
Submitted:
18 October 2024
Posted:
18 October 2024
You are already at the latest version
Abstract
Recurrent laryngeal nerve palsy remains a significant complication following minimally invasive esophagectomy for esophageal cancer. Despite advancements in surgical techniques and lymphadenectomy precision, the incidence of recurrent laryngeal nerve palsy has not been improved. Recurrent laryngeal nerve palsy predominantly affects the left side and may lead to unilateral or bilateral vocal cord paralysis, resulting in hoarseness, dysphagia, and an increased risk of aspiration pneumonia. While most cases of recurrent laryngeal nerve palsy are temporary and resolve within 6 to 12 months, some patients may result in permanent nerve dysfunction, severely impacting patient quality of life.
Prevention strategies, such as nerve integrity monitoring, robotic-assisted minimally invasive esophagectomy, and advanced dissection techniques, aim to minimize nerve injury, though their effectiveness varies. Management of recurrent laryngeal nerve palsy includes voice and swallowing rehabilitation, reinnervation techniques, and, in severe cases, surgical interventions such as thyroplasty and intracordal injection. As recurrent laryngeal nerve palsy can lead to significant postoperative respiratory complications, a multidisciplinary approach involving surgical precision, early detection, and comprehensive rehabilitation is crucial to improving patient outcomes and minimizing long-term morbidity in minimally invasive esophagectomy.
Keywords:
esophageal cancer
; minimally invasive esophagectomy
; recurrent laryngeal nerve
1. Introduction
Lymph node dissection around the recurrent laryngeal nerve (RLN) is a critical component of esophageal cancer surgery, especially in thoracic esophageal carcinoma, where metastasis to the lymph nodes around RLN is frequently observed. The incidence of this RLN lymph node metastasis in thoracic esophageal cancer is reported to be between 30% and 50% [1,2,3,4]. Although RLN lymph node metastasis is associated with poorer overall survival compared to cases without nodal involvement [3,4,5], comprehensive RLN lymphadenectomy has demonstrated efficacy in improving survival outcomes and reducing local recurrence [6,7]. However, this procedure is technically challenging due to the close proximity of the RLN, increasing the risk of nerve injury, which can lead to vocal cord paralysis and aspiration.
Recent advances in minimally invasive surgery for esophageal cancer (MIE) have improved the precision of lymphadenectomy, including the dissection of RLN lymph nodes, as evidenced by a study showing a significant increase in the number of RLN lymph nodes retrieved compared to traditional open approaches [8,9,10]. Also, the enhanced visualization provided by thoracoscopic techniques allows for more precise dissection while reducing tissue trauma around the RLN, minimizing the risk of RLN palsy. However, despite these advancements in surgical precision, the incidence of postoperative RLN palsy has not significantly decreased between minimally invasive and open surgical approaches, suggesting that while MIE improves lymphadenectomy accuracy, it does not necessarily mitigate the risk of nerve damage [9,10,11]. This can be attributed to several factors. First, the complexity of lymph node dissection around the RLN remains challenging, regardless of the surgical approach. Second, the prolonged operative time of MIE may increase the risk of RLN injury. Furthermore, the improved visualization provided by MIE, which allows for better identification of the RLN, may encourage more aggressive lymph node dissection in this region compared to open thoracotomy, inadvertently raising the risk of nerve damage. As a result, RLN palsy rates remain similar between MIE and open procedures, emphasizing the need for refined surgical techniques and post-operative management to reduce RLN palsy and fatal complication. Given those consideration, this review will address the ongoing issue of RLN palsy in MIE, discussing current strategies and management to improve surgical outcomes and patient quality of life.
2. Risk
Reported incidences of RLN palsy in MIE vary widely, with several studies documenting rates between 11% and 88% with variations depending on the type of surgery, definition of RLN palsy and patient population. [9,10,12,13,14]. Although it usually occurs unilaterally, mostly on the left side, 1.7-15.9% of cases were bilaterally [1,12,14,15]. The left RLN is longer compared to the right side, which requires a longer dissection distance, making it more prone to palsy. Additionally, since the approach to the thoracic cavity is usually from the right side, the esophagus tends to be retracted forward during dissection, causing significant flexion of the RLN via the esophageal branches, which can be one of the reasons for the RLN palsy. The McKeown procedure, which involves a three-field lymphadenectomy, is often associated with a higher risk of RLN injury due to extensive lymph node dissection around the RLN, while Ivor Lewis has lower incidence of RLN palsy [16,17]. This can be attributed not only to the omission of cervical lymph node dissection around RLN lymph node, but also to the fact that aggressive lymph node dissection around the RLN is generally not required in the patient for which this Ivor Lewis procedure is indicated. RLN palsy is also influenced by patient-specific anatomical factors. According to a study published, a narrower RLN is more susceptible to injury due to reduced resistance to traction and compression, as it offers less resistance to traction and compression [18]. Additionally, preoperative CT imaging reveals RLN anatomical variations and proximity to critical surgical areas, aiding in risk assessment and surgical planning [19].
The areas of upper mediastinal LN dissection are anatomically close to the RLN, and the presence of large tumor or lymph node metastasis in this area increases the risk of direct nerve trauma, traction injury, or thermal damage from electrocautery. The method of dissection, such as blunt dissection, influenced the risk of nerve damage due to stretching or compression [20]. Thermal damage is another significant risk, as the heat generated during hemostasis or tissue dissection can inadvertently affect the RLN, leading to nerve dysfunction [21]. Especially under a wet condition, the high temperature of steam from energy device can easily cause thermal damage and recommend steam safe distances of 3mm for ultrasonic device and 10mm for bipolar sealing device [21].
Most of the cases of RLN palsy results in temporally impairment which would recover within 6-12month [22,23]. However, permanent nerve dysfunction would happen if the nerve were completely transected or extensively damaged beyond its capacity for self-repair. Permanent RLN palsy occurs in approximately 4-13% of cases following esophagectomy [12,24], particularly when aggressive dissection is required near the nerve’s pathway [25]. If symptoms persist beyond six months to one year, the likelihood of complete recovery diminishes significantly [22,23] and further treatments, as described later, would be necessary.
