
Submitted:
19 October 2024
Posted:
21 October 2024
You are already at the latest version
Abstract
Background: Neurofeedback (NFB) or EEG-Biofeedback is a non-invasive therapeutic method, based on the theory of operating conditioning, and designed to change the functioning of the brain by sending feedback that provides positive or negative reinforcement. The goal is to teach the patient how to perceive specific cortical activation states and how to achieve them on purpose. NFB has been used to treat various mental disorders, including Post-traumatic Stress Disorder (PTSD). Traditional treatments for PTSD have several limitations; very few individuals are willing to relive the traumatic experience. Placing itself as an effective alternative, Neurofeedback allows the unresponsive patient to recourse to an alternative intervention to relieve their symptoms without reliving the anguish of trauma, consequently presuming a lower percentage of drop-out. Considering the importance of integrated approaches to clinical practice, NFB was integrated with Trauma-Informed Motivational Interviewing (TIMI). The TIMI approach is a new therapeutic paradigm for clinical interviews that aims to help users work through their trauma and transform it from a point of weakness to a point of strength. Integrating TIMI with NFB can help overcome the current trend of passive implementation of intervention tools, leading to greater user responsiveness and fewer residual symptoms. To improve treatment adherence, moreover, it has been suggested to incorporate Virtual Reality (VR) into the NFB system. VR, through the "sense of presence," provides a more immersive experience than 2D visualization, potentially resulting in faster cortical training. Lastly, the research protocol aims to focus on a population at high risk of PTSD that is often overlooked in research, such as workers who are victims of occupational PTSD.Methods: The study design involves in-depth analysis of a specific clinical case. Baseline measurements were taken for enrollment and at the following time points: T1 (pre-treatment), T2 (post-treatment), and T3 (follow-up). These measurements included various psychometric assessments to evaluate PTSD symptoms, treatment acceptability, safety, and adherence, as well as biological measures related to the brain's electrophysiological activity.Results and Conclusion: Our research reveals that the synergy between virtual reality-mediated Neurofeedback and trauma-motivational interviewing produces significant results. TIMINB stands out as a low-cost, effective, and completely risk-free procedure. This approach could represent a groundbreaking innovation in the field of Cyberpsychology and psychological therapies.
Keywords:
Neurofeedback
; EEG-Biofeedback
; Post-Traumatic Stress Disorder
; Virtual Reality
; Cyber Health Psychology
; Occupational PTSD
; Trauma-Informed Motivational Interviewing
1. Introduction
1.1. Neurofeedback or EEG-Biofeedback
Neurofeedback (NFB) or EEG-Biofeedback is a non-invasive therapeutic method, based on the theory of operating conditioning, and designed to change the functioning of the brain by sending feedback that provides positive or negative reinforcement. The goal is to teach the patient how to perceive specific cortical activation states and how to achieve them on purpose [1]. When discussing NFB as a control system and electrophysiological training, it is important to clarify that it is not similar to the electroshock therapies of the past [2]; instead, NFB is a computer-brain interface that utilizes sensors placed on specific areas of the scalp to provide the brain with instant feedback via EEG. This enables the user to sense the frequencies of brain waves [3]. NFB can involve images, films, or videogames that adjust certain scene parameters according to the brain wave patterns set by clinicians. According to scientific literature, NFB has been shown to be a valid and effective therapy for treating several clinical psychological conditions, including anxiety disorders [4], stress-related disorders [4], sleep disorders [5], and ADHD [6].
In this context, a particular field of intervention of the NFB is related to the Post-Traumatic Stress Disorder (PTSD) [7,8,9]. According to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR), Post-Traumatic Stress Disorder (PTSD) is a severe psychiatric condition that can develop following exposure to one or more traumatic events, including life-threatening situations, serious accidents, or acts of violence [10]. PTSD is defined by the presence of persistent symptoms that have been present for a minimum of one month. These symptoms include avoidance of stimuli and environments related to the traumatic event, alterations in mood and cognition, insomnia, and difficulty concentrating [7,9].
Currently, the most commonly used therapy by psychotherapists is the Cognitive-Behavioral Exposure Therapy [11,12,13,14]. This therapy involves gradually and controlled exposing the participant to the triggering stimulus in order to develop desensitization and cognitive restructuring [15]. Exposure therapy is a valid and effective treatment [16]. However, about one-third of patients do not respond to this treatment [11]. This is due to the concept of “Retraumatization”. Many people, in fact, are unwilling to relive and expose themselves to trauma in order to work on it [17].
Placing itself as an effective alternative, NFB allows the unresponsive patient to recourse to an alternative intervention to relieve their symptoms without reliving the anguish of trauma [7].
1.2. Virtual Reality applied to Neurofeedback
In the majority of Neurofeedback research protocols, the neuromodulatory tool utilizes 2D visual feedback featuring bars that fluctuate in height based on the brain’s electrophysiological activity [18,19]. However, the unengaging 2D design of this feedback can make sessions demotivating and tiresome. Considering this, it is imperative to develop more engaging and interactive NFB protocols.
To fill this research gap, the research protocol aimed to integrate Neurofeedback with Virtual Reality systems. With the term Virtual Reality (VR) we refer to a three-dimensional environment generated by the computer, in which subjects interact with the environment as if they were really inside it [15]. VR allows complete control of the X-Y-Z coordinates, also completely isolating the user from any form of noise variables [15,16,20,21].
1.2. Neurofeedback and Trauma-Informed Motivational Iterviewing: The Importance Of Integrated Approaches In Clinical Practice
In PTSD treatment literature, it was found that patients who complete any form of treatment continue to report residual symptoms [26]. We can assume that the presence of these residual symptoms is explained by the lack of integration between the different therapeutic tools and methods. Therapists often overlook the profound impact of trauma and adverse experiences on patients’ thought patterns and behaviors [27].
Consequently, by mechanically implementing the care tools, they can paradoxically traumatize the patient [3]. For this reason, VR and NFB have been incorporated into Trauma-Informed Motivational Interviewing (TIMI), an innovative therapeutic approach that melds Motivational Interviewing (MI) with Trauma-Informed Care (TIC). This integration addresses the need for trauma-sensitive interventions in therapy [17,27,28]. It focuses on enhancing motivation by restructuring cognition, transforming trauma from stressors into sources of resilience and strength. The TIMI approach is based on fundamental principles, including reflective listening, safety, self-efficacy, empowerment, collaboration, reciprocity, and respect for cultural, historical, and gender issues [27,29,30,31].
1.3. Occupational Post-Traumatic Stress Disorder
One final research gap in the literature concerns the type of sampling. Even though PTSD is commonly associated with war veterans, its diagnosis can include a wide spectrum of traumas related to different moments in an individual’s life, such as occupational traumas – ranging from assault to work accidents. In recent years, there has been little focus on preventing and treating the mental health consequences of workplace accidents. Occupational PTSD [32] can affect a wide range of individuals, managers, or employees [33,34]. This fact underlines the importance of effective treatments that restore an optimum health condition and achieve the objective of returning the individual to his place of work in the best possible condition, not only physically but also mentally.
2. Materials and Methods
The purpose of our study was to empirically test the effectiveness of combining Neurofeedback, Virtual Reality, and Trauma-Informed Motivational Interviewing on addressing the impact of occupational traumas that can lead to PTSD. The research design focuses on an in-depth analysis of a specific clinical case. Treating a single patient provided us with the opportunity to conduct a comprehensive analysis of the underlying psychological dynamics and gain a deep understanding of the complexity characterizing this specific psychological disorder [35]. The University of Catania’s Internal Ethics Review Board of Psychology Research (IERB) has been informed of the research. Since it is a case report inherent to clinical practice and without invasive therapies, no formal approval is required. Baseline measurements were taken for enrollment and at the following time points: T1 (pre-treatment), T2 (post-treatment), and T3 (follow-up).
