1. Introduction
Low back pain (LBP) affects over 60% of people during their lives, impacting nearly one in ten annually. [
1,
2,
3,
4] It can lead to significant daily life implications, including work absenteeism and reduced quality of life. [
5] Misdiagnosis of conditions like facet joint pain (FJP) is common, often resulting in ineffective treatments and unnecessary healthcare resource consumption. [
6,
7] The complex anatomy of the spine, combined with the lack of clear biomarkers from radiological findings or diagnostic tests, complicates accurate diagnosis and treatment. [
8,
9,
10,
11,
12,
13] Although imaging methods like computed tomography (CT) and magnetic resonance imaging (MRI) are used, they do not consistently correlate with clinical symptoms. [
14,
15,
16] Consequently, effective management of LBP and FJP remains challenging, necessitating more precise diagnostic techniques and treatment approaches to address this prevalent issue. [
17,
18]
This narrative review provides an overview of the relevant existing literature on LBP and FJP. It evaluates current diagnostic tools, such as imaging techniques, and their effectiveness in accurately identifying pain sources. Additionally, it examines available interventions, including medial branch blocks (MBBs) and radiofrequency ablation (RFA), assessing their efficacy and role in pain management. Through this comprehensive analysis, the review aims to highlight gaps in knowledge and suggest future directions for research and practice.
RFA is regarded as the gold standard for interventional treatment for FJP, supported by the most robust evidence in the literature. [
2,
12,
17,
19,
20,
21,
22] Its effectiveness is significantly enhanced when performed after MBBs, which help confirm the diagnosis and predict treatment outcomes. [
23,
24] By ensuring accurate targeting of the medial branches (MB), RFA can provide substantial pain relief and improve function in well-selected patients, solidifying its role in managing chronic LBP.
2. Clinical Presentation
Clinical Presentation
LBP is a symptom of multiple potential pain generators such as disc degeneration, facet joint disease, or spinal stenosis. [
25] The clinical diagnosis of facetogenic pain is therefore challenging, as it is not easily distinguished from pain caused by other lower back structures. [
26,
27] In addition to spinal causes, the pain may also indicate visceral pathology or mood disorders. [
6] Due to the difficulty in identifying a precise source, facetogenic pain is often categorized as nonspecific low back pain. [
27]
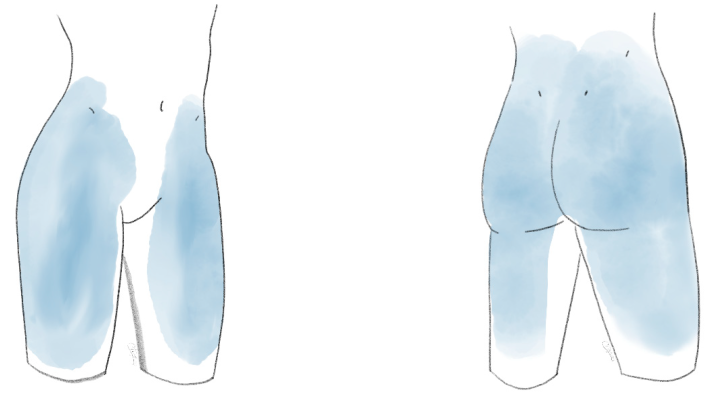
The pain is located in the paravertebral region of the lower back and presents uni- or bilateral with possible radiation over the gluteal area, the groin, or thighs. [
12,
17] The pain in the low back is more prominent than the radiating pain to the leg and there is often no clear dermatomal pattern present, in contrast to radicular pain. Hence, the term pseudo-radicular pain is used. [
12] Facetogenic pain typically does not extend beyond the knee. If pain radiates further, it is more likely due to a non-facetogenic cause, except in cases involving facet joint cysts. In rare instances, facetogenic pain may also present as pelvic or abdominal discomfort. [
28]
Concerning pain intensity, complaints are more pronounced with short-lived stiffness in the morning or after periods of immobilization. Light exercises, such as walking or gentle stretching, can help reduce pain intensity. However, more strenuous activities like walking uphill tend to exacerbate the pain. [
29]
Fukui et al. described particular pain patterns for the referred pain after applying provocation tests to specific individual facet joints. [
30] The L1-L2 facet joint refers pain to the lumbar spinal region. In addition, the L2-L3 facet joint rarely projects to the trochanteric, gluteal, and lateral thigh regions. The L3-L4 facet joint more prominently projects to the aforementioned areas as well as the groin area less frequently. The L4-L5 facet joint refers to the lumbar spine, gluteal, lateral, and posterior thigh, trochanteric, and groin area. The L5-S1 facet joint refers to the same pain pattern with the exception of the lumbar spine. [
30] Even with the specific patterns known or proven, the location of pain is predominantly a clue, rather than a direct correlation to a specific level. [
27] Practically, the pain distribution could be described as a region covered by cycling shorts.
Facet joint disease may lead to synovial cyst formation, which can act as space occupying lesions. The cysts may compress nerve roots or the dorsal root ganglia (DRGs) and possibly create a stenosis in the spinal canal. These symptoms resemble radicular signs, similar to those in disc herniation or spinal canal stenosis. A clearer dermatomal spread, as well as potentially radicular pain protruding in the lower limb is seen, which reaches beyond the knee, potentially to the foot and toes. [
31]
Clinical Examination
Diagnosing the cause of LBP is often complex due to its multifactorial nature and concurrent medical conditions. Although proper clinical examination plays a significant role in the diagnosis of many diseases, it has not been proven to objectify facetogenic pain even though many clinicians have tried.
Revel et al. proposed seven criteria, corresponding to a higher success rate of intra-articular facet joint infiltration. [
32] However, these criteria were not consistently found by other researchers. [
33]
Stuber et al. found a limited negative predictive value in Kemp’s test. This pain provocation test is expected to elicit facetogenic or discogenic pain and involves backward flexion or extension, simultaneously with rotation of the upper body. [
13]
Paravertebral tenderness and pain on palpation over the facet joints can be found, although this is found to correlate only poorly with response to facet joint treatment. [
17]
Unless nerve root or DRG compression is present due to facet joint cysts, the straight leg test is negative. [
34]
3. Epidemiology
LBP affects over 60% of individuals during their lifetime and impacts nearly one in ten people annually. [
2,
3,
4,
11] In 50% of patients, the pain subsides spontaneously within two weeks, and in 90%, it resolves within 12 weeks. Despite this, LBP remains the leading cause of years lived with disability. It is often only treated when it affects mobility, and may otherwise be overlooked or dismissed. [
9]
Persistent pain lasting three to six months or longer leads to work absenteeism, diminished quality of life, and increased healthcare costs. [
5] This can result in social isolation, limitations in daily activity, chronic pain and extended withdrawal from the workforce. [
5] Several factors, including medication overuse, excessive healthcare resource consumption in search of a diagnosis, and unwarranted interventions (minimally invasive or surgical), further increase the cost and burden of LBP. [
6,
7]
Quantifying the societal cost of LBP is difficult. In 2016, the costs related to neck and lower back pain in the U.S. were estimated to surpass
$130 billion, primarily due to lost labour and increasing healthcare expenses. [
4] In 2007, the annual healthcare costs associated with LBP were estimated at
$3.9 billion in the Netherlands and over
$50 billion in Germany. [
12]
FJP is estimated to occur in 27% to 40% of patients with LBP [
12,
17,
26,
34] Despite being a leading cause of LBP, FJP is often misunderstood, leading to frequent misdiagnosis or inappropriate treatment. In FJP patients, osteoarthritis of the facet joint is the most frequent problem with estimated incidence in the overall adult population of 10 to 15% and higher in the more senior population. [
12,
35]
4. Anatomy and Biomechanics
Anatomy and Pathological Changes of the Facet Joint
Understanding the anatomy and pathology of lumbar facet joints (LFJs) is essential for diagnosing low back pain and related conditions. LFJs are paired joints, formed by the inferior articular process (IAP) of the vertebra above and the superior articular process (SAP) from the level below. They connect adjacent vertebrae, enabling movement and stabilizing the spinal column. [
8] These synovial joints contain poorly vascularized hyaline cartilage, which inhibits proper healing after injury.