3. Influence
In the early postoperative period, RLN palsy can lead to unilateral or bilateral vocal cord palsy, resulting in hoarseness, dysphagia and an impaired ability to cough effectively [12,14,24,25]. Hoarseness is one of the most common symptoms of RLN palsy which affect the movement of vocal code and impacts the patient’s ability to communicate. However, some cases do not cause hoarseness even RLN palsy had occurred. This is because the vocal cord on the unaffected side would compensatory move towards the affected side, allowing for glottic closure and vocalization. Therefore, RLN palsy cannot be accurately diagnosed just by the presence of hoarseness alone and needs laryngoscope for exact diagnosis. RLN palsy also causes compromises glottic closure by impairment of elevating hyoid bone [26] and results in dysphagia and ineffective cough. Dysphagia after esophagectomy makes oral intake difficult due to incomplete closure of the glottis and weakened swallowing function, leading to poor quantity of food intake and worsening quality of life [27]. Ineffective cough results in reduced intrathoracic pressure generation necessary for an effective cough reflex. This inability to close glottis can also cause impairment of airway protection, which may lead to aspiration and further lead to pneumonia. This aspiration pneumonia is one of the most common and serious postoperative complications caused by RLN palsy, prolonging hospital stay and increasing morbidity [12,28,29,30]. On the other hand, RLN palsy itself does not necessarily contribute to pneumonia-related mortality or overall survival [12,30,31,32]. Although further evaluation is needed, this indicates that RLN palsy would induce respiratory complication in the short-term but may not have significant impact on long-term prognosis.
4. Prevention
To prevent RLN palsy and ensure sufficient LN dissection around RLN, the most important consideration is to perform the dissection at the anatomically appropriate plane (Figure 1 and Figure 2). This does not mean isolating the RLN by digging this nerve out from the surrounding adipose tissue, but rather dissecting the mesentery-like tissue that contains the lymph nodes around the nerve [33]. Achieving this requires not only a thorough understanding of the relevant anatomy but also adhering to fundamental surgical techniques, such as minimizing bleeding to maintain a clear view of the anatomical structures, avoiding rough manipulation around the nerve, and refraining from the use of energy devices in close proximity to the nerve. Based on those principles, recent efforts have introduced various techniques to further reduce the risk of RLN injury such as the concept of maintain RLN anatomical position to avoid any stress on the RLN [34], use of mini-clips [35], magnetic anchoring [36] and elastic suspension of left RLN [37].
The use of Nerve Integrity Monitor (NIM) is also an effective method to reduce the incidence of RLN injury during esophagectomy. The principle of NIM involves the placement of electrodes on the vocal cords via an endotracheal tube, which detect electromyographic (EMG) signals from the vocal code. When the RLN is stimulated by electrical impulses during surgery, the resulting EMG activity provides real-time feedback on the nerve’s functional integrity, allowing for precise identification of RLN and avoid inadvertent nerve damage during surgery (Figure 3). Several studies have demonstrated that the usage of NIM significantly decreases the risk of RLN palsy compared to traditional surgical methods [38,39,40,41]. Furthermore, continuous NIM provides real-time feedback on RLN function by continuously assessing electromyographic signals from the vocal cords, providing immediate feedback on RLN function throughout the surgical procedure [42,43]. This real-time feedback alerts the surgeon to any impending nerve injury, enabling immediate corrective actions, such as adjusting surgical maneuvers, thus preventing permanent RLN damage. However, there are some limitations in this continuous NIM, such as the need for specialized equipment and extra surgical time to attach sensor to cervical vagal nerve before approaching to RLN.
Robot-assisted minimally invasive esophagectomy (RAMIE) has gained attention as a promising approach to reduce RLN palsy during esophageal cancer surgery. Using the robot, those enhanced dexterity, precision, and three-dimensional visualization offered by robotic systems are thought to facilitate meticulous dissection along the anatomical layers, potentially lowering the risk of RLN injury compared to conventional MIE [44,45]. However, the benefits of RAMIE in preventing RLN palsy are not universally accepted [46,47]. The reason for this may be due to the strong forces exerted by the use of the robot, which can result in more forceful retraction of the esophagus and increased flexion of the nerve, potentially contributing to RLN palsy. To demonstrate the effectiveness of RAMIE for RLN palsy, prospective, multicenter trials with standardized methodologies are essential.
As a new approach, the use of artificial intelligence (AI) in preventing RLN palsy during esophageal surgery has shown promising potential [48]. AI systems enhance RLN preservation by utilizing real-time image analysis and machine learning algorithms. However, there remain some issues including the need for large datasets for AI training and difficulties in integrating AI into clinical workflows.
5. Management
If the RLN has been severed or irreversibly damaged during surgery, reinnervation techniques are critical for restoring laryngeal function and improving patient outcomes. Although primary end-to-end anastomosis is desirable for RLN repair, usually both nerve stumps are not available. Laryngeal reinnervation using the ansa cervicalis nerve to the RLN can be performed even when the proximal RLN stump is not available, and this procedure has been shown to improve glottic closure, vocal quality, and reduce aspiration by redirecting motor inputs from the ansa cervicalis to the denervated laryngeal muscles [49,50]. This nerve anastomosis is performed using 7-0 or 8-0 polypropylene, and is typically carried out under a microscope by plastic surgeons. Although this technique does not fully restore normal nerve function, they significantly enhance laryngeal competence and voice quality compared to non-reinnervated cases.
When recurrent nerve palsy occurs, its treatment differs depending on whether it is bilateral or unilateral. Patient with bilateral RLN palsy has a narrow rima glottidis, impaired airway function and inspiratory dyspnoea. This complication can be fatal especially in postoperative esophageal cancer patients due to high sputum production by thoracic procedure and longer operation time and often leading to life threatening respiratory distress. Although about two third of patients with bilateral RLN palsy could avoid tracheostomy according to previous reports [12,14,15], this tracheotomy should not be delayed in order to avoid fatal complications, as the tracheal tube can be removed once the patient's condition improves. In the case which bilateral RLN palsy lasted for long without severe complication but glottic stenosis had not improved, laser cordotomy can be considered [51]. Although this procedure may improve airway patency, consultation with an ENT specialist is essential to determine the appropriate indication.
When RLN palsy occurred unilaterally, or bilaterally but without any respiratory distress, the following management would contribute to patient recovery. Rehabilitation is a critical component in the management of RLN palsy, aiming to restore vocal function, improve swallowing, and enhance overall quality of life. Voice therapy targeted exercises that strengthen the laryngeal muscles, improve glottic closure, and enhance breath support during phonation [52,53]. Swallowing rehabilitation is also crucial for patients with RLN palsy who experience dysphagia and aspiration risk. Swallowing therapy often includes exercises that strengthen the muscles, improve airway protection, and facilitate bolus clearance [54,55]. In addition to those rehabilitation, combination with neuromuscular electrical stimulation targeting the pharyngeal muscles demonstrated certain efficacy in preventing aspiration in stroke patients [56,57]. Although further investigation is needed to establish its effectiveness in the condition of RLN palsy, this technique may hold potential for preventing aspiration in those RLN palsy patients.