These measurements included various psychometric assessments to evaluate PTSD symptoms, treatment acceptability, safety, and adherence; as well as biological measures related to the brain’s electrophysiological activity.
2.1. Neurofeedback System
2.1.1. Alpha-Theta Protocol
The Alpha-Theta protocol, also called deep-state training, is probably the most famous in the field of PTSD, addictions, and peak performance [3]. The Alpha-Theta protocol in Neurofeedback is a technique used to guide the brain through gentle oscillations between dominant states of Alpha and Theta. These two terms refer to different frequency bands of brain activity. Alpha is a state of disconnected relaxation and represents the central organizational frequency of our cortex. When the brain is in an alpha-dominant state, we are generally awake and focused [36,37].
Theta, on the other hand, is a slower frequency band. When theta is dominant, our brain is typically closer to sleep and our cortical activity is lower, in favor of more basic sub-cortical structures [36,38].
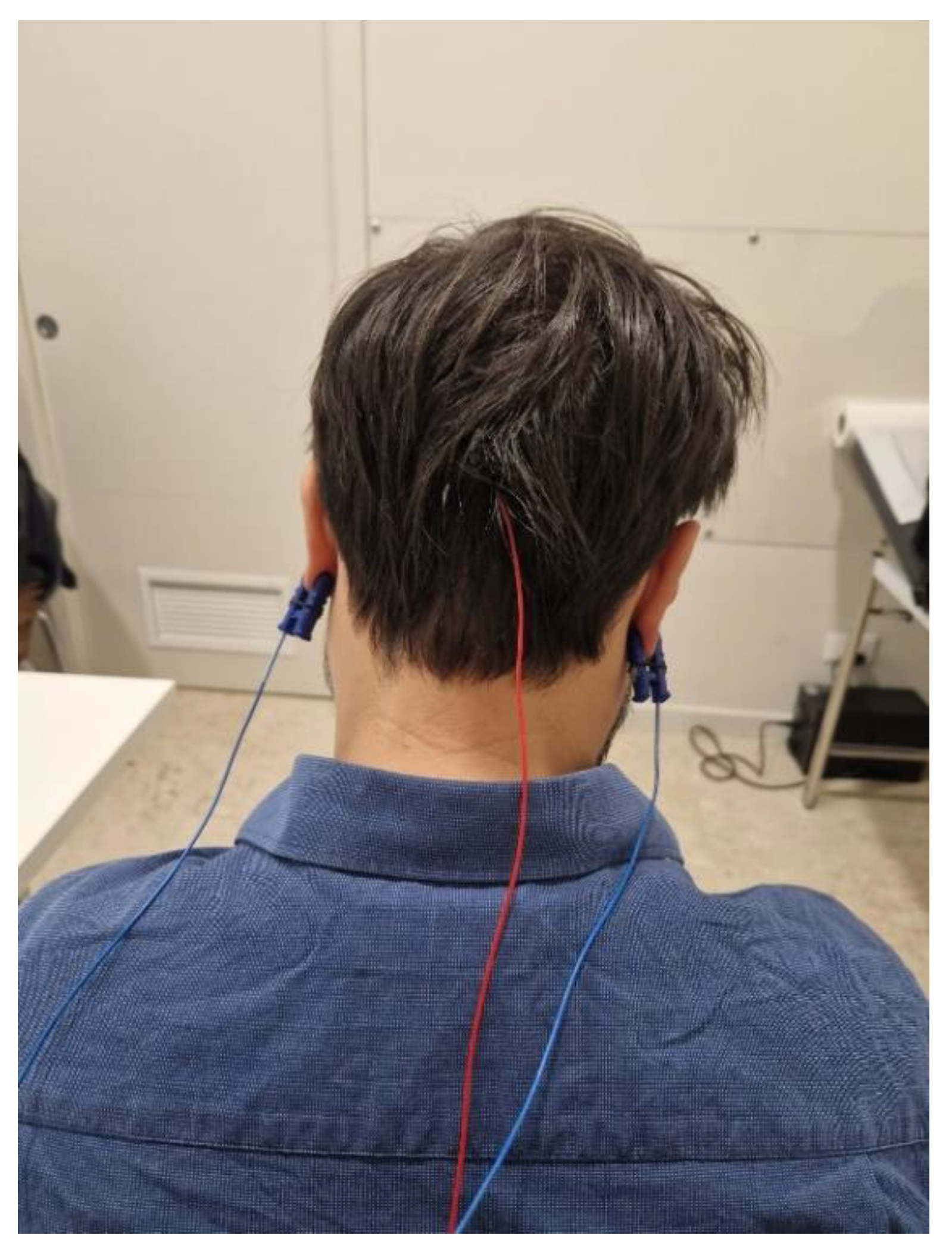
Our research protocol aimed to increase alpha wave oscillations while inhibiting theta waves through Neurofeedback training. This approach has specific objectives: enhancing alpha frequencies (8-12Hz) can promote alert awareness, improve creativity, problem-solving skills, and intuition, while suppressing theta frequencies (4-8Hz) can enhance cognitive control. Research indicates that balancing these wave patterns can induce a state of calm vigilance, akin to being half-asleep yet fully cognizant, with optimal cognitive control [36,38,39,40,41,42]. The assembly of the electrodes for the Alpha-Theta protocol requires placing a single electrode at the Oz position (Occipital Medial, 10-20 system) and attaching the clamps for Reference (R) and Neutral (N).
Figure 1.
Neurofeedback Setup and Electrode Placement.
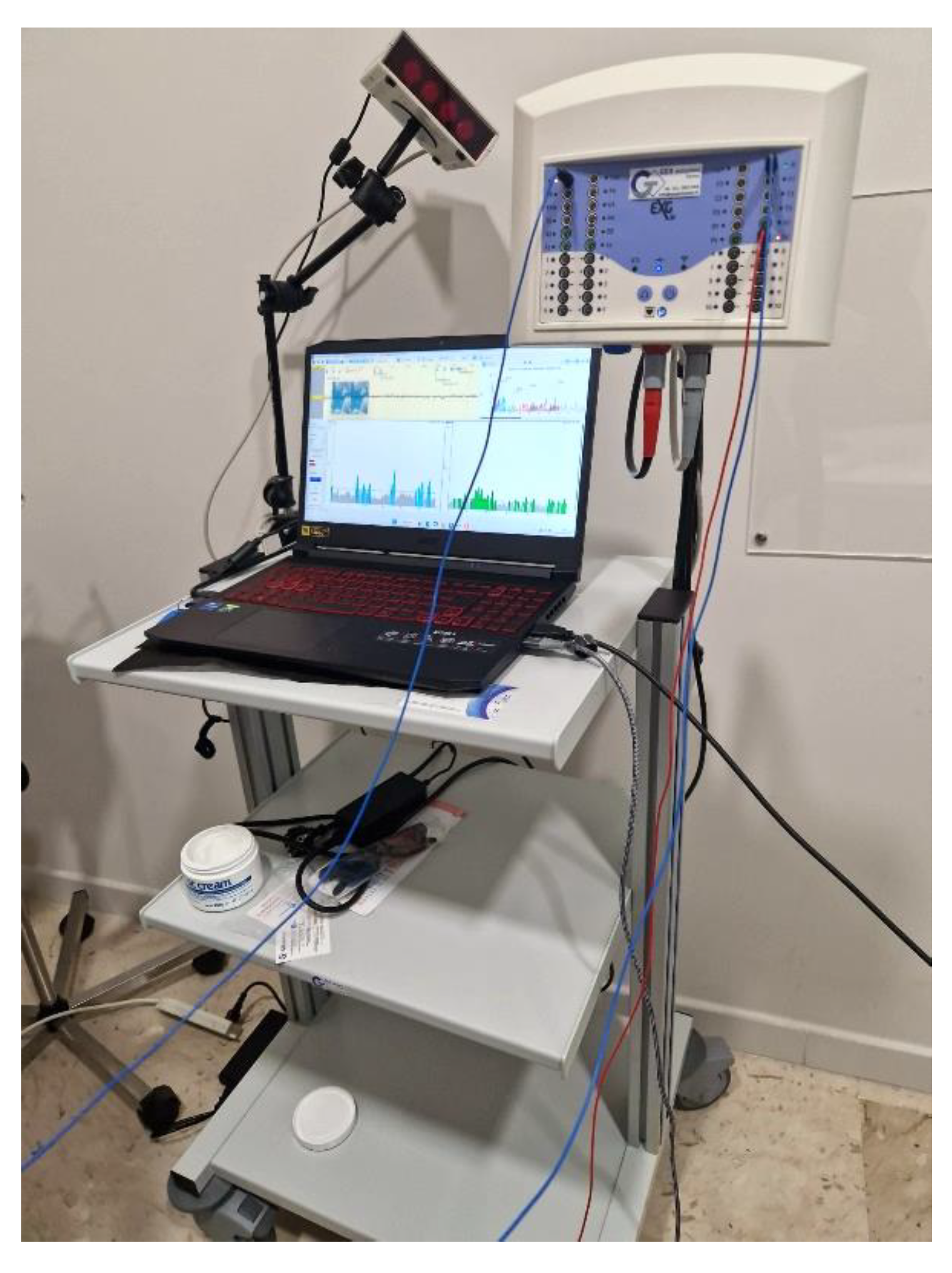
Figure 2.
