
Submitted:
23 October 2024
Posted:
24 October 2024
You are already at the latest version
Abstract
Stereotactic Body Radiotherapy has been established as a viable treatment option for inoperable early-stage Non-Small Cell Lung Cancer or secondary lesions mainly in oligoprogressive/oligometastatic scenarios. Treating lesions in the so-called “no flight zone” has always been challenging and conflicting data never cleared how to safely treat these lesions. This is truer considering ultra-central lesions, i.e. directly abutting or whose PTV is overlapping critical mediastinal organs. While historical retrospective data is abundant but mostly heterogenous in terms of definition of ultra-central lesions, dosing regimens and outcomes, prospective data remains scarce, even though recently published studies have given new encouraging results for such delicate treatment scenarios. For this reason, we aimed to review and summarize current knowledge on stereotactic radiation treatment for ultra-central thoracic lesions, highlighting the most recent advances and the messages that can be taken from them. Lastly, we propose a workflow of the necessary steps to identify and treat such patients, therefore helping in elucidating them with advantages and caveats of such treatment option.
Keywords:
SBRT
; ultra-central
; NSCLC
; oligometastasis
; oligoprogression
1. Introduction
For patients with early-stage NSCLC who are deemed inoperable, stereotactic body radiotherapy (SBRT) has been established as a viable treatment option [1,2,3,4,5,6], yielding comparable survival rates and lower risk of treatment-related mortality than surgery and better OS than conventional radiotherapy (RT) [7]. Furthermore, SBRT is currently one of the most widely adopted options for metastasis- directed therapy (MDT) in the setting of oligometastatic/oligoprogressive disease [8,9].
Indeed, SBRT allows delivery of high doses of radiation per fraction, with steep dose gradients, by multiple co-planar and non- coplanar beams, and guided by a set of coordinates. To achieve an ablative effect, dose schedules must be equivalent to a biological effective dose (BED) of at least 100 Gy: accumulating evidence shows that infield control exceeds 85% and grade 3 toxicities are rare (<5%) [2,10]. However, most of the available literature on SBRT outcomes in lung lesions comes from treatment of peripherally located tumors, whereas for centrally located tumors, the use of SBRT is still debated [11,12,13,14,15,16,17]. In this scenario, Timmerman et al showed that hilar and perihilar tumors treated with SBRT to 60–66 Gy in 3 fractions had an 11-fold increased risk of severe toxicity and a 2-year freedom from severe events of 54% compared with 83% of peripheral tumors, thus defining a new category of “central” lesions, i.e. located within 2cm of the proximal bronchial tree (PBT), in the so-called “no fly zone”, where moderate hypofractionation is recommended [11]. Yet, in the pivotal RTOG 0813 dose-escalation study, the 5-fractions regimen with a maximum of 12 Gy/fraction proved to be safe, with a grade 3-4 toxicity of 7% and a 2-year local control (LC) rate of 88% in centrally located NSCLC stage I patients [18]. However, selecting risk-adapted schedules of SBRT (RT), some experiences have demonstrated that RT can be safely administered also to a subset of central tumors that abut the central airway, esophagus, or other mediastinal structures, “ultra-central” (UC) tumors [10,11,12]. A recent systematic review and meta-analysis of this population confirmed a pooled incidence of grade 3–4 toxicity events of 6 %, most commonly pneumonitis, after SBRT [19]. Although no increased toxicity was reported in the 50Gy in 4-5 fraction retrospective study, other series investigating UC lung tumors have reported grade 3-5 of 30% or higher, raising concerns about the potential risk of fatal complications [20,21,22]. While dose to PBT did not increase toxicity rates, esophageal injury, such as esophageal fistula, and radiation pneumonitis were related to maximum esophageal dose and mean lung dose, respectively [23]. To this day, the literature is still contradictory and mostly based on retrospective data. Hence, the definition of UC tumors and the role of SBRT in this setting is still an unanswered question and often debated. Therefore, we performed an overview of the recent advances and current challenges in SBRT for UC lung tumors. We speculate that analyzing the general and technical requirements for prescription and dosimetric constraints could contribute to SBRT being administered safely and effectively for UC lung tumors.
2. Definition of Ultra-Central Tumors
Ultra-central definition was first introduced by Chaudhuri et al. in 2015 to indicate a subset of central tumors directly abutting the central airway (i.e., trachea and PBT) [24].
Other authors have further broadened its meaning, including in the classification of UC also those lesions with a PTV overlapping with other hilar structures (i.e. esophagus or pulmonary vessels.) [20,25,26]. However, different definitions (Table 1) have been introduced by the retrospective cohorts of UC tumors, pointing out the lack of consensus among the experts. The HILUS phase 2 trial, defined UC tumors as lesions located 1-cm zone around the carina, main bronchi, intermedius bronchus, and lobar bronchi [27]. Some authors considered planning tumor volume (PTV) and others the gross tumor volume (GTV) approaching the organ at risk (OAR). The most commonly recognized UC regions of interest are PBT, trachea and esophagus but also heart, pulmonary vein and artery are cautionally included in some definitions. The demanding dosimetric constraints recommended for the central airways and esophagus might justify this selection and the correlated risk of severe complications after SBRT of UC lung tumors. According to the meta-analysis by Yan and colleagues [19], all studies included the overlap of PTV with the PBT in their definitions, while only 59% considered GTV. The PTV overlap with other mediastinal structures, including the great vessels and esophagus, was reported in 52% of articles, whereas only 4 studies permitted direct contact of the GTV with these OAR [19].
3. State of the Art for SBRT for Ultra-Central Tumors
To better describe the actual state of the art for SBRT in UC thoracic lesions, we conducted a critical review of the available data, searching through medline, EMBASE and Google Scholar for published articles reporting a specific research string (hypofractionated[tw] OR stereotactic[tw] OR SABR[tw] OR SBRT[tw] OR radiosurgery[mh] AND (ultracentral*[tw] OR ultracentral*[tw] OR ultra-central*[tw] OR central*[tw]) AND (lung[tw] OR thorac*[tw] OR pulmonary[tw] OR lung neoplasms[mh]) and a time span between 01 Jan 2019 to 09 Feb 2022. Among the 301 results, 105 articles were selected by titles. We excluded 1/retrospective case series of less than 10 patients, 2/series of central lesions only or mixed for which no UC data was retrievable, 3/papers regarding only quality assurance or dosimetry calculations and 4/articles regarding SBRT to other disease sites. Hence, we included 38 articles whose authors, year of publication, definition of UC applied, design, dose fractionation and main findings are summarized in Table 1. We adopted 01 January 2019 as starting point for our research due to the systematic review published by Chen H and colleagues [28]. Since 2019 only 6 prospective studies including UC lesions treated with SBRT results were published, while all the rest of data is provided by retrospective series.

Table 1.
Summary of main findings from studies on treatment of Ultra-central lung tumors.
| First Author and year [reference] | Sample size (treatment years) |
Type | Definition of Ultra-Central |
Primary Lung cancer pts | Met pts | Fractions*dose per fraction | Median tumor max D or GTV volume | Median FuP (mo) | SBRT technique |
Main Results and comments |
|---|---|---|---|---|---|---|---|---|---|---|
| Swaminath, 2024 [32] |
23 pts (2014 – 2020) |
Phase III (RCT conventional RT vs SBRT, not stratified for UC tumors) | Tumors abutting PBT or mediastinal organs | 23 (100%) | 0 | 8*7,5 Gy | 25 mm (general population) | 36,1 | 3DCRT, VMAT, IMRT, CK allowed |
3-ys LC 87.6%, EFS 49,1%, OS 63,5% (overall SBRT population). 1 (4,3%) late (12 months) G5 hemoptysis in a tumor abutting proximal bronchus. 4 (17,4%) G≥3 TRAEs. No dosimetry issues according to protocol were found in G5 event. |
| Giuliani, 2024 [31] |
30 pts (2018-2021) |
Phase I | PTV touches or overlaps the central bronchial tree, esophagus, pulmonary vein, or pulmonary artery | 30 (100%) | 0 | 8*7,5 | 26 mm | 36 | 3DCRT, VMAT, CK allowed | 3-ys OS 72.5%, PFS 66.1%, LC 89.6%, RC 96.4%, and DC 85.9%. 6.7% G3-5 TRAEs: 1 G3 dyspnea and 1 G5 pneumonia. PTV Dmax limited to 120%; tumors with endobronchial invasion were excluded. |
| Levy, 2024 [30] |
6/31 pts UC (2015-2017) |
Phase II | GTV ≤1cm from trachea or mainstem bronchi; central: ≤2 cm from PTB or immediately adjacent to pericardial or mediastinal pleura | 6 (100%) | 0 | 8*7,5 | 26 mm | 43 | IMRT, VMAT, Tomotherapy allowed | 3-ys cumulative rate of LP 6,7%. 3-ys PFS and OS 81.5% and 61.1%. 16,1% G≥3 and 3,2% G5 (pneumonitis) early AEs. 58.1% G≥3 and 3.2% G5 (hemoptysis after bronchoscopy) late AEs. |
| Rim, 2024 [41] |
20 (2017-2021) |
Retrospective | Tumor abutting or invading PTB. | 20 (100%); 2 recurrents, 1 SCLC. |
0 | 10*4,5 (5%) 10*5-6 (95%) |
35 mm | 15,8 | IMRT, VMAT | 1-y and 2-ys OS rates were 79.4% and 62.4%, 1-y and 2-ys LC rates were 87.1% and 76.2%. 1 (5%) G≥3 AE = G5 hemoptisis (patient with endobronchial involvement) = 5%. Dmax <110% |
| Bryant, 2024 [42] |
14 (2019-2021) |
Retrospective | GTV ≤1cm from trachea or mainstem bronchi | 9 (64,3%) | 5 (35,7%) |
8*7,5Gy | 17,8 cc | 17,2 | IMRT MRI-guided |
2-ys LC, LFFS, OS, and PFS rates were 92.9%, 85.7%, 92.9%,and 64.3% No acute or late G≥3 AEs. Adaptive plan permitted PBTDmax of 5,7 Gy and GTV D95% at 99,8%. Hotspots ≤120%. |
| Li, 2024 [38] |
154 (2009-2019) |
Retrospective | PTV abutting or overlapping central bronchial tree or esophagus |
32 (20%) treated in curative setting |
122 (80%) | 5*10 most common (42%) 5*6-11 (median 9) |
