
Submitted:
22 October 2024
Posted:
23 October 2024
You are already at the latest version
Abstract
Background and Objective: Obtaining reliable and up-to-date information on mortality causes is essential for planning and implementation of effective preventive interventions. We present here an analysis of the leading causes of death in the US in 2022. Material and Methods: We conducted an electronic search of the US Centers for Control and Prevention (CDC) Web-based Injury Statistics Query and Reporting System (WISQARS) to obtain information on the leading causes of death in the US for the most recent searchable year (2022), stratified by age and sex. Results: Overall, heart disease was the leading cause of death (26.2% of all deaths), followed by malignant neoplasms (22.7%), unintentional injuries (8.5%) and coronavirus disease 2019 (COVID-19; 6.9%). Although heart disease and malignant neoplasms remained the leading causes of death in both sexes, unintentional injuries were the third cause for men (10.5%), while strokes were the third cause in women (7.5%). COVID-19 remained the fourth most common cause of death in both sexes (7.1% in men and 6.8% in women). The ten most common causes of death showed an increasing mortality tendency in parallel with the aging of population, with similar trends for both sexes. The only exception was unintentional injury, which was the most common cause of death in both sexes between the ages of 15 and 44 years, then reached a plateau, for increasing again in people aged 65 years or older. Conclusions: Greater efforts should be put into prevention and education, as heart disease, cancer and even unintentional injuries are preventable diseases.
Keywords:
Mortality
; Epidemiology
; Statistics
Introduction
Reliable and up-to-date statistics on mortality in the general population are crucial for several reasons. First, they can support public health planning and policy making by helping governments and health organizations to better allocate resources in areas with higher mortality rates or where certain causes of death are more common [1]. The identification of mortality trends and causes also makes it possible to plan tailored health interventions and programs to address specific health needs and for monitoring actual effectiveness of public health interventions and efficiency of healthcare services [2]. In particular, healthcare planning and resource allocation (e.g., number and location of healthcare facilities, number of beds in hospitals and/or intensive care units, amount of medical and paramedical staff, funding, etc.), can be provided in areas of higher needs.
The analysis of risk factors is another important aspect that can benefit from updated mortality statistics, as these data support the investigation of causal relationships between mortality and biological, lifestyle or even environmental risk factors, paving the way for development of effective preventive measures [3]. Accurate mortality data is then essential for predicting demographic changes, which can impact economic planning, social service delivery and infrastructure development [4], but is also very useful when it comes to addressing health inequalities, especially for highlighting disparities between different populations (e.g., by age, sex, ethnicity, socioeconomic status, geographic location), thus providing useful insights for providing a more equitable healthcare [5]. Last but not least, an accurate analysis of the leading causes of death enables the comparison between different continents, nations, and other geographic areas, which helps reflecting global health trends and identifying health practices or behaviors associated with fewer mortality from a given disease in a certain geographical location, as well as driving clinical practice and research priorities [6].
The crisis triggered by the recent and still unresolved coronavirus disease 2019 (COVID-19) pandemic has clearly demonstrated the unpreparedness and vulnerability of most (if not all) healthcare systems globally [7,8], highlighting notable gaps in response capabilities and supply chain vulnerabilities, but also disproportionately affecting marginalized countries and/or communities, in particular frail, co-morbid or elderly patients who experienced significantly higher infection rates, more severe disease trajectories and disproportionately high mortality. This also applies to racial and ethnic minorities, who very often did not have sufficient access to preventive measures (i.e., personal protective equipment, especially face masks), treatments and vaccines [9].
It is hence clear that obtaining reliable and updated information on mortality and, especially, on the most frequent causes of death, is now unavoidable for planning and delivering effective clinical, social and even economic policies. To this end, we aim to provide here the most recent statistics on the leading causes of death in the US.
