Submitted:
23 October 2024
Posted:
24 October 2024
You are already at the latest version
Abstract
In the United States, autism spectrum disorder (ASD) affects 1 in 33 children and is characterized by atypical social interactions, communication difficulties, and intense, restricted interests. Microbial dysbiosis in the gastrointestinal (GI) tract is frequently observed in individuals with ASD, potentially contributing to behavioral manifestations and correlating with worsening severity. Moreover, dysbiosis may contribute to the increased prevalence of GI comorbidities in the ASD population and exacerbate immune dysregulation, further worsening dysbiosis. Over the past 25 years, research on the impact of microbial manipulation on ASD outcomes has gained substantial interest. Various approaches to microbial manipulation have been preclinically and clinically tested, including antibiotic treatment, dietary modifications, prebiotics, probiotics, and fecal microbiota transplantation. Each method has shown varying degrees of success in reducing the severity of ASD behaviors and/or GI symptoms and varying long-term efficacy. In this review, we discuss these microbiome manipulation methods and their outcomes. We also discuss potential microbiome manipulation early in life, as this is a critical period for neurodevelopment.
Keywords:
autism
; prebiotics
; synbiotics
; probiotics
; diet
; fetal microbiota transplant
; antibiotics
; GI
; gut
; inflammation
; behavior
; brain-gut
; gastrointestinal symptoms
Introduction
Autism spectrum disorder (ASD) is defined as having restricted interests and atypical social and communicative behaviors[1]. ASD individuals also face a suite of co-morbidities, with the most prominent being gastrointestinal issues (GI) which include abdominal pain, constipation and diarrhea[2]. A suggested reason for the increased prevalence of GI issues is microbial dysbiosis – a deviation of commensal microbial abundance and function – within the GI tract[3]. The most pre-dominate phyla of commensal gut microbes in humans include Bacillota (previously known as Firmicutes) and Bacteroidetes, followed by smaller populations composed of Actinobacteria, Proteobacteria, and Verrucomicrobia[4,5]. In gut biopsies from ASD children, shifts in the abovementioned phyla occur, with increased Bacillota, namely those part of the class Clostridia, and decreased Bacteroidetes[6]. This is opposite to what is found in stool samples, as Bacteroidetes, Proteobacteria and Actinobacteria are higher in severe ASD cases while Bacillota is lower[7,8]. In mice that received fecal transplants from ASD children, ASD like behavior, including reduced socialness and increased anxiety was observed[9]. However, in this instance, Actinobacteria was significantly reduced in mice that received ASD donor stool, as well as Candidative S., whereas the Temericutes phyla was increased[9]. Based on these and similar studies, it has been hypothesized that microbial dysbiosis is one of the contributing factors in ASD etiology or pathophsiology, and therefore manipulation of the microbiome may be of critical clinical importance.
Given the importance of the gut microbiota in host physiology and health, and its influence on the central nervous system via the microbiota-gut-brain axis, it has become a popular therapeutic target for neurological disorders. Therapeutic approaches targeting the gut microbiota in ASD are of great interest, as they are relatively easy to administer and non-invasive. Dietary supplementation of pre and probiotics, fecal microbiota transfer (FMT) therapy, as well as dietary changes and antibiotic treatments, have all been used as potential treatments in ASD for GI symptoms and aberrant behaviors. Below, we provide an updated overview of microbial-based interventions used to treat the behavioral aspects and co-occurring conditions in the context of ASD (Table 1).
Antibiotics
Sandler and colleagues were among the first to document the use of antibiotics to correct ASD related microbial dysbiosis[10]. In their seminal study, 11 ASD children were treated with vancomycin 23 times a day for 8 weeks, followed by 4 weeks of probiotic treatment of Lactobacillus acidophilus, L. bulgaricus, and Bifidobacterium bifidum in an open-label trial[10]. Despite short term behavioral improvements, long term benefits were non-apparent, with some subject's behavioral improvements returning to baseline no less than 2 weeks after treatment termination. A time period much less than most placebo effects[11]. Since then, a few case reports have documented the use of metronidazole, amoxicillin, cefazolin and Bactrim (medication brand) and reported corresponding behavioral improvements, though again short-lived, in ASD children[12,13]. Antibiotic usage to treat other neurological conditions are mixed, as a recent systemic review evaluating the efficacy of antibiotics for schizophrenia found little significant impact[14]. In fact, antibiotic treatment itself has been associated with adverse neuropsychiatric events[15]. There are several reasons why antibiotic therapy in ASD may not be the most appropriate approach, including antibiotic resistance, however, these early works were important in establishing the connection in treating ASD symptomology via microbial manipulation.
Dietary Interventions
Several dietary interventions strategies have been proposed to help ameliorate GI and behavioral symptoms in ASD, with the most common interventions including casein, gluten, and/or carbohydrate (ketogenic)-free diets[16]. Implementing dietary interventions in young children with ASD may be challenging, due to textural/sensory sensitivities, food aversion and/or food restriction. Consequently, the nutritional profile of the child is often limited, and the microbiome is shifted towards one that is associated with the diet that is impacted by such food aversions/restrictions[17]. In a recent national survey polling 818 caregivers and adults with ASD, a healthy diet was associated with an overall benefit, with a gluten and casein-free (GFCF) and ketogenic diets being among the most popular dietary form of intervention, and also the ones with the largest perceived benefit[18]. Both GFCF and ketogenic diets were reported to improve cognition and social interaction and understanding, however, with only the ketogenetic diet improving constipation and seizures[18]. Similar findings were observed in an open-label clinical trial, where 15 ASD children were given a ketogenic gluten-free diet with medium chain triglycerides (MCT)[19]. Autism Diagnostic Observation Schdule-2 (ADOS-2) cumulative scores were reduced 3 months after the modified ketogenic diet introduction, as well as reduced ADOS-2 Social Affect. Several measures on the CARS-2 assessment were also improved, including imitation, body use, and fear and nervousness. Lastly, a modified ketogenic diet reduced BMI and the percentage of peripheral eosinophils[19]. Increased eosinophil infiltrate into the duodenum has previously been shown in ASD, with a recent meta-analysis reporting a relationship between eosinophilic GI disorders and ASD[20,21]. Whether similar decreases in intestinal eosinophils occurs after ketogenic diet in ASD has so far not been tested.
Regarding GFCF diets, a recent meta-analysis evaluating the effectiveness of GFCF diets across 8 studies found that stereotypical behaviors and cognition were significantly improved, but not social and communication issues[22]. Other studies have found no differences or profound improvements between GFCF diets in ASD behaviors[23,24]. It is hypothesized that the benefits from exclusion diets of this nature are related to excess opioids, where gluten and casein derived peptides (gliadamorphine and casomorphine) that are functionally similar to opioids act on the central nervous system to exacerbate ASD symptoms[25]. Increased IgA and IgG antibodies targeting proteins found in whey and cow’s milk have been observed in ASD, therefore it is also possible that the elimination of gluten and casein derived antigens improves behavior by reducing the severity of antibody mediated food allergies[26].
Prebiotics
Prebiotics are non-digestible compounds that benefit the host by supporting beneficial microbial growth[27]. Carbohydrates and oligosaccharides are the largest class of prebiotics, though other non-carbohydrates and dietary-related compounds can also be considered prebiotics such as plant-derived fibers, guar gum, and resistant starches[27]. Health benefits because of dietary supplementation with prebiotics have been observed to reduce severity in a variety of health conditions, including those characterized by GI issues. For instance, in individuals suffering from constipation, short-term supplementation with partially hydrolyzed guar gum (PHGG) results in increased bowel movements and beta diversity of bacterial populations[28]. Moreover, daily supplementation for two months with PHGG resulted in an increased abundance of Bloutia and Acidaminoccus spp. and improved irritability[29]. PHGG also reduced GI symptoms and lowered serum levels of the proinflammatory cytokine IL-1β. Prebiotics also impact neurological health. For instance, fructo-oligosaccharides (FOS) and galacto -oligosaccharides (GOS) have anti-depressant effects, likely though reducing cortisol levels and inflammation[30].
