
Submitted:
11 October 2024
Posted:
14 October 2024
You are already at the latest version
Abstract
Mosquito-borne diseases are a major public health issue. The United States has experienced mosquito-borne disease outbreaks, including West Nile virus, Zika, dengue, and malaria, highlighting widespread risk across the country. In the United States, exposure to mosquito vectors primarily occurs outdoors. Individuals experiencing unsheltered homelessness are particularly vulnerable to mosquito-borne diseases due to their increased exposure to mosquito vectors, limited access to healthcare, and high prevalence of underlying conditions. This review aims to examine the literature on mosquito-borne disease infections among individuals experiencing homelessness in the United States between 1999 and 2024. Our search strategy used Boolean methods on PubMed, Scopus, and Web of Science to select relevant publications. Two queries were used: the first query focuses on individuals experiencing homelessness and mosquito-borne diseases, and the second one focuses on epidemiological analyses of mosquito-borne disease outbreaks in the US. Only studies reporting at least 1 infection among individuals experiencing homelessness were included. Our search resulted in the identification of 347 studies. After screening them, 8 were ultimately included in this review. Half of the studies identified West Nile virus among individuals experiencing homelessness and the other half reported cases of malaria. These studies show that individuals experiencing homelessness are more exposed to mosquitoes, face a higher risk of infection, and have an increased likelihood of hospitalization due to mosquito-borne diseases compared to the general population. The full extent of mosquito-borne disease exposure among individuals experiencing homelessness remains unclear. With climate change and globalization, there is a consensus in the literature showing an increasing risk of mosquito-borne disease transmission in the next decades, and we have already started to witness this increasing trend. Therefore, we argue that developing policies aimed at providing homeless populations with housing during mosquito-borne disease outbreaks could be instrumental in protecting this segment of the population and promoting health equity.
Keywords:
Aedes
; Anopheles
; Culex
; chikungunya
; dengue
; malaria
; West Nile
; Zika
Introduction
Mosquito-borne diseases (MBDs) represent a constant public health threat. In the United States, the risk of MBDs varies based on differences in occupational and socioeconomic conditions. In the United States, exposure to mosquito vectors primarily occurs outdoors [1,2] and is predominantly attributed to occupational settings, socioeconomic conditions, and outdoor leisure activities [3,4,5]. For example, blue-collar occupations where the work is conducted primarily outdoors have shown positive associations with the risk of exposure to mosquito vectors [6]. Additionally, mosquito vector abundance is higher in low-income communities, increasing the risk of exposure to mosquito vectors in these areas [3]. This leads to a highly variable health burden and risk of exposure to MBDs for different population groups [7,8,9,10,11].
People experiencing unsheltered homelessness – people living in places not meant for human habitation [12] – spend a disproportionate amount of time outdoors [13], increasing their risk of exposure to mosquito vectors. Unsheltered homelessness is a large and growing problem in the United States, and the growth in unsheltered homelessness is responsible for the recent steep increases in the overall nationwide homeless population [12]. Currently, approximately 653,000 people are homeless on any given night in the United States, of which 40% are unsheltered, however, existing data severely underestimates the true size of the unsheltered population [14,15].
Many vulnerable and marginalized populations, who face a higher risk for poor health outcomes, are overrepresented in the unsheltered homeless population. These groups include Black and Indigenous people [16], military veterans, people exiting incarceration, and older adults [17,18,19]. Additionally, individuals experiencing homelessness have worse overall health [20,21,22,23,24] and are disproportionately affected by other diseases, including mental disorders, substance misuse, and premature death [25]. The unsheltered homeless population also has less access to health care compared to the housed resident population [21]. Consequently, this places them at an increased risk of severe health outcomes in case of an infection [26].
In this study, we conduct a literature review to provide insights into the transmission of mosquito-borne disease infections among the population experiencing homelessness in the United States over the period from 1999 to 2024.
Methods
Diseases of Interest
Search Queries
A search strategy using Boolean methods on PubMed (https://pubmed.ncbi.nlm.nih.gov), Scopus (https://www2.scopus.com), and Web of Science (https://mjl.clarivate.com) was used to select the existing publications about homelessness and mosquito-borne diseases in the United States. The search was conducted on September 17, 2024, considering the title, abstract, keywords, and main text. To conduct this search, we used two independent queries:
- Query 1: (homeless* OR "transient population" OR "transient communit*") AND (mosquito* OR arbovir* OR dengue OR malaria OR Zika OR chikungunya OR "West Nile" OR DENV OR CHIKV OR ZIKV OR WNV) AND ("United States" OR "USA")
- Query 2: (Outbreak OR Epidemic) AND (locally acquired OR autochthonous) AND (Mosquito-borne OR Mosquito-Transmitted OR arbovir* OR dengue OR malaria OR Zika OR chikungunya OR "West Nile" OR DENV OR CHIKV OR ZIKV OR WNV) AND ("United States" OR "USA")
The first query focuses on individuals experiencing homelessness and mosquito-borne diseases, and the second one focuses on epidemiological analyses of mosquito-borne disease outbreaks in the US. The second query allows us to retrieve papers whose focus is not on individuals experiencing homelessness, but where cases of mosquito-borne diseases may have been reported in this population group. For both queries, we limited the search period from 1999, the year when WNV was first introduced in the US, to 2024.