The capsule, consisting of two layers, has a volume of approximately 1cc due to its recesses. Additionally, the capsule is rich in sensory nerve endings. These encapsulated and free nerve endings can be activated by injury or inflammation, leading to pain. [
36,
37] Inflammation typically results from mechanical stress, joint instability, or the degeneration of nearby tissues, with pro-inflammatory cytokines like TNF-α, IL-1, and IL-6 as well as Substance P playing key roles in the pain-generation mechanisms, correlating to mechanisms seen in rheumatoid arthritis. [
2,
36,
37]
Biomechanics of the Lower Vertebral Element
Biomechanically, both LFJ together with de intervertebral discs form a three-joint complex, where the LFJs are essential for stabilizing the spine during movement. [
8] The surface of the IAP is convex, whereas the SAP is concave. Each facet joint bears a notable portion of the axial load, carrying 10 to 20% in physiological circumstances. Particularly when the intervertebral discs are compromised or dehydrated, the stress on the joints increases and leads to degeneration, especially prevalent at levels L4/L5 and L5/S1. [
8,
17,
27,
34,
36] During hyperextension or cyclic flexion movements, significant strain can occur across the LFJ capsules, since they are shorter and more tough than the cervical facet joints. This strain can potentially result in fibrocartilaginous metaplasia and increased laxity of the joints. [
27,
36] This creates a complex interaction where the degeneration in one facet joint can influence the biomechanics and integrity of the entire spinal segment, further exacerbating pain and dysfunction. [
8,
9]
Variations in the lumbar spine, such as sacralization or lumbarization, are common in the general population and may complicate surgical interventions. A retrospective analysis found a 9.9% prevalence of lumbosacral transitional vertebrae (LSTV), with lumbarized S1 occurring in 5.8% and sacralized L5 in 4.1% of cases. Of the LSTV cases, 69,6% were not identified by the reporting radiologist, and occasional misreporting between sacralization and lumbarization occurred. [
12,
38]
In case of asymmetry in the orientation of the articular planes of the LFJ’s at the same level, the terminology tropism is used. Misalignment up to 5 or 10% is considered normal, although formal consensus is lacking. [
8] It was hypothesized that tropism would result in or accelerate osteoarthritis (OA) due to an imbalance of forces. This was not found in cadaver studies, nor in studies evaluating facet joint orientation and tropism on CT scans in different study population. [
10,
14]
Anatomy of the Nerves
The medial branch (MB) of the dorsal ramus plays a crucial role in innervating the facet joints and adjacent structures, including the multifidi muscles, interspinous ligament, and supraspinous ligament. [
39] It is the sole supplier of motor fibres to the multifidus muscles, while also providing sensory input to the facet joints and ligaments. The MB courses along the lateral neck of the SAP in the groove formed by the SAP and the transverse process, descending caudally and posteriorly, often accompanied by vessels from the lumbar artery and vein. [
8,
39,
40] In middle two quarters of the neck, the MB adheres to the periosteum and is well exposed and susceptible to denervation for a limited length. [
41,
42] Before entering the fibro-osseous canal, the nerve gives rise to small articular branches that innervate the lateral and inferior aspects of the LFJ. The nerve’s position near the mamilloaccessory ligament offers a relatively predictable target for MB neurotomy. However, variations in the anatomy of the MB can complicate accurate electrode placement, especially at different points along the SAP.
The L1–3 MBs descend 1–2 vertebrae, while the L4–5 MBs descend 2–3 vertebrae, extending their innervation to the lumbosacral joint and the dorsal aspect of the sacrum. [
39] These branches form a network with adjacent medial and lateral branches as well as the dorsal rami, creating a complex system of nerve connections.
Research in rats indicates that labelled neurons from the L5-L6 facet joints originate in ipsilateral DRGs from L1 to L5 and in paravertebral sympathetic ganglia from T12 to L6, highlighting the intricate relationship between the sensory and sympathetic systems. Some sensory fibres from the facet joints may even pass through the paravertebral sympathetic trunk and reach the L1 or L2 DRGs, which could explain referred pain patterns such as inguinal or anterior thigh pain in cases of lower LFJ lesions. [
43]
Repeated trauma or injury to the spine and facet joints can lead to the compression or retraction of the medial and lateral branches, resulting in chronic low back pain. [
39] Additionally, the close association of the MB with the posterior branch of the lumbar artery increases the risk of minor complications during repeated interventions such as MB neurotomy, potentially leading to vascular injury or hematoma formation.
Despite anatomical consistency in some areas, such as the MB’s course through the mamilloaccessory notch, variability in other regions, and the presence of complex neural plexuses, including connections with the intermediate branch, complicates diagnosis and treatment. Precision in targeting the medial branch is crucial, as improper needle placement during neurotomy can inadvertently affect the lateral or intermediate branches. [
41]
5. Diagnostic Interventions
There is no clear consensus on how to best evaluate LFJ OA with imaging. Imaging often does not correlate well with clinical symptoms of LBP, and its primary utility may lie in ruling out more severe conditions (red flags) rather than identifying symptomatic facet joint arthritis. [
11,
12,
16] Despite extensive imaging findings in asymptomatic individuals, such as disc degeneration or facet joint pathology, these findings often lack specificity for diagnosing the source of LBP. [
2,
10,
44]
5.1. X-Ray
Oblique radiographs provide the best view of LFJs, offering a "Scottie dog" view, which is useful for identifying degenerative changes. However, X-rays are limited in providing detailed information on facet joint degeneration.
5.2. CT
CT scans improve anatomical evaluation of facet joints and are considered the preferred method for imaging LFJ OA. They reveal joint space narrowing, sclerosis, subchondral erosions, and osteophyte formation, among other degenerative signs. CT scans show a high prevalence of facet joint degeneration, but the relationship between these findings and actual pain is weak. [
10]
5.3. MRI
MRI is highly sensitive and specific for detecting facet joint degeneration, including surrounding neural impingement. However, studies have shown inconsistent correlations between MRI findings and clinical symptoms, with some degenerative changes found in patients without pain. [
45,
46] MRI has a slight advantage over CT in evaluating neural impingement but may underestimate the severity of LFJ OA compared to CT. [
47]
5.4. Single Photon Emission Computed Tomography-CT (SPECT-CT)
SPECT-CT is increasingly recognized for its potential in diagnosing LFJ disease. It can detect areas of increased metabolic activity, or "hot spots", that may indicate active inflammation in the facet joints, helping identify pain sources more accurately. Studies show that pathological findings are present in 86% of lumbar SPECT-CT scans, although not all detected abnormalities correlate with pain. Approximately 65% of these identified areas are linked to facet joint pain. [
48]
Research indicates that patients with SPECT-positive scans are more likely to respond to medial branch blocks (MBBs). [
49] This suggests that SPECT-CT may help predict outcomes following treatment. Additionally, patients with SPECT-positive scans experienced greater reductions in pain scores at one-month follow-up. [
50]
A notable advantage of SPECT-CT is its ability to provide a whole-body map of metabolic activity with occurrence of hot spots of high activity. These hot spots are significantly more frequently found in the lumbar spine in the presence of LBP. [
15]
Although SPECT-CT shows promise, its routine clinical use remains limited due to concerns about specificity, as some patients with positive imaging findings may not experience pain. Moreover, further research is needed to assess its cost-effectiveness and refine its role in diagnosing lumbar facet joint disease. [
9,
22]
5.5. Intra-Articular Infiltration
Intra-articular (IA) injections target the facet joint itself, injecting a combination of local anaesthetic and possibly corticosteroid directly into the joint space. These injections are used both for diagnostic purposes and for therapeutic management of facet joint-mediated LBP. However, like MBBs, their efficacy as a long-term treatment has not been proven. Cohen et al. even suggested that IA infiltrations should not be considered therapeutic, given the absence of long term effects. [
2,
24]
IA injections can be used diagnostically to confirm that a specific facet joint is the source of pain. If the injection significantly reduces pain, it is assumed that the facet joint is contributing to the patient’s symptoms. However, compared to MBBs, IA injections are less commonly used purely for diagnostic purposes given many guidelines recommend the usage of MBBs. [
20,
24]
The diagnostic accuracy of IA injections can also be compromised by the spread of the injectate beyond the joint capsule, potentially anesthetizing other structures and leading to false-positive results. IA injections are technically more challenging to perform than MBBs due to the difficulty of accurately entering the small joint space. This is particularly true in patients with advanced degenerative changes in the facet joints, where joint space narrowing and osteophyte formation can make needle placement more difficult. Failure rates can reach up to 29%. [
24] However, pericapsular injection was found to be as effective as proper intracapsular. [
24,
51] As with MBBs, fluoroscopic or ultrasound guidance is typically applied to ensure proper needle placement and avoid intravascular uptake.
Steroid injections play a dual role in managing OA pain, including LFJ OA, by reducing inflammation and interrupting nociceptive inputs at both the central and peripheral levels. However, their long-term efficacy remains questionable, and they are often used as part of a broader treatment strategy that may include physical therapy, medications, and other interventions. [
2]
In terms of risks, IA injections carry similar complications to MBBs, such as infection, bleeding, and injury to surrounding structures. Additionally, the use of corticosteroids can lead to potential side effects, including localized tissue atrophy and systemic effects such as elevated blood sugar levels in diabetic patients.