Materials and Methods
We conducted an electronic search of the US Centers for Control and Prevention (CDC) WISQARS (Web-based Injury Statistics Query and Reporting System) database [10], an interactive collection of modules containing official fatal and nonfatal statistics and injury cost data from a variety of reliable sources such as the US National Vital Statistics System (NVSS), which collects and compiles nationwide data on births, deaths, marriages, divorces and fetal deaths from vital records offices, as well as the death certificates which contain detailed information on cause of death, demographics (e.g., sex, age, ethnicity), and geographic location. The causes of death are coded using the International Classification of Diseases 10th Revision (ICD-10), a standardized coding system officially endorsed by the World Health Organization (WHO). All data are systematically reviewed by the National Center for Health Statistics (NCHS) to ensure their consistency and accuracy. The user can access the WISQARS online resource for making specific queries according to age, sex, ethnicity and geographical location [10]. The database is updated regularly with the latest available data, to provide the most recent information (the last searchable statistics on mortality are those for the year 2022). The main purpose of the database is supporting epidemiological and clinical research aimed at investigating and attenuating the leading causes of death [10].
We specifically searched the leading causes of death in the US, using data filters as follows: data years: “2022” (i.e., the last searchable year); number of causes: “20 intent of injury” AND “all deaths with drilldown to ICD codes”; Geography: “United States”; Age group format: “1-14 in 5-year groups; 15-65+ in 10-year groups”; Sex: “Both” AND “Males” AND “Females”; Race: “All races ethnicity”. The data was downloaded as a CSV (comma-separated value) file, converted into columns and finally transferred to an Excel spreadsheet, where it was analyzed graphically. This study was exempt from institutional review board review because CDC WISQARS is an anonymized and publicly accessible database.
Results
The results of our study, which are limited to the ten most common causes of death in 2022, are summarized in Figure 1. Heart disease was the leading cause of death in the US, accounting for an average of 702,880 deaths (26.2% of all deaths), followed by malignant neoplasms (608,371 deaths; 22.7%), unintentional injuries (227,039 deaths; 8.5%) and COVID-19 (186,552 deaths; 6.9%). We found some differences between men and women; although heart disease (26.8% of all deaths for men and 25.4% for women) and malignant neoplasms (22.1% of all deaths for men and 23.3% for women) remained the leading causes of death for both sexes, unintentional injuries were the third leading cause of death for men (10.5% of all deaths), while strokes were the third leading cause of death for women (7.5% of all deaths). Notably, COVID-19 was still the fourth leading cause of death for both sexes (7.1% for men and 6.8% for women). The only sex differences in the list of the 10 leading causes of death were suicide (8th cause of death in men) and hypertension (10th cause of death in women).
The cumulative and sex-specific age distribution of the number of deaths in the US in 2022 is shown in Figure 1. The ten leading causes of death show an increasing trend parallel to the aging of the population, which is similar for both males (Figure 2) and females (Figure 3). The only exception was mortality for unintentional injuries, whose curve exhibited a sudden increase after the age of 10 years and became the leading cause of death between the ages of 15 and 44 years for both sexes, then reached a plateau followed by a further increase in those aged 65 years or older. An almost identical trend was observed for male suicides, with a peak between the ages of 35 and 44 years, followed by a plateau that continued into the older age cohort. In both sexes, mortality from Alzheimer’s disease became relevant after the age of 60 years and continued to rise thereafter, becoming the 5th causes of death in very old women and the ninth causes of death in very old men.
Discussion
There is no question that analyzing mortality data is a fundamental tool for improving public health, driving policy decisions, advancing scientific research, enabling social justice, and ultimately improving population well-being [11]. The purpose of our analysis is exactly in line with these concepts, as we aim to provide here the most up-to-date data on mortality in the US, one of the most important and representative countries in the world. The main strength of our study lies in the source of information, as the mortality data generated by our search using the WISQARS Leading Causes of Death Visualization Tool are obtained from the NVSS and death certificates, standardized using ICD-10 coding, and further processed by the NCHS. Taken together, this process provides reliable, up-to-date information on mortality trends and causes of death that can be useful for supporting a variety of public health, research and policy-making activities.
As summarized in Table 1, heart disease and cancer remained the leading causes of death in the US in 2022, echoing previously published data for 2015-2020 [12], when the leading causes of death were also heart disease, cancer, unintentional injuries and stroke, with the exception of the year 2020, when COVID-19 became the third leading cause of death in the US. Thus, four years into the COVID-19 pandemic, which has nearly revolutionized healthcare and society [13], the epidemiology of the cause of deaths in the US has remained nearly stable.
