others (n=5) did not mention intensity levels. The EG utilized two types of technology: console-based formats such as Wii, Microsoft Kinect, computer-based or TV-based (n=11), and digital environments implemented in virtual reality (VR) (n=2). The primary focus of EG was balance, stepping and sometimes sport-based movements (i.e., soccer, baseball…). Cycling was also leveraged, with added cognitive tasks on screen to enhance the gamified experience. Two studies involving Parkinson or MCI patients, used games that targeted upper-limb coordination.
3.3. Neural Correlates of Exergame Interventions
The effects were structured regarding the impact on: gray-matter volume, connectivity, and neuroplasticity biomarkers.
3.3.1. Healthy Older Adults
A first Magnetic Resonance Imaging (MRI) study with a voxel-based-morphometric analysis reported no gray-matter volume change after EG intervention on 31 participants (54). On the contrary, another study found an increase in the global volume of whole-brain gray matter as well as in superior parietal lobule and frontal gyrus. However, this latter study used less conservative statistical threshold (uncorrected for multiple comparisons) and did not included covariates such as sex or the total intracranial volume (55). Critically, both studies reported improved global cognition or executive functions (54,55).
Regarding neurofunctional results, a first study involving a justified sample size of 52 older adults and corrected statistical threshold showed low movement-related EEG features (event-related desynchronization (ERD), contingent negative variation (CNV)) during stepping tasks, particularly during gait initiation (56). EG-related brain changes were also found during cognitive tasks (attention, working memory) as outlined by low oxyhemoglobin in the PFC assessed by fNIRS (57). There were also reduced hemodynamic activity within PFC, sensory or motor cortices during motor tasks (balance, stepping or walking) with both fNIRS (58) and functional MRI (fMRI) methods (59). Furthermore, changes in characteristic EEG features of event related potentials (delayed latency of N2 and P3 after stimulus presentation) were also found in other studies, though with a limited number of participants (60,61). Noteworthy, each time where the above-mentioned functional markers were observed, the studies also reported enhanced performances during cognitive evaluations (56,58–61).
In addition to the previous macroscopic structural and functional changes, there was an increase in BDNF levels (62,63), cerebral blood flow (CBF) and cerebrospinal fluid (CSF)(55), suggestive of vascular resistance and increased neuroplasticity.
3.3.2. Older Adults with a Neurocognitive Disorder
An MRI study exhibited a correlation between increased volumes in the PFC, the anterior cingulate cortex and improved performance on cognitive evaluations in 8 MCI patients (64). Other changes in brain activity were reported during resting state period and included fMRI data of enhanced precuneus activity in Parkinson patients (65) but without direct comparison between classical brain network mapped during resting state (i.e., DMN, VIS, DAN, etc.). One study also found EEG markers of enhanced resting-state activity in MCI patients, including decreases in parietal theta activity, the theta-to-beta ratio (TBR), and the delta-to-alpha ratio (DAR) in frontal and temporal lobes, along with increased alpha connectivity (66). However, the study primarily compared EG interventions to a conventional exercise group, and post-hoc statistical comparisons with a passive control group were not reported. In addition, BDNF levels also increased in one study involving MCI patients (64). Furthermore, one study revealed that the inclusion of challenging cognitive tasks in the EG would increase the benefits (enhanced activity in some regions during resting state) in MCI patients (64). Noteworthy all these neural correlates of EG interventions in older adults were accompanied by enhanced performances in evaluations of global cognition and executive functioning (64–66).
3.3.3. EG vs Conventional Interventions
The studies that compared EG interventions and conventional trainings yielded controversial results. Four studies with healthy older adults suggested that EG interventions and conventional trainings had the same effects on brain functions(56–58,60), whereas two studies suggested that EG interventions induced more benefits (BDNF level and theta activity) than conventional aerobic and resistance trainings (61,63). This superiority regarding the effects of EG was also found in another study with Parkinson patients with enhanced activity in the precuneus during resting state (65). Only one study, conducted in MCI patients, found more benefits (enhanced activity during resting state) in conventional trainings compare to EG interventions (66).
3.4. Quality Assesment
Among the 13 studies reviewed, 6 were identified as having a low risk of bias(54,56–58,61,65), three had a moderate risk of bias (59,63,64), and the remaining four were highly biased (55,60,62,66). The moderate risk of bias was primarily due to an unclear explanation of the randomization process. Regarding the four studies with a high risk of bias the reasons were the following: absence of randomization or calculation of a sample size with sufficient statistic power before the experiment, and one-arm studies lacking a control group.
Additionally, several neuroimaging studies faced methodological limitations that may hinder the interpretation and generalizability of their findings. In studies examining brain volume changes, appropriate morphometric analyses to avoid the risk of false positive results were not consistently applied. Furthermore, key task- or rest-related neural networks were often overlooked, with a focus placed instead on specific brain regions relevant to the task, which may have obscured a comprehensive understanding of the activity within classical neural networks assessed during resting-state paradigm
4. Discussion
The present review focused on the neural correlates of EG interventions in older adults with or without a neurocognitive disorder. The post-intervention effects identified in healthy older adults included increased brain volumes and changes in the activities of certain brain regions during the execution of both cognitive and motor tasks. In addition, EG interventions also benefited Parkinson and MCI patients with positive changes in the brain structure and particularly enhanced activities in certain brain regions during resting state. Moreover, these benefits were accompanied by neuroplastic changes with augmented BDNF levels or improved neurovascular coupling in both populations.