In ASD, the supplementation of prebiotics has generally resulted in improved behaviors, reduced quantities of potentially pathogenic microbes, and lower inflammatory markers. In a recent randomized control trial (RCT) led by Girimaldi and colleagues, supplementation with the beta- galactooligosaccharide mixture B-GOS, in combination with a gluten or casein-free diet, resulted in improved sociability scores on the Autism Treatment Evaluation Checklist (ATEC) and a trend towards reduced GI symptoms[31]. Improvements in behavior and inflammation may be due to the influence of B-GOS on bacterial populations. In a continuous culture system cultured with the fecal microbiota from ASD children, supplementation with B-GOS resulted in increased Bifidobacteria spp[32]. Promoting the growth of beneficial microbes can positively impact behavior, as the administration of Bifidobacterium longum is associated with increased social resiliency[33]. In another study, daily administration of AFO-202, a glycan produced by Aureobasidium pullulans, alongside L-carnosine and behavioral therapy, resulted in significant behavioral improvement and microbial shifts/re-adjustment[34]. Lower abundances of Enterobacter and Desulfovibrio species and increases in Faecalibacterium prancer, B. longum, and the CAG:124 Bacillota member were also found. In a separate study testing the efficacy of bovine colostrum product (BCP) and B. Infantis treatment, BCP alone resulted in improved abhorrent behaviors, reduced GI symptoms, and reduced frequencies of TNFα+CD8+ T cells[35].
Probiotics
Probiotics are live microorganisms that, when ingested in sufficient amounts, can confer health benefits[27]. Standard probiotic treatment includes the administration of specific bacterial strains. The most common types are Lactobacilli and Bifidobacteria. Generally speaking, probiotics occupy microbial niches or utilize nutrients that otherwise would have supported pathogenic bacterial populations[36]. They also directly promote GI homeostasis by producing factors that promote anti-inflammatory immune cell phenotypes and indirectly by promoting GI barrier integrity[37].
Microbial dysbiosis and its resulting microbial-derived metabolites are implicated in ASD etiology and severity [38,39]. In ASD, probiotic supplementation helps balance out microbial dysbiosis and results in improved behavioral outcomes. In a study by Tamavo et al, administration of Lactobacillus, Bifidobacteria, and Streptococcus reduced overall Bacillota and Desulfovibrio[40]. Administration of single-strain probiotics has also generated beneficial results with improvement of ASD related behaviors. For example, daily supplementation with Lactobacillus plantarum PS128 in 131 ASD children from Italy generally resulted in increased attention span, communication skills and autonomy, but with no significant improvements in GI symptoms[41]. In a double-blind placebo controlled study of 36 Taiwanese ASD children, supplementation with L. plantarum for 4 weeks resulted in minimal behavioral improvements, with the largest improvements being related to anxiety and rule-breaking behaviors, with many of the improvements also related to participant age[42]. Differences in study outcomes may be due to geographical location, since probiotic usage may be more effective for microbiomes from one area/region/country than in those from other countries[43]. In model systems, oral supplementation with Bacteroides fragilis effectively reduced repetitive behaviors, anxiety, and sensorimotor gating issues in a mouse model of altered neurodevelopment induced by maternal immune activation during pregnancy[44]. In Shank3 KO mice, which have several ASD-relevant behaviors due to synaptic dysfunction and regulation, as well as gut dysbiosis and increased intestinal inflammation, treatment with Lactobacillus reuteri improved sociability and repetitive behaviors in male mice[45,46]. Improved behaviors were not mediated by changing the specific composition of the gut microbiota but rather through the stimulation of the vagal nerve and subsequent signaling of oxytocinergic social reward systems[46]. Targeting of the vagal nerve/oxytocin pathway may explain why the dual administration of intranasal oxytocin and L. plantarum S128 resulted in improved behavioral and social domains, and lower levels of the inflammatory markers SB100 and IL-1β, in recent placebo-controlled RCT[47].Behavioral improvements after probiotic usage may also be due to changes in brain hyperactivity, which was previously found to be improved in ASD children after six months of probiotic supplementation with VISBIOME –a proprietary blend of Lactobacilli, Bifidobacterium, Streptococcus thermophilus, and starch[48].
Probiotics and/or the metabolites they produce can have effects on local gut physiology include mucosal immune responses. Probiotic intake commonly results in increases in beneficial metabolites, such as short chain fatty acids (SCFA)[49]. Butyrate, a SCFA commonly produced by commercial probiotic strains, promotes the development of colonic regulatory T cells (cTregs), that help maintain homeostasis and the balance between inflammatory and regulatory mechanisms, thus making butyrate a potent anti-inflammatory metabolite at mucosal surfaces[50]. Inflammation often exacerbates preexisting GI issues, which are prevalent in ASD[51]. After probiotic supplementation with 3 Lactobacillus, 2 Bifidumbacteria, and 1 Streptococcus strains, lower fecal TNFα levels were observed in ASD children, which was also associated with fewer GI symptoms[40]. In a study by West and colleagues, daily supplementation with Lactobacillus, Bifidobacteria, and L. ramus lysates resulted in improved diarrhea and constipation symptoms, as well as improvements in all behavioral domains in the ATEC[52]. More recent studies have confirmed similar findings. In a crossover trial led by Arnold and colleagues, administration of VISBIOME, a probiotic mixture containing Lactobacilli and Bifidobacteria species, resulted in improved scores on the pediatric quality of life inventory GI module (PedsQL-GI) that persisted for eight weeks after administration[53]. However, health benefits from consuming probiotics may be limited to ASD individuals experiencing GI issues. In a six-month RCT testing the efficacy of VISBIOME in 31 ASD children, no significant behavioral improvements were noted in the group as a whole[54]. However, when GI status was considered, VISBIOME supplementation resulted in not only GI improvements but significantly more behavioral improvements than in the children without GI issues. The variability of findings in probiotic studies may be attributed to co-occurring GI conditions and small sample sizes that prevent comparison between ASD children with or without GI symptoms. ASD children with GI issues have been reported to have more impaired speech sociability and lower cognitive and sensory awareness[55].
Synbiotics
The combined use of prebiotics and probiotics, referred to as synbiotics, can have greater health benefits than pre or probiotics used alone. Synbiotics aid in the survival and stability of probiotic species by providing nutritional niches or protecting the bacteria from low gastric pH[27]. In this way, the health benefits of the probiotics can be prolonged. The study of symbiotic therapies for ASD has increased and can overcome some disadvantages of other microbial-based therapies previously used for ASD[10]. It may also explain why in some studies, the administration of prebiotics or probiotics alone has fewer therapeutic benefits than combined[56].
There is evidence that suggests synbiotic therapy improves ASD symptomology. In a recent trial testing the efficacy of the combined probiotics Bifidobacterium and Lactobacillus species and prebiotic FOS in 26 ASD children, improved ATEC scores in speech-language communication and sociability were noted 60 days after beginning supplementation[57]. Reduced abundance of Clostridium and Ruminococcus as well as increased levels of the fecal SCFA acetate, butyric, and propionic acid were also observed. Furthermore, using the Simulator of the Human Intestinal Microbial Ecosystem (SHIME) gut culture system, synbiotic supplementation with GOS plus L. reuteri, B. longum in the fecal microbiota from ASD children, reduced the abundance of Desulfovibrio and Bacillota, while increasing the abundance of beneficial microbes like Lactobacillus, Bifidobacterium and Blaotia spp[58]. Increases in SCFA, namely, acetic and butyric acid were also noted. The SCFA findings of Duque and colleagues' contrast those of Adams et al, who observed lower total SCFA content in ASD children taking probiotics[55,58]. Nevertheless, SCFA can have therapeutic potential when properly balanced, with an imbalance in either direction undesirable.
While synbiotic microbial and prebiotic supplementation generally results in improved behavior, inconsistencies regarding the extent of their benefits exist. For instance, a pilot study by Sanctuary and colleagues found no therapeutic advantage of using a symbiotic treatment on behavior but did show improvement in GI symptoms[35]. However, their relatively small sample size (8 ASD subjects) and lack of controls limits interpretation of the efficacy of symbiotic therapy in ASD. Inconsistencies may also be because no signature panel of microbes or metabolites has been observed in microbial dysbiosis in the context of ASD. Addressing an imbalance is therefore often personalized and not easily translated to the ASD population as a whole or even to subgroups within the ASD spectrum or based on specific comorbidities. Therefore, supplementation with one type of pre-, pro-, or symbiotic is not likely addressing inter-individual variation in gut dysbiosis. Precision biotics may be essential for overcoming these obstacles. In a new clinical trial using the Sun Genomics product Flore, customized administration of pre- and probiotics in 296 ASD individuals for three months improved receptive and expressive language, cognitive scores, and decreased overall GI symptom severity[59].