Neurofeedback Setup and Electrode Placement.
2.1.2. Videogame
The Neurofeedback protocol utilized a VR videogame called “Flying Carpet.” In this VR environment, users observed Aladdin on his magic carpet, with the carpet’s flight dynamics directly linked to their brainwave activity. Increased alpha rhythm raised the carpet’s altitude, while reduced theta rhythm controlled its direction. Success was achieved when users observed Aladdin flying upward and in the opposite direction to their own orientation.
2.1.3. Setup
A typical neurofeedback system comprises a computer with dual displays: one showing the EEG track for the therapist’s analysis, and another—in our case, a Head-Mounted Display—for the user to view media or interact with a videogame. For optimal therapy conditions, sessions should take place in a quiet, distraction-free environment. It’s essential for the therapist to create a welcoming atmosphere and provide supportive guidance throughout the user’s training process.
A critical aspect of neurofeedback is electrode placement and physical contact, which can be complex in psychotherapy, especially with traumatized patients [3,19]. It’s essential to approach this process empathetically, clearly communicating each step to the patient. The necessary “touching” involved in attaching, detaching, and preparing the skin for sensors presents a unique opportunity for rehabilitation through “caring” contact [43].
From a technical perspective, maintaining low impedance (below 20 kΩ) between the skull and sensors is crucial for optimal signal quality and neurofeedback accuracy. This requires careful attention to sensor/electrode implementation.
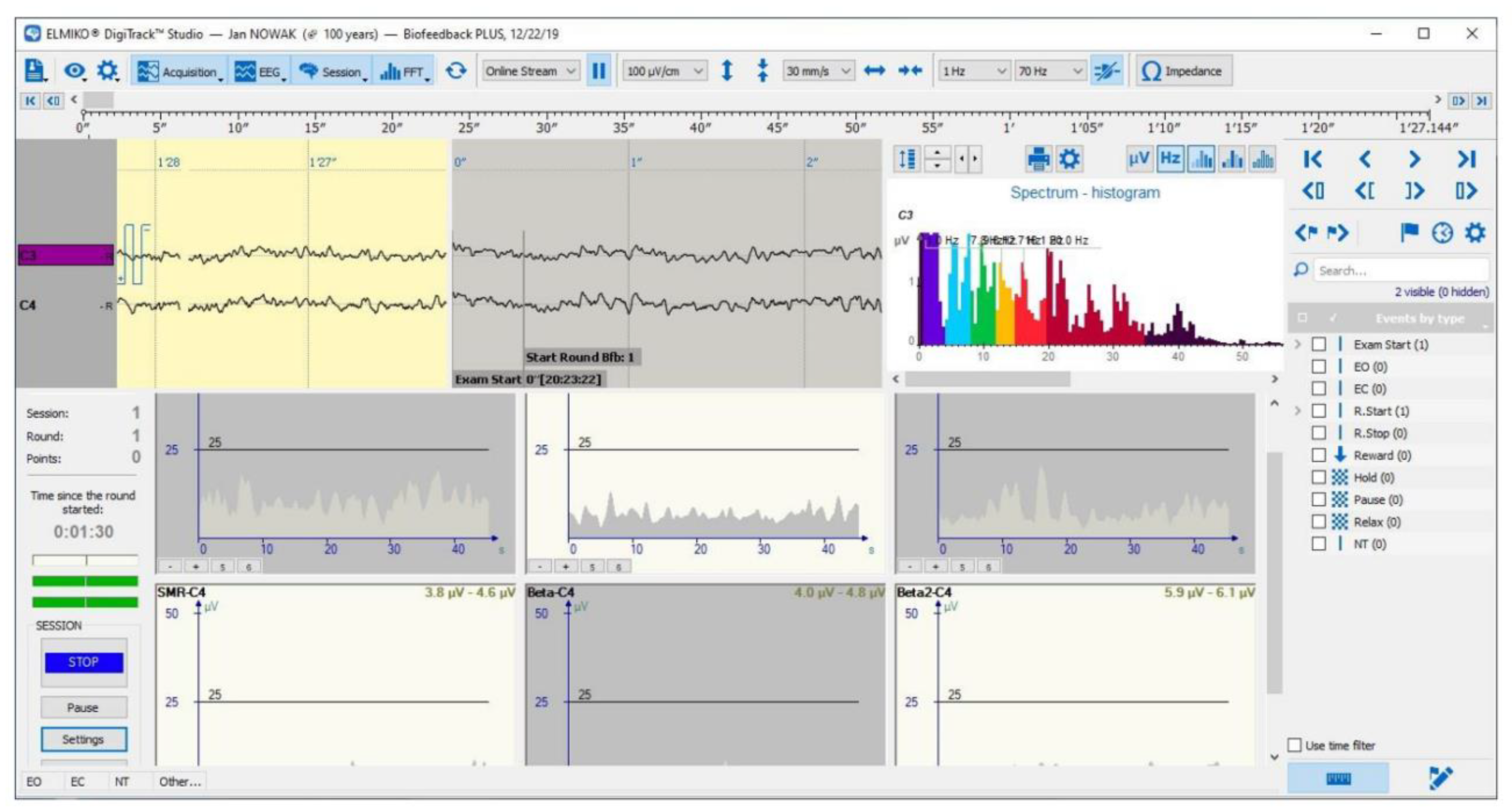
Figure 3.
Neurofeedback Dashboard from the therapist’s perspective.
2.2. Trauma-Informed Motivational Interviwing
As mental health professionals, it is crucial to consistently apply a set of interconnected basic principles when engaging with patients during the study. This methodological section outlines the fundamental principles of the TIMI approach [29,30] [44].
- SAFETY: The patient should feel safe both emotionally and physically. It’s important to make sure the interview room is private and that no one can unintentionally listen in or enter. If the patient doesn’t feel safe, they might leave out important details about their trauma during the interview.
- RELIABILITY AND TRANSPARENCY: The therapist needs to be as transparent as possible with the patient. It is important for the therapist to inform the patient about all procedures being performed, the purpose of the study, the expected results, the rationale behind specific decisions, and the use of the results. During the interview, it is important to provide objective feedback on the differences between the subject’s current behavior and the desired objectives, all while maintaining a sensitive, empathetic, and cordial attitude.