Usually, the RLN palsy improves within a few months, and if aspiration can be prevented during this period through rehabilitation, the problem is solved. However, if the RLN palsy does not improve and aspiration continues, surgical intervention, such as intracordal injection, thyroplasty and arytenoid adduction, would be the next treatment options [58,59]. Intracordal injection involves injecting materials such as autologous fat, collagen, or synthetic fillers into the paralyzed vocal fold to improve glottic closure and voice quality [58,59,60,61]. This procedure is minimally invasive and can be performed under local anesthesia. However, multiple intervention may be necessary to maintain the effect as the injected material can be reabsorbed over time. Thyroplasty, specifically Type I thyroplasty, involves implanting a silicone or other synthetic material medially within the thyroid cartilage to reposition the paralyzed vocal fold [58,59]. This procedure is designed to provide a permanent improvement in voice quality and glottic closure. It is highly effective in patients with unilateral vocal cord palsy, as it restores vocal fold tension and improves voice projection. Arytenoid adduction is a more complex surgical approach that repositions the arytenoid cartilage to improve glottic closure by mimicking the normal position of the vocal fold during phonation [59,62]. This technique is particularly beneficial when there is significant posterior glottic gap that cannot be adequately addressed by thyroplasty alone.
If aspiration pneumonia is repeated despite these efforts, laryngotracheal separation, specifically the Lindeman procedure [63], may be necessary to prevent aspiration by separating the larynx from the trachea. In recent years, various innovations have been added to this technique and have demonstrated improved safety profiles and reduced complications, making them valuable alternatives to the traditional Lindeman procedure [64,65]. However, speech function is permanently lost even with these technological advances. To avoid this situation which has a significant impact on quality of life, it is necessary to place emphasis on preventing severe RLN injury during surgery.
6. Conclusions
RLN palsy remains a significant challenge in MIE, with varying incidence rates depending on surgical techniques and patient factors. While RLN palsy can lead to complications such as vocal cord dysfunction, dysphagia, and respiratory issues, its impact on long-term survival is uncertain. Preventive measures like NIM and RAIMIE might be useful, but further validation is needed. Management strategies, including rehabilitation and surgical interventions, aim to restore function and improve outcomes. Future research efforts should focus on refining preventive measures and optimizing therapeutic interventions to mitigate the impact of RLN palsy on patient quality of life following esophagectomy.
Funding
This research received no external funding.
Conflicts of Interest
All the authors of this manuscript have no potential conflicts of interest to disclose.
References
- Ninomiya, I.; Osugi, H.; Fujimura, T.; Fushida, S.; Okamoto, K.; Maruzen, S.; Oyama, K.; Kinoshita, J.; Tsukada, T.; Kitagawa, H.; Takamura, H.; Nakagawara, H.; Tajima, H.; Hayashi, H.; Makino, I.; Ohta, T. Thoracoscopic esophagectomy with extended lymph node dissection in the left lateral position: technical feasibility and oncologic outcomes. 2014 Dis Esophagus. 2014, 27,159-167.
- Jang, H.J.; Lee, H.S.; Kim, M.S.; Lee, J.M.; Zo, J.I. Patterns of lymph node metastasis and survival for upper esophageal squamous cell carcinoma. Ann Thorac Surg. 2011, 92, 1091-1097.
- Kanemura, T.; Makino, T.; Miyazaki, Y.; Takahashi, T.; Kurokawa, Y.; Yamasaki, M.; Nakajima, K.; Takiguchi, S.; Mori, M.; Doki, Y. Distribution patterns of metastases in recurrent laryngeal nerve lymph nodes in patients with squamous cell esophageal cancer. Dis Esophagus. 2017, 30, 1-7.
- Taniyama, Y.; Nakamura, T.; Mitamura, A.; Teshima, J.; Katsura, K.; Abe, S.; Nakano, T.; Kamei, T.; Miyata, G.; Ouchi, N. A strategy for supraclavicular lymph node dissection using recurrent laryngeal nerve lymph node status in thoracic esophageal squamous cell carcinoma. Ann Thorac Surg. 2013, 95, 1930-1937.
- Wu, J.; Chen, Q.X.; Zhou, X.M.; Mao, W.M.; Krasna, M.J. Does recurrent laryngeal nerve lymph node metastasis really affect the prognosis in node-positive patients with squamous cell carcinoma of the middle thoracic esophagus? BMC Surg. 2014, 12, 14:43.
- Hong, T.H.; Kim, H.K.; Lee, G.; Shin, S.; Cho, J.H.; Choi, Y.S.; Zo, J.I.; Shim, Y.M. Role of recurrent laryngeal nerve lymph node dissection in surgery of early-stage esophageal squamous cell carcinoma. Ann Surg Oncol. 2022, 29, 627-639.
- Xu, S.; Chen, D.; Liu, Z.; Song, P.; Zheng, Y.; Xue, X.; Sang, Y.; Li, Z.; Chen, Y. Impact of the extent of recurrent laryngeal nerve lymphadenectomy on thoracic esophageal squamous cell carcinoma: a real-world multicentre study. Eur J Cardiothorac Surg. 2023, 63. ezad168.
- Liu, F.; Yang, W.; Yang, W.; Xu, R.; Chen, L.; He, Y.; Liu, Z.; Zhou, F.; Hou, B.; Zhang, L.; Zhang, L.; Zhang, F.; Cai, F.; Xu, H.; Lin, M.; Liu, M.; Pan, Y.; Liu, Y.; Hu, Z.; Chen, H.; He, Z.; Ke, Y. Minimally invasive or open esophagectomy for treatment of resectable esophageal squamous cell carcinoma? Answer from a real-world multicenter study. Ann Surg. 2023, 277, e777-e784.
- Mao, Y.; Gao, S.; Li, Y.; Chen, C.; Hao, A.; Wang, Q.; Tan, L.; Ma, J.; Xiao, G.; Fu, X.; Fang, W.; Li, Z.; Han, Y.; Chen, K.; Zhang, R.; Li, X.; Rong, T.; Fu, J.; Liu, Y.; Mao, W.; Xu, M.; Liu, S.; Yu, Z.; Zhang, Z.; Fang, Y.; Fu, D.; Wei, X.; Yuan, L.; Muhammad, S.; He, J. Minimally invasive versus open esophagectomy for resectable thoracic esophageal cancer (NST 1502): a multicenter prospective cohort study. J Natl Cancer Cent. 2023, 3, 106-114.
- Na, K.J.; Kang, C.H.; Park, S.; Park, I.K.; Kim, Y.T. Robotic esophagectomy versus open esophagectomy in esophageal squamous cell carcinoma: a propensity-score matched analysis. J Robot Surg. 2022, 16, 841-848.
- Takeuchi, H.; Miyata, H.; Ozawa, S.; Udagawa, H.; Osugi, H.; Matsubara, H.; Konno, H.; Seto, Y.; Kitagawa, Y. Comparison of short-term outcomes between open and minimally invasive esophagectomy for esophageal cancer using a nationwide database in Japan. Ann Surg Oncol. 2017, 24, 1821-1827.