Each retrieved study was independently assessed by 3 reviewers (A.B.B.W., M.D.H., and A.G.K.). Any discrepancies in study selection and/or its content were addressed through discussion and consensus.
Inclusion and Exclusion Criteria
Studies were included if they satisfied the following criteria: (1) the study focused on West Nile, chikungunya, dengue, Zika, or malaria; (2) the study investigated local transmission in the United States between 1999 and 2024; (3) the study reported at least 1 infection among individuals experiencing homelessness.
We excluded study protocols, media news, commentaries, or manuscripts where the full text was unavailable (e.g., conference abstract).
Scope of Review and Analysis
In this literature review we did not perform a meta-analysis, sensitivity analysis, or other synthesis methods. As such, there is no description of statistical heterogeneity, summary statistics, models, effect measures, or assessment of bias and certainty. Furthermore, no methods were employed to explore causes of heterogeneity, such as subgroup analysis or meta-regression. Therefore, no software packages were utilized or described.
Data Availability
The data supporting this systematic review are drawn from previously reported studies, all of which have been cited. All necessary data for replicating the study’s findings are available within the manuscript.
Results
Our search resulted in the identification of 347 studies, 22 from Query 1 and 325 from Query 2 (Figure 1). Among them, 41 studies (9 from Query 1 and 32 from Query 2) were excluded as they did not focus on West Nile, chikungunya, dengue, Zika, or malaria; 242 studies (3 from Query 1 and 239 from Query 2) were excluded as they did not investigate local transmission of one of these diseases in the United States between 1999 and 2024; 56 studies (6 from Query 1 and 50 from Query 2) did not report at least 1 infection among the population experiencing homelessness. None of the retrieved results was a study protocol, media news, commentary, or a manuscript where the full text was unavailable. As per the inclusion/exclusion criteria, we identified 8 articles (4 from Query 1 and 4 from Query 2) to include in this review [7,32,33,34,35,36,37,38].
The identified studies provide evidence of MBD infection among the homeless population. The two most recent malaria outbreaks in the US, which took place in 2003 and 2023, reported cases among individuals experiencing homelessness [33,36,37,39]. In the 2003 outbreak, 1 of the 8 cases of malaria was an individual experiencing homelessness [36,39]. The same strain of Plasmodium vivax was identified in all eight cases through laboratory hematology [39]. In 2023, 3 of the 8 locally acquired cases were among individuals experiencing homelessness [33]. Several of the studies identified West Nile virus among individuals experiencing homelessness [7,32,38]. One study tested for West Nile virus among pets, identifying 10 positive cases where 50% were among pets of unhoused owners [34]. None of the studies reported evidence of chikungunya virus, dengue virus, or Zika virus in the population experiencing homelessness.
A key element among all the included studies was the emphasis on risk factors associated with MBDs. In particular, they highlight the positive associations between time spent outdoors with the risk of MBDs [7,35,36,37], with one study showing that >6 hours of outdoor exposure increases the risk of West Nile virus infection [7]. There was also a greater risk of severe health outcomes resulting in hospitalizations among individuals experiencing homelessness compared to the general population [32]. Furthermore, a positive association was found between the risk of MBDs and HIV infection as well as risk-taking behaviors (i.e., injection drug use and heavy drinking) among individuals experiencing homelessness [38], supporting the greater risk of severe health outcomes.
Table 1 provides a summary of the findings relevant to the risk of MBDs among individuals experiencing homelessness for all studies identified in this review.
Discussion
Our literature review yielded a small number of studies that examine the transmission of MBD infections among individuals experiencing homelessness in the US between 1999 and 2024. The 8 studies eligible for this review provide evidence of MBD infection among individuals experiencing homelessness. Half of the studies in this review identified West Nile virus among individuals experiencing homelessness. To properly interpret this finding, it is important to consider that among the diseases analyzed in this review, West Nile is the only one endemic in the continental US, with thousands of locally acquired infections reported every year [40]. Our review also provides evidence of malaria cases in the population experiencing homelessness. A possible contributing factor is that both West Nile virus and Plasmodium species mosquito vectors are nocturnal, exhibiting heightened host-seeking activity during the night when individuals experiencing homelessness are asleep and thus more exposed to infective bites [41]. On the other hand, none of the studies included in this review reported Zika, chikungunya, or dengue among individuals experiencing homelessness. For Zika and chikungunya, this is likely due to the low level of local circulation in the continental US: 13 reported locally acquired chikungunya virus infection in 2014-2015, and 231 reported locally acquired Zika virus infection in 2016-2017; for both diseases, no other recent locally acquired infections have been reported [42,43]. Local outbreaks of dengue have occurred each year for the last three years (2022 – 2024) [44]; however, estimates from the CDC suggest that the number of locally transmitted dengue cases is greatly underreported in the United States and a multiplication factor of 21-105 is needed to correct for the under-reporting of the number of laboratory-positive dengue inpatients (i.e., reporting rate of 1.0%-4.8%) [45]. This highlights the challenges in identifying dengue cases among the population experiencing homelessness. Nonetheless, it is worth remarking that competent mosquito vector species for all the focus diseases are present and locally abundant in the continental US [46,47]; therefore, the evidence of West Nile virus and malaria among individuals experiencing homelessness found in this review could expand to other MBDs in the near future.