- COLLABORATION AND RECIPROCITY, WORKING WITH RESISTANCE: It is important to involve the patient as much as possible in decision-making and not to provide therapy mechanically. Therefore, it is crucial to listen to the patient. If the patient becomes tired or if something goes wrong, don’t hesitate to break away from the rigidity of the protocol. It’s always beneficial to try to understand the patient’s resistances and work with them, making sure to document all these deviations on a sheet that will be digitized later.
- PEER SUPPORT: One of the main features of TIMI is to be able to confront "others" who are also suffering from the same discomfort. Thus, we can create a group of mutual help. If the "other" has lived an experience similar to mine, who could understand and support me better than him?
- EMPOWERMENT: The traumatic experience is the pivot of the interview. The ideal goal is to make such a trauma from weakness to strength and resilience. (The experience of my trauma, the fact that I can tell it and now everything is over, must make me understand the strength I had, and the strength I can have in everyday life). It is also important to convey confidence in the patient’s change with encouragement and compliments in case of proactive behaviors.
- RESPECT FOR DIFFERENCES: Therapists are required to show maximum respect for any gender, socio-cultural, and personal differences in their relationships with patients. Every patient should be welcomed without judgment, and the patient should never perceive any implicit judgment from the therapist.
- REFLECTIVE LISTENING: The patient comes to us with a request for help. It is therefore of utmost importance to listen carefully, reflecting on the intrinsic and extrinsic meaning of his words and showing empathy for what has happened. Often a bad therapeutic relationship arises precisely because the patient does not feel heard but "visited" as if he were an automaton. Showing empathy also means not criticizing the patient for any dysfunctional behavior put in place as a result of the trauma, trying rather to make the patient himself grasp this dysfunction; For Example “This behavior put in place as a result of the trauma as it made you feel, would you like to change this behavior or do not think you need it, and if you don’t think so why?”.
- SELF-EFFICACY: During therapy sessions, it’s common for patients to ask for quick fixes or instant solutions to their problems. However, a good therapist should help the patient realize that true change comes from within themselves. By offering specific advice or instructions, the therapist may unintentionally undermine the patient’s autonomy and create resistance. Instead, it’s more effective to ask open-ended questions that encourage the patient to express their own thoughts and feelings, fostering a sense of self-discovery and empowerment.
2.3. Measures
2.3.1. Psychometric Measures
- Structured Clinical Interview for DSM-5 (SCID-5): Researchers have planned to use the SCID-5 during the baseline phase to assess eligibility for recruitment. The SCID-5 consists of a semi-structured interview divided into modules, each corresponding to different psychiatric disorders in the DSM-5 [45]. Within each module, there is a checklist for the clinician to complete, assigning a score from 0 to 3 based on the severity of different symptoms observed during the interview. Once the threshold required by the manual is exceeded, it is possible to proceed with the diagnosis of PTSD [45].
- Post-Traumatic Stress Disorder Checklist-5 (PCL-5): It is a self-report questionnaire composed of 20 items, related to the four symptomatic clusters of PTSD according to the DSM-5-TR [46]. Each item is evaluated by a 5-point Likert scale (from 0 = "Not at All" to 4 = "Extremely"). PCL-5 can be used to confirm the diagnosis of PTSD after SCID-5 or to hypothesize a PTSD to be confirmed with SCID-5. The administration of PCL-5 takes about 5/10 minutes. The 20 items that make up the questionnaire can be divided into 4 clusters: Cluster A (Items 1-2-3-4-5); Cluster B (Items 6-7) Cluster C (Items 8-9-10-11-12-13-14) Cluster D (Items 15-16-17-18-19-20). According to DSM-5-TR, any item with response 2 or higher can be considered an approved symptom. A provisional diagnosis of PTSD can be obtained by assessing the presence of at least 1 symptom of Cluster A, 1 symptom of Cluster B, 2 symptoms of Cluster C, and 2 symptoms of Cluster D. Recent literature, however, suggests that it is preferable to increase the threshold value to avoid false positives, with a cut-off point between 31 and 33. As regards post-treatment, according to existing literature, a change of 5-10 points indicates a reliable change not due to time; whereas a change of 10-20 points indicates a clinically significant change [47,48]. PCL-5 was administered to both T1 and T2.
- Beck Anxiety Inventory (BAI): The BAI [49] is a self-report questionnaire consisting of 21 multiple-choice items used to measure the severity of anxiety in adolescents and adults aged 17 years and older [50]. The items of the BAI can be evaluated by a 4-point Likert scale (from 0= "Not at All" to 3 = "Severely"); examples of items are: "Feeling Hot", "Unable to relax" and "Fear of losing control". The final score is obtained by adding up the values assigned to each item. Scores can range from 0 to 63: minimum anxiety levels correspond to a score between 0 and 7, mild anxiety corresponds to a score between 8 and 15, moderate anxiety corresponds to a score between 16 and 25, Finally, severe anxiety corresponds to a score between 26 and 63 [51]. BAI was administered to both T1 and T2.
- Beck Depression Inventory (BDI-II): The BDI [52,53], now in its second edition, is a self-report questionnaire composed of 21 multiple choice items that assess the severity of symptoms characterizing depressive disorder, often related to PTSD. Again, the score is obtained by adding up the scores given to individual items. Three types of information can be obtained from the administration of BDI-II: (1) A general score; (2) A score concerning somatic affective manifestations, such as: sleep alterations, appetite, agitation and crying; (3) A score for cognitive aspects, such as pessimism, self-criticism, self-esteem, and guilt. The threshold value for clinically significant impairment is 15-16 points. Specifically, a score >10 indicates mild depressive symptoms, a score >20 moderate depressive symptoms, a score >30 severe depressive symptoms. BDI-II was administered to both T1 and T2.
- Somatic Symptom Scale-8 (SSS-8): The “somatization” is a phenomenon characterized by the transfer of psychological suffering on an organ or body apparatus through the appearance of recurring physical symptoms. Several scientific studies have shown that patients suffering from PTSD show comorbidity with somatization symptoms [54]. The SSS-8 [55] was administered to evaluate the phenomenon of somatization and its course. SSS-8 is, specifically, a self-report questionnaire composed of 8 items, evaluated by a Likert scale at 5 points (from 0 = "Not at all " to 4 = "Very much"). The final score is obtained by adding up the values assigned to each item. Increasing scores indicate incrementally higher levels of discomfort: low (4 to 7); medium (8 to 11); high (12 to 15); very high (16 to 23). SSS-8 was administered to both T1 and T2.
2.3.2. Acceptance Measures of the Virtual Environment
- Simulator Sickness Questionnaire (SSQ): The main structural limitation of VR technologies is the so-called "Cybersickness" (CS) or "Motion sickness"[56,57] which can be defined as a kind of seasickness resulting from prolonged exposure to the three-dimensional environment by Head-Mounted Display. CS is a disabling element that can alter the correct functioning of the treatment. The SSQ [58] was used to measure this aspect; it is composed, in particular, of 16 items evaluated on a 4-point Likert scale (from 0="None" to 3="Severe"). Examples of items are: "Nausea", "Blurred vision" and "Dizziness". Based on existing literature guidelines, SSQ will be administered before and after each exposure session in VR-NFB [21]. SSQ can be divided into three subscales: Nausea (N = items 1,6,7,8,9,15,16); Oculomotor Disorder (O = items 1,2,3,4,5,9,11) and Disorientation (D =items 5,8,10,11,12,13,14). The final score is obtained by adding up the score assigned to individual items. According to the literature a score <5 indicates insignificant symptoms, a score between 5 and 10 indicates minimal symptoms, a score between 10 and 15 indicates significant symptoms, and a score between 15 and 20 indicates significant and considerable symptoms; Finally, a score of >20 is considered "extremely bad" [59].
2.3.3. Physiological Measurements
During each neurofeedback session, we will evaluate the amplitude, frequency, and coherence of the brain’s electrophysiological aspects [40]. Specifically, we will use EEG to assess brain waves, focusing on the Alpha and Theta waves, which are associated with the production of anxiety and stress [60].