Fecal Microbiota Transfer
Despite the therapeutic benefits that come with antibiotic and probiotic treatment, their efficacy to manage microbial dysbiosis in ASD is limited. Fecal microbiota transfer (FMT) therapy, first approved for the treatment of Clostridioides difficile infection in 2022, has been used to successfully treat GI conditions caused by microbial dysbiosis, such as ulcerative colitis (UC) and Crohn’s Disease (CD)[60]. More recently, FMT therapy has been considered for conditions originating outside of the GI tract, including neurological conditions and neurodevelopmental disorders, including ASD. In a now seminal clinical trial from Kang and colleagues published in 2017, FMT therapy using standardized human gut microbiota (SHGM) and its impact on ASD related behavior and GI symptoms was tested in 18 ASD children with GI symptoms[61]. Using a combination of vancomycin treatment, high dose rectal and oral SHGM administration, and maintenance SHGM doses for 10 weeks afterwords, followed by an 8 week observation period, significant improvements in ASD behavior and GI assessment scores were apparent by week 10, and continued for 8 weeks after treatment[61]. Behavioral and GI symptom improvements were followed by shifts in the abundance of Bifidobacterium, Prevotella and Desulfovibro members. In a separate open-label clinical trial with 40 ASD participants with GI issues, FMT therapy was administered for 4 weeks without prior antibiotic treatment, followed by an 8-week observation period[62]. Gastrointestinal Symptom Rating Scale (GSRS), ABC and CARS scores improved after the 4-week period FMT administration and remained improved until the end of the study observation period[62]. In ASD participants that responded to FMT therapy versus those that did not (defined by having less than a 50% reduction in average GSRS score following FMT treatment), Eubacterium coprostanolegenes, a member of the Bacillota phyla, was significantly reduced in the ASD responders after therapy[62]. Since these initial studies, several recent studies also suggest positive outcomes after FMT treatment. In a study by Li and colleagues, administration of lyophilized donor stool of FMT orally once every 4 weeks (with a 12-week study end point) resulted in improved behavioral (ABC and CARS) and GI (GSRS) symptoms [63]. Similar to Kangs 2017 study, the abundance of bacterial species changed following FMT treatment, while diversity did not[63]. An increased abundance of the genera Eubacterium, Anaerostipes, Fusicatenibacteria, Collinsella, and Dorea were noted, whereas Blautia, Prevotella, and Sellimonas were decreased 12 weeks after treatment[63]. Recent case reports of FMT treatments in ASD individuals also report significant behavioral improvements[64,65]. Changes in the abundance of microbial community members can impact the metabolomic profile of both the gut and peripheral blood, which may also contribute to behavioral improvements [66]. Before FMT therapy, plasma metabolites involved in energy metabolism and anti-oxidation were distinctly lower in ASD children, most notably including nicotinamide riboside, indolepropionate, methylsuccinate, inosine monophosphate, and sarcosine. After FMT therapy, these metabolites were similar in concentration to controls[67]. A similar pattern of changes occurs in fecal samples, where the metabolites of ASD children become more like control children, although the effect is less pronounced[68]. Serum levels of neurotransmitters that are also dysregulated in ASD, such as serotonin (5-HT), gamma-aminobutyric acid (GABA), and dopamine (DA), were also improved after FMT[62].
Although results from FMT are encouraging, an 8–10-week observation period is associated with moderate placebo effects in functional GI disorder studies[69]. Unique to FMT therapy in ASD, and no other mode of microbiome therapies, is that these positive effects of FMT persisted for a significant period outside of the study period. In a follow up study with the participants from the Kang et. al, 2017 study, behavioral (as determined by the ABC, CARS, and Vineland Adaptive Behavior Scale [VABS] assessments) and GI symptoms (determined by the GSRS) were determined. It was shown that 2 years post treatment persistent behavioral improvement and GI symptom remission could be detected[70]. Intrigingly, some improvements were enhanced even further than at end of the original study, CARS scores were 47% lower after 2 years follow up than 23% lower after the initial study ended[70]. Such long-term improvements may be due to increased abundances of Bifidobacterium, Prevotella, and Desulfovibro found during the follow-up period[70]. Furthermore, a longitudinal study evaluating the long-term outcomes in 328 Chinese ASD children found that improvements in behavioral and GI symptoms could be seen 2-3 years post-FMT treatment, but were largely lost 5 years post-FMT[71]. These encouraging results warrant further study, and investigations also need to be made to determine the long-term effects of other microbial manipulation strategies that so far have been lacking in the literature.
Early Life Microbial Interventions
Several avenues of research remain to be investigated in terms of the therapeutic potential of microbial manipulation in ASD. More recently, microbial supplementation during critical periods of brain development holds promise. In the maternal immune activation (MIA) model of altered neurodevelopment, supplementation with the synbiotic combination of Bifidobacteria, Lactobacillus, FOS, and maltodextrin during gestation protects the MIA offspring from ASD like behaviors, likely by reducing levels of IL-17A and IL-6 in the brain and promoting the differentiation of inhibitory neuronal cells[72]. In cross-fostering experiments where MIA offspring are exposed to the microbiota of healthy dams during the early post-natal period, behaviors are also rescued, with reduced inflammation also seen[38]. In the idiopathic BTBR model of ASD, the administration of sodium butyrate in utero and in adulthood reduces ASD-like repetitive behaviors and increases sociability[73,74]. In a human trial investigating probiotic supplementation during pregnancy, probiotics were associated with reduced risk of neuropsychiatric disorders like ADHD and ASD[75]. However, no difference was found in a more extensive study testing probiotic supplementation from 35 weeks gestation until two years of age[76]. Moreover. Microbial induced imbalances in SCFA may also have adverse effects on neurodevelopment. For instance, exposure to moderate propionic acid concentrations shifts neuronal development towards excitatory phenotypes and increases inflammatory gene expression in human neural stem cells[77].
The establishment of the early life microbiome is directly tied with the development of immune tolerance, and because immune dysregulation is a common finding in ASD, microbial manipulation that targets immune education may be a unique therapeutic opportunity[3,78]. Early life exposure to gut dysbiosis, such as maternal antibiotic administration during labor, delivery method (e.g, cesarean section) and diet (e.g, formula), are all associated with ASD outcomes, and negatively impact the development of immune tolerance in offspring[79,80,81,82]. The importance of the gut-microbiota in tolerance development is observed in germ-free (GF) mice, which lack gut microbial communities[83]. GF mice have reduced thymus size and cellularity, and reduced expression of the autoimmune regulator (AIRE) transcription factor (reviewed in [84]). AIRE expression in the thymus is essential for the development of regulatory T cells (Tregs), a critical component involved in immune tolerance and, decreased frequencies and function of these cells are also implicated in ASD pathology. Failure to express AIRE results in autoimmunity and inflammation[85]. In pregnant and lactating dams fed a high-fiber diet, offspring had elevated serum levels of butyrate, resulting in increased AIRE expression and Tregs frequency[82]. This may be related to butyrate’s ability to epigenetically modify transcriptional sites necessary for Tregs development [50,86]. In human cohorts of expectant mothers, elevated maternal serum acetate during gestation positively correlates with thymus size and offspring Tregs frequency several years after birth[87]. Mechanistically, this may also be due to histone modifications at essential Tregs promoter sites. In mice, maternal acetate was also found to suppress allergic airway disease in offspring by enhancing Tregs development via acetylation at Tregs promoter sites[88]. Similar results have been seen with early life probiotic administration/exposure. Administration of Bifidobacterium breve to preterm infants resulted in increased serum levels of TGF-β1, a regulatory cytokine largely associated with Treg activity[89,90].
Conclusions and Future Directions
Manipulating the gut microbiota presents a promising avenue for modulating certain ASD behaviors and associated comorbidities (Figure 1). Future research should focus on the longevity of these microbiome manipulation approaches and explore whether a combination of therapies (e.g., probiotic use and fecal microbiota transplantation) is more effective than any single approach. Moreover, it is crucial to investigate the timing of interventions, particularly the differences between early childhood and adolescence. Future studies should also consider the development of non-traditional approaches to microbial manipulation, such as personalized microbiome therapies or novel dietary strategies. Lastly, a multidisciplinary approach to microbial manipulation would likely aid in therapeutic efficacy, particularly from fields involved in nutrition, immunology, microbiology and psychology.
Acknowledgments
This study was funded by the National Institute of Child Health and Disease (R01HD090214), National Institutes of Mental Health (R01MH118209), Autism Speaks Foundation, Autism Research Institute, the Jane Botsford Johnson Foundation, Grace Gardner Johnson Foundation, the Brain Foundation, and Jonty Foundation.