4.1. Neural Correlates of EG Interventions in Healthy Older Adults
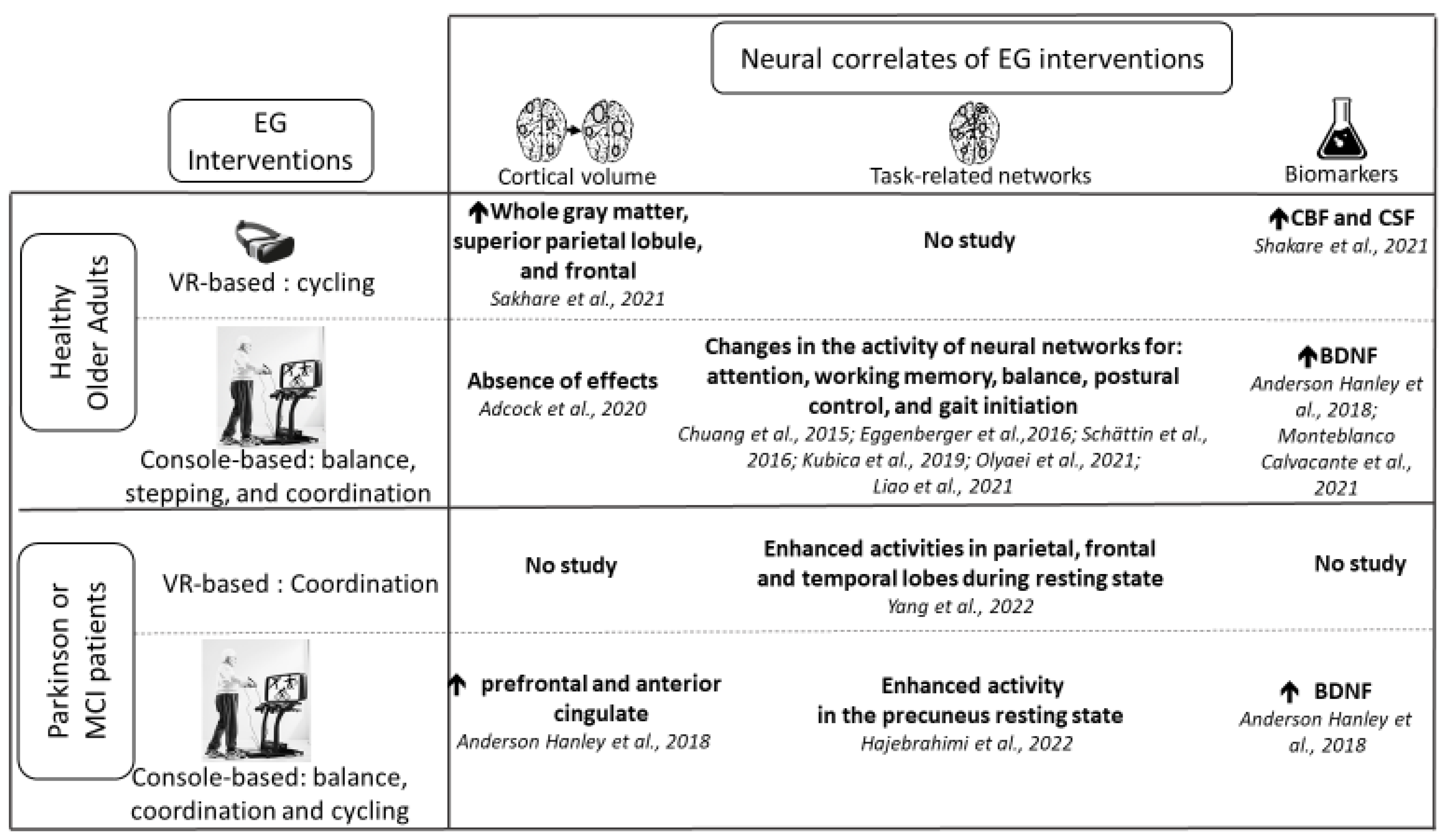
A summary of the current knowledge can be found in Figure 2 which displays key neural correlates of EG interventions relevant for brain health in both healthy and pathological aging.
Regarding healthy older adults, several findings on the effects of EG interventions are in line with the results of the previous review studies conducted on the topic: changes of activity in brain regions during cognitive tasks (e.g., attention, working memory), and elevated levels of BDNF (46–48).
Furthermore, restricting the search strategy exclusively to studies that investigated neural correlates proved beneficial, as we identified three recent studies involving healthy older adults that were not included in previous review studies. One such study found after the EG intervention, increased brain volumes including in parietal and frontal regions in MRI scans, which is a new finding (55). The absence of the effects of EG intervention on brain volume has been previously explained by the light intensity of intervention (54). This might align with the findings of Sakhare et al. (55), whose intervention involved moderate to vigorous intensity. Nevertheless, it is important to note that these findings remain preliminary with some methodological concerns. Indeed, the study employed a one-arm design without limiting the risk of inflation for Type I error or accounting for covariables such as sex and total brain volume. More conservative neuroimaging studies are required to confirm this result. Noteworthy, they further identified new insights into the effects of EG regarding neuroplastic changes including increased CBF and CSF dynamics (55) which align with the known positive effects of exercise on cardiovascular fitness (67) and the clearance and dynamics of CSF(68,69).
Moreover, other studies reported in the present review also suggest that compared to baseline values, there was a decrease in hemodynamic activity in brain areas responsible for postural control (59), and reduced motor-related EEG features (ERD and CNV) during gait initiation (56), after the intervention. One can hypothesize that this could be a result of efficient processing of neural networks during the execution of these tasks. This would be a consequence of EG interventions that benefited motor functions by improving their cognitive control (measured here by changes in neural networks). Indeed, it is well documented that EG involves several cognitive-motor challenges (34), thereby enhancing the need for supplementary cognitive control of motor tasks. Thus, increases in attentional control required during these complex situations are thought to benefit task-related neural networks and to enhance performance (70–72). Nevertheless, as the effects of EG interventions on physical abilities are not widely documented (17,34), it remains to be confirmed whether improvements in motor functions following EG interventions are linked to changes in well identified neural networks.
4.2. Neural Correlates of EG Interventions in Older Adults with a Neurocognitive Disorder
Extending the population to include older adults with neurocognitive disorders revealed new and interesting findings of the neural correlates of EG interventions in MCI and Parkinson patients. A study found increased volumes in prefrontal and anterior cingulate cortices following EG interventions in MCI patients (64). This is particularly interesting as it suggests that EG interventions lead to increased volume in regions crucial for cognitive functions such as memory, attention, and executive functions, which are especially relevant for patients with this neurocognitive disorder. Consequently, such interventions could potentially slow the reduction of brain volume in these areas, leading to functional benefits. However, this study employs correlational methods and analyzed the data of only 8 participants exposing some serious statistical limits. Since one may recognize the challenges of patient recruitment, future studies using statistical methods tailored for small sample sizes could offer valuable insights (73).
Some other authors further reported changes in post-intervention resting-state activity in some brain regions [decreases in parietal theta, TBR and DAR, increase in alpha (66) and increased activity in the precuneus cortex (65)] compared to baseline values, in Parkinson patients. These findings on resting-state connectivity are interesting as the neuroimaging indicators reported are closely associated with networks such as the DMN (74–76) which is known to be enhanced by PA (37,38). However, there remain certain limitations regarding the neuroimaging indicator reported, including the lack of investigation into specific networks or weak effect sizes in the results. In addition, it remains to be determined whether there exists a direct relationship between EG interventions and improvements in brain functional connectivity during resting state. This information is even more relevant since most neurocognitive disorders in aging are progressive, with each stage of the disease affecting functional brain connectivity differently (77,78). Therefore, future studies are warranted to identify which specific aspects of functional connectivity are improved by EG and to apply the intervention at the most appropriate stage of the disease.