However, if we compare the number of deaths from heart disease and cancer between the years 2022 and 2020 [12], a modest increase can be noted for both (heart disease: 702,880 vs. 690,882, +1.7%; cancer: 608,371 vs. 598.932, +1.6%), while the mortality for COVID-19 has fallen by nearly half (354,323 vs. 186,552, -47.3%), surpassed in the 2022 list by unintentional injuries, whose mortality also increased remarkably between the years 2022 and 2020 (227,039 vs. 192,176, +18.1%). Regarding specifically heart disease, the modest but not meaningless increase can be attributed at least in part to the impact of the COVID-19 pandemic, as severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection is per se a trigger of myocardial ischemia and thrombosis [14]. The increase in cancer mortality is also a predictable phenomenon of the pandemic, as this has been accompanied by significant delays in cancer screening and cancer-related care [15]. As concerns unintentional injuries, our data are consistent with those recently presented in a systematic literature review that included 189 articles from many countries around the world [16], showing higher incidence of injuries/trauma (especially in men) during the pandemic. Notably, the increase relative to 2020 data can also be explained by a possible bias due to avoidance of referrals to healthcare facilities for overcrowding of emergency rooms and/or fear of infection during the initial period of the pandemic [17]. As then concerns the other causes of death, the mortality for stroke has recorded a slight increase between 2022 and 2020 (165,393 vs. 159,050, +4.0%), which can also be attributed to the greater prevalence of COVID-19 cases and the direct biological impact of SARS-CoV-2 on vascular ischemic disease. [18]. In contrast to the trend observed for the previous diseases, the 2022-2020 variation in mortality for chronic lower respiratory diseases was negative (147,382 vs. 151,637, -2.8%), as was that for Alzheimer's disease (120,122 vs. 151,637, -20.8%), although the figures for the latter case may be biased by the death of several older people in the first two years of the pandemic, which may have then contributed to reduce the overall mortality for Alzheimer's disease and other forms of dementia in 2022 [19]. Interestingly, the number of deaths for diabetes mellitus remained almost stable comparing the years 2022 and 2020 (101,209 vs. 101,106, +0.1%). Although the prevalence of diabetes has tended to increase during the pandemic [20], the almost unvaried mortality is not really surprising as it can take several years for diabetic complications to develop and become potentially fatal. It may therefore take years before the effects of an increased number of diabetes diagnoses recorded during the pandemic will translate into an increased diabetes-related mortality.
It is also worth noting that the cumulative number of suicides, which ranks 11th on the list of leading causes of death in the US in both 2022 and 2020, has also considerably increased by over 10% in the last two years (i.e., 49,476 vs. 44,834, +10.1%). This is also plausible given that a kaleidoscope of psychiatric illnesses (including depression) has increased significantly over the past three years for a variety of reasons, including direct biological injury to the brain from the virus, fear of disease, and the inevitable impact of societal restrictions that have severely limited personal freedom [21].
Conclusions
The results of our analysis confirm that heart disease, cancer, and unintentional injuries have remained the leading causes of death in the US in recent times. Therefore, reinforced efforts should be put into prevention and education, as heart disease, cancer and even unintentional injuries could be prevented by becoming aware of the risk of dying from these conditions and implementing effective lifestyle changes specifically focused on reducing the risk factors associated with these pathologies.
Competing interests
The author declares no conflicts of interest.