Our initial search of the literature highlighted the difficulty in identifying literature to include due to the rarity of studies that examine MBDs among individuals experiencing homelessness as their main focus. For this reason, we included a second search query that focused on all local outbreaks in the US between 1999 and 2024 and included those where at least one infection among the homeless population was reported. However, we expect a high level of underreporting in this population group given their lower access to healthcare [20,21,22,23,24]. Moreover, the notification rate for the focus diseases is relatively low and the number of local outbreaks of MBDs in the continental US is limited.
The identified studies showed that individuals experiencing homelessness are at a greater risk of MBDs compared to the general population. Identified factors that increase the risk of MBDs included spending extended periods of time outdoors and engaging in risk-taking behaviors, such as drug and alcohol use, and HIV infection. However, these conclusions about the risk factors for MBDs among homeless populations are based on a limited pool of studies and cannot be assessed through a systematic meta-analysis. Nevertheless, these findings suggest important implications about potential risk factors that can be further examined in future studies.
Mosquito control is the most commonly adopted method to reduce MBD risk of transmission and associated health burden [48,49]. Other options include installing mosquito screens and AC units [50,51]. Assistance programs may be set up to provide support to low-income households or they could be required in rental properties. However, for individuals experiencing homelessness, other options should be considered. During the malaria outbreak in Florida in 2003, which included one case among the population experiencing homelessness, the public health response included outreach activities in homeless shelters [35]. Other targeted strategies may be worth of consideration. For example, rapid rehousing pairs time-limited financial assistance used for housing-related expenses with supportive services (e.g., landlord mediation, connections to health services) to move individuals experiencing homelessness into housing as quickly as possible [52]. A targeted influx of funding could be used to quickly scale up this intervention to help the unsheltered population get into housing during MBD outbreaks. Another option could be permanent supportive housing which pairs an ongoing, full housing subsidy with intensive supportive services (e.g., intensive case management, connections to behavioral health services) [53] and provides a long-term positive impact on housing stability [54]. This intervention could be targeted to certain unsheltered homeless individuals who would otherwise be unable to exit homelessness on their own or with a less intensive intervention like rapid rehousing. Finally, in many communities, congregate emergency shelter (i.e., dormitory/barracks-style arrangements) is the only emergency housing available for people who are homeless, but they cannot accommodate the entire unsheltered population. In response to the COVID-19 pandemic, individuals experiencing homelessness were placed in private hotel and motel rooms [55] which had positive health, psychological, and housing impacts [56]. A similar approach could be used to quickly house a large number of unsheltered persons in the context of an MBD outbreak. The implementation of combinations of these non-mutually exclusive public health interventions targeting both mosquito and human populations could be considered to reduce the risk of mosquito-borne disease transmission.
Given the challenges of implementing the aforementioned policies in the current situation for the US, which is characterized by a low incidence of MBDs [44,57], the effectiveness of these interventions can be tested with mathematical models [58,59]. These models can be developed to simulate the implementation of interventions in-silico prior to their real-world implementation, providing key indications to policymakers as was the case in previous epidemics [45,60,61,62,63]. With climate change and globalization, there is a consensus in the literature showing an increasing risk of MBD transmission in the next decades [28,29,64,65,66] and policies aimed at reducing the impact of climate change in urban areas (e.g., planting trees, reducing impervious surfaces) could contribute to the proliferation of mosquito vector species [67]. We have already started to witness this increasing trend in mosquito-borne disease activity. For example, local dengue outbreaks were reported in the last three years (2022 to 2024) in Miami-Dade County, Florida [44], and local transmission of malaria took place in Florida and Texas in 2023 after 20 years of absence [33,35]. This highlights the need for strengthening preparedness and response capacity to respond to MBD outbreaks.
In conclusion, we have provided evidence of MBD transmission in the homeless population, but the extent to which individuals experiencing unsheltered homelessness are disproportionately exposed to mosquito-borne diseases remains largely unknown. This vulnerable population already faces significant disparities in mortality rates and various health outcomes [25]. Therefore, gaining a better understanding of the scope and impact of their increased vulnerability to mosquito-borne infections is essential for devising policy measures aimed at reducing preventable health inequalities.
