
Submitted:
16 October 2024
Posted:
18 October 2024
Read the latest preprint version here
Abstract
Background: Several studies hypothesized a therapeutic role of probiotics in the management of chronic bacterial prostatitis (CBP) patients. Here, we assessed the effect of probiotics as an add-on treatment in patients with clinical recurrences of CBP, through gut microbiota modification analysis. Methods: This study has been planned as a randomized, double-blind, placebo-controlled, multicenter clinical trial examining the efficacy and safety of consumption of probiotics containing human Lactobacillus casei DG® or placebo following 1 month-treatment with ciprofloxacin. Twenty-four patients with CBP were recruited and treated for 3 months with placebo (n. 12) or with Lactobacillus Casei DG® (n. 12). During the enrollment and follow-ups, IPSS, NIH-CPSI and SF-36 were used. Urological examinations and microbiological tests were performed to analyze the symptomatology, recurrences frequency, and gut and seminal microbiota. Results: The treatment with Lactobacillus Casei DG® induced a significantly (p<0.01) faster recovery of symptoms (2 days vs. 8 days) than placebo and an increased time free from symptoms (86 days vs. 42 days) without the occurrence of adverse events. In the treatment group, the appearance of Lactobacilli after 30 days (T1) was higher in the probiotic group, and a significant reduction of Corynebacterium, Peptoniphilus, Pseudomonas, Veillonella, Staphylococcus and Streptococcus has been observed. Conclusion: These data suggest that in patients with CBP, the use of Lactobacillus casei DG after an antimicrobial treatment is safe and effective in improving the days free of symptoms and the quality of life.
Keywords:
microbiota
; chronic bacterial prostatitis
; antibiotic resistance
; lactobacillus casei DG
1. Introduction
Chronic prostatitis is a chronic inflammation of the prostate gland affecting men of all ages with a prevalence of 14% under 50 years of age; of these, 10% would be of bacterial origin [1,2]. Clinical symptoms include genital pain, painful ejaculation, urinary dysfunctions (nocturia, dysuria, hematuria, stranguries), haemospermia, and fever that present as relapses typical of the chronic condition after variably prolonged periods of remission. Without a specific treatment, chronic bacterial prostatitis can lead to complications such as persistent urination disorders, prostate abscesses, and bacteremia [3]. Chronic bacterial prostatitis requires the use of long-lasting treatments with fluoroquinolones (from 6 weeks to 3 months up to 6 months) depending on the severity of symptoms, with an increased risk of antibiotic resistance as well as interactions in poly-treated patients [4]. Recent evidences hypothesized that probiotics in association with antibiotic treatment might reduce the adverse effects of the treatment, the risk of recurrence and improve patients’ quality of life, through an effective modification of gut microbiota [5]. This study aims to evaluate the clinical efficacy and safety of probiotics in patients with chronic bacterial prostatitis already treated with fluoroquinolones by analyzing the symptomatology, the frequency of relapses, and the composition of gut microbiota.
2. Materials and Methods
2.1. Study Design
This is a randomized, double-blind, placebo-controlled, multicenter clinical trial examining the efficacy and safety of consumption of probiotics containing human Lactobacillus casei DG®, according to European Society of Urology (EAU) guidelines [4] vs placebo both following treatment with ciprofloxacin in patients with chronic bacterial prostatitis. The study was conducted by the Pharmacology and Pharmacovigilance Unit of the Magna Graecia University of Catanzaro, Dulbecco University Hospital of Catanzaro, Urology Unit of the territorial health department of Catanzaro and Urology Unit of Dulbecco University Hospital of Catanzaro from March 2022 to April 2024. During the intervention period, the enrolled participants consumed their assigned products twice a day for 3 months.
Patients were enrolled at baseline (T0) and then were monitored at 30 days (T1), 90 days (T2), and 180 days (T3) to evaluate adherence to treatment. At the beginning of the study, participants were asked not to change their usual dietary habits during treatment.
2.2. Participants
In this study, 24 patients were enrolled from Urology Unit of the territorial health department of Catanzaro and Urology Unit of Dulbecco University Hospital of Catanzaro, according to the following eligibility criteria:
- (1)
- Subject between 18 and 55 years old with clinical, instrumental, and microbiological diagnosis of chronic prostatitis, according to indications of the EAU and history of symptomatology related to the diagnosis of chronic bacterial prostatitis for more than 6 months [4].
- (2)
- Isolation of uropathogens, according to EAU indications, in microbiological samples from Meares-Stamy tests or semen culture [4].
- (3)
- NIH-CPSI >9 and change in IPSS and SF-36 questionnaires (no significant cut-off is indicated), in line with EAU recommendations [4].
- (4)
- Subjects who can follow the study and give their consent to enroll in the study.
Patients with established organic bowel disease (including celiac disease or inflammatory bowel disease), allergies related to fluoroquinolones, infectious intestinal diseases, psychiatric illnesses and/or psychological disorders, active malignancy of any type or history of malignancy (patients with a history of other malignancies that have been surgically removed and who have no evidence of relapses for at least five years prior to study enrollment are also acceptable), were excluded. In the investigator's judgment, the Charson-Comorbility Index >2 or with any severe pathology that may interfere with study treatment. We also excluded subjects who have carried out prior antibiotic therapy (for any indication) within the last 3 months or current antibiotic therapy, chronic use of probiotics or supplements/herbal remedies in the month before the start of the trial, or who have undergone previous abdominal surgeries. Also considered as exclusion criteria were episodes of viral or bacterial enteritis within 2 months prior to the study, recent history or suspicion of alcohol or drug abuse, inadequate reliability or presence of conditions that may lead to patient non-compliance/adherence to the protocol or prior participation in this study or concurrent with other clinical trials.
2.3. Drugs
During the study patients were treated for 3 months with
- − 1 capsule/day containing 24 billion live cells of Lactobacillus Casei DG® (Enterolactis® plus), supported by Alfasigma S.p.A. - Via Ragazzi del ‘99, 5 - Bologna (Italy).
- − 1 capsule/day in packaging identical to probiotic with the same color, weight, smell and taste, but without bacteria, supported by Alfasigma S.p.A. - Via Ragazzi del ‘99, 5 - Bologna (Italy).
2.4. Experimental Protocol
Enrolled patients were randomized, using a 1:1 protocol of randomization, into two groups: Group A: probiotic (n: 12). and Group B: placebo (n: 12). The subjects were identified with a numerical code to preserve privacy. Before the beginning of the study, and during follow-up(s), urological evaluation was performed, and urologists administered questionnaires. Clinical and laboratory data were collected directly by the medical staff involved in the study.
2.5. Questionnaires
Patients were administered the following questionnaires:
- (1)
- International Prostatic Symptoms Score (IPSS) consists of 8 questions used to screen, diagnose and monitor symptoms linked to benign prostatic hyperplasia. The answers are given points on a scale of 0 to 5. The IPSS values were classified as mild (scores 0–7), moderate (scores 8–19), and severe (scores 20–35) non-neurologic lower urinary tract symptoms, specifically incomplete bladder emptying, frequency, intermittency, urgency, weak stream, straining to void, and nocturia [6].
- (2)
- NIH-Chronic Prostatitis Symptom Index (NIH-CPSI), consisting of 9 items and used to assess the symptom severity of prostatitis and the effectiveness of treatment. NIH-CPSI includes three subscales with a total score ranging from 0 to 43: pain or discomfort (4 items with a total score ranging from 0 to 21), urinary symptoms (2 items with a total score ranging from 0 to 10), impact on the quality of life (3 items with a total score ranging from 0 to 12 points). The scores will also be higher as the symptoms get more severe [7].
- (3)
- International Index of Erectile Function (IIEF-5), consisting of 5 questions indicating the presence of erectile dysfunction, each of which can be scored from 0 or 1 (representing the worst) to 5 (representing the best). The final score ranges from 1 to 25 points. Erectile dysfunction is classified based on the overall score as severe (score 0 to 7), moderate to severe (score 8 to 11), mild to moderate (score 12 to 16), mild (score 17 to 21) and absent (score 22 to 25) [8].
- (4)
- The 36-Item Short Form Health Survey (SF-36), consisting of 36 questions and used to assess quality of life about pathology and the effectiveness of treatment. Quality of life is defined as the subjective perception of one's own well-being within socio-cultural context or as the satisfaction of desires and pleasures. Questions are summarized in two component summary scores, the Physical Component Summary (PCS) and the Mental Component Summary (MCS) scores representing eight concepts of health: physical functioning (PF), bodily pain (BP), role limitations due to physical health problems (RP), role limitations due to personal or emotional problems (RE), general mental health (MH), social functioning (SF), energy/fatigue or vitality (VIT), and general health perceptions (GH). A higher score represents better health while a low score corresponds to a lower quality of life [9,10].
- (5)
- Zung’s Self-Rating Anxiety Scale (Zung SAS) consists of a 20-item question scale that rates the four common characteristics of anxiety, both psychological and somatic. Responses are given on a 4-point scale which range from 1 (none, or a little of the time) to 4 (most, or all of the time). Items include both negative and positive experiences. The final score ranges from 20 to 80 points. Anxiety is classified as normal (score 0 to 44), moderate (score 45 to 59) and severe (score 60 to 80) [11].