27 mm | 21,5 | IMRT, VMAT | mOS 44 months, mPFS 8.8 months. 3-ys LC 86%. G3 acute AEs = 3%, 2 esophagitis, 1 atrial fibrillation, 1 pericarditis, 1 pleural effusion. G≥3 late AEs = 4,9%, 3 G3 pneumonitis, 1 G3 chest wall pain, 1 G3 bronchopleural fistula; 1 G4 esophagitis, 1 G4 bronchial obstruction; 1 G5 pneumonitis. Tumor volume overlapping with esophagus correlated with worse LC. Predictors of severe toxicity = PTV size, decreased PTV V95%, lung V5 Gy, and lung V20 Gy. |
| Lee, 2024 [54] |
19 (2019-2022) |
Retrospective | GTV abutting PTB, esophagus or great vessels. GTV ≤2 cm from PTB and mediastinum considered central. | 0 | 19 (100%) | 5*7-12 (median 10) | NR | 19 | IMRT MRI-guided adaptive RT | 1-y and 2-ys LC was 94% and 86%. Median time to distant recurrence 6,6 months. 32% G2 acute toxicities, no other AEs. Plan adapted with isotoxic approach. Re-optimization showed better PTV coverage than original plan. 85% patients had immune and TKI therapy <1 months before SBRT. VEGFRi held >4 weeks before. |
| Ahmadsei, 2023 [52] |
60 (2014-2021) |
Retrospective | PTV overlapping or abutting the PBT, trachea or esophagus | 27 (45%) | 33 (55%) | 8*5-6 Gy 10*4,5-5Gy |
30-70 mm for 66,7% patients. | 26,4 | VMAT | 2-ys OS 65,9% 1-y and 2-ys LC 84,4% and 76,8% 2-ys DC 45% 3% G≥3 Aes: 1 G3 and G4 pneumonitis. 20% cardiovascular events at 2 years: 10% valvopathy, 8,3% atrial fibrillation. Hypothetic association between dose to pulmonary artery and superior cava vein and non-cancer related deaths. No other cardiac substructures dosimetry concerns. |
| Iovoli, 2023 [88] |
49/93 UC pts (2007-2021) | Retrospective | Directly abutting any of proximal airway, mediastinum, great vessels, spinal cord. ≤2 cm categorized as central |
93 (100%) | 0 | 5*10-12 Gy | NR | 32,4 | 3DCRT, VMAT | SAN Dmax and Dmean significantly associated with worse OS with cut-off values of 1309 and 836cGy. |
| Lindberg, 2023 [29] |
230 pts/238 lesions (2010-2018) |
Phase II (65 pts) + retrospective series (165 pts) | UC (groups A,B,D) 1-cm zone around the carina, main bronchi, intermedius bronchus, and lobar bronchi (i.e., the PBT) C (group C): 1-2 cm around the PBT |
196 (77%) | 54 (23%) | 8*7 Gy | 35 mm | 24 (phase II series, nr for overall cohort) | VMAT | 1-y, 3-ys and 5-ys LC rates at were 92%, 84% and 78%. 1-y, 3-ys and 5-ys OS rates were 78%, 40% and 27%. G 3-4 toxicity in 15% pts, and 13% (30pts) had G5 tox (20 hemoptysis, 7 pneumonia, 2 cardiac failures, 1 COPD). Tumor compression of PBT and high maximum dose to the mainstem or intermediate bronchus increased the risk of fatal toxicity. |
| Song, 2023 [46] |
27 pts (2013-2018) |
Retrospective | PTV touching or overlapping the central bronchial tree, esophagus, or pulmonary artery | 27 (100%); 4 recurrent | 0 | 10*6 Gy 7*8 Gy |
37 mm | 41 | IMRT | mOS and mPFS 48 months and 36 months. G≥3 AEs in 5 pts (18,5%): 1 G3 pneumonitis, 2 G3 bronchial obstructions, 1 G5 bronchial obstruction, 1 G5 esophageal perforation. No difference in outcomes, but higher toxicity when compared to analogous central tumors series (G3 =0), with higher Dmax to lungs, bronchus, esophagus and heart. |
| Tonneau, 2023 [33] |
65 lesions (2009-2019) | Retrospective | PTV touching or overlapping the central bronchial tree, esophagus, pulmonary vein, or pulmonary artery. |
65 (100%) | 0 | Mostly 5*10 Gy | NR | 37,6 | VMAT, Cyberkinfe, Tomotherapy | After 37,6 months median follow-up: 10% LR, mOS 37,3 months and mDFS 36,6 months. 2 G5 TRAEs: pneumonitis. Comparison with central and peripheral pts from same center: higher RR e DR with UC lesions (CHR 2.44, 2.15); shorter OS and PFS versus central and peripheral lesions. BED10 <120 correlated with higher LR, RR e DR risks. |
| Tekatli, 2023 [49] |
94 pts (2008-2015) |
Retrospective | GTV ≤1cm from PBT | 94 (100%) | 0 | 8*7,5 Gy 12*5 Gy |
44 mm | 40,5 | VMAT | Considering additional 33 C lesions: mOS 25 months; 3-ys and 5-ys LC 78% and 69%; 3-ys and 5-ys RC 81% and 72%. G≥3 AEs = 20% of which 21% pulmonary, 1% bone fracture. G5 = 12%, all pulmonary, mostly >12 months. Location ≤1 cm from trachea or bronchus and PS 2-3 correlated with pulmonary toxicity. |
| Regnery, 2023 [47] |
16 patients/ 16 lesions 2020-2021 |
Prospective database | PTV overlapping with the PBT or esophagus |
4 (25%) | 12 (75%) | 12*5 Gy 10*5.0-6Gy 8*7,5 Gy 8*5 Gy 6*5 Gy 5*6 Gy |
NR |
24 | IMRT MRI guided adaptive RT | 2-ys OS 67%, 2-ys PFS 37%, 2-ys LC 93%. AEs G≥2 = 56%, 1 G3 bronchial bleeding, 1 G4 bronchial bleeding (further treated with VEGFRi), 1 G3 esophagitis. Lowest BED fractionations used for tumors abutting esophagus. Comparison with C tumors treated with MRI-IMRT: Higher AEs rates but no difference in outcomes. |
| Sandoval, 2023 [37] |
38/47 ultra- central patients (2019-2021) |
Retrospective | GTV ≤1cm from trachea, mainstem bronchi or PBT. C lesions defined as ≤2cm from PBT, mediastinum or pericardium |
22 (46,8%) | 25 (53,2%) | 3*18 (3,5%) 5*10-12 (25,6%) 8*7,5 (47%) 10*5 (6%) 15*4 (17,9%) |
NR | 22,9 | IMRT-MRI guided adaptive RT | 1-y LC 87% (median NR), 1-y OS was 82% (median NR), 1-y PFS was 54%. No acute G≥3 toxicity, 5% late G3 toxicities: esophagitis and pneumonitis. G2 toxicity associated with GTV volume. No statistical outcome differences between UC vs non-UC lesions. |
| Rock 2023 [89] |
50 patients (2009-2020) | Retrospective | PTV overlap or direct tumor abutment with the major vessels, esophagus, or central airway | 34 (68%) | 16 (32%) | 10*4-7 Gy (median 6,5) | NR | 13 (range 0,3 -102) | 3DCRT; IMRT; VMAT | Primary NSCLC: 1-y LC = 83.8%, 3-ys LC = 65.4%; 1-y PFS = 50.1%, 3-ys PFS = 26.8%; 1-y OS = 93.7%, 3-ys OS = 70.5%. Oligometastatic: 1-y LC = 85.2%; 1-y PFS = 12.5%, 1-y OS = 88.9%, 3-ys OS = 44.4%. G≥2 Aes = 22%: 12% G2 pneumonitis, 2% G3 pneumonitis, 2% G2 airway obstruction, 4% G3 obstruction, 2% G5 hemoptysis. |
| Hiroshima, 2022 [43] |
16 patients (2017-2020) | Retrospective | Within 2cm within the PBT | 16 (100%) | 0 | 10*6Gy 4*13,75Gy |
NR | 14,4 | IMRT or VMAT (1-4 fiducials; 4D CT scan) | No LR. OS, cancer-specific survival and PFS at 2 ys: 54.6%, 85.1%, and 33.7% 1 G3 radiation pneumonitis (no other G≥3 Aes). |
| Ligtenberg, 2022 [44] |
12 patients, (2017-2019) | Retrospective | Proximity to the mediastinum | 12 (100%) | 0 | 8*7,5Gy | NR | NR | IMRT or VMAT | MidP-based treatment yield lower OAR doses compared to ITV-based treatment plans on the MR- linac (Mean lung dose significantly lower, difference: -0.3 Gy; p < 0.042). |
| Farrugia, 2022 [53] |
83 patients, (2010 – 2019) | Retrospective | C: < 2 cm within the proximal airway, mediastinum, great vessels, or spinal cord; UC: directly abutting any of the above structures |
83 (100%) | 0 | 5*10Gy; 5*11Gy. | <20mm 68,7% | 33,4 | 3DCRT/ VMAT |
At log rank test and MVA, D45% right atria constraint (candidate cutoff values of 890cGy) was significantly associated with non-cancer associated survival and overall survival. |
| Salvestrini, 2022 [48] |
122 pts/126 lesions (2006/2020) | Retrospective | PTV touches or overlaps the trachea, mainstem-, intermediate-, upper-, middle- or lower- lobe bronchus or the esophagus |
68 (54%) | 58 (46%) | 7*7-8 Gy 6*8 Gy 5*9-12Gy |
37,5 mm | 23 | Cyberknife | 1-,2-, and 5- ys OS rates were 75%, 58%, and 23% 1-, 2- and 5-ys PFS rates at were 63%, 41%, and 15% 1-, 2-, and 5-ys LC rates were 86%, 78%, and 61%. Acute G2 dysphagia, cough, and dyspnea were 11%, 5%, 3%. Acute G3 dyspnea was 0,8%. Late G3 AEs rate = 4%. Tumor size and location close to the trachea rather than PBT correlated with better OS. |
| Wang, 2022 [90] |
58 pts (2010-2018) |
Retrospective | PTV touching or overlapping the PBT, trachea, esophagus, heart, pulmonary vein, or pulmonary artery within 2 cm around the bronchial tree in all directions | 58 (100%) | 0 | 7*8 Gy, 8*7Gy, 6*9,3Gy |
NR | 57 |
Cyberknife | 1-, 2- and 5-ys OS rates were 94.7%, 75.0%, and 45.0%. 1-, 2- and 5-ys LC rates were 91.5%, 78.0%, and 58.6%. G≥3 Aes = 3.5%. Pts with PTV <53.0 cc = better OS. |
| Guillaume, 2021 [56] |
74 pts/ 74 lesions (2012-2018) |
Retrospective | PTV overlapped one of the following OARs: the trachea, right and left main bronchi, intermediate bronchus, lobe bronchi, oesophagus, heart. |
37 (50%) | 37 (50%) | 5-10* (4.5-10 Gy) | 18,3 cc | 25 | CyberKnife, VMAT |
1-y LC rate 96.7%, 2-ys LC rate 87.6% mPFS 12 months. mOS 31 months. G3 AEs = 2.7%. No G4-5 AEs. The type of OAR overlapping with PTV didn’t relate to AE risk. LR more common with GTV receiving Dmin BED10 ≤50 Gy (p = 0.002). |
| Farrugia, 2021 [50] |
43 pts (2010-2019) |
Retrospective | GTV abutting the proximal bronchial tree, trachea, mediastinum, aorta, or spinal cord. | 43 (100%) | 0 | 5* (10-11Gy) | 12,4 cc | 29 | 3DCRT/ VMAT |
UC location was associated with worse non-cancer associated survival and OS, supposedly due to excessive D4cc (of 18Gy) dose to the proximal airways. |
| Breen, 2021 [59] |
110 pts (2008-2019) |
Retrospective | GTV directly touching the PBT or trachea. 2) PTV overlapping the trachea or mainstem bronchi.GTV within 1 cm of the PBT. |
110 (100%) | 0 | 4-8* (7.5-12Gy) (no 7 fractions) |
17.7cc | 30 | 3DCRT, VMAT | OS at 1, 2, and 5 ys was 78%, 57%, and 32% Local progression at 1, 2, and 5 ys was 4%, 16%, and 21%. Acute and late grade 2 + toxicity was seen in 18% and 27%. Four patients (4%) had fatal toxicity. |
| Lodeweges, 2021 [51] |
72 pts (2012-2020) |
Retrospective | PTV abutting or overlapping the main bronchi, trachea and/or esophagus | 72 (100%) | 0 | 12* 5Gy | NR | 19 | VMAT | 3-ys and 2-ys LC rates were 98% and 85%. OS rates at 1- and 2-ys were 77% and 52%. G ≥ 3 was observed in 21%, of which 10 patients (14%) with G≥5 bronchopulmonary hemorrhage. grade >3 toxicity found correlated with Dmean to the main bronchus (p = 0.003), with cutoff value of BED3 = 91 Gy. |
| Mihai, 2021 [57] |
57 pts (2008-2016) |
Retrospective | (GTV) abutting or involving trachea, main or lobar bronchi. | 37 (65%) | 20 (35%) | 4-10* (5-12Gy) (no 7 fractions) |
NR | 26.5 | IMRT | mOS was 34.3. Freedom from local progression at 2 and 4 years was 92 and 79.8%. Fatal hemoptysis 8.7%. |
| Regnery, 2021 [35] |
51 pts (2012-2019) |
Retrospective | Overlap of the PTV with the PBT | 37 (72.5%) | 14 (27.5%) |