Funding
A.B.B.W.: M.D.H., X.H., H.L., J.C., S.R., and M.A. were supported by the National Science Foundation (DMS-2424605/2424606/2424607). J.C.B. was supported by the Miami-Dade Mosquito Control Division and by the CDC grant U01CK000662: Southeastern Regional Center of Excellence in Vector-Borne Diseases: The Gateway Program. The CDC and NSF had no role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
Conflict of Interest
All authors declare no conflict of interest.
References
- Mutebi, J.-P.; Wilke, A.B.B.; Ostrum, E.; Vasquez, C.; Cardenas, G.; Carvajal, A. , et al. Diel activity patterns of two distinct populations of Aedes aegypti in Miami, FL and Brownsville, TX. Sci Rep. 2022;12: 5315. [CrossRef]
- Smith, M.; Dixon, D.; Bibbs, C.; Autry, D.; Xue, R. De. Diel patterns of Aedes aegypti (Diptera: Culicidae) after resurgence in St. Augustine, Florida as collected by a mechanical rotator trap. Journal of Vector Ecology. 2018;43: 201–204.
- Martin, E.; Medeiros, M.C.I.; Carbajal, E.; Valdez, E.; Juarez, J.G.; Garcia-Luna, S. , et al. Surveillance of Aedes aegypti indoors and outdoors using Autocidal Gravid Ovitraps in South Texas during local transmission of Zika virus, 2016 to 2018. Acta Trop. 2019;192: 129–137. [CrossRef]
- Koyoc-Cardeña, E.; Medina-Barreiro, A.; Cohuo-Rodríguez, A.; Pavía-Ruz, N.; Lenhart, A.; Ayora-Talavera, G. , et al. Estimating absolute indoor density of Aedes aegypti using removal sampling. Parasit Vectors. 2019;12: 250. [CrossRef]
- Mutebi, J.P.; Hughes, H.R.; Burkhalter, K.L.; Kothera, L.; Vasquez, C.; Kenney, J.L. Zika virus MB16-23 in mosquitoes, Miami-Dade County, Florida, USA, 2016. Emerg Infect Dis. 2018;24: 808–810. [CrossRef]
- Ventura, P.C.; Wilke, A.B.B.; Chitturi, J.; Kummer, A.G.; Agrawal, S.; Vasquez, C. , et al. Unveiling the role of mosquito and human diel activity patterns in the risk of mosquito-borne disease infection. medRxiv. 2024. [Google Scholar] [CrossRef]
- Meyer, T.E.; Bull, L.M.; Holmes, K.C.; Pascua, R.F.; Travassos da Rosa, A.; Gutierrez, C.R. , et al. West Nile Virus Infection among the Homeless, Houston, Texas. Emerg Infect Dis. 2007;13: 1500–1503. [CrossRef]
- Molaei, G.; Andreadis, T.G.; Armstrong, P.M.; Bueno, R.; Dennett, J.A.; Real, S.V. , et al. Host feeding pattern of Culex quinquefasciatus (Diptera: Culicidae) and its role in transmission of West Nile virus in Harris County, Texas. American Journal of Tropical Medicine and Hygiene. 2007;77: 73–81. [CrossRef]
- LaDeau, S.; Leisnham, P.; Biehler, D.; Bodner, D. Higher mosquito production in low-income neighborhoods of Baltimore and Washington, DC: Understanding ecological drivers and mosquito-borne disease risk in temperate cities. Int J Environ Res Public Health. 2013;10: 1505–1526. [CrossRef]
- Rothman, S.E.; Jones, J.A.; Ladeau, S.L.; Leisnham, P.T. Higher West Nile virus infection in Aedes albopictus (Diptera: Culicidae) and Culex (Diptera: Culicidae) mosquitoes from lower income neighborhoods in urban Baltimore, MD. J Med Entomol. 2021;58: 1424–1428. [CrossRef]
- Ajelli, M.; Moise, I.K.; Hutchings, T.C.S.G.; Brown, S.C.; Kumar, N.; Johnson, N.F. , et al. Host outdoor exposure variability affects the transmission and spread of Zika virus: Insights for epidemic control. PLoS Negl Trop Dis. 2017;11: e0005851. [CrossRef]
- US Department of Housing and Urban Development. The 2020 Annual Homeless Assessment Report to Congress, Part 1: Point-In-Time Estimates of Homelessness. Washington, DC; 2021.
- Petrovich, J.C.; Cronley, C.C. Deep in the heart of Texas: A phenomenological exploration of unsheltered homelessness. American Journal of Orthopsychiatry. 2015;85: 315–323. [CrossRef]
- Hopper, K.; Shinn, M.; Laska, E.; Meisner, M.; Wanderling, J. Estimating numbers of unsheltered homeless people through plant-capture and postcount survey methods. Am J Public Health. 2008;98: 1438–1442. [CrossRef]
- US Department of Housing and Urban Development. The 2023 Annual Homeless Assessment Report to Congress, Part 1: Point-in-Time Estimates of Homelessness. Washington, DC: U.S. Department of Housing and Urban Development.