5.6. Medial Branch Block
MBBs are widely used as a diagnostic tool to identify facet joint-mediated pain and as a prognostic indicator for the success of subsequent RFA. However, their diagnostic accuracy is subject to limitations, including high false-positive rates, which range from 25% to 40%. [
52,
53] This variability is influenced by factors such as placebo effects, spread of injectate to other pain-generating structures, and excessive use of local anaesthetic. [
54] False-negative MBBs have been less studied but remain a concern. Vascular uptake during the procedure, reported in 6% to 30% of cases, and aberrant innervation are potential causes of false negatives. [
27,
39,
55,
56] Intravascular uptake can often be missed, making it essential to confirm with contrast imaging, despite the increased radiation exposure.
The technique of performing MBBs also varies widely. International consensus guidelines advocate for using ultrasound or fluoroscopic guidance and smaller volumes of local anaesthetic (0.25–0.5 mL) to prevent the spread to adjacent structures and increase diagnostic accuracy. [
54,
55,
57] Larger volumes or inadvertent spread to other structures, such as the intervertebral foramina or posterior muscles, can lead to misdiagnosis.
There is no clear consensus on how to define a "positive" block. [
21,
23,
58] While some authors argue that 50% pain relief should be the threshold, others suggest a stricter criterion of 70% to 80% pain relief. A confirmatory second block is often recommended to reduce the false-positive rate, which can reach up to 45%. [
24] Studies show that patients with 80% or more pain relief after the first MBB are significantly more likely to achieve similar relief after a second block. [
57] Therefore, some guidelines recommend performing two diagnostic MBBs and requiring at least 80% pain relief to confirm a diagnosis. [
19,
20] However, even with stringent criteria, anatomical variations and aberrant innervation complicate diagnosis.
Studies also highlight the therapeutic potential of MBBs, with some patients experiencing prolonged pain relief, though the mechanisms behind this are not fully understood. [
59,
60] Despite this, most rigorous studies have not supported the routine use of MBBs as a therapeutic intervention, and their primary role remains diagnostic.
Cost-effectiveness studies, such as the one conducted by Cohen et al., offer insight into the financial considerations of using MBBs. [
61] In a randomized comparative study of 151 patients, the effectiveness and cost of 0, 1, or 2 diagnostic MBBs prior to RFA were evaluated. The group with no diagnostic MBBs had a 33% success rate at a cost of
$6,286 USD per successful outcome. In contrast, the group that received one diagnostic MBB had a lower success rate of 16% at
$17,142 USD, while the group that received two MBBs had a 22% success rate at
$15,241 USD. These findings highlight the cost-benefit trade-offs associated with using multiple diagnostic MBBs before RFA.
Given the high costs and variability in outcomes, cost-effectiveness analyses suggest that a single set of MBBs with at least 50% pain relief may be sufficient in clinical practice. However, for more stringent scenarios, such as clinical trials, two sets of blocks may be necessary to ensure the highest likelihood of successful outcomes from RFA. [
20,
22]
6. Therapeutic Interventions
6.1. Conservative Medical Management
Conservative management of chronic low back pain involves a comprehensive approach that integrates both medication and physical therapy. Pain relief may be sought through short-term use of painkillers like paracetamol or non-steroidal anti-inflammatory medication (NSAIDs), though these offer limited long-term benefits and must be used cautiously due to potential side effects. [
11,
17,
44,
62] Physical therapy is equally critical, focusing on core strengthening, reducing lumbar lordosis with pelvic tilting, and incorporating aerobic exercises. A Cochrane review, conducted in 2021, found clinical improvement in the short- and intermediate-term. The results on long-term improvement were inconclusive. [
63]
According to the National Institute for Health and Care Excellence (NICE) guidelines, patients should be encouraged to continue their normal activities and engage in group exercise programs that combine biomechanical, aerobic, and mind-body approaches for optimal recovery. [
64]
Manual therapy, such as spinal manipulation or soft tissue techniques, is advised only as part of a broader treatment plan that includes exercise, and possibly psychological support. The goal is to promote a return to daily activities, including work, while avoiding specific interventions like belts, foot orthotics, acupuncture, or electrical nerve stimulation, which have not shown long-term efficacy. [
64]
In cases where NSAIDs are unsuitable or ineffective, weak opioids may be considered for acute low back pain. Medications like selective serotonin reuptake inhibitors (SSRIs), serotonin and norepinephrine reuptake inhibitors (SNRIs), tricyclic antidepressants (TCA), gabapentinoids, or antiepileptics are not appropriate for managing LBP, as is paracetamol as monotherapy. [
33] For a more holistic approach, patient education, self-care, and continued participation in normal daily routines, combined with tailored physical therapy, are key elements in improving pain management outcomes. [
63]
6.2. Intra-Articular Injection
Injections like IA and MBBs are commonly used to treat lumbar facet joint pain, but their therapeutic effectiveness has been inconsistent. [
17,
24,
65] Comparisons between IA injections and placebo treatments have shown no significant long-term benefit. IA injections did not provide lasting pain relief or delay the need for RFA. [
66] Thus, clinical evidence does not support the widespread use of IA injections. [
67] As a result, several medical societies recommend against routine IA procedures due to their limited efficacy in managing FJP. [
19,
20,
23,
68]
An alternative gaining attention is platelet-rich plasma (PRP) therapy, which uses a patient's own blood components to promote healing and reduce inflammation. Some studies suggest that PRP injections may be more effective than traditional steroid-based injections for treating FJP. [
69,
70] However, further research is needed to confirm its long-term effectiveness and broader applicability.
6.3. Radio Frequency Ablation
RFA or radiofrequency denervation is a procedure used to alleviate chronic pain by applying radiofrequency (RF) energy to targeted nerves. This technique encompasses both continuous and pulsed RF. Continuous RF generates an electromagnetic field that causes ionic agitation in the tissues surrounding the needle's tip, producing heat that disrupts nerve function through denaturation, thereby blocking pain signals. [
12,
62,
71] In contrast, pulsed RF creates short but intense electromagnetic fields that minimize damage to surrounding tissues by maintaining a temperature below 42°C. [
72] The precise mechanism by which pulsed RF alleviates pain is not fully understood. Cooled RF, a variation of continuous RF, employs cold saline as a heatsink to create larger, controlled lesions, potentially allowing for more extensive pain relief. [
65]
The success of RFA is highly dependent on proper patient selection. [
12,
17,
57,
73] Diagnostic blocks are crucial for identifying patients with FJP who are most likely to benefit from the procedure. While RFA can offer temporary relief, the effects are not permanent, as the nerves eventually regenerate. Therefore, the procedure can be repeated, with a recommended limit of up to two treatments per year. [
12] Although widely used, some studies have raised concerns about its long-term efficacy, suggesting that its benefits may be limited for certain patient groups. [
2,
25,
64]
6.4. Continuous Radio Frequency Ablation
Diagnostic MBBs, especially with dual blocks achieving 75% to 100% pain relief, have strong evidence supporting their use in identifying candidates for RFA. Lesser relief, around 50% to 74%, also shows fair evidence, but single diagnostic blocks provide more limited validation. [
74]
RFA is widely considered the "gold standard" for interventional treatment of facet joint-related LBP, with meta-analyses demonstrating significant pain reduction lasting up to 12 months. [
17,
20,
21,
75] Studies report a significant reduction in pain, typically a 2–3 point decrease on the visual analogue scale (VAS), compared to control groups. [
12]
6.4.1. Technique
RFA for FJP requires precise needle placement near the MB. [
5,
51,
69] Historically a perpendicular approach was used, but a parallel needle placement is now widely accepted given the ellipsoid cauterisation lesion rather than a spherical lesion at the tip. There is international consensus that a longer lesion of the MB correlates to a longer duration of relief. [
17,
19,
21,
77] Advanced imaging is recommended, with fluoroscopy being the most commonly used, though ultrasound is an option. Sterile precautions, such as disinfecting the skin and wearing a mask, gown, and sterile gloves, are essential. The procedure can be performed with or without light sedation, though general anaesthesia is not routinely recommended. Local anaesthesia is often used to facilitate the introduction of RF needles.
The needle is guided toward the junction of the SAP and the transverse process, commonly referred to as the "eye of the Scotty dog”. The goal is to target the medial aspect of the lateral side of the SAP, with position verified using anteroposterior, oblique, and lateral imaging, along with electrical stimulation. [
40] Motor stimulation is strongly advised to confirm proximity to the target nerve through contraction of the multifidus muscle, while avoiding stimulation of the ventral ramus, which could cause a lower limb response. A safety threshold of 2V is recommended for motor stimulation, while sensory stimulation should ideally be less than 0.5V. Typically, RF is applied at 80°C for 90–120 seconds, with the option to inject steroids afterward to reduce the chance of post-procedural inflammation and neuritis. [
20,
22]
Patient-specific factors like age, comorbidities, and anatomy play a critical role in determining RF outcomes. Though sensory stimulation is widely used, studies show it may not significantly impact long-term pain relief. [
78] Other methods, such as targeting anatomical landmarks and using motor responses like paraspinal muscle contractions, have demonstrated positive results. Multiple lumbar levels are often treated simultaneously due to the challenge of pinpointing the exact facet joint responsible for the pain and because each facet joint is innervated by two medial branches.