2.3.4. Qualitative and Satisfaction Measures
At the end of the protocol sessions, participants will complete a brief "Patient Satisfaction Questionnaire" (PSQ) to assess therapy satisfaction. Sample questions may include: (1) Would you recommend this treatment? (2) What could be improved? (3) What didn’t go as expected?
3. Detailed Case Description
Figure 4.
Setting Neurofeedback.

User Z is a 50-year-old woman who has approached the research team at the University of Catania after a report from the Occupational Medicine Section of the Policlinico G. Rodolico - San Marco University Hospital. After consulting with specialists, the woman underwent a semi-structured clinical interview for DSM-5, which is necessary for PTSD diagnosing.
Once the eligibility criteria were met, the user Z. was informed about the objectives of the research protocol. She is provided with explanations about how Neurofeedback works, the necessary instructions for the user, and the role of Trauma-Informed Motivational Interviewing. All the details, including the commitment regarding the number of sessions and the required time, are also documented in the Informed Consent form that the woman agrees to sign. The clinician reminds her that she is free to stop the intervention at any time.
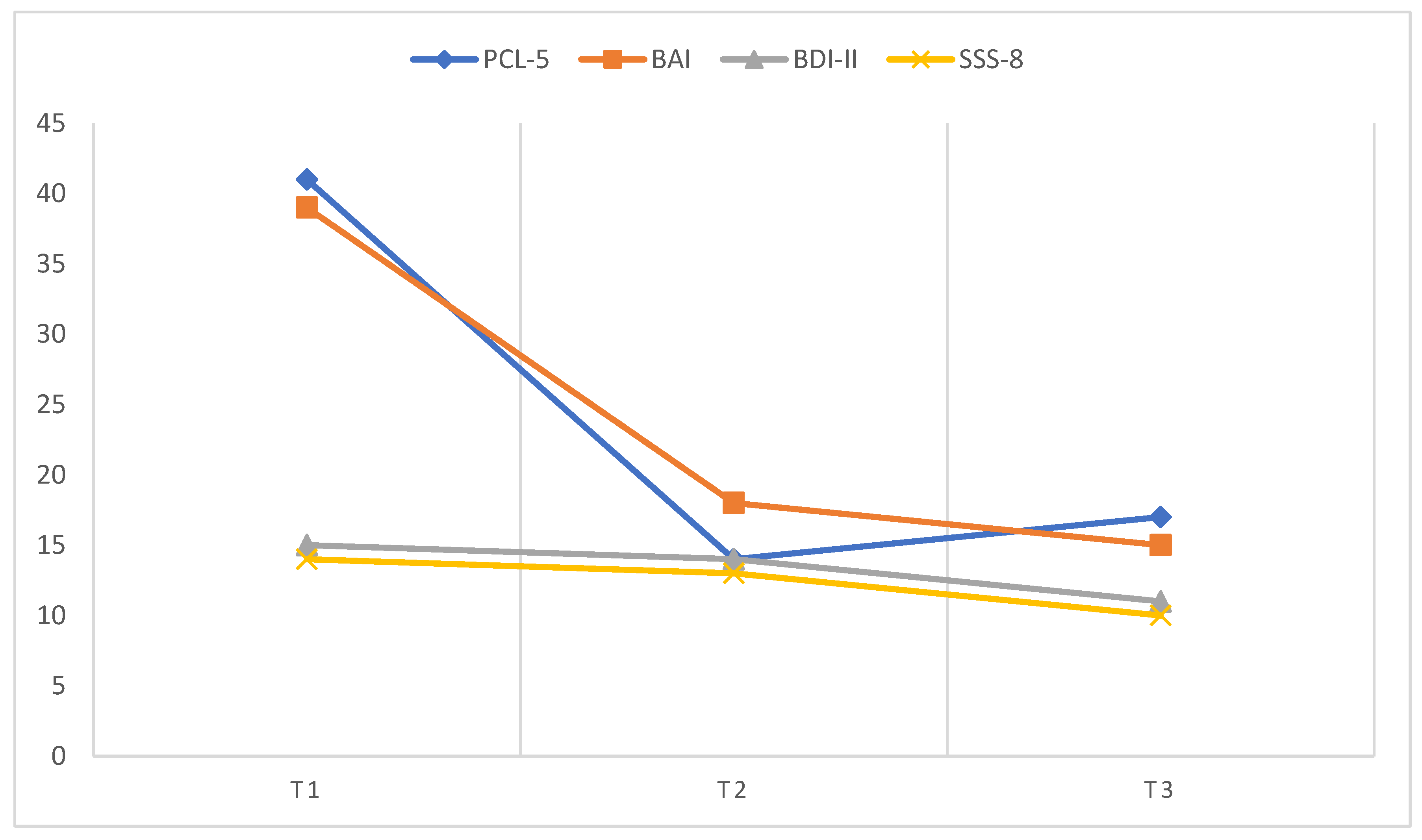
At this stage, the pre-treatment assessments are conducted (T1). In the PCL-5, the individual shows 5 confirmed symptoms of Cluster A, 1 symptom of Cluster B, 2 symptoms of Cluster C, and 7 symptoms of Cluster D, resulting in an overall score of 41 which surpasses the cut-off (31-33) for PTSD diagnosis. Additional assessments yielded the following scores: 39 on the BAI, indicating severe anxiety; 15 on the BDI-II, falling below the threshold for considering the presence of depressive symptoms; and 14 on the SSS-8, signifying a high level of discomfort.
The first meeting with user Z. begins with a compassionate and reassuring reception. The therapist encourages the user to freely share their story and uses reflective listening to understand the origins of their psychological issues. This helps establish a therapeutic relationship based on safety, trust, and transparency. The user explains how their work-related accident has led to symptoms of avoidance, insomnia, and nightmares. After allowing the user to express themselves freely for some time, the therapist explains how they will train for Neurofeedback.
Consequently, the researcher carefully provides for the assembly and delivery of tasks: "A video game will be projected into your HMD that will interact with your Alpha and Theta waves. Your goal in reaching a state of relaxed alertness will be to increase the alpha wave and reduce the theta wave. As you increase Alpha, Aladdin will fly higher and higher, while reducing Theta will turn Aladdin back. All you need to do is relax and breathe slowly”.
The user has responded positively to the intervention in various meetings (12 in total). Their Neurofeedback scores have shown an excellent learning curve, maintaining an average frequency of 7.02 Theta and 11.64 Alpha [3,41]. To help the user train to reach the desired cortical state, tips on using controlled breathing are also provided. At the end of each session, the SSQ is administered and has never highlighted significant adverse events.
One clinically interesting aspect that emerges from interviews conducted in the various meetings is the link between anxiety symptoms and poor perception of social support. The Z. user’s work injury is not itself indicative of a possible psychological trauma. It is a normal fall accident. However, this incident is part of a larger family narrative. During the same period, Z.’s husband also experienced a similar accident. This has led to significant challenges in managing their children, which is linked to recurring nightmares of not being able to "do everything that is necessary," and maintaining the household. Moreover, Z. has mentioned difficulties in seeking help from their social support network, which exacerbates feelings of social isolation.
Based on these elements we work on the user’s empowerment capacity and its self-efficacy. We also provide a psychoeducation on the importance of overcoming "shame" in seeking help from the extended socio-family system. In the meetings, it is recommended to try to replicate the modulations of the Neurofeedback - without this crutch - even when experiencing an increase in arousal and anxiety symptoms in daily life.
Over time, the user reports a significant reduction in anxiety symptoms. In the last meeting, post-treatment measures are taken (T2). The PCL-5 score is 14, indicating a remarkable improvement and no diagnosis of PTSD. The BAI shows a change from severe to moderate anxiety (39 to 18). The BDI-II score remains unchanged at 14, while SSS-8 indicates continued high levels of discouragement with a score of 13. It must be contextualized, however, that the user has undergone surgery following the accident with the application of a metal plate, which gives a physical discomfort in which one cannot intervene psychologically.