- Taniyama, Y.; Miyata, G.; Kamei, T.; Nakano, T.; Abe, S.; Katsura, K.; Sakurai, T.; Teshima, J.; Hikage, M.; Ohuchi, N. Complications following recurrent laryngeal nerve lymph node dissection in esophageal cancer surgery. Interact Cardiovasc Thorac Surg. 2015, 20, 41-46.
- Li, Z.G.; Zhang, X.B.; Wen, Y.W.; Liu, Y.H.; Chao, Y.K. Incidence and predictors of unsuspected recurrent laryngeal nerve lymph node metastases after neoadjuvant chemoradiotherapy in patients with esophageal squamous cell carcinoma. World J Surg. 2018, 42, 2485-2492.
- Lee, J.O.; Yun, J.K.; Jeong, Y.H.; Lee, Y.S.; Kim, Y.H. Management for recurrent laryngeal nerve paralysis following oesophagectomy for oesophageal cancer: thoracic surgeon perspective. J Thorac Dis. 2024, 16, 3805-3817.
- Jeon, Y.J.; Cho, J.H.; Lee, H.K.; Kim, H.K.; Choi, Y.S.; Zo, J.I.; Shim, Y.M. Management of patients with bilateral recurrent laryngeal nerve paralysis following esophagectomy. Thorac Cancer. 2021, 12, 1851-1856.
- Van Workum, F.; Berkelmans, G.H.; Klarenbeek, B.R.; Nieuwenhuijzen, G.A.P.; Luyer, M.D.P.; Rosman, C. McKeown or Ivor Lewis totally minimally invasive esophagectomy for cancer of the esophagus and gastroesophageal junction: systematic review and meta-analysis. J Thorac Dis. 2017, 9, S826-S833.
- Wang, J.; Hu, J.; Zhu, D.; Wang, K.; Gao, C.; Shan, T.; Yang, Y. McKeown or Ivor Lewis minimally invasive esophagectomy: a systematic review and meta-analysis. Transl Cancer Res. 2020, 9, 1518-1527.
- Saito, Y.; Takeuchi, H.; Fukuda, K.; Suda, K.; Nakamura, R.; Wada, N.; Kawakubo, H.; Kitagawa, Y. Size of recurrent laryngeal nerve as a new risk factor for postoperative vocal cord paralysis. Dis Esophagus. 2018, 31, 1-8.
- Ohi, M.; Toiyama, Y.; Yasuda, H.; Ichikawa, T.; Imaoka, H.; Okugawa, Y.; Fujikawa, H.; Okita, Y.; Yokoe, T.; Hiro, J.; Kusunoki, M. Preoperative computed tomography predicts the risk of recurrent laryngeal nerve paralysis in patients with esophageal cancer undergoing thoracoscopic esophagectomy in the prone position. Esophagus. 2021, 18, 228-238.
- Liu, N.; Chen, B.; Li, L.; Zeng, Q.; Sheng, L.; Zhang, B.; Liang, W.; Lv, B. Mechanisms of recurrent laryngeal nerve injury near the nerve entry point during thyroid surgery: a retrospective cohort study. Int J Surg. 2020, 83, 125-130.
- Hayami, M.; Watanabe, M.; Mine, S.; Imamura, Y.; Okamura, A.; Yuda, M.; Yamashita, K.; Shoji, Y.; Toihata, T.; Kozuki, R.; Ishizuka, N. Steam induced by the activation of energy devices under a wet condition may cause thermal injury. Surg Endosc. 2020, 34, 2295-2302.
- Sulica, L. The natural history of idiopathic unilateral vocal fold paralysis: evidence and problems. Laryngoscope. 2008, 118, 1303-1307.
- Lee, D.H.; Lee, S.Y.; Lee, M.; Seok, J.; Park, S.J.; Jin, Y.J.; Lee, D.Y.; Kwon, T.K. Natural course of unilateral vocal fold paralysis and optimal timing of permanent treatment. JAMA Otolaryngol Head Neck Surg. 2020, 146, 30-35.
- Kuo, C.T.; Chiu, C.H.; Fang, T.J.; Chao, Y.K. Prognostic factors for recovery from left recurrent laryngeal nerve palsy after minimally invasive McKeown esophagectomy: a retrospective study. Ann Surg Oncol. 2024, 31, 1546-1552.
- Shimizu, H.; Shiozaki, A.; Fujiwara, H.; Konishi, H.; Kosuga, T.; Komatsu, S.; Ichikawa, D.; Okamoto, K.; Otsuji, E. Short- and long-term progress of recurrent laryngeal nerve paralysis after subtotal esophagectomy. Anticancer Res. 2017, 37, 2019-2023.
- Takatsu, J.; Higaki, E.; Abe, T.; Fujieda, H.; Yoshida, M.; Yamamoto, M.; Shimizu, Y. Critical swallowing functions contributing to dysphagia in patients with recurrent laryngeal nerve paralysis after esophagectomy. Esophagus. 2024, 21, 111-119.
- Baba, M.; Aikou, T.; Natsugoe, S.; Kusano, C.; Shimada, M.; Nakano, S.; Fukumoto, T.; Yoshinaka, H. Quality of life following esophagectomy with three-field lymphadenectomy for carcinoma, focusing on its relationship to vocal cord palsy. Dis Esophagus. 1998, 11, 28-34.
- Scholtemeijer, M.G.; Seesing, M.F.J.; Brenkman, H.J.F.; Janssen, L.M.; van Hillegersberg, R.; Ruurda, J.P. Recurrent laryngeal nerve injury after esophagectomy for esophageal cancer: incidence, management, and impact on short- and long-term outcomes. J Thorac Dis. 2017, 9, S868-S878.
- Oshikiri, T.; Takiguchi, G.; Hasegawa, H.; Yamamoto, M.; Kanaji, S.; Yamashita, K.; Matsuda, T.; Nakamura, T.; Suzuki, S.; Kakeji, Y. Postoperative recurrent laryngeal nerve palsy is associated with pneumonia in minimally invasive esophagectomy for esophageal cancer. Surg Endosc. 2021, 35, 837-844.
- Yang, Y.; Li, B.; Xu, X.; Liu, Z.; Jiang, C.; Wu, X.; Yang, Y.; Li, Z. Short-term and long-term effects of recurrent laryngeal nerve injury after robotic esophagectomy. Eur J Surg Oncol. 2023, 49, 107009.
- Booka, E.; Takeuchi, H.; Nishi, T.; Matsuda, S.; Kaburagi, T.; Fukuda, K.; Nakamura, R.; Takahashi, T.; Wada, N.; Kawakubo, H.; Omori, T.; Kitagawa, Y. The impact of postoperative complications on survival after esophagectomy for esophageal cancer. Medicine (Baltimore). 2015, 94, e1369.