6.4.2. Orientation
The C-arm is typically positioned ipsilateral at a minimal oblique angle (10–20°) and in a caudad-cephalad direction. A recent study advocates for a more caudal angulation than was previously accepted, with caudal angulation reaching up to more than 40° from the cranial endplate of the designated vertebral level. [
76]
6.4.3. Needle Characteristics and RF Settings
A wide range of needles is available. There is variation in the length of the active needle tip, ranging from 2 mm up to 15 mm. A longer active tip results in a longer lesion. [
63] Most commonly used needles for MB denervation have an active tip of 5 to 10mm. [
20,
21,
22]
The tip can either be straight, curved or can be deployed when it is in the right location. Curved tips are considered more easily steerable and are able to follow the curvature of the SAP, resulting in a more pronounced overlap with the nerve. Some needles can be deployed or unfolded, resulting in a bigger lesion, thus increasing the chance of capturing the MB. [
20]
RF needles come in various sizes, with the more frequently used sizes ranging from 16 to 22 gauge. Bigger needles create a bigger lesion but cause more procedural pain or discomfort.
When the temperature of the probe is increased, the heat will spread further, resulting in a bigger lesion. At high temperatures charring and vaporization of the tissue can occur. This should be avoided. Therefore the recommended temperature is 80 to 90°C. [
20,
22]
Cosman et al. published an overview of different parameters and the effect on lesion size. For example, they found that a 16ga needle with a temperature set at 90°C for 3 minutes, resulted in a lesion of 11,1mm in diameter. Whereas a 18ga needle with a temperature set at 80°C for 2 minutes, resulted in a lesion of 7,6mm in diameter. [
71]
6.4.4. Complications
RFA is generally considered safe, though it does carry some risks. [
79] Potential complications include infection, haemorrhage, increased pain, numbness, or dysesthesias. Most adverse events are mild and self-limiting, such as superficial infections, rashes, or vasovagal episodes. Serious complications like neuraxial infections or nerve root irritation are exceedingly rare. Considering infection, the risk from RFA may even be lower than that of diagnostic blocks due to the protective heat used during the procedure. [
24,
61,
74]
Muscle-related side effects, particularly involving the multifidus muscle, are a concern with RFA. Studies indicate that while multifidus dysfunction occurs post-procedure, it may be more severe than in other surgical interventions, such as posterior lumbar fusion, due to nerve damage rather than direct muscle injury. [
80,
81,
82] Post-procedure neuritis, lasting several weeks, affects 1-10% of patients, and some may experience neuropathic pain over the lumbar paraspinal muscles. [
17] Although multifidus atrophy after RFA has not been conclusively proven, it remains a plausible concern requiring further investigation.
6.5. Cooled Radiofrequency Ablation
Cooled radiofrequency ablation (C-RFA) has shown promising results in treating FJP, offering advantages over traditional RF techniques. By creating larger, spherical lesions, it allows for greater flexibility in probe placement and improves the likelihood of targeting nerves effectively, particularly in cases with anatomical variations. A study comparing C-RFA to IA infiltrations found that patients treated with C-RFA were more likely to experience significant pain relief. These findings suggest that C-RFA may be a more effective option for long-term pain management in well-selected patients. [
65]
6.6. Pulsed Radiofrequency Ablation
Multiple randomized trials and systematic reviews have shown that pulsed radiofrequency ablation (P-RFA) is less effective than conventional RFA for treating FJP. [
9] P-RFA provides minimal benefits through 12 months and is less effective at reducing pain and improving function. As a result, P-RFA cannot replace conventional RFA for long-term pain management.
6.7. Chemical Denervation
Afifi et al. (2022) compared RFA of LFJ with chemical neurolysis using ethyl alcohol (EA-95) or glycerol (Gly-20) in 95 patients. The study found that RFA provided significantly better pain relief and quality of life improvements than both chemical agents. RFA patients reported lower pain scores at 6 weeks, 6 months, and 1 year compared to those treated with EA-95 and Gly-20. In contrast, chemical neurolysis was associated with risks like tissue necrosis, neuritis, and uncontrolled diffusion, leading to complications like painful paraesthesia months after treatment. [
83]
6.8. Cryodenervation
Cryodenervation, developed in the 1970s, uses a cryoprobe to freeze nerves to -50°C with medical-grade CO2, causing endoneural oedema and nerve cell death. This method, used for facet joint neurotomy, achieves successful outcomes in about 65-70% of cases. [
12,
51] Unlike RFA, cryodenervation doesn't require precise probe placement although sensory stimulation is advisable. Peri-procedural pain is generally tolerable. While it has shown promising results, such as pain reduction at 6 weeks, 3 months, and 6 months, no direct comparative studies with RFA for FJP are available. Therefore, further research is needed to confirm its long-term effectiveness compared to other techniques. [
84]
6.9. Endoscopic Denervation
Endoscopic denervation (ED) is an advanced form of RFA targeting the MB, providing direct visualization of anatomical structures like the nerve root and articular capsule. This allows for more precise nerve detection and complete denervation, leading to stable and long-lasting pain relief. [
75,
84,
85] Compared to traditional RFA, ED reduces the risk of nerve injury and sensory loss while offering more thorough ablation. However, the procedure is more surgical in nature, taking longer to perform and requiring extended recovery time, as well as incurring higher costs. Despite these drawbacks, ED provides better and longer-lasting analgesia than percutaneous RFA.
Patients treated with ED saw their VAS scores drop substantially, with 58% pain relief after six weeks and 38% sustained relief after twelve months. [
86] ED has shown even greater efficacy for patients with isolated facet joint OA. Although some patients required re-operations due to recurring symptoms, the technique can be repeated without causing structural changes, making it a viable long-term treatment for chronic FJP. [
85]
7. Surgical Possibilities
7.1. Controversy Regarding Surgery and Other Invasive Procedures
The role of surgery in managing LBP is controversial, particularly when neural compression or structural deformity is absent. NICE guidelines strongly advise against spinal fusion or disc replacement in LBP management, recommending these procedures only within controlled clinical trials. [
44] Despite the lack of robust evidence, the number of elective lumbar spine surgeries, including fusions, have significantly increased, particularly for degenerative conditions like spondylolisthesis. [
87,
88] The effectiveness of procedures such as lumbar fusion remains debated, with some studies showing no clear advantage over conservative treatments like cognitive behavioural therapy. [
89] Placebo effects and the natural course of LBP further complicate the assessment of surgery's long-term efficacy. [
87]
7.2. Spine Surgery with Facet Arthroplasty
Facet arthroplasty, using devices like TOPS and FENIX, has been proposed as a treatment option for mechanical LBP, particularly in cases involving conditions like spondylolisthesis. [
90,
91] The TOPS device, designed for dynamic stabilization, showed improvement in patient outcomes, including significant reductions in pain scores. However, it’s crucial to note that the trials were primarily designed for patients with radicular symptoms, such as neurogenic claudication or radiculopathy, rather than for low back pain itself. As a result, its application in treating low back pain, especially when neural compression isn’t involved, remains controversial. The long-term benefits, particularly for non-radicular mechanical pain, are not well-established, and more focused studies are needed to confirm its role.
In contrast, the FENIX device, specifically designed for facet joint-related pain, has shown more targeted results. In a small proof-of-concept and feasibility study, patients experienced significant pain relief and functional improvements, with most maintaining full mobility at 24 months post-surgery. However, the limited size and scope of this trial imply that its outcomes, though encouraging, should be interpreted cautiously. [
90] Broader, longer-term studies are necessary to substantiate its efficacy for treating FJP and confirm its safety profile, particularly in avoiding complications like adjacent segment disease.
Given the mixed evidence and limited scope of current studies, both the TOPS and FENIX devices should be considered experimental options. Their use for purely mechanical LBP remains unproven, and more rigorous trials specifically designed to address this condition are needed before their widespread adoption in clinical practice.
7.3. Multifidus Stimulation for Chronic Low Back Pain
Multifidus stimulation, using devices such as the ReActiv8 (Mainstay Medical, Dublin, Ireland), represents an emerging treatment for chronic mechanical LBP, particularly in patients who have not responded to conservative therapy, including RFA. [
88,
92] This restorative neurostimulation approach targets motor control deficits in the multifidus muscle, which are often implicated in chronic LBP, thus the treatment is not specifically aimed at people suffering from facetogenic pain. Early studies suggest that patients can achieve significant improvements in their LBP, with some experiencing a 50% reduction in pain scores and improved disability outcomes over three years of treatment. [
93] However, while the ReActiv8 device shows promise, especially for patients with long-standing, refractory LBP, it remains an evolving therapy.