- (6)
- Zung’s Self-Rating Depression Scale (Zung SDS) consists of a 20-item question scale that rates the four common characteristics of depression. Items tap psychological and physiological symptoms: 10 express negative experiences, and 10 express positive experiences. Responses are given on a 4-point scale ranging from 1 (none, or a little of the time) to 4 (most, or all of the time). Total raw scores range from 20 to 80. Depression is classified as normal (score 20 to 49), mild (score 50 to 59), moderate (score 60 to 69) and severe (score 70 to 80) [12].
2.6. Meares-Stamey Test
Patients enrolled in the study underwent a thorough microbiological evaluation with the Meares-Stamey test to identify bacteria and leukocyturia in three/four biological samples: first void urine (VB1), second void urine (VB2), prostate massage secretion (EPS), post-massage urine (VB3) [13].
2.7. Fecal Samples
The samples were kept at ambient temperature until analysis, which was usually performed within 4 to 5 h of receipt. Analysis was performed 7 days a week, and then were tested within 24 h of collection.
2.8. Microbiological Identification Tests
Gut Microbiota was analyzed using both QIAstat-Dx® Gastrointestinal Panel and culture isolation tests. The analysis with QIAstat-Dx® Gastrointestinal Panel 1 was used according to the manufacturer’s instructions. The analysis requires approximately 50–200 mg of feces collected with a focked swab from the FaecalSwab sample collection system (Copan, Brescia, Italy) that has to be resuspended in 2 mL of CaryBlair transport medium. A total of 200 μL of the FaecalSwab suspension was collected using a transfer pipette and loaded into the liquid sample port of a QIAstat-Dx® Gastrointestinal Panel cartridge. All reactions are performed by the closed QIAstat-Dx® system within the loaded cartridge and included lysis, extraction, amplification, and measurements of fluorescence of the amplified PCR products. The QIAstat-Dx® Analyzer Software interprets the results and generates test reports used to evaluate potential gastrointestinal pathogen findings. An internal control is included in the assay to monitor the quality of the reactions for a given sample. If the internal control is reported positive, all results are valid. If the internal control is reported negative, only positive results for targets are valid while negative results for targets are invalid. Running a sample with the QIAstat-Dx® Gastrointestinal Panel takes approximately 70 min/sample. In agreement with manufacture, the QIAstat-Dx® Gastrointestinal Panel detects the following pathogens: Campylobacter spp. (C. jejuni, C. upsaliensis, and C. coli), Clostridioides difficile tcdA/tcdB, enteroaggregative E. coli (EAEC), enteropathogenic E. coli (EPEC), enterotoxigenic E. coli (ETEC) eltA/estA, Shiga toxin–producing E. coli (STEC) stx1/stx2, Shiga toxin–producing E. coli (STEC) stx1/stx2 O157, enteroinvasive E. coli (EIEC)/Shigella (S. sonnei, S. fexneri, S. boydii, and S. dysenteriae), Plesiomonas shigelloides, Salmonella spp., Vibrio cholerae, Vibrio parahaemolyticus, Vibrio vulnifcus, Yersinia enterocolitica, Cyclospora cayetanensis, Cryptosporidium spp. (C. parvum, C. hominis, C. felis, and C. meleagridis), Entamoeba histolytica, Giardia lamblia, adenovirus F40/F41, norovirus GI and GII, rotavirus, and sapovirus (I, II, IV, and V).
Microbiological tests and phase-contrast microscope (Phase contrast 2, Nikon, Tokyo, Japan) were used to evaluate the other bacteria. Microbiological test included Gram staining, evaluation of catalase, oxidase, urease, methyl red, citrate, triple sugar iron, gas formation, and fermentation for the identification of lactic acid bacteria isolates. The results were interpreted according to Bergey’s manuals [14].
2.9. Admission (T0)
All patients underwent urological and rectal examinations during the admission, and IPSS, NIH-CPSI, IIEF-5, Zung SAS, Zung SDS and SF-36 questionnaires were administered. Following international guidelines, subjects who met the inclusion criteria were enrolled and treated with Ciprofloxacin 1000 mg daily for 4 weeks. At the end of antibiotic therapy, all patients underwent microbiological evaluation with Meares-Stamey test and a stool sample was collected from each patient to analyze gut and seminal microbiota. Afterward, subjects were randomized into either the placebo group or the probiotic group.
2.10. Follow-Up Visits (T1, T2, T3)
Starting at T0, 30 days (T1), 90 days (T2) and the end of the study at 180 days (T3) were considered as follow-ups. At each follow-up, patients underwent urological examination and rectal examination, and each was administered the IPSS, NIH-CPSI, IIEF-5, Zung SAS, Zung SDS, and SF-36 questionnaires. In addition, microbiological evaluation with Meares-Stamey test, and/or semen culture, were performed and a stool sample was collected to assess any changes in the gut and seminal microbiota associated with probiotic intake. The dedicated database evaluated and recorded any systemic or local side effects.
2.11. Outcomes
The primary outcomes included a statistically significant reduction (P<0.05) in the number of prostatitis exacerbations in the human Lactobacillus Casei DG® group vs the placebo group, both taken from the end of antibiotic therapy. Instead, the second outcome included evaluation of the different evolutions of gut microbiota in the human Lactobacillus Casei DG® group vs. the placebo group, evaluation in the development of adverse events (assessed with Naranjo Scale), reduction of recovery time of the disease relapses and reduction in the intensity of prostatitis symptoms.
2.12. Statistical Analysis and Ethical Considerations
The microbial composition of the samples was analyzed using the VSEARCH software (version v2.22.1). The inter-group differences were evaluated by parametric methods (t-test). Correlation quotients were assessed by means of a non-parametric Spearman criterion. Normality was evaluated using Shapiro-Wilk test and T-test was used to analyze the differences between the groups. For all comparisons, differences were considered significant for p <0.05. All methods of collecting biological samples from stool used under this medical examination were taken with the approval of the attending physician. The study was conducted in accordance with guidelines of the 1964 Declaration of Helsinki and its later amendments. All patients or their guardians signed a written informed consent. This study was approved by the Local Ethical Committee of Calabria Centro (ID number 258 of 19 September 2019).
3. Results
3.1. Population
During the study, 82 patients with chronic bacterial prostatitis were evaluated, and 24 patients who satisfied the inclusion criteria were enrolled and signed the informed consent. Moreover, they were randomized into two groups: probiotic group (n 12) and placebo group (n 12) (Table 1). The Shapiro-Wilk test documented a normality distribution between the groups (p = 0.91, w = 0.96).
Of the 24 patients with chronic bacterial prostatitis who participated in the study, all completed the course of treatment.
3.2. Gut Microbiota Analysis
At T0, gut microbiota analysis documented the absence of pathogens (Table 2).
Microbiological culture documented that bacteroides, parabacteroides and lactobacilluss GG were absent or of negligible quantity at admission (T0), testifying to the presence of dysbiosis (Figure 1). During the follow-up (T1) the reappearance of Bacteroides, Parabacteroides and lactobacillus GG were recorded. In contrast, in placebo group, it was necessary to wait 90 days (T2) to find the development of Lactobacilli. At T3, the gut microbiota revealed a normalization of the bacterial population in all participants of both groups, but with a higher presence of Lactobacilli in the probiotic group (Figure 1 and Figure 2).
3.3. Seminal Microbiota Analysis
In the study, the presence of many bacterial species in the seminal fluid was evaluated and, at T0, it was found that all patients with chronic infectious prostatitis, following antibiotic treatment with ciprofloxacin, had a microbial population characterized mainly by Corynebacterium, Peptoniphilus, and Veillonella (Figure 3 and Figure 4). During the follow-up visits, the seminal fluid was re-evaluated and we documented a normalization of the microbiota in the probiotic and placebo groups, with the appearance of Lactobacilli after 30 days (T1), even if this was most significantly in probiotic group (P<0.01) (Figure 3 and Figure 4).
3.4. Questionnaire Analysis
Regarding the severity of symptoms and disease recurrence, the NIH-CPSI questionnaire was completed by all participants. It showed a non-significant difference between the placebo group and the placebo group from T0 (p = 0.00) to T3 (p = 0.187), with a comparable decrease between the two groups during the treatment (Figure 5). The IPSS test used to evaluate urinary symptoms also produced a similar result. In this case, the difference was not significant (pT3 = 0.546) (Figure 6).
All participants completed the IIEF-5 questionnaire. Total IIEF-5 score ranged between 0 and 25. In the probiotic group compared to the placebo group, we documented an improvement in erective function, as shown in the Table 3.
3.5. Clinical Evaluation
Patients enrolled in L. Casei DG® group documented a significant faster recovery (P<0.01) compared to placebo, with a decrease in the duration of disease relapse and the appearance of milder symptoms with a remarkable improvement in both quality of life and mood. SF-36 questionnaire score showed a time-related significant difference (P<0.01) between the two groups studied (Figure 7). In particular in T1 we recorded a significant improvement (P<0.01) in SF-36 score vs T0 and also respect to placebo group. Same data were recorded in T2 and T3 (P<0.01) (Figure 7). In addition, comparing the mean Zung SDS and Zung SAS between placebo and control group we observed, at T3, a higher score in the placebo group compared to T0 when the difference between the groups was significant (P<0.01) (Figure 8 and Figure 9).