10*5Gy | NR | NR | 3D, helical Tomotherapy, or VMAT | 2-ys local failure rate UC = 26.9%; C = 14.6%. 2-ys OS C = 55.4%; UC = 54.9%. 2-ys AE G≥3 15.3% for UC and 7.3% for C lesions. No grade 4 toxicity and only 1 potential grade 5 tox in UC cohort. |
| Cooke, 2020 [66] |
27 pts | Retrospective | NR | 0 | 22 (81%) | 6* 10Gy (no 7 fractions) | 6.6 cc | 11.6 | IMRT, VMAT | 1-year OS 82.7 2-year OS 69.5 1-year IFC 95.2% 2-year IFC 85.7% No AEs G>3 |
| Loi, 2020 [39] |
109 pts (NR) | Retrospective | PTV overlapping with central bronchial tree, esophagus, pulmonary vein, or pulmonary artery |
0 | 109 (100%) | 5-10*(6-10) Gy | 60 cc | 17 | VMAT | 2-ys LC 87%. Improved LC was correlated to PTV V95% > 85% and to GTV< 90cc. Overall and G≥3 toxicity incidence was 20% and 5%, respectively. |
| Shahi, 2020 [60] |
52 pts (84 mets) (2014-2019) | Retrospective | NR | 0 | 52 (100%) | 5* (6-10) Gy | 20 mm | 20 | VMAT | 2-ys Local failure was 9.0%. Median PFS was 4.0 months, and median OS was 31.7 months. AEs G>3 in 6 (11.5%) pts, 71% transient. There was a single (1.9%) G 5 toxicity (radiation pneumonitis). |
| Wang, 2020 [23] |
88 pts (2008-2017) |
Retrospective | GTV abutting the proximal bronchial tree or PTV overlapping esophagus | 53 (60%) | 35 (40%) | 5 * 9-10Gy 8 * 7,5 Gy 15 * 4 Gy |
NR | 19,5 | IMRT, VMAT | 1 and 2-ys rates of local failure were 12.2 % and 19.0 %. 1, 2 and 3-ys OS rates for pts with primary NSCLC were 78.6 %, 64.5 % and 53.1 %. AEs G≥3 22%, including 6 (7%) G≥3 radiation pneumonitis and 4 (4%) G≥3 esophageal injury. TRAEs G5 in ten pts (11.4 %) = hemoptysis, radiation pneumonitis, respiratory failure. BED10 ≥ 100 didn’t correlate with local control (UVA); lung V20 correlated with G≥2 pneumonitis, not dose to PBT; Dmax, D2.5cc, D5cc to esophagus correlated with G≥3 esophageal AE. |
| Zhao, 2020 [40] |
98 (2013-2017) |
Retrospective | PTV overlapping with PBT, esophagus, pulmonary vein or pulmonary artery | 76 (77.6%) | 22 (22.4%) | 8*7,5Gy | NR | 22.9 | 3DCRT, IMRT or VMAT | 2-ys and 3-ys LC, 97.8 and 84.5%. AEs G3 = 3 in the C group (2 dyspnea, 1 pneumonitis) and 2 in the UC group (1 dyspnea, 1 hemoptysis). No G>3 toxicities. ITV predictor for LC (p = 0.001). |
| Yang, 2020 [45] |
21 patients, 2012 – 2018 | Retrospective | UC: PTV abutting or overlapping central structures (including PBT, heart, and great vessels but not the esophagus) | 21 (100%) | 0 | 8*7,5Gy | NR | 15 | VMAT | The 1- and 2-ys OS rates were 87.5% and 76.6%. The 1- and 2-ys PFS rates were 71.1% and 64.0%. The 1- and 2-ys LC rates were 92.9% and 92.9%. AEs G2 19.1%. No G ≥ 3. |
| Duijm, 2019 [58] |
188 patients, 2012 – 2016 | Retrospective | UC: GTV ≤ 2 cm of the esophagus, trachea, mainstem, intermediate, upper, middle or lower lobe bronchus | 154 (82%) | 34 (18%) | 8*7,5Gy; 12*5Gy |
36 mm | NR | VMAT | Acute AEs: G1 (n = 19) and G2 (n = 10) only. Late AEs: 2 possible treatment-related deaths and 2 G3. DVH significantly correlated to acute and late AEs. |
| Meng, 2019 [34] |
80 patients, 2006 – 2015 | Retrospective | C: GTV < 2 cm of, but not abutting, the PBT UC: GTV abutting the PBT |
80 patients (100%) | 0 | 10*6Gy (C); 7*8Gy (UC) |
NR | 44,5 | CK | UC tumors showed worse OS, PFS, and LC compared to C lesions. On MVA, UC and PTV were poor prognostic factors. Toxicity profile similar in the two groups (UC vs C). |
| Cong, 2019 [91] |
51 patients, 2014 – 2017 | Retrospective | UC: GTV abutting or over- lapping the trachea or PBT | 51 patients (100%) | 0 | 5*7Gy | 68 mm | 17 | CK | Median LC was 17 months for stage III pts and 11 months for stage IV or recurrent pts. G3 radiation pneumonitis was recorded in 3 pts (5.9%) and possible treatment-related death in 2 pts (3.9%). |
| Bezjak, 2019 [18] |
120 patients (100 pts PP analysis, 17 UC), (2009 – 2013) |
Prospective, phase I/II study | C: GTV< 2 cm around the PBT or immediately adjacent to the mediastinal or pericardial pleura | 120 (100%) (100 pts PP analysis) | 0 | q 2 day fractionation X 5 fractions over 1.5-2 weeks: Dose Level 1: 5*8Gy 2: 5*8,5GY 3: 5*9GY 4: 5*9,5GY 5: 5*10Gy 6: 5*10,5GY 7: 5*11GY 8: 5*11,5Gy 9: 5*12Gy Protocol treatment begins at Level 5. Levels 1-4 employed if DLT is seen with the Level 5 |
11,2 cc |
37,2 | 3DCRT; VMAT; IMRT | MTD was 12.0 Gy/fx, with a probability of a DLT of 7.2%. 2-year LC rate in this cohort was 87.9%. 2-year PFS in this arm was 54.5%. 2-year OS was 72.7%. Four pts (12.1%) experienced G3 AE during the first year; 1 pts (3%) reported G5 toxicity >1year. |
| Nguyen, 2019 [36] |
68 patients, (2009 – 2017) | Retrospective | C: PTV <2 cm of the PBT UC: PTV overlapped the PBT or esophagus |
53 (78%) | 15 (22%) | 8*5Gy 5*8Gy; 5*10Gy; 4*12,5Gy; 5*11Gy; 8*7Gy; 8*7,5Gy; 5*12Gy. |
NR | 19,7 | IMRT; VMAT | The 2-year estimates of LC (89% and 85%; p 0.72) and OS (76% and 73%; p 0.75) for UC and C tumors were similar. UC tumors increased risk of G2 tox (57.6% vs 14.2%; p 0.007) at 2 years. One patient with an UC tumor developed G5 respiratory failure. |
Abbreviation: UC, Ultra-central; C, central; LC, Local control; OS, Overall survival; G, grade; pts, patients; EFS, Event-free survival; PFS, progression-free survival; NR, not reported; AE, adverse events; TRAE, treatment-related adverse events; NSCLC, non-small-cell lung cancer; DVH, dose-volume histogram; MTD, maximum tolerated dose; DLT, dose limiting toxicities; MVA, multivariate analysis; PTV, planning target volume; ITV, internal target volume; OAR, organ at risk; tox, toxicity; IMRT, Intensity Modulated Radiation Therapy; VMAT, Volumetric Modulated Arc Therapy; CK, Cyberknife; 3DCRT, Three-dimensional conformal Radiation Therapy; SAN sinoatrial node; LR, local recurrence; RR, regional recurrence; DR, distant recurrence; MRI, magnetic resonance imaging; MidP, Mid position.
3.1. Survival Outcomes and Toxicity with SBRT for Ultra-Central Tumors: Prospective Data
Prospective studies so far published enrolled a maximum of roughly 30 patients with UC thoracic lesions in dedicated or mixed cohorts. From the first historical phase I/II study RTOG 0813 trial, it was reported a 2-years LC, PFS and OS rates of 87.9%, 54.5% and 72.7%, respectively, in patients treated with 60Gy/5fx dose level (deemed to be the maximum tolerated dose within the study) even though most UC patients were treated within the 57,5Gy/5fx level. Treatments were delivered with IMRT, VMAT or 3DCRT. Notably, within the highest dose level (60Gy/5fx) only 1 patient reported a late G5 event (3%) [18].
In 2023 an expanded group analysis of the Hilus trial was published, confirming the warning points previously highlighted from the original prospective phase II study which enrolled a total of 65 patients. In order to report outcomes coming from a larger population, the authors added a retrospective series of 165 UC patients (defined as per Hilus protocol within groups A, B, D) that were all treated with 56Gy/8fx schema. Control and OS rates were aligned with RTOG study, with 1-year, 3-years and 5-years LC and OS rates at 92%, 84%, 78% and 78%, 40%, 27% (to be noted that patients with unresectable early stage or metastatic NSCLC were included), respectively. The warning sign coming from this study when treating UC tumors with SBRT is the treatment-related toxicity rates reported with 30 (13%) fatal toxicities: 20 hemoptysis, 7 pneumonitis, 2 cardiac failures and 1 COPD. Authors found out also that treating a tumor compressing the PBT and the Dmax to mainstem or intermediate bronchi were correlated with a higher risk of fatal toxicity and for this reason they eventually suggested that dose constraints used for main bronchi should be applied to intermediate bronchi as well when treating such high-risk lesions [29].
More prospective data raising concerns on the treatment of UC lesions comes from the Lungtech trial recently published. The trial was closed early due to poor accrual, slowed also for enrollment suspensions due to fatal AEs. Thirty-one patients with centrally located tumors including 6 patients with UC primary NSCLC were treated per protocol with IMRT, VMAT or Tomotherapy at 60 Gy/8fx dose. Survival outcomes were favorable for tumor control and overall survival (OS), with 3-y cumulative local recurrence at 6,7%, 3-y OS and PFS at 61,1% and 81,5%. Toxicity rates were once again concerning, with early G≥3 AEs at 16,1% and 1 fatal pneumonitis and late G≥3 AEs rate at 58,1% (mainly pulmonary): 1 fatal hemoptysis occurred after a procedural bronchoscopy. Even though not strictly treatment-correlated, other 5 late fatal AEs were also reported (for a total of 19,4% reported G5 AEs). These are the tolerability results even though the dose constraints adopted within the trial were more cautionary than the other prospective trials, with GTV Dmax hotspots <130% vs 150% in the Hilus trial, Dmax EQD2 to the PTB 81,9 Gy (the lowest within trials presented so far) and 5 mm PTV expansion. Another concern highlighted from the study is the risk of complications in patients undergoing thoracic invasive procedure after having received SBRT for UC lesions, mainly with regards of the PBT [30]. Such trial highlights the importance of considering patients’ comorbidities at baseline and of following up patients carefully even at distance from treatment for the emergence of late severe adverse events.
On the other hand, completely positive data in treating UC lesions with SBRT comes from the more recent SUNSET trial. It is a phase I study where treatment dose for the first patients was established at 60 Gy/8 fx. Subsequent dosing might be, per protocol, escalated or de-escalated (60 Gy/5-6 fx or in 10-15 fx) according to toxicity outcomes (i.e. time-to-event continual reassessment method). After amendment only de-escalation option was allowed and eventually all 30 patients with primary NSCLC enrolled in the trial received the 60 Gy/8fx schedule. Outcomes data were comparable to the other studies reported: 3-years OS was 72.5%, PFS 66.1%, LC 89.6%. Crude regional control (RC) and distant control (DC) rates were 96.4% and 85.9%, respectively. Toxicity data reported only two patients (6.7%) experiencing G3-5 adverse events related to treatment: 1 G3 dyspnea and 1 G5 pneumonia. Such important results were possible probably thanks to strict patient selection and dosimetry constraints: the PTV Dmax hotspot was limited to 120% and tumors with endobronchial invasion were excluded [31].