- Qu, R.; Tu, D.; Ping, W.; Fu, X. The impact of recurrent laryngeal nerve injury on prognosis after McKeown esophagectomy for ESCC. Cancer Manag Res. 2021, 13, 1861-1868.
- Tsunoda, S.; Shinohara, H.; Kanaya, S.; Okabe, H.; Tanaka, E.; Obama, K.; Hosogi, H.; Hisamori, S.; Sakai, Y. Mesenteric excision of upper esophagus: a concept for rational anatomical lymphadenectomy of the recurrent laryngeal nodes in thoracoscopic esophagectomy. Surg Endosc. 2020, 34, 133-141.
- Otsuka, K.; Murakami, M.; Goto, S.; Ariyoshi, T.; Yamashita, T.; Saito, A.; Kohmoto, M.; Kato, R.; Lefor, A.K.; Aoki, T. Minimally invasive esophagectomy and radical lymph node dissection without recurrent laryngeal nerve paralysis. Surg Endosc. 2020, 34, 2749-2757.
- Saeki, H.; Nakashima, Y.; Hirose, K.; Sasaki, S.; Jogo, T.; Taniguchi, D.; Edahiro, K.; Korehisa, S.; Kudou, K.; Nakanishi, R.; Kubo, N.; Ando, K.; Kabashima, A.; Oki, E.; Maehara, Y. “Energy-less technique” with mini-clips for recurrent laryngeal nerve lymph node dissection in prone thoracoscopic esophagectomy for esophageal cancer. Am J Surg. 2018, 216, 1212-1214.
- Fu, J.; Li, Y.; Wang, Z.; Cheng, Y.; Chen, N.; Sun, X.; Zhang, B.; Peng, Z.; Chen, W.; Qian, R.; Shi, A.; Yan, X.; Wang, H.; Ma, F.; Lv, Y.; Zhang, Y. The role of magnetic anchoring and traction technique in thoracoscopic lymphadenectomy along the left recurrent laryngeal nerve. Surg Endosc. 2022, 36, 3653-3662.
- Dongming, G.; Yuequan, J.; Qi, Z.; Huajie, X.; Zhiqiang, W. A novel technique for lymphadenectomy along the left recurrent laryngeal nerve during minimally invasive esophagectomy: a retrospective cohort study. BMC Surg. 2023, 23, 355.
- Hikage, M.; Kamei, T.; Nakano, T.; Abe, S.; Katsura, K.; Taniyama, Y.; Sakurai, T.; Teshima, J.; Ito, S.; Niizuma, N.; Okamoto, H.; Fukutomi, T.; Yamada, M.; Maruyama, S.; Ohuchi, N. Impact of routine recurrent laryngeal nerve monitoring in prone esophagectomy with mediastinal lymph node dissection. Surg Endosc. 2017, 31, 2986-2996.
- Kanemura, T.; Miyata, H.; Yamasaki, M.; Makino, T.; Miyazaki, Y.; Takahashi, T.; Kurokawa, Y.; Takiguchi, S.; Mori, M.; Doki, Y. Usefulness of intraoperative nerve monitoring in esophageal cancer surgery in predicting recurrent laryngeal nerve palsy and its severity. Gen Thorac Cardiovasc Surg. 2019, 67, 1075-1080.
- Huang, C.L.; Chen, C.M.; Hung, W.H.; Cheng, Y.F.; Hong, R.P.; Wang, B.Y.; Cheng, C.Y. Clinical outcome of intraoperative recurrent laryngeal nerve monitoring during thoracoscopic esophagectomy and mediastinal lymph node dissection for esophageal cancer. J Clin Med. 2022, 11, 4949.
- Chen, B.; Yang, T.; Wang, W.; Tang, W.; Xie, J.; Kang, M. Application of intraoperative neuromonitoring (IONM) of the recurrent laryngeal nerve during esophagectomy: a systematic review and meta-analysis. J Clin Med. 2023, 12, 565.
- Wong, I.; Tong, D.K.H.; Tsang, R.K.Y.; Wong, C.L.Y.; Chan, D.K.K.; Chan, F.S.Y.; Law, S. Continuous intraoperative vagus nerve stimulation for monitoring of recurrent laryngeal nerve during minimally invasive esophagectomy. J Vis Surg. 2017, 3, 9.
- Komatsu, S.; Konishi, T.; Matsubara, D.; Soga, K.; Shimomura, K.; Ikeda, J.; Taniguchi, F.; Fujiwara, H.; Shiozaki, A.; Otsuji, E. Continuous recurrent laryngeal nerve monitoring during single-port mediastinoscopic radical esophagectomy for esophageal cancer. J Gastrointest Surg. 2022, 26, 2444-2450.
- Oshikiri, T.; Goto, H.; Horikawa, M.; Urakawa, N.; Hasegawa, H.; Kanaji, S.; Yamashita, K.; Matsuda, T.; Nakamura, T.; Kakeji, Y. Incidence of recurrent laryngeal nerve palsy in robot-assisted versus conventional minimally invasive McKeown esophagectomy in prone position: a propensity score-matched study. Ann Surg Oncol. 2021, 28, 7249-7257.
- Chao, Y.K.; Li, Z.; Jiang, H.; Wen, Y.W.; Chiu, C.H.; Li, B.; Shang, X.; Zhou, D.; Li, Y.; Yan, X.; Wu, H. Comparative study of surgical outcomes between robot-assisted and video-assisted thoracoscopic esophagectomy for esophageal cancer: a meta-analysis. Surg Endosc. 2023, 37, 3443-3455.
- Watanabe M, Kuriyama K, Terayama M, Okamura A, Kanamori J, Imamura Y. Robotic- Assisted Esophagectomy: Current Situation and Future Perspectives. Ann Thorac Cardiovasc Surg. 2023, 29, 168-176.
- Yang, Y.; Li, B.; Yi, J.; Hua, R.; Chen, H.; Tan, L.; Li, H.; He, Y.; Guo, X.; Sun, Y.; Yu, B.; Li, Z. Robot-assisted versus conventional minimally invasive esophagectomy for resectable esophageal squamous cell carcinoma: early results of a multicenter randomized controlled trial: the RAMIE trial. Ann Surg. 2022, 275, 646-653.
- Sato, K.; Fujita, T.; Matsuzaki, H.; Takeshita, N.; Fujiwara, H.; Mitsunaga, S.; Kojima, T.; Mori, K.; Daiko, H. Real-time detection of the recurrent laryngeal nerve in thoracoscopic esophagectomy using artificial intelligence. Surg Endosc. 2022, 36, 5531-5539.
- Natsugoe, S.; Okumura, H.; Matsumoto, M.; Ishigami, S.; Owaki, T.; Nakano, S.; Aikou, T. Reconstruction of recurrent laryngeal nerve with involvement by metastatic node in esophageal cancer. Ann Thorac Surg. 2005, 79, 1886-1889.