4.3. Moderators of the Effects of EG Interventions on Brain Functions
Interestingly, the technology used to perform the EG appears to target different neural correlates (Figure 2). One study using VR-based EG interventions improved cortical volume (55) in healthy older adults. Given that the immersive nature of VR technologies has been shown to significantly impact brain activity (79), it can be assumed that VR-based EG interventions may engage different neural networks compared to console-based EG. Nevertheless, with the current state of knowledge and the design of studies included in this review, it is speculative to conclude about the specific effects of different technologies on brain functions. Given the significant potential of VR-based or more generally XR-based EG in engaging older adults in PA, further research is needed to clarify its specific benefits.
Furthermore, only a few studies in the present review have analyzed how specific features impact the effects of EG interventions on the brain. Most studies reported moderate intensity levels of PA for EG, suggesting that this intensity is sufficient to induce benefits. However, none of the studies considered the intensity as a variable to examine its impact on the effects of EG. One study showed that incorporating complex cognitive tasks positively influence brain outcomes (increased brain volume; (64)). Since additional cognitive tasks require increased executive control, it might be possible that the recruitment of certain networks during the EG execution correlates with post-intervention benefits. To confirm this hypothesis, it is necessary to determine which specific networks are activated during this addition of more cognitive tasks during EG execution. However, to achieve this, it is crucial to understand how EG execution alters brain in the first place. Our search in the present review indicates that this information is still missing from the existing literature.
4.4. Real-Time Neural Responses to the Execution of EG
While the post-intervention effects of EG interventions on brain functions have been well described in the studies included in this review, evidence of how EG modifies brain functions during gameplay is still lacking. This information is crucial for deepening our understanding of the benefits of the efficiency of neural networks by clarifying how executing EG contributes to strengthening the recruitment of specialized networks (80). In addition, it may also shed light on the strategies that older adults employ to adapt to complex situations in the EG, particularly whether they rely on compensatory mechanisms as suggested by the CRUNCH hypothesis (50,51). During our literature search, we found two studies that have examined how the brain behave during the execution of the EG. We could not include these studies in the present review as they did not meet the eligibility criteria. However, we discussed below their intriguing insights which deserve to be confirmed in future studies.
The first study conducted in healthy older adults found that engaging in balance and stepping EG triggered increased theta activity in the frontal region (81). Authors attributed this to the heightened attentional demand during the EG, as frontal theta activity is strongly associated with attentional control(82–84). This study also observed a decrease in alpha-activity in the parietal lobe, which also aligns with increase attentional demand in previous findings involving a dual-task training among older adults (85). In the second study involving Parkinson patients, there was an increase in overall beta activity, as well as temporal and frontal alpha activity during the execution of a VR-based EG with upper-limb coordination (86). This result supports the previous one in healthy older adults (81) since the role of beta activity in attentional process is well studied (87). However, it was unexpected that EG would trigger a rise in alpha activity, which is known to occur in relaxation states. The authors speculated that the immersive nature of VR-based EG, which minimizes external environmental interference, might enhance this relaxation and thus memory capacity as previously suggested (88). This is noteworthy as VR-based EGs, or more generally XR-based, have the potential to overcome environmental barriers and engage more people in PA (15–18). Nevertheless, it is important to consider that Munoz et al.'s study (86) was conducted in Parkinson patients and include only upper-limb coordination movements in the EG. Thus, it remains to be determined whether baseline health status or other types of EG can influence the observed effects of immersive VR technology on brain functions. Overall, these two studies present evidence supporting the idea that while executing an EG there could be an increase in attentional demand and memory capacity in older adults which can be measured by EEG features (81,86)
Interestingly, it is plausible that the benefits of EG interventions on neural networks might be the result of neuroplastic changes (e.g., synaptogenesis, potentiation) due to the repetitive recruitment of such networks during the execution of the EG (80). This hypothesis is particularly enlightening given the fact that reduced frontal theta activity was one of the post-intervention effects of EG interventions (58,61) and that the execution of a similar EG triggered an increase in the same frontal theta activity (81). Thus, training to recruit specialized networks during the EG execution might be one of the reasons of the benefits on neural networks in related tasks measured here with frontal theta activity. Nevertheless, this hypothesis remains to be confirmed as brain activity during EG was delineated at the lobe level (81,86) and thus need to be investigated with neuroimaging techniques with higher spatial resolution. The fMRI stands out as a strong option but is limited to the application of motor imagery to perform an EG as participants need to limit movements in the MRI scanner. Conversely, EEG could offer valuable insights as it can be applied during motor tasks and allows for analyses such as signal coherence or phase synchronization-based measures, which can serve as proxies for MRI brain functional connectivity measures (89–91).
Moreover, the two studies that investigated how EG modifies brain functions (81,86) provided averaged brain activity across the entire EG session without specific information about each stage of the games. Since EG involves complex decision-making processes (6), different stages of the game may differentially impact neural networks. Thus, some stages might be more cognitively demanding or more effective in recruiting and strengthening neural networks, than others. This information is crucial for optimizing the potential of EG in enhancing neural network efficiency.
4.5. Future Directions
Considering the present findings, we propose a series of experiments to better understand the underlying neurobiology of an EG, which has shown clinical benefits and is well accepted by older adults. First, it is crucial to investigate how EG modifies brain functions by examining attentional control networks and other specialized networks throughout different stages of the game and according to the intensity and the type of technology used. Additionally, it could be valuable to investigate the emotional states and motivation of participants during each stage of the EG by leveraging well-described EEG features associated with relaxation or focus (92,93). Identifying such markers could help boost positive emotions, encouraging more older adults to engage in EG, as its primary goal is to use the gamified elements to improve adherence (6). This approach will allow us to optimize the game design, enhancing stages that are most likely to induce the most neural efficiency or positive emotions. Comparing older adults to younger counterparts could help determine if certain effects are more pronounced or specific to older adults. At this stage, an optimized game design of EG can be developed leveraging neural correlates that are the most positively impacted during the EG execution. Following this, post-intervention effects should be examined with neuroimaging techniques with high spatiotemporal resolution to identify specific changes (e.g., functional connectivity, brain volume) that can be indicative of certain stages of neurocognitive disorders or other age-related diseases. This will aid in designing appropriate interventions for patients at various stages of these conditions. EEG technique can be applied in this study of the brain activity during mobility, as it offers a reliable solution to detect age-related brain changes that are relevant to various types of neurocognitive disorders (94).