The most recent prospective data comes from the LUSTRE trial. This is the only phase III randomized trial including UC lesions reported so far, even though not specifically designed for UC tumors. The trial aimed to assess the superiority of SBRT (48 Gy/4fx or 60Gy/8fx for central/UC lesions) vs. conventional radiotherapy (60Gy/15fx) in treating primary early-stage NSCLC. Even though not stratified for UC lesions specifically, but generically for peripheral vs. central/UC lesions, it included 23 (15%) UC lesions in the SBRT arm. So far, outcome data has been reported only for the whole SBRT arm population, with three-years LC 87.6%, event-free survival (EFS) 49,1%, OS 63,5%, but toxicity data was reported separately, with only 1 (4,3%) late (occurring at 12 months follow-up) G5 hemoptysis in a tumor abutting proximal bronchus. Overall, 4 (17,4%) G≥3 treatment-related events in the UC SBRT sub-population were reported [32].
3.2. Survival Outcomes and Toxicity with SBRT for Ultra-Central Tumors: Retrospective Data
While prospective data mainly point to assess feasibility and toxicity of 60 Gy/8fx dose regimen, retrospective data have a higher variability with different impact on survival and toxicity outcomes (Table 1).
Treatment regimens reported vary from 4 to 12 fractions and from 4,5 Gy to 13,75 Gy per fraction with survival outcomes roughly superposable with those of prospective data, when accounted for commons biases related to retrospective series, having some of them also including very few patients.
Some series found out anyway worse local control when compared to analogously treated central lesions [33,34,35], while others didn’t [36,37]. A possible explanation to that could be the mean higher tumor volume for UC lesions and closer proximity to critical structures such as PBT or esophagus among others which could ultimately lead in a worse PTV dose coverage or lower total dose prescription as reported from the statistical analysis in some series, where such parameters correlated with LC [33,38,39,40], even though in another series of 88 patients treated with IMRT or VMAT between 2008 and 2017 a BED10≥100 didn’t correlate with LC at univariate analysis [23].
With respect to toxicity the rates of severe adverse events are variable and this may be due to different dose regimens used, reporting biases and small population numbers in some series [41,42,43,44,45], but even within small series important toxicity warnings are sometimes shown, with G≥3 AEs rates of 18% [46,47] and G5 events that are confirmed within many series even though sporadically.
The most common severe up to G5 AEs reported are respiratory (pneumonitis, hemoptysis, fistulae) and esophageal (fistulae), with higher rates reported according to lesions location, volume or specific dosimetry parameters. Specifically, higher AEs rates and grades were found across many series to be correlated with endobronchial invasion or close proximity to PTB rather than trachea [41,48,49,50], which is in accordance with prospective data reported. Other parameters linked to this concept reported to be correlated with worse toxicity outcomes are the GTV/ITV rather than the PTV [37,38,48] or Dmax to bronchi, lungs or esophagus rather than lungs V5 or V20 [38,46]. Notably, in the series from Wang et al., including 88 patients, esophagus D2.5cc and D5cc were significantly correlated with the risk to develop G≥3 esophageal events [23], whereas the main bronchus Dmean BED3 >91Gy increased significantly the risk of G≥3 respiratory AEs in another series of 72 patients from Lodeweges et al. [51].
According to some series there seems to be a possible reporting bias risk in studies for SBRT in UC lung lesions with regards especially to cardiac toxicity, where some studies do not report severe cardiac SBRT-related toxicity, while non-cancer related mortality is sensibly increased even several years after SBRT. A study from Ahmadsei et al. evaluated dosimetry to cardiac substructures in 60 patients who underwent SBRT for UC lesions. While only 3% G≥3 AEs were reported, at a follow-up of 2 years it was detected a 20% incidence of cardiovascular events (valvulopathy and atrial fibrillation mainly), with a positive correlation between dose to pulmonary artery and superior cava vein and non-cancer related deaths in this population [52]. Similarly in a 49 patients series treated with 50-60Gy/5fx from Iovoli et al., Dmax and Dmean to the sinoatrial node were found to be correlated with worse OS at cut-off values of 1309 and 836cGy respectively. Moreover, in a multivariate analysis of another 83-patients series treated with 50-55Gy/5fx it was reported that D45% right atrium constraint (with candidate cutoff values of 890cGy) was significantly associated with non-cancer related survival and overall survival [53].
Of note, there is a growing interest with regards to adaptive radiotherapy with MRI-based linacs, which enables an optimal tumor tracking, permitting ablative doses with better-tailored dose distribution and less target uncertainty.
In 2023 Sandoval et al., reported a retrospective series of 38 patients treated with this technique. Prescribed dose was in roughly half of cases 60Gy/8fx and efficacy outcomes where comparable with CT-based linacs, but with no acute toxicities and only 5% late G3 toxicities, with no differences between central et UC lesion treated from the same series [37].
Other two more recent series were published this year with a total of 36 patients that were treated with 50Gy/5fx (as a median) or 60Gy/8fx, respectively. Both series, even though numerically small, report no adverse acute or late G≥3 events at a median follow-up of about 1,5 years. One series reported a PTB Dmax improvement of 5,7Gy ((59.4 Gy vs. 65.1 Gy) [42] and the other showed that the adaptive-RT approach permitted a more adequate PTV coverage compared to the original plan [54].
A series of patients from prospectively maintained databases with MRI-Linac was published in 2023 and included 16 UC patients that were treated at different dose levels ranging from 30-60 Gy in 5 fx, with the lowest dose levels prescribed to lesions abutting to esophagus. At a median follow-up of 24 months, LC was 93% and 1 G3 esophagitis, 1 G3 bronchial bleeding and 1 G4 bronchial bleeding (in a patient receiving also VEGFR inhibitors) were reported [47].
4. A Proposal for Practical Workflow for Treatment of Ultra-Central Tumors
The following sections will overview the general and technical requirements for the treatment of UC tumors. Each phase of the patient workflow in the radiotherapy department will be described and reviewed according to available literature. This includes the patient's eligibility for SBRT, the completion of treatment, and the subsequent follow-up. Figure 1 outlines the workflow of the topics covered in the next sections.
4.1. Patient Eligibility
Patient eligibility for lung SBRT follows specific indications, with no age absolute contraindications [55]. Many studies have included and analyzed patients of a wide age range with no reported special concerns [18,27,36,39,40,45,51,57,58,59,60]. Historically, SBRT for lung lesions was recommended as a therapeutic option for a subset of patients who were not suitable for surgery due to medical comorbidities, anatomic limitations, or even patient refusal [61]. As per ESMO guidelines, the postoperative morbidity and mortality can be assessed by defined models which have not been validated specifically for cancer patients. Indeed, it is mandatory to test cardiac and pulmonary function before planning surgical resection in order to estimate the risk of surgical morbidity [62]. The inoperability condition is also determined by poor lung function, which is evaluated using the following parameters: predicted forced expiratory volume in 1 second (FEV1) < 40%, predicted postoperative FEV1 < 30%, baseline hypoxemia (≤70 mmHg), hypercapnia (>50 mmHg), predicted reduced diffusing capacity < 40%, and predicted exercise capacity < 50%. Other severe comorbidities, such as severe pulmonary hypertension, diabetes mellitus with end organ damage, severe cerebral, cardiovascular, or peripheral vascular disease, or severe chronic heart disease, contribute to a condition of inoperability [2,63]. Unlike surgery, SBRT does not have a cut off for lung function or other conditions, making it a viable therapeutic alternative even for patients with poor pulmonary function [63,64]. On the other hand, patients with estimated life expectancy of <1 year, active systemic, pulmonary, or pericardial infection, and pregnant or lactating women was identified as contraindications for thoracic SBRT [2,6]. Conversely, eligible criteria for lung SBRT consisted of a centrally located inoperable primary lung cancer or a metastasis from any other solid tumor [27]. Eligible patients should have a good performance status, defined as an Eastern Cooperative Oncology Group score of 0 to 2, and an early-stage tumor (T1-T3, N0, M0 as per the American Joint Committee on Cancer 8th edition staging) [31]. Regarding tumor size for defining the eligibility of patients for SBRT, a cut-off of 5 cm has been established by some authors [2,50,63]. However, more recently the recommended tumor size was extended to 6 cm [31].
4.2. Simulation Phase and Immobilization Devices
The simulation phase for SBRT of UC lung tumors must consider two critical issues: the tumor motion assessment and the patient immobilization strategy [65].
Regarding the need to evaluate tumor movement, the images required for simulation and planning often include detailed 4D-CT scan. The 4D-CT is adopted for analyzing the respiratory motion of the target with or without contrast enhancement. Its application in clinical practice for simulation scan of patients with UC cancer is often reported in literature [27,31,35,36,40,45,51,56,57,58,59,60,66]. When this technology is not available, the tumor movement can be estimate performing two CT scans, one on inspiration and one on expiration phase [67]. Patients typically also undergo three-dimensional (3D) CT acquisition, which may involve the use of intravenous contrast injection [56,66].
The choice of slice thickness depends on the protocol used and the type of CT scanner available. Normally, the slice thickness ranges between 2 and 3 mm [27,36,59,66]. The acquisition protocol generally extends from the lower mandibular margin to the lower hepatic margin and includes both lungs [45,67].
Regarding the immobilization device, SBRT already deviates from conventional treatments in the simulation phase and requires specific immobilization devices that cover a large part of the patient body both above and below the tumor [68]. Patients commonly undergo CT simulation in the supine position with arms above the head using a wing board, a specific device for thoracic treatment, a vac-lok bag or, in some centers, thermoplastic body mask, and a knee and foot lock [69]. This setup optimizes reproducibility and minimizes motion or wobbling during radiotherapy. Despite the heterogeneity of different immobilization devices among centers, there is agreement in many studies regarding the use of vacuum cushions with other complementary devices in clinical practice for the treatment of UC pulmonary lesions [27,35,36,50,57,59,60,66]. Patients with upper mediastinal lymph nodes targeted were immobilized in an extended thermoplastic head and shoulder mask with their arms in down position along their body [57,60]. Active motion management techniques, such as breath hold techniques and abdominal compression, often are not used or described in most studies due to reduced motion of UC lesions and therefore not broadly recommended. Regarding the abdominal compression, this device is not used as an immobilization device in all studies and also not in all RT centers. For example, in the study by Lindberg et al. it is reported that only 4 out of 9 participating centers used this device [27]. Notably, abdominal compression is employed under specific conditions; for instance, Nguyen et al. used it to limit diaphragmatic excursion to ≤1 cm [36]. In addition, Regnery et al. used the device if the tumor was located in a lower lung lobe [35]. The study by Giuliani et al. highlighted the need for abdominal compression in tumors with more than 1 cm of motion [31]. It has also been used in other studies [50,60]. It is important to emphasize that the choice of immobilization device depends on the protocol, availability, and internal experience of each institution.
The use of deep inspiration breath hold is rare for UC lung lesions. In fact, Zhao et al. reported that this technique was systematically not used [40], and Breen et al. noted that it was employed in only 10% of cases [59]. Mihai et al.'s study highlighted the use of the breath hold technique only when tumor motion exceeded 5 mm in any direction [57].
Based on the included studies, Figure 2 summarizes the modalities of CT planning acquisition and the immobilization devices used in patients with UC lung tumors.
4.3. Treatment Volume
From the analysis of the included articles, it emerges that the methodology used for delineation of treatment volumes is heterogeneous. Starting with the Gross Tumor Volume (GTV), it is evident that this can be delineated on the 3DCT acquired using a lung window [39,66] and with the aid of co-registered images obtained from contrast-enhanced CT and PET-CT scans [58]. Alternatively, GTV can be defined using 4D CT images by outlining it on both inspiratory and expiratory scans [31,60], in the end-expiration phase [57] or by delineating it using the average phase of the 4D CT [40]. In patients treated with breath-hold techniques, GTV is contoured on CT scans acquired during the breath-hold phase [57].
Most of the included studies agree on the definition of an Interal Target Volume (ITV) and describe its creation by expanding the GTV contour to encompass tumor shifts across all respiratory phases of the 4D CT linked with the breathing cycle (35, 39, 40, 45, 57, 58, 60, 66], therefore the 4D CT scan plays a crucial role in defining tumor motion and allows delineation of the ITV contour during all phases of respiration [70]. In lung SBRT practice, it is not common to add a margin from the GTV to the Clinical Target Volume (CTV) [57,59,63,65]. However, in some studies, a CTV is defined by adding a 2-5 mm margin to the GTV-ITV [35,71].