Based on the analysis of the patient’s accounts, test results, and EEG trace, it appears that the patient has significantly improved from the initial diagnosis. In a short patient satisfaction questionnaire (PSQ), the user expressed tangible benefits from the intervention and recommended the treatment to other users.
After 6 months, the user is contacted to perform a follow-up (T3). The extrapolated data show results similar to those obtained in T2, demonstrating the stability of the intervention over time. User Z reports no longer suffering from nightmares or further symptoms of avoiding the workplace when it is fully operational again.
We greet each other with good wishes for the future.

Table 1.
Comparison of results from T1 to T3.
| Measures | T1 | T2 | T3 |
|---|---|---|---|
| PCL-5 | 41 | 14 | 17 |
| BAI | 39 | 18 | 15 |
| BDI-II | 15 | 14 | 11 |
| SSS-8 | 14 | 13 | 10 |
Figure 5.
Graphical representation of improvement curve.
4. Discussion
According to our research results, the combination of VR-mediated Neurofeedback and Trauma-Informed Motivational Interviewing has shown promising preliminary results. There was a clinically significant reduction in psychometric measurements that showed a considerable level of severity such as PCL-5 and BAI. SSQ has never produced significant adverse events of clinical attention. Furthermore, the comparison with the analysis of the EEG path pre-treatment and post-treatment is more stable (Average pre-treatment frequencies = 5,73 Theta 4,91 Alpha/ Post-treatment frequencies = 7,02 Theta 11,64 Alpha), with a positive learning curve at the desired frequencies. With the passing of the meetings, the achievement of the cortical activation state has been faster and immediate, testifying to the learning and stability of the same over time. Consistent with the initial hypotheses, Neurofeedback is a viable treatment alternative for those users who are not willing to relive the trauma experience. The implementation of Trauma-Informed Motivational Interviewing alongside the Digital Tool has allowed a qualitative intervention that explored the user’s disadaptive thoughts and beliefs, promoting a positive and more adaptive cognitive restructuring. Integration with TIMI has been emphasized In addition, the importance of considering the Digital Tools not as instruments that replace the therapist but rather as instruments to be integrated into clinical practice where the therapist continues to cultivate human contact with the patient creating a dynamic dialogue between Classical psychotherapy and new technologies. The TIMINB protocol is a highly cost-effective intervention with no collateral risk, apart from the "possible failure to function." Although the initial results were promising, the study has clear limitations that need to be acknowledged. Firstly, our single-case design only allows for a qualitative analysis, limiting the ability to establish clear causal relationships and draw broad correlations. In other words, our case report provides valuable insight into the complexity of the mental health system, but it cannot be generalized to other users. Additionally, we encountered an issue with the visual quality of the Neurofeedback Videogame, which failed to meet the photorealism necessary for maintaining a high sense of presence. The video game comprised very static tasks, leading to some boredom during the latest sessions. Lastly, a specific practical problem was the conductive paste used to connect the electrodes with the user’s skin, requiring the user to wash their hair after each use. This posed significant operational challenges, particularly for users who couldn’t immediately return home, with a particular impact on women.
5. Conclusions
This case report provides for the first time a detailed insight into the effectiveness of a treatment combined with Neurofeedback, Virtual Reality, and Trauma-Informed Motivational Interviewing. The protocol has been effective in recovering mental well-being following an accident in one’s work environment. This case report also confirms the importance of integrating new technologies into clinical practice, overcoming the resistance of those who statically implement only digital tools and those who reject technology in its entirety [15,16,61]. The hope is to conduct a randomized controlled study based on these findings to confirm and generalize the results. Future research should focus on developing highly engaging and gamified video games that can be modulated with Neurofeedback. The goal is to create a modular video game with Neurofeedback, structured into chapters representing various encounters, and designed with the input of mental health professionals.
This could be an innovative approach in the field of Cyberpsychology and psychological therapies, leading to improved patient compliance. This is the line drawn for offering effective, low-cost, and side-effect-free interventions.
Author Contributions
Conceptualization: P.C . , S.T. , M.C. |Methodology: P.C . , S.T. , M.C. | Formal analysis, S.T., E.U. , P.C. | Investigation, S.T., E.U. , P.C. | Data curation, S.T., P.C. | Writing—original draft preparation: P.C . , S.T. , M.C. | Writing—review and editing: P.C . , S.T. , M.C., E.U., N.M.V. , A.F.| Visualization: S.T., M.C. | Supervision: P.C. , V.R. , A.F.| Project administration: P.C.Funding: This research received no external funding.
Institutional Review Board Statement
Institutional Review Board Statement: The University of Catania’s Internal Ethics Review Board of Psychology Research (IERB) has been informed of the research. Since it is a case report inherent to clinical practice and without invasive therapies, no formal approval is required. Specifically, The patient provided informed consent for the writing and anonymous publication of the report according to CARE guidelines, that no require institutional review board ethics consent is not applicable. (https://www.care-statement.org/checklist, accessed on 29 September 2024).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The detailed presented data are available upon request from the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Tolin, D.F.; Davies, C.D.; Moskow, D.M.; Hofmann, S.G. Biofeedback and Neurofeedback for Anxiety Disorders: A Quantitative and Qualitative Systematic Review. In Anxiety Disorders; Kim, Y.-K., Ed.; Advances in Experimental Medicine and Biology; Springer Singapore: Singapore, 2020; ISBN 978-981-329-704-3. [Google Scholar]
- Asioli, F.; Fioritti, A. Elettroshock (ESK) and Electroconvulsive Therapy (ECT). Epidemiol. Psichiatr. Soc. 2000, 9, 99–102. [Google Scholar] [CrossRef] [PubMed]
- Sebern F Fisher Neurofeedback Nel Trattamento Dei Traumi Dello Sviluppo; Raffaello Cortina Editore, 2017.
- Micoulaud-Franchi, J.A.; Jeunet, C.; Pelissolo, A.; Ros, T. EEG Neurofeedback for Anxiety Disorders and Post-Traumatic Stress Disorders: A Blueprint for a Promising Brain-Based Therapy. Curr. Psychiatry Rep. 2021, 23, 84. [Google Scholar] [CrossRef] [PubMed]
- Bergmann, A.; Edelhoff, D.; Schubert, O.; Erdelt, K.-J.; Pho Duc, J.-M. Effect of Treatment with a Full-Occlusion Biofeedback Splint on Sleep Bruxism and TMD Pain: A Randomized Controlled Clinical Trial. Clin. Oral Investig. 2020, 24, 4005–4018. [Google Scholar] [CrossRef] [PubMed]
- Enriquez-Geppert, S.; Smit, D.; Pimenta, M.G.; Arns, M. Neurofeedback as a Treatment Intervention in ADHD: Current Evidence and Practice. Curr. Psychiatry Rep. 2019, 21, 46. [Google Scholar] [CrossRef]
- Chiba, T.; Kanazawa, T.; Koizumi, A.; Ide, K.; Taschereau-Dumouchel, V.; Boku, S.; Hishimoto, A.; Shirakawa, M.; Sora, I.; Lau, H.; et al. Current Status of Neurofeedback for Post-Traumatic Stress Disorder: A Systematic Review and the Possibility of Decoded Neurofeedback. Front. Hum. Neurosci. 2019, 13, 233. [Google Scholar] [CrossRef]
- McLean, C.P.; Levy, H.C.; Miller, M.L.; Tolin, D.F. Exposure Therapy for PTSD: A Meta-Analysis. Clin. Psychol. Rev. 2022, 91, 102115. [Google Scholar] [CrossRef]
- Steingrimsson, S.; Bilonic, G.; Ekelund, A.-C.; Larson, T.; Stadig, I.; Svensson, M.; Vukovic, I.S.; Wartenberg, C.; Wrede, O.; Bernhardsson, S. Electroencephalography-Based Neurofeedback as Treatment for Post-Traumatic Stress Disorder: A Systematic Review and Meta-Analysis. Eur. Psychiatry 2020, 63, e7. [Google Scholar] [CrossRef]
- American Psychiatric Association Diagnostic and Statistical Manual of Mental Disorders; DSM-5-TR.; American Psychiatric Association Publishing, 2022; ISBN 978-0-89042-575-6.