Despite these promising results, caution is warranted, as its long-term effectiveness and its comparative efficacy with other treatments like RFA remain unclear. Further research is needed to determine its role within the larger spectrum of LBP management, especially considering the mixed success of neuromodulation therapies in this field.
8. Summary
Low back pain (LBP) affects about 10% of individuals yearly and is a leading cause of disability and healthcare resource consumption globally. [
4,
12] Facet joint pain (FJP) occurs in 27% to 40% of LBP patients, complicating diagnosis due to overlapping symptoms with conditions like disc degeneration and stenosis. [
6,
9,
26] Both clinical examinations and radiological studies demonstrate limited predictive value for diagnosing FJP. [
27]
The lumbar facet joints (LFJs) are synovial joints that form a three-joint-complex with intervertebral discs. [
8,
37] Degeneration of a facet joint or an intervertebral disc can exacerbate pain and dysfunction across the spinal segment. [
9,
17] Conservative management typically involves short-term NSAIDs and physical therapy, while strong opioids are not recommended for chronic LBP. [
62,
63,
64]
Medial branch blocks (MBBs) are frequently used to diagnose facet joint-mediated pain and predict the success of radiofrequency ablation (RFA). [
19,
23,
44] However, they have high false-positive rates (25-40%) and varying accuracy, fuelling the debate whether 0, 1 or 2 MBBs are ideal. [
20,
23,
24,
74] There is insufficient evidence to support the routine use of intra-articular injections for FJP. [
24,
65,
66,
67]
RFA is recognized as the gold standard for interventional treatment for FJP, utilizing heat to disrupt nerve function and block pain signals. [
2,
9,
12,
17,
20,
75] The success of RFA is contingent upon precise needle placement near the medial branch, with a low complication rate. [
61,
76,
79] Alternatives like cooled-RFA, cryodenervation and endoscopic denervation show promise, offering enhanced targeting and pain relief, while pulsed-RFA has proven less effective. [
9,
51,
65,
75,
84] Current literature lacks evidence for surgical options such as spinal fusion outside of controlled trials for facetogenic low back pain. Further research is needed to validate emerging treatments like multifidus stimulation. [
12,
44,
87,
88]
Author Contributions
Conceptualization and writing original draft preparation W.V.O.; review P.V.C., F.C., E.V.d.K, V.D. All authors have read and agreed to the published version of the manuscript. ChatGPT-4 was used for advanced spelling and grammar corrections.
Funding
This research received no external funding.
Ethical approval
No ethical approval was warranted for this literature review.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| C-RFA |
Cooled radiofrequency ablation |
| CT |
Computed tomography |
| DRG |
dorsal root ganglion |
| ED |
Endoscopic denervation |
| FJP |
Facet joint pain |
| IA |
Intra-articular |
| IAP |
inferior articular process |
| LFJ |
lumbar facet joints |
| LPB |
Low back pain |
| LSTV |
lumbosacral transitional vertebrae |
| MB |
medial branch |
| MBB |
medial branch block |
| MRI |
Magnetic Resonance Imaging (MRI ) |
| NICE |
National Institute for Health and Care Excellence |
| NSAID |
non-steroidal anti-inflammatory medication |
| OA |
osteoarthritis |
| P-RFA |
Pulsed radiofrequency ablation |
| PRP |
platelet-rich plasma |
| RF |
radiofrequency |
| RFA |
radiofrequency ablation |
| SAP |
superior articular process |
| SNRI |
serotonin and norepinephrine reuptake inhibitors |
| SPECT-CT |
Single Photon Emission Computed Tomography-CT |
| SSRI |
selective serotonin reuptake inhibitors |
| TCA |
tricyclic antidepressants |
| VAS |
visual analogue scale |
References
- Alexander, E. Gaal Most Occurrences of Low Back Pain Are Resolve without Interventi MSgeneRion over the Years. This Notion Is Supported by the Strong Ass Etween the Aaa : | The Most Frequent Etiology of with Symptoms Is Often Localized Low Back Anes Remodeling, in Ca. 2024.
- Manchikanti, L.; Hirsch, J.A.; Falco, F.J.E.; Boswell, M. V. Management of Lumbar Zygapophysial (Facet) Joint Pain. World J. Orthop. 2016, 7, 315–337. [Google Scholar] [CrossRef] [PubMed]
- Rubin, D.I. Epidemiology and Risk Factors for Spine Pain. Neurol. Clin. 2007, 25, 353–371. [Google Scholar] [CrossRef] [PubMed]
- The Lancet Rheumatology The Global Epidemic of Low Back Pain. Lancet Rheumatol. 2023, 5, e305. [CrossRef] [PubMed]
- Karin Due Bruun; Lars Bye-Moller; Henrik Bjarke Vaegter IASP FACT SHEET: Higt-Impact Chronic Pain Available online:. Available online: https://www.iasp-pain.org/resources/fact-sheets/high-impact-chronic-pain/ (accessed on 3 September 2024).
- Ambrosio, L.; Vadalà, G.; Russo, F.; Pascarella, G.; De Salvatore, S.; Papalia, G.F.; Ruggiero, A.; Di Folco, M.; Carassiti, M.; Papalia, R.; et al. Interventional Minimally Invasive Treatments for Chronic Low Back Pain Caused by Lumbar Facet Joint Syndrome: A Systematic Review. Glob. Spine J. 2023, 13, 1163–1179. [Google Scholar] [CrossRef]
- Hoy, D.; March, L.; Brooks, P.; Blyth, F.; Woolf, A.; Bain, C.; Williams, G.; Smith, E.; Vos, T.; Barendregt, J.; et al. The Global Burden of Low Back Pain: Estimates from the Global Burden of Disease 2010 Study. Ann. Rheum. Dis. 2014, 73, 968–974. [Google Scholar] [CrossRef]
- Kapetanakis, S.; Gkantsinikoudis, N. Anatomy of Lumbar Facet Joint: A Comprehensive Review. Folia Morphol. 2021, 80, 799–805. [Google Scholar] [CrossRef]
- Du, R.; Xu, G.; Bai, X.; Li, Z. Facet Joint Syndrome: Pathophysiology, Diagnosis, and Treatment. J. Pain Res. 2022, 15, 3689–3710. [Google Scholar] [CrossRef]
- Kalichman, L.; Guermazi, A.; Li, L.; Hunter, D.J.; Suri, P. Facet Orientation and Tropism: Associations with Spondylolysis. J. Spinal Disord. Tech. 2010, 23, 101–105. [Google Scholar] [CrossRef]
- Alexander, C.E.; Cascio, M.A.; Varacallo, M. Lumbosacral Facet Syndrome; StatPearls Publishing: Treasure Island (FL), 2023. [Google Scholar]
- Perolat, R.; Kastler, A.; Nicot, B.; Pellat, J.M.; Tahon, F.; Attye, A.; Heck, O.; Boubagra, K.; Grand, S.; Krainik, A. Facet Joint Syndrome: From Diagnosis to Interventional Management. Insights Imaging 2018, 9, 773–789. [Google Scholar] [CrossRef]
- Stuber, K.; Lerede, C.; Kristmanson, K.; Sajko, S.; Bruno, P. The Diagnostic Accuracy of the Kemp’s Test: A Systematic Review. J. Can. Chiropr. Assoc. 2014, 58, 258–267. [Google Scholar]
- Grogan, J.; Nowicki, B.H.; Schmidt, T.A.; Haughton, V.M. Lumbar Facet Joint Tropism Does Not Accelerate Degeneration of the Facet Joints. Am. J. Neuroradiol. 1997, 18, 1325–1329. [Google Scholar] [PubMed]
- Van de Kelft, E.; Verleye, G.; Van de Kelft, A.S.; Melis, K.; Van Goethem, J. Validation of Topographic Hybrid Single-Photon Emission Computerized Tomography with Computerized Tomography Scan in Patients with and without Nonspecific Chronic Low Back Pain. A Prospective Comparative Study. Spine J. 2017, 17, 1457–1463. [Google Scholar] [CrossRef] [PubMed]
- Kalichman, L.; Li, L.; Kim, D.H.; Guermazi, A.; Berkin, V.; OʼDonnell, C.J.; Hoffmann, U.; Cole, R.; Hunter, D.J. Facet Joint Osteoarthritis and Low Back Pain in the Community-Based Population. Spine (Phila. Pa. 1976). 2008, 33, 2560–2565. [Google Scholar] [CrossRef] [PubMed]
- Van den Heuvel, S.A.S.; Cohen, S.P.C.; de Andrès Ares, J.; Van Boxem, K.; Kallewaard, J.W.; Van Zundert, J. 3. Pain Originating from the Lumbar Facet Joints. Pain Pract. 2024, 24, 160–176. [Google Scholar] [CrossRef]
- Cohen, S.P.; Moon, J.Y.; Brummett, C.M.; White, R.L.; Larkin, T.M. Medial Branch Blocks or Intra-Articular Injections as a Prognostic Tool before Lumbar Facet Radiofrequency Denervation: A Multicenter, Case-Control Study. Reg. Anesth. Pain Med. 2015, 40, 376–383. [Google Scholar] [CrossRef]
- Srinivas Chiravuri, MD Director, Chad M. Brummett, MD, Lynn Kohan, M. ASRA - Facet Joint Pain. Available online: https://www.asra.com/news-publications/asra-updates/blog-landing/legacy-b-blog-posts/2019/08/06/facet-joint-pain (accessed on 28 August 2024).