5. Conclusion
The present systematic review aimed to deepen our understanding of the neural correlates of EG interventions in older adults, both with and without neurocognitive disorders. On average, moderate-intensity EG interventions led to increased brain volumes in crucial areas for brain health, such as the PFC, and changes in neural networks responsible for postural control and gait initiation in healthy older adults. Notably, individuals with MCI and Parkinson's disease also experienced similar benefits from EG interventions, showing increased brain volume and improved neural networks, particularly in resting activity networks. To be fully validated, some of these findings, especially those related to changes in brain structure or functional networks, require further investigations in higher-quality studies. Moreover, the structural and functional changes in brain functions were further supported by evidence on markers of enhanced neuroplasticity. The present findings highlight the potential of EG interventions to improve brain functions and suggest that carefully considering these effects can help maximize the benefits.
References
- McPhee JS, French DP, Jackson D, Nazroo J, Pendleton N, Degens H. Physical activity in older age: perspectives for healthy ageing and frailty. Biogerontology. 2016 Jun;17(3):567–80. [CrossRef]
- Eckstrom E, Neukam S, Kalin L, Wright J. Physical Activity and Healthy Aging. Clin Geriatr Med. 2020 Nov;36(4):671–83. [CrossRef]
- Clemente Remón ÁL, Jiménez Díaz-Benito V, Jiménez Beatty JE, Santacruz Lozano JA. Levels of Physical Activity Among Older Adults in the European Union. J Aging Phys Act. 2021 Apr 1;29(2):242–9.
- Bethancourt HJ, Rosenberg DE, Beatty T, Arterburn DE. Barriers to and Facilitators of Physical Activity Program Use Among Older Adults. Clin Med Res. 2014 Sep;12(1–2):10–20. [CrossRef]
- Rúa-Alonso M, Bovolini A, Costa-Brito AR, Vaz C, Marques E, Serra N, et al. Exploring Perceived Barriers to Physical Activity among Older Adults Living in Low-Population Density Regions: Gender Differences and Associations with Activity Dimensions. Healthcare (Basel). 2023 Nov 11;11(22):2948. [CrossRef]
- Mazeas A, Duclos M, Pereira B, Chalabaev A. Evaluating the Effectiveness of Gamification on Physical Activity: Systematic Review and Meta-analysis of Randomized Controlled Trials. J Med Internet Res. 2022 Jan 4;24(1):e26779.
- Vázquez FL, Otero P, García-Casal JA, Blanco V, Torres ÁJ, Arrojo M. Efficacy of video game-based interventions for active aging. A systematic literature review and meta-analysis. PLOS ONE. 2018 Dec 11;13(12):e0208192. [CrossRef]
- Baranowski T, Buday R, Thompson DI, Baranowski J. Playing for Real: Video Games and Stories for Health-Related Behavior Change. Am J Prev Med. 2008 Jan;34(1):74-82.e10.
- Sardi L, Idri A, Fernández-Alemán JL. A systematic review of gamification in e-Health. J Biomed Inform. 2017 Jul;71:31–48. [CrossRef]
- Altorfer P, Adcock M, de Bruin ED, Graf F, Giannouli E. Feasibility of Cognitive-Motor Exergames in Geriatric Inpatient Rehabilitation: A Pilot Randomized Controlled Study. Front Aging Neurosci. 2021;13:739948. [CrossRef]
- Gallou-Guyot M, Mandigout S, Marie R, Robin L, Daviet JC, Perrochon A. Feasibility and potential cognitive impact of a cognitive-motor dual-task training program using a custom exergame in older adults: A pilot study. Front Aging Neurosci. 2023;15:1046676. [CrossRef]
- Sturnieks DL, Hicks C, Smith N, Ratanapongleka M, Menant J, Turner J, et al. Exergame and cognitive training for preventing falls in community-dwelling older people: a randomized controlled trial. Nat Med. 2024 Jan;30(1):98–105. [CrossRef]
- Levac DE, Huber ME, Sternad D. Learning and transfer of complex motor skills in virtual reality: a perspective review. J Neuroeng Rehabil. 2019 Oct 18;16(1):121. [CrossRef]
- Béraud-Peigné N, Maillot P, Perrot A. The User Experience of an Immersive and Interactive Wall Exergame in Older Adults. Games Health J. 2023 Jun;12(3):220–7. [CrossRef]
- Campo-Prieto P, Cancela-Carral JM, Rodríguez-Fuentes G. Feasibility and Effects of an Immersive Virtual Reality Exergame Program on Physical Functions in Institutionalized Older Adults: A Randomized Clinical Trial. Sensors (Basel). 2022 Sep 6;22(18):6742. [CrossRef]
- Drazich BF, Anokye D, Zhu S, Teleb J, Galik E, Colloca L, et al. Motivating older adults through immersive virtual exercise (MOTIVE): A randomized pilot study. Geriatr Nurs. 2023;54:229–36. [CrossRef]
- Gallou-Guyot M, Mandigout S, Bherer L, Perrochon A. Effects of exergames and cognitive-motor dual-task training on cognitive, physical and dual-task functions in cognitively healthy older adults: An overview. Ageing Res Rev. 2020 Nov;63:101135. [CrossRef]
- Sokolov AA, Collignon A, Bieler-Aeschlimann M. Serious video games and virtual reality for prevention and neurorehabilitation of cognitive decline because of aging and neurodegeneration. Curr Opin Neurol. 2020 Apr;33(2):239–48. [CrossRef]
- Chen M, Tang Q, Xu S, Leng P, Pan Z. Design and Evaluation of an Augmented Reality-Based Exergame System to Reduce Fall Risk in the Elderly. Int J Environ Res Public Health. 2020 Oct 1;17(19):7208. [CrossRef]
- Chao YY, Scherer YK, Montgomery CA. Effects of using Nintendo WiiTM exergames in older adults: a review of the literature. J Aging Health. 2015 Apr;27(3):379–402.