- Bradley, R.; Greene, J.; Russ, E.; Dutra, L.; Westen, D. A Multidimensional Meta-Analysis of Psychotherapy for PTSD. Am. J. Psychiatry 2005, 162, 214–227. [Google Scholar] [CrossRef]
- Cusack, K.; Jonas, D.E.; Forneris, C.A.; Wines, C.; Sonis, J.; Middleton, J.C.; Feltner, C.; Brownley, K.A.; Olmsted, K.R.; Greenblatt, A.; et al. Psychological Treatments for Adults with Posttraumatic Stress Disorder: A Systematic Review and Meta-Analysis. Clin. Psychol. Rev. 2016, 43, 128–141. [Google Scholar] [CrossRef]
- Hoppen, T.H.; Jehn, M.; Holling, H.; Mutz, J.; Kip, A.; Morina, N. The Efficacy and Acceptability of Psychological Interventions for Adult PTSD: A Network and Pairwise Meta-Analysis of Randomized Controlled Trials. J. Consult. Clin. Psychol. 2023, 91, 445–461. [Google Scholar] [CrossRef]
- Karatzias, T.; Murphy, P.; Cloitre, M.; Bisson, J.; Roberts, N.; Shevlin, M.; Hyland, P.; Maercker, A.; Ben-Ezra, M.; Coventry, P.; et al. Psychological Interventions for ICD-11 Complex PTSD Symptoms: Systematic Review and Meta-Analysis. Psychol. Med. 2019, 49, 1761–1775. [Google Scholar] [CrossRef] [PubMed]
- Caponnetto, P.; Triscari, S.; Maglia, M.; Quattropani, M.C. The Simulation Game—Virtual Reality Therapy for the Treatment of Social Anxiety Disorder: A Systematic Review. Int. J. Environ. Res. Public. Health 2021, 18, 13209. [Google Scholar] [CrossRef] [PubMed]
- Caponnetto, P.; Casu, M. Update on Cyber Health Psychology: Virtual Reality and Mobile Health Tools in Psychotherapy, Clinical Rehabilitation, and Addiction Treatment. Int. J. Environ. Res. Public. Health 2022, 19, 3516. [Google Scholar] [CrossRef]
- Rudolph, K. Ethical Considerations in Trauma-Informed Care. Psychiatr. Clin. North Am. 2021, 44, 521–535. [Google Scholar] [CrossRef] [PubMed]
- Doppelmayr, M.; Weber, E. Effects of SMR and Theta/Beta Neurofeedback on Reaction Times, Spatial Abilities, and Creativity. J. Neurother. 2011, 15, 115–129. [Google Scholar] [CrossRef]
- Marzbani, H.; Marateb, H.; Mansourian, M. Methodological Note: Neurofeedback: A Comprehensive Review on System Design, Methodology and Clinical Applications. Basic Clin. Neurosci. J. 2016, 7. [Google Scholar] [CrossRef]
- Riva, G.; Baños, R.M.; Botella, C.; Mantovani, F.; Gaggioli, A. Transforming Experience: The Potential of Augmented Reality and Virtual Reality for Enhancing Personal and Clinical Change. Front. Psychiatry 2016, 7. [Google Scholar] [CrossRef]
- Bouchard, S.; Dumoulin, S.; Robillard, G.; Guitard, T.; Klinger, É.; Forget, H.; Loranger, C.; Roucaut, F.X. Virtual Reality Compared with in Vivo Exposure in the Treatment of Social Anxiety Disorder: A Three-Arm Randomised Controlled Trial. Br. J. Psychiatry 2017, 210, 276–283. [Google Scholar] [CrossRef]
- Bellotti, F.; Berta, R.; De Gloria, A. Games and Learning Alliance (GaLA) Supporting Education and Training through Hi-Tech Gaming. In Proceedings of the 2012 IEEE 12th International Conference on Advanced Learning Technologies; IEEE: Rome, Italy, July 2012; pp. 740–741.
- Diaz Hernandez, L.; Rieger, K.; Koenig, T. Low Motivational Incongruence Predicts Successful EEG Resting-State Neurofeedback Performance in Healthy Adults. Neuroscience 2018, 378, 146–154. [Google Scholar] [CrossRef]
- Kleih, S.C.; Nijboer, F.; Halder, S.; Kübler, A. Motivation Modulates the P300 Amplitude during Brain–Computer Interface Use. Clin. Neurophysiol. 2010, 121, 1023–1031. [Google Scholar] [CrossRef]
- Nijboer, F.; Furdea, A.; Gunst, I.; Mellinger, J.; McFarland, D.J.; Birbaumer, N.; Kübler, A. An Auditory Brain–Computer Interface (BCI). J. Neurosci. Methods 2008, 167, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Larsen, S.E.; Bellmore, A.; Gobin, R.L.; Holens, P.; Lawrence, K.A.; Pacella-LaBarbara, M.L. An Initial Review of Residual Symptoms after Empirically Supported Trauma-Focused Cognitive Behavioral Psychological Treatment. J. Anxiety Disord. 2019, 63, 26–35. [Google Scholar] [CrossRef] [PubMed]
- Mendel, W.E.; Sperlich, M.; Fava, N.M. “Is There Anything Else You Would like Me to Know?”: Applying a Trauma-informed Approach to the Administration of the Adverse Childhood Experiences Questionnaire. J. Community Psychol. 2021, 49, 1079–1099. [Google Scholar] [CrossRef] [PubMed]
- Martins, R.K.; McNeil, D.W. Review of Motivational Interviewing in Promoting Health Behaviors. Clin. Psychol. Rev. 2009, 29, 283–293. [Google Scholar] [CrossRef]
- Champine, R.B.; Lang, J.M.; Nelson, A.M.; Hanson, R.F.; Tebes, J.K. Systems Measures of a Trauma-Informed Approach: A Systematic Review. Am. J. Community Psychol. 2019, 64, 418–437. [Google Scholar] [CrossRef]
- Counts, J.M.; Gillam, R.J.; Perico, S.; Eggers, K.L. Lemonade for Life—A Pilot Study on a Hope-Infused, Trauma-Informed Approach to Help Families Understand Their Past and Focus on the Future. Child. Youth Serv. Rev. 2017, 79, 228–234. [Google Scholar] [CrossRef]
- Rollnick, S.; Miller, W.R. What Is Motivational Interviewing? Behav. Cogn. Psychother. 1995, 23, 325–334. [Google Scholar] [CrossRef]
- Lee, W.; Lee, Y.-R.; Yoon, J.-H.; Lee, H.-J.; Kang, M.-Y. Occupational Post-Traumatic Stress Disorder: An Updated Systematic Review. BMC Public Health 2020, 20, 768. [Google Scholar] [CrossRef]
- Brennan, C.J.; Roberts, C.; Cole, J.C. Prevalence of Occupational Moral Injury and Post-Traumatic Embitterment Disorder: A Systematic Review and Meta-Analysis. BMJ Open 2024, 14, e071776. [Google Scholar] [CrossRef]
- Zhu, H.; Yang, X.; Xie, S.; Zhou, J. Prevalence of Burnout and Mental Health Problems among Medical Staff during the COVID-19 Pandemic: A Systematic Review and Meta-Analysis. BMJ Open 2023, 13, e061945. [Google Scholar] [CrossRef]
- Ortega-Loubon, C.; Culquichicón, C.; Correa, R. The Importance of Writing and Publishing Case Reports During Medical Training. Cureus 2017. [Google Scholar] [CrossRef] [PubMed]
- Mohan, U.R.; Zhang, H.; Ermentrout, B.; Jacobs, J. The Direction of Theta and Alpha Travelling Waves Modulates Human Memory Processing. Nat. Hum. Behav. 2024. [Google Scholar] [CrossRef] [PubMed]
- Kamiya J Operant Control of the EEG Alpha Rhythm and Some of Its Reported Effects on Consciousness. 1969.