- Cohen, S.P.; Bhaskar, A.; Bhatia, A.; Buvanendran, A.; Deer, T.; Garg, S.; Hooten, W.M.; Hurley, R.W.; Kennedy, D.J.; McLean, B.C.; et al. Consensus Practice Guidelines on Interventions for Lumbar Facet Joint Pain from a Multispecialty, International Working Group. Reg. Anesth. Pain Med. 2020, 45, 424–467. [Google Scholar] [CrossRef]
- Eldabe, S.; Tariq, A.; Nath, S.; Gulve, A.; Antrobus, H.; Baloch, M.; Buczkowski, P.; Collighan, N.; Fernandez, T.; Fritz, A.K.; et al. Best Practice in Radiofrequency Denervation of the Lumbar Facet Joints: A Consensus Technique. Br. J. Pain 2020, 14, 47–56. [Google Scholar] [CrossRef]
- Occhigrossi, F.; Carpenedo, R.; Leoni, M.L.G.; Varrassi, G.; Chinè, E.; Cascella, M. Delphi-Based Expert Consensus Statements for the Management of Percutaneous Radiofrequency Neurotomy in the Treatment of Lumbar Facet Joint Syndrome. Pain Ther. 2023, 12, 863–877. [Google Scholar] [CrossRef]
- Assavanop, S.; Bhatia, A. Evidence for Diagnostic Blocks Prior to Radiofrequency Ablation of Innervation to the Lumbar Facet Joints – None, Once, or Twice? ASRA News 2024, 49, 1–9. [Google Scholar] [CrossRef]
- Cohen, S.P.; Doshi, T.L.; Constantinescu, O.C.; Zhao, Z.; Kurihara, C.; Larkin, T.M.; Griffith, S.R.; Jacobs, M.B.; Kroski, W.J.; Dawson, T.C.; et al. Effectiveness of Lumbar Facet Joint Blocks and Predictive Value before Radiofrequency Denervation. Anesthesiology 2018, 129, 517–535. [Google Scholar] [CrossRef]
- Juch, J.N.S.; Maas, E.T.; Ostelo, R.W.J.G.; George Groeneweg, J.; Kallewaard, J.W.; Koes, B.W.; Verhagen, A.P.; Van Dongen, J.M.; Huygen, F.J.P.M.; Van Tulder, M.W. Effect of Radiofrequency Denervation on Pain Intensity among Patients with Chronic Lowback Pain the Mint Randomized Clinical Trials. JAMA - J. Am. Med. Assoc. 2017, 318, 68–81. [Google Scholar] [CrossRef] [PubMed]
- Manchikanti, L.; Boswell, M. V.; Singh, V.; Pampati, V.; Damron, K.S.; Beyer, C.D. Prevalence of Facet Joint Pain in Chronic Spinal Pain of Cervical, Thoracic, and Lumbar Regions. BMC Musculoskelet. Disord. 2004, 5, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Binder, D.S.; Nampiaparampil, D.E. The Provocative Lumbar Facet Joint. Curr. Rev. Musculoskelet. Med. 2009, 2, 15–24. [Google Scholar] [CrossRef] [PubMed]
- Piraccini, E.; Calli, M.; Corso, R.M.; Byrne, H.; Maitan, S. Abdominal and Pelvic Pain: An Uncommon Sign in Lumbar Facet Joint Syndrome. Minerva Anestesiol. 2017, 83, 104–105. [Google Scholar] [CrossRef]
- Allegri, M.; Montella, S.; Salici, F.; Valente, A.; Marchesini, M.; Compagnone, C.; Baciarello, M.; Manferdini, M.E.; Fanelli, G. Mechanisms of Low Back Pain : A Guide for Diagnosis and Therapy [ Version 2 ; Peer Review : 3 Approved ]. 2022, 5.
- Fukui, S.; Ohseto, K.; Shiotani, M.; Ohno, K.; Karasawa, H.; Naganuma, Y. Distribution of Referred Pain from the Lumbar Zygapophyseal Joints and Dorsal Rami. Clin. J. Pain 1997, 13, 303–307. [Google Scholar] [CrossRef]
- Grgić, V. [Lumbosacral facet syndrome: functional and organic disorders of lumbosacral facet joints]. Lijec. Vjesn. 2011, 133, 330–336. [Google Scholar]
- Revel, M.; Poiraudeau, S.; Auleley, G.R.; Payan, C.; Denke, A.; Nguyen, M.; Chevrot, A.; Fermanian, J. Capacity of the Clinical Picture to Characterize Low Back Pain Relieved by Facet Joint Anesthesia. Proposed Criteria to Identify Patients with Painful Facet Joints. Spine (Phila. Pa. 1976). 1998, 23, 1972–1976, discussion 1977. [Google Scholar] [CrossRef]
- Laslett, M.; Öberg, B.; Aprill, C.N.; McDonald, B. Zygapophysial Joint Blocks in Chronic Low Back Pain: A Test of Revel’s Model as a Screening Test. BMC Musculoskelet. Disord. 2004, 5, 43. [Google Scholar] [CrossRef]
- Yoo, Y.M.; Kim, K.H. Facet Joint Disorders: From Diagnosis to Treatment. Korean J. Pain 2024, 37, 3–12. [Google Scholar] [CrossRef]
- Edmond, S.L.; Felson, D.T. Function and Back Symptoms in Older Adults. J. Am. Geriatr. Soc. 2003, 51, 1702–1709. [Google Scholar] [CrossRef]
- Cavanaugh, J.M.; Ozaktay, A.C.; Yamashita, H.T.; King, A.I. Lumbar Facet Pain: Biomechanics, Neuroanatomy and Neurophysiology. J. Biomech. 1996, 29, 1117–1129. [Google Scholar] [CrossRef] [PubMed]
- Igarashi, A.; Kikuchi, S.I.; Konno, S.I. Correlation between Inflammatory Cytokines Released from the Lumbar Facet Joint Tissue and Symptoms in Degenerative Lumbar Spinal Disorders. J. Orthop. Sci. 2007, 12, 154–160. [Google Scholar] [CrossRef] [PubMed]
- French, H.D.; Somasundaram, A.J.; Schaefer, N.R.; Laherty, R.W. Lumbosacral Transitional Vertebrae and Its Prevalence in the Australian Population. Glob. Spine J. 2014, 4, 229–232. [Google Scholar] [CrossRef] [PubMed]
- Shuang, F.; Hou, S.X.; Zhu, J.L.; Liu, Y.; Zhou, Y.; Zhang, C.L.; Tang, J.G. Clinical Anatomy and Measurement of the Medial Branch of the Spinal Dorsal Ramus. Med. (United States) 2015, 94, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Lau, P.; Mercer, S.; Govind, J.; Bogduk, N. The Surgical Anatomy of Lumbar Medial Branch Neurotomy (Facet Denervation). Pain Med. 2004, 5, 289–298. [Google Scholar] [CrossRef]
- Tran, J.; Campisi, E.; Roa Agudelo, A.; Agur, A.M.; Loh, E. High-Fidelity 3D Modelling of the Lumbar Dorsal Rami. Interv. Pain Med. 2024, 3, 100401. [Google Scholar] [CrossRef]
- Tran, J.; Lawson, A.; Billias, N.; Loh, E. 3D Nerve Proximity Mapping of the Medial Branch of Lumbar Dorsal Ramus: An Anatomical Study. Interv. Pain Med. 2024, 3, 100414. [Google Scholar] [CrossRef]
- Suseki, K.; Takahashi, Y.; Takahashi, K.; Chiba, T.; Tanaka, K.; Morinaga, T.; Nakamura, S.I.; Moriya, H. Innervation of the Lumbar Facet Joints: Origins and Functions. Spine (Phila. Pa. 1976). 1997, 22, 477–485. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence (NICE) Low Back Pain and Sciatica in over 16s: Assessment and Management (NG59). Available online: http://www.nice.org.uk/guidance/ng59 (accessed on 1 September 2024).