Finally, to create the planning target volume (PTV), a margin was added to the ITV to account for set-up uncertainties. The isotropic growth to create the PTV was generally around 5 mm [18,31,39,40,45,56,58,59,60,66]. Sometimes the isotropic margin added from the ITV to the PTV was reduced up to 3 mm [51,57,66], or the longitudinal (cranio-caudal) margin was increased [58]. In many centers that participated in the Lindberg et al. study, the margin was widened up to 10 mm [27]. In the breath-hold technique, the GTV was defined on the CT images acquired in breath-hold, the creation of the ITV was not mandatory and the PTV was created by adding an isotropic margin of 5 mm to the GTV [57,63].
4.4. Treatment Dose and Fractionation
An overview of the treatment dose and fractionation used in each study included is reported in Table 1. While older retrospective data may vary in terms of fractionation and doses, the most recent retrospective series and prospective data aimed to assess the feasibility of 60 Gy in 8 fractions, with alternate results, but most recently reassuring data. Overall data shows that when adequately selected and planned, this fractionation regimen seems to provide high local control rates with acceptable toxicity profile [31,34,40,45]. High caution and probably a dose de-escalation should be used when treating tumors with endobronchial invasion or abutting PTB or esophagus, combined with a careful long-term follow-up and benefit/risk evaluation for later thoracic invasive procedures (ie bronchoscopy) [30,37,47]. Moreover, it seems that limiting PTV Dmax ≤110-120% helps in lowering the toxicity rates [31,41,42].
4.5. Setup and Motion Management Systems
A comprehensive image guidance and motion management strategy needs to be applied and maintained with sufficient technology and procedures to ensure safe and effective positioning and mitigate motion-related errors [72]. Depending on the equipment used in clinical practice, various technologies can be employed to assess patient positioning and verify tumor motion during treatment. Based on the study by Caillet et al. [69], it is possible to recognize the Image Guided RT (IGRT) strategies and motion management systems employed in room but prior to the treatment delivery and those that are used during the treatment.
According to most studies, prior to treatment, daily imaging verification is performed to assess patient positioning and correct any potential setup errors [31,40,45,51,57,59,60,66,73]. In recent years, studies have highlighted the adoption of kV Cone Beam Computed Tomography (kV-CBCT) as a key modality for IGRT acquisition with online correction performed by multidisciplinary team [31,40,45,51,57,59,60,66,73]. In particular, the use of 3D-IGRT modalities, such as kV-CBCT, is preferable to 2D techniques like Electronic Portal Imaging Devices or kV Orthogonal Imaging offers a more comprehensive evaluation of patient deformation, rotation, showing the internal anatomy of the patient and providing higher contrast visibility of soft tissues [69,74,75]. The main limitation of 3D kV-CBCT for lung imaging is that it averages projections from different respiratory phases to produce a single 3D scan, which can lead to blurred areas and provide incorrect information about the actual tumor amplitude and its relative position during the respiratory phases [69,76,77]. The 4D CBCT provides daily motion data resulting in precise information about the tumor’s trajectory on that day. This helps to maintain tighter margins around the target and reduces inter-observer variability in patient positioning [69,78].
In addition, for optimal alignment correction, it is important to use a six-degree-of-freedom robotic couch, which makes it possible to correct not only translation but also rotational displacements, which are assessed during IGRT to account for the patient's internal movement and rotation, as in the study by Shahi et al. [60,69,79]. Additionally, patient positioning can be evaluated using an optical system that registers and correlates the patient's surface. In recent years, multiple optical systems have become commercially available, and these devices are increasingly being used for interfraction setup in SBRT lung tumor treatments [69,80,81]. Moreover, the major advantage of the use of optical systems is the control and detection of the intrafraction patient motion during treatment delivery, without the use of ionizing radiation or invasive procedures [80,82]. In addition, the optical system can automatically interrupt the beam, interfacing with the linear accelerator, if the patient moves beyond a predefined tolerance threshold [83]. In SBRT performed with the DIBH technique, the optical system is used to guide patients in performing deep voluntary inspirations with reproducibility and to provide visual feedback to ensure accuracy [84]. Breathing control methods also include immobilization devices, as previously mentioned, as well as those that use abdominal compression. These devices mechanically limit abdominal motion during respiration and can be applied in various ways [69].
In the study by Guillaume et al., Cyberknife is used in high percentage for the treatment of UC lung tumors [56]. The real-time tumor tracking by the placement of markers in or near the tumor is often adopted to treat patients with the Cyberknife system [83]. The markers can be placed by different approach depending on the risk of complication such as pneumothorax: via the percutaneous, intra- or extra-pulmonary, or via the vascular approach [86,87]. Percutaneous marker placement typically relied on fluoroscopy or CT-guidance to position platinum markers either within or near the tumor (intrapulmonary technique) or on the thoracic wall adjacent to the ribs (extrapulmonary technique). The vascular method entailed deploying embolization coils into small subsegmental branches of the pulmonary artery near the tumor via a catheter in order to reduce the risk of complications related to the insertion procedure, particularly pneumothorax [87]. Commonly, at least three markers are inserted to correct for translational and rotational target motions. The motion of implanted markers is usually detected through a series of orthogonal X-ray images performed during breathing in order to build a respiratory model correlated with external positional information extrapolated from infrared detectors [85].
4.6. Follow-Up
The follow-up protocols of the various studies on UC lung SBRT show some similarities, particularly with regard to timing, imaging methods and toxicity assessment. In most studies, clinical follow-up and imaging examinations were performed every 3 months, especially in the first year after treatment [18,27,31,36,45,50,56,57,58,66,73]. For the second year, follow-up examinations were usually scheduled every 3 to 6 months, followed by semi-annual or annual check-ups in the subsequent period [18,27,31,35,36,40,45,56,57,58,60,66].
In terms of imaging modality, CT scans of the chest with or without contrast were found to be the main imaging modality used to monitor disease progression and response to treatment [27,31,35,40,45,51,56,59]. In addition to chest imaging, some studies included broader imaging protocols, such as CT scans of the abdomen and pelvis or brain imaging with CT or magnetic resonance imaging (MRI) to assess possible distant metastasis [45,56,57].
Almost all studies included additional imaging such as PET-CT in the follow-up protocol if CT findings were indeterminate or suggestive of progression [18,27,31,35,40,45,50,56,57,58,59,66,73]. The use of the Response Evaluation Criteria in Solid Tumors (RECIST) version 1.0/1.1 to evaluate tumor response was consistent across several studies [18,27,31,35,39,40,45,56,60,73].
Toxicity was graded according to the Common Terminology Criteria for Adverse Events (CTCAE) version 4.0 / 4.03 [18,27,31,36,39,45,58,66,73] or 5.0 grading system [35,40,51,59,60]. In addition to radiological examinations and physical examinations, electrocardiography and pulmonary function tests can also be carried out during follow-up care [18,27,31,35].
5. Conclusions
To the best of our knowledge, this is the first overview about the treatment workflow of patients treated with SBRT for UC lung tumors. By providing a critical review of dedicated literature and a “roadmap” on the general and technical requirements for prescription, motion management, patient selection and dosimetric constraints, it could contribute to SBRT being administered safely and effectively for UC lung tumors among centers with different expertise. The role of SBRT in this setting is still an unanswered question. Indeed, the literature is still sparse, contradictory, and mostly based on retrospective data. Further prospective and randomized studies are awaited in order to provide high quality data and strong evidence on the optimal SBRT technique, schedule and dosimetry constraints.