- Koyanagi, K.; Igaki, H.; Iwabu, J.; Ochiai, H.; Tachimori, Y. Recurrent laryngeal nerve paralysis after esophagectomy: respiratory complications and role of nerve reconstruction. Tohoku J Exp Med. 2015, 237, 1-8.
- Filauro, M.; Vallin, A.; Marcenaro, E.; Missale, F.; Fragale, M.; Mora, F.; Marrosu, V.; Sampieri, C.; Carta, F.; Puxeddu, R.; Peretti, G. Quality of life after transoral CO2 laser posterior cordotomy with or without partial arytenoidectomy for bilateral adductor vocal cord paralysis. Eur Arch Otorhinolaryngol. 2021, 278, 4391-4401.
- Tarihci Cakmak E, Sen EI, Doruk C, Sen C, Sezikli S, Yaliman A. The Effects of Neuromuscular Electrical Stimulation on Swallowing Functions in Post-stroke Dysphagia: A Randomized Controlled Trial. Dysphagia. 2023, 38, 874-885.
- Wang Z, Xiao Z, Shen Q, Zhao N, Zhang W. Neuromuscular Electrical Stimulation for Post-Stroke Dysphagia Treatment: A Systemic Evaluation and Meta-Analysis of Randomized Controlled Trials. Dysphagia. 2024, 39, 424-432.
- Mattioli, F.; Menichetti, M.; Bergamini, G.; Molteni, G.; Alberici, M.P.; Luppi, M.P.; Nizzoli, F.; Presutti, L. Results of early versus intermediate or delayed voice therapy in patients with unilateral vocal fold paralysis: our experience in 171 patients. J Voice. 2015, 29, 455-458.
- Walton, C.; Carding, P.; Flanagan, K. Perspectives on voice treatment for unilateral vocal fold paralysis. Curr Opin Otolaryngol Head Neck Surg. 2018, 26, 157-161.
- Kojima, K.; Fukushima, T.; Kurita, D.; Matsuoka, A.; Ishiyama, K.; Oguma, J.; Daiko, H. Perioperative decrease in tongue pressure is an intervenable predictor of aspiration after esophagectomy. Dysphagia. 2023, 38, 1147-1155.
- Yu, Y.; Li, Y.; Lu, Y.; Hua, X.; Ma, H.; Li, H.; Wei, X.; Zhang, J.; Chen, X.; Liu, Q.; Zhu, Z.; Xu, L.; Zhang, R.; Sun, H.; Wang, Z. Chin-down-plus-larynx-tightening maneuver improves choking cough after esophageal cancer surgery. Ann Transl Med. 2019, 7, 376.
- Chen, X.; Wan, P.; Yu, Y.; Li, M.; Xu, Y.; Huang, P.; Huang, Z. Types and timing of therapy for vocal fold paresis/paralysis after thyroidectomy: a systematic review and meta-analysis. J Voice. 2014, 28, 799-808.
- Hasukawa, A.; Mochizuki, R.; Sakamoto, H.; Shibano, A.; Kitahara, T. Type I thyroplasty or fat injection laryngoplasty versus arytenoid adduction: effects of surgery on voice recovery in patients with unilateral vocal fold paralysis. Ear Nose Throat J. 2023, 19, 1455613231176153.
- Jeong, G.E.; Lee, D.H.; Lee, Y.S.; Ahn, D.S.; Lee, D.K.; Choi, S.H.; Nam, S.Y.; Kim, S.Y. Treatment efficacy of voice therapy following injection laryngoplasty for unilateral vocal fold paralysis. J Voice. 2022, 36, 242-248.
- Haddad, R.; Ismail, S.; Khalaf, M.G.; Matar, N. Lipoinjection for unilateral vocal fold paralysis treatment: a systematic review and meta-analysis. Laryngoscope. 2022, 132, 1630-1640.
- Watanabe, K.; Hirano, A.; Kobayashi, Y.; Sato, T.; Honkura, Y.; Katori, Y. Long-term voice evaluation after arytenoid adduction surgery in patients with unilateral vocal fold paralysis. Eur Arch Otorhinolaryngol. 2023, 280, 5011-5017.
- Lindeman, R.C. Diverting the paralyzed larynx: a reversible procedure for intractable aspiration. Laryngoscope. 1975, 85, 157-180.
- Ninomiya, H.; Yasuoka, Y.; Inoue, Y.; Toyoda, M.; Takahashi, K.; Miyashita, M.; Furuya, N. Simple and new surgical procedure for laryngotracheal separation in pediatrics. Laryngoscope. 2008, 118, 958-961.
- Shino, M.; Yasuoka, Y.; Murata, T.; Ninomiya, H.; Takayasu, Y.; Takahashi, K.; Chikamatsu, K. Improvement of tracheal flap method for laryngotracheal separation. Laryngoscope. 2013, 123, 440-445.
Figure 1.
Dissection of right RLN lymph nodes using a robot. a) Dorsal side of lymph nodes along the right recurrent laryngeal nerve (RLN) are being dissected as the same plane with dorsal side of the esophagus. This figure demonstrates that the lymphatic chain forming these nodes exhibits a mesenteric-like structure. b) The lymphatic chain is dissected from the trachea, with the right recurrent laryngeal nerve and subclavian artery serving as the base, resembling a mesenteric structure. c) As the lymphatic chain is dissected dorsally from the right subclavian artery, the recurrent laryngeal nerve (black arrowhead) naturally becomes visible under the thin membrane. d) After dividing the esophageal branch of the recurrent laryngeal nerve and dissect from lateral wall of the trachea, en bloc resection of the lymphatic chain will be possible (yellow dots).
Figure 1.
Dissection of right RLN lymph nodes using a robot. a) Dorsal side of lymph nodes along the right recurrent laryngeal nerve (RLN) are being dissected as the same plane with dorsal side of the esophagus. This figure demonstrates that the lymphatic chain forming these nodes exhibits a mesenteric-like structure. b) The lymphatic chain is dissected from the trachea, with the right recurrent laryngeal nerve and subclavian artery serving as the base, resembling a mesenteric structure. c) As the lymphatic chain is dissected dorsally from the right subclavian artery, the recurrent laryngeal nerve (black arrowhead) naturally becomes visible under the thin membrane. d) After dividing the esophageal branch of the recurrent laryngeal nerve and dissect from lateral wall of the trachea, en bloc resection of the lymphatic chain will be possible (yellow dots).