Acknowledgments
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
List of Abbreviations:
COVID-19, coronavirus disease 2019
CDC, Centers for Control and Prevention
WISQARS, Web-based Injury Statistics Query and Reporting System
ICD-10, International Classification of Diseases 10th Revision
WHO, World Health Organization
NCHS, National Center for Health Statistics
References
- Adair T, Mikkelsen L, Hooper J, et al., 2023, Assessing the policy utility of routine mortality statistics: a global classification of countries. Bull World Health Organ, 101(12): 777–785. [CrossRef]
- Kreuter MW, Thompson T, McQueen A, et al., 2021, Addressing Social Needs in Health Care Settings: Evidence, Challenges, and Opportunities for Public Health. Annu Rev Public Health, 42: 329–344. [CrossRef]
- Mehta NK, Zheng H, Myrskylä M. 2019, How do age and major risk factors for mortality interact over the life-course? Implications for health disparities research and public health policy. SSM Popul Health, 8: 100438. [CrossRef]
- Janssen F. 2018, Advances in mortality forecasting: introduction. Genus, 74(1): 21. [CrossRef]
- Fantini MP, Lenzi J, Franchino G, et al., 2014, Mortality amenable to health care services and health inequalities among Italian Regions. Epidemiol Prev, 38(2): 100–7.
- Nolte E, McKee M. 2003, Measuring the health of nations: analysis of mortality amenable to health care. BMJ, 327(7424): 1129. [CrossRef]
- Mattiuzzi C, Lippi G. 2020, Which lessons shall we learn from the 2019 novel coronavirus outbreak? Ann Transl Med, 8(3): 48.
- Filip R, Gheorghita Puscaselu R, Anchidin-Norocel L, et al. 2022, Global Challenges to Public Health Care Systems during the COVID-19 Pandemic: A Review of Pandemic Measures and Problems. J Pers Med, 12(8): 1295. [CrossRef]
- Foster TB, Fernandez L, Porter SR, et al., 2024, Racial and Ethnic Disparities in Excess All-Cause Mortality in the First Year of the COVID-19 Pandemic. Demography, 61(1): 59–85. [CrossRef]
- Centers for Disease Control and Prevention (CDC). 2024, WISQARS Leading Causes of Death Visualization Tool, viewed June 19, 2024, https://wisqars.cdc.gov/lcd/.
- Pollack Porter KM, Rutkow L, McGinty EE. 2018, The Importance of Policy Change for Addressing Public Health Problems. Public Health Rep, 133(1_suppl): 9S–14S. [CrossRef]
- Ahmad FB, Anderson RN. 2021, The Leading Causes of Death in the US for 2020. JAMA, 325(18): 1829–30. [CrossRef]
- Khalifa SAM, Swilam MM, El-Wahed AAA, et al., 2021, Beyond the Pandemic: COVID-19 Pandemic Changed the Face of Life. Int J Environ Res Public Health, 18(11): 5645. [CrossRef]
- Lippi G, Sanchis-Gomar F, Lavie CJ. 2024, Excess mortality for acute myocardial infarction in the United States during the first two years of the COVID-19 pandemic. Prog Cardiovasc Dis. 2024 Mar 20:S0033-0620(24)00051-3. Epub ahead of print. [CrossRef]
- Keim-Malpass J, Vavolizza RD, Cohn WF, et al., 2023 Cancer Screening and Treatment Delays During the COVID-19 Pandemic and the Role of Health Literacy in Care Re-engagement: Findings from an NCI-Designated Comprehensive Cancer Center sample. J Cancer Educ, 38(5): 1405–1412. [CrossRef]
- Karmali S, Saxena S, Richards O, et al., 2024, What was the impact of COVID-19 restrictions on unintentional injuries, in Canada and globally? A scoping review investigating how lockdown measures impacted the global burden of unintentional injury. Front Public Health, 12: 1385452. [CrossRef]
- Quercioli C, Bosco R, Bova G, et al., 2023, Evaluating the effect of COVID-19 incidence on Emergency Departments admissions. Results from a retrospective study in Central Italy during the first year of pandemic. Ann Ig, 35(5): 572–85. [CrossRef]
- Luo W, Liu X, Bao K, et al., 2022 Ischemic stroke associated with COVID-19: a systematic review and meta-analysis. J Neurol, 269(4): 1731–1740. [CrossRef]
- Sorrell JM. 2021, Losing a Generation: The Impact of COVID-19 on Older Americans. J Psychosoc Nurs Ment Health Serv, 59(4): 9–12. [CrossRef]
- Li R, Shen M, Yang Q, et al., 2023, Global Diabetes Prevalence in COVID-19 Patients and Contribution to COVID-19- Related Severity and Mortality: A Systematic Review and Meta-analysis. Diabetes Care, 46(4): 890–897. [CrossRef]
- Shetty PA, Ayari L, Madry J, et al., 2023, The Relationship Between COVID-19 and the Development of Depression: Implications on Mental Health. Neurosci Insights, 21; 18:26331055231191513. [CrossRef]
Figure 1.