Author Contributions
Conceptualization, V.Sa., A.L.; Methodology V.Sa., M.B., M.L.; Validation M.G.C., P.G., E.O.; Formal Analysis G.S., G.F., P.B.; Data Curation R.R., Y.W., D.G.; Drafting – Original draft preparation V.Sa., A.L., M.B.; Drafting – review and editing V.Sa, V.Sc., I.D., L.L.; Visualization A.L., M.B.; Supervision L.L.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- >Lagerwaard, F. J.; Haasbeek, C. J.; Smit, E. F.; Slotman, B. J.; Senan, S. Outcomes of risk-adapted fractionated stereotactic radiotherapy for stage I non-small-cell lung cancer. Int J Radiat Oncol Biol Phys 2008, 70 (3), 685-692. [CrossRef]
- Timmerman, R.; Paulus, R.; Galvin, J.; Michalski, J.; Straube, W.; Bradley, J.; Fakiris, A.; Bezjak, A.; Videtic, G.; Johnstone, D.; et al. Stereotactic body radiation therapy for inoperable early stage lung cancer. JAMA 2010, 303 (11), 1070-1076. [CrossRef]
- Chang, J. Y.; Liu, H.; Balter, P.; Komaki, R.; Liao, Z.; Welsh, J.; Mehran, R. J.; Roth, J. A.; Swisher, S. G. Clinical outcome and predictors of survival and pneumonitis after stereotactic ablative radiotherapy for stage I non-small cell lung cancer. Radiat Oncol 2012, 7, 152. [CrossRef]
- Taremi, M.; Hope, A.; Dahele, M.; Pearson, S.; Fung, S.; Purdie, T.; Brade, A.; Cho, J.; Sun, A.; Bissonnette, J. P.; et al. Stereotactic body radiotherapy for medically inoperable lung cancer: prospective, single-center study of 108 consecutive patients. Int J Radiat Oncol Biol Phys 2012, 82 (2), 967-973. [CrossRef]
- Videtic, G. M. M.; Donington, J.; Giuliani, M.; Heinzerling, J.; Karas, T. Z.; Kelsey, C. R.; Lally, B. E.; Latzka, K.; Lo, S. S.; Moghanaki, D.; et al. Stereotactic body radiation therapy for early-stage non-small cell lung cancer: Executive Summary of an ASTRO Evidence-Based Guideline. Pract Radiat Oncol 2017, 7 (5), 295-301. [CrossRef]
- Guckenberger, M.; Andratschke, N.; Dieckmann, K.; Hoogeman, M. S.; Hoyer, M.; Hurkmans, C.; Tanadini-Lang, S.; Lartigau, E.; Méndez Romero, A.; Senan, S.; et al. ESTRO ACROP consensus guideline on implementation and practice of stereotactic body radiotherapy for peripherally located early stage non-small cell lung cancer. Radiother Oncol 2017, 124 (1), 11-17. [CrossRef]
- Shirvani, S. M.; Jiang, J.; Chang, J. Y.; Welsh, J. W.; Gomez, D. R.; Swisher, S.; Buchholz, T. A.; Smith, B. D. Comparative effectiveness of 5 treatment strategies for early-stage non-small cell lung cancer in the elderly. Int J Radiat Oncol Biol Phys 2012, 84 (5), 1060-1070. [CrossRef]
- Rusthoven, K. E.; Kavanagh, B. D.; Burri, S. H.; Chen, C.; Cardenes, H.; Chidel, M. A.; Pugh, T. J.; Kane, M.; Gaspar, L. E.; Schefter, T. E. Multi-institutional phase I/II trial of stereotactic body radiation therapy for lung metastases. J Clin Oncol 2009, 27 (10), 1579-1584. [CrossRef]
- Chang, H. J.; Ko, H. L.; Lee, C. Y.; Wu, R. H.; Yeh, Y. W.; Jiang, J. S.; Kao, S. J.; Chi, K. H. Hypofractionated radiotherapy for primary or secondary oligometastatic lung cancer using Tomotherapy. Radiat Oncol 2012, 7, 222. [CrossRef]
- Tateishi, Y.; Takeda, A.; Horita, N.; Tsurugai, Y.; Eriguchi, T.; Kibe, Y.; Sanuki, N.; Kaneko, T. Stereotactic Body Radiation Therapy With a High Maximum Dose Improves Local Control, Cancer-Specific Death, and Overall Survival in Peripheral Early-Stage Non-Small Cell Lung Cancer. Int J Radiat Oncol Biol Phys 2021, 111 (1), 143-151. [CrossRef]
- Timmerman, R.; McGarry, R.; Yiannoutsos, C.; Papiez, L.; Tudor, K.; DeLuca, J.; Ewing, M.; Abdulrahman, R.; DesRosiers, C.; Williams, M.; et al. Excessive toxicity when treating central tumors in a phase II study of stereotactic body radiation therapy for medically inoperable early-stage lung cancer. J Clin Oncol 2006, 24 (30), 4833-4839. [CrossRef]
- Milano, M. T.; Chen, Y.; Katz, A. W.; Philip, A.; Schell, M. C.; Okunieff, P. Central thoracic lesions treated with hypofractionated stereotactic body radiotherapy. Radiother Oncol 2009, 91 (3), 301-306. [CrossRef]
- Chang, J. Y.; Balter, P. A.; Dong, L.; Yang, Q.; Liao, Z.; Jeter, M.; Bucci, M. K.; McAleer, M. F.; Mehran, R. J.; Roth, J. A.; et al. Stereotactic body radiation therapy in centrally and superiorly located stage I or isolated recurrent non-small-cell lung cancer. Int J Radiat Oncol Biol Phys 2008, 72 (4), 967-971. [CrossRef]
- Haasbeek, C. J.; Lagerwaard, F. J.; Slotman, B. J.; Senan, S. Outcomes of stereotactic ablative radiotherapy for centrally located early-stage lung cancer. J Thorac Oncol 2011, 6 (12), 2036-2043. [CrossRef]
- Rowe, B. P.; Boffa, D. J.; Wilson, L. D.; Kim, A. W.; Detterbeck, F. C.; Decker, R. H. Stereotactic body radiotherapy for central lung tumors. J Thorac Oncol 2012, 7 (9), 1394-1399. [CrossRef]
- Nuyttens, J. J.; van der Voort van Zyp, N. C.; Praag, J.; Aluwini, S.; van Klaveren, R. J.; Verhoef, C.; Pattynama, P. M.; Hoogeman, M. S. Outcome of four-dimensional stereotactic radiotherapy for centrally located lung tumors. Radiother Oncol 2012, 102 (3), 383-387. [CrossRef]
- Corradetti, M. N.; Haas, A. R.; Rengan, R. Central-airway necrosis after stereotactic body-radiation therapy. N Engl J Med 2012, 366 (24), 2327-2329. [CrossRef]
- Bezjak, A.; Paulus, R.; Gaspar, L. E.; Timmerman, R. D.; Straube, W. L.; Ryan, W. F.; Garces, Y. I.; Pu, A. T.; Singh, A. K.; Videtic, G. M.; et al. Safety and Efficacy of a Five-Fraction Stereotactic Body Radiotherapy Schedule for Centrally Located Non-Small-Cell Lung Cancer: NRG Oncology/RTOG 0813 Trial. J Clin Oncol 2019, 37 (15), 1316-1325. [CrossRef]
- Yan, M.; Louie, A. V.; Kotecha, R.; Ashfaq Ahmed, M.; Zhang, Z.; Guckenberger, M.; Kim, M. S.; Lo, S. S.; Scorsetti, M.; Tree, A. C.; et al. Stereotactic body radiotherapy for Ultra-Central lung Tumors: A systematic review and Meta-Analysis and International Stereotactic Radiosurgery Society practice guidelines. Lung Cancer 2023, 182, 107281. [CrossRef]
- Tekatli, H.; Haasbeek, N.; Dahele, M.; De Haan, P.; Verbakel, W.; Bongers, E.; Hashemi, S.; Nossent, E.; Spoelstra, F.; de Langen, A. J.; et al. Outcomes of Hypofractionated High-Dose Radiotherapy in Poor-Risk Patients with "Ultracentral" Non-Small Cell Lung Cancer. J Thorac Oncol 2016, 11 (7), 1081-1089. [CrossRef]
- Song, S. Y.; Choi, W.; Shin, S. S.; Lee, S. W.; Ahn, S. D.; Kim, J. H.; Je, H. U.; Park, C. I.; Lee, J. S.; Choi, E. K. Fractionated stereotactic body radiation therapy for medically inoperable stage I lung cancer adjacent to central large bronchus. Lung Cancer 2009, 66 (1), 89-93. [CrossRef]
- Haseltine, J. M.; Rimner, A.; Gelblum, D. Y.; Modh, A.; Rosenzweig, K. E.; Jackson, A.; Yorke, E. D.; Wu, A. J. Fatal complications after stereotactic body radiation therapy for central lung tumors abutting the proximal bronchial tree. Pract Radiat Oncol 2016, 6 (2), e27-33. [CrossRef]
- Wang, C.; Rimner, A.; Gelblum, D. Y.; Dick-Godfrey, R.; McKnight, D.; Torres, D.; Flynn, J.; Zhang, Z.; Sidiqi, B.; Jackson, A.; et al. Analysis of pneumonitis and esophageal injury after stereotactic body radiation therapy for ultra-central lung tumors. Lung Cancer 2020, 147, 45-48. [CrossRef]
- Chaudhuri, A. A.; Tang, C.; Binkley, M. S.; Jin, M.; Wynne, J. F.; von Eyben, R.; Hara, W. Y.; Trakul, N.; Loo, B. W.; Diehn, M. Stereotactic ablative radiotherapy (SABR) for treatment of central and ultra-central lung tumors. Lung Cancer 2015, 89 (1), 50-56. [CrossRef]
- Daly, M.; Novak, J.; Monjazeb, A. P2.05-056 Safety of Stereotactic Body Radiotherapy for Central, Ultracentral, and Paramediastinal Lung Tumors. Journal of Thoracic Oncology 2017, 12, S1066. [CrossRef]
- Raman, S.; Yau, V.; Pineda, S.; Le, L. W.; Lau, A.; Bezjak, A.; Cho, B. C. J.; Sun, A.; Hope, A. J.; Giuliani, M. Ultracentral Tumors Treated With Stereotactic Body Radiotherapy: Single-Institution Experience. Clin Lung Cancer 2018, 19 (5), e803-e810. [CrossRef]
- Lindberg, K.; Grozman, V.; Karlsson, K.; Lindberg, S.; Lax, I.; Wersäll, P.; Persson, G. F.; Josipovic, M.; Khalil, A. A.; Moeller, D. S.; et al. The HILUS-Trial-a Prospective Nordic Multicenter Phase 2 Study of Ultracentral Lung Tumors Treated With Stereotactic Body Radiotherapy. J Thorac Oncol 2021, 16 (7), 1200-1210. [CrossRef]
- Chen, H.; Laba, J. M.; Zayed, S.; Boldt, R. G.; Palma, D. A.; Louie, A. V. Safety and Effectiveness of Stereotactic Ablative Radiotherapy for Ultra-Central Lung Lesions: A Systematic Review. J Thorac Oncol 2019, 14 (8), 1332-1342. [CrossRef]
- Lindberg, S.; Grozman, V.; Karlsson, K.; Onjukka, E.; Lindbäck, E.; Jirf, K. A.; Lax, I.; Wersäll, P.; Persson, G. F.; Josipovic, M.; et al. Expanded HILUS Trial: A Pooled Analysis of Risk Factors for Toxicity From Stereotactic Body Radiation Therapy of Central and Ultracentral Lung Tumors. Int J Radiat Oncol Biol Phys 2023, 117 (5), 1222-1231. [CrossRef]