References
- Maenner, M.J. , et al., Prevalence and Characteristics of Autism Spectrum Disorder Among Children Aged 8 Years — Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2020. MMWR Surveillance Summaries, 2023. 72(2): p. 1-14.
- Chaidez, V.; Hansen, R.L.; Hertz-Picciotto, I. Gastrointestinal Problems in Children with Autism, Developmental Delays or Typical Development. J. Autism Dev. Disord. 2014, 44, 1117–1127. [Google Scholar] [CrossRef] [PubMed]
- Hughes, H.K.; Rose, D.; Ashwood, P. The Gut Microbiota and Dysbiosis in Autism Spectrum Disorders. Curr. Neurol. Neurosci. Rep. 2018, 18, 81. [Google Scholar] [CrossRef] [PubMed]
- Huttenhower, C. , et al., Structure, function and diversity of the healthy human microbiome. Nature, 2012. 486(7402): p. 207-214.
- Oren, A.; Garrity, G.M.; Moore, E.R.B.; Sutcliffe, I.C.; Trujillo, M.E. The International Journal of Systematic and Evolutionary Microbiology moves to ‘true continuous publication’ at the beginning of 2021: Proposals to emend Rule 24b (2), Note 1 to Rule 27 and Note 2 to Rule 33b of the International Code of Nomenclature of Prokaryotes. Int. J. Syst. Evol. Microbiol. 2021, 71, 004732. [Google Scholar] [CrossRef]
- Williams, B.L.; Hornig, M.; Buie, T.; Bauman, M.L.; Paik, M.C.; Wick, I.; Bennett, A.; Jabado, O.; Hirschberg, D.L.; Lipkin, W.I. Impaired Carbohydrate Digestion and Transport and Mucosal Dysbiosis in the Intestines of Children with Autism and Gastrointestinal Disturbances. PLOS ONE 2011, 6, e24585. [Google Scholar] [CrossRef] [PubMed]
- Finegold, S.M.; Dowd, S.E.; Gontcharova, V.; Liu, C.; Henley, K.E.; Wolcott, R.D.; Youn, E.; Summanen, P.H.; Granpeesheh, D.; Dixon, D.; et al. Pyrosequencing study of fecal microflora of autistic and control children. Anaerobe 2010, 16, 444–453. [Google Scholar] [CrossRef]
- Plaza-Díaz, J.; Gómez-Fernández, A.; Chueca, N.; De La Torre-Aguilar, M.J.; Gil, Á.; Perez-Navero, J.L.; Flores-Rojas, K.; Martín-Borreguero, P.; Solis-Urra, P.; Ruiz-Ojeda, F.J.; et al. Autism Spectrum Disorder (ASD) with and without Mental Regression is Associated with Changes in the Fecal Microbiota. Nutrients 2019, 11, 337. [Google Scholar] [CrossRef]
- Avolio, E.; Olivito, I.; Rosina, E.; Romano, L.; Angelone, T.; De Bartolo, A.; Scimeca, M.; Bellizzi, D.; D'Aquila, P.; Passarino, G.; et al. Modifications of Behavior and Inflammation in Mice Following Transplant with Fecal Microbiota from Children with Autism. Neuroscience 2022, 498, 174–189. [Google Scholar] [CrossRef]
- Sandler, R.H.; Finegold, S.M.; Bolte, E.R.; Buchanan, C.P.; Maxwell, A.P.; Väisänen, M.-L.; Nelson, M.N.; Wexler, H.M. Short-Term Benefit From Oral Vancomycin Treatment of Regressive-Onset Autism. J. Child Neurol. 2000, 15, 429–435. [Google Scholar] [CrossRef]
- Finniss, D.G.; Kaptchuk, T.J.; Miller, F.; Benedetti, F. Biological, clinical, and ethical advances of placebo effects. Lancet 2010, 375, 686–695. [Google Scholar] [CrossRef]
- Ramirez, P.L.; Barnhill, K.; Gutierrez, A.; Schutte, C.; Hewitson, L. Improvements in Behavioral Symptoms following Antibiotic Therapy in a 14-Year-Old Male with Autism. Case Rep. Psychiatry 2013, 2013, 1–2. [Google Scholar] [CrossRef]
- Reduction of Ritualistic Behavior in a Patient with Autism Spectrum Disorder treated with Antibiotics: A Case Report.
- Vasillu, O. Vaslle, and V. Voicu, Efficacy and tolerability of antibiotic augmentation in schizophrenia spectrum disorders – A systematic literature review. Romanian Journal of Military Medicine, 2020.
- Essali, N.; Miller, B.J. Psychosis as an adverse effect of antibiotics. Brain, Behav. Immun. - Heal. 2020, 9, 100148. [Google Scholar] [CrossRef] [PubMed]
- Ekmekci, A.M. and O. Erbas, The role of intestinal flora in autism and nutritional approaches | 2020, Volume 5 - Issue 1-2 | Demiroglu Science University Florence Nightingale Journal of Transplantation. Demiroglu Science University Florence Nightingale Journal of Transplantation, 2020.
- Önal, S.; Sachadyn-Król, M.; Kostecka, M. A Review of the Nutritional Approach and the Role of Dietary Components in Children with Autism Spectrum Disorders in Light of the Latest Scientific Research. Nutrients 2023, 15, 4852. [Google Scholar] [CrossRef] [PubMed]
- Matthews, J.S.; Adams, J.B. Ratings of the Effectiveness of 13 Therapeutic Diets for Autism Spectrum Disorder: Results of a National Survey. J. Pers. Med. 2023, 13, 1448. [Google Scholar] [CrossRef]
- Lee, R.W.Y.; Corley, M.J.; Pang, A.; Arakaki, G.; Abbott, L.; Nishimoto, M.; Miyamoto, R.; Lee, E.; Yamamoto, S.; Maunakea, A.K.; et al. A modified ketogenic gluten-free diet with MCT improves behavior in children with autism spectrum disorder. Physiol. Behav. 2018, 188, 205–211. [Google Scholar] [CrossRef] [PubMed]
- Ashwood, P.; Murch, S.H.; Anthony, A.; Pellicer, A.A.; Torrente, F.; Thomson, M.A.; Walker-Smith, J.A.; Wakefield, A.J. Intestinal Lymphocyte Populations in Children with Regressive Autism: Evidence for Extensive Mucosal Immunopathology. J. Clin. Immunol. 2003, 23, 504–517. [Google Scholar] [CrossRef]
- Lima, R.V.; Muniz, M.C.R.; Barroso, L.L.; Pinheiro, M.C.A.; Matos, Y.M.T.; Nogueira, S.B.R.; Nogueira, H.B.R. Autism in patients with eosinophilic gastrointestinal disease: A systematic review with meta-analysis. Pediatr. Allergy Immunol. 2024, 35, e14122. [Google Scholar] [CrossRef]
- Quan, L.; Xu, X.; Cui, Y.; Han, H.; Hendren, R.L.; Zhao, L.; You, X. A systematic review and meta-analysis of the benefits of a gluten-free diet and/or casein-free diet for children with autism spectrum disorder. Nutr. Rev. 2021, 80, 1237–1246. [Google Scholar] [CrossRef]
- Knivsberg, A.; Reichelt, K.; Høien, T.; Nødland, M. A Randomised, Controlled Study of Dietary Intervention in Autistic Syndromes. Nutr. Neurosci. 2002, 5, 251–261. [Google Scholar] [CrossRef]
- Navarro, F. , et al., Are ‘leaky gut’ and behavior associated with gluten and dairy containing diet in children with autism spectrum disorders? Nutritional Neuroscience, 2015. 18(4): p. 177-185.
- Woodford, K.B. Casomorphins and Gliadorphins Have Diverse Systemic Effects Spanning Gut, Brain and Internal Organs. Int. J. Environ. Res. Public Heal. 2021, 18, 7911. [Google Scholar] [CrossRef]
- Trajkovski, V.; Petlichkovski, A.; Efinska-Mladenovska, O.; Trajkov, D.; Arsov, T.; Strezova, A.; Ajdinski, L.; Spiroski, M. Higher Plasma Concentration of Food-Specific Antibodies in Persons With Autistic Disorder in Comparison to Their Siblings. Focus Autism Other Dev. Disabil. 2008, 23, 176–185. [Google Scholar] [CrossRef]
- Pandey, K.R. R. Naik, and B.V. Vakil, Probiotics, prebiotics and synbiotics- a review. Journal of Food Science and Technology, 2015. 52(12): p. 7577-7587.