- Sanchez-Rodriguez, L.M.; Bezgin, G.; Carbonell, F.; Therriault, J.; Fernandez-Arias, J.; Servaes, S.; Rahmouni, N.; Tissot, C.; Stevenson, J.; Karikari, T.K.; et al. Personalized Whole-Brain Neural Mass Models Reveal Combined Aβ and Tau Hyperexcitable Influences in Alzheimer’s Disease. Commun. Biol. 2024, 7, 528. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.-J.; Kim, H.-G.; Cheon, E.-J.; Kim, K.; Choi, J.-H.; Kim, J.-Y.; Kim, J.-M.; Koo, B.-H. The Analysis of Electroencephalography Changes Before and After a Single Neurofeedback Alpha/Theta Training Session in University Students. Appl. Psychophysiol. Biofeedback 2019, 44, 173–184. [Google Scholar] [CrossRef]
- Rodriguez-Larios, J.; Alaerts, K. EEG Alpha–Theta Dynamics during Mind Wandering in the Context of Breath Focus Meditation: An Experience Sampling Approach with Novice Meditation Practitioners. Eur. J. Neurosci. 2021, 53, 1855–1868. [Google Scholar] [CrossRef]
- Gruzelier, J. A Theory of Alpha/Theta Neurofeedback, Creative Performance Enhancement, Long Distance Functional Connectivity and Psychological Integration. Cogn. Process. 2009, 10, 101–109. [Google Scholar] [CrossRef]
- Bonança, G.M.; Gerhardt, G.J.L.; Molan, A.L.; Oliveira, L.M.A.; Jarola, G.M.; Schönwald, S.V.; Rybarczyk-Filho, J.L. EEG Alpha and Theta Time-Frequency Structure during a Written Mathematical Task. Med. Biol. Eng. Comput. 2024, 62, 1869–1885. [Google Scholar] [CrossRef]
- Torre, M.A.L. Touch and Psychotherapy. Perspect. Psychiatr. Care 2009, 36, 105–106. [Google Scholar] [CrossRef]
- Goldstein, E.; Topitzes, J.; Benton, S.F.; Sarino, K.P. Evaluation of a Motivation-Based Intervention to Reduce Health Risk Behaviors among Black Primary Care Patients with Adverse Childhood Experiences. Perm. J. 2020, 24, 19–233. [Google Scholar] [CrossRef]
- Shabani, A.; Masoumian, S.; Zamirinejad, S.; Hejri, M.; Pirmorad, T.; Yaghmaeezadeh, H. Psychometric Properties of Structured Clinical Interview for DSM-5 Disorders-Clinician Version (SCID-5-CV). Brain Behav. 2021, 11, e01894. [Google Scholar] [CrossRef]
- Blevins, C.A.; Weathers, F.W.; Davis, M.T.; Witte, T.K.; Domino, J.L. The Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5): Development and Initial Psychometric Evaluation. J. Trauma. Stress 2015, 28, 489–498. [Google Scholar] [CrossRef] [PubMed]
- Bovin, M.J.; Marx, B.P.; Weathers, F.W.; Gallagher, M.W.; Rodriguez, P.; Schnurr, P.P.; Keane, T.M. Psychometric Properties of the PTSD Checklist for Diagnostic and Statistical Manual of Mental Disorders–Fifth Edition (PCL-5) in Veterans. Psychol. Assess. 2016, 28, 1379–1391. [Google Scholar] [CrossRef] [PubMed]
- Wortmann, J.H.; Jordan, A.H.; Weathers, F.W.; Resick, P.A.; Dondanville, K.A.; Hall-Clark, B.; Foa, E.B.; Young-McCaughan, S.; Yarvis, J.S.; Hembree, E.A.; et al. Psychometric Analysis of the PTSD Checklist-5 (PCL-5) among Treatment-Seeking Military Service Members. Psychol. Assess. 2016, 28, 1392–1403. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.T.; Epstein, N.; Brown, G.; Steer, R. Beck Anxiety Inventory 2012.
- Leyfer, O.T.; Ruberg, J.L.; Woodruff-Borden, J. Examination of the Utility of the Beck Anxiety Inventory and Its Factors as a Screener for Anxiety Disorders. J. Anxiety Disord. 2006, 20, 444–458. [Google Scholar] [CrossRef]
- Halfaker, D.A.; Akeson, S.T.; Hathcock, D.R.; Mattson, C.; Wunderlich, T.L. Psychological Aspects of Pain. In Pain Procedures in Clinical Practice; Elsevier, 2011; pp. 13–22 ISBN 978-1-4160-3779-8.
- Beck A.T.; R.A., S.; Brown G. Beck Depression Inventory–II. Psychological assessment 1996.
- Wang, Y.-P.; Gorenstein, C. Psychometric Properties of the Beck Depression Inventory-II: A Comprehensive Review. Rev. Bras. Psiquiatr. 2013, 35, 416–431. [Google Scholar] [CrossRef]
- Astill Wright, L.; Roberts, N.P.; Barawi, K.; Simon, N.; Zammit, S.; McElroy, E.; Bisson, J.I. Disturbed Sleep Connects Symptoms of Posttraumatic Stress Disorder and Somatization: A Network Analysis Approach. J. Trauma. Stress 2021, 34, 375–383. [Google Scholar] [CrossRef]
- Gierk, B.; Kohlmann, S.; Kroenke, K.; Spangenberg, L.; Zenger, M.; Brähler, E.; Löwe, B. The Somatic Symptom Scale–8 (SSS-8): A Brief Measure of Somatic Symptom Burden. JAMA Intern. Med. 2014, 174, 399. [Google Scholar] [CrossRef]
- Bouchard; St-Jacques; Renaud; Wiederhold SIde effectS of ImmerSIonS In vIrtual realIty for People SufferIng from anxIety dISorderS. J. CyberTherapy Rehabil. 2009, 2.
- Martirosov, S.; Bureš, M.; Zítka, T. Cyber Sickness in Low-Immersive, Semi-Immersive, and Fully Immersive Virtual Reality. Virtual Real. 2022, 26, 15–32. [Google Scholar] [CrossRef]
- Kennedy, R.S.; Lane, N.E.; Berbaum, K.S.; Lilienthal, M.G. Simulator Sickness Questionnaire: An Enhanced Method for Quantifying Simulator Sickness. Int. J. Aviat. Psychol. 1993, 3, 203–220. [Google Scholar] [CrossRef]
- Bimberg, P.; Weissker, T.; Kulik, A. On the Usage of the Simulator Sickness Questionnaire for Virtual Reality Research. In Proceedings of the 2020 IEEE Conference on Virtual Reality and 3D User Interfaces Abstracts and Workshops (VRW); IEEE: Atlanta, GA, USA, March 2020; pp. 464–467.
- Markiewcz, R. The Use of EEG Biofeedback/Neurofeedback in Psychiatric Rehabilitation. Psychiatr. Pol. 2017, 51, 1095–1106. [Google Scholar] [CrossRef]
- Casu, M.; Triscari, S.; Battiato, S.; Guarnera, L.; Caponnetto, P. AI Chatbots for Mental Health: A Scoping Review of Effectiveness, Feasibility, and Applications. Appl. Sci. 2024, 14, 5889. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