- Levy, A.; Adebahr, S.; Hurkmans, C.; Ahmed, M.; Ahmad, S.; Guckenberger, M.; Geets, X.; Lievens, Y.; Lambrecht, M.; Pourel, N.; et al. Stereotactic Body Radiotherapy for Centrally Located Inoperable Early-Stage NSCLC: EORTC 22113-08113 LungTech Phase II Trial Results. J Thorac Oncol 2024, 19 (9), 1297-1309. [CrossRef]
- Giuliani, M. E.; Filion, E.; Faria, S.; Kundapur, V.; Toni Vu, T. T. T.; Lok, B. H.; Raman, S.; Bahig, H.; Laba, J. M.; Lang, P.; et al. Stereotactic Radiation for Ultra-Central Non-Small Cell Lung Cancer: A Safety and Efficacy Trial (SUNSET). Int J Radiat Oncol Biol Phys 2024, 120 (3), 669-677. [CrossRef]
- Swaminath, A.; Parpia, S.; Wierzbicki, M.; Kundapur, V.; Faria, S.; Okawara, G. S.; Tsakiridis, T. K.; Ahmed, N.; Bujold, A.; Hirmiz, K.; et al. Stereotactic vs Hypofractionated Radiotherapy for Inoperable Stage I Non-Small Cell Lung Cancer: The LUSTRE Phase 3 Randomized Clinical Trial. JAMA Oncol 2024. [CrossRef]
- Tonneau, M.; Richard, C.; Routy, B.; Campeau, M. P.; Vu, T.; Filion, E.; Roberge, D.; Mathieu, D.; Doucet, R.; Beliveau-Nadeau, D.; et al. A competing risk analysis of the patterns and risk factors of recurrence in early-stage non-small cell lung cancer treated with stereotactic ablative radiotherapy. Radiother Oncol 2023, 185, 109697. [CrossRef]
- Meng, M. B.; Wang, H. H.; Zaorsky, N. G.; Sun, B. S.; Zhu, L.; Song, Y. C.; Li, F. T.; Dong, Y.; Wang, J. S.; Chen, H. M.; et al. Risk-adapted stereotactic body radiation therapy for central and ultra-central early-stage inoperable non-small cell lung cancer. Cancer Sci 2019, 110 (11), 3553-3564. [CrossRef]
- Regnery, S.; Eichkorn, T.; Weykamp, F.; Held, T.; Weusthof, K.; Dinges, L. A.; El-Shafie, R. A.; Winter, H.; Thomas, M.; Debus, J.; et al. Safety and Efficacy of Stereotactic Body Radiotherapy in Ultracentral Lung Tumors Using a Risk-optimized Fractionation Scheme. Clin Lung Cancer 2021, 22 (4), 332-340.e333. [CrossRef]
- Nguyen, K. N. B.; Hause, D. J.; Novak, J.; Monjazeb, A. M.; Daly, M. E. Tumor Control and Toxicity after SBRT for Ultracentral, Central, and Paramediastinal Lung Tumors. Pract Radiat Oncol 2019, 9 (2), e196-e202. [CrossRef]
- Sandoval, M. L.; Sim, A. J.; Bryant, J. M.; Bhandari, M.; Wuthrick, E. J.; Perez, B. A.; Dilling, T. J.; Redler, G.; Andreozzi, J.; Nardella, L.; et al. Magnetic Resonance-Guided Stereotactic Body Radiation Therapy/Hypofractionated Radiation therapy for Metastatic and Primary Central and Ultracentral Lung Lesions. JTO Clin Res Rep 2023, 4 (5), 100488. [CrossRef]
- Li, G. J.; Tan, H.; Nusrat, H.; Chang, J.; Chen, H.; Poon, I.; Shahi, J.; Tsao, M.; Ung, Y.; Cheung, P.; et al. Safety and Efficacy of Stereotactic Body Radiation Therapy for Ultra-central Thoracic Tumors: A Single Center Retrospective Review. Int J Radiat Oncol Biol Phys 2024, 120 (2), 359-369. [CrossRef]
- Loi, M.; Franceschini, D.; Dominici, L.; Franzese, C.; Chiola, I.; Comito, T.; Marzo, M.; Reggiori, G.; Mancosu, P.; Tomatis, S.; et al. Stereotactic Radiotherapy for Ultra-Central Lung Oligometastases in Non-Small-Cell Lung Cancer. Cancers (Basel) 2020, 12 (4). [CrossRef]
- Zhao, Y.; Khawandanh, E.; Thomas, S.; Zhang, S.; Dunne, E. M.; Liu, M.; Schellenberg, D. Outcomes of stereotactic body radiotherapy 60 Gy in 8 fractions when prioritizing organs at risk for central and ultracentral lung tumors. Radiat Oncol 2020, 15 (1), 61. [CrossRef]
- Rim, C. H.; Yoon, W. S.; Park, S. Safety and Efficacy of Moderate-Intensity Stereotactic Body Radiation Therapy for Ultra-Central Lung Tumor. Medicina (Kaunas) 2024, 60 (4). [CrossRef]
- Bryant, J. M.; Cruz-Chamorro, R. J.; Gan, A.; Liveringhouse, C.; Weygand, J.; Nguyen, A.; Keit, E.; Sandoval, M. L.; Sim, A. J.; Perez, B. A.; et al. Structure-specific rigid dose accumulation dosimetric analysis of ablative stereotactic MRI-guided adaptive radiation therapy in ultracentral lung lesions. Commun Med (Lond) 2024, 4 (1), 96. [CrossRef]
- Hiroshima, Y.; Tamaki, Y.; Sawada, T.; Ishida, T.; Yasue, K.; Shinoda, K.; Saito, T.; Kaburagi, T.; Kiyoshima, M.; Okumura, T.; et al. Stereotactic Body Radiotherapy for Stage I Lung Cancer With a New Real-time Tumor Tracking System. Anticancer Res 2022, 42 (6), 2989-2995. [CrossRef]
- Ligtenberg, H.; Hackett, S. L.; Merckel, L. G.; Snoeren, L.; Kontaxis, C.; Zachiu, C.; Bol, G. H.; Verhoeff, J. J. C.; Fast, M. F. Towards mid-position based Stereotactic Body Radiation Therapy using online magnetic resonance imaging guidance for central lung tumours. Phys Imaging Radiat Oncol 2022, 23, 24-31. [CrossRef]
- Yang, D.; Cui, J.; Zhao, J.; You, J.; Yu, R.; Yu, H.; Jiang, L.; Li, D.; Xu, B.; Shi, A. Stereotactic ablative radiotherapy of 60 Gy in eight fractions is safe for ultracentral non-small cell lung cancer. Thorac Cancer 2020, 11 (3), 754-761. [CrossRef]
- Song, X.; Zhao, L.; Jiang, N.; Ding, N.; Zong, D.; Zhang, N.; Wang, D.; Wen, J.; He, X.; Kong, C.; et al. Long-term outcomes in patients with central and ultracentral non-small cell lung cancer treated with stereotactic body radiotherapy: single-institution experience. Curr Probl Cancer 2023, 47 (3), 100956. [CrossRef]
- Regnery, S.; Katsigiannopulos, E.; Hoegen, P.; Weykamp, F.; Sandrini, E.; Held, T.; Deng, M.; Eichkorn, T.; Buchele, C.; Rippke, C.; et al. To fly or not to fly: Stereotactic MR-guided adaptive radiotherapy effectively treats ultracentral lung tumors with favorable long-term outcomes. Lung Cancer 2023, 179, 107175. [CrossRef]
- Salvestrini, V.; Duijm, M.; Loi, M.; Nuyttens, J. J. Survival and Prognostic Factors of Ultra-Central Tumors Treated with Stereotactic Body Radiotherapy. Cancers (Basel) 2022, 14 (23). [CrossRef]
- Tekatli, H.; Giraud, N.; van Eekelen, R.; Lagerwaard, F. J.; Senan, S. Ten years outcomes after SABR in central and ultracentral primary lung tumors. Radiother Oncol 2023, 188, 109848. [CrossRef]
- Farrugia, M.; Ma, S. J.; Hennon, M.; Nwogu, C.; Dexter, E.; Picone, A.; Demmy, T.; Yendamuri, S.; Yu, H.; Fung-Kee-Fung, S.; et al. Exceeding Radiation Dose to Volume Parameters for the Proximal Airways with Stereotactic Body Radiation Therapy Is More Likely for Ultracentral Lung Tumors and Associated with Worse Outcome. Cancers (Basel) 2021, 13 (14). [CrossRef]
- Lodeweges, J. E.; van Rossum, P. S. N.; Bartels, M. M. T. J.; van Lindert, A. S. R.; Pomp, J.; Peters, M.; Verhoeff, J. J. C. Ultra-central lung tumors: safety and efficacy of protracted stereotactic body radiotherapy. Acta Oncol 2021, 60 (8), 1061-1068. [CrossRef]
- Ahmadsei, M.; Thaler, K.; Gasser, E.; Pouymayou, B.; Dal Bello, R.; Christ, S. M.; Willmann, J.; Kovacs, B.; Balermpas, P.; Tanadini-Lang, S.; et al. Dosimetric analysis of 17 cardiac Sub-structures, Toxicity, and survival in ultra central lung tumor patients treated with SBRT. Clin Transl Radiat Oncol 2023, 43, 100675. [CrossRef]
- Farrugia, M.; Yu, H.; Ma, S. J.; Iovoli, A. J.; Pokharel, S.; Sharma, U. C.; Fung-Kee-Fung, S.; Malik, N.; Singh, A. K.; Malhotra, H. Right Atrial Dose Is Associated with Worse Outcome in Patients Undergoing Definitive Stereotactic Body Radiation Therapy for Central Lung Tumors. Cancers (Basel) 2022, 14 (6). [CrossRef]
- Lee, G.; Han, Z.; Huynh, E.; Tjong, M. C.; Cagney, D. N.; Huynh, M. A.; Kann, B. H.; Kozono, D.; Leeman, J. E.; Singer, L.; et al. Widening the therapeutic window for central and ultra-central thoracic oligometastatic disease with stereotactic MR-guided adaptive radiation therapy (SMART). Radiother Oncol 2024, 190, 110034. [CrossRef]
- Ricco, A.; Davis, J.; Rate, W.; Yang, J.; Perry, D.; Pablo, J.; D'Ambrosio, D.; Sharma, S.; Sundararaman, S.; Kolker, J.; et al. Lung metastases treated with stereotactic body radiotherapy: the RSSearch® patient Registry's experience. Radiat Oncol 2017, 12 (1), 35. [CrossRef]
- Guillaume, E.; Tanguy, R.; Ayadi, M.; Claude, L.; Sotton, S.; Moncharmont, C.; Magné, N.; Martel-Lafay, I. Toxicity and efficacy of stereotactic body radiotherapy for ultra-central lung tumours: a single institution real life experience. Br J Radiol 2022, 95 (1129), 20210533. [CrossRef]
- Mihai, A. M.; Armstrong, P. J.; Hickey, D.; Milano, M. T.; Dunne, M.; Healy, K.; Thirion, P.; Heron, D. E.; ElBeltagi, N.; Armstrong, J. G. Late Toxicity and Long-Term Local Control in Patients With Ultra-Central Lung Tumours Treated by Intensity-Modulated Radiotherapy-Based Stereotactic Ablative Body Radiotherapy With Homogenous Dose Prescription. Clin Oncol (R Coll Radiol) 2021, 33 (10), 627-637. [CrossRef]
- Duijm, M.; van der Voort van Zyp, N. C.; van de Vaart, P.; Oomen-de Hoop, E.; Mast, M. E.; Hoogeman, M. S.; Nuyttens, J. J. Predicting High-Grade Esophagus Toxicity After Treating Central Lung Tumors With Stereotactic Radiation Therapy Using a Normal Tissue Complication Probability Model. Int J Radiat Oncol Biol Phys 2020, 106 (1), 73-81. [CrossRef]