- Reider, S.J.; Moosmang, S.; Tragust, J.; Trgovec-Greif, L.; Tragust, S.; Perschy, L.; Przysiecki, N.; Sturm, S.; Tilg, H.; Stuppner, H.; et al. Prebiotic Effects of Partially Hydrolyzed Guar Gum on the Composition and Function of the Human Microbiota—Results from the PAGODA Trial. Nutrients 2020, 12, 1257. [Google Scholar] [CrossRef] [PubMed]
- Inoue, R.; Sakaue, Y.; Kawada, Y.; Tamaki, R.; Yasukawa, Z.; Ozeki, M.; Ueba, S.; Sawai, C.; Nonomura, K.; Tsukahara, T.; et al. Dietary supplementation with partially hydrolyzed guar gum helps improve constipation and gut dysbiosis symptoms and behavioral irritability in children with autism spectrum disorder. J. Clin. Biochem. Nutr. 2019, 64, 217–223. [Google Scholar] [CrossRef]
- Burokas, A.; Arboleya, S.; Moloney, R.D.; Peterson, V.L.; Murphy, K.; Clarke, G.; Stanton, C.; Dinan, T.G.; Cryan, J.F. Targeting the Microbiota-Gut-Brain Axis: Prebiotics Have Anxiolytic and Antidepressant-like Effects and Reverse the Impact of Chronic Stress in Mice. Biol. Psychiatry 2017, 82, 472–487. [Google Scholar] [CrossRef]
- Grimaldi, R.; Gibson, G.R.; Vulevic, J.; Giallourou, N.; Castro-Mejía, J.L.; Hansen, L.H.; Gibson, E.L.; Nielsen, D.S.; Costabile, A. A prebiotic intervention study in children with autism spectrum disorders (ASDs). Microbiome 2018, 6, 133. [Google Scholar] [CrossRef] [PubMed]
- Grimaldi, R. , et al., In vitro fermentation of B-GOS: impact on faecal bacterial populations and metabolic activity in autistic and non-autistic children. FEMS Microbiology Ecology, 2017. 93(2): p. fiw233.
- Yang, C.; Fujita, Y.; Ren, Q.; Ma, M.; Dong, C.; Hashimoto, K. Bifidobacterium in the gut microbiota confer resilience to chronic social defeat stress in mice. Sci. Rep. 2017, 7, srep45942. [Google Scholar] [CrossRef]
- Raghavan, K.; Dedeepiya, V.D.; Yamamoto, N.; Ikewaki, N.; Sonoda, T.; Iwasaki, M.; Kandaswamy, R.S.; Senthilkumar, R.; Preethy, S.; Abraham, S.J. Benefits of Gut Microbiota Reconstitution by Beta 1,3–1,6 Glucans in Subjects with Autism Spectrum Disorder and Other Neurodegenerative Diseases. J. Alzheimer's Dis. 2023, 94, S241–S252. [Google Scholar] [CrossRef] [PubMed]
- Sanctuary, M.R.; Kain, J.N.; Chen, S.Y.; Kalanetra, K.; Lemay, D.G.; Rose, D.R.; Yang, H.T.; Tancredi, D.J.; German, J.B.; Slupsky, C.M.; et al. Pilot study of probiotic/colostrum supplementation on gut function in children with autism and gastrointestinal symptoms. PLOS ONE 2019, 14, e0210064. [Google Scholar] [CrossRef]
- Dobson, A. , et al., Bacteriocin Production: a Probiotic Trait? Applied and Environmental Microbiology, 2012. 78(1): p. 1-6.
- Oelschlaeger, T.A. , Mechanisms of probiotic actions – A review. International Journal of Medical Microbiology, 2010. 300(1): p. 57-62.
- Kim, E.; Paik, D.; Ramirez, R.N.; Biggs, D.G.; Park, Y.; Kwon, H.-K.; Choi, G.B.; Huh, J.R. Maternal gut bacteria drive intestinal inflammation in offspring with neurodevelopmental disorders by altering the chromatin landscape of CD4+ T cells. Immunity 2021, 55, 145–158. [Google Scholar] [CrossRef]
- Needham, B.D.; Funabashi, M.; Adame, M.D.; Wang, Z.; Boktor, J.C.; Haney, J.; Wu, W.-L.; Rabut, C.; Ladinsky, M.S.; Hwang, S.-J.; et al. A gut-derived metabolite alters brain activity and anxiety behaviour in mice. Nature 2022, 602, 647–653. [Google Scholar] [CrossRef]
- Tomova, A.; Husarova, V.; Lakatosova, S.; Bakos, J.; Vlkova, B.; Babinska, K.; Ostatnikova, D. Gastrointestinal microbiota in children with autism in Slovakia. Physiol. Behav. 2015, 138, 179–187. [Google Scholar] [CrossRef]
- Mensi, M.M.; Rogantini, C.; Marchesi, M.; Borgatti, R.; Chiappedi, M. Lactobacillus plantarum PS128 and Other Probiotics in Children and Adolescents with Autism Spectrum Disorder: A Real-World Experience. Nutrients 2022, 13, 2036. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.-W.; Liong, M.T.; Chung, Y.-C.E.; Huang, H.-Y.; Peng, W.-S.; Cheng, Y.-F.; Lin, Y.-S.; Wu, Y.-Y.; Tsai, Y.-C. Effects of Lactobacillus plantarum PS128 on Children with Autism Spectrum Disorder in Taiwan: A Randomized, Double-Blind, Placebo-Controlled Trial. Nutrients 2019, 11. [Google Scholar] [CrossRef] [PubMed]
- Porras, A.M.; Shi, Q.; Zhou, H.; Callahan, R.; Montenegro-Bethancourt, G.; Solomons, N.; Brito, I.L. Geographic differences in gut microbiota composition impact susceptibility to enteric infection. Cell Rep. 2021, 36, 109457. [Google Scholar] [CrossRef] [PubMed]
- Hsiao, E.Y.; McBride, S.W.; Hsien, S.; Sharon, G.; Hyde, E.R.; McCue, T.; Codelli, J.A.; Chow, J.; Reisman, S.E.; Petrosino, J.F.; et al. Microbiota Modulate Behavioral and Physiological Abnormalities Associated with Neurodevelopmental Disorders. Cell 2013, 155, 1451–1463. [Google Scholar] [CrossRef]
- Tabouy, L.; Getselter, D.; Ziv, O.; Karpuj, M.; Tabouy, T.; Lukic, I.; Maayouf, R.; Werbner, N.; Ben-Amram, H.; Nuriel-Ohayon, M.; et al. Dysbiosis of microbiome and probiotic treatment in a genetic model of autism spectrum disorders. Brain, Behav. Immun. 2018, 73, 310–319. [Google Scholar] [CrossRef]
- Sgritta, M.; Dooling, S.W.; Buffington, S.A.; Momin, E.N.; Francis, M.B.; Britton, R.A.; Costa-Mattioli, M. Mechanisms Underlying Microbial-Mediated Changes in Social Behavior in Mouse Models of Autism Spectrum Disorder. Neuron 2019, 101, 246–259. [Google Scholar] [CrossRef]
- Kong, X.-J.; Liu, J.; Liu, K.; Koh, M.; Sherman, H.; Liu, S.; Tian, R.; Sukijthamapan, P.; Wang, J.; Fong, M.; et al. Probiotic and Oxytocin Combination Therapy in Patients with Autism Spectrum Disorder: A Randomized, Double-Blinded, Placebo-Controlled Pilot Trial. Nutrients 2021, 13, 1552. [Google Scholar] [CrossRef]
- Billeci, L.; Callara, A.L.; Guiducci, L.; Prosperi, M.; Morales, M.A.; Calderoni, S.; Muratori, F.; Santocchi, E. A randomized controlled trial into the effects of probiotics on electroencephalography in preschoolers with autism. Autism 2023, 27, 117–132. [Google Scholar] [CrossRef]
- Markowiak-Kopeć, P.; Śliżewska, K. The Effect of Probiotics on the Production of Short-Chain Fatty Acids by Human Intestinal Microbiome. Nutrients 2020, 12, 1107. [Google Scholar] [CrossRef]
- Furusawa, Y.; Obata, Y.; Fukuda, S.; Endo, T.A.; Nakato, G.; Takahashi, D.; Nakanishi, Y.; Uetake, C.; Kato, K.; Kato, T.; et al. Erratum: Commensal microbe-derived butyrate induces the differentiation of colonic regulatory T cells. Nature 2014, 506, 254–254. [Google Scholar] [CrossRef]
- Hsiao, E.Y. Gastrointestinal Issues in Autism Spectrum Disorder. Harv. Rev. Psychiatry 2014, 22, 104–111. [Google Scholar] [CrossRef]
- West, R. , et al., Improvements in Gastrointestinal Symptoms among Children with Autism Spectrum Disorder Receiving the Delpro ® Probiotic and Immunomodulator Formulation | Semantic Scholar. Prebiotics & Health, 2013.