Leading causes of death in the US, year 2022, obtained from the US Centers for Control and Prevention (CDC) WISQARS (Web-based Injury Statistics Query and Reporting System) database. Cumulative number.
Figure 1.
Leading causes of death in the US, year 2022, obtained from the US Centers for Control and Prevention (CDC) WISQARS (Web-based Injury Statistics Query and Reporting System) database. Cumulative number.
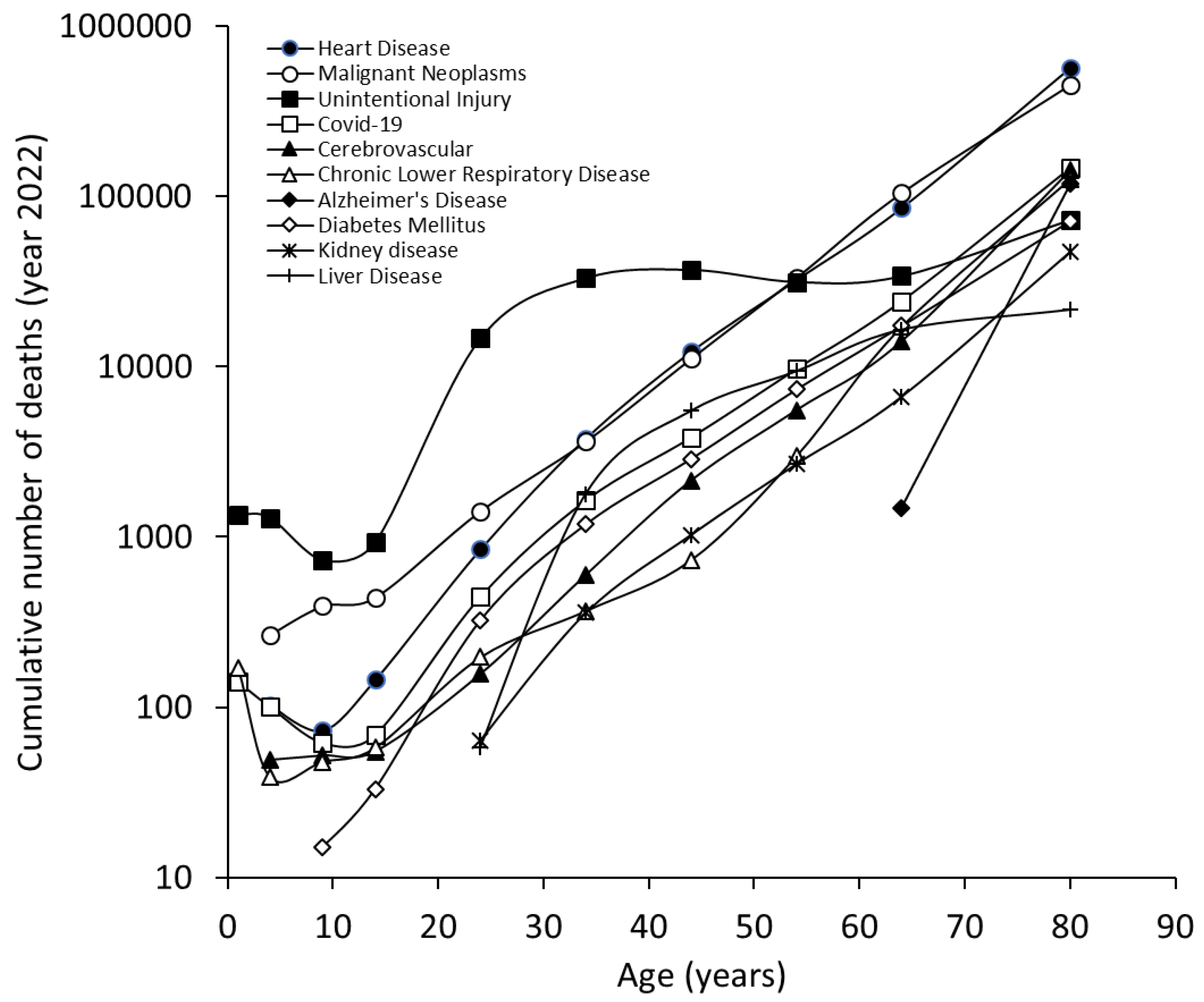
Figure 2.