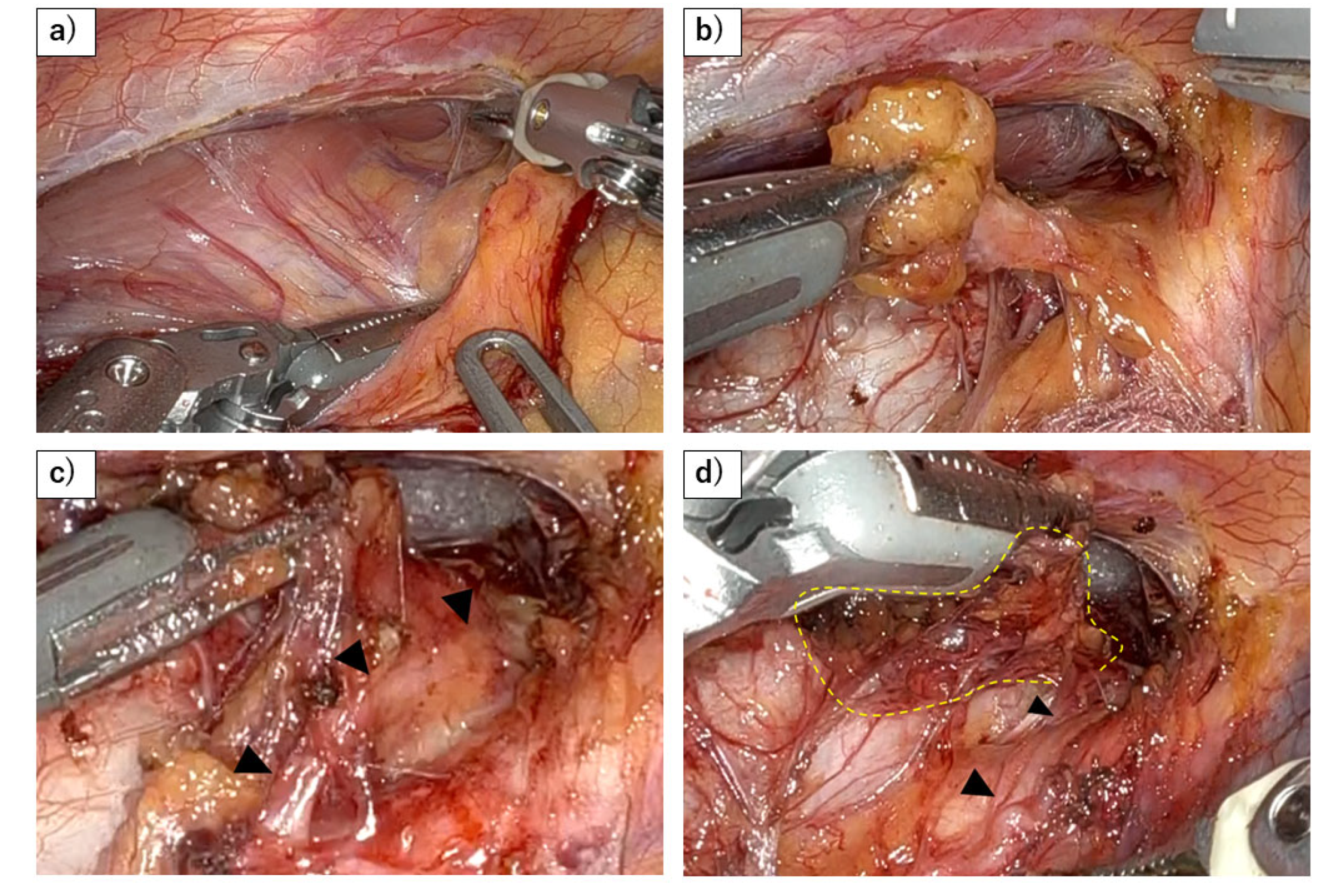
Figure 2.
Dissection of left RLN lymph nodes using a robot. a) A stable surgical field is achieved by retracting the esophagus dorsally with gauze and using the robot to fix the trachea in place. b) Dissection of the left side of the trachea from the lymphatic chain. The use of the robot allows precise hemostasis while maneuvering over the trachea. c) The sympathetic cardiac branch (black arrowhead) is revealed behind the thin membrane, as the lymphatic chain is flipped up. d) The left RLN (white arrowhead) and its esophageal branch has been preserved, after flipping up the lymphatic chain.
Figure 2.
Dissection of left RLN lymph nodes using a robot. a) A stable surgical field is achieved by retracting the esophagus dorsally with gauze and using the robot to fix the trachea in place. b) Dissection of the left side of the trachea from the lymphatic chain. The use of the robot allows precise hemostasis while maneuvering over the trachea. c) The sympathetic cardiac branch (black arrowhead) is revealed behind the thin membrane, as the lymphatic chain is flipped up. d) The left RLN (white arrowhead) and its esophageal branch has been preserved, after flipping up the lymphatic chain.
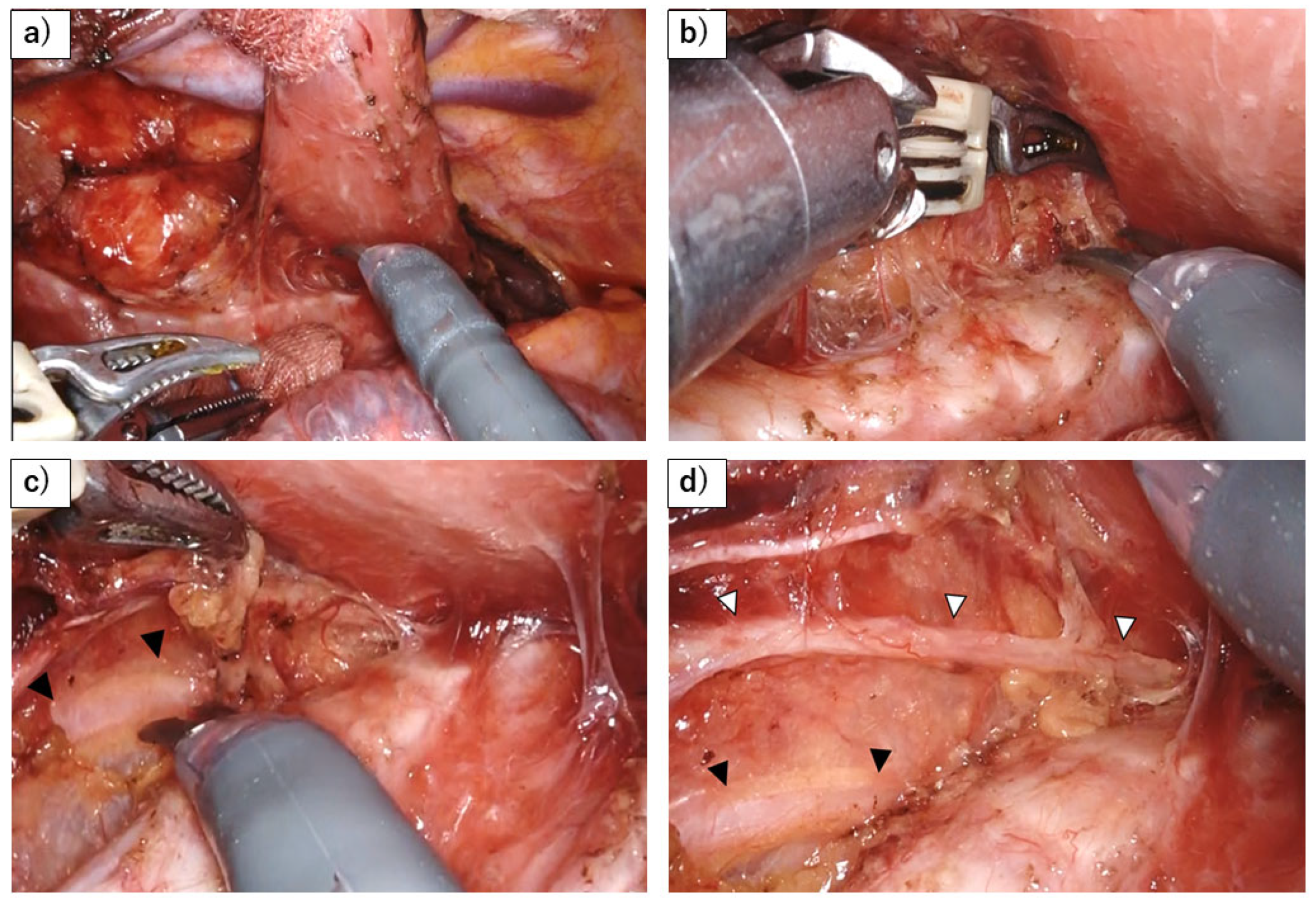
Figure 3.