- Yen HY, Chiu HL. Virtual Reality Exergames for Improving Older Adults’ Cognition and Depression: A Systematic Review and Meta-Analysis of Randomized Control Trials. J Am Med Dir Assoc. 2021 May;22(5):995–1002. [CrossRef]
- Fernandes CS, Magalhães B, Lima A, Nóbrega P, Silva M, Santos C. Impact of Exergames on the Mental Health of Older Adults: A Systematic Review and GRADE Evidence Synthesis. Games Health J. 2022 Jul 11; [CrossRef]
- Chen Y, Zhang Y, Guo Z, Bao D, Zhou J. Comparison between the effects of exergame intervention and traditional physical training on improving balance and fall prevention in healthy older adults: a systematic review and meta-analysis. J Neuroeng Rehabil. 2021 Nov 24;18(1):164. [CrossRef]
- Chan JKY, Klainin-Yobas P, Chi Y, Gan JKE, Chow G, Wu XV. The effectiveness of e-interventions on fall, neuromuscular functions and quality of life in community-dwelling older adults: A systematic review and meta-analysis. Int J Nurs Stud. 2021 Jan;113:103784. [CrossRef]
- Abd-Alrazaq A, Alajlani M, Alhuwail D, Toro CT, Giannicchi A, Ahmed A, et al. The Effectiveness and Safety of Serious Games for Improving Cognitive Abilities Among Elderly People With Cognitive Impairment: Systematic Review and Meta-Analysis. JMIR Serious Games. 2022 Mar 10;10(1):e34592. [CrossRef]
- Ogawa EF, You T, Leveille SG. Potential Benefits of Exergaming for Cognition and Dual-Task Function in Older Adults: A Systematic Review. J Aging Phys Act. 2016 Apr;24(2):332–6. [CrossRef]
- van der Willik KD, Licher S, Vinke EJ, Knol MJ, Darweesh SKL, van der Geest JN, et al. Trajectories of Cognitive and Motor Function Between Ages 45 and 90 Years: A Population-Based Study. J Gerontol A Biol Sci Med Sci. 2021 Jan 18;76(2):297–306.
- Attoh-Mensah E, Pothier K, Loggia G, Morello R, Chavoix C, Marcelli C. Involvement of cognitive abilities in the occurrence of fractures in fallers aged 55 years or older: a cross-sectional study. Aging Clin Exp Res. 2024 Aug 30;36(1):180. [CrossRef]
- Gavelin HM, Dong C, Minkov R, Bahar-Fuchs A, Ellis KA, Lautenschlager NT, et al. Combined physical and cognitive training for older adults with and without cognitive impairment: A systematic review and network meta-analysis of randomized controlled trials. Ageing Res Rev. 2021 Mar;66:101232. [CrossRef]
- Manser P, Herold F, de Bruin ED. Components of effective exergame-based training to improve cognitive functioning in middle-aged to older adults – A systematic review and meta-analysis. Ageing Research Reviews. 2024 Aug 1;99:102385. [CrossRef]
- Wollesen B, Wildbredt A, van Schooten KS, Lim ML, Delbaere K. The effects of cognitive-motor training interventions on executive functions in older people: a systematic review and meta-analysis. Eur Rev Aging Phys Act. 2020 Dec;17(1):9. [CrossRef]
- Abd-Alrazaq A, Alhuwail D, Ahmed A, Househ M. Effectiveness of Serious Games for Improving Executive Functions Among Older Adults With Cognitive Impairment: Systematic Review and Meta-analysis. JMIR Serious Games. 2022 Jul 25;10(3):e36123. [CrossRef]
- Abd-Alrazaq A, Alhuwail D, Al-Jafar E, Ahmed A, Shuweihdi F, Reagu SM, et al. The Effectiveness of Serious Games in Improving Memory Among Older Adults With Cognitive Impairment: Systematic Review and Meta-analysis. JMIR Serious Games. 2022 Aug 9;10(3):e35202. [CrossRef]
- Torre MM, Temprado JJ. A Review of Combined Training Studies in Older Adults According to a New Categorization of Conventional Interventions. Front Aging Neurosci [Internet]. 2022 Feb 1 [cited 2024 Oct 3];13. Available from: https://www.frontiersin.org/journals/aging-neuroscience/articles/10.3389/fnagi.2021.808539/full. [CrossRef]
- Suleiman-Martos N, García-Lara R, Albendín-García L, Romero-Béjar JL, Cañadas-De La Fuente GA, Monsalve-Reyes C, et al. Effects of active video games on physical function in independent community-dwelling older adults: A systematic review and meta-analysis. J Adv Nurs. 2022 May;78(5):1228–44. [CrossRef]
- Leal JC, Belo VS, Santos IM, Ferreira RV, de Melo SN, da Silva ES. Exergames in Older Adult Community Centers and Nursing Homes to Improve Balance and Minimize the Risk of Falls in Older Adults: A Systematic Review and Meta-Analysis. Healthcare (Basel). 2023 Jun 28;11(13):1872. [CrossRef]
- Stillman CM, Esteban-Cornejo I, Brown B, Bender CM, Erickson KI. Effects of Exercise on Brain and Cognition Across Age Groups and Health States. Trends Neurosci. 2020 Jul;43(7):533–43. [CrossRef]
- Boa Sorte Silva NC, Barha CK, Erickson KI, Kramer AF, Liu-Ambrose T. Physical exercise, cognition, and brain health in aging. Trends Neurosci. 2024 Jun;47(6):402–17. [CrossRef]
- Erickson KI, Voss MW, Prakash RS, Basak C, Szabo A, Chaddock L, et al. Exercise training increases size of hippocampus and improves memory. Proc Natl Acad Sci U S A. 2011 Feb 15;108(7):3017–22. [CrossRef]
- Erickson KI, Leckie RL, Weinstein AM. Physical activity, fitness, and gray matter volume. Neurobiol Aging. 2014 Sep;35 Suppl 2:S20-28.
- Hötting K, Röder B. Beneficial effects of physical exercise on neuroplasticity and cognition. Neurosci Biobehav Rev. 2013 Nov;37(9 Pt B):2243–57. [CrossRef]
- Cassilhas RC, Tufik S, de Mello MT. Physical exercise, neuroplasticity, spatial learning and memory. Cell Mol Life Sci. 2016 Mar;73(5):975–83.