4. Discussion
In this study, we demonstrated that, compared to patients who took only placebo following antibiotic therapy, participants who took the probiotic containing Lactobacillus casei DG® achieved milder symptoms and a faster recovery from prostatitis relapses. Prostatitis is an inflammation of the prostate gland quite common. As described in a systematic review, on a population exceeding 10.000 patients, prevalence can be estimated of 8.2%, with 35-50% of men that reported to have experienced a symptomatic prostatitis event in their lifetime [15]. Chronic prostatitis, which we have examined, can present with very debilitating symptoms as urogenital pain, lower urinary tract symptoms (nocturia, dysuria, hematuria, stranguries), haemospermia, fever and/or sexual dysfunction [16,17]. The symptoms usually continue for at least 3 months and that present as relapses typical of the chronic condition after variably prolonged periods of remission [18]. As numerous studies demonstrate, Bacterial infection is considered a causal factor that triggers the prostatic inflammatory response [19,20,21]. Hence, the use of antibiotics as a treatment for chronic prostatitis, especially fluoroquinolones which have the best pharmacological properties for treating bacterial prostatitis. Antibiotics with good penetration into the prostate tissue also include trimethoprim-sulfamethoxazole, clindamycin, doxycycline, and azithromycin [22]. Antibiotic therapy for chronic bacterial prostatitis is effective. However, it requires the use of a long-lasting treatments (fluoroquinolones up to 6 months, depending on the severity of the pathological form) and which therefore increases the risk of developing antibiotic resistance and triggering interactions especially in poly-treated patients [22]. Probiotics are active microorganisms belonging to strains already present in the human intestine and which, once they reach the enteric tract, multiply and rebalance the intestinal microflora. Therefore, probiotics must resist the digestive action of gastric juice, bile salts and digestive enzymes and, once it reaches the intestine, it must be able to adhere to intestinal cells, multiply and colonize them. Therefore, it must give a beneficial effect by antagonizing pathogenic microorganisms without, however, triggering immune reactions. Probiotics are commonly used to strengthen intestinal immunity and counteract enteritis and diarrhea that is infectious, drug-related or food intolerance. Currently, however, many studies are underway to find new possible therapeutic uses given the varied influence that the microbiota regulation exerts on many systems. The gut microbiota, in fact, is considered almost as a "forgotten organ" capable of establishing multidirectional communications with other organs [5]. Many studies reveal that probiotics promote the development of the postnatal immune system inhibiting the activated CD4+ T cells [23].
Moreover, lactobacilli promote the activation of dendritic cells, which are essential for activating the immune response [24]. In our study, we evaluated the effects of a formulation containing 24 billion live cells of Lactobacillus casei DG® in managing chronic prostatitis. Lactobacillus casei DG® is a Gram-positive bacterium normally present in our gut flora and commonly used to modulate the structure and functionality of the gut microbiota [25,26,27]. All enrolled patients completed the study and showed a normalization in the composition of gut and seminal microorganisms at the end of the treatment. However, patients enrolled in Lactobacillus casei DG® group presented a faster recovery from prostatitis and milder symptoms than patients who took placebo alone. It is probably the reason for a faster clinical recovery demonstrated also by other authors [22,28]. Psychosocial and psychiatric disorders, as anxiety and depression, are usually also associated with chronic diseases and negatively affect the quality of life [29,30]. In agreement with this study, we reported that patients with chronic prostatitis show anxiety and depression with a decrease in the quality of life. These symptoms improved at the end of the study with a time-dependent pattern, particularly in patients enrolled in the probiotic group. Finally, in enrolled patients, we did not record the development of adverse drug reactions or drug interactions, revealing the probiotics are safe in all people. The low number of enrolled patients and the absence of a specific evaluation of inflammatory or immune biomarkers represent a limitation of the present study.
5. Conclusions
Our data suggest that in patients with chronic prostatitis, the use of Lactobacillus casei DG® after an antimicrobial treatment is safe and effective in the improvement of the days free of symptoms and is also able to improve the quality of life, through an early restoration of gut microbiota.
Author Contributions
Conceptualization, L.G., A.P. and T.C.; methodology, C.V., D. MAG., and E.C.; software, T.Ce., S.B.; formal analysis, V.R., G.M., C.P. and L.C.; investigation, M.C., G.LC., I.M.P.; resources, A.P.; data curation, L.G.; writing—original draft preparation, C.V.; writing—review and editing, L.G. and T.C.; supervision, G. DS.. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Local Ethical Committee of Calabria Centro (ID number 258 of 19 September 2019).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patient(s) to publish this paper.
Data Availability Statement
Data is unavailable due to privacy or ethical restrictions in accordance to Italian bylaw.
Acknowledgments
None.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Rees, J.; Abrahams, M.; Doble, A.; Cooper, A. Prostatitis Expert Reference Group (PERG). Diagnosis and treatment of chronic bacterial prostatitis and chronic prostatitis/chronic pelvic pain syndrome: A consensus guideline. BJU Int 2015, 116, 509–525. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Cai, T.; Alidjanov, J.; Palagin, I.; Medina-Polo, J.; Nickel, J.C.; Wagenlehner, F.M.E. Chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS): Look to the future. Prostate Cancer Prostatic Dis 2024, 27, 239–241. [Google Scholar] [CrossRef] [PubMed]
- He, H.; Luo, H.; Xu, H.; Qian, B.; Zou, X.; Zhang, G.; Zeng, F.; Zou, J. Preclinical models and evaluation criteria of prostatitis. Front Immunol 2023, 14, 1183895. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kranz, J.; Bartoletti, R.; Bruyère, F.; Cai, T.; Geerlings, S. , Köves, B.; Schubert, S.; Pilatz, A.; Veeratterapillay, R.; Wagenlehner, F.M.E.; Bausch, K.; Devlies, W.; Horváth, J.; Leitner, L.; Mantica, G.; Mezei, T.; Smith, E.J.; Bonkat, G. European Association of Urology Guidelines on Urological Infections: Summary of the 2024 Guidelines. Eur Urol 2024, 86, 27–41. [Google Scholar] [CrossRef] [PubMed]
- Cai, T.; Gallelli, L.; Cione, E.; Perletti, G.; Ciarleglio, F.; Malossini, G.; De Pretis, G.; Palmieri, A.; Mirone, V.; Bartoletti, R.; Johansen, T.E.B. The use of Lactobacillus casei DG® prevents symptomatic episodes and reduces the antibiotic use in patients affected by chronic bacterial prostatitis: Results from a phase IV study. World J Urol 2021, 39, 3433–3440. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Badia, X.; Garcia-Losa, M.; Dal-Re, R. Ten-language translation and harmonization of the International Prostate Symptom Score: Developing a methodology for multinational clinical trials. Eur Urol 1997, 31, 129–140. [Google Scholar] [CrossRef]
- Giubilei, G.; Mondaini, N.; Crisci, A.; Raugei, A.; Lombardi, G.; Travaglini, F.; Del Popolo, G.; Bartoletti, R. The Italian version of the National Institutes of Health Chronic Prostatitis Symptom Index. Eur Urol 2005, 47, 805–811. [Google Scholar] [CrossRef]
- Cappelleri, J.C.; Rosen, R.C.; Smith, M.D.; Mishra, A.; Osterloh, I.H. Diagnostic evaluation of the erectile function domain of the International Index of Erectile Function. Urology 1999, 54, 346–351. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Qu, B.; Lun, S.S.; Guo, Y.; Liu, J. The 36-item short form health survey: Reliability and validity in Chinese medical students. Int J Med Sci 2012, 9, 521–526. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Laucis, N.C.; Hays, R.D.; Bhattacharyya, T. Scoring the SF-36 in Orthopaedics: A Brief Guide. J Bone Joint Surg Am 2015, 97, 97,1628–34. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Dunstan, D.A.; Scott, N. Norms for Zung's Self-rating Anxiety Scale. BMC Psychiatry 2020, 20, 90. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Dunstan, D.A.; Scott, N. Clarification of the cut-off score for Zung's self-rating depression scale. BMC Psychiatry 2019, 19, 177. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Cai, T.; Tamanini, I.; Odorizzi, K.; Gallelli, L.; Lanzafame, M.; Mazzoli, S.; Lanzafame, P.; Massidda, O.; Palmieri, A.; Wagenlehner, F.M.E.; Bjerklund Johansen, T.E.; De Nunzio, C. The diagnostic yield of the Meares & Stamey test can be significantly improved by symptom-based patient selection and the experience of the test performer. Prostate Cancer Prostatic Dis 2024, 27, 300–304. [Google Scholar] [CrossRef] [PubMed]
- Cossart, Y. Bergey’s Manual of Systematic Bacteriology Volume 2. Pathology 1987, 19, 324; Holt, J.G.; Krieg, N.R.; Sneath, P.H.A. Bergey’s Manual of Determinative Bacterology; The Williams and Wilkins Co.: Baltimore, MD, USA, 1994.