- Arnold, L.E.; Luna, R.A.; Williams, K.; Chan, J.; Parker, R.A.; Wu, Q.; Hollway, J.A.; Jeffs, A.; Lu, F.; Coury, D.L.; et al. Probiotics for Gastrointestinal Symptoms and Quality of Life in Autism: A Placebo-Controlled Pilot Trial. J. Child Adolesc. Psychopharmacol. 2019, 29, 659–669. [Google Scholar] [CrossRef] [PubMed]
- Santocchi, E.; Guiducci, L.; Prosperi, M.; Calderoni, S.; Gaggini, M.; Apicella, F.; Tancredi, R.; Billeci, L.; Mastromarino, P.; Grossi, E.; et al. Effects of Probiotic Supplementation on Gastrointestinal, Sensory and Core Symptoms in Autism Spectrum Disorders: A Randomized Controlled Trial. Front. Psychiatry 2020, 11. [Google Scholar] [CrossRef] [PubMed]
- Adams, J.B.; Johansen, L.J.; Powell, L.D.; Quig, D.; Rubin, R.A. Gastrointestinal flora and gastrointestinal status in children with autism–Comparisons to typical children and correlation with autism severity. BMC Gastroenterol. 2011, 11, 22. [Google Scholar] [CrossRef] [PubMed]
- Adıgüzel, E.; Çiçek, B.; Ünal, G.; Aydın, M.F.; Barlak-Keti, D. Probiotics and prebiotics alleviate behavioral deficits, inflammatory response, and gut dysbiosis in prenatal VPA-induced rodent model of autism. Physiol. Behav. 2022, 256, 113961. [Google Scholar] [CrossRef]
- Wang, Y.; Li, N.; Yang, J.-J.; Zhao, D.-M.; Chen, B.; Zhang, G.-Q.; Chen, S.; Cao, R.-F.; Yu, H.; Zhao, C.-Y.; et al. Probiotics and fructo-oligosaccharide intervention modulate the microbiota-gut brain axis to improve autism spectrum reducing also the hyper-serotonergic state and the dopamine metabolism disorder. Pharmacol. Res. 2020, 157, 104784. [Google Scholar] [CrossRef]
- Duque, A.L.R.F.; Demarqui, F.M.; Santoni, M.M.; Zanelli, C.F.; Adorno, M.A.T.; Milenkovic, D.; Mesa, V.; Sivieri, K. Effect of probiotic, prebiotic, and synbiotic on the gut microbiota of autistic children using an in vitro gut microbiome model. Food Res. Int. 2021, 149, 110657. [Google Scholar] [CrossRef]
- Phan, J.; Calvo, D.C.; Nair, D.; Jain, S.; Montagne, T.; Dietsche, S.; Blanchard, K.; Treadwell, S.; Adams, J.; Krajmalnik-Brown, R. Precision synbiotics increase gut microbiome diversity and improve gastrointestinal symptoms in a pilot open-label study for autism spectrum disorder. mSystems 2024, 9, e0050324. [Google Scholar] [CrossRef]
- Antushevich, H. Fecal microbiota transplantation in disease therapy. Clin. Chim. Acta 2020, 503, 90–98. [Google Scholar] [CrossRef]
- Kang, D.-W.; Adams, J.B.; Gregory, A.C.; Borody, T.; Chittick, L.; Fasano, A.; Khoruts, A.; Geis, E.; Maldonado, J.; McDonough-Means, S.; et al. Microbiota Transfer Therapy alters gut ecosystem and improves gastrointestinal and autism symptoms: an open-label study. Microbiome 2017, 5, 1–16. [Google Scholar] [CrossRef]
- Li, N.; Chen, H.; Cheng, Y.; Xu, F.; Ruan, G.; Ying, S.; Tang, W.; Chen, L.; Chen, M.; Lv, L.; et al. Fecal Microbiota Transplantation Relieves Gastrointestinal and Autism Symptoms by Improving the Gut Microbiota in an Open-Label Study. Front. Cell. Infect. Microbiol. 2021, 11. [Google Scholar] [CrossRef]
- Li, Y.; Xiao, P.; Cao, R.; Le, J.; Xu, Q.; Xiao, F.; Ye, L.; Wang, X.; Wang, Y.; Zhang, T. Effects and microbiota changes following oral lyophilized fecal microbiota transplantation in children with autism spectrum disorder. Front. Pediatr. 2024, 12, 1369823. [Google Scholar] [CrossRef] [PubMed]
- Hu, C. , et al., Fecal microbiota transplantation in a child with severe ASD comorbidities of gastrointestinal dysfunctions—a case report. Frontiers in Psychiatry, 2023. 14: p. 1219104.
- Huang, H.-L.; Xu, H.-M.; Liu, Y.-D.; Shou, D.-W.; Chen, H.-T.; Nie, Y.-Q.; Li, Y.-Q.; Zhou, Y.-J. First Application of Fecal Microbiota Transplantation in Adult Asperger Syndrome With Digestive Symptoms—A Case Report. Front. Psychiatry 2022, 13, 695481. [Google Scholar] [CrossRef] [PubMed]
- Segal, J.P.; Mullish, B.H.; Quraishi, M.N.; Iqbal, T.; Marchesi, J.R.; Sokol, H. Mechanisms underpinning the efficacy of faecal microbiota transplantation in treating gastrointestinal disease. Ther. Adv. Gastroenterol. 2020, 13. [Google Scholar] [CrossRef] [PubMed]
- Kang, D.-W.; Adams, J.B.; Vargason, T.; Santiago, M.; Hahn, J.; Krajmalnik-Brown, R. Distinct Fecal and Plasma Metabolites in Children with Autism Spectrum Disorders and Their Modulation after Microbiota Transfer Therapy. mSphere 2020, 5. [Google Scholar] [CrossRef]
- Qureshi, F.; Adams, J.; Hanagan, K.; Kang, D.-W.; Krajmalnik-Brown, R.; Hahn, J. Multivariate Analysis of Fecal Metabolites from Children with Autism Spectrum Disorder and Gastrointestinal Symptoms before and after Microbiota Transfer Therapy. J. Pers. Med. 2020, 10, 152. [Google Scholar] [CrossRef]
- Enck, P.; Klosterhalfen, S. Placebo Responses and Placebo Effects in Functional Gastrointestinal Disorders. Front. Psychiatry 2020, 11, 797. [Google Scholar] [CrossRef]
- Kang, D.-W.; Adams, J.B.; Coleman, D.M.; Pollard, E.L.; Maldonado, J.; McDonough-Means, S.; Caporaso, J.G.; Krajmalnik-Brown, R. Long-term benefit of Microbiota Transfer Therapy on autism symptoms and gut microbiota. Sci. Rep. 2019, 9, 5821. [Google Scholar] [CrossRef]
- Ye, C.; et al. Long-term outcomes of 328 patients with of autism spectrum disorder after fecal microbiota transplantation. Chinese Journal of Gastrointestinal Surgery, 2022. 25(09): p. 798-803.
- Wang, X. , et al., Oral probiotic administration during pregnancy prevents autism-related behaviors in offspring induced by maternal immune activation via anti-inflammation in mice. Autism Research, 2019. 12(4): p. 576-588.