- Enokida, S.; Tanishima, S.; Tanida, A.; Mihara, T.; Takeda, C.; Yamashita, E.; Nagashima, H. Evaluation of Age-Related Changes in Lumbar Facet Joints Using T2 Mapping. J. Orthop. Sci. 2020, 25, 46–51. [Google Scholar] [CrossRef]
- Hofmann, U.K.; Keller, R.L.; Walter, C.; Mittag, F. Predictability of the Effects of Facet Joint Infiltration in the Degenerate Lumbar Spine When Assessing MRI Scans. J. Orthop. Surg. Res. 2017, 12, 180. [Google Scholar] [CrossRef]
- Kasch, R.; Truthmann, J.; Hancock, M.J.; Maher, C.G.; Otto, M.; Nell, C.; Reichwein, N.; Bülow, R.; Chenot, J.F.; Hofer, A.; et al. Association of Lumbar MRI Findings with Current and Future Back Pain in a Population-Based Cohort Study. Spine (Phila. Pa. 1976). 2022, 47, 201–211. [Google Scholar] [CrossRef] [PubMed]
- Matar, H.E.; Navalkissoor, S.; Berovic, M.; Shetty, R.; Garlick, N.; Casey, A.T.H.; Quigley, A.-M. Is Hybrid Imaging (SPECT/CT) a Useful Adjunct in the Management of Suspected Facet Joints Arthropathy? Int. Orthop. 2013, 37, 865–870. [Google Scholar] [CrossRef]
- Freiermuth, D.; Kretzschmar, M.; Bilecen, D.; Schaeren, S.; Jacob, A.L.; Aeschbach, A.; Ruppen, W. Correlation of 99mTc-DPD SPECT/CT Scan Findings and Diagnostic Blockades of Lumbar Medial Branches in Patients with Unspecific Low Back Pain in a Randomized-Controlled Trial. Pain Med. (United States) 2015, 16, 1916–1922. [Google Scholar] [CrossRef] [PubMed]
- Pneumaticos, S.G.; Chatziioannou, S.N.; Hipp, J.A.; Moore, W.H.; Esses, S.I. Low Pain: Prediction of Short-Term Outcome of Facet Joint Injection with Bone Scintigraphy. Radiology 2006, 238, 693–698. [Google Scholar] [CrossRef] [PubMed]
- Birkenmaier, C.; Veihelmann, A.; Trouillier, H.H.; Hausdorf, J.; von Schulze Pellengahr, C. Medial Branch Blocks Versus Pericapsular Blocks in Selecting Patients for Percutaneous Cryodenervation of Lumbar Facet Joints. Reg. Anesth. Pain Med. 2007, 32, 27–33. [Google Scholar] [CrossRef]
- Schwarzer, A.C.; Aprill, C.N.; Derby, R.; Fortin, J.; Kine, G.; Bogduk, N. The False-Positive Rate of Uncontrolled Diagnostic Blocks of the Lumbar Zygapophysial Joints. Pain 1994, 58, 195–200. [Google Scholar] [CrossRef]
- Manchikanti, L.; Pampati, V.; Fellows, B.; Bakhit, C.E. Prevalence of Lumbar Facet Joint Pain in Chronic Low Back Pain. Pain Physician 1999, 2, 59–64. [Google Scholar] [CrossRef]
- Wahezi, S.E.; Alexeev, E.; Georgy, J.S.; Haramati, N.; Erosa, S.A.; Shah, J.M.; Downie, S. Lumbar Medial Branch Block Volume-Dependent Dispersion Patterns as a Predictor for Ablation Success: A Cadaveric Study. PM R 2018, 10, 616–622. [Google Scholar] [CrossRef]
- Dreyfuss, P.; Schwarzer, A.C.; Lau, P.; Bogduk, N. Specificity of Lumbar Medial Branch and L5 Dorsal Ramus Blocks. Spine (Phila. Pa. 1976). 1997, 22, 895–902. [Google Scholar] [CrossRef]
- Lee, C.J.; Kim, Y.C.; Shin, J.H.; Nahm, F.S.; Lee, H.M.; Choi, Y.S.; Lee, S.C.; Ko, J.S.; Kim, T.H.; Sim, W.S.; et al. Intravascular Injection in Lumbar Medial Branch Block: A Prospective Evaluation of 1433 Injections. Anesth. Analg. 2008, 106, 1274–1278, table of contents. [Google Scholar] [CrossRef]
- Veizi, E.; Mchaourab, A. Medial Branch Blocks and Facet Joint Injections as Predictors of Successful Radiofrequency Ablation. Tech. Reg. Anesth. Pain Manag. 2011, 15, 33–38. [Google Scholar] [CrossRef]
- Assavanop, S.; Alomari, A.; Bhatia, A. Diagnostic Block(s) before Radiofrequency Ablation of Innervation to the Spinal Facet Joints: None, Once or Two Times – an International Survey of Pain Medicine Physicians. Reg. Anesth. Pain Med. 2024, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Shaparin, N.; Nair, S.; Kim, R.S.; Hascalovici, J.R. Chronic Low Back Pain: The Therapeutic Benefits of Diagnostic Medial Branch Nerve Blocks. Pain Physician 2021, 24, E521–E528. [Google Scholar] [PubMed]
- Manchikanti, L.; Singh, V.; Falco, F.J.E.; Cash, K.A.; Pampati, V. Evaluation of Lumbar Facet Joint Nerve Blocks in Managing Chronic Low Back Pain: A Randomized, Double-Blind, Controlled Trial with a 2-Year Follow-Up. Int. J. Med. Sci. 2010, 7, 124–135. [Google Scholar] [CrossRef]
- Cohen, S.P.; Williams, K.A.; Kurihara, C.; Nguyen, C.; Shields, C.; Kim, P.; Griffith, S.R.; Larkin, T.M.; Crooks, M.; Williams, N.; et al. Multicenter, Randomized, Comparative Cost-Effectiveness Study Comparing 0, 1, and 2 Diagnostic Medial Branch (Facet Joint Nerve) Block Treatment Paradigms before Lumbar Facet Radiofrequency Denervation. Anesthesiology 2010, 113, 395–405. [Google Scholar] [CrossRef]
- Rodriguez-Merchan, E.C.; Delgado-Martinez, A.D.; Andres-Ares, J. De Radiofrequency Ablation for the Management of Pain of Spinal Origin in Orthopedics. Arch. Bone Jt. Surg. 2023, 11, 666–671. [Google Scholar] [CrossRef]
- Hayden, J.A.; Ellis, J.; Ogilvie, R.; Malmivaara, A.; van Tulder, M.W. Exercise Therapy for Chronic Low Back Pain. Cochrane Database Syst. Rev. 2021, 2021. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence (NICE) Low Back Pain and Sciatica in over 16s: Quality Standard (SQ155) Available online:. Available online: http://www.nice.org.uk/guidance/sq155 (accessed on 1 September 2024).
- McCormick, Z.L.; Conger, A.; Kendall, R.; Wagner, G.; Michael Henrie, A.; Littell, M.; Sperry, B.P.; Petersen, R.; Cooper, A.N.; Teramoto, M.; et al. A Pragmatic Randomized Prospective Trial of Cooled Radiofrequency Ablation of the Medial Branch Nerves versus Facet Joint Injection of Corticosteroid for the Treatment of Lumbar Facet Syndrome: 12 Month Outcomes. Pain Med. (United States) 2023, 24, 1318–1331. [Google Scholar] [CrossRef]
- Kennedy, D.J.; Fraiser, R.; Zheng, P.; Huynh, L.; Levin, J.; Smuck, M.; Schneider, B.J. Intra-Articular Steroids vs Saline for Lumbar Z-Joint Pain: A Prospective, Randomized, Double-Blind Placebo-Controlled Trial. Pain Med. (United States) 2019, 20, 246–251. [Google Scholar] [CrossRef]
- Carette, S.; Marcoux, S.; Truchon, R.; Grondin, C.; Gagnon, J.; Allard, Y.; Latulippe, M. A Controlled Trial of Corticosteroid Injections into Facet Joints for Chronic Low Back Pain. N. Engl. J. Med. 1991, 325, 1002–1007. [Google Scholar] [CrossRef]
- Sayed, D.; Grider, J.; Strand, N.; Hagedorn, J.M.; Falowski, S.; Lam, C.M.; Francio, V.T.; Beall, D.P.; Tomycz, N.D.; Davanzo, J.R.; et al. The American Society of Pain and Neuroscience ( ASPN ) Evidence-Based Clinical Guideline of Interventional Treatments for Low Back Pain; 2022; ISBN 9135885521.