- Olivet, J.; Wilkey, C.; Richard, M.; Dones, M.; Tripp, J.; Beit-Arie, M. , et al. Racial inequity and homelessness: Findings from the SPARC Study. Ann Am Acad Pol Soc Sci. 2021;693: 82–100. [CrossRef]
- Geller, A.; Curtis, M.A. A sort of homecoming: Incarceration and the housing security of urban men. Soc Sci Res. 2011;40: 1196–1213. [CrossRef]
- Fargo, J.; Metraux, S.; Byrne, T.; Munley, E.; Montgomery, A.E.; Jones, H. , et al. Prevalence and risk of homelessness among US veterans. Prev Chronic Dis. 2012;9: E45. [CrossRef]
- Culhane, D.P.; Metraux, S.; Byrne, T.; Stino, M.; Bainbridge, J. The age structure of contemporary homelessness: Evidence and implications for public policy. Analyses of Social Issues and Public Policy. 2013;13: 228–244. [CrossRef]
- Roncarati, J.S.; Baggett, T.P.; O’Connell, J.J.; Hwang, S.W.; Cook, E.F.; Krieger, N. , et al. Mortality among unsheltered homeless adults in Boston, Massachusetts, 2000-2009. JAMA Intern Med. 2018;178: 1242. [CrossRef]
- Levitt, A.J.; Culhane, D.P.; DeGenova, J.; O’Quinn, P.; Bainbridge, J. Health and social characteristics of homeless adults in Manhattan who were chronically or not chronically unsheltered. Psychiatric Services. 2009;60: 978–981.
- Montgomery, A.E.; Szymkowiak, D.; Marcus, J.; Howard, P.; Culhane, D.P. Homelessness, unsheltered status, and risk factors for mortality. Public Health Reports. 2016;131: 765–772.
- Nyamathi, A.M.; Leake, B.; Gelberg, L. Sheltered versus nonsheltered homeless women. J Gen Intern Med. 2000;15: 565–572. [CrossRef]
- Byrne, T.; Montgomery, A.E.; Fargo, J.D. Unsheltered homelessness among veterans: Correlates and profiles. Community Ment Health J. 2016;52: 148–157. [CrossRef]
- Fazel, S.; Geddes, J.R.; Kushel, M. The health of homeless people in high-income countries: Descriptive epidemiology, health consequences, and clinical and policy recommendations. The Lancet. 2014;384: 1529–1540. [CrossRef]
- Anderson, M.-C.; Hazel, A.; Perkins, J.; Almquist, Z. The ecology of unsheltered homelessness: Environmental and social-network predictors of well-being among an unsheltered homeless population. Int J Environ Res Public Health. 2021;18: 7328. [CrossRef]
- Centers for Disease Control and Prevention (CDC). Arbovirus Catalog. Available at: https://wwwn.cdc.gov/arbocat/.
- Zardini, A.; Menegale, F.; Gobbi, A.; Manica, M.; Guzzetta, G.; D’Andrea, V. , et al. Estimating the potential risk of transmission of arboviruses in the Americas and Europe: A modelling study. Lancet Planet Health. 2024;8: e30–e40. [CrossRef]
- Monaghan, A.J.; Eisen, R.J.; Eisen, L.; McAllister, J.; Savage, H.M.; Mutebi, J.P. , et al. Consensus and uncertainty in the geographic range of Aedes aegypti and Aedes albopictus in the contiguous United States: Multi-model assessment and synthesis. PLoS Comput Biol. 2019;15: 1–19. [CrossRef]
- Wilke, A.B.B.; Vasquez, C.; Beier, J.C. Presence and abundance of malaria vector species in Miami-Dade County, Florida. Malar J. 2023; 1–8. [CrossRef]
- Levine, R.S.; Peterson, A.T.; Benedict, M.Q. Distribution of members of Anopheles quadrimaculatus say s.l. (Diptera: Culicidae) and implications for their roles in malaria transmission in the United States. J Med Entomol. 2004;41: 607-13. [CrossRef]
- Murray, K.O.; Baraniuk, S.; Resnick, M.; Arafat, R.; Kilborn, C.; Cain, K. , et al. Risk factors for encephalitis and death from West Nile virus infection. Epidemiol Infect. 2006;134: 1325–1332. [CrossRef]
- Blackburn, D.; Drennon, M.; Broussard, K.; Morrison, A.M.; Stanek, D.; Sarney, E. , et al. Outbreak of locally acquired mosquito-transmitted (autochthonous) malaria - Florida and Texas, May-July 2023. MMWR Morb Mortal Wkly Rep. 2023;72: 973-978.