- Monteiro-Junior RS, da Silva Figueiredo LF, Maciel-Pinheiro P de T, Abud ELR, Braga AEMM, Barca ML, et al. Acute effects of exergames on cognitive function of institutionalized older persons: a single-blinded, randomized and controlled pilot study. Aging Clin Exp Res. 2017 Jun;29(3):387–94. [CrossRef]
- Pellegrini-Laplagne M, Dupuy O, Sosner P, Bosquet L. Acute Effect of a Simultaneous Exercise and Cognitive Task on Executive Functions and Prefrontal Cortex Oxygenation in Healthy Older Adults. Brain Sci. 2022 Mar 28;12(4):455. [CrossRef]
- Pellegrini-Laplagne M, Dupuy O, Sosner P, Bosquet L. Effect of simultaneous exercise and cognitive training on executive functions, baroreflex sensitivity, and pre-frontal cortex oxygenation in healthy older adults: a pilot study. Geroscience. 2023 Feb;45(1):119–40. [CrossRef]
- Torre MM, Temprado JJ. Effects of Exergames on Brain and Cognition in Older Adults: A Review Based on a New Categorization of Combined Training Intervention. Front Aging Neurosci. 2022 Mar 30;14:859715. [CrossRef]
- Yang Y, Wang K, Liu S, Liu H, Zhang T, Luo J. Exergames improve cognitive function in older adults and their possible mechanisms: A systematic review. J Glob Health. 13:04177. [CrossRef]
- Stojan R, Voelcker-Rehage C. A Systematic Review on the Cognitive Benefits and Neurophysiological Correlates of Exergaming in Healthy Older Adults. J Clin Med. 2019 May 23;8(5):734. [CrossRef]
- Reuter-Lorenz PA, Park DC. How Does it STAC Up? Revisiting the Scaffolding Theory of Aging and Cognition. Neuropsychol Rev. 2014 Sep;24(3):355–70. [CrossRef]
- Reuter-Lorenz PA, Lustig C. Brain aging: reorganizing discoveries about the aging mind. Current Opinion in Neurobiology. 2005 Apr 1;15(2):245–51. [CrossRef]
- Festini SB, Zahodne L, Reuter-Lorenz PA. Theoretical Perspectives on Age Differences in Brain Activation: HAROLD, PASA, CRUNCH—How Do They STAC Up? In: Oxford Research Encyclopedia of Psychology [Internet]. Oxford University Press; 2018 [cited 2024 Jun 7]. Available from: https://oxfordre.com/psychology/view/10.1093/acrefore/9780190236557.001.0001/acrefore-9780190236557-e-400.
- Zhao Y, Feng H, Wu X, Du Y, Yang X, Hu M, et al. Effectiveness of Exergaming in Improving Cognitive and Physical Function in People With Mild Cognitive Impairment or Dementia: Systematic Review. JMIR Serious Games. 2020 Jun 30;8(2):e16841. [CrossRef]
- Manser P, Michels L, Schmidt A, Barinka F, de Bruin ED. Effectiveness of an Individualized Exergame-Based Motor-Cognitive Training Concept Targeted to Improve Cognitive Functioning in Older Adults With Mild Neurocognitive Disorder: Study Protocol for a Randomized Controlled Trial. JMIR Res Protoc. 2023 Feb 6;12:e41173. [CrossRef]
- Adcock M, Fankhauser M, Post J, Lutz K, Zizlsperger L, Luft AR, et al. Effects of an In-home Multicomponent Exergame Training on Physical Functions, Cognition, and Brain Volume of Older Adults: A Randomized Controlled Trial. Front Med [Internet]. 2020 Jan 28 [cited 2024 Jul 19];6. Available from: https://www.frontiersin.org/journals/medicine/articles/10.3389/fmed.2019.00321/full. [CrossRef]
- Sakhare A, Stradford J, Ravichandran R, Deng R, Ruiz J, Subramanian K, et al. Simultaneous Exercise and Cognitive Training in Virtual Reality Phase 2 Pilot Study: Impact on Brain Health and Cognition in Older Adults. Brain Plast. 2021;7(2):111–30. [CrossRef]
- Olyaei G, Khanmohammadi R, Talebian S, Hadian MR, Bagheri H, Najafi M. The effect of exergaming on cognition and brain activity in older adults: A motor- related cortical potential study. Physiol Behav. 2022 Oct 15;255:113941. [CrossRef]
- Liao YY, Chen IH, Hsu WC, Tseng HY, Wang RY. Effect of exergaming versus combined exercise on cognitive function and brain activation in frail older adults: A randomised controlled trial. Ann Phys Rehabil Med. 2021 Sep;64(5):101492. [CrossRef]
- Eggenberger P, Wolf M, Schumann M, de Bruin ED. Exergame and Balance Training Modulate Prefrontal Brain Activity during Walking and Enhance Executive Function in Older Adults. Front Aging Neurosci. 2016;8:66. [CrossRef]
- Kubica J, Szymura J, Domagalik A, Golda S, Wiecek M, Fafrowicz M, et al. Systematic Balance Exercises Influence Cortical Activation and Serum BDNF Levels in Older Adults. J Clin Med. 2019 Nov 7;8(11). [CrossRef]
- Chuang LY, Hung HY, Huang CJ, Chang YK, Hung TM. A 3-month intervention of Dance Dance Revolution improves interference control in elderly females: a preliminary investigation. Exp Brain Res. 2015 Apr;233(4):1181–8. [CrossRef]
- Schättin A, Arner R, Gennaro F, de Bruin ED. Adaptations of Prefrontal Brain Activity, Executive Functions, and Gait in Healthy Elderly Following Exergame and Balance Training: A Randomized-Controlled Study. Front Aging Neurosci. 2016;8:278.
- Monteblanco Cavalcante M, Fraga I, Dalbosco B, De Marchi P, Iraci L, Baechtold da Silva ME, et al. Exergame training-induced neuroplasticity and cognitive improvement in institutionalized older adults: A preliminary investigation. Physiol Behav. 2021 Nov 1;241:113589. [CrossRef]
- Anderson-Hanley C, Arciero PJ, Brickman AM, Nimon JP, Okuma N, Westen SC, et al. Exergaming and older adult cognition: a cluster randomized clinical trial. Am J Prev Med. 2012 Feb;42(2):109–19.