- Krieger, J.N.; Lee, S.W.; Jeon, J.; Cheah, P.Y.; Liong, M.L.; Riley, D.E. Epidemiology of prostatitis. Int J Antimicrob Agents 2008, 31, S85–90. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Holt, J.D.; Garrett, W.A.; McCurry, T.K.; Teichman, J.M. Common Questions About Chronic Prostatitis. Am Fam Physician 2016, 93, 290–296. [Google Scholar] [PubMed]
- Bartoletti, R.; Cai, T.; Mondaini, N.; Dinelli, N.; Pinzi, N.; Pavone, C.; Gontero, P.; Gavazzi, A.; Giubilei, G.; Prezioso, D.; Mazzoli, S.; Boddi, V.; Naber, K.G.; Italian Prostatitis Study Group. Prevalence, incidence estimation, risk factors and characterization of chronic prostatitis/chronic pelvic pain syndrome in urological hospital outpatients in Italy: Results of a multicenter case-control observational study. J Urol discussion 2415. 2007, 178, 2411–2415. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Liang, C.; Shang, X.; Li, H. Chronic Prostatitis/Chronic Pelvic Pain Syndrome: A Disease or Symptom? Current Perspectives on Diagnosis, Treatment, and Prognosis. Am J Mens Health 2020, 14, 1557988320903200. [Google Scholar] [CrossRef] [PubMed]
- Murphy, S.F.; Schaeffer, A.J.; Thumbikat, P. Immune mediators of chronic pelvic pain syndrome. Nat Rev Urol 2014, 11, 259–269. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hou, D.S.; Long, W.M.; Shen, J.; Zhao, L.P.; Pang, X.Y.; Xu, C. Characterisation of the bacterial community in expressed prostatic secretions from patients with chronic prostatitis/chronic pelvic pain syndrome and infertile men: A preliminary investigation. Asian J Androl 2012, 14, 566–573. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Nickel, J.C.; Alexander, R.B.; Schaeffer, A.J.; Landis, J.R.; Knauss, J.S.; Propert, K.J.; Chronic Prostatitis Collaborative Research Network Study Group. Leukocytes and bacteria in men with chronic prostatitis/chronic pelvic pain syndrome compared to asymptomatic controls. J Urol 2003, 170, 818–822. [Google Scholar] [CrossRef] [PubMed]
- Magri, V.; Perletti, G.; Cai, T.; Stamatiou, K.; Trinchieri, A.; Montanari, E. Levofloxacin for NIH Category II Chronic Bacterial Prostatitis: A Real-Life Study. Chemotherapy 2019, 64, 8–16. [Google Scholar] [CrossRef] [PubMed]
- Isolauri, E.; Sütas, Y.; Kankaanpää, P.; Arvilommi, H.; Salminen, S. Probiotics: Effects on immunity. Am J Clin Nutr 2001, 73, 444S–450S. [Google Scholar] [CrossRef] [PubMed]
- Mohamadzadeh, M.; Olson, S.; Kalina, W.V.; Ruthel, G.; Demmin, G.L.; Warfield, K.L.; Bavari, S.; Klaenhammer, T.R. Lactobacilli activate human dendritic cells that skew T cells toward T helper 1 polarization. Proc Natl Acad Sci U S A 2005, 102, 2880–2885. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Löhr, J.M.; Dominguez-Munoz, E.; Rosendahl, J.; Besselink, M.; Mayerle, J.; Lerch, M.M.; Haas, S.; Akisik, F.; Kartalis, N.; Iglesias-Garcia, J.; Keller, J.; Boermeester, M.; Werner, J.; Dumonceau, J.M.; Fockens, P.; Drewes, A.; Ceyhan, G.; Lindkvist, B.; Drenth, J.; Ewald, N.; Hardt, P.; de Madaria, E.; Witt, H.; Schneider, A.; Manfredi, R.; Brøndum, F.J.; Rudolf, S.; Bollen, T.; Bruno, M.; HaPanEU/UEG Working Group. United European Gastroenterology evidence-based guidelines for the diagnosis and therapy of chronic pancreatitis (HaPanEU). United European Gastroenterol J 2017, 5, 153–199. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Aragón, I.M.; Herrera-Imbroda, B.; Queipo-Ortuño, M.I.; Castillo, E.; Del Moral, J.S.; Gómez-Millán, J.; Yucel, G.; Lara, M.F. The Urinary Tract Microbiome in Health and Disease. Eur Urol Focus 2018, 4, 128–138. [Google Scholar] [CrossRef] [PubMed]
- Arora, H.C.; Eng, C.; Shoskes, D.A. Gut microbiome and chronic prostatitis/chronic pelvic pain syndrome. Ann Transl Med 2017, 5, 30. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Vicari, E.; La Vignera, S.; Castiglione, R.; Condorelli, R.A.; Vicari, L.O.; Calogero, A.E. Chronic Bacterial Prostatitis and Irritable Bowel Syndrome: Effectiveness of Treatment With Rifaximin Followed by the Probiotic VSL#3. Asian J Androl 2014, 16, 735–739. [Google Scholar]
- Chen, J.; Chen, J.; Fang, Y.; Shen, Q.; Zhao, K.; Liu, C.; Zhang, H. Microbiology and immune mechanisms associated with male infertility. Front Immunol 2023, 14, 1139450. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Šutulović, N.; Vesković, M.; Puškaš, N.; Zubelić, A.; Jerotić, D.; Šuvakov, S.; Despotović, S.; Grubač, Ž.; Mladenović, D.; Macut, D.; Rašić-Marković, A.; Simić, T.; Stanojlović, O.; Hrnčić, D. Chronic Prostatitis/Chronic Pelvic Pain Syndrome Induces Depression-Like Behavior and Learning-Memory Impairment: A Possible Link with Decreased Hippocampal Neurogenesis and Astrocyte Activation. Oxid Med Cell Longev 2023, 2023, 3199988. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
Figure 1.
Gut microbiota analysis during the study in probiotic group. T0: admission; T1: 1 month from T0; T2: 3 months from T0; T3: 6 months from T0. **P<0.01 increase (T1vsT0; T2vsT1; T3vsT2).
Figure 1.
Gut microbiota analysis during the study in probiotic group. T0: admission; T1: 1 month from T0; T2: 3 months from T0; T3: 6 months from T0. **P<0.01 increase (T1vsT0; T2vsT1; T3vsT2).
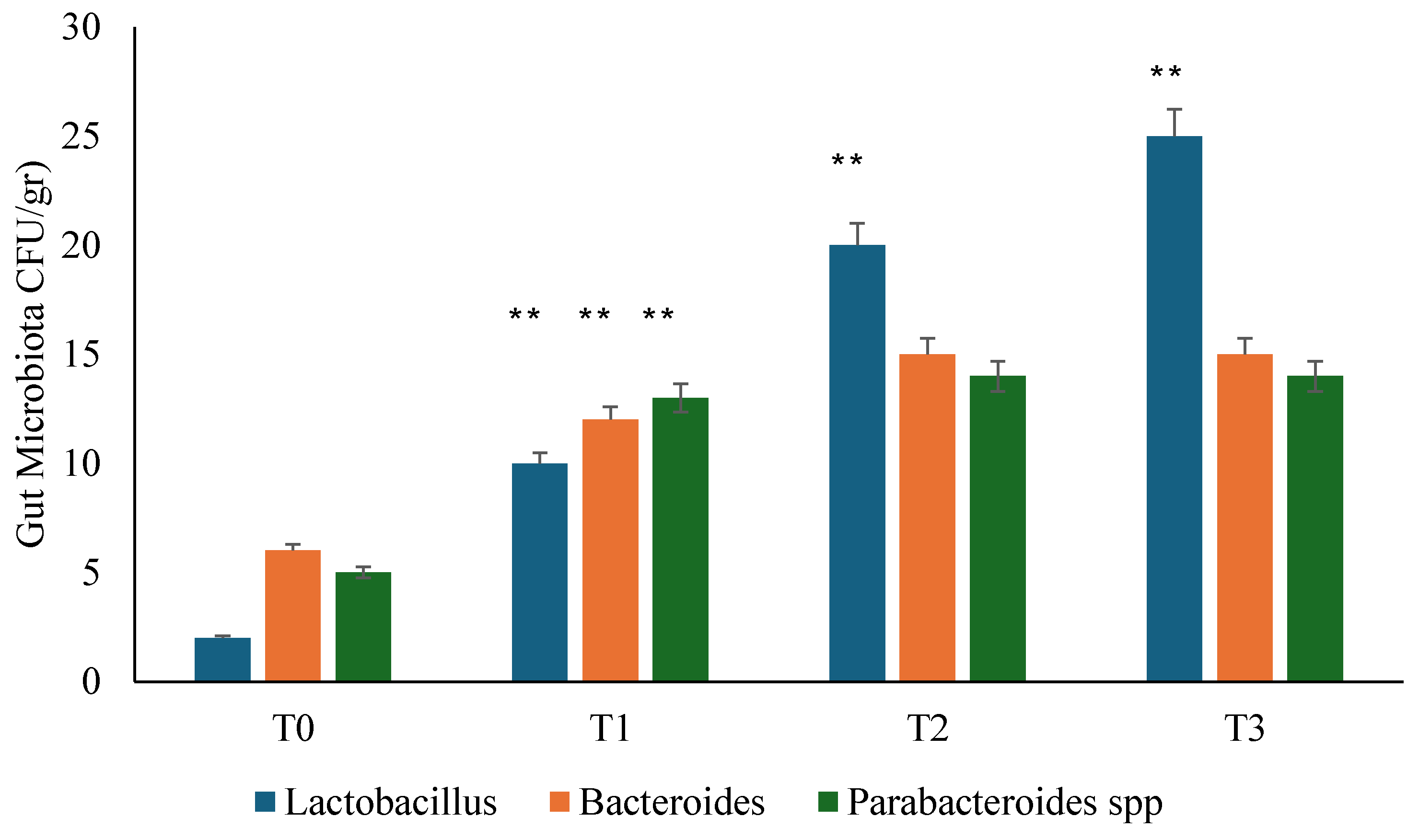
Figure 2.