- Kratsman, N.; Getselter, D.; Elliott, E. Sodium butyrate attenuates social behavior deficits and modifies the transcription of inhibitory/excitatory genes in the frontal cortex of an autism model. Neuropharmacology 2016, 102, 136–145. [Google Scholar] [CrossRef]
- Cristiano, C.; Hoxha, E.; Lippiello, P.; Balbo, I.; Russo, R.; Tempia, F.; Miniaci, M.C. Maternal treatment with sodium butyrate reduces the development of autism-like traits in mice offspring. Biomed. Pharmacother. 2022, 156, 113870. [Google Scholar] [CrossRef]
- Pärtty, A.; Kalliomäki, M.; Wacklin, P.; Salminen, S.; Isolauri, E. A possible link between early probiotic intervention and the risk of neuropsychiatric disorders later in childhood: a randomized trial. Pediatr. Res. 2015, 77, 823–828. [Google Scholar] [CrossRef] [PubMed]
- Slykerman, R.F.; Kang, J.; Van Zyl, N.; Barthow, C.; Wickens, K.; Stanley, T.; Coomarasamy, C.; Purdie, G.; Murphy, R.; Crane, J.; et al. Effect of early probiotic supplementation on childhood cognition, behaviour and mood a randomised, placebo-controlled trial. Acta Paediatr. 2018, 107, 2172–2178. [Google Scholar] [CrossRef] [PubMed]
- Abdelli, L.S.; Samsam, A.; Naser, S.A. Propionic Acid Induces Gliosis and Neuro-inflammation through Modulation of PTEN/AKT Pathway in Autism Spectrum Disorder. Sci. Rep. 2019, 9, 1–12. [Google Scholar] [CrossRef]
- Hughes, H. ; R.J.Moreno, R.J.; Ashwood, P. Innate immune dysfunction and neuroinflammation in autism spectrum disorder (ASD). Brain, Behav. Immun. [CrossRef]
- Moya-Pérez, A.; Luczynski, P.; Renes, I.B.; Wang, S.; Borre, Y.; Ryan, C.A.; Knol, J.; Stanton, C.; Dinan, T.G.; Cryan, J.F. Intervention strategies for cesarean section–induced alterations in the microbiota-gut-brain axis. Nutr. Rev. 2017, 75, 225–240. [Google Scholar] [CrossRef]
- Madany, A.M.; Hughes, H.K.; Ashwood, P. Antibiotic Treatment during Pregnancy Alters Offspring Gut Microbiota in a Sex-Dependent Manner. Biomedicines 2022, 10, 1042. [Google Scholar] [CrossRef]
- Tabilas, C.; Iu, D.S.; Daly, C.W.P.; Mon, K.J.Y.; Reynaldi, A.; Wesnak, S.P.; Grenier, J.K.; Davenport, M.P.; Smith, N.L.; Grimson, A.; et al. Early microbial exposure shapes adult immunity by altering CD8+ T cell development. Proc. Natl. Acad. Sci. 2022, 119. [Google Scholar] [CrossRef] [PubMed]
- Nakajima, A.; Kaga, N.; Nakanishi, Y.; Ohno, H.; Miyamoto, J.; Kimura, I.; Hori, S.; Sasaki, T.; Hiramatsu, K.; Okumura, K.; et al. Maternal High Fiber Diet during Pregnancy and Lactation Influences Regulatory T Cell Differentiation in Offspring in Mice. J. Immunol. 2017, 199, 3516–3524. [Google Scholar] [CrossRef]
- Al-Asmakh, M.; Zadjali, F. Use of Germ-Free Animal Models in Microbiota-Related Research. J. Microbiol. Biotechnol. 2015, 25, 1583–1588. [Google Scholar] [CrossRef] [PubMed]
- Nanjundappa, R.H.; Umeshappa, C.S.; Geuking, M.B. The impact of the gut microbiota on T cell ontogeny in the thymus. Cell. Mol. Life Sci. 2022, 79, 1–14. [Google Scholar] [CrossRef]
- Rosenblum, M.D., K. A. Remedios, and A.K. Abbas, Mechanisms of human autoimmunity. Journal of Clinical Investigation, 2015. 125(6): p. 2228-2233.
- Vieira, E.L.; Leonel, A.J.; Sad, A.P.; Beltrão, N.R.; Costa, T.F.; Ferreira, T.M.; Gomes-Santos, A.C.; Faria, A.M.; Peluzio, M.C.; Cara, D.C.; et al. Oral administration of sodium butyrate attenuates inflammation and mucosal lesion in experimental acute ulcerative colitis. J. Nutr. Biochem. 2012, 23, 430–436. [Google Scholar] [CrossRef]
- Hu, M. , et al., Decreased maternal serum acetate and impaired fetal thymic and regulatory T cell development in preeclampsia. Nature Communications, 2019. 10(1): p. 3031.
- Thorburn, A.N.; McKenzie, C.I.; Shen, S.; Stanley, D.; Macia, L.; Mason, L.J.; Roberts, L.K.; Wong, C.H.Y.; Shim, R.; Robert, R.; et al. Evidence that asthma is a developmental origin disease influenced by maternal diet and bacterial metabolites. Nat. Commun. 2015, 6, 7320. [Google Scholar] [CrossRef] [PubMed]
- Fujii, T. , et al., Bifidobacterium Breve Enhances Transforming Growth Factor &bgr;1 Signaling by Regulating Smad7 Expression in Preterm Infants. Journal of Pediatric Gastroenterology and Nutrition, 2006. 43(1): p. 83-88.
- Weiss, A. and L. Attisano, The TGFbeta Superfamily Signaling Pathway. Wiley Interdisciplinary Reviews: Developmental Biology, 2013. 2(1): p. 47-63.
Figure 1.
Similarities and differences in microbial based therapies used in ASD. A variety of microbial-based therapies have been explored for autism spectrum disorder (ASD), with the most common methods including probiotics (along with prebiotics and synbiotics), dietary changes, and, more recently, fecal microbiota transplantation (FMT). Each method has unique advantages—such as the ease of use of probiotics and the potent effects of FMT. These therapies share characteristics, and in some cases, they may demonstrate enhanced therapeutic effects when administered in combination rather than individually. Moreso, their combined use may prove to hold greater and longer lasting behavioral and gastrointestinal improvements in individuals with ASD. .
Figure 1.
Similarities and differences in microbial based therapies used in ASD. A variety of microbial-based therapies have been explored for autism spectrum disorder (ASD), with the most common methods including probiotics (along with prebiotics and synbiotics), dietary changes, and, more recently, fecal microbiota transplantation (FMT). Each method has unique advantages—such as the ease of use of probiotics and the potent effects of FMT. These therapies share characteristics, and in some cases, they may demonstrate enhanced therapeutic effects when administered in combination rather than individually. Moreso, their combined use may prove to hold greater and longer lasting behavioral and gastrointestinal improvements in individuals with ASD. .
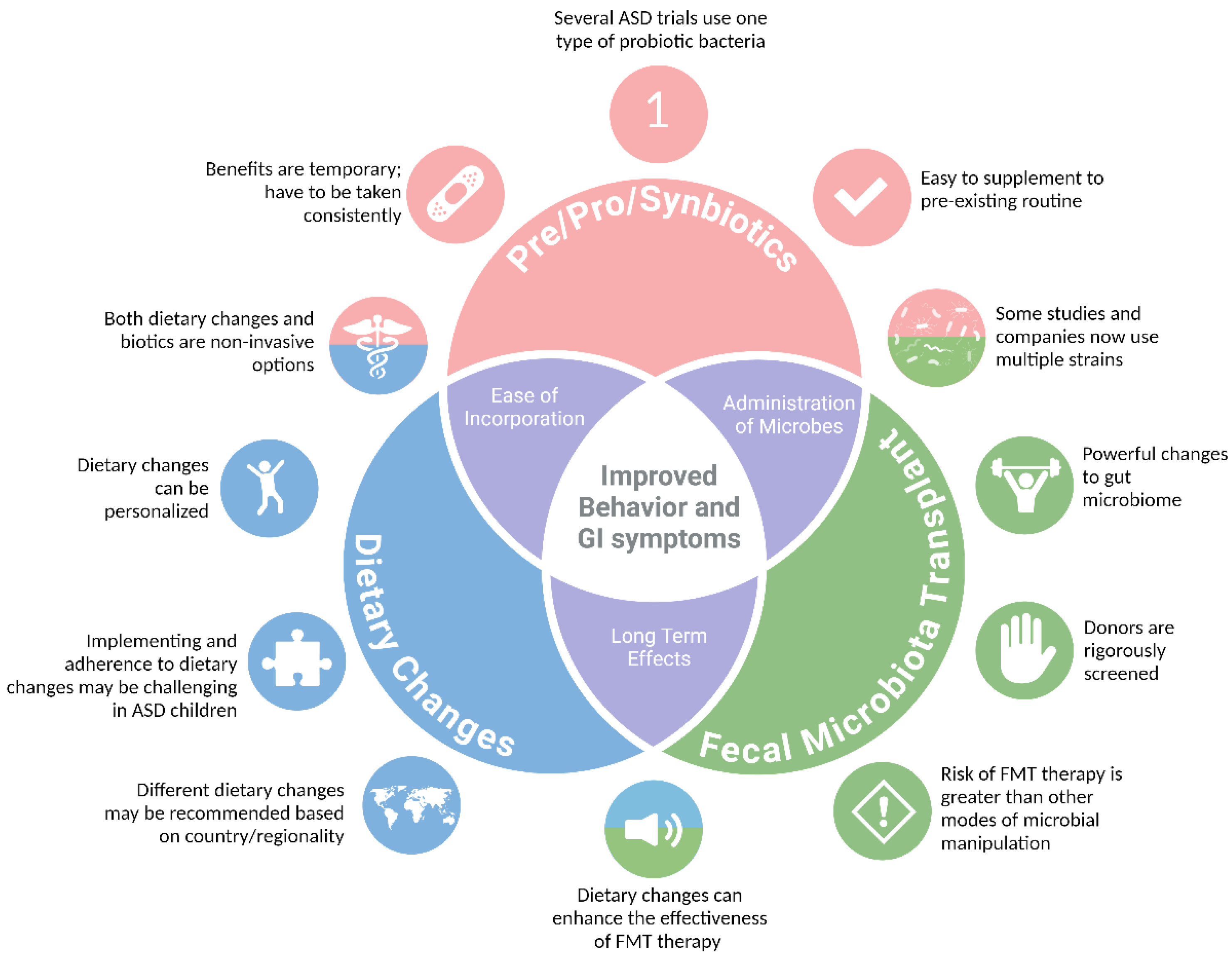

Table 1.