- Anderson-Hanley C, Barcelos NM, Zimmerman EA, Gillen RW, Dunnam M, Cohen BD, et al. The Aerobic and Cognitive Exercise Study (ACES) for Community-Dwelling Older Adults With or At-Risk for Mild Cognitive Impairment (MCI): Neuropsychological, Neurobiological and Neuroimaging Outcomes of a Randomized Clinical Trial. Front Aging Neurosci. 2018;10:76. [CrossRef]
- Hajebrahimi F, Velioglu HA, Bayraktaroglu Z, Helvaci Yilmaz N, Hanoglu L. Clinical evaluation and resting state fMRI analysis of virtual reality based training in Parkinson’s disease through a randomized controlled trial. Sci Rep. 2022 May 16;12(1):8024. [CrossRef]
- Yang JG, Thapa N, Park HJ, Bae S, Park KW, Park JH, et al. Virtual Reality and Exercise Training Enhance Brain, Cognitive, and Physical Health in Older Adults with Mild Cognitive Impairment. Int J Environ Res Public Health. 2022 Oct 15;19(20). [CrossRef]
- van der Kleij LA, Petersen ET, Siebner HR, Hendrikse J, Frederiksen KS, Sobol NA, et al. The effect of physical exercise on cerebral blood flow in Alzheimer’s disease. Neuroimage Clin. 2018;20:650–4. [CrossRef]
- Frederiksen KS, Gjerum L, Waldemar G, Hasselbalch SG. Effects of Physical Exercise on Alzheimer’s Disease Biomarkers: A Systematic Review of Intervention Studies. J Alzheimers Dis. 2018;61(1):359–72. [CrossRef]
- Miyazaki M, Malis V, Yamamoto A, Kungsamutr J, McEvoy LK, McDonald MA, et al. Physical Exercise Alters Egress Pathways for Intrinsic CSF Outflow: An Investigation Performed with Spin-labeling MR Imaging. Magn Reson Med Sci. 2024 Apr 1;23(2):171–83. [CrossRef]
- Xiao Y, Yang T, Shang H. The Impact of Motor-Cognitive Dual-Task Training on Physical and Cognitive Functions in Parkinson’s Disease. Brain Sci. 2023 Mar 3;13(3):437. [CrossRef]
- Grosboillot N, Gallou-Guyot M, Lamontagne A, Bonnyaud C, Perrot A, Allali G, et al. Towards a Comprehensive Framework for Complex Walking tasks: Characterization, Behavioral Adaptations, and Clinical Implications in Ageing and Neurological Populations. Ageing Research Reviews. 2024 Aug 15;102458. [CrossRef]
- Attoh-Mensah E, Huret A, Leger M, Loggia G, Nee G, Largilliere S, et al. A Dual-Task Paradigm Combining Physical and Cognitive Training in Mice: Application to Aging. Aging Dis. 2024 Feb 14; [CrossRef]
- Schwarzkopf DS, Huang Z. A simple statistical framework for small sample studies [Internet]. bioRxiv; 2023 [cited 2024 Sep 25]. p. 2023.09.19.558509. Available from: https://www.biorxiv.org/content/10.1101/2023.09.19.558509v1.
- Massar S a. A, Rossi V, Schutter DJLG, Kenemans JL. Baseline EEG theta/beta ratio and punishment sensitivity as biomarkers for feedback-related negativity (FRN) and risk-taking. Clin Neurophysiol. 2012 Oct;123(10):1958–65. [CrossRef]
- Fransson P, Marrelec G. The precuneus/posterior cingulate cortex plays a pivotal role in the default mode network: Evidence from a partial correlation network analysis. Neuroimage. 2008 Sep 1;42(3):1178–84. [CrossRef]
- Thibes RB, Novaes NP, Lucato LT, Campanholo KR, Melo LM, Leite CC, et al. Altered Functional Connectivity Between Precuneus and Motor Systems in Parkinson’s Disease Patients. Brain Connect. 2017 Dec;7(10):643–7. [CrossRef]
- Tessitore A, Cirillo M, De Micco R. Functional Connectivity Signatures of Parkinson’s Disease. J Parkinsons Dis. 2019;9(4):637–52. [CrossRef]
- Malotaux V, Dricot L, Quenon L, Lhommel R, Ivanoiu A, Hanseeuw B. Default-Mode Network Connectivity Changes During the Progression Toward Alzheimer’s Dementia: A Longitudinal Functional Magnetic Resonance Imaging Study. Brain Connect. 2023 Jun;13(5):287–96. [CrossRef]
- Lier EJ, Oosterman JM, Assmann R, de Vries M, van Goor H. The effect of Virtual Reality on evoked potentials following painful electrical stimuli and subjective pain. Sci Rep. 2020 Jun 3;10(1):9067. [CrossRef]
- van Balkom TD, van den Heuvel OA, Berendse HW, van der Werf YD, Vriend C. The Effects of Cognitive Training on Brain Network Activity and Connectivity in Aging and Neurodegenerative Diseases: a Systematic Review. Neuropsychol Rev. 2020 Jun;30(2):267–86. [CrossRef]
- Müller H, Baumeister J, Bardal EM, Vereijken B, Skjæret-Maroni N. Exergaming in older adults: the effects of game characteristics on brain activity and physical activity. Front Aging Neurosci. 2023;15:1143859. [CrossRef]
- Cavanagh JF, Frank MJ. Frontal theta as a mechanism for cognitive control. Trends Cogn Sci. 2014 Aug;18(8):414–21. [CrossRef]
- Büchel D, Lehmann T, Ullrich S, Cockcroft J, Louw Q, Baumeister J. Stance leg and surface stability modulate cortical activity during human single leg stance. Exp Brain Res. 2021 Apr;239(4):1193–202. [CrossRef]
- Jacobsen NSJ, Blum S, Witt K, Debener S. A walk in the park? Characterizing gait-related artifacts in mobile EEG recordings. Eur J Neurosci. 2021 Dec;54(12):8421–40. [CrossRef]
- Bohle H, Rimpel J, Schauenburg G, Gebel A, Stelzel C, Heinzel S, et al. Behavioral and Neural Correlates of Cognitive-Motor Interference during Multitasking in Young and Old Adults. Neural Plast. 2019;2019:9478656. [CrossRef]
- Muñoz D, Barria P, Cifuentes CA, Aguilar R, Baleta K, Azorín JM, et al. EEG Evaluation in a Neuropsychological Intervention Program Based on Virtual Reality in Adults with Parkinson’s Disease. Biosensors (Basel). 2022 Sep 12;12(9). [CrossRef]
- Sauseng P, Klimesch W. What does phase information of oscillatory brain activity tell us about cognitive processes? Neurosci Biobehav Rev. 2008 Jul;32(5):1001–13.