Gut microbiota analysis during follows up in placebo group. T0: admission; T1: 1 month from T0; T2: 3 months from T0; T3: 6 months from T0. **P<0.01 increase (T1vsT0; T2vsT1; T3vsT2).
Figure 2.
Gut microbiota analysis during follows up in placebo group. T0: admission; T1: 1 month from T0; T2: 3 months from T0; T3: 6 months from T0. **P<0.01 increase (T1vsT0; T2vsT1; T3vsT2).
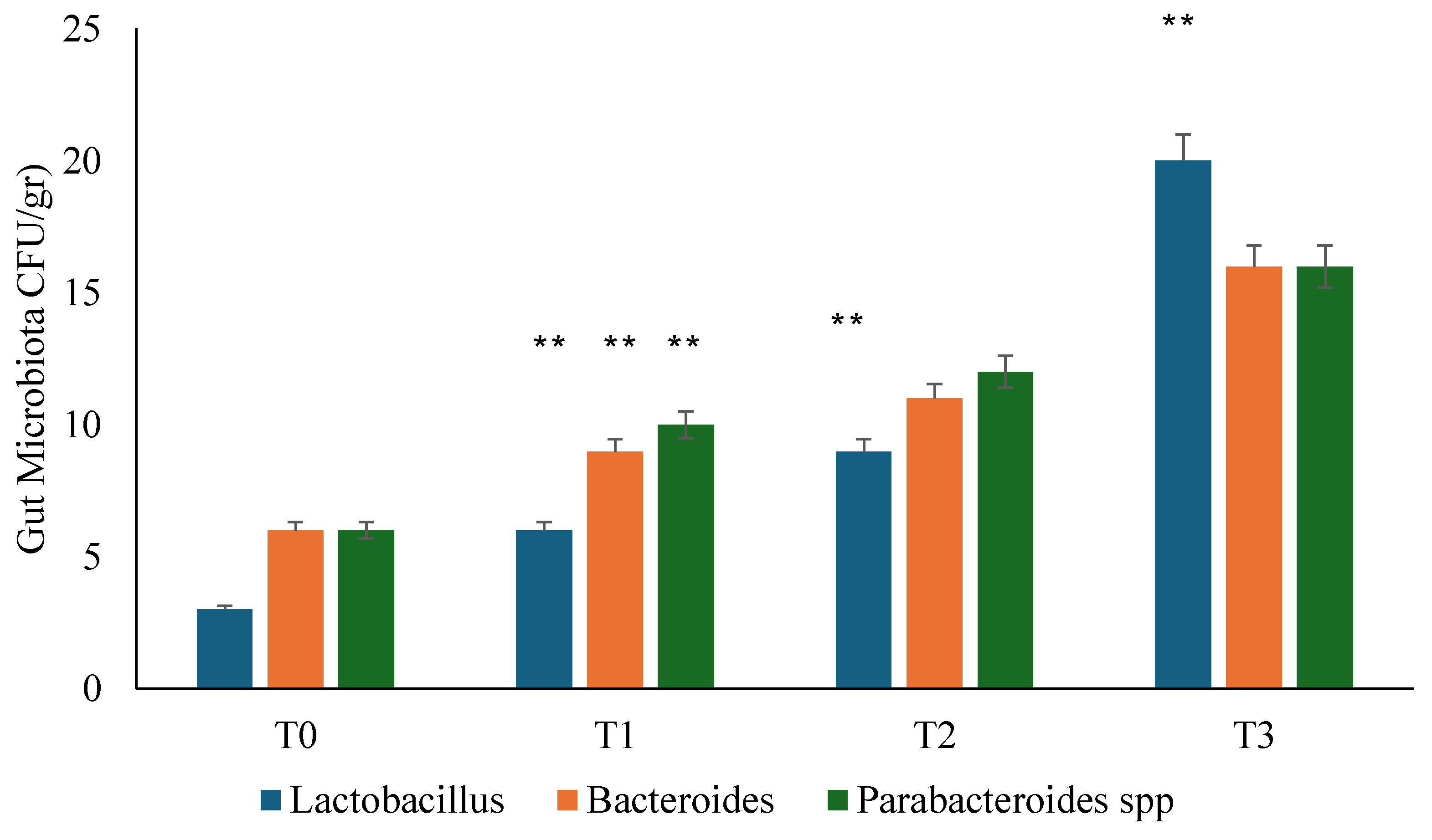
Figure 3.
Seminal microbiota analysis was performed during follow-up in the probiotic group. T0: admission; T1: 1 month from T0; T2: 3 months from T0; T3: 6 months from T0. **P<0.01 increase (T1vsT0; T2vsT1; T3vsT2); ++P<0.01decrease (T1vsT0).
Figure 3.
Seminal microbiota analysis was performed during follow-up in the probiotic group. T0: admission; T1: 1 month from T0; T2: 3 months from T0; T3: 6 months from T0. **P<0.01 increase (T1vsT0; T2vsT1; T3vsT2); ++P<0.01decrease (T1vsT0).
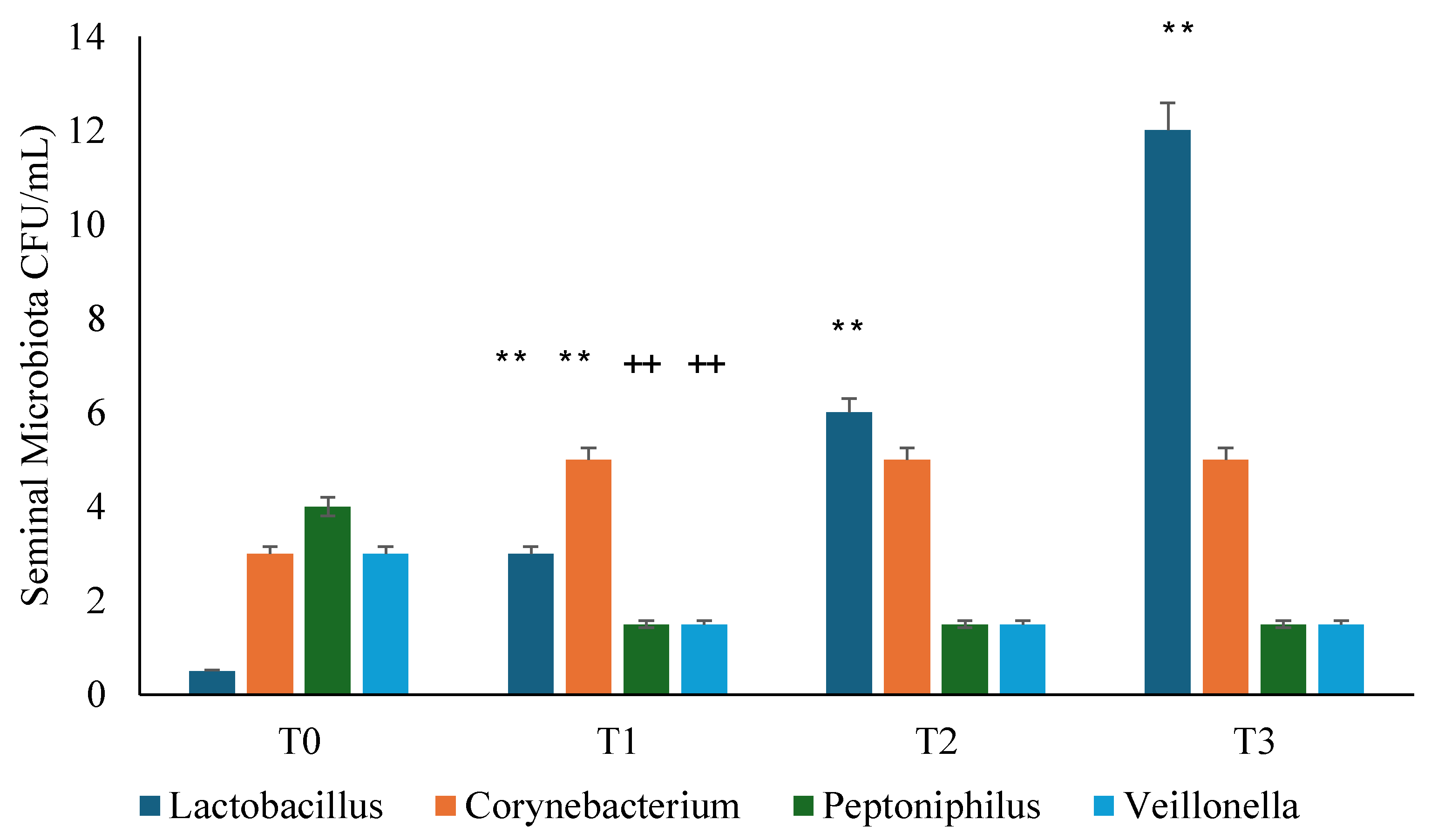
Figure 4.