Leading causes of death in the US, year 2022, in males, obtained from the US Centers for Control and Prevention (CDC) WISQARS (Web-based Injury Statistics Query and Reporting System) database.
Figure 2.
Leading causes of death in the US, year 2022, in males, obtained from the US Centers for Control and Prevention (CDC) WISQARS (Web-based Injury Statistics Query and Reporting System) database.
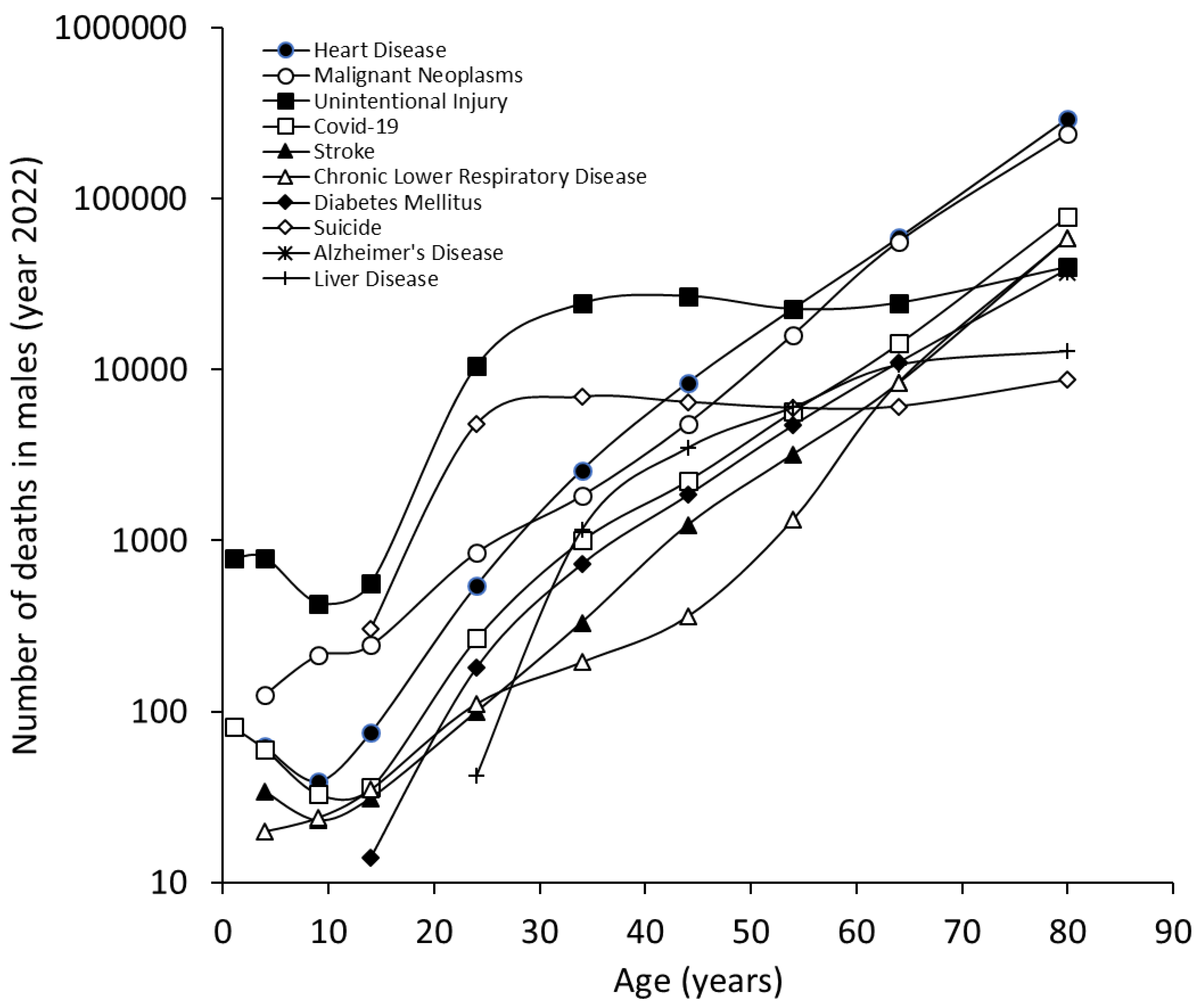
Figure 3.