- Magosso E, De Crescenzio F, Ricci G, Piastra S, Ursino M. EEG Alpha Power Is Modulated by Attentional Changes during Cognitive Tasks and Virtual Reality Immersion. Computational Intelligence and Neuroscience. 2019;2019(1):7051079. [CrossRef]
- Shamsi F, Haddad A, Najafizadeh L. Early classification of motor tasks using dynamic functional connectivity graphs from EEG. J Neural Eng. 2021 Feb 22;18(1). [CrossRef]
- Gérard M, Bayot M, Derambure P, Dujardin K, Defebvre L, Betrouni N, et al. EEG-based functional connectivity and executive control in patients with Parkinson’s disease and freezing of gait. Clin Neurophysiol. 2022 May;137:207–15. [CrossRef]
- Hatlestad-Hall C, Bruña R, Liljeström M, Renvall H, Heuser K, Taubøll E, et al. Reliable evaluation of functional connectivity and graph theory measures in source-level EEG: How many electrodes are enough? Clin Neurophysiol. 2023 Jun;150:1–16.
- Kalashami MP, Pedram MM, Sadr H. EEG Feature Extraction and Data Augmentation in Emotion Recognition. Comput Intell Neurosci. 2022;2022:7028517. [CrossRef]
- Hu W, Zhang Z, Zhao H, Zhang L, Li L, Huang G, et al. EEG microstate correlates of emotion dynamics and stimulation content during video watching. Cereb Cortex. 2023 Jan 5;33(3):523–42. [CrossRef]
- Ramanoël S, Durteste M, Delaux A, de Saint Aubert JB, Arleo A. Future trends in brain aging research: Visuo-cognitive functions at stake during mobility and spatial navigation. Aging Brain. 2022 Jan 1;2:100034. [CrossRef]
Figure 1.
Flowchart of study selection.
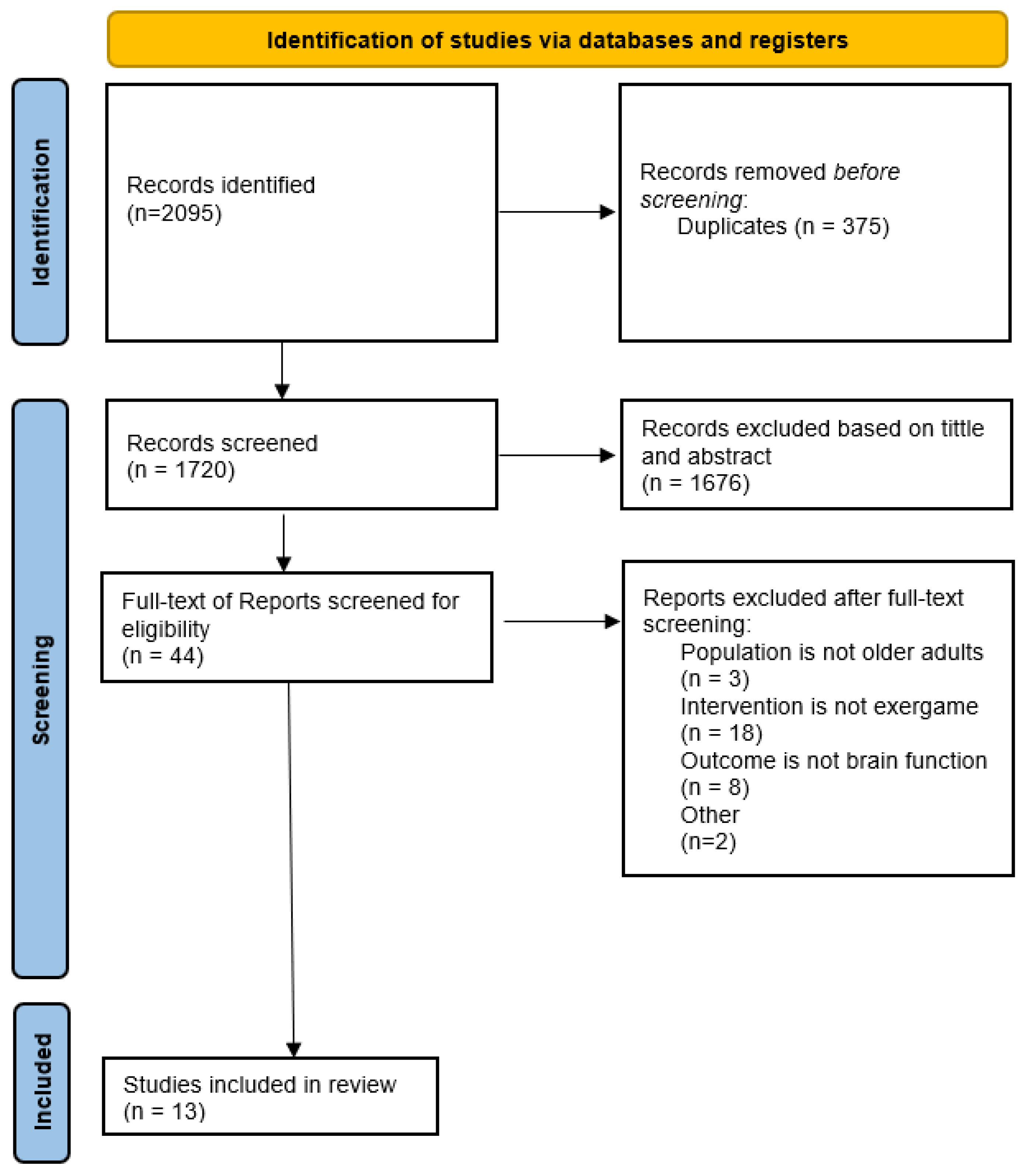
Figure 2.
Summary of the current literature on the neural correlates of exergame (EG) interventions in older adults with or without cognitive disorders. The left column lists various types of EG interventions, and the technologies used to implement them. The right column details the post-intervention effects of EG. The rows represent the segregation of older adults according to their health status. MCI: Mild Cognitive Impairment; VR: virtual reality; CBF: Cerebral Blood Flow; CSF: Cerebrospinal Fluid; BDNF: Brain-derived Neurotrophic Factor.
Figure 2.
Summary of the current literature on the neural correlates of exergame (EG) interventions in older adults with or without cognitive disorders. The left column lists various types of EG interventions, and the technologies used to implement them. The right column details the post-intervention effects of EG. The rows represent the segregation of older adults according to their health status. MCI: Mild Cognitive Impairment; VR: virtual reality; CBF: Cerebral Blood Flow; CSF: Cerebrospinal Fluid; BDNF: Brain-derived Neurotrophic Factor.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