Seminal microbiota analysis during the study in placebo group. T0: admission; T1: 1 month from T0; T2: 3 months from T0; T3: 6 months from T0. **P<0.01 increase (T1vsT0; T2vsT1; T3vsT2); ++P<0.01decrease (T1vsT0; T2vsT1).
Figure 4.
Seminal microbiota analysis during the study in placebo group. T0: admission; T1: 1 month from T0; T2: 3 months from T0; T3: 6 months from T0. **P<0.01 increase (T1vsT0; T2vsT1; T3vsT2); ++P<0.01decrease (T1vsT0; T2vsT1).
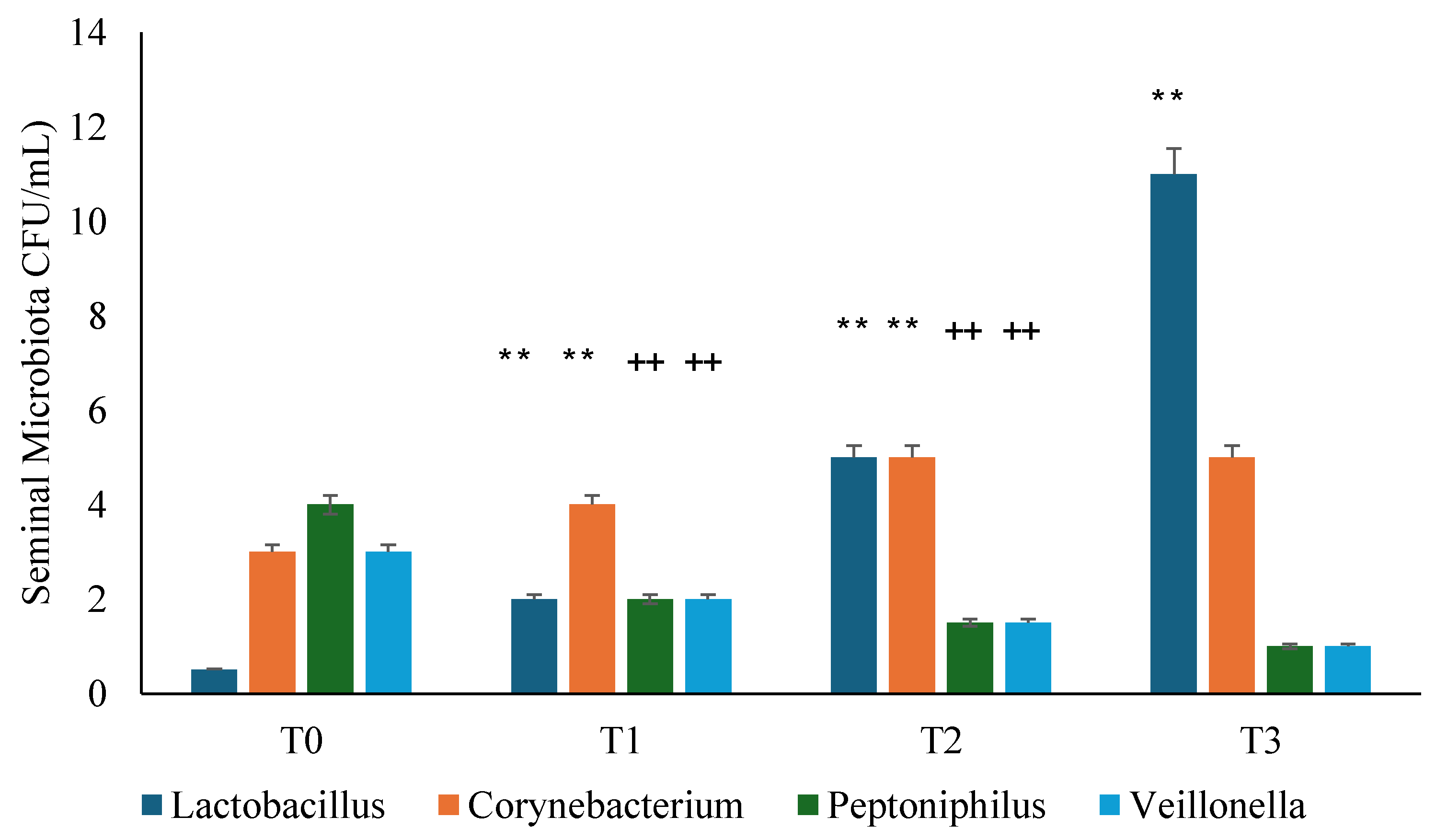
Figure 5.
NIH-CPSI analysis during follow ups in placebo and probiotic groups. Data are expressed as mean ± standard deviation. **P<0.01 vs T0.
Figure 5.
NIH-CPSI analysis during follow ups in placebo and probiotic groups. Data are expressed as mean ± standard deviation. **P<0.01 vs T0.
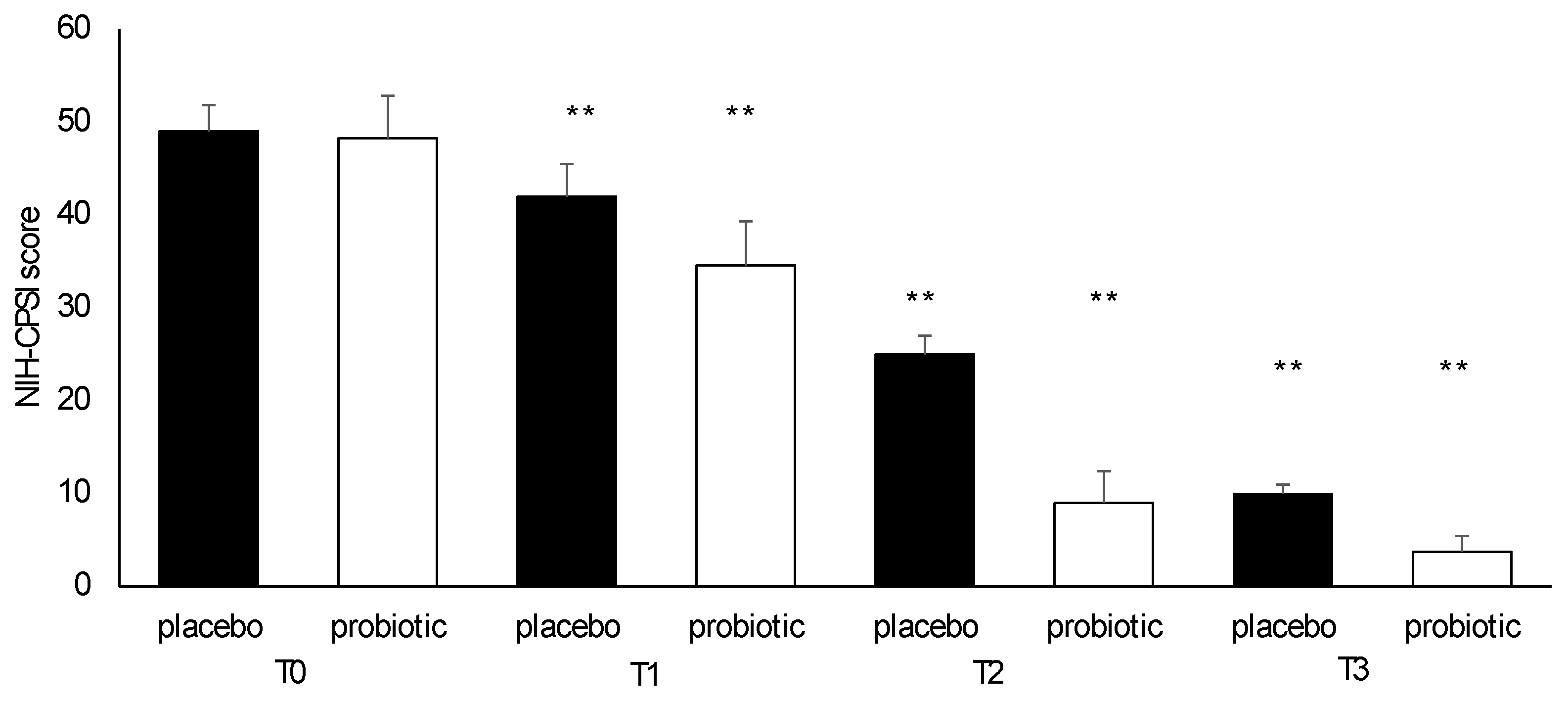
Figure 6.