- Conway, K.L.; Jasuja, R.M.; Hauser, N.E.; Foley, J.E. Benefits, companion animal zoonotic disease prevalence and public perceptions of pet ownership among people experiencing homelessness in northern California. Zoonoses Public Health. 2022;69: 806–815. [CrossRef]
- Centers for Disease Control and Prevention, Filler SJ, MacArthur JR, Parise M, Wirtz R, Eliades MJ, et al. Locally acquired mosquito-transmitted malaria: a guide for investigations in the United States. MMWR Recomm Rep. 2006;55: 1-9.
- Eliades, M.J.; Shah, S.; Nguyen-Dinh, P.; Newman, R.D.; Barber, A.M.; Nguyen-Dinh, P. , et al. Malaria surveillance--United States, 2003. MMWR Surveill Summ. 2005;54: 25–40.
- Centers for Disease Control and Prevention (CDC). Local transmission of Plasmodium vivax malaria--Palm Beach County, Florida, 2003. MMWR Morb Mortal Wkly Rep. 2003;52: 908-11.
- Leibler, J.H.; Zakhour, C.M.; Gadhoke, P.; Gaeta, J.M. Zoonotic and vector-borne infections among urban homeless and marginalized people in the United States and Europe, 1990–2014. Vector-Borne and Zoonotic Diseases. 2016;16: 435–444. [CrossRef]
- Perez, M.T.; Morand, J.; Bush, L.M.; Crankshaw, K.; Sudduth, N.C. Hematological laboratory findings in patients of an autochthonous Plasmodium vivax Malaria Outbreak. Lab Med. 2004;35: 420–426.
- Centers for Disease Control and Prevention (CDC). West Nile virus disease cases reported to CDC by state of residence. Available at: https://www.cdc.gov/west-nile-virus/data-maps/index.html.
- Ramin, B.; Svoboda, T. Health of the homeless and climate change. Journal of Urban Health. 2009;86: 654–664. [CrossRef]
- Centers for Disease Control and Prevention (CDC). Chikungunya disease cases reported to CDC by state of residence. Available at: https://www.cdc.gov/chikungunya/data-maps/chikungunya-us.html.
- Centers for Disease Control and Prevention (CDC). Zika disease cases reported to CDC by state of residence. Available at: https://www.cdc.gov/zika/zika-cases-us/index.html.
- Centers for Disease Control and Prevention (CDC). Dengue disease cases reported to CDC by state of residence. Available at: https://www.cdc.gov/dengue/areaswithrisk/in-the-us.html.
- Shankar, M.B.; Rodríguez-Acosta, R.L.; Sharp, T.M.; Tomashek, K.M.; Margolis, H.S.; Meltzer, M.I. Estimating dengue under-reporting in Puerto Rico using a multiplier model. PLoS Negl Trop Dis. 2018;12: e0006650. [CrossRef]
- Walter Reed Biosystematics Unit. Systematic Catalog of Culicidae. Available at: https://wrbu.si.edu.
- Centers for Disease Control and Prevention. Arbovirus Catalog. Available at: https://wwwn.cdc.gov/Arbocat/Default.aspx.
- World Health Organization. Handbook for integrated vector management. World Health Organization; 2012.
- Lizzi, K.M.; Qualls, W.A.; Brown, S.C.; Beier, J.C. Expanding Integrated Vector Management to promote healthy environments. Trends Parasitol. 2014;30: 394–400. [CrossRef]
- Lindsay, S.W.; Jawara, M.; Paine, K.; Pinder, M.; Walraven, G.E.L.; Emerson, P.M. Changes in house design reduce exposure to malaria mosquitoes. Tropical Medicine and International Health. 2003;8: 512–517. [CrossRef]
- Centers for Disease Control and Prevention (CDC). West Nile Virus in the United States: Guidelines for Surveillance, Prevention. Available at: https://www.cdc.gov/westnile/resources/pdfs/wnvGuidelines.pdf.
- Byrne, T.; Huang, M.; Nelson, R.E.; Tsai, J. Rapid rehousing for persons experiencing homelessness: A systematic review of the evidence. Hous Stud. 2021; 1–27. [CrossRef]
- Rog, D.J.; Marshall, T.; Dougherty, R.H.; George, P.; Daniels, A.S.; Ghose, S.S. , et al. Permanent supportive housing: Assessing the evidence. Psychiatric Services. 2014;65: 287–294. [CrossRef]
- Baxter, A.J.; Tweed, E.J.; Katikireddi, S.V.; Thomson, H. Effects of Housing First approaches on health and well-being of adults who are homeless or at risk of homelessness: Systematic review and meta-analysis of randomised controlled trials. J Epidemiol Community Health. 2019;73: 379–387. [CrossRef]
- Padgett, D.K.; Herman, D. From Shelters to hotels: An enduring solution to ending homelessness for thousands of Americans. Psychiatric Services. 2021;72: 986–987. [CrossRef]
- Colburn, G. .; Fyall, R.., Ed.; Thompson, S., et al. Impact of hotels as non-congregate emergency shelters: An analysis of investments in hotels as emergency shelter in King County, WA during the COVID-19 pandemic. University of Washington. November 2020. Available at: https://kcrha.org/wp-content/uploads/2020/11/Impact-of-Hotels-as-ES-Study_Full-Report_Final-11302020.pdf. [Google Scholar]
- Rosenberg, R.; Lindsey, N.P.; Fischer, M.; Gregory, C.J.; Hinckley, A.F.; Mead, P.S. , et al. Vital Signs: Trends in reported vectorborne disease cases - United States and Territories, 2004-2016. MMWR Morb Mortal Wkly Rep. 2018;67: 496-501.