- Breen, W. G.; Jeans, E. B.; Gergelis, K. R.; Garces, Y. I.; Park, S. S.; Merrell, K. W.; Peikert, T. D.; Mansfield, A. S.; Wigle, D. A.; Harmsen, W. S.; et al. Ablative radiotherapy for ultracentral lung cancers: Dosimetric, geometric, and volumetric predictors of outcomes and toxicity. Radiother Oncol 2021, 158, 246-252. [CrossRef]
- Shahi, J.; Poon, I.; Ung, Y. C.; Tsao, M.; Bjarnason, G. A.; Malik, N. H.; Zhang, L.; Louie, A. V.; Cheung, P. Stereotactic Body Radiation Therapy for Mediastinal and Hilar Lymph Node Metastases. Int J Radiat Oncol Biol Phys 2021, 109 (3), 764-774. [CrossRef]
- Wegner, R. E.; Abel, S.; Hasan, S.; Schumacher, L. Y.; Colonias, A. Stereotactic Body Radiotherapy (SBRT) for Oligometastatic Lung Nodules: A Single Institution Series. Front Oncol 2019, 9, 334. [CrossRef]
- Postmus, P. E.; Kerr, K. M.; Oudkerk, M.; Senan, S.; Waller, D. A.; Vansteenkiste, J.; Escriu, C.; Peters, S.; Committee, E. G. Early and locally advanced non-small-cell lung cancer (NSCLC): ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol 2017, 28 (suppl_4), iv1-iv21. [CrossRef]
- Gutiérrez, E.; Sánchez, I.; Díaz, O.; Valles, A.; Balderrama, R.; Fuentes, J.; Lara, B.; Olimón, C.; Ruiz, V.; Rodríguez, J.; et al. Current Evidence for Stereotactic Body Radiotherapy in Lung Metastases. Curr Oncol 2021, 28 (4), 2560-2578. [CrossRef]
- Koba, A.; Hayashi, K.; Suzuki, O.; Kawaguchi, Y.; Ogawa, K.; Chatani, M. Stereotactic body radiotherapy feasibility for patients with peripheral stage I lung cancer and poor pulmonary function. Oncol Lett 2020, 19 (3), 2515-2521. [CrossRef]
- Dahele, M.; Pearson, S.; Purdie, T.; Bissonnette, J. P.; Franks, K.; Brade, A.; Cho, J.; Sun, A.; Hope, A.; Marshall, A.; et al. Practical considerations arising from the implementation of lung stereotactic body radiation therapy (SBRT) at a comprehensive cancer center. J Thorac Oncol 2008, 3 (11), 1332-1341. [CrossRef]
- Cooke, R.; Camilleri, P.; Chu, K. Y.; O'Cathail, S. M.; Robinson, M.; Van Den Heuvel, F.; Hawkins, M. A. Stereotactic body radiotherapy for moderately central and ultra-central oligometastatic disease: Initial outcomes. Tech Innov Patient Support Radiat Oncol 2020, 13, 24-30. [CrossRef]
- Kirkbride, P.; Cooper, T. Stereotactic body radiotherapy. Guidelines for commissioners, providers and clinicians: a national report. Clin Oncol (R Coll Radiol) 2011, 23 (3), 163-164. [CrossRef]
- Solberg, T. D.; Balter, J. M.; Benedict, S. H.; Fraass, B. A.; Kavanagh, B.; Miyamoto, C.; Pawlicki, T.; Potters, L.; Yamada, Y. Quality and safety considerations in stereotactic radiosurgery and stereotactic body radiation therapy: Executive summary. Pract Radiat Oncol 2012, 2 (1), 2-9. [CrossRef]
- Caillet, V.; Booth, J. T.; Keall, P. IGRT and motion management during lung SBRT delivery. Phys Med 2017, 44, 113-122. [CrossRef]
- Slotman, B. J.; Lagerwaard, F. J.; Senan, S. 4D imaging for target definition in stereotactic radiotherapy for lung cancer. Acta Oncol 2006, 45 (7), 966-972. [CrossRef]
- Grills, I. S.; Hugo, G.; Kestin, L. L.; Galerani, A. P.; Chao, K. K.; Wloch, J.; Yan, D. Image-guided radiotherapy via daily online cone-beam CT substantially reduces margin requirements for stereotactic lung radiotherapy. Int J Radiat Oncol Biol Phys 2008, 70 (4), 1045-1056. [CrossRef]
- Keall, P. J.; Mageras, G. S.; Balter, J. M.; Emery, R. S.; Forster, K. M.; Jiang, S. B.; Kapatoes, J. M.; Low, D. A.; Murphy, M. J.; Murray, B. R.; et al. The management of respiratory motion in radiation oncology report of AAPM Task Group 76. Med Phys 2006, 33 (10), 3874-3900. [CrossRef]
- Loi, M.; Franceschini, D.; Dominici, L.; Chiola, I.; Franzese, C.; D'Agostino, G. R.; Navarria, P.; Marzo, M.; Paganini, L.; Comito, T.; et al. Dose coverage impacts local control in ultra-central lung oligometastases treated with stereotactic radiotherapy. Strahlenther Onkol 2021, 197 (5), 396-404. [CrossRef]
- Bujold, A.; Craig, T.; Jaffray, D.; Dawson, L. A. Image-guided radiotherapy: has it influenced patient outcomes? Semin Radiat Oncol 2012, 22 (1), 50-61. [CrossRef]
- Jaffray, D. A.; Drake, D. G.; Moreau, M.; Martinez, A. A.; Wong, J. W. A radiographic and tomographic imaging system integrated into a medical linear accelerator for localization of bone and soft-tissue targets. Int J Radiat Oncol Biol Phys 1999, 45 (3), 773-789. [CrossRef]
- Shah, C.; Grills, I. S.; Kestin, L. L.; McGrath, S.; Ye, H.; Martin, S. K.; Yan, D. Intrafraction variation of mean tumor position during image-guided hypofractionated stereotactic body radiotherapy for lung cancer. Int J Radiat Oncol Biol Phys 2012, 82 (5), 1636-1641. [CrossRef]
- Schulze, R.; Heil, U.; Gross, D.; Bruellmann, D. D.; Dranischnikow, E.; Schwanecke, U.; Schoemer, E. Artefacts in CBCT: a review. Dentomaxillofac Radiol 2011, 40 (5), 265-273. [CrossRef]
- Sweeney, R. A.; Seubert, B.; Stark, S.; Homann, V.; Müller, G.; Flentje, M.; Guckenberger, M. Accuracy and inter-observer variability of 3D versus 4D cone-beam CT based image-guidance in SBRT for lung tumors. Radiat Oncol 2012, 7, 81. [CrossRef]
- Fu, C.; Ma, C.; Shang, D.; Qiu, Q.; Meng, H.; Duan, J.; Yin, Y. Geometric accuracy evaluation of a six-degree-of-freedom (6-DoF) couch with cone beam computed tomography (CBCT) using a phantom and correlation study of the position errors in pelvic tumor radiotherapy. Transl Cancer Res 2020, 9 (10), 6005-6012. [CrossRef]
- Guo, H. L.; Wu, W. W.; Huan, Y.; Zhang, H. W. SGRT-based stereotactic body radiotherapy for lung cancer setup accuracy and margin of the PTV. J Appl Clin Med Phys 2024, 25 (3), e14195. [CrossRef]
- Sarudis, S.; Karlsson, A.; Bäck, A. Surface guided frameless positioning for lung stereotactic body radiation therapy. J Appl Clin Med Phys 2021, 22 (9), 215-226. [CrossRef]
- Heinzerling, J. H.; Hampton, C. J.; Robinson, M.; Bright, M.; Moeller, B. J.; Ruiz, J.; Prabhu, R.; Burri, S. H.; Foster, R. D. Use of surface-guided radiation therapy in combination with IGRT for setup and intrafraction motion monitoring during stereotactic body radiation therapy treatments of the lung and abdomen. J Appl Clin Med Phys 2020, 21 (5), 48-55. [CrossRef]
- Foster, R. D.; Moeller, B. J.; Robinson, M.; Bright, M.; Ruiz, J. L.; Hampton, C. J.; Heinzerling, J. H. Dosimetric Analysis of Intra-Fraction Motion Detected by Surface-Guided Radiation Therapy During Linac Stereotactic Radiosurgery. Adv Radiat Oncol 2023, 8 (3), 101151. [CrossRef]
- Nguyen, D.; Reinoso, R.; Farah, J.; Yossi, S.; Lorchel, F.; Passerat, V.; Louet, E.; Pouchard, I.; Khodri, M.; Barbet, N. Reproducibility of surface-based deep inspiration breath-hold technique for lung stereotactic body radiotherapy on a closed-bore gantry linac. Phys Imaging Radiat Oncol 2023, 26, 100448. [CrossRef]
- van der Voort van Zyp, N. C.; Prévost, J. B.; Hoogeman, M. S.; Praag, J.; van der Holt, B.; Levendag, P. C.; van Klaveren, R. J.; Pattynama, P.; Nuyttens, J. J. Stereotactic radiotherapy with real-time tumor tracking for non-small cell lung cancer: clinical outcome. Radiother Oncol 2009, 91 (3), 296-300. [CrossRef]
- Nuyttens, J. J.; Prévost, J. B.; Praag, J.; Hoogeman, M.; Van Klaveren, R. J.; Levendag, P. C.; Pattynama, P. M. Lung tumor tracking during stereotactic radiotherapy treatment with the CyberKnife: Marker placement and early results. Acta Oncol 2006, 45 (7), 961-965. [CrossRef]
- Prévost, J. B.; Nuyttens, J. J.; Hoogeman, M. S.; Pöll, J. J.; van Dijk, L. C.; Pattynama, P. M. Endovascular coils as lung tumour markers in real-time tumour tracking stereotactic radiotherapy: preliminary results. Eur Radiol 2008, 18 (8), 1569-1576. [CrossRef]
- Iovoli, A. J.; Yu, H.; Advani, P. G.; Turecki, L.; Malhotra, H. K.; Malik, N. K.; Fung-Kee-Fung, S.; Singh, A. K.; Farrugia, M. K. Sinoatrial Node Dose Is Associated With Worse Survival in Patients Undergoing Definitive Stereotactic Body Radiation Therapy for Central Lung Cancers. Pract Radiat Oncol 2024, 14 (1), e40-e47. [CrossRef]
- Rock, C.; Sood, S.; Cao, Y.; Shelton, S.; Chen, R. C.; Wang, F. Ten fraction hypofractionated stereotactic body radiotherapy for the management of ultracentral lung tumors: a retrospective analysis of dosimetry, outcomes, and toxicity. Radiat Oncol 2023, 18 (1), 128. [CrossRef]
- Wang, B.; Dong, Y.; Yu, X.; Li, F.; Wang, J.; Chen, H.; Niu, Z.; Song, Y.; Yuan, Z.; Tao, Z. Safety and Efficacy of Stereotactic Ablative Radiotherapy for Ultra-Central Lung Cancer. Front Oncol 2022, 12, 868844. [CrossRef]
- Cong, Y.; Sun, B.; Wang, J.; Meng, X.; Xuan, L.; Zhang, J.; Liu, J.; Shen, G.; Wu, S. Outcomes and toxicity of stereotactic body radiation therapy for advanced stage ultra-central non-small cell lung cancer. Thorac Cancer 2019, 10 (7), 1567-1575. [CrossRef]
Figure 1.
Treatment workflow of patients with Ultra-central lung Tumor.
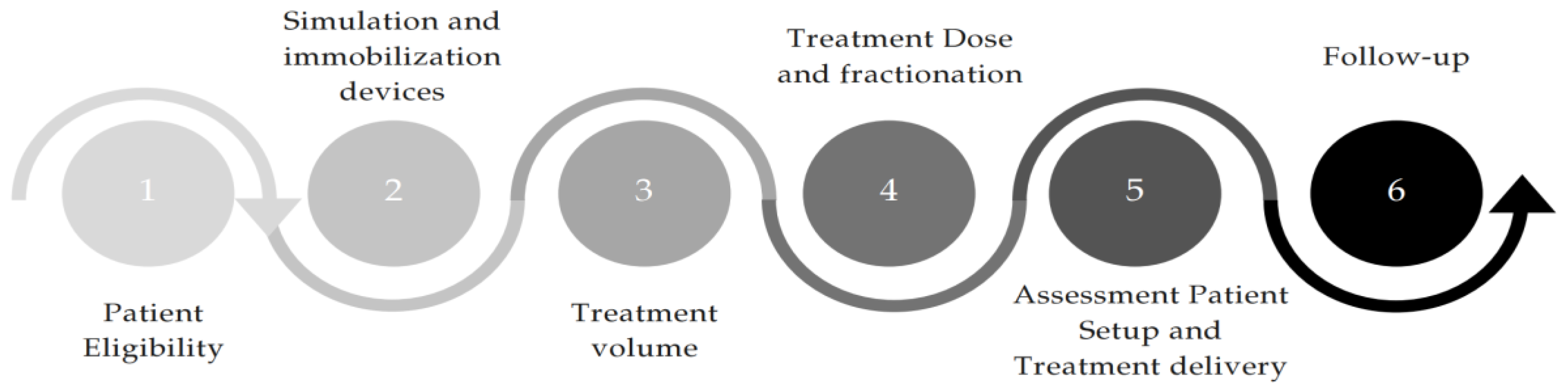
Figure 2.
The simulation phase for SBRT planning of Ultra-central Lung tumors.
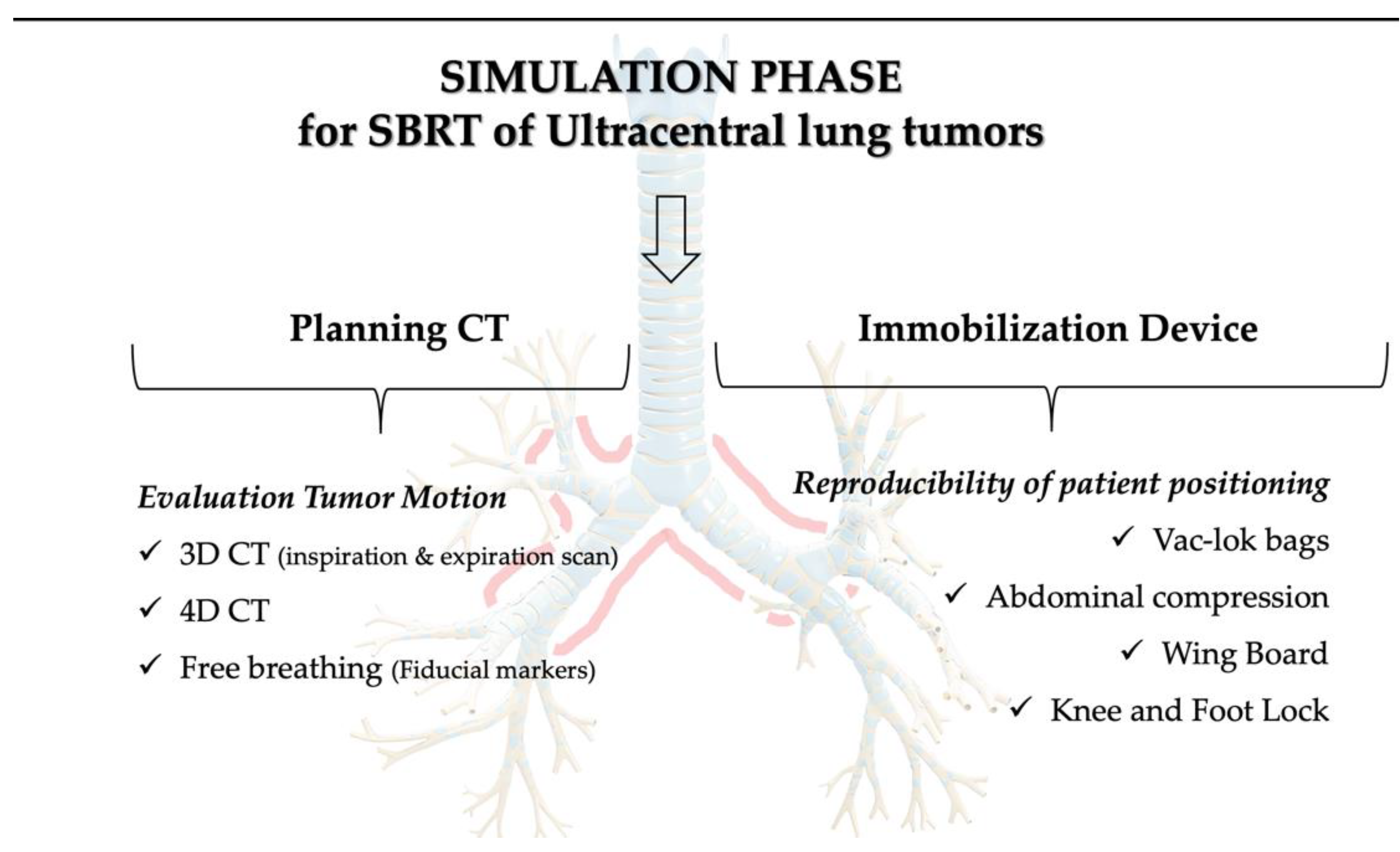
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