IPSS analysis during follow ups in placebo and probiotic groups. Data are expressed as mean ± standard deviation. **P<0.01 vs T0.
Figure 6.
IPSS analysis during follow ups in placebo and probiotic groups. Data are expressed as mean ± standard deviation. **P<0.01 vs T0.
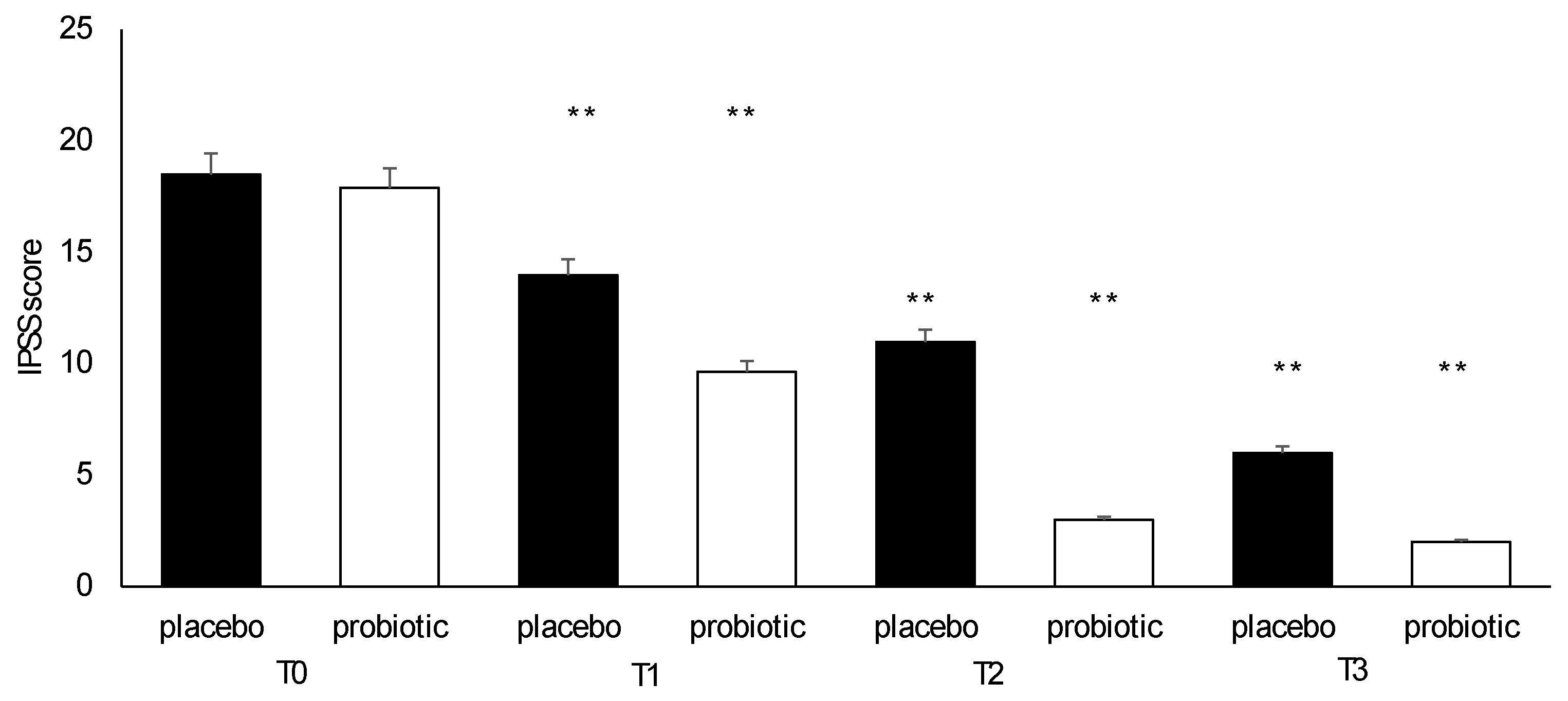
Figure 7.
SF-36 analysis during follow ups in placebo and probiotic groups. Data are expressed as mean ± standard deviation. *P<0.01 vs T0.
Figure 7.
SF-36 analysis during follow ups in placebo and probiotic groups. Data are expressed as mean ± standard deviation. *P<0.01 vs T0.
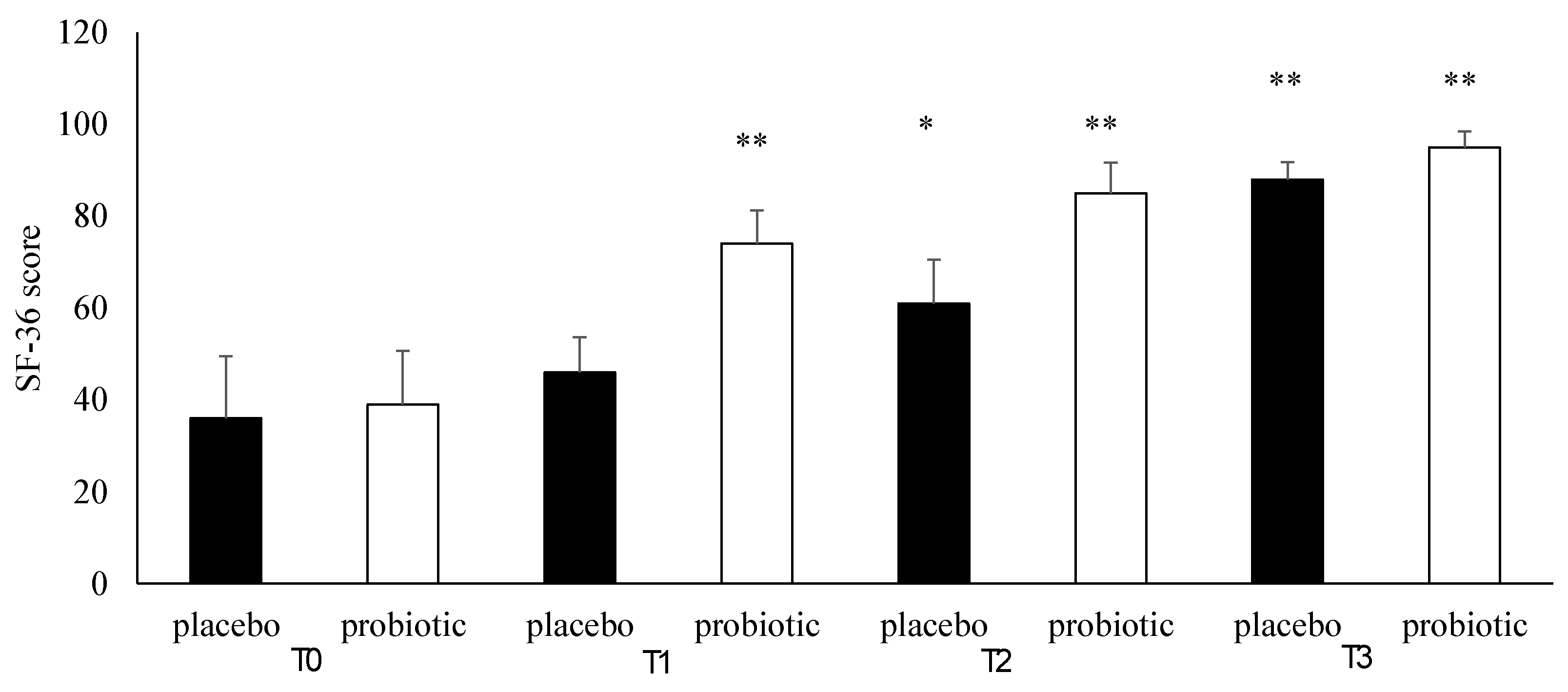
Figure 8.
Zung SAS analysis during follow ups in placebo and probiotic groups. Data are expressed as mean ± standard deviation. *P<0.01.
Figure 8.
Zung SAS analysis during follow ups in placebo and probiotic groups. Data are expressed as mean ± standard deviation. *P<0.01.