- Reiner, R.C.; Perkins, T.A.; Barker, C.M.; Niu, T.; Chaves, L.F.; Ellis, A.M. , et al. A systematic review of mathematical models of mosquito-borne pathogen transmission: 1970–2010. J R Soc Interface. 2013;10: 20120921. [CrossRef]
- Smith, D.L.; Perkins, T.A.; Reiner, R.C.; Barker, C.M.; Niu, T.; Chaves, L.F. , et al. Recasting the theory of mosquito-borne pathogen transmission dynamics and control. Trans R Soc Trop Med Hyg. 2014;108: 185–197. [CrossRef]
- Lega, J.; Brown, H.E.; Barrera, R. A 70% Reduction in mosquito populations does not require removal of 70% of mosquitoes. J Med Entomol. 2020;57: 1668–1670. [CrossRef]
- Morin, C.W.; Monaghan, A.J.; Hayden, M.H.; Barrera, R.; Ernst, K. Meteorologically driven simulations of dengue epidemics in San Juan, PR. PLoS Negl Trop Dis. 2015;9: e0004002. [CrossRef]
- Puggioni, G.; Couret, J.; Serman, E.; Akanda, A.S.; Ginsberg, H.S. Spatiotemporal modeling of dengue fever risk in Puerto Rico. Spat Spatiotemporal Epidemiol. 2020;35: 100375. [CrossRef]
- Tjaden, N.B.; Caminade, C.; Beierkuhnlein, C.; Thomas, S.M. Mosquito-borne Diseases: advances in modelling climate-change impacts. Trends Parasitol. 2018;34: 227–245. [CrossRef]
- Gibb, R.; Colón-González, F.J.; Lan, P.T.; Huong, P.T.; Nam, V.S.; Duoc, V.T. , et al. Interactions between climate change, urban infrastructure and mobility are driving dengue emergence in Vietnam. Nat Commun. 2023;14: 8179. [CrossRef]
- Ryan, S.J.; Carlson, C.J.; Mordecai, E.A.; Johnson, L.R. Global expansion and redistribution of Aedes-borne virus transmission risk with climate change. PLoS Negl Trop Dis. 2019;13: e0007213. [CrossRef]
- Caminade, C.; Kovats, S.; Rocklov, J.; Tompkins, A.M.; Morse, A.P.; Colón-González, F.J. , et al. Impact of climate change on global malaria distribution. Proceedings of the National Academy of Sciences. 2014;111: 3286–3291. [CrossRef]
- Wilke, A.B.B.; Chang, N.B.; Townsend, J.; Benelli, G.; Ajelli, M. Unintended effects of urban policies on the risk of arbovirus transmission. Trends Parasitol. 2023;39: 1001-1003. [CrossRef]
Figure 1.
Study flow diagram.