Leading causes of death in the US, year 2022, in females, obtained from the US Centers for Control and Prevention (CDC) WISQARS (Web-based Injury Statistics Query and Reporting System) database. Cumulative number.
Figure 3.
Leading causes of death in the US, year 2022, in females, obtained from the US Centers for Control and Prevention (CDC) WISQARS (Web-based Injury Statistics Query and Reporting System) database. Cumulative number.
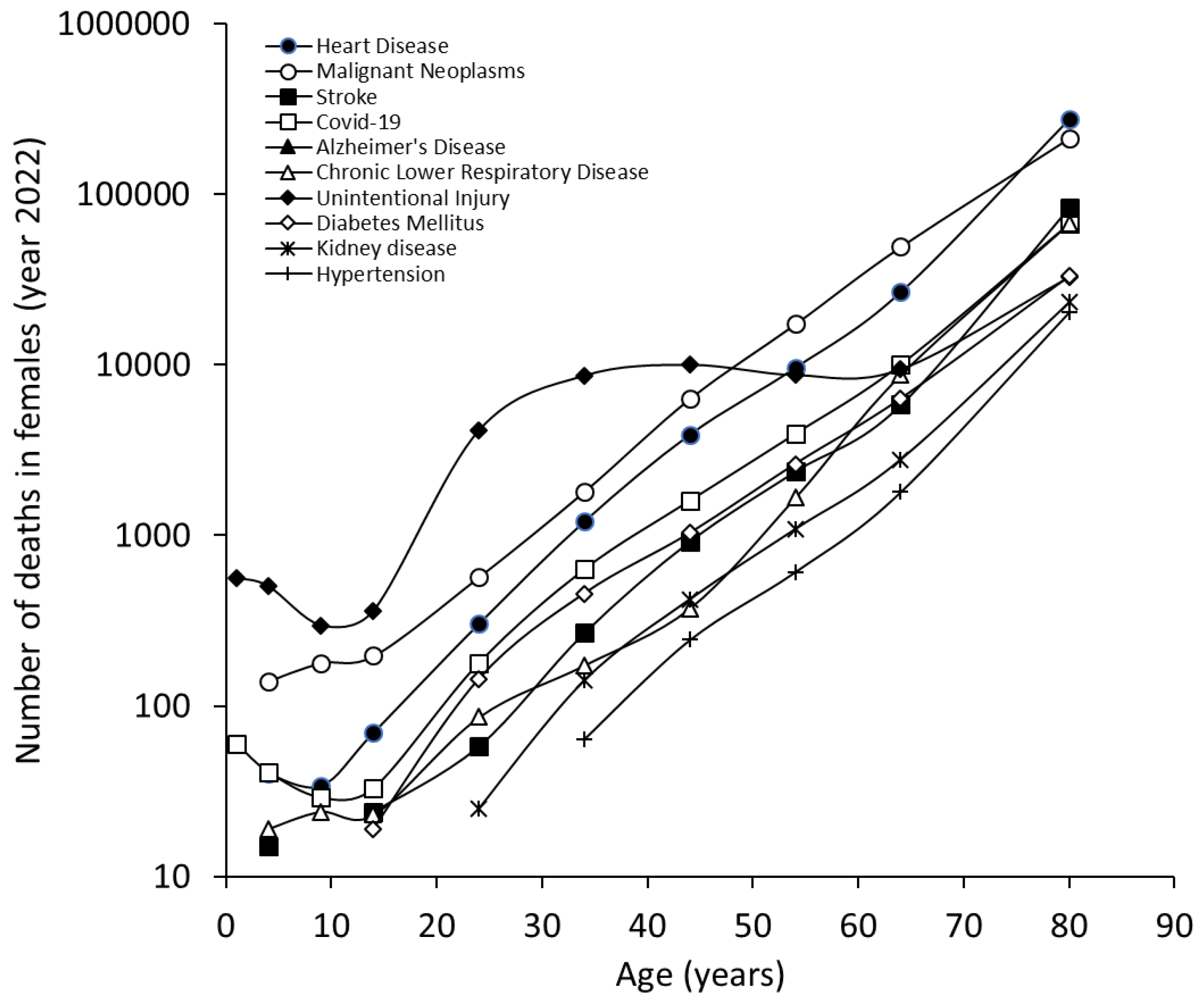

Table 1.