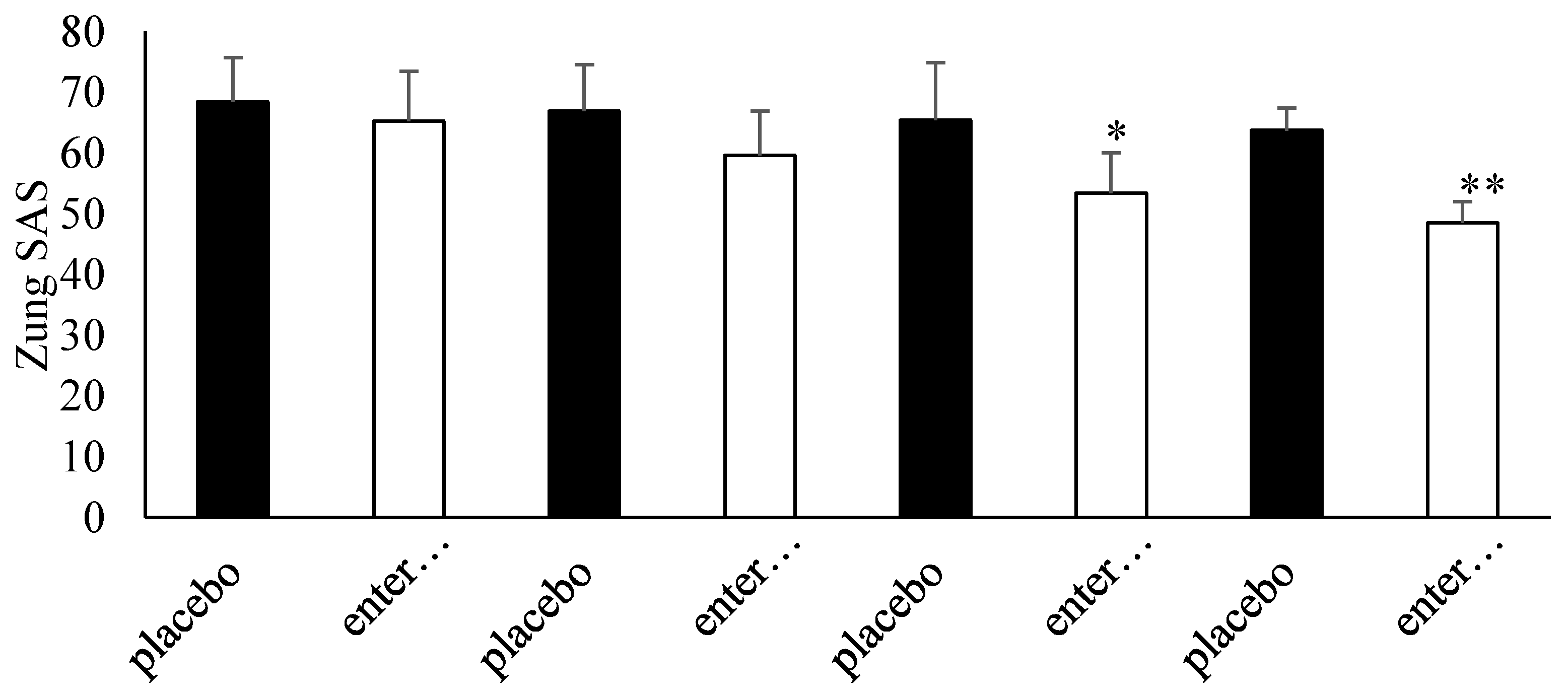
Figure 9.
Zung SDS analysis during follow ups in placebo and probiotic groups. Data are expressed as mean ± standard deviation. *P<0.01 vs T0.
Figure 9.
Zung SDS analysis during follow ups in placebo and probiotic groups. Data are expressed as mean ± standard deviation. *P<0.01 vs T0.
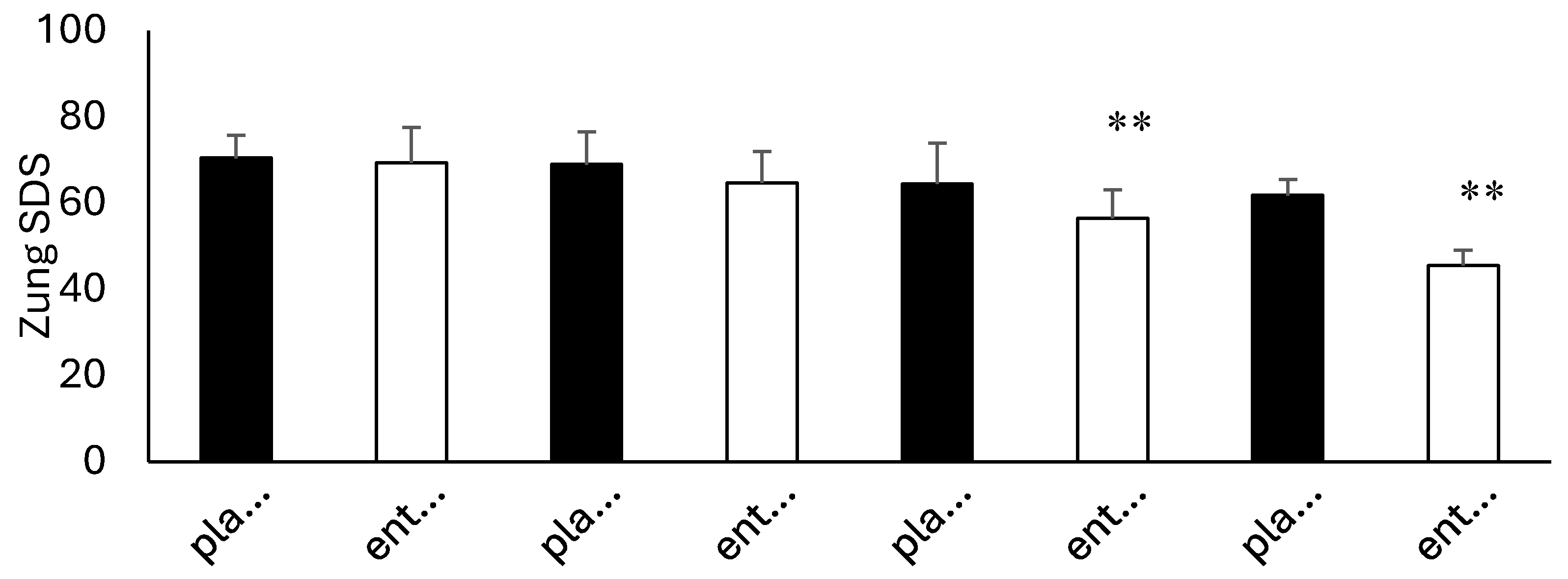

Table 1.
Demographics and Clinical characteristics of 24 enrolled patients. Data are expressed as mean ± standard deviation or as number (percentages).
Table 1.
Demographics and Clinical characteristics of 24 enrolled patients. Data are expressed as mean ± standard deviation or as number (percentages).
| Characteristics | Data | Probiotic Group | Placebo Group |
|---|---|---|---|
| Age | 50 ± 3.1 | 50.4 ± 2.5 | 49.7 ± 3.4 |
| Body Mass Index (Kg/m2) | 27.7 ± 2.7 | 28.0 ± 2.5 | 27.4 ± 2.7 |
| Occupation Status | |||
| Sedentary | 11 | 4 | 7 |
| Manual | 13 | 8 | 5 |
| Comorbidity | |||
| Copd | 3 | 2 | 1 |
| Diabetes Mellitus Type 2 | 6 | 3 | 3 |
| Hypertension | 8 | 1 | 7 |
| Dyslipidemia | 4 | 4 | 0 |
| Metabolic Syndrome | 3 | 2 | 1 |
Table 2.
QIAstat-Dx® Gastrointestinal Panel evaluation. Data are expressed as total cycle for each run. Data lower than 29 represents positive values; data from 32 to 39 require a clinical evaluation.
Table 2.
QIAstat-Dx® Gastrointestinal Panel evaluation. Data are expressed as total cycle for each run. Data lower than 29 represents positive values; data from 32 to 39 require a clinical evaluation.
| Bacteria | T0 | T1 | T2 | T3 |
|---|---|---|---|---|
| Escherichia coli | 36 | 34 | 38 | 36 |
| C. difficile | 51 | 49 | 52 | 54 |
| Campylobacter spp. (C. jejuni, C. upsaliensis, and C. coli) | 59 | 53 | 54 | 56 |
| Clostridioides difficile tcdA/tcdB | 51 | 52 | 51 | 54 |
| Enteroaggregative E. coli | 56 | 58 | 59 | 59 |
| Enteropathogenic E. coli | 57 | 58 | 59 | 58 |
| Enterotoxigenic E. coli eltA/estA | 61 | 62 | 59 | 62 |
| Shiga toxin–producing E. coli stx1/stx2 | 59 | 62 | 61 | 58 |
| Shiga toxin–producing E. coli stx1/stx2 O157 | 56 | 58 | 59 | 61 |
| enteroinvasive E. coli /Shigella (S. sonnei, S. fexneri, S. boydii, and S. dysenteriae) | 61 | 62 | 64 | 62 |
| Plesiomonas shigelloides | 59 | 60 | 58 | 59 |
| Salmonella spp. | 63 | 64 | 61 | 62 |
Table 3.
IIEF-5 score achieved at admission (T0) and at T3 in placebo and probiotic groups (normal range 0-25).
Table 3.
IIEF-5 score achieved at admission (T0) and at T3 in placebo and probiotic groups (normal range 0-25).
| Symptoms | ||||
| IIEF-5 (range: 0–25 points) | Groups at T0 | Groups at T3 | ||
| Probiotic | Placebo | Probiotic | Placebo | |
| Normal (IIEF-5 22–25 points) | 1 | 2 | 4 | 2 |
| Mild (IIEF-5 17–21 points) | 5 | 5 | 7 | 6 |
| Mild to moderate (IIEF 12–16 points) | 3 | 1 | 1 | 2 |
| Moderate to severe (IIEF 8–11 points) | 1 | 2 | 0 | 1 |
| Severe (IIEF-5 0–7 points) | 2 | 2 | 0 | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