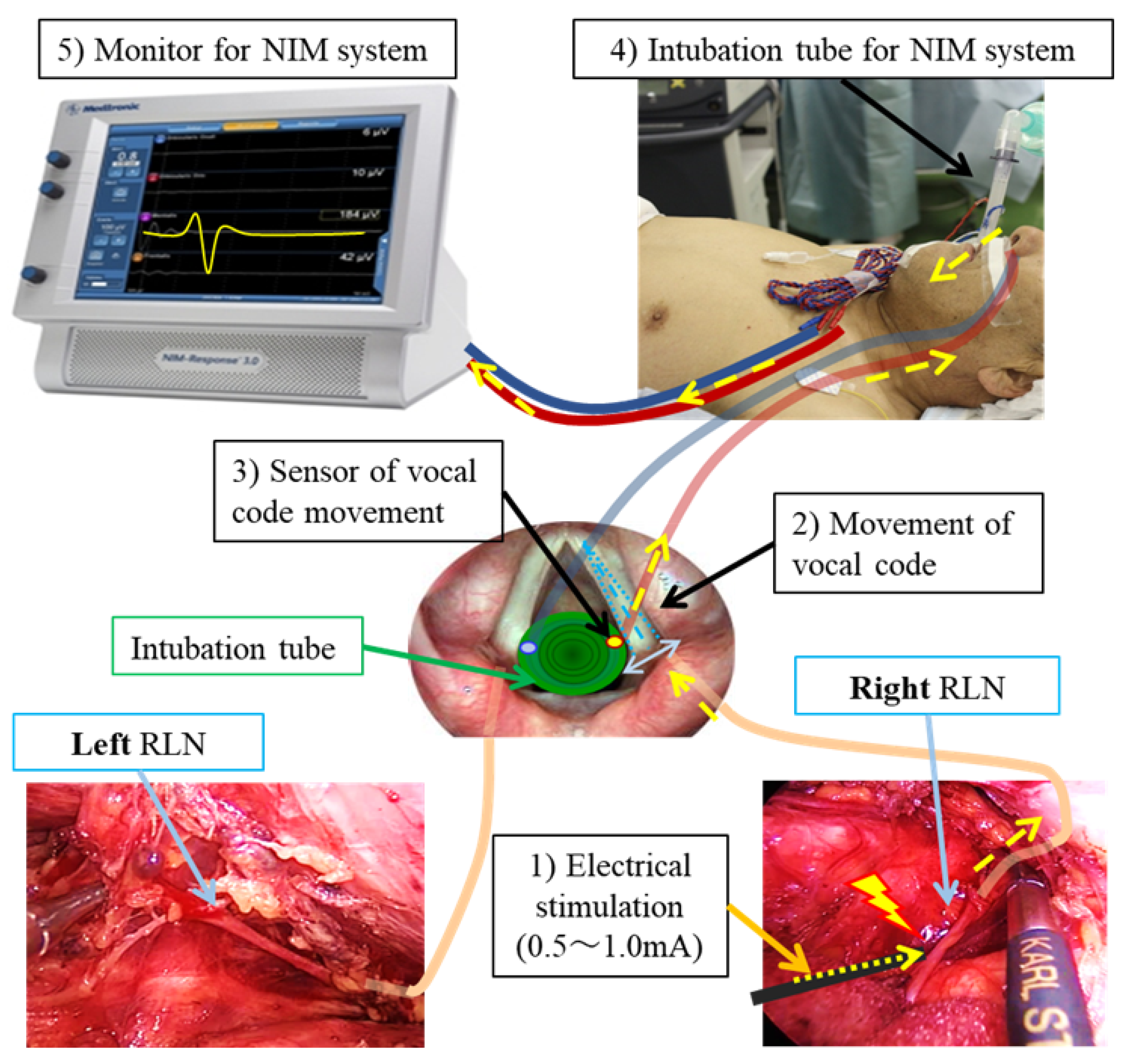
Schematic diagram of NIM (Nerve Integrity Monitoring). This diagram illustrates the mechanism of electrical stimulation of the vagus and RLN, which causes vocal cord movement detected via sensors attached to the endotracheal tube. The process is as follows: 1) The RLN is stimulated with a current of 0.5–1.0 mA. 2) The vocal cords move in response to the stimulation. 3) The sensor detects this vocal code movement. 4) The signal is transmitted as electrical impulses through the cord of NIM endotracheal tube. 5) The stimulation is displayed as an electromyographic signals on the NIM monitor.
Figure 3.
Schematic diagram of NIM (Nerve Integrity Monitoring). This diagram illustrates the mechanism of electrical stimulation of the vagus and RLN, which causes vocal cord movement detected via sensors attached to the endotracheal tube. The process is as follows: 1) The RLN is stimulated with a current of 0.5–1.0 mA. 2) The vocal cords move in response to the stimulation. 3) The sensor detects this vocal code movement. 4) The signal is transmitted as electrical impulses through the cord of NIM endotracheal tube. 5) The stimulation is displayed as an electromyographic signals on the NIM monitor.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