Leading causes of death in the US, year 2022, obtained from the US Centers for Control and Prevention (CDC) WISQARS (Web-based Injury Statistics Query and Reporting System) database.
Table 1.
Leading causes of death in the US, year 2022, obtained from the US Centers for Control and Prevention (CDC) WISQARS (Web-based Injury Statistics Query and Reporting System) database.
| n. | Cause | Number of deaths | Crude rate | Percentage of all deaths |
|---|---|---|---|---|
| Cumulative | ||||
| 1 | Heart Disease | 702880 | 210.9 | 26.2% |
| 2 | Malignant Neoplasms | 608371 | 182.5 | 22.7% |
| 3 | Unintentional Injury | 227039 | 68.1 | 8.5% |
| 4 | COVID-19 | 186552 | 56 | 6.9% |
| 5 | Stroke | 165393 | 49.6 | 6.2% |
| 6 | Chronic Lower Respiratory Disease | 147382 | 44.2 | 5.5% |
| 7 | Alzheimer's Disease | 120122 | 36 | 4.5% |
| 8 | Diabetes Mellitus | 101209 | 30.4 | 3.8% |
| 9 | Kidney disease | 57937 | 17.4 | 2.2% |
| 10 | Liver Disease | 54803 | 16.4 | 2.0% |
| Males | ||||
| 1 | Heart Disease | 386766 | 234 | 26.8% |
| 2 | Malignant Neoplasms | 319336 | 193.2 | 22.1% |
| 3 | Unintentional Injury | 151629 | 91.7 | 10.5% |
| 4 | COVID-19 | 102660 | 62.1 | 7.1% |
| 5 | Stroke | 71819 | 43.5 | 5.0% |
| 6 | Chronic Lower Respiratory Disease | 69004 | 41.7 | 4.8% |
| 7 | Diabetes Mellitus | 57557 | 34.8 | 4.0% |
| 8 | Suicide | 39273 | 23.8 | 2.7% |
| 9 | Alzheimer's Disease | 37475 | 22.7 | 2.6% |
| 10 | Liver Disease | 34340 | 20.8 | 2.4% |
| Females | ||||
| 1 | Heart Disease | 316114 | 188.2 | 25.4% |
| 2 | Malignant Neoplasms | 289035 | 172 | 23.3% |
| 3 | Stroke | 93574 | 55.7 | 7.5% |
| 4 | COVID-19 | 83892 | 49.9 | 6.8% |
| 5 | Alzheimer's Disease | 82647 | 49.2 | 6.7% |
| 6 | Chronic Lower Respiratory Disease | 78378 | 46.7 | 6.3% |
| 7 | Unintentional Injury | 75410 | 44.9 | 6.1% |
| 8 | Diabetes Mellitus | 43652 | 26 | 3.5% |
| 9 | Kidney disease | 27759 | 16.5 | 2.2% |
| 10 | Hypertension | 23056 | 13.7 | 1.9% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