| Major clinical trials evaluating the efficacy of different microbial manipulation methods in ASD.
Table 1.
| Major clinical trials evaluating the efficacy of different microbial manipulation methods in ASD.
| First Author & Year | Method | Therapy | Study Length | N | Behavioral Outcomes | GI Changes | Microbiome Changes | Other Changes | Ref |
| Sandler et al., 2001 | Antibiotic | Vancomycin | 8 weeks, 3x daily | ASD = 11(3 – 7 years) | ↑ communication and behavior | N/A | ↓ anaerobic cocci | Behavioral improvements diminished within 2 weeks of treatment | 10 |
| Inoue et al., 2019 | Prebiotic | PHGG | 2-15 months | ASD = 13(4-9 years) | ↓irritability | ↓constipation |
↓ α-diversity ↓Streptococcus, Odoribacter, Eubacterium ↑Blautia, Acidaminococcus |
↓IL-1β, IL-6 | 29 |
| Grimaldi et al., 2018 | Prebiotic | B-GOS and and/or dietary intervention | 6 weeks, daily | ASD = 13(5 – 10 years) | A trend towards improved sleep patterns ↑ Social behavior ↓ antisocial behavior |
Children on exclusion diets had improved abdominal pain and bowel movements | ↑ Bifidobacterium spp., Ruminococcus spp., members of Lachnospiraceae, Eubacterium dolichum, TM7-3 family and Mycobacteriaceae. | Positive associations with B-GOS intake and ethanol, DMG and SCFA metabolites Negative associations between B-GOS intake and amino acids and lactate |
31 |
| Tomova et al., 2014 |
Probiotic | Mixture of Bifidobacteria, Lactobacillus, and Streptococcus | 4 months, 3x daily | ASD = 10 (2-9 years) ASD Siblings = 9 (5-17 years) TD = 10(2-11 years) |
N/A | N/A | ↓Bacteroidetes, Bacillota, Bifidobacterium spp. and Desulfovibro spp. | ↓fecal TNFα Positive association between GI Symptoms and Behavior Association between Desulfovibro and restrictive/repetitive behaviors |
40 |
| Liu et al., 2019 |
Probiotic | Lactobacillus plantarum PS 128 | 4 Weeks | ASD = 71; 39 Placebo, 36 PS128 (7 – 15 years) | ↓ Body and object use, SRS-total, anxiety, rule-breaking behaviors, SNAP-IV total scores, hyperactivity, and impulsivity (exploratory analysis only) | N/A | N/A | Behaviors improved more in 7–12-year-old children | 42 |
| West et al., 2013 | Probiotic | Delpro Supplement – a mixture of Lactocillus, Lactobacillus, and Bifidobacteria strains and Del-Immune V powder derived from L. rhamnousus | 21 days,3x daily | ASD = 33(3-16 years) | ↓ ATEC scores (speech/language, sociability, sensory/cognitive awareness, and physical behavior) | ↓ constipation ↓ diarrhea |
N/A | Several caregivers reported that it would take longer than 21 days to see improvements. Caregivers also reported the “immunity booster” in the Delpro supplement seemed to make a difference compared to their last probiotic experiences |
52 |
| Arnold et al., 2018 |
Probiotic | VISBIOME – a mixture of Lactobacilli, Bifidobacterium, Streptococcus thermophilus and starch | 19 Weeks (8 daily weeks treatment, 3 weeks washout, 8 weeks cross-over daily treatment) | ASD = 10 (3-12 years) | Trend of improved ABC irritability, ABC hyperactivity, PSI total stress and CSHQ assessments | Trend of improved PedsQL GI total score | No changes in α-diversity |
↑ % of Lactobacillus associated with improved Peds QL Scores | 53 |
| Billeci et al., 2022 |
Probiotic | VISBIOME - a mixture of Lactobacilli, Bifidobacterium, Streptococcus thermophilus and starch | 6 months | ASD receiving probiotic = 26 ASD receiving placebo = 20 |
↓ frontopolar power ↑ beta and gamma waves in the frontopolar coherence (concentration and working memory) |
N/A | N/A | Negative correlation between frontopolar coherence and peripheral TNFα Decreased power related to decreased RBS-R total scores. Increase in coherence related to increased VABS-II “Writing skills |
48 |
| Mensi et al., 2021 | Probiotic | Lactobacillus plantarum PS 128 | 6 months | ASD = 131(mean age = 7) | Improved Clinical Global Impression scores | N/A | N/A | There was an association between younger age and probiotic mediated behavioral improvements | 41 |
| Kang et al., 2017 | FMT | 2-week vancomycin treatment followed by Fecal Microbiota Transfer (1 initial high rectal or oral dose, followed by daily, oral, maintenance doses) | 18 weeks (10-week treatment, 8-week observation) | ASD = 18 (7-16 years) TD = 20(age/sex matched, no treatment) |
↑ increased total scores on the CARS, SRS, ABC, and VABS-II assessment | ↓ for abdominal pain, indigestion, diarrhea, and constipation ↓ GSRS scores |
↑ bacterial diversity ↑ Bifidobacterium, Prevotella, and Desulfovibro |
No difference between oral or rectal initial doses Bacteriophage richness and evenness were largely unchanged following treatment |
61 |
| Li et al., 2021 | FMT | Weekly FMT, rectal or oral, therapy for 4 weeks. No vancomycin or additional medication given prior to treatment. | 12 weeks (4 weekly treatment/8-week observation) | ASD = 40 (3-17 years) TD = 16 (age/sex matched, no treatment) |
↓ CARS, SAS, and SRS total scores | ↓ Hard, soft, and abnormal stools | No changes in α-diversity Reduced uniFrac distances between ASD and donor Lower Eubacterium coprostanoligenes in FMT responders |
↓5-HT, GABA, DA | 63 |
5-HT: Serotonin; ABC: Aberrant Behavior Checklist; ASD: Autism Spectrum Disorder; ATEC: Autism Treatment Evaluation Checklist; B-GOS: Biologically Active Galacto-Oligosaccharides; CARS: Childhood Autism Rating Scale; CSHQ: Child Sleep Habits Questionnaire; DA: Dopamine; DMG: Dimethylglycine; FMT: Fecal Microbiota Transfer; GABA: gamma-aminobutyric acid; GI: Gastrointestinal; GSRS: gastrointestinal symptom rating scale; IL: Interleukin; N/A: Not Applicable; PedsQL: Pediatric Quality of Life Inventory; PSI: Parenting Stress Index; RBS-R: Repetitive Behavior Scale-Revised; SAS: Social Responsiveness Scale; SRS: Social Responsiveness Scale; SCFA: Short-Chain Fatty Acids; SNAP-IV: Swanson, Nolan, and Pelham-IV-Taiwan version; TD: Typically Developing; TNF: Tumor Necrosis Factor; VABS-II: Vineland Adaptive Behavior Scales, Second Edition.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