- Wu, J.; Zhou, J.; Liu, C.; Zhang, J.; Xiong, W.; Lv, Y.; Liu, R.; Wang, R.; Du, Z.; Zhang, G.; et al. A Prospective Study Comparing Platelet-Rich Plasma and Local Anesthetic (LA)/Corticosteroid in Intra-Articular Injection for the Treatment of Lumbar Facet Joint Syndrome. Pain Pract. 2017, 17, 914–924. [Google Scholar] [CrossRef] [PubMed]
- Kotb, S.Y.; Sherif, N.M.; Saleh, H.A.; Ahmed, S.F.; Sakr, H.M.; Taeimah, M.O. The Role of Intra-Articular Injection of Autologous Platelet-Rich Plasma versus Corticosteroids in the Treatment of Synovitis in Lumbar Facet Joint Disease. Saudi Med. J. 2022, 43, 1200–1208. [Google Scholar] [CrossRef] [PubMed]
- Cosman, E.R.; Dolensky, J.R.; Hoffman, R.A. Factors That Affect Radiofrequency Heat Lesion Size. Pain Med. (United States) 2014, 15, 2020–2036. [Google Scholar] [CrossRef] [PubMed]
- Van Boxem, K.; Huntoon, M.; Van Zundert, J.; Patijn, J.; Van Kleef, M.; Joosten, E.A. Pulsed Radiofrequency: A Review of the Basic Science as Applied to the Pathophysiology of Radicular Pain: A Call for Clinical Translation. Reg. Anesth. Pain Med. 2014, 39, 149–159. [Google Scholar] [CrossRef]
- Van Zundert, J.; Mekhail, N.; Vanelderen, P.; Van Kleef, M. Diagnostic Medial Branch Blocks before Lumbar Radiofrequency Zygapophysial (Facet) Joint Denervation: Benefit or Burden? Anesthesiology 2010, 113, 276–278. [Google Scholar] [CrossRef]
- Falco, F.J.E.; Manchikanti, L.; Datta, S.; Sehgal, N.; Geffert, S.; Onyewu, O.; Singh, V.; Bryce, D.A.; Benyamin, R.M.; Simopoulos, T.T.; et al. An Update of the Systematic Assessment of the Diagnostic Accuracy of Lumbar Facet Joint Nerve Blocks. Pain Physician 2012, 15, 869–908. [Google Scholar] [CrossRef]
- Meloncelli, S.; Germani, G.; Urti, I.; Divizia, M.; Rosciano, M.; Puntillo, F.; Paladini, A.; Varrassi, G. Endoscopic Radiofrequency Facet Joint Treatment in Patients with Low Back Pain: Technique and Long-Term Results. A Prospective Cohort Study. Ther. Adv. Musculoskelet. Dis. 2020, 12, 1759720X2095897. [Google Scholar] [CrossRef]
- Tran, J.; Alboog, A.; Barua, U.; Billias, N.; Loh, E. Optimal Caudal Needle Angulation for Lumbar Medial Branch Denervation: A 3D Cadaveric and Clinical Imaging Comparison Study. Interv. Pain Med. 2024, 3, 100433. [Google Scholar] [CrossRef]
- Schneider, B.J.; Doan, L.; Maes, M.K.; Martinez, K.R.; Gonzalez Cota, A.; Bogduk, N. Systematic Review of the Effectiveness of Lumbar Medial Branch Thermal Radiofrequency Neurotomy, Stratified for Diagnostic Methods and Procedural Technique. Pain Med. (United States) 2020, 21, 1122–1141. [Google Scholar] [CrossRef]
- Cohen, S.P.; Strassels, S.A.; Kurihara, C.; Lesnick, I.K.; Hanling, S.R.; Griffith, S.R.; Buckenmaier, C.C.; Nguyen, C. Does Sensory Stimulation Threshold Affect Lumbar Facet Radiofrequency Denervation Outcomes? A Prospective Clinical Correlational Study. Anesth. Analg. 2011, 113, 1233–1241. [Google Scholar] [CrossRef]
- Manchikanti, L.; Malla, Y.; Wargo, B.W.; Cash, K.A.; Pampati, V.; Fellows, B. Complications of Fluoroscopically Directed Facet Joint Nerve Blocks: A Prospective Evaluation of 7,500 Episodes with 43,000 Nerve Blocks. Pain Physician 2012, 15, 143–150. [Google Scholar] [CrossRef]
- Sadeghi, S.; Bible, J.E.; Cortes, D.H. Quantifying Dysfunction of the Lumbar Multifidus Muscle After Radiofrequency Neurotomy and Fusion Surgery: A Preliminary Study. J. Eng. Sci. Med. Diagnostics Ther. 2020, 3, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Saito, T.; Steinke, H.; Miyaki, T.; Nawa, S.; Umemoto, K.; Miyakawa, K.; Wakao, N.; Asamoto, K.; Nakano, T. Analysis of the Posterior Ramus of the Lumbar Spinal Nerve: The Structure of the Posterior Ramus of the Spinal Nerve. Anesthesiology 2013, 118, 88–94. [Google Scholar] [CrossRef]
- Dreyfuss, P.; Stout, A.; Aprill, C.; Pollei, S.; Johnson, B.; Bogduk, N. The Significance of Multifidus Atrophy after Successful Radiofrequency Neurotomy for Low Back Pain. PM R 2009, 1, 719–722. [Google Scholar] [CrossRef]
- Afifi, A.; Ringe, M.; Sobottke, R.; Oikonomidis, S.; Teuben, M.P.J. Lumbar Facet Joint Radiofrequency Denervation Therapy for Chronic Low Back Pain: Enhanced Outcome Compared With Chemical Neurolysis (Ethyl Alcohol 95% or Glycerol 20%). Int. J. spine Surg. 2022, 16, 33–41. [Google Scholar] [CrossRef]
- Wallscheid, F.; Manthey, M.; Olsen, J.; Oikonomidis, S.; Meyer, C.; Eysel, P.; Löhrer, L.; Bredow, J. Endoscopic Facet Joint Denervation on the Lumbar Spine: A Retrospective Analysis. Asian Spine J. 2023, 17, 382–391. [Google Scholar] [CrossRef]
- Walter, S.G.; Struwe, C.; Scheidt, S.; Strohmenger, L.; Bornemann, R.; Wirtz, D.C.; Pflugmacher, R.; Rommelspacher, Y. Endoscopic Facet Joint Denervation for Treatment of Chronic Lower Back Pain. Clin. Neurol. Neurosurg. 2020, 195, 105904. [Google Scholar] [CrossRef]
- Woiciechowsky, C.; Richter, L.M. Endoscopic 4-MHz Radiofrequency Treatment of Facet Joint Syndrome Is More Than Just Denervation: One Incision for Three Facets. J. Neurol. Surgery, Part A Cent. Eur. Neurosurg. 2020, 81, 238–242. [Google Scholar] [CrossRef]
- Evans, L.; O’Donohoe, T.; Morokoff, A.; Drummond, K. The Role of Spinal Surgery in the Treatment of Low Back Pain. Med. J. Aust. 2023, 218, 40–45. [Google Scholar] [CrossRef]
- Thomson, S.; Williams, A.; Vajramani, G.; Sharma, M.; Love-Jones, S.; Chawla, R.; Eldabe, S. Restorative Neurostimulation for Chronic Mechanical Low Back Pain – Three Year Results from the United Kingdom Post Market Clinical Follow-up Registry. Br. J. Pain 2023, 17, 447–456. [Google Scholar] [CrossRef]
- Surgery of the Spine and Spinal Cord; van de Kelft, E. , Ed.; Springer International Publishing: Cham, 2016; ISBN 978-3-319-27611-3. [Google Scholar]
- De Kelft, E. V. Lumbar Facet Resurfacing: First Experience with the FENIX Implant. Clin. Spine Surg. 2016, 29, E475–E481. [Google Scholar] [CrossRef] [PubMed]
- Pinter, Z.W.; Freedman, B.A.; Nassr, A.; Sebastian, A.S.; Coric, D.; Welch, W.C.; Steinmetz, M.P.; Robbins, S.E.; Ament, J.; Anand, N.; et al. A Prospective Study of Lumbar Facet Arthroplasty in the Treatment of Degenerative Spondylolisthesis and Stenosis: Results from the Total Posterior Spine System (TOPS) IDE Study. Clin. Spine Surg. 2023, 36, E59–E69. [Google Scholar] [CrossRef] [PubMed]
- Deckers, K.; De Smedt, K.; Mitchell, B.; Vivian, D.; Russo, M.; Georgius, P.; Green, M.; Vieceli, J.; Eldabe, S.; Gulve, A.; et al. New Therapy for Refractory Chronic Mechanical Low Back Pain—Restorative Neurostimulation to Activate the Lumbar Multifidus: One Year Results of a Prospective Multicenter Clinical Trial. Neuromodulation 2018, 21, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Gilligan, C.; Volschenk, W.; Russo, M.; Green, M.; Gilmore, C.; Mehta, V.; Deckers, K.; De Smedt, K.; Latif, U.; Sayed, D.; et al. Five-Year Longitudinal Follow-Up of Restorative Neurostimulation Shows Durability of Effectiveness in Patients With Refractory Chronic Low Back Pain Associated With Multifidus Muscle Dysfunction. Neuromodulation 2024, 27, 930–943. [Google Scholar] [CrossRef]
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).