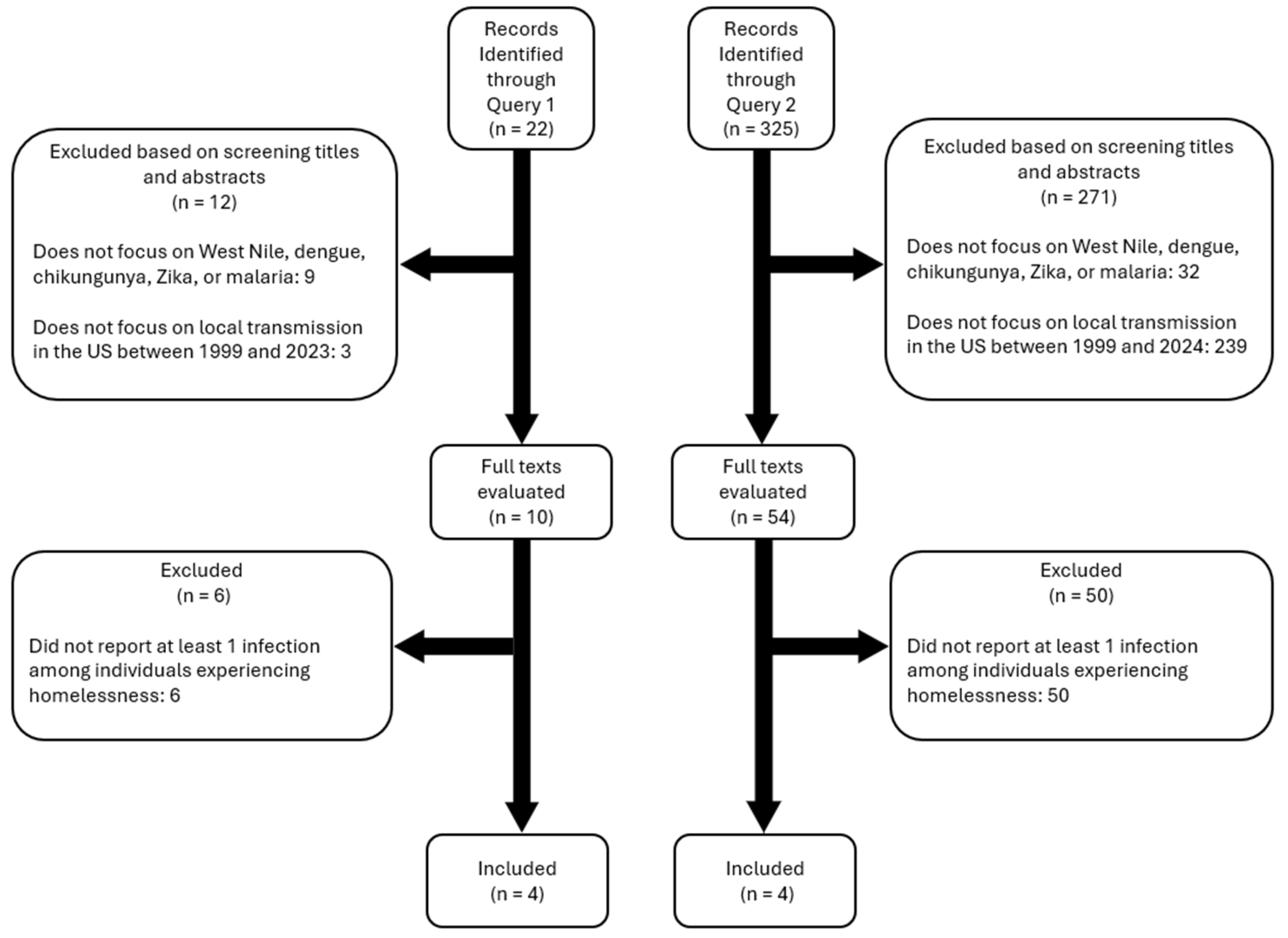

Table 1.
Summary of studies available in the literature.
| Reference | Title | Relevant findings for homelessness and MBDs |
|---|---|---|
| Murray et al. [32] | Risk factors for encephalitis and death from West Nile virus infection. | Individuals experiencing homelessness showed a higher likelihood of hospitalization due to West Nile compared to the general population. |
| Meyer et al. [7] | West Nile virus infection among the homeless, Houston, Texas. | Factors associated with an increased risk of West Nile infection were found to be chronic homelessness and >6 hours outdoor exposure to mosquitoes. |
| Blackburn et al. [33] | Outbreak of locally acquired mosquito-transmitted (autochthonous) malaria - Florida and Texas, May-July 2023. | Eight cases of locally acquired Plasmodium vivax malaria were reported in Florida and Texas. Three of the eight patients were reported experiencing homelessness. |
| Conway et al. [34] | Benefits, companion animal zoonotic disease prevalence and public perceptions of pet ownership among people experiencing homelessness in northern California. | Five out of 42 samples taken from dogs of unhoused owners tested positive for West Nile virus. |
| Eliades et al. [36] | Malaria surveillance--United States, 2003 | In 2003, eight cases of locally transmitted malaria were reported in Palm Beach County, Florida. The 8 affected individuals were found to spend extended periods outdoors, including one homeless individual. |
| CDC et al. [37] | Local transmission of Plasmodium vivax malaria--Palm Beach County, Florida, 2003 | Examines seven cases of Plasmodium vivax malaria that occurred in Palm Beach County, Florida, during July and August 2003. One case involved a man who had been sleeping in an outdoor homeless camp near a canal. |
| Leibler et al. [38] | Zoonotic and vector-borne infections among urban homeless and marginalized people in the United States and Europe, 1990-2014. | Serological evidence of exposure to pathogens, including Rickettsia typhi, West Nile virus, and Seoul hantavirus in individuals experiencing homelessness. HIV infection, injection drug use, and heavy drinking were common risk factors for these infections. |
| Perez et al. [39] | Hematological laboratory findings in patients of an autochthonous Plasmodium vivax malaria outbreak | Hematological findings of the 2003 malaria outbreak in Palm Beach County, Florida, showed that all 8 reported cases, one of which is an individual experiencing homelessness, carried the same strain of Plasmodium vivax. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